Hepatitis E Epidemie in NL - Virology...
32
Joost PH Drenth Department of Gastroenterology and Hepatology, Radboudumc Nijmegen, The Netherlands 28 november 2018 Epidemie in NL Hepatitis E
Transcript of Hepatitis E Epidemie in NL - Virology...

Joost PH Drenth
Department of Gastroenterology and Hepatology, RadboudumcNijmegen, The Netherlands28 november 2018
Epidemie in NL
Hepatitis E

Disclosure of Conflicts of Interest
• I herewith declare the following paid or unpaid consultancies, businessinterests or sources of honoraria payments since October 1, 2016, andanything else which could potentially be viewed as a conflict of interest:
• Joost PH Drenth has served on advisory boards of AbbVie, Gilead, andIntercept, His Department receives research funding from Gilead, Abbvie,and Ipsen. All reimbursements go to the Radboudumc

Case
• 70-year old male
• No relevant medical history• Presentation with jaundice & pruritis• Laboratory
• At presentation bilirubine total 309 umol/l, AP 170U/l, gGT 47U/l, ASAT 93U/l, en ALAT 97 U/L

Liver biopsy
Disturbed architecture of the liver parenchyma apoptic hepatocytes, extensive
cholestasis and infiltration of the portal fields with a mixed cell infiltrate consisting of
eosinophils, lymphocytes and neutrophils

Diagnosis of (viral) hepatitis
• Clinical presentation
• Biochemical markers• Serology: auto-antibodies • Detection of viral material
• Indirect: Serology• Direct : Detection of virus particles
• In this case• HEV serology positive (IgM as well as IgG)
• Diagnosis hepatitis E

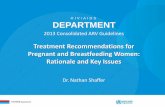
Hepatitis E identified in various hosts
Debing Y, et al. J Hepatol 2016;65:200–12

Hepatitis E virus, genotype 3• Cause:
• Food‐borne zoonosis• Genotype 3 host species: pigs, deer, rabbits, mongoose, sheep and
horses
• Transmission• Contaminated food products (eg, pork)• Blood products
• Solid organ transplantation• Presentation
• Immunocompetent: Acute hepatitis
• Immunosuppressed: Chronic hepatitis
Aliment Pharmacol Ther. 2017;46:126 141.

Hepatitis E source• Consumption of undercooked meat from pigs, wild boar, and deer
• 3 min @ 70 C for decontamination • Risk of patient-to-patient transmission is poorly defined
• Sexual transmission has been described in MSM
• Stool contains high amounts of infectious HEV particles• A vaccine has been developed but is only licensed in China
• Hepatitis E-virus in the Netherlands• 69/70 varkensbedrijven serologisch HEV positief • Onderzoek Sanquin
• Varkensvleesproducten HEV PCR positief • 43 / 55 (78%) leverworsten • 12 / 15 (80%), Varkens paté monsters
• Onderzoek NVWA • 48 / 58 (83%) leverworsten
https://www.veearts.nl/2017/hev-vrij-varkensvlees-is-voorlopig-een-utopie/http://rivm-lci.m13.mailplus.nl/genericservice/code/servlet/React?encId=9vRn24CiVmfDuRp&actId=507413&command=openhtml

Acute hepatitis E
• Acute HEV GT 3 infection is clinically silent in most patients
• <5% may develop symptoms of acute hepatitis• Elevated liver enzymes, jaundice and non-specific symptoms
• Immunocompetent patients clear the infection spontaneously
• Progression to ALF is rare with HEV GT 3• ACLF occurs occasionally
• Non-sterilizing immunity develops after infection has cleared
• Re-infection possible, but with lower risk of symptomatic hepatitis
• Extrahepatic manifestations
• Neurological • Neuralgic amyotrophy; Guillain–Barré syndrome; Meningoencephalitis;
Mononeuritis multiplex; Myositis• Renal
• Membranoproliferative and membranous glomerulonephritis; IgA
nephropathy
EASL CPG HEV. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.005 [
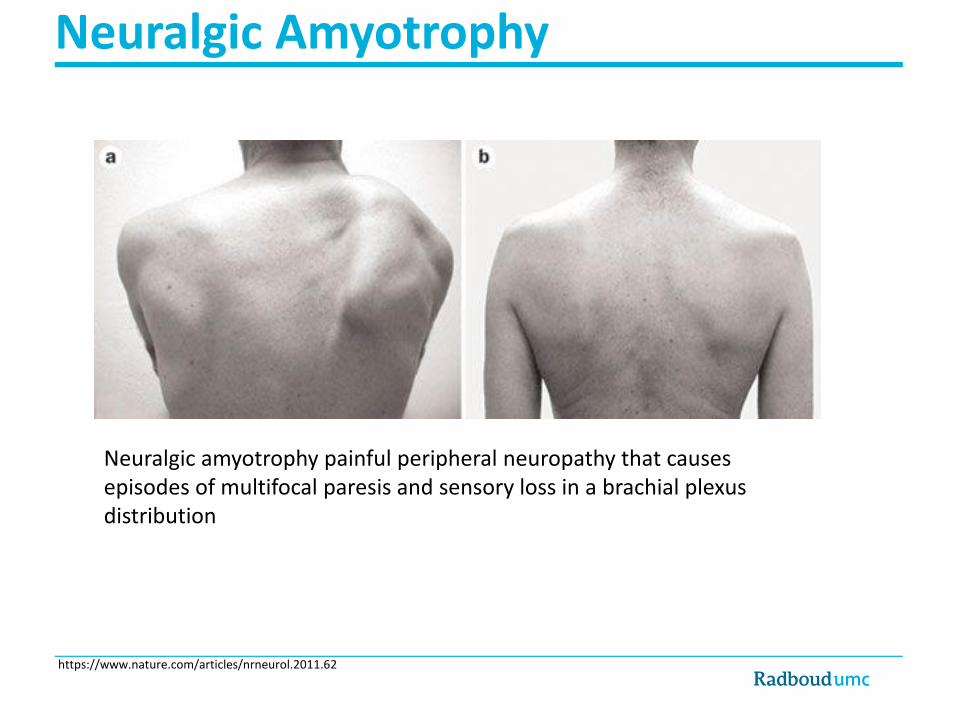
Neuralgic Amyotrophy
Neuralgic amyotrophy painful peripheral neuropathy that causes episodes of multifocal paresis and sensory loss in a brachial plexus distribution
https://www.nature.com/articles/nrneurol.2011.62

Chronic Hepatitis E
• Immunosuppressed patients can fail to clear HEV infection
• Progression to chronic hepatitis• Immunosuppressed groups include:
• Solid organ transplant recipients
• ~50–66% of HEV-infected organ transplant recipients develop chronic hepatitis
• Patients with haematological disorders
• HIV positives • Rheumatic disorders with intense immunosuppression
• Most patients are asymptomatic and present with mild and persistent LFT
abnormalities
EASL CPG HEV. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.005 [

Hepatitis E after transplantation
40−50%
Solid organ transplanted individual
Clearance
50−60%*
HEV is cleared in ~30% of patientsby reducing immunosuppression
Cirrhosis~10% rapidprogression
DeathNeed for LTx
Chronic infection
HEV epidemiology
• European Map
Netherlands • Infections seen in Dutch Laboratories• Infections in University hospitals
• Infections in Blood donors• Screening of Plasma Donors

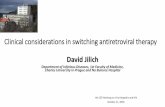
HEV ‘hot spots’ in Europe
J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.005
Scotland, 2016: 1:2,481 donors viraemic1
SW France, 2016: incidence 3−4%2
The Netherlands, 2014: 1:600 donors viraemic3
Western Germany, 2015: 1:616 donors viraemic4
Czech Republic, 2015: 400 lab-confirmed cases5
Abruzzo, Italy, 2016:seroprevalence 49%6
Western/Central Poland, 2017:seroprevalence 50%7

HEV infections in Germany
http://dx.doi.org/10.1016/j.jcv.2016.06.010 1386-6532/© 2016 Published by Elsevier B.V.

HEV epidemiology in the Netherlands

HEV cumulative

Hepatitis E in Nederland
• UMCG 2012-2017
• 75 patientsImmunocompetent : n=40Immunosuppressed: n=35
• Radboudumc 2013-2017• 42 patients
• Chronic HEV n=22 • Acute HEV n=20
• AMC 2011-2016• 32 patients• Chronic HEV n=14
• Acute HEV n=14• Unclear n=4
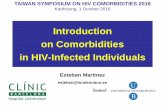
Incident HEV cases
2012 2014 2016 20180
5
10
15
20
25
Year
nu
mb
er
of
cases
Dr. Erik Verschuuren UMCG, H.L.Zaaijer, AMC 2018

• HEV PCR op pools van 24 donaties. Pool = pos: dan deconstructie naar donor(s).
• Sinds 3-7-17: 565.207 donaties (tm wk44 2018), gemid. 8074 donaties per week.
• 231/565.207 donaties HEV bevestigd PCR positief, oftewel 1 : 2447 donaties.
• Significante dalende trend.
Dutch HEV PCR donorscreening

Viral Load
Ditribution of HEV virale load
• in 231 PCR positieve bloed donors

Risk factors for HEV positivity among donors• 2100 plasma samples of blood donors from all over the Netherlands aged
18-70 years were tested for anti-HEV IgG antibodies
• IgG-seroprevalence was 31% (648/2100) and increased with age
• 1562 participants completed the questionnaire
• Risk factors : Frequent consumption of • Raw sausages “cervelaat”, “fijnkost”, “salami” (OR 1.5; 95%CI 1.2-1.9)• Bovine steak (OR 1.3; 95%CI 1.0-1.7)
• Smoked beef (OR 1.3 95%CI 1.0-1.7)• Contact with contaminated water (OR 2.5; 95%CI 1.5-4.4).
https://doi.org/10.1186/s12879-018-3078-9

Screening of Plasma donations
- HEV PCR screening van 2000 a 3000 plasmadonaties / maand, in pools van 96.- Piek medio 2014 - op willekeurige dag was 1:600 Nederlanders HEV viremisch incidentie van ~ 1% / jaar.

HEV by numbers • Estimation of HEV in the Netherlands:
• 61,000 HEV infections per year; • 85 via blood transfusion (= 1:700)• 60915 via other routes
• HEV donor screening (in pools of 24) of blood • 79 HEV transmissions prevented, 6 HEV infections slipped through
• 1722 Organ- and bone marrow transplant patients per year• HEV infections
• via food: 5.5 chronic cases of hepatitis E / year• via bloodtransfusion: 2.2 chronic cases of hepatitis E / year.
HEV donor screening prevents 79 of 85 transfusion transmissions, and• 2.0 of the 2.2 transfusion associated chronic hep E cases annually.
• 1.4 M€ testing costs/year; ~ € 700,000 per prevented chronic case.

Gezondheidsraad advies
• De commissie adviseert het testen van alle bloeddonaties op hepatitis E-
virus voorlopig voort te zetten• Bloeddonoren zijn regelmatig met HEV geïnfecteerd, zonder dat zij
ziekteverschijnselen vertonen die bloeddonatie zouden beletten.
• Bloedproducten kunnen een HEV-infectie overgedragen• Voor immuungecompromitteerde mensen, die veel bloedproducten
ontvangen, kan een HEV-infectie ernstige of zelfs fatale gevolgen hebben
• HEV-NAT-screening is effectief: het vermindert het aantal besmettingen door bloedproducten van 187 tot 13 besmettingen per jaar
• Er zijn geen alternatieve maatregelen die kunnen voorkomen dat
bloedproducten besmet zijn met HEV.
Treatment of acute HEV infection
EASL CPG HEV. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.005 [Epub ahead of print]
• Acute HEV infection does not usually require antiviral therapy
• Most cases of HEV infection are spontaneously cleared• Some patients may progress to liver failure
• Ribavirin
• Early therapy of acute HEV may shorten course of disease and reduce
overall morbidity

Hepatitis E treatment
• Chronic Hepatitis E• Wait for 3 months (to establish chronicity) • Two strategies
Ribavirin 600-900 mg/d
Reduceimmunesuppression
Immune system

Management of chronic HEV
EASL CPG HEV. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.005
HEV clearance
Relapse after
ceasing ribavirin
No HEV clearance
3-month course of
ribavirin monotherapy
Chronic HEV infection
Serum and stool
HEV RNA negative
No response to
ribavirin or intolerant
6-month course of
ribavirin monotherapy
Persistent HEV replication
in serum or HEV relapse
Pegylated interferon for 3 months in LTx patients
No alternative available therapy in other transplant patients
Reduction of immunosuppression

Resultsn = 27
n = 1 died of complicated colon surgery before HEV
infection could be evaluated
n = 26
n = 18 ribavirin treatment
GROUP B
n = 8Stop/lower
immunosuppressantsGROUP A

Comparing treatment strategies
• Cohort Study
• 25 patients• Renal transplantation 11/25
• Strategy
• Reduction Immunosuppression • cure 9/9
• Ribavirin
• cure 14/16
Cohort of 25 chronic HEV patients
Tjwa EASL 2017

Ribavirin therapy
• What is the correct ribavirin dosage ?
• 600 mg/ day some favor higher dosages (SVR~80%) • How long should I treat HEV infection with ribavirin for?
• For chronic HEV infection, the initial course of ribavirin therapy should
be for 3 months• If the patient is immunosuppressed, eg, is a solid organ transplant
recipient, consider a trial of a reduction in immunosuppression in the
first instance• What should I do in the case of ribavirin nonresponse?
• Extend course of ribavirin therapy for a further 3 months
• If still no response, continue ribavirin for further 6 months• Consider trial of pegylated interferon for 3 months (not in renal
transplant recipients
Aliment Pharmacol Ther. 2017;46:126–141

Case
• 1981 diffuse membranoproliferatieve glomerulonefritis
2004 renal transplantation 2013 diabetes mellitus type 2
• Medication • Tacrolimus 2dd 1 mg (prograft) prednison 1dd 7.5mg
• Biochemistry • ALAT 258 IU/L, ASAT 156 IU/L, Gamma GT 681 IU/L, AF 142 IU/L, Bili 14
umol/L

Case
• September 2015 & May 2016 positive PCR HEV
• Juni-december 2016. • 24 weeks Ribavine
• 27 june 2016: 600 mg ribavirine • 18 july 2016 : 400 mg ribavirine
• Maart 2017 HEV PCR negative: SVR