Presentazione di PowerPoint - Virology...
29
HIV/AIDS DEPARTMENT 2013 Consolidated ARV Guidelines Treatment Recommendations for Pregnant and Breastfeeding Women: Rationale and Key Issues Dr. Nathan Shaffer
Transcript of Presentazione di PowerPoint - Virology...

H I V / A I D S
DEPARTMENT 2013 Consolidated ARV Guidelines
Treatment Recommendations for
Pregnant and Breastfeeding Women: Rationale and Key Issues
Dr. Nathan Shaffer

o Background
• New guidelines • PMTCT context
o Overview of Key Recommendations: • When to Start ART • Breastfeeding • What ART to Start • Treatment Monitoring
o Issues and challenges
Overview of Presentation

OPERATIONAL
GUIDANCE FOR PROGRAMME
MANAGERS
CLINICAL
Consolidated ARV Guidelines: what is different?
WHAT TO DO? HOW TO DO IT?
HOW TO DECIDE WHAT TO DO, WHERE AND WHEN?
Consolidation across populations and ages o Adults (including pregnant women and serodiscordant couples) o Adolescents o Children o IDUs, MSMs, Sex workers o TB and Hepatitis co-infected
Consolidation along the continuum of care Consolidation of existing relevant guidance

Guiding Principles: Treatment 2.0

Clinically relevant o Earlier initiation of ART (CD4 ≤ 500) o Immediate ART for children < 5 years o ART initiation for all pregnant and
breastfeeding women (Option B/B+) and lifelong ART (Option B+)
o Harmonization of ART across populations (e.g., adults and pregnant women) and age groups
o Simplified, fewer, and less toxic 1st-line regimens (TDF/XTC/EFV)
New Recommendations in 2013 WHO Guidelines
Operationally relevant o Use of Fixed Dose Combinations as a
preferred approach o Improved patient monitoring to
support better adherence and detect earlier treatment failure (increased use of VL)
o Recommend task shifting, decentralization, and integration
o Community based testing to complement broader HTC

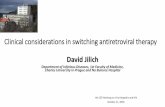
Evolution of WHO’s PMTCT ARV Recommendations
2001 2006 2010 2004 Launch July 2013
PMTC
T 4 weeks AZT; AZT+ 3TC, or SD NVP
AZT from 28 wks + SD NVP
AZT from 28wks + sdNVP +AZT/3TC 7days
Option A (AZT +infant NVP) Option B (triple ARVs)
Option B or B+ Moving to ART for all PW/BF
ART No
recommendation CD4 <200 CD4 <200 CD4 <350 CD4 <500
Move towards: more effective ARV drugs, extending coverage throughout MTCT risk period, and ART for the mother’s health

• Benefit for mother’s health, prevention of infant infections, prevention of partner infections
• Prophylaxis vs. lifelong treatment • Access to CD4 testing; determination of “eligibility” • Need for simplified regimens and algorithms • Harmonizing with adult ART regimen • Safety of drugs during pregnancy and breastfeeding • Retention and follow up • Monitoring treatment response – access to viral load
Key Issues for Treatment and Care of Pregnant and Breastfeeding Women

Progress and Barriers
o Limited coverage and implementation of PMTCT and ART for pregnant women in many high burden countries • Poor access to ANC/MCH services • Lack of testing • Failure to identify / initiate ART in eligible
women • High loss to follow-up along PMTCT cascade
o Complexity of Option A • Different treatment and prophylaxis regimens
through pregnancy and breastfeeding • Long-term NVP dosing for infants is especially
difficult • Requirement for CD4 to determine eligibility • Follow up along the PMTCT cascade is very low.
o Current approach needs to be optimized to achieve universal access and elimination
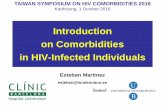
2000 2005 2010 2015
New child HIV infections, low and middle income countries (thousands)
0
100
200
300
400
500
600
Steady progress reducing infant infections •2009: ~430,000 infant infections •2012: ~290,000 infant infections •2015: Global Plan target <40,000

Number of pregnant women with HIV needing and receiving ARVs for PMTCT (2005-2011)
(From Fig 1.12, 2013 Global ART Report, WHO)
~ 35-40% receiving ART)

Source: 2013 Global AIDS Response Reporting (WHO/UNICEF/UNAIDS) and 2012 UNAIDS/WHO estimates.
Note: Numbers from 2009 include single-dose nevirapine. Numbers from 2010-2012 exclude single-dose nevirapine.
PMTCT ARV coverage in “Global Plan countries” increased to 65% in 2012

When to Start ART

Summary of Changes in Recommendations: When to Start in Adults
TARGET POPULATION (ARV-NAIVE)
2010 ART GUIDELINES 2013 ART GUIDELINES STRENGTH OF
RECOMMENDATION & QUALITY OF EVIDENCE
HIV+ ASYMPTOMATIC CD4 ≤350 cells/mm3
CD4 ≤500 cells/mm3 (CD4 ≤ 350 cells/mm3 as a priority)
Strong, moderate-quality evidence
HIV+ SYMPTOMATIC WHO clinical stage 3 or 4 regardless of CD4 cell count No change
Strong, moderate-quality evidence
PREGNANT AND BREASTFEEDING WOMEN WITH HIV
CD4 ≤350 cells/mm3 or WHO clinical stage 3 or 4
Regardless of CD4 cell count or WHO clinical stage
Strong, moderate-quality evidence
HIV/TB CO-INFECTION Presence of active TB disease, regardless of CD4 cell count No change Strong, low-quality evidence
HIV/HBV CO-INFECTION
Evidence of chronic active HBV disease, regardless of CD4 cell count
Evidence of severe chronic HBV liver disease, regardless of CD4 cell count
Strong, low-quality evidence
HIV+ PARTNERS IN SERODISCORDANT COUPLE RELATIONSHIP(S)
No recommendation established Regardless of CD4 cell count or WHO clinical stage
Strong, high-quality evidence

“Option B+” “Option B”
For programmatic and operational reasons, particularly in generalized epidemics, all pregnant and breastfeeding women infected with HIV should initiate ART as lifelong treatment. (conditional recommendation, low-quality evidence)
All pregnant and breastfeeding women infected with HIV should initiate triple ARVs (ART), which should be maintained at least for the duration of mother-to-child transmission risk. Women meeting treatment eligibility criteria should continue lifelong ART . (strong recommendation, moderate-quality evidence)
In some countries, for women who are not eligible for ART for their own health, consideration can be given to stopping the ARV regimen after the period of mother-to-child transmission risk has ceased. (conditional recommendation, low-quality evidence)
Recommendations

“Option B+” “Option B” Algorithms

Rationale: Shift from Option A to B+ or B
Major issue now is not “when to start” but really “whether to stop”
BENEFITS FOR MOTHER AND CHILD BENEFITS FOR PROGRAM DELIVERY & PUBLIC HEALTH
Ensures all ART eligible women initiate treatment
Reduction in number of steps along PMTCT cascade
Prevents MTCT in future pregnancies Same regimen for all adults (including pregnant women)
Potential health benefits of early ART for non-eligible women
Simplification of services for all adults
Reduces potential risks from treatment interruption
Simplification of messaging
Improves adherence with once daily, single pill regimen
Protects against transmission in discordant couples
Reduces sexual transmission of HIV Cost effective

• Initiate all HIV+ pregnant and breastfeeding women on ART • Major issue now is not “when to start” but “when to stop” or
“whether to stop” • Operational and programmatic advantages to lifelong ART for pregnant
and breastfeeding women (“B+”), particularly in settings: – Generalized epidemic – High fertility (though need to strengthen FP) – Long duration of breastfeeding – Limited access to CD4 to determine ART eligibility
• National programmes need to decide B or B+
When to start ART: pregnant and breastfeeding women

Rapid transition from short-course prophylaxis to Option B+, Malawi
Option B+ begins

2013 (no change from 2010)
National agencies should decide between promoting mothers with HIV to either breastfeed and receive ARV interventions or to avoid all breastfeeding
Where the national choice is to promote BF, mothers whose infants are HIV uninfected or of unknown HIV status should: • exclusively breastfeed their infants for the first six months of life • introduce appropriate complementary foods thereafter, and continue breastfeeding
for the first 12 months of life • breastfeeding should then only stop once a nutritionally adequate and safe diet
without breast-milk can be provided (strong recommendation, high-quality evidence for the first 6 months; low-quality evidence for the recommendation of 12 months)
ARVs and duration of breastfeeding

WHAT ART REGIMEN TO START

FIRST-LINE REGIMENS (PREFERRED ARV REGIMENS)
TARGET POPULATION
2010 ART GUIDELINES 2013 ART GUIDELINES STRENGTH & QUALITY OF EVIDENCE
HIV+ ARV-NAIVE ADULTS
AZT or TDF + 3TC (or FTC) + EFV or NVP
TDF + 3TC (or FTC) + EFV (as fixed-dose combination)
Strong, moderate-quality evidence
HIV+ ARV-NAIVE PREGNANT WOMEN
AZT + 3TC + NVP or EFV
HIV/TB CO-INFECTION
AZT or TDF + 3TC (or FTC) + EFV
HIV/HBV CO-INFECTION
TDF + 3TC (or FTC) + EFV
Summary of Changes in Recommendations: What to Start in Adults

• WHO Technical Update: Use of EFV During Pregnancy (June 2012) • Reassuring evidence on safety of EFV during pregnancy • Clinical and programmatic advantages compared
with NVP
• Harmonized with 1st line adult regimen • Decreasing cost
Rationale: One Regimen For All Safety of EFV in pregnancy
• Optimized once daily FDC: TDF/3TC(FTC)/EFV

No increased risk of birth defects with EFV when compared with other ARVs
Evidence Summary: Safety of EFV and TDF in Pregnancy
o Systematic review (including Antiretroviral Pregnancy Registry), reported outcomes for 1502 live births to women receiving EFV in the first trimester and found no increase in overall birth defects
o Can exclude > 3 fold increased risk in overall birth defects
Source: Ford N et al. AIDS, 2011. Ford N et al. AIDS, 2013. Ekouevi DK et al.J AIDS, 2011. WHO, Geneva Use of EFV during pregnancy. 2012. http://www.who.int/hiv/pub/treatment2/efavirenz/en Nightingale SL. JAMA, 1998. British HIV Association. Guidelines for the management of HIV infection in pregnant women. HIV Medicine. 2012. De Santis M et al. Arch of Int Medicine, 2002. Source: Antiretroviral Pregnancy Registry Steering Committee http://www.APRegistry.com Siberry GK et al. AIDS, 2012
EFV
o Potential concerns include renal toxicity, adverse birth outcomes and effects on bone density
o Systematic review assessed the toxicity of fetal exposure to TDF in pregnancy
• In the Antiretroviral Pregnancy Registry, the prevalence of all birth defects with TDF exposure in 1st trimester was 2.4% (same as background)
o Limited studies showed no difference in fetal growth between exposed/unexposed
o No studies of TDF among lactating women, who normally have bone loss during breastfeeding
o More extensive studies ongoing
TDF

HOW TO MONITOR AND WHEN TO SWITCH

RECOMMENDATION STRENGTH Viral load is recommended as the preferred monitoring approach to diagnose and confirm ARV treatment failure
Strong recommendation, low-quality evidence
If viral load is not routinely available, CD4 count and clinical monitoring should be used to diagnose treatment failure
Strong recommendation, moderate-quality evidence
Recommendations: Monitoring for ART Response
Major challenge for PMTCT and MNCH settings: • How to expand access to VL monitoring? • How to utilize CD4 data, especially for women with high baseline CD4?

Implementation Issues
• Adequate planning for changes in guidelines • Expansion and integration of ART into PMTCT sites
— Supply chain for ARVs (avoidance of stock-outs) — Task-shifting for ART initiation — Adherence, retention, follow up, linkages with chronic ART — Assuring access at peripheral sites — All MNCH sites become ART sites
• Toxicity and efficacy monitoring: access to CD4, viral load, acess to standard lab monitoring where needed
• Quality assurance

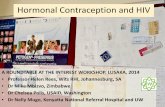
Transition in PMTCT Regimens in the 22 Global Plan Priority Countries
After 2010 WHO PMTCT ARV guidelines As of June 2013
2013
Option AOption BOption B+ Planned/pilotingOption B+ ImplementingNot a priority country

Key research questions: Pregnant Women
ARV toxicity surveillance: • What is the safety of lifelong ART for pregnant and breastfeeding women
especially in RLS, where malnutrition and co-morbidities are common? • What do we need to understand about maternal toxicity, pregnancy toxicity
(stillbirth, low birth weight, prematurity, birth defects) and infant toxicity?
Mother-to-child transmission and mother and child health impact: • What is the impact on overall HIV-free survival and the MTCT rate at the end of
breastfeeding as well as at 6-weeks? • What is the impact on maternal morbidity and mortality, sexual transmission to
partners and the long-term success of first-line ART?
Adherence and retention: • What is the acceptability of ART to women especially those who initiate lifelong
ART before they meet the adult eligibility criteria? • How good is adherence and retention for women with both low and high CD4? • What health systems and community interventions are needed to achieve high
levels of adherence and retention in setting of universal ART?

Comprehensive ART / MCH Services

Acknowledgements
Special thanks and acknowledgements to: Maternal and Child Health GDG Co-Chairs:
Elaine Abrams (International Center for AIDS Care and Treatment Programs, Mailman School of Public Health, Columbia University, USA) and Denis Tindyebwa (African Network for the Care of Children Affected by AIDS, Uganda)
MCH GDG members, special contributors, peer reviewers Members of all the GDGs contributing to the consolidated guidelines WHO Secretariat