considerations…. from the - Virology...
34
A case, and some pharmacological considerations…. from the perspective of a virologist Anna Maria Geretti University of Liverpool, United Kingdom 1
Transcript of considerations…. from the - Virology...

A case, and some
pharmacological
considerations…. from the
perspective of a virologist
Anna Maria Geretti
University of Liverpool, United Kingdom
1

Case History: Mr RS
• 53-year-old male
• Diagnosed HIV positive in 1999
• Baseline CD4 count 46 cells
• Baseline viral load 83,000 cps
• Subtype C
• Past hepatitis B infection
• Hepatitis C negative
• Oct 1999 starts AZT/3TC + IDV

Medical and ART historyDate started
Date stopped
ART Viral load CD4 Resistance
Oct 1999 Oct 2000 AZT/3TC IDV 442 83
Oct 2000 Nov 2001 ABC/3TC EFV 31,500 127
RT: 67N 215Y 184V 74V 100I 103N
Nov 2001 Jul 2004TDF d4T 3TC
LPV/r<50 280
Jul 2004 Jul 2008 TDF ATV FPV/r 771 399RT:
NonePR: 32I
Jul 2008 Nov 2011TDF RAL DRV/r (600/100 bid)
<50 to 175 447

Mr RS Which is your preferred strategy?
1. Do nothing as long as the viral load is <200 cps
2. Address patient-related psyco-social issues &
adherence
3. Address sample- and/or lab-related technical issues
4. Request more tests – which?
5. Change or intensify the ART regimen

Management strategies
Review:
• Technical issues of viral load testing
• Adherence, tolerability, psycho-social issues
• Expected potency of the regimen
• Drug-drug interactions (DDIs) and food requirements
• Reasonable to perform a drug resistance test
• Reasonable to check drug levels
• CD4 nadir and pre-ART viral load inform
Size of HIV DNA reservoir
Likelihood of compartmentalised virus replication

Plasma HIV-1 RNA during ART
Spivak et al. Trends Mol Med 2016

Cellular HIV-1 DNA load during suppressive ART
Geretti et al. Int. Workshop HIV & Hepatitis Viruses Drug Resistance 2013; Ruggiero et al. EBioMed 2015
HIV
-1 D
NA
log 1
0 c
ps
pe
r 1
06
CD
4 T
-ce
lls
Years of suppressive ART
Cohort started 2 NRTIs + EFV or NVP, achieved VL <50 cps within 6 months, and during subsequent follow-up had VL consistently <50 cps (no blips or interruptions) while remaining on the initial NNRTI (n=104)
Mean change integrated HIV-1 DNA for 10 yrs of ART (log10 cps/106 PBMC)
+0.2 [95% CI -0.2, +0.6; p 0.28]

Virus replication in sanctuary compartments due to poor drug penetration or activity
Virus reactivation in latently infected cells, with presence
of ART ensuring that new cells cannot be productively
infected

Untimed drug levels & resistance test at LLV predict viral load rebound >1000 cps
• First LLV plasma sample: PI/NNRTI concentration and resistance test (n=328)
• Concentrations classed as ‘therapeutic' or ‘suboptimal' based on target Ctrough
• Genotypic sensitivity score (GSS) of regimen by Stanford algorithm
Independent predictors of
VL rebound >1000 cps (adjOR)
o Suboptimal drug levels = 2.53
(95% CI 1.72-3.72; p<0.001)
o GSS <3 = 1.55
(95% CI 1.02-2.34; p=0.04)
o LLV (cps):
250-499 = 2.48 (95% CI 0.99-6.22)
500-749 = 2.36 (95% CI 0.91-6.11)
750-999 = 3.65 (95% CI 1.42-
9.39)(p<0.001)
Gonzalez-Serna et al. CROI 2015

Low drug levels predict faster resistance
Gonzalez-Serna et al. CROI 2015

Case History: Mr RS
• DRV plasma concentration in range
• Plasma resistance test (RT, PR, IN) wild-type X 3
• CSF HIV RNA 3128 cps/ml
• CSF resistance testRT: 67N 215Y 184V 100I 103NPR: wild-typeIN: RT 155H

Nightingale et al. J NeuroVirol 2016
HIV-1 RNA Detection in CSF according to LLV
• HIV-1 RNA measured in paired plasma and CSF of 43 subjects with plasma VL <50 cps over ≥12 months of ART and in 40 subjects with a history of LLV
• HIV-1 RNA detected in CSF in 0/43 vs. 9/40 (22%) respectively
• Detection of HIV-1 RNA in CSF associated with low nadir CD4 count (p=0.030) and black heterosexual exposure group (p=0.007) but not with drug concentration or CPE score

• ART-experienced, INI-naïve
• TDF FTC + DTG 50 mg OD
PDVF= Protocol-defined virological failure;
FC = Fold change; RC = Replication capacity
Underwood et al. European HIV & Hepatitis Workshop 2015
10
100
1000
10000
0 12 24 36 48 60 72 84 96 108 120 132 144
PDVF
Wk 120
622 cps/mL
Confirm
Wk 132
1054 cps/mL
Day 1 PDVF Confirm.
HIV-1 RNA 733 622 1054
INI
mutation
- A49G,
S230R,
R263K
A49G,
S230R,
R263K
DTG FC 0.73 3.82 5.77
RAL FC 0.54 2.39 2.62
INI RC 20% 7.1% 12%
No NRTI resistance at any time point
386 cps/mL
HIV
-1 R
NA
cp
s/m
LSAILING Case-1

• ART-experienced, INI-naïve
• ABC 3TC + DTG 50 mg OD
10
100
1000
10000
100000
0 12 24 36 48 60 72 84 96 108 120
PDVF
Wk 108
3895 cps/mL
Confirm
Wk 108 retest
407 cps/mL
Day 1 PDVF
HIV-1 RNA 25105 3895
IN mutation - N155H
DTG FC 0.97 1.8
RAL FC 1.18 12
IN RC NRb NR
PDVF BR: No emergent resistance, loss of M184M/V
Week
HIV
-1 R
NA
cp
s/m
L
Underwood et al. European HIV & Hepatitis Workshop 2015
PDVF= Protocol-defined virological failure;
FC = Fold change; RC = Replication capacity
SAILING Case-2

You plan to modify the ART regimen Which is your preferred strategy?
1. DRV/b + DTG
2. DRV/b + DTG + ETR
3. DRV/b + DTG + MVC
4. DRV/b + MVC + ETR
5. DRV/b + DTG + MVC + ETR
Add TDF or TAF to any of the above, +/- FTC?
Which dose of DTG?

Pharmacology of integrase inhibitors
DTG EVG RALDose 50mg od
(50-100mg bd)150mg od(boosted)
400mg bd
• Potent inhibitors of integrase enzyme
• Protein binding-adjusted IC90/95 values in the low ng/ml range - High inhibitory quotient (IQ) - DTG > EVG > RAL
• Each INI has unique PK/PD properties
• PK variability highest for RAL and lowest for DTG

• Different hepatic metabolism: RAL and DTG minimal cytochrome P450 (CYP) involvement; EVG primarily thorugh CYP3A4
• RAL and DTG have minimal DDI profiles
• EVG requires boosting to be amenable to OD dosing and has greater DDI potential – manageable as with RTV
Pharmacology of integrase inhibitors
Podany et al. 2016

Pharmacology of integrase inhibitors
DTG EVG RALDose 50mg od
(bd if INI experienced)150mg od(boosted)
400mg bd
Food effect on drug exposure
Take with food if possibility of INI
resistance
Low (33%), moderate (41%), and high (33%) fat
meals increased AUC
Take with food
Light (36%), and high (91%) fat meals
increased AUC
Take without regard to food
High fat doubles AUC, food increases variability
• Absorption affected by divalent / trivalent cations, such as those found in multivitamins and antacids

DT
G m
ean
plas
ma
conc
entr
atio
n (n
g/m
L)
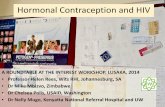
Effect of food on DTG exposure - healthy volunteers
*50 mg formulation
Song et al. Antimicrob Agents Chemother 2012
Low, moderate, and high fat meals increase DTG AUC by 33%, 41%, and 66%, respectively. In INI-naive patients, dose with or without food.
In INI-resistant patients, dose with food.
Low fatFasting
Moderate fatHigh fat
PA-IC90 0.064 µg/mL
Time (hours)
0 10 20 30 40 50 60
4500
4000
3500
3000
2500
2000
1500
1000
500
0

Dolutegravir + antacid 2h later
Dolutegravir alone
0 10 20 30 40 50 8060 70
2.0
1.8
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0Mea
n D
TG
con
cent
ratio
n (µ
g/m
L)
26%
74%
Time (hrs)
Dolutegravir +antacid
Patel et al. JAC 2011; Pommier et al. Nat Rev 2005; Stribild SmPC June 23rd 2015; Tivicay SmPc Oct 1st 2015
INI chelation with cations
Mg2+
Mg2+
Binding of integrase inhibitors
Mg
Mg
EVG AUC EVG Cmin
Al/Mg containing antacid takentogether
Decreased 45%
Decreased 41%
Antacid +/- 2h after EVG
↔ ↔
Not recommended – RAL Separate – DTG and EVG/c

Impact of acid-reducing agents and multivitamins on DTG exposure
1. Tivicay SmPC January 2014
2. Patel et al. J Antimicrob Chemother 2011
Co-administered drug
DTG C or C24
Geometric mean change Recommendation
Antacids and supplements≠
Magnesium / aluminium-
containing antacid
AUC*↓74%
Take antacids and supplements a minimum of
2 hours after or 6 hours before DTG1Calcium supplements ↓39%
Iron supplements ↓56%
Multivitamins ↓32%
Acid-lowering agents
Omeprazole ↓5% No significant effect observed2
C: Trough concentration

Pharmacology of integrase inhibitors
DTG EVG RALDose 50mg od
(bd if INI experienced)150mg od(boosted)
400mg bd
Food effect Take with food if possibility of INI
resistance
Low (33%), moderate (41%), and high (33%) fat
meals increased AUC
Take with food
Light (36%), and high (91%) fat meals
increased AUC
Take without regard to food
High fat doubles AUC, food increases variability
MetabolismUGT1A1
(CYP3A 10-15%)CYP3A / UGT1A1/3 UGT1A1
Protein binding >99% 99% 76-83%
Half life 11-12h 9h 9h
Dose-exposure Dose proportional up to 100mg
Less than dose-proportional
Nearly dose-proportional

DTG distribution and CSF penetration
Plasma protein binding: >99%1
Blood:plasma ratio: 0.44–0.54 → minimal association with blood cellular components1
A Phase IIIb study assessed the distribution of DTG in CSF2
DTG concentrations observed in CSF at both Week 2 and Week 16 averaged 18 ng/ml (comparable to unbound concentration) and exceeded the in vitro IC50 against wild-type viruses (0.2 ng/mL)2 for all subjects, suggesting that DTG was able to achieve therapeutic concentrations in the CSF
1. Tivicay SmPC, January 2014;
2. Letendre et al. CROI 2013

Special groups
DTG EVG RALSwallowing Granule being
developed( bioavailability)
Cannot be chewed or crushed
Chewable tablets, granules
(bioavailability)
Children Not licensed <12y Not licensed <18y, avoid <6y
Licensed from 4 weeks
Pregnancy No dataFDA Cat B
Limited dataFDA Cat B
Some data FDA Cat C
Renal impairment
No adjustmentDTG exposure reduced in severe renal disease
FDC with TDF not <70, stop <50
FDC with TAF >30
No adjustment
Cirrhosis CP-A
CP C
No adjustment
Caution
No adjustment
Not recommended
No adjustment
Caution

Dose-exposure relationship for DTG
*PA-IC90 is the protein-adjusted 90% inhibitory concentration †Inhibitory quotient is defined as C/PA–IC90
1. van Lunzen et al. Lancet Infect Dis 2012;
2. Rockstroh et al. HIV10 2010
DTG PK parameters at Week 2 by dose in the SPRING-1 Phase IIb trial1,2
QD dose
Cmax
(μg/mL)
AUC0–
(µg·h/mL)
C
(µg/mL) IQ†
10 mg1,2 1.10 (37) 16.0 (40) 0.30 (71) 4.7
25 mg1,2 1.71 (43) 23.1 (48) 0.54 (67) 8.4
50 mg1,2 3.40 (27) 48.1 (40) 1.20 (62) 19
●DTG shows low to moderate PK variability1,2
●All drug levels well above the in-vitro PA-IC90 of 0.064 μg/mL1,2
Values shown are geometric means (CV%)
0 5
Post-dose time (hours)
10.0
1.0
Mea
n D
TG
con
cent
ratio
n (µ
g/m
L)
0.1
10 15 20 25
10 mg QD2
25 mg QD2
50 mg QD2
PA-IC90 0.064 µg/mL*

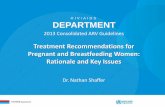
SAILING: Response rates by quartile of DTG c0_avg
The average plasma concentration of DTG was a significant predictor of virological response: subjects in the lowest quartile had a lower response
SAILING: Phase III study in ART-experienced, INI-naïve subjects
Song et al. ICAAC 2013
100
80
60
40
20
0 0–25
0.304 μg/mL
(0.000–0.555)
Response rate
63.5%
25–50
0.805 μg/mL
(0.557–1.069)
Response rate
72.9%
50–75
1.347 μg/mL
(1.072–1.793)
Response rate
82.4%
75–100
2.665 μg/mL
(1.805–8.673)
Response rate
75.3%
C0_avg quartile
Res
po
nd
ers,
%
Responders Non-responders

DDI liability
DTG EVG RAL
Metabolism UGT1A1
(CYP3A 10-15%)
CYP3A
UGT1A1/3
UGT1A1
Perpetrator of
DDIs
No effect on CYPs,
UGTs.
Inhibits OCT2
Cobicistat – potent
CYP3A, mod CYP2D6
and MATE1
EVG – mod inducer
of CYP2C9
No effect on CYPs,
UGT or PgP
Divalent cations Al/Mg/Ca/Fe/Multivit
amins
Separate -6 or +2h
Al/Mg antacids ±2h
Multivitamins ±4h
Al/ Mg contraindicated
Ca: not clinically
meaningful
Gastric pH No significant
interaction
No significant
interaction
RAL absorption with
OMP (39%) / FAM
(45%); no adjustment
needed

DTG interactions
Commonly used medications Interactions
Oral contraceptives1 No dose adjustment necessary
H2-receptor antagonists (e.g.,ranitidine, cimetidine)2 No dose adjustment necessary
Prednisone1, Methadone1, Rifabutin1 No dose adjustment necessary
Metformin1 Limit the total daily dose of metformin to 1,000 mg. When stopping DTG, the
metformin dose may require an adjustment. Monitoring of blood glucose when initiating
concomitant use and after withdrawal of DTG recommended
Multivitamins, calcium supplements, iron supplements1 DTG to be administered 2 hours before or 6 hours after taking these agents
Magnesium/aluminium-containing antacids1 DTG to be administered 2 hours before or 6 hours after taking these agents
Carbamazepine, rifampicin, efavirenz; nevirapine andtipranavir/r1
The recommended dose of DTG is 50 mg twice daily when co-administered with these
agents. In the presence of INI resistance, combination with these agents should be
avoided Note: Co-administration of dofetilide and dolutegravir is contraindicated.1,2
1. TIVICAY Summary of Product Characteristics. September 20152. TRIUMEQ Summary of Product Characteristics. September 2015

Co-administered drug
DTG C or C24
Geometric mean change Recommendation1
Protease inhibitors
DRV/r 600/100 mg BID* ↓38% No DTG dose adjustment required
ATV 400 mg OD*¥ ↑180% No DTG dose adjustment required
ATV/r 300/100 mg OD* ↑121% No DTG dose adjustment required
NNRTIs
RPV 25 mg OD ↑22% No DTG dose adjustment required
EFV 600 mg OD ↓75% DTG 50 mg BID should be given‡
ETR 200 mg BD ↓88% DTG should not be given with ETR without
co-administration of ATV/r, DRV/r or LPV/r
NRTIs
TDF 300 mg OD ↓8% No DTG dose adjustment required
Impact of ARVs on DTG exposure
*DTG 30 mg OD studied; ¥ Unboosted ATV is not licensed in the EU; ‡INI-
naive patients; alternative combinations should be considered where possible
for INI-experienced patients with certain
INI-associated resistance substitutions or clinically suspected INI resistance1.Tivicay SmPC January 2014
C: Trough concentration

DTG AUC 70%
DTG 50mg qd
+ ETR 200mg bd
+ LPVr 400/100 bd
+ DRVr 600/100 bd
DTG AUC ↔
DTG AUC 25%
DTG + ETR without bPI DTG + ETR with bPI twice daily
Song et al. AAC 2011
DTG with ETR

VIIV EUROPEAN SCIENTIFIC REVIEW FORUM ON DOLUTEGRAVIR

ETR + MVC = MVC (600mg or 150 bd without/with PI/b) RTV + MVC = MVC (150mg bd)RTV + DTG = potentially DTG ETR + DTG = DTG

You plan to modify the ART regimen Which is your preferred strategy?
1. DRV/b + DTG
2. DRV/b + DTG + ETR
3. DRV/b + DTG + MVC
4. DRV/b + MVC + ETR
5. DRV/b + DTG + MVC + ETR
Added TAF/FTC
DTG 100mg bd

Thanks to
Saye Khoo (UoL)
David Back (UoL)
Romina Quercia (ViiV)
34