Guidelines and Levels of Care for Pediatric Intensive...
12
Guidelines and Levels of Care for Pediatric Intensive Care Units 166 PEDIATRICS Vol. 92 No. I July 1993 Committee on Hospital Care and Pediatric Section of the Society of Critical Care Medicine Pediatric critical care medicine has matured dra- matically during the past two decades. Knowledge of the pathophysiology of life-threatening processes and the technologic capacity to monitor and treat pediatric patients suffering from them have ad- vanced rapidly during this period. Along with the scientific and technical advances has been the evolu- tion of the pediatric intensive care unit (PICU), where the special needs of critically ill or injured children can be met by pediatric specialists. In 1985, the American Board of Pediatrics recog- nized the new subspecialty of Pediatric Critical Care Medicine and established criteria for subspecialty certification. The American Boards of Medicine, Sur- gery, and Anesthesiology gave similar recognition to the subspecialty. In 1990, the Residency Review Committee of the Accreditation Council for Graduate Medical Education completed its first accreditation of Pediatric Critical Care Medicine Training Pro- grams. In view of these developments, the Pediatric Sec- tion of the Society of Critical Care Medicine and the American Academy of Pediatrics Section on Critical Care Medicine and Committee on Hospital Care be- lieve that existing published1 guidelines should now be revised for the pediatric intensive care unit. This policy represents the consensus of the three above- mentioned groups who believe the recommenda- tions that follow are current, necessary, and attain- able in 1993. The guidelines are not intended as a statement of the ideal or ultimate requirements for PICUs. We expect standards for PICUs to rise as critical care medicine continues to develop and ap- propriately trained providers become more readily available. Pediatric critical care is provided primarily at one level. However, we recognize a need for an addi- tional level of care in geographically isolated regions with a small population base, to allow stabilization of critically ill children before transfer to another center and to avoid long-distance transfers for disorders of less complexity or of low acuity. Thus, two separate sets of guidelines were developed. Requirements for Level I PICUs are discussed in detail in the text and summarized in the Table. Requirements for Level II PICUs differ primarily with respect to the level of These Guidelines are being published simultaneously in Critical Care Med- icine. The recommendations in this statement do not indicate an exdusive course of treatment or procedure to be followed. Variations, taking into account individual circumstances, may be appropriate. PEDIATRICS (ISSN 0031 4005). Copyright C 1993 by the American Acad- emy of Pediatrics. staffing and facilities necessary. Whereas other spe- cial observation areas may be appropriate for hospi- tals with small pediatric services, they should not be considered PICUs. The Level I PICU must be capable of providing definitive care for a wide range of complex, progres- sive, rapidly changing, medical, surgical, and trau- matic disorders, often requiring a multidisciplinary approach, occurring in pediatric patients of all ages, excluding premature newborns. Such units are usu- ally found in major medical centers or within child- ren’s hospitals. Level H units exist primarily in areas distant from a Level I PICU that do not have the population base to support a Level I unit; these units will generally care for fewer severely ill patients. Patients in Level II units will have less complex and more stable disorders whose course is more predict- able. As a consequence of the difference in patient population, both the physicians and their specialized services will differ between levels. Level I PICUs will have a complete complement of subspecialists, in- cluding pediatric intensivists, whereas Level II P1- CUs will not require the full spectrum of subspecial- ists or their services. Each Level II unit must have a well-established communications system with a Level I unit for timely referral of patients who need care unavailable at the Level II PICU. It is understood that Level I PICUs are variable in size, personnel, physical characteristics, and equip- ment, and that they differ in the types of specialized care (ie, care following transplantation or cardiac sur- gery) that they provide. Similarly, Level II units also vary in scope and personnel. Level II units should be located according to documented demand (need) and in concert with accepted principles or regional- ization of medical care. This document and the Table provide minimum guidelines for the following aspects of critical care: (1) Level I and Level II pediatric intensive care fad- ities and services; (2) hospital facilities and services; (3) personnel; (4) prehospital care and interhospital transport; (5) quality assurance; and (6) research and training. These guidelines are intended to assist: (1) hospitals, in properly staffing and equipping these units; (2) physicians, as a reference in referral and care of critically ill infants and children; (3) Emer- gency Medical Services (EMS) personnel, for proper prehospital triage; and (4) the Level I and H PICUs themselves as a means of ensuring proper patient care and professional credibility. These guidelines are not static, because future changes reflecting new knowledge and technologies are anticipated. by guest on August 24, 2018 www.aappublications.org/news Downloaded from
Transcript of Guidelines and Levels of Care for Pediatric Intensive...

Guidelines and Levels of Care for Pediatric Intensive Care Units
166 PEDIATRICS Vol. 92 No. I July 1993
Committee on Hospital Care and Pediatric Section of the Society ofCritical Care Medicine
Pediatric critical care medicine has matured dra-matically during the past two decades. Knowledge ofthe pathophysiology of life-threatening processesand the technologic capacity to monitor and treatpediatric patients suffering from them have ad-vanced rapidly during this period. Along with thescientific and technical advances has been the evolu-tion of the pediatric intensive care unit (PICU), wherethe special needs of critically ill or injured childrencan be met by pediatric specialists.
In 1985, the American Board of Pediatrics recog-nized the new subspecialty of Pediatric Critical CareMedicine and established criteria for subspecialtycertification. The American Boards of Medicine, Sur-gery, and Anesthesiology gave similar recognition tothe subspecialty. In 1990, the Residency ReviewCommittee of the Accreditation Council for GraduateMedical Education completed its first accreditationof Pediatric Critical Care Medicine Training Pro-grams.
In view of these developments, the Pediatric Sec-tion of the Society of Critical Care Medicine and theAmerican Academy of Pediatrics Section on CriticalCare Medicine and Committee on Hospital Care be-lieve that existing published1 guidelines should nowbe revised for the pediatric intensive care unit. Thispolicy represents the consensus of the three above-mentioned groups who believe the recommenda-tions that follow are current, necessary, and attain-able in 1993. The guidelines are not intended as astatement of the ideal or ultimate requirements forPICUs. We expect standards for PICUs to rise ascritical care medicine continues to develop and ap-propriately trained providers become more readilyavailable.
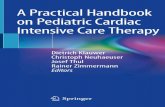
Pediatric critical care is provided primarily at onelevel. However, we recognize a need for an addi-tional level of care in geographically isolated regionswith a small population base, to allow stabilization ofcritically ill children before transfer to another centerand to avoid long-distance transfers for disorders ofless complexity or of low acuity. Thus, two separatesets of guidelines were developed. Requirements forLevel I PICUs are discussed in detail in the text andsummarized in the Table. Requirements for Level IIPICUs differ primarily with respect to the level of
These Guidelines are being published simultaneously in Critical Care Med-
icine.
The recommendations in this statement do not indicate an exdusive courseof treatment or procedure to be followed. Variations, taking into accountindividual circumstances, may be appropriate.
PEDIATRICS (ISSN 0031 4005). Copyright C 1993 by the American Acad-emy of Pediatrics.
staffing and facilities necessary. Whereas other spe-cial observation areas may be appropriate for hospi-tals with small pediatric services, they should not beconsidered PICUs.
The Level I PICU must be capable of providingdefinitive care for a wide range of complex, progres-sive, rapidly changing, medical, surgical, and trau-matic disorders, often requiring a multidisciplinary
approach, occurring in pediatric patients of all ages,excluding premature newborns. Such units are usu-ally found in major medical centers or within child-ren’s hospitals. Level H units exist primarily in areasdistant from a Level I PICU that do not have thepopulation base to support a Level I unit; these unitswill generally care for fewer severely ill patients.Patients in Level II units will have less complex andmore stable disorders whose course is more predict-able. As a consequence of the difference in patientpopulation, both the physicians and their specializedservices will differ between levels. Level I PICUs willhave a complete complement of subspecialists, in-cluding pediatric intensivists, whereas Level II P1-CUs will not require the full spectrum of subspecial-ists or their services. Each Level II unit must have awell-established communications system with aLevel I unit for timely referral of patients who needcare unavailable at the Level II PICU.
It is understood that Level I PICUs are variable insize, personnel, physical characteristics, and equip-ment, and that they differ in the types of specializedcare (ie, care following transplantation or cardiac sur-gery) that they provide. Similarly, Level II units alsovary in scope and personnel. Level II units should belocated according to documented demand (need)and in concert with accepted principles or regional-ization of medical care.
This document and the Table provide minimumguidelines for the following aspects of critical care:(1) Level I and Level II pediatric intensive care fad-ities and services; (2) hospital facilities and services;(3) personnel; (4) prehospital care and interhospitaltransport; (5) quality assurance; and (6) research andtraining. These guidelines are intended to assist: (1)hospitals, in properly staffing and equipping theseunits; (2) physicians, as a reference in referral andcare of critically ill infants and children; (3) Emer-gency Medical Services (EMS) personnel, for properprehospital triage; and (4) the Level I and H PICUsthemselves as a means of ensuring proper patientcare and professional credibility. These guidelines arenot static, because future changes reflecting newknowledge and technologies are anticipated.
by guest on August 24, 2018www.aappublications.org/newsDownloaded from
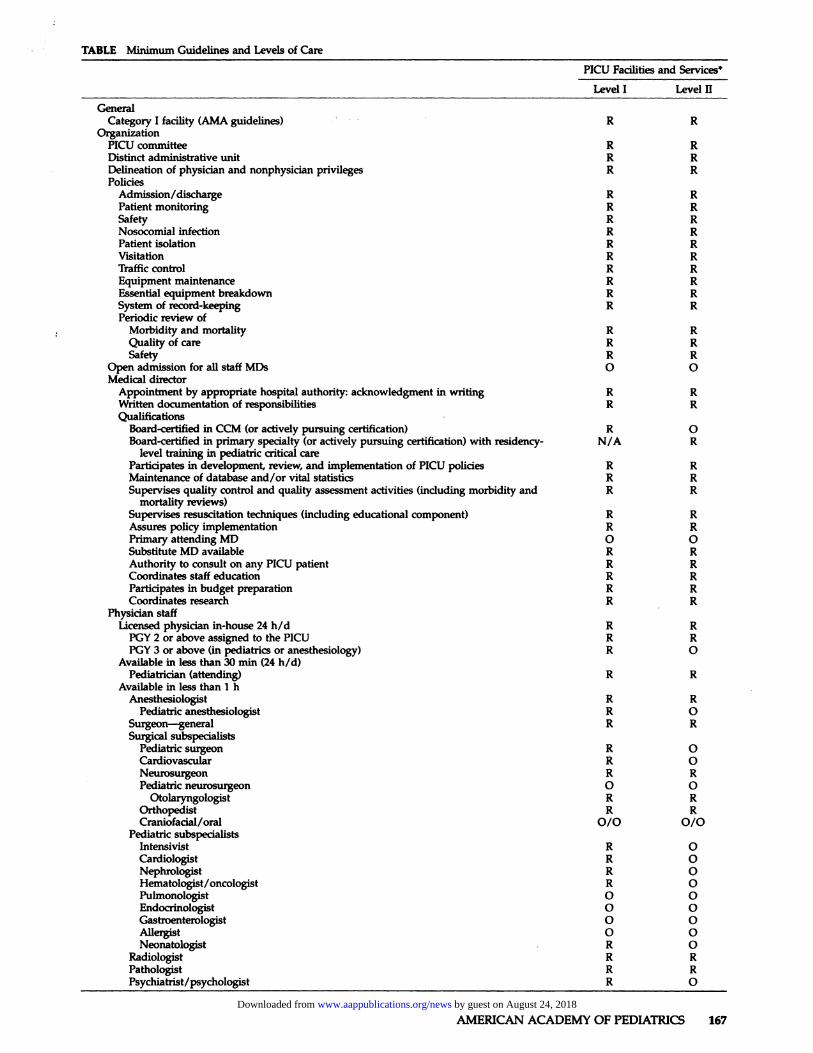
TABLE Minimum Guidelines and Levels of Care PIW Facilities
and Services*
Level I Level II
General
Category I facility (AMA guidelines) � , . � R ROrganization
PICU committee R R
Distinct administrative unit R RDelineation of physician and nonphysician privileges R R
PoliciesAdmission/discharge R R
Patient monitoring R R
Safety R R
Nosocomial infection R R
Patient isolation R R
Visitation R RTraffic control R R
Equipment maintenance R REssential equipment breakdown R R
System of record-keeping R R
Periodic review ofMorbidity and mortality R R
Quality of care R R
Safety R R
Open admission for all staff MDs 0 0Medical director
Appointment by appropriate hospital authority: acknowledgment in writing R R
Written documentation of responsibilities R R
Qualifications
Board-certified in CCM (or actively pursuing certification) R 0Board-certified in primary specialty (or actively pursuing certification) with residency- N/A R
level training in pediatric critical care
Participates in development, review, and implementation of PICU policies R R
Maintenance of database and/or vital statistics R R
Supervises quality control and quality assessment activities (induding morbidity and R Rmortality reviews)
Supervises resuscitation techniques (induding educational oomponent) R RAssures policy implementation R RPrimary attending MD 0 0Substitute MD available R R
Authority to consult on any PICU patient R RCoordinates staff education R R
Participates in budget preparation R RCoordinates research R R
Physician staff
Ucensed physician rn-house 24 h/d R R
PGY 2 or above assigned to the PICU R RPGY 3 or above (in pediatrics or anesthesiology) R 0
Available in less than 30 mm (24 h/d)Pediatrician (attending) R R
Available in less than I hAnesthesiologist R R
Pediatric anesthesiologist R 0Surgeon-general R RSurgical subspecialists
Pediatric surgeon R 0Cardiovascular R 0Neurosurgeon R R
Pediatric neurosurgeon 0 0Otolaryngologist R R
Orthopedist R R
Craniofacial/oral 0/0 0/0Pediatric subspecialists
Intensivist R 0Cardiologist R 0Nephrologist R 0Hematologist/oncologist R 0Pulmonologist 0 0Endocrinologist 0 0Gastroenterologist 0 0Aller�t 0 0Neonatologist . R 0
Radiologist R R
Pathologist R R
Psychiatrist/psychologist R 0
AMERICAN ACADEMY OF PEDIATRICS 167 by guest on August 24, 2018www.aappublications.org/newsDownloaded from
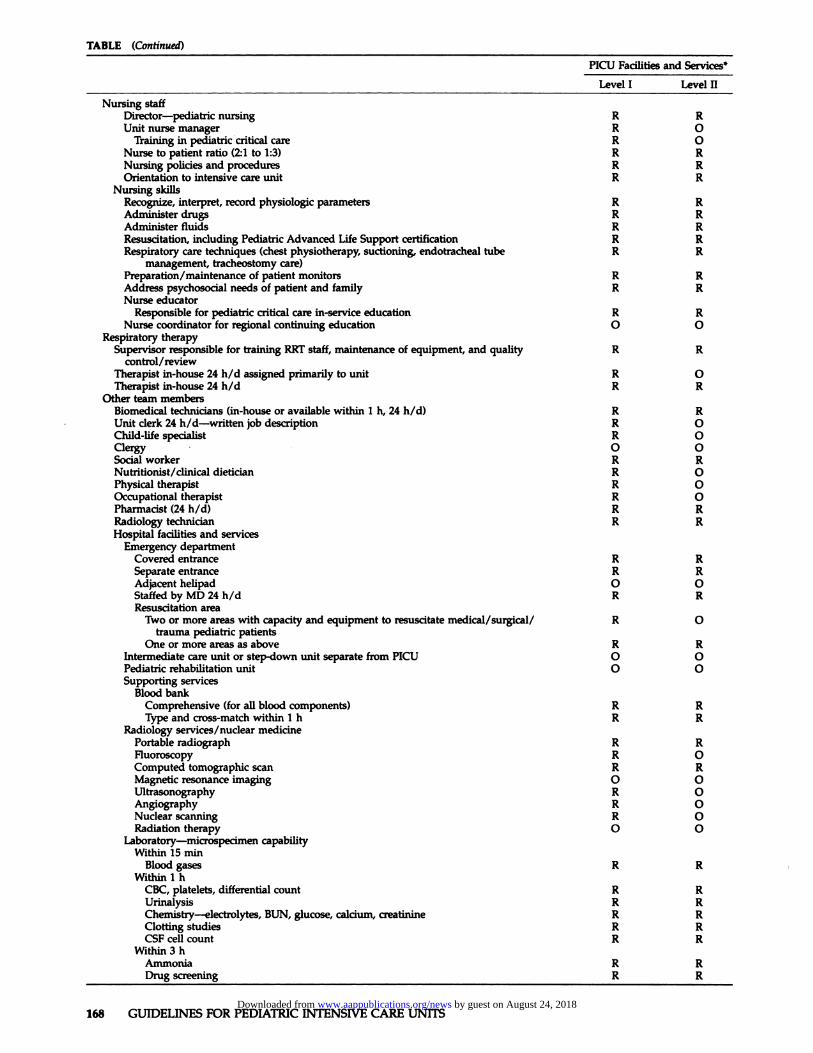
TABLE (Continued)
PICU Facilities and Service?
Level I Level II
Nursing staff
Director-pediatric nursing R R
Unit nurse manager R 0Training in pediatric critical care R 0
Nurse to patient ratio (21 to 1:3) R RNursing policies and procedures R R
Orientation to intensive care unit R RNursing skills
Recognize, interpret, record physiologic parameters R RAdminister drugs R RAdminister fluids R RResuscitation, including Pediatric Advanced Life Support certification R RRespiratory care techniques (chest physiotherapy, suctioning, endotracheal tube R R
management, tracheostomy care)
Preparation/maintenance of patient monitors R RAddress psychosocial needs of patient and family R R
Nurse educatorResponsible for pediatric critical care in-service education R R
Nurse coordinator for regional continuing education 0 0Respiratory therapy
Supervisor responsible for training RRT staff, maintenance of equipment, and quality R R
control/review
Therapist in-house 24 h/d assigned primarily to unit R 0Therapist in-house 24 h/d R R
Other team membersBiomedical technicians (in-house or available within 1 h, 24 h/d) R RUnit derk 24 h/d-written job description R 0Child-life specialist R 0Clergy #{149} 0 0Social worker R RNutritionist/clinical dietician R 0Physical therapist R 0Occupational therapist R 0Pharmacist (24 h/d) R RRadiology technician R RHospital facilities and services
Emergency department
Covered entrance R R
Separate entrance R R
Adjacent helipad 0 0StaffedbyMD24h/d R RResuscitation area
Two or more areas with capacity and equipment to resuscitate medical/surgical/ R 0trauma pediatric patients
One or more areas as above R R
Intermediate care unit or step-down unit separate from PICU 0 0Pediatric rehabifitafion unit 0 0Supporting services
Blood bank
Comprehensive (for all blood components) R R
Type and cross-match within I h R RRadiology services/nudear medicine
Portable radiograph R RFluoroscopy R 0Computed tomographic scan R RMagnetic resonance imaging 0 0Ultrasonography R 0Angiography R 0Nudear scanning R 0Radiation therapy 0 0
Laboratory-microspecimen capability
Within 15 nunBlood gases R R
Within I hCBC, platelets, differential count R RUrinalysis R RChemistry-electrolytes, BUN, glucose, calcium, creatinine R R
Clotting studies R RCSF cell count R R
Within 3 hAmmonia R R
Drug screening R R
168 GUIDELINES FOR PEDIATRIC INTENSWE CARE UNITS by guest on August 24, 2018www.aappublications.org/newsDownloaded from
TABLE (Continued)
PICU Facilities and Service?
Level I Level II
Osmolanty R R
Magnesium, phosphorus R R
Preparation available-24 h/d
Bacteriology: culture and Gram stain R R
Operating room
Available within 30 mm, 24 h/d R 0Available within 60 mm, 24 h/d R RSecond OR available within 45 mm, 24 h/d R 0Capabilities
Cardiopulmonary bypass R 0Bmnchoscopy, pediatric R 0Endoscopy, pediatric R 0RadiographinOR R R
Cardiology-pediatric capability
Electrocardiogram R REchocardiography
1. Two-dimensional R 0with Doppler 0 0
2. M-mode R 0Catheterization laboratory R 0
Neurodiagnostic laboratory
EEC R 0Evoked potentials 0 0Transcranial Doppler flow 0 0
Hemodialysis R 0Pharmacy-pediatric capability R R
24h/dforallrequests R R
In dose proximity to PICU 0 0Bedside urgent drug dosage form R R
Physical therapy department R 0Physical facility: external
Distinct, separate unit R R
Controlled access (no through traffic) R R
Proximity toElevators R 0Operating room 0 0Emergency department 0 0Recovery room 0 0MD on-call room R 0Nurse Manager’s office 0 0Medical Director’s office 0 0Waiting room R R
Separate roomsFamily counseling room R RConference room 0 0Staff lounge 0 0Staff locker room 0 0Patients’ personal effects storage (may be internal) R R
Physical facility: internal
Patient isolation capacity R R
Patient privacy provision R R
Medication station with drug refrigerator and locked narcotics cabinet R R
Emergency equipment storage R RClean utility (linen) room R R
Soiled utility (linen) room R R
Nourishment station R R
Counter, cabinet space R R
Staiftoilet R R
Patient toilet R RHandwasbing facility R R
Clocks R RTelevisions, radios R 0Easy, rapid access to head of bed R RThrelve or more compressed air outlets/bed R RTwo oxygen outlets/bed R R
Two or more compressed air outlets/bed R R
Two vacuum outlets/bed R R
Computerized laboratory reporting or efficient equivalent R 0Building code or federal code conforming
Heating, ventilation, air conditioning R R
Firesafety R R
Electrical grounding R R
AMERICAN ACADEMY OF PEDIATRICS 169 by guest on August 24, 2018www.aappublications.org/newsDownloaded from
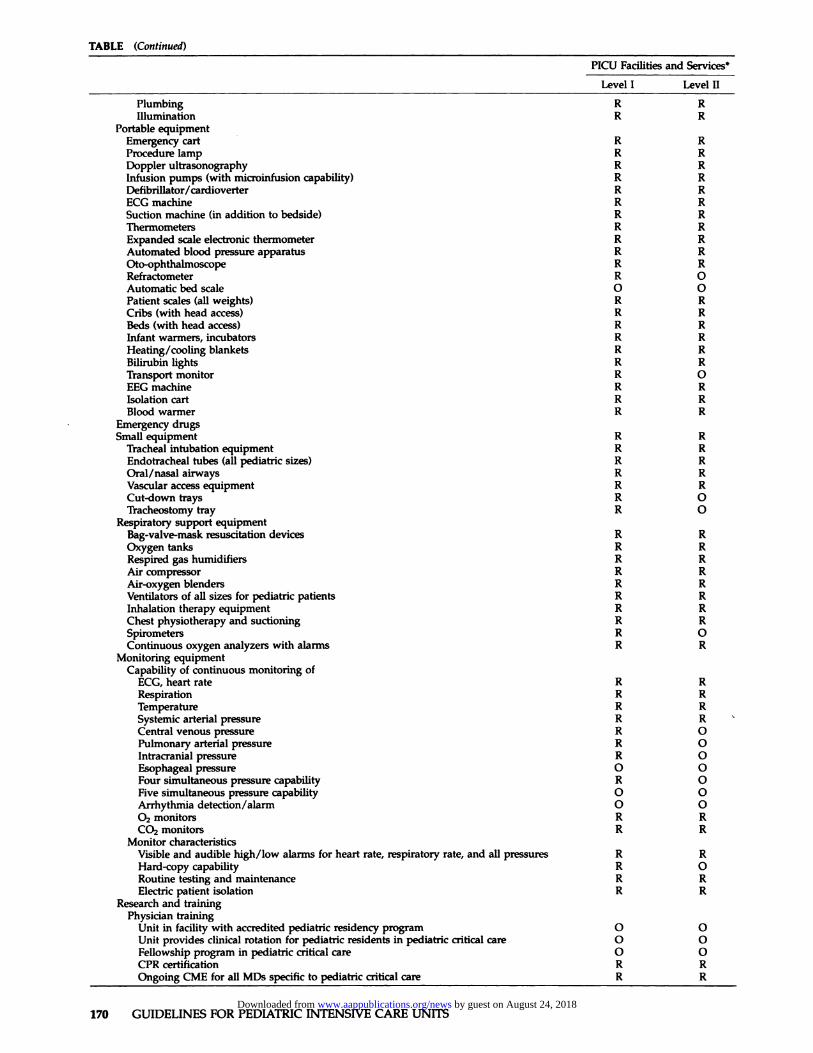
TABLE (Continued)
PICU Facilities and Services*
Level I Level H
Plumbing R Rifiumination R R
Portable equipment
Emergency cart R R
Procedure lamp R RDoppler ultrasonography R Rinfusion pumps (with mkrth�fusion capability) R R
Defibrillator/cardioverter R R
ECG machine R R
Suction machine (in addition to bedside) R RThermometers R R
Expanded scale electronic thermometer R RAutomated blood pressure apparatus R ROto-ophthalmoscope R RRefractometer R 0Automatic bed scale 0 0
Patient scales (all weights) R RCribs (with head access) R RBeds (with head access) R R
Infant warmers, incubators R R
Heating/cooling blankets R R
Bilirubin lights R RTransport monitor R 0
EEC machine R RIsolation cart R RBlood warmer R R
Emergency drugsSmall equipment R R
Tracheal intubation equipment R R
Endotracheal tubes (all pediatric sizes) R ROral/nasal airways R RVascular access equipment R RCut-down trays R 0Tracheostomy tray R 0
Respiratory support equipmentBag-valve-mask resuscitation devices R ROxygen tanks R R
Respired gas humidifiers R RAir compressor R R
Air-oxygen blenders R R
Ventilators of all sizes for pediatric patients R R
Inhalation therapy equipment R RChest physiotherapy and suctioning R RSpirometers R 0Continuous oxygen analyzers with alarms R R
Monitoring equipmentCapability of continuous monitoring of
ECG, heart rate R RRespiration R RTemperature R R
Systemic arterial pressure R R
Central venous pressure R 0Pulmonary arterial pressure R 0Intracranial pressure R 0Esophageal pressure 0 0Four simultaneous pressure capability R 0Five simultaneous pressure capability 0 0Arrhythmia detection/alarm 0 002 monitors R RC0� monitors R R
Monitor characteristics
Visible and audible high/low alarms for heart rate, respiratory rate, and all pressures R RHard-copy capability R 0Routine testing and maintenance R RElectric patient isolation R R
Research and training
Physician training
Unit in facility with accredited pediatric residency program 0 0Unit provides clinical rotation for pediatric residents in pediatric critical care 0 0Fellowship program in pediatric critical care 0 0CPR certification R ROngoing CME for all MDs specific to pediatric critical care R R
170 GUIDELINES FOR PEDIATRIC INTENSIVE CARE UNITS by guest on August 24, 2018www.aappublications.org/newsDownloaded from
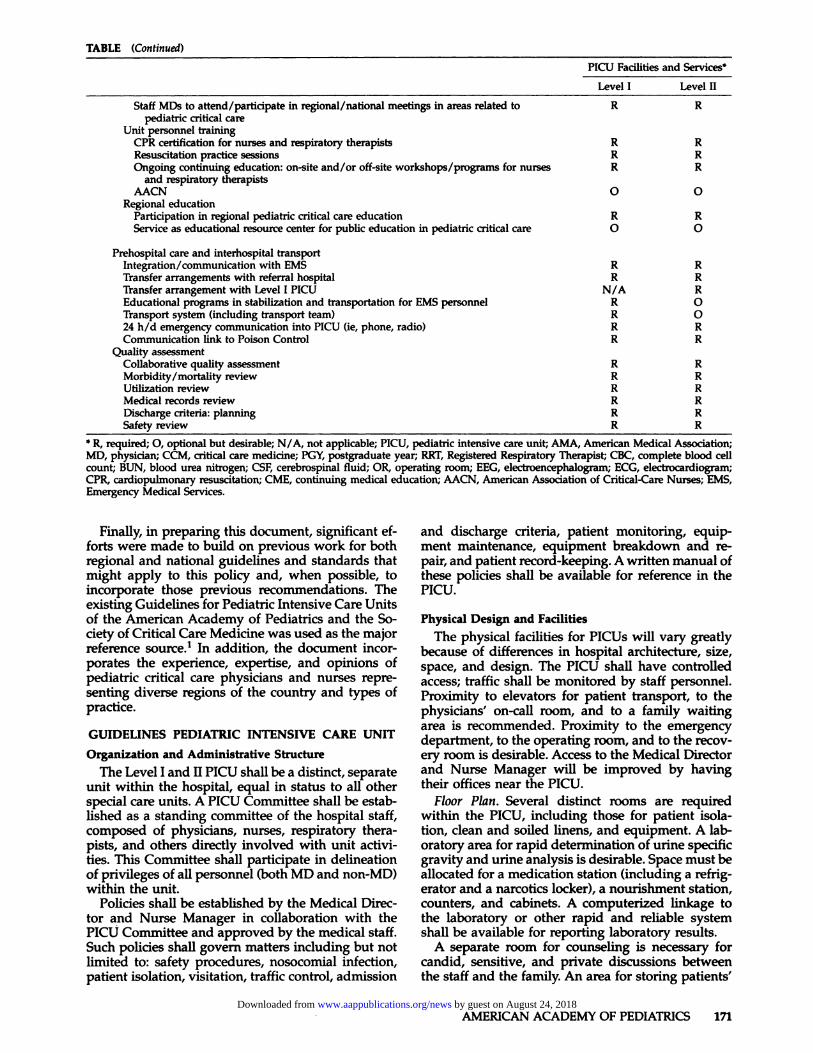
TABLE (Continued)
AMERICAN ACADEMY OF PEDIATRICS 171
PICU Facilities and Service?
Level I Level H
Staff MDs to attend/participate in regional/national meetings in areas related to R Rpediatric critical care
Unit personnel trainingCPR certification for nurses and respiratory therapists R R
Resuscitation practice sessions R R
Ongoing continuing education: on-site and/or off-site workshops/programs for nurses R Rand respiratory therapists
AACN 0 0Regional education
Participation in regional pediatric critical care education R R
Service as educational resource center for public education in pediatric critical care 0 0
Prehospital care and interhospital transportIntegration/communication with EMS R R
Transfer arrangements with referral hospital R RTransfer arrangement with Level I P1W N/A REducational programs in stabilization and transportation for EMS personnel R 0Transport system (including transport team) R 024 h/d emergency communication into PICU (ie, phone, radio) R RCommunication link to Poison Control R R
Quality assessmentCollaborative quality assessment R RMorbidity/mortality review R R
Utilization review R RMedical records review R R
Discharge criteria: planning R RSafety review R R
* R, required; 0, optional but desirable; N/A, not applicable; PICU, pediatric intensive care unit; AMA, American Medical Association;
MD, physician; CCM, critical care medicine; PGY, postgraduate year; RRT, Registered Respiratory Therapist; CBC, complete blood cellcount; BUN, blood urea nitrogen; CSF, cerebrospinal fluid; OR, operating room; EEC, electroencephalogram; ECG, electrocardiogram;CPR, cardiopulmonary resuscitation; CME, continuing medical education; AACN, American Association of Critical-Care Nurses; EMS,Emergency Medical Services.
Finally, in preparing this document, significant ef-forts were made to build on previous work for bothregional and national guidelines and standards thatmight apply to this policy and, when possible, toincorporate those previous recommendations. Theexisting Guidelines for Pediatric Intensive Care Unitsof the American Academy of Pediatrics and the So-ciety of Critical Care Medicine was used as the majorreference source.’ In addition, the document incor-porates the experience, expertise, and opinions ofped iatric critical care physicians and nurses repre-senting diverse regions of the country and types ofpractice.
GUIDELINES PEDIATRIC INTENSIVE CARE UNIT
Organization and Administrative Structure
The Level I and II PICU shall be a distinct, separateunit within the hospital, equal in status to all otherspecial care units. A PICU Committee shall be estab-lished as a standing committee of the hospital staff,composed of physicians, nurses, respiratory thera-pists, and others directly involved with unit activi-ties. This Committee shall participate in delineationof privileges of all personnel (both MD and non-MD)within the unit.
Policies shall be established by the Medical Direc-tor and Nurse Manager in collaboration with thePICU Committee and approved by the medical staff.Such policies shall govern matters including but notlimited to: safety procedures, nosocomial infection,patient isolation, visitation, traffic control, admission
and discharge criteria, patient monitoring, equip-ment maintenance, equipment breakdown and re-pair, and patient record-keeping. A written manual ofthese policies shall be available for reference in thePICU.
Physical Design and Facilities
The physical facilities for PICUs wifi vary greatlybecause of differences in hospital architecture, size,space, and design. The PICU shall have controlledaccess; traffic shall be monitored by staff personnel.Proximity to elevators for patient transport, to thephysicians’ on-call room, and to a family waitingarea is recommended. Proximity to the emergencydepartment, to the operating room, and to the recov-ery room is desirable. Access to the Medical Directorand Nurse Manager will be improved by havingtheir offices near the PICU.
Floor Plan. Several distinct rooms are requiredwithin the PICU, including those for patient isola-tion, clean and soiled linens, and equipment. A lab-oratory area for rapid determination of urine specificgravity and urine analysis is desirable. Space must beallocated for a medication station (including a refrig-erator and a narcotics locker), a nourishment station,counters, and cabinets. A computerized linkage tothe laboratory or other rapid and reliable systemshall be available for reporting laboratory results.
A separate room for counseling is necessary forcandid, sensitive, and private discussions betweenthe staff and the family. An area for storing patients’
by guest on August 24, 2018www.aappublications.org/newsDownloaded from
172 GUIDELINES FOR PEDIATRIC INTENSIVE CARE UNITS
personal effects also is required. A lounge, lockerspace, and conference area for staff personnel arehighly desirable and could be located either inside oroutside the unit. A staff toilet is required.
Bedside Facilities. The head of each bed or crib shallbe rapidly accessible for emergency airway manage-ment. Electrical power, oxygen, medical compressedair, and vacuum outlets sufficient in number to sup-ply all necessary equipment will meet local code orother accrediting requirements. In most cases 12 ormore electrical outlets and a minimum of two com-pressed air outlets, two oxygen outlets, and two vac-uurn outlets will be necessary. Reserve emergencypower and gas supply is essential. All outlets, heat-ing, ventilation, air conditioning, fire safety, electricalgrounding, plumbing, and illumination must adhereto all appropriate local, state, and national codes.Walls or curtains must be provided to ensure pa-tients’ privacy. Clocks shall be visible to both patientsand staff.
Personnel
Medical Director. A Medical Director shall be ap-pointed. A record of the appointment and acceptanceshould be in writing. Medical Directors of Level IPICUs must be: (1) Board-certified in pediatrics andboard-certified or in the process of certification inPediatric Critical Care Medicine; (2) board-certifiedin anesthesiology with practice limited to infants andchildren and with special qualifications (as definedby the American Board of Anesthesiology) in criticalcare medicine; or (3) board-certified in pediatric sur-gery with added qualifications in surgical criticalcare medicine (as defined by the American Board ofSurgery). Medical Directors must achieve certifica-tion within 5 years of their initial acceptance into thecertification process for critical care medicine. ForLevel II PICUs the Medical Director does not need tobe board-certified or eligible in critical care medicine.
The Medical Director shall participate in develop-ing and reviewing PICU policies, promote policy im-plementation, participate in budget preparation, helpcoordinate staff education, maintain a databasewhich describes unit experience and performance,supervise resuscitation techniques, lead quality fin-provement activities, and coordinate research. 0th-ers may supervise these activities, but the MedicalDirector shall participate in each.
The Medical Director shall name qualified substi-tutes to fulfill his or her duties during absences. TheMedical Director or designated substitute shouldhave the institutional authority to consult on the careof all PICU patients when indicated. He or she may
serve as the Attending Physician on all, some, ornone of the patients in the unit.
Physician Staff. The PICUs must have at least onephysician of at least the postgraduate year 2 levelassigned to the PICU in-house 24 hours per day. Aphysician in-house at the postgraduate year 3 level orabove in pediatrics or anesthesiology is strongly rec-ommended for all units caring for critically ifi chil-dren. Depending on the unit size and patient popu-lation, more physicians at higher training levels maybe required. Other physicians including the Attend-
ing Physician or his or her designee shall be availablewithin 30 minutes. For Level I units, available phy-sicians must indude a pediatric anesthesiologist, apediatric surgeon, a neurosurgeon (preferably withdemonstrated training and experience in pediatrics),
an otolaryngologist, an orthopedic surgeon, a cardio-thoracic surgeon (preferably with demonstratedtraining and experience in pediatrics), a pediatric in-tensivist, a pediatric cardiologist, a pediatric neurol-ogist, a radiologist, a pathologist, and a psychiatristor psychologist. It is desirable to have available onshort notice a craniofacial (plastic) surgeon, an oralsurgeon, a pediatric pulmonologist, a pediatrichematologist/oncologist, a pediatric endocrinologist,a pediatric gastroenterologist, and a pediatric aller-gist or immunologist. For Level II PICUs, a cardio-thoracic surgeon and pediatric subspecialists are not
Nursing Staff. A Nurse Manager dedicated to thePICU shall be available to all Level I PICUs. TheNurse Manager shall be supervised by the Directorof Pediatric Nursing (or equivalent) and shall havespecific training and experience in pediatric criticalcare; certification by the American Association ofCritical-Care Nurses is desirable. The Nurse Man-ager shall participate in the development of written
policies and procedures for the PICU, coordination ofstaff education, coordination, or research, and budgetpreparation with the Medical Director, in collabora-tion with the PICU Committee. The Nurse Managershall name qualffied substitutes to fulfill his or her
duties during absences.Nurse-to-patient ratios vary with patient needs,
usually ranging from 2 to 1 to I to 3. Required skillsfor PICU nurses include: recognition, interpretation,and recording of various physiologic variables, drugadministration, fluid administration, resuscitation(including cardiopulmonary resuscitation certifica-tion), respiratory care techniques (chest physiother-apy, endotracheal suctioning and management, tra-cheostomy care), preparation and maintenance ofpatient monitors, and psychosocial skills to meet theneeds of both patient and family.
The nursing organization shall provide a preparedorientation for new staff members. The nursing or-ganization shall also provide a nurse educatorand/or clinical nurse specialist for in-service pro-grams in pediatric critical care.
Respiratory Therapy Staff. The Respiratory TherapyDepartment shall have a supervisor responsible forperformance and training of staff, maintaining
equipment, and monitoring quality improvementand review. Under the supervisor’s direction, respi-ratory therapy staff assigned primarily to the Level IPICU shall be in-house 24 hours per day. Level IIPICUs require a respiratory therapist in-house at alltimes but do not require one assigned primarily tothe PICU 24 hours per day.
Ancillary Support Personnel. Biomedical techni-cians shall be either in-house, or available within Ihour, 24 hours per day for both Level I and II PICUs.Unit secretaries (derks) shall be in the Level I P1W24 hours per day. A pharmacist and radiology tech-
by guest on August 24, 2018www.aappublications.org/newsDownloaded from
AMERICAN ACADEMY OF PEDIATRICS 173
nician must be in-house 24 hours per day in Level IPICUs. In addition, social workers, physical thera-pists, occupational therapists, and nutritionists mustbe available. The availability of child life specialists
and clergy is strongly encouraged.
Hospital Facilities and Services
The Level I PICU shall be located in a Category Ifacility as defined by the American Medical Associ-ation. The Emergency Department shall have a sep-arate, covered entrance. An adjacent helipad is verydesirable. Two or more areas within the EmergencyDepartment shall have the capacity and equipmentto resuscitate any pediatric patient with medical, sur-gical, or traumatic illness in hospitals with a Level IPICU. Hospitals with Level II units need only one
such area. The Emergency Department shall bestaffed by physicians 24 hours per day in all hospitalswith PICUs.
The hospital operating suite shall have at least oneroom available within 30 minutes 24 hours per dayand a second room available within 45 minutes. Ca-pabilities in the operating room in hospitals withLevel I PICUs must include cardiopulmonary by-pass, pediatric bronchoscopy, endoscopy, and radi-ography.
The Blood Bank must have all blood componentsavailable 24 hours per day in hospitals with either aLevel I or II PICU. Unless some unusual antibody isencountered, blood typing and cross-matching shallallow transfusion within I hour.
Radiology services in hospitals with Level I PICUsmust include portable radiography, fluoroscopy,computerized tomography scanning, ultrasonogra-phy, nuclear scanning angiography. Magnetic reso-nance imaging and radiation therapy are desirablebut not required.
The clinical laboratories shall have microspecimencapability and 1-hour turnaround time for dottingstudies and for measurements of complete blood cellcount, differential count, platelet count, urinalysis,electrolytes, blood urea nitrogen, creatinine, glucose,calcium, prothrombin time, partial prothrombintime, and cerebrospinal fluid cell counts. Blood gasvalues must be available within 15 minutes. Resultsof drug screening and levels of serum ammonia, se-rum and urine osmolarity, phosphorus, and magne-sium shall all be available within 3 hours for Level IPICUs. Preparation of Gram stains and bacteriologiccultures shall be available 24 hours per day.
The hospital pharmacy must be capable of dis-pensing all necessary medications for pediatric pa-tients of all types and ages 24 hours per day. A sat-effite pharmacy close to the unit is desirable. At eachbedside there should be a form that lists urgent and
resuscitation drugs, complete with dosages appropri-ate for the individual patient.
Diagnostic cardiac and neurologic studies shall beavailable for infants and children in hospitals withLevel I PICUs. Electrocardiograms, two-dimensionaland M-mode echocardiograms, and electroencepha-lograms shall be available within 30 minutes of beingrequested. A catheterization laboratory or angiogra-phy suite must be present. Doppler ultrasonography
devices and evoked potential monitoring equipmentare optional. Hemodialysis equipment and techni-cians experienced with children should be available24 hours per day.
Hospital facilities shall include a comfortable wait-ing room, private consultation areas, a place to eat, aconference area, and preferably sleeping accommo-dations for patients’ families.
Drugs and Equipment
Drugs for resuscitation and pediatric advanced lifesupport must be present and immediately availablefor any patient in the PICU. These shall include atleast atropine, epinephrine, sodium bicarbonate, glu-cose, calcium chloride, lidocaine, bretylium, dopam-ine, dobutamine, isoproterenol, and mannitol. Otherdrugs which should be immediately available in-dude, but are not limited to, diazepam, neuromus-cular relaxant, narcotic analgesic, naloxone, pheny-toin, and diazoxide.
The life-saving, therapeutic, and monitoringequipment detailed below must be present or imme-diately available in each Level I PICU.
Portable Equipment. Portable equipment shall in-dude an emergency (“code” or “crash”) cart, a pro-cedure lamp, sphygmomanometers for systemic ar-terial blood pressure determination, a Dopplerultrasonography device, an electrocardiograph, adefibrillator/cardioverter, thermometers (with arange sufficient to identify extremes of hypothermiaand hyperthermia), an automated blood pressure ap-paratus, devices for accurate measuring of bodyweight, cribs and beds with head access, infantwarmers, heating and cooling blankets, bilirubinlights, pacemakers, a blood-warming apparatus, anda transport monitor. A suitable number of infusionpumps with microcapabifity (0.1 mL/h) must beavailable. Oxygen tanks are needed, both for trans-port and for backup of the central oxygen supply.Similarly, portable suction machines are needed fortransport and backup. Volumetric infusion pumps,air-oxygen blenders, an air compressor, gas humidi-fiers, bag-valve-mask resuscitators, an otoscope/ophthalmoscope, and isolation carts must be readilyavailable. A portable electroencephalographic ma-chine must be available in the hospital for recordingsinside the Level I PICU.
Additional equipment such as a refractometer,flashlights, and automated (metabolic) bed scales arevery helpful but not required. Televisions, radios,and rocking chairs shall be available for patients whowould benefit from their use.
Small Equipment. Certain small equipment must beimmediately available at all times. Such equipmentincludes: suction catheters, tracheal intubationequipment (laryngoscope handles, sizes, and types ofblades adequate to intubate patients of all ages, Mag-ill forceps), endotracheal tubes of all sizes (cuffed anduncuffed), oral and nasal airways, central cathetersfor vascular access, thoracostomy tubes, and surgicaltrays for cutdowns, open-chest procedures, and tra-cheostomies.
Respiratory Equipment. Mechanical ventilators suit-able for pediatric patients must be available for each
by guest on August 24, 2018www.aappublications.org/newsDownloaded from

174 GUIDELINES FOR PEDIATRIC INTENSIVE CARE UNITS
Level I PICU bed. Equipment for chest physiother-apy and suctioning, spirometers, and oxygen analyz-ers must always be available for every patient. Oxy-gen monitors (pulse oximeters, transcutaneousoxygen monitors, ear oximeters) are required; CO2monitors (transcutaneous, end-tidal) and portable(transport) ventilators are desirable.
Bedside Monitors. Bedside monitors in all PICUsmust have the capabifity for continuously monitor-ing heart rate and rhythm, respiratory rate, temper-ature, and one hemodynamic pressure. Bedside mon-itoring in Level I PICUs also must be capable ofsimultaneously monitoring systemic arterial, centralvenous, pulmonary arterial, and intracranial pres-sures. Arrhythmia detection and capability for a fifthsimultaneous pressure measurement are helpful butnot essential. These monitors must have high andlow alarms for heart rate, respiratory rate, and allpressures. The alarms must be both audible and vis-ible. A permanent hard copy of the rhythm strip mustbe available in Level I PICUs. Hard copy capabilityfor all monitored variables is desirable. All monitorsmust be maintained and tested routinely.
Prehospital Care
Often patients who are admitted to the PICU re-quire transport from an accident scene, another hos-pital, or an emergency at home, playground, orschool. Accordingly, PICUs shall be integrated withthe regional EMS system. The method of communi-cation may vary, but a standard, written approach toemergencies involving both the EMS system and thePICU shall be prepared. All Level I PICUs must havemultiple telephone lines so that outside calls can bereceived even at very busy times. Rapid access to aPoison Control Center is essential.
Each Level I PICU must endeavor to meet theneeds of other hospitals less well-equipped to handlecertain types of care. Formal transfer arrangementsare encouraged, but in many areas informal agree-ments have proved satisfactory. Each PICU shallhave or be affiliated with a transport system andteam to assist other hospitals in arranging safe pa-tient transport.
Policies shall describe mechanisms which achievesmooth and timely exchange of patients betweenemergency department, operating room, imaging fa-cilities, special procedure areas, regular inpatientcare areas, and the PICU.
Quality Assessment
The PICU must employ a collaborative quality as-sessment process. Objective methods should be usedto compare observed and predicted mortality ratesfor the severity of ifiness in the population examined.
Training and Continuing Education
Each PICU shall train health care professionals inbasic aspects of pediatric critical care and serve as afocus for continuing education programs in Pediatric
Critical Care. In addition, all staff working in thePICU should routinely attend or participate in re-gional and national meetings with course contentpertinent to pediatric critical care.
Many Level I PICUs will possess sufficient patient
volume, teaching expertise, and research capabilityto support a Fellowship Program in Pediatric CriticalCare. Programs providing subspecialty training incritical care must possess approval by the ResidencyReview Committee (RRC) of the Accreditation Coun-cil on Graduate Medical Education (ACGME).
Nurses and respiratory therapists must have BasicLife Support certification, must participate in resus-
citation practice sessions, and should be encouragedand supported to attend appropriate on-site or off-site educational programs.
Each Level I PICU shall participate in regional pe-diatric critical care education for EMS providers, foremergency department and transport personnel, andfor the general public. Some PICUs wifi be suited toserve as an educational resource center for publiceducation in areas pertinent to pediatric critical care.
Research is essential for improving our under-standing of the pathophysiology affecting vital organsystems. Such knowledge is vital to improve patientcare techniques and therapies and thereby decreasemorbidity and mortality. Every Level I PICU canserve as a laboratory for clinical research. Obviously,larger Level I PICUs will be better able to providesuch a forum, but even small units contain patients ofwhom observations can be made and important ob-servations reported.
Co�iri-r� or�i HOSPITAL Ciuu�, 1992 to 1993James E. Shira, MD, ChairpersonJess Diamond, MDMary E. O’Connor, MDRussell C. Raphaely, MDMarleta Reynolds, MDHenry A. Schaeffer, MDRichard S. Woff, MD
Li#usor� REPREsENTATIvEs
Ross R. Black, American Academy ofFamily Physicians
Mary Perkins, RN, DNSC, Society ofPediatric Nurses
Barbara-Jeanne Seabury� Association forthe Care of Children’s Health
Russell K. Tolman, National Associationof Children’s Hospitals andRelatedInstitutions
Paul R. VanOstenberg, DDS, MS, JointCommission on AccreditationofHealthcare Organizations
Stuart W. Williams, American HospitalAssociation
AAP SECrION Li,usot�iTheodore Striker, MD, Section on
Anesthesiology
PEDIATRIC SECTION, SOCIETY OF CRiTICAL C�uu�MEDICINE ADVISORY Co�.o�uu�, 1992 to1993
J. Michael Dean, MD, ChairmanDebra H. Finer, MD,
Secretary/Chairman-electDaniel A. Notterman, MD,
Member-at-large
Jayant K. Deshpande, MD,Member-at-large
by guest on August 24, 2018www.aappublications.org/newsDownloaded from

AMERICAN ACADEMY OF PEDIATRICS 175
Thomas P. Green, MD, Member-at-largeAnn E. Thompson, MD, Past chairman
PICU GUIDELINES SUBcOMMrfrEE
Curt M. Steinhart, MDMurray M. Pollack, MDLucian DiNicola, MDFrank R. Gioia, MDStephen D. Levine, MDRobert R. Moody, MDWiffiam H. Perloff, MDSims M. Sconyers, MD
Charles L Shabino, MDFernando Stein, MDSamuel J. Tilden, MDJoseph A. Weinberg, MD
REFERENCES
1. American Academy of Pediatrics, Committee on Hospital Care and
Pediatric Section of the Society ofCritical Care Medicine. Guidelines for�iatric intensive care units. Pediatrics. 1983;72:364-371 and Crit Care
Med. 1983;11:753
by guest on August 24, 2018www.aappublications.org/newsDownloaded from
1993;92;166Pediatrics Guidelines and Levels of Care for Pediatric Intensive Care Units
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/92/1/166including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlentirety can be found online at: Information about reproducing this article in parts (figures, tables) or in its
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on August 24, 2018www.aappublications.org/newsDownloaded from
1993;92;166Pediatrics Guidelines and Levels of Care for Pediatric Intensive Care Units
http://pediatrics.aappublications.org/content/92/1/166the World Wide Web at:
The online version of this article, along with updated information and services, is located on
Copyright © 1993 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.been published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
by guest on August 24, 2018www.aappublications.org/newsDownloaded from