
GOVERNING BODY MEETING - Wirral CCG › media › 4477 › governing-body...GOVERNING BODY MEETING...
51
GOVERNING BODY MEETING – A meeting in public Tuesday 10 th April 2018 Pacific Road Art Centre, 1 Pacific Rd, Birkenhead CH41 1LJ 1pm - 2pm AGENDA Ref No. No Time Item Action Papers GB17- 18/00 75 1. 1.00p m PRELIMINARY BUSINESS/ADMINISTRATIVE ITEMS (Chair) 1.1 Apologies for Absence 1.2 Chair’s Announcements To Inform 1.3 Declarations of Interest 1.4 Welcome and Comments/questions from members of the public (10 mins) 1.5 Minutes and Action Points of Last Meeting 6 th March 2018 Action Points To Approve 3 DRAFT WCCG Governing Body PUBL 3a. GB Action Log .pdf 1.6 Matters Arising To Inform 1.7 Chief Officer’s Update (Simon Banks) To Inform/ Assure 4. Chief Officer Report April 2018.doc GB17- 18/00 76 3. 1.30p m FINANCE 3.1 Chief Financial Officer’s Report (Mike Treharne) To Assure/ Endorse 5. Report cover sheet Finance GB.docx 5a. GB finance report.docx 5b. Copy of Appendix 1 Finance Co 5c. Copy of Appendix 2 1718 M11 WUTH Fin GB17- 18/00 77 4. 1.50p m PERFORMANCE AND COMMISSIONING NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 1 of 51
Transcript of GOVERNING BODY MEETING - Wirral CCG › media › 4477 › governing-body...GOVERNING BODY MEETING...
GOVERNING BODY MEETING – A meeting in public
Tuesday 10th April 2018
Pacific Road Art Centre, 1 Pacific Rd, Birkenhead CH41 1LJ
1pm - 2pm
AGENDA
Ref No.
No Time Item Action Papers
GB17-18/0075
1. 1.00pm
PRELIMINARY BUSINESS/ADMINISTRATIVE ITEMS (Chair)
1.1 Apologies for Absence 1.2 Chair’s Announcements To
Inform
1.3 Declarations of Interest 1.4 Welcome and
Comments/questions from members of the public (10 mins)
1.5 Minutes and Action Points of Last Meeting
6th March 2018
Action Points
To Approve
3 DRAFT WCCG Governing Body PUBL
3a. GB Action Log .pdf
1.6 Matters Arising To Inform
1.7 Chief Officer’s Update (Simon Banks)
To Inform/ Assure
4. Chief Officer Report April 2018.doc
GB17-18/0076
3. 1.30pm
FINANCE
3.1 Chief Financial Officer’s Report (Mike Treharne)
To Assure/ Endorse
5. Report cover sheet Finance GB.docx
5a. GB finance report.docx
5b. Copy of Appendix 1 Finance Co
5c. Copy of Appendix 2 1718 M11 WUTH Fin
GB17-18/0077
4. 1.50pm
PERFORMANCE AND COMMISSIONING
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 1 of 51
Ref No.
No Time Item Action Papers
4.1 Improving Access to Psychological Services (IAPT) Update (Nesta Hawker)
To Approve
6. Governing Body Report Cover Sheet -
6a. Governing Body Report April 2018 Fina
6b. appendix 1 - March IAPT projection
6c. Appendix 2 - IAPT Wirral Capacity Optio
6d. Appendix 3 IAPTCommunications a
6e. Appendix 4 Draft risk sharing agreemen
4.2 Public Health – Hypertension (Julie Webster)
To Inform
HYPERTENSION7. CCG CB cover sheet B
7a. BP PROJECT INTERIM REPORT JH v
GB17-18/0078
5. 3.40pm
ANY OTHER BUSINESS
Communications from this meeting
Date and Time of Next Meeting:
Tuesday 8th May 2018 (Formal), Exmouth Suite, The Lauries Centre, Birkenhead Please send any apologies to [email protected]
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 2 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
NHS WIRRAL CLINICAL COMMISSIONING GROUP
Governing Body Meeting Minutes of Meeting – Public Session
Tuesday 6th March 2018
1pm – 3.30pm Nightingale Room, Old Market House
Present: Dr Sue Wells (SW) (Chair) Chair WCCG Simon Banks (SB) Chief Officer Michael Treharne (MT) Chief Financial Officer Paul Edwards (PE) Director of Corporate Affairs Nesta Hawker (NH) Director of Commissioning Sylvia Cheater (SC) Lay Member (Patient Champion) Alan Whittle (AW) Lay Member (Audit & Governance) Lorna Quigley (LQ) Director of Quality & Patient Safety Dr Laxman Ariaraj (LA) GP Lead – Planned Care Dr Paula Cowan (PC) Medical Director Dr Helen Downs (HD) GP Lead – Unplanned Care Dr Simon Delaney (SD) GP Lead – Primary Care Dr Sian Stokes (SS) GP Lead – Long Term Conditions Dr James Sowery (JS) Chair, Membership Council Linda Roberts (LR) Lay Member (Quality) Dr Richard Sturgess (RS) Secondary Care Doctor In Attendance: Grace Price – Jones (GPJ) Senior Corporate Officer Jo Watts (JWat) Senior Commissioning Manager – Mental Health
Ref No.
Minute Action
GB17-18/0066
Preliminary Business 1.1 Apologies for absence: Apologies were received by Lesley Doherty, Dr Richard Williams, Julie Webster and Graham Hodkinson.
1.2 Chairs Announcements/Opening Remarks The Chair welcomed all attendees to today’s meeting, and noted that no members of the public were in attendance. The Chair reminded the members that there will be a change to th e dates of the Governing Body Meetings from April 2018 and these will now take place on the second Tuesday of the month to allow for the flow of papers from subcommittees to be improved. 1.3 Declarations of Interest The Chair reminded the Governing Body members of their obligations to declare any interest they may ha ve on any items arising at that might conflict with t he business of NHS Wirral CCG.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 3 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
Ref No.
Minute Action
JS declared an interest in item number 4.1 the Wirral Palliative and End of Life Ca re Strategy 2017-2021, as his spouse was the CCG’s clinical lead in th is area. The Chair advised that she was comfortable for JS to remain in the room throughout the discussion but that he would not participate in any decision making. 1.4 Comments/questions from members of the public There were no members of the public in attendance at the meeting. 1.5 Minutes & Action Points from previous meeting held on the 6th February 2018 Minutes The minutes of the previous meeting held on 6 th February 2018 were agreed as a tru e account of the meeting. It was noted that an action within the minutes was omitted from the action log. Action Points Members reviewed the outstanding actions recorded on the action log and noted th e updates provided on the progress to date. AP 28 - it was noted that this piece of work is being prod uced jointly with the Local Authority and will be submitted to the Shadow Joint Strategic Commissioning Board for consideration. It was agreed that the due date should be revised to after this meeting has taken place. Due date updated to July in the interim. AP 29 - it was agreed that as the updates are included wit hin the Director of Corporate Affairs report that this action can now be closed. AP 32 - the Chair reminded the Governing Body of the importance of providing updates to any outstanding actions. It was agreed that this action can now be closed as it should be business as usual. AP 33 - The Governin g Body were informed that the be nchmarking information is included within the Director of Quality and Pati ent Safety update. As a result, it wa s agreed that this action can now be closed. 1.6 Matters Arising There were no matters arising discussed by the Governing Body. AW advised that the Fraud Inspectio n scheduled by Mersey Internal Audit Agency was postponed due to staffing issues on their part. 1.7 Patient Story A transcript was playe d which described a gentleman’s experience of being referred under the two week rule and who was then diagnosed with prostate cancer. The patient explained his treatment and the services that are supporting him in the community. 1.8 Chief Officer’s Report The Governing Body reviewed and noted the report submitted. SB advised that he had attended the Chief Officers monthly meeting that morning. The Planning Guidance for 2018-19, which had just been published by NHS England (NHSE),
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 4 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
Ref No.
Minute Action
was discussed in d etail. There w as a prese ntation at t he meeting that provided information on the Operating Planning timetable, the key deliverables, local assura nce plans, information regarding the Better Care Fund and sanctions. It was also highlighted at the meeting that, from the latest data, demand in the winter period is not yet declining and that th ere is a high rate of f lu. SB agreed to distrib ute the pre sentation to the Governing Body for information. It was clear that financially the future will continu e to be a ch allenge and that there will be no additional winter funding in 2018/19. A separate winter demand and capacity plan will be required for 30th April 2018. ACTION: Presentation from the monthly Chief Officers’ meeting to be distributed to the Governing Body.
SB/GPJ
GB17-18/0067
2.1 Risk Register The Governing Body reviewed the Risk Register. PE gave an update on the discussions and recommendations from the February Quality and Performance (QP) Committee (where the risk register is considered in detail): 16-17C – An Action Pla n has been received by the Serious Incident Group, but some concerns remained and hence were raised at WUTH and CCG Board to Board held on 17th February 2018. The CCG is also planning to undertake a quality and safety visit on 27th February 2018. Until outcome of this and feedback following Board to Board are known, scores proposed to remain the same. 16-17D – The RTT Strategic Board has met and additional funding from NHS England to undertake audit has been agreed. Harm reviews have also been undertaken. No change to scores was proposed and will be next due for review at March 2018 QP. 17/18A – Based on discussion at Finance Committee, members agreed that this action should be closed becau se the CCG cannot ac hieve a break even financial position. A new risk was propose d based on a revised forecast of a £9.8m d eficit. It was recommended that the impact rema ins as a 4 as per previous risk and likelihood was proposed as 3. 17/18B – Still awaiting i nspection at present, so no change and next du e for review at April 2018 QP. 17/18C – LQ updated on Dynamic Purchasing System (Adam) at QP and stated patients, homes and local councillors are not satisfied with aspects of the system and hence this is a reputational risk and scores to remain the same, with LQ to look at CHC Programme Board risk register to ensure consistent approach to scoring risk by those CCGs who also use the Adam system. Next due for review at March 2018 QP. Governing Body accepted all the recommenda tions of QP and Finance committ ees around amendments to the Risk Register.
GB17-18/0068
3.1 Chief Financial Officer’s Report MT highlighted to the Governing Body the main headlines in the Finance report, at Month 10:
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 5 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
Ref No.
Minute Action
£9.23 million year to date deficit against Resource Limit. Year to date pressures continue to be within NHS Acute contracts predominantly
within the Wirral University Teaching Hospitals NHS FT contract £4.6m and the Liverpool Heart and Chest NHS FT contract £948k.
Continuing Healthcare and other packages of care overspending continues with a year to date pressure of £4.1m.
The CCG has reported a forecast out turn deficit of £9.8m t o NHS England as part of month 10 submissions which is consistent with the month 9 risk adjusted position.
There does however remain significant risk to the CCG in achieving th is £9.8m deficit if acute contracts and packages of care continue to overspend during the remaining months of the financial year.
There is also a further risk should the QIPP p rogramme including mitigating management and clinical actions fail to deliver the forecast savings.
MT advised the Governing Body that the forecast has been agreed by NHS England of a £9.8m deficit and there are still a number of areas that a re being worked on in an attempt to create a more favourable position at the end of the financial year. Finance Committee Chair’s report The Governing Body noted the briefing from the Chair of the Finance Committee. No further comments were made.
GB17-18/0069
4.1 Director of Commissioning’s Report The Governing Body noted the report submitted. NH highlighted the CCG’s delivery of the financial recovery plan and updated on the schemes that are included in it. NH discussed performance against the NHS Constitutional Standards and advised that the A&E and Walk-in centre perfor mance fell below national standard at 78.36%. The Urgent Care Operational Group and QP Committee will be completing some deep dives to investigate the levels of performance further. Referral to Treatment (RTT) has been affected due to winter pressures and, as elect ive activity was cance lled throughout January, there will be a further drop in performance. NH asked t he Governing Body to note the NHS England CCG Improvement and Assessment Dashboard. The Dashboard will be submitted to QP Committee. Wirral Palliative & End of Life Care Strategy 2017 - 2021 NH presented the End of Life Strategy to the Governing Body. The strategy has been developed by the Palliat ive & End o f Life Care Clinical Group and creates a focus to achieve the aspirations of both commissioners and providers. AW noted that the date on the Operational Plan requires updating. The strategy was approved. The implementation of the strategy will be overseen by QP Committee. Ambulance Performance Update
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 6 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
Ref No.
Minute Action
NH advised the Governing Body that the national standards on the ambulance response rate was changed last July and the paper outlines the current performance of North West Ambulance Service (NWAS). NH advised that this paper has been escalated to NHS England (NHSE) and NHS Improvement (NHSI) and the CCG a re awaiting an improvement plan. Con cerns in regards to th e delay in ambulance handovers were discussed. It was agreed by the Governing Body that a risk should be added due to the possible impact that the delay in handovers could have on patients. T his detail of this would be d iscussed at the next QP Co mmittee. It was queried h ow North West Ambulance Service (NWAS) categorise patien ts. NH advised that the r esponse will be reviewed by the QP Committee. ACTION: Risk to be raised at next QP following concerns in relation to the delays of ambulance handovers. Improving Access to Psychological Services (IAPT) Update Jo Watts, Senior Commissioning Manager - Mental Health, joined the meeting to provide the group with an update in regards to the IAPT performance and the future procurement process. JWat advised that the current IAPT provider contract is due to come to an end on the 30th June 2018. The provider has been advised that the contract is going to be re-procured. The secondary care provider contract is in place until March 2019. In an attempt to align both IAPT and Secondary mental health providers’ contracts, there were a number of recom mendations to align the re-pr ocurement processes. The recommended option to the group was to extend the curre nt IAPT provider until March 2019 to align with the secondary care provider contract term and then refresh the specifications to meet the CCG’s needs in line with the Commissioning Strategy. JWat advised that a quality impact assessment has been completed following the request at the February Private Governing Body. She also advised that the CCG has met with NHS England, NHS Improvement and the current provider to discuss performance. There was a reco gnition of the poor pe rformance but a positive conversation on h ow improvements can be made. There is an interim arrangement to clear the current waiting list which is part of the contract extension. JW at and LQ were asked to conduct harm reviews for the patients currently on the waiting list. ACTION: LQ and Jo Watts to produce a harm review on the current patient waiting list. A number of the Governing Body members e xpressed concerns about extending the contract for a provider that has been underperforming. JWat provided further assurance that the provider will be monitored and that an improvement schedule has been put into place. The Intensive Support Team will also continue to offer support. The contract will be monitored by QP Committee going forward. A vote was held on whether to extend the current contract to supp ort the future commissioning of an integrated service, as some concerns were raised given t he performance of the current provider. PC and HD abstained, but all other members presented voted in support. Therefore, the proposal was approved.
NH LQ/JWat
GB17-18/0070
5.1 Director of Quality and Patient Safety
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 7 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
Ref No.
Minute Action
The Governing Body noted the report submitted. Following the request at the last meeting LQ drew to Governing Body’s attention to the benchmarking data provided by Public Health regarding Health Care Acquired Infections. The Board to Board meeting with WUTH took place on the 15th February 2018. The CCG has written to WUTH formally with an assessment of its assurance in the areas covered at the meeting and the monitoring of the response will take place at the QP Committee once received. No further comments were made.
GB17-18/0071
6.1 Director of Corporate Affairs’ Report The Governing Body noted the report submitted. PE gave an update on the integration of commissioning with Wirral Council and advised that the development of the Commi ttee in Common was progressing w ith input fro m respective legal teams The Directors have also agreed pr ovisional portfolios and the plans for moves/IT works to support co-location were being developed. A staff briefing will be held on 20 th March 2018 t o update st aff from both organisations on the se developments. PE drew attention to Statutory and Mandatory Training compliance data. He stated that, having discussed at QP, he and Gareth James, HR Business Partne r, Midlands and Lancashire Commissioning Support Unit, would be invest igating reasons for no n-compliance before further action was taken.
GB17-18/0072
7.1 Medical Director’s Report PC advised the Govern ing Body that the Wirral Care Record and Health Information Exchange are rolling out across Wirral with 51 GP Practices now on board. The Health Information Exchange will be available to Secondary Care from next week. Clinical Senate Chair’s Report The Governing Body noted the report submitted. No further comments were made
GB17-18/0073
8.1 Committee Meeting Minutes The committee minutes were noted by the Governing Body. There were no further comments.
GB17-18/0074
9. Any Other Business No further business was discussed. Communications from this meeting The following points are to be communicated:
The extension of the Improving Access to Psychological Therapies contract. Approval of the Wirral Palliative and End of Care Strategy.
Date and Time of Next Public Meeting
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 8 of 51
Minutes – Wirral Governing Body Meeting PUBLIC SESSION – 6th March 2018
Ref No.
Minute Action
Date and time of next meeting: Tuesday 10th April 2018 1pm – 4pm, Exmouth Suite, The Lauries Centre, Birkenhead. Please forward any apologies to [email protected]
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 9 of 51
Item NoDate
Opened
Agenda
Item NoRef no Item of discussion Action Points
Responsibi
lityDate Due Status Status and progress (including updates)
Closure
dateOutcome of action
Requires
review?
Date of
review
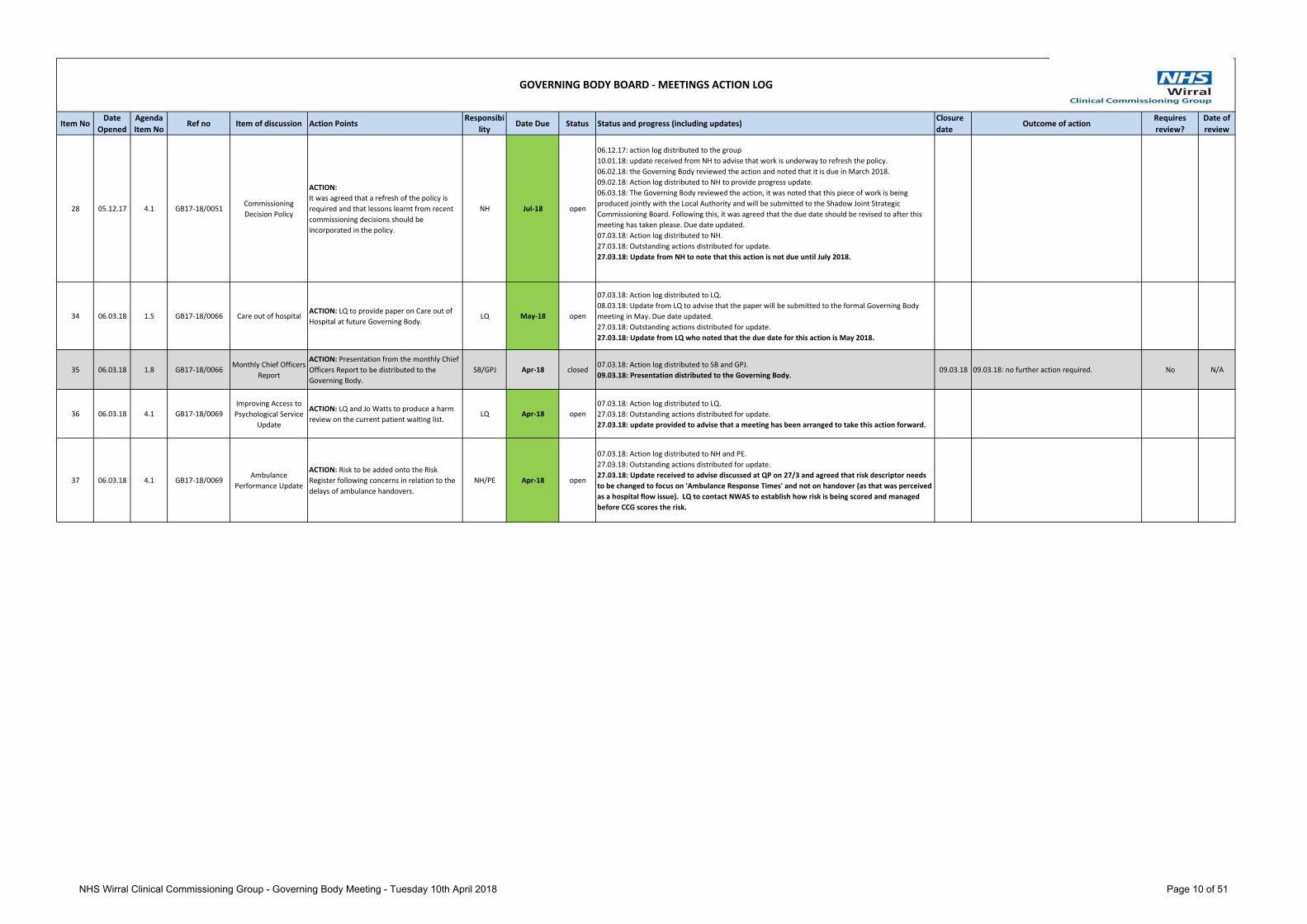
28 05.12.17 4.1 GB17-18/0051Commissioning
Decision Policy
ACTION:
It was agreed that a refresh of the policy is
required and that lessons learnt from recent
commissioning decisions should be
incorporated in the policy.
NH Jul-18 open
06.12.17: action log distributed to the group
10.01.18: update received from NH to advise that work is underway to refresh the policy.
06.02.18: the Governing Body reviewed the action and noted that it is due in March 2018.
09.02.18: Action log distributed to NH to provide progress update.
06.03.18: The Governing Body reviewed the action, it was noted that this piece of work is being
produced jointly with the Local Authority and will be submitted to the Shadow Joint Strategic
Commissioning Board. Following this, it was agreed that the due date should be revised to after this
meeting has taken please. Due date updated.
07.03.18: Action log distributed to NH.
27.03.18: Outstanding actions distributed for update.
27.03.18: Update from NH to note that this action is not due until July 2018.
34 06.03.18 1.5 GB17-18/0066 Care out of hospitalACTION: LQ to provide paper on Care out of
Hospital at future Governing Body. LQ May-18 open
07.03.18: Action log distributed to LQ.
08.03.18: Update from LQ to advise that the paper will be submitted to the formal Governing Body
meeting in May. Due date updated.
27.03.18: Outstanding actions distributed for update.
27.03.18: Update from LQ who noted that the due date for this action is May 2018.
35 06.03.18 1.8 GB17-18/0066Monthly Chief Officers
Report
ACTION: Presentation from the monthly Chief
Officers Report to be distributed to the
Governing Body.
SB/GPJ Apr-18 closed07.03.18: Action log distributed to SB and GPJ.
09.03.18: Presentation distributed to the Governing Body. 09.03.18 09.03.18: no further action required. No N/A
36 06.03.18 4.1 GB17-18/0069
Improving Access to
Psychological Service
Update
ACTION: LQ and Jo Watts to produce a harm
review on the current patient waiting list. LQ Apr-18 open
07.03.18: Action log distributed to LQ.
27.03.18: Outstanding actions distributed for update.
27.03.18: update provided to advise that a meeting has been arranged to take this action forward.
37 06.03.18 4.1 GB17-18/0069Ambulance
Performance Update
ACTION: Risk to be added onto the Risk
Register following concerns in relation to the
delays of ambulance handovers.
NH/PE Apr-18 open
07.03.18: Action log distributed to NH and PE.
27.03.18: Outstanding actions distributed for update.
27.03.18: Update received to advise discussed at QP on 27/3 and agreed that risk descriptor needs
to be changed to focus on 'Ambulance Response Times' and not on handover (as that was perceived
as a hospital flow issue). LQ to contact NWAS to establish how risk is being scored and managed
before CCG scores the risk.
GOVERNING BODY BOARD - MEETINGS ACTION LOG
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 10 of 51
GOVERNING BODY BOARD REPORT
Risk Please indicate Detail of Risk Description
High Medium Low
n/a
Clinical engagement taken place n/a
Patient and public involvement taken place n/a
Equality Analysis/Impact Assessment completed n/a
Quality Impact Assessment n/a
CHIEF OFFICER’S REPORT
Agenda Item: 1.7 Reference GB17-18/0075
Public / Private Public Meeting Date 10th April 2018
Lead Officer/Author of paper
Simon Banks, Chief Officer
Contributors Simon Banks, Chief Officer
To Approve
To Inform Yes
To Assure
To Endorse
Executive Summary This report sets out some key areas of work, in addition to their usual duties, for the Chief Officer since the last Governing Body meeting. The report covers the period from 7th March to 10th April 2018.
Recommendations The Governing Body is asked to: • Note the contents of the report.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 11 of 51
GOVERNING BODY BOARD REPORT
Strategic Themes
To empower the people of Wirral to improve their physical, mental health and general well being Y
To reduce health inequalities across the Wirral Y
To adopt a health and well-being approach in the way services are both commissioned and provided Y
To commission and contract for services that:
Demonstrate improved person centred outcomes Are high quality and seamless for the patient Are safe and sustainable Are evidenced based Demonstrate value for money
Y
To be known as one of the leading Clinical Commissioning Groups in the country Y
Provide systems leadership in shaping the Wirral health and social care system so as to be fit for purpose both now and in five years time
Y
Governance route prior to Governing Body
Meeting Date Objective/Outcome
CCG Governing Body n/a
Quality and Performance Committee n/a
Finance Committee n/a
Audit Committee n/a
Remuneration Committee n/a
Health and Wellbeing Board n/a
Clinical Senate n/a
Quality & Improvement Group n/a
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 12 of 51
GOVERNING BODY BOARD REPORT
CHIEF OFFICER’S REPORT
This report sets out some key areas of work, in addition to their usual duties, for the Chief Officer since the last Governing Body meeting. The report covers the period from 7th March 2018 to 10th April 2018. Working in partnership with other organisations Monthly Clinical Commissioning Group (CCG) Chief Officers Meetings The meetings are convened by NHS England and chaired by Graham Urwin, Director of Commissioning Operations, NHS England (Cheshire and Merseyside). They are a mechanism through which Graham and his team exchange information and ke y messages with the Chief Officers from Cheshire and Merseyside CCGs. The next meeting is scheduled for 20th April 2018. The Chief Officer gave a verbal update on the meeting held on 6th March 2018 at the last Governing Body. Delivering Healthy Wirral The Chief Officer has engaged in a number of activities that are designed to deliver the Healthy Wirral vision, objectives and outcomes by 2020. To deliver Healthy Wirral, NHS Wirral CCG and Wirral Council are on a path to integrating our commissioning functions so that we commission an integrated health and care system in which providers come together and have accountability for using a defined set of resources to provide the best possible quality of care and health outcomes for the people of Wirral. This has included:
Arranging and participating with the Chair and other Executive Team members in a whole system session to develop a System Sustainability Plan on 9th March 2018.
Attending, with the Chair, the Health and Care Partnership for Cheshire and Merseyside Summit on 14th March 2018 with the Chair.
Attended the Health and Care Partnership for Cheshire and Merseyside Elective Care meeting on 16th March 2018.
Chaired the Healthy Wirral Partners Board on 22nd March 2018.
The Director of Commissioning and Medical Director attended the Wirral Health and Wellbeing Board on 14th March 2018 on behalf of the Chief Officer and Chair as it c lashed with the Health and Care Partnership for Cheshire and Merseyside Summit. The papers for this meeting can be found at https://democracy.wirral.gov.uk/ieListDocuments.aspx?CId=630&MId=6024&Ver=4
Cheshire and Merseyside Women’s and Children’s Service Partnership The Chief Officer is the Senior Responsible Officer for the Cheshire and Merseyside Women’s and Children’s Services Partnership. The work of the Partnership is incorporated into Delivering the 5 Year Forward View structures across Cheshire and Merseyside as a cross-cutting theme. The Partnership also brings together national funding as a New Care Models Acute Care Collaboration Vanguard, a pioneer site for choice and personalisation in maternity services and as an Early Adopter to deliver the outcomes of the National Maternity Review – Better Births. Activity in the last month has included:
Weekly team meetings with the Partnership team. Meeting with Felicity Dowling and another colleague from Save Liverpool Women’s Hospital on
7th March 2018. Attending the Maternity Transformation Board North on 12th March 2018. Supporting the opening of the Seacombe Freestanding Midwife Led service and attending the
opening on 20th March 2018.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 13 of 51
GOVERNING BODY BOARD REPORT
Chairing the Cheshire and Merseyside Local Maternity System meeting on 26th March 2018.
Attending the national Better Births celebration event on 27th March 2018 to mark two years since the publication of the report.
Attending the North West Neonatal Operational Delivery Network meeting on 28th March 2018. Chairing the Cheshire and Merseyside Women’s and Children’s Services Partnership Board in
5th April 2018. Assurance by NHS England There are no items to report in regard to assurance by NHS England. Being accessible and accountable to local communities Question Time The Chair, Chief Officer and Executive Team attended a public question time on the evening of 8th March 2018 in Heswall Hall, Heswall. The meeting was well attended given the inclement weather and was an excellent opportunity to meet local people. Adult Care and Health Overview and Scrutiny Committee The Chair and Chief Officer attended a meeting of the Adult Care and Health Overview and Scrutiny Committee on 20th March 2018. The agenda included an independent review of Patient Led Repeat Ordering, an update on phlebotomy services, the Future Commissioning Strategy for All Age Disabilities, a verbal update on Thorn Heys and a paper on the Eastham Walk In Centre. The papers can be found at: https://democracy.wirral.gov.uk/ieListDocuments.aspx?CId=819&MId=6121&Ver=4 Angela Eagle MP The Chief Officer met with Angela Eagle MP on 23rd March 2018. Items for discussion included funding for the NHS, the responsiveness of the urgent care system in winter, care homes, the impact of the pay increase for NHS staff and the Seacombe Freestanding Midwife Led service.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 14 of 51
GOVERNING BODY REPORT
1/2
Risk Please indicate Detail of Risk Description
High Yes Medium Low
Clinical engagement taken place N
Patient and public involvement taken place N
Equality Analysis/Impact Assessment completed N
Quality Impact Assessment N
Strategic Themes
To empower the people of Wirral to improve their physical, mental health and general well being Y
To reduce health inequalities across the Wirral Y
To adopt a health and well-being approach in the way services are both commissioned and provided Y
FINANCE REPORT MONTH 11 – FEBRUARY 2017/18 FINANCIAL YEAR
Agenda Item: 3.1 Reference GB17-18/0068
Public / Private Public Meeting Date 10th April 2018
Lead Officer/Author of paper
Mike Treharne – Chief Finance Officer
Contributors Clare Shelley – Senior Reporting and Planning Accountant Ken Jones - Deputy Chief Finance Officer
To Approve
To Inform Yes
To Assure Yes
To Endorse
Executive Summary Financial performance as at 28th February 2018 and high level identification of risks for 2017/18.
Recommendations The Finance Committee is asked to: Note the contents of the report Note the risks identified in the report
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 15 of 51
GOVERNING BODY REPORT
2/2
To commission and contract for services that:
Demonstrate improved person centred outcomes Are high quality and seamless for the patient Are safe and sustainable Are evidenced based Demonstrate value for money
Y
To be known as one of the leading Clinical Commissioning Groups in the country Y
Provide systems leadership in shaping the Wirral health and social care system so as to be fit for purpose both now and in five years’ time
Y
This section gives details not only of where the actual paper has previously been submitted and what the outcome was but also of its development path i.e. other papers that are directly related to the current paper under discussion.
Governance route prior to Clinical Senate
Meeting Date Objective/Outcome
CCG Governing Body
Quality and Performance Committee
Clinical Senate
Audit Committee
Remuneration Committee
Health and Wellbeing Board
Quality & Improvement Group
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 16 of 51
GOVERNING BODY REPORT
1.0. INTRODUCTION
1.1 This report sets out the financial position for NHS Wirral Clinical Commissioning Group (Wirral CCG) as at the end of February (Month 11) 2017/18. The main headlines are -
£8.8m year to date deficit against Revenue Resource Limit. Year to date pressure s continue to be experienced within NHS Acut e
contracts, predominantly within the Wirral University Teaching Hospitals NHS FT contract (£3.6m) and the Liverpool Heart and Chest NHS FT contract (£852k).
Continuing Healthcare overspends also continue with a year to date pressure of £4.8m.
The CCG h as reported a forecast out turn def icit position of £9.8m to NHS England as part of month 11 repo rting which is consistent with month 10 submissions.
There does remain an element of risk to the CCG in ach ieving this £9.8m deficit particularly if NHS acute cont racts and CHC continue to overspend significantly during the final month of the financial year over and above the forecast.
QIPP plans continue to be monitored for 2017/ 18 to ensure delivery against the revised targets.
It is important that focu s remains on the CCG QIPP programme leading into 2018/19 with supporting management and clin ical actions in maintaining the CCG’s expenditure within budgets for the new financial year.
2.0. KEY ISSUES/MESSAGES
2.1. For month 11 the CCG is report ing a year to d ate operational deficit of £8.8m before any further management and clinical actions.
2.2. The table b elow shows the breakd own of this deficit by expenditure area; a more detailed breakdown is shown in Appendix 1.
Report Title Finance Report for the period - 1st April to 28th February 2018
M11 – 2017/18 Financial Year Lead Officer Mike Treharne Recommendations 1. To note the financial position of the CCG at Month 11.
2. To note the high level budget/expenditure summary for 2017/18.
3. To note further risks attached to achieving the 2017/18 revised risk adjusted forecast position.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 17 of 51
GOVERNING BODY REPORT
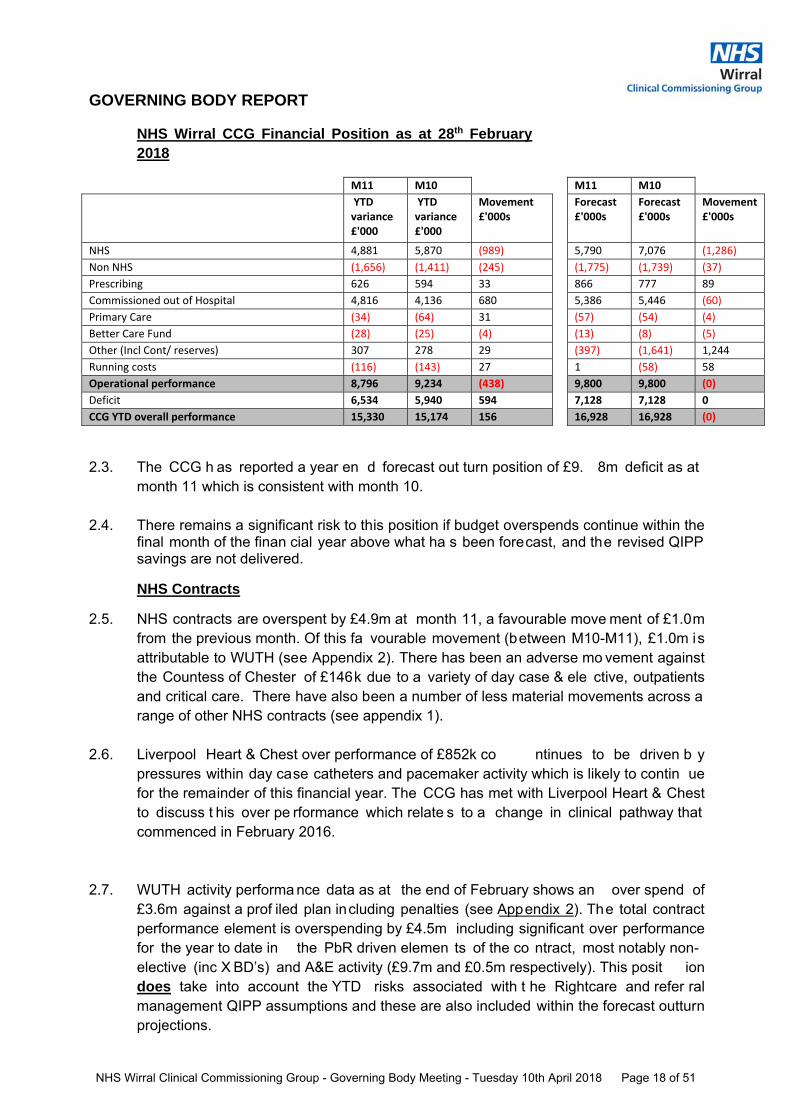
NHS Wirral CCG Financial Position as at 28th February 2018
M11 M10 M11 M10
YTD variance £'000
YTD variance £'000
Movement £'000s
Forecast £'000s
Forecast £'000s
Movement £'000s
NHS 4,881 5,870 (989) 5,790 7,076 (1,286)
Non NHS (1,656) (1,411) (245) (1,775) (1,739) (37)
Prescribing 626 594 33 866 777 89
Commissioned out of Hospital 4,816 4,136 680 5,386 5,446 (60)
Primary Care (34) (64) 31 (57) (54) (4)
Better Care Fund (28) (25) (4) (13) (8) (5)
Other (Incl Cont/ reserves) 307 278 29 (397) (1,641) 1,244
Running costs (116) (143) 27 1 (58) 58
Operational performance 8,796 9,234 (438) 9,800 9,800 (0)
Deficit 6,534 5,940 594 7,128 7,128 0
CCG YTD overall performance 15,330 15,174 156 16,928 16,928 (0)
2.3. The CCG h as reported a year en d forecast out turn position of £9. 8m deficit as at month 11 which is consistent with month 10.
2.4. There remains a significant risk to this position if budget overspends continue within the final month of the finan cial year above what ha s been forecast, and the revised QIPP savings are not delivered.
NHS Contracts
2.5. NHS contracts are overspent by £4.9m at month 11, a favourable move ment of £1.0m from the previous month. Of this fa vourable movement (between M10-M11), £1.0m is attributable to WUTH (see Appendix 2). There has been an adverse mo vement against the Countess of Chester of £146k due to a variety of day case & ele ctive, outpatients and critical care. There have also been a number of less material movements across a range of other NHS contracts (see appendix 1).
2.6. Liverpool Heart & Chest over performance of £852k co ntinues to be driven b y pressures within day case catheters and pacemaker activity which is likely to contin ue for the remainder of this financial year. The CCG has met with Liverpool Heart & Chest to discuss t his over pe rformance which relate s to a change in clinical pathway that commenced in February 2016.
2.7. WUTH activity performa nce data as at the end of February shows an over spend of £3.6m against a prof iled plan including penalties (see Appendix 2). The total contract performance element is overspending by £4.5m including significant over performance for the year to date in the PbR driven elemen ts of the co ntract, most notably non-elective (inc X BD’s) and A&E activity (£9.7m and £0.5m respectively). This posit ion does take into account the YTD risks associated with t he Rightcare and refer ral management QIPP assumptions and these are also included within the forecast outturn projections.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 18 of 51
GOVERNING BODY REPORT
Non NHS Contracts
2.8. Non NHS contracts are under spent by £1.7m at the end of Fe bruary. This is predominantly due to the Spire Murrayfield cont ract underspending by £1.5m (£171k favourable movement from the January position). This p osition is based on Ja nuary data including an estimate for F ebruary activity with underperformance against all points of delivery; however these reduced activity levels are not expected to contin ue indefinitely. Locally commissioned services are also underperforming by £346k at t he end of February, largely due to physio.
Prescribing
2.9. The position at the en d of Februa ry is £626k overspent, based on 9 months a ctual prescribing data and 2 months estimate. This includes a brought forward pressure from 2016/17 of £100k.
2.10. There are still poten tial issues in respect of category M savings and NCSO (No Cheaper Stock Obtainable) supply issues and these are being worked through with th e CSU Medicines Management Team and the CCG BI team. Whilst this is a nat ional issue there is a significant pressure for the CCG of circa £2m forecast to the end of the financial year. Figures are reported monthly t o NHS Eng land, their guidance is to include these pressures within the year to date position and now within the year end forecast outturn position (a change from month 9 ). The CCG continues t o report these pressures on this basis in line with NHS England expectations.
Continuing Healthcare
2.11. As at the end of Feb ruary, Packages of Care are £4.8 m overspent, an adver se movement of £680k from the January reported position. Of this, fully funded continuing healthcare packages are £4.4m overspent. This is du e to an ong oing trend of increases in new packages approved with backdated cost s, high package cost s and fewer than anticipated packages ceasing in year.
2.12 Joint Funded CHC is £65k underspent spent year to date; we have seen a fur ther favourable movement in month of £277k (between M10-11) in addition to the favourable movement of £470k that we saw between months 9-10. Th e key reason for this swing follows the outcome of a detailed review of ceased packages undertaken by the admin team.
2.13 Funded Nursing Care is £355k underspent at month 11, this is based on the information provided by the CHC team and populated within the Broadcare database.
2.14 Fully funded Personal Health bu dgets (PHB’s) are £49 6k over sp ent an adverse movement of £58k in month.
2.15 CHC Children is showing an under spend of £109k.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 19 of 51
GOVERNING BODY REPORT
Primary Care
2.16 At the end of February Primary Care budgets are £34k under spent. This is largely due to Think P harmacy (level 1 only provided) and some small benefit s from 201 6/17 fallouts.
Better Care Fund
2.17 The Better Care Fund pooled budget shows a £28k favourable variance at the end of February. This continu es to b e due to differ ences between a num ber of 201 6/17 accruals and actual payments made. Any known slippage or pressures will be managed via the Better Care Fund Board.
Other (Incl Reserves)
2.18 An element of the contingency reserve was utilised in month 2 to fund the prescribi ng practice budgets. The remaining £1.3m of this contingency (previously profiled in month 12) was re-profiled in month 9 which has now offset some of the YTD pressures such as NHS contract over performance and QIPP slippage.
2.19 Headroom of £2.4m (0.5%) remains uncommitted and profiled in M12, under instruction from NHS England. N HS England has confirmed this re source is to be relea sed in month 12 to support the CCG’s deficit position in line with similar directions issued at the end of 2016/17.
2.20 The reported reserves overspend of £94k as at the end of February rel ates primarily to realised pressures from 2016/17.
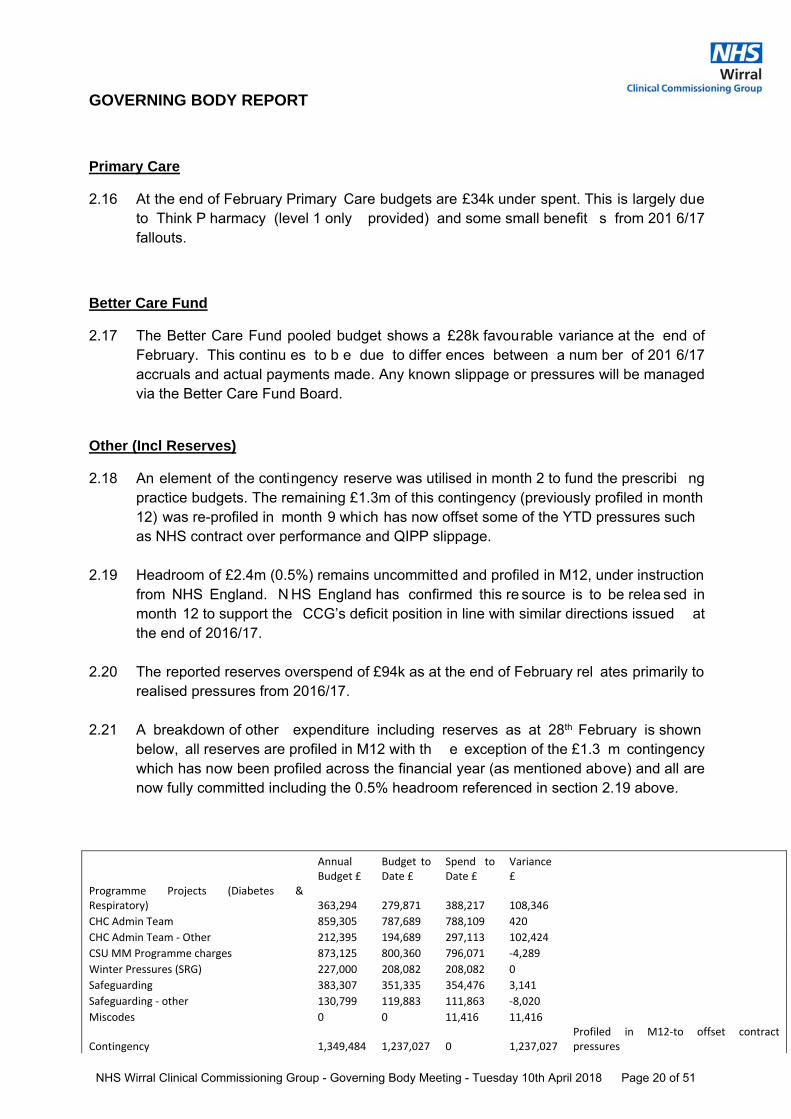
2.21 A breakdown of other expenditure including reserves as at 28th February is shown below, all reserves are profiled in M12 with th e exception of the £1.3 m contingency which has now been profiled across the financial year (as mentioned above) and all are now fully committed including the 0.5% headroom referenced in section 2.19 above.
Annual Budget £
Budget to Date £
Spend to Date £
Variance £
Programme Projects (Diabetes & Respiratory) 363,294 279,871 388,217 108,346
CHC Admin Team 859,305 787,689 788,109 420
CHC Admin Team ‐ Other 212,395 194,689 297,113 102,424
CSU MM Programme charges 873,125 800,360 796,071 ‐4,289
Winter Pressures (SRG) 227,000 208,082 208,082 0
Safeguarding 383,307 351,335 354,476 3,141
Safeguarding ‐ other 130,799 119,883 111,863 ‐8,020
Miscodes 0 0 11,416 11,416
Contingency 1,349,484 1,237,027 0 1,237,027 Profiled in M12‐to offset contract pressures
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 20 of 51
GOVERNING BODY REPORT
In year spend 0 0 1,330,665 1,330,665
MH5Y4V 17,930 0 0 0
Risk Reserve 2,483,600 0 0 0 0.5% committed per NHSE
Other 156,259 0 0 0
Contracts 1,167,544 0 0 0 Committed
8,224,041 3,978,936 4,286,012 307,076
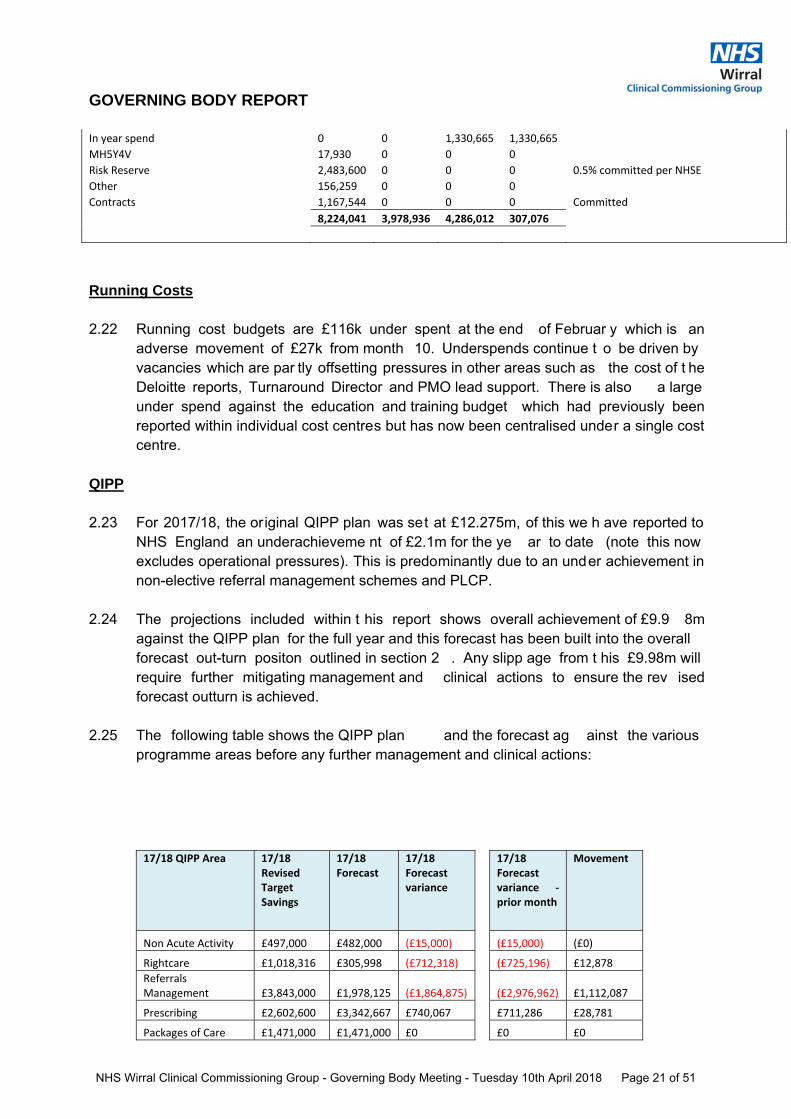
Running Costs 2.22 Running cost budgets are £116k under spent at the end of Februar y which is an
adverse movement of £27k from month 10. Underspends continue t o be driven by vacancies which are par tly offsetting pressures in other areas such as the cost of t he Deloitte reports, Turnaround Director and PMO lead support. There is also a large under spend against the education and training budget which had previously been reported within individual cost centres but has now been centralised under a single cost centre.
QIPP 2.23 For 2017/18, the original QIPP plan was set at £12.275m, of this we h ave reported to
NHS England an underachieveme nt of £2.1m for the ye ar to date (note this now excludes operational pressures). This is predominantly due to an under achievement in non-elective referral management schemes and PLCP.
2.24 The projections included within t his report shows overall achievement of £9.9 8m against the QIPP plan for the full year and this forecast has been built into the overall forecast out-turn positon outlined in section 2 . Any slipp age from t his £9.98m will require further mitigating management and clinical actions to ensure the rev ised forecast outturn is achieved.
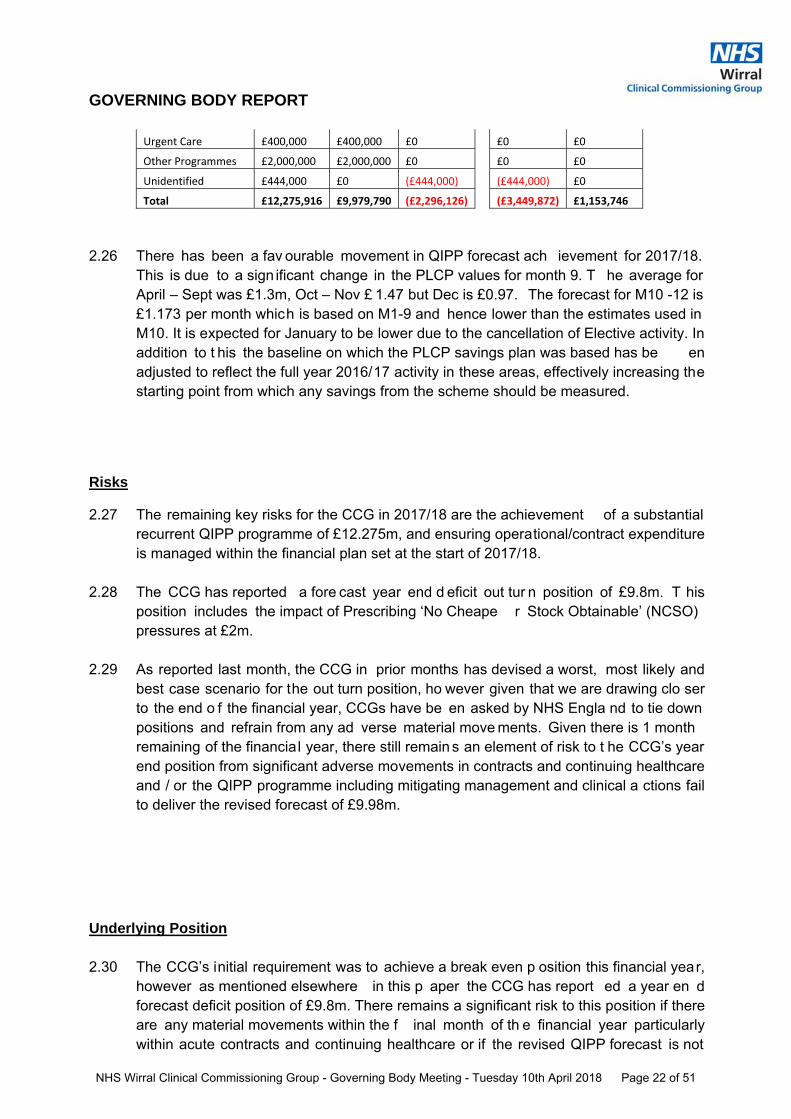
2.25 The following table shows the QIPP plan and the forecast ag ainst the various programme areas before any further management and clinical actions:
17/18 QIPP Area 17/18 Revised Target Savings
17/18 Forecast
17/18 Forecast variance
17/18 Forecast variance ‐ prior month
Movement
Non Acute Activity £497,000 £482,000 (£15,000) (£15,000) (£0)
Rightcare £1,018,316 £305,998 (£712,318) (£725,196) £12,878
Referrals Management £3,843,000 £1,978,125 (£1,864,875) (£2,976,962) £1,112,087
Prescribing £2,602,600 £3,342,667 £740,067 £711,286 £28,781
Packages of Care £1,471,000 £1,471,000 £0 £0 £0
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 21 of 51
GOVERNING BODY REPORT
Urgent Care £400,000 £400,000 £0 £0 £0
Other Programmes £2,000,000 £2,000,000 £0 £0 £0
Unidentified £444,000 £0 (£444,000) (£444,000) £0
Total £12,275,916 £9,979,790 (£2,296,126) (£3,449,872) £1,153,746
2.26 There has been a fav ourable movement in QIPP forecast ach ievement for 2017/18. This is due to a sign ificant change in the PLCP values for month 9. T he average for April – Sept was £1.3m, Oct – Nov £ 1.47 but Dec is £0.97. The forecast for M10 -12 is £1.173 per month which is based on M1-9 and hence lower than the estimates used in M10. It is expected for January to be lower due to the cancellation of Elective activity. In addition to t his the baseline on which the PLCP savings plan was based has be en adjusted to reflect the full year 2016/17 activity in these areas, effectively increasing the starting point from which any savings from the scheme should be measured.
Risks
2.27 The remaining key risks for the CCG in 2017/18 are the achievement of a substantial recurrent QIPP programme of £12.275m, and ensuring operational/contract expenditure is managed within the financial plan set at the start of 2017/18.
2.28 The CCG has reported a fore cast year end d eficit out tur n position of £9.8m. T his position includes the impact of Prescribing ‘No Cheape r Stock Obtainable’ (NCSO) pressures at £2m.
2.29 As reported last month, the CCG in prior months has devised a worst, most likely and best case scenario for the out turn position, ho wever given that we are drawing clo ser to the end o f the financial year, CCGs have be en asked by NHS Engla nd to tie down positions and refrain from any ad verse material move ments. Given there is 1 month remaining of the financial year, there still remain s an element of risk to t he CCG’s year end position from significant adverse movements in contracts and continuing healthcare and / or the QIPP programme including mitigating management and clinical a ctions fail to deliver the revised forecast of £9.98m.
Underlying Position 2.30 The CCG’s initial requirement was to achieve a break even p osition this financial year,
however as mentioned elsewhere in this p aper the CCG has report ed a year en d forecast deficit position of £9.8m. There remains a significant risk to this position if there are any material movements within the f inal month of th e financial year particularly within acute contracts and continuing healthcare or if the revised QIPP forecast is not
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 22 of 51
GOVERNING BODY REPORT
delivered. I t must also be noted t hat the CCG still ha s a cumulative deficit of £7.1m brought forward from 2016/17.
Cash Management
2.31 The recorded CCG cas h book balance at the end of February was £9k. This is in line with current NHS England guidance that CCGs hold cash balances up to 1.25% of the current month cash drawdown.
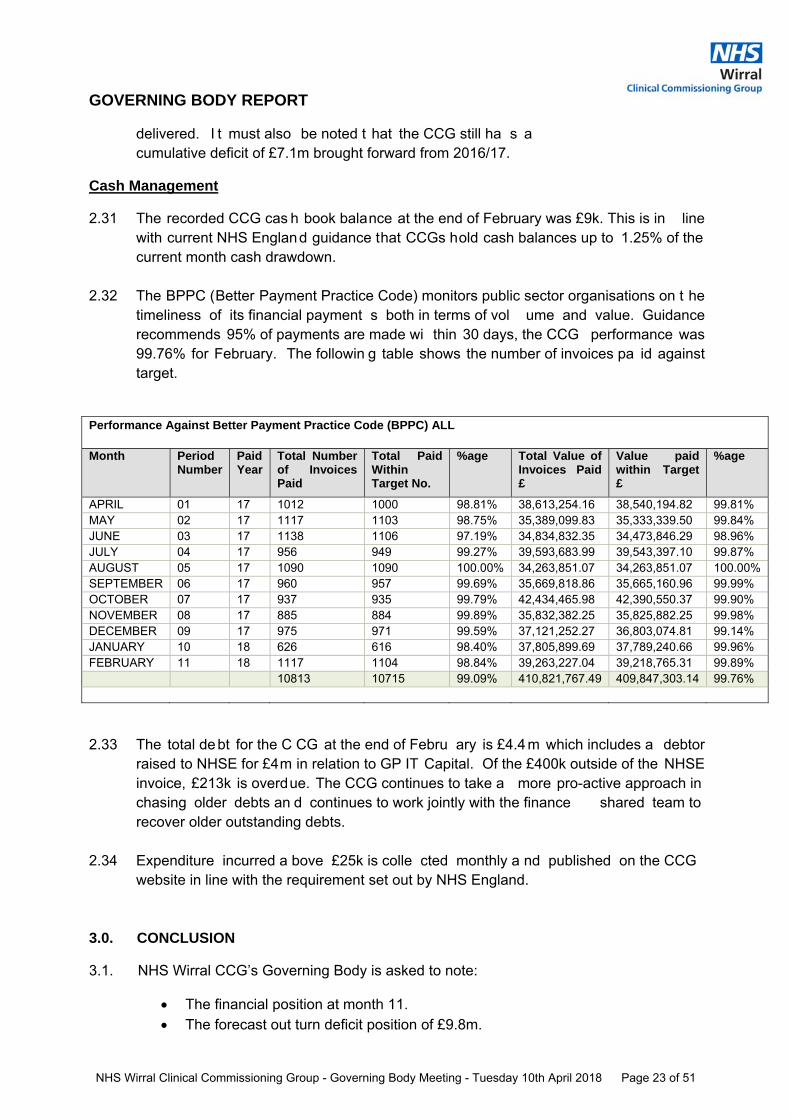
2.32 The BPPC (Better Payment Practice Code) monitors public sector organisations on t he timeliness of its financial payment s both in terms of vol ume and value. Guidance recommends 95% of payments are made wi thin 30 days, the CCG performance was 99.76% for February. The followin g table shows the number of invoices pa id against target.
Performance Against Better Payment Practice Code (BPPC) ALL Month Period
Number Paid Year
Total Number of Invoices Paid
Total Paid Within Target No.
%age Total Value of Invoices Paid £
Value paid within Target £
%age
APRIL 01 17 1012 1000 98.81% 38,613,254.16 38,540,194.82 99.81% MAY 02 17 1117 1103 98.75% 35,389,099.83 35,333,339.50 99.84% JUNE 03 17 1138 1106 97.19% 34,834,832.35 34,473,846.29 98.96% JULY 04 17 956 949 99.27% 39,593,683.99 39,543,397.10 99.87% AUGUST 05 17 1090 1090 100.00% 34,263,851.07 34,263,851.07 100.00% SEPTEMBER 06 17 960 957 99.69% 35,669,818.86 35,665,160.96 99.99% OCTOBER 07 17 937 935 99.79% 42,434,465.98 42,390,550.37 99.90% NOVEMBER 08 17 885 884 99.89% 35,832,382.25 35,825,882.25 99.98% DECEMBER 09 17 975 971 99.59% 37,121,252.27 36,803,074.81 99.14% JANUARY 10 18 626 616 98.40% 37,805,899.69 37,789,240.66 99.96% FEBRUARY 11 18 1117 1104 98.84% 39,263,227.04 39,218,765.31 99.89% 10813 10715 99.09% 410,821,767.49 409,847,303.14 99.76%
2.33 The total debt for the C CG at the end of Febru ary is £4.4m which includes a debtor raised to NHSE for £4m in relation to GP IT Capital. Of the £400k outside of the NHSE invoice, £213k is overdue. The CCG continues to take a more pro-active approach in chasing older debts an d continues to work jointly with the finance shared team to recover older outstanding debts.
2.34 Expenditure incurred a bove £25k is colle cted monthly a nd published on the CCG
website in line with the requirement set out by NHS England.
3.0. CONCLUSION
3.1. NHS Wirral CCG’s Governing Body is asked to note:
The financial position at month 11. The forecast out turn deficit position of £9.8m.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 23 of 51
GOVERNING BODY REPORT
The further risks to achieving this foreca st deficit position for the financial year 2017/ 18 if there are any material movements in expenditure or QIPP delivery during the final month of the financial year.
It is important that focus remains on the CCG QIPP programme leading into 2018/19 with supportin g management and clin ical actions in managing CCG budgets for the new financial year.
Mike Treharne
Chief Financial Officer NHS Wirral Clinical Commissioning Group 20th March 2018
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 24 of 51
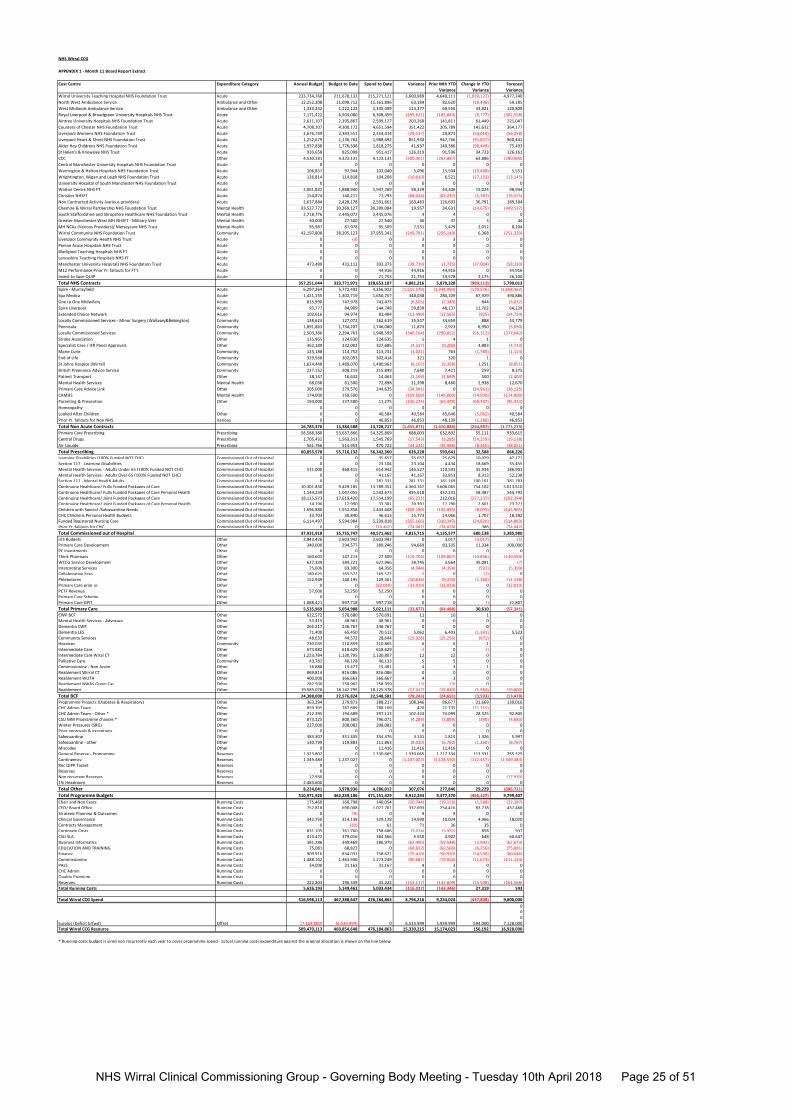
NHS Wirral CCG
APPENDIX 1 - Month 11 Board Report Extract
Cost Centre Expenditure Category Annual Budget Budget to Date Spend to Date Variance Prior Mth YTD
Variance
Change In YTD
Variance
Forecast
Variance
Wirral University Teaching Hospital NHS Foundation Trust Acute 233,734,760 211,670,132 215,271,121 3,600,989 4,640,111 (1,039,122) 4,977,240
North West Ambulance Service Ambulance and Other 12,252,208 11,098,712 11,161,896 63,184 82,620 (19,436) 59,185
West Midlands Ambulance Service Ambulance and Other 1,333,242 1,222,122 1,335,499 113,377 69,556 43,821 120,809
Royal Liverpool & Broadgreen University Hospitals NHS Trust Acute 7,171,422 6,504,080 6,308,459 (195,621) (185,844) (9,777) (302,558)
Aintree University Hospitals NHS Foundation Trust Acute 2,611,107 2,395,867 2,599,127 203,260 141,811 61,449 221,047
Countess of Chester NHS Foundation Trust Acute 4,708,107 4,300,172 4,651,594 351,422 205,789 145,632 364,177
Liverpool Womens NHS Foundation Trust Acute 2,676,749 2,383,551 2,354,414 (29,137) 24,873 (54,010) (56,258)
Liverpool Heart & Chest NHS Foundation Trust Acute 1,252,679 1,136,762 1,988,692 851,930 947,766 (95,837) 960,441
Alder Hey Childrens NHS Foundation Trust Acute 1,937,838 1,776,338 1,818,275 41,937 140,386 (98,449) 75,493
St Helen's & Knowsley NHS Trust Acute 910,658 825,098 951,417 126,319 91,596 34,723 126,161
CCC Other 4,530,181 4,323,131 4,123,131 (200,001) (263,887) 63,886 (280,000)
Central Manchester University Hospitals NHS Foundation Trust Acute 0 0 0 0 0 0 0
Warrington & Halton Hospitals NHS Foundation Trust Acute 106,857 97,944 103,040 5,096 15,504 (10,408) 5,551
Wrightington, Wigan and Leigh NHS Foundation Trust Acute 126,814 114,818 104,208 (10,610) 6,521 (17,131) (13,145)
University Hospital of South Manchester NHS Foundation Trust Acute 0 0 0 0 0 0 0
Walton Centre NHS FT Acute 2,061,832 1,888,940 1,947,269 58,329 43,306 15,024 98,944
Christies NHSFT Acute 154,874 140,217 71,793 (68,424) (63,237) (5,187) (76,555)
Non Contracted Activity (various providers) Acute 2,637,884 2,428,178 2,591,661 163,483 126,693 36,791 189,384
Cheshire & Wirral Partnership NHS Foundation Trust Mental Health 33,527,772 30,269,127 30,289,084 19,957 34,631 (14,675) (449,537)
South Staffordshire and Shropshire Healthcare NHS Foundation Trust Mental Health 2,718,776 2,445,072 2,445,076 4 4 0 0
Greater Manchester West MH NHSFT - Military Vets Mental Health 30,000 27,500 27,540 40 37 3 44
MH NCAs (Various Providers)/ Merseycare NHS Trust Mental Health 95,987 87,978 95,509 7,531 5,479 2,052 8,204
Wirral Community NHS Foundation Trust Community 42,197,808 38,205,123 37,955,342 (249,781) (256,149) 6,368 (251,320)
Liverpool Community Health NHS Trust Acute 0 (3) 0 3 3 0 0
Penine Acute Hospitals NHS Trust Acute 0 0 0 0 0 0 0
Blackpool Teaching Hospitals NHS FT Acute 0 0 0 0 0 0 0
Lancashire Teaching Hospitals NHS FT Acute 0 0 0 0 0 0 0
Manchester University Hospitals NHS Foundation Trust Acute 473,489 431,112 392,373 (38,739) (1,735) (37,004) (58,310)
M12 Performance Prior Yr. fallouts for FT's Acute 0 0 44,916 44,916 44,916 0 44,916
Invest to Save QUIP Acute 0 0 21,753 21,753 19,578 2,175 26,100
Total NHS Contracts 357,251,044 323,771,971 328,653,187 4,881,216 5,870,328 (989,112) 5,790,013
Spire - Murrayfield Acute 6,297,264 5,772,492 4,256,922 (1,515,570) (1,344,994) (170,576) (1,658,462)
Spa Medica Acute 1,421,155 1,302,719 1,650,757 348,038 280,109 67,929 390,886
One to One Midwifery Acute 815,990 747,978 741,473 (6,505) (7,349) 844 (3,032)
Spire Liverpool Acute 93,777 84,909 144,748 59,839 48,137 11,702 64,129
Extended Choice Network Acute 103,616 94,974 81,484 (13,490) (12,565) (925) (14,724)
Locally Commissioned Services - Minor Surgery (Wallasey&Bebington) Community 138,624 127,072 162,619 35,547 34,659 888 44,779
Peninsula Community 1,891,863 1,734,207 1,746,080 11,873 2,923 8,950 (5,050)
Locally Commissioned Services Community 2,503,386 2,294,763 1,948,599 (346,164) (290,852) (55,312) (377,642)
Stroke Association Other 135,965 124,630 124,635 5 4 1 0
Specialist Care / IFR Panel Approvals Other 362,189 332,002 327,685 (4,317) (9,200) 4,883 (4,713)
Marie Curie Community 125,188 114,752 113,731 (1,021) 763 (1,785) (1,114)
End of Life Community 329,568 302,093 302,414 321 320 1 0
St Johns Hospice (Wirral) Community 1,624,448 1,489,070 1,480,963 (8,107) (9,358) 1,251 (8,851)
British Pregnancy Advice Service Community 227,152 208,219 215,899 7,680 7,421 259 8,375
Patient Transport Other 18,147 16,632 14,463 (2,169) (2,669) 500 (2,403)
Mental Health Services Mental Health 68,038 61,500 72,898 11,398 8,460 2,938 12,670
Primary Care Advice Link Other 305,000 279,576 244,635 (34,941) 0 (34,941) (38,125)
CAMHS Mental Health 174,000 159,500 0 (159,500) (145,000) (14,500) (174,000)
Parenting & Prevention Other 150,000 137,500 11,275 (126,225) (65,479) (60,747) (95,433)
Homeopathy 0 0 0 0 0 0 0
Looked After Children Other 0 0 40,584 40,584 45,646 (5,062) 40,584
Prior Yr. fallouts for Non NHS Various 0 0 46,853 46,853 48,139 (1,286) 46,853
Total Non Acute Contracts 16,785,370 15,384,588 13,728,717 (1,655,871) (1,410,883) (244,987) (1,775,273)
Primary Care Prescribing Prescribing 58,588,380 53,637,866 54,325,869 688,003 632,892 55,111 933,615
Central Drugs Prescribing 1,705,432 1,563,313 1,545,769 (17,543) (3,285) (14,259) (19,138)
Air Liquide Prescribing 561,766 514,953 470,722 (44,231) (35,966) (8,265) (48,251)
Total Prescribing 60,855,578 55,716,132 56,342,360 626,228 593,641 32,588 866,226
Learning Disabilities (100% Funded NOT CHC) Commissioned Out of Hospital 0 0 35,657 35,657 25,629 10,029 47,171Section 117 - Learning Disabilities Commissioned Out of Hospital 0 0 23,104 23,104 4,434 18,669 35,455Mental Health Services - Adults Under 65 (100% Funded NOT CHC) Commissioned Out of Hospital 511,000 468,415 614,942 146,527 110,593 35,934 186,901Mental Health Services - Adults Over 65 (100% Funded NOT CHC) Commissioned Out of Hospital 0 0 41,167 41,167 32,853 8,313 52,238Section 117 - Mental Health Adults Commissioned Out of Hospital 0 0 281,331 281,331 181,169 100,161 381,783Continuing Healthcare/ Fully Funded Packages of Care Commissioned Out of Hospital 10,301,830 9,429,185 13,789,352 4,360,167 3,606,065 754,102 5,013,610Continuing Healthcare/ Fully Funded Packages of Care Personal Health Commissioned Out of Hospital 1,144,239 1,047,055 1,542,673 495,618 437,231 58,387 544,793Continuing Healthcare/ Joint Funded Packages of Care Commissioned Out of Hospital 18,115,573 17,619,420 17,554,199 (65,221) 212,016 (277,237) (182,394)Continuing Healthcare/ Joint Funded Packages of Care Personal Health Commissioned Out of Hospital 14,196 12,990 33,381 20,391 17,790 2,601 23,271Children with Special /Safeguarding Needs Commissioned Out of Hospital 1,696,880 1,552,858 1,443,668 (109,190) (101,095) (8,095) (145,905)CHC Childrens Personal Health Budgets Commissioned Out of Hospital 33,703 30,840 46,613 15,773 14,066 1,707 18,382Funded Registered Nursing Care Commissioned Out of Hospital 6,114,497 5,594,984 5,239,818 (355,166) (330,347) (24,820) (514,883)Prior Yr. fallouts for CHC Commissioned Out of Hospital 0 0 (74,442) (74,442) (74,828) 386 (74,442)
Total Commissioned out of Hospital 37,931,918 35,755,747 40,571,462 4,815,715 4,135,577 680,138 5,385,980
LES Budgets Other 2,843,426 2,603,942 2,603,942 0 3,017 (3,017) (1)Primary Care Development Other 340,000 294,577 389,246 94,669 83,335 11,334 100,000PC Investments Other 0 0 0 0 0 0 0Think Pharmacy Other 160,603 147,213 27,509 (119,704) (108,867) (10,836) (130,593)WCCG Service Development Other 637,339 584,221 622,966 38,745 3,664 35,081 (7)Interpreting Services Other 75,606 69,300 64,356 (4,944) (4,354) (591) (5,399)Collaborative Fees Other 180,625 165,572 165,572 () 0 (1) 0Phlebotomy Other 152,949 140,195 129,561 (10,634) (9,274) (1,360) (11,138)Primary Care prior yr Other 0 0 (32,010) (32,010) (32,010) 0 (32,010)PCTF Revenue Other 57,000 52,250 52,250 0 0 0 0Primary Care Scheme Other 0 0 0 0 0 0 0Primary Care GPIT Other 1,088,421 997,718 997,718 0 0 () 21,807
Total Primary Care 5,535,969 5,054,988 5,021,111 (33,877) (64,488) 30,610 (57,341)
CWP BCF Other 622,572 570,680 570,691 11 10 1 0Mental Health Services - Advocacy Other 53,415 48,961 48,961 0 0 0 0Dementia CWP Other 265,217 246,767 246,767 0 0 0 0Dementia LES Other 71,400 65,450 70,512 5,062 6,403 (1,341) 5,522Community Services Other 48,633 44,572 28,644 (15,928) (15,256) (671) 0Hospices Community 230,035 210,859 210,865 6 6 1 0Intermediate Care Other 674,882 618,629 618,629 () 0 () 0Intermediate Care Wiral CT Other 1,223,784 1,130,795 1,130,807 12 12 0 0Palliative Care Community 43,782 40,128 40,133 5 5 0 0Commissioning - Non Acute Other 16,888 15,477 15,481 4 3 1 0Reablement Wirral CT Other 869,814 816,086 816,086 0 0 0 0Reablement WUTH Other 400,000 366,663 366,667 4 3 0 0Reablement NWAS Green Car Other 282,500 258,962 258,959 (3) (3) 0 0Reablement Other 19,585,078 18,142,795 18,125,378 (17,417) (15,833) (1,583) (19,000)
Total BCF 24,388,000 22,576,824 22,548,581 (28,243) (24,651) (3,593) (13,478)
Programme Projects (Diabetes & Respiratory) Other 363,294 279,871 388,217 108,346 86,677 21,669 130,016CHC Admin Team Other 859,305 787,689 788,109 420 21,735 (21,315) 0CHC Admin Team - Other * Other 212,395 194,689 297,113 102,424 74,099 28,325 92,805CSU MM Programme charges * Other 873,125 800,360 796,071 (4,289) (3,899) (390) (4,683)Winter Pressures (SRG) Other 227,000 208,082 208,082 0 0 0 0Prior approvals & exceptions Other 0 0 0 0 0 0 0Safeguarding Other 383,307 351,335 354,476 3,141 1,815 1,326 5,997Safeguarding - other Other 130,799 119,883 111,863 (8,020) (6,760) (1,260) (8,767)Miscodes Other 0 0 11,416 11,416 11,416 0 0General Reserve - Programme Reserves 1,323,802 0 1,330,665 1,330,665 1,217,334 113,331 755,325Contingency Reserves 1,349,484 1,237,027 0 (1,237,027) (1,124,570) (112,457) (1,349,484)Rec QIPP Target Reserves 0 0 0 0 0 0 0Reserves Reserves 0 0 0 0 0 0 0Non recurrent Reserves Reserves 17,930 0 0 0 0 0 (17,930)1% Headroom Reserves 2,483,600 0 0 0 0 0 0
Total Other 8,224,041 3,978,936 4,286,012 307,076 277,846 29,229 (396,721)
Total Programme Budgets 510,971,920 462,239,186 471,151,429 8,912,243 9,377,370 (465,127) 9,799,407
Chair and Non Execs Running Costs 175,460 160,798 140,054 (20,744) (19,156) (1,588) (22,387)CEO/ Board Office Running Costs 752,818 690,008 1,027,701 337,693 254,416 83,278 437,468Strategic Planning & Outcomes Running Costs 0 (9) 0 9 9 0 0Clinical Governance Running Costs 342,750 314,138 329,128 14,990 10,024 4,966 18,020Contracts Management Running Costs 0 (10) 61 71 36 35 0Corporate Costs Running Costs 831,105 761,760 758,686 (3,074) (3,932) 858 937CSU SLA Running Costs 413,472 379,016 384,566 5,550 4,902 648 60,647Business Informatics Running Costs 381,286 349,469 286,979 (62,490) (59,548) (2,942) (62,673)EDUCATION AND TRAINING Running Costs 75,081 68,822 0 (68,822) (62,566) (6,256) (75,081)Finance Running Costs 909,916 834,031 758,621 (75,410) (50,910) (24,500) (80,646)Commissioning Running Costs 1,488,102 1,363,936 1,273,249 (90,687) (79,014) (11,673) (111,124)PALS Running Costs 34,000 31,163 31,167 4 3 0 0CHC Admin Running Costs 0 0 0 0 0 0 0Quality Premium Running Costs 0 0 0 0 0 0 0Reserves Running Costs 222,203 196,339 43,222 (153,117) (137,609) (15,508) (164,568)Total Running Costs 5,626,193 5,149,461 5,033,434 (116,027) (143,346) 27,319 593
Total Wirral CCG Spend 516,598,113 467,388,647 476,184,863 8,796,216 9,234,024 (437,808) 9,800,000
000
Surplus (Deficit b/fwd) Offset (7,128,000) (6,533,999) 0 6,533,999 5,939,999 594,000 7,128,000Total Wirral CCG Resource 509,470,113 460,854,648 476,184,863 15,330,215 15,174,023 156,192 16,928,000
* Running costs budget is vired non recurrently each year to cover programme spend - actual running costs expenditure against the original allocation is shown on the line below
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 25 of 51
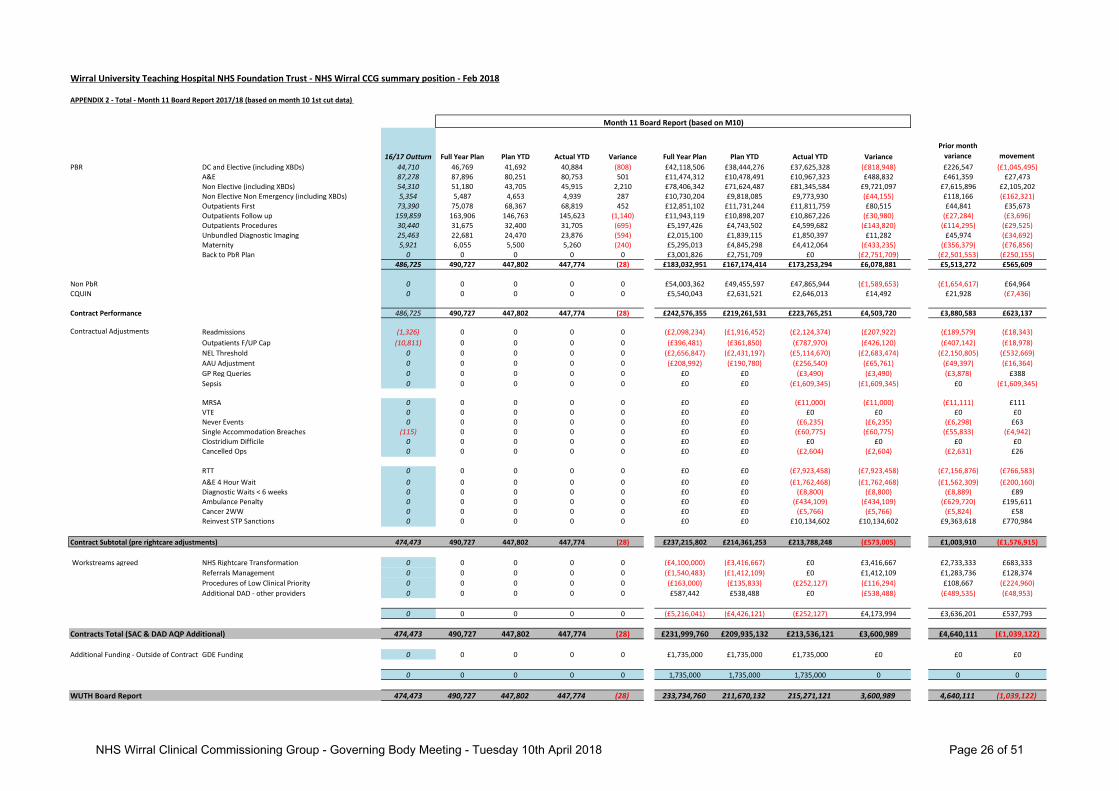
Wirral University Teaching Hospital NHS Foundation Trust - NHS Wirral CCG summary position - Feb 2018
APPENDIX 2 - Total - Month 11 Board Report 2017/18 (based on month 10 1st cut data)
16/17 Outturn Full Year Plan Plan YTD Actual YTD Variance Full Year Plan Plan YTD Actual YTD Variance
Prior month
variance movement
PBR DC and Elective (including XBDs) 44,710 46,769 41,692 40,884 (808) £42,118,506 £38,444,276 £37,625,328 (£818,948) £226,547 (£1,045,495)A&E 87,278 87,896 80,251 80,753 501 £11,474,312 £10,478,491 £10,967,323 £488,832 £461,359 £27,473Non Elective (including XBDs) 54,310 51,180 43,705 45,915 2,210 £78,406,342 £71,624,487 £81,345,584 £9,721,097 £7,615,896 £2,105,202Non Elective Non Emergency (including XBDs) 5,354 5,487 4,653 4,939 287 £10,730,204 £9,818,085 £9,773,930 (£44,155) £118,166 (£162,321)Outpatients First 73,390 75,078 68,367 68,819 452 £12,851,102 £11,731,244 £11,811,759 £80,515 £44,841 £35,673Outpatients Follow up 159,859 163,906 146,763 145,623 (1,140) £11,943,119 £10,898,207 £10,867,226 (£30,980) (£27,284) (£3,696)Outpatients Procedures 30,440 31,675 32,400 31,705 (695) £5,197,426 £4,743,502 £4,599,682 (£143,820) (£114,295) (£29,525)Unbundled Diagnostic Imaging 25,463 22,681 24,470 23,876 (594) £2,015,100 £1,839,115 £1,850,397 £11,282 £45,974 (£34,692)Maternity 5,921 6,055 5,500 5,260 (240) £5,295,013 £4,845,298 £4,412,064 (£433,235) (£356,379) (£76,856)Back to PbR Plan 0 0 0 0 0 £3,001,826 £2,751,709 £0 (£2,751,709) (£2,501,553) (£250,155)
486,725 490,727 447,802 447,774 (28) £183,032,951 £167,174,414 £173,253,294 £6,078,881 £5,513,272 £565,609
Non PbR 0 0 0 0 0 £54,003,362 £49,455,597 £47,865,944 (£1,589,653) (£1,654,617) £64,964CQUIN 0 0 0 0 0 £5,540,043 £2,631,521 £2,646,013 £14,492 £21,928 (£7,436)
Contract Performance 486,725 490,727 447,802 447,774 (28) £242,576,355 £219,261,531 £223,765,251 £4,503,720 £3,880,583 £623,137
Contractual Adjustments Readmissions (1,326) 0 0 0 0 (£2,098,234) (£1,916,452) (£2,124,374) (£207,922) (£189,579) (£18,343)
Outpatients F/UP Cap (10,811) 0 0 0 0 (£396,481) (£361,850) (£787,970) (£426,120) (£407,142) (£18,978)
NEL Threshold 0 0 0 0 0 (£2,656,847) (£2,431,197) (£5,114,670) (£2,683,474) (£2,150,805) (£532,669)
AAU Adjustment 0 0 0 0 0 (£208,992) (£190,780) (£256,540) (£65,761) (£49,397) (£16,364)
GP Reg Queries 0 0 0 0 0 £0 £0 (£3,490) (£3,490) (£3,878) £388
Sepsis 0 0 0 0 0 £0 £0 (£1,609,345) (£1,609,345) £0 (£1,609,345)
MRSA 0 0 0 0 0 £0 £0 (£11,000) (£11,000) (£11,111) £111VTE 0 0 0 0 0 £0 £0 £0 £0 £0 £0Never Events 0 0 0 0 0 £0 £0 (£6,235) (£6,235) (£6,298) £63Single Accommodation Breaches (115) 0 0 0 0 £0 £0 (£60,775) (£60,775) (£55,833) (£4,942)Clostridium Difficile 0 0 0 0 0 £0 £0 £0 £0 £0 £0Cancelled Ops 0 0 0 0 0 £0 £0 (£2,604) (£2,604) (£2,631) £26
RTT 0 0 0 0 0 £0 £0 (£7,923,458) (£7,923,458) (£7,156,876) (£766,583)
A&E 4 Hour Wait 0 0 0 0 0 £0 £0 (£1,762,468) (£1,762,468) (£1,562,309) (£200,160)Diagnostic Waits < 6 weeks 0 0 0 0 0 £0 £0 (£8,800) (£8,800) (£8,889) £89Ambulance Penalty 0 0 0 0 0 £0 £0 (£434,109) (£434,109) (£629,720) £195,611Cancer 2WW 0 0 0 0 0 £0 £0 (£5,766) (£5,766) (£5,824) £58Reinvest STP Sanctions 0 0 0 0 0 £0 £0 £10,134,602 £10,134,602 £9,363,618 £770,984
Contract Subtotal (pre rightcare adjustments) 474,473 490,727 447,802 447,774 (28) £237,215,802 £214,361,253 £213,788,248 (£573,005) £1,003,910 (£1,576,915)
Workstreams agreed NHS Rightcare Transformation 0 0 0 0 0 (£4,100,000) (£3,416,667) £0 £3,416,667 £2,733,333 £683,333
Referrals Management 0 0 0 0 0 (£1,540,483) (£1,412,109) £0 £1,412,109 £1,283,736 £128,374
Procedures of Low Clinical Priority 0 0 0 0 0 (£163,000) (£135,833) (£252,127) (£116,294) £108,667 (£224,960)
Additional DAD - other providers 0 0 0 0 0 £587,442 £538,488 £0 (£538,488) (£489,535) (£48,953)
0 0 0 0 0 (£5,216,041) (£4,426,121) (£252,127) £4,173,994 £3,636,201 £537,793
Contracts Total (SAC & DAD AQP Additional) 474,473 490,727 447,802 447,774 (28) £231,999,760 £209,935,132 £213,536,121 £3,600,989 £4,640,111 (£1,039,122)
Additional Funding - Outside of Contract GDE Funding 0 0 0 0 0 £1,735,000 £1,735,000 £1,735,000 £0 £0 £0
0 0 0 0 0 1,735,000 1,735,000 1,735,000 0 0 0
WUTH Board Report 474,473 490,727 447,802 447,774 (28) 233,734,760 211,670,132 215,271,121 3,600,989 4,640,111 (1,039,122)
Month 11 Board Report (based on M10)
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 26 of 51
GOVERNING BODY REPORT
Risk Please indicate Detail of Risk Description
High Medium Yes Low
Risk of continued non achievement of national IAPT standards
Clinical engagement taken place Y
Patient and public involvement taken place N
Equality Analysis/Impact Assessment completed N
Quality Impact Assessment N
Strategic Themes
IMPROVING ACCESS TO PSYCHOLOGICAL SERVICES (IAPT)
– PERFORMANCE TRAJECTORY 2018-19
Agenda Item: 4.1 Reference GB17-18/0077
Public / Private Public Meeting Date 10th April 2018
Lead Officer/Author of paper
Nesta Hawker, Director of Commissioning
Contributors Jo Watts, Senior Commissioning Lead Mental Health Dr Peter Arthur, Mental Health Clinical Lead
To Approve Yes
To Inform
To Assure Yes
To Endorse
Executive Summary The report provides an overview of the improvement projections for IAPT performance for 2018-19. It identifies the associated investment to meet the trajectories and the associated risk sharing agreement between the CCG and the Provider.
Recommendations The Governing Body is asked to: 1. To note update on the IAPT progress; 2. To decide on the option appraisal for additional investment; 3. To approve the proposed delivery plan and associated trajectories for
submission to NHS England, To endorse the communications and engagement plan;
4. To agree the risk sharing agreement.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 27 of 51
GOVERNING BODY REPORT
To empower the people of Wirral to improve their physical, mental health and general well being N
To reduce health inequalities across the Wirral N
To adopt a health and well-being approach in the way services are both commissioned and provided N
To commission and contract for services that:
Demonstrate improved person centred outcomes Are high quality and seamless for the patient Are safe and sustainable Are evidenced based Demonstrate value for money
Y
To be known as one of the leading Clinical Commissioning Groups in the country N
Provide systems leadership in shaping the Wirral health and social care system so as to be fit for purpose both now and in five years time
N
This section gives details not only of where the actual paper has previously been submitted and what the outcome was but also of its development path i.e. other papers that are directly related to the current paper under discussion.
Governance route prior to Governing Body
Meeting Date Objective/Outcome
CCG Governing Body
Quality and Performance Committee
Finance Committee
Audit Committee
Remuneration Committee
Health and Wellbeing Board
Clinical Senate
Quality & Improvement Group
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 28 of 51
GOVERNING BODY REPORT
1. INTRODUCTION Further to the IAPT update report presented in March 2018 and the requirement to agree the proposed trajectories for submission to NHS England (NHSE) and NHS Improvement (NHSI), this report provides an updated plan and delivery model which has been co-produced by the provider and commissioner outlining the trajectories and associated actions to improve the Wirral IAPT performance during the period of April 2018 – March 2019. To enable the development of the delivery plan, a meeting was held between the provider and Commissioning lead supported by the Clinical Lead for Mental Heal th from the CCG. This meeting was held on the 15th March 2018 which resulted in a draft proposal being submitted to NHSE and NHSI on the 15th March 2018 (Appendix 1) in line with the requested timeframes. The submission outlined the proposed trajectories for improvement and confirmed the need to further “test” some of the assumptions made within the planning return through the involvement of the Intensive Support Team (IST). The IST lead visited the service on the 20th March and has offered some high level views on the proposals submitted.
2. KEY ISSUES / MESSAGES
2.1 The provider and CCG have work ed collaboratively to develop a plan to improve IAPT performance through the extension of the contract term from July 2018 to March 2019 supported by additional investment. Initial projections for additional investment were provisionally agreed as an additional £419,671 to achieve continued waiting list reduction and increase to access targets, this would result in overall contract value of £3,279,000.
2.2 It should be noted that the additional investment was calculated on the basis of IST assumptions of national IAPT services. Given the historic demand on Wirral IAPT services and the level of complexity presenting to the service based on demographic information, at Step 3 (out side of national trends), the provider was asked to remodel the additional investment required to ensure that the trajectories identified are achievable and sustainable.
Report Title Improving Access to Psychological Services (IAPT) – Performance Trajectory 2018-19
Lead officer Nesta Hawker, Director of Commissioning Contributor Jo Watts, Senior Commissioning Manager – Mental Health
Dr Peter Arthur, Mental Health Clinical Lead
Recommendations 1. To note update on the IAPT progress; 2. To decide on the option appraisal for additional investment; 3. To approve the proposed delivery plan and associated trajectories
for submission to NHS England, To endorse the communications and engagement plan
4. To agree the risk sharing agreement
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 29 of 51
GOVERNING BODY REPORT
2.3 Whilst the provider has tried to remain within a lower cost envelope this posed additional risk in
that the investment may not meet clinical need and deliver the reduced waiting list and improved access identified within the delivery plan.
2.4 The provider ha s submitted an options appraisal identifying 3 options for in vestment and workforce configuration for deci sion. Appendix 2 details the Options Appraisal. Given the complexity of the patients presenting to the service historically requiring step 3 intervention, the Senior Commissioning Lead would recommend that Option 3 is agreed as the preferred option for implementation, this has been further supported by the IST lead following her vi sit to the service and is endorsed by our Mental Health Clinical Lead. Governing B ody are asked to consider the proposals and discuss this recommendation. Option 3 would result in an investment of £616,322 resulting in an overall contract value of £3,475,651.
2.5 The delivery plan attached in Appendix 1 outlines the trajectories to deliver the following
national standards:
Access to first treatment - 18wk (95% per month) Access to first treatment - 6wk (75% per month) Waiting clearance times (<10 weeks) Recovery rate (50% rolling qtr) Access rate (16.8%)
2.6 In line with IST recommendations the provider and CCG have agreed that the primary focus for
service delivery is the removal of the waiting list. The additional waiting list monies will continue (circa 285,000 – 18/19) and the provider will continue to submit bi-weekly patient tracker reports to support the monitoring of the reduction and provide assurance to the CCG. The most recent tracker demonstrates clearance of 559 patients who have been removed from the waiting list since the initiative commenced in November 17. This is in excess of the i nitial projected 400 from the provider.
2.7 It is projected that a continued reduction of circa 147 pat ients per month will be achieved, this
projection has been based on performance to date and will be facilitated through the additional investment identified earlier within the report (£616,322). The provider is current ly exploring alternative solutions to support the waiting list reduction including agency staff, use of digital platforms etc.
2.8 As the primary focus of the service delivery is to reduce the current waiting list, the CCG and
provider have agreed t hat the access target should only be increased once this has been achieved. Given the access level delivered during 2017/18 is currently at 8.82%, it is appropriate that we agree an improvement target of 16.8% access to be delivered with effect from October 2018 once the waiting list has been reduced.
2.9 It is acknowledged that current confidence in the service delivery from key stakeholders and the public are impacting on lower levels of referrals being made to t he service, this in turn is impacting on the ability to achieve access standards and that referrals are more likely to be from the moderate to severe patient cohort.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 30 of 51
GOVERNING BODY REPORT
2.10 The improvement target of 16.8% delivers a stretch to the current provider and will result in an approx. increase of 50% more referrals being needed to deliver the target. In order to manage the risk of any significant increase of referrals, the CCG proposes to increase access levels over the periods 18/19 and 19/20 to ensure patient safety and sufficient workforce capacity to deliver. It is acknowledged that this will not deliver the constitutional target of 19% access for 2018/19.
2.11 The revised trajectories will also allow for robust stakeholder communications and engagement to support the delivery of 16.8% access. The CCG has developed a communication plan to support this achievement. (appendix 3)
2.12 The communication plan has clinical leadership from the Mental Health Clinical lead to support the communication to GPs and other health partners to increase referrals into the service. Further work will be undertaken over the coming weeks to identify which targeted groups should be considered to support this plan i.e. long term conditions and self-referrals including those 65+.
2.13 To support the delivery of the increased capacity the provider has identified the need f or additional premises to support group therapy provision across 5 days a week. The commissioner is currently liaising with public health colleagues to explore alternative venues that could offer this resource; in addition the provider is exploring the possibility of extending current premises and the associated costs.
3 IMPLICATIONS 3.1 To ensure the delivery of the continued reduction of the waiting list and the increase to access
standards there is an additional financial investment required of either £419,671 or £616,322 dependent on which option is agreed.
3.2 Despite the additional investment, the CCG will not meet IAPT constitutional targets relating to access or recovery for 2018/19. The projections identify that access of 16.8% will be achieved on a pro rata basis from October 2018 against national target of 19% and recovery will achieve 40% against national standard of 50%.
3.3 A robust communication plan will need to b e implemented to ensure sufficient referrals from professionals and self-referrals to ensure deliver y of the increased access standard. Current attrition from referral to entering treatment is approx. 40%, therefore to achieve the access standard; there will need to be an average of 950 referrals to the service each month.
3.4 Additional premises need to be secured to ensure delivery of waiting list reduction and increased access without impacting on the investment to increase staffing levels and within the financial envelope.
3.5 Recruitment will need to commence immediately to ensure additional resource is employed to meet planned trajectories, the provider is conf ident that this should be achievable given their understanding of the market and those individuals completing relevant training qualifications. The CCG and provider will continue to work collaboratively to access nat ional training places and training relating to Long Term Condition which will support ongoing natural attrition. The increase of workforce will place the CCG in a stronger position to achieve the access standard of 19% in 2019/20 and any ongoing increases.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 31 of 51
GOVERNING BODY REPORT
3.6 To support the delivery of the plan a risk sharing agreement has been developed to identify the
expectations and accountability of both the CCG and the provider in delivering to the plans. If either party fail to adhere to the principles agreed, this could impact on the successful delivery of the proposed trajectories. Appendix 4 details the risk sharing agreement.
4. CONCLUSION
Governing Body is asked to:-
1. To note update on the IAPT progress 2. To decide on the option appraisal for additional investment 3. To approve the proposed delivery plan and associated trajectories for submission to NHS
England, noting the failure to achieve national constitutional standards 4. To endorse the communications and engagement plan 5. To agree the risk sharing agreement
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 32 of 51
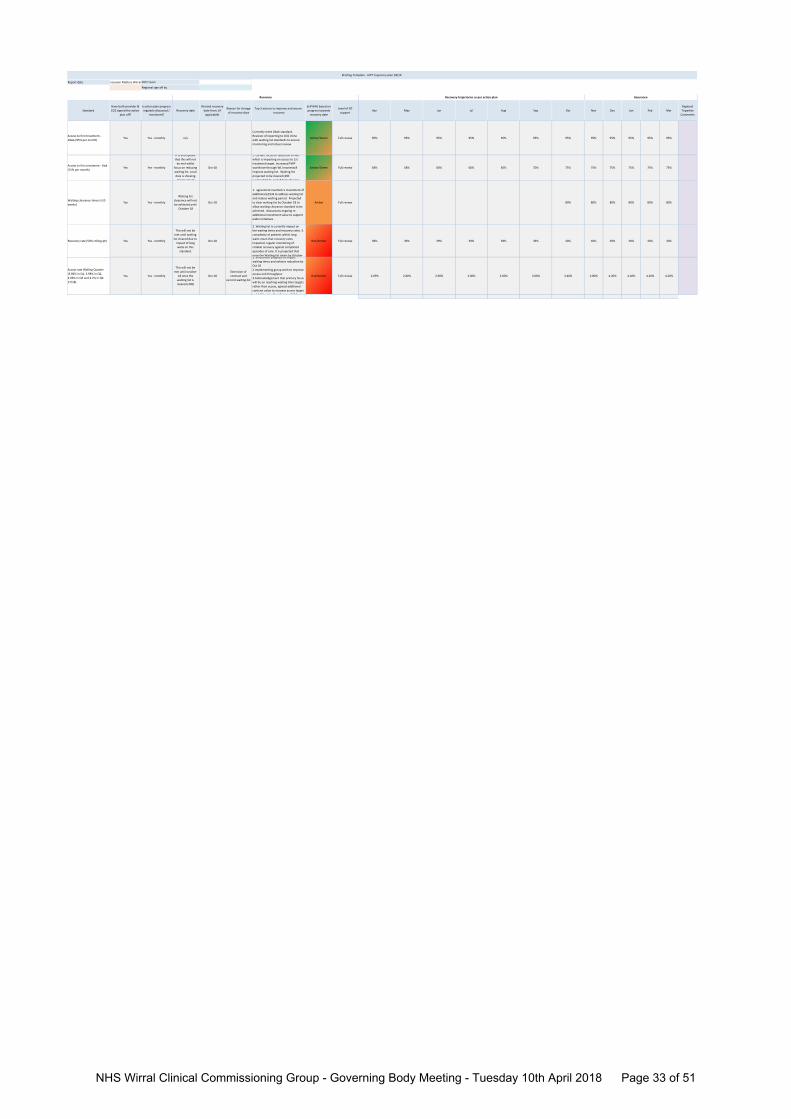
Report date nclusion Matters Wirral
Standard
Have both provider &
CCG signed the action
plan off?
Is action plan progress
regularly discussed /
monitored?
Recovery date
Revised recovery
date from: (if
applicable)
Reason for change
of recovery date
Top 3 actions to improve and secure
recovery
Self‐RAG based on
progress towards
recovery date
Level of IST
supportApr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Regional
Tripartite
Comments
Access to first treatment ‐
18wk (95% per month)Yes Yes ‐ monthly n/a
Currently meet 18wk standard.
Revision of reporting to CCG inline
with waiting list standards to ensure
monitoring and robust review
Amber/Green Full review 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Access to first treatment ‐ 6wk
(75% per month)Yes Yes ‐ monthly
It is anticipated
that this will not
be met whilst
focus on reducing
waiting list. Local
data is showing
improvement
Oct‐18
1. current focus on reduction of WLI
which is impacting on access to 1st
treatment target. Increased PWP
workforce through WLI monieswill
improve waiting list. Waiting list
projected to be cleared (400
sustainable) by end of Sept allowing
Amber/Green Full review 58% 58% 60% 60% 65% 70% 75% 75% 75% 75% 75% 75%
Waiting clearance times (<10
weeks)Yes Yes ‐ monthly
Waiting list
clearance will not
be achieved until
October 18
Oct‐18
1. agreement reached re investment of
additional £253k to address waiting list
and reduce waiting period. Projected
to clear waiting list by October 18 to
allow waiting clearance standard to be
achieved. discussions ongoing re
additional investment value to support
wider initiatives .
Amber Full review 80% 80% 80% 80% 80% 80%
Recovery rate (50% rolling qtr) Yes Yes ‐ monthly
This will not be
met until waiting
list cleared due to
impact of long
waits on this
standard.
Oct‐18
2. Waiting list is currently impact on
the waiting times and recovery rates. 3.
complexity of patients within long
waits mean that recovery rates
impacted, regular monitoring of
reliable recovery against completed
episodes of care. It is projected that
once the Waiting list clears by October
Red/Amber Full review 38% 39% 39% 39% 39% 39% 40% 40% 40% 40% 40% 40%
Access rate (Rolling Quarter
(3.86% in Q1, 3.98% in Q2,
4.09% in Q3 and 4.2% in Q4
17/18)
Yes Yes ‐ monthly
This will not be
met until october
18 once the
waiting list is
cleared (400)
Oct‐18
Extension of
contract and
current waiting list
1. Investment proposal to impact
waiting times and achieve reduction by
Oct 18
2.Implementing group work to improve
access and throughput.
3.Acknowledgement that primary focus
will be on reaching waiting time targets
rather than access, agreed additional
contract value to increase access target
to 16 8% with effect October 2018
Red/Amber Full review 2.69% 2.80% 2.90% 3.00% 3.00% 3.00% 3.40% 3.80% 4.20% 4.20% 4.20% 4.20%
Assurance
Briefing Template ‐ IAPT trajectory plan 18/19
Regional sign off by
Recovery Recovery trajectories as per action plan
DCO Team
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 33 of 51
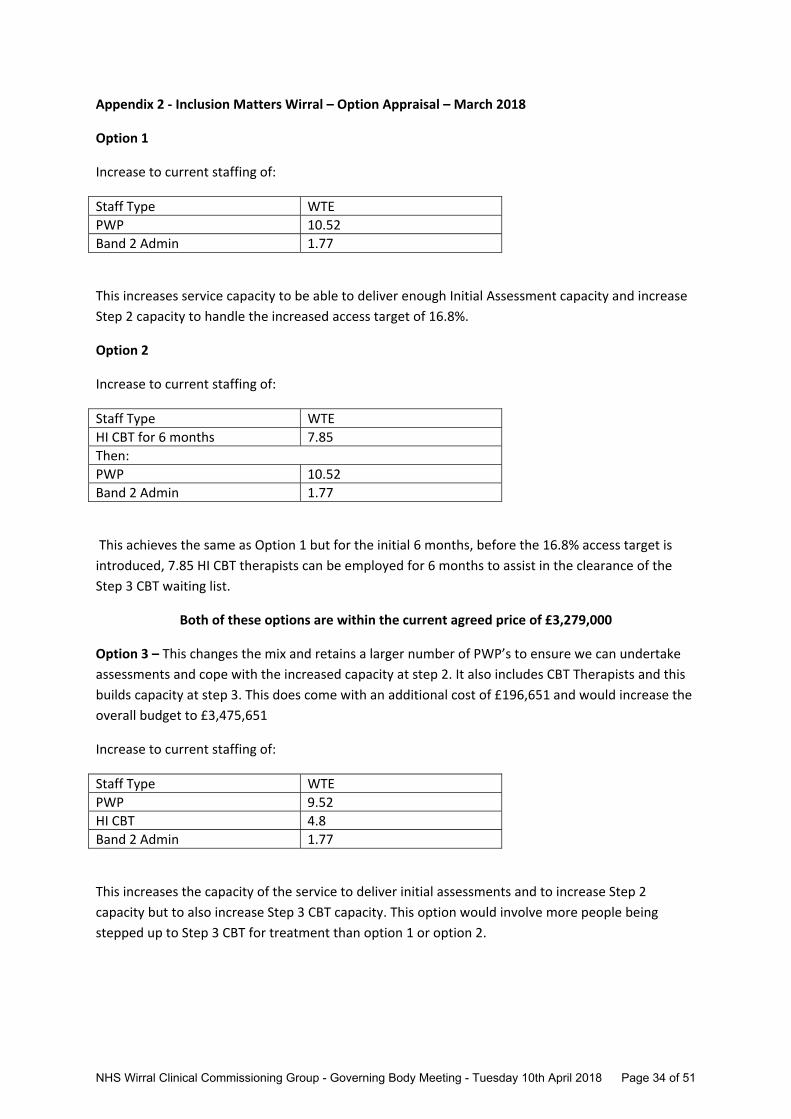
Appendix 2 ‐ Inclusion Matters Wirral – Option Appraisal – March 2018
Option 1
Increase to current staffing of:
Staff Type WTE
PWP 10.52
Band 2 Admin 1.77
This increases service capacity to be able to deliver enough Initial Assessment capacity and increase
Step 2 capacity to handle the increased access target of 16.8%.
Option 2
Increase to current staffing of:
Staff Type WTE
HI CBT for 6 months 7.85
Then:
PWP 10.52
Band 2 Admin 1.77
This achieves the same as Option 1 but for the initial 6 months, before the 16.8% access target is
introduced, 7.85 HI CBT therapists can be employed for 6 months to assist in the clearance of the
Step 3 CBT waiting list.
Both of these options are within the current agreed price of £3,279,000
Option 3 – This changes the mix and retains a larger number of PWP’s to ensure we can undertake
assessments and cope with the increased capacity at step 2. It also includes CBT Therapists and this
builds capacity at step 3. This does come with an additional cost of £196,651 and would increase the
overall budget to £3,475,651
Increase to current staffing of:
Staff Type WTE
PWP 9.52
HI CBT 4.8
Band 2 Admin 1.77
This increases the capacity of the service to deliver initial assessments and to increase Step 2
capacity but to also increase Step 3 CBT capacity. This option would involve more people being
stepped up to Step 3 CBT for treatment than option 1 or option 2.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 34 of 51
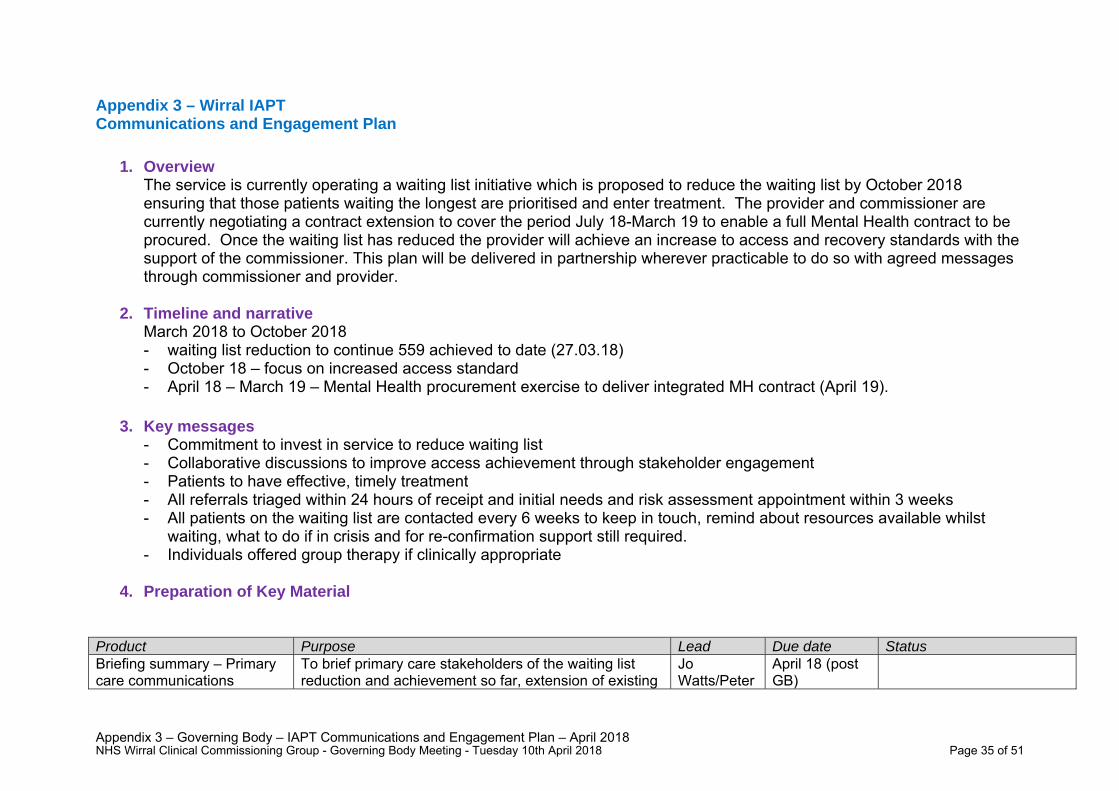
Appendix 3 – Governing Body – IAPT Communications and Engagement Plan – April 2018
Appendix 3 – Wirral IAPT Communications and Engagement Plan
1. Overview
The service is currently operating a waiting list initiative which is proposed to reduce the waiting list by October 2018 ensuring that those patients waiting the longest are prioritised and enter treatment. The provider and commissioner are currently negotiating a contract extension to cover the period July 18-March 19 to enable a full Mental Health contract to be procured. Once the waiting list has reduced the provider will achieve an increase to access and recovery standards with the support of the commissioner. This plan will be delivered in partnership wherever practicable to do so with agreed messages through commissioner and provider.
2. Timeline and narrative March 2018 to October 2018 - waiting list reduction to continue 559 achieved to date (27.03.18) - October 18 – focus on increased access standard - April 18 – March 19 – Mental Health procurement exercise to deliver integrated MH contract (April 19).
3. Key messages - Commitment to invest in service to reduce waiting list - Collaborative discussions to improve access achievement through stakeholder engagement - Patients to have effective, timely treatment - All referrals triaged within 24 hours of receipt and initial needs and risk assessment appointment within 3 weeks - All patients on the waiting list are contacted every 6 weeks to keep in touch, remind about resources available whilst
waiting, what to do if in crisis and for re-confirmation support still required. - Individuals offered group therapy if clinically appropriate
4. Preparation of Key Material
Product Purpose Lead Due date Status Briefing summary – Primary care communications
To brief primary care stakeholders of the waiting list reduction and achievement so far, extension of existing
Jo Watts/Peter
April 18 (post GB)
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 35 of 51
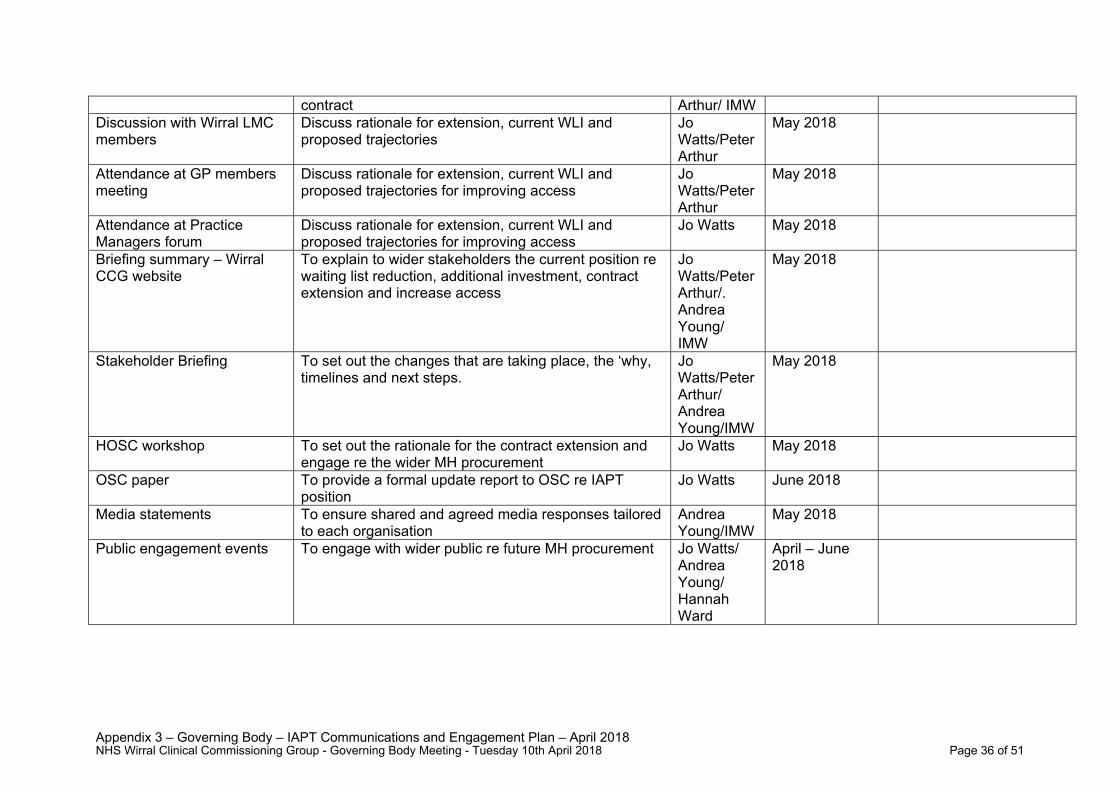
Appendix 3 – Governing Body – IAPT Communications and Engagement Plan – April 2018
contract Arthur/ IMW Discussion with Wirral LMC members
Discuss rationale for extension, current WLI and proposed trajectories
Jo Watts/Peter Arthur
May 2018
Attendance at GP members meeting
Discuss rationale for extension, current WLI and proposed trajectories for improving access
Jo Watts/Peter Arthur
May 2018
Attendance at Practice Managers forum
Discuss rationale for extension, current WLI and proposed trajectories for improving access
Jo Watts May 2018
Briefing summary – Wirral CCG website
To explain to wider stakeholders the current position re waiting list reduction, additional investment, contract extension and increase access
Jo Watts/Peter Arthur/. Andrea Young/ IMW
May 2018
Stakeholder Briefing To set out the changes that are taking place, the ‘why, timelines and next steps.
Jo Watts/Peter Arthur/ Andrea Young/IMW
May 2018
HOSC workshop To set out the rationale for the contract extension and engage re the wider MH procurement
Jo Watts May 2018
OSC paper To provide a formal update report to OSC re IAPT position
Jo Watts June 2018
Media statements To ensure shared and agreed media responses tailored to each organisation
Andrea Young/IMW
May 2018
Public engagement events To engage with wider public re future MH procurement Jo Watts/ Andrea Young/ Hannah Ward
April – June 2018
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 36 of 51
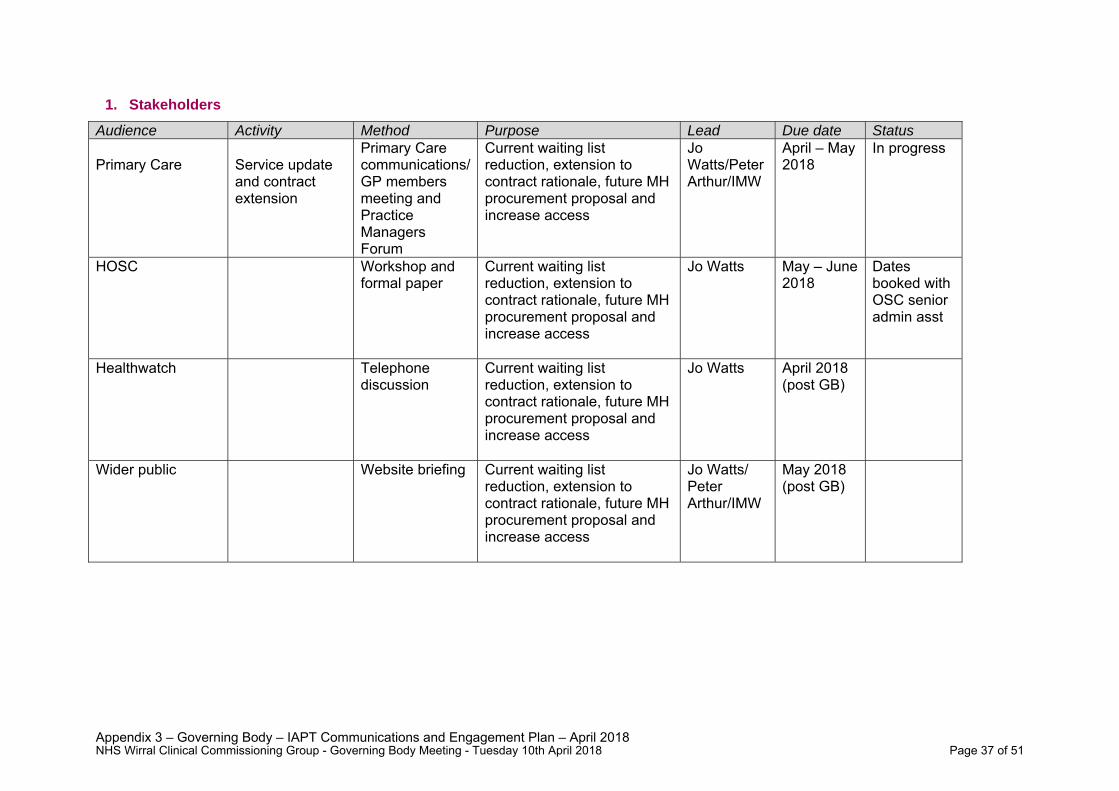
Appendix 3 – Governing Body – IAPT Communications and Engagement Plan – April 2018
1. Stakeholders
Audience Activity Method Purpose Lead Due date Status Primary Care
Service update and contract extension
Primary Care communications/ GP members meeting and Practice Managers Forum
Current waiting list reduction, extension to contract rationale, future MH procurement proposal and increase access
Jo Watts/Peter Arthur/IMW
April – May 2018
In progress
HOSC
Workshop and formal paper
Current waiting list reduction, extension to contract rationale, future MH procurement proposal and increase access
Jo Watts May – June 2018
Dates booked with OSC senior admin asst
Healthwatch Telephone discussion
Current waiting list reduction, extension to contract rationale, future MH procurement proposal and increase access
Jo Watts April 2018 (post GB)
Wider public Website briefing Current waiting list reduction, extension to contract rationale, future MH procurement proposal and increase access
Jo Watts/ Peter Arthur/IMW
May 2018 (post GB)
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 37 of 51
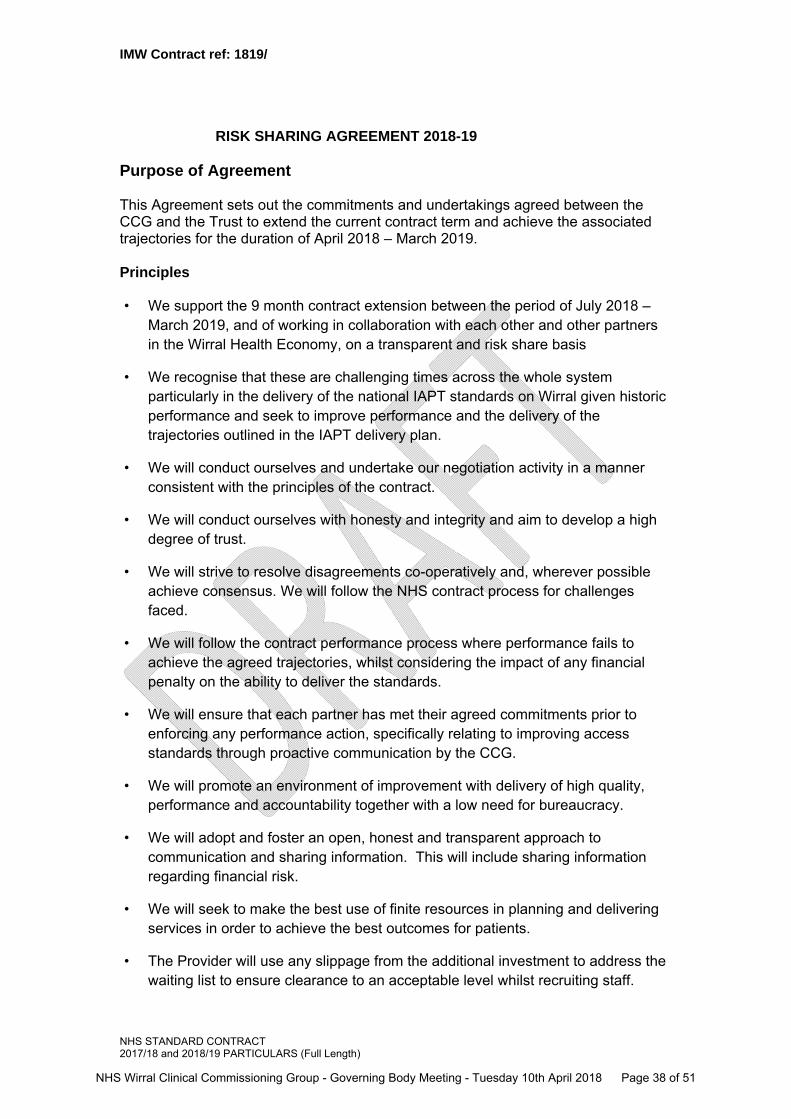
IMW Contract ref: 1819/
NHS STANDARD CONTRACT 2017/18 and 2018/19 PARTICULARS (Full Length)
RISK SHARING AGREEMENT 2018-19
Purpose of Agreement
This Agreement sets out the commitments and undertakings agreed between the CCG and the Trust to extend the current contract term and achieve the associated trajectories for the duration of April 2018 – March 2019. Principles • We support the 9 month contract extension between the period of July 2018 –
March 2019, and of working in collaboration with each other and other partners in the Wirral Health Economy, on a transparent and risk share basis
• We recognise that these are challenging times across the whole system particularly in the delivery of the national IAPT standards on Wirral given historic performance and seek to improve performance and the delivery of the trajectories outlined in the IAPT delivery plan.
• We will conduct ourselves and undertake our negotiation activity in a manner consistent with the principles of the contract.
• We will conduct ourselves with honesty and integrity and aim to develop a high degree of trust.
• We will strive to resolve disagreements co-operatively and, wherever possible achieve consensus. We will follow the NHS contract process for challenges faced.
• We will follow the contract performance process where performance fails to achieve the agreed trajectories, whilst considering the impact of any financial penalty on the ability to deliver the standards.
• We will ensure that each partner has met their agreed commitments prior to enforcing any performance action, specifically relating to improving access standards through proactive communication by the CCG.
• We will promote an environment of improvement with delivery of high quality, performance and accountability together with a low need for bureaucracy.
• We will adopt and foster an open, honest and transparent approach to communication and sharing information. This will include sharing information regarding financial risk.
• We will seek to make the best use of finite resources in planning and delivering services in order to achieve the best outcomes for patients.
• The Provider will use any slippage from the additional investment to address the waiting list to ensure clearance to an acceptable level whilst recruiting staff.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 38 of 51
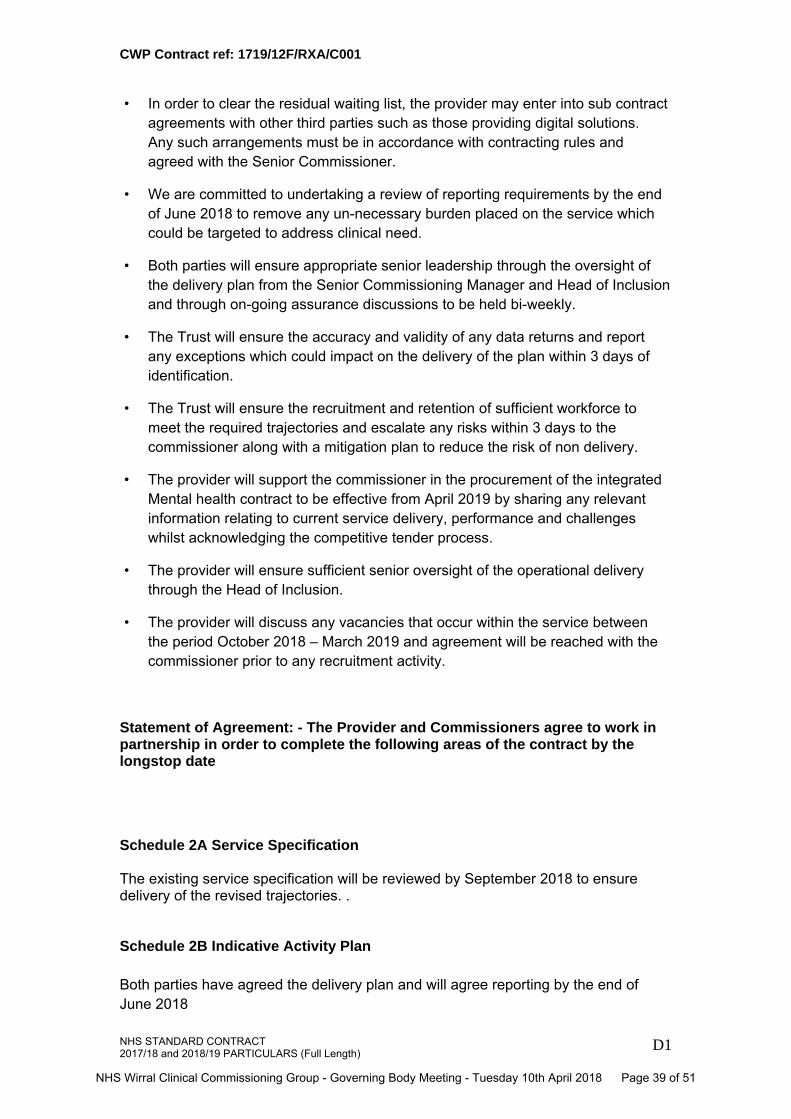
CWP Contract ref: 1719/12F/RXA/C001
NHS STANDARD CONTRACT 2017/18 and 2018/19 PARTICULARS (Full Length)
D1
• In order to clear the residual waiting list, the provider may enter into sub contract agreements with other third parties such as those providing digital solutions. Any such arrangements must be in accordance with contracting rules and agreed with the Senior Commissioner.
• We are committed to undertaking a review of reporting requirements by the end of June 2018 to remove any un-necessary burden placed on the service which could be targeted to address clinical need.
• Both parties will ensure appropriate senior leadership through the oversight of the delivery plan from the Senior Commissioning Manager and Head of Inclusion and through on-going assurance discussions to be held bi-weekly.
• The Trust will ensure the accuracy and validity of any data returns and report any exceptions which could impact on the delivery of the plan within 3 days of identification.
• The Trust will ensure the recruitment and retention of sufficient workforce to meet the required trajectories and escalate any risks within 3 days to the commissioner along with a mitigation plan to reduce the risk of non delivery.
• The provider will support the commissioner in the procurement of the integrated Mental health contract to be effective from April 2019 by sharing any relevant information relating to current service delivery, performance and challenges whilst acknowledging the competitive tender process.
• The provider will ensure sufficient senior oversight of the operational delivery through the Head of Inclusion.
• The provider will discuss any vacancies that occur within the service between the period October 2018 – March 2019 and agreement will be reached with the commissioner prior to any recruitment activity.
Statement of Agreement: - The Provider and Commissioners agree to work in partnership in order to complete the following areas of the contract by the longstop date Schedule 2A Service Specification The existing service specification will be reviewed by September 2018 to ensure delivery of the revised trajectories. . Schedule 2B Indicative Activity Plan Both parties have agreed the delivery plan and will agree reporting by the end of June 2018
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 39 of 51
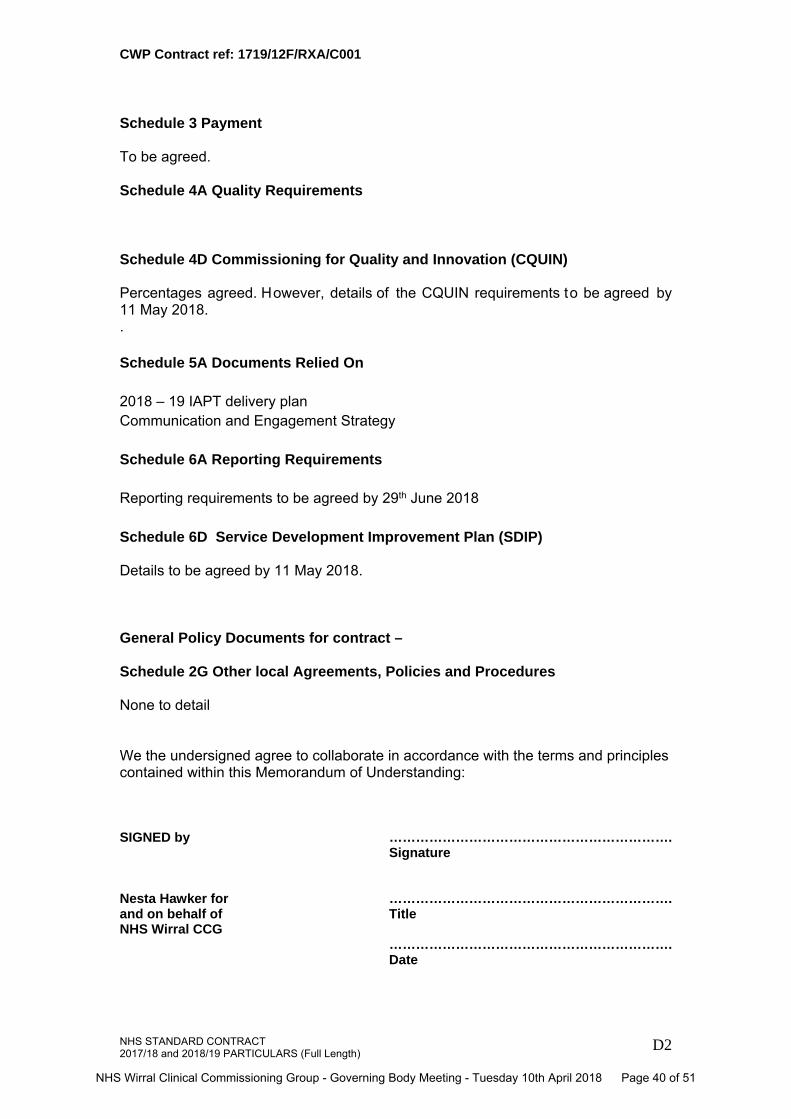
CWP Contract ref: 1719/12F/RXA/C001
NHS STANDARD CONTRACT 2017/18 and 2018/19 PARTICULARS (Full Length)
D2
Schedule 3 Payment To be agreed. Schedule 4A Quality Requirements
Schedule 4D Commissioning for Quality and Innovation (CQUIN) Percentages agreed. However, details of the CQUIN requirements to be agreed by 11 May 2018. . Schedule 5A Documents Relied On 2018 – 19 IAPT delivery plan Communication and Engagement Strategy Schedule 6A Reporting Requirements Reporting requirements to be agreed by 29th June 2018 Schedule 6D Service Development Improvement Plan (SDIP) Details to be agreed by 11 May 2018. General Policy Documents for contract – Schedule 2G Other local Agreements, Policies and Procedures None to detail We the undersigned agree to collaborate in accordance with the terms and principles contained within this Memorandum of Understanding:
SIGNED by
……………………………………………………….Signature
Nesta Hawker for and on behalf of NHS Wirral CCG
……………………………………………………….Title ……………………………………………………….Date
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 40 of 51
CWP Contract ref: 1719/12F/RXA/C001
NHS STANDARD CONTRACT 2017/18 and 2018/19 PARTICULARS (Full Length)
D3
SIGNED by ……………………………………………………….Signature
Neil Carr, Chief Executive, South Staffordshire & Shropshire NHS Foundation Trust
……………………………………………………….Title ……………………………………………………….Date
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 41 of 51
GOVERNING BODY REPORT
1/2
Risk Please indicate Detail of Risk Description
High Medium Low Yes
Clinical engagement taken place Yes
Patient and public involvement taken place Yes
Equality Analysis/Impact Assessment completed No
Quality Impact Assessment No
Strategic Themes
To empower the people of Wirral to improve their physical, mental health and general well being Yes
To reduce health inequalities across the Wirral Yes
To adopt a health and well-being approach in the way services are both commissioned and provided Yes
UPDATE ON WIRRAL HYPERTENSION ACTION PLAN
Agenda Item: 4.2 Reference GB17-18/0077
Public / Private Public Meeting Date 10th April 2018
Lead Officer/Author of paper
Jane Harvey, Consultant in Public Health, Wirral Council Dr Bruce Taylor, GP Clinical Lead, Wirral BP Beacon Project
Contributors Wirral Blood Pressure Beacon Practices Matt Gilmore, CCG Intelligence team
To Approve
To Inform Yes
To Assure Yes
To Endorse
Executive Summary The Wirral Blood Pressure Beacon project was developed towards the end of 2016 in response to the clear need for improved management of high blood pressure and as a key component of the Wirral Blood Pressure Action Plan. The project was set up to run for 2 years and is due to come to an ‘end’ in December 2018. This report represents an interim evaluation of the work. There will also be a verbal update of the supporting activity from the Wirral Blood Pressure Action plan.
Recommendations The Governing Body is asked to: Note the contents of the report Discuss ways to embed the key findings into widespread practice
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 42 of 51
GOVERNING BODY REPORT
2/2
To commission and contract for services that:
Demonstrate improved person centred outcomes Are high quality and seamless for the patient Are safe and sustainable Are evidenced based Demonstrate value for money
Yes
To be known as one of the leading Clinical Commissioning Groups in the country Yes
Provide systems leadership in shaping the Wirral health and social care system so as to be fit for purpose both now and in five years time
Yes
This section gives details not only of where the actual paper has previously been submitted and what the outcome was but also of its development path i.e. other papers that are directly related to the current paper under discussion.
Governance route prior to Governing Body
Meeting Date Objective/Outcome
CCG Governing Body
Quality and Performance Committee
Finance Committee
Audit Committee
Remuneration Committee
Health and Wellbeing Board
Clinical Senate
Quality & Improvement Group
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 43 of 51
1
Interim Evaluation Report (1 year) March 2018
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 44 of 51
2
This report summarises the progress to date of the Beacon Practice Bloo d Pressure project, which is now just over a year into its intende d two yea r lifespan. 1. Why was the project set up?
a. It has long been rec ognised that poorly controlled hypertension carries
significant cardiovascular risk for patients. Almost all of the major types of cardiovascular disease including st roke, ischaemic heart disease, heart failure and Atrial fibrillation hav e hypertension as one of their main aetiological factors.
b. There is clear economic evidence t hat treating hypertension effectively on
a population basis carries significant cost benefits to the NHS over the medium to long term apart from indiv idual benefit to pati ents in terms of reduction of premature morbidity and mortality. In addition, hypertension is simple to diagnose and has a r ange of effective treatments, which have been well documented through successive British Hypertension Society guidelines and robust evidence based NICE standards.
c. There is clear evidence both nationally as well as locally that hypertension
remains both under diagnos ed and under treated. On Wirral it has been calculated that th ere are over 35,000 pat ients with undiagnosed hypertension and of those diagnosed, only 45% are treated to a minimal target of 150/90 (in Canada, where they have been running an outstanding hypertension programme for many years, the figure is now well over 65%). Wide variation across practices is also evident. With all of this in mind, it is clear that there is scope for significant improvement locally.
d. NHS England and Public Health have made treating hypertension a key
priority in recent years. Treating hypertension been accepted as a core work stream in the recent regional card iovascular STP and the public health consortium working across the Mers ey and Cheshire region known as CHAMPS produced an impressive and ambitious strategy in 2016 called ‘Saving Lives, Reducing Press ure’ that seeks to drive coordinate and support work tacking this issue. http://www.champspublichealth.com/sites/default/files/FINAL%20BP%20Strategy%2017.5.16_0.pdf
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 45 of 51
3
2. How was the project set up?
a. After a successful Wirral Hypertension Summit in 2016 and the
establishment of a local hypertension board, the ‘Beacon Practic e Blood Pressure Project’ was developed in order to explore different ways of improving hypertension care within a local primary care setting.
b. Following a selection process (further details av ailable on request), five
practices were chosen to take part. The following four practices remain active in the project (the fifth withdr ew after nine months citing workload commitments, but continues to send in monitoring data):
Paxton Medical Centre Somerville Medical Centre Eastham Medical Centre The Warrens Medical Centre
c. Whilst participation in this project is entirely voluntary, an informal ‘contract’
was set up with each practice that clarif ied the expectations of the practice (eg to attend regular development se ssions, to share data, to develop an action plan) and also clarified the s upport that would be available to the Beacon practices (eg the loan of equi pment, education & training, support with data systems).
d. The project was designed to run for tw o years and is jointly supported by
Wirral CCG and Wirral Public Health. e. Practices were initially tasked with reviewing their current systems, policies
and practices in relation to blood pressure detection and management. They were then asked to develop individual action plans to address the following key issues:
How to increase the numbers of patients being appropriately tested and
diagnosed with hypertension through opportunistic screening and better overall community links
How to manage est ablished hypertension patients more effectively within primary care
How to empower more patients to monitor and treat their own hypertension more effectively
NOTE: A key principle of this project is that practices would have the freedom to test out ways that t hey believe may improve t he management of BP within the practice setting. With this in mind, each practice has chosen to focus upon specific elements of BP management.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 46 of 51
4
3. Activity to date Practices have: a. Produced detailed individual action plans and have continued to meet on a
quarterly basis throughout the progr amme to discuss progress (and barriers).
b. Helped to design and have subsequent ly had access to an interactive
dashboard (produced by the IT department of the CCG) that shows overall progress against NICE standards and numbers of patients treated.
c. Developed their own templates to improve overall data collection within the
practice and to ensure that all appropria te initial inves tigations are being performed.
d. Had access to a training progra mme designed, run and delivered by the
British Heart Foundation (BHF has al so provided some promotional materials).
e. Had dedicated IT training from an independent contractor to help wit h
individual practice template production to enhance data collection and audit capability
f. Contributed to the development of Community Testing Guidelines for
Cheshire & Merseyside (which are now being used widely) g. Contributed to the development of a dedicated EMIS web based template
for the management of blood pressure. h. Led the Primary Care session within the Cheshire & Merseyside BP event
(held in April 2017). The event built on the two years of progress since the C&M High Blood Pressure ‘call to ac tion’ event co-hosted by P HE and Champs in 2015 and was attended by over 60 delegates from a range of sectors and organisations
Related activity: i. Community testing events have tak en place throughout the past year in
order to i ncrease awareness of blood pressure amongst the local population. To date, approximatel y 4,000 tests have been carried out through this route, with an average of 25-27% falling into the ‘higher than optimal’ category and 3% having very high blood pressure (>180mmHg).
j. In March 2017 Champs and PHE with a number of system partners was
successful in a joint bid for Britis h Heart Foundation (BHF) funding to support innovative ways to detect high BP in community settings. A second bid, aimed at increasing testing capacit y within the community, is currently awaiting a decision.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 47 of 51
5
4. Progress and impact to date NOTE: The Wirral Beacon Practice work features significantly in the annual report for the Cheshire & Merseyside Blood Pressure Strategy http://www.champspublichealth.com/news/annual-report-cheshire-merseyside-blood-pressure-strategy-released-today a. The table below compares the per formance of Beacon Practices vs non-
Beacon practices on NICE Hypertension Quality Standards (March 2018). From these figures, the Beacon Practices appear to have demonstrated:
An improved rate of detection of new hypertensives (NM66) which has
been accompanied by a significant r eduction in hidden hypertensives e.g. patients receiving medication but not coded as being hypertensive
A significant increase in adherenc e to the recommended tests as per NICE guidelines (eg NM75/76/77)
b. Whilst performance against the ‘overall BP management’ standards (NM53
and NM54) is showing no significant difference between the two groups, this data is under review. Quer ies run from the indiv idual Beacon Practice systems are showing a much higher per formance than that of the Wirral CCG dashboard. This will be reported on in due course.
Source: Wirral CCG Hypertension dashboard
c. Beacon Practices are now using specific Hypertension templates as a tool
for management of high blood pressure.
d. Levels of self-monitoring have improved. With concerted effort and attention eg highly visible self-testing areas within waiting rooms, it has been possible
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 48 of 51
6
for one of the practices to achieve 8-10% of all BP readings per month to be via self-monitoring.
e. Three of the four Beacon Practi ces have attached pharmacies that have
been registered as Healthy Living P harmacies (HLPs) and are undergoing additional training to enable them to do more BP testing and monitoring of patients with particular emphasis on compliance with medication
5. Discussion points and further recommendations a. Despite working in very challenging times for Primary Care, four out of the
original five practices remain commi tted to the projec t and deserve much credit for doing so. A pragmatic appr oach has been crucial to ma intaining the commitment of the practices invo lved. Acknowledging that progress against action plans must take plac e within the context of changing priorities, pressures, workloads and staff changes has been an important feature of this work to date. Recomm endations arising from this work will not be implemented successfully if the reality of daily life within general practice has not been taken into account.
b. At present, compar ison data of Beacon Practice performance vs non-
Beacon Practices on overall hypertension control (eg NM53) is not reliable enough to share. Reflections from prac tices at this stage is that making improvements to various elements of the system within practice takes time. As is evident from the audit fi gures, clear improvements have been achieved against specific elements of blood pressure management /quality standards, but this cannot yet be tr anslated into overall control improvements.
c. It is increasingly clear that an effective well-motivated, trained and correctly
resourced practice nursing team can lead the delivery of good basic hypertension care. This allows GP principals to focus on confirmation of initial diagnosis, making treatment changes and involvement in more complex cases.
d. The mandatory use of hypertension templates by all relevant clinical staff
would appear to be necessary to ensure good data capture and the organisation of an effective recall system
e. To date, there is little evidence of a significant population shift in the
awareness of good blood pressure control amongst the general population. Whilst this continues to form a major part of the Wirral action plan, Public Health England needs to do more to promote this message and the benefits of healthy lifestyle in treating and preventing the condition. The national ‘Know Your Numbers’ campaign needs greater traction.
f. More support needs to be given to developing and promot ing patient self
empowerment tools including the use of technology eg remote monitoring and health related APPs in relative population groups. This is a major focus of the successful Round 1 BHF bid, which is being led by Champs.
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 49 of 51
7
g. The role of community pharmacy needs to be much more significant
within the BP strategy (both locally and across Cheshire & Merseyside). The recent increase in Health Living Pharmacies has created a potential opportunity. This will be further explored over the coming months.
h. Wirral Public health and CHAMPS have been overwhelming supportive but
CCG involvement to date has been rela tively low key but the necessary implementation of STP polices on hypertension may require Wirral CCG to become more active involv ed in supporting and promoting the Beacon Practice work. The pressure on the need to find short-term solutions to financial pressures by the CCG is understandable, but a long-term investment strategy within practices to improve Hypertension care would pay greater economic benefits
i. With the predicted imminent demis e of the QOF scheme of payments,
urgent CCG consideration should be given to allowing the participation in a Beacon Practice project to be included in any list of incentive payment schemes that until recently have been limited to prescribing, admission and referral rates. Similar incentive pay ments could be offered for other well-evaluated QI schemes
6. Next steps The Beacon Practice BP project has anothe r nine months to run. During this time, practices will continue to implement their individual action plans and we will use the collec tive knowledge and experiences to i nform final recommendations. In addition to the work of the Beacon Practices, local activity will include: Attendance by the project clinical lead, support team and Beacon Practice
representatives at Wirral PLT events in order to share learning on local blood pressure work.
A review of the accuracy of l ocal performance data on NICE quality standards
Continuation of community testing events across Wirral The training of non-clinical staff ac ross a variety of non-NHS settings in
blood pressure testing Exploration of potential to expand the role of community pharmacy Bruce Taylor Jane Harvey GP clinical lead Consultant in Public Health Wirral BP Beacon project Wirral Council
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 50 of 51
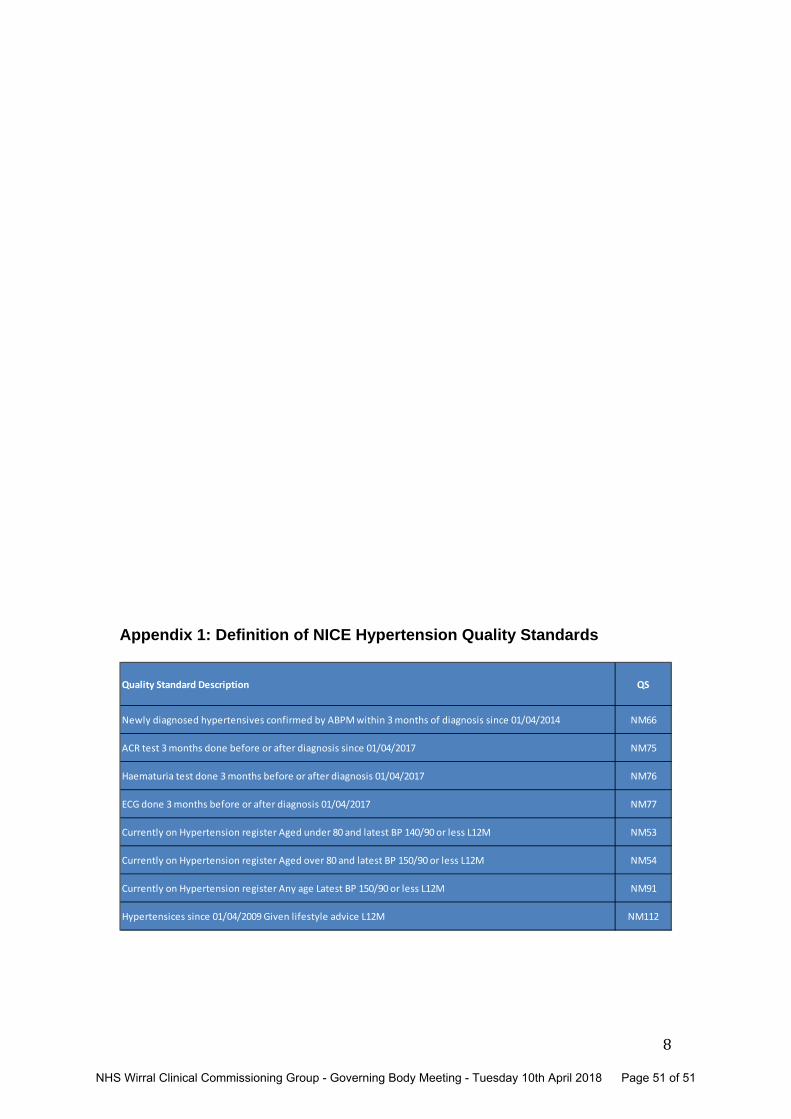
8
Appendix 1: Definition of NICE Hypertension Quality Standards
Quality Standard Description QS
Newly diagnosed hypertensives confirmed by ABPM within 3 months of diagnosis since 01/04/2014 NM66
ACR test 3 months done before or after diagnosis since 01/04/2017 NM75
Haematuria test done 3 months before or after diagnosis 01/04/2017 NM76
ECG done 3 months before or after diagnosis 01/04/2017 NM77
Currently on Hypertension register Aged under 80 and latest BP 140/90 or less L12M NM53
Currently on Hypertension register Aged over 80 and latest BP 150/90 or less L12M NM54
Currently on Hypertension register Any age Latest BP 150/90 or less L12M NM91
Hypertensices since 01/04/2009 Given lifestyle advice L12M NM112
NHS Wirral Clinical Commissioning Group - Governing Body Meeting - Tuesday 10th April 2018 Page 51 of 51


















