
Governing Body Meeting in Public - greenwichccg.nhs.uk body... · Governing Body Meeting in Public...
158
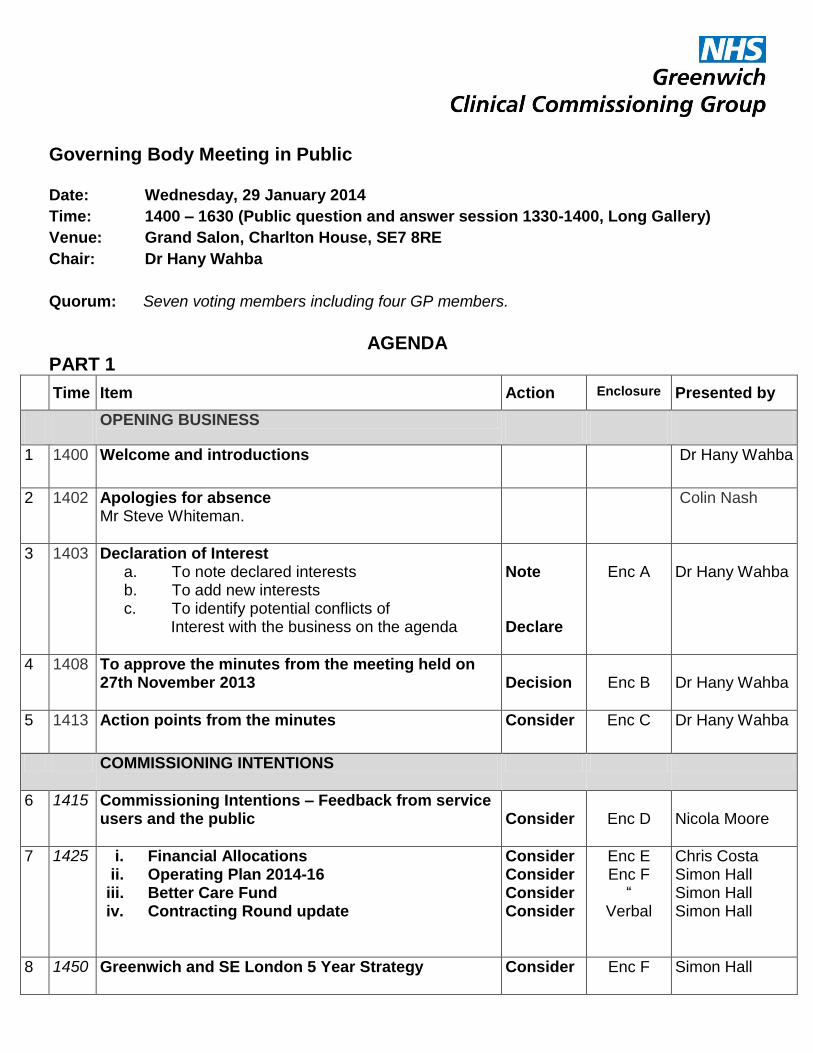
Governing Body Meeting in Public Date: Wednesday, 29 January 2014 Time: 1400 – 1630 (Public question and answer session 1330-1400, Long Gallery) Venue: Grand Salon, Charlton House, SE7 8RE Chair: Dr Hany Wahba Quorum: Seven voting members including four GP members. AGENDA PART 1 Time Item Action Enclosure Presented by OPENING BUSINESS 1 1400 Welcome and introductions Dr Hany Wahba 2 1402 Apologies for absence Mr Steve Whiteman. Colin Nash 3 1403 Declaration of Interest a. To note declared interests b. To add new interests c. To identify potential conflicts of Interest with the business on the agenda Note Declare Enc A Dr Hany Wahba 4 1408 To approve the minutes from the meeting held on 27th November 2013 Decision Enc B Dr Hany Wahba 5 1413 Action points from the minutes Consider Enc C Dr Hany Wahba COMMISSIONING INTENTIONS 6 1415 Commissioning Intentions – Feedback from service users and the public Consider Enc D Nicola Moore 7 1425 i. Financial Allocations ii. Operating Plan 2014-16 iii. Better Care Fund iv. Contracting Round update Consider Consider Consider Consider Enc E Enc F “ Verbal Chris Costa Simon Hall Simon Hall Simon Hall 8 1450 Greenwich and SE London 5 Year Strategy Consider Enc F Simon Hall
Transcript of Governing Body Meeting in Public - greenwichccg.nhs.uk body... · Governing Body Meeting in Public...
Governing Body Meeting in Public
Date: Wednesday, 29 January 2014
Time: 1400 – 1630 (Public question and answer session 1330-1400, Long Gallery)
Venue: Grand Salon, Charlton House, SE7 8RE
Chair: Dr Hany Wahba
Quorum: Seven voting members including four GP members.
AGENDA
PART 1
Time Item Action Enclosure Presented by
OPENING BUSINESS
1 1400
Welcome and introductions Dr Hany Wahba
2 1402
Apologies for absence Mr Steve Whiteman.
Colin Nash
3 1403
Declaration of Interest a. To note declared interests b. To add new interests c. To identify potential conflicts of
Interest with the business on the agenda
Note Declare
Enc A
Dr Hany Wahba
4 1408
To approve the minutes from the meeting held on 27th November 2013
Decision
Enc B
Dr Hany Wahba
5 1413
Action points from the minutes
Consider Enc C Dr Hany Wahba
COMMISSIONING INTENTIONS
6 1415 Commissioning Intentions – Feedback from service users and the public
Consider
Enc D
Nicola Moore
7 1425
i. Financial Allocations ii. Operating Plan 2014-16
iii. Better Care Fund iv. Contracting Round update
Consider Consider Consider Consider
Enc E Enc F
“ Verbal
Chris Costa Simon Hall Simon Hall Simon Hall
8 1450
Greenwich and SE London 5 Year Strategy
Consider Enc F Simon Hall

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
2
9 1500
To note the Procurement Forward Plan
Note Enc H Simon Hall
INTEGRATED GOVERNANCE
10 1505
QUALITY 1. Quality Report 2. Progress Report on Patient Engagement
Consider Consider
Enc I Enc J
Nicola Moore Nicola Moore
11 1525
Finance, QIPP and Performance Report – Month 9
Consider Enc L
Chris Costa
12 1535 Risk Register and Risk Management Report
Consider Enc M and N
Nicola Moore
13 1545 Board Assurance Framework: To note content
Consider Enc O
Nicola Moore
14 1550 NHS Greenwich CCG Constitution update Note Verbal Nicola Moore
15 1555
To ratify Urgent Decisions (Chairs action) under Standing Order 3.10:- a. to approve the extension of the consultation
period for “Right Care, First Time”
Ratify
Enc P
Dr Hany Wahba/ Simon Hall
OPERATIONAL DELIVERY
16 1600 Eltham Community Hospital update Consider Enc Q
Chris Costa
21 1605 Strengthening Delivery – consultation Information Enc V Annabel Burn
FOR INFORMATION ONLY
17 1610 To note confirmed minutes from Governing Body Committees
i. Audit (Part 1) - 4th September 2013 ii. Finance, Performance and QIPP – 28th
October 2013 iii. Quality - 16th October
iv. Market Management and Procurement
Committee – 17th October 2013
Note Note Note Note
Enc R
Enc S Enc T
Enc U
18 1615 Questions from the public related to business on the agenda
Dr Hany Wahba

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
3
19 1630 Date of next meeting The next public meetings are scheduled to take place on:- 26th February 2014, 1330-1630 (Additional Meeting) 26th March 2014, 1330-1630
20 Resolution to move to Part 2 of the meeting To agree that, in accordance with section 1(2) of the Public Bodies (Admissions to Meetings) Act 1960, representatives of the press and members of the public now be excluded from the meeting, because publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted.
Decision Dr Hany Wahba

Enclosure A
Declaration of personal and financial interests - Cumulative 2013/14 Updated: January 2014
PART 1
Members of NHS Greenwich Clinical Commissioning Group
NAME Position/Role Date of
meeting
Potential or actual area
where interest could occur
Action taken to
mitigate risk
Comments
Dr Junaid Bajwa GP Conway PMS
Essential Guides, Director (educational provider for
GPs and GP trainees)
Director (education lead for GPCC
Greenwich LMC, Member
Public Health Associate
Advisor --MSD’s Business Unit GB
7 August
2013
Agenda item 6 Pilot Project Mapping
Across Greenwich
Agenda item was taken off
the agenda 06/08/2013
Bexleyheath, Triager for RMBS
London Deanery, Programme Director VTS
Clinical Director CareTech
Annabel Burn Chief Officer, NHS Greenwich Clinical
Commissioning Group
Trustee of the Greenwich TPCT Charitable Fund,
Charity Commission ref 1097722
Chris Costa Chief Financial Officer, NHS Greenwich Clinical
Commissioning Group
Trustee of the Greenwich TPCT Charitable Fund,
Charity Commission ref 1097722
Councillor John
Fahy
Cabinet member for Health, Adults and Older People
Services, Royal Borough of Greenwich Council
GB
7 August
2013
Agenda item 8a Spending review This declaration was noted
and it was agreed that the
Governing body would
benefit from hearing the
views of the Royal Borough
on this matter and no
conflict arose.
Simon Hall Director of Integrated Commissioning, NHS

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
5
Members of NHS Greenwich Clinical Commissioning Group
NAME Position/Role Date of
meeting
Potential or actual area
where interest could occur
Action taken to
mitigate risk
Comments
Greenwich Clinical Commissioning Group
Dr Eugenia Lee GP Partner in Thamesmead Medical Associate
GB
5 June
2013
Agenda item 12iii – The Support for
Care Homes Local Enhanced
Services
Meeting to be aware of the
interest.
Agenda item 17 – SEL NHS 111
Meeting to be aware of the
interest. No conflict because
information to be discussed
is in the public domain.
Education lead for Population Health London
Deanery
Trustee for Christian Medical Fellowship Charity
Commission Ref 1131658
Education Tutor for PRIME (Partnership in Medical
Education Charity commission ref 1111521
Member of Labour Party (no pay)
GRABADOC Clinical Governance Lead GB
27 Nov
2013
Agenda item 8 – Update of
unscheduled Care
Meeting to be aware of the
interest.
GB
29 Jan
2013
Agenda item 8 – “Right Care, First
Time” update on public consultation
and 15 – Ratify approval of
consultation period for “Right Care,
First Time”
Meeting to be aware of the
interest.
GP Appraiser NHS England
Nicola Moore Director of Integrated Governance, NHS Greenwich
Clinical Commissioning Group
Yemi Osho Director, East London NHS Foundation Trust
Director and Founder of The Wellberry Foundation.
Director, ROTVIC consulting
Bexley CCG, Nurse
Dr Nayan Patel Medical Director GRABADOC GB Agenda item 9 – Tier 1 Meeting to be aware of the
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
6
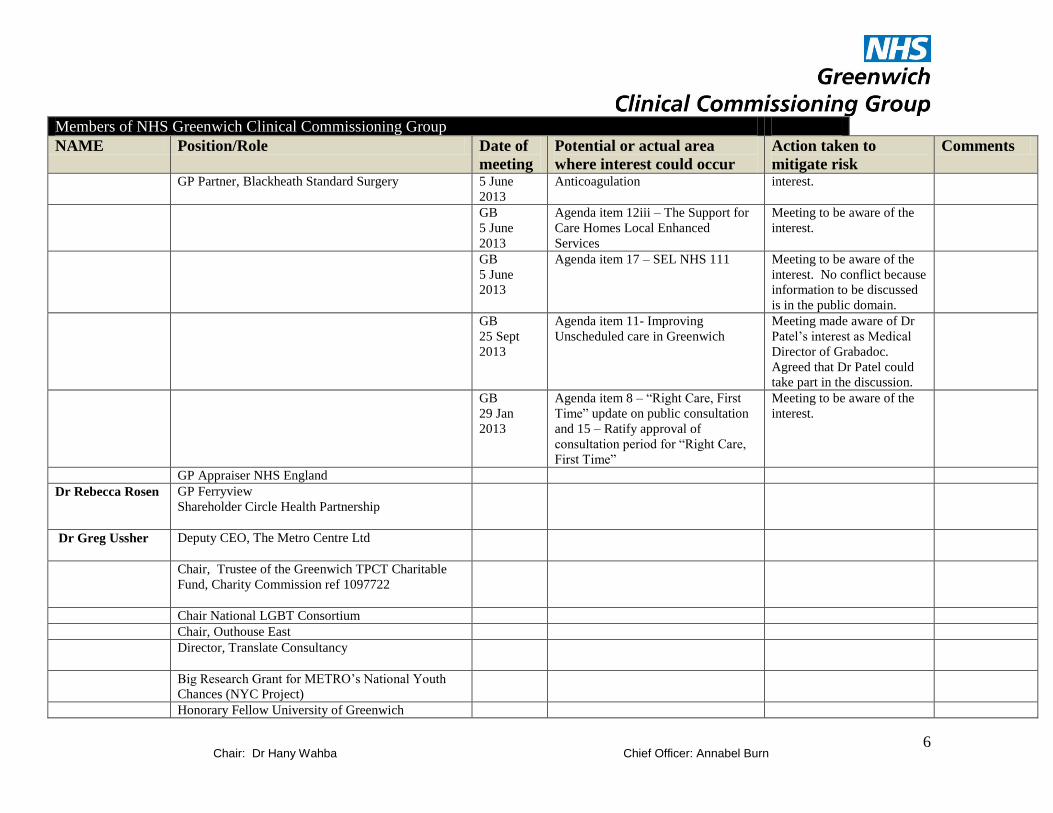
Members of NHS Greenwich Clinical Commissioning Group
NAME Position/Role Date of
meeting
Potential or actual area
where interest could occur
Action taken to
mitigate risk
Comments
GP Partner, Blackheath Standard Surgery 5 June
2013
Anticoagulation interest.
GB
5 June
2013
Agenda item 12iii – The Support for
Care Homes Local Enhanced
Services
Meeting to be aware of the
interest.
GB
5 June
2013
Agenda item 17 – SEL NHS 111
Meeting to be aware of the
interest. No conflict because
information to be discussed
is in the public domain.
GB
25 Sept
2013
Agenda item 11- Improving
Unscheduled care in Greenwich
Meeting made aware of Dr
Patel’s interest as Medical
Director of Grabadoc.
Agreed that Dr Patel could
take part in the discussion.
GB
29 Jan
2013
Agenda item 8 – “Right Care, First
Time” update on public consultation
and 15 – Ratify approval of
consultation period for “Right Care,
First Time”
Meeting to be aware of the
interest.
GP Appraiser NHS England
Dr Rebecca Rosen GP Ferryview
Shareholder Circle Health Partnership
Dr Greg Ussher Deputy CEO, The Metro Centre Ltd
Chair, Trustee of the Greenwich TPCT Charitable
Fund, Charity Commission ref 1097722
Chair National LGBT Consortium
Chair, Outhouse East
Director, Translate Consultancy
Big Research Grant for METRO’s National Youth
Chances (NYC Project)
Honorary Fellow University of Greenwich

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
7
Members of NHS Greenwich Clinical Commissioning Group
NAME Position/Role Date of
meeting
Potential or actual area
where interest could occur
Action taken to
mitigate risk
Comments
Dr Mohammad
Tan Vandal
[until 9.9.13]
Co- Director, Essex Urology services
Spire Hartswood Hospital, Brentwood
NHS Bromley, Tower Hamlets, Havering Barking &
Dagenham, Secondary Care Doctor
Dr Iyngaran
Vanniasegarum
(from 8.1.14)
Director Russets Healthcare Ltd with 25% share
holding
NELFT (North East London Foundation Trust)
Consultant in Audio-Vestibular Medicine
Local Lead for multi-centre research project
(Genetics)
Dr Hany Wahba GP partner at St Mark's Medical Centre.
Will be working to provide minor surgery with
Bromley Health under AQP contract.
Steve Whiteman
Director of Public Health, Royal Borough of
Greenwich Public Health & Wellbeing
Jim Wintour Director, Mountfield Gardens Residents Association
Trustee of the Greenwich TPCT Charitable Fund,
charity Commission ref 1097722
Director, United St Saviour Charity
Dr Ellen Wright GP Vanbrugh PMS GB
5 June
2013
Agenda item 9 – Tier 1
Anticoagulation
Meeting to be aware of the
interest.
Clinical Academic Fellow at Kings College London
Director GPCC

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
8
Members of NHS Greenwich Clinical Commissioning Group
NAME Position/Role Date of
meeting
Potential or actual area
where interest could occur
Action taken to
mitigate risk
Comments
In attendance Alison Goodlad Associate Director Service Redesign
Marion Joynson Associate Director of Finance
Caroline Linden HR Business Partner
Andrew Thomas Associate Director Strategy, Performance and QIPP,
Greenwich Clinical Commissioning Group
Jennifer
Wickenden
Associate Director Acute Commissioning, NHS
South London CSU
Christian Adams Head of Contracting, NHS South London CSU
Maggie Aiken Associate Director Governance and Quality
Commissioning, Greenwich Clinical Commissioning
Group
Langley Gifford Associated Director Integrated Commissioning,
Greenwich Clinical Commissioning Group
Irene Grayson Associate Director Engagement and Organisational
Development (Interim), Greenwich Clinical
Commissioning Group
Dilo Lalande Associated Director Communications & Engagement
(interim)
Rena Amin Joint Chief Pharmacist, Greenwich Clinical
Commissioning Group
Sadhna Murphy Joint Chief Pharmacist, Greenwich Clinical
Commissioning Group

DRAFT Enclosure B
MINUTES OF THE GOVERNING BODY (BUSINESS) MEETING (PART 1)
27th November 2013
Grand Salon, Charlton House
IN ATTENDANCE:
There were 13 members of the public present at the meeting.
121/2013 WELCOME AND INTRODUCTIONS
Dr Wahba welcomed all those attending this public meeting of the Governing Body.
122/2013 APOLOGIES FOR ABSENCE
Dr Hany Wahba Chair
NHS Greenwich CCG
Dr Junaid Bajwa GP Member NHS Greenwich CCG (for part of the meeting)
Mrs Annabel Burn Chief Officer NHS Greenwich CCG
Mr Chris Costa Chief Financial Officer NHS Greenwich CCG
Cllr John Fahy Local Authority Nominee (Non-voting member)
Royal Borough of Greenwich
Dr Eugenia Lee GP Member NHS Greenwich CCG
Ms Yemi Osho Registered Nurse NHS Greenwich CCG
Dr Nayan Patel GP Member NHS Greenwich CCG
Dr Greg Ussher Lay Member (Patient and Public Participation)
NHS Greenwich CCG
Mr Steve Whiteman Acting Director of Public Health (Non-voting member)
Royal Borough of Greenwich
Mr Jim Wintour Vice Chair and Lay Member (Audit, Remuneration and conflicts of Interest)
NHS Greenwich CCG
Ms Maggie Aiken Associate Director Governance and Quality
NHS Greenwich CCG (for Ms Havutcu)
Mr Simon Hall Director of Integrated Commissioning
NHS Greenwich CCG
Mr Colin Nash Corporate Secretary (Minutes) NHS Greenwich CCG
Ms Sherry Scheel Executive Assistant NHS Greenwich CCG
Mr Simon Shenton-Tan
Head of Integrated Commissioning
NHS Greenwich CCG (for item 133/2013)

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
10
Ms Havutcu, Dr Rosen and Dr Wright.
DECLARATION OF INTERESTS
123/2013 a. To note declared interests The Governing Body (GB) NOTED the declaration of personal and financial interests – relevant to the meeting. As recommended in Department of Health guidelines this identified actual or potential conflicts of interest with business on the agenda and the action to be taken to mitigate that risk.
124/2013 b. To add new interests Dr Lee GP Appraiser for NHS England. Clinical Governance Lead for GRABADOC. Dr Patel GP Appraiser for NHS England Dr Ussher Honorary Fellow University of Greenwich
CN/SS
125/2013 c. To identify potential conflicts of interest In addition to the interests recorded in a. above, Dr Lee declared her interest as Clinical Governance Lead for Grabadoc in relation to item 132/2013, Update on Unscheduled Care “Right Care, First Time” Consultation. The Governing Body noted this interest and AGREED that Dr Lee could participate in the discussion of this item. The Declaration of Interests would be updated accordingly.
CN/SS
126/2013 d. Update on declarations from the wider Clinical Commissioning Group
Dr Wahba referred to the paper updating the Governing Body that in addition to the Governing Body Members, the CCG was requesting declarations of interests from the CCG Membership and directly employed staff. The Governing Body NOTED the report.
127/2013 MINUTES OF THE MEETINGS HELD ON 25th SEPTEMBER 2013
The minutes were APPROVED.
128/2013 ACTION POINTS FROM THE MINUTES
The Governing body NOTED that all the actions recorded in Enclosure C had been completed.
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
11
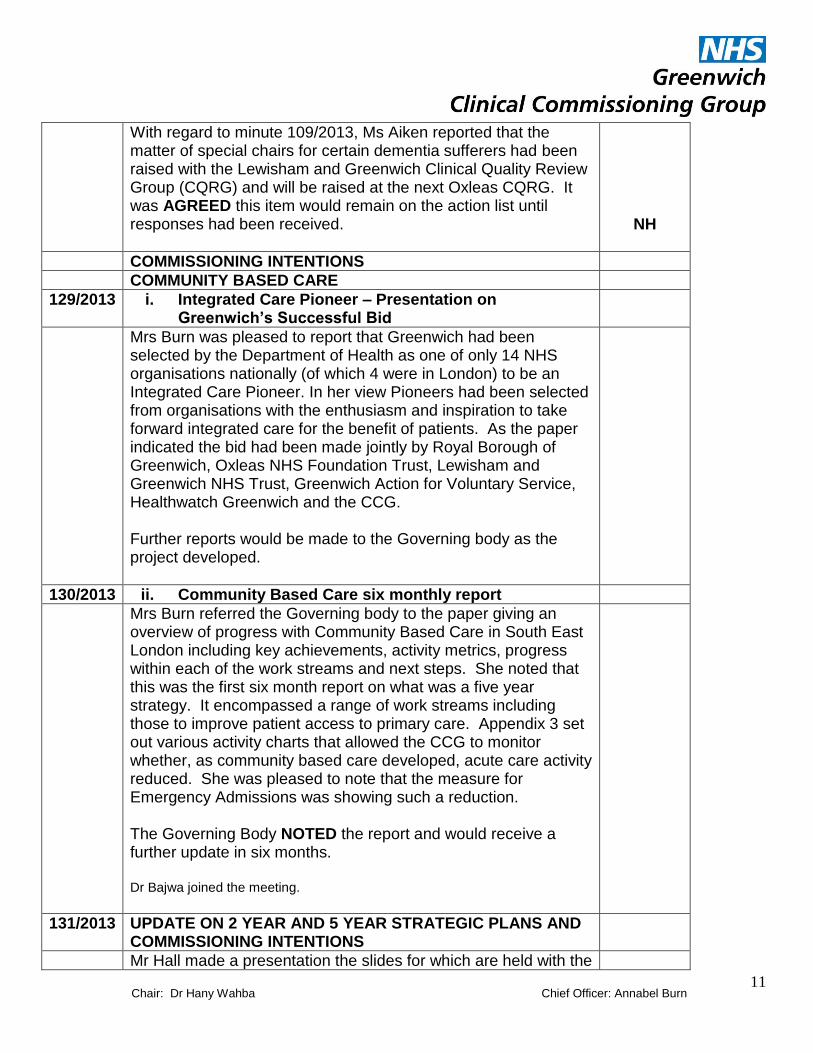
With regard to minute 109/2013, Ms Aiken reported that the matter of special chairs for certain dementia sufferers had been raised with the Lewisham and Greenwich Clinical Quality Review Group (CQRG) and will be raised at the next Oxleas CQRG. It was AGREED this item would remain on the action list until responses had been received.
NH
COMMISSIONING INTENTIONS
COMMUNITY BASED CARE
129/2013 i. Integrated Care Pioneer – Presentation on Greenwich‟s Successful Bid
Mrs Burn was pleased to report that Greenwich had been selected by the Department of Health as one of only 14 NHS organisations nationally (of which 4 were in London) to be an Integrated Care Pioneer. In her view Pioneers had been selected from organisations with the enthusiasm and inspiration to take forward integrated care for the benefit of patients. As the paper indicated the bid had been made jointly by Royal Borough of Greenwich, Oxleas NHS Foundation Trust, Lewisham and Greenwich NHS Trust, Greenwich Action for Voluntary Service, Healthwatch Greenwich and the CCG. Further reports would be made to the Governing body as the project developed.
130/2013 ii. Community Based Care six monthly report
Mrs Burn referred the Governing body to the paper giving an overview of progress with Community Based Care in South East London including key achievements, activity metrics, progress within each of the work streams and next steps. She noted that this was the first six month report on what was a five year strategy. It encompassed a range of work streams including those to improve patient access to primary care. Appendix 3 set out various activity charts that allowed the CCG to monitor whether, as community based care developed, acute care activity reduced. She was pleased to note that the measure for Emergency Admissions was showing such a reduction. The Governing Body NOTED the report and would receive a further update in six months. Dr Bajwa joined the meeting.
131/2013 UPDATE ON 2 YEAR AND 5 YEAR STRATEGIC PLANS AND COMMISSIONING INTENTIONS
Mr Hall made a presentation the slides for which are held with the

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
12
papers for the meeting. Slide 1 described the planning guidance for CCGs issued by NHS England. Mr Hall highlighted that all CCGs had had a proportion of their funding placed into an Integrated Transformation Fund which could only be accessed through a joint plan agreed with the Local Authority. He also highlighted that the CCG had begun a consultation process with its membership and the public on its commissioning intentions. Mr Costa referred to the London Region Proposed Planning Assumptions, set out in slide 3. Although these would not be confirmed until mid-December he was pleased to note that the proposed assumptions were consistent with those to which the CCG was already planning. The only new assumptions were those concerning the new Integrated Transformation Fund. Slide four described the local population characteristics and health needs. Progress had been made with teenage conceptions, childhood immunisation rates, maternity outcomes for mothers and children, mortality from infectious diseases and infant mortality. However challenges remained with regard to obesity, physical inactivity, healthy eating, alcohol consumption and related conditions, HIV/STI incidence the prevalence of common mental health illness. The CCG‟s commissioning intentions should aim to address these priorities. In addition, NHS England compared each CCG with 10 similar peers, to identify areas where they believe improvements in quality and value for money could be made. This “Commissioning for Value” exercise had identified seven potential areas (see slide 7). The CCG would be expected to address these in its commissioning intentions too. Mr Hall then took the meeting through the slides describing the CCG‟s existing commissioning priorities and existing plans to meet them. He was pleased to report that the business case for the Eltham Community Hospital had recently received a letter of support from NHS England. Finally Mr Hall drew attention to the Emerging commissioning Themes for 2014-16, set out in slide 11. Dr Lee expressed her support for plans aimed at prevention of ill health and those developing partnership working.
Mrs Burn noted that the CCG aimed to present plans to address

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
13
its commissioning intentions to the January Governing body meeting. Mr Hall replied that there was a process to do this that included discussion at the Health and Wellbeing Board.
SH
Cllr Fahy made two points. Firstly, in an environment of continuing financial restraint, would the CCG be able to ensure that commissioned services remain located within the Borough. Secondly, he emphasised the importance of commissioned services that addressed the health needs of the population as identified in the Joint Strategic Needs Assessment (JSNA). He also suggested, given the large number of priorities, whether the CCG could focus upon a smaller number initially. Mrs Burn replied that the CCG was funded to provide health services for local people and this funding would follow the patient wherever they were treated. The CCG was required to develop a five year strategy in conjunction with its fellow South East London CCGs, but it was to the advantage of local people, that services across the sector were aligned as far as possible. With regard to priorities, the CCG had to keep in mind that, in order to improve the health of the local population as speedily as possible, it would be necessary for it to make progress in a range of priority areas. Dr Ussher wished to ensure that the health needs identified in slide four were adequately reflected in the commissioning intentions. Mr Hall replied that the CCG responsibility for HIV/STI incidence had now passed to NHS England. The CCG would ensure the remainder were appropriately reflected. He also noted that the CCG was discussing its intentions with the public through a Reference Group. He felt however it would be too soon for that Group to report before the January Governing Body meeting. Mrs Burn replied that although the January meeting would discuss commissioning plans, they would not be signed off until March and this would allow time for the Reference Group to inform the process.
132/2013 UPDATE ON UNSCHEDULED CARE: “ RIGHT PLACE, FIRST TIME” CONSULTATION
Mr Hall referred to the consultation document included with the papers. The consultation process had commenced and so far, attendance at public consultation events had been good. It was hoped to be able to arrange at least one event over the weekend so that those who worked during the week had an opportunity to participate.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
14
133/2013 PERSONALISED HEALTH BUDGETS – PRESENTATION ON NHS GREENWICH‟S PILOT PROJECT
Dr Wahba welcomed Mr Simon Shenton-Tan who made a slide presentation (slides held with the papers for the meeting) highlighting the following points. The initiative to personalise healthcare was now around 10 years old. In 2009 the PCT had successfully applied to become a pilot site for personalised budgets for certain patients with either mental health or learning difficulties. The current plans built upon the lessons learned and the CCG had adopted an integrated approach with the Royal Borough of Greenwich (RBG). From 1st April 2014 adults eligible for NHS Continuing Healthcare will have a right to ask for a personalised health budget (PHB), including direct payment for healthcare. From October 2014, those patients will have a right to have a personalised health budget. These rights also apply to parents of children and young people eligible for support under the National Framework for Children and Young People‟s Continuing Care. From April 2015, CCGs will be expected to offer PHBs to other people with long term conditions likely to benefit from increased choice and control. PHBs were intended to give patients greater choice, control and support to achieve the health and wellbeing outcomes they desired. They would also require a different conversation between patients and health professionals, where shared decision making was the norm. PHBs required a system that facilitated freedoms and flexibilities with appropriate checks and balances. Mr Shenton-Tan took the meeting through the progress made with PHBs within Greenwich to date, as set out in the slides. He emphasied that all PHBs must be supported by a care plan. The CCG would also be using a new resource allocation system that ensured resources are allocated equitably and ethically and based upon the needs of the patient and the respite needs of their carers. The CCG had also commissioned “eformsapp” to automatically populate the five patient facing continuing health care forms saving a large amount of data entry time for professionals.
Mr Wintour commended the joint approach with RBG and the voluntary sector. He asked that the Governing Body receive information about the number of patients on PHBs on an on-
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
15
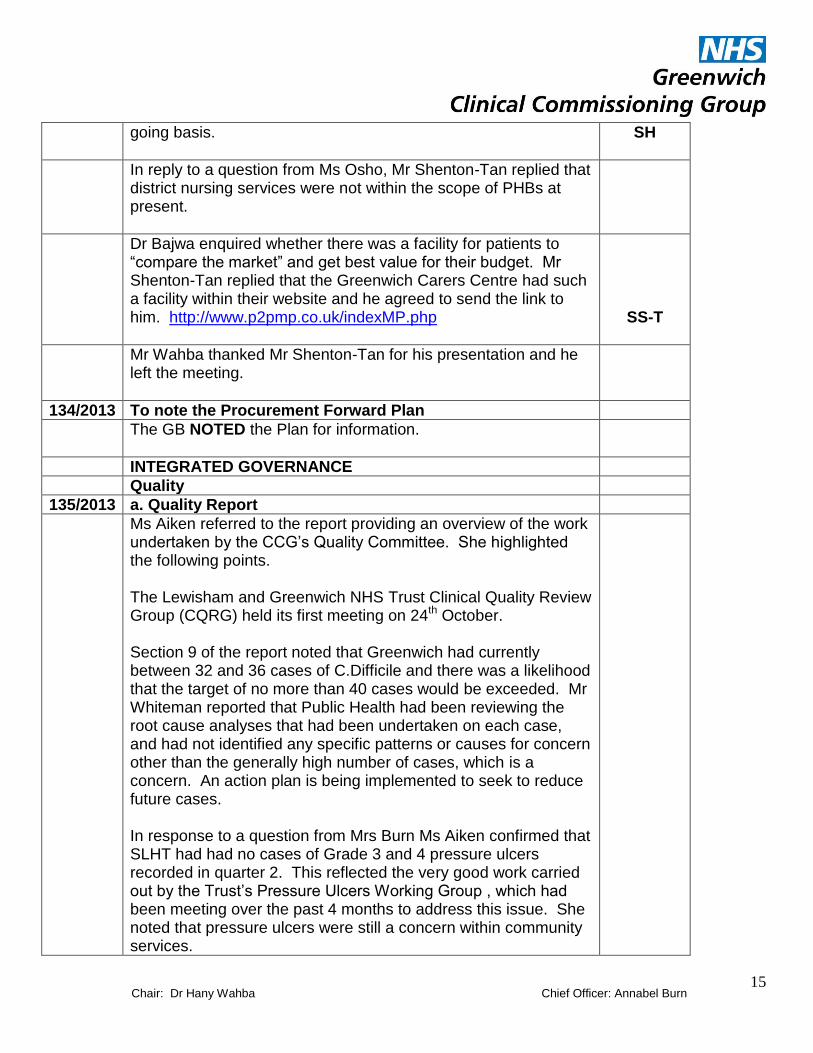
going basis.
SH
In reply to a question from Ms Osho, Mr Shenton-Tan replied that district nursing services were not within the scope of PHBs at present.
Dr Bajwa enquired whether there was a facility for patients to “compare the market” and get best value for their budget. Mr Shenton-Tan replied that the Greenwich Carers Centre had such a facility within their website and he agreed to send the link to him. http://www.p2pmp.co.uk/indexMP.php
SS-T
Mr Wahba thanked Mr Shenton-Tan for his presentation and he left the meeting.
134/2013 To note the Procurement Forward Plan
The GB NOTED the Plan for information.
INTEGRATED GOVERNANCE
Quality
135/2013 a. Quality Report
Ms Aiken referred to the report providing an overview of the work undertaken by the CCG‟s Quality Committee. She highlighted the following points. The Lewisham and Greenwich NHS Trust Clinical Quality Review Group (CQRG) held its first meeting on 24th October. Section 9 of the report noted that Greenwich had currently between 32 and 36 cases of C.Difficile and there was a likelihood that the target of no more than 40 cases would be exceeded. Mr Whiteman reported that Public Health had been reviewing the root cause analyses that had been undertaken on each case, and had not identified any specific patterns or causes for concern other than the generally high number of cases, which is a concern. An action plan is being implemented to seek to reduce future cases. In response to a question from Mrs Burn Ms Aiken confirmed that SLHT had had no cases of Grade 3 and 4 pressure ulcers recorded in quarter 2. This reflected the very good work carried out by the Trust‟s Pressure Ulcers Working Group , which had been meeting over the past 4 months to address this issue. She noted that pressure ulcers were still a concern within community services.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
16
Referring to the Integrated Quality Dashboard on page 3 of the report, Dr Patel noted the poor performance with regard to complaint response times at SLHT, Kings and Lewisham Trusts. Mrs Burn acknowledged that that this had been an on-going problem. She noted that there were proposals to change the national NHS complaints procedure to improve performance. Ms Aiken added that complaints performance was monitored every month as part of the Lewisham and Greenwich Trust Recovery Plan. In response to a question from Cllr Fahy, Mrs Burn replied that the CCG‟s Quality Committee received detailed information on complaints performance as did the Boards of the provider organisations. The Governing Body NOTED the report.
136/2013 b. Six monthly report on implementation of the Francis Report Action Plan
Ms Aiken referred the Governing Body to the report describing progress against the two overarching themes emerging from the Francis Report. Mr Wintour emphasised the importance of the CCG listening to its staff and developing ways to improve this. Dr Ussher enquired about the systems and processes providers have in place to listen to staff and patients. Mrs Burn replied that the CCG wished to give Lewisham and Greenwich Trust, as a new provider organisation, time to develop and implement a suitable structure. The CCG would monitor this process closely and support the new organisation in this work. Dr Lee added that the GP alert sytem, which enabled GPs to flag quality concerns which could be escalated with providers when necessary, was proving a helpful quality tool with which the GP Membership were becoming increasingly familiar. Dr Patel left the meeting.
137/2013 c. NHS Greenwich CCG response to “A Promise to Learn- Commitment to Act”: Improving the Safety of Patients in England
Ms Aiken referred to the paper summarising the ten recommendations made by Professor Berwick, who had been asked by the Prime Minister to review patient safety in the light of
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
17
the Francis Report. The recommendations, set out on page three of the paper, aimed to enable NHS bodies to become learning organisations. The Governing Body NOTED the report.
138/2013 d. Progress report on Patient Engagement
Ms Aiken referred to the paper updating the Governing Body on progress being made with communications and patient and public engagement within the CCG. Dr Ussher drew attention to the Patient Engagement Programme Board with representation from Healthwatch, Public health, Greenwich Action for Voluntary Services and Citizen UK. This Board would be responsible for developing, implementing and reviewing progress on the CCG‟s public involvement strategy. The GB NOTED the report.
139/2013 Finance, QIPP and Performance Report – Month 7
Mr Costa Referred the Governing Body to the Executive Summary on page 3 of the report. He was pleased to report that the CCG was expecting to meet all its financial targets for the year and this expectation had been confirmed by NHS England. There were over spends netted off by underspends and these were summarised on page 6 of the report. Cllr Fahy enquired whether the overspend on acute care was the result of reductions in the non-acute budget. Mr Costa replied that the reductions in non-acute expenditure were mainly the result of the CCG enabling more patients to receive their care within the local area, rather than a reduction in the amount of care and treatment delivered. The CCG was also expecting to meet its QIPP target for the year. This was shown in Section 6 of the report. Some schemes had not achieved the savings anticipated, but these were expected to deliver later in the year and would contribute to the QIPP in 2014/15. NHS Constitution Standards The CCG‟s performance against the NHS Constitution Standards had deteriorated over the month, as shown in section 7. With regard to the 4 hour A&E target, Mr Hall reported that as a challenged trust, SLHT had received additional funding to improve its performance. The CCG had committed additional
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
18
resources too and had expanded the capacity of the Urgent Care Centre at Queen Elizabeth Hospital. It had also opened an additional 14 intermediate care beds to improve the throughput of patients at the hospital. It was anticipated that these additional measures would lift performance to 93% of patients being seen within 4 hours in the New Year, but unlikely to allow the target to be meet for the full year. Mr Hall reassured the Governing Body that patients who were waiting over 4 hours were being cared for appropriately at the hospital. Mrs Burn added that the Clinical Quality Review Group were overseeing the plans to improve A&E performance. She was pleased to report a high level of cooperation from all those involved. In response to a question from Cllr Fahy she confirmed that the funding for challenged trusts, referred to above was separate from the Winter Pressures money released by the Department of Health. The CCG had submitted a bid for the latter and were awaiting news on whether or not this had been successful. Dr Lee emphasised the importance of ensuring that all clinically fit patients were discharged from hospital, with any necessary support, as soon as possible. NHS Outcomes Framework Mr Costa also reported deterioration in the performance against the NHS Outcome Framework Indicators, as set out in Section 8. One of the measures used was the potential years of life lost from causes amendable to healthcare. There had been an improvement in this measure for males but that for females had declined. Mr Costa cautioned that the data upon which the measures were based pre dated the creation of the CCG. The Governing Body NOTED the report.
140/2013 Risk Register and Risk Management Report
The Governing Body NOTED the current Risk Register for the CCG. Mrs Burn took the Governing Body through the Risk Management Performance Report for November and drew attention to a new box on page 2 listing the risks on the register by type. Referring to the risks rated 12 and above she asked the Governing Body to note the target rating and where this had not been achieved, the actions the CCG was taking to reach it. No

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
19
new risks had been added to the Register during the month. In response to a question by Dr Lee Mrs Burn confirmed that risk 109 on the Register covered these issues with regard to A&E performance discussed above. The Governing Body NOTED the report.
141/2013 Board Assurance Framework: To note Progress
Mrs Burn referred to the report updating the Governing Body on the CCG‟s progress against its strategic objectives. The table identified the risks to those objectives, internal controls and assurance, gaps in those controls and assurances and planned actions to address them. The aim was to ensure each objective was green by the end of the financial year. The Governing Body considered those objectives currently red or amber. Objective 5, enhancing the use of information on all aspects of commissioning (the only red item), was red because of the current restrictions on the CCG using patient confidential information to support is commissioning function.
As a new report, Mrs Burn asked members to let Ms Havutcu know if they felt any improvements in formatting could be made. The Governing Body NOTED the report.
ALL
142/2013 To ratify Urgent Decisions (Chair‟s Action) under Standing Order 3.10 To approve amendments to the CCG Constitution To approve the appointment of Grayling to conduct the Unscheduled Care Consultation To approve the Quarter 2 Balanced Scorecard self-assessment
This item was taken after 134/2013.
The Governing Body considered the three papers explaining the urgent decisions made between meetings and RATIFIED those decisions.
OPERATIONAL DELIVERY
143/2013 Information Governance and Accredited Safe Haven (ASH) Update
Mr Costa referred to the paper informing the Governing Body that the CCG had raised its performance against the Information Governance Toolkit requirements necessary to apply for ASH

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
20
accreditation. ASH accreditation was required for CCGs to be regarded as organisations trusted to handle certain confidential data necessary to achieving their strategic objectives. The ASH application had been passed to the relevant team within NHS England for approval and the CCG was waiting to hear when its application would be considered. Mr Wintour emphasised the importance of an early decision so the CCG could make progress in a number of key areas dependent upon the analysis of data it was currently not permitted to handle. On behalf of the Governing Body he commended the CCG‟s staff (and particularly the Data Analysis Department) for their work in undertaking information governance training and making the other changes necessary to make the ASH application. The Governing Body NOTED the report.
144/2013 Election of seventh GP Member of the Governing Body
Dr Wahba referred the Governing Body to the paper informing them that in December recruitment to the vacant GP position on the Governing Body would commence. Applicants must have practiced as a GP in Greenwich for at least two years, hold a contract with NHS Greenwich, or a contact of employment with a Greenwich general practice and be on the Greenwich GP Performers List. The Governing Body NOTED the report.
FOR INFORMATION ONLY
145/2013 To note confirmed minutes from Governing Body Committees Finance, Performance and QIPP (9th September 2013) Quality (21st August and 23rd September 2013) Market Management and Procurement (17th September 2013)
The GB NOTED the minutes.
146/2013 QUESTIONS FROM MEMBERS OF THE PUBLIC RELATED TO BUSINESS ON THE AGENDA
These were recorded, together with those asked in the question and answer session before the Governing Body meeting, in a separate document.
147/2013 DATE OF NEXT MEETING

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
21
The next public meeting was scheduled for 1400-1630, Wednesday 29th January 2013, at, Charlton House. A public question and answer session would precede the meeting between 1330-1400.
148/2013 RESOLUTION TO MOVE TO PART 2 OF THE MEETING
The Governing Body APPROVED the motion that, in accordance with section 1(2) of the Public Bodies (Admissions to Meetings) Act 1960, representatives of the press and members of the public now be excluded from the meeting, because publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted.
ACRONYMS
ASH Accredited Safe Haven
BAF Board Assurance Framework
CCG Clinical Commissioning Group
CQRG Clinical Quality Review Group
CSU Commissioning Support Unit
GB Governing Body
PHB Personal Health Budget
QIPP Quality, Innovation, Productivity and Prevention
RBG Royal Borough of Greenwich
SLHT South London Healthcare NHS Trust

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
22
Enclosure C
ACTIONS FROM – GOVERNING BODY
Date 27.11.13
Minute number
Action Action owner
To be completed by
Comments
ACTIONS BROUGHT FORWARD
QUESTIONS FROM MEMBERS OF THE PUBLIC RELATED TO BUSINESS ON THE AGENDA
108/2013 Raise with providers the use of special seating to prevent certain dementia patients from wandering and causing a danger to themselves.
NH As soon as possible
ACTIONS FROM THIS MEETING
125/2013 c. To identify potential conflicts of interest
Update declarations of interest in line with the minutes.
CN/SS As soon as possible.
131/2013 UPDATE ON 2 YEAR AND 5 YEAR STRATEGIC PLANS AND COMMISSIONING INTENTIONS
Present plans to implement Commissioning Intentions to the next public Governing Body meeting.
SH 29.1.14
133/2013 PERSONALISED HEALTH BUDGETS
Provide information on the numbers of patients on PHBs possibly as part of the Performance report.
SH/CC As soon as possible
141/2013 Board Assurance Framework
Inform Ms Havutcu of any improvements in the format of the report could be made.
ALL
If necessary
Colin Nash 6.12.13
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
23
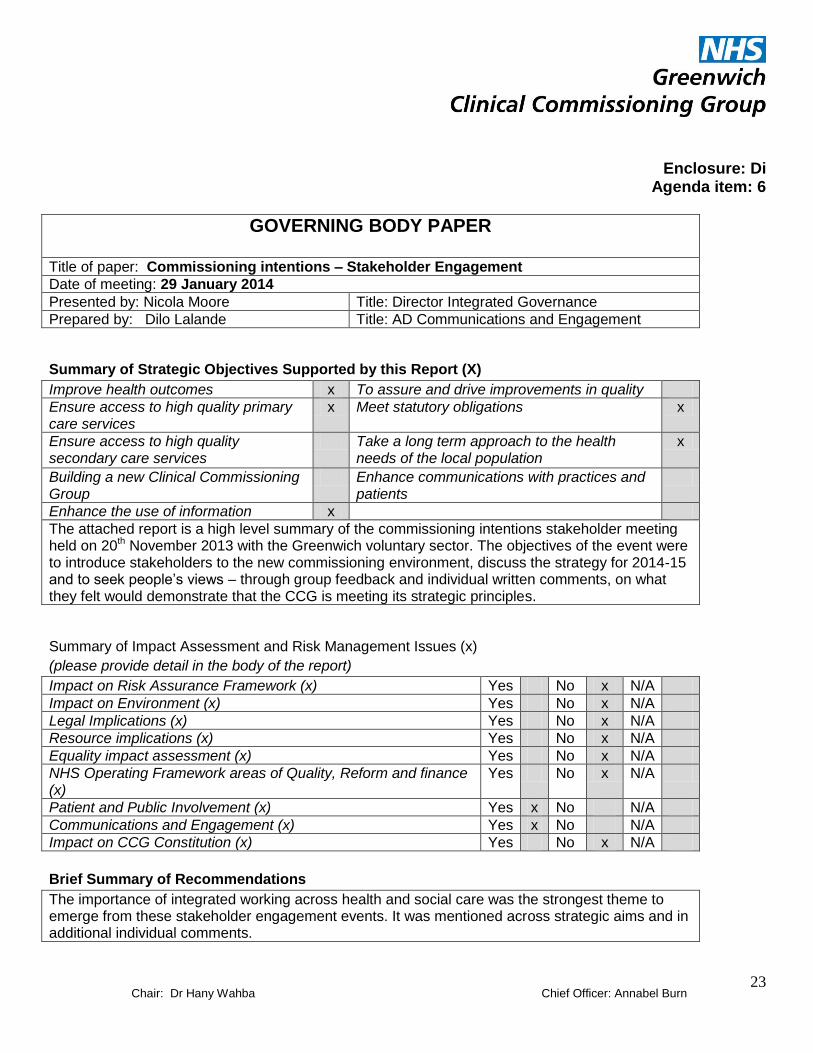
Enclosure: Di Agenda item: 6
GOVERNING BODY PAPER
Title of paper: Commissioning intentions – Stakeholder Engagement
Date of meeting: 29 January 2014
Presented by: Nicola Moore Title: Director Integrated Governance
Prepared by: Dilo Lalande Title: AD Communications and Engagement
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes x To assure and drive improvements in quality
Ensure access to high quality primary care services
x Meet statutory obligations x
Ensure access to high quality secondary care services
Take a long term approach to the health needs of the local population
x
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
Enhance the use of information x
The attached report is a high level summary of the commissioning intentions stakeholder meeting held on 20th November 2013 with the Greenwich voluntary sector. The objectives of the event were to introduce stakeholders to the new commissioning environment, discuss the strategy for 2014-15 and to seek people‟s views – through group feedback and individual written comments, on what they felt would demonstrate that the CCG is meeting its strategic principles.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes No x N/A
Impact on Environment (x) Yes No x N/A
Legal Implications (x) Yes No x N/A
Resource implications (x) Yes No x N/A
Equality impact assessment (x) Yes No x N/A
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes No x N/A
Patient and Public Involvement (x) Yes x No N/A
Communications and Engagement (x) Yes x No N/A
Impact on CCG Constitution (x) Yes No x N/A
Brief Summary of Recommendations
The importance of integrated working across health and social care was the strongest theme to emerge from these stakeholder engagement events. It was mentioned across strategic aims and in additional individual comments.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
24
1. Executive Summary – Exception Report
1.1
The CCG has published a number of presentations, targeted at particular stakeholders, as part of its remit on engaging on the Planning Cycle for 2014 – 2016. As at the end of November and during December 2013, the senior management team of the CCG gave a number of presentations, these included: Royal Borough of Greenwich Lewisham and Greenwich NHS Trust Information published in Commissioning Voice and on the CCG Website CCG Membership (presentation given to each Syndicate Meeting) Feedback has not been received on the commissioning intentions from the syndicates at this stage. A further commissioning intentions discussion will be held at the next Greenwich Executive and syndicates meeting on the 22 January 2014 where feedback will be collated and presented at the next Greenwich Executive meeting. Engagement on the specific themes of our Commissioning Intentions will continue i.e. unscheduled care consultation with a proposed end date of 10 January 2014, with further engagement when responses are collated. Below details the feedback from the event that was held with the voluntary sector. Engagement Event: Commissioning intentions – stakeholder workshop Purpose of Event: Event held to engage with service users and voluntary sector on NHS Greenwich CCG commissioning intentions for 2014/15 through group feedback and individual written comments, on what they felt would demonstrate that the CCG is meeting its strategic principles Date of Event: 20 November 2013 Venue The Forum Time: 11 – 1pm Type of Engagement: Round table world café event
2. Impact Assessment and Risk Management Issues
2.1 The event was extensively advertised through Greenwich Action for Voluntary Service (GAVs) using a poster with the key aims of the event being advertised. Communication methods used were: Voluntary Sector Groups Telephone cold calling Mailouts to stakeholders The event was advertised with 4 weeks prior notice. Interactive day with workshops, discussion on commissioning intentions etc.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
25
Patient Engagement Feedback
Objective To present and engage on the NHS Greenwich CCG Commissioning Intentions
Who did we engage with?
Voluntary and Community Groups
When did we engage?
Wednesday 20th November – 11am to 1pm Round table event – World Cafe
Purpose of engagement
The objectives of the events were: to introduce stakeholders to the CCG, the new commissioning environment and the strategy for 2014-15 and to seek people‟s views – through group feedback and individual written comments, on what they felt would demonstrate that the CCG is meeting its strategic principles.
Who from the CCG attended?
Rebecca Rosen Clinical Commissioner – Long Term Conditions Simon Hall – Director of Integrated Commissioning Alison Goodlad - Associate Director Service redesign Alun Bayliss Head of integrated Commissioning - Adult Mental Health, Learning Disabilities and CAMHS Simon Shenton-Tan – End of Life and Cancers Katy Gorden – Cardiac Irene Grayson – Service Redesign Dilo Lalande – Associate Director of Communications & Engagement Kerry Cleaver Communications & Engagement
Who from the public attended?
Greenwich Carers Centre
HER Centre
Advocacy in Greenwich
Mums-Aid
Pre School Learning Alliance (PSLA)
Feel Good Co-Operative
Family Action
Mothers of Sexually Abused Children (MOSAC)
Somali Parents Network
Drug & Alcohol Service London (DASL) Greenwich Co-Operative Development Agency (GCDA)
Ajoda Community Alliance (ACA) (formerly Greenwich Ajoda Organisation)
Greenwich Mind
Oasis Care and Training Agency (OCTA) (formerly Somali Care Agency (SORAG))
Enclosure Dii

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
26
Age UK Bromley and Greenwich
Children's Society - Participation Project
Family Matters
Home Start Greenwich
South London Counselling Services National Autistic Society (NAS) Greenwich Branch
Somali Parents Network
Quaggy Development Trust Greenwich Toy and Leisure Library Association (GTLLA) Greenwich Toy and Leisure Library Association (GTLLA)
Listening Ears
Relate Bromley
Deborah Ubee Trust
Avante Partnership
Greenwich Association of Disabled people's Centre for Independent Living (GAD)
Ajoda Community Alliance (ACA) (formerly Greenwich Ajoda Organisation)
Tryangle Project 2011
Avante Partnership
Advocacy for Older People in Greenwich
Turnout? 35 representatives from the Greenwich voluntary and community sector.
Where did engagement take place?
The Forum
Issues Identified Engagement in general In addition to feedback on the strategic principles other comments, questions and suggestions were recorded. The themes to emerge are listed below.
Integration of health and social care – the importance of integrated working across health and social care was the strongest theme to emerge from these stakeholder engagement events. It was mentioned across strategic aims and in additional individual comments.
Carers - recognition of the vital role that carers play was a very prominent theme – particularly within individual written comments. The importance of providing appropriate training and support and commissioning appropriately for carers were all mentioned.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
27
GPs and commissioning local services– a number of questions were asked, suggestions made and comments given regarding quality monitoring, locality and out of hours services, voluntary and community groups. These are all responded to within the feedback table. The general consensus at the workshop felt that better access to GP appointments will deter people from turning up at A&E. Clinical Commissioning Programmes (CCPs) – a number of questions were asked and comments made regarding dementia, learning disabilities, maternity, end of life care, stroke, cardiology and assistive technologies and respiratory services. Services should be conveniently located and accessible
•Patients should know how to access services and get information to support self-management
•GPs needn‟t be the only gatekeeper to services
•There should be stronger links with other types of care /more integrated services
•Services should be patient-centred
•Not all enhanced or out of hospital services can be offered in every practice or locality, service models need to take into account efficiency and best use of resources Patients want to have an extended range of services available at GP practices and pharmacies General Engagement – Need to inform residents when the engagement events are taking place and not just when the CCG what to engage on specific areas of work. Therefore, regular engagement is needed on what is happening within the CCG. An external stakeholder newsletter is needed to keep the public up to date as not all have access to the internet to view the organisations website. Providing opportunities for stakeholders to participate in the development of the outcomes through outcome based commissioning.
How could the event have gone better?
Attendees to the workshop were not aware of health promotion initiatives within the borough. For the next large scale event, it is intended to invite colleagues from Public Health with health promotion material.
Learning? The engagement event provided a very good opportunity to provide the rationale for engagement and an opportunity to raise awareness of the commissioning intentions.
The CCG communications team have a proactive media plan which explains how we will try to increase public understanding and perception of the Clinical
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
28
Commissioning Group and all of the projects that it undertakes.
As part of our engagement work, rather than waiting for people to come to our meetings we are going out into the community to talk and listen to local people about their issues, as well as helping them to understand our vision for local healthcare.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
29
Enclosure: Ei Agenda item: 7i
GOVERNING BODY PAPER
Title of paper: Allocations Update
Date of meeting: Wednesday 29th January 2014
Presented by: Chris Costa Chief Finance Officer
Prepared by: Chris Costa
Chief Finance Officer
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes To assure and drive improvements in quality
Ensure access to high quality primary care services
Meet statutory obligations x
Ensure access to high quality secondary care services
Take a long term approach to the health needs of the local population
x
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
Enhance the use of information Please provide brief executive summary:-
The attached paper provides the Governing Body with an update on Greenwich‟s allocations for the next two years. It notes that the allocation announcements have minimal impact on the planning assumptions previously reported to the Governing Body.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes
Impact on Environment (x) N/A
Legal Implications (x) No
Resource implications (x) Yes
Equality impact assessment (x) No
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes
Patient and Public Involvement (x) N/A
Communications and Engagement (x) No
Impact on CCG Constitution (x) N/A
Brief Summary of Recommendations
The Governing Body is asked to : • Note the 2014/15 and 2015/16 allocations • Note the Better Care Fund Allocation that will be transferred to Royal Borough of Greenwich • Note that the updated planning assumptions are broadly unchanged from those previously reported to the Governing Body

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
30
Enclosure: Fi Agenda item: 7
GOVERNING BODY PAPER
Title of paper: Commissioning Intentions and Strategy
Date of meeting: Wednesday 29th January 2014
Presented by: Simon Hall Chris costa
Title: Director of Integrated Commissioning Chief Finance Officer
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes x To assure and drive improvements in quality x
Ensure access to high quality primary care services
x Meet statutory obligations x
Ensure access to high quality secondary care services
x Take a long term approach to the health needs of the local population
x
Building a new Clinical Commissioning Group
x Enhance communications with practices and patients
x
Enhance the use of information x
Please provide brief executive summary:- The presentation provides an update on progress against the four main elements of the annual planning round and a summary of the guidance issued by NHS England on the 20
th December.
By the 14
th February GCCG must submit: an Operational plan, comprised of self-certification questions and
trajectories for outcome measures and secondary care activity; a Financial Plan; and a plan for the Better Care Fund. The latter must be approved by the Health and Wellbeing Board. Final plans are due by the 4
th
April. A concurrent planning process is underway for South East London, led by the Commissioning Strategy Programme Office. A first draft submission was made on the 18
th December. The draft SEL Strategic Plan is
due by the 4th April.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes x No N/A
Impact on Environment (x) Yes x No N/A
Legal Implications (x) Yes x No N/A
Resource implications (x) Yes x No N/A
Equality impact assessment (x) Yes No x N/A
NHS Operating Framework areas of Quality, Reform and finance (x) Yes x No N/A
Patient and Public Involvement (x) Yes x No N/A
Communications and Engagement (x) Yes x No N/A
Impact on CCG Constitution (x) Yes No x N/A
Summary of Recommendations
To note and discuss.
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
31
Enclosure Eii
Allocations Update
Background
The Government has committed to the principle that the NHS will receive a minimum of real terms growth
in 2014/15 and 2015/16. The total available gross funding uplift for NHS England has now been set at
3% for 2014/15 and 2.3% for 2015/16. These funds are intended to meet the real terms growth
commitment, fund service priorities as set out in the NHS mandate and allow for some additional growth
funding for financially 'challenged CCGs.
Pace of Change
NHS England has agreed to adopt a funding formula which establishes the 'target' financial
allocation for each CCG. This target allocation is based on a combination of key drivers of
healthcare costs which are in summary:
Population
Population age
Population health inequalities resulting from deprivation for example' and
Geographical cost factors e.g. It is generally more expensive to buy goods and services in London than
elsewhere in England.
The current CCG funding baselines (their actual funding) are those which have been inherited from predecessor Primary Care Trusts. The difference between the CCG actual funding and their target funding is referred to as the 'distance from target'. Funding which reduces the financial gap between actual and target allocations is referred to as 'Pace of Change' funding movements.
NHS England has sought to address imbalances between actual funding and target allocations through
the development of an appropriate mechanism for moving to target funding within the available financial
envelope. This approach balances the requirement to provide additional funding to financially challenged
CCGs with that of not destabilising local and regional health economies by enacting rapid and large-scale
movement of resources from over-funded to under-funded CCGs.
Allocations 2014/15 and 2015/16
CCG allocations for 2014/15 and 2015/16 were agreed by the NHS England Board on 18th December 2013.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
32
NHSE‟s funding envelope has been increased by 3.1% a real terms increase of 1% above inflation forecast at 2.1% using the GDP Deflator index. Nationally a flat increase of 2.1% has been applied to the 2013/14 CCG programme budgets to derive
2014/15 CCG allocations. This ensures that all CCGs receive real-terms funding growth.
In addition, a fund of £180 million has been made available nationally to redistribute resources to under-target CCGs. London CCGs were allocated about half of this fund. The maximum increase given to any CCG in 2014/15 is 4.92% per cent; the following year it will be 4.49%. Greenwich is marginally over target (0.41%) and will therefore only receive the flat rate increase of 2.1% in 2014/15. It should be noted that Greenwich will move slightly below target by the end of 2014/15 (0.68%). We will again receive the minimum uplift of 1.7% in 2015/16 and will then be 0.91% below target. The main factor driving Greenwich‟s movement closer to target than previously reported is that the formula has now reinstated a weighting for deprivation. Our movement would have been even greater had population estimates used in the national formula recognised known developments in the Borough. The formula instead uses trend analysis which understates Greenwich‟s population. This will be corrected when the model is updated for the 2016/17 allocation round. All other CCGs in South East London have received funds above the minimum uplift recognizing their distance from target and/or population changes. The following table shows London CCG allocations for the next two years:

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
33
Better Care Fund Allocation 2015/16 The allocations announcement also details the final allocation of the Better Care Fund which combines existing funding into a single health and social care pot. Appendix A summarises the Better Care Fund allocations for 2014/15 and 2015/16. Impact on Financial Planning Assumptions The final allocations and associated assumptions have not changed significantly from those previously reported to the Governing Body.
2014/15 2015/16 2014/15 2015/16
% % % %
GDP Deflator 1.90 1.80 2.14 1.70
Allocation Growth 2.00 1.90 2.14 1.70
Efficiency (4.0) (4.0) (4.0) (4.0)
Composite Tariff Uplift 2.50 2.40 2.50 2.40
Net Tariff Change (1.5) (1.6) (1.5) (1.6)
Demographic Growth 1.90 1.20 1.90 1.20
Non-Dem. Growth 2.00 2.00 0.90 0.90
Cost Increase Assumptions:
Acute & Community
Mental Health
Specialist Service
Primary Care 1.50 1.50 1.50 1.50
Prescribing 5.00 5.00 5.00 5.00
LD & Cont Care
Business Rules:
Non-rec. Requirement for CCG 2.00 2.00 1.50 2.00
Comm. Surplus 2.00 2.00 2.00 2.00
Transformation Fund (NR) 1.00 1.00
Funding for ITF (Recurrent) 0.00 (3.0) 0.00 (3.3)
CCG Running Cost Allowance (2.1) (10.0)
Pay Award 2.60 2.50 1.50 1.60
Non-Pay Award 1.90 1.80 2.80 2.70
Contingency 0.50 0.50 0.50 0.50
Greenwich (Original Assumptions) Greenwich Revised
The Governing Body is asked to :
Note the 2014/15 and 2015/16 allocations
Note the Better Care Fund Allocation that will be transferred to Royal Borough of Greenwich
Note that the updated planning assumptions are broadly unchanged from those previously reported
to the Governing Body.

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
34
Appendix A
Greenwich Better Care Fund 2013/14 to 2015/16
`
13/14 14/15 15/16
Funding Transfer to RBG 2013/14 (s256):
Community equipment and adaptations
350,000 350,000 350,000
Telecare
450,000 450,000 450,000
Integrated crisis and rapid response services
300,000 300,000 300,000
Maintaining eligibility criteria
450,000 450,000 450,000
Bed-based intermediate care services
250,000 250,000 250,000
Early supported hospital discharge schemes
350,000 350,000 350,000
Mental health services
150,000 150,000 150,000
Other preventative services
400,000 400,000 400,000
Social care packages
1,761,282 1,761,282 1,761,282
Sub Total
4,461,282 4,461,282 4,461,282
Reablement service
300,000 300,000 300,000
S 256 Agreement 2013/14 4,761,282 4,761,282 4,761,282
Carers - NHS Funded
530,000
Transfer to LAs (£900m nationally)
811,000 811,000 811,000
Further Transfer (£200m nationally)
530,000 530,000
Other / Rounding
-5,282 -5,282 -5,282
NHS Funded Other 6,097,000 6,097,000 6,097,000
Better Care Fund 11,913,000
NHS FUNDED 6,097,000 6,097,000 18,010,000
Local Authority Funded
Disabilities Fund
1,020,000 1,020,000 1,020,000
Social Care Capital Grant
741,000 741,000
LOCAL AUTHORITY FUNDED 1,020,000 1,761,000 1,761,000
BETTER CARE FUND TOTAL 7,117,000 7,858,000 19,771,000

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
35

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
36

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
37

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
38

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
39

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
40

NHS Greenwich CCG: Procurement Forward Planner (April 2013 - April 2015)
Planned procurements
Ap
r-13
May
Jun
e
July
Au
g
Sept
Oct
No
v
Dec
Jan-1
4
Feb
Mar
Ap
ril
May
Jun
Jul
Au
g
Sept
Oct
No
v
Dec
Jan-1
5
Feb
Mar
Ap
r
Musculo-Skeletal Services (inc associated diagnostics)
Continence Services
Long Term Conditions (inc diagnostics; diabetes/cardiology etc.)
Ophthalmology (Community & Hospital) WITH BEXLEY CCG
Referral Management Booking Service WITH BEXLEY CCG ❶
GP Services to Care Homes (AQP)
Anti-Coagulation (AQP)
Phlebotomy (AQP) - Service Expansion
All Children's Community Services (inc CAMHS) WITH RBG
Procurements planned but exact details not yet known
Urgent Care Services ❷
Malnutrition/Food Supplements
Diabetes: replacement for existing LES
Remainder Community Contract (Pioneer) LIKELY WITH RBG❸
KEY TO COLOUR CODING:
Patient Engagement & Impact Assessments
Information correct as at 22 January 2014
Note: All timings and numbers of days are approximate
Procurement Start
For most up-to-date version check www.greenwichccg.nhs.uk

Chair: Dr Hany Wahba Chief Officer: Annabel Burn
42
❶ = Procurement with CSU/Solent Support
Procurement Underway
❷ = Subject to Public Consultation Contract Awarded
❸ = Timetable under review Mobilisation
New Service Goes Live
Chair: Dr Hany Wahba Chief Officer: Annabel Burn
43
Enclosure: Ii Agenda item: 10.1
GOVERNING BODY PAPER
Title of paper: QUALITY REPORT
Date of meeting: Wednesday 29th January 2014
Presented by: Nicola Moore Title: Director of Governance & Quality
Prepared by: Maggie Aiken Title: AD Governance & Quality
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes X To assure and drive improvements in quality X
Ensure access to high quality primary care services
X Meet statutory obligations X
Ensure access to high quality secondary care services
X Take a long term approach to the health needs of the local population
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
X
Enhance the use of information Please provide brief executive summary:-
See below.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes No N/A
Impact on Environment (x) Yes No N/A
Legal Implications (x) Yes No N/A
Resource implications (x) Yes No N/A
Equality impact assessment (x) Yes No N/A
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes No N/A
Patient and Public Involvement (x) Yes No N/A
Communications and Engagement (x) Yes No N/A
Impact on CCG Constitution (x) Yes No N/A
Brief Summary of Recommendations to the Greenwich Executive Group
The Quality Report provides an overview to the NHS Greenwich Clinical Commissioning Governing Body on the work of the NHS Greenwich Clinical Commissioning Group Quality Committee. The Governing Body is asked to receive assurance that the Committee is acting to complete the full scope of its responsibilities and conform to the agreed structure of delegation.
Page 45 of 158
Enclosure Iii

Page 46 of 158

Page 47 of 158

Page 48 of 158

Page 49 of 158

Page 50 of 158

Page 51 of 158

Page 52 of 158

Page 53 of 158
Page 54 of 158
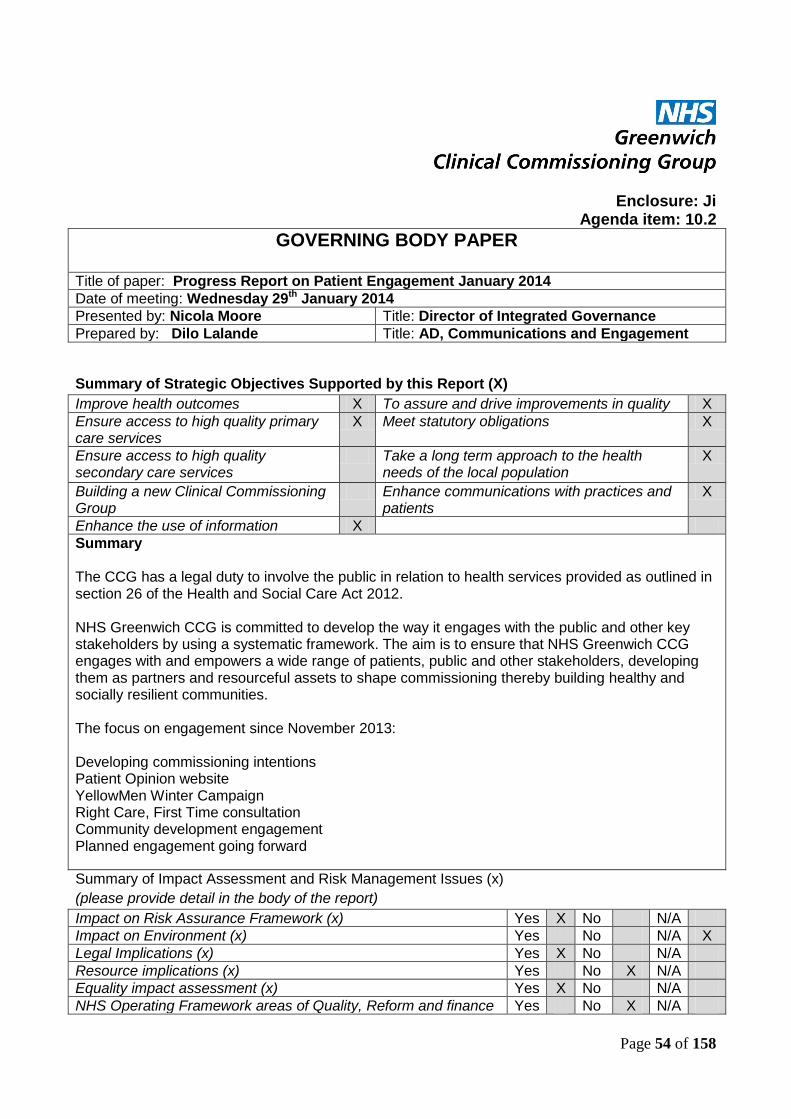
Enclosure: Ji Agenda item: 10.2
GOVERNING BODY PAPER
Title of paper: Progress Report on Patient Engagement January 2014
Date of meeting: Wednesday 29th January 2014
Presented by: Nicola Moore Title: Director of Integrated Governance
Prepared by: Dilo Lalande Title: AD, Communications and Engagement
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes X To assure and drive improvements in quality X
Ensure access to high quality primary care services
X Meet statutory obligations X
Ensure access to high quality secondary care services
Take a long term approach to the health needs of the local population
X
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
X
Enhance the use of information X
Summary The CCG has a legal duty to involve the public in relation to health services provided as outlined in section 26 of the Health and Social Care Act 2012. NHS Greenwich CCG is committed to develop the way it engages with the public and other key stakeholders by using a systematic framework. The aim is to ensure that NHS Greenwich CCG engages with and empowers a wide range of patients, public and other stakeholders, developing them as partners and resourceful assets to shape commissioning thereby building healthy and socially resilient communities. The focus on engagement since November 2013: Developing commissioning intentions Patient Opinion website YellowMen Winter Campaign Right Care, First Time consultation Community development engagement Planned engagement going forward
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes X No N/A
Impact on Environment (x) Yes No N/A X
Legal Implications (x) Yes X No N/A
Resource implications (x) Yes No X N/A
Equality impact assessment (x) Yes X No N/A
NHS Operating Framework areas of Quality, Reform and finance Yes No X N/A

Page 55 of 158
(x)
Patient and Public Involvement (x) Yes X No N/A
Communications and Engagement (x) Yes X No N/A
Impact on CCG Constitution (x) Yes X No N/A
Executive Summary This paper provides an update on the progress being made on Patient and Public Engagement for NHS Greenwich CCG. Our engagement activities are steadily moving forward. We are involved in a number of key engagement projects as our commissioning managers continue to review and develop services. We are also working with other key partner organisations to share good practice and agree joint approaches where appropriate. These engagement activities will culminate in informing options for major service redesign over the coming months. From this potential for change to services there is the opportunity to secure improvements in the quality and safety of those services for Greenwich. The developments are entirely consistent with the CCG‟s strategic direction and the emerging themes reinforce priorities of safety, quality and improving local access. The processes followed and the findings or emerging themes from these specific engagement activities will inform future CCG engagement.
Patient Engagement
Patient Engagement Programme Board
A Patient Engagement Programme Board (PEPB) has been established in accordance with NHS Greenwich CCG‟s Constitution and the CCG‟s Communication and Engagement Strategy under Objective 2. The Patient Engagement Programme Board (PEPB), chaired by NHS Greenwich CCG Lay Member Greg Ussher. The remit of the Patient Engagement Programme Board is to oversee and monitor engagement, and to develop, implement, and review progress on our patient and public involvement strategy. The group also provides guidance to our commissioners, helping to ensure that involvement is embedded into every step of the commissioning cycle. Patient and Public Engagement strategy 2013-15 This strategy has been reviewed in conjunction with the PEPB and will outline how the CCG will undertake both communications and patient and community engagement activities as part of its role as commissioners in Greenwich. The PEPB, at its last meeting on 9th December ‟13 worked together to define the core aims and objectives of the strategy. The draft strategy was discussed with patients and stakeholders and the feed back received and will be imbedded within the document. The strategy will be offered to the Governing Body for final approval. Developing commissioning priorities 2014/15 The development of commissioning intentions is an on-going process to ensure delivery of high quality care to meet the local population needs, within the financial constraints. Whilst the process is on-going, the CCG must review, refresh and develop commissioning intentions each year. To contribute to the development of 2014/15 priorities, the CCG has involved a wide range of stakeholders including clinicians and patients at two separate events. Right Care, First Time engagement

Page 56 of 158
Over 2,000 public consultation documents and response forms have been distributed so far in English. 500 have been sent to all general practices and walk-in centres. Documents are also available on a display stand at the Queen Elizabeth Hospital. Easy-read versions of the public consultation document are also available in print and online, alongside translated versions of the public consultation documents.
So far over 160 people have responded to the public consultation formally. Five events in
Greenwich, Woolwich, Eltham and Charlton have seen many people come along and feedback
directly to the consultation team, CCG staff and local GPs. Focus groups have been held with key
community groups in the borough such as the Nepalese community, Advocacy in Greenwich,
The Her Centre.
We are also holding a further drop-in event in Woolwich on Saturday 18 January. The drop in event
will take place between 11 am and 2pm in General Gordon Square. On 20 January we will be at
Morrisons Supermarket in Thamesmead from 3pm to 6pm. There will also be a live twitter Q&A
from 4pm to 6pm on 20 January.
There have been adverts in the Greenwich Time and The News Shopper advertising the
extension of the consultation and future events.
Hearing from patients - „Talking with our community‟ In December 2013, the CCG held community engagement events entitled “Talking with our Community” in order to understand patients‟ views and experiences of local services. More than 45 patients shared their thoughts. The events talked about many different topics including; long term conditions, planned care, prescribing, urgent care, end of life care, older peoples and carers services, mental health and learning disabilities. During both sessions, attendees participated in interactive discussions where people shared their thoughts and experiences about local services. Patients told us they liked the “market stall approach. It allowed people the opportunity to pick areas of interest and means that they can give as little or as much of their time as they choose”. In order to keep patients informed and involved in future it was felt their needed to be “Regular events or communication over a period of time”. Following this event, patients‟ feedback was made available in the format of an easy read report, which was shared via social media, on the website and through the Greenwich Action Voluntary Service (GAVs). Feedback – see commissioning intentions paper. YellowMen Winter campaign - Don‟t just go to A&E The campaign in Greenwich to tackle unnecessary A&E admissions highlighted alternative places people can obtain expert advice and treatment, including: NHS11, pharmacies, GP, the two walk-in centres and the Urgent Care Centre. The campaign was launched just before Christmas with buses and bus shelters in Greenwich showing seven foot statues with various aliments from minor to serious highlighting the message, „Don‟t just go to A&E, you can get quicker treatment closer to home‟. This was followed up on 9 January in General Gordon Square, Woolwich. There were seven foot statues around the square, with staff giving out leaflets and explaining what the campaign was about. There was a lot of interest shown by the public with over 4,000 leaflets being handed out.

Page 57 of 158
There appeared to be an awareness from a large section of the community who had seen the campaign, which also captured the imagination of local children. This gave staff the opportunity to talk to their parents about the healthcare services in Greenwich. In general, the feedback received from the public was the difficulty in obtaining GP appointments. This has been fed back to the Greenwich commissioning team. Patient Opinion The CCG have set up an account to the online forum 'Patient Opinion', which 'carries the voices of patients and carers into the heart of the NHS to help improve care for everyone'. The site encourages people to log their experiences of health care, both good and bad, and allows the organisation concerned to post a response (or multiple responses in a dialogue). Patient Opinion will support the CCG with information on how to promote the site to the public and our providers. Our subscription will be set up so that we receive stories from people living in our CCG area. In addition, where we are also lead commissioner for a particular service, Patient Opinion will arrange for us to receive all stories relating to that particular service. The information provided by Patient Opinion will be monitored by the Communications team to form part of the overall service feedback flow.
Patient Participation Groups NHS Greenwich CCG has undertaken some initial scoping work on Practice Patient Groups across Greenwich and have linked practices into an initiative commissioned with Citizen UK, an organisation with strong local community links, to obtain feedback from our local population on health issues.
We are building on this by developing a locality approach to PPE and reviewing and continually improving our stakeholder and population maps, and developing a cohesive patient engagement model.
Plans are already in progress. Our main focus will be the use of peoples„ and patients‟ experience to inform commissioning at a local level, led by each locality clinical lead. Planned Engagement
We will engage with patients and the public, including local voluntary organisations in order to help us inform our priorities for Commissioning Intentions, QIPP and re-designing local health services. This will include engagement events throughout January to March 2014 with local stakeholders to discuss commissioning intentions.
The team are working to support key projects to engage patients and the public in redesign proposals. The CCG and local NHS providers continue to improve its engagement with patients and the public. It is recognised that there is work to do to ensure we are always engaging with the right people at the right time in the decision making process. The review recommendations include the need to ensure that patient and public engagement is a key element of all CCG contracts with our provider organisations along with arrangements to ensure effective coordination of public engagement across the local NHS. This work is included in the Implementation Plan and the patient engagement calendar. Engagement Calendar A number of engagement events have taken place throughout the year which can be found in appendix A. Future work programme The engagement workplan for the remainder of the financial year is set out below: Engagement on commissioning intentions and the ‟12 themes‟
Page 58 of 158
Develop the engagement for the Right Care, First Time consultation including a Twitter Q&A Jan 14
Development and Implementation of the NHS Greenwich CCG PPE Strategy Jan 14
Develop the Patient & Public Engagement Stakeholder and Events Calendar Jan 14
Strengthen Community and Local Links with all Partners Ongoing
Staff development in Patient & Public Engagement (March 14)
Further dates to be added when confirmed.
Page 59 of 158
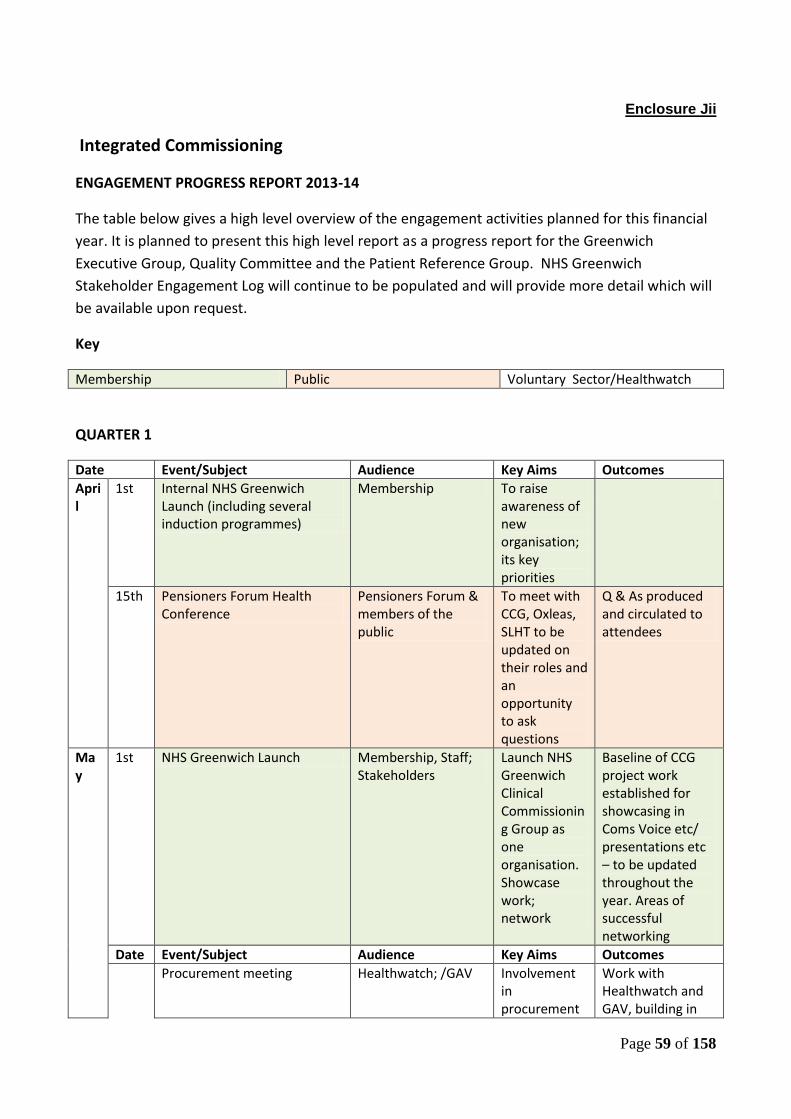
Enclosure Jii
Integrated Commissioning
ENGAGEMENT PROGRESS REPORT 2013-14
The table below gives a high level overview of the engagement activities planned for this financial
year. It is planned to present this high level report as a progress report for the Greenwich
Executive Group, Quality Committee and the Patient Reference Group. NHS Greenwich
Stakeholder Engagement Log will continue to be populated and will provide more detail which will
be available upon request.
Key
Membership Public Voluntary Sector/Healthwatch
QUARTER 1
Date Event/Subject Audience Key Aims Outcomes
April
1st Internal NHS Greenwich Launch (including several induction programmes)
Membership To raise awareness of new organisation; its key priorities
15th Pensioners Forum Health Conference
Pensioners Forum & members of the public
To meet with CCG, Oxleas, SLHT to be updated on their roles and an opportunity to ask questions
Q & As produced and circulated to attendees
May
1st NHS Greenwich Launch Membership, Staff; Stakeholders
Launch NHS Greenwich Clinical Commissioning Group as one organisation. Showcase work; network
Baseline of CCG project work established for showcasing in Coms Voice etc/ presentations etc – to be updated throughout the year. Areas of successful networking
Date Event/Subject Audience Key Aims Outcomes
Procurement meeting Healthwatch; /GAV Involvement in procurement
Work with Healthwatch and GAV, building in
Enclosure Jii

Page 60 of 158
communications handling and scrutiny
PPI into the procurement process.
21 Learning disability event People with LD & carers
To look at health & housing
Issues raised GP access Lack of signage at hospital
22 Series of Induction /Education Meetings
Syndicate and Clinical Leads
To ensure that Syndicate and Clinical leads have a full understanding of NHS Greenwich priorities, structures and tools and techniques available to support them in their work
This will an on-going rolling programme
June
3-16 Safeguarding Week Voluntary Sector; public; Healthcare Professionals
The emphasis of the fortnight is the ‘Toxic Trio’ Domestic Violence, Substance Misuse and Parental Mental Illness.
NHS Greenwich Safeguarding team …….
Public
Membership/Healthcare Professionals
5 Public Board Mtg Public Observe and Q&A session
Q&As to be recorded and responded and published
6 GWF – Care Planning Membership Educational Event on Care Planning – a different approach to primary care management
10 Pilot practices coming forward to take up training in September and October 2013.
19 RMBS Membership Report back on performance; discuss and agree future options regarding procurement of a referral
Engagement taking place with syndicate meetings for feedback and to inform the ballot on procurement

Page 61 of 158
service in Greenwich
Date Event/Subject Audience Key Aims Outcomes
28
Childrens Services
Health Watch
Briefing with Healthwatch to gain views on how focus areas for the 10 July workshop
Areas to look at: Access – working parents access services out of hours – what is needed? Empowering parents to make the right decisions. Spreading Good Practice for healthy lifestyles using schools, public health Ims & Vac: what stops parents wanting vacs; how do we inform parents about choice
29 Great Get Together, Woolwich
Public 1.Raise awareness of NHS Greenwich; Members of Gov Body available to answer questions; 2.showcasing some of our good work 3. introduce web site; PPI and how to get involved, survey, How to complain
Over 150 Parent Survey Questionnaires completed to inform the Children Services workshop being held on 10 July 2013. Public raised many concerns around access to primary care. Survey results 81% Parents had not had any difficulty accessing health services in Greenwich 85% thought a Greenwich smart phone app to alert re: immunisations was a good idea 72% didn’t know there were services to help

Page 62 of 158
their child maintain a healthy weight Positive experiences of services GP SALT Health Visitors Children’s centres Children’s A&E
QUARTER 2
Date
Event/Subject Audience Key Aims Outcomes
JULY
Equalities Public To engage on if the CCG is meeting its public sector equality duty
Website Public To gain feedback on new website
Virtual Group being used to gain views from the public
10 Children Services Public Work Shop 3 Themes: Gaps in services – why is there high attendances at A&E for children; Ways to educate and communicate on Ims and Vacs How to promote healthy lifestyles for children. Parent Survey – information from the
No Attendees. This led to good discussion on how we need to get out to where people are, piggy back on other events, use leisure centres, children’s centres, supermarkets, school fetes etc.

Page 63 of 158
Great Get Together being used to inform work shops
? Citizen UK Project PPGs Details to be worked up – possibly involve GAV re linking in voluntary groups who could support the work being undertaken with PPGs’ Report on progress went to August Quality Ctttee.
On-going
30 MSK Review Patient experience to inform Service Spec for procurement
Patient Survey designed to be given out in clinics w/c 16 Sept, also survey Monkey, Twitter, comms to publicise in local media, website
On-going
Aug
16 Learning Disability Event The Forum
Health Quality Checkers commissioned by the CCG to check services for people with LDs
Service user involvement and assessment of local services in both primary and secondary care
Good feedback on people feeling safe in residential homes Training needed on how to complain
Inpatient Mental Health Rehabilitation
Public
QUARTER 3
Date
Event/Subject Audience Key Aims Outcomes

Page 64 of 158
Sept
4 GAV/CCG Presentations GAV+ voluntary Sector Services
Market event to raise awareness of the CCG and voluntary sector organisations –
Great networking event, 20 plus voluntary/community groups attended – keen to find ways of working together
18 Greenwich Wide Forum Membership Primary Care Strategy workshop – Membership input into development
19 Unscheduled Care for Children
Membership, staff, RBG, Oxleas
Continence Procurement Public
Currently the service has no contract to support it and it needs to be consolidated into a proper contract. In the last six months we have reviewed the service, so we are now able to set up long-term contract arrangements.
Briefing written and passed to comms for dissemination Letter to go to all service users and follow up once service has been running for six months
Date Event/Subject Audience Key Aims Outcomes
25 Governing Body Public Meeting
Public Q&A Session
25 RMBS workshop Staff/GPs
Health watch Launch Public Launch of Health Watch networking opportunity
Inpatient Mental Health Rehab Procurement
Public
Ophthalmology Public
Oct Family Nurse Partnership Public Raise awareness, good news story
Diagnostics Public
8 Big Health Check Day People with Learning Service users

Page 65 of 158
disabilities experience of Health & Social Care using workshops, theatre group
A&E,UCC, WIC, 111, Public Picker Institute leading on public face to face engagement to ascertain why patients are using urgent care facilities
Gypsy & Traveller Outreach (LINK)
Internal, Health Watch, Citizens UK
LINK produced a report on their experiences of accessing primary & secondary care
Group set up to see how we can engage/facilitate further to improve experiences Citizen UK may take up together with Healthwatch
25 Meeting with GAVS To plan event 28 Nov To share commissioning intentions
16 Commissioning intentions GAVS To have regular meetings building PPI into commissioning
Build stronger more joined up relationship around PPI
Anticoagulation/Phlebotomy/LES Diabetes/Cardiology/opthomology
Public Patient experience to inform Service Spec for procurement
Nov Community Services Public
4th 1.15-145
Tea with a Talk (Time on their agenda)
Public Meeting with CANE Community Ass of New Eltham to share

Page 66 of 158
commissioning intentions
Maternity Services Public Across six boroughs, Martin Wilkinson (Lewisham CCG) is leading with Simon Hall
Long Term Conditions Public Set up working groups
Meet with Healthwatch Set regular meetings and share work intentions
Care Homes Public Inform
11 Unscheduled Care Consultation begins
Public
13 Meeting with Healtwatch
18 South Greenwich Forum AGM St Mary’s Community Centre Eltham High St
Public Attend AGM to discuss Unscheduled Care Consultation & Eltham Community Hospital
21 Event with targeted Community/Voluntary groups
to share commissioning intentions and have discussion
21 Greenwich Wide Forum Membership
26 Unscheduled care public meeting, The Ten Centre Greenwich
Public
28 MSK event Public World Café Workshop to improve pathways
29 Unscheduled Care Public meeting Woolwich Town Hall
Public
Dec 6 Unscheduled Care Public Meeting Woolwich Town Hall
Public
17 Overview & Scrutiny Committee Unscheduled Care
RBG Simon & Hany
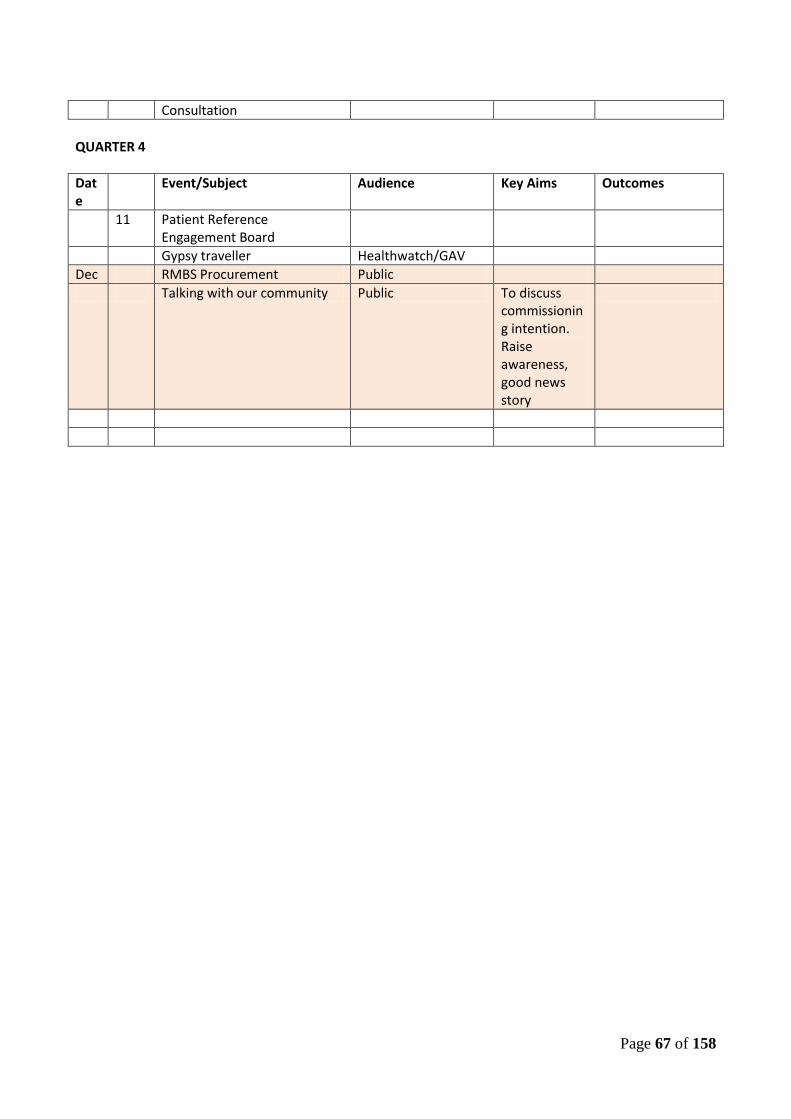
Page 67 of 158
Consultation
QUARTER 4
Date
Event/Subject Audience Key Aims Outcomes
11 Patient Reference Engagement Board
Gypsy traveller Healthwatch/GAV
Dec RMBS Procurement Public
Talking with our community Public To discuss commissioning intention. Raise awareness, good news story
Enclosure Jii Enclosure Jii
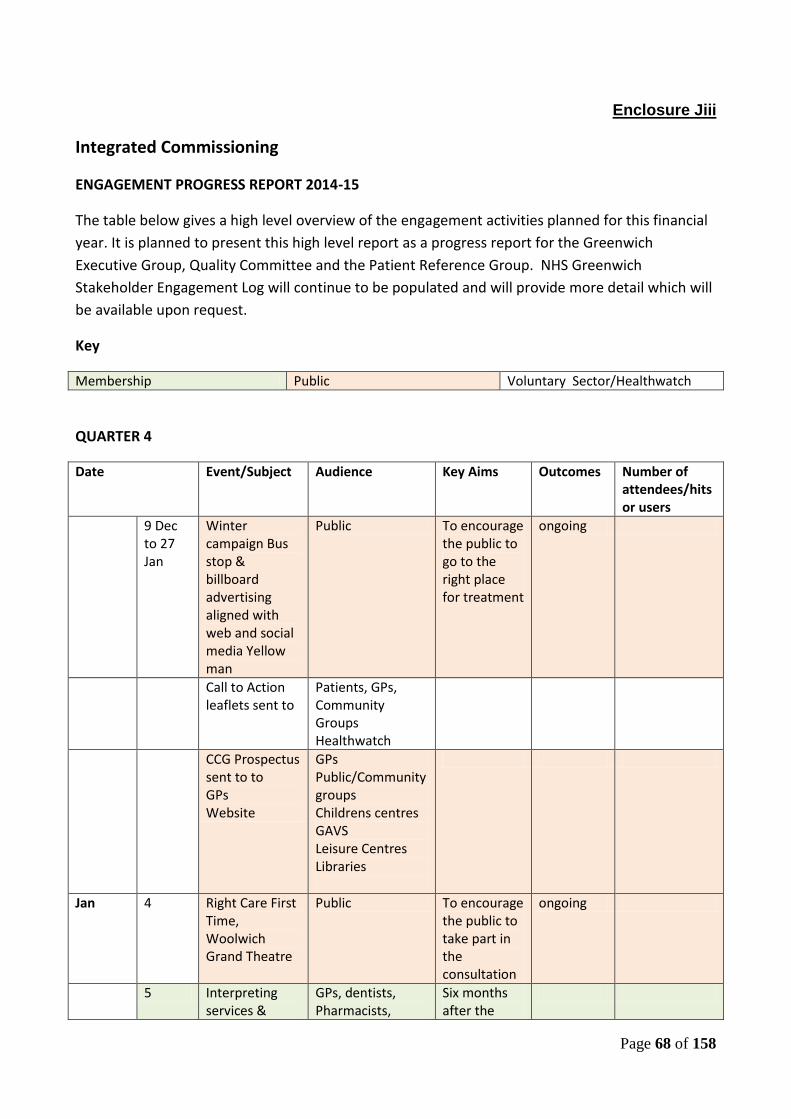
Page 68 of 158
Enclosure Jiii
Integrated Commissioning
ENGAGEMENT PROGRESS REPORT 2014-15
The table below gives a high level overview of the engagement activities planned for this financial
year. It is planned to present this high level report as a progress report for the Greenwich
Executive Group, Quality Committee and the Patient Reference Group. NHS Greenwich
Stakeholder Engagement Log will continue to be populated and will provide more detail which will
be available upon request.
Key
Membership Public Voluntary Sector/Healthwatch
QUARTER 4
Date Event/Subject Audience Key Aims Outcomes Number of attendees/hits or users
9 Dec to 27 Jan
Winter campaign Bus stop & billboard advertising aligned with web and social media Yellow man
Public To encourage the public to go to the right place for treatment
ongoing
Call to Action leaflets sent to
Patients, GPs, Community Groups Healthwatch
CCG Prospectus sent to to GPs Website
GPs Public/Community groups Childrens centres GAVS Leisure Centres Libraries
Jan 4 Right Care First Time, Woolwich Grand Theatre
Public To encourage the public to take part in the consultation
ongoing
5 Interpreting services &
GPs, dentists, Pharmacists,
Six months after the
Enclosure Jiii

Page 69 of 158
Language line questionnaire on Survey Monkey
opticians launch of the service to see if it is being used/any issues
7 Diabetes User Group QE Hospital
User Group Self-help group Guest speakers Newsletter
7 Telecon all engagements leads
SEL engagement leads
Emerging case for change
7 Next steps forward
Meeting with GAVS
Next steps for engagement in Greenwich
9 Meeting with Lewisham and Greenwich Healthcare Trust
Engagement Leads Next steps for engagement in Greenwich and Lewisham
9 Key Yellowmen engagement General Gordon Square
Public/Press Awareness campaign
Jan/Feb Yellowmen engagement campaign
Pensioners Forum Carers Age UK LTC support Groups Greenwich University Faith Groups BME groups
To encourage the public to go to the right place for treatment
15 BME Mental Health
CCG, Healthwatch, RBG
18 Right Care, First Time General Gordon Square, Woolwich
Public To encourage the public to take part in the consultation
20 Right Care, First Time Morrison’s Thamesmead
Public To encourage the public to take part in the consultation
20 Right Care, First Time, Live Twitter Q&A
Public To encourage the public to take part in

Page 70 of 158
4pm-6pm the consultation
February Date 19
Event/Subject Statutory Sector Liaison Group (SSLG)
Audience Healthwatch, RBG, Oxleas,
Key Aims Outcomes Number of Attendees/hits or users
March Date Event/Subject Audience Key Aims Outcomes Number of attendees/hits or users

Page 71 of 158
Enclosure: Li Agenda item: 11
GOVERNING BODY PAPER
Title of paper: Finance, Performance & QIPP Report Month 9
Date of meeting: Wednesday 29th January 2014
Presented by: Chris Costa Chief Finance Officer,
Prepared by: Geoff Berg, Marion Joynson, Andrew Thomas
Senior Strategy Manager, AD Finance and AD Strategy Performance & QIPP
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes X To assure and drive improvements in quality X
Ensure access to high quality primary care services
X Meet statutory obligations X
Ensure access to high quality secondary care services
X Take a long term approach to the health needs of the local population
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
Enhance the use of information X Please provide brief executive summary:-
The Month 9 Finance Performance & QIPP Report summarises key performance indicators across finance, QIPP, NHS Constitution Standards and the NHS Outcomes Framework.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes x No N/A
Impact on Environment (x) Yes No x N/A
Legal Implications (x) Yes No x N/A
Resource implications (x) Yes x No N/A
Equality impact assessment (x) Yes No N/A x
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes x No N/A
Patient and Public Involvement (x) Yes No x N/A
Communications and Engagement (x) Yes No x N/A
Impact on CCG Constitution (x) Yes No x N/A
Brief Summary of Recommendations
For consideration.

Page 72 of 158

Page 73 of 158
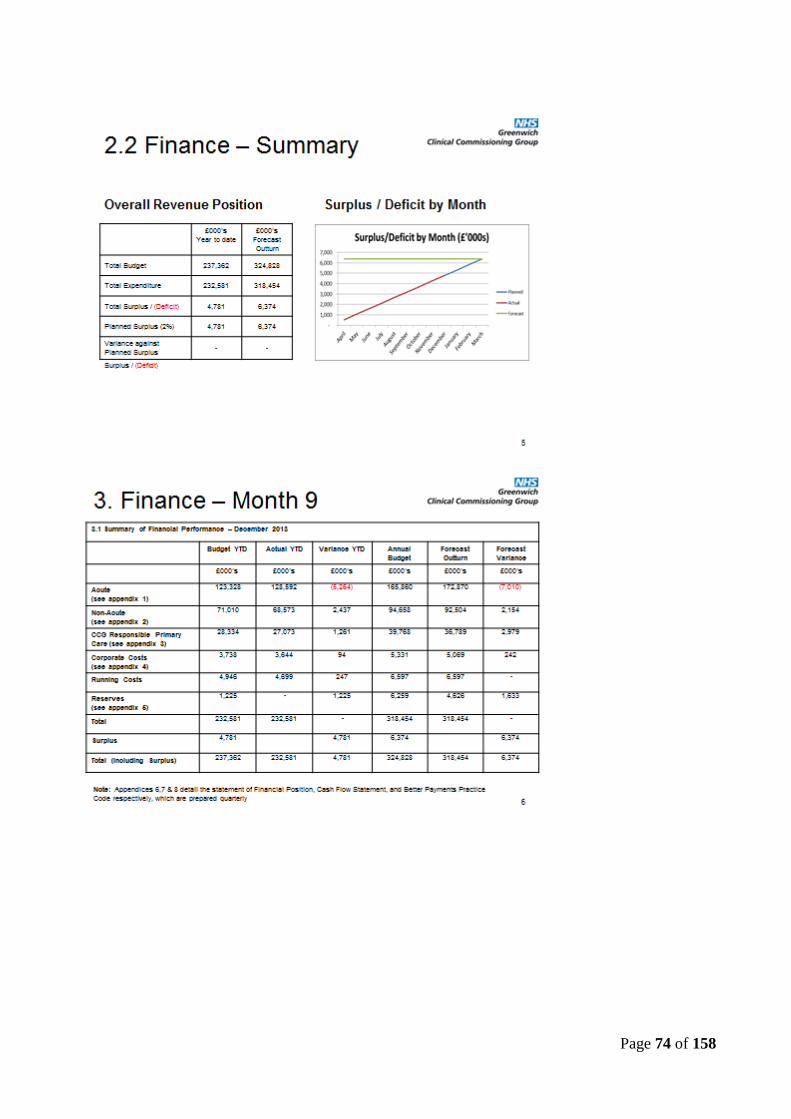
Page 74 of 158

Page 75 of 158

Page 76 of 158

Page 77 of 158

Page 78 of 158

Page 79 of 158
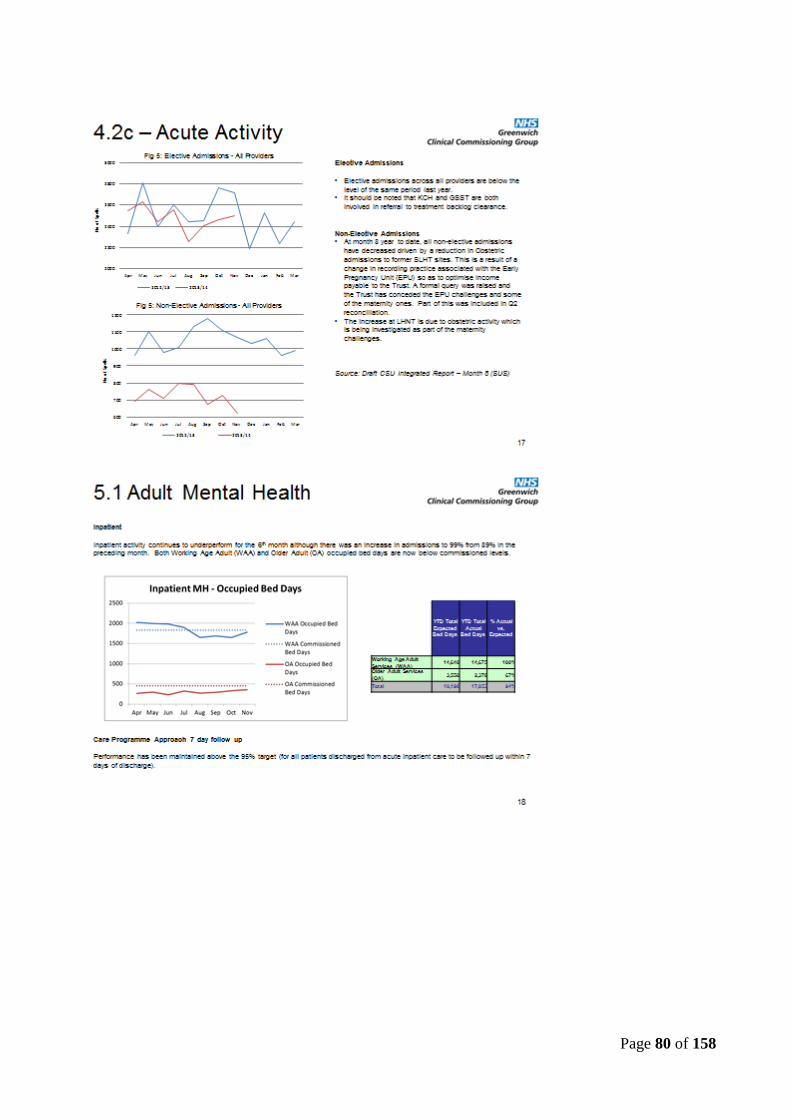
Page 80 of 158

Page 81 of 158

Page 82 of 158
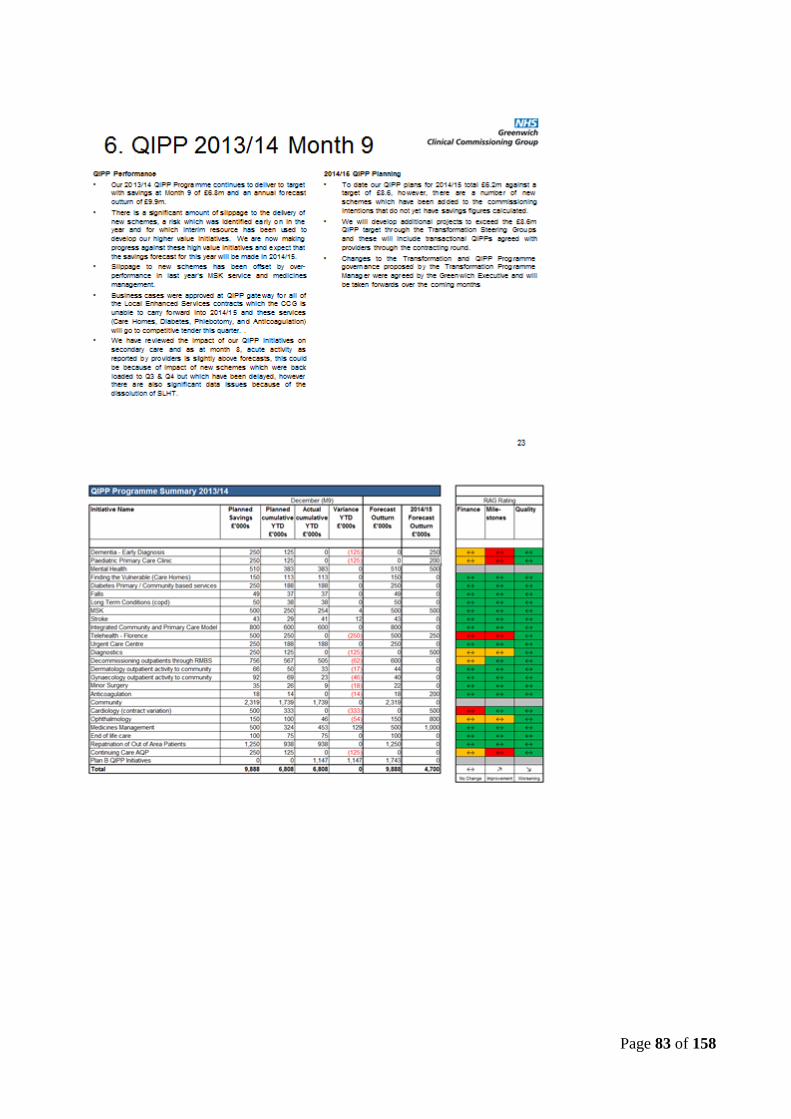
Page 83 of 158

Page 84 of 158

Page 85 of 158
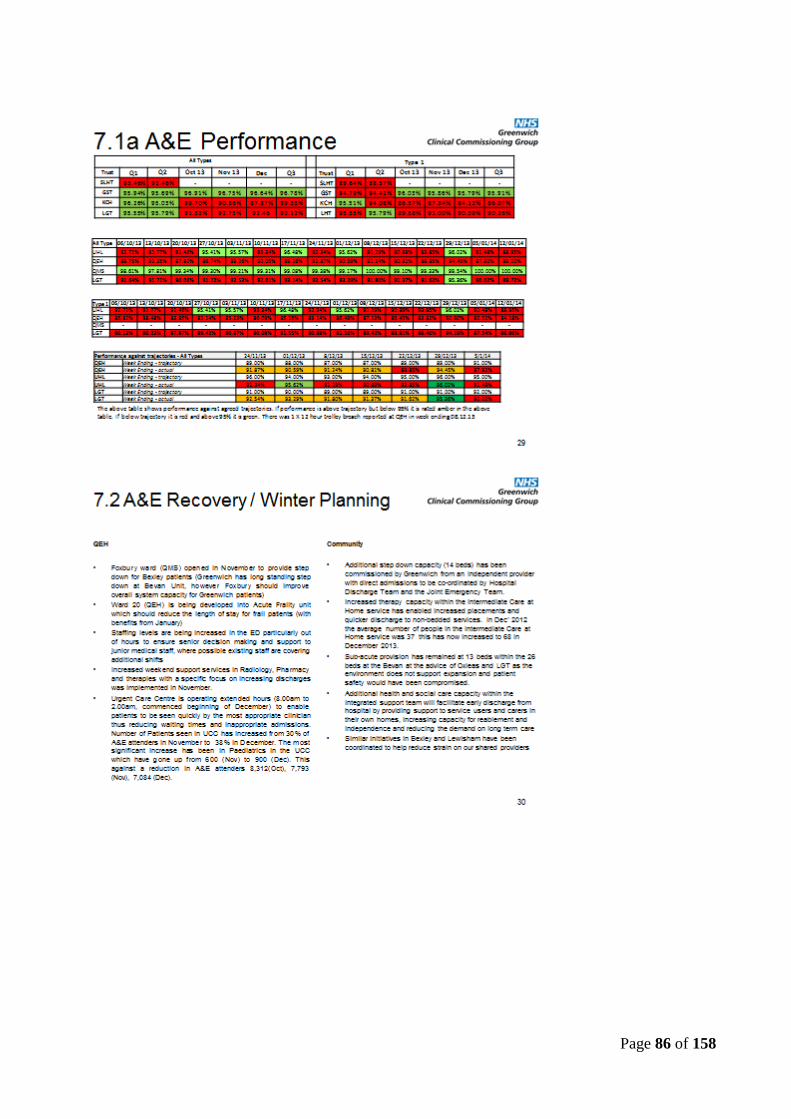
Page 86 of 158

Page 87 of 158

Page 88 of 158

Page 89 of 158

Page 90 of 158

Page 91 of 158

Page 92 of 158

Page 93 of 158

Page 94 of 158
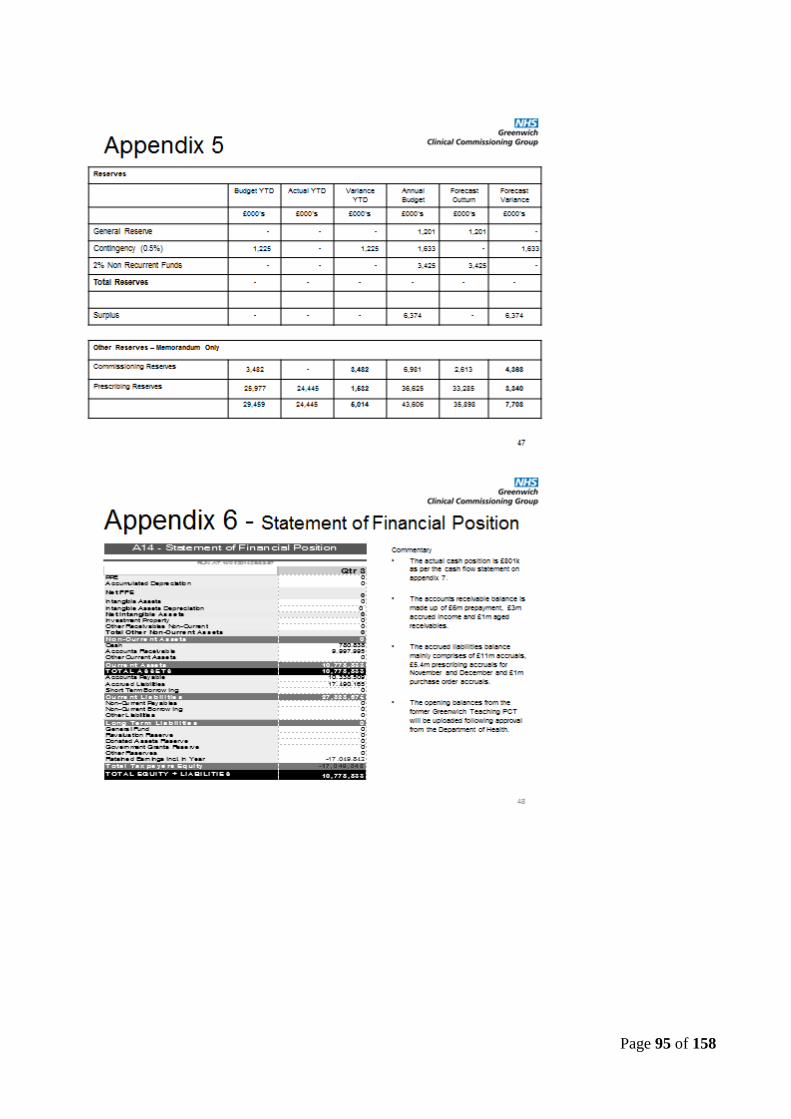
Page 95 of 158

Page 96 of 158
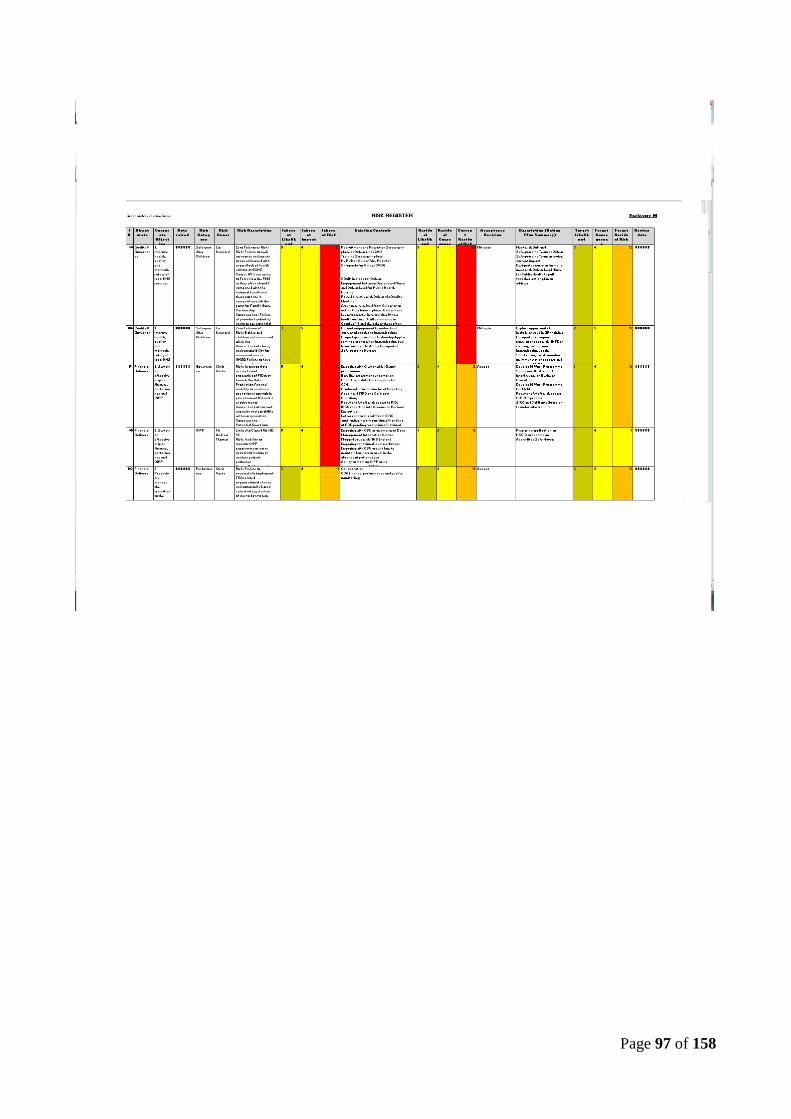
Page 97 of 158

Page 98 of 158
Enclosure: Ni
Agenda item: 12
GOVERNING BODY PAPER
Title of paper: RISK MANAGEMENT REPORT
Date of meeting: Wednesday 29th January 2013
Presented by: Nicola Moore Title: Director of Integrated Governance
Prepared by: Nicola Moore Title: Director of Integrated Governance
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes x To assure and drive improvements in quality x
Ensure access to high quality primary care services
x Meet statutory obligations
Ensure access to high quality secondary care services
x Take a long term approach to the health needs of the local population
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
Enhance the use of information x Please provide brief executive summary:-
This bi-monthly risk management report to the Governing Body provides an overview of new entries on to the risk register (Datix) and assurance on overall risk management performance.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes x No N/A
Impact on Environment (x) Yes No N/A x
Legal Implications (x) Yes x No N/A
Resource implications (x) Yes x No N/A
Equality impact assessment (x) Yes No N/A
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes x No N/A
Patient and Public Involvement (x) Yes No N/A x
Communications and Engagement (x) Yes No N/A x
Impact on CCG Constitution (x) Yes No N/A x
Brief Summary of Recommendations
To consider the report.

Page 99 of 158
Enclosure Nii
Risk Management Performance Report
January „14
This bi-monthly risk management report to the Greenwich Clinical Commissioning Committee (GCCC) provides an overview of new entries on to the risk register (Datix) and assurance on overall risk management performance. Risk Register As of 17th January „14, the risk register holds a total of 32 open risks.
21/8/12 21
13/9/12 21
23/10/12 25
23/11/12 27
13/1/13 27
27/3/13 26
3/6/13 29
12/9/13 31
8/11/13 30
17/1/14 30
Risk Distribution Risk Distribution 17th January ‟14 Risk distribution as at 8th November ‟13
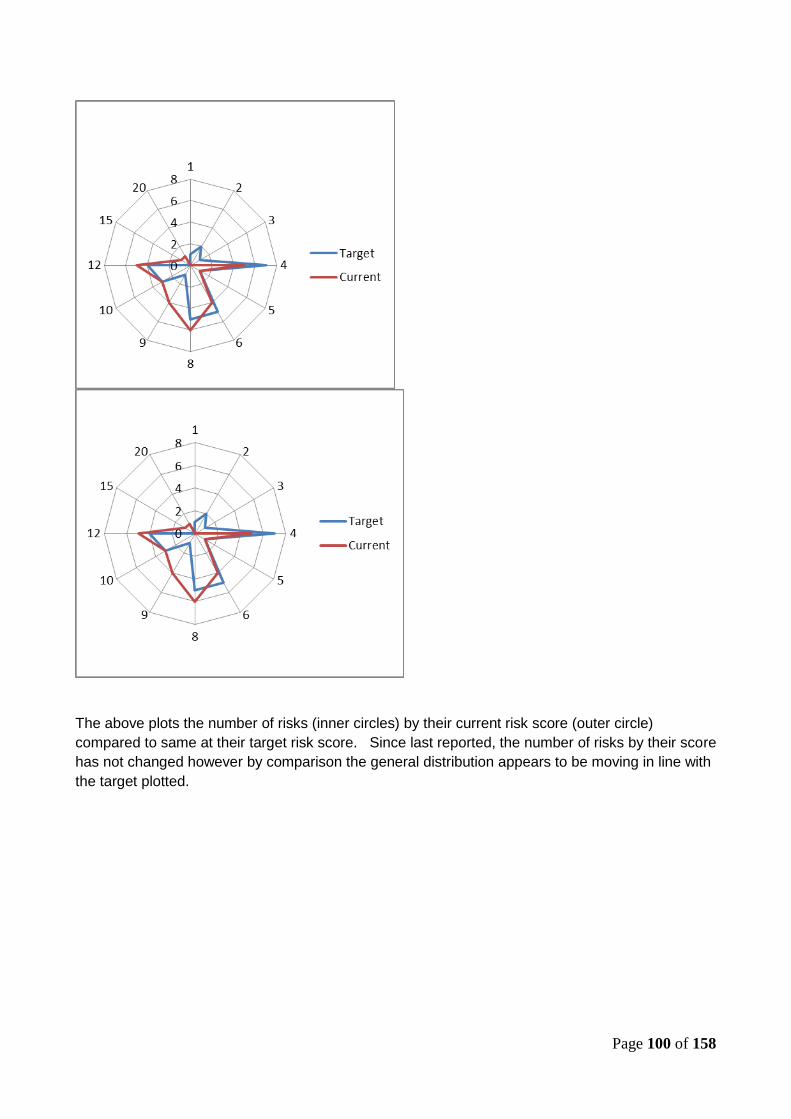
Page 100 of 158
The above plots the number of risks (inner circles) by their current risk score (outer circle)
compared to same at their target risk score. Since last reported, the number of risks by their score
has not changed however by comparison the general distribution appears to be moving in line with
the target plotted.

Page 101 of 158
Risks by Sub-Type
New Entries There have been no new risk entries since last reported to the Governing Body in November „13.
High Risks = >12 ID Description Controls in place Rating Target
Rating Action Action Due Date
80 Zero Tolerance Risk! Risk: Failure to seek assurance and ensure issues addressed with regard lack of health visitors at Oxleas Cause: Londonwide shortage of HV‟s and competition with Family Nurse Partnership roles Consequence: Failure of provider to identify and manage potential safeguarding issues; Non-compliance with national standards with significant risk to patients if unresolved (4)
Recruitment and Retention Strategy in place at Oxleas since 2012; Training Strategy in place; HV Risk on Oxleas Risk Register; CQuIN in place for Oxleas; Engagement between Designated Nurse and Oxleas Lead for Public Health Nursing Raised directly with Oxleas via Quality Meeting; Assurance received from Oxleas as to action they have in place. Oxleas have been successful in recruiting 10 new health visitors. 3 will commence in October „13 and the others thereafter.
20
↔
12 Meet with DoN and Safeguarding Team at Oxleas Oxleas asked to review current impact of capacity on ability to meet statutory safeguarding duties Designated nurse to formally meet with Oxleas Lead Nurse for Public Health to pull together action plan to address
31/03/2013 31/1/14 30/10/2012
Finance 11
Governance 3
Health and Safety 1
Operations 1
Performance 2
QIPP 2
Quality (affecting providers' services)
2
Safeguarding Children 8
Total 30

Page 102 of 158
ID Description Controls in place Rating Target Rating
Action Action Due Date
106 Zero Tolerance! Risk: Babies and children not immunised when due Cause: Lack of clarity and responsibility for immunisations at NHSE; Failure to have in place robust systems in primary care to follow up non-attenders for immunisations Consequence: Babies and children at risk of developing avoidable infections which may lead to hospital admission, disability or death; missed opportunity to identify any other possible safeguarding issues or health needs
Patient engagement to understand current obstacles to immunisation; Project group in place to develop App to remind parents when immunisation due; Issue raised with GP's by Designated Safeguarding Nurses;
15
↔
15 Explore opportunity to include as issue in GP training Designated safeguarding nurse to engage with NHSE on strategy to improve immunisation uptake Survey of GP practices to seek assurance of processes in place to follow up immunisations overdue (results pending)
05/09/2013 11/08/2013 31/11/13
58 Risk: Inappropriate access to and processing of PID may breach the Data Protection Act and inability to evidence operational controls in place to meet IG toolkit requirements Cause: Lack of current capacity and capability within organisation Consequence: Potential fines from the Information Commissioner, reputation damage and civil action by any patients affected. Leading to costs, risk and failure to fulfil business functions; failure to meeting required IG Toolkit levels
Engaging with Cluster wide IG work programmeBaseline assessment undertaken; Undertaken data flow mapping for CCG; Produced Information Asset Register; Appointed SIRO and Caldicott Guardian; Register of staff with access to PID; IGSG reporting into Greenwich Business Executive; Letter sent to all staff from SIRO confirming interim position of handling of PCD pending resolution of national issues IG Work Programme for 13/14 in place; Current audited compliance at level 2 66%
12
↔
12 Develop IG Work Programme Set up new IGSG reporting into Greenwich Business Executive Develop IG Work Programme for 13/14 Register of staff with access to PID in process SIRO and Caldicott Guardian to undertake training
31/03/2013 30/11/2012 01/06/2013 31/12/2012 31/12/2012
95 Linked to Closed Risk ID 92 Risk: Inability to monitor QIPP programme or carry risk stratification or analyse patient pathways Cause: Not being able to access national IT and reporting systems under the new CCG organisation
Engaging with CSU as an emergent Data Management Integration Centre Flagged issue with NHS England Engaging at national level workshops Engaging with CSU around how to
12
↔
4 Preparing application to HSCIC to become an Accredited Safe Haven – ASH Status now confirmed
30/09/2013
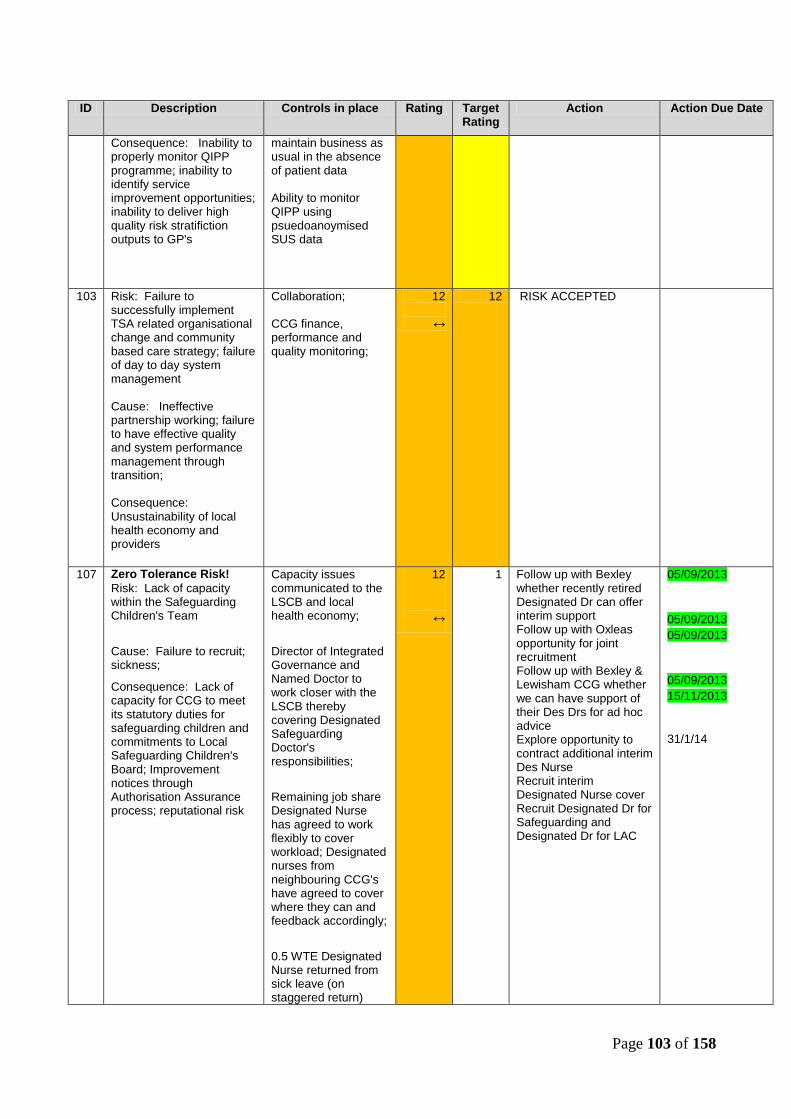
Page 103 of 158
ID Description Controls in place Rating Target Rating
Action Action Due Date
Consequence: Inability to properly monitor QIPP programme; inability to identify service improvement opportunities; inability to deliver high quality risk stratifiction outputs to GP's
maintain business as usual in the absence of patient data Ability to monitor QIPP using psuedoanoymised SUS data
103 Risk: Failure to successfully implement TSA related organisational change and community based care strategy; failure of day to day system management Cause: Ineffective partnership working; failure to have effective quality and system performance management through transition; Consequence: Unsustainability of local health economy and providers
Collaboration; CCG finance, performance and quality monitoring;
12
↔
12 RISK ACCEPTED
107 Zero Tolerance Risk!
Risk: Lack of capacity within the Safeguarding Children's Team
Cause: Failure to recruit; sickness;
Consequence: Lack of capacity for CCG to meet its statutory duties for safeguarding children and commitments to Local Safeguarding Children's Board; Improvement notices through Authorisation Assurance process; reputational risk
Capacity issues communicated to the LSCB and local health economy;
Director of Integrated Governance and Named Doctor to work closer with the LSCB thereby covering Designated Safeguarding Doctor's responsibilities;
Remaining job share Designated Nurse has agreed to work flexibly to cover workload; Designated nurses from neighbouring CCG's have agreed to cover where they can and feedback accordingly;
0.5 WTE Designated Nurse returned from sick leave (on staggered return)
12
↔
1 Follow up with Bexley whether recently retired Designated Dr can offer interim support Follow up with Oxleas opportunity for joint recruitment Follow up with Bexley & Lewisham CCG whether we can have support of their Des Drs for ad hoc advice Explore opportunity to contract additional interim Des Nurse Recruit interim Designated Nurse cover Recruit Designated Dr for Safeguarding and Designated Dr for LAC
05/09/2013
05/09/2013
05/09/2013
05/09/2013
15/11/2013
31/1/14
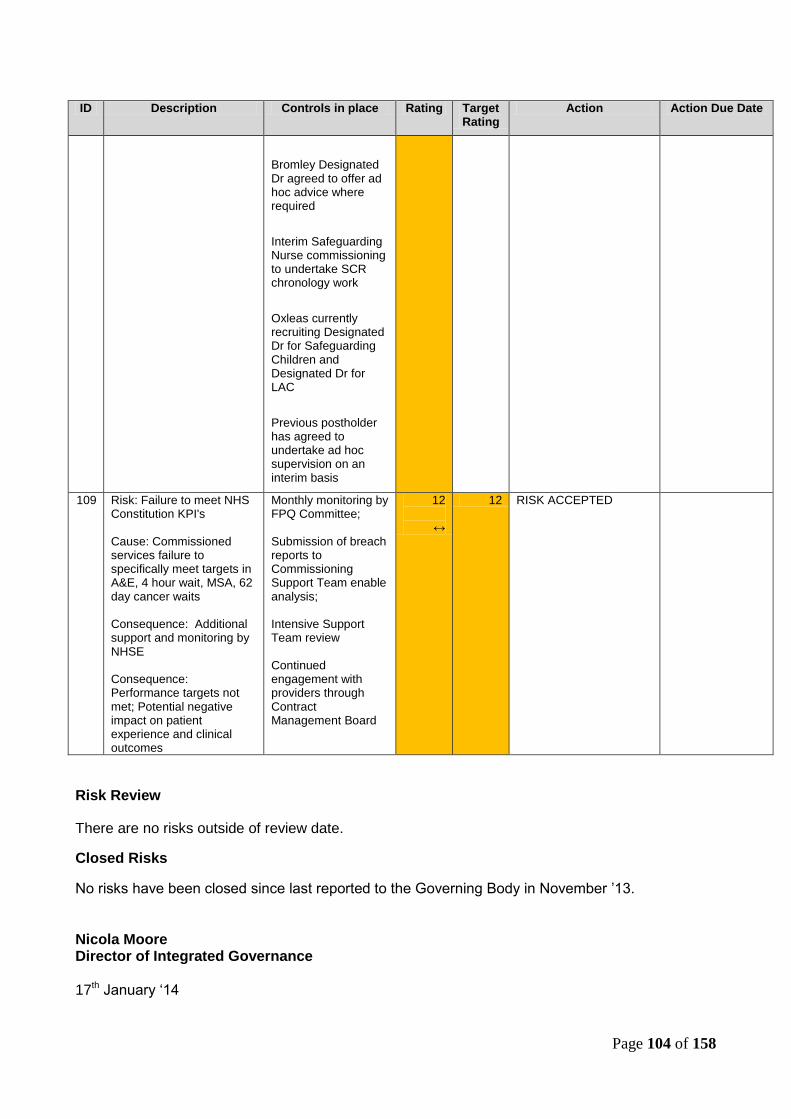
Page 104 of 158
ID Description Controls in place Rating Target Rating
Action Action Due Date
Bromley Designated Dr agreed to offer ad hoc advice where required
Interim Safeguarding Nurse commissioning to undertake SCR chronology work
Oxleas currently recruiting Designated Dr for Safeguarding Children and Designated Dr for LAC
Previous postholder has agreed to undertake ad hoc supervision on an interim basis
109 Risk: Failure to meet NHS Constitution KPI's Cause: Commissioned services failure to specifically meet targets in A&E, 4 hour wait, MSA, 62 day cancer waits Consequence: Additional support and monitoring by NHSE Consequence: Performance targets not met; Potential negative impact on patient experience and clinical outcomes
Monthly monitoring by FPQ Committee; Submission of breach reports to Commissioning Support Team enable analysis; Intensive Support Team review Continued engagement with providers through Contract Management Board
12
↔
12 RISK ACCEPTED
Risk Review
There are no risks outside of review date.
Closed Risks
No risks have been closed since last reported to the Governing Body in November ‟13.
Nicola Moore Director of Integrated Governance 17th January „14
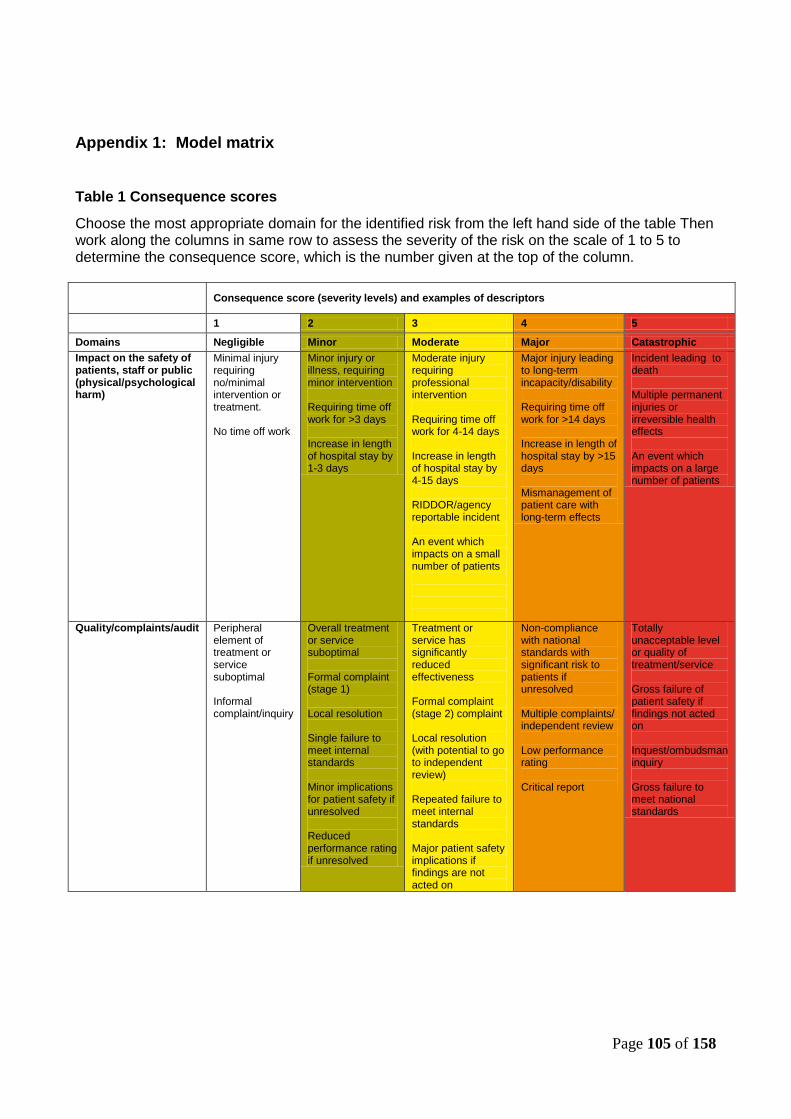
Page 105 of 158
Appendix 1: Model matrix
Table 1 Consequence scores
Choose the most appropriate domain for the identified risk from the left hand side of the table Then work along the columns in same row to assess the severity of the risk on the scale of 1 to 5 to determine the consequence score, which is the number given at the top of the column.
Consequence score (severity levels) and examples of descriptors
1 2 3 4 5
Domains Negligible Minor Moderate Major Catastrophic
Impact on the safety of patients, staff or public (physical/psychological harm)
Minimal injury requiring no/minimal intervention or treatment. No time off work
Minor injury or illness, requiring minor intervention Requiring time off work for >3 days Increase in length of hospital stay by 1-3 days
Moderate injury requiring professional intervention Requiring time off work for 4-14 days Increase in length of hospital stay by 4-15 days RIDDOR/agency reportable incident An event which impacts on a small number of patients
Major injury leading to long-term incapacity/disability Requiring time off work for >14 days Increase in length of hospital stay by >15 days Mismanagement of patient care with long-term effects
Incident leading to death Multiple permanent injuries or irreversible health effects An event which impacts on a large number of patients
Quality/complaints/audit Peripheral element of treatment or service suboptimal Informal complaint/inquiry
Overall treatment or service suboptimal Formal complaint (stage 1) Local resolution Single failure to meet internal standards Minor implications for patient safety if unresolved Reduced performance rating if unresolved
Treatment or service has significantly reduced effectiveness Formal complaint (stage 2) complaint Local resolution (with potential to go to independent review) Repeated failure to meet internal standards Major patient safety implications if findings are not acted on
Non-compliance with national standards with significant risk to patients if unresolved Multiple complaints/ independent review Low performance rating Critical report
Totally unacceptable level or quality of treatment/service Gross failure of patient safety if findings not acted on Inquest/ombudsman inquiry Gross failure to meet national standards

Page 106 of 158
Human resources/ organisational development/staffing/ competence
Short-term low staffing level that temporarily reduces service quality (< 1 day)
Low staffing level that reduces the service quality
Late delivery of key objective/ service due to lack of staff Unsafe staffing level or competence (>1 day) Low staff morale Poor staff attendance for mandatory/key training
Uncertain delivery of key objective/service due to lack of staff Unsafe staffing level or competence (>5 days) Loss of key staff Very low staff morale No staff attending mandatory/ key training
Non-delivery of key objective/service due to lack of staff Ongoing unsafe staffing levels or competence Loss of several key staff No staff attending mandatory training /key training on an ongoing basis
Statutory duty/ inspections
No or minimal impact or breech of guidance/ statutory duty
Breech of statutory legislation Reduced performance rating if unresolved
Single breech in statutory duty Challenging external recommendations/ improvement notice
Enforcement action Multiple breeches in statutory duty Improvement notices Low performance rating Critical report
Multiple breeches in statutory duty Prosecution Complete systems change required Zero performance rating Severely critical report
Adverse publicity/ reputation
Rumours Potential for public concern
Local media coverage – short-term reduction in public confidence Elements of public expectation not being met
Local media coverage – long-term reduction in public confidence
National media coverage with <3 days service well below reasonable public expectation
National media coverage with >3 days service well below reasonable public expectation. MP concerned (questions in the House) Total loss of public confidence
Business objectives/ projects
Insignificant cost increase/ schedule slippage
<5 per cent over project budget Schedule slippage
5–10 per cent over project budget Schedule slippage
Non-compliance with national 10–25 per cent over project budget Schedule slippage Key objectives not met
Incident leading >25 per cent over project budget Schedule slippage Key objectives not met
Finance including claims
Small loss Risk of claim remote
Loss of 0.1–0.25 per cent of budget Claim less than £10,000
Loss of 0.25–0.5 per cent of budget Claim(s) between £10,000 and £100,000
Uncertain delivery of key objective/Loss of 0.5–1.0 per cent of budget Claim(s) between £100,000 and £1 million Purchasers failing to pay on time
Non-delivery of key objective/ Loss of >1 per cent of budget Failure to meet specification/ slippage Loss of contract / payment by results Claim(s) >£1 million
Service/business interruption Environmental impact
Loss/interruption of >1 hour Minimal or no impact on the environment
Loss/interruption of >8 hours Minor impact on environment
Loss/interruption of >1 day Moderate impact on environment
Loss/interruption of >1 week Major impact on environment
Permanent loss of service or facility Catastrophic impact on environment

Page 107 of 158
Table 2 Likelihood score (L)
What is the likelihood of the consequence occurring?
The frequency-based score is appropriate in most circumstances and is easier to identify. It should be used whenever it is possible to identify a frequency.
Likelihood score 1 2 3 4 5
Descriptor Rare Unlikely Possible Likely Almost certain
Frequency How often might it/does it happen
This will probably never happen/recur
Do not expect it to happen/recur but it is possible it may do so
Might happen or recur occasionally
Will probably happen/recur but it is not a persisting issue
Will undoubtedly happen/recur,possibly frequently
Note: the above table can be tailored to meet the needs of the individual organisation.
Some organisations may want to use probability for scoring likelihood, especially for specific areas of risk which are time limited. For a detailed discussion about frequency and probability see the guidance notes.
Table 3 Risk scoring = consequence x likelihood ( C x L )
Likelihood
Likelihood score 1 2 3 4 5
Rare Unlikely Possible Likely Almost certain
5 Catastrophic 5 10 15 20 25
4 Major 4 8 12 16 20
3 Moderate 3 6 9 12 15
2 Minor 2 4 6 8 10
1 Negligible 1 2 3 4 5
Note: the above table can to be adapted to meet the needs of the individual trust.
For grading risk, the scores obtained from the risk matrix are assigned grades as follows
1 - 3 Low risk 4 - 6 Moderate risk
8 - 12 High risk
15 - 25 Extreme risk
Instructions for use
1 Define the risk(s) explicitly in terms of the adverse consequence(s) that might arise from the risk.
2 Use table 1 (page 13) to determine the consequence score(s) (C) for the potential adverse
outcome(s) relevant to the risk being evaluated.
3 Use table 2 (above) to determine the likelihood score(s) (L) for those adverse outcomes. If possible,
score the likelihood by assigning a predicted frequency of occurrence of the adverse outcome. If this is not
possible, assign a probability to the adverse outcome occurring within a given time frame, such as the

Page 108 of 158
lifetime of a project or a patient care episode. If it is not possible to determine a numerical probability then
use the probability descriptions to determine the most appropriate score.
4 Calculate the risk score the risk multiplying the consequence by the likelihood: C (consequence) x L
(likelihood) = R (risk score)
5 Identify the level at which the risk will be managed in the organisation, assign priorities for remedial
action, and determine whether risks are to be accepted on the basis of the colour bandings and risk ratings,
and the organisation‟s risk management system. Include the risk in the organisation risk register at the
appropriate level.
Page 109 of 158
Enclosure: O
Agenda item: 13
GOVERNING BODY PAPER
Title of paper: BOARD ASSURANCE FRAMEWORK
Date of meeting: Wednesday 29th January „14
Presented by: Nicola Moore Title: Director of Integrated Governance
Prepared by: Nicola Moore Title: Director of Integrated Governance
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes x To assure and drive improvements in quality x
Ensure access to high quality primary care services
x
Meet statutory obligations x
Ensure access to high quality secondary care services
x
Take a long term approach to the health needs of the local population
x
Building a new Clinical Commissioning Group
x
Enhance communications with practices and patients
x
Enhance the use of information x Please provide brief executive summary:-
None.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Board Assurance Framework (x) Yes x No N/A
Impact on Environment (x) Yes x No N/A
Legal Implications (x) Yes x No N/A
Resource implications (x) Yes No N/A
Equality impact assessment (x) Yes x No N/A
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes x No N/A
Patient and Public Involvement (x) Yes x No N/A
Communications and Engagement (x) Yes x No N/A
Impact on CCG Constitution (x) Yes x No N/A
Brief Summary of Recommendations
The Governing Body is asked to review and agree the latest updated BAF, its scoring and outstanding actions.

Page 110 of 158
1. Executive Summary
1.1
This report provides an update of the Board Assurance Framework since last reported to the Governing Body on 27th November ‟13.
2. Impact Assessment and Risk Management Issues
2.1 N/A
2.2 N/A
3. Recommendations to the Governing body
3.1
The Governing Body is asked to review and agree the latest updated BAF, its scoring and outstanding actions.
Introduction
The BAF enables the CCG to focus on those risks that might compromise achieving its most
important (principal) annual objectives; and to map out both the key controls that should be in
place to manage those objectives and confirm the Governing Body has gained sufficient assurance
about the effectiveness of those controls.
In line with best practice the BAF is now subject to contemporaneous review by the Senior
Executive Team. This report provides a progress update and identifies outstanding actions and
significant gaps in assurance.
Ongoing Review and Monitoring
Much effort has been made in reviewing the BAF, and ensuring the right controls and assurances
have been populated. Risk scoring has also been reviewed and changed so that now each
strategic objective is scored against the risk of not being achieved (consequence score) by the
likelihood of this occurring as a result of any gaps in control (likelihood). Scoring for each objective
is based on the worst case risk scenario.
2.1 Controls:
To date, the BAF broadly provides assurance of the controls in place that mitigate the risks that
may prevent the CCG meeting its annual Strategic Objectives. Since last reported, a number of
actions have been met and as a result these have now strengthened controls. Additionally, a
number of actions have been added where either further gaps in control and assurances have
been identified.
Of those outstanding actions within deadline to strengthen controls where the risk score is greater
than 12 the following are included:
Objective 1: To improve the health outcomes of the population of Greenwich and reduce
inequalities through commissioning clinical effective care pathways that meet the needs
identified in the JSNA and deliver the NHS Mandate
(c) Update HWB Strategy (HWB to do)
(c) Establishment of SEL Strategic Partnering arrangements will bring together joint commissioning
with NHSE
Objective 3: To ensure access to high quality, integrated secondary care services

Page 111 of 158
(c ) Establish a performance recovery process triggered by early warning systems
(c ) Establishment of SEL Strategic Partnering arrangements to develop new five year strategy
Objective 6: To enhance the use of information in all aspects of commissioning
(a) Develop a longer term strategy to achieve objective and integrated information from different
systems (via ASH Status)
There is one action that has missed its deadline. This is the action to increase the generation of
quality alerts which has plateaued. The CCG is currently reviewing the Quality Alert process with
LGNT. Since the merger of Lewisham and QE, there have been some teething problems with
LGNT responding to alerts which may have contributed to a lack of confidence in the system.
2.2 Significant Gaps in Assurance
There is one significant gap in assurance which relates to the failure to meet all NHS Constitution
Standards. Currently, there is a gap in control : Lack of performance recovery process triggered
by early warning systems. CCG is currently underperforming against the NHS Constitution
Standards for 4 hr wait; MSA; C Diff; Cancer 62 day wait and 18 week. This will be mitigated
through the actions set out in Objective 3 above.
Recommendation
The Governing Body is asked to review and agree the scoring of the BAF, and note the actions
remaining.
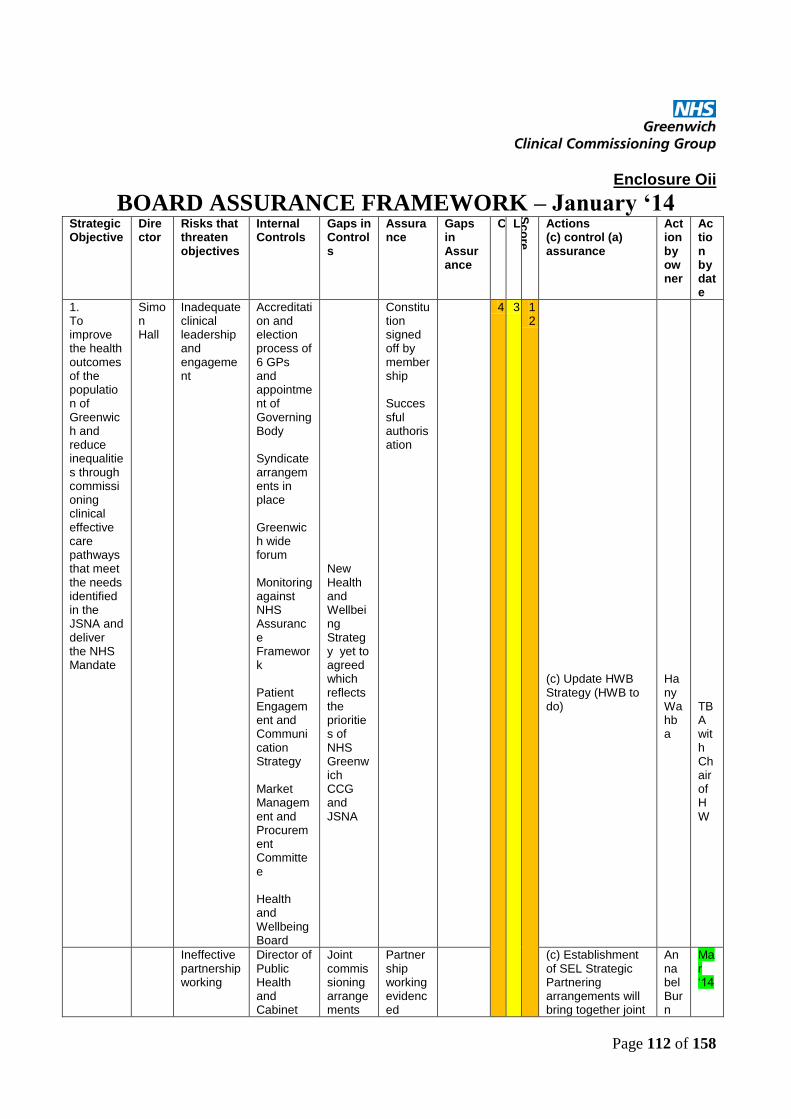
Page 112 of 158
Enclosure Oii
BOARD ASSURANCE FRAMEWORK – January ‘14 Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
1. To improve the health outcomes of the population of Greenwich and reduce inequalities through commissioning clinical effective care pathways that meet the needs identified in the JSNA and deliver the NHS Mandate
Simon Hall
Inadequate clinical leadership and engagement
Accreditation and election process of 6 GPs and appointment of Governing Body Syndicate arrangements in place Greenwich wide forum Monitoring against NHS Assurance Framework Patient Engagement and Communication Strategy Market Management and Procurement Committee Health and Wellbeing Board
New Health and Wellbeing Strategy yet to agreed which reflects the priorities of NHS Greenwich CCG and JSNA
Constitution signed off by membership Successful authorisation
4 3 12
(c) Update HWB Strategy (HWB to do)
Hany Wahba
TBA with Chair of HW
Ineffective partnership working
Director of Public Health and Cabinet
Joint commissioning arrangements
Partnership working evidenced
(c) Establishment of SEL Strategic Partnering arrangements will bring together joint
Annabel Burn
Mar „14
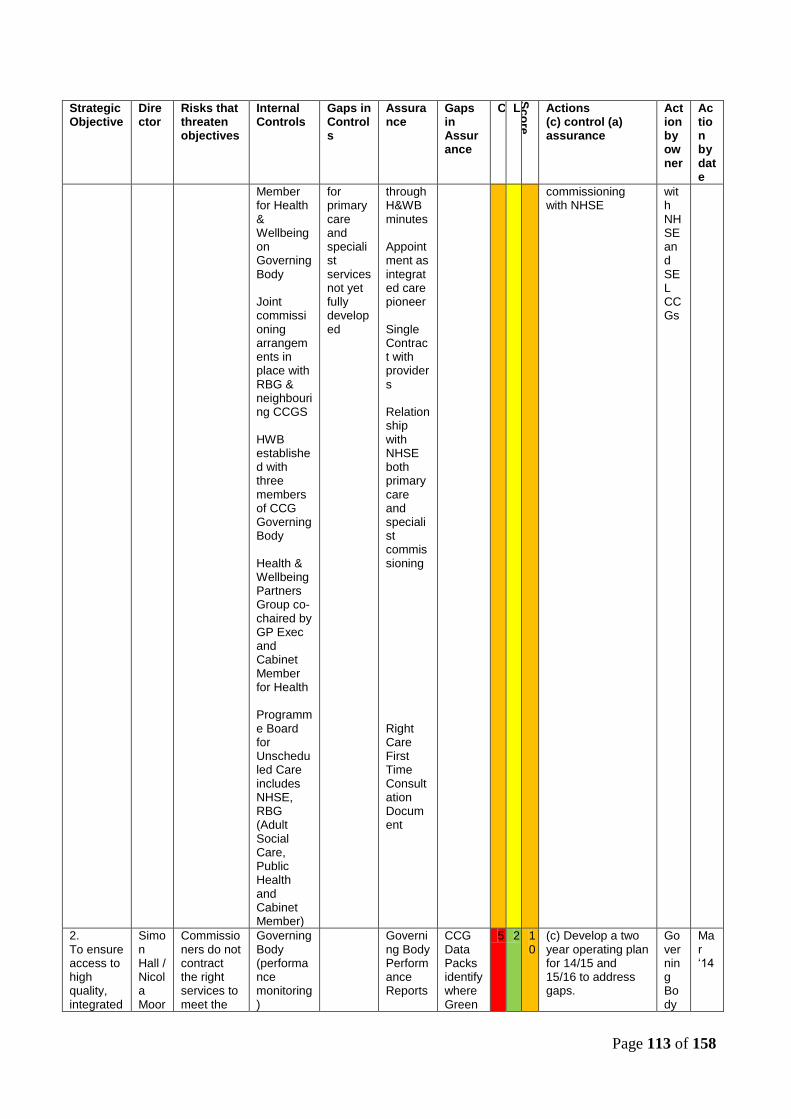
Page 113 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
Member for Health & Wellbeing on Governing Body Joint commissioning arrangements in place with RBG & neighbouring CCGS HWB established with three members of CCG Governing Body Health & Wellbeing Partners Group co-chaired by GP Exec and Cabinet Member for Health Programme Board for Unscheduled Care includes NHSE, RBG (Adult Social Care, Public Health and Cabinet Member)
for primary care and specialist services not yet fully developed
through H&WB minutes Appointment as integrated care pioneer Single Contract with providers Relationship with NHSE both primary care and specialist commissioning Right Care First Time Consultation Document
commissioning with NHSE
with NHSE and SEL CCGs
2. To ensure access to high quality, integrated
Simon Hall / Nicola Moor
Commissioners do not contract the right services to meet the
Governing Body (performance monitoring)
Governing Body Performance Reports
CCG Data Packs identify where Green
5 2 10
(c) Develop a two year operating plan for 14/15 and 15/16 to address gaps.
Governing Body
Mar „14
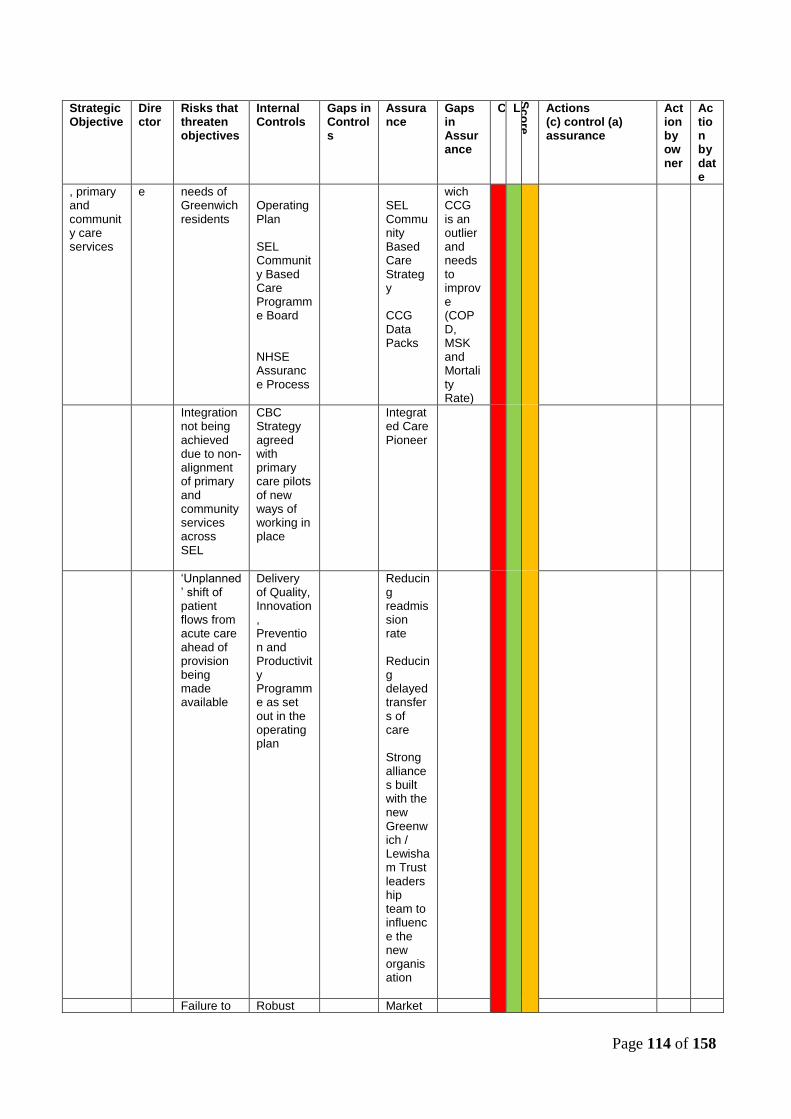
Page 114 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
, primary and community care services
e needs of Greenwich residents
Operating Plan SEL Community Based Care Programme Board NHSE Assurance Process
SEL Community Based Care Strategy CCG Data Packs
wich CCG is an outlier and needs to improve (COPD, MSK and Mortality Rate)
Integration not being achieved due to non-alignment of primary and community services across SEL
CBC Strategy agreed with primary care pilots of new ways of working in place
Integrated Care Pioneer
„Unplanned‟ shift of patient flows from acute care ahead of provision being made available
Delivery of Quality, Innovation, Prevention and Productivity Programme as set out in the operating plan
Reducing readmission rate Reducing delayed transfers of care Strong alliances built with the new Greenwich / Lewisham Trust leadership team to influence the new organisation
Failure to Robust Market

Page 115 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
move towards 7 day model
procurement framework
Management and Procurement Committee
Lack of capacity to monitor small providers
Regular contracting meetings with providers
Oversight by the Quality Committee
Unable to synthesise quality assurance for safeguarding adults
(a ) Short life project to strengthen quality assurance of small providers
Nicola Moore
Mar „14
Failure to up-skill primary care to manage planned care follow-ups
Training and Development Strategy for Primary Care
(c ) Development of Training and Development Strategy for Primary Care as part of GP Development plan
Eugenia Lee/ Rebecca Rosen
Mar „14
Failure to meet NHS Constitution Access Standards
Performance monitoring through FQP Committee
Lack of a performance recovery process triggered by early warning systems
Performance against NHS England Assurance Framework C Diff in the community
(c ) Establish a performance recovery process triggered by early warning systems – specifically for C Diff
Annabel Burn
Mar „14
3. To ensure access to high quality, integrated secondary care services
Simon Hall
Failure to meet NHS Constitution Access Standards
Performance monitoring through FQP Committee
Lack of a performance recovery process triggered by early warning systems
Performance against NHS England Assurance Framework 4 hr wait; MSA; C Diff; Cancer 62 day wait
5 3 15
(c ) Establish a performance recovery process triggered by early warning systems
Annabel Burn
Mar „14
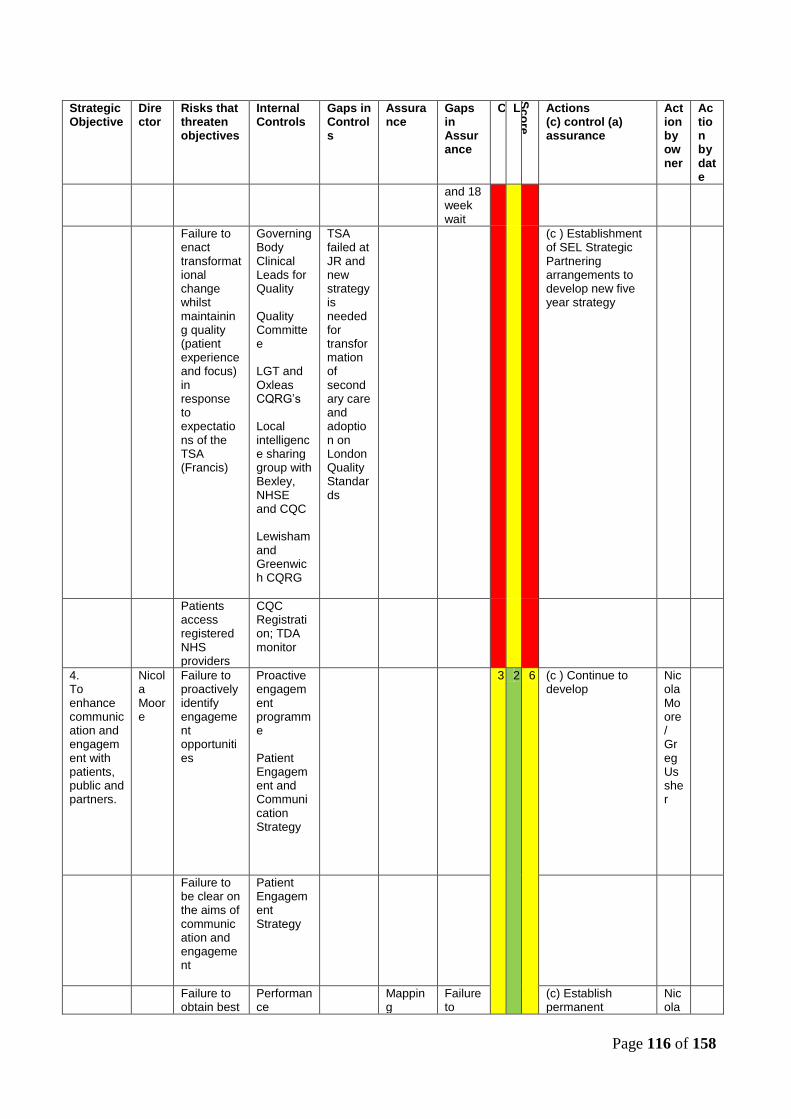
Page 116 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
and 18 week wait
Failure to enact transformational change whilst maintaining quality (patient experience and focus) in response to expectations of the TSA (Francis)
Governing Body Clinical Leads for Quality Quality Committee LGT and Oxleas CQRG‟s Local intelligence sharing group with Bexley, NHSE and CQC Lewisham and Greenwich CQRG
TSA failed at JR and new strategy is needed for transformation of secondary care and adoption on London Quality Standards
(c ) Establishment of SEL Strategic Partnering arrangements to develop new five year strategy
Patients access registered NHS providers
CQC Registration; TDA monitor
4. To enhance communication and engagement with patients, public and partners.
Nicola Moore
Failure to proactively identify engagement opportunities
Proactive engagement programme Patient Engagement and Communication Strategy
3 2 6 (c ) Continue to develop
Nicola Moore / Greg Ussher
Failure to be clear on the aims of communication and engagement
Patient Engagement Strategy
Failure to obtain best
Performance
Mapping
Failure to
(c) Establish permanent
Nicola
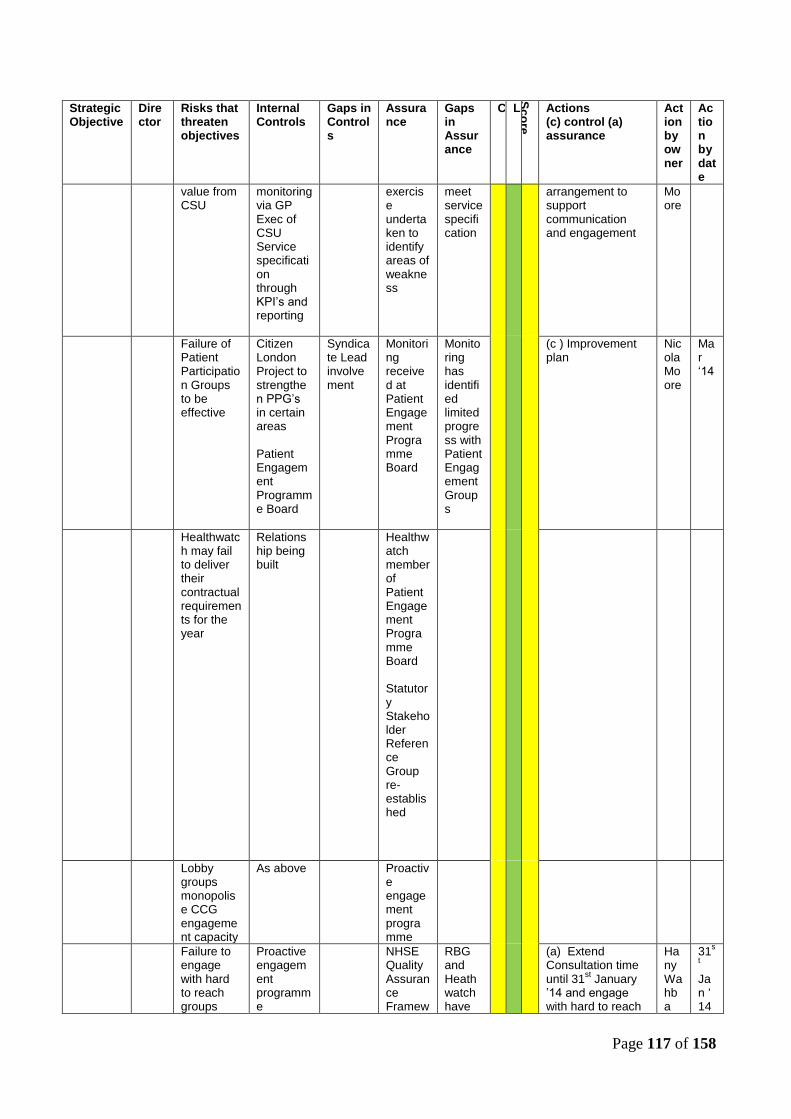
Page 117 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
value from CSU
monitoring via GP Exec of CSU Service specification through KPI‟s and reporting
exercise undertaken to identify areas of weakness
meet service specification
arrangement to support communication and engagement
Moore
Failure of Patient Participation Groups to be effective
Citizen London Project to strengthen PPG‟s in certain areas Patient Engagement Programme Board
Syndicate Lead involvement
Monitoring received at Patient Engagement Programme Board
Monitoring has identified limited progress with Patient Engagement Groups
(c ) Improvement plan
Nicola Moore
Mar „14
Healthwatch may fail to deliver their contractual requirements for the year
Relationship being built
Healthwatch member of Patient Engagement Programme Board Statutory Stakeholder Reference Group re-established
Lobby groups monopolise CCG engagement capacity
As above Proactive engagement programme
Failure to engage with hard to reach groups
Proactive engagement programme
NHSE Quality Assurance Framew
RBG and Heathwatch have
(a) Extend Consultation time until 31
st January
‟14 and engage with hard to reach
Hany Wahba
31s
t Jan „ 14

Page 118 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
Knowledge Transfer Project Engagement Tool to ensure engagement with 9 Protected Groups Stakeholder database being developed Patient Engagement Programme Board
ork Transformation Programme Communication and Engagement Plans Reports to the Governing Body
asked CCG to increase engagement with hard to reach groups as part of Right Care First Time Consultation
groups and Simon Hall
5. To build the new NHS Greenwich Clinical Commissioning Group as „one organisation‟ with a shared culture and behaviours which is driven by its membership. Develop the Governing Body to facilitate delivery of our mission within the accountability framework with NHS England
Failure to have in place an effective Organisational Development Plan
HR CSU support built into service specification OD Partner in place
Membership Engagement Strategy Refresh of OD Plan
No reporting available as plan not in place
4 2 8 (c) Produce Membership Engagement Strategy (c) OD Partner development of OD plan through OD programme
Nicola Moore Nicola Moore
Mar „14 Mar „14

Page 119 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
(incl. statutory duty to break even and duty of quality).
Failure to operationalise strategic objectives
Objective setting with governing body cascaded through the organisation Appraisal policy
Personal appraisal throughout the year Staff survey
Mid-year appraisals not all completed
(c ) OD Partner strengthening clinical commissioner roles objectives and personal development planning
Annabel Burn
Mar „14
Lack of leadership commitment and capacity Conflict of clinical - v – CCG priorities
Cascade objectives to Governing Body, Syndicate Leads, CPL and employed teams and monitor these OD to promote and improve engagement with members and widen participation in the commissioning cycle throughout the year All CPL‟s have been set objectives
Develop personal development plans to support delivery.
Routine oversight of CPL work programmes underdeveloped Syndicate Development required to engage wider membership
(c ) OD Partner supporting GP Executive to improve oversight of CPL‟s and support Syndicate Leads in fulfilling their role
Annabel Burn
March „14
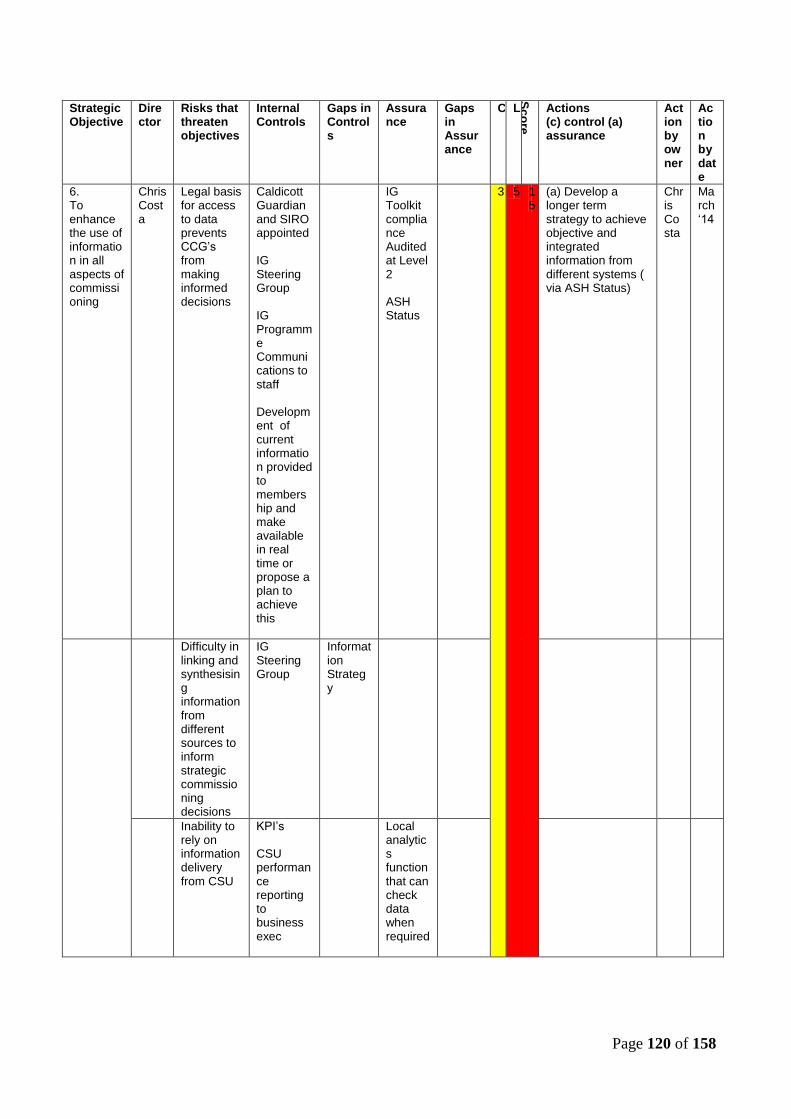
Page 120 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
6. To enhance the use of information in all aspects of commissioning
Chris Costa
Legal basis for access to data prevents CCG‟s from making informed decisions
Caldicott Guardian and SIRO appointed IG Steering Group IG Programme Communications to staff Development of current information provided to membership and make available in real time or propose a plan to achieve this
IG Toolkit compliance Audited at Level 2 ASH Status
3 5 15
(a) Develop a longer term strategy to achieve objective and integrated information from different systems ( via ASH Status)
Chris Costa
March „14
Difficulty in linking and synthesising information from different sources to inform strategic commissioning decisions
IG Steering Group
Information Strategy
Inability to rely on information delivery from CSU
KPI‟s CSU performance reporting to business exec
Local analytics function that can check data when required
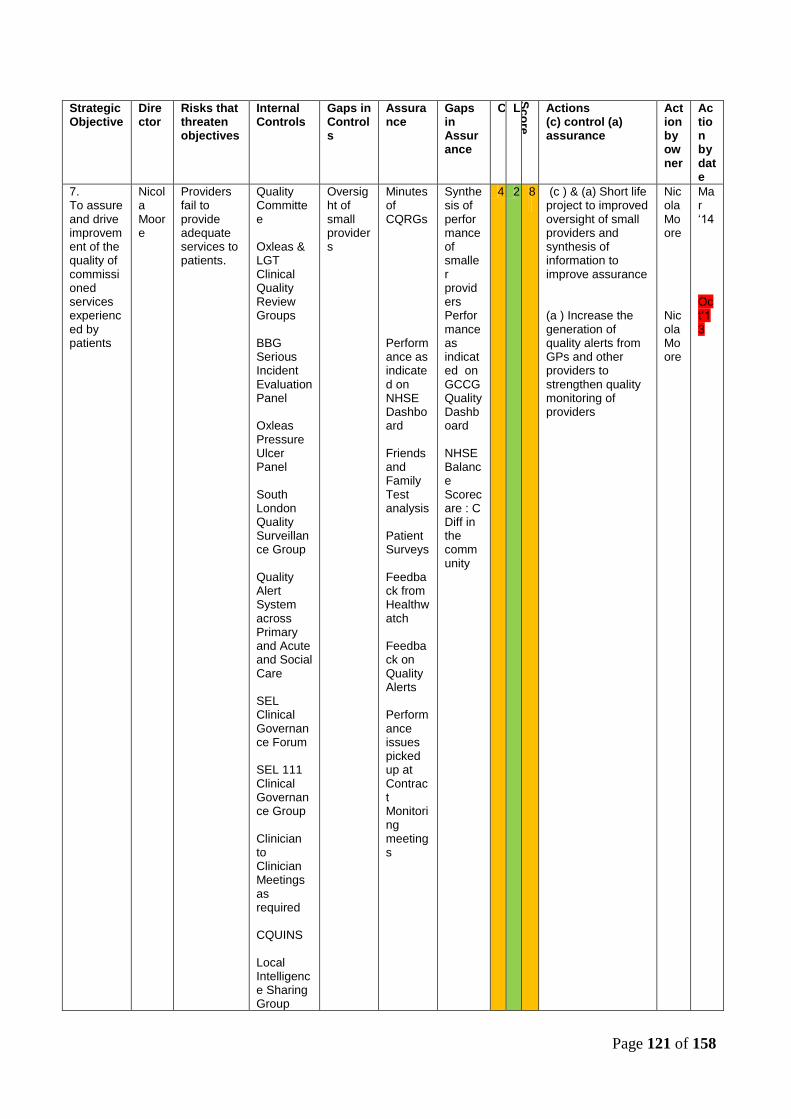
Page 121 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
7. To assure and drive improvement of the quality of commissioned services experienced by patients
Nicola Moore
Providers fail to provide adequate services to patients.
Quality Committee Oxleas & LGT Clinical Quality Review Groups BBG Serious Incident Evaluation Panel Oxleas Pressure Ulcer Panel South London Quality Surveillance Group Quality Alert System across Primary and Acute and Social Care SEL Clinical Governance Forum SEL 111 Clinical Governance Group Clinician to Clinician Meetings as required CQUINS Local Intelligence Sharing Group
Oversight of small providers
Minutes of CQRGs Performance as indicated on NHSE Dashboard Friends and Family Test analysis Patient Surveys Feedback from Healthwatch Feedback on Quality Alerts Performance issues picked up at Contract Monitoring meetings
Synthesis of performance of smaller providers Performance as indicated on GCCG Quality Dashboard NHSE Balance Scorecare : C Diff in the community
4 2 8
(c ) & (a) Short life project to improved oversight of small providers and synthesis of information to improve assurance (a ) Increase the generation of quality alerts from GPs and other providers to strengthen quality monitoring of providers
Nicola Moore NicolaMoore
Mar „14 Oct„13

Page 122 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
Consistency and completeness of quality data and failure to triangulate with soft intelligence
Provider Safety and Quality Reports Quality Accounts Data Sharing Protocols with NHSCIC Recently gained access to secondary use data
Making use of Internal Audit
Awaiting access to data (expected January ‟14)
Loss of soft intelligence to NHS England
Local Intelligence Sharing Group
Minutes from the Local Intelligence Sharing Group
Reports yet to be received from NHSE to identify key issues
(a ) NHSE to present local intelligence to Local Intelligence Sharing Group
Nicola Moore
Feb „14
Non-adoption of Francis principals, e.g. honesty, transparency and candour
New relationship established with Healthwatch
Progress report to the Governing Body
Improve performance on the annual staff survey
8. Meet the statutory obligations of the organisation including as outlined in the DH publication „Functions of CCGs‟: General planning, finance and
Chris Costa/Nicola Moore
Failure to achieve financial duties, including keeping spend within budget
Robust financial reporting system Reporting to FQP and challenge
Internal and external audit NHSE Annual report and accounts
4 1
4
(a )Financial balance with 2% surplus Compliance with legal requirements
Chris Costa
April „14
Non-implementation of statutory duty assurance systems
Risk register tracks risks throughout the year
Statutory Duty Assurance Framework to be
(c )Develop Statutory Duty Assurance Framework
Chris Costa
Mar „ 14

Page 123 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
governance
developed
Inappropriate use of resources
Counterfraud Policy and training in place Whistleblowing Policy
Audit Committee monitors counterfraud plan
Failure to monitor external and/or third parties to deliver statutory compliance
CSU performance reporting to business exec CSU checkpoint process
CSU Internal Audit
Budget is reduced (risk minimal)
Scenario planning
Internal Audit
9. To take a long term approach to the health needs of the population of Greenwich planning capacity to meet the growing population over a 5 year time horizon
Simon Hall
Ineffective partnership working
Inadequate capacity to develop strategic plans with partners
4
2
8
(c ) Increase CCG capacity to develop a new 5 year Strategy for Greenwich
Annabel Burn
Mar „14
CSU or Functions within Public Health MoU not delivered
CSU performance reporting to business exec; Performance reporting on PIR process through Quality Committee
PIR‟s are investigated in a timely way
Failure to define a 5 year strategy and embed
GCCG Commissioning Strategy Group
5 year strategy for Greenwich and
TSA Programme failed
(c ) Refresh the organisation‟s strategy ensuring that the operating plan for ‟14-‟15
Simon Hall
March „14

Page 124 of 158
Strategic Objective
Director
Risks that threaten objectives
Internal Controls
Gaps in Controls
Assurance
Gaps in Assurance
C L
Sc
ore
Actions (c) control (a) assurance
Action by owner
Action by date
into day-to-day operations i.e. operationalise strategy
(meeting x 3 per year); SEL Clinical Strategy Committee; TSA Partnership
SE London
addresses the health needs of Greenwich and improves the quality and safety of services and work with partners to create SEL 5 year strategy
Failure to deliver the first year of the 5 year time horizon
GCCG Commissioning Strategy Group (meeting x 3 per year); Governing Body Meetings; Business and GP Executive
(c ) Continue the development work for Eltham Community Hospital and the Greenwich Centre so that these new premises are specified to accommodate the shift of work into community settings and that we enable their completion in 2014
Simon Hall
Ongoing
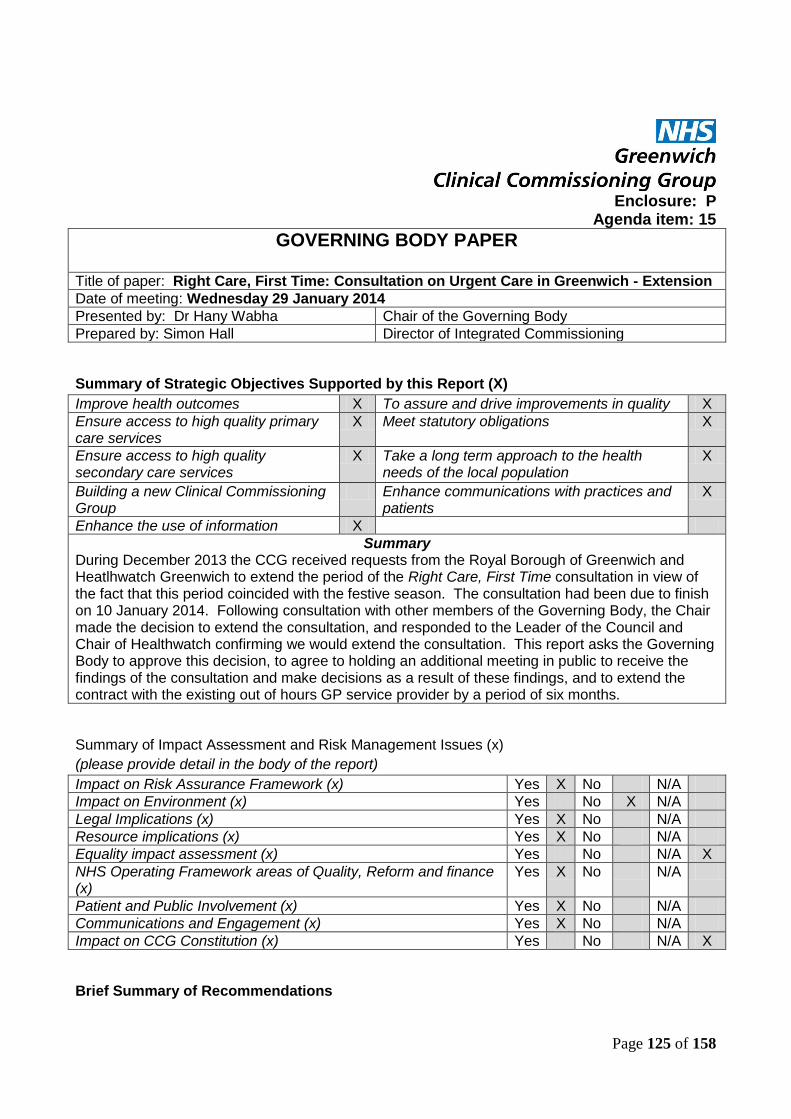
Page 125 of 158
Enclosure: P
Agenda item: 15
GOVERNING BODY PAPER
Title of paper: Right Care, First Time: Consultation on Urgent Care in Greenwich - Extension
Date of meeting: Wednesday 29 January 2014
Presented by: Dr Hany Wabha Chair of the Governing Body
Prepared by: Simon Hall Director of Integrated Commissioning
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes X To assure and drive improvements in quality X
Ensure access to high quality primary care services
X Meet statutory obligations X
Ensure access to high quality secondary care services
X Take a long term approach to the health needs of the local population
X
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
X
Enhance the use of information X
Summary During December 2013 the CCG received requests from the Royal Borough of Greenwich and Heatlhwatch Greenwich to extend the period of the Right Care, First Time consultation in view of the fact that this period coincided with the festive season. The consultation had been due to finish on 10 January 2014. Following consultation with other members of the Governing Body, the Chair made the decision to extend the consultation, and responded to the Leader of the Council and Chair of Healthwatch confirming we would extend the consultation. This report asks the Governing Body to approve this decision, to agree to holding an additional meeting in public to receive the findings of the consultation and make decisions as a result of these findings, and to extend the contract with the existing out of hours GP service provider by a period of six months.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes X No N/A
Impact on Environment (x) Yes No X N/A
Legal Implications (x) Yes X No N/A
Resource implications (x) Yes X No N/A
Equality impact assessment (x) Yes No N/A X
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes X No N/A
Patient and Public Involvement (x) Yes X No N/A
Communications and Engagement (x) Yes X No N/A
Impact on CCG Constitution (x) Yes No N/A X
Brief Summary of Recommendations

Page 126 of 158
Further to the decision made at the September 2013 Governing Body, the CCG received requests from the Royal Borough of Greenwich and Heatlhwatch Greenwich to extend the period of the Right Care, First Time consultation in view of the fact that this period coincided with the festive season. The consultation had been due to finish on 10 January 2014. In accordance with Standing Order 3.10 of our Constitution, the Chair and the acting Chief Officer consulted with two Governing Body members – Dr Rebecca Rosen and Mr Jim Wintour (who chaired the Steering Group that had produced the urgent care recommendations). Following their agreement, the Chair made the decision to extend the consultation, and responded to the Leader of the Council and Chair of Healthwatch confirming we would extend the consultation on 3 January 2014. This extension has subsequently been publicised in Greenwich Time, on the CCG website, and at all the events that we had undertaken since then. A consequence of extending the consultation is that the contract for our out of hours provider (Grabadoc) currently finishes on 31 March 2014. Leaving a decision on the future of urgent care, and this contract, to the (additional) Governing Body meeting on 26 February will give us insufficient time to reprocure the service. Legal advice has been sought, and has recommended that we are able to extend the current contract given we will have firm plans to reprocure, based on the decision we will make at our February 2014 meeting. Governing Body is therefore asked to agree to the extension of this contract, it having a value in excess of £1m per annum, but for a period of six months from its current end date. This additional period of consultation has enabled the CCG to run a number of additional public sessions, including in General Gordon Square in Woolwich, Morrison‟s Supermarket in Thamesmead, and ASDA in Charlton. A twitter discussion has been undertaken, as have additional focus groups in conjunction with Healthwatch Greenwich. These additional weeks have seen the interest in the consultation rise considerably, and has enabled us to get even more local engagement on our plans.
Recommendations
1. Governing Body is asked to approve Chair‟s action to extend the Right Care, First Time consultation by three weeks until 31 January 2013. 2. Governing Body is asked to agree to holding a specific session to consider the report following on from the Right Care, First Time consultation on urgent care services on 26 February 2014 in public. At this session decisions will be made that will affect all the future contracts for urgent care services funded by NHS Greenwich CCG, and a timetable for procurement of those services will be set. 3. Governing Body is asked to agree to the extension of the contract with the current out of hours GP service provider – Grabadoc Healthcare Society – for a period of six months until 30 September 2014.

Page 127 of 158
Enclosure: Q
Agenda item: 16
GOVERNING BODY PAPER
Title of paper: Eltham Community Hospital Update
Date of meeting: Wednesday 29th January 2014
Presented by: Chris Costa Chief Finance Officer
Prepared by: Chris Costa
Chief Finance Officer
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes To assure and drive improvements in quality
Ensure access to high quality primary care services
X Meet statutory obligations
Ensure access to high quality secondary care services
Take a long term approach to the health needs of the local population
X
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
Enhance the use of information Please provide brief executive summary:-
This paper informs the Governing Body that NHS England have formally approved the Eltham Community Hospital Business Case and that Community Health Partnerships have achieved financial close and the scheme is progressing as planned.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes x No N/A
Impact on Environment (x) Yes x No N/A
Legal Implications (x) Yes x No N/A
Resource implications (x) Yes x No N/A
Equality impact assessment (x) Yes x No N/A
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes x No N/A
Patient and Public Involvement (x) Yes x No N/A
Communications and Engagement (x) Yes x No N/A
Impact on CCG Constitution (x) Yes No x N/A
Brief Summary of Recommendations
To note and discuss.

Page 128 of 158
6th January 2014
Eltham Community Hospital gets the green light
A significant improvement to local healthcare in Greenwich has been agreed with contracts being
signed for the new Eltham Community Hospital (ECH).
The purpose-built 4,200sqm facility will eventually serve the health and well-being needs of
thousands of local people in Eltham and Greenwich. Among the services to be based at the
hospital will be two GP practices, Eltham Palace Surgery and Eltham Medical Practice. Combined,
these surgeries serve the needs of almost 16,000 patients.
In addition, the hospital‟s diagnostic suites will give GPs and health professionals access to
equipment including ECG, non-obstetric ultrasound, echocardiogram and X-Ray. There will be 40
intermediary care beds, out-patient consulting rooms with the capacity to treat around 32,000
people per year, as well as a minor surgery suite to deliver up to 1,500 low complexity procedures
per year.
Meanwhile, a variety of community services will also be relocated to the hospital, such as mental
health, community nursing, physiotherapy and paediatric departments.
Eltham Community Hospital is being developed through the Local Improvement Finance Trust
(LIFT) programme by BBG Lift Company, a public private partnership between Community Health
Partnerships (CHP) and LIFT Healthcare Investments Ltd, a consortium of four companies. NHS
Greenwich CCG, the Royal Borough of Greenwich, CHP and BBG LIFTCo have worked closely to
ensure feedback from residents has been incorporated to create a good facility for local people.
Hany Wahba, local GP and chair of NHS Greenwich Clinical Commissioning Group, said: “We are
delighted that this project is going ahead to provide excellent new healthcare services for local
people in Greenwich. This new community hospital has been developed as a coordinated care
service to integrate GPs, district nurses and social care. This will benefit patients by bringing health
and social care together in one place for easy access.
Enclosure Qii

Page 129 of 158
“This will be especially beneficial for those with complex needs and long term conditions as
services will be working together to help patients and carers to learn about self-management at
home.”
Preparations for construction works have already began and the building work is scheduled for
completion by December 2014. It is hoped that services will begin to move to the site from the start
of 2015 at the latest.
Neil McElduff, Executive Director at Community Health Partnerships, which is the national LIFT
Programme lead, said: “The new Eltham Community Hospital will be a modern facility, which will
enable the delivery of high quality integrated clinical and community services, which the local
population is desperate for. The LIFT programme has successfully delivered a significant range of
health and regeneration benefits for some of the most disadvantaged parts of England through the
creation of community-based buildings and facilities, which deliver 21st century health and social
care. Eltham Community Hospital will be a fine addition to the LIFT portfolio.”
The new facility has the strong endorsement of the local authority, professional staff and other key
stakeholders and has met the four key National “Tests” set by the Secretary of State in 2010. It is
ideally sited in line with the needs of the local population in particular providing services
appropriate for and accessible to the particular needs of an area with higher than average numbers
of older people, and significant pockets of deprivation.
Jonathan Holmes, CEO of Ashley House Plc, the developer for BBG LIFT, says “The facility has
been designed with local residents and P+HS Architects to maximise flexibility in the use of space
and drive greater efficiency across the local healthcare estate by housing two GP practice, 40
intermediary beds and a range of community mental health, diagnostic, out of hospital
consultations and minor surgery services.”
This is one the first schemes that CHP has taken through to financial close since the restructure of
the NHS, working closely with Greenwich CCG to complete the approvals process.
Speaking about the development, Dr Dermot Kenny, from Eltham Medical Practice, said: “We are
delighted to be moving our practice into the new Community Hospital. We are sad to be leaving
Court Yard after over fifty years but the opportunity was too good to miss. This development is the
most significant in the South of the borough for many years and will be to the benefit of all
residents of Eltham.”

Page 130 of 158
Ends
____________________________________________________________________
Notes to editor
Community Based Care is currently a key aim within Greenwich, by health and social care partners
working collaboratively in an integrated model, to move care out of hospitals and into the
community to provide the right care, in the right place and at the right time for local people.
About NHS Greenwich CCG
NHS Greenwich Clinical Commissioning Group (CCG) is responsible for commissioning most of
the healthcare services for the people of Greenwich. This means it is responsible for planning
which services need to be in place and ensuring that there are a range of healthcare providers able
to deliver care high quality care to patients when they need it.
For more information about NHS Greenwich CCG please visit www.greenwichccg.nhs.uk
About Community Health Partnerships
Community Health Partnerships is owned by the Department of Health and is the national lead for
the LIFT (Local Improvement Finance Trust) programme. CHP has a 40% shareholding in BBG
LIFTCo.
The LIFT programme continues to provide modern, purpose-built, clean and safe facilities for over
500 GP Practices, Pharmacies and a wide range of community and social care providers across
England.
For more information about Community Health Partnerships and LIFT please visit
www.communityhealthpartnerships.co.uk

Page 131 of 158
For further information and visuals contact: Mark Marston - [email protected] or 01628
600375. For further information about Ashley House, please visit www.ashleyhouseplc.com
For further media enquiries please contact: Sundeep Sehijpal or Michelle Simpson on 01527
579555 or email [email protected] or [email protected] or Stephen McCulloch
via [email protected] or 0203 049 9887
Issued on behalf of Community Health Partnerships and NHS Greenwich CCG by Gough Bailey Wright,
Kembrey House, 5 Worcester Road, Bromsgrove, Worcester, B61 7DL.

Enclosure: Ii Agenda item: 10.1
MEASURE
Traj
ect
ory
LEWISHAM &
GREENWICH OXLEAS - MH & COMMUNITY GUY'S KINGS DARTFORD & GRAVESHAM SLHT
LEWISHAM
Q3 Q1 Q2 Q3 Q1 Q2 Q3 Q1 Q2 Q3 Q1 Q2 Q3 Q1 Q2 Q1 Q2
Patient Throughput 0.938m 0.665m 0.373m 1.035m 0.353m
Contract Value £84.36m £30.51m £15.86m £112.45m £13.81m
Pat
ien
t Ex
per
ien
ce
Inpatient Survey
PEAT: Privacy & Dignity
Complaints 86 51 53 272 144 202 208 134 76 74 285 160 120 133
Complaint Response Times 82% 75% 96% 93.50% 54.53% 54.40% 53.67% 39.20% 67% 61%
Ombudsman's Rating 7
PEAT: Environment
PEAT: Food
Mixed Sex Accommodation 0 0 0 0 9 0 0 97 56 126 0 0 0 9 28 0 0
Friends & Family Test 38
Patient Voice Comments
Safe
ty
Number Incidents Reported 2297 2611 1052 1346
Serious Incidents 17 12 17 29 6 25 35 4 13 41 13 33 43
Never Events 0 6 0 2 0 1 1 0 1 0 1 1
Medical Errors
MRSA 0 0 0 1 2 2 0 2 0 1 2 0 0
C.Diff 6 1 0 3 9 8 13 13 4 3 15 1 3
Pressure Ulcers
Grade 1 55
Grade 2 121 96 93 101 117 60 29 28
Grade 3 0 21 20 26 30 10 27 2 0 39 53
Grade 4 0 4 3 13 24 6 8 2 0 25 15
Safety Thermometer
Idicators
Harm Free
Data Submitted
Data Submitted
Data Submitted
Data Submitted
Data Submitted
Data Submitted
Data Submitted
Data Submitted
Data Submitted
88.61%
Data Submitted
Data Submitted
Pressure Ulcers
7.26%
Falls 1.97%
Catheters 2.09%
Enclosure I A3 size

Page 133 of 158
& UTI
VTE 0.62%
Clinical Negligence Scheme Payments
Rule 43 Coroner Reports 1
MEASURE
Traj
ect
o
ry LEWISHAM
& GREENWICH
OXLEAS - MH & COMMUNITY GUY'S KINGS DARTFORD & GRAVESHAM SLHT LEWISHAM
Q3 Q1 Q2 Q3 Q1 Q2 Q3 Q1 Q2 Q3 Q1 Q2 Q3 Q1 Q2 Q1 Q2
Wo
rkfo
rce
Vacancy Rate 7% 7.50% 9% 8% 10.4%
Agency Spend 2150 2455
Sickness Rate 3.50% 3.45% 4.1% 3.47% 3.77%
Staff Retention Rate
Clin
ical
& O
per
atio
nal
Effe
ctiv
enes
s
VTE (Risk Assessment Compliance)
90% 93.1% 96.4% 96.5% 96.2% 98.1% 98.5% 94.1% 96.3% 95.7% 95.3% 95.9% 94.6% 95.1% 90.0%
Mortality Rate (SHMI) <1 0.8264 0.8038 0.9255 0.9146 95 87 1.0334 1.0456 0.9300
Mortality Rate (HSMR) 86 4.7% 90.80
Readmissions
RTT 18 Weeks
Admitted 90% 92.6% 96.0% 96.0% 96.6% 89.7% 88.6% 87.6% 91.3% 92.6% 92.9% 94.8% 91.7%
Non-
admitted 95% 98.0% 93.1% 93.1% 93.0% 97.2% 96.3% 97.3% 97.6% 97.7% 97.5% 98.9% 99.2%
Incomplete 92% 93.8% 93.7% 93.7% 93.5% 92.3% 92.1% 92.1% 95.4% 99.2% 95.3%
A&E Waiting times 95% 92.1% 99.6% 99.8% 99.8% 95.9% 95.7% 96.8% 96.3% 95.0% 89.4% 95.3% 94.5% 94.4% 93.5% 92.5% 95.7% 0.0%
Cancelled Operations 104 116 201 164 84 44 244 243 41 58
Lead
ersh
ip &
Go
vern
ance
Monitor Governance Rating
Monitor Financial Rating
Incident Reporting Culture
CQC Outcomes
1 Warning
notice (June)
Enclosure: Ii Agenda item: 10.1
Enclosure R
FINAL Minutes of the Audit Committee Wednesday, 4 September 2013, 1000-1200
31-37 Greenwich Park Street, Large Meeting room PRESENT: Jim Wintour (JW) Chair, Lay Member Greenwich CCG Dr M T Vandal (MTV) Secondary Care Doctor
Lay Member Greenwich CCG IN ATTENDANCE: Terry Blackman (TB) External Auditor Grant Thornton Annabel Burn (AB) Chief Officer Greenwich CCG Chris Costa (CC) Chief Finance Officer Greenwich CCG Kam Johal (KJ) Counter Fraud London Audit Consortium Marion Joynson (MJ) AD, Finance Greenwich CCG Fleur Nieboer (FN) Internal Auditor KPMG Sherry A Scheel (SAS) Minute Taker Greenwich CCG Dr Hany Wahba (HW) Chair, CCG Greenwich CCG 1. Welcome and introductions The chair welcomed everyone.
2. Apologies for absence Yemi Osho (YO) Nurse, Lay Member Greenwich CCG Dr Gregg Ussher (GU) PPE, Lay Member Greenwich CCG Simon Hall (SH) Director, Integrated
Commissioning Greenwich CCG 3. Declaration of Interest
There were no conflicts of interest declared. The chair asked representatives from the Internal and External Auditors to leave the room during agenda item 11 Procurement of CCG Internal Audit Services. 4. MINUTES OF LAST MEETING Minutes from the meeting held on 1st May 2013 were authorised and agreed to be accurate. 5. Matters arising not on the agenda MJ reported that the pension fund deficit on the GTP Annual Accounts was 1.43% of the overall liabilities of the pension fund. FN reported that she circulated the documents on Audit arrangement to SEL CSU.

Page 135 of 158
6. Internal Audit 6a. Internal Audit Plan
The committee noted the internal audit plan and asked FN to remove emergency planning
and prison health as the CCG is now a category II responder and prison health is no
longer the CCG‟s responsibility.
ACTIONS: FN to remove emergency planning and prison health from the risk assessment
and schedule of internal audit reviews.
6b. Audit Reviews
FN reported that there were inconsistencies between the authority delegated to the Quality
and the Audit Committee and the terms of reference for those committees. Areas where
the CCG could have delegated authority more appropriately i.e. a decision to approve the
budget which according to the scheme of delegation is a decision reserved to the
membership. Inconsistencies were also noted between authorisation limits in the scheme
of delegation and operational limits within the Oracle financial system operated by SBS.
Recommendations were provided in enclosure 4 titled “Scheme of Delegation”.
It was noted that approval of policies should be reserved to the Governing Body on the
recommendation of the Policy Committee to ensure effective review process.
6c. Internal Audit Progress Report - FN reported that there are 9 of the PCT Legacy
recommendations outstanding.
User access to Personal Identifiable Data (PID) – The CCG compiled a PID register in
2012/13 which has been updated for 2013/14. This will be reported to the next IG Steering
Group in September, prior to submission of the IG toolkit at the end of September.
FN informed the committee that they had agreed to swap the data protection audit with the
IG Toolkit audit and has agreed a review date ahead of the safe haven accreditation date.
CC informed the committee that CCG staff have completed the IG training and plans to
achieve Safe Haven level II status by October 2013. CC was pleased that the SEL CSU is
closed to achieving their level II status.
PC Port Control – this has not been implemented at this time. This has been formally
escalated by CC to CSU senior management for action
6d. Greenwich PCT Head of Internal Audit Opinion 2012/13

Page 136 of 158
There were no significant issues outstanding as at the year-end which impact on Head of
Internal Audit‟s opinion.
7. External Audit
The committee noted the report presented by Terry Blackman.
8. Counter Fraud KJ presented the final Counter Fraud work plan for 2013/14 and informed the committee of the progress made by the counter fraud team across the key areas of the NHS Counter Fraud Strategy. The committee approved the policies below and will be forwarded for ratification to the Governing Body. Anti-Fraud and Fraud Response Plan Anti-Bribery Policy AB asked if HR has adequate vetting checks KJ stated that she did have a conversation with HR, SEL CSU about vetting checks and that they did have procedures in place. It was noted that this should also be added in the contract to manage appropriate procedures and that it is being followed. 9. CCG Security Management Progress Report May 2013 CC presented a report to the committee and informed the group that LSMS will be
undertaking work covering Trust assets and Controlled Drugs.
10. Governance
10a. Audit Committee Forward Plan - this was reviewed resulting minor amendments to the plan. ACTIONS: SS to move External Audit report to May 2014. ACTIONS: SS to add item Board Assurance Framework (3.4.1) to every meeting 10b. Board Assurance Framework (BAF) - It was suggested that BAF should be a standing item for Audit Committee and continually gets updated. 10c. Risk Register – the Risk Register is discussed in several committees however, it was suggested that the Risk Assurance process is reviewed by the Audit Committee to ensure appropriate challenge. AB suggested that the committee looks at the lastest Risk Register that the Governing Body has received. ACTIONS: Nicola Havutcu to add a movement arrow in the current residual risk rating column and a covering paper to accompany the risk register, with a brief description of the changes from the last Governing Body.

Page 137 of 158
10e. Waiver of Tender - The committee noted the paper on Waiver of Tender 10h. Greenwich PCT Annual report – the committee noted there was no AGM for the PCT and no annual report would be presented to a Department of Health (DoH) AGM. Any Other Business The committee discussed the Terms of Reference (ToR), particularly quorum and
membership.
It was suggested that the vacant post of the GP executives could be made into a Non-
Executive Director.
The committee agreed that the revised ToR should be considered for approval by the
Governing Body.
ACTIONS: Nicola Havutcu to write a paper and identify all options.
ACTIONS: SS to change the wording to NON-Executive on Membership on the ToR
Procurement of Internal Audit Services – see Part II confidential minutes.
11. Next Meeting will be held on 13 December 2013, 10:00 – 12:30, 31-37 Greenwich Park Street SE10 9LR.

Page 138 of 158
Enclosure S FINANCE, PERFORMANCE AND QIPP COMMITTEE
Minutes of a Meeting held in the Large Meeting Room, GPS
28 October 2013 at 14:00
PRESENT: Jim Wintour (JWin) Chair, NHS Greenwich Clinical Commissioning Group (GCCG) Chris Costa (CC) Chief Finance Officer, GCCG Dr Hany Wahba (HW) Chair, Governing Body, GCCG IN ATTENDANCE: Geoff Berg (GB) Senior Strategy Manager, GCCG Langley Gifford) LG) Associate Director, Integrated Commissioning, GCCG Simon Hall (SH) Director, Integrated Commissioning, GCCG Nicola Havutcu (NH) Director, Integrated Governance, GCG Sherry A Scheel (SAS) Minute Taker, GCCG Andrew Thomas (AT) Associate Director, Strategy, Performance & QIPP, GCCG
1. Welcome and Apologies
The chair welcomed everyone to the meeting. 2. APOLOGIES:
Dr Junaid Bajwa (JB) GP Executive of the Governing Body, GCCG Annabel Burn (AB) Chief Officer, GCCG Alison Goodlad (AG) Associate Director, Service Redesign, Integrated Commissioning, GCCG Marion Joynson (MJ) Associate Director, Finance, GCCG Dr Eugenia Lee (EL) GP Executive of the Governing Body, GCCG Dr Nayan Patel (NP) GP Executive of the Governing Body, GCCG Ike Phillip (IP) Senior Acute Contracts Manager, NHS SLC Support Unit Rebecca Rosen (RR) GP Executive of the Governing Body Jennifer Wickenden (JWic) Associate Director, Acute Contracts SEL CSU, Ellen Wright (EW) GP Executive of the Governing Body
3. Declaration of Interests The Chair declared his interest on agenda item 8. that his wife is involved with Eltham Community Hospital on behalf of NHS The committee noted the declaration and agreed no further action required
4. Minutes It was agreed that the minutes of the previous meeting held on 9th September 2013 is an accurate record pending corrections.
5. Matters Arising not covered on the agenda None
6. Finance Performance & QIPP

Page 139 of 158
NHSE Balanced Scorecard AT reported that he will be submitting the NHS balance score card this week and that the submission date is prior to the Governing Body meeting therefore a Chair‟s Action will be required. ACTION: SAS to complete a Chair‟s Action form and submit to the next Governing Body meeting. Finance Month 6 CC reported that year to date and forecast surplus positions are within plan. All financial key performance indicators have a green rating based on most current data. At Month 6 there are overspends against the acute (£2.0m) budget and underspends against non-acute (£1.1m) and CCG Responsible Primary Care (£806k). The CCG was factoring in a risk of £7.3m. The CCG has now received a £5.7m allocation back from NHSE and 31.3m has been vired from the budget for specialist NCAs. The remaining uncovered risk is £256k which has been covered by underspends in on acute. There is an overspent in contract and agency staff, which have been extrapolated to the year-end resulting in £148k overspend. Financial risks that were identified were: Specialist services criteria – at month 6 the CCG received an allocation of £5.7m leaving a balance of £256k which has been mitigated through reserves and underspends. Delivery of financial savings through QIPP scheme – of the £9.9m programme, £6.9m has been agreed through contracts remaining business cases are being developed for progression through QIPP gateway Acute over performance – the financial forecast already includes £3.2m of acute over-performance which has been mitigated through use of the 0.5% contingency and commissioning reserves. This includes £6.8m over-performance with SLHT against planned activity. The worst case scenario assumes for further deterioration on SLHT in agreement of the M6 freeze position as part of the dissolution of the Trust. Continuing healthcare retrospective claims- This is based on two successful claims and have been at a higher rate than anticipated, and possibly the number of claims estimated can materialise at a higher rate, however, it is more than likely the number of claims will be less than forecast; SH team is currently reviewing this. Better Payments Practice Code – the CCG slid back in the month of September In the total number of invoices paid. And had done a lot of remedial work to include MJ meeting with people who are holding on to invoices in their workflow.

Page 140 of 158
It was noted that some of the invoices in the workflow were also being held up at CSU level and MJ has spoken to CSU and CCG managers about this. Performance AT reported that Acute activity reported through monthly monitoring returns (MAR) are in line with projections and decreased acute activities by POD Non Acute – Adult Mental Health Bed occupancy has come down over the summer months and additionally new initiatives designed to improve the occupancy rates have been introduced. Non-Acute IAPT LG reported that recovery rates at 44.5% for Q1 are holding up at above the London average but below the 50% standard. Non Acute Community Community services at Oxleas are above (JET, HID) and below (cardiology) targets. QIPP As at month 6 QIPP (Quality, Innovation, Productivity & Prevention) is delivering to plan, implementation of new initiatives in year has been slower than planned but additional project resource and business cases are now in place. Activity data is consistent with the shift of activity from acute to community. NHS Constitution Standards AT informed the committee that the CCG Assurance meeting is in November and asked everyone to think about building the narrative around to address issues around A&E waits, Cancer Waits, Mixed Sex Accommodation breaches and Cancelled Operations Cancer waits SH reported that Guy‟s & St Thomas is reluctant to share its data on Cancer waits with the Intensive Support Team. SH has raised this issue with CSU and it was recommended that SH raise this directly with the Lambeth CCG and NH will raise it through quality channels. ACTION: SH to take it up with Lambeth CCG on Cancer waits and NH to raise through quality channels A&E Performance Weekly exception reports highlight increased attendances, above the expected average, starting the day with patients in A&E with a decision to admit, availability of cubicle space, bed capacity, high numbers of ambulance attendances, high acuity of patients and delayed discharges. SH‟s team has been looking at several ways to help with the pressure i.e. to get the Trust to extend the UCC hours to 24/7; looking at acute bed capacity. The Chair asked for an estimated cost and benefits in operating 24/7 for UCC,

Page 141 of 158
someone to help with patient discharge in the weekend, opening an additional ward Referral to Treatment Performance (RTT) AT expressed concerns on the RTT performance and cancelled operations. ACTION: SH to take up with CSU on the performance of King‟s Hospital Performance on C.Diff has deteriorated with 10 new cases in August. Quality issues in particular, at SLHT is being reviewed at CQRG and has action plans in place. ACTION: SH to speak with Steve Whiteman Risk Significant risks to the organisation exist from the lack of access to PCD, this is being mitigated by our application for Accredited Safe Haven status.
7. Information Governance AT reported that they are close to submitting for Level II status this week.
8. Eltham Update CC reported that Community Health Partnerships (CHP) have now finalised the Full Business Case that will be submitted to NHS England for approval. The version attached to these papers removes certain Commercial in Confidence material but is substantially unchanged from the version that was approved by Greenwich PCT and the shadow CCG earlier in the year. CHP has asked for an updated letter of support from the CCG. A draft letter will be circulated before the meeting. This needs to be done urgently as to prevent squatters moving in. HW agreed to sign the updated letter.
9. SLHT Closedown Arrangements CC reported that SLHT closedown arrangement is this week. Simon Weldon and his team are standing by if it goes to arbitration.
10. 2014/15 – 2015/16 Planning Commissioning intention is to be submitted by November, the first submission is the operating plan (2 year) and strategic plan (5 year) by January 2014. There are engagement events throughout October 1013 to March 2014 with local stakeholders to discuss commissioning intentions. Healthwatch will be part of the Patient Reference Group and will be represented on the transformation steering groups to ensure that local knowledge, experience of care and the views of the wider community are taken into account.

Page 142 of 158
11. Any other Business none
12. Date of Next Meeting The next meeting is scheduled to be held on 16 December 2013, 1400 -1600, Greenwich Park Street, SE10 9LR
Page 143 of 158
Enclosure T Quality Committee 16 October 2013
Greenwich Park Street 10:00 – 12:00 PART ONE
PRESENT Dr Rebecca Rosen (RR) - Chair
Clinical Commissioner GCCG Governing Body
Dr Nike Arowobusoye (NA) Consultant in Public Health Greenwich Public Health Langley Gifford (LG) AD Integrated
Commissioning NHS Greenwich CCG
Nicola Havutcu (NH) Maggie Aiken (MA)
Director of Integrated Governance AD Governance & Quality
NHS Greenwich CCG NHS Greenwich CCG
Dr Eugenia Lee (EL) Clinical Commissioner GCCG Governing Body Andrew Thomas (AT) AD Strategy, Performance &
QIPP NHS Greenwich CCG
IN ATTENDANCE Clare Abberton (CA) Project Manager / Patient
Safety Officer - SI Manager NHS Greenwich CCG
Rena Amin (RA) Chief Pharmacist NHS Greenwich CCG Carol Berry (CB) Compliance Manager NHS Greenwich CCG Elena Lepore Governing Body Support
Officer NHS Greenwich CCG
APOLOGIES FOR ABSENCE Yemi Osho
Nurse Member (Chair) GCCG Governing Body
Ike Phillips Contracts Manager SL CSU Dr Greg Ussher Lay Member GCCG Governing Body Dr Ellen Wright Clinical Commissioner GCCG Governing Body
1. Welcome and Introductions Dr Rosen welcomed and thanked everyone for attending. As apologies had been received from Yemi
Osho and Dr Ellen Wright , Dr Rosen would Chair this meeting
Apologies for Absence As noted above. 3. Conflict of Interest None recorded. 4. Minutes of the previous meeting The minutes of the meeting held on 23rd September 2013 were not agreed as an accurate record of the discussion and actions. Subject to amendments required, these will be re-issued to members and approved. ACTION: EL 5. Matters Arising LA (Public Health) representation on the Quality Committee Dr Nike Arowobusoye was to contact Jay Stickland about representing RBG on the Greenwich CCG Quality Committee on an ad hoc basis.The group discussed this and it was agreed it would be helpful if Jay Strickland could attend on an ad hoc basis.

Page 144 of 158
ACTION: NA to follow up. Safeguarding Training for General Practice Dr Lee has been trying to arrange Adult Safeguarding training for her practice without success. This is part of mandatory training for General Practices. RBG should be delivering this training and it should be accessible to GPs. However, it is not Greenwich CCG‟s responsibility to ensure GPs are trained because the CCG does not commission them. It is for NHSE to pursue this. If nothing has happened by the time of the next meeting, consideration will be given to taking Adult Safeguarding training to QIPP Gateway. A reminder to be sent via „Commissioning Voice‟ on the availability of e learning packages. ACTION: Nicola Havutcu will take this up with SAMAG and LBG. ACTION: LG to follow up with NHSE ACTION: CB/KB to advise on e learning packages for mandatory training on Safeguarding. 3
Page 145 of 158
Quality of Services In Care Homes Review of cases from Care Homes to A&E and aligning LAS data with Care Homes. ACTION: LG to follow up with Magda Moorey the matter about A&E admissions from care homes. Infection Control Training for General Practice NA highlighted the need to ensure that there is Infection control training for GPs Practices and Care Homes around Infection Prevention and Control. The group considered whether this could become part of the workforce development strategy. She said a Greenwich practice has requested IC training and as an interim measure NA has been in touch with an infection control nurse to provide this. Public Health will fund this training as part of contribution to MOU. It was also further suggested that IC training could be done electronically ACTION: NA to report back. BOARD TO BOARD WITH OXLEAS RR would like to progress a Board to Board Meeting with Oxleas. Case studies suggested to date are:
It was suggested that the Board to Board meeting could take on the format of either one standard Board Meeting or a sub-group of both boards. Getting non-executives sighted on these issues would be useful. ACTION: NH and Maggie Aiken. Diabetic access for podiatry services (foot pathology) was discussed as part of the Compliance Report and continues to be an issue. ACTION: LG : Eligibility criteria to be reviewed with Oxleas with input from Melanie Lawless, who is running the Long Term Conditions work stream 6. Update on CQRG Arrangements The Terms of Reference have been agreed for the Lewisham and Greenwich CQRG. There are representatives from each of the three CCGs, Bexley, Greenwich & Lewisham. CQUINs will not feature greatly on the agenda – these will be discussed at a sub-group assuring sufficient time to discuss quality issues. A pre- 4

Page 146 of 158
meet has been agreed to be held two weeks before the CQRG to ensure the provider can respond appropriately to agenda items. ACTION: MA to distribute the Terms of Reference for this group to the committee. 7. Pressure Ulcer Report NH explained a Pressure Ulcer Working Group across Bexley, Bromley and Greenwich, and more recently including Lewisham, has been meeting for nearly a year with Karen Bates as chair. The boroughs have shared information and learnt from each other‟s experiences. As a result, there has been a reduction in the incidences of grade 2 and 3 ulcers. NHS England is working on a similar concept on a wider scale and is considering piloting the scheme across Bexley, Bromley and Greenwich. The concept is to have a standard method of treating pressure ulcers from one site to another, from hospital to home (care), so that everyone works to the same standards across the whole of south east London. Rena Amin informed the committee of her recent bid for foundation funds. It was unsuccessful as the treatment of pressure ulcers is not seen as a Primary Care function. A considerable amount of work has been put into this Medicines Management project, which involves an electronic monitoring system for use in the Primary Care setting. However, Tissue Viability Nurses do not see this as a Primary Care issue. ACTION: RA to discuss this with Dr Wright and Irene Grayson so that it can be included in the Primary Care Strategy, under „Access and Quality‟, for pursuit in the future. 8. Themed Review : Response to the National Recommendtions from Winterbourne View. LG presented the action plan in response to the national recommendations from Winterbourne View Hospital. NHS Greenwich CCG has been working with the Royal Borough of Greenwich and partners on this high profile safeguarding report. There are 16 recommendations in the report with more sub headings. All current placements will be reviewed and anyone who has been placed in a hospital inappropriately will be moved to community based support as soon as possible. 5

Page 147 of 158
By April 2014 each area will have a joint plan to ensure high quality care and support services for all people with learning disabilities, Autism and mental health conditions or behaviour described as challenging in line with best practice. There is a reciprocal arrangement for Greenwich patients in care homes outside Greenwich. RBG is the lead commissioner for learning difficulties but there are no specialist hospitals in the borough. However, there are nursing homes providing specialist nursing care. Therefore, these patients only have temporary residency status. The report covers a range of patient severity. Unannounced visits are partly contractual obligations and partly a quality and governance requirement. Unannounced visits at community based bed service homes should be undertaken as part of the norm. ACTION: MA/LG to create a recommendation for criteria for unannounced visits in care homes, including the Royal Borough of Greenwich, and involve John Nawrockyi. This requires joint work across Integrated Commissioning, Integrated Governance and RBG. ACTION: MA to schedule a further themed review for the Quality Committee to review implementation of the action plan. 9. Medicines Management Report NH presented a report on the pilot project to support GP prescribers manage patients scripted for BZD. Following the closure of a practice with high rates of Benzodiazepine (BZD) prescribing, a pilot project was approved to support GP prescribers managing patients who have been prescribed this drug inappropriately. Two more practices will now take part in this pilot with funding from last year‟s budget. Should a full roll out take place next year, the proposal should be linked up with budget setting to see whether this quality initiative fits with commissioning and Primary Care. This work could be linked to the work of the Amber Project because it ties in with vulnerable families. ACTION: NH to ensure MM team work with the Amber Project to take forward. 10. Public Health Updates Post Infection Review (PIR) NA informed the meeting of the new responsibility to complete a Post infection reviews for MRSA bacteremia . There have been 2 cases of MRSA and 28 cases of C. Diff cases reported by month 5 , 18 of which were community acquired . The trajectory set of these per 6

Page 148 of 158
annum is 40. AT raised the risk that we would breach this based on the current numbers The group discussed the trend and what could be done to reduce HCAIS. NA mentioned that some work she was doing showed that in general GPs were not all aware of their responsibilities around infection control, They also seemed unaware that a root cause analysis was required NA is exploring this further with Dr Ellen Wright and MA ACTION: NA to follow up with EW and MA. NA reported that there have been two MRSA cases, both assigned to the Acute Trust. 11. Quality Risk Report The current Quality Risk Report was distributed for noting. There were no new risks reported. The low uptake of immunisations was discussed and whether the low uptake can be attributable to poor GP training on immunisations and vaccinations. 12. Documents for Noting The following documents were distributed for information: a) Minutes of the Oxleas (Community) CQRG meeting (19.9.13)
b) Minutes of the SLHT CQRG meeting (last one of SLHT CGRG on 13.9.13)
c) Minutes of the GSCB (Greenwich Safeguarding Children Board) meeting Minutes of the Medicines Management Sub-Committee meetings will be distributed at future QC meetings. 13. Any Other Business 13.1. Seasonal Flu Vaccinations We are now in the seasonal flu season and practices have started vaccinating their patients. NHS England London have commissioned community pharmacists to support GPs and also vaccinate people from eligible risk groups To support local awareness PH have commissioned Healthwatch to raise awareness with local communities. Community Healthcare workers in Greenwich have proven to have the worst uptake in flu vaccination. This will be promoted through the Care Homeworkers Support Team through messaging. ACTION: NA to keep group informed of how the campaign is progressing 7

Page 149 of 158
13.2. Quality Strategy A Quality Strategy Planning Workshop will be planned to be held in Jan 2014.. Frequency of Quality Committee meetings was discussed and while Lewisham having just taken over responsibility for Queen Elizabeth Hospital and with winter pressures members agreed close scrutiny was required. It was agreed that 6 weekly meetings would be established. These would move to bi-monthly from April 2014 when the new CQRGs should be running smoothly. 13.3. Referral Management Booking System (RMBS) There is growing concern about the partial provision of services by AQPs, for example Blackheath Hospital, which has causing frustration for some patients. Specifics should be made absolutely clear at the time of contract negotiation. ACTION: LG to review as contracts are negotiated. 13.4. Complaints There have been reports about issues of GPs behaviour towards District Nurses. These complaints should be channelled through the appropriate body, that is formally to NHS England. The Medical Director, Jane Fryer‟s advice may be sought on this. ACTION: Carol Berry to follow up with NHSE.
Page 150 of 158
Notes of the Market Management and
Procurement Committee Meeting
17th October 2013
LMR, GREENWICH PARK STREET
PRESENT: Jim Wintour Chair Chris Costa Chief Finance Officer Ellen Wright Clinical Commissioner Leceia Gordon-Mackenzie Health Watch, Greenwich Jan Matthews Procurement and Delivery Manager Jillian Prescott Senior Procurement and Delivery Manager Alison Goodlad AD Service Redesign Irene Grayson AD Engagement In Attendance: Patricia Kanneh-Fitzgerald Support Officer Apologies: Nicola Havutcu Director, Integrated Governance Simon Hall Director, Integrated Commissioning
1. WELCOME AND INTRODUCTIONS ACTION
JW welcomed the group to the meeting
2. APOLOGIES FOR ABSENCE
As listed above.
3. CONFLICTS OF INTEREST
Declaration of Interest from Ellen Wright in terms of MSK procurement and will not take part in the discussion of this bidding.
4. Minutes and Matters Arising
Minutes – The following amendments were made. Matters arising on page 1: The group was informed that engagement will take place in November 2013. Item 5- RMBS Procurement It was agreed to go out to procurement with Bexley Item 6 – Local Enhanced Services – Diabetes: No decision was made. Item 8 – Contract Review and Writing Process - It was decided that this item be included in the Agenda of the meeting taking place in November.
5. MSK
AG informed the group of the following:
Over the last three years, Greenwich has been commissioning community MSK services on a pilot basis from Oxleas NHS Foundation Trust as an alternative for secondary based care.
Enclosure U
Page 151 of 158
Although this project appears to have been successful, a more comprehensive service, much broader in scope, now needs to be procured to meet the future needs of MSK services for the population of Greenwich.
Previously the former PCT planned to commission MSK services in partnership with Bexley; however Bexley have now commenced procurement for services inclusive of all MSK services including in-patient activity, for Bexley alone. This has led to an individual procurement being required for Greenwich.
The project aims to improve the patient‟s journey through the MSK service, ensuring that there are reduced non added value steps for the patient, enabling them to go through the service quicker.
The aim has been to redesign the service to look at a wider multidisciplinary team delivery, encompassing rheumatology, podiatry, low back pain and chronic pain.
MSK services are currently commissioned from a number of providers namely: Oxleas NHS Foundation Trust – Adult MSK Pilot Service, Physiotherapy, Podiatry South London Healthcare Trust – Rheumatology, Physiotherapy, Elective orthopaedics, Podiatry, chronic pain management Vanbrugh Clinic – Chronic pain management Areas to consider are:
The schemes are independent of one another meaning that they do not easily inter-relate.
Different providers provide different schemes, which can mean that there are not many providers that can offer all services, resulting in a potentially complicated care pathway.
Improving the entire patient pathway from primary care through to secondary care to ensure that the appropriate patients are on the right pathway at the right time.
Identification of waste in the system where there are high levels of DNAs
Ensuring supportive education for Primary care to help manage the patient pathway
Option 1: To procure the community service for 3 years Option 2: Prime contractor route for entire pathway via the restricted procurement route Option 3: Prime contractor route for entire pathway- via competitive dialogue. Option 4: Do nothing LG-M – wanted to know how the patient would be impacted and what engagement are we going to be doing. AG confirmed that we have already employed someone to carry out research around patient engagement. EW advised that we should use our commission intentions and other documents as a guide CC was unsure of what the committee is required to do. He is also unclear

Page 152 of 158
about what has been done in terms of managing the services. AG responded that it has gone through QIPP Gateway 1 and the next stage will be Gateway 2 The group made a partial decision excluding EW that they are leaned towards Option 2 but agreed with CC that it needs a lot of work.
6. Outcomes Based Commissioning
JP informed the group of the following:
CCGs are being tasked with adopting the use of outcomes based commissioning. By 2015 all CCGs will be required to have at least one outcomes based contract.
The 2014/15 Planning Guidance due in December 2013 will begin to direct CCGs to use outcomes based commissioning, and the 2014/15 NHS Standard Contract will accommodate outcomes based contracts.
JP advised the group that this approach takes longer and requires commissioners to be clear and confident about their required outcomes and the indicators they will use to measure their achievement. Public and patient engagement is required throughout the process, but particularly at the beginning to inform the outcomes chosen. JP will be feeding back to the group JP also informed the group that the timeline for pre procurement engagement is 12 – 15 weeks and that outcomes based commissioning is the prescribed direction of travel for everyone. CC confirmed that NHS England recommends that by 2015 all CCGs are expected to have done an outcome based commissioning. IG advised that we will have to provide a CQUINN for outcome based. JW advised that there are a lot of risks attached so we have to be careful who we offer the contracts to.
7. ANY OTHER BUSINESS
The will be in the agenda for the next meeting: - Report of Engagement - Diabetic Service Issues - Contract Review and Writing Process - Commissioning Support Services
LG-M AG LG
8. DATE OF NEXT MEETING
TBC

Page 153 of 158
Enclosure: Vi Agenda item: 21
GOVERNING BODY PAPER
Title of paper: Strengthening Delivery – Staff Consultation
Date of meeting: Wednesday 29th January 2014
Presented by: Annabel Burn Chief Officer
Prepared by: Annabel Burn
Chief Officer
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes To assure and drive improvements in quality
Ensure access to high quality primary care services
Meet statutory obligations
Ensure access to high quality secondary care services
Take a long term approach to the health needs of the local population
Building a new Clinical Commissioning Group
x Enhance communications with practices and patients
Enhance the use of information Please provide brief executive summary:-
This paper informs the Governing Body that a two week staff consultation has commenced on a proposal to change the senior management structure of the CCG. The case for change is set out in the paper.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes No x N/A
Impact on Environment (x) Yes No x N/A
Legal Implications (x) Yes No x N/A
Resource implications (x) Yes x No N/A
Equality impact assessment (x) Yes No x N/A
NHS Operating Framework areas of Quality, Reform and finance (x)
Yes No x N/A
Patient and Public Involvement (x) Yes x No N/A
Communications and Engagement (x) Yes x No N/A
Impact on CCG Constitution (x) Yes x No N/A
Brief Summary of Recommendations
To note.

Page 154 of 158
Enclosure Vii
Strengthening Delivery Consultation with NHS Greenwich CCG Employees
14 January 2014
1. Background & Scope After functioning for 9 months the Chair and Chief Officer have reviewed the structure of the senior leadership of Greenwich CCG and in this paper propose changes. These affect many staff employed in the organisation and so a consultation is being undertaken for a 2 week period from 20th January – 2nd February. There are no posts being made redundant through this process. It is acknowledged that there will be a reduction in the money that can be spent on management fees from April next year. The proposals here are affordable even after the increase in investment.
2. Case for Change
It has been recognised that there is too great a focus on the immediate operational concerns of the organisation and that although this has served the organisation well (delivering QIPP, financial stability) there are some areas that need greater attention and focus that the team has not been able to manage (performance issues, partnership working, Greenwich & SEL strategic development). The organisation is working hard to develop clinical commissioning as the way it does business. There are some strong examples of clinical commissioning that the CCG is rightly proud of. However this is not yet the norm. Although improvements in working practices (better prioritisation, improved communication etc) can be achieved through development, it is felt that there is just not sufficient capacity in the SMT to take the organisation to the next level of achievement. From the review the key areas that need additional investment have been identified as:
- Greater strategic focus o The organisation developed clear principles & priorities and supporting
workstreams but has not formally agreed its strategy in a way that allows work to be prioritised.
o The governing body held an away day a year ago (February 2013) and agreed to 5 strategic priorities and a work plan for the first 9 months of the CCGs existence. From this a set of one year objectives were agreed
Page 155 of 158
for the organisation and these are on track. However there has been little or no development of the longer term horizon and a fully developed strategy is not being actively developed.
o Areas of co commissioning between CCG/ NHSE/ RGB need greater exploration for the longer term. Short term arrangements are working but specialised commissioning, transfer for HV etc requires greater exploration of opportunities and a longer term plan is required for conditions where patients access primary, community, hospital including specialised services for example cancer.
- Greater engagement with RBG, SEL PMO and partner organisations and
providers at senior level but not reliant solely on the CO o Engagement has been strong but the implications of workstreams and
alignment of governance arrangements is more ad hoc and falls between functions.
o Engagement has been reactive and driven by external deadlines rather than driven by the strategic intent of Greenwich CCG.
o The CCG has not developed a clear plan concerning its engagement with
neighbours and partners beyond the desire to work collaboratively. This will require time to develop.
- Performance management
o Routine reporting of performance and use of the contracts is in place and working. Performance reporting is of a high quality. However where performance has slipped (or predicted to) and recovery plans by providers have not improved the situation there needs to be a response that brings performance back on track using all of the resources available to the CCG (managerial, contractual, clinical and influence). There is no single person responsible for this in the current organisational structure.
- Getting the most out of clinical commissioning o Clinical commissioners (GP Exec, SL, CPLs) are well engaged with
specific workstreams which are change programmes under QIPP. There are some good examples of GP Executive engagement through committees or formal structures on „business as usual‟ but clinical commissioners are not involved in the usual business outside this. The current structure has not yet integrated the work programmes fully. The Commissioning Directorate programme structure has started this through and has been refreshed recently but the work on Syndicate Leads sits outside this in a different directorate and this may not be helping the organisation work as one.

Page 156 of 158
- CO role stretched outside the organisation and within o To support the lack of capacity amongst the SMT the CO (who does not
hold a portfolio for specific functions within the organisation) has taken a leadership role in delivery over the last 10 months to support the organisation in the „start up‟ phase (communications and engagement, organisational development, strategy and performance management). Although helpful to the capacity at Director level this focus may have inadvertently reduced influence and impact externally (RBG, SEL, NHSE) and created more work for everyone and anyway is not sustainable.
- Organisational development o There is no formal OD resource within the organisation and although OD
is everyone‟s business the entity of a CCG is particularly complex. The work of the CCG is done with many partners and needs to draw on members, syndicates, RBG, NHSE and CCGs in SEL. Ways of working with different partners requires complex and sophisticated organisational responses and the current capability sits within the CO and Directors but tends to be treated as an add on or responsive act rather than a forward looking development.
o The focus for staff development (appraisal and development) is very limited and is likely to create problems as the organisation matures.
As the structure is reviewed it is worth bearing in mind the need for succession planning.
3. Proposals to address these problems
3.1 Current structure:
CO (VSM)
CFO (Band 9
DIC (Band 9) DIG (band 9)
Finance QIPP&
performance monitoring
Service redesign,
procurement, contract
management including
through joint commissioning;
strategy; procurement
Quality, communication
& engagement, governance,
OD
Membership management
Missing: performance management on behalf of the Governing Body

Page 157 of 158
3.2 Proposed Structure:
Create a Deputy CO role (VSM) with a portfolio for Strategy (including OD) & Performance which is similar to option 1 but empowers the Deputy CO to take a leadership role „first amongst equals‟ and by default to deputise for the CO
CO VSM Deputy CO VSM
CFO Band 9 DIC Band 9 DIG Band 9 Strategy Performance
OD Membership engagement
Finance QIPP&
performance monitoring
Service redesign,
procurement, contract
management including
through joint commissioning;
procurement
Quality, communication
& engagement, governance,
3.3 Supporting structures
With the establishment of a new Directorate of Strategy & Performance some individual staff will need to migrate to be part of this new team. The detailed substructures for Directorates will be designed once the chosen configuration has been identified but the following changes are proposed for all options:
The Head of Clinical Engagement and Membership Development manager currently works across The DIG and the DIC. The logical location for this function will be full time in the new Directorate focusing on membership engagement helping bring the clinical commissioning function into the mainstream of the work of the organisation.
The Directorate of Integrated Commissioning requires one additional senior post to support the Integrated Care Pioneer work and to manage winter surge which is now an all year activity. It is proposed that an additional 8d post is funded to lead this work funded from S256 monies. This could be offered as a secondment opportunity within the organisation in the first instance and any vacated post subsequently recruited to.
The new Directorate would also require support from the AD of Strategy, Performance and QIPP and the Senior Strategy Manager and these two posts would move from the Finance Directorate to the new Directorate.
There is an option to align management of the administrative pool with the new OD function in the Directorate of Strategy & Performance although the current

Page 158 of 158
manager of the administrative pool, the Executive Manager, needs to remain in the Directorate of Integrated Governance and it is proposed that this element of the change is consulted on and a decision is made once responses have been received.
5. Consultation 5.1 The period of consultation will start on 20th January 2014 for a period of two weeks. Copies of this paper will be sent to all employees in the CCG and job descriptions for the new and revised posts will be available during this period. All individuals affected by the proposals will have the opportunity of a meeting with their Line Manager and an HR representative.
5.2 Staff are asked to respond to this set of proposals by 1st February 2014. They can make any comments they wish but the template overleaf has been issued as some staff like to have a structure for responses. Please respond to any of the questions you would want to express a view on (ie you do not need to respond to all questions posed – please see these as prompts). Please respond to Caroline Linden, HR Business Partner ([email protected]) Manager. Questions of clarification are also welcomed so that the changes proposed are fully understood prior to implementation. After the period of consultation is completed, feedback and comments from staff will be collated and reviewed and a final outcome of the consultation and the way forward will be confirmed in writing to staff.
Annabel Burn Chief Officer, NHS Greenwich


















