Glomerulonephritis Medical Student Lecture 2
67
Glomerulonephritis Glomerulonephritis Dr G.O Ogun Dr G.O Ogun Department of Pathology, Department of Pathology, College of Medicine College of Medicine University of Ibadan University of Ibadan 1
-
Upload
ibnbasheer -
Category
Documents
-
view
3.023 -
download
1
Transcript of Glomerulonephritis Medical Student Lecture 2

GlomerulonephritisGlomerulonephritisDr G.O OgunDr G.O Ogun
Department of Pathology,Department of Pathology,College of Medicine College of Medicine University of IbadanUniversity of Ibadan
11

INTRODUCTIONINTRODUCTION
Disorder of glomerular structures and Disorder of glomerular structures and functions.functions.
Constitute major problems in nephrology.Constitute major problems in nephrology.
Most common cause of CRF/ESRD.Most common cause of CRF/ESRD.
$8 Billion expenditure on dialysis alone by $8 Billion expenditure on dialysis alone by US Government.US Government.
22

INTRODUCTION…ContdINTRODUCTION…Contd
Glomerulonephritis is an inflammation of Glomerulonephritis is an inflammation of glomerulus.glomerulus.
Glomerulopathy is all-embracing term for Glomerulopathy is all-embracing term for the disorders affecting this structures.the disorders affecting this structures.
Diagnosis hinges on identification of Diagnosis hinges on identification of derangement of normal glomerular derangement of normal glomerular configuration.configuration.
These changes are recongnised by LM, IM, These changes are recongnised by LM, IM, EM.EM.
33

Structure Of GlomerulusStructure Of Glomerulus
Anastomosing capillary networkAnastomosing capillary networkRenal artery > A&P >ILA > AA > ILBA > AFA.Renal artery > A&P >ILA > AA > ILBA > AFA.An afferent arteriole branching from an An afferent arteriole branching from an interlobular artery supplies the glomerulus with interlobular artery supplies the glomerulus with blood.blood. Within the glomerulus are many capillary loops Within the glomerulus are many capillary loops supported by mesangium. supported by mesangium. The mesangium can function both for filtration The mesangium can function both for filtration and phagocytosis. and phagocytosis. The glomerular capillaries have a fenestrated The glomerular capillaries have a fenestrated endothelium for filtration. endothelium for filtration.
44

GLOMERULAR CELLSGLOMERULAR CELLS
Epithelial cellsEpithelial cells
i. Visceral (podocytes)i. Visceral (podocytes)
ii. Parietalii. Parietal
Mesangial cellsMesangial cells
Endothelial cellsEndothelial cells 55

Structure of GlomerulusStructure of Glomerulus
66

Structure Of GlomerulusStructure Of Glomerulus
The capillary loops are surrounded by The capillary loops are surrounded by podocytes that have foot processes podocytes that have foot processes forming slits. forming slits.
A negative (anionic) charge on podocyte A negative (anionic) charge on podocyte foot processes helps keep negatively foot processes helps keep negatively charged proteins from filtering through. charged proteins from filtering through.
The urine consisting of water and waste The urine consisting of water and waste products (and some solutes to be products (and some solutes to be recovered later) collects initially in recovered later) collects initially in Bowman's space in the glomerulus.Bowman's space in the glomerulus.
77

STRUCTURE OF NORMAL GLOMERULISTRUCTURE OF NORMAL GLOMERULI
88

99

Structure of GlomerulusStructure of Glomerulus
1010

Structure of BMStructure of BMGBM- Lamina rara externa, Lamina densa, Lamina GBM- Lamina rara externa, Lamina densa, Lamina rara interna.rara interna.Collagen Type IV, laminin,polyanionic proteoglycans, Collagen Type IV, laminin,polyanionic proteoglycans, fibronectin, entactinfibronectin, entactinThe buiding block (monomer) is a triple helical The buiding block (monomer) is a triple helical molecule that are made up of three α chains, molecule that are made up of three α chains, composed of one or more of six α1-α6 (COL4A1-composed of one or more of six α1-α6 (COL4A1-COL4A6).COL4A6).Triple helix 3α. Triple helix 3α. α1α1- α2- α1combination (common)- α2- α1combination (common)Each molecule has 3 partsEach molecule has 3 parts
1.1. 7s domain (amino terminus)7s domain (amino terminus)2.2. Triple helical domain (middle)Triple helical domain (middle)3.3. Globular NC1 domain (carboxyl terminus).Globular NC1 domain (carboxyl terminus).
Antigen in the NC1 domain are the main target of anti Antigen in the NC1 domain are the main target of anti GBM nephritis and Goodpasture syndrome.GBM nephritis and Goodpasture syndrome.
1111

THE GLOMERULAR SYNDROMESTHE GLOMERULAR SYNDROMES
Acute nephritic syndromeAcute nephritic syndrome Hematuria, azotemia, variable Hematuria, azotemia, variable proteinuria, oliguria, proteinuria, oliguria,
edema,edema,and hypertensionand hypertension
Rapidly progressive GNRapidly progressive GN Acute nephritis, proteinuria, and Acute nephritis, proteinuria, and acute renal failureacute renal failure
Nephrotic syndromeNephrotic syndrome >3.5 gm proteinuria, >3.5 gm proteinuria, HypoalbuminemiaHypoalbuminemia
hyperlipidemia, lipiduriahyperlipidemia, lipiduriaChronic renal failureChronic renal failure Azotemia uremia progressing Azotemia uremia progressing
over the yearsover the yearsAsymptomatic hematuriaAsymptomatic hematuria Glomerular hematuria; Glomerular hematuria;
or proteinuria or proteinuria subnephrotic proteinuriasubnephrotic proteinuria
1212

CLASSIFICATIONCLASSIFICATION
AETIOLOGICALAETIOLOGICALPrimary (Renal)Primary (Renal)
Secondary (Systemic disorders)Secondary (Systemic disorders)• To exogenous Antigens To exogenous Antigens (eg Poststrep., (eg Poststrep.,
drug-related)drug-related)
• To endogenous Antigens (eg SLE)To endogenous Antigens (eg SLE)
1313

CLASSIFICATIONCLASSIFICATION
WHOWHODistribution Distribution
When many glomeruli are involved.When many glomeruli are involved.• Focal – affecting some glomeruliFocal – affecting some glomeruli• Diffuse – most glomeruliDiffuse – most glomeruli
When single glomeruli is consideredWhen single glomeruli is considered• Segmental – involving parts of glomerulusSegmental – involving parts of glomerulus• Global – involving entire glomerulusGlobal – involving entire glomerulus
1414

1515

AGENTS INVOLVED IN RENAL AGENTS INVOLVED IN RENAL GLOMERULAR DISEASESGLOMERULAR DISEASES
1. Infectious and Post Infectious (Bacteria, 1. Infectious and Post Infectious (Bacteria, Viruses, Spirochetes, Protozoa, Parasites, ? Viruses, Spirochetes, Protozoa, Parasites, ? Fungi)Fungi)
2. Tissue Antigens (DNA, RNA)2. Tissue Antigens (DNA, RNA)3. Intravascular Coagulation3. Intravascular Coagulation4. Chemical Agents 4. Chemical Agents 5. Physical Agents5. Physical Agents6. Mechanical Factors6. Mechanical Factors7. Metabolic7. Metabolic8. Genetic8. Genetic
1616

Immune Mechanism of Glomerular InjuryImmune Mechanism of Glomerular Injury1.1. Antibody- Mediated InjuryAntibody- Mediated InjuryIn situ immune complex DepositionIn situ immune complex Deposition
Fixed intrinsic tissue antigensFixed intrinsic tissue antigensNC1 domain of collagen Type IV antigen ( anti-GBM induced NC1 domain of collagen Type IV antigen ( anti-GBM induced nephritis)nephritis)Heymann antigen ( membranous glomerulopathy)Heymann antigen ( membranous glomerulopathy)Mesangial antigensMesangial antigensothersothers
Planted antigensPlanted antigensEndogenous antigens (e.g DNA, nulcear proteins, Ig, Endogenous antigens (e.g DNA, nulcear proteins, Ig, immmune complexes, IgA)immmune complexes, IgA)Exogenous antigens (e.g infectious agents, drugs)Exogenous antigens (e.g infectious agents, drugs)
1717

Anti-GBM Antibody- Induced NephritisAnti-GBM Antibody- Induced Nephritis
1818

HEYMANN-MODELHEYMANN-MODEL
Experimental GN (Rats)Experimental GN (Rats)
Induced in rats by injection of an antigen Induced in rats by injection of an antigen preparation (megalin/LDLP) derived from preparation (megalin/LDLP) derived from tubular brush borders. The rats develop tubular brush borders. The rats develop antibodies to this antigen and antibodies to this antigen and membranous GP resembling human MGP, membranous GP resembling human MGP, subepithelial granular deposits.subepithelial granular deposits.
1919

2020

2121

Immune Mechanism of Glomerular InjuryImmune Mechanism of Glomerular Injury1.1. Antibody- Mediated InjuryAntibody- Mediated Injury
In situ immune complex DepositionIn situ immune complex Deposition
Circulating Immune Complex DepositionCirculating Immune Complex Deposition
Endogenous antigens (e.g DNA, tumour antigens)Endogenous antigens (e.g DNA, tumour antigens)
Exogenous antigens (e.g infectious products)Exogenous antigens (e.g infectious products)
2.2. Cytotoxic Antibodies to glomerular cellsCytotoxic Antibodies to glomerular cells
3.3. Cell mediated ImmunityCell mediated Immunity
4.4. Activation of Alternate Pathway of complementActivation of Alternate Pathway of complement
2222

Mediators of Glomerular InjuryMediators of Glomerular Injury
Cells- Neutrophils, Monocytes,T-cell, NK cells, Platelets, Cells- Neutrophils, Monocytes,T-cell, NK cells, Platelets, Resident glomerular cells- especially mesangial cellsResident glomerular cells- especially mesangial cellsSoluble mediators-Soluble mediators-
1.1. Complement- C5b-C9, also stimulate mesangial cellsComplement- C5b-C9, also stimulate mesangial cells2.2. Ecosanoids, NO, angiotensin and endothelin- involved in Ecosanoids, NO, angiotensin and endothelin- involved in
haemodynamic changeshaemodynamic changes3.3. Cytokines- IL1, TNFCytokines- IL1, TNF4.4. Chemokines and growth factors- PDGF- involved in Chemokines and growth factors- PDGF- involved in
msangial proliferation and TGF-msangial proliferation and TGF-ββ and FGF are critical for and FGF are critical for ECM deposition and glomerulosclerosis in chronic injuryECM deposition and glomerulosclerosis in chronic injury
5.5. Coagulation system- Fibrin leak serve as stimulus for the Coagulation system- Fibrin leak serve as stimulus for the formation of crescentsformation of crescents
2323

2424

MORPHOLOGYMORPHOLOGY
HYPERCELLULARITY (cellular HYPERCELLULARITY (cellular proliferation, inflammation)proliferation, inflammation)
BASEMENT MEMBRANE THICKENING BASEMENT MEMBRANE THICKENING (BM proper, IC deposits)(BM proper, IC deposits)
HYALINIZATION (BM, protein, HYALINIZATION (BM, protein, mesangial matrix)mesangial matrix)
SCLEROSIS (loss of structure)SCLEROSIS (loss of structure)2525

Mechanism of Progression- FSGS- Mechanism of Progression- FSGS- Renal ablationRenal ablation
2626

FACTORS AFFECTING FACTORS AFFECTING LOCALIZATIONLOCALIZATION
Size and chargesSize and charges
ChargeCharge Highly cationic tend to cross the BM to Highly cationic tend to cross the BM to
subepithsubepith Highly anionic molecules are located Highly anionic molecules are located
subendothelially/non-nephrogenic.subendothelially/non-nephrogenic. Neutral charge accumulates in the Neutral charge accumulates in the
mesangium.mesangium.
2727

IMMUNE DEPOSITSIMMUNE DEPOSITS
SUBEPITHELIALSUBEPITHELIAL (DPGN, MPGN1, (DPGN, MPGN1, SLE, Memb)SLE, Memb)
ANTI-GBMANTI-GBM (GPS) (GPS)
SUBENDOTHELIALSUBENDOTHELIAL (SLE, MPGN1, (SLE, MPGN1, cryo, HUS)cryo, HUS)
INTRAMEMBRANOUSINTRAMEMBRANOUS (MPGN2, late (MPGN2, late Memb)Memb)
MESANGIALMESANGIAL (IgA, IgM, SLE, MPGN2) (IgA, IgM, SLE, MPGN2) 2828

GlomerulonephritisGlomerulonephritis
Acute- Is characterised by inflammatory Acute- Is characterised by inflammatory alterations in the glomeruli and clinically alterations in the glomeruli and clinically by syndrome of acute nephritisby syndrome of acute nephritis
2929

GLOMERULOPATHIES- GLOMERULOPATHIES- PrimaryPrimary
Acute diffuse proliferative GNAcute diffuse proliferative GN1.1. PoststreptococcalPoststreptococcal2.2. Non –post streptococcalNon –post streptococcal
Rapidly progressive (crescentic) GNRapidly progressive (crescentic) GNMembranous glomerulopathyMembranous glomerulopathyMinimal change diseaseMinimal change diseaseMembrano-proliferative GNMembrano-proliferative GNFocal segmental glomerulosclerosisFocal segmental glomerulosclerosisIgA NephropathyIgA NephropathyChronic glomerulonephitisChronic glomerulonephitis
3030

Nil Disease (lipoid nephrosis, Nil Disease (lipoid nephrosis, minimal change minimal change
glomerulonephropathy)glomerulonephropathy)Characterized by Characterized by
Acute nephrotic syndrome on presentationAcute nephrotic syndrome on presentation
Normal renal functionNormal renal function• ATN if present must be related to Rx (diuretics or NSAID Rx)ATN if present must be related to Rx (diuretics or NSAID Rx)
Hypertension – typically absentHypertension – typically absent
Haematuria – typically absentHaematuria – typically absent
Selective proteinuria in childrenSelective proteinuria in children
Good response to steroid RxGood response to steroid Rx
Excellent prognosisExcellent prognosis
3131

Minimal Change DiseaseMinimal Change Disease
LM: few if any changes (other than LM: few if any changes (other than changes secondary to proteinuria changes secondary to proteinuria ( swollen visceral epithelial cells)( swollen visceral epithelial cells)IF: usually negative; may have mesangial IF: usually negative; may have mesangial IgMIgMEM: only “fusion” of foot processes, other EM: only “fusion” of foot processes, other nonspecific changesnonspecific changesCourse: 85% responsive to steroidsCourse: 85% responsive to steroids
3232

This is minimal change disease (MCD) which is characterized by This is minimal change disease (MCD) which is characterized by effacement of the epithelial cell (podocyte) foot processes and loss of effacement of the epithelial cell (podocyte) foot processes and loss of the normal charge barrier such that albumin selectively leaks out and the normal charge barrier such that albumin selectively leaks out and
proteinuria ensues. By light microscopy, the glomerulus is normalproteinuria ensues. By light microscopy, the glomerulus is normal
3333

Focal Segmental Focal Segmental GlomerulosclerosisGlomerulosclerosis
Although similar to MCD it differs in many important respects. It is more Although similar to MCD it differs in many important respects. It is more likely to:likely to:Have HaematuriaHave HaematuriaHave hypertension, HGFR, Non-selective ProteinuriaHave hypertension, HGFR, Non-selective ProteinuriaExhibit poor response to steroid Rx.Exhibit poor response to steroid Rx.Progress to ESRD in 10yrs in 50% of cases, rate is increased to Progress to ESRD in 10yrs in 50% of cases, rate is increased to 70% if initial presentation is NS.70% if initial presentation is NS.SCD, Obesity, Congenital 19q13SCD, Obesity, Congenital 19q13Primary/Secondary – HIV, Heroin/Reflux Nep.Primary/Secondary – HIV, Heroin/Reflux Nep.Focal/SegmentalFocal/SegmentalPathological lesion is sclerosis/Fibrosis e.g. glomerulusPathological lesion is sclerosis/Fibrosis e.g. glomerulusHyalinization of the feeding arteriolesHyalinization of the feeding arteriolesEarly lesion show a mesangial matrix and mesengial Early lesion show a mesangial matrix and mesengial hypercellularity.hypercellularity.
3434

3535

Focal Segmental Focal Segmental Glomerulonephropathy (focal Glomerulonephropathy (focal
sclerosis)sclerosis)LM: some glomeruli (esp. juxtamedullary ones) LM: some glomeruli (esp. juxtamedullary ones) with segmental sclerosis (mesangial matrix with segmental sclerosis (mesangial matrix material, collapse, basement membrane-like material, collapse, basement membrane-like material) hyalinosismaterial) hyalinosisIF: Usually negative except in sclerotic segment IF: Usually negative except in sclerotic segment which may have Ig M, C3.which may have Ig M, C3.EM: Just accumulation of matrix-like material in EM: Just accumulation of matrix-like material in collapse loops collapse loops Course: 15% responsive to steroids; over 1/3 Course: 15% responsive to steroids; over 1/3 progress to end stage renal disease.progress to end stage renal disease.
3636

This is focal segmental glomerulosclerosis (FSGS). An area of collagenous This is focal segmental glomerulosclerosis (FSGS). An area of collagenous sclerosis runs across the middle of this glomerulus. In contrast to minimal sclerosis runs across the middle of this glomerulus. In contrast to minimal change disease, patients with FSGS are more likely to have non-selective change disease, patients with FSGS are more likely to have non-selective
proteinuria, hematuria, progression to chronic renal failure, and poor response proteinuria, hematuria, progression to chronic renal failure, and poor response
to corticosteroid therapy.to corticosteroid therapy.
3737

This trichrome stain of a glomerulus in a patient with focal segmental This trichrome stain of a glomerulus in a patient with focal segmental glomerulosclerosis (FSGS) demonstrates blue collagen deposition. glomerulosclerosis (FSGS) demonstrates blue collagen deposition. FSGS accounts for about a sixth of cases of nephrotic syndrome in FSGS accounts for about a sixth of cases of nephrotic syndrome in
adults and children.adults and children.
3838

Membranous GNMembranous GN
Usually presents as NS in adultsUsually presents as NS in adultsProteinuria is non-selectiveProteinuria is non-selectiveAssoc. with higher incidence of renal vein thrombosis Assoc. with higher incidence of renal vein thrombosis than any other cause of NS.than any other cause of NS.
Macro haematuria rare but micro haematuria is Macro haematuria rare but micro haematuria is commoncommonA cause may be readily found – SLE, Hepatitis, A cause may be readily found – SLE, Hepatitis, Malaria, Neoplasm (in elderly) of lungs, bowel, Malaria, Neoplasm (in elderly) of lungs, bowel, drugs.drugs.Relatively high spontaneous remission in Relatively high spontaneous remission in idiopathic formidiopathic formEffective Rx is controversial though steroids & Effective Rx is controversial though steroids & cytotoxic drugs have been tried.cytotoxic drugs have been tried.
3939

Membranous Membranous GlomerulonephropathyGlomerulonephropathy
LM: Normal to extreme diffuse thichkening of the LM: Normal to extreme diffuse thichkening of the capillary wall “tuft hypercellularity, foam cells in capillary wall “tuft hypercellularity, foam cells in interstitium”interstitium”
IF: Finely granular diffuse capillary wall staining IF: Finely granular diffuse capillary wall staining – IgG, C3.– IgG, C3.
EM: Numerous subepithelial deposits, spikes of EM: Numerous subepithelial deposits, spikes of GBM between capillariesGBM between capillaries
Course: 1/3 progress, 1/3 remit, 1/3 proteinuria Course: 1/3 progress, 1/3 remit, 1/3 proteinuria only.only.
4040

4141

Here is the light microscopic appearance of membranous Here is the light microscopic appearance of membranous glomerulonephritis in which the capillary loops are thickened and glomerulonephritis in which the capillary loops are thickened and
prominent, but the cellularity is not increased. Membranous GN is the prominent, but the cellularity is not increased. Membranous GN is the
most common cause for nephrotic syndrome in adults.most common cause for nephrotic syndrome in adults.
4242

A silver stain of the glomerulus highlights the proteinaceous basement A silver stain of the glomerulus highlights the proteinaceous basement membranes in black. There are characteristic "spikes" seen with membranes in black. There are characteristic "spikes" seen with
membranous glomerulonephritis seen here in which the black membranous glomerulonephritis seen here in which the black basement membrane material appears as projections around the basement membrane material appears as projections around the
capillary loopscapillary loops
4343

Membranous glomerulonephritis is an immunologically mediated Membranous glomerulonephritis is an immunologically mediated disease in which deposits of mainly IgG and complement collect in the disease in which deposits of mainly IgG and complement collect in the
basement membrane and appear in a diffuse granular pattern by basement membrane and appear in a diffuse granular pattern by
immunofluorescence, as seen here.immunofluorescence, as seen here.
4444

Diffuse Mesangial Proliferative Diffuse Mesangial Proliferative GNGN
Ig A nephropathy is the prototype of this Ig A nephropathy is the prototype of this histopathological variant.histopathological variant.Recurrent macro haematuria – characteristic Recurrent macro haematuria – characteristic presentation; often assoc. with URT inf. presentation; often assoc. with URT inf. (haematuria occurs at the peak of the illness)(haematuria occurs at the peak of the illness)
Other presenting syndromes include:Other presenting syndromes include:Chronic GNChronic GNRPGNRPGNARFARFDysuria with loin pain (may confuse with haem cystitis)Dysuria with loin pain (may confuse with haem cystitis)
4545

Diffuse Mesangial Proliferative GN Diffuse Mesangial Proliferative GN (Contd)(Contd)
Other findings include:Other findings include:
Proteinuria – usually mild < 1gm/dayProteinuria – usually mild < 1gm/day
Elevated plasma Ig A in up to 50% of casesElevated plasma Ig A in up to 50% of cases
Pericapillary depo of Ig A and C3 on skin biopsyPericapillary depo of Ig A and C3 on skin biopsy
Clinical indicators of poor prognosis include:Clinical indicators of poor prognosis include:Decrease GFR at presentationDecrease GFR at presentation
Persistent heavy proteinuriaPersistent heavy proteinuria
Persistent heavy haematuriaPersistent heavy haematuria
Severe hypertensionSevere hypertension
4646

Diffuse Mesangial Hypercellularity Diffuse Mesangial Hypercellularity in Nephrotic Syndromein Nephrotic Syndrome
LM: 3 or more cells in a mesangial region LM: 3 or more cells in a mesangial region in a thin section away from the vascular in a thin section away from the vascular polepole
IF:IF: IgM in mesangial regionsIgM in mesangial regions
EM: mesangial depositsEM: mesangial deposits? Part of nil disease? Part of nil disease
? Relationship to IgM nephropathy? Relationship to IgM nephropathy
4747

Diffuse Proliferative GNDiffuse Proliferative GN
Poststrep GN is the prototype and is one of the Poststrep GN is the prototype and is one of the few cases where the cause, clinical and few cases where the cause, clinical and pathological features correlates sufficiently to pathological features correlates sufficiently to justify labelling the disease by aetiology.justify labelling the disease by aetiology.
Diffuse Post-infectious GN (Post-streptococcal GN)Diffuse Post-infectious GN (Post-streptococcal GN)LM:LM: Proliferative, exudative (PMNs) “ cresentsProliferative, exudative (PMNs) “ cresentsIF:IF: Granular lumpy-bumpy cap, wall-IgG C3Granular lumpy-bumpy cap, wall-IgG C3EM:EM: Subepithelial humps, small Subepithelial humps, small
subendothelial/mesangial depositssubendothelial/mesangial depositsCourse:Course: Resolves in vast majority of cases.Resolves in vast majority of cases.DX:DX: ASO up, complement down, nephritic syndrome, ASO up, complement down, nephritic syndrome,
hypertensionhypertension
4848

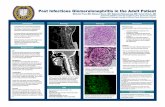
This glomerulus is hypercellular and capillary loops are poorly defined. This glomerulus is hypercellular and capillary loops are poorly defined. This is a type of proliferative glomerulonephritis known as post-This is a type of proliferative glomerulonephritis known as post-
streptococcal glomerulonephritis.streptococcal glomerulonephritis.
4949

Post-streptococcal glomerulonephritis is immunologically mediated, Post-streptococcal glomerulonephritis is immunologically mediated, and the immune deposits are distributed in the capillary loops in a and the immune deposits are distributed in the capillary loops in a
granular, bumpy pattern because of the focal nature of the deposition granular, bumpy pattern because of the focal nature of the deposition
process.process.
5050

Membranoproliferative GNMembranoproliferative GN
Clinical presentationClinical presentationNS – with significant haematuria, hypertension NS – with significant haematuria, hypertension and impaired renal functionand impaired renal functionAcute Nephritis or combination with NSAcute Nephritis or combination with NSChronic proteinuria & haematuriaChronic proteinuria & haematuria
110 0 MPGN- Type 1 and Type 2( dense-deposit MPGN- Type 1 and Type 2( dense-deposit disease)disease)
Persistently depressed plasma C3Persistently depressed plasma C3Circ. C3-nephritic factor (Ig G ab to C3-convertase)Circ. C3-nephritic factor (Ig G ab to C3-convertase)
10yr renal survival for Type 1 is 40% with 10yr renal survival for Type 1 is 40% with nephrosis and even worse for Type 2nephrosis and even worse for Type 2
5151

Membranoproliferative GN, Type 1 Membranoproliferative GN, Type 1 (mesangiocapillary GN)(mesangiocapillary GN)
LM:LM: Proliferative, PMNs, lobulation, tram-Proliferative, PMNs, lobulation, tram-trackingtracking
IF:IF: Broad capillary wall deposits – C3 is Broad capillary wall deposits – C3 is deposited in a granular pattern. C1q and C4 deposited in a granular pattern. C1q and C4 are also depositedare also deposited
EM:EM: Massive subendothelial electron dense Massive subendothelial electron dense deposits, mesangial deposits may be presentdeposits, mesangial deposits may be present
Course: progressive (many to renal failure)Course: progressive (many to renal failure)DX:DX: low complement, nephritic and/or low complement, nephritic and/or
nephrotic syndrome.nephrotic syndrome.
5252

Membranoproliferative GN Type II Membranoproliferative GN Type II (Dense Deposit Disease)(Dense Deposit Disease)
LM:LM: any glomerular pattern (membranous, any glomerular pattern (membranous, membranoproliferative, normal, crescentic GN, membranoproliferative, normal, crescentic GN, etc.)etc.)
IF: Broad capillary wall deposits – C3 is present in IF: Broad capillary wall deposits – C3 is present in irregular or linear foci in the BM on either side irregular or linear foci in the BM on either side but not in the dense deposits, but not in the dense deposits,
EM:EM: large electron dense in the GBM proper.large electron dense in the GBM proper.
Course:progressive (many to renal failure)Course:progressive (many to renal failure)
DX:DX: low complement (persistent), low complement (persistent), nephritic/nephrotic.nephritic/nephrotic.
5353

This is membranoproliferative glomerulonephritis (MPGN). This is membranoproliferative glomerulonephritis (MPGN). As seen here, the glomerulus has increased overall As seen here, the glomerulus has increased overall
cellularity, mainly mesangial. cellularity, mainly mesangial.
5454

This silver stain demonstrates a double contour to many basement This silver stain demonstrates a double contour to many basement membranes, or the "tram-tracking" that is characteristic of membranes, or the "tram-tracking" that is characteristic of
membranoproliferative glomerulonephritis (MPGN) type I that results membranoproliferative glomerulonephritis (MPGN) type I that results from basement membrane reduplication. from basement membrane reduplication.
5555

Diffuse Crescentic GNDiffuse Crescentic GN
Associated withAssociated with
Rapidly deteriorating renal functionRapidly deteriorating renal function
Macroscopic haematuriaMacroscopic haematuria
Proteinuria – usually >1g/dayProteinuria – usually >1g/day
Hypertension is often absent.Hypertension is often absent.
Profound oligo-anuria means damage is irrev.Profound oligo-anuria means damage is irrev.
Systemic dis. in 30-50%, Goodpasture’s, SLE or Systemic dis. in 30-50%, Goodpasture’s, SLE or necrotizing vasculitis.necrotizing vasculitis.
5656

IMMUNOPATHOLOGIC CLASSIFICATION OF IMMUNOPATHOLOGIC CLASSIFICATION OF CRESCENTIC GLOMERULONEPHRITISCRESCENTIC GLOMERULONEPHRITIS
I. I. Crescentic GN with granular immune depositsCrescentic GN with granular immune deposits ~ ~ 40%40%> 3/4 with well-defined clinical disorders> 3/4 with well-defined clinical disorders
(e.g., SLE, postinfectious)(e.g., SLE, postinfectious)< 1/4 apparently idiopathic< 1/4 apparently idiopathic (50% of these have small deposits)(50% of these have small deposits)
II. II. Crescentic GN with Anti-GBM antibodiesCrescentic GN with Anti-GBM antibodies ~ ~ 5%5%> 2/3 with pulmonary hemorrhage> 2/3 with pulmonary hemorrhage< 1/3 without pulmonary hemorrhage< 1/3 without pulmonary hemorrhage
III. III. Crescentic GN without “significant” glomerularCrescentic GN without “significant” glomerular deposits deposits ~ 55%~ 55%
5757

Crescentic GN (Rapidly Crescentic GN (Rapidly Progressive GN)Progressive GN)
LM:Over 50% of glomeruli with crescents, LM:Over 50% of glomeruli with crescents, hypercellularity.hypercellularity.IF: 1/3 granular (immune complex GN, e.g. IF: 1/3 granular (immune complex GN, e.g. SLE, SLE, postinfectious)postinfectious)
1/3 linear (probably anti-GBM) (Goodpasture’s 1/3 linear (probably anti-GBM) (Goodpasture’s disease)disease)
1/3 no deposits (e.g., polyarteritis, Wegener’s, 1/3 no deposits (e.g., polyarteritis, Wegener’s, vasculitisvasculitis
EM: either glomerular deposits anywhere (immune EM: either glomerular deposits anywhere (immune complex) or no deposits (either anti-GBM or no deposit complex) or no deposits (either anti-GBM or no deposit disease)disease)Course: Terrible (progression to end stage renal disease, Course: Terrible (progression to end stage renal disease, except post infectious)except post infectious)DX:DX: anti-GBM antibodies in serum (radioimmunoassay)anti-GBM antibodies in serum (radioimmunoassay)
5858

Seen here within the glomeruli are crescents composed of proliferating Seen here within the glomeruli are crescents composed of proliferating epithelial cells. Crescentic glomerulonephritis is also known as rapidly epithelial cells. Crescentic glomerulonephritis is also known as rapidly
progressive glomerulonephritis (RPGN) progressive glomerulonephritis (RPGN)
5959

This immunofluorescence micrograph of a glomerulus demonstrates This immunofluorescence micrograph of a glomerulus demonstrates positivity with antibody to fibrinogen. With a rapidly progressive GN, the positivity with antibody to fibrinogen. With a rapidly progressive GN, the
glomerular damage is so severe that fibrinogen leaks into Bowman's glomerular damage is so severe that fibrinogen leaks into Bowman's space, leading to proliferation of the epithelial cells and formation of a space, leading to proliferation of the epithelial cells and formation of a
crescent.crescent.
6060

6161

IgA Nephropathy (Berger’s IgA Nephropathy (Berger’s Disease)Disease)
LM: any glomerular pattern (most normal to LM: any glomerular pattern (most normal to focal GN)focal GN)EM: always mesangial depositsEM: always mesangial deposits
Peripheral capillary wall deposit unusualPeripheral capillary wall deposit unusual
IF: Mesangial granular IgA by definition (in IF: Mesangial granular IgA by definition (in absence of SLE, HSP, active liver disease)absence of SLE, HSP, active liver disease)
Prognosis: 2%/year to end stage renal Prognosis: 2%/year to end stage renal diseasedisease
?relationship to Henoch-Schonlein ?relationship to Henoch-Schonlein purpura poorly understood.purpura poorly understood.
6262

LIGHT MICROSCOPIC CHANGES IN IGA LIGHT MICROSCOPIC CHANGES IN IGA NEPHROPATHY: GLOMERULARNEPHROPATHY: GLOMERULAR
1)1) Normal or essentially normal glomeruliNormal or essentially normal glomeruli
2)2) Focal/segmental mesangial Focal/segmental mesangial hypercellularityhypercellularity
3)3) Diffuse mesangial hypercellularityDiffuse mesangial hypercellularity
4)4) Focal glomerulonephritisFocal glomerulonephritis
6363

IgA NEPHROPATHY- Mesangial IgA IgA NEPHROPATHY- Mesangial IgA depositsdeposits
6464

CHRONIC CHRONIC GLOMERULONEPHRITISGLOMERULONEPHRITIS
End stage glomerular disease by various End stage glomerular disease by various specific types of GN.specific types of GN.Post streptococcal (1-2%)Post streptococcal (1-2%)RPGN(90), RPGN(90), MGN(30-60%)MGN(30-60%)FSGS(50-80%)FSGS(50-80%)MPGN(50%)MPGN(50%)IgA(30-50%) and others IgA(30-50%) and others
6565

Morphology- (CGN)Morphology- (CGN)
Kidneys are symmetrically contracted Kidneys are symmetrically contracted diffuse granular cortex. diffuse granular cortex. Thin cortex with increase in perinephric fat.Thin cortex with increase in perinephric fat.MG/MPGN, MG/MPGN, Hyaline obliteration of glomeruli/acellular eosinophilic Hyaline obliteration of glomeruli/acellular eosinophilic masses (proteins, matrix, BM-like material and masses (proteins, matrix, BM-like material and collagen).collagen).Arterial and arteriolar sclerosis. Arterial and arteriolar sclerosis. Tubular atrophy, Tubular atrophy, interstitial fibrosis, interstitial fibrosis, mononuclear leucocytic infiltration of intersitium.mononuclear leucocytic infiltration of intersitium.
6666

The microscopic appearance of the "end stage kidney" is similar The microscopic appearance of the "end stage kidney" is similar regardless of cause, which is why a biopsy in a patient with chronic regardless of cause, which is why a biopsy in a patient with chronic renal failure yields little useful information. The cortex is fibrotic, the renal failure yields little useful information. The cortex is fibrotic, the glomeruli are sclerotic, there are scattered chronic inflammatory cell glomeruli are sclerotic, there are scattered chronic inflammatory cell
infiltrates, and the arteries are thickened. infiltrates, and the arteries are thickened.
6767