Garnering the for Teaching - New Jersey Medical...
44
University of Medicine & Dentistry of New Jersey Volume 4 Number 1 Summer 2006 BIKE RIDE FOR GLOBAL HEALTH ANATOMY RECONFIGURED ALUMNI NEWS AND FEATURES Gold for Teaching Garnering the
Transcript of Garnering the for Teaching - New Jersey Medical...

U n i v e r s i t y o f M e d i c i n e & D e n t i s t r y o f N e w J e r s e y
Volume 4 Number 1 Summer 2006
BIKE RIDE FOR GLOBAL HEALTH ANATOMY RECONFIGURED ALUMNI NEWS AND FEATURES
Goldfor Teaching
Garnering the

THE movement inherent in an academic setting propels all
of us—faculty, students and staff—along each day, each
week, each month until, believe it or not, another year has
passed. One class of students reaches an incredible milestone
while another prepares to begin the journey. I hope you’ll enjoy
reading about the Class of 2006 Convocation during which the
renowned pediatric neurosurgeon Dr. Benjamin Carson
addressed the class with a rather moving speech.
This issue of Pulse spotlights a number of our faculty who
have moved their students in many ways, enough to garner the
coveted Golden Apple Award for Excellence in Teaching. One
has even implemented a novel method of teaching anatomy that
has been documented to improve how students learn.
We’ve also profiled a selection of students whose dedication to
humanism moved their fellow peers and professors to nominate them to the Gold Humanism Honor Society.
Our researchers are moving forward in many areas as well—we document some of their discoveries in brain
repair, sepsis and tuberculosis in this issue.
And to play out the theme of motion quite literally, you’ll also read about an NJMS student who rode his
bicycle 3,700 miles across the country to raise money for and awareness of global health issues.
I trust you’ll find this a “moving” issue of Pulse magazine.
In Health,
Robert L. Johnson, MD, FAAPThe Sharon and Joseph L. Muscarelle Endowed Dean (Interim)
Interim DeanUMDNJ–New Jersey MedicalSchoolRobert L. Johnson, MD
DirectorUniversity MarketingCommunicationsBarbara Hurley
DirectorMarketing and CommunicationsNew Jersey Medical SchoolMelissa Campbell
Senior Editor, NJMS PulseEve Jacobs
PresidentNJMS Alumni Associationand AlumniFocus EditorJoseph V. DiTrolio, MD
AlumniFocus CoordinatorDianne Mink
Contributing WritersMaryann Brinley Jill SpotzJim Fausto
DesignSherer Graphic Design
Message from the Dean
pulse VOLUME 4 NUMBER 1 SUMMER 2006 UNIVERSITY OF MEDICINE & DENTISTRY OF NEW JERSEY
Keep In Touch…NJMS Pulse is published twice each year by UMDNJ–New Jersey Medical School (NJMS). We welcome let-ters to the editor and suggestions for future articles.
Send all correspondence to:Pulse EditorOffice of University Marketing CommunicationsUniversity Heights –P.O. Box 1709, Room 132865 Bergen StreetNewark, NJ 07101–1709or via email to [email protected]
PHOTO: JOHN EMERSON

Cover photo by John Emerson
INSIDE INFORMATION
2 Convocation 20064 Seeds of Change4 NJMS Autism Center Benefit5 A Match Work Quilt5 Cultural Competency Summit6 NJ Nets Team Up to Fight Asthma
NEW AND NOTABLE
7 Med Students Embrace Humanism11 Happy Anniversary
PEOPLE IN THE NEWS
12 Bike Ride for Global Health14 NJMS Student Pursues Research at NIH14 Accolades15 A Large Step Forward for Tuberculosis Research
FEATURES
16 Leaders, Role Models, Mentors and MoreEach year NJMS students award their most exceptional teachers Golden Apples. Meet some of the faculty who earnedthe highest marks from their toughest critics.
24 Anatomy ReconfiguredThis first-year medical school course has traditionally been anightmare for future doctors…that is until one inspired teacherdecided to forever change the experience at NJMS.
28 All the Right MovesThey came through the night—from Manhattan to Newark—with 61 years of stored pathogens in tow. Now, five years later,PHRI officially joins hands with the medical school.
VOICES
32 Physicians With Disabilities: Why Aren’t There More of Them?
ALUMNI FOCUS
34 News of special interest to NJMS graduates
ALUMNI PROFILE
36 Beyond the Black BagFor alum Deborah Bessen, making house calls is no old-fashioned notion.
FOCUS ON PHILANTHROPY
40 Gift Provides Food for Thought40 Brotherly Love
pulse
Summer 2006
12
36
24
2

2 P U L S E S U M M E R 2 0 0 6
I N S I D E I N F O R M AT I O N
PHOTOS: PETER BYRON
1
2
3
4

UMDNJ’s Interim President BruceVladeck, PhD, congratulated the class of2006 for setting a standard that willensure success not only for the graduatesbut for the school and University aswell. He remarked that the Universitywould thrive because of the energy,commitment and talent of the peopleassociated with it.
A number of those people—includ-ing students, faculty and communityleaders—were honored during the cere-mony with awards recognizing excel-lence in teaching, academic excellence,commitment to humanism, and serviceto others.
Benjamin Carson, MD, professor anddirector for pediatric neurosurgery atJohns Hopkins Medical Institutions,then delivered the keynote address,reflecting on the early challenges of hislife, the joys of a humanistic approach tomedicine, and the power of expectations.
“When I was in the fifth grade, Ithought I was stupid, so I conducted
myself like a stupid person and achievedlike a stupid person. When I was in theseventh grade, I thought I was smart: Iconducted myself like a smart personand achieved like a smart person. Whatdoes that say about expectations andabout human potential? This is what wemust learn to develop.”
He then urged the graduates to fullydevelop their talents to become invalu-able to the people around them, but tonot abuse their sphere of influence. “Wecan encourage or discourage. Givinghope is a tremendous advantage, notonly in healing the body, but in healingthe spirit.”
During his address, Guy Manetti,Student Council President, elicited achuckle from the crowd as he recalledhis first test in medical school. It camein the form of a pop quiz from a fellowstudent. Question: What is the “coolest”joint in the body? Answer: The “hip”joint, of course.
But Manetti also passed on more seri-ous words of wisdom that his father leftwith him: Be proud of your achieve-ments, but also remember that life isnot just a matter of milestones, but ofmoments.
“Now that we have reached thisimportant achievement of graduatingfrom medical school, it will be temptingfor us to focus on our next milestone,”said Manetti. “However, it is themoments that we share with thosearound us that will continue to mold usas physicians. Enjoy the moments.”
Lisa Pompeo, MD, assistant profes-sor, Department of Obstetrics,Gynecology and Women’s Health, then led the students in reciting theHippocratic Oath before receiving theirdegrees. As the newest class of doctorsexited the hall, buoyed with hope,excitement and celebration, it was clearthey were truly living in the moment. �
N E W J E R S E Y M E D I C A L S C H O O L 3
N E W S A B O U T N J M S E V E N T S , F A C U LT Y, G R A N T S , R E S E A R C H A N D M O R E
2006NEW JERSEY MEDICAL SCHOOL’S 2006 Convocation, held at
the New Jersey Performing Arts Center in Newark on May 22,
proved a time of reflection, celebration and humor.
1. Students don caps and gowns.2. Dr. Benjamin Carson delivers the keynote
address.3. Dean Johnson congratulates Elena Perez on
receiving the Distinguished Citizen Award.4. Recessing students begin the next phase
of their journey.
SECTION COMPILED BY MELISSA CAMPBELL

Seeds of Change
PERHAPS the most critical aspect of medical science researchis translating findings so they are widely available to
those who can benefit. Making the leap from bench tobedside involves many factors, not the least of which isan interested investor and financial backing. A newventure capital company established by theFoundation of UMDNJ has been created to fillthose needs for researchers at UMDNJ. TheFoundation Venture Capital Group, LLC, willinvest $5 million over the next five years to fundearly stage research and development companiesthat have the potential to develop technologies thatwill change the future of healthcare.
The group will collaborate with the Officeof Patents and Licensing at UMDNJ toidentify the most promising research and provide greater support and opportuni-ties for newly formed start-up companies. The goal of the fund is to develop the
fledgling companies so that they are more attractive to larger investors.James M. Golubieski, president of Foundation Venture Capital Group, LLC,
says this forward-thinking concept can prove transformational for the Foundation ofUMDNJ, for researchers at the University by funding projects that might not ordi-narily receive support, and for patients who will be able to take advantage ofadvances resulting from this effort. �
4 P U L S E S U M M E R 2 0 0 6
A SPATE OF HEROINOVERDOSES inCamden, NJ, led health
officials at the NewJersey Poison Information
and Education System(NJPIES)—located at NJMS—to alert theCDC to an unusually strong form ofheroin containing fentanyl, a powerfulpainkiller many times stronger than mor-phine. The CDC, in turn, sent out anational alert. NJPIES is collecting andanalyzing information from emergencyroom personnel, which they hope willprovide police with helpful informationthat may prevent additional overdoses.
TO REFLECT a growing interna-tional effort to eradicate TB,the National TuberculosisCenter at UMDNJ-NewJersey Medical Schoolhas become the GlobalTuberculosis Institute. Lastyear, it received a $7.5 millionfederal grant over five years to fundone of four Regional Training andMedical Consultation Centers in the U.S.
RAISING money for autism couldn’t have tasted or sounded any better.
Eric Asimov, chief wine critic for TheNew York Times, and Steven Sacco,noted composer, along with the interna-tionally renowned American BrassQuintet, hosted a wine tasting andrecital on April 10 to benefit TheAutism Center of New Jersey MedicalSchool at UMDNJ. More than 115 peo-ple attended, helping to raise $25,000.
The event, titled “In Tune withAutism,” took place at Montclair StateUniversity’s Alexander Kasser Theaterand marked the world premiere ofSacco’s latest composition.
Guests enjoyed tasting eight “terrificunder twenty (dollars)” wines fromaround the world, particularly a 2004
Greek white, BoutariMoschofilero. The recital fea-tured a range of pieces includ-ing a set of 16th centuryVenetian works, a selection of19th century American bandmusic and two Sacco composi-tions . One piece was inspired bythe composer’s son and his experi-ence with autism spectrum disorder.
The event tied into an innovativeprogram developed by The AutismCenter of New Jersey Medical School,and funded by The Daniel JordanFiddle Foundation, called “MostlyMusic,” which offers parents and theirchildren with autism a night of dinnerand musical entertainment in a family-friendly and supportive atmosphere.
The Autism Centerof New Jersey MedicalSchool and Montclair
State University arecollaborators in theNew Jersey ArtHealth Initiative, a
project that facilitates,documents and demon-
strates the relationship betweenthe arts and health.
This collaboration aims to raiseawareness of the positive effects of thearts on the health of both individualsand communities from preventionthrough treatment. The goal is to devel-op programs and opportunities for indi-viduals with autism and their families toparticipate in the arts. �
NJMS Autism Center Benefit
I N S I D E I N F O R M AT I O N
TOP LEFT: JIM WEHTJE; TOP RIGHT: G. BRIAN KARAS; CENTER: CDC/ RONALD W. SMITHWICK; BOTTOM: MICHAEL DINGES

N E W J E R S E Y M E D I C A L S C H O O LPHOTOS: PETER BYRON; ILLUSTRATION: LISA ZADOR 5
CulturalCompetencySummitABOUT 50 UMDNJ physicians
attended New Jersey’s firstcredit-bearing continuing educationcultural competency conference onApril 24 in Princeton. The day-longsession entitled “Caring for NewJersey’s Multicultural Population: ACultural Competency Summit” wasorganized by Maria Soto-Greene,MD, vice dean, NJMS, andCatherine Bolder, UMDNJ associ-ate vice president, AA/EEO.Participants satisfied the mandate oflegislation passed in 2005 thatrequires the completion of culturalcompetency training as a conditionof licensure for medical profession-als. The law aims to end race- andgender-based disparities in the pro-vision of healthcare.
The conference was funded byThe Bildner Family Foundation–New Jersey Campus DiversityInitiative, the UMDNJ CulturalCompetency Project, the UMDNJOffice of Multicultural Affairs andthe NJMS Hispanic Center ofExcellence. �
AFTER learning where they would spend the next phase of their
medical education, students at NJMSplaced tiny toothpick flags on a map ofthe U.S., creating a “Match Work” quiltpattern across the country. Residenciesfor the 156 graduates began this summer.
Medical students across the countrylearned their fate on Match Day, March16, as white envelopes detailing theirassignments were handed out at the pre-scribed hour of noon. The match rate atNJMS was 99 percent this year, consid-erably higher than the national rate of93 percent.
About half of the NJMS grads arepursuing some type of primary caretraining in internal medicine, familypractice or pediatrics. Other popularspecialties include emergency medicine,obstetrics/gynecology, surgery and radi-ology. About one third of the studentswill remain in New Jersey and 26 ofthem will pursue residencies atUMDNJ-University Hospital.
Guy Manetti, student council presi-
dent, opted for an early match program, which did not diminish hisenjoyment of Match Day. He and several other early matchers set up beachchairs to reflect their relaxed state ofmind. One nice surprise for Manetti,who was accepted into Yale-New HavenMedical Center’s urology program, wasthat seven of his classmates will join him there. �
A Match Work Quilt
Claudia Mosquera learns that she hasmatched to the obstetrics and gynecology program at UMDNJ-University Hospital.

TOP: CDC / JAMES GATHANY; BOTTOM LEFT: COMSTOCK; BOTTOM RIGHT: ELENA MITCHELL6
I N S I D E I N F O R M AT I O N
A SYMPOSIUM on the Immunology ofInfectious Diseases on April
11 and 12 broughttogether researchersfrom the U.S. andCanada to discussrecent discoveries
regarding the regula-tion and function of the
immune response thatmay lead to new vaccines and
immunotherapies. William C. Gause,PhD, senior associate dean for researchand a noted expert in the field, andPadmini Salgame, PhD, NJMS professorof medicine, were the program directors.
RESEARCHERS AT NJMS have beenawarded a five-year, $8.1 million grantfrom the NIH’s National Institute ofGeneral Medical Sciences to investigategender differences in response to injuryand sepsis. The focus of their researchis the pathogenesis of multiple organfailure, the most common cause ofdeath in the intensive care unit, and whymen are more likely to succumb to mul-tiple organ failure. The principal investi-gator is Edwin A. Deitch, MD, professorand chair, Department of Surgery, highlyregarded for his work in abdominal, trau-ma, critical care and bloodless surgery.
A RECENT STUDY led by SteveLevison, PhD, professor, Department ofNeurosciences, indicates that the brainhas a broader capacity for repair thanpreviously thought. The team has identi-fied two stem cell receptors—EGFR andNotch1,gp-130—that are important tobrain regeneration following injury. If thebrain’s natural response could beenhanced, then these findings mayeventually be applicable to conditionssuch as cerebral palsy, multiple sclero-sis, stroke andtraumaticbrain injury.Study resultswere pub-lished in TheJournal ofNeurosciencein April.
NJ Nets Team Up toFight AsthmaJOUMANA Kidd and Ellen Carter,
wives of Nets basketball starsJason and Vince, respectively, haveinitiated a full court press to helpraise money for the Asthma Centerof Excellence at NJMS. The center-piece of their fundraising effort is at-shirt with the images of Vince andJason portrayed as “Fire and Ice” fortheir well-known playing styles. Theshirts debuted at the ContinentalAirlines Arena during the NBAplayoffs in April and proceeds willbenefit the asthma program at theschool. Sales of the shirts will con-tinue into next season.
According to Deborah Johnson,MD, FAAP, a pediatrician and theassociate dean for clinical enterpriseat NJMS, the dream of making adifference in the care of childrenwith asthma is now a reality thanksto the combined efforts and com-mitment of the Kidds, the Cartersand the Nets.
Asthma represents a serioushealth concern for children in NewJersey. A staggering 13 percent ofchildren under the age of 18 areaffected by asthma, according to theNew Jersey Department of Healthand Senior Services, with the major-ity of these children concentrated inurban areas.
Nationally, asthma accounts formore than 14.7 million missedschool days per year according tothe Centers for Disease Control.
This team effort will play animportant role in improving the dayto day lives of kids and their fami-lies—a slam dunk for everyoneaffected by asthma. �
Representatives from the Asthma Center of Excellence at NJMS and theFoundation of UMDNJ accept a checkfrom Joumana Kidd (center) during a Nets game.
P U L S E S U M M E R 2 0 0 6

N E W J E R S E Y M E D I C A L S C H O O LSTEPHANIE CARTER 7
N E W & N O TA B L E
Med Students Embrace
Humanism
U NDERSTANDING these words of medicine’s founding father
is not enough for students at NJMS, where acting on their
understanding is critical to becoming compassionate physicians.
This spring 34 students were recognized for their humanistic
actions by being inducted into the Gold Humanism Honor
Society. Sponsored by the Arnold P. Gold Foundation, the organi-
zation honors medical students, residents and physician-teachers who demonstrate excellence in clinical
care, leadership, compassion, scientific achievement and dedication to service.
Fourth-year students are nominated by their peers, faculty and residents, and are evaluated on their inter-
actions with patients, faculty, staff and fellow students, as well their academic and clinical experiences.
Two faculty members were also inducted—Lillian Pliner, MD, Department of Medicine, Division of
Hematology/Oncology, and Lisa Pompeo, MD, Department of Obstetrics, Gynecology and Women’s Health. The
evening’s keynote address was provided by Pliner, who said: “When I first became a physician, I thought my
biggest challenge would be keeping my skills and knowledge base up to date. Now I have come to find the real
challenge is working humanistically within systems that are often at odds with patients’ best interests.”
When Pompeo accepted her award, she told students that even though she is a teacher, she learns from
her students, and that she is a better teacher, physician and person because of her interactions with students.
Students conducted a service project entitled “Voices of University Hospital: Spending Time in a Patient’s
Shoes,” in which they interviewed patients about what they believe makes a good doctor. The new NJMS
members join colleagues from 49 other medical schools who have been inducted into the Gold Humanism
Honor Society since it was founded in 2001. A few profiles follow. —MELISSA CAMPBELL
“Wherever the art of medicine is loved,
there is also a love of humanity.”– HIPPOCRATES

PHOTOS: A. J. SUNDSTROM8
N E W & N O TA B L E
P U L S E S U M M E R 2 0 0 6
Beauty is Not Only Skin Deep
Richard Huggins
IN Ethiopia, leprosy sufferers whowere once socially isolated, stigma-
tized and feared, are now treated andcured with anaggressive multi-drug regimen. InHolland, individualsinflicted with vitili-go, who onceendured constantgawking and embar-rassment, now havetheir condition cor-rected through lasersurgery and skingrafting. Not manymedical studentsknow as much about these types of skindiseases as Richard Huggins, MD.Through his externships in Africa at theAll Africa Leprosy Center in AddisAbaba, Ethiopia, and in Holland at theNational Center for Blistering Disordersand the Netherlands Institute forPigment Disorders, Huggins witnessedfirst-hand the psychological effects ofthese conditions and how to treat them.
The Johns Hopkins University gradu-ate realized in his junior year of collegethat he enjoys working with people andhelping them. “I believe my personalityallows me to see things from anotherperson’s perspective, both professionallyand privately,” he explains. “I always tryto put myself in my patients’ shoes tobetter understand their problems.” Hiscompassion and understanding garneredhim a spot in the Gold HumanismHonor Society. Huggins mentored sev-eral teens in Newark, coaching them onhow to better their lives. One particularstudent from Malcolm X ElementarySchool is near to Huggins’ heart. Afterthree years of coaching him, the fifthgrader was recently promoted out of
special needs classes and is doing verywell. “His dedication to medical schooland to the community personifies thetype of physician he will become,”explains Lonnie Wright, director ofundergraduate and pre-matriculationprograms at NJMS, and the person
Huggins creditswith helping himchoose his careerpath.
Hugginsbecame interestedin dermatologyduring medicalschool—particu-larly pigment dis-orders like vitili-go, tuberous scle-rosis and sclero-derma. “Skin
issues are chronic and affect your bodyas well as your self esteem,” he explains.“This specialty allows me to counselpatients as well as treat them, which isvery rewarding.”
His externships have allowed Hugginsto learn about other cultures and thesimilarities and differences of treatingpatients in other countries. “It amazedme how much time is spent counselingpatients inHolland,” heexplains.“Physicians in thedermatology clinictake the time totalk to patients andhelp them throughthe emotionalaspects of dealingwith a disfiguringskin disorder.” Hiswork was partiallyfunded through anAmerican Academy of Dermatologyminority medical student mentor schol-arship, which offered Huggins theopportunity to be mentored by a foreign
dermatologist. He started his internshipthis summer at the State University ofNew York–Buffalo.
Of Music and Medicine
MarciaKlein-Patel
MARCIA Klein-Patel, MD, wasn’tsupposed to become a doctor. As
an accomplished concert pianist, sheplayed competitively before even enter-ing high school. It all started with anold piano and several piano books thather great aunt gave her when she was 2years old. Since her aunt was a pianoteacher, Klein-Patel received lessons andby age 3, could read music and playsimple songs. Her talent flourished andshe started competing while in grammarschool under the direction of a profes-sional piano teacher/coach. It wasn’tuntil her mentor suddenly passed awaythat she “hung up” her keys. “I justcouldn’t work with anyone else,” sheexplains.
Prior to entering Syracuse University,she slowly started playing again and was
accepted with adouble major—biology and music.“It was one of thefew schools thatwould admit mewith such a varieddouble major,” sheexplains. The work-load for both disci-plines was so sub-stantial that afterseveral semesters,she was forced to
drop one. She chose to follow throughwith biology. “I loved biology just asmuch as music and it was very difficultfor me to accept that I could not pursue
RICHARD HUGGINS
MARCIA KLEIN-PATEL

N E W J E R S E Y M E D I C A L S C H O O L 9
both. Eventually science won out.”When she looks back on her medical
school experience, she says she choseNew Jersey Medical School because “Ifit here. After my interview at NJMSand I knew I was accepted, I cancelledthe remaining interviews. I just knewthis was the right choice.” Klein-Patelwas offered a scholarship to attend theMD/PhD program and was one of threestudents who graduated with this dualdegree this year. She completed her PhDin 2004. Her research on the effects ofair pollutant particles on airway hostdefense was funded by the Environ-mental Protection Agency.
During her third year at NJMS,Klein-Patel chose to enter obstetricssince she thoroughly enjoyed her obstet-rics clinical rotation. She decided that ifshe liked her labor and delivery rotationjust as much, then it definitely was theright specialty for her.
Fast forward to the present. Klein-Patel started her residency in obstetricsand gynecology at Magee–Women’sHospital of the University of PittsburghMedical Center. She chose Mageebecause it is one of six national centersof excellence in women’s health and alsooffers her the opportunity to pursueresearch interests at the Magee Women’sResearch Institute. Her current researchis focused on subclinical infection inpregnancy. It’s a far cry from air pollu-tion but she rationalizes that “they areboth mucosal systems, therefore similar.”
This Resident Comes Full Circle
ClaudiaMosquera
WHO would you choose to haveby your side during a medical
emergency? When asked this very ques-tion, the majority of faculty, residents
and fourth year medical students fromNew Jersey Medical School choseClaudia Mosquera, MD, the extremelydedicated and energetic member of theclass of ’06.
Four years ago, as she donned herwhite lab coat for the first time duringthe annual WhiteCoat Ceremony,the excited andproud medicalstudent knew thatno matter howlong and difficultmedical schoolmight be, itwould all be worth it. She was right. In her fourth year,Mosquera wasinducted into theGold Humanism Honor Society for herdedication and compassion for patients.
Medical school was part ofMosquera’s “big plan” since she was 14years old. As a high school student, sheattended the Hispanic Center ofExcellence Summer Youth Program atNJMS. A family friend, Maria Soto-Greene, MD, vice dean of NJMS anddirector of the Hispanic Center ofExcellence, led this program. She recallsMosquera’s participation: “I am happyto see Claudia evolve from a teenager toa wonderful young woman who under-stands what it is to serve others.” Now,as Mosquera begins her residency inobstetrics and gynecology at UMDNJ-University Hospital, Soto-Greene cancall her a colleague.
Prior to entering NJMS, Mosqueralaunched her pre-doctoral career atBrown University, where she received aBA in biology. She chose obstetrics andgynecology because the field lends itselfto all areas of primary care, includingsurgery and women’s health. Mosquerasees this evolving speciality as a chal-
lenge for future physicians due to risinginsurance and healthcare costs butbelieves that patients will come toappreciate this field even more in thefuture. “Patients rely heavily on theirobstetrician-gynecologists to coordinatetheir primary care needs, which is creat-
ing a niche for thisspecialty in the pri-mary care field,”she explains.“Many womenonly go to theirOb/Gyn.” True toher humanisticside, Mosquerafeels that obstetricsand gynecologyalso offers her theability to formlong-lasting rela-tionships with her
patients and provide continuity of care,an option that is not as strongly presentin some other specialties.
When asked to describe her mostvivid memory of medical school,Mosquera recalls her first night on-callduring her Ob/Gyn clinical rotation: “A 30-year-old woman in her thirdtrimester of pregnancy was brought intolabor and delivery by EMS. Before Iknew it, she was rushed into the operat-ing room. I watched as the obstetriciansdelivered the baby and the pediatricianstried to resuscitate him. Unfortunatelythe baby died. I cannot explain howmuch my heart hurt for the mother asshe received the terrible news. It was anexperience that I will never forget.”
Mosquera feels that her training atNJMS could not have been better.“Given University Hospital’s designationas a Level 1 Trauma Center, and myexposure to a large variety of complexclinical scenarios, I could not be moreprepared to care for patients than I amright now,” she explains.
CLAUDIA MOSQUERA

10
N E W & N O TA B L E
P U L S E S U M M E R 2 0 0 6
The Art of Listening
Indroneil Mukerji
WITH a history of counselingthird-world orphans, college
freshmen and even classical musicians,Indroneil Mukerji, MD, can’t imagineanything more rewarding than helpingpatients discover their inner strength topersevere during a crisis. This callingprompted him to pursue a career in psy-chiatry and he started his residency thissummer at Long Island Jewish MedicalCenter. His four years will encompassinpatient and outpatient psychiatry,neurology, as well as general medicinework. “I excel at listening with empa-thy,” he explains. “During medicalschool my most satisfying clinicalencounters have been the ones where Ioften unknowingly played the role ofpsychiatrist.”
One of those most rewarding experi-ences involved Mukerji counseling a 72-year-old gentleman with advanced-stagegastric adenocarcinoma. “Although heknew that his body was failing, he exud-ed an almost tangible passion for life,”Mukerji recalls. “As I listened to himtalk about his fears of pain, death and ofbecoming a burden tohis family, I realizedthat although I couldnot save him, he feltbetter discussing hisissues with me.”
In addition to therewards of counselingothers, Mukerji wasdrawn to academicpsychiatry as he enjoysresearch and teaching.He feels fortunate tohave been guided byPranela Rameshwar, PhD, associate pro-fessor of medicine at NJMS. He workedin her lab for three years as a researchfellow and his group’s work on neuro-
blastoma, a child-hood cancer, waspublished in theJournal of Neuro-Oncology last year.
Mukerji’s eclec-tic list of personalaccomplishmentsincludes: travelingabroad toHonduras, wherehe worked in anorphanage; learn-ing to play the violin in the secondgrade, thanks to the prompting of hisgrandfather; and ballroom dancing,which he is still perfecting.
A Cut Above
Diego Reino
DIEGO Reino, MD, is looking for-ward to testing his surgical abili-
ties. The extremely personable and verydedicated New Jersey Medical Schoolgraduate began his surgical residency atUMDNJ–University Hospital (UH) thissummer. Though his five years of resi-dency at UH have just begun, Reino hit
the ground run-ning with thesame focus anddedication thathe applied to hisfour years ofmedical school.
GoldHumanismHonor Societyinductees arechosen for theirability to showcompassion,
empathy and respect for diversity,among other attributes. Reino under-stands the importance of these princi-ples and worked hard to meet them.
Involved in manyactivities and stu-dent groups such asthe Student NationalMedical Association,Boricua LatinoHispanicOrganization andthe Three DoctorsFoundation, he vol-unteered at healthscreenings and othercommunity events
to promote health awareness for minori-ty groups in the Newark area.
Reino credits his mentor—David H.Livingston, MD, the Wesley J. HoweProfessor and chief of trauma surgery atNJMS—for teaching him how to be anaccomplished surgeon and for “leadingby example.” As a first year student,Reino worked with Livingston on hisresearch on the impact of bone healingin trauma surgery. The experiencehelped shape his decision to choosetrauma surgery as his niche. UniversityHospital was also the perfect match forReino due to its Level 1 Trauma Centerstatus, as well as the vast number of crit-ical care cases and diverse population.
“As a physician, it is important toprovide care in an environment that fos-ters respect and dignity for the patient,”Reino says. “As Hippocrates states:‘Wherever the art of medicine is loved,there is also a love of humanity.’”
To Follow in a Family’s Footsteps
Sarita Sonalkar
S ARITA Sonalkar, MD, has medicinein her blood. Her mother, aunt and
three of her grandmother’s sisters werephysicians in Bombay. One of her great-aunts even started a women’s clinic thathas operated there for more than 30years. Sonalkar spent six months prior
INDRONEIL MUKERJI
DIEGO REINO

to starting medical school working atthe clinic. Naturally, she chose to pursuea medical career. “My experience at mygreat-aunt’s clinic sparked my interest inwomen’s health,” she explains. “Sincethe center provided general medical andfamily planning services for women, Iwas able to experience medicine firsthand.” The Penn State graduate was ini-tially interested in marine biology butswitched to biology halfway throughschool. It was her thorough enjoymentof science and her experience inBombay that tipped the scales towardmedicine.
While at New Jersey Medical School,Sonalkar was involved in several organi-zations including Medical Students for
Choice, a groupwith more than 100chapters at medicalschools nationwide.The organizationaims to include thediscussion of com-prehensive repro-ductive healthcare,such as contracep-tion and abortion,in the standardmedical educationcurriculum. Sonalkar feels that her expe-rience with the organization “truly fueledmy passion for complete reproductivehealthcare for women.”
Her participation in the Student
Family Health CareCenter, which pro-vides free health-care to patients,was also a reward-ing experience.Sonalkar explainsthat the programchallenges studentsto learn about clini-cal medicine muchearlier than theymight have in
another medical school. “Our involve-ment in the health center taught us howto treat and counsel patients and gave usthe opportunity as third and fourth yearstudents to mentor underclassmen. Itwas truly a hands-on experience.”
Her most memorable point of med-ical school was her third year clerkshipin obstetrics and gynecology. “I lovedthe fast pace of the specialty, the combi-nation of primary care and surgery andthe connections that I made withwomen during pregnancy, birth andmenopause—important emotionaltimes of their lives.”
Sonalkar understands that a compe-tent physician accommodates differentcultures, family values and traditions.Her goal is to work with patients andfamilies to develop management plansthat take into account these diverselifestyles. “For example, if my patient isnot adhering to her medication sched-ule, I want to know why and we can try to come up with an alternate plan to solve the problem together,” sheexplains.
Prior to starting her obstetrics andgynecology residency at UCLA thissummer, Sonalkar traveled to Ecuadorand Peru. As an avid lover of the out-doors, she enjoys camping, hiking andtravel. A family planning fellowshipand/or a master’s in public health arenext on her long “to do” list. – JILL SPOTZ
N E W J E R S E Y M E D I C A L S C H O O L 11
Happy AnniversaryTHE Student Family Health Care Center is gearing up for its 40th
anniversary during the 2007–2008 academic year. Established in thefall of 1967 in the aftermath of the Newark race riots, the student-run centerprovides health services for area residents who are uninsured or underinsured.
Appointments are available on Tuesday and Thursday evenings. On aver-age, six patients are seen per night. A team of three to five students inter-acts with each patient with an upperclassman mentoring the first- and sec-ond-year students as they take histories and perform a physical exam. Third-and fourth-year students, with their broader knowledge base, develop a treat-ment plan for the patient. An attending physician also meets with thepatient and then reviews the team’s plan. The program provides a greatopportunity for student learning while simultaneously providing patient care.
There is no cost to the patient for the visit. If additional tests are needed,patients can receive help in enrolling in University Hospital’s charity care pro-gram. Students also established a free drug formulary consisting of medica-tions to treat high blood pressure, diabetes, high cholesterol and depression.
In the last year, 321 students participated, offering a total of 4,770 hoursof community service to the health care center. During these hours, 216patient visits were recorded and the remaining time was spent in clinicalteaching sessions. Sixteen faculty members volunteer as attending physi-cians for the center, many of whom were involved in the program when theywere students at NJMS.
Current student directors are compiling a history of the center and want tohear from previous student leaders. If you helped run the clinic, please con-tact Carolyn Feuerstein via e-mail at [email protected] withyour name and class year as well as any other information you can provide.
SARITA SONALKAR

12 P U L S E S U M M E R 2 0 0 6
THE saying “It’s just like riding
a bike” took on new meaning
for fourth-year student Jim Fausto
this spring. An avid cyclist in high
school and college, he and his bike
had become somewhat estranged
during medical school. But as
one of 24 medical professionals
selected to participate in a
3,700-mile bike ride to raise
money for and awareness of
global health issues, Fausto had
to get back in the saddle while
studying for exams and juggling
residency interviews.
The inaugural Ride for World Health (R4WH) kicked off on
April 2 in San Francisco and concluded May 22 in Washington,
D.C. Along the way, the group hosted 34 lectures in various
schools, community centers and medical offices. Fausto, of
Randolph, NJ, served on the education committee, coordinating
10 of the lectures.
The cyclists wanted to raise $250,000 for Partners in Health,
a global nonprofit organization, but first, each needed to raise
$2,500 to cover expenses during the seven and a half week
journey. Fausto, who enjoyed tremendous support from his col-
leagues at New Jersey Medical School, personally raised $3,900.
Fausto finished the ride and quickly made his way back to
New Jersey for Convocation. He had a few weeks of rest before
beginning his residency training in Family Practice at the Albert
Einstein College of Medicine in Bronx, NY. Fausto plans to spe-
cialize in addiction medicine. During medical school, he spent
time studying at the Betty Ford Center for Addiction Disorders.
Fausto’s other volunteer interests have taken him to Ireland,
Canada and Ecuador, but on all three occasions, he left his bike
at home. —MELISSA CAMPBELL
P E O P L E I N T H E N E W S
San Francisco, April 2Well, this is it. We start today. After dip-ping our back wheels in the SanFrancisco Bay, the inaugural Ride 4World Health will begin making its wayacross the country. The plan is to ride20 miles, then stop for a snack break,ride another 20 miles, stop for lunch,then log another 40 miles in the after-noon stopping half way, before retiringfor the evening. We’ll take turns drivingthe support vans, taking care of theequipment, planning the route, andcooking meals so every fifth day we geta chance to re-charge.
Bike Ride for Global Health
Ride for World Health
TravelogueBy Jim Fausto
COURTESY OF JIM FAUSTO

NevadaCan’t believe it snowed in the SierraNevada Mountains today. Once we gotdown over the pass, it was a beautifulspring day—quite a contrast.
UtahWe’ve logged over 900 miles so far andwe are all a little sore. Ibuprofen is nowreferred to as Vitamin I. I forgot howsore I was, though, while we camped at Bryce Canyon. We arrived around 3 p.m. and had some time to explore.What amazing views.
In a small town outside of Boulder, apark ranger we had been in contact withprior to the ride arranged for us to staywith a few of the other park rangers inthe area. We had become very accus-tomed to sleeping communally in highschool gyms, our regular accommoda-tions, so it was almost a little lonely tobe with just a few people. We werescheduled to present a lecture here andwere overwhelmed by the generosity ofthe 150 people who prepared a potluckdinner for us before the talk. YUM!
Colorado – Monarch PassThe high point of the ride, literally, wasMonarch Pass, which topped out at11,312 feet. Going up the eleven milehill took some of us close to two hours,but coming down, it took only about 45minutes—my top speed was about 53miles an hour!
KansasThe flatlands of Kansas were definitely awelcome sight after the hilly terrain ofthe previous states. We met a veryfriendly Vietnamese potbelly pig alongthe way who made us feel very welcome.We did a lot of smart riding along theway, drafting to cut down on windresistance and taking turns breaking thewind. There were a few experiencedcyclists among the group as well as some
relatively new to the sport with the rest of us somewhere in between. Every day we hadabout three or fourflats; over the course ofthe trip, I’d estimatewe must have fixedclose to 200 tires.
MissouriEach morning, afterwaking up, eating andgetting our bikes andbrains ready for the day, we would circleup and go over the day’s route. We insti-tuted another morning tradition, thenomination of the All-Star award forgoing above and beyond and the GoofBall award for, well, just about anythingwe deemed goofy. One woman managedto hold onto that honor for a wholeweek! I won’t say what she did todeserve it, because, after all, what hap-pens on the Ride 4 World Health, stayson the Ride 4 World Health!
N E W J E R S E Y M E D I C A L S C H O O L 13
Probably the best part of the ride was
not the ride itself, but the opportunity to see America from a completely different perspective.
SAN FRANCISCO
KANSAS
UTAH
(continued on page 15)

14
P E O P L E I N T H E N E W S
P U L S E S U M M E R 2 0 0 6
WHAT can be better for a third yearmedical student than to witness
the excitement of discovery, while work-ing alongside the world’s most brilliantscientists. That is exactly what happenedto Hiral Patel, thanks to the urging of themedical student’s mentor PranelaRameshwar, PhD, associate professor ofmedicine at NJMS, who encouraged herto apply to the Howard Hughes MedicalInstitute Research Scholars program. Shewas accepted and last year moved to theNational Institutes of Health campus inBethesda, MD, for 12 months. There,along with 40 other medical and dentalstudents from the U.S., Patel chose amentor and research project to pursue.She attended weekly presentations fromrenowned scientists and had the opportu-nity to collaborate with researchers fromseveral different fields, including derma-tology, diabetes and ophthalmology.
Patel chose to work in the lab ofThomas Waldmann, MD, developing
new ways to enhance the body’simmune system to fight cancer. Sinceshe wants to pursue a career in oncolo-gy, conducting both clinical and transla-tional research at the NIH was a reward-ing experience. “Knowing that my workcould help further the understanding ofcancer pathology and lead to bettertreatments kept me going on days whennothing seemed to go right in the lab,”she explained. The Howard HughesMedical Institute employs more than300 investigators who direct researchlaboratories on campuses and universi-ties throughout the U.S. Since 1998 theInstitute has awarded $1.5 billion ingrants.
Now back at NJMS, she continues tofind cancer pathology fascinating andchallenging. “During clinical rotations Iam inspired by my patients’ courage atsuch a difficult time in their lives,” sheexplains. “Their conviction pushes meto work harder.” – JILL SPOTZ
PHOTO: PETER BYRON; ILLUSTRATION: PHILLIP DVORAK
NJMS Student PursuesResearch at NIH
WILLIAM GLUCKMAN, DO, chief of thedivision of emergency medicine andassistant professor of surgery, receivedthe Educator of the Year Award from theNew Jersey State Chapter of theAmerican College of EmergencyPhysicians. In addition to serving asmedical director for University Hospital’sEmergency Medical Services, Gluckmanis also the advisor for the medicalschool’s Emergency Medicine InterestGroup, which provides opportunities forstudents to learn more about the fieldhands on.
DAN BOUTSIKARIS’08, a member ofthe Emergency Medicine InterestGroup, was selected to receive theMedical Student of the Year award fromthe same organization.
EILEEN MOSER, MD, FACP, director ofResident Professional Development, waselected Northern Governor of the NewJersey Chapter of the American Collegeof Physicians. In this capacity, she willbe responsible for chairing the chapter’smembership committee and co-chairingthe 2007 Scientific Program.
JOEL DELISA, MD, professor and chair,Department of Physical Medicine andRehabilitation, was named vice-chair ofthe American Board of MedicalSpecialties. DeLisa previously served onthe group’s executive committee andheld the office of treasurer.
HARVEY OZER, MD, professor anddirector of the New Jersey MedicalSchool-University Hospital CancerCenter, was reappointed as commissionmember to the New Jersey StateCommission on Cancer Research, serv-ing through June 2008.
THE DEPARTMENT OF FAMILY MED-ICINE celebrated its 15th anniversary.
accolades

Zipper Day!It was somewhere in Missouri that wereached the halfway point of our jour-ney. Because the bike route was printedhorizontally across the front of our bikejerseys, we knew we were half way whenwe made it to the zipper. We had beenkeeping track of our progress thanks tothose great zippers.
12 days of rainIt’s hard to believe that for almost twoweeks it rained. It started in St. Louis,and somehow we managed to ride withthe storm front through Illinois, Ohio,Indiana and West Virginia. We were aninteresting collection of people, equallydivided between primary care and sur-gery. My thought is that we reflect thetwo types of people who would find thistrip compelling—the easygoing, hippy
types who want to save the world andthe sporty, competitive types who thriveon a challenge. Guess that’s what makesthe world go ’round!
OhioRiding into Ohio was akin to a home-coming. Since the ride was conceived bya group of medical students at OhioState University Medical Center, therewas a lot of excitement abounding whenwe rolled into town. A number of peoplemet up with us outside of town and rodein with us. The school had designated itGlobal Health Day and we presentedseveral of our lectures to a huge crowd.We had prepared a total of four lecturesfor the trip and all of us were able todeliver any of them: HIV/AIDS, GlobalHealth 101, Childhood Health andSurvival, and Access to Health Care.
West VirginiaIt’s amazing how surprised people arewhen they hear most of the statistics wecite in our lectures, for instance, 11 mil-
lion children die needlessly each yearfrom AIDS, TB, malaria, parasites, andmalnutrition. And at least two-thirds ofthese deaths are preventable. A $3 insec-ticide treated mosquito net can savehundreds of dollars in medical treat-ment for malaria and can save a life ifthe medical treatment is not available, asis the case in so many places.
Washington, DCHome stretch. Probably the best part ofthe ride was not the ride itself, but theopportunity to see America from a com-pletely different perspective. I was con-tinuously overwhelmed by the supportand generosity of the many people wemet along the way, most of them com-plete strangers. And of course, I havemade friends for life. We have allpledged to do an alumni ride next year,joining the 2007 riders for a leg at somepoint along the way. Even after 3,700miles of sore knees, tired muscles androad rash, I can honestly say I am look-ing forward to it! �
N E W J E R S E Y M E D I C A L S C H O O L 15CDC/ DR. GEORGE KUBICA
DAVID Alland,MD, chief
of the Division ofInfectious Disease at NJMS, iscollaborating with scientists from theCepheid Corporation, a Sunnyvale,California-based molecular diagnosticscompany, to apply their latest biotechinnovations to develop a simple, accu-rate, rapid and affordable diagnostic testto identify those who have TB.
The collaboration between Allandand the Cepheid Corporation wasarranged by the Foundation forInnovative Diagnostics and is supportedby a $3.7 million grant over the nextthree years by the Bill and MelindaGates Foundation. Last year, there were
approximately three millionTB cases reported worldwide.
There were 485 documentedcases in New Jersey in 2005. Alland explained that this diagnostic
instrument will be integrated into desk-top equipment. Sputum samples frompatients suspected of having TB will beadded directly to a small cartridge thatwill be inserted into the instrument. Areadout will be produced by the appara-tus in less than two hours.
“This new technology will have thesensitivity to provide healthcare profes-sionals with rapid results that currentlyrequire days to weeks to produce,”Alland explained. “Our medical schoollaboratory developed the TB assay and
adapted it to the Cepheid-manufacturedcartridge. This will be the first time thatsputum samples are processed automati-cally for fully integrated and automatednucleic acid analysis.” The device alsowill predict whether a patient has TBthat is resistant to the drug rifampin,which usually indicates that the TB ismulti-drug resistant.
Today’s standard culture method ofTB detection takes days to process and frequently is inaccurate. With fasterdetection, physicians can better treatpatients. A chronic bacterial infection,TB causes more deaths worldwide thanany other infectious disease. �
Bike Ridecontinued from page 13
A Large for Tuberculosis Diagnostics

Leaders, Role Models, Mentors and More
A top-quality education depends upon exceptional teachers.
Golden Apple awards are given by New Jersey Medical School students to honor their
outstanding teachers for providing excellent learning experiences in the classroom, the laboratory,
the hospital and other patient care settings, in addition to serving as mentors.
This year, 13 faculty members and six residents were singled out for this significant honor. Many
of the faculty members on the list have been awarded Golden Apples year after year.
We salute all of the winners and provide you with short profiles of four of them to illustrate the
qualities that make a good teacher—as determined by the students.
The GoldenApple Award
By Eve Jacobs

N E W J E R S E Y M E D I C A L S C H O O LLEFT: JOHN EMERSON; TOP: COURTESY OF ALAN BEITLER 17
Alan BeitlerMILITARY MAN—AT EASE
Twenty-seven years in the army is more than likely to leave itsmark, but neither Alan Beitler’s bearing nor his demeanor giveany indication of his long military history. He retired from theU.S. Armed Forces in December 2005 and that month becameChief of General Surgery at the VeteransAdministration New Jersey Healthcare System.He is currently an associate professor of sur-gery at NJMS.
A native of Long Island, Beitler entered theUnited States Military Academy at West Pointin 1973. Why did he choose to take a militarypath? “The price was right,” he quips. “It wasfree.”
“The education there is great,” he contin-ues. “And the values of ‘duty, honor, country’guide me to this day. I didn’t know what I wanted back then,but the curriculum is broad-based, and you can go on to doanything. Some of my friends have done incredible things.” Infact, some of the doctor’s classmates did go on to do extraordi-nary things, among them José María Figueres Olsen, class of’79, who served as president of Costa Rica from 1994 to 1998.
But despite the glowing report he gives the education and hisfellow students, Beitler comments: “West Point was not a pleas-ant place in the 1970s. It was the end of the Vietnam War—not a kind and gentle time, not a good time to be part of themilitary.”
Following graduation in 1977, Beitler served as an infantry-man in Italy. Three years into his military commitment, heremembers riding on the back of a truck with a colleague, cov-ered with manure. “We were dirty, miserable and lamentingthat this was no way to live a life. Then he started talking to meabout his plans to go to medical school.”
The then-24-year-old recalls thinking those plans “soundedso appealing—no one telling you what to do, no regimentation,and the opportunity for helping people.” Without any priorserious thought on what his next step in life would be, Beitlerdecided then and there that medical school and medical prac-tice sounded pretty darn good. So, when he returned to theStates, he took “catch up courses” at night, applied and wasaccepted at SUNY School of Medicine and Biomedical Sciencesat Buffalo.
What he found there was “such a different life from WestPoint, which was so time consuming, so regimented and so all-consuming. Medical school, on the other hand, was thorough-ly enjoyable.”
Of course, he understands, that “the perspective of havingbeen an infantryman in the army helped.” While many of hisclassmates found medical school to be a grind, “I thought it wasgreat! After slogging around in mud for years, being back in theclassroom was a treat,” he says.
Although he initially thought he was headed into pediatrics,Beitler switched gears during his fourth year of medical school.“The fundamental approach of surgery really appealed to me,”he explains. “While pediatrics is largely detective work, surgerygives you the opportunity to sort out problems, do somethingto address them and oftentimes fix them.”
SO WHY DOES ALAN BEITLER THINK THE CLASS OF 2007 CONSIDERS
HIM WORTHY OF A GOLDEN APPLE? “I THINK IT’S BECAUSE I TREAT THE
STUDENTS AND RESIDENTS WITH RESPECT.
I believe that how you deal with people makes an enormous difference.”
Dr. Alan Beitler in Afghanistan

18 P U L S E S U M M E R 2 0 0 6
“I see surgeons as more complete doctors,” he continues,“because they can often see a problem through to completion.”
Beitler first completed a general surgery residency atFitzsimons Army Medical Center in Aurora, Colorado (east ofDenver), where, he points out, John Kerry was born onDecember 11, 1943. The hospital closed in 1999.
He then chose to specialize in surgical oncology because itafforded him the opportunity to “spend more time building arapport with patients who are facing such a significant event intheir lives. You can do so much good,” he says. “Instead of apatient’s last days being torture, you can make a difference, evenif you can’t operate. You can make their quality of life, anddeath, better.”
On the technical front, he finds specializing in oncology tobe more rewarding because “you operate all over the body—you’re not limited to a narrow focus.”
But it’s the combination of doctoring and teaching that hefinds so satisfying. “To do your 400th hernia operation mightnot be terribly exciting, but to do that surgery with someone whois in there for the first time—that’s a great experience!” he says.
He admits that there is some angst when you’re the seniorperson doing that surgery with a first-timer. “You give up ameasure of control,” he states, “but it’s well worth it.”
So why does he think the Class of 2007 voted their new pro-fessor worthy of a Golden Apple? “I think it’s because I treat thestudents and residents with respect. I believe that how you dealwith people makes an enormous difference,” he says. “All ofthese students are bright and energetic.”
He also believes that how a teacher relays information is veryimportant. “I try to transmit information in a way that makessense. ‘Keep it simple, stupid!’ is always in my mind, but I alsolike to give a multi-tiered explanation—something for every-one.”
“You have to understand the material and keep up with theliterature, but teachers don’t have to be brilliant,” he comments.“You don’t have to be the brightest bulb to light up the room.”
He thinks students really appreciate time and attention. “Mysense is that sometimes they’re ignored,” he says.
A portion of the third year medical students spend a three-week surgery rotation at the Veterans Administration MedicalCenter in East Orange, where Beitler is stationed most of thetime. The students divide their time between vascular surgeryand general surgery, attending a series of conferences, going ondaily rounds and observing actual operations.
Beitler believes that even students who already know thatsurgery will not figure in their future work should be exposedto the goings-on in the OR. “It’s good to know what other spe-cialties do,” he says. “It paves the way for improved communi-cation and cooperation.”
He likes working at the Veterans Hospital because, he says,the pace is not quite so pounding. “You have the time to spendwith patients, and also to teach. Plus, caring for veterans is animportant public service.”
Beitler achieved the position of colonel in the army beforeretiring. His last years in the military were spent at the preciseplace that he started his career—West Point—but this time hewas Chief of Surgery at their hospital. On looking back andlooking forward, he says “I had a rich and rewarding career inthe military, filled with clinical, administrative and leadershipopportunities in the United States and abroad.”
“This is what I want to do now. I want to be around to raisemy family and I want to teach people how to be good doctorsand take good care of patients.” His wife, Ruth, is an associateprofessor of international relations and comparative politics atWest Point, and he has two daughters, Eliyana and Hannah,both age 7.
It’s obvious that Alan Beitler is doing an A-1 job. His stu-dents certainly salute his efforts—and it’s not often they handout their highest honors to someone who’s been “back toschool” for a mere 18 months.
Sylvia ChristakosA BARRELFUL OF GOLDEN APPLES
Success is rarely handed out on a silver platter—it’s earned byhard work, talent, focus and a certain “je ne sais quoi,” or inde-finable something. Sylvia Christakos, PhD, professor of bio-chemistry and molecular biology at NJMS, is an indisputablesuccess. Her accomplishments speak for themselves: 25 years ofteaching and NIH-funded research at NJMS, earning tenure in1985 and a full professorship in 1990; establishing a lab that isnow among the top three worldwide for Vitamin D research;publishing 125 peer-reviewed articles; serving as the thirdwoman president in 2004/2005 of her professional organiza-tion—the American Society for Bone and Mineral Research—and as associate editor of its journal; and last but not least, win-ning 13 Golden Apple awards for excellence in teaching med-ical students.
Her love of teaching gets her going every morning and hasbeen a consistent thread throughout her professional life. And itis her unwavering belief in the value of learning that propelled herto earn a doctorate in molecular biology at a time when “women”and “science” were not often married in the same sentence. Infact, she comes from a line of strong, determined women, who allcarved out their successes despite serious hurdles.

The Greek island of Chios—home to Hippocrates andHomer—was also home to Christakos’ grandmother, who leftthere to set sail for the U.S. with her young daughter in theearly 1900s.
The young émigré made success happen—establishing inlower Manhattan what became the first Greek school in NewYork City, teaching Greek language, customs and history to thechildren of immigrants. “Shewas a real trailblazer whobelieved in the value of educa-tion,” says her granddaughterproudly.
Unfortunately, Christakos’grandmother died of breast can-cer in her early 40s, leaving an18-year-old daughter, who verymuch wanted a college education, but suddenly needed to sup-port herself. Despite that major setback the daughter estab-lished floral businesses—with her husband—which became“the best” in Queens. After her husband’s death in his 50s,Christakos’ mother not only managed but expanded the origi-nal business.
“My mother read The Wall Street Journal and invested in thestock market. She worked 14-hour-days in the 1950s, whenmost women stayed at home,” Christakos comments.
Christakos kept those early lessons in mind when she head-ed off to college. She credits her four years at a small, women-only college with providing an excellent learning environment.She had a talent for science, and also a facility for writing, acombination of abilities that has allowed her to continuouslywin the grant money that has supported her research and thatof six PhD students and post docs in her lab for 25 years.
In her next 10 years she married Manny Christakos (now asurgeon in private practice) in 1970, earned a PhD inendocrinology from the State University of New York at Buffaloin 1973, completed a post doc in physiology at Roswell ParkMemorial Institute, SUNY Buffalo, in 1974, a post doc in bio-chemistry from SUNY Buffalo in 1976, and another post docin biochemistry in 1980 from the University of California,Riverside.
She says her acceptance into a National Science Foundationprogram at Cornell Medical School during one high schoolsummer introduced her to high level science. Then “excellentmentors” from her graduate and post doc programs helped herprogress along the right path.
Her motto for herself is: “Give it 150 percent,” a drive thathas certainly contributed to her excelling as a teacher and aresearcher.
But what Christakos brings to the table that everyone recog-nizes as truly golden is her “caring about the students and car-ing enough about their learning to want to facilitate it in anyway I can.”
Add to that her feeling that “it’s a privilege to teach NJMSstudents. They’re down-to-earth, idealistic and enthusiastic.They make it a pleasure to come to work every day.”
The researcher sees molecular biology and biochemistry as
the “hottest area, the one where you can make the biggest dif-ference in treating disease.” There is an enormous amount ofbasic science information for her to teach and for her studentsto learn, which she makes pertinent by infusing the clinical cor-relations into her lectures. She explains that this course givesstudents the biochemical bases for their future patient care.
N E W J E R S E Y M E D I C A L S C H O O L 19
SYLVIA CHRISTAKOS FEELS “IT’S A PRIVILEGE TO TEACH NJMS STUDENTS.
THEY’RE DOWN-TO-EARTH, IDEALISTIC AND ENTHUSIASTIC.
They make it a pleasure to come to work every day.”
JOHN EMERSON

She not only sparks the enthusiasm of first year students, butalso PhD candidates and post docs who work in her lab, whichhas been consecutively funded for almost three decades by theNIH—oftentimes by more than one grant at a time.
In the course of her career, Christakos has trained 19 PhDstudents and 11 post doc fellows. “My lab is my other family,”she says. She proudly rattles off their accomplishments: “One ofmy MD/PhDs is now at Novartis doing drug safety work; oneheads her own lab at Wyeth/Hearst; another is an associate pro-fessor at the University of Connecticut; one is a dean of researchat Marquette Dental School; another does clinical trials researchat Novartis; another is a resident in pathology at Duke,” and soit goes, on and on.
Her advice to those she helps train is the same she has givenher own three children as they establish their paths in life:“Never become complacent. Maintain your ideals. Never losesight of why you chose your profession. Never think of it as justa job—keep in mind your larger purpose and you’ll always behappy.”
There’s no doubt that her students are wowed—they’ve givenher a barrelful of golden apples over the years. One studentsummed up her merits simply: “Dr. Christakos could very wellbe the world’s perfect professor.”
The admiration is mutual. Christakos recognizes that thesestudents—just starting to prepare for their careers—will be theones to change the delivery of patient care and teaching in thefuture. She says: “Do it your way. Set yourself the goal to makeit all better.” And she believes that they will.
Kenneth M. KleinTEACHING UNDER THE MICROSCOPE
To the naked eye, humor and pathology appear to have little incommon. But under the microscope, it’s a whole different story.Kenneth M. Klein, MD, has been teaching pathology at NJMSfor 30 years and at least some of his success can be attributed tothe fact that his “funny bone” is still intact.
When asked why he thinks second year medical studentsaward him the Golden Apple year after year, he uses cartoonhumor to illustrate his point. A visiting lecturer presented thiscartoon, Klein explains, and it struck a nerve.
Cartoon panel 1: A little boy and a little girl are talking.There is a dog by their side. The little boy says: “I taught Spothow to talk.” The little girl answers: “I don’t believe you.”
Panel 2: The little boy says, “OK, I’ll show you.” He address-es the dog: “Spot, talk!”
Panel 3: Both children watch Spot.Panel 4: The girl says, “I thought you said you taught Spot
how to talk.” The boy answers: “I did. But I didn’t say helearned it.”
It’s a point well taken. Klein says that if he gives a fabulouslecture and Spot attends the class, but doesn’t learn the lesson,then his teaching deserves to earn a failing grade. There aremany faculty members at all universities who feel their respon-sibility ends with the delivery of information, he says, and thatsituation has gotten worse with the popularity of Powerpoint.
“There are teachers who onlyread the bullet points out loudfrom their slides. Can youimagine?” he says.
Lest you think the patholo-gist entertains in his lecturehall, think again. His style ofteaching is traditional—nobells and whistles, no SaturdayNight Live routines. But hisplain and simple approach evi-dently works. He’s received 23annual teaching awards fromhis students in 30 years, andonly a rule stating that a facul-ty member cannot be awardedthe Golden Apple for morethan two out of three consecu-tive years running gives him animperfect score.
PETER BYRON20 P U L S E S U M M E R 2 0 0 6

He says modestly: “I present information that is interestingand useful.” But clearly there’s more here than initially meetsthe eye.
“Pathology is not a specialty that is a popular career choicefor American medical students,” states Klein. Despite beingcrucial to the practice of medicine, most of a pathologist’s workis conducted behind the scenes and does not involve directpatient care.
Pathology, however, provides the scientific basis for medicalpractice by using basic research methods to uncover informa-tion that supports or refutes a diagnosis and helps the physicianmap out the course oftreatment. Accordingto the department’sWeb site, pathologistslook for gross andmicroscopic changesin cells, tissues andorgans caused by dis-ease processes, as wellas conducting biochemical and microbiological tests on bodyfluids, cells and tissues. In other words, a physician’s care plan isbased on the pathologist’s work, so no matter which specialty astudent eventually chooses, he or she will have to collaboratewith a pathologist.
“Useful” learning is the key here. Klein helps students grasphow the volume of information taught under the rubric ofpathology relates to health and disease, and so to their futuredoctoring. Second year students—overwhelmed with the sheerquantity of facts they’re asked to absorb—often don’t under-stand the relevance of such a course to their future professionalpractice.
But Klein has the talent—and also has honed the skills—toengage his students. To what does he attribute his success as ateacher? “I project an attitude that I’m interested in my stu-dents.” (And he is.) “I look at every student in the room—Idon’t talk to the screen.
“I know my lectures cold, I talk slowly and try to makemyself understood. I have predigested the material and I pres-ent what’s relevant. I answer questions during the lecture—Idon’t wait until the end and I occasionally throw questions outto the students. I observe what good teachers are doing andincorporate what I can.”
In other words, he cares that his students learn. A graduate ofthe Bronx High School of Science, he says he went to medicalschool “to learn as much as I could about disease. My goal wasto be a researcher.” His medical school years were sharedbetween SUNY Downstate Medical Center and CatholicUniversity in Belgium.
After a residency in pathology at NYU-Bellevue, he remainedon the faculty at NYU for four years and discovered that he hadsome talent for teaching. “I didn’t set out to be a teacher,” hesaid. “The students liked my teaching.”
When he moved in 1976 to NJMS, Klein had to make a dif-ficult choice. “I enjoyed the teaching and I enjoyed the service.I saw that research would require too much of a time commit-ment. I didn’t want to be a jack of all trades, master of none.”So he homed in on what he liked best, developing a reputationin gastrointestinal and liver pathology, and also as a masterteacher. He was elected into UMDNJ’s Master Educators Guild
in 2003 and NJMS’sAlpha Omega Alpha-beta chapter in 2004.
Does he think stu-dents have changedmuch since 1976? As a group they’vechanged very little,he says. But he has
noticed that many have shorter attention spans and rely heavilyon visual material. “Everyone is computer savvy. Everythingpresented in class must be posted on Web CT so students canaccess it,” he comments.
Labs and small group sessions in pathology are mandatory,but lectures are not. Although all lectures are available on theWeb, Klein continues to believe in the value of classroom teach-ing. Although attendance at lectures started to drop off at allmedical schools in the 70s, and has continued to do so, he says:“There is something lost for those students. They miss thehuman exchange, the stress placed on certain words, the per-sonal anecdotes.”
With the new Jubilee Curriculum that was launched atNJMS last year, pathology has been absorbed into a moreencompassing course called “Disease Processes, Prevention andTherapeutics.” Klein is OK with that. “It’s more cohesive,” hesays. “We’re tying together the information from what were pre-viously several tightly marked disciplines.” He believes the newapproach encourages students to see the relevance of the basicsciences to their clinical work and has allowed the faculty toweed out the redundancies as well as fill in the gaps.
“I like what I do,” he says simply in conclusion. “And whenI bump into former students, which is frequent, they come upand talk to me about something they remember from my classyears ago.”
Klein’s efforts on behalf of his students do not go unrecog-nized—and it doesn’t take a high-powered microscope to detectthat.
N E W J E R S E Y M E D I C A L S C H O O L 21
KENNETH KLEIN SAYS THAT IF HE GIVES A FABULOUS LECTURE
AND A STUDENT ATTENDS THE CLASS, BUT DOESN’T LEARN THE LESSON,
then the professor’s teachingdeserves to earn a failing grade.

Lisa PompeoTALKING ABOUT A LEGACY
At a time in our country’s history when the topic of immigra-tion finds its way into numerous conversations, Lisa Pompeo,MD, brings up her immigrant father with obvious pride. Hecame to this country alone from a small town in rural Italy atage 16 speaking no English, she says, and went “from pushinga broom to vice president of his company.” Along the way heinstilled in his daughter certain of his own principles that havebecome integral to her personal world view—chief among themhis great respect for education and his insistence that “you dothings because they’re right, not because they’re expedient.”Pompeo’s Golden Apple is rooted in those seeds planted by herfather.
She became the first person in her family to graduate from afour-year college, and then there was no stopping her. She “grewup seeing myself as a doctor,” but, in fact, took a bit of a detouralong the way. She was introduced to biomedical research by adynamic faculty member at the University of Dallas, a small lib-eral arts college in Texas where she did her undergraduate work,and fell in love with molecular biology and life in the laborato-ry. While working in research labsafter graduating, she matriculatedin a master’s program at NYU,where, again, she was inspired tochange course by “a prominenthematologist who was an amazingclinician.” Dr. Robert Silber, shesays, “helped so many people. Hehad such a wonderful relationshipwith his patients that they oftencame to visit him in his lab.”
Pompeo realized that doctoringtruly was her calling. In 1990, shebegan her studies at SUNY-StonyBrook’s School of Medicine, ini-tially intending to become arheumatologist. But her Ob/Gynrotation made her “so happy” thatshe immediately understood herlife’s work.
The Resident Match Programlanded her at UMDNJ-New JerseyMedical School and UniversityHospital (UH) in July 1994 andshe says that within three days, sheknew she was “a lifer. On my first
day I was scared to death and three people said hello to me—Isaw it was a friendly place. I love being here. I love the students.I love the hospital. I love the atmosphere.”
Most important, she says, “There is an underlying under-standing that everyone cares about the patients…This is themost important component.”
Put “caring” about people—whether they are students,patients, family or other relationships—right at the top ofPompeo’s own priorities. She finished her residency and becamean attending at UH in July 1998. After just one year on the job,she was asked “to keep an eye on the medical students” byGerard Hanson, MD, an associate professor in the department.Then, over a two-year period, she became site director atUniversity Hospital—eventually taking on the responsibility ofall educational activities there for the NJMS Department ofObstetrics, Gynecology and Women’s Health. Two summersago she became the clerkship director, setting the educationalagenda, goals and objectives, and taking charge of the educa-tional programs for third year medical students at all of the siteswhere the department provides training (University Hospital,Hackensack University Medical Center and MorristownMemorial Hospital).
Now she is the director of medical student education for the
PETER BYRON22
WHAT DOES LISA POMPEO LOVE BEST ABOUT HER JOB? “IT’S THE STUDENTS AND
RESIDENTS – that ’s the reason for being here.”
P U L S E S U M M E R 2 0 0 6

department. Additionally, she is the associate director of theOb/Gyn residency program at NJMS.
How much of her day is spent teaching? She says that’s real-ly impossible to assess. “Every single thing I do clinically, thereis someone with me in a training capacity—I may be teachinga medical student or resident, or supervising a resident.”
“Teaching is the most important thing we do,” she contin-ues. “It’s our legacy.”
“Just think, a doctor who educates future doctors touches thelives of all of her own patients and all of the patients on downthe line whom those future physicians take care of,” she says.“And looking at it from a very selfish standpoint, these are thedoctors who will take care of me when I get old and sick.”
For Pompeo, Ob/Gyn has been perfect. “It totally fits withmy personality,” she says. What she likes best is “being there atsome of the most significant times in a person’s life, taking careof them through all ages and stages—from their teens to theirtwilight years.”
She enjoys the intimacy of the bonds that are formed. “Youestablish a connection with the entire family—not just thewoman. There is a lot of counseling in addition to the hands-on doctoring.”
Why does Pompeo think students value her teaching? “I real-ly care,” she says. “I want them to have a good experience and Iwant them to learn.”
“Students also say I’m very fair,” she continues. “I don’t see abenefit to making things more difficult than they have to be—there’s no value in tripping someone up. If you need to knowsomething as a doctor, then you need to learn it.”
She is determined that third-year students come away fromthe clerkship feeling that they really have learned something.She wants to give them a hands-on experience during deliveriesand in the OR learning to suture. She wants them to participatein these “significant times with patients.”
When asked what she loves best about her job, she says: “It’sthe students and residents—that’s the reason for being here. Wecould all make more money in private practice or doing researchat a pharmaceutical company or at the NIH.”
She has been actively involved incorporating women’s healthinto the new Jubilee Curriculum at NJMS. “We need to expandwomen’s health into every discipline,” she states. “We need tolearn more physiologically and pharmacologically about the dif-ferences between men and women and how they react to illness.We need more research into health disparities, such as why menare more likely to have angioplasties.”
Pompeo’s father died at age 61 from complications of dia-betes. Within one month and one hospitalization, he had firstone amputation, then had complications from a diagnostic testin preparation for another and went into multi-organ failure and
passed away. This was early on in her medical school career andshe was living at home at the time. She remembers the medicalschool dean telling her not to take her exam right after herfather’s death, but she was determined. She took the test, passingby one point. Now she recognizes that she made a mistake.
“We’re professionals,” she concludes. “We need to recognizethese times in our own lives and in the lives of others.”
For her dedication to their success as professionals and ashuman beings, and her intent to always do what’s right ratherthan what’s expedient, the NJMS class of ’06 has awardedPompeo “the gold.” �
N E W J E R S E Y M E D I C A L S C H O O L 23
Class of 2006RESIDENTS
Dr. Naga Ramasubramaniam Dr. Basil Hubbi Dr. Anthony Rosania
FACULTY
Dr. Kenneth Swan Dr. Dorian Wilson Dr. Lisa Pompeo Dr. Ziad Sifri
Class of 2007RESIDENTS
Dr. Pedro VieraDr. Shauna WilliamsDr. Lisa-Ann Michaels
FACULTY
Dr. JoAnn ReteguizDr. Alan BeitlerDr. Anand Srinivasan
Class of 2008FACULTY
Dr. Kenneth KleinDr. Marjorie BrandrissDr. Christine Gerula
Class of 2009FACULTY
Dr. David DeFouwDr. Nagaswami VasanDr. Sylvia Christakos
ADMINISTRATOR
Heidi Schwalb
Thi
s Yea
r’s
Gold
en A
pple
Win
ners
Over the years, NJMS professor Nagaswami Vasan, DVM, PhD,has witnessed an array of reactions to the task at hand, many ofthem incredibly intense. Following their first few sessions in thegross anatomy lab, students are often shaken and wrestle withthoughts of their own mortality and that of their loved ones, hesays. Witnessing a cadaver “up close and personal” may makedeath and dying real to many students for the first time. Andthat is just the beginning. In less than four months, Vasan andteaching partner David DeFouw, PhD—both of whom havebeen awarded numerous Golden Apples by their students—willshepherd this group through their emotional roller-coaster rideas well as what has traditionally been one of the hardest coursesacademically in the four-year medical school curriculum. Andit’s certainly one of the courses they can least afford to fail. All oftheir subsequent learning about health and disease will be basedon a basic understanding of how the human body is construct-ed and how it functions, which they can only learn here.
This is the challenge that greets Vasan anew every year as eachfreshman medical school class steps up to the plate, but it’s achallenge that calls to his heart. Even after almost 30 years doingthis job and doing it well, he is always looking for a better way.
In fact, just five years ago, Scribner published a 272-pagebook entitled Body of Knowledge by Asbury Park Press reporterSteve Giegerich detailing his observations after spending an
entire semester with the medical students around Vasan’s grossanatomy dissection tables. The book received critical acclaimfrom many sources, including Publisher’s Weekly and LibraryJournal. There has even been some talk lately about a made-for-TV movie, or series, based on the riveting action in this lab.
The book follows one group of NJMS students as they workon “their” cadaver for the 15-week class. All have since graduat-ed from NJMS with their MD degrees. The writer focuses oneach individual’s reactions and the group’s dynamics as the fourwould-be-doctors work at their dissection, a task that is bothemotionally and mentally demanding. The students, many ofwhom have never held a scalpel, must cut into human flesh,carving out the organs, bones, muscles, joints, ligaments andtendons, of their anonymous cadaver.
Giegerich tells readers the background of the donated corpse.He was a man by the name of Tom Lewis, a public schooladministrator in New Jersey, who had a strong commitment tofurthering science and a willingness to put that belief on the line.The journalist records the students’ struggles, particularly theirhesitation on having to cut into a human face, a kind-of “sacredground” that they perceive as housing the personality.
It’s clear that Vasan welcomed the reporter—and photogra-pher Noah K. Murray—into this classroom because he has histeaching of gross anatomy “down to a science.” There probably
24 P U L S E S U M M E R 2 0 0 6
Reconfigured
To “steady the hands” of 170 freshman medical students as they begin their dissection
of a human cadaver is no small undertaking.
ANATOMICAL TRAVELOGUE / PHOTO RESEARCHERS, INC
By Eve Jacobs

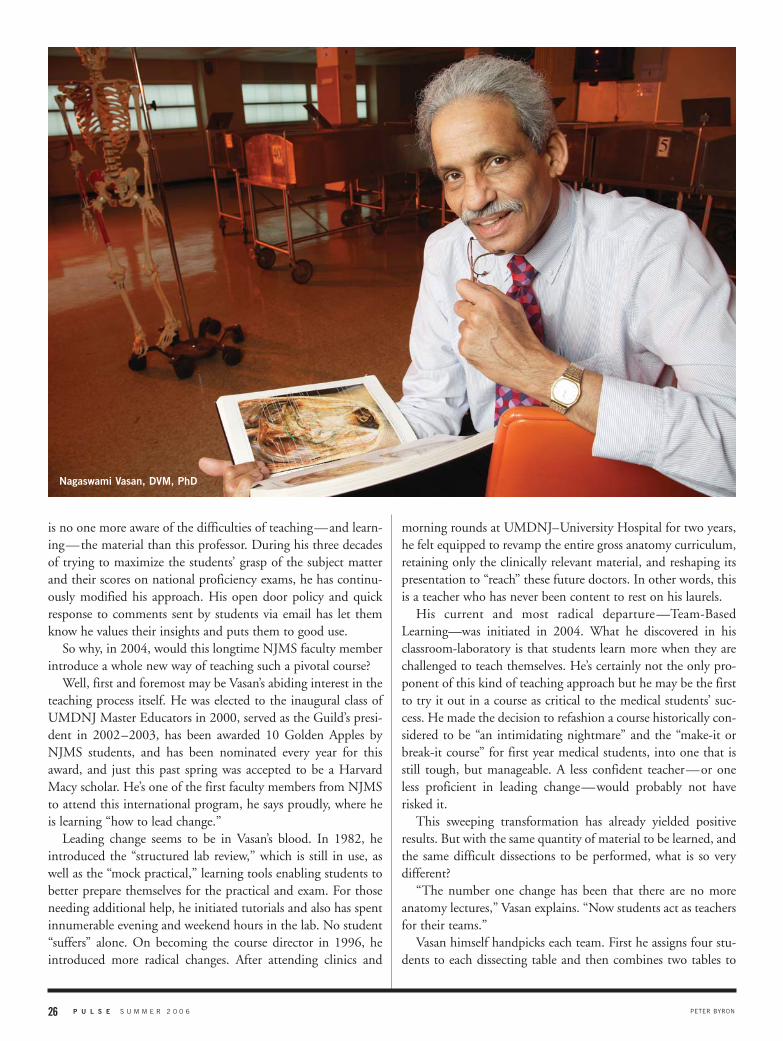
is no one more aware of the difficulties of teaching—and learn-ing—the material than this professor. During his three decadesof trying to maximize the students’ grasp of the subject matterand their scores on national proficiency exams, he has continu-ously modified his approach. His open door policy and quickresponse to comments sent by students via email has let themknow he values their insights and puts them to good use.
So why, in 2004, would this longtime NJMS faculty memberintroduce a whole new way of teaching such a pivotal course?
Well, first and foremost may be Vasan’s abiding interest in theteaching process itself. He was elected to the inaugural class ofUMDNJ Master Educators in 2000, served as the Guild’s presi-dent in 2002–2003, has been awarded 10 Golden Apples byNJMS students, and has been nominated every year for thisaward, and just this past spring was accepted to be a HarvardMacy scholar. He’s one of the first faculty members from NJMSto attend this international program, he says proudly, where heis learning “how to lead change.”
Leading change seems to be in Vasan’s blood. In 1982, heintroduced the “structured lab review,” which is still in use, aswell as the “mock practical,” learning tools enabling students tobetter prepare themselves for the practical and exam. For thoseneeding additional help, he initiated tutorials and also has spentinnumerable evening and weekend hours in the lab. No student“suffers” alone. On becoming the course director in 1996, heintroduced more radical changes. After attending clinics and
morning rounds at UMDNJ–University Hospital for two years,he felt equipped to revamp the entire gross anatomy curriculum,retaining only the clinically relevant material, and reshaping itspresentation to “reach” these future doctors. In other words, thisis a teacher who has never been content to rest on his laurels.
His current and most radical departure—Team-BasedLearning—was initiated in 2004. What he discovered in hisclassroom-laboratory is that students learn more when they arechallenged to teach themselves. He’s certainly not the only pro-ponent of this kind of teaching approach but he may be the firstto try it out in a course as critical to the medical students’ suc-cess. He made the decision to refashion a course historically con-sidered to be “an intimidating nightmare” and the “make-it orbreak-it course” for first year medical students, into one that isstill tough, but manageable. A less confident teacher—or oneless proficient in leading change—would probably not haverisked it.
This sweeping transformation has already yielded positiveresults. But with the same quantity of material to be learned, andthe same difficult dissections to be performed, what is so verydifferent?
“The number one change has been that there are no moreanatomy lectures,” Vasan explains. “Now students act as teachersfor their teams.”
Vasan himself handpicks each team. First he assigns four stu-dents to each dissecting table and then combines two tables to
PETER BYRON26 P U L S E S U M M E R 2 0 0 6
Nagaswami Vasan, DVM, PhD

make teams of eight. While these groups could be assembled ran-domly, he explains, they are far more successful if the experiencesof the members are very varied. “I mix mature and young peo-ple, women and men, students with differing work experienceand those from different ethnic backgrounds. The group will failif its members have all had similar experiences,” he states.
Why does this matter when learning human anatomy? Thecourse director explains that through the group’s discussions,these students will learn differential diagnosis. Being able toidentify body parts is the easy part of the lesson, he contends.More important is the development of critical thinking skills totake that knowledge to thenext step.
“Students will learn howto discuss a problem, tak-ing into account varyingperspectives, and to thinkthings through to a satisfac-tory end,” he says.
The class of 170 stu-dents meets three timeseach week for three hours of dissection time. That constitutes 65percent of the course time. “That has not changed,” says Vasan.Each of the team-based sessions—which have taken the place ofthe lectures—lasts 90 to 120 minutes.
Students are given a hefty reading assignment and learningissues that must be completed before each class; and each classkicks off with a quiz. “This provides for continuous self-assess-ment and ‘fast tracking,’” he says.
If a student is falling behind, Vasan says it becomes apparentimmediately. “I can pull that student out and ask what’s goingon,” he explains. “In most cases, the student is studying thewrong way. I can put the student back on the right track veryquickly.”
He says that his data has shown that students whose perform-ance on weekly quizzes is consistently “borderline” will be in thelower percentile by the end of the class. “Now we will approachthose students early and tell them where they are lacking,” hestates.
Although classes this large often have a dozen facilitators tomake small group learning effective, Vasan says proudly that inthis course, there are just two. He and DeFouw are always pres-ent in the TBL sessions and each “visits” half of the teams—spending a few minutes with each—during every session. Thefacilitator observes the group dynamics, assesses if the team isdoing okay, refocuses team members if the group is off-base; andmight give them a “one-minute lecture,” which the course direc-tor calls “micro-teaching.”
“The team must arrive ready to critically discuss what they’veread,” he says. Fifteen percent of a student’s grade in this course
will come from his “team effort,” according to the anatomyteacher.
Exams are given five times during the semester. When theexams are taken away, explains Vasan, the team assembles to dis-cuss each question, arriving at a group answer. “The conversa-tions are really intense,” he says. “Team members discuss why anincorrect answer is wrong. There is a lot of teaching going onduring those sessions.”
Perhaps one of the more critical elements of team-based learn-ing in gross anatomy is peer evaluation. Students critique eachother five times during the course—on punctuality, prepared-
ness, contribution to thegroup, respect for eachother and flexibility (con-sidering other points ofview). If a student is notcontributing enough,according to the teamreport, then one of thefacilitators will talk withhim or her.
Communication, communication, communication. Vasanhas demonstrated that when the communication lines areopened between students and facilitators, and students and theirfellow students, “no one should fall behind.”
The feedback on this new approach has been “outstanding,”he says. Students learn quickly that there is a limit to one per-son’s knowledge, and that team members have to talk with eachother and rely on each other. “It teaches future doctors to workas a team,” he says. “Memorization no longer works. Team mem-bers are forced to think critically.”
Vasan does admit that the course is a lot of work for the twofacilitators, who are responsible for the success of all 170 stu-dents. Every week the students’ data is input in Excel, he says, sothat the facilitators can chart each student’s performance.
What has become apparent is that when the data from 2002and 2003 (when gross anatomy was taught traditionally) is com-pared with the 2004 and 2005 data, the students are doing muchbetter now. National test scores are rising, too.
“Medical students are competitive,” Vasan says. “So whenthey see it works for one course, they figure why not try it inother classes as well.”
Next year the gross anatomy teacher will work with the bio-chemistry faculty at NJMS to initiate team-based learning inthat course. And other medical schools across the country areasking for his help, too.
Vasan does not take these successes lightly. He knows thatteachers are tested even more strenuously than those theyteach—and that an A+ from students is hard-earned and a verysweet thing. �
N E W J E R S E Y M E D I C A L S C H O O L 27
“The number one change HAS BEEN THAT
THERE ARE NO MORE ANATOMY LECTURES,” VASAN EXPLAINS.
“NOW STUDENTS ACT AS TEACHERS FOR THEIR TEAMS.”


N E W J E R S E Y M E D I C A L S C H O O LJOHN EMERSON 29
The timing was perfectly
terrible: it was just a few monthsafter the September 11th terrorists’attack on the World Trade Center andthe subsequent anthrax outbreaks.
Fears about bio-weapons were on everyone’s mind. Even open-ing ordinary mail had become fraught with danger. So the ideaof moving 61 years worth of stored pathogens—a scientifictreasure trove of the world’s most dangerous infectious agentsand potential weapons of mass destruction including everythingfrom mycobacterium tuberculosis (source of TB) to major hospi-tal acquired bacteria—out of the safety of their freezers and intothe streets of New York City, might have sounded like a prank.Yet, moving day for the Public Health Research Institute(PHRI) was fast approaching.
For David Perlin, PhD, PHRI’s scientific director, the logis-tics of this legitimate task—no joke at all—looked doable butnot without myriad problems. His biomedical research organi-zation, which specializes in understanding the molecular basisof disease by studying bacteria, fungi, and viruses, had been aNew York City icon for decades, and was located within theNYC Department of Health’s Bureau of Laboratories buildingin downtown Manhattan. PHRI, which conducts basic andapplied biomedical research in infectious diseases, had out-grown its quarters and needed expanded lab space. This is theplace where infectious nightmares like polio, typhoid fever,influenza and smallpox were studied before and during theemergence of the antibiotic era. Through the years, PHRIresearchers have made landmark discoveries that have advancedmajor scientific disciplines including virology, bacteriology,immunology and biochemistry. “We have a rich history of join-ing science with medicine and our research has to go from benchto bed and back again. We always ask ourselves: where can wemake a difference?” Perlin explains. But in 2001, “Just to accom-modate our TB program, we’d been running the small BiosafetyLevel 3 (BSL3) containment area 24 hours a day, seven days a week.”
So, after extensive negotiations, PHRI and UMDNJ officialsagreed the move to the International Center for Public Health(ICPH) in Science Park, Newark, would be beneficial for bothparties. The new building, with its open landscape architectureand state of the art laboratories, is just down the street from NewJersey Medical School (NJMS)’s main campus on land owned bythe University. “There are no walls between the labs and every-thing about us fosters interaction.”
Perlin himself was involved in every construction phase andhad even talked his 17 principal researchers into moving and
leaving all their old equipment behind in exchange for custom-designed research space and new equipment. “This building haswon awards and so has our architect. We’re now the model formany National Institutes of Health Biosafety Level 3 spaces.”Every single lab director moving to New Jersey was interviewedby the architects to make sure research needs would be met.“We believed that this wonderful new space would also help usrecruit new scientists pursuing infectious disease research”—adream that has since materialized for PHRI and NJMS andsomething that makes Perlin very proud. Just last March,UMDNJ’s Board of Trustees gave the green light for the devel-opment of an agreement for PHRI to become a formal centerof the New Jersey Medical School. This year also marks the 65thanniversary of PHRI as an institution.
In his sunny, second floor office on Warren Street, Perlinreaches for an old copy of Life Magazine with its cover story onviolence in the streets of Newark and a stark black and whitephoto of a gunshot victim which leaves nothing to the imagi-nation. At first, when confronted with a relocation to new quar-ters, across the Hudson River, “a lot of the PHRI faculty said tome, ‘You must be crazy.’”
Many of his staff members are confirmed New Yorkers whohave since grown to love their new work space, even with itscommute. “There was already a small group of medicalresearchers here at NJMS working in infectious diseases,” herecalls. “Our move to the medical school has complementedthis existing program.” PHRI played a central role in the awardfrom NIH for construction of a new building to house aRegional Biocontainment Laboratory with additional BSL3areas and more room for scientists to conduct pathogen relatedresearch.
In fact, Perlin describes the last few years here in Newark as“a fabulous experience” and credits the specialized facility aswell as innovative investigators, all determined to have animpact on the infectious and parasitic diseases that kill or dis-able millions of people each year. From using DNA to finger-print more than 21,000 strains of TB worldwide to inventingsimple probes for faster diagnosis of bacterial, fungal and certainviral infections, PHRI researchers are “focused on making animpact on disease,” Perlin says. Because of the current uncer-tainties in funding from NIH and other sources, “You need tobe daring, perhaps a little crazy and ahead of the scientificcurve.” PHRI grants and financial sources have been growingsince the move. The organization’s annual research budgetexceeds $12 million and is derived from grants as well as government, foundation and industry contracts. PHRI inven-
By Maryann B. Brinley

TOP: PETER BYRON; BOTTOM: JOHN EMERSON30 P U L S E S U M M E R 2 0 0 6
tions have resulted in more than $20 million of licensing rev-enue in the past 10 years.
Yet, back in early 2002, the picture wasn’t quite as clear andPerlin had one very big basic hurdle to overcome: transportingthose troublesome collections of bacteria, fungi, and infectiousmicro-organisms. “Even the freezers were a challenge. Funny,”he says, “but prior to 9–11, no one would have cared about usmoving these biological agents. It would have been just us, per-haps sitting in mid-town traffic. I would have been nervous, ofcourse,” but the environment after 9–11 changed everything.The New York City authorities didn’t want anyone, certainlynot the media, to know PHRI was relocating.
“By and large, preparing for that move was a nightmare fortwo months,” he recalls. To make arrangements, one of his firstcalls was to the Office of Emergency Management (OEM),which had been housed in the World Trade Center but was tem-porarily located at Pier 96 on the Hudson River. At a meetingPerlin won’t ever forget, there were “cops, cops and more cops”representing every law enforcement authority with any jurisdic-tion in the area, from the Metropolitan TransportationAuthority (MTA), to the New York City Police Department(NYPD), the New Jersey State Police, local New Jersey policedepartments, and the Port Authority police who controlled tun-nels and bridges.
“They had asked me to prepare a list of the pathogens wewould be taking and I put it in the center of the table,” hestates. Officials gathered around.
After a moment of silence, someone picked up the list,
looked at it and threw it back onto the table. “Not through mytunnel,” this guy announces.
“He was in charge of the Holland Tunnel,” Perlin recalls. Now in the comfort of his office, he can laugh a little but at
the time, tension mounted and heads started shaking from sideto side. To a chorus of “No way…no way…no way,” Perlinargued his case. “No one wanted the responsibility.”
Finally, the gentleman representing OEM declared, “We’renot leaving here today until we find a way to make this happen.We will come up with a solution.”
From there, the discussion took the PHRI pathogens on var-ious hypothetical routes through the city, even zig-zaggingthrough the streets, from the lower east side, up across theGeorge Washington Bridge and down the New Jersey bank ofthe Hudson.
“I was shaking my head to that suggestion, thinking, ‘Not agood idea,’” Perlin remembers. “Did we really want to be driv-ing these pathogens throughout the entire city?”
David Perlin, PhD

Ultimately, for three consecutive weeks in late February andearly March, 2002, on Wednesday nights from midnight to 4a.m., the research legacies of PHRI, housed in unplugged freez-ers, were loaded onto trucks, driven up First Avenue, across34th Street and through the Lincoln Tunnel. Accompanied byarmies of police convoys, PHRI movers were passed along pro-tectively from one jurisdictional authority to the next, all theway to UMDNJ campus police, who were wonderful, he says.“We had a two hour window before the freezers would start los-ing their temperature and would need to be plugged back in,”Perlin explains. “All kinds of simulations had been carried outto see what might happen and we also had dry ice along in caseof an emergency. But it was scary.”
There were two episodes that first night of moving that stillmake this specialist in fungal infections marvel about whatmight have happened. Though police had blocked off all crossstreets in Manhattan, a speeding van “going at least 100 milesan hour down Sixth Avenue,” raced past the roadblock and
through their caravan with the pathogen-loaded trucks. “Thatvan just missed my car by inches. Strewn pathogens could haveended up everywhere.” When they arrived at the tunnelentrance on the New York side, the PHRI crew was met by 50official vehicles with lights flashing and sirens going. Authoritieshad also sealed off the tunnel and blocked traffic for an hour.Later, when the movers reached their new headquarters andbegan plugging in the old as well as new freezers, all the “lightsand power in the building went out. One breaker after anotherwas getting tripped. Fortunately, we had an electrician therewho got us right back up.
“It was chaotic and harrowing, complicated and exciting,” hesays, but in the end, PHRI had made all the right moves incoming to UMDNJ. “Becoming part of the University and acore here on campus are real milestones, especially for our 65thanniversary as an institution.” �
� Founded in 1941 by New York City Mayor Fiorello LaGuardia, thePublic Health Research Institute (PHRI) was established as a non-profit organization to address public health issues facing the city.Currently, the Institute’s mission is to help eliminate worldwideinfectious disease threats.
� PHRI is one of only a few private research organizations whichconcentrate on infectious disease. Its 18 laboratories, each headedby a principal investigator, are staffed by approximately 85 scien-tists and support personnel.
� PHRI holds 26 NIH grants, and in the past year, scientists at theInstitute were co-investigators for three grants on TB and HIV fund-ed by the Bill and Melinda Gates Foundation.
� PHRI is one of the largest private tuberculosis research centers inthe U.S. with eight independent labs and 60 scientists working onall aspects of TB. In the past 10 years, it has obtained more than$50 million for TB research.
� Besides TB, PHRI researchers are studying vaccine candidates forHIV; biodefense; molecular epidemiology of hospital-acquired infec-tions; drug resistance in pathogenic bacteria and fungi; molecular-based rapid diagnostics; drug discovery, as well as fundamentalissues in biology.
� Under the PHRI umbrella are programs like the PHRI TB Center,the New Jersey Hospital Infections Program (with more than 45 par-ticipating hospitals) as well as clinical research operations in SouthAfrica and China.
� Working together, PHRI and NJMS led the grant initiative result-ing in a $21 million award from NIH to NJMS for the creation of theRegional Biocontainment Laboratory which is going up as an addi-tion to the International Center for Public Health (ICPH) building.
� In the history of modern medicine, PHRI people are everywhereand always in the frontlines battling epidemics of influenza, polio,malaria, rabies, tuberculosis, malignant cancers, as well as bacterialand viral infections. When asked to name names, PHRI DirectorDavid Perlin hardly knows where to begin but quickly mentions pastleaders like Jules Freund, an icon in immunology and winner of theLasker Award in 1957 who developed a simple test for rheumatoidarthritis, and Efraim Racker, “a legendary biochemist, who helpedbuild the field of bioenergetics and is considered one of the top sci-entists in the country in the 70s.” Sarah Ratner, a pioneering bio-chemist and one of only a few women in her generation elected tothe National Academy of Sciences, revolutionized studies of aminoacid metabolism and elucidated key features of the urea cycle.
Among others were: Eric Kandel, 2000 winner of the Nobel Prize forhis work on the biochemistry and physiology of memory, and RichardNovick, a newly elected member of the National Academy ofSciences, whose understanding of Staphylococcus aureus led him tothe characterization of toxic shock syndrome. For more backgroundon this institution and updates on the work of their current principalinvestigators, visit the website: http://www.phri.org.
The Story Behind PHRI
N E W J E R S E Y M E D I C A L S C H O O L 31

ALTHOUGH people with disabilitiesmake up about 20 percent of the
nation’s population, only a tiny fractionof medical school matriculants have dis-abilities. Why? First, let’s consider somerelevant history from the AAMC itself.
In 1997, AAMC President Jordan J.Cohen, MD, issued a moral charge tothe medical profession. Writing inAcademic Medicine, he called for “activesteps to ensure that our health care practitioner community mirrors society’sgender, racial, and ethnic mix.” In amore recent essay, in the June 2004AAMC Reporter, Cohen expanded thescope of the issue beyond considerationsof race, ethnicity, and gender to includedisability.
“Technological advances have made ahost of things possible, both in medi-cine and in virtually every other walk oflife, that were way beyond many peo-ple’s abilities not so long ago,” Cohenobserved. “Compelling examples ofindividuals, albeit still relatively few innumber, with mobility, auditory, and
visual disabilities who are valued mem-bers of the profession argue that it’s timeto reconsider our traditional, oftenstereotypic, view of what it takes to be acapable doctor.”
Significantly, the recently released andwidely supported “Compact BetweenResident Physicians and Their Teachers,”drafted by the AAMC, also includes thedisability issue. Among 10 faculty com-mitments in the document is this one:“We will demonstrate respect for all resi-dents as individuals, without regard togender, race, national origin, religion,disability, or sexual orientation.”
So why don’t we have more physi-cians with disabilities? In my experience,no American medical school has a “wel-come sign” for individuals with physicaldisabilities. We need to do much more.
In an article in the January 2005American Journal of Physical Medicine &Rehabilitation, I discussed the need toreassess our policies regarding physicianswith disabilities and the physician work-force and made recommendations to the
AAMC on how current policies couldbe changed to achieve this goal. I arguedthat medical schools’ core competenciesand technical standards have not keptpace with technological changes, diversespecialization, and changing practiceoptions.
A recent AAMC publication,“Medical Students With Disabilities: AGeneration of Practice,” offers the med-ical education community a practicalguide for furthering its work with stu-dents with disabilities. But I believe thatsome of the report’s analysis and recom-mendations carry a negative and less-than-constructive tone. I am especiallyconcerned about language meant toguide universities in their treatment ofstudents with disabilities that could bebetter categorized as a guide to keepphysically disabled applicants out.
One key issue concerns the so-calledundifferentiated curriculum versus theundifferentiated student. I favor theundifferentiated curriculum.
Medical specialization has segmented
32
V O I C E S
P U L S E S U M M E R 2 0 0 6
JOEL DELISA, MD, MSProfessor and Chair, Physical Medicine and RehabilitationPresident and CEO, Kessler Medical Rehabilitation Research and Education Corp.
Physicians With Disabilities:Why Aren’t There More of Them?
PETER BYRON

N E W J E R S E Y M E D I C A L S C H O O LCOMSTOCK
the physician workforce—from a morehomogenous group into one concentrat-ing on specific body systems or diseaseentities. That is the reality of practice inthe United States. My view is that sig-nificant differentiation of physiciansinto various specialties and subspecial-ties can serve as an argument for lessrigidity in demanding that all studentsdemonstrate competence in proceduresthat are not relevant to their expectedpractices.
The undifferentiated curriculumwould allow students to meet compe-tency requirements through multipleoptions, even including the role ofphysician extender, or mid-level healthcare provider. But I absolutely opposeusing a tracking system, in which some-one is admitted to medical school underthe presumption that he or she will bedesignated to a specific postgraduatespecialty. Each student must be handledon a case-by-case basis. The residentinterviews by each specialty can handlethat issue.
Clearly, admitting someone with aphysical disability to medical school iscontroversial. In training competentphysicians, we must protect both thewell-being of all patients and the rightsof all trainees. All medical students musthave the appropriate intellectual capaci-ty, ethical attitude, humanistic qualities,and desire to become doctors.
At the same time, we must respectcreative solutions that people with dis-abilities often employ to perform tasksin alternate ways. The ability to performthe task at a defined level of qualityshould be emphasized, rather than theprocess by which the task is accom-plished. We need to be flexible and con-sider what is possible through hard workand the use of technology.
The need for program modificationsand reasonable accommodations differsfor students, residents, and facultymembers. A student’s focus is on educa-
tional requirements and on meeting thediverse demands of the basic sciencesand clinical years. Faculty members withdisabilities tailor their practices to mini-mize the need for accommodations, andorganized medicine accepts and readilysupports this.
Residency, however, is truly a mixtureof service and education, and it offersperhaps the greatest challenges in termsof disability considerations. Residentsmay need to perform certain servicesessential to their residency program thatare not necessary for students or faculty
members. Even within a specialty, notall programs have the same “service”requirements. Should this work obliga-tion be a barrier to satisfactory comple-tion of residency training?
These issues must be studied; theywill not go away. If diversity is an essen-tial goal, as it should be, we must workto reach it. Otherwise, it could be saidthat we, as medical educators, are partof the problem.
Editor’s Note: This article first appearedin the AAMC Reporter (February 2006).
33
Compelling examples of individuals, albeit still relatively
few in number, with mobility, auditory, and visual
disabilities who are valued members of the profession
argue that it’s time to reconsider our traditional,often stereotypic, view of what it takes to be a capable doctor.

NewJerseyMedicalSchool alumnifocus
TOP: MFXINC.COM; BOTTOM: MELISSA CAMPBELL34 P U L S E S U M M E R 2 0 0 6
T HE Alumni Association has just signed a contractwith the eBay “iSOLD It” stores, which are in
numerous locations throughout New Jersey. This willallow anyone to bring any saleable item into the eBaystore, asking that the proceeds of the sale be donated tothe Alumni Association for either stem cell research/edu-cation or the General Fund. You will get a tax donationcredit for the full sale price from the Alumni Associa-tion. I expect this to be a very beneficial fundraisingentity for the Alumni Association; it will allow us toclean out all the junk we are never going to use and helpthose who need it. This is the first time this has everbeen attempted by an alumni association and I wouldappreciate your support. To find your nearest drop-offlocation, go to www.i-soldit.com/locations.asp.
Having already mentioned stem cell research, theAlumni Association has “adopted” the Student Societyfor Stem Cell Research, an organization comprised ofour medical students who are interested in stem cellresearch and education. Two members have recentlyreturned from the national meeting in California, repre-senting the New Jersey Medical School Chapter. Themission of this organization is to assist the population ofthe State of New Jersey on an unbiased educationalquest on the topics of embryonic and adult stem cellresearch, and to remove the mystery and false beliefswhich affect public opinion.
Since our mission is to build on the quality educationwe have received at New Jersey Medical School, I feelthis is a perfect match for both organizations.
Stay positive and keep donating.
M ORE than 150 students attended the AlumniAssociation’s career nights on March 6 and 8. Many of
them postponed studying for a critical exam so they couldtake advantage of the popular event.
Alumni and faculty physicians participated in a panel dis-cussion, fielding questions about work-life balance, repaymentof student loans and the importance of research experience.
Many of the panelists were non-traditional students:Barbara-Ann Britten, MD’97, entered medical school at theage of 46; Peter Wenger, MD’89, played the saxophone for 15years before starting medical school; and Joseph DiTrolio, MD’79, president of the Alumni Association, worked on fiberoptics at NASA before becoming a urologist. Some of hisNASA patents are the basis for fiber optic scopes used in thepractice of urology.
On the question of work-life balance, panelists were mostpassionate. “You can structure your life any way you want,”said Bruce DeCotiis, MD’75, who has five children, coachedcross country for many years and runs a successful allergy andimmunology practice in Belmar, NJ.
“You can set your own life,”said Gerson Weiss, MD,chair of the NJMSDepartment ofObstetrics, Gyncologyand Women’s Health.He implored studentsto adopt the ‘fun prin-ciple,’ saying “If youare good at something,you’ll enjoy it. If youenjoy it, you’ll do it well.”
DiTrolio echoed that senti-ment: “When you are doing some-thing you love, it doesn’t feel like work.”
After the panel discussion, students had informal discus-sions with alumni. Thirty specialties were represented.
Mark Bobbin, a second-year student who is interested inradiology, appreciated that alumni took the time to share theirexperiences. “We don’t get many opportunities to investigatevarious specialties in the first and second year, so this was avaluable experience for me.” �
Alumni Physicians ShareCareer Insights with Students
A Messagefrom thePresident
Joseph V. DiTrolio, MD’79

N E W J E R S E Y M E D I C A L S C H O O LA.J. SUNDSTROM 35
News of special interest to NJMS graduates
M ORE than 400 New Jersey Medical School students and alumni gathered onApril 1 for a joint celebration to mark reunion milestones and excellence in
teaching. Members of the classes of 1961, 1971, 1976, 1986, 1991, 1996 and 2001enjoyed a dinner-dance with current students who convened to honor their favoriteteachers with Golden Apple awards.
Alumni came from as far away as Arizona to re-connect with classmates and enjoyan Oscar-themed awards ceremony complete with a red carpet and student ushers forawardees. Sponsored by the NJMS Student Council, the Golden Apple awards recog-nize professors who demonstrate a particular commitment to teaching. Students fromeach class nominate faculty whom they deem deserving of the award; third- andfourth-year students also recognize the teaching efforts of residents. In all, 19 GoldenApple awards were presented.
In addition, the Alumni Association presented Suzanne Atkin, MD’79, UniversityHospital Chief of Staff, with the Charles L. Brown Award; Dennis Quinlan, Sr., MD’69, associate professor, NJMS Department of Medicine, with the DistinguishedProfessor Award; and Lester Lieberman of The Healthcare Foundation of New Jerseywith the Honorary Alumnus Award. �
Calling All Classmates, Past and Present
Thursday, September 14Board of Trustees MeetingRosemary Gellene Room, MSB B515
6:00 p.m.
Thursday, October 12Executive Committee MeetingStudent Affairs Conference Room
MSB C–654
6:00 p.m.
Thursday, November 2Scholarship Awards Dinner The Grand Foyer
Medical Science Building
6:00 p.m.
Saturday, March 31, 2007Alumni Reunion /Golden Apple Dinner DanceThe Sheraton Hotel, Parsippany, NJ
1. Assistant Registrar Heidi Schwalb is escorteddown the red carpet by student usher JamesFlynn’08.
2. Members of the class of 1981 Drs. SusanMorrison and Barbara Nahas, standing, and Drs.Barry Prystowsky and Robert Melis, seated, enjoycatching up.
3. From left, Drs. Robert L. Johnson’72, InterimDean, Dennis P. Quinlan, Sr.’69, recipient of theDistinguished Professor Award, and SuzanneAtkin’79, recipient of the Charles L. BrownAward, are congratulated by Alumni AssociationPresident Joseph V. DiTrolio, MD’79.
alumni calendar
Above: Reminiscing are members of the 45thAnniversary Class of 1961. From left, Drs. JohnWrable, Vincent Napoliello, Charles Dooley andRobert Chernaik.
1
2
3

alumnifocus P R O F I L E
36 P U L S E S U M M E R 2 0 0 6
Deborah Bessen, MD’99, is one of agrowing number of physicians across thecountry changing the dynamic of thedoctor/patient relationship by taking hervirtual office to the patient.
Bessen practices family medicinethrough Visiting Physician Services, aNew Jersey-based physician group thatspecializes in old fashioned house calls.She sees approximately 30 patients aweek—substantially fewer than a doctorin a typical practice, but enjoys thelighter case load because it allows her tospend more time with her patients.“Large offices lose the social aspect thata family doctor provides,” she explains.“I like that I can visit my patients intheir surroundings, where they are mostcomfortable. This allows me to witnessfamily dynamics and how it influencescare.”
Bessen explains that the majority ofservices a physician provides from theoffice can also be performed at home. “Idraw blood, give cortisone injections ororder in-home X-rays and EKGs,” sheexplains. “Through my connections witharea medical personnel, I can refer my
Deborah Bessen, MD’99
Deborah Bessen, MD, consults with one ofher patients during a house call.
Beyond The Black Bag
REMEMBER the “good old days” when doctors made house
calls? When physicians like Marcus Welby, MD, took their
black bags on the road and cared for sick patients in
their homes? In that early 1970s television show, Welby’s patients
never had to wait in a doctor’s office, impatiently turning magazine
pages and wondering if the nurse was ever going to call their names.
By Jill Spotz
PETER BYRON

N E W J E R S E Y M E D I C A L S C H O O L 37
patient to a podiatrist who also performshouse calls, or contact a company tocoordinate oxygen therapy in the home.”
The majority of Bessen’s patients areelderly and/or home-bound withdementia, arthritis, Parkinson’s disease,multiple sclerosis and advanced chronicobstructive pulmonary disease. “Severalof my patients hadn’t seen a doctor inyears because they had various illnessespreventing them from doing so,” sheexplains. “Or they were wheelchair-bound and had to rely on ambulancetransportation to take them to an emer-gency room. It is a great challenge formany families and caregivers to trans-port loved ones who are bedridden to adoctor’s office.”
According to research published inThe Journal of the American MedicalAssociation, the number of Medicarebeneficiaries receiving medical care athome has been rising since 1998. In2004, Medicare reimbursed approxi-mately 2 million home visits. Why the
increase? “Because our elderly populationis growing,” explains Bessen. “Plus wehave begun to realize the limitations ofhospitals. In certain instances, it is morepractical for patients to be cared for intheir homes. My patients with dementiafeel safe in their environment and aremore likely to follow my plan of care.”
The positive aspects of home-care areendless: reduced hospital stays, whichare less taxing on the healthcare system;a more dignified and comfortable end-of-life situation for elderly patients; andmajor financial benefits, to name a few.
Bessen explains that herpatients also have a high-er compliance rate fortaking their medications.“I search the home forclues as to why they arenot taking their medica-tions and get to the rootof the problem,” sheexplains.
With an average driv-ing distance of 40 to 50miles a day, Bessen pre-dominantly sees patientsin central and northernNew Jersey. When askedwhat makes a house-callsdoctor different, sheexplains, “We do nothave the same limitationsas physicians operating ina typical practice. Whencaring for a patient in hishome, I am able to seethe whole story—the
pictures on the walls, the interactionwith family members, and the quality oflife. When a patient says to me ‘Dr.Bessen I can’t figure out why I am notlosing weight,’ I don’t just look at thechart. I open the refrigerator and tellthem why.”
Bessen and her husband, who bothgraduated from New Jersey MedicalSchool in 1999, were the first marriedcouple admitted to the school. Theirfirst child was 16 months old when theystarted and they had their second babyduring their third year of study. “It was
very difficult,” she admits. “We bothtook a year off consecutively to care forour small children but were able tograduate together.” Bessen completedher residency at Overlook FamilyPractice and wanted to maintain a flexi-ble schedule. The position with VisitingPhysician Services was a perfect match.
Bessen credits her alma mater withpreparing her to be a competent physi-cian. “We received a hands-on educationand were able to work with patients—not just observe the attending physicians.Even now I will remember a certain lecture or class and how it applies to acurrent situation. I use what I learned inmedical school every day.” �
Bessen lives in Montclair with her husband and two children.
“When caring for a patient in his home, I am able to see thewhole story—the pictures on the walls, the interaction with family
members, and the quality of life.”

alumnifocus C L A S S N O T E S
1960Daniel D. Cowell, MD, has beenpromoted to senior associate deanfor graduate medical education atthe Joan C. Edwards School ofMedicine at Marshall University inHuntington, WV.
1964Robert A. Orlando, MD, PhD,has retired as chair of the patholo-gy department at Beverly Hospitalin California, but is continuing asdirector of their laboratories. Healso plays the trumpet with the LosAngeles Doctors Symphony, theUniversity of Southern CaliforniaConcert Orchestra, and partici-pates in various studio projects.
1968James (Jay) Phelan, MD, retiredfrom the Navy in September 2005and commutes between his work atNASA in Houston, TX, and hishome in Hoover, AL.
1971John Penek, MD, has been namedmedical director of the ChiltonMemorial Hospital Sleep DisordersCenter in Pompton Plains, NJ.
Richard Weyer, MD, writes aboutthe accomplishments of his threechildren. His son Chris will gradu-ate in June 2006 from KirksvilleCollege of Osteopathic Medicinein MO, where he was elected toWho’s Who Among MedicalStudents. His daughter Elizabethgraduated from NorthwesternUniversity in 2004 and now worksin NY. His daughter Allisonattends Seton Hall Law School.
1972Thomas Dayspring, MD, FACP,became a diplomate of theAmerican Board of ClinicalLipidology in December 2005.He is a board member of theNortheast Chapter of the NationalLipid Association (NLA). In April
2006, Dr. Dayspring presented alecture on high density lipoproteinbiology and function at the nation-al meeting of the NLA in Boston.
1976Stuart Shoengold, MD, is directorof the division of urology at SaintBarnabas Medical Center andNewark Beth Israel Medical Centerin NJ.
1977Stephen C. Blank, MD, plans tointroduce the first shoe developedfor pregnant women this year.
Toni H. Field, MD, is working atthe Harlem Health Center, one offour clinics providing primaryhealthcare to Hotel Trade Councilmembers in New York. Dr. Field isan internist specializing in primaryand urgent care.
Rhonda R. Nichols, MD,resigned in January 2005 fromJersey City Medical Center whereshe held the posts of chair, vicepresident, president of the med-ical/dental staff and executivedirector of the faculty practice.She is now in private practice inMillburn, NJ.
1982Louis E. Rios, Jr, MD, is com-pleting his MPH with an emphasison bioterrorism/biodefense/syn-dromic surveillance. He resides inOrange Park, FL.
1985Russell Rentler, MD, has retiredfrom the practice of medicine andis now pursuing his passion—music. He works part time at ahospital in NJ, writes folk musicand has recorded four CDs. Dr.Rentler also volunteers annually ata clinic in Port-au-Prince, Haiti,treating patients with malnutrition,malaria, tuberculosis, worms andinfections caused by starvation.
1986Lawrence M. Fox, MD, is a cap-tain in the U.S. Public HealthService, responsible for respondingto natural and man-made disasters.His next site visit will be toCambodia.
Kathy Ann Irish-Benjamin, MD,has joined the medical staff of thepediatric department at the RomeMemorial Hospital in Rome, NY.
Kevin Lavery, MD, practices ophthalmology in Battle Creek,MI, and has performed eye surgeryin Cuba, China, India, Bangladesh,Peru, Kyrgyzstan, Ethiopia andLibya as a volunteer with Orbis.This is a New York-based world-wide charity organization dedicat-ed to restoring sight and prevent-ing blindness for people in developing countries.
38 P U L S E S U M M E R 2 0 0 6
The Alumni Association extends our deepest sympathy to the familiesand friends of our alumni who have passed away.
Joseph Edwards, MD’74, died on March 17, 2006. Dr. Edwards, astaff surgeon at St. Peter’s University Hospital and Robert WoodJohnson University Hospital at Rahway, maintained a general prac-tice in South Plainfield, NJ. He is survived by his wife Rhona, sonsSteven and Michael, daughters Lisa Scheiner and Jennifer Friedman,brother Frank and four grandchildren.
Michael C. McDonough, MD’82, a pulmonary and critical carespecialist, passed away on April 28, 2006. Dr. McDonough prac-ticed in Bayonne for many years and was the pulmonary director ofthe Lung Transplant Program at Newark Beth Israel Medical Center.He is survived by his son Michael, daughter Allison, his motherSophie McDonough, and a sister Michele Barone.
Frank V. Mignogna, MD’65, passed away on May 29, 2006. Dr.Mignogna was a head and neck surgeon, practicing in Harrison,NY. He is survived by his wife Holly, children James, Lisa andAnthony and two grandchildren.
Ida Marie Onorato, MD’73, passed away on May 31, 2006 inAtlanta, GA. She is survived by her husband, Robert S. Janssen, MD,brother Vincent Alfait, PhD, niece Fione Alfait, and stepchildrenJulia and Kevin Janssen. Dr. Onorato was the Deputy AssociateDirector for Science at the National Center for HIV, STD and TBPrevention at the CDC. In 2002, UMDNJ honored her with aDistinguished Alumnus Award for “highly regarded infectious diseaseresearch that has made significant contributions, particularly in thefields of HIV/AIDS and multi-drug resistant tuberculosis.”
Lawrence J. Pizzo, MD’59, of Mahwah, NJ, died on February 8,2006. An otolaryngologist, Dr. Pizzo was one of the founders of theWayne Surgical Center and president of the Advanced PracticeSystems and Advanced Surgical Arts. He was a past president of themedical and dental staff and chairman of the same-day/outpatientsurgery unit at Chilton Memorial Hospital. Dr. Pizzo is survived byhis wife Vita, children Christopher, Jenna and Megan, his motherLouise Pizzo and one grandchild.
I n M e m o r i a m

1987Fred A. Caruso, MD, practicespediatric radiology at Cape FearValley Medical Center, Fayetteville,NC, where Gene Finch, MD,practices pediatric preventive care.
Philip Chaikin, MD, is executivevice president for development andinternational development andhead of Kyowa Pharmaceuticals,Inc. in Princeton, NJ.
Jean DeMarchis Tabin, MD,writes that she has relocated toPark City, UT.
1990Maria Millan, MD, is the director,Liver Cell Transplant Program atStemCells, Inc. in Palo Alto, CA.Upon completion of her work withStemCells, Dr. Millan plans toreturn to her position as associateprofessor of surgery, Division ofMulti-Organ Transplant, and direc-tor, Pediatric Transplant Programs,Kidney & Liver, at StanfordUniversity School of Medicine.
Felix Dailey Sterling, MD, is thedirector of the cardiac catheteriza-tion lab at St. Michaels MedicalCenter and the MeadowlandsHospital in NJ. He is board certi-fied in internal medicine, cardiologyand interventional cardiology. Dr.Sterling and his wife Karen Sterling,MD’95, have three children.
1991John R. Patterson, MD, practicesin Virginia Beach, VA, and isamong the small number of doc-tors who make house calls. Dr.Patterson practices family andholistic medicine, working out ofhis home office.
Gregory Swank, MD, FACS, aplastic surgeon, has joined themedical staff of Frye RegionalMedical Center in Hickory, NC.
1993Randeep Kahlon, MD, receivedthe Annual Young Physician Awardat the 216th annual meeting of theMedical Society of Delaware. Dr.Kahlon is a partner of First StateOrthopaedics and was chosen forhis leadership and service tonumerous state and national med-ical organizations and boards. Hehelped to establish the OrthopaedicTrauma Service at ChristianaCarein DE and is noted for performingthe first-ever carbon finger jointreplacement in his state.
1995Eugenio Rocksmith, MD, is aneurologist at the RehabilitationHospital of South Jersey, workingwith stroke and brain injurypatients as well as patients withParkinson’s disease and multiplesclerosis.
1996Debbie Salas-Lopez, MD, MPH,assistant professor and chief,Division of Academic Medicine,Geriatrics and CommunityPrograms, Department ofMedicine, NJMS, recently present-ed “Developing and ImplementingCultural Competency Curricula forAcademic Health Centers” at theGreater New York HospitalAssociation Best Practices Forumon Cultural Competency Trainingfor residents in New York City.
1998Mary Cantey, MD, MA, assistantprofessor, Department ofMedicine, NJMS, recently present-ed “Transitioning Young Peoplewith Special Health Care Needsfrom Pediatric to Adult HealthCare” at the 103rd AnnualConvention and ScientificAssembly of the National MedicalAssociation in New York City.
Winifred Fong, MD, has returnedto the state as a faculty member at
Robert Wood Johnson UniversityHospital’s Department ofEmergency Medicine.
Katharine O’Connell, MD,MPH, was married on April 2,2006, to Chad Scott White. Dr.O’Connell is an assistant clinicalprofessor of obstetrics and gynecol-ogy at the Columbia College ofPhysicians and Surgeons in NewYork.
Sanjay Ramchandani, MD,completed his obstetrics and gyne-cology residency at TempleUniversity Hospital inPhiladelphia, PA, where hereceived several awards for excel-lence in teaching and research andwas written up in the CorpusChristi Caller-Times (Texas).
Benjamin Rudin, MD, who practices internal medicine andpediatrics, is a member of the med-ical staff of North Adams RegionalHospital and has joined Adamsinternists in Adams, MA.
2001William Schafranek, MD, andwife Mila announce the birth oftheir second son in November2005.
2002Prashant A. Patel, MD, is currently a CA3 anesthesiology resident at New York PresbyterianMedical Center -ColumbiaCampus, where she will remain fora pain management fellowship forthe academic year 2006 –2007.
Stay in Touch!You are important to us, and we would like to hear from you. Mail thisform to: Alumni Association of New Jersey Medical School, 185 SouthOrange Avenue, P.O. Box 1709, MSB-B504, Newark, NJ 07101–1709.Photos are welcome. You can also send your news via e-mail to: [email protected] or fax us at 973-972-2251.
Name Graduation Year
Home Phone Office Fax
E-Mail Address
Mailing Address
What I Have Been Doing (enclose photos)
I would like to be a representative for my class.
Please join the Alumni Association of New Jersey Medical School.
General Dues $50.00Resident in Training $15.00Lifetime Membership $1,000.00
Visit http://njms.umdnj.edu/, click on Alumni and Alumni Associationand then Online Dues Payment to pay your dues online.
The Lifetime Membership is being offered to our alumni as a means toperpetuate the goals of the Alumni Association and enable its membersto sustain their support in a more meaningful way. All categories ofmembership will afford you the opportunity to keep connected with us.You will continue to receive all membership benefits, including NJMSPulse magazine, information about upcoming events and reunions, andlibrary privileges.
N E W J E R S E Y M E D I C A L S C H O O L 39
http://www.umdnj.edu/njalmweb/

40
F O C U S O N P H I L A N T H R O P Y
P U L S E S U M M E R 2 0 0 6
WHEN Thomas Infusinoannounced his retirement as
chairman and CEO of Wakefern FoodCorporation—owner of the ShopRitesupermarket name and supplier of itsstores—he had no idea this would pro-vide a springboard to future scientificdiscoveries.
A native of Irvington, NJ, Infusinoopened his first grocery store in Newarkin 1945. He joined Wakefern in 1953,was elected to its board of directors in1959 and became its chairman in 1971.
As a tribute to him, Wakefern boardmembers presented Infusino with anendowed chair of his choosing at NJMS.After a challenging selection process, hechose Andrew Thomas, PhD, professorand chair of the NJMS Department ofPharmacology and Physiology since1997, and an internationally recognizedexpert on the hormonal regulation ofmetabolism. Thomas, who has publishedmore than 140 papers, was professor ofpathology, anatomy and cell biology atThomas Jefferson University before com-ing to the medical school.
During his tenure as chair, his depart-
ment’s research funding has increasedfrom $1 million in 1997 to more than$6 million today. He also recruited 12new faculty members into the Pharma-cology and Physiology department.
Thomas serves on several journal editorial boards and grant review panels,and chairs an NIH special emphasispanel on post-baccalaureate research
education for minority students. He hasbeen a regular consultant for theNational Institute of Alcohol Abuse andAlcoholism at the NIH, and is a leadingauthority on calcium signaling, the regu-lation of metabolism, and alcoholic heartand liver disease.
For the next five years, the EndowedChair will provide for the appointmentof a junior faculty member to further theresearcher’s work, with a new focus onmetabolic sensing in the brain. In addi-tion, each year a clinical resident fromone of the medical or surgical specialtieswill be appointed to the Thomas P.Infusino Clinical Research Fellowship,allowing the fellow to focus solely onbasic science research in the areas ofmetabolic sensing and cardiovascular dis-ease for one year. Funds will also be pro-vided for an annual lecture by a leadingscientific figure whose work is related tothis research.
Metabolic sensing in the brain plays acritical role in the regulation of appetiteand eating behavior; a dysfunctional system can lead to diabetes and obesity.Research in metabolic disorders may leadto new treatments for these conditions.—MELISSA CAMPBELL
Thomas Infusino (left) and Andrew Thomas, PhD
Gift Provides Food for Thought
Brotherly LoveSEVERAL YEARS AGO, Richard Pozen,
MD’74 (top right in yearbook photo)established a scholarship honoring his olderbrother, Michael, MD’70 (below), who died inhis early 30s. Recently, Dr. Pozen endowedthe fund, so that it will be a permanent lega-cy at their alma mater, benefiting future gen-erations of talented medical students.
He says: “I’m thankful to New Jersey Medical School for giving me the opportunity to achieve. I donate as a way to givesomething back to the organization that gave me my start.”
For information about creating a legacy scholarship, pleasecontact Elizabeth Ketterlinus at the Foundation of UMDNJ, 973-972-2486, toll-free at 866-44-UMDNJ, or via the internet to [email protected].
TOP: COURTESY OF WAKEFERN

That you can make a difference in findingreal cures, educating new healthcare
professionals, and improving patient care.
That you can choose the specific area ofmedical research, education or healthcareyou wish to support.
That 100% of the dollars you contribute go directly to the program you wish
to sponsor, with no administrative fees diluting their power.
That your generosity will work miracles forso many people right here in New Jersey.
Now, imagine how fulfilling it would be if your donation could do all of
these things. Through the Foundation of UMDNJ it can, by funding research,
education and patient care programs atthe UMDNJ-New Jersey Medical School.
For more information, call Elizabeth Ketterlinus, vice president of
development, toll-free at 866-44-UMDNJ,or visit us at www.umdnj.edu/foundation.
NEWARK, NEW BRUNSWICK, STRATFORD
Imagine the differenceyou can make
UMD165_pulseadkid8.312x11.125v3.qxd 6/2/06 11:41 AM Page 1
University of Medicine and Dentistry of New JerseyNew Jersey Medical School185 South Orange AvenueP.O. Box 1709Newark, New Jersey 07101–1709
http://njms.umdnj.edu
Non-profit OrganizationU.S. Postage
PA I DPermit No. 5287
Newark, New Jersey
Made of O-gauge die-cast metal, the Rapid
Surgical Response Train has 8 curved tracks, 8
straight tracks, steam locomotive, coal car, NJMS
medical supplies boxcar, helicopter, caboose and
transformer. The accessory car is an operational
handcar on a depressed flat car.
Special Package Deal—Train PLUS New Accessory Car
$350 includes shipping
Accessory Car ONLY (for those who already own the train)
$75 plus shipping
To order, call 973-972-6864 (outside NJ call 800-477-7040) or email [email protected] support student scholarships and programming.