Financial Success with PDPM - VHCA · Rule during the May 1 Skilled Nursing Facility/Long-term Care...
57
Financial Success with PDPM Sam Phillips, CPA, MBA, RAC-CT WALKER-PHILLIPS HEALTHCARE CONSULTING
Transcript of Financial Success with PDPM - VHCA · Rule during the May 1 Skilled Nursing Facility/Long-term Care...

Financial Success with PDPM
Sam Phillips, CPA, MBA, RAC-CT
WALKER-PHILLIPSHEALTHCARE CONSULTING

2 On July 31, 2018, the Centers for Medicare and Medicaid Services (CMS)
published the Prospective Payment System (PPS) and Consolidated Billing for Skilled Nursing Facilities (SNF) final rule for FY19.
In this rule, CMS finalized a proposal to replace the current SNF PPS payment model with a new per-diem payment system called the Patient-Driven Payment Model (PDPM).
The first all-new SNF Medicare reimbursement system change in 20 years
PDPM attempts to unwind the unintended consequence of the current SNF case-mix methodology (RUG-IV) that encourages treatment to payment incentive, largely driven by rehab minutes. The “big stick” approach to SNF care redesign
Overhaul seeks to more accurately define the medical services a patient needs, rather than lumping the patient in one of 66 different payment buckets.
PDPM system moves in the direction of a patient-centered approach over a services-rendered approach.
PDPM rates are set according to the complexity of a condition instead of the number of therapy minutes a patient receives. Therapy minutes driving reimbursement will be a thing of the past.
What is PDPM?

Patient-Driven Payment Model (PDPM) Basics 3
It is hoped that PDPM will shift Medicare payments from volume to value.
CMS’ intended goal is to eliminate counting therapy minutes as primary reimbursement driver.
Takes effect on October 1, 2019 with no transition (unlike transition to PPS 20 years ago).
Retains per diem methodology as under PPS (not an episode-based payment).
OCT
1
24

Patient-Driven Payment Model (PDPM) Basics 4
This pattern implies that more than half of Medicare Part A days utilized only a patients therapy minutes and Activities of Daily Living (ADL) scores to determine payment.
During FY17, of the 66 possible RUG classifications,
90%over
Over 90% of the Medicare Part A days were billed using one
of the 23 Rehabilitation RUGs.
Over 60% of the FY17 Medicare Part A days were billed
using an Ultra-High category.
60%over
23 Rehabilitation RUGs Ultra-High category

Patient-Driven Payment Model (PDPM) Basics 5
Skilled nursing facilities should save approximately $2 billion in aggregate reduced administrative costs over the next 10 years ($12,000 and 183 hours in savings per provider annually).
- Officials with the Centers for Medicare & Medicaid Services (CMS) in a review of key aspects of the Fiscal Year (FY) 2019 SNF PPS Proposed Rule during the May 1 Skilled Nursing Facility/Long-term Care Open Door Forum.
PDPM creates a separate component for non-therapy ancillaries (NTA) Makes caring for medically
complex residents more attractive
3x rate for 1st 3 days – not sure this should be viewed as “Rate Tapering”
3x rate helps in covering the high pharmacy costs associated with the first few days of new admissions.
Only source of savings sited by CMS is related to MDS
No mention of reduced rehab costs (yet this appears to have been CMS’ focus?).
Other items could add cost: ICD-10 coding training and
hiring Interim Payment
Assessments - (IPA) are now optional / Very BIG deal and gift to SNFs

Patient-Driven Payment Model (PDPM) Benefits 6
The new PDPM payment methodology will encourage shorter Medicare stays due to “Rate Tapering” (We are not convinced of this, more tapering may be occurring under PPS – example to follow).
PDPM should be an improvement over the current RUG-IV classification since payments will be predominantly based on clinical characteristics rather than therapy minutes.
Virginia SNF providers are estimated to benefit by this transition (+2.4% or $16.3M based on Medicare FY17 data).
**This implies NO change in provider behavior adapting to PDPM.
Virginia SNFs will likely benefit by PDPM due to their lower Ultra-High Therapy utilization, as compared to national averages.
It is believed that therapy minutes may not be driven so much from the patient’s individual characteristics, but rather from the amount of therapy the SNF and rehab group decide to provide to the patient.

Why PDPM Success is so Important to SNFs? 7
Medicare Part A Patients
make up a small percentage of
days but almost all the profits.
FY16 marginal profit, a measure of the relative attractiveness of treating Medicare fee-for-service
(FFS) beneficiaries, was at least 19.6% for
freestanding facilities (96% of SNFs.)
The average non-Medicare margin (all non-Medicare FFS SNF patients) was -2.3%.
Medicare’smedian payment
per day was $470 (so average profit was
approximately $92 ppd.)
Medicare FFS beneficiary staysconstituted 11% of
total facility days but accounted for
20% of facility revenue.
SNF admissions and stays continue to decrease/
(MedPAC | Report to Congress: Medicare Payment Policy | March 2018)
19.6
% -2.3%
$470 11%(FY16 Covered
days per admission:
25.7)

Patient-Driven Payment Model (PDPM) Assessments 8
PDPM requires only 2 assessments. Eliminates 14, 30, 60, 90- day scheduled assessments –OMRAS (SOT, COT, EOT) or unscheduled assessments
What is the final assessment going to be used for if it does not drive payment?
Confirm facilities really were providing more therapy than needed (compliance audits of prior years)?
Data collection for future Medicare rate adjustments, most likely reductions?
Did we just leave a lot of rope on the floor?
2assessments

Patient-Driven Payment Model (PDPM) Assessments 9
We stated in the proposed rule (83 FR 21065) that, given that the RCS–I model and PDPM both present the potential for providers to reduce significantly the amount of therapy provided to SNF residents as compared to RUG–IV, we believe that the same potential result may occur under the proposed PDPM as commenters identified with RCS–I. To better track therapy utilization under PDPM, and to better ensure that residents continue to receive an appropriate amount of therapy commensurate with their needs, given the reduction in the frequency of resident assessments required under the proposed PDPM, we proposed to add therapy collection items to the PPS Discharge assessment and to require providers to complete these items beginning October 1, 2019, in conjunction with the proposed implementation of the PDPM.
Federal Register /Vol. 83, No. 153/Wednesday, August 8, 2018/Rules and Regulations

Interim Payment Assessments (IPAs) 10
BIG reimbursement opportunity IPAs are much like the current Significant Change but with only
the upside (if measured appropriately). Will there be any IPAs that reduce payments? Probably not.
IPAs are a “gift” from CMS and could be required for all significant changes in the future.
Your MDS team needs to be very in-tune with each patient and know what events could trigger an IPA that would increase payments.
IPAs reset patient classification but not tapering.
Develop an “IPA Checklist” for floor staff.

Lessons From The Transition to PPS 11
CMS makes changes when they want the industry to make a change in behavior.
PPS was developed to control escalating SNF costs in the 1990s under the prior cost-based system.
Then… CMS blames SNFs for behaving in the manner SNFs are financially rewarded for (i.e., delivering the most possible therapy because SNFs are financially incentivized to do so).
SNFs, that prepared for PPS, were nimble (very important), changed their practices, and were much better off financially with PPS than with the prior cost-based system.
SNFs, particularly the large for-profit public chains with high fixed costs, could not adapt fast enough which caused massive bankruptcies in the industry.
If history is an indicator, we have 2 – 4 years to thrive and adapt under PDPM before CMS will likely have good measurements and will then make adjustments to minimize profits (i.e., start requiring IPAs for all significant resident changes whether good or bad for reimbursement, freeze payments, ect.).

Winners Under PDPM
The new PDPM reimbursement system moves our industry away from paying providers by the therapy minutes provided. Instead, CMS will reward SNFs that serve the patients with more complex medical needs and higher non-rehab expenses.
12
Patients - With bigger incentives for low hospital readmission rates, facilities will focus more on effective treatments for patients and will work harder to discharge patients at the appropriate time and to the appropriate place.
SNFs - The benefit of lower hospital readmissions benefit providers in two ways: Better Medicare rates through
better Incentive Payment Multiplier (IPM) scores (VBP Program)
Hospital referrals (hospitals may know more about your readmission patterns than you do and they are acting on this information)
Specialty facilities - Facilities adapted with specialty equipment that enable them to more easily care for medically complex patients (i.e., higher paying payments under the new PDPM model). This would include items such as O2 and suctioning available in all patient rooms.

Winners Under PDPM 13
Medically complex patients (some currently in LTCHS or traditional nursing homes) – These patients will be more profitable and sought after by SNFs under PDPM. In the past, some facilities would not accept these patients by stating they were not able to care for these type of patients. Facilities may want to change this approach and instead place an emphasis on attracting these patients.
Longer inpatient stay facilities that have historically not catered to the growing demand for high-paying rehab patients (i.e., non-profits and older facilities) Since there will be higher paying rates for medically complex patients, these facilities are already well positioned to thrive under PDPM.
Facilities serving the following types of higher paying patients under PDPM: IVs Wounds Behavioral issues Diabetes Longer inpatient stays
SNFs with excellent assessment measures as reported in the SNF Quality Reporting Program (QRP). CMS plans to publicly display the assessment
measures in a manner that has more visibility than prior reporting.
Disclosure will benefit facilities that wish to distinguish themselves with “more sunshine.”

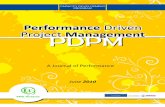
Winners Under PDPM 14
There are more winners than losers (175 winners and 90 losers), and the winners are winning by larger amounts than loser are losing by
Source: CMS SNF Enhanced Provider Specific File
42
38
62
24
9
0 10 20 30 40 50 60 70
$1-$49,999
$50,000-$99,9999
$100,000-$249,999
$250,000-$499,999
$500,000-$999,999
Virginia PDPM Winners
24%
22%35%
14%
5%
Virginia PDPM Winners - %
$1-$49,999 $50,000-$99,9999
$100,000-$249,999 $250,000-$499,999
$500,000-$999,999

Losers Under PDPM 15
Rehab companies –Many SNFs outsource their rehab services. Consequently, an entire industry grew from the demand for SNFs to outsource their rehab services. Most contracts currently
incentivize both parties to provide as much therapy as possible (up to the Ultra-High category).
Payments are now shifting from therapy to more acute medical conditions. Rehab companies could have the most to lose under PDPM.
Rehab savings for providers could be upwards of 20% - 30%.
Rehab-heavy facilities – Facilities not adjusting to the upcoming changes. These facilities may want to start attracting medically complex patients. Rehab-heavy facilities seem to be many of the “losers” under CMS’ FY17 modeling – slide to follow).
Facilities not equipped with advancements (i.e., oxygen, suction, …) Facilities who
currently “cherry-pick” low acuity patients.

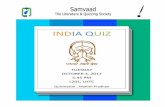
Losers Under PDPM 16
Majority of revenue losses are projected to be less than $250k. There are more winners than losers (175 winners and 90 losers), and the winners are winning by larger amounts
than loser are losing by
Source: CMS SNF Enhanced Provider Specific File
31
16
32
10
1
0 5 10 15 20 25 30 35
-$1-$49,999
-$50,000-$99,9999
-$100,000-$249,999
-$250,000-$499,999
-$500,000-$999,999
Virginia PDPM Losers
34%
18%
36%
11%
1%
Virginia PDPM Losers - %
-$1-$49,999 -$50,000-$99,9999
-$100,000-$249,999 -$250,000-$499,999
-$500,000-$999,999

What Projected Winners and Losers Have in Common? 17
0%10%20%30%40%50%60%70%80%90%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Ultra-High Therapy RUGs
Top 15 Losers VA Average Top 15 Winners- Ultra-High Therapy RUGs (% or Rehab RUG categories billed at Ultra-High levels)- VA Average per PEPPER - SNF Q4FY17 National Target Area Analysis
Avg. LOS= 26 days
VA Avg. LOS= 26.3 days
Avg. LOS= 28 days

Setting PDPM Payment Rates 18
$ Non-case mix set the same as under PPS.
All categories are individually case-mix adjusted (CMIs) but one (Non-Case Mix set).
Market-basket indexes and wage indexes still apply, same methodology as PPS.
PDPM rates will also be impacted by Value-Based Purchasing (VBP) like PPS rates were effective on October 1, 2018.
CMIs are different for each component but, PT and OT are calculated the same.

PPS Rate Calculations 19
PPS - Rate Component
Nursing (Case-Mix)
Therapy (Case-Mix)
Non Case-Mix Therapy Non-Case-Mix Total
Urban Per Diem$181.44 $136.67 $18.00 $92.60
RUX 2.67 1.87 n/a n/a
RUX Payment$484.44 $255.57 - $92.60 $832.61
* Above example has not been adjusted for Wage Indexes – FY19 Labor-related: 70.5%
Nursing (Case-Mix) Base Rate x Nursing CMI = Nursing Rate
Therapy (Case-Mix) Base Rate x Therapy CMI = Therapy Rate
Non Case-Mix Therapy Base Rate (only applies to non-rehab RUG categories Non CM Therapy Rate
Non-Case-Mix Base Rate Non-Case-Mix Rate

PDPM Rate Calculation 20
PT Base Rate x PT CMI (same CM group as OT but
different CM index) xAdjustment Factor = PT Rate
OT Base Rate x OT CMI (same CM
group as PT but different CM index) x
Adjustment Factor = OT Rate
SLP Base Rate x SLP CMI = SLP Rate
Nursing (Case-Mix) Base Rate x Nursing CMI = PT Rate
Non-Therapy Ancillary Services
(NTAS)Base Rate x NTAS CMI x Adjustment Factor = PT Rate
Non-Case Mix Non-Case Mix Rate

Rate Tapering
PDPM rates are reduced over time (Variable Per-Diem Adjustment Factors).
Variable Per-Diem Adjustment Factors change per diem payments to make them more episodic-like.
Adjustment Factors only impact PT, OT, and Non-therapy ancillary services (NTAS).
PT and OT are reduced every 7 days starting on the 21st day of stay.
NTAS really is not a rate tapering reduction. Providers are instead paid a 3X premium for first 3 days of stay, and then the NTAS rate is reduced to actual rate.
Current “tapering” under PPS could be as much, maybe more?
21

PDPM Variable Per-Diem Adjustment Factors 22
Table 30- Variable Per-Diem Adjustment Factor and Schedule - PT & OTMedicare Payment
Days
Adjustment Factor
1 - 20 1.00
21 - 27 0.98
28 - 34 0.96
35 - 41 0.94
42 - 48 0.92
49 - 55 0.90
56 - 62 0.88
63 - 69 0.86
70 - 76 0.84
77 - 83 0.82
84 - 90 0.80
91 - 97 0.78
98 - 100 0.76
Table 31- Variable Per-Diem Adjustment Factor and Schedule –
Non-therapy Ancillary Services (NTAS)
Medicare Payment
Days
Adjustment Factor
1 - 3 3.00
4 - 100 1.00

PDPM Rate Calculation Example 23
* Above example has not been adjusted for Wage Indexes – FY19 Labor-related: 70.5%
PDPM - Rate Component PT OT SLP Nursing NTA Non-Case-Mix Total
Urban Per Diem $59.33 $55.23 $22.15 $103.46 $78.05 $92.63
Case-Mix Group TD TD SL ES2 NA
Case-Mix Index 1.92 1.53 4.19 3.06 3.25
Adjustment Factor (Days 1 - 3) 1.00 1.00 3.00
Adjustment Factor (Days 4 - 20) 1.00 1.00 1.00
Adjustment Factor (Days 21 - 27) 0.98 0.98 1.00
Adjustment Factor (Days 28 - 34) 0.96 0.96 1.00 Adjustment Factor (Days 98 -
100) 0.76 0.76 1.00
PDPM Rate (Days 1 - 3) 113.91 84.50 92.81 316.59 760.99 92.63 $ 1,461.43
PDPM Rate (Days 4 - 20) 113.91 84.50 92.81 316.59 253.66 92.63 954.10
PDPM Rate (Days 21 - 27) 111.64 82.81 92.81 316.59 253.66 92.63 950.14
PDPM Rate (Days 28 - 34) 109.36 81.12 92.81 316.59 253.66 92.63 946.17
PDPM Rate (Days 98 - 100) 86.57 64.22 92.81 316.59 253.66 92.63 906.48

PPS vs. PDPM Rates
Important to note that starting October 1, 2018 (FY19), each nursing home’s 66 RUG payment rates will be unique to them. Rates will no longer be the same by CBSA (Core-Based Statistical Areas) codes due to Incentive Payment Multiplier (IPM) scores.
Providers will go from 66 Medicare payment rates under PPS to a possibility of being paid up to 28,800 possible rates under PDPM (starting October 1, 2019) 16 possible PT/OT rate variations (excludes Tapering) 12 possible ST rate variations 25 possible Nursing variations 6 NTAS rate variations (excludes Tapering) (16 x 12 x 25 x 6 = 28,800 possible rates)
PDPM rates will also be impacted by Value-Based Purchasing (VBP) and wage indexes just like current PPS rates.
24

Management of Rehabilitation Costs
With RUG-IV, the current contract structure is aligned to create success for both rehab providers and SNFs. Under PDPM, can a “perfect” alignment exist? We think “Yes.”
How will PDPM impact my therapy department? Staffing: With a projected reduction in total therapy minutes provided, facilities can anticipate a
decrease in the demand for therapists in the SNF setting. Rehab staff could be easier to recruit and retain. Only time will tell given fewer rehab staff work in a LTC setting than many think.
Managing Care: Unlike RUG-IV which incentivizes Ultra-High volumes of therapy to capture the maximum payment, PDPM requires the provider to carefully manage how they deliver services to provide just the right level of care for each patient. It will no longer be all about RUs.
Will we revert to pre-PPS (cost-based) payment models? Before PPS, many contract rehab groups were paid by time on-site or minutes of therapy. This model was not effective under PPS because of the rehab breakpoints (i.e., RUs = 720 minutes
over 7 days, RVs = 500 minutes over 7 days, ect.). If not careful under PDPM, rehab contractors could be incentivized to provide more therapy than
needed with no benefit to the patient or increased reimbursement benefit to SNF.
25

Management of Rehabilitation Costs
Whether you have in-house or contract therapy, you should be preparing for the new PDPM payment model.
Management of Rehab costs Rehab therapy cost reduction – biggest cost reduction opportunity of PDPM Begin planning when and how to renegotiate your rehab contract. Add a clause stating that the rehab contract can be negotiated whenever Medicare makes a
fundamental change in reimbursement. Have the option to renegotiate the contract after the start of PDPM (6-months in?). This is “new to
everyone” clause. Should you bring rehab service in-house? The answer could be “yes” in certain situations and geographic markets.
Regardless of whether you choose contract or in-house therapy, managing delivery of therapy focused on patient outcomes verses volume will be critical PPS has been in place for 20 years – an entire generation of therapist have been conditioned to
manage minutes, not outcomes.
26

Management of Rehabilitation Costs
Group and Concurrent Therapy – CMS is expanding the group limitation to include concurrent therapy as well. CMS has limited group and concurrent treatment provided (combined) to a resident to 25% of the minutes provided per discipline. How will this impact your rehab contract?
More than 99% of current Medicare Part A therapy in SNFs is performed on an individual basis. Group and concurrent therapy could be a great cost saving opportunity.
Since minutes no longer drive reimbursement, rehab providers and SNFs will want to focus on optimizing the net margin associated with providing therapy.
Warning – Under-delivering therapy could lead to poor patient outcomes and potential Medicare audits and take-backs.
Can you achieve “contract-like” results while managing your therapy in-house? We think “yes” and have seen this done very well, but it is difficult. PDPM makes in-house therapy an even more attractive option than under PPS.
27

Management of Rehabilitation Costs
The best PDPM rehab pricing models will achieve the following: Ensure desired patient outcomes are attained.
Support the critical care management elements that also drive revenue (i.e., MDS Section GG, ICD10 coding, etc..) to ensure the most optimal and appropriate reimbursement is captured.
Minimize misalignments of risk created between the SNF and therapy group.
Provide a strong compliance environment.
Don’t forget – SNFs are in the driver seat with rehab contract negotiations.
28

Management of Rehabilitation Costs 29
Rehab Pricing Models we have seen discussed and which one we believe is the best?
#1 Risking Sharing with SNF
Similar to current RUGs per diem model.
SNF will be guaranteed a profit for each PDPM rehab Group (16 PT and OT groups and 12 SLP PDPM groups).
Rate may be constructed as a percent of the rehab portion of the PDPM rate.
SNF and rehab contractor share in the upside and downside of rehab categories, diagnosis coding, MDS Section GG coding, …
Insulates SNF from the risk associated with referral and patient mix
#2 Flat Per Diem (Capitated) Rate
Simple approach that has one daily rate that covers all patients.
This approach could result in the SNF not being guaranteed a profit for each PDPM group.
Creates a potentially disproportionate financial risk should patient acuity or experience changes.
Incentives between SNF and rehab contractor may not be aligned.
We lack industry experience with PDPM so how do we create?
#3 Time On-site Simple model where
pricing is set based on rehab hours worked and paid at a set billing rate.
Rehab group not incentivized to drive better outcomes or improve operation efficiencies (model breeds inefficiencies).
Since the rehab group is only paid for hours worked, this model creates no risk or case management incentive.
#4 Per Part A Therapy Minute
Simple but unpredictable model.
SNF and rehab group have incentives that are misaligned.
Therapy group gets paid for care delivered, no risk or incentive for good case management.

Management of Rehabilitation Costs
We believe the winner is… #1This model best aligns all parties’ incentives and interests while at the same time adding accountability to both parties to deliver on patient outcomes, regulatory compliance, and financial success.
30
#1 Risking Sharing
with SNF

Management of Rehabilitation Costs
Current Medicare Part A Contracts are mostly written to reimburse the contract therapy group based on a RUG-IV rehab category and percent of Part B billings.
31
RUG Category RUG Minutes / Week Per Diem Charge Charge / Minute
Ultra High 720 $102.86 $1.00
Very High 500 71.43 1.00
High 325 46.43 1.00
Medium 150 21.43 1.00
Low 45 6.43 1.00
Non-Rehab varies varies 1.00

Management of Rehabilitation Costs
What is your current rehabilitation revenue under PPS?
32
PPS - Urban (Rehab) $136.67
RUG Distribution Therapy CMI Therapy Payment RUG Distributions Estimated Rehab Revenue PPD
Ultra High 1.87 $ 255.57 86% $219.79
Very High 1.28 174.94 8% 14.00
High 0.85 116.17 3% 3.49
Medium 0.55 75.17 1% 0.75
Low 0.28 38.27 1% 0.38
Non-Rehab - 18.00 1% 0.18
Medicare A – PPD 100% $238.59

Management of Rehabilitation Costs
What percent of revenue are you currently paying under PPS?
33
RUG Distribution RUG Minutes / Week RUG Minutes / Day RUG Distributions
Average MCR-A Rehab Minutes Per
Day
Ultra High 720 103 86% 88
Very High 500 71 8% 6
High 325 46 3% 1
Medium 150 21 1% 0
Low 45 6 1% 0
Non-Rehab - - 1% -
100% 96
Cost Per Minute $1.04
Average Medicare A Therapy Costs PPD $100.00
Ratio of Cost to Revenue: 42%

Management of Rehabilitation Costs
What will your projected rehabilitation revenue be under PDPM?
34
Rehab Type PT OT ST Total Rehab -PPD
PDPM - Urban $59.33 $55.23 $22.15
Average Therapy CMI
1.49 1.49 1.41
Estimated Therapy Payment - PPD
$88.40 $82.29 $31.23 $201.93
Average Medicare A Therapy Costs PPD @ 42%= $ 84.81

Management of Rehabilitation Costs 35
Description PPS PDPM Diff ($) Diff (%)
Revenue PPD 239 202 (37) -15%Ratio of Cost to Revenue 42% 42%
Cost PPD 100 85 (15) -15%
Profit PPD 138 117 (21) -15%
Discount for Group/Concurrent, Coverage, … -25%Adjusted Ratio of Cost to Revenue 32%
Adjusted Cost PPD 100 64 (37) -37%
Adjusted Profit PPD 138 138 (0) 0%
Patient Days (25 residents x 365) 9,125
Rehab Savings under PDPM $ (333,974)

Management of Rehabilitation Costs
If you decide to risk share on your rehab rate, you need to know: What is your current rehab cost to therapy ratio (42% in the example provided)?
What is your projected PPD rehab revenue projected to be under PDPM?
What adjustment (reduction) should you be making to this percent for Group and Concurrent Therapy?
Perform your own calculations and compare to data provided by rehab vendor
If you decide to keep rehab in-house, does it make sense to have an independent expert review billings and outcomes? We have seen this work well for pharmacy.
“We have two generations of rehab therapists that have not needed and likely not developed the skill to evaluate the amount of therapy a resident really needs.” - Mark McDavid | Seagrove Rehab Partners
36

How do I Calculate the Cost of Care? 37
Many providers began analyzing costs by resident and type of resident under PPS, but most discontinued over time. Time to restart? We think “Yes.”
Do you need to rethink your patient mix?• SNFs should begin evaluating what it should be, what the facility is strong at, which
patients have the highest profit, and which do not.• PDPM is designed to pay more for more medically complex residents• SNFs will likely want to specialize instead of focusing on everything, especially in urban
markets.• What is my niche?
SNFs should know the cost of the different types of patients and how much they will be paid under PDPM for each different type. This will help pinpoint what your facility wants to focus on. You should know this before the start of PDPM.
PDPM payment model changes will likely incentivize better access for medically complex patients. How much are these residents going to cost me?

How Do I Calculate the Cost of Care? 38

How Do I Calculate the Cost of Care? 39

How Do I Calculate the Cost of Care? 40
Patient Name: Sample ResidentMonth: Oct-18
Revenue RUG Score Rate Days Medicare Reimbursement
022 Room & Board RUA $ 473.48 8 $ 3,788 022 Room & Board n/a - - -022 Room & Board n/a - - -022 Room & Board n/a - - -022 Room & Board n/a - - -
Total Reimbursement 8 $ 3,788
Expenses Units Charges RCC120 Room Charge 8 $ 2,824.00 207.12 $ 1,657 250 Pharmacy 200.25 41.45% 83 270 Medical Supplies 16.80 102.36% 17 300 Laboratory - 17.65% -420 Physical Therapy 1,345.00 53.38% 718
430 Occupational Therapy1,370.00 52.18% 715
440 Speech Therapy - 55.05% -Total UB04 Charges 5,756.05 Total Estimated Expense $ 3,190
Estimated Profit/(Loss) $ 598.26 Estimated Profit/(Loss) - PPD $ 74.78

41
PDPM - Rate Component - Left leg weakness (unsteady gait) PT OT SLP Nursing NTA
Non-Case-Mix Daily Rate Days Total Rate
Urban Per Diem $59.33 $55.23 $22.15 $103.46 $78.05 $92.63 Case-Mix Group TJ TJ SA PBC2 NFCase-Mix Index 1.42 1.44 0.68 1.21 0.72Adjustment Factor (Days 1 - 3) 1 1 3Adjustment Factor (Days 4 - 20) 1 1 1Adjustment Factor (Days 21 - 27) 0.98 0.98 1Adjustment Factor (Days 28 - 34) 0.96 0.96 1Adjustment Factor (Days 35 - 41) 0.94 0.94 1Adjustment Factor (Days 42 - 48) 0.92 0.92 1
PDPM Rate (Days 1 - 3) 84.25 79.53 15.06 125.19 168.59 92.63 565.25 3 1,695.74 PDPM Rate (Days 4 - 20) 84.25 79.53 15.06 125.19 56.20 92.63 452.85 17 7,698.52 PDPM Rate (Days 21 - 27) 82.56 77.94 15.06 125.19 56.20 92.63 449.58 7 3,147.05 PDPM Rate (Days 28 - 34) 80.88 76.35 15.06 125.19 56.20 92.63 446.30 7 3,124.12 PDPM Rate (Days 35 - 41) 79.19 74.76 15.06 125.19 56.20 92.63 443.03 7 3,101.19 PDPM Rate (Days 42 - 48) 77.51 73.17 15.06 125.19 56.20 92.63 439.75 4 1,759.01 Total 456.13 45 20,525.64 PPS RUG RUC 14 631.22 RUB 16 631.22 584.61 45 26,307.48
Increase | (Decrease) - $ RUA 6 527.80 RVA 9 467.12 -35% (5,781.84)Increase | (Decrease) - % -22%
PPS to PDPM Resident Example #1

PPS to PDPM Resident Example #2 42
PDPM - Rate Component - Pneumonia PT OT SLP Nursing NTANon-Case-
Mix Daily Rate Days Total Rate
Urban Per Diem $59.33 $55.23 $22.15 $103.46 $78.05 $92.63
Case-Mix Group TJ TJ SH LBC1 NF
Case-Mix Index 1.42 1.44 2.85 1.43 0.72
Adjustment Factor (Days 1 - 3) 1 1 3
Adjustment Factor (Days 4 - 20) 1 1 1
Adjustment Factor (Days 21 - 27) 0.98 0.98 1
PDPM Rate (Days 1 - 3) 84.25 79.53 63.13 147.95 168.59 92.63 636.07 3 1,908.22
PDPM Rate (Days 4 - 20) 84.25 79.53 63.13 147.95 56.20 92.63 523.68 17 8,902.58
PDPM Rate (Days 21 - 27) 82.56 77.94 63.13 147.95 56.20 92.63 520.41 5 2,602.03
Total 536.51 25 13,412.83
PPS RUG RVC 541.51 25 13,537.75
Increase | (Decrease) - $ (124.92)
Increase | (Decrease) - % -0.9%

PPS to PDPM Resident Example #3 43
PDPM - Rate Component - Surgical wound related to cancer PT OT SLP Nursing NTA
Non-Case-Mix Daily Rate Days Total Rate
Urban Per Diem $59.33 $55.23 $22.15 $103.46 $78.05 $92.63
Case-Mix Group TK TK SA LBC1 NF
Case-Mix Index 1.52 1.54 0.68 1.43 0.72
Adjustment Factor (Days 1 - 3) 1 1 3
PDPM Rate (Days 1 - 3) 90.18 85.05 15.06 147.95 168.59 92.63 599.46 1 599.46
Total 1 599.46
PPS RUG LC1 331.96 1 331.96
Increase | (Decrease) - $ 274.53 267.50
Increase | (Decrease) - % 81%

PPS to PDPM Resident Example #4 44
PDPM - Rate Component - COPD PT OT SLP Nursing NTANon-Case-
Mix Daily Rate Days Total Rate
Urban Per Diem $59.33 $55.23 $22.15 $103.46 $78.05 $92.63
Case-Mix Group TK TK SA HBC1 NE
Case-Mix Index 1.52 1.54 0.68 1.85 0.96
Adjustment Factor (Days 1 - 3) 1 1 3
Adjustment Factor (Days 4 - 20) 1 1 1
PDPM Rate (Days 1 - 3) 90.18 85.05 15.06 191.40 224.78 92.63 699.11 3 2,097.34
PDPM Rate (Days 4 - 20) 90.18 85.05 15.06 191.40 74.93 92.63 549.26 7 3,844.80
Total 594.21 10 5,942.14
PPS RUG HC1 10.00 379.13 379.13 10 3,791.30
Increase | (Decrease) - $ 215.08 2,150.84
Increase | (Decrease) - % 57%

Management of Medicare Part A Pharmacy Costs Nothing unique to PDPM, but great opportunity!
We consistently find SNFs with similar RUG distributions, located in the same urban market with the same pharmacy provider and similar contract, that have significantly different PPD pharmacy costs. Why? We believe pharmacy cost management is: 80% pharmacy utilization management / 20%
pharmacy contract pricing. Savings can easily be $15 - $25 ppd
45
Two keys to lower pharmacy costs
Identification of high cost drugs and development of protocols and substitutes
Therapeutic Equivalents Develop groups of drugs that produce the same outcomes Automate therapeutic interchange with your Medical Director so
the lower cost drug is chosen automatically
Every $ saved on pharmacy costs goes directly to your bottom line!

Preparing for Success Under PDPM
With no operational changes, evaluate whether your facility is projected to be a winner or loser under PDPM. Data can be obtained from FY17 CMS “Enhanced Provider Specific File.”
Begin evaluating how you are going to manage rehab costs.
Begin by enabling each therapist to provide more treatments to more patients through the use of group and concurrent modes of treatment. Focus rehab resources on Medicaid (Medicare Part B) residents. This can be a double win since Medicaid rates can be
materially improved by rehab, if coordinated with your MDS team.
Train MDS staff for upcoming changes (ICD-10 training). Most MDS coordinators are not certified coders (very rare), and SNFs typically don’t employ certified coders – different skill
set.
Evaluation and investment in your team to improve coding accuracy.
Providers should start to identify and perhaps incentivize a team member(s) in their facility to attain a professional codingdesignation available through the American Academy of Professional Coders (AAPC).
Start training all staff on PDPM.
46

Preparing for Success Under PDPM
Review regulatory and compliance requirements for PDPM
Quantify and model the impact of PDPM on your facility’s current reimbursement How does this compare to CMS’ model?
Staff a certified ICD-10 coder or train someone internally?
Determine how your facility will rethink its workflow process since patients will need to be assessed much more accurately.
You may only have one shot to get the payment rate correct. Once the patient is assessed at the beginning of the stay, the payment has been set in motion. It will be difficult to change the payment category, even if the patient has a change in condition.
If you get this first MDS wrong, payment could be inappropriately too low.
47

Preparing for Success Under PDPM
Provide training to staff so they feel more comfortable providing care to more complex residents. Under PDPM, these will be the new higher categories and are more likely to receive higher reimbursements.
Non-Therapy Ancillaries (NTAs) better account for drug, lab, respiratory, and medical supplies. Residents with high costs in these areas may have been avoided in the past but could be profitable in the future. Providers need to evaluate this.
Management will need to understand how patient information is captured and what “moves the payment needle.”
Interim Payment Assessments (IPA) – (BIG reimbursement opportunity) IPAs are a “gift” from CMS and could be required for all significant changes in the future
Develop an “IPA Checklist” for floor staff
48

Preparing for Success Under PDPM
Better management of Medicare Part A Pharmacy costs. This is not PDPM specific but a great cost savings opportunity for many providers.
Make sure your EMR Software vendor is equipped with advanced business intelligence (BI), and data analysis tools can help you predict your future needs and manage costs under PDPM. This is something most providers planned to do with PPS, but most did not follow through.
Ask you EMR vendor what capabilities they have, or will have, to support your transition to PDPM.
Develop treatment protocols (with assistance from EMR software) that will allow you to deliver the appropriate level of care for each unique resident.
Triple check process as important as ever.
Increase Medicare Part A mix by making a move to caring for more medically complex residents.
49

Preparing for Success Under PDPM
Do you need to rethink your patient mix? SNFs should evaluate what it might focus on under PDPM and what the facility is strong at. PDPM is designed to pay more for more medically complex residents. SNF may want to specialize instead of focusing on everything.
Reduce barriers between nursing and therapy. Therapy can no longer operate separately from everyone else (another potential bonus of moving to in-house therapy).
Understand each patient's expected reimbursement at the beginning of their stay (easier than ever).
Learn the niches of the other nursing homes in your market. Is there an underserved area you can help your referral sources fill?
Work with referring hospital to help place challenging patients (more financially rewarding than in the past).
50

Value-Based Purchasing (VBP) Impact
SNF VBP Program began impacting Medicare payments on October 1, 2018.
This program offers Medicare incentive payments to SNFs based on their performance on specific measures of readmissions.
Patients admitted to SNFs between January 1, 2017 and December 31, 2017 are the measure currently used.
Uses the complete list of SNF FFS stays for CY17 to calculate the performance period risk-standardized readmission rate (RSRR).
This measure assesses SNF patients’ hospital readmissions within 30 days of being discharged from a prior hospital stay.
SNF VBP Program provides a strong incentive for facilities to coordinate care.
51

Value-Based Purchasing (VBP) Impact
The 30-day readmission period during which an unplanned readmission may be counted, referred to as the risk window, begins when a patient is discharged from an inpatient hospitalization and is subsequently admitted to a SNF within one day. The risk window ends 30 days from its start or when a patient is readmitted to a hospital, whichever occurs first. Example: If a patient is discharged from a hospital to a SNF on 10/01/18, then readmitted to
the hospital on 10/10/18, the 30-day risk window started on 10/01/18 and ended on 10/10/18 when the patient is readmitted to the hospital. A new 30-day risk-window begins if the patient is subsequently discharged from the hospital and admitted back to the SNF.
Aims to protect patients from potential harms or adverse events associated with hospital readmissions.
2% of SNFs’ Medicare payments withheld to fund incentive payments.
Caught many SNFs off guard last month.
52

Value-Based Purchasing (VBP) Impact
Only 60% of the total amount withheld from SNFs’ Medicare payments for that FY will be paid as incentive payments to SNFs based on their performance in the program.
The Incentive Payment Multiplier (IPM) is the number that will be applied to the Medicare RUG IV rates to determine your final payment for claims that are submitted for service dates starting October 1, 2018.
SNF VBP incentive payments do not apply to any other type of claim (such as Medicare Advantage claims).
SNFs can access all reports though Quality Improvement Evaluation System (QIES) Certification and Survey Provider Enhances Report (CASPER) system.
IPM can range from 0.98 (equivalent to a 2% withhold) to 1.0165, which reflects a 1.65% increase and is the highest incentive payment.
This data will eventually become public information.
53

Value-Based Purchasing (VBP) Impact
Performance period and baseline periods for performance scoring
54
Term FY19 Program FY20 Program
Performance Period CY17(January 1, 2017 – December 31, 2017)
FY18(October 1, 2017 – September 30, 2018)
Baseline Period CY15(January 1, 2015 – December 31, 2015)
FY16(October 1, 2015 – September 30, 2016)

Value-Based Purchasing (VBP) Impact 55
Your SNF's FY 2019 SNF VBP Program PerformanceSAMPLE HEALTH AND REHABAnnual Performance Score Report
Performance InformationBaseline Period (CY 2015) RSRR 0.19807Improvement Threshold (Baseline Period Inverted RSRR) 0.80193Performance Period (CY 2017) RSRR 0.17633Performance Period Inverted RSRR 0.82367FY 2019 Achievement Threshold 0.79590FY 2019 Benchmark 0.83601SNF VBP Achievement Score 67.31114SNF VBP Improvement Score 58.79108SNF VBP Performance Score 67.31114SNF VBP Program Rank 1,977Incentive Payment Multiplier 1.0111900874
Note: There were 5,249 unique (non-tied) performance scores in the FY 2019 SNF VBP Program and 15,421 SNFs eligible for the Program nationally. RSRR = Risk-Standardized Readmission Rate; CY = Calendar Year; FY = Fiscal Year; N/A = Not Applicable

Conclusions
We believe PDPM will be a positive change for both providers and patients. What we learned from the transition to Price-based Medicaid in SY15 and the Medicaid 48-
Grouper last July (almost everyone who focused on success in these new environments succeeded),
Measurements have been made assuming no operational changes (good for us, for a while).
While providers will be paid less for therapy-intensive patients, they will be paid substantially more for clinically complex patients. This will cause providers to provide therapy services based on patient need and not reimbursement (CMS’s goal to start with).
Providers that prepare and adapt for PDPM will achieve the greatest benefits.
PDPM will provide more flexibility in servicing patients with more acute and complex conditions (we believe great for patients and facilities).
56

Conclusions
Most of the focus of PDPM has been on the revenue side. We believe there is much to gain on the expense side by focusing on appropriate therapy services (begin planning on when and how you want to negotiate your therapy contract or bring rehab in-house). Also, don’t forget about improved pharmacy cost management.
Don’t worry if you are not projected to financially benefit under PDPM. We believe almost all providers can financially benefit under PDPM if they make proactive adjustments and are nimble (plan now!).
Opportunities could be reduced in the future by CMS (2 – 4 year window of opportunity before good measurements are made by CMS and actions are taken).
Good Luck!
57