FA&P Bones and Joints
51
Functional Functional Anatomy and Anatomy and Physiology Physiology Bones and Joints Bones and Joints
description
Transcript of FA&P Bones and Joints

Functional Anatomy Functional Anatomy and Physiologyand Physiology
Functional Anatomy Functional Anatomy and Physiologyand Physiology
Bones and JointsBones and Joints

Terminology for the Location
of Body Structures To allow people to describe the location of the body structure, we use an Anatomical Reference System. This reference system has three parts
• Direction• Plane• Cavity
To give location of the body part, it is assumed that the body is in the Anatomical Position. This is standing erect, facing forward, arms by sides and palms forward.

Body Planes
Median: Dividing the body into left / right halves
Sagittal: Dividing the body into unequal left and right parts and parallel to the median
planeCoronal / Frontal: Dividing the body into
front and back (anterior and posterior)
Transverse / Horizontal: Dividing the body into upper and lower (superior and inferior)

Body Cavity A body structure may be located in a particular cavity. Each cavity contains particular organs. For example the Thoracic cavity contains the heart and lungs and is separated from the abdominal cavity by the diaphragm.There are five major cavities
• Pelvic Cavity• Abdominal Cavity• Thoracic Cavity – pleural (lungs)
Pericardial (heart)• Spinal Cavity• Cranial Cavity

Directional TermsTERM DEFINITION DIAGRAM EXAMPLE
Superior (cranial)
Toward the head or upper part of the body; above
The heart is superior to the liver
Inferior(caudal)
Away from the head toward the lower part; below
The stomach is inferior to the lungs
Anterior(ventral)
Toward or at the front of the body; in front of
The sternum is anterior to the
heart
Posterior(dorsal)
Toward or at the back of the body; behind
The calcaneous is posterior to the
phalanges
Medial Toward or at the midline of the body; inner side
The ulna is on the medial side of the
forearm
Lateral Away from the midline of the body; outer side
The lungs are lateral to the heart
Proximal Closer to the origin or point of attachment to trunk
The humerus is at the proximal end of
the radius
Distal Farther from origin or point of attachment to trunk
The phalanges are distal to the
carpals
Superficial Towards or at the body surface
The skin is superficial to the skeleton
Deep Away from the body surface; more internal
The ribs are deep to the skin of the
chest.

Body structure and Movement of
the Musculoskeletal System. The musculoskeletal system is a combination of the skeletal, muscular and articular systems of the body and is responsible for the movement and locomotion of the body.
Skeleton – framework
Muscles – force
Joints – movement

The Skeletal SystemSome facts:• The human skeleton is an endoskeleton ie it lies
within the soft tissue of the body. It differs from the exoskeleton of an insect or crayfish.
• It is the major supporting structure of the body• It is a living structure, capable of growth, adaptation
and repair.• The human body contains a total of 206 bones.
– Bones are approximately 50% solid matter and 50% water– By weight, bone is 65% mineral and 35 % cells, fibres and
blood vessels– Bones are living structures containing blood vessels and
nerves that grow, adapt and repair– Bones continue to grow in length until girls are 13 – 15
years and boys are 16 – 18 years.• Is 20% of total body weight.

Functions of the Skeletal System The skeletal system has four main functions:
• Body Movement – there are up to 206 bones in the skeleton, all of which provide sites for muscle attachment. When a muscle contracts, it moves the bones to which it is attached and thus creates movement. Any irregularity on a bone surface provides a possible site for muscle attachment.
• Support and Protection – the skeleton provides support for the body and helps battle forces of gravity. The strong protective skeletal layer protects vital organs eg the rib cage protects heart, lungs, kidneys from all but the most traumatic injuries.
• There are two main types of bone tissue:– Compact bone – found in the shaft (diaphysis of the long bone. It surrounds
the cavity of the long bone, giving body rigid framework. Collagen is the central ingredient in providing compact bone rigidity and strength.
– Cancellous bone – or spongy bone, provides some of the shock absorption required at end of long bones or at edges of more irregular bones.
• Mineral storage sites – bone tissue stores a number of minerals important for health. Calcium, phosphorus, sodium and potassium all contribute to maintenance of bone tissue as well as other roles in the body.
• Production of blood cells – essential production of new Red Blood Cells occurs within cavity of the long bones. Production levels are high during growth years, reducing as age increases and need for high rates of RBC decreases. Haemoglobin transports 02 inside RBC and much of adult’s bone activity are filled with yellow bone marrow, a source of long-term energy.

Bone Formation and Growth Most bones of the human embryo are formed in cartilage and then replaced by bone. This process is called Ossification.
– Cartilage is softer than bone, less rigid and slightly elastic. Cartilage forms the temporary skeleton of the developing foetus, but is gradually replaced almost entirely by bone. It is retained throughout life on the articular (joint) surfaces of most bones and as costal, nasal, laryngeal, tracheal and bronchial cartilage.
– Cartilage is made up of:• Chondroblasts – active growing cell form of cartilage• Chondrocytes – mature cell form of cartilage. These
occupy spaces in the matrix (lacunae) ie matrix of chondrin (protein) and collagen (tough) and elastin fibres.
BLAST = FORMINGCLAST = DESTROYING


Bone growth and Remodelling The ossification of cartilage into bone, or osteogenesis, begins about the 9th week of foetal development. The diaphyses of long bones are formed by birth, and the epiphyses begin to ossify about that time. Below are the stages of bone growth and remodelling of the epiphyses of a long bone.
Creation of an ossification centre:At about the 9th month, an ossification centre develops in the epiphysis. Some cartilage cells enlarge and stimulate ossification of surrounding cells. The enlarged cells die, leaving small cavities. New cartilage continues to develop.
Osteoblasts form bone:Osteoblasts begin to form bone on the remaining cartilage, creating the trabeculae network of cancellous bone. Cartilage continues to form on the outer surfaces of the epiphysis and along the upper surface of the epiphyseal plate.

Bone growth and Remodelling
cont ..... Bone length grows
Cartilage is replaced by compact bone near the outer surfaces of the epiphysis. Only cartilage cells on the upper surface of the diaphyseal plate continue to multiply rapidly, pushing the epiphysis away from the diaphysis. This new cartilage ossifies, creating trabeculae on the medullary side of the epiphyseal plate.
Remodelling:Osteoclasts produce enzymes and acids that reduce trabeculae created in the epiphyseal plate, thus enlarging the medullary cavity. In the epiphysis, osteoclasts reduce bone, making its calcium available for new osteoblasts that give the epiphysis its adult shape and proportion. In young adults, the epiphyseal plate completely ossifies (closes) and becomes the epiphyseal line; longitudinal growth of bone then ceases.

Increase in Bone Length and Diameter Length• As long as the epiphyseal plate remains present bones can
increase in length.• Cartilage cells divide making the epiphyseal plate thicker.• At the same time the side of the plate closest to the diaphysis
is replaced by bone.• This results in the diaphysis becoming longer and the
epiphysis remaining the same size.• Eventually the cartilage stops growing and the laying down of
bone takes over until the growth plate is gone (about 25 in males, younger in females).
Diameter• Osteoblasts beneath the periosteum deposit layers of bone.• At the same time bone is being removed from inside the
cavity.• The net effect is an increase in bone diameter, but not bone
thickness.

Factors Affecting Bone Development
1. Stress– A bone can adjust its strength in proportion to the degree
of stress to which it is subjected– stress = bone deposited– stress = bone is withdrawn– Bones are exposed to 2 major forms of stress
Gravity – supporting the weight of the bodyFunction – pull exerted by muscle contraction
2. HormonesA combination of hormone activity stimulates the formation of new bone, especially in young people
3. NutritionFor bone development to occur the body requires several essential substances – for example vitamin D promotes absorption of calcium.

Bone Growth Summary Infancy and Youth • Long bones lengthen by growth of the epiphyseal plates (growth
plates).• Cartilage cells stack on top of each other causing bone to
lengthen.• Cells at top divide meanwhile older chondrocytes closer to the
shaft enlarge and die and surrounding cartilage matrix deteriorates.
Adolescence • Cartilage cells of epiphyseal plates divide less and plated thin
until replaced by bone tissue. Growth ends when epiphysis and diaphysis fuses.
Adults• Constant bone remodelling. Bone formation and bone
resorption is balanced.
Elderly• Resorption predominates.


Bones of the body

Bones of the body

Bones

Bones

Bones

Bones

Bones

Bones

Bones

Major bones of the Skeleton The skeleton is divided
into two main parts:– Axial skeleton, which
provides a central support axis and includes the skull, vertebral column, sternum and ribs
– Appendicular skeleton, which includes the bones of the limbs, together with the shoulder girdle and pelvic girdle, which support and attach them to the axial skeleton.

Axial Skeleton
• Skull – cranium consists of (8) bones fused together, the face has (14) bones, some fused, some moving independently. The skull protects the brain, eyes and ears and provides attachment of muscles for head and jaw movement.
• Spine – (7) cervical, (12) thoracic and (5) lumbar vertebrae. Bottom (9) bones, (5 in the sacrum, 4 in the coccyx) are fused together to form one solid bone. The first cervical vertebra is the atlas and the second cervical vertebra is the axis. The coccyx is said to be the remnants of a tail. The bones of the vertebral column protect the spinal cord and provide support and movement.
• Thorax – (12) pairs of ribs, which join thoracic vertebrae. Top (10) pairs are joined to the sternum at the front by cartilage; the remaining (2) pairs have free ends. The thorax encloses and protects the heart and lungs and provides support for the shoulder girdle. Each typical rib forms a hinge joint with 2 adjacent thoracic vertebrae and their disc.

Appendicular skeleton:
• Shoulder girdle – consists of the clavicle joined at the top of the sternum at one end and holding the scapula away from the rib cage at the other.
• Arm – the humerus joins the radius and ulna at the elbow, in turn joins to a highly mobile wrist and hand.
• Wrist – Ulna and radius join (2) rows of carpal bones at the wrist.• Hand – the palm of each hand consists of (5) metacarpal bones,
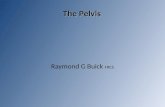
which join with the phalanges of the thumb and fingers.• Pelvic girdle – consists of the ilium (largest and uppermost
portion), Ischium (lower and posterior portion) and the pubis (superior and anterior to the ischium).
• Leg – the femur is the longest, heaviest and strongest bone in the body. It fits into a socket (acetabulum) in the pelvis and joins the tibia to form the knee. The patella protects this joint; the fibula acts as a support to the ankle and muscles of the lower leg.
• Foot – (7) tarsals and (5) metatarsals support the body weight. (14) phalanges are smaller and have little active function.

Vertebral column:
The vertebral column has some special features.• Each vertebra has a hollow centre through which the spinal
cord travels which controls most conscious movements within the body.
• Vertebras increase in size as they descend from – cervical– thoracic– lumbar region.
• Helps to support the weight of the body.• Movement between the (2) vertebrae is limited, but
movement of the vertebral column as a whole is great allowing bending and twisting.
• Provides a central structure for maintenance of good posture. This is dependent on the person maintaining correct levels of strength and flexibility of muscles groups that connect with the vertebral column.
• The cervical vertebrae support the head and neck, the thoracic vertebra anchor the ribs and strong weight bearing regions towards the bottom of the vertebral column and provide a stable centre of gravity during movement.

Classifications of bones
according to shape. 1. Long Bones – are
longer than they are wide and have a hollow shaft containing marrow. They are best suited to weight bearing and can withstand heavy stress. Long bones allow the limbs to make a range of large and powerful movements eg femur, tibia, fibula, phalanges, humerus, ulna, radius.

Classifications of bones
according to shape. 2. Short Bones – are
roughly cubical with same width and length. They allow the body to perform fine motor movements and help absorb heavy impacts eg carpals of wrist and tarsals of the feet.

Classifications of bones
according to shape. 3. Flat Bones – provides
flat areas for muscle attachment and usually enclose cavities for protecting organs. These bones consist of two smooth, flat plates of compact bone enclosing a layer of spongy bone tissue eg scapula, ribs, sternum and skull.

Classifications of bones
according to shape. 4. Irregular Bones
– have no shape characteristics and include bones not yet classified eg vertebrae and bones of the face

Classifications of bones
according to shape. 5. Sesamoid
Bones – a small bone that has developed in tendons around some joints, of which the patella is the largest one

Classifications of bones
according to shape. 6. Sutural Bones
– small bones located between some joints of the some cranial bones.

Structure of a Bone A typical bone has a shaft called a diaphysis. It consists of compact bone with a central cavity, called the medullary cavity (a hollow cylinder of compact bone filled with yellow bone marrow.) The medullary cavity is lined with a thin connective tissue layer called the endosteum. The diaphysis resists bending forces. The epiphyseal line separates it from the epiphysis.
The two ends of the bone are called the epiphysis. It is largely cancellous (spongy) bone and contains red marrow (blood cell production). It is separated from the diaphysis by a variably sized cartilage plate (epiphyseal plate or growth plate) for about the first 20 years of life. Most bones develop from cartilage models. Bone development occurs in the epiphysis and the diaphysis and slowly advances toward the intervening cartilage from both ends. The cartilage progressively thins to a line and ultimately disappears – causing the two to meet and resulting in the end of bone growth.
Articular cartilage caps the epiphysis and is smooth, slippery and bloodless. It is kept moist by the egg-white-like fluid from the synovial lining of the joint cavity. Bones of a synovial joint make physical contact at their cartilaginous ends.
A double layer of connective tissue called the periosteum covers the outer surface of the bone. It is well supplied with blood vessels and nerves – some of which enter the bone. The diaphysis of the bone contains an oblique tunnel for the passage of a nutrient artery, where it enters the medullary cavity and branch throughout. Periosteum does not cover articular cartilage.

Summary:
• Shaft - Diaphysis. Thick, compact bone surrounding the cavity.
Contains fat (yellow marrow)
• Two Ends - Epiphysis. Spongy bone surrounded by
compact bone (red marrow inside). In children, epiphyseal cartilage allows bone to lengthen.
• Periosteum - Double layered membrane of connective tissue and
osteoblasts (bone forming cells).



Bone Structure continued ..... • The weight bearing part of the bone is called compact
bone and is arranged into distinctive patterns called haversian systems or osteons.
• Here bone cells called osteocytes are arranged in concentric circles (lamellae) surrounded by a mineralised matrix.
• In the centre of each set of lamellae is a canal that carries small vessels.
• Nutrients and oxygen reach the isolated osteocytes by way of small canals that radiate away from the cells like legs from an insect.
• Between individual haversian systems, bone destroying cells called osteoclasts can be found breaking down existing patterns, freeing the calcium phosphate complexes to enter the blood as ions.
• At the ends of bones and along the marrow cavities we find cancellous bone called trabeculae interlock to form a somewhat open network.
• Red (blood cell-producing) and yellow (fat storing) marrow are located among the trabeculae.


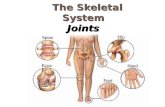
The Articular
System
An articulation is the place of union between two or more bones.There are three different types of articulation (or joints), determined by the degree of movement they permit
1. Fibrous joint (immovable joint) Bones are united by short bands of fibrous tissue at their ends eg skull bones, pelvic bones and sternum.

The Articular
System
2. Cartilaginous joint (slightly immovable joint)
Bones are united by a disc of tough fibrous cartilage separating the ends allowing a small amount of movement eg vertebral column, pubic bones, diaphysis and epiphysis, ribs joining the sternum.

The Articular
System 3. Synovial joints
(moveable joints)
– All synovial joints have a capsule that encloses the joint space
– Synovial membrane lines the inner surface of the capsule and secretes synovial fluid into the joint cavity to keep it lubricated.
– Shock absorbent articular cartilage is found on the ends of the bones to protect then from wear and tear.
– Eg knee, hip, elbow joints

Types of Synovial joints

Types of Synovial joints
Hinge Joint
Pivot Joint
Ovoid (ellipsoid) joint
Gliding (plane) joint
Saddle Joint
Ball and Socket joint
JOINT TYPE DESCRIPTION EXAMPLE
Allows back and forth movement, such as bending and straightening.Uniaxial.
Knee, knuckle, ankle and elbow
Allows rotation only.Uniaxial.
Between atlas and axis, between radius and humerus.
Allows back and forth and side to side movement,Biaxial.
Between carpals and radius; between metacarpal and phalange.
Flat bones slide on each other. Side to side and back and forth movement.Biaxial.
Between carpals, tarsals, ribs and thoracic vertebrae.
Allows back and forth and side to side movements.Biaxial.
Between carpal and metacarpals of thumb
Allows side to side, back and forth and rotational movement. Triaxial.
Hip and shoulder joint; head of femur/humerus fits into pelvis/scapula.

Structures within the Synovial Joints Joint Capsule• Is made up of tough, fibrous connective tissue running from one bone to another -
completely surrounding and enclosing the joint like a sleeve. It provides stability to the joint and is reinforced by ligaments.
Ligaments• Ligaments cross over joints, joining bone to bone. They are designed to assist the
joint capsule and maintain stability by limiting specific movements and can also control the degree and direction of movement that occurs. Joint can become unstable with injury (eg overstretching).
Synovial Membrane• Is a thin sheet that lines the interior of a joint capsule. It secretes synovial fluid
into the cavity.Synovial Fluid• Acts as a lubricant, keeping the joint well oiled ant the moving surfaces apart.
The fluid forms a cushion like protection between joints that don’t always fit together, as well as removes waste and provides nutrition for the cartilage. The viscosity of the fluid can vary according to the physical activity of the joint. A decrease in temperature increases the viscosity of the joint while an increase in temperature decreases the viscosity.
Hyaline Cartilage• This cartilage is smooth, shiny elastic tissue that covers the ends of bones in
synovial joints. It allows them to move freely over each other.Tendons• Tendons are inelastic and strong tissue that attaches muscle to bone. They assist
in movement – helping muscles pull across the joints on the bones.Bursae• They are closed sacs, which are lined with synovial membrane. Bursae can be
found in spaces where friction is likely to occur such as between tendons and ligaments. They also secrete synovial fluid in order to reduce friction and prevent wear and damage.

Structures within the Synovial Joints

Structures within the Synovial Joints

Movements of the Synovial Joints

Movements of the Synovial Joints and their
definitions Flexion A decrease in the angle of a joint
Extension In increase in the angle of a joint
Lateral Flexion Flexion sideways
Hyperextension Extension beyond that seen in the anatomical position
Horizontal flexion Flexion in the shoulder joint where the arm moves close to the body in a horizontal plane
Horizontal extension Extension in the shoulder joint where the arm moves away from the body in a horizontal plane
Abduction Movement of a body part away from the midline of the body
Adduction Movement of a body part back toward the midline of the body
Rotation Movement of a body part around its longitudinal axis
Pronation Rotation of the palm of the hand downwards or inwards
Supination Rotation of the palm of the hand upwards or outwards
Plantar flexion An increase in the angle between the foot and the tibia in the ankle joint (toes pointed)
Dorsi flexion A decrease in the angle between the foot and the tibia in the ankle joint
Elevation Upward movement of the scapula
Depression Downward movement of the scapula
Inversion Movement of the sole of the foot inwards at the ankle
Eversion Movement of the side of the foot outwards at the ankle
Circumduction Movement of the end of the bones in a circular motion