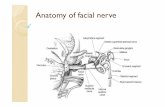
Facial Nerve 1
25
PRESENTED BY:- JYOTI
Transcript of Facial Nerve 1

PRESENTED BY:-
JYOTI

Segment Location Length,mm
Supranuclear Cerebral cortex NA
Brain stem Motor nucleus of facial nerve, superior salivatory nucleus of tractus solitarius
NA
Meatal segment Brain stem to IAC 13-15
Labyrinthine segment Fundus of IAC to facial hiatus 3-4
Tympanic segment Geniculate ganglion to pyramidal eminence
8-11
Mastoid segment Pyramidal process to stylomastoid foramen
10-14
Extratemporal segment Stylomastoid foramen to terminal branches
15-20
Segmental Description of the Facial Nerve and Central Connections
INTRODUCTION

• EMBRYOLOGY OF FACIAL NERVEBy the third week of gestation, the
fascioacoustic primordium gives rise to cranial nerves VII and VIII.
By the eleventh week, the facial nerve has arborized extensively.

Brancial motor(special visceral efferent)
Supplies the muscles of facial expression; posterior belly of digastric muscle; stylohyoid, and stapedius.
Visceral motor(general visceral efferent)
Parasympathetic innervation of the lcrimal, submandibular, and sublingual glands, as well as mucous membranes of nasopharynx, hard and soft palate.
Special sensory(special afferent)
Taste sensation from the anterior 2/3 of tongue; hard and soft palates.
General sensory(general somatic afferent)
General sensation from the skin of the concha of the auricle and from a small area behind the ear.
Component Overview
The facial nerve has four components with distinct functions:



• The facial nerve consists of a motor and a sensory part, the latter being frequently described under the name of the nervus intermedius
COURSE AND RELATIONS The facial nerve emerges from the brain stem with the
nerve of Wrisberg, i.e, the nervus intermedius ) The nervus intermedius conveys (1) afferent taste fibers
from the chorda tympani nerve, which come from the anterior two thirds of the tongue; (2) taste fibers from the soft palate via the palatine and greater petrosal nerves; and (3) preganglionic parasympathetic innervation to the submandibular, sublingual, and lacrimal glands. The fibers for taste originate in the nucleus of the tractus solitarius (NTS), and the fibers to the lacrimal, nasal, palatal mucus, and submandibular glands originate in the superior salivatory nucleus. Fibers to the lacrimal gland are carried with the greater superficial petrosal nerve until it exits the skull, where they branch off as the Vidian nerve

Proximal or labyrinthine segment
The labyrinthine segment of the facial nerve lies beneath the middle cranial fossa and is the shortest segment in the fallopian canal (approximately 3.5-4 mm in length).
The labyrinthine segment is the narrowest part of the facial nerve and is susceptible to compression by means of edema. This is the only segment of the facial nerve that lacks anastomosing arterial cascades, making the area vulnerable to embolic phenomena, low-flow states, or vascular compression

Tympanic or horizontal segment • The tympanic segment extends from the geniculate
ganglion to the horizontal semicircular canal and is 8-11 mm in length.
• The nerve passes behind the cochleariform process and the tensor tympani.
• The most important landmarks for identifying the facial nerve in the mastoid are the horizontal semicircular canal, the fossa incudis, and the digastric ridge.
• The digastric ridge points to the lateral and inferior aspect of the vertical course of the facial nerve in the temporal bone.
• The chorda tympani nerve and the fossa incudis can be used to identify the nerve when performing a facial recess approach.


Mastoid segment • The second genu marks the beginning of the mastoid
segment. The second genu is lateral and posterior to the pyramidal process.
• The mastoid segment is the longest part of the intratemporal course of the facial nerve, approximately 10-14 mm long. During middle ear surgery, the facial nerve is most commonly injured at the pyramidal turn.
• The 3 branches that exit from the mastoid segment of the facial nerve are (1) the nerve to the stapedius muscle, (2) the chorda tympani nerve, and (3) the nerve from the auricular branch of the vagus.
• The facial nerve exits the fallopian canal via the stylomastoid foramen. The nerve travels between the digastric and stylohyoid muscles and enters the parotid gland.
• A sensory branch exits the nerve just below the stylomastoid foramen and innervates the posterior wall of the external auditory canal and a portion of the tympanic membrane

NUCLEI
The fibres of the nerve arise from four nuclei situated in the lower pons
Motor nucleus(branchiomotor)Superior salivatory nucleus
(parasympathetic)Lacrimatory nucleus (parasympathetic)Nucleus of tractus solitarius(gustatory)

Branches of Communication.—The branches of communication of the facial nerve may be arranged as follows:
In the internal acoustic meatus………………
With the acoustic nerve.
At the genicular ganglion……………………
With the sphenopalatine ganglion by the greater superficial petrosal nerve.
With the otic ganglion by a branch which joins the lesser superficial petrosal nerve.
With the sympathetic on the middle meningeal artery.
In the facial canal…………………………… With the auricular branch of the vagus.
At its exit from the stylomastoid foramen……
With the glossopharyngeal.
With the vagus.
With the great auricular.
With the auriculotemporal.
Behind the ear……………………………… With the lesser occipital.
On face………………………………… With the trigeminal.
In the neck………………………………… With the cutaneous cervical

Branches of Distribution.—The branches of distribution of the facial nerve may be thus arranged:
With the facial canal…………………………..
Nerve to the Stapedius muscle.
Chorda tympani.
At its exit from the stylomastoid foramen………
Posterior auricular.
Digastric.
Stylohyoid.
On the face……………………………………
Temporal.
Zygomatic.
Buccal.
Mandibular.
Cervical.

• The greater superficial petrosal nerve (large superficial petrosal nerve) arises from the genicular ganglion, and consists chiefly of sensory branches which are distributed to the mucous membrane of the soft palate; but it probably contains a few motor fibers which form the motor root of the sphenopalatine ganglion.
• The Nerve to the Stapedius (n. stapedius; tympanic branch) arises opposite the pyramidal eminence ; it passes through a small canal in this eminence to reach the muscle.
• The Chorda Tympani Nerve is given off from the facial canal as it passes downward behind the tympanic cavity, about 6 mm. from the stylomastoid foramen.
• Before uniting with the lingual nerve the chorda tympani is joined by a small branch from the otic ganglion.
• The Posterior Auricular Nerve arises close to the stylo-mastoid foramen, and runs upward in front of the mastoid process; here it is joined by a filament from the auricular branch of the vagus, and communicates with the posterior branch of the great auricular, and with the lesser occipital.
• The auricular branch supplies the posterior auricle and the intrinsic muscles on the cranial surface of the auricle. The occipital branch, the larger, passes backward along the superior nuchal line of the occipital bone, and supplies the Occipitalis


The Digastric Branch The Stylohyoid Branch The Temporal Branches The Zygomatic Branches The Buccal Branches The Mandibular Branch The Cervical Branch
GANGLIA OF THE FACIAL NERVE• THE GENICULATE GANGLION• THE SUBMANDIBULAR GANGLION• Sympathetic root is derived from the plexus on the facial
artery ,consisting of postganglionic fibres arising from superior cervical ganglion and pass through submandibular ganglion without synapsing.
• Motor or parasympathetic root is formed by the posterior filament. It conveys preganglionic fibres from superior salivatory nucleus .
• PTERYGOPALATINE GANGLION
VASCULAR SUPPLY OF FACIAL NERVE

• ANATOMY OF FACIAL NERVE IN A CHILD AND ADULT
• Surgical landmarks to the facial nerve include the tympanomastoid suture line, the tragal pointer, and the posterior belly of the digastric muscle.
• The modified Blair incision most commonly used in adults is often avoided in children because the facial nerve is located more superficially, and the risk of injury is increased with elevation of the skin flaps.
• The main nerve trunk bifurcation is reported to be 15.6 mm inferior to the posterior aspect of tragus of ear or 23 mm inferior to the lowest concavity of the bony external auditory canal.
• Facial nerve damage following TMJ surgery usually results in eyebrow lag with occasional decrease in orbicularis oculi function,preventing complete closure of eyelid.
• Mandibular nerve is identified approximately 3.7 cm (range 3-4.2 cm) cephalad to the inferior limit of the submandibular gland.
• EVALUATION• FNFI (facial nerve function index)• APPLIED ANATOMY

• TESTING THE INTEGRITY OF FACIAL NERVE• FACIAL PALSYThis is paralysis due to the disease of neurons of the seventh
cranial nerve at Nucleus of origin Pons Passage through the facial canal In the stylomastoid foramenFacial nerve paralysis: Signs Facial asymmetry Eyebrow droop Loss of forehead &d nasolabial folds Drooping of corner of mouth Uncontrolled tearing Inability to close eye Lips cannot be held tightly together: Difficulty keeping food in mouth Facial muscle atrophy (Late).

• Signs and symptoms depends on the location of the lesions Lesions outside
stylomastoid foramen Lesions in the facial
canal(chorda tympani) Lesion higher in the facial
canal( nerve to stapedius) At the geniculate ganglion In internal auditory meatus In pons
MANAGEMENT

DIFFERENTIAL DIAGNOSIS OF 7TH NERVE DISOREDERS• Unilateral VII weakness
– Idiopathic: Bell's palsy – Sarcoid & other granulomatous disorders – Infection
• Leprosy: Especially with paralysis of upper face • Otitis media • Lyme disease • Herpes Zoster (Ramsay Hunt syndrome)
– Neoplasm & Masses – Trauma – Cardiofacial syndrome: Lower lip or complete facial palsy – Familial – CNS lesions
• Bilateral VII weakness – Melkersson syndrome – Möbius syndrome – Guillain Barré – Motor neuron disorders – Myasthenia gravis – Myopathies – Leprosy
• An-α-lipoproteinemia (Tangier)

• Central VII lesions – Pyramidal: Lower face paralysis with voluntary
motion – Emotional2: Face paralysis with emotion
• Anatomy: Dorsolateral pons lesion • Disorders
– Superior cerebellar artery infarction » Unilateral » With Deafness, Horner's, or reduced Sweating
– Extrapyramidal disorders » Bilateral » Parkinsonis

• FACIAL NERVE TRAUMA AND TUMOURS• Trauma
– Petrous bone fracture – Surgery: Middle ear; Mastoidectomy; Parotid gland
• Tumors & Masses– Tumor types
• Neuroma/Neurinoma/Schwannoma: Most common • Meningioma • Hemangioma: Produce defects even with small size • Cholesteatoma • Parotid gland • Metastasis • Carcinomatous meningitis • Paget: Osteopetrosis
– Tumor location
• Most common: Geniculate ganglion & Tympanic region • Tumors along multiple segments of VII nerve common • Rare: Middle cranial fossa

• FORCEPS DELIVERY AND FACIAL NERVE• DISSECTION OF THE FACIAL NERVE
INDICATIONS • The indications for superficial parotidectomy are as follows:
• Benign tumours or low-grade malignant tumours of small size and without involvement of the facial nerve in the superficial lobe of the parotid gland.
• Chronic inflammation of the parotid gland, resistant to conservative treatment.
• Tumour-like lesions in the parotid, such as nodular Sjögrens syndrome; oxyphilic lymphogranuloma

Dissection of the facial nerve and resection of the gland
Three surgical manoeuvres are used to identify the facial nerve trunk as
it exits the stylomastoid foramen. The blood free plane immediately in front of the cartilaginous external acoustic
meatus can be opened by blunt dissection ,and this leads the surgeon to the skull bases just superficial to the stolid process and stylomastoid foramen
• Second the trunk of the nerve can be identified by exposing the anterior border of sternocleidomastoid just below its insertion into tme mastoid process and retracting the muscle posteriorly to expose the posterior belly of digastric,which is then traced upwards and backwards to the mastoid process. This point lies immediately below the stylomastoid foramen and the facial nerve trunk
• Thirdly, a terminal branch is identified peripherally and it is traced back centripetally until the facial nerve trunk is identified.
• .