Evidence-Based Review and Consensus Statement on Monitoring of Hemodynamics and Oxygen Transport...
61
Introduction The Pediatric Cardiac Intensive Care Society evidence-based review and consensus statement on monitoring of hemodynamics and oxygen transport balance Paul A. Checchia, MD, FCCM, FACC; Ronald A. Bronicki, MD E very 2 yrs, the Pediatric Car- diac Intensive Care Society convenes a group of experts to develop and publish a scien- tific statement based on the available ev- idence and consensus opinion. Previous versions have dealt with the diagnosis and management of myocarditis and the acute management of pulmonary hyper- tension. This version addresses the mon- itoring of hemodynamics and oxygen transport balance in critically ill children. The primary objective in managing critically ill patients is to make a timely and accurate assessment of tissue oxy- genation. Studies in children and adults have demonstrated that the assessment of cardiovascular function and tissue oxy- genation based on the interpretation of conventional clinical data, such as the physical examination, blood pressure, and central venous pressure, is often dis- cordant from measured values. A writing committee was formed to examine the evidence and develop recommendations for various monitoring modalities. The findings were presented at the eighth In- ternational Meeting of the Pediatric Car- diac Intensive Care Society in December 2010. This supplement is meant to bring the reader from standard hemodynamic measurements such as blood pressure and heart rate through pulmonary artery cath- eters and ultimately to emerging technol- ogies just entering the marketplace. In addition to the presentation of the available evidence and recommendations, we sought to express an editorial opinion on the use of each modality. These are represented as perspectives and insights from leaders in the fields of neonatology, pediatric critical care medicine, pediatric cardiac critical care medicine, and pedi- atric critical care nursing. Additionally, we sought to interpret the evidence and recommendations from the perspective of critical care practitioners outside the boundaries of the United States. This supplement represents the re- sults of the work of the committee. As the Chairmen of the Writing Committee and Guest Editors of this supplement to Pe- diatric Critical Care Medicine, we would like to thank each committee member for his or her substantial efforts. Writing Committee: Paul A. Checchia, MD, FCCM, FACC, Cochair; Ronald A. Bronicki, MD, Cochair; Meredith Allen, MBBS, FRACP, FRCPCH, PhD, London, UK; Nick Anas, MD, Orange, CA; Jon T. Berger, MD, Washington, DC; Desmond Bohn, MB BCh, FFARCS, MRCP, FRCPC, Toronto, Ontario, Canada; David S. Cooper, MD, St. Petersburg, FL; Heidi J. Dalton, MD, Phoenix, AZ; Michelle Domico, MD, Orange, CA; Neil N. Finer, MD, San Diego, CA; Avihu Z. Gazit, MD, St. Louis, MO; Nancy S. Ghanayem, MD, Milwaukee, WI; Mary Fran Hazinski, MSN, FAAN, FAHA, BERC, Nashville, TN; George M. Hoffman, MD, Milwaukee, WI; John P. Kinsella, MD, Denver, CO; Niranjan Kissoon, MD, FRCPC, Vancouver, British Columbia, Can- ada; Darren Klugman, MD, MMS, Washing- ton, DC; Peter C. Laussen, MBBS, Boston, MA; Graeme MacLaren, MBBS, FCICM, FRACP, FCCM, Melbourne, Australia, and Singapore; Duncan J. Macrae, MB ChB, London, UK; Ronald M. Perkin, MD, MA, Greenville, NC; V. Ben Sivarajan, MD, FRCPC, Toronto, Ontario, Canada; Neil Spenceley, MB ChB, MRCPCH, Glasgow, Scotland; Dawn Tucker, MSN, CPNP-PC/ AC, Kansas City, MO; Gil Wernovsky, MD, Philadelphia, PA; and Hector R. Wong, MD, Cincinnati, OH. From the St. Louis Children’s Hospital (PAC), Washington University School of Medicine, St. Louis, MO; Children’s Hospital of Orange County (RAB), Uni- versity of California, Orange, CA; and the David Geffen School of Medicine at the University of California (RAB), Los Angeles, CA. Dr. Checchia has received honoraria from Edwards Lifesciences and Medimmune and grants from Ikaria. Dr. Bronicki has not disclosed any potential conflicts of interest. Copyright © 2011 by the Society of Critical Care Medicine and the World Federation of Pediatric Inten- sive and Critical Care Societies DOI: 10.1097/PCC.0b013e318220e64f S1 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
-
Upload
susanita1974 -
Category
Documents
-
view
289 -
download
12
Transcript of Evidence-Based Review and Consensus Statement on Monitoring of Hemodynamics and Oxygen Transport...

Introduction
The Pediatric Cardiac Intensive Care Society evidence-based reviewand consensus statement on monitoring of hemodynamics andoxygen transport balance
Paul A. Checchia, MD, FCCM, FACC; Ronald A. Bronicki, MD
Every 2 yrs, the Pediatric Car-diac Intensive Care Societyconvenes a group of experts todevelop and publish a scien-
tific statement based on the available ev-idence and consensus opinion. Previousversions have dealt with the diagnosisand management of myocarditis and theacute management of pulmonary hyper-tension. This version addresses the mon-itoring of hemodynamics and oxygentransport balance in critically ill children.
The primary objective in managingcritically ill patients is to make a timelyand accurate assessment of tissue oxy-genation. Studies in children and adultshave demonstrated that the assessment ofcardiovascular function and tissue oxy-genation based on the interpretation ofconventional clinical data, such as the
physical examination, blood pressure,and central venous pressure, is often dis-cordant from measured values. A writingcommittee was formed to examine theevidence and develop recommendationsfor various monitoring modalities. Thefindings were presented at the eighth In-ternational Meeting of the Pediatric Car-diac Intensive Care Society in December2010. This supplement is meant to bringthe reader from standard hemodynamicmeasurements such as blood pressure andheart rate through pulmonary artery cath-eters and ultimately to emerging technol-ogies just entering the marketplace.
In addition to the presentation of theavailable evidence and recommendations,we sought to express an editorial opinionon the use of each modality. These arerepresented as perspectives and insightsfrom leaders in the fields of neonatology,pediatric critical care medicine, pediatriccardiac critical care medicine, and pedi-atric critical care nursing. Additionally,we sought to interpret the evidence andrecommendations from the perspective ofcritical care practitioners outside theboundaries of the United States.
This supplement represents the re-sults of the work of the committee. As theChairmen of the Writing Committee andGuest Editors of this supplement to Pe-diatric Critical Care Medicine, we would
like to thank each committee member forhis or her substantial efforts.
Writing Committee: Paul A. Checchia,MD, FCCM, FACC, Cochair; Ronald A.Bronicki, MD, Cochair; Meredith Allen,MBBS, FRACP, FRCPCH, PhD, London,UK; Nick Anas, MD, Orange, CA; Jon T.Berger, MD, Washington, DC; DesmondBohn, MB BCh, FFARCS, MRCP, FRCPC,Toronto, Ontario, Canada; David S. Cooper,MD, St. Petersburg, FL; Heidi J. Dalton,MD, Phoenix, AZ; Michelle Domico, MD,Orange, CA; Neil N. Finer, MD, San Diego,CA; Avihu Z. Gazit, MD, St. Louis, MO;Nancy S. Ghanayem, MD, Milwaukee, WI;Mary Fran Hazinski, MSN, FAAN, FAHA,BERC, Nashville, TN; George M. Hoffman,MD, Milwaukee, WI; John P. Kinsella, MD,Denver, CO; Niranjan Kissoon, MD,FRCPC, Vancouver, British Columbia, Can-ada; Darren Klugman, MD, MMS, Washing-ton, DC; Peter C. Laussen, MBBS, Boston,MA; Graeme MacLaren, MBBS, FCICM,FRACP, FCCM, Melbourne, Australia, andSingapore; Duncan J. Macrae, MB ChB,London, UK; Ronald M. Perkin, MD, MA,Greenville, NC; V. Ben Sivarajan, MD,FRCPC, Toronto, Ontario, Canada; NeilSpenceley, MB ChB, MRCPCH, Glasgow,Scotland; Dawn Tucker, MSN, CPNP-PC/AC, Kansas City, MO; Gil Wernovsky, MD,Philadelphia, PA; and Hector R. Wong, MD,Cincinnati, OH.
From the St. Louis Children’s Hospital (PAC),Washington University School of Medicine, St. Louis,MO; Children’s Hospital of Orange County (RAB), Uni-versity of California, Orange, CA; and the David GeffenSchool of Medicine at the University of California (RAB),Los Angeles, CA.
Dr. Checchia has received honoraria from EdwardsLifesciences and Medimmune and grants from Ikaria.Dr. Bronicki has not disclosed any potential conflicts ofinterest.
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e318220e64f
S1Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Hemodynamic Monitoring
Monitoring of standard hemodynamic parameters: Heart rate,systemic blood pressure, atrial pressure, pulse oximetry, andend-tidal CO2
V. Ben Sivarajan, MD, FRCPC; Desmond Bohn, MB, FRCPC
Clinical assessment and fre-quent reassessment is essen-tial in critically ill childrenbecause “normal” parameters
are less guided by published populationcurves (Table 1) and more by trends es-tablished during monitoring of the indi-vidual patient.
The goal of such monitoring is to al-low anticipatory management of infantsand children. Relationships between spe-cific hemodynamic variables are complex
enough in states of health. In diseasestates, the specific responses of heartrate, central venous pressure, and bloodpressure to treatments are essential torapid diagnosis and curative therapy.
Appropriate monitoring allows one tocomprehend etiologic and compensatoryfactors contributing to shock pathophys-iology. This allows the clinician to calcu-late secondary parameters (Table 2) thatare paramount in executing specific ther-apeutic strategies (1). However, the pri-macy of monitoring lies in documenta-tion of improved outcomes based onhemodynamic monitor-driven treat-ments in controlled clinical studies. Thequestion of whether there is sufficientscientific evidence supporting or discour-aging standard monitoring practices inpediatric critical care is the basis for thisreview.
Process
MEDLINE, EMBASE, PubMed, andCochrane Database searches were con-ducted to find controlled trials regardingthe use of heart rate, noninvasive andinvasive pressure, end-tidal carbon diox-ide, and pulse oximetry monitoring.Adult and pediatric data were considered.
Guidelines published by the Society forCritical Care Medicine, the AmericanHeart Association, the American Acad-emy of Pediatrics, and the InternationalLiaison Committee on Resuscitation werereviewed, including further review of ref-erences cited.
Background
As the discipline of critical care med-icine evolved out of the battlefields ofNormandy and the MASH (Mobile ArmySurgical Hospital) units of Korea, the im-portance of objective vital sign monitor-ing became singularly apparent. In 1952,a study by Ibsen (2, 3) had demonstratedthat operating room techniques such astracheotomy and curare could be used inan intensive care unit setting. In 1953, heconverted the surgical recovery ward inCopenhagen’s Kommunehospital into thefirst intensive care unit (ICU) (2, 4). TheICU established by Dr. Peter Safar at Bal-timore City Hospital emphasized bedsideresuscitative interventions and the pri-mary importance of maintenance of air-way and breathing (5). At the Universityof Southern California, Drs. Max Weil andHerbert Shubin became interested in whypatients died suddenly after a myocardial
From the Divisions of Cardiac Critical Care andCardiology (VBS), Departments of Critical Care Medi-cine and Paediatrics, The Labatt Family Heart Centre,The Hospital for Sick Children, Toronto, Ontario, Can-ada, and the Department of Critical Care Medicine andPaediatrics, Faculty of Medicine, University of Toronto,Toronto, Ontario, Canada; and the Department of Crit-ical Care Medicine (DB), Hospital for Sick Children,Professor of Anaesthesia and Paediatrics, University ofToronto, Department of Critical Care Medicine, Hospitalfor Sick Children, Toronto, Ontario, Canada.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e318220e7ea
Background: Continuous monitoring of various clinical param-eters of hemodynamic and respiratory status in pediatric criticalcare medicine has become routine. The evidence supporting thesepractices is examined in this review.
Methodology: A search of MEDLINE, EMBASE, PubMed, and theCochrane Database was conducted to find controlled trials ofheart rate, electrocardiography, noninvasive and invasive bloodpressure, atrial pressure, end-tidal carbon dioxide, and pulseoximetry monitoring. Adult and pediatric data were considered.Guidelines published by the Society for Critical Care Medicine, theAmerican Heart Association, the American Academy of Pediatrics,and the International Liaison Committee on Resuscitation werereviewed, including further review of references cited.
Results and Conclusions: Use of heart rate, electrocardiogra-phy, noninvasive and arterial blood pressure, atrial pressure,
pulse oximetry, and end-tidal carbon dioxide monitoring in thepediatric critical care unit is commonplace; this practice, how-ever, is not supported by well-controlled clinical trials. Despitethe majority of literature being case series, expert opinion wouldsuggest that use of routine pulse oximetry and end-tidal carbondioxide is the current standard of care. In addition, literaturewould suggest that invasive arterial monitoring is the currentstandard for monitoring in the setting of shock. The use of heartrate, electrocardiography. and atrial pressure monitoring is ad-vantageous in specific clinical scenarios (postoperative cardiacsurgery); however, the evidence for this is based on numerouscase series only. (Pediatr Crit Care Med 2011; 12[Suppl.]:S2–S11)
KEY WORDS: hemodynamic monitoring; heart rate; systemicblood pressure; atrial pressure; pulse oximetry; end-tidal CO2
S2 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

infarction, serious illness, or in the post-operative period (6). They realized thatthe absence of continuous vital sign as-sessment practically precluded the oppor-tunities for lifesaving measures. The es-tablishment of their initial four-bedshock unit, that combined efforts of ded-icated ICU physicians, nurses, engineers,and technicians, was one of the first tofocus on monitoring, measurement, andalarms in real time to target appropriatelifesaving interventions (6, 7).
Pulse, heart rate, andelectrocardiographic monitoring
Galen first provided physiological de-scriptions of pulse in the second centuryAD; however, its use was noted by theearly Egyptians (8). In the Western world,assessment of vital signs continued to bedismissed as “quackery” as recently as themid-19th century. The advent of coro-
nary care units, resuscitative practices,and definitive therapies made continuousvital sign assessment necessary and prac-tical (9, 10).
Pulse assessment is currently providedby a number of complementary methods:intermittent assessment using direct pal-pation or cuff sphygmomanometry, orcontinuous assessment through pulseoximetry or invasive arterial pressuremonitoring. Recognizing the nuances ofpulse contour and strength can provideinstantaneous insights into the underly-ing pathologic process. With the adventof widespread application of pulse oxim-etry technology, continuous pulse moni-toring became practicable and providedearlier clues to potential bradycardic ortachycardic states (11). Confirmation ofthese states and their potential effects oncardiac output, systemic oxygen delivery,and tissue perfusion still requires a com-plementary clinical assessment.
Heart rate trend review, available onbedside monitors since the early 1990s,provides insight into underlying mecha-nisms of disease. For example, a period ofpostoperative tachycardia can be re-viewed and decisions can be made regard-ing the pathologic process and its appro-priate therapy (Fig. 1).
Electrocardiographic monitoring be-came routinely used in adult critical carethroughout the 1970s and in the 1980s,bedside arrhythmia analysis and bed-to-bed switching allowed its widespread useso that a central monitoring station wasnot required. Widespread adoption in pe-diatric ICUs did not occur until the late1980s with the advent of modular unitsthat allowed input from various devices.At this time the potential for arrhythmiain postoperative cardiac (12) and variousorgan dysfunction states was becomingappreciated. Focused attention to ST-segment changes has been commonplaceafter operations that involve manipula-tion of the coronary origins such as thearterial switch operation and the Rossoperation (Fig. 2). This potential use ofST-segment analysis needs to be balancedby the limitations of algorithms used bycurrently available software for this pur-pose in the pediatric population.
“Evidenced-based” guidelines were re-cently published for electrocardiographicmonitoring in adults and children, sug-gesting that all patients requiring inten-sive care and children after cardiac sur-gery have class I indications for suchmonitoring. However, the references pro-
Figure 1. The value of trend heart rate monitor-ing is illustrated here in differentiating the causeof tachycardia. Patient A has an abrupt onset andtermination diagnostic of a re-entrant mecha-nism, whereas patient B has the gradual increaseassociated with an automatic focus (most com-monly sinus tachycardia).
Table 1. Vital signs at various ages
AgeHeart Rate(beats/min)
Blood Pressure (mmHg)(systolic/diastolic)
RespiratoryRate (breaths/min)
Premature 120–170 55–75/35–45 40–700–3 mo 100–150 65–85/45–55 35–553–6 mo 90–120 70–90/50–65 30–456–12 mo 80–120 80–100/55–65 25–401–3 yr 70–110 90–105/55–70 20–303–6 yr 65–110 95–110/60–75 20–256–12 yr 60–95 100–120/60–75 14–22�12 yr 55–85 110–135/65–85 12–18
Adapted from Mathers LH, Frankel LR. The acutely ill child. In: Nelson Textbook of Pediatrics 17thedition. Berhman, Kliegman, Jenson (Eds). Philadelphia, PA, Saunders, an Imprint of Elsevier Science,2003.
Table 2. Primary and derived hemodynamicparameters from hemodynamic monitoring
Primary hemodynamic parametersHR, beats/minMAP, mm HgCVP or RAP, mm HgLAP or PAOP, mm HgPAP, mm HgCO, L/mina
SaO2, %SpO2 as an estimate of SaO2, %SvO2, %Hb, g/LHeight and weight needed to calculate BSA, m2
Derived hemodynamic parametersCI � CO/BSA, L/min/m2
Stroke volume � CO/HR � 1000, mL/minStroke index � stroke volume/BSA, mL/m2
LV stroke work � stroke volume �(MAP � PAOP), mL�mm Hg
LV stroke work index � LV strokework/BSA, mL�mm Hg/m2
Total peripheral resistance � (MAP/CO) �80, dyne�s/cm5
Systemic vascular resistance �(�MAP � RAP�)/CO � 80, dyne�s/cm5
Pulmonary vascular resistance �(�PAP – PAOP�/CO) � 80, dyne�s/cm5
Global DO2b � CO � (SaO2 � SvO2) � Hb �
1.36 � 1000, mL oxygen/minGlobal DO2 indexb � CI � (SaO2 � SvO2)
Hb � 1.36, mL oxygen/minGlobal VO2
b � CO � SaO2 � Hb � 1.36 �1000, mL oxygen/min
Global VO2 indexb � CI � SaO2 � Hb �1.36 � 1000, mL oxygen/min
MAP, mean arterial pressure; CVP, central ve-nous pressure; HR, heart rate; RAP, right atrialpressure; LAP, left atrial pressure; PAOP, pulmo-nary arterial occlusion pressure; PAP, mean pulmo-nary artery pressure; CO, cardiac output; SaO2, ar-terial oxygen saturation; SvO2, central/mixedvenous oxygen saturation; Hb, hemoglobin; BSA,body surface area; CI, cardiac index; VO2, oxygenconsumption; DO2, systemic oxygen delivery.
aContinuous measurement not reliable insmall children and in those with shunt lesions;bSpO2 can be substituted for arterial oxygen sat-uration in these calculations.
S3Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

vided do not support this level of asser-tion in the pediatric population (13).
Evidence and recommendations forthe use of heart rate and electrocardio-graphic monitoring. Pulse and heart ratemonitoring with 12- to 15-lead electrocar-diographic monitoring has been adopted asa standard during surgery (cardiac or oth-erwise), cardiac catheterization, and forpostoperative ICU care. It improves diag-nostic precision and is a major enhance-ment to patient safety and quality care.There is sufficient evidence to support itsroutine use in these situations but, likemany monitoring devices, this recommen-
dation is based on case series and observa-tional studies (level of evidence: IV; grade ofrecommendation: C).
Blood pressure monitoring
History. Despite the observation ofblood “pulsating” from shorn blood ves-sels throughout recorded history, it wasnot until the mid-18th century when thefirst recorded measurements of invasiveblood pressure were made on a horse byStephen Hale (14).
In 1828, Poiseuille described the useof a mercury manometer connected to an
arterial cannula to measure arterial pres-sure as part of his doctoral dissertation(15). Poiseulle’s innovation enabled CarlLudwig to develop the kymograph (orwave-writer) in 1847. This advance pavedthe way for modifications used today suchas the myograph (developed by Helm-holtz in 1850 for recording muscle move-ments) and the sphygmograph (devel-oped by Vierordt in 1855).
Noninvasive Blood Pressure Measure-ment. Until 1855, a noninvasive methodof blood pressure assessment in the clin-ical situation remained elusive. Vierordthypothesized that indirect assessmentmight be made by assessing the counterpulsation necessary to cause cessation ofthe arterial pulse. Although his devicewas somewhat cumbersome, a modifica-tion by Marey gained wide acceptance inmedical practice (Fig. 3).
In the 1870s, von Basch developed theidea of sphygmomanometry, the present-day technique of which is based on Riva-Rocci’s method reported in 1896 (16).The advantages of this technology are:ease of application; rapidity in action;precision; and patient comfort. Thismethod was useful for systolic pressuremeasurement but was useless for accu-rate diastolic pressure measurement. Hilland Barnard (17) subsequently developeda small portable apparatus that used theoscillatory method with a needle pressuregauge sensitive enough to precisely re-cord the diastolic pressure. In 1905,Korotkoff, a Russian surgeon, reportedthe auscultatory method, in which hecontrolled the pressure in the Riva-Roccicuff while listening with a monaural de-vice that was a direct descendant of Laen-nec’s rod (16).
Current Noninvasive Methods ofBlood Pressure Assessment in the Pediat-ric ICU. Use of the oscillometric methodwith devices such as the Dinamap (Devicefor Indirect Non Invasive Measurement ofBlood Pressure; GE Healthcare, Wauke-sha, WI) represents the usual standard fornoninvasive measurement in most pedi-atric settings. Park and colleagues estab-lished in a number of landmark studiesthe degree of reproducibility and reliabil-ity of this technique for pediatric agegroups (18–22) in the outpatient setting.Friesen and Lichtor (23) were the first toshow the high degree of precision andreliability of oscillometric systolic bloodpressure compared with indwelling arte-rial lines in a series of neonates. A studyby Cullen et al subsequently analyzed 260paired comparisons from 16 neonates
Figure 2. Demonstration of midprecordial ST-segment elevation after an arterial switch operation.These findings should prompt urgent investigation and therapy directed toward establishing theadequacy of the coronary anastomosis.
Figure 3. A, Vierordt’s sphygmograph, invented in 1854. Pad b is applied over the radial artery. Weightsare placed in the large cup until the pulse wave is traced; then weights are placed in the smaller cupwhich acts as a fine adjuster. B, A direct sphygmograph attributed to Marey, circa 1881. Reproducedwith permission from the Wellcome Institute for the History of Medicine and Booth J: A short historyof blood pressure measurement. Proc R Soc Med 1977; 70:793–799.
S4 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

with indwelling arterial lines during an-esthesia. A regression analysis over a widerange of blood pressures demonstratedhigh correlation for heart rate and sys-tolic blood pressure with moderate cor-relation for mean blood pressure andpoor correlation for diastolic blood pres-sure. They concluded that the oscillomet-ric technique represented an accuratetrend monitor for heart rate and bloodpressure for stable neonates with greaterbias at lower blood pressures.
It is important to take pause to notethat the goal is to monitor and optimizecardiac output; however, we generallyrely on clinical examination and monitor-ing of surrogates such as heart rate andblood pressure. Thus, a “good” bloodpressure does not always indicate ade-quate cardiac output. It is a well-recog-nized phenomenon that lowering bloodpressure (with afterload reduction) im-proves cardiac output in selected clinicalsituations. However, a number of studieshave demonstrated that inadequatelytreated hypotension and arterial hypoxemiacan be predictive of mortality in variousshock states (24–26) and after cardiac ar-rest (27–30). Thus, in these critically illpatients, it is vital to ensure the most ap-propriate modalities of monitoring.
A number of emergency departmentand operating room-based studies inadults have recently shown that oscillo-metric methods may have a role (31–33)in mild shock. Regardless of age group,traditional noninvasive methods havebeen shown to be unreliable and inade-quate for diastolic pressure assessment aswell as in patients with low cardiac output,hypotension, and/or dysrhythmias (34–38).Despite current guidelines supporting inva-sive arterial pressure monitoring in septicshock (39), a recent survey of adult inten-sivists (40) indicated that in hypotensiveand frank shock states, 73% and 47%, re-spectively, relied solely on noninvasivemethods. The standard in these clinical sit-uations continues to be invasive arterialpressure measurement.
Invasive Arterial Blood Pressure Mea-surement: Principles and Technique. De-spite refinements over the centuries, thetechnique of arterial pressure measure-ment is essentially unchanged from themethods described in the study by Hale(14). Invasive arterial measurement con-tinues to constitute the gold standard formeasurement in critically ill patientsboth in pediatrics and adults. The inva-sive arterial pressure monitor allowstitration of both inspired oxygen (by
monitoring the alveolar–arterial PO2 gra-dient) and vasoactive medications.
Invasive pressure monitoring, however,has technical limitations that can make thedisplayed information inaccurate. Invasivepressure measurement systems are indirectand thus require calibration to a reference(41) (right atrium for cardiovascular pres-sures, tragus of the ear for intracranialpressure monitoring).
Monitoring systems are based on theprinciple of transmitting pressurechanges from a column of uncompress-ible fluid (in an ideally incompressibletube) to a mechanical transducer. Themechanical transducer is basically a dis-placeable diaphragm, which convertsphysical fluid displacement into a propor-tional electrical signal, which can be pro-cessed and displayed. Factors that mayaffect the quality of measurement includethe compliance, resistance, and imped-ance of the system; this can result in thealteration of the recorded signal. Seem-ingly minor issues such as bubbles in thetubing can result in “dampening” of thepressure waveform. Other important fac-tors include the frequency response ofthe system and the sampling rate.
The usual sites of arterial pressuremonitoring in pediatrics include the ra-dial, femoral, and posterior tibial arteries.Less frequently used sites, especially insmaller infants, include the brachial andaxillary arteries. During a 6-yr period,Mortenson and colleagues (42) collecteddetails and follow-up on almost 3200 ar-terial cannulations in 2360 patients. Thisstudy informed refinement of accesstechniques and locations both for moni-toring and catheterization studies. Can-nulations were performed by percutane-ous needle puncture, a percutaneousSeldinger technique, or cutdown arteri-otomy. The overall minor complicationrate (pain, bleeding, transient loss ofpulse) was approximately 10% with majorcomplication rates of 1% to 2% (distalischemia, loss of limb). The complicationrate was increased with the Seldingertechnique, use of the brachial arterialsite, and in children aged �10 yrs (thecomplication rate approached 30% in thispopulation). Contemporary studies havealso discouraged cannulation of the bra-chial artery based on higher complicationrates (43, 44).
Evidence and Recommendations forthe Use of Blood Pressure Monitoring.Routine blood pressure monitoring hasbecome an accepted standard for all pe-diatric patients undergoing surgery, as
well as for those patients who warrantpostoperative monitoring in an ICU envi-ronment. The choice of frequency andmodality are based on the severity of ill-ness as well as the need for additionaldata such as an accurate diastolic bloodpressure or arterial blood gases. Invasivearterial pressure monitoring in all intra-operative and postoperative ICU patients(especially those requiring cardiac sur-gery) continues to be the accepted stan-dard. In addition, most patients duringcardiac catheterization and all patientswith shock should have attempts to se-cure invasive arterial pressure monitor-ing. There is sufficient evidence to sup-port its routine use in these situations(level of evidence: IV; grade of recom-mendation: C).
Central venous and left atrialpressure monitoring
Central Venous Pressure Monitoring.Continuous assessment of pressure wave-forms and filling pressures is provided bycentral venous pressure monitoring. Thecentral venous pressure is often used in-appropriately to assess the intravascularvolume status. It is important to notethat the truly important intravascularvolume parameter is the left ventricularend-diastolic volume because this di-rectly impacts stroke volume and ulti-mately systemic cardiac output. Assess-ing at the bedside on a continuous basisis both imprecise and impractical. As aresult, because the instantaneous rela-tionship between pressure and volume isknown (assuming loading conditions donot change and the patient is maintainedon the same pressure–volume curve),monitoring of left ventricular end-diastolic pressure can impart this sameinformation. In the absence of significantmitral valve stenosis, the left atrial pres-sure also provides this information. Mon-itoring catheters in the proximal circula-tion (i.e., central venous pressure orSwan-Ganz as opposed to direct left atrialpressure) are routinely placed at the bed-side by intensivists. Catheters in thesepositions minimize complication ratesand reduce dependence on surgical place-ment; however, such measures are oftenpoor estimates of left ventricular end-diastolic volume as a result of the multi-ple additional assumptions as well as theeffect of cardiopulmonary interactions.As a result, central venous pressure isbest used to assess the relative impedanceto systemic venous return imposed by the
S5Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
right heart. If the central venous pressureis high, the patient will require a highermean circulatory filling pressure (eitherby infusion of volume or by augmentingvenoconstriction) to maintain right ven-tricular preload. In addition, the changein central venous pressure to a fluid chal-lenge is also a valuable assessment ofventricular compliance.
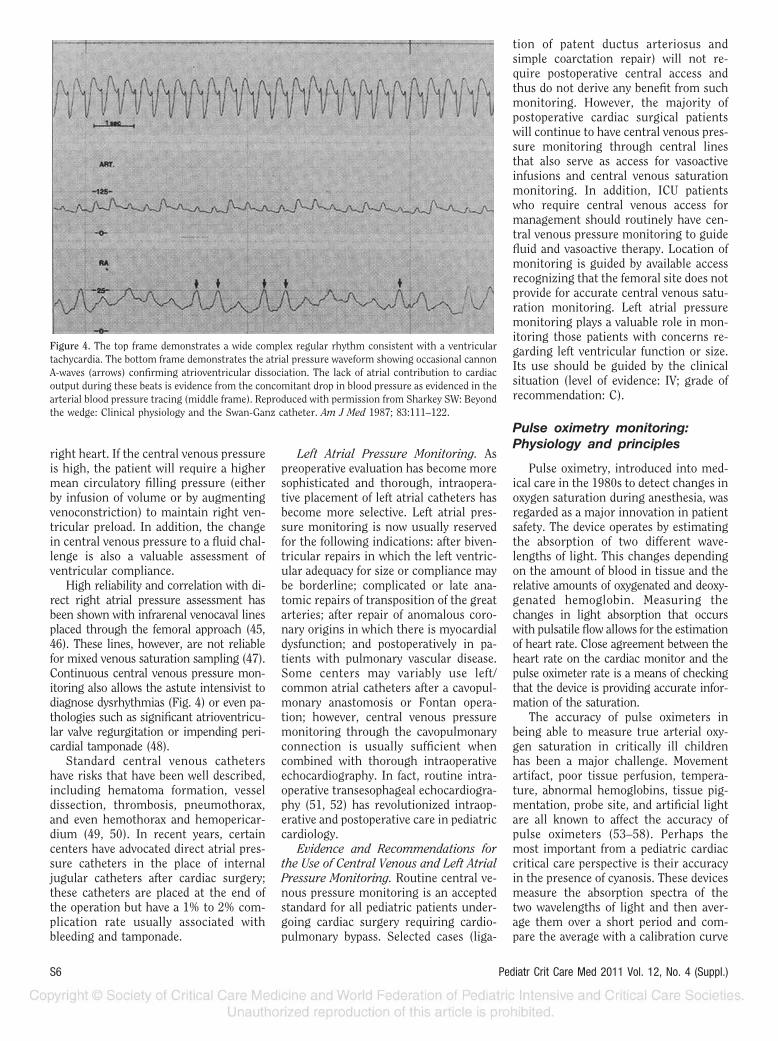
High reliability and correlation with di-rect right atrial pressure assessment hasbeen shown with infrarenal venocaval linesplaced through the femoral approach (45,46). These lines, however, are not reliablefor mixed venous saturation sampling (47).Continuous central venous pressure mon-itoring also allows the astute intensivist todiagnose dysrhythmias (Fig. 4) or even pa-thologies such as significant atrioventricu-lar valve regurgitation or impending peri-cardial tamponade (48).
Standard central venous cathetershave risks that have been well described,including hematoma formation, vesseldissection, thrombosis, pneumothorax,and even hemothorax and hemopericar-dium (49, 50). In recent years, certaincenters have advocated direct atrial pres-sure catheters in the place of internaljugular catheters after cardiac surgery;these catheters are placed at the end ofthe operation but have a 1% to 2% com-plication rate usually associated withbleeding and tamponade.
Left Atrial Pressure Monitoring. Aspreoperative evaluation has become moresophisticated and thorough, intraopera-tive placement of left atrial catheters hasbecome more selective. Left atrial pres-sure monitoring is now usually reservedfor the following indications: after biven-tricular repairs in which the left ventric-ular adequacy for size or compliance maybe borderline; complicated or late ana-tomic repairs of transposition of the greatarteries; after repair of anomalous coro-nary origins in which there is myocardialdysfunction; and postoperatively in pa-tients with pulmonary vascular disease.Some centers may variably use left/common atrial catheters after a cavopul-monary anastomosis or Fontan opera-tion; however, central venous pressuremonitoring through the cavopulmonaryconnection is usually sufficient whencombined with thorough intraoperativeechocardiography. In fact, routine intra-operative transesophageal echocardiogra-phy (51, 52) has revolutionized intraop-erative and postoperative care in pediatriccardiology.
Evidence and Recommendations forthe Use of Central Venous and Left AtrialPressure Monitoring. Routine central ve-nous pressure monitoring is an acceptedstandard for all pediatric patients under-going cardiac surgery requiring cardio-pulmonary bypass. Selected cases (liga-
tion of patent ductus arteriosus andsimple coarctation repair) will not re-quire postoperative central access andthus do not derive any benefit from suchmonitoring. However, the majority ofpostoperative cardiac surgical patientswill continue to have central venous pres-sure monitoring through central linesthat also serve as access for vasoactiveinfusions and central venous saturationmonitoring. In addition, ICU patientswho require central venous access formanagement should routinely have cen-tral venous pressure monitoring to guidefluid and vasoactive therapy. Location ofmonitoring is guided by available accessrecognizing that the femoral site does notprovide for accurate central venous satu-ration monitoring. Left atrial pressuremonitoring plays a valuable role in mon-itoring those patients with concerns re-garding left ventricular function or size.Its use should be guided by the clinicalsituation (level of evidence: IV; grade ofrecommendation: C).
Pulse oximetry monitoring:Physiology and principles
Pulse oximetry, introduced into med-ical care in the 1980s to detect changes inoxygen saturation during anesthesia, wasregarded as a major innovation in patientsafety. The device operates by estimatingthe absorption of two different wave-lengths of light. This changes dependingon the amount of blood in tissue and therelative amounts of oxygenated and deoxy-genated hemoglobin. Measuring thechanges in light absorption that occurswith pulsatile flow allows for the estimationof heart rate. Close agreement between theheart rate on the cardiac monitor and thepulse oximeter rate is a means of checkingthat the device is providing accurate infor-mation of the saturation.
The accuracy of pulse oximeters inbeing able to measure true arterial oxy-gen saturation in critically ill childrenhas been a major challenge. Movementartifact, poor tissue perfusion, tempera-ture, abnormal hemoglobins, tissue pig-mentation, probe site, and artificial lightare all known to affect the accuracy ofpulse oximeters (53–58). Perhaps themost important from a pediatric cardiaccritical care perspective is their accuracyin the presence of cyanosis. These devicesmeasure the absorption spectra of thetwo wavelengths of light and then aver-age them over a short period and com-pare the average with a calibration curve
Figure 4. The top frame demonstrates a wide complex regular rhythm consistent with a ventriculartachycardia. The bottom frame demonstrates the atrial pressure waveform showing occasional cannonA-waves (arrows) confirming atrioventricular dissociation. The lack of atrial contribution to cardiacoutput during these beats is evidence from the concomitant drop in blood pressure as evidenced in thearterial blood pressure tracing (middle frame). Reproduced with permission from Sharkey SW: Beyondthe wedge: Clinical physiology and the Swan-Ganz catheter. Am J Med 1987; 83:111–122.
S6 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
of arterial saturations developed from ex-periments on volunteers (59). These ex-periments were not done at the low sat-urations seen in cyanotic congenitalheart disease, and hence there will besome discrepancy between pulse oxime-try and directly measured saturations inthis group of patients. Most of these caseseries consist of �50 patients of differentage groups and consist of a mixture ofcyanotic and acyanotic forms of congen-ital heart disease. When saturations are�90%, most devices have a precision ofapproximately � 2%. However, in therange of significant desaturation(�80%), an increasing bias has been ob-served with a tendency for pulse oxime-ters to overread the true saturation whencompared with direct arterial sampling(11, 60–67). The accuracy of devices hasalso been shown to be enhanced by ap-plying the probe to the finger rather thanthe foot (68, 69).
Pulse Oximetry in the PerioperativeSetting and During Cardiac Catheteriza-tion. An extensive experience has beenaccumulated in the use of pulse oxime-ters during pediatric surgery and cardiaccatheterization. One of the original stud-ies that secured its widespread accep-tance as an essential monitoring device inpediatric anesthesia was the single-blindstudy by Cote et al (70) in 1988 in which152 children undergoing elective surgerywere divided into two groups. In onegroup the oximeter data and alarms wereavailable to the anesthesia team, and inthe second group a trained observer re-corded all episodes of drop in saturationon the monitor but only informed theanesthesia team of major events, i.e.,when the pulse oximetry was �85%.There were three times as many events inthe trained observer group and thesewere most common in children �2 yrs ofage. The patients in this study did notinclude children with congenital heartdisease; however, since then, pulse oxi-meters have been used extensively inmonitoring patients undergoing heartsurgery, in the postoperative period inthe ICU, or during cardiac catheteriza-tion (11, 58–62, 64–69, 71–77).
Evidence and Recommendations forthe Use of Pulse Oximetry. Pulse oxime-try has been adopted as a standard mon-itoring device during cardiac surgery,postoperative ICU care, and cardiac cath-eterization and is a major enhancementto patient safety. There is sufficient evi-dence to support its routine use in thesesituations but, as with many monitoring
devices, this recommendation is based oncase series and observational studies(level of evidence: IV; grade of recom-mendation: C).
Capnography and end-tidal CO2
monitoring: Physiology andprinciples
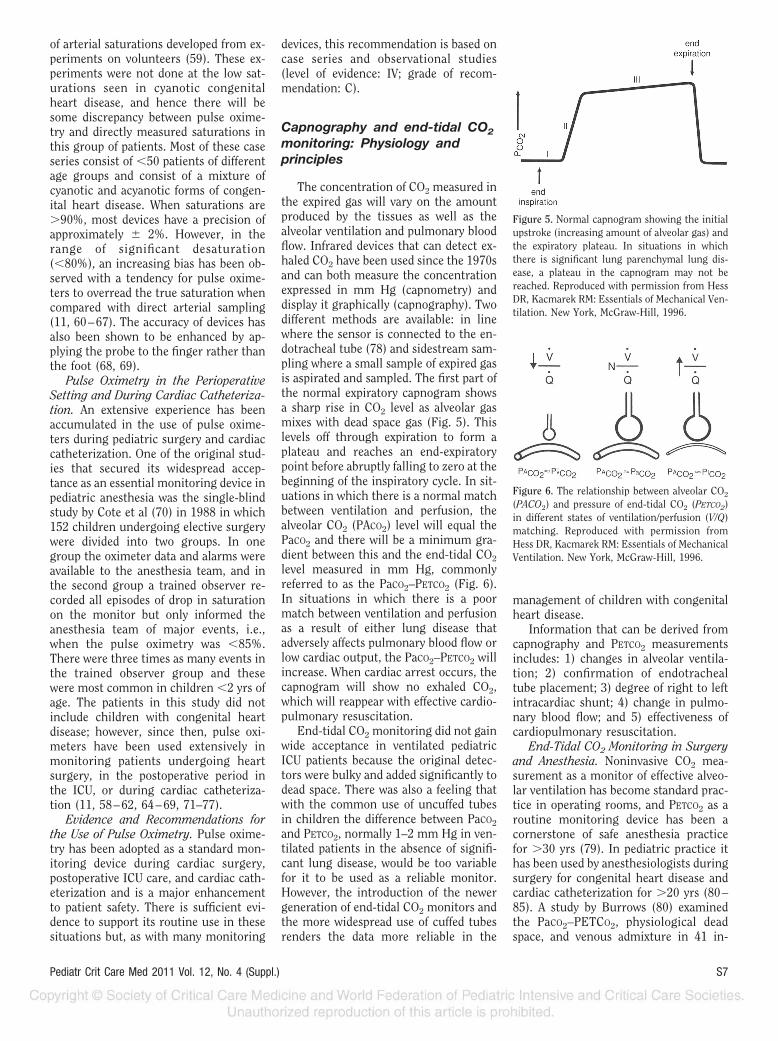
The concentration of CO2 measured inthe expired gas will vary on the amountproduced by the tissues as well as thealveolar ventilation and pulmonary bloodflow. Infrared devices that can detect ex-haled CO2 have been used since the 1970sand can both measure the concentrationexpressed in mm Hg (capnometry) anddisplay it graphically (capnography). Twodifferent methods are available: in linewhere the sensor is connected to the en-dotracheal tube (78) and sidestream sam-pling where a small sample of expired gasis aspirated and sampled. The first part ofthe normal expiratory capnogram showsa sharp rise in CO2 level as alveolar gasmixes with dead space gas (Fig. 5). Thislevels off through expiration to form aplateau and reaches an end-expiratorypoint before abruptly falling to zero at thebeginning of the inspiratory cycle. In sit-uations in which there is a normal matchbetween ventilation and perfusion, thealveolar CO2 (PACO2) level will equal thePaCO2 and there will be a minimum gra-dient between this and the end-tidal CO2
level measured in mm Hg, commonlyreferred to as the PaCO2–PETCO2 (Fig. 6).In situations in which there is a poormatch between ventilation and perfusionas a result of either lung disease thatadversely affects pulmonary blood flow orlow cardiac output, the PaCO2–PETCO2 willincrease. When cardiac arrest occurs, thecapnogram will show no exhaled CO2,which will reappear with effective cardio-pulmonary resuscitation.
End-tidal CO2 monitoring did not gainwide acceptance in ventilated pediatricICU patients because the original detec-tors were bulky and added significantly todead space. There was also a feeling thatwith the common use of uncuffed tubesin children the difference between PaCO2
and PETCO2, normally 1–2 mm Hg in ven-tilated patients in the absence of signifi-cant lung disease, would be too variablefor it to be used as a reliable monitor.However, the introduction of the newergeneration of end-tidal CO2 monitors andthe more widespread use of cuffed tubesrenders the data more reliable in the
management of children with congenitalheart disease.
Information that can be derived fromcapnography and PETCO2 measurementsincludes: 1) changes in alveolar ventila-tion; 2) confirmation of endotrachealtube placement; 3) degree of right to leftintracardiac shunt; 4) change in pulmo-nary blood flow; and 5) effectiveness ofcardiopulmonary resuscitation.
End-Tidal CO2 Monitoring in Surgeryand Anesthesia. Noninvasive CO2 mea-surement as a monitor of effective alveo-lar ventilation has become standard prac-tice in operating rooms, and PETCO2 as aroutine monitoring device has been acornerstone of safe anesthesia practicefor �30 yrs (79). In pediatric practice ithas been used by anesthesiologists duringsurgery for congenital heart disease andcardiac catheterization for �20 yrs (80–85). A study by Burrows (80) examinedthe PaCO2–PETCO2, physiological deadspace, and venous admixture in 41 in-
Figure 5. Normal capnogram showing the initialupstroke (increasing amount of alveolar gas) andthe expiratory plateau. In situations in whichthere is significant lung parenchymal lung dis-ease, a plateau in the capnogram may not bereached. Reproduced with permission from HessDR, Kacmarek RM: Essentials of Mechanical Ven-tilation. New York, McGraw-Hill, 1996.
Figure 6. The relationship between alveolar CO2
(PACO2) and pressure of end-tidal CO2 (PETCO2)in different states of ventilation/perfusion (V/Q)matching. Reproduced with permission fromHess DR, Kacmarek RM: Essentials of MechanicalVentilation. New York, McGraw-Hill, 1996.
S7Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

fants and children undergoing heart sur-gery. Patients were divided into acyanoticwith normal or increased pulmonaryblood flow and cyanotic with either rightto left intracardiac shunts or completemixing lesions. He found that in the acya-notic lesions the PaCO2–PETCO2 differencewas minimal but that the PETCO2 under-estimates the PaCO2 in children with cy-anotic congenital heart disease attribut-able largely to venous admixture, afinding confirmed by another study (83).Both the study by Fletcher (81) and thestudy by Wilson et al (86) have confirmedthe increase in PaCO2–PETCO2 in childrenwith cyanotic coronary heart disease andright to left intracardiac shunts and the-orized that there would be a relationshipbetween this increase and reduced satu-ration levels (87), a finding confirmed byothers (72). Both the study by Yates et al(88) and the study by Tugrul et al (89) inwhich PETCO2 was monitored during theinsertion of systemic to pulmonary arteryshunts showed that the effectiveness ofthe procedure could be demonstrated bya rise in SaO2 coincident with a reductionin PaCO2–PETCO2. This observation canalso be applied in the ICU when there isconcern about possible shunt occlusionas a widening of the PaCO2–PETCO2 gradi-ent may be observed even before there isa change in hemodynamics or a fall insaturation (85). PETCO2 can change dra-matically when pulmonary blood flow iscompromised as reported in a 7-month-old patient with tetralogy of Fallot and apulmonary valve replacement in whichobstruction of the main pulmonary arteryby a transesophageal probe resulted inthe PETCO2 reading falling rapidly to zero(90). A study by Smolinsky et al (91), inwhich capnography was used during pul-monary artery banding procedures in pa-tients with excessive pulmonary bloodflow, demonstrated an average reductionof 3.8 mm Hg in the PETCO2 at the end ofthe procedure. However, any inferencesabout pulmonary blood flow drawn fromthe use of PETCO2 should take into ac-count the state of the lung parenchyma.Despite previous studies about PaCO2–PETCO2 values being increased in cyanoticcoronary heart disease, a study by Shortet al (92) found that in children under-going cardiac surgery, there was a higherthan predicted PaCO2–PETCO2 gradient inthose patients with heart failure withhigh pulmonary blood flow and pulmo-nary congestion probably due to in-creased ventilation–perfusion mismatch.
Capnography and PETCO2 Monitoringin Critical Care. Although end-tidal CO2
monitoring is part of routine care inadult ICUs, its adoption has been slowerin pediatrics because of concerns aboutits accuracy when uncuffed tubes areused. A study by McDonald et al (93)evaluated the comparison between PaCO2
and PETCO2 in 129 ventilated children in apediatric ICU, 30% of whom had cardiacdisease. They found that the PaCO2–PETCO2 difference was within 5 mm Hg in54% of paired samples but that the dif-ference increased with increasing severityof oxygenation failure as manifested by areduction in the PaO2/FIO2 ratio. Despitethis, there are many reasons to supportits use as a routine monitor in ventilatedpediatric postoperative cardiac patients;the most compelling is that the cardiacICU is an extension of the care providedin the operating room. The importance ofthis is illustrated in the study of patientsundergoing sternal closure in the ICU(94) in which expired tidal volume andCO2 elimination 30 mins before and aftersternal closure in 17 patients decreasedby 17% and 29%, respectively. This re-flects a decrease in effective alveolar ven-tilation resulting from a reduction in re-spiratory system compliance. The samestrictures apply to use of end-tidal CO2
monitoring during the performance oftransesophageal echocardiography in in-fants who are being ventilated becausethe probe can obstruct either the endo-tracheal tube or vascular structureswithin the mediastinum (95, 96). In bothsituations, this can be detected by a fall inPETCO2.
Capnography During Pediatric Emer-gencies. End-tidal CO2 monitoring has anumber of applications in emergency sit-uations in children, including confirma-tion of endotracheal tube placement (97).The American Society of Anesthesiolo-gists guidelines for the management ofthe difficult airway recommend that con-firmation of correct placement of thetube into the trachea is verified by eitherstandard infrared capnometry or the useof a disposable colorimetric CO2 detector(2). A study by Roberts et al (98) on ne-onates undergoing urgent or emergentintubation used a capnograph with side-stream sampling to detect CO2 and wasable to identify correctly 39 of 40 esoph-ageal intubations by capnography. The dis-posable colorimetric CO2 connector is nowmore commonly used in emergency situa-tions. This is a portable device that is con-nected to the endotracheal tube and
changes color from purple (0.03 to �0.5%,area A) to tan (0.5 to �2.0%, area B) oryellow (2.0 to 5%, area C) in the presence ofCO2. It has been shown to accurately iden-tify correct tube placement in infants andsmall children (99). If no color change fromthe purple zone is noted during emergencyairway placement and the tube is con-firmed to be in the trachea by other means,then the likely explanation is that no CO2 isbeing produced during loss of cardiac out-put. Capnography and end-tidal CO2 con-centration have been used to identify boththe effectiveness of cardiopulmonary resus-citation and as a prognostic indicator forthe return of a perfusing cardiac rhythm(100–103). In studies of cardiac arrest inadults, a PETCO2 level of 15 mm Hg has beenassociated with effective cardiopulmonaryresuscitation and restoration of cardiacoutput (100, 101). In the study of pediatricemergency intubations and resuscitationsby Bhende and Thompson (104) in whichthe colorimetric CO2 detector method wasused during cardiopulmonary resuscita-tion, only patients with a reading in the Crange had return of spontaneous circula-tion and survived to ICU admission. Thisuse of capnography and colormetric CO2
detection form part of the American HeartAssociation guidelines for cardiopulmonaryresuscitation in children (105).
Finally, capnography is an importantpart of the monitoring of ventilation dur-ing pediatric transport both within thehospital and in the prehospital setting(78, 102, 106, 107). Studies have shownthat in situations in which tight controlof PaCO2 is required, this is more readilyachieved by monitoring end-tidal CO2
(78, 108).Evidence and Recommendations for
the Use of Capnography and End-TidalCO2 Monitoring. End-tidal CO2 monitor-ing is routinely used during anesthesiafor cardiac surgery and cardiac catheter-ization as a measure of effective ventila-tion and is recommended because it addssignificantly to patient safety. There isalso a significant amount of evidence thatsupports its routine use in ventilated pa-tients in ICU or during transport. Capnog-raphy is also recommended to verify thecorrect placement of endotracheal tubesand the effectiveness of cardiopulmonaryresuscitation. Like many monitoring de-vices, the evidence to support these recom-mendations is based on case series and ob-servational studies (level of evidence: IV;grade of recommendation: C).
S8 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

REFERENCES
1. Weil MH, Shubin H: Shock following acutemyocardial infarction. Current understand-ing of hemodynamic mechanisms. ProgCardiovasc Dis 1968; 11:1–17
2. American Society of Anesthesiologists TaskForce on Management of the Difficult Air-way Management: Practice guidelines formanagement of the difficult airway: An up-dated report by the American Society ofAnesthesiologists Task Force on Manage-ment of the Difficult Airway. Anesthesiol-ogy 2003; 98:1269–1277
3. Ibsen B: The anaesthetist’s viewpoint on thetreatment of respiratory complications inpoliomyelitis during the epidemic in Co-penhagen, 1952. Proc R Soc Med 1954; 47:72–74
4. Ibsen B: My life as a physician. [Danish]Dan Medicinhist Arbog 1993:33–45
5. Safar P, Escarraga LA, Elam JO: A compar-ison of the mouth-to-mouth and mouth-to-airway methods of artificial respiration withthe chest-pressure arm-lift methods.N Engl J Med 1958; 258:671–677
6. Ristagno G, Weil MH: The history of criticalcare medicine: The past, the present and thefuture. In: Intensive and Critical Care Med-icine. Gullo A, Besso J, Lumb PD, et al(Eds). Milan, Italy, Springer-Verlag, 2009,pp 3–17
7. Weil MH, Shubin H, Rosoff L: Fluid reple-tion in circulatory shock: Central venouspressure and other practical guides. JAMA1965; 192:668–674
8. Gipsen JGW: ‘Measuring’ the patient in an-cient Egyptian medical texts. Janus 1967;54:224–227
9. Weil MH, Martin R, Carrington JH, et al:Advances in the design and implementationof automated techniques for hemodynamicmeasurements on patients. Electroen-cephalogr Clin Neurophysiol 1969; 27:653–654
10. Weil MH, Shubin H: The ‘VIP’ approach tothe bedside management of shock. JAMA1969; 207:337–340
11. Fanconi S, Doherty P, Edmonds JF, et al:Pulse oximetry in pediatric intensive care:Comparison with measured saturations andtranscutaneous oxygen tension. J Pediatr1985; 107:362–366
12. Valsangiacomo E, Schmid ER, SchupbachRW, et al: Early postoperative arrhythmiasafter cardiac operation in children. AnnThorac Surg 2002; 74:792–796
13. Drew BJ, Califf RM, Funk M, et al: Practicestandards for electrocardiographic moni-toring in hospital settings: An AmericanHeart Association scientific statementfrom the Councils on CardiovascularNursing, Clinical Cardiology, and Cardio-vascular Disease in the Young: endorsedby the International Society of Computer-ized Electrocardiology and the AmericanAssociation of Critical-Care Nurses. Circu-lation 2004; 110:2721–2746
14. Hales S: Statistical essays: Containing Hae-mostaticks. London, UK, Innyes and Manby,1733
15. Booth J: A short history of blood pressuremeasurement. Proc R Soc Med 1977; 70:793–799
16. Lewis WH: The evolution of clinical sphyg-momanometry. Bull N Y Acad Med 1941;17:871
17. Hill L, Barnard H: A simple and accurateform of sphygmometer or arterial pressuregauge contrived for clinical use. BMJ 1897;2:904
18. Park MK, Menard SM: Accuracy of bloodpressure measurement by the Dinamapmonitor in infants and children. Pediatrics1987; 79:907–914
19. Park MK, Menard SM: Normative oscillo-metric blood pressure values in the first 5years in an office setting. Am J Dis Child1989; 143:860–864
20. Park MK, Menard SW, Schoolfield J: Oscil-lometric blood pressure standards for chil-dren. Pediatr Cardiol 2005; 26:601–607
21. Park MK, Menard SW, Yuan C: Comparisonof blood pressure in children from threeethnic groups. Am J Cardiol 2001; 87:1305–1308
22. Park MK, Menard SW, Yuan C: Comparisonof auscultatory and oscillometric bloodpressures. Arch Pediatr Adolesc Med 2001;155:50–53
23. Friesen RH, Lichtor JL: Indirect measure-ment of blood pressure in neonates andinfants utilizing an automatic noninvasiveoscillometric monitor. Anesth Analg 1981;60:742–745
24. Brierley J, Carcillo JA, Choong K, et al:Clinical practice parameters for hemody-namic support of pediatric and neonatalseptic shock: 2007 update from the Ameri-can College of Critical Care Medicine. CritCare Med 2009; 37:666–688
25. Lin SM, Huang CD, Lin HC, et al: A modi-fied goal-directed protocol improves clinicaloutcomes in intensive care unit patientswith septic shock: A randomized controlledtrial. Shock 2006; 26:551–557
26. Rivers E, Nguyen B, Havstad S, et al: Earlygoal-directed therapy in the treatment ofsevere sepsis and septic shock. N Engl J Med2001; 345:1368–1377
27. Kilgannon JH, Jones AE, Shapiro NI, et al:Association between arterial hyperoxia fol-lowing resuscitation from cardiac arrestand in-hospital mortality. JAMA 2010; 303:2165–2171
28. Kilgannon JH, Roberts BW, Reihl LR, et al:Early arterial hypotension is common inthe post-cardiac arrest syndrome and asso-ciated with increased in-hospital mortality.Resuscitation 2008; 79:410–416
29. Trzeciak S, Jones AE, Kilgannon JH, et al:Outcome measures utilized in clinical trialsof interventions for post-cardiac arrest syn-drome: A systematic review. Resuscitation2009; 80:617–623
30. Trzeciak S, Jones AE, Kilgannon JH, et al:
Significance of arterial hypotension afterresuscitation from cardiac arrest. Crit CareMed 2009; 37:2895–2903; quiz 2904
31. Bur A, Herkner H, Vlcek M, et al: Factorsinfluencing the accuracy of oscillometricblood pressure measurement in critically illpatients. Crit Care Med 2003; 31:793–799
32. Bur A, Hirschl MM, Herkner H, et al: Accu-racy of oscillometric blood pressure mea-surement according to the relation betweencuff size and upper-arm circumference incritically ill patients. Crit Care Med 2000;28:371–376
33. Lakhal K, Ehrmann S, Runge I, et al: Track-ing hypotension and dynamic changes inarterial blood pressure with brachial cuffmeasurements. Anesth Analg 2009; 109:494–501
34. Cohn JN, Luria MH: Studies in clinicalshock and hypotension; the value of bedsidehemodynamic observations. JAMA 1964;190:891–896
35. Gevers M, van Genderingen HR, LafeberHN, et al: Accuracy of oscillometric bloodpressure measurement in critically ill neo-nates with reference to the arterial pressurewave shape. Intensive Care Med 1996; 22:242–248
36. Pytte M, Dybwik K, Sexton J, et al: Oscillo-metric brachial mean artery pressures arehigher than intra-radial mean artery pres-sures in intensive care unit patients receiv-ing norepinephrine. Acta AnaesthesiolScand 2006; 50:718–721
37. Roberts LN, Smiley JR, Manning GW: Acomparison of direct and indirect blood-pressure determinations. Circulation 1953;8:232–242
38. Van Bergen FH, Weatherhead DS, TreloarAE, et al: Comparison of indirect and directmethods of measuring arterial blood pres-sure. Circulation 1954; 10:481–490
39. Dellinger RP, Levy MM, Carlet JM, et al:Surviving Sepsis Campaign: Internationalguidelines for management of severe sepsisand septic shock: 2008. Crit Care Med 2008;36:296–327
40. Chatterjee A, DePriest K, Blair R, et al:Preliminary results of a survey of bloodpressure monitoring by intensivists in crit-ically ill patients. Crit Care Med 2010; 38:2335–2338
41. Rice WP, Fernandez EG, Jaroq D, et al: Acomparison of hydrostatic leveling methodsin invasive pressure monitoring. Crit CareNurs 2000; 20:20, 22–30
42. Mortensen JD: Clinical sequelae from arte-rial needle puncture, cannulation, and inci-sion. Circulation 1967; 35:1118–1123
43. Barnes RW, Foster EJ, Janssen GA, et al:Safety of brachial arterial catheters as mon-itors in the intensive care unit—Prospec-tive evaluation with the Doppler ultrasonicvelocity detector. Anesthesiology 1976; 44:260–264
44. Barnes RW, Petersen JL, Krugmire RB Jr, etal: Complications of brachial artery cathe-terization: prospective evaluation with the
S9Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
Doppler ultrasonic velocity detector. Chest1974; 66:363–367
45. Chait HI, Kuhn MA, Baum VC: Inferior venacaval pressure reliably predicts right atrialpressure in pediatric cardiac surgical pa-tients. Crit Care Med 1994; 22:219–224
46. Fernandez EG, Green TP, Sweeney M: Lowinferior vena caval catheters for hemody-namic and pulmonary function monitoringin pediatric critical care patients. PediatrCrit Care Med 2004; 5:14–18
47. Davison DL, Chawla LS, Selassie L, et al:Femoral-based central venous oxygen satu-ration is not a reliable substitute for sub-clavian/internal jugular-based central ve-nous oxygen saturation in patients who arecritically ill. Chest 2010; 138:76–83
48. Sharkey SW: Beyond the wedge: Clinicalphysiology and the Swan-Ganz catheter.Am J Med 1987; 83:111–122
49. Askegard-Giesmann JR, Caniano DA, Ken-ney BD: Rare but serious complications ofcentral line insertion. Semin Pediatr Surg2009; 18:73–83
50. Smith-Wright DL, Green TP, Lock JE, et al:Complications of vascular catheterizationin critically ill children. Crit Care Med1984; 12:1015–1017
51. Couture P, Denault AY, McKenty S, et al:Impact of routine use of intraoperativetransesophageal echocardiography duringcardiac surgery. Can J Anaesth 2000; 47:20–26
52. Siwik ES, Spector ML, Patel CR, et al: Costsand cost-effectiveness of routine trans-esophageal echocardiography in congenitalheart surgery. Am Heart J 1999; 138:771–776
53. Ralston AC, Webb RK, Runciman WB: Po-tential errors in pulse oximetry. III: Effectsof interferences, dyes, dyshaemoglobins andother pigments. Anaesthesia 1991; 46:291–295
54. Ralston AC, Webb RK, Runciman WB: Po-tential errors in pulse oximetry. I. Pulseoximeter evaluation. Anaesthesia 1991; 46:202–206
55. Webb RK, Ralston AC, Runciman WB: Po-tential errors in pulse oximetry. II. Effectsof changes in saturation and signal quality.Anaesthesia 1991; 46:207–212
56. Clayton DG, Webb RK, Ralston AC, et al: Acomparison of the performance of 20 pulseoximeters under conditions of poor perfu-sion. Anaesthesia 1991; 46:3–10
57. Clayton DG, Webb RK, Ralston AC, et al:Pulse oximeter probes. A comparison be-tween finger, nose, ear and forehead probesunder conditions of poor perfusion. Anaes-thesia 1991; 46:260–265
58. Villanueva R, Bell C, Kain ZN, et al: Effect ofperipheral perfusion on accuracy of pulseoximetry in children. J Clin Anesth 1999;11:317–322
59. Salyer JW: Neonatal and pediatric pulse oxi-metry. Respir Care 2003; 48:386–396; dis-cussion 397–398
60. Boxer RA, Gottesfeld I, Singh S, et al: Non-
invasive pulse oximetry in children withcyanotic congenital heart disease. Crit CareMed 1987; 15:1062–1064
61. Carter BG, Carlin JB, Tibballs J, et al: Ac-curacy of two pulse oximeters at low arterialhemoglobin–oxygen saturation. Crit CareMed 1998; 26:1128–1133
62. Fanconi S: Reliability of pulse oximetry inhypoxic infants. J Pediatr 1988; 112:424–427
63. Gerstmann D, Berg R, Haskell R, et al: Op-erational evaluation of pulse oximetry inNICU patients with arterial access. J Peri-natol 2003; 23:378–383
64. Lebecque P, Shango P, Stijns M, et al: Pulseoximetry versus measured arterial oxygensaturation: A comparison of the NellcorN100 and the Biox III. Pediatr Pulmonol1991; 10:132–135
65. Lynn AM, Bosenberg A: Pulse oximetry dur-ing cardiac catheterization in children withcongenital heart disease. J Clin Monit 1986;2:230–233
66. Schmitt HJ, Schuetz WH, Proeschel PA, etal: Accuracy of pulse oximetry in childrenwith cyanotic congenital heart disease.J Cardiothorac Vasc Anesth 1993; 7:61–65
67. Torres A Jr, Skender KM, Wohrley JD, et al:Pulse oximetry in children with congenitalheart disease: Effects of cardiopulmonarybypass and cyanosis. J Intensive Care Med2004; 19:229–234
68. Iyer P, McDougall P, Loughnan P, et al:Accuracy of pulse oximetry in hypothermicneonates and infants undergoing cardiacsurgery. Crit Care Med 1996; 24:507–511
69. Sedaghat-Yazdi F, Torres A Jr, Fortuna R, etal: Pulse oximeter accuracy and precisionaffected by sensor location in cyanotic chil-dren. Pediatr Crit Care Med 2008;9:393–397
70. Cote CJ, Goldstein EA, Cote MA, et al: Asingle-blind study of pulse oximetry in chil-dren. Anesthesiology 1988; 68:184–188
71. Cannesson M, Henaine R, Di Filippo S, et al:Clinical usefulness of new-generation pulseoximetry in the paediatric cardiac surgerysetting [in French]. Ann Fr Anesth Reanim2008; 27:808–812
72. De Vries JW, Plotz FB, Van Vught AJ: Pulseoximeter-enhanced accuracy of capnometryin children with cyanotic heart disease. In-tensive Care Med 2002; 28:1336–1339
73. Macnab AJ, Baker-Brown G, Anderson EE:Oximetry in children recovering from deephypothermia for cardiac surgery. Crit CareMed 1990; 18:1066–1069
74. Miyasaka K: Pulse oximetry in the manage-ment of children in the PICU. Anesth Analg2002; 94(Suppl):S44–S46
75. Poets CF, Urschitz MS, Bohnhorst B: Pulseoximetry in the neonatal intensive care unit(NICU): Detection of hyperoxemia and falsealarm rates. Anesth Analg 2002; 94(Suppl):S41–S43
76. Tachibana C, Fukada T, Hasegawa R, et al:Accuracy of a pulse oximeter during hyp-oxia [in Japanese]. Masui 1996; 45:479–482
77. Thilo EH, Andersen D, Wasserstein ML, etal: Saturation by pulse oximetry: Compari-son of the results obtained by instrumentsof different brands. J Pediatr 1993; 122:620–626
78. Tobias JD, Lynch A, Garrett J: Alterations ofend-tidal carbon dioxide during the intra-hospital transport of children. PediatrEmerg Care 1996; 12:249–251
79. Eichhorn JH: Prevention of intraoperativeanesthesia accidents and related severe in-jury through safety monitoring. Anesthesi-ology 1989; 70:572–577
80. Burrows FA: Physiologic dead space, venousadmixture, and the arterial to end-tidal car-bon dioxide difference in infants and chil-dren undergoing cardiac surgery. Anesthe-siology 1989; 70:219–225
81. Fletcher R: Relationship between alveolardeadspace and arterial oxygenation in chil-dren with congenital cardiac disease. Br JAnaesth 1989; 62:168–176
82. Lindahl SG: Oxygen consumption and car-bon dioxide elimination in infants and chil-dren during anaesthesia and surgery. Br JAnaesth 1989; 62:70–76
83. Lazzell VA, Burrows FA: Stability of theintraoperative arterial to end-tidal carbondioxide partial pressure difference in chil-dren with congenital heart disease. Can JAnaesth 1991; 38:859–865
84. Lindahl SG, Yates AP, Hatch DJ: Relation-ship between invasive and noninvasive mea-surements of gas exchange in anesthetizedinfants and children. Anesthesiology 1987;66:168–175
85. Schuller JL, Bovill JG, Nijveld A: End-tidalcarbon dioxide concentration as an indica-tor of pulmonary blood flow during closedheart surgery in children. A report of twocases. Br J Anaesth 1985; 57:1257–1259
86. Wilson J, Russo P, Russo J, et al: Noninva-sive monitoring of carbon dioxide in infantsand children with congenital heart disease:End-tidal versus transcutaneous tech-niques. J Intensive Care Med 2005; 20:291–295
87. Fletcher R: The relationship between thearterial to end-tidal PCO2 difference andhemoglobin saturation in patients withcongenital heart disease. Anesthesiology1991; 75:210–216
88. Yates AP: Pulmonary blood flow duringclosed heart surgery. Use of a modifiedQp/Qs ratio to assess adequacy of palliationof systemic-pulmonary artery shunts. Br JAnaesth 1988; 60:768–772
89. Tugrul M, Camci E, Sungur Z, et al: Thevalue of end-tidal carbon dioxide monitor-ing during systemic-to-pulmonary arteryshunt insertion in cyanotic children. J Car-diothorac Vasc Anesth 2004; 18:152–155
90. Preisman S, Yusim Y, Mishali D, et al: Com-pression of the pulmonary artery duringtransesophageal echocardiography in a pe-diatric cardiac patient. Anesth Analg 2003;96:85–87
91. Smolinsky AK, Shinfield A, Paret G, et al:
S10 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

End-tidal CO2 levels are a reliable indicatorof band tightness in pulmonary artery band-ing. Ann Thorac Surg 1995; 60(Suppl):S523–S524
92. Short JA, Paris ST, Booker PD, et al: Arterialto end-tidal carbon dioxide tension differ-ence in children with congenital heart dis-ease. Br J Anaesth 2001; 86:349–353
93. McDonald MJ, Montgomery VL, Cerrito PB,et al: Comparison of end-tidal CO2 andPaco2 in children receiving mechanicalventilation. Pediatr Crit Care Med 2002;3:244–249
94. Main E, Elliott MJ, Schindler M, et al:Effect of delayed sternal closure after car-diac surgery on respiratory function inventilated infants. Crit Care Med 2001;29:1798 –1802
95. Frommelt PC, Stuth EA: Transesophagealechocardiographic in total anomalouspulmonary venous drainage: Hypotensioncaused by compression of the pulmonaryvenous confluence during probe passage.J Am Soc Echocardiogr 1994; 7:652– 654
96. Lunn RJ, Oliver WC Jr, Hagler DJ, et al:Aortic compression by transesophagealechocardiographic probe in infants and
children undergoing cardiac surgery. Anes-thesiology 1992; 77:587–590
97. Sullivan KJ, Kissoon N, Goodwin SR: End-tidal carbon dioxide monitoring in pediatricemergencies. Pediatr Emerg Care 2005; 21:327–332; quiz 333–335
98. Roberts WA, Maniscalco WM, Cohen AR, etal: The use of capnography for recognitionof esophageal intubation in the neonatalintensive care unit. Pediatr Pulmonol 1995;19:262–268
99. Bhende MS, Thompson AE, Cook DR, et al:Validity of a disposable end-tidal CO2 detec-tor in verifying endotracheal tube place-ment in infants and children. Ann EmergMed 1992; 21:142–145
100. Sanders AB, Kern KB, Otto CW, et al: End-tidal carbon dioxide monitoring during car-diopulmonary resuscitation. A prognosticindicator for survival. JAMA 1989; 262:1347–1351
101. Callaham M, Barton C: Prediction of out-come of cardiopulmonary resuscitationfrom end-tidal carbon dioxide concentra-tion. Crit Care Med 1990; 18:358–362
102. Bhende MS, Karr VA, Wiltsie DC, et al:Evaluation of a portable infrared end-tidalcarbon dioxide monitor during pediatric in-
terhospital transport. Pediatrics 1995; 95:875–878
103. Falk JL, Rackow EC, Weil MH: End-tidalcarbon dioxide concentration during car-diopulmonary resuscitation. N Engl J Med1988; 318:607–611
104. Bhende MS, Thompson AE: Evaluation ofan end-tidal CO2 detector during pediatriccardiopulmonary resuscitation. Pediatrics1995; 95:395–399
105. Kleinman ME, Chameides L, SchexnayderSM, et al: Pediatric advanced life support:2010 American Heart Association guide-lines for cardiopulmonary resuscitation andemergency cardiovascular care. Circulation2010; 122(Suppl 3):S876–S908
106. Bhende MS: End-tidal carbon dioxide mon-itoring in pediatrics—Clinical applications.J Postgrad Med 2001; 47:215–218
107. Bhende MS, Thompson AE, Orr RA: Utilityof an end-tidal carbon dioxide detector dur-ing stabilization and transport of criticallyill children. Pediatrics 1992; 89:1042–1044
108. Palmon SC, Liu M, Moore LE, et al: Cap-nography facilitates tight control of venti-lation during transport. Crit Care Med1996; 24:608–611
S11Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Pulmonary artery catheters
Ronald M. Perkin, MD, MA; Nick Anas, MD
I n 1970, the introduction of thepulmonary artery (PA) catheterrevolutionized the care of criti-cally ill patients by allowing the
clinician to directly measure importantcardiovascular variables at the bedside (1,2). As a result, the use of the PA catheterbecame a central part of the managementof critically ill patients in adult and pedi-atric intensive care units (3–7).
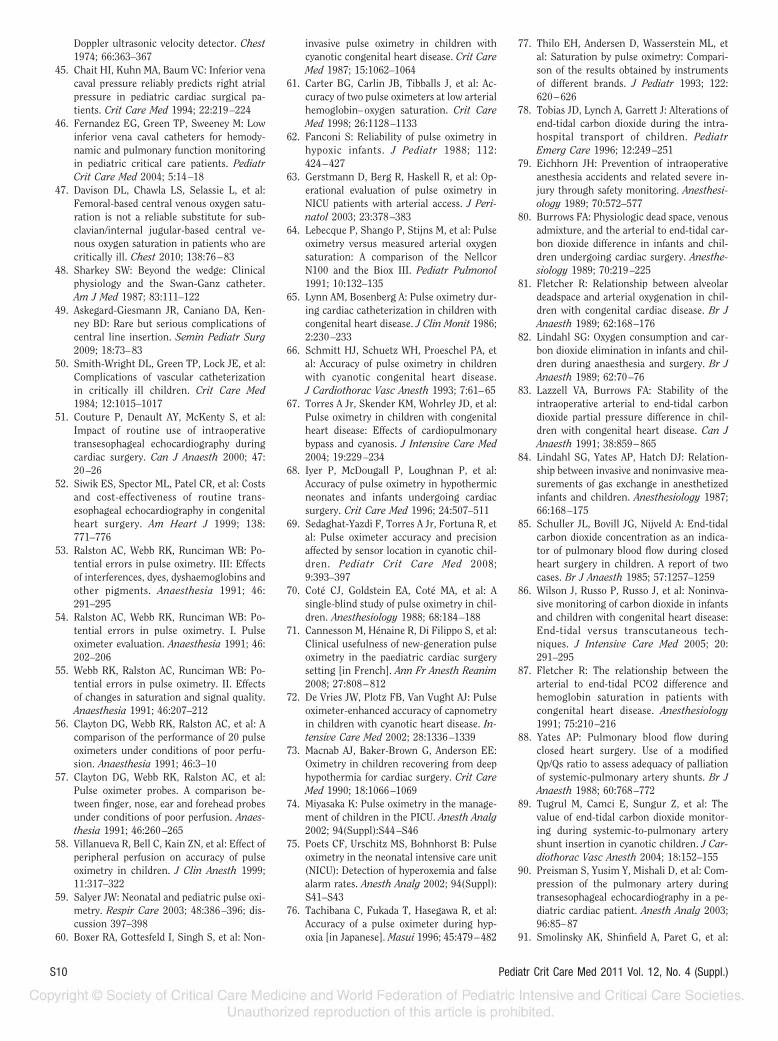
The standard PA catheter has four lu-mens, which allow assessment of the pa-tients’ hemodynamic condition throughdirect intracardiac and PA pressure mon-itoring (Tables 1 and 2; Fig. 1). The di-rectly measured physiological data avail-able from the PA catheter include thepressures in the right atrium, right ven-tricle, PA, and PA occlusion pressure;mixed venous oxygenation; and tempera-ture (Figs. 2 and 3). From these variablesand three other measured variables,namely systemic arterial pressure, heart
rate, and cardiac output, a large array ofcalculated information is available, in-cluding stroke volume, systemic vascularresistance, pulmonary vascular resis-tance, oxygen transport, oxygen con-sumption, and oxygen extraction ratio(Table 3).
There are several technologies avail-able for the measurement of cardiac out-put. The thermodilution technique fordetermining cardiac output is appliedwidely and represents a major use of thePA catheter. The procedure can be per-formed rapidly, and clinical studies haveshown good correlation between ther-modilution cardiac outputs and theFick or dye dilution method. This tech-nique takes advantage of the fact thatcold water can be injected into the cen-tral circulation and that venous return(cardiac output) may be estimated byexamining the dilution of cold waterwith warm blood (8).
There are several principles of ther-modilution measurement of cardiac out-put. A known quantity of cold injectate isintroduced into the circulation at onepoint (right atrium), becomes adequatelymixed (two heart chambers), and the re-sultant change in intravascular tempera-ture is measured downstream. Recordingof the resulting cooling curve at thedownstream site allows calculation of netblood flow. Cardiac output is inverselyproportional to the fall in temperature. Inpractice, a known quantity of cooled glu-
cose or saline is injected into the proxi-mal part of the PA catheter. The therm-istor, located distantly, allows recordingof baseline PA temperature and the sub-sequent cooling curve. This tempera-ture–time curve is similar to the one pro-duced by the indicator–dilution method.The temperature change integrated overtime (Stuart-Hamilton equation) yieldsthe cardiac output (8).
A normal curve characteristicallyshows a sharp upstroke from rapid injec-tion of the injectate. This is followed by asmooth curve and slightly prolongeddownslope back to the baseline. Becausethis curve is representing a change fromwarmer temperature to cooler and thenback to warmer temperature, the actualcurve is in a negative direction. For con-tinuity of most graphs, the curve is pro-duced in an upright fashion. The areaunder the curve is inversely proportionalto the cardiac output.
When cardiac output is low, moretime is required for the temperature toreturn to baseline, producing a largerarea under the curve. With high cardiacoutput, the cooler injectate is carriedfaster through the heart, and the temper-ature returns to baseline faster. This pro-duces a smaller area under the curve(Fig. 4).
A modified Stewart-Hamilton equa-tion is used to calculate the cardiac out-put taking into consideration the changein temperature as the indicator; modifi-
From the Department of Pediatrics (RMP), BrodySchool of Medicine at East Carolina University,Greenville, NC; and Pediatric Critical Care (NA),Children’s Hospital of Orange County, Department ofPediatrics, David Geffen School of Medicine atUCLA, Los Angeles, CA.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e318220f079
Background: After its introduction in 1970, the use of the pul-monary artery catheter became a central part of the management ofcritically ill patients in adult and pediatric intensive care units.However, because it was introduced as a class II device, efficacy forits safety and clinical benefit did not exist during the early years ofuse. This review describes the pulmonary artery catheter and re-views the literature supporting its use.
Methodology: A search of MEDLINE, PubMed, and the CochraneDatabase was made to find literature about pulmonary arterycatheter use. Literature for both adult and pediatric patients wasreviewed. Guidelines published by the Society for Critical CareMedicine and the American Heart Association were reviewed,including further review of references cited.
Results and Conclusions: The evidence supporting the use ofthe pulmonary artery catheter is mostly limited to level IV (non-randomized, historical controls, and expert opinion) and level V(case series, uncontrolled studies, and expert opinion). A higherlevel of evidence supports the use of the pulmonary arterycatheter in selected pediatric patients, especially those withpulmonary arterial hypertension and shock refractory to stan-dard fluid resuscitation and vasoactive agents. There are nodata to suggest that use of the pulmonary artery catheterincreases mortality in children. (Pediatr Crit Care Med 2011;12[Suppl.]:S12–S20)
KEY WORDS: pulmonary artery; catheter; pediatric; acute lunginjury; shock; pulmonary hypertension
S12 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

cations include the measured tempera-ture of the injectate and the patient’sblood temperature along with the specificgravity of the solution injected.
CO �
V � (TB � SI)
A�
(SI � CI)
(SB � CB)�
60 � CT � K
1
Where CO � cardiac output; V � volumeof injectate (mL); A � area of thermodi-
lution curve in square millimeters di-vided by paper speed (mm/sec); K � cal-ibration constant in mm/°C; TB, TI �temperature of blood (B) and injectate(I); SB, SI � specific gravity of blood andinjectate; CB, CI � specific heat of blood
and injectate;(SI � CI)
(SB � CB)� 1.08 when 5%
dextrose is used; 60 � 60 sec/min; andCT � correction factor for injectatewarming.
The thermistor port of the catheter isattached to a computer or monitor. Cal-culations are performed internally withthe results displayed on the screen. Somecomputers and monitors can also displaythe actual cardiac output time–tempera-ture curve. By observing the actual ther-modilution curve, assessment of injec-tion technique and artifactual influencescan be noted (Fig. 4).
It is important to enter the computa-tion constant into the computer or mon-itor. The correct computation will be de-pendent on the injectate temperature,injectate volume, catheter model, and in-jectate system (9).
The temperature of the injectate canbe iced or room temperature. Available
data suggest that there will be less vari-ability in cardiac output determinations ificed solution is used. The computer isregistering a change (signal) in tempera-ture from the patient’s baseline (noise).In some conditions, a variation in tem-perature of 0.05°C may occur with respi-rations. This decreases the “signal-to-noise” ratio and may produce anabnormally low cardiac output value (10).
Conditions in which the thermodilu-tion method may produce unreliable re-sults are those that have a backward flowof blood on the right side, tricuspid orpulmonic valve regurgitation, and ven-tricular or atrial septal defects (8–12).
The advantages of this technique overthe other methods previously mentionedare the reliability and ease of performingat the bedside. Also, serial cardiac outputsare performed without requiring bloodsampling.
Accuracy of the thermodilution tech-nique involves very rapid injection rates,accurate measurement of the injectanttemperature and volume, thorough mix-ing of the injectant and venous return,and no loss of injectant. Falsely elevatedcardiac output will occur with slow injec-tion rates and small injectant volumes.Falsely depressed cardiac output valuesoccur with the use of solutions coolerthan or injectant volumes greater thanvalues initially programmed on the car-diac output computer. The principle onwhich the thermodilution technique isbased assumes a constant blood flow dur-ing the time the indicator solution travelsfrom the right atrium to the thermistor.Also, the normal pulsatile nature of bloodflow and respiratory variations in in-trathoracic pressures may affect all ther-modilution determinations (8–12). To re-duce the impact of this latter problem,most investigators recommend averagingthree consecutive measurements per-formed in the same phase of the respira-tory cycle.
Cardiac output measurements in chil-dren are further complicated for the fol-lowing reasons: 1) Multiple measure-ments of cardiac output may result influid overload in a small child. The in-jected volume can be as little as 3 mL;however, the tradeoff is a greater likeli-hood of an erroneous measurement;2) The position of the proximal port ofthe PA catheter affects the accuracy ofboth thermodilution cardiac output de-terminations and RA pressure measure-ments (13). In small children, the proxi-mal port may be in the right ventricle.Figure 1. Standard four-lumen pulmonary artery catheter.
Table 1. PA catheter port locations and port functions
Location Function
Distal Monitors PA pressureMonitors wedge pressureAllows sampling of blood for mixed venous oxygen saturation
determinationProximal Monitors RA pressure
Used for cardiac output injectate fluidBalloon gate value Syringe used to inflate balloon for placement and obtain
wedge pressure valueThermistor connector Measures blood temperature 4 cm from distal tip (7F) or 2.5 cm
from distal tip (5F)
PA, pulmonary artery; RA, right atrium.
Table 2. Standard pulmonary artery cathetercomparisons
5F 7F
Length 75 cm 110 cmProximal injectate port
(distance from tip)15 cm 30 cm
Recommendedintroducer
6 or 6.5 8.5 or 9
(French size)Balloon volume 0.8 cc 1.5 ccThermodilution
injectatevolume
3, 5, 10 cc 5, 10 cc
S13Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
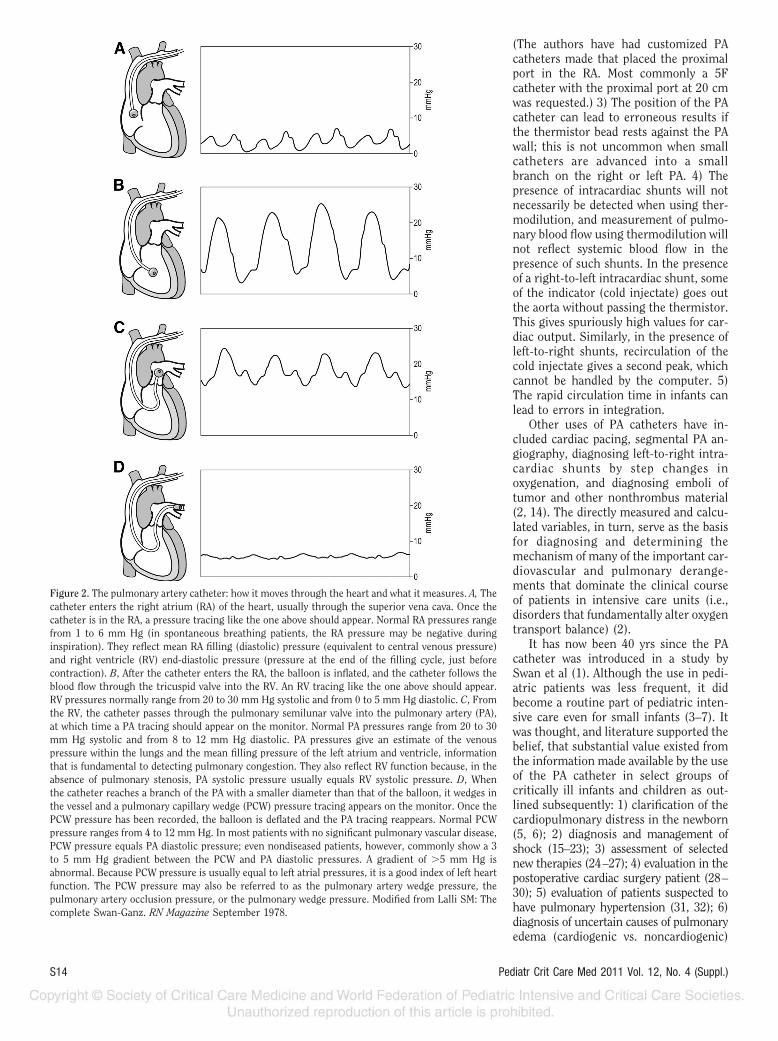
(The authors have had customized PAcatheters made that placed the proximalport in the RA. Most commonly a 5Fcatheter with the proximal port at 20 cmwas requested.) 3) The position of the PAcatheter can lead to erroneous results ifthe thermistor bead rests against the PAwall; this is not uncommon when smallcatheters are advanced into a smallbranch on the right or left PA. 4) Thepresence of intracardiac shunts will notnecessarily be detected when using ther-modilution, and measurement of pulmo-nary blood flow using thermodilution willnot reflect systemic blood flow in thepresence of such shunts. In the presenceof a right-to-left intracardiac shunt, someof the indicator (cold injectate) goes outthe aorta without passing the thermistor.This gives spuriously high values for car-diac output. Similarly, in the presence ofleft-to-right shunts, recirculation of thecold injectate gives a second peak, whichcannot be handled by the computer. 5)The rapid circulation time in infants canlead to errors in integration.
Other uses of PA catheters have in-cluded cardiac pacing, segmental PA an-giography, diagnosing left-to-right intra-cardiac shunts by step changes inoxygenation, and diagnosing emboli oftumor and other nonthrombus material(2, 14). The directly measured and calcu-lated variables, in turn, serve as the basisfor diagnosing and determining themechanism of many of the important car-diovascular and pulmonary derange-ments that dominate the clinical courseof patients in intensive care units (i.e.,disorders that fundamentally alter oxygentransport balance) (2).
It has now been 40 yrs since the PAcatheter was introduced in a study bySwan et al (1). Although the use in pedi-atric patients was less frequent, it didbecome a routine part of pediatric inten-sive care even for small infants (3–7). Itwas thought, and literature supported thebelief, that substantial value existed fromthe information made available by the useof the PA catheter in select groups ofcritically ill infants and children as out-lined subsequently: 1) clarification of thecardiopulmonary distress in the newborn(5, 6); 2) diagnosis and management ofshock (15–23); 3) assessment of selectednew therapies (24–27); 4) evaluation in thepostoperative cardiac surgery patient (28–30); 5) evaluation of patients suspected tohave pulmonary hypertension (31, 32); 6)diagnosis of uncertain causes of pulmonaryedema (cardiogenic vs. noncardiogenic)
Figure 2. The pulmonary artery catheter: how it moves through the heart and what it measures. A, Thecatheter enters the right atrium (RA) of the heart, usually through the superior vena cava. Once thecatheter is in the RA, a pressure tracing like the one above should appear. Normal RA pressures rangefrom 1 to 6 mm Hg (in spontaneous breathing patients, the RA pressure may be negative duringinspiration). They reflect mean RA filling (diastolic) pressure (equivalent to central venous pressure)and right ventricle (RV) end-diastolic pressure (pressure at the end of the filling cycle, just beforecontraction). B, After the catheter enters the RA, the balloon is inflated, and the catheter follows theblood flow through the tricuspid valve into the RV. An RV tracing like the one above should appear.RV pressures normally range from 20 to 30 mm Hg systolic and from 0 to 5 mm Hg diastolic. C, Fromthe RV, the catheter passes through the pulmonary semilunar valve into the pulmonary artery (PA),at which time a PA tracing should appear on the monitor. Normal PA pressures range from 20 to 30mm Hg systolic and from 8 to 12 mm Hg diastolic. PA pressures give an estimate of the venouspressure within the lungs and the mean filling pressure of the left atrium and ventricle, informationthat is fundamental to detecting pulmonary congestion. They also reflect RV function because, in theabsence of pulmonary stenosis, PA systolic pressure usually equals RV systolic pressure. D, Whenthe catheter reaches a branch of the PA with a smaller diameter than that of the balloon, it wedges inthe vessel and a pulmonary capillary wedge (PCW) pressure tracing appears on the monitor. Once thePCW pressure has been recorded, the balloon is deflated and the PA tracing reappears. Normal PCWpressure ranges from 4 to 12 mm Hg. In most patients with no significant pulmonary vascular disease,PCW pressure equals PA diastolic pressure; even nondiseased patients, however, commonly show a 3to 5 mm Hg gradient between the PCW and PA diastolic pressures. A gradient of �5 mm Hg isabnormal. Because PCW pressure is usually equal to left atrial pressures, it is a good index of left heartfunction. The PCW pressure may also be referred to as the pulmonary artery wedge pressure, thepulmonary artery occlusion pressure, or the pulmonary wedge pressure. Modified from Lalli SM: Thecomplete Swan-Ganz. RN Magazine September 1978.
S14 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
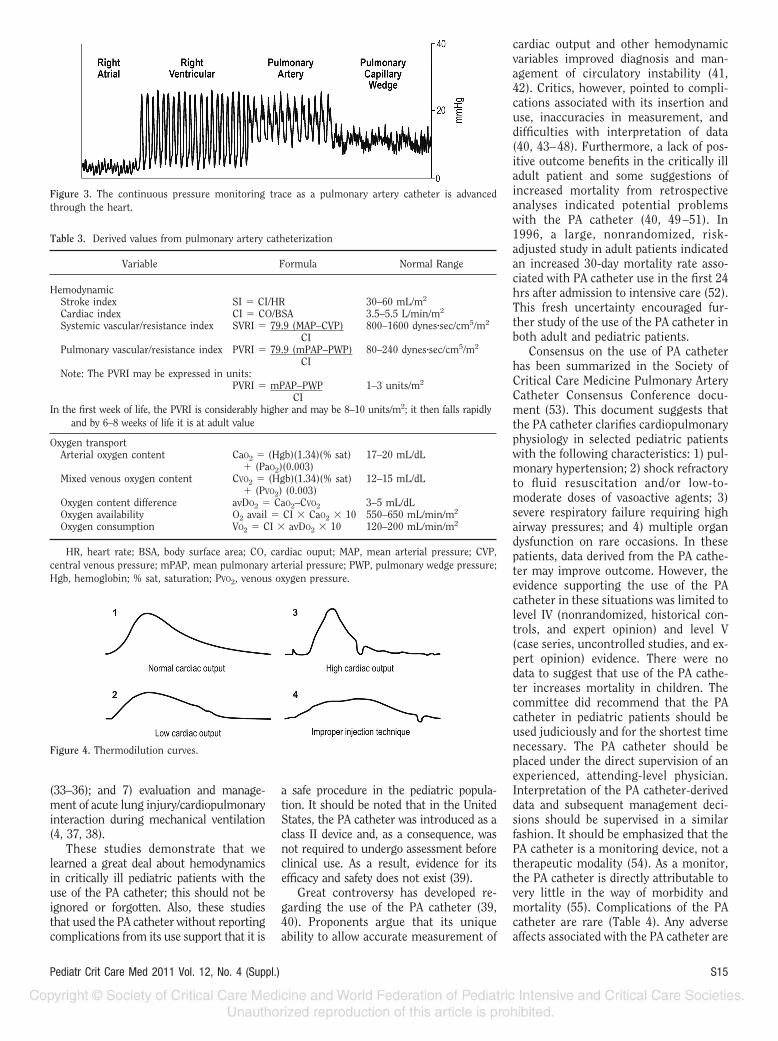
(33–36); and 7) evaluation and manage-ment of acute lung injury/cardiopulmonaryinteraction during mechanical ventilation(4, 37, 38).
These studies demonstrate that welearned a great deal about hemodynamicsin critically ill pediatric patients with theuse of the PA catheter; this should not beignored or forgotten. Also, these studiesthat used the PA catheter without reportingcomplications from its use support that it is
a safe procedure in the pediatric popula-tion. It should be noted that in the UnitedStates, the PA catheter was introduced as aclass II device and, as a consequence, wasnot required to undergo assessment beforeclinical use. As a result, evidence for itsefficacy and safety does not exist (39).
Great controversy has developed re-garding the use of the PA catheter (39,40). Proponents argue that its uniqueability to allow accurate measurement of
cardiac output and other hemodynamicvariables improved diagnosis and man-agement of circulatory instability (41,42). Critics, however, pointed to compli-cations associated with its insertion anduse, inaccuracies in measurement, anddifficulties with interpretation of data(40, 43–48). Furthermore, a lack of pos-itive outcome benefits in the critically illadult patient and some suggestions ofincreased mortality from retrospectiveanalyses indicated potential problemswith the PA catheter (40, 49 –51). In1996, a large, nonrandomized, risk-adjusted study in adult patients indicatedan increased 30-day mortality rate asso-ciated with PA catheter use in the first 24hrs after admission to intensive care (52).This fresh uncertainty encouraged fur-ther study of the use of the PA catheter inboth adult and pediatric patients.
Consensus on the use of PA catheterhas been summarized in the Society ofCritical Care Medicine Pulmonary ArteryCatheter Consensus Conference docu-ment (53). This document suggests thatthe PA catheter clarifies cardiopulmonaryphysiology in selected pediatric patientswith the following characteristics: 1) pul-monary hypertension; 2) shock refractoryto fluid resuscitation and/or low-to-moderate doses of vasoactive agents; 3)severe respiratory failure requiring highairway pressures; and 4) multiple organdysfunction on rare occasions. In thesepatients, data derived from the PA cathe-ter may improve outcome. However, theevidence supporting the use of the PAcatheter in these situations was limited tolevel IV (nonrandomized, historical con-trols, and expert opinion) and level V(case series, uncontrolled studies, and ex-pert opinion) evidence. There were nodata to suggest that use of the PA cathe-ter increases mortality in children. Thecommittee did recommend that the PAcatheter in pediatric patients should beused judiciously and for the shortest timenecessary. The PA catheter should beplaced under the direct supervision of anexperienced, attending-level physician.Interpretation of the PA catheter-deriveddata and subsequent management deci-sions should be supervised in a similarfashion. It should be emphasized that thePA catheter is a monitoring device, not atherapeutic modality (54). As a monitor,the PA catheter is directly attributable tovery little in the way of morbidity andmortality (55). Complications of the PAcatheter are rare (Table 4). Any adverseaffects associated with the PA catheter are
Figure 3. The continuous pressure monitoring trace as a pulmonary artery catheter is advancedthrough the heart.
Figure 4. Thermodilution curves.
Table 3. Derived values from pulmonary artery catheterization
Variable Formula Normal Range
HemodynamicStroke index SI � CI/HR 30–60 mL/m2
Cardiac index CI � CO/BSA 3.5–5.5 L/min/m2
Systemic vascular/resistance index SVRI � 79.9 (MAP–CVP) 800–1600 dynes�sec/cm5/m2
CIPulmonary vascular/resistance index PVRI � 79.9 (mPAP–PWP) 80–240 dynes�sec/cm5/m2
CINote: The PVRI may be expressed in units:
PVRI � mPAP–PWP 1–3 units/m2
CIIn the first week of life, the PVRI is considerably higher and may be 8–10 units/m2; it then falls rapidly
and by 6–8 weeks of life it is at adult value
Oxygen transportArterial oxygen content CaO2 � (Hgb)(1.34)(% sat) 17–20 mL/dL
� (PaO2)(0.003)Mixed venous oxygen content CVO2 � (Hgb)(1.34)(% sat) 12–15 mL/dL
� (PVO2) (0.003)Oxygen content difference avDO2 � CaO2–CVO2 3–5 mL/dLOxygen availability O2 avail � CI � CaO2 � 10 550–650 mL/min/m2
Oxygen consumption VO2 � CI � avDO2 � 10 120–200 mL/min/m2
HR, heart rate; BSA, body surface area; CO, cardiac ouput; MAP, mean arterial pressure; CVP,central venous pressure; mPAP, mean pulmonary arterial pressure; PWP, pulmonary wedge pressure;Hgb, hemoglobin; % sat, saturation; PVO2, venous oxygen pressure.
S15Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

likely, therefore, to be related to the ther-apeutic changes associated with the dataobtained from the monitor. Cliniciansmust interpret that data provided by thePA catheter and use that data with rele-vant protocols (42, 54). It is this alteredtherapeutic strategy that will favorablyalter outcome, not the PA catheter (53).
With these categories in mind, a re-view of more recent evidence is dis-cussed.
Pulmonary Hypertension
Pulmonary arterial hypertension inchildren is a critical determinant of mor-bidity and mortality in diverse pediatriccardiac and pulmonary disorders as wellas diseases affecting coagulation, inflam-mation, and immunity (56–59). Struc-ture and function of the pulmonary cir-culation can be altered by primaryaberrations of lung growth and develop-ment or secondary to injury associatedwith acute respiratory failure, chroniclung disease after premature birth,chronic hypoventilation, congenital heartdisease, and chronic hemolysis. Whereasthe impact of pulmonary arterial hyper-tension on the clinical course of childrenwith congenital heart disease and per-sistent pulmonary hypertension of thenewborn are clearly appreciated, thecontribution of pulmonary arterial hy-pertension to the course and ultimateoutcome of children with lung disease is
often overlooked or underestimated (56).Without therapy, high pulmonary vascu-lar resistance contributes to progressiveright ventricular failure, low cardiac out-put, and high mortality (56, 57).
Determining the etiology of pulmo-nary hypertension is the key to initialmanagement strategies (58). The goals ofdiagnostic evaluations are to characterizethe etiology and severity of pulmonaryhypertension, recognize and correct un-derlying causes, ascertain the reversibil-ity of the pulmonary hypertension, deter-mine initial treatment strategy, andassess the prognosis (58).
Right heart or PA catheterization isthe gold standard for the diagnosis ofpulmonary hypertension (58, 60–66). PAcatheterization is necessary for the he-modynamic differential diagnosis of pul-monary arterial hypertension; presentlyno noninvasive tests are available for theaccurate diagnosis of precapillary, post-capillary, and mixed types of pulmonaryarterial hypertension (41). Despite cur-rent controversies regarding the use ofPA catheters in the intensive care unit,hemodynamic data are valuable in thecare of critically ill patients with pulmo-nary hypertension (60, 66). Severe tricus-pid regurgitation and elevated PA pres-sure often make placing a PA catheterchallenging, and many necessitate theuse of fluoroscopy. Accurate determina-tion of cardiac output by thermodilutionmay be limited in patients with tricuspidregurgitation or low cardiac output (9,67–69).
Complications of PA catheterization inpatients with pulmonary hypertensioncan be life-threatening. In pediatric pa-tients, two studies have found that majorcomplications, including arrhythmia,pulmonary hypertensive crisis, and car-diac arrest, were 5% and 6%, respec-tively (70, 71).
Standard diagnostic criteria for pul-monary hypertension include the pres-ence of mean pulmonary artery pressure�25 mm Hg with pulmonary artery oc-clusion pressure �15 mm Hg and pul-monary vascular resistance �3 Woodunits/m2 (58). Hemodynamics deter-mined at the time of catheterization mayalso reflect prognosis (58, 72); elevatedmean pulmonary artery pressure and re-duced cardiac index predict a less favor-able prognosis. Angiography at catheter-ization should include evaluation ofpulmonary vessels for PA morphology,pulmonary vein flow, and aortogram to
exclude significant aortopulmonary con-nections.
Patients benefiting from therapiesthat serve as nitric oxide donors or fromlong-term calcium channel blockers maybe identified by acute vasodilator chal-lenge during right heart catheterization(58). Potential agents used in testing mayinclude inhaled nitric oxide, intravenousadenosine, or intravenous epoprostenol.Additional medications may also betested, acutely, including oral sildenafil,oral nifedipine, and inhaled prostacyclin(63). Response to vasodilator therapy isdefined as mean pulmonary artery pres-sure decrease by 10 mm Hg to reach amean pulmonary artery pressure of �40mm Hg with normal or high cardiac out-put. Children are more likely to respondto acute vasodilator testing than adultsand response to acute vasodilator testingpredicts both response to long-term va-sodilator therapy and survival (58).
Recommendations for the use of rightheart or PA catheterization in the assess-ment of pediatric pulmonary hyperten-sion are as follows (58, 72): 1) hemody-namic catheterization is recommended toconfirm the diagnosis and establish se-verity (class I, level of evidence C); and 2)right heart catheterization with vasodila-tor testing is recommended to guide ini-tial determination of therapy (class I,level of evidence B).
Shock
The primary physiological task of thecardiovascular system is to deliverenough O2 to meet the metabolic de-mands of the body. Shock and tissue hyp-oxia occur when the cardiorespiratorysystem is unable to meet the metabolicdemand adequately. Sustained tissuehypoxia is one of the most importantcofactors in the pathophysiology of organdysfunction (73). Therefore, determiningthe adequacy of tissue oxygenation incritically ill patients is central to ascer-taining the health of the patient and theresponse to therapy. Unfortunately, normalvalues in blood pressure, central venouspressure, heart rate, and blood gases do notrule out tissue hypoxia or imbalances be-tween whole-body oxygen supply and de-mand (73–75). This discrepancy has led toincreased interest in more direct indicatorsof adequacy of tissue oxygenation such asmixed and central venous oxygen satura-tions. PA catheterization allows obtainingtrue mixed venous oxygen saturation,whereas measuring central venous oxygen
Table 4. Complications of pulmonary arterycatheter placement
Problems with vesselcannulation
Arterial puncturePneumothoraxHemothoraxHydrothoraxAir embolismThoracic injuryBronchial injury
Insertion problemsArrhythmiasCardiac conduction
disturbancesCatheter looping
and knottingPulmonary artery
perforationValve damage
Maintenance problemsPulmonary infarctionVenous thrombosisInfectionsAseptic endocarditisThrombocytopeniaBalloon rupture
S16 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

saturation through a central venous cathe-ter reflects principally the degree of oxygenextraction for the brain and the upper partof the body.
A study by Ceneviva et al categorized50 children with fluid-refractory septicshock according to hemodynamic state(based on hemodynamic data obtainedwith the pulmonary artery catheter) intoone of three possible cardiovascular de-rangements: 1) hyperdynamic state char-acterized by high cardiac output (�5.5L/min/m2 body surface area) and low sys-temic vascular resistance (SVR) (�800dynes·sec/cm5) (classically referred to aswarm shock); 2) a hypodynamic statecharacterized by low cardiac output(�3.3 L/min/m2 body surface area) andlow SVR; or 3) a hypodynamic state char-acterized by low cardiac output and highSVR (�1200 dynes·sec/cm5) (classicallyreferred to as cold shock) (76). In con-trast to adults in which the early stages ofseptic shock are characterized by highcardiac output and low SVR, most ofthese children were in a hypodynamicstate characterized by low cardiac outputand high SVR (cold shock) and required theaddition of vasodilators to decrease SVR,increase cardiac output, decrease myocar-dial oxygen consumption, and improve pe-ripheral perfusion (76). Children with lowcardiac output (as defined by a cardiac in-dex �2.0 L/min/m2 body surface area) hadthe highest risk of mortality.
This study as well as literature re-ferred to early in this article supports theuse of the PA catheter to define the exacthemodynamic state in the patient withrefractory shock (Table 5) (77). The newinformation gained allows for therapiesto be tailored to address the hemody-namic derangements determined to bepresent on institution of PA cathetermonitoring. An independent review ofthis topic interpreted the results in theCeneviva study to support the use of the
PA catheter in the select group of chil-dren with septic shock whose hemody-namic profile and clinical condition werenot improved by the application of ther-apies based on the data obtained by pe-ripheral arterial and central venous pres-sure and oxygen saturation monitoring(78). In the clinical practice parametersfor hemodynamic support of pediatricand neonatal patients in septic shock ar-ticle, Carcillo and colleagues (77) recom-mended that a PA catheter should be con-sidered when poor perfusion, includingreduced urine output, acidosis, or hypo-perfusion, persists despite use of hemo-dynamic therapies guided by clinical ex-amination, blood pressure analysis,echocardiographic analysis, and arterialand superior vena cava oxygen saturationanalysis.
Once the PA catheter is placed, ther-apy should be adjusted to maintain mixedvenous oxygen saturation �70%, cardiacindex �3.3 L/min/m2, and a normal per-fusion pressure for age (mean arterialpressure–central venous pressure) withthe ultimate goal of restoration of normalperfusion (77). These recommendationswere considered a level II recommenda-tion (reasonably justified by scientific ev-idence and strongly supported by expertcritical care opinion). These goals werereaffirmed in the 2007 clinical practiceparameters for hemodynamic support ofpediatric and neonatal septic shock (79).
At one time, hemodynamic therapyaimed at achieving supranormal valuesfor cardiac index and oxygen delivery wasencouraged for critically ill patients (80,81). This therapeutic strategy was basedon the observations that patients whosurvived had values for cardiac index andoxygen delivery that were higher thanthose of patients who died and, more im-portant, higher than standard physiolog-ical values (82, 83). Recent studies fail toshow a benefit of increasing oxygen de-
livery beyond the point of oxygen con-sumption plateau (77, 80, 84, 85).
Recommendations for the use of PAcatheterization in the assessment andmanagement of shock are that the PAcatheter can be used in those patientswho remain in shock despite therapiesdirected to clinical signs of perfusion,mean arterial pressure–central venouspressure, central venous oxygen satura-tion, and echocardiographic analyses(class IIa, level of evidence C) (79).
Acute Lung Injury
A common diagnostic indication for theuse of a PA catheter is pulmonary edemawhen there is doubt concerning the natureor cause (i.e., cardiogenic vs. noncardio-genic pulmonary edema) (33–36).
The diagnosis of noncardiogenic pul-monary edema or the acute respiratorydistress syndrome (ARDS) is based onphysical and radiologic evidence of bilat-eral pulmonary infiltrates consistent withedema, refractory hypoxemia, and normalleft ventricular filling pressure (38).
Almost all currently available forms ofmechanical ventilation can have pro-nounced direct and/or indirect effects ona patient’s circulatory function and car-diopulmonary reserve (86). Biphasic fluc-tuations in airway and intrathoracic pres-sures change the preload conditions onthe right side of the heart by alteringvenous return, transmural pressure gra-dients, and pulmonary vascular resis-tance. Altering positive end-expiratorypressure in the management of patientswith ARDS may significantly affect pul-monary blood flow and ventilation/perfusion matching; these changes inphysiology will best be determined by thedata obtained from the PA catheter.
Patients with ARDS may have an un-predictable response to mechanical ven-tilation and the physical findings may notbe helpful in assessment of the adequacyof tissue oxygen delivery (87–90). Contin-uous arterial pressure monitoring withmeasurement of systemic blood flow andPA catheterization with mixed venousoxyhemoglobin saturation monitoringmay prove valuable in these vulnerablepatients (87, 88). It has been postulatedthat monitoring both right and left ven-tricular filling pressures (right atrial andpulmonary capillary wedge pressures)and cardiac output will facilitate themaintenance of volume status and regu-lation of vasopressor and inotropic ther-apy in patients with ARDS (41). It has
Table 5. Cardiopulmonary failure patterns
CO PCWP SVR C(a–V�O2) PV
�O2 O2Ext
Hypovolemic 2 2 1 1 2 1Cardiogenic 2 1 1 1 2 1Obstructive 2 1 1 1 2 1Septic
High output 1 2 2 2 1 2Low output 2 1 1 1 2 1
C(a–V�O2), arteriovenous oxygen content difference; PV�O2 mixed venous oxygen partial pressure;O2Ext, oxygen extraction; CO, cardiac output; PCWP, pulmonary capillary wedge pressure; SVR,systolic vascular resistance.
S17Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

been suggested that such hemodynamicmonitoring with the use of PA cathetersis superior to the use of central venouscatheters to monitor central venous pres-sure alone and is likely to produce a bet-ter outcome. Indeed, many nonrandom-ized clinical studies have recommended,for routine bedside hemodynamic moni-toring, the use of PA catheters for man-agement of ARDS (89). However, in adultpatients, a recent study suggested that PAcatheter-guided therapy in patients withacute lung injury did not improve sur-vival or organ function but was associatedwith more complications than central ve-nous pressure-guided therapy (91). Sim-ilar studies do not exist in children.
Strategies for managing ARDS includenot only the manipulation of mechanicalventilation, but also nonventilatory modal-ities such as fluid restriction and selectiveuse of pulmonary vasodilators (92, 93).
Fluid administration increases hydro-static pressure in the lungs and promotesfluid filtration and edema formation, par-ticularly in states of increased microvas-cular permeability such as ARDS. In ran-domized clinical trials, a conservativefluid management strategy for patientswith ARDS resulted in lower intravascu-lar pressure, less extravascular lung wa-ter, shorter duration of mechanical ven-tilation, and shorter intensive care unitlength of stay (93, 94). The exact fluidstrategy will vary from patient to patient;in some patients, the use of the PA cath-eter may be necessary to achieve the op-timal cardiac hemodynamic profile.
Pulmonary hypertension, resultingfrom vasoconstriction and occlusion ofthe pulmonary microvasculature, iswidely recognized as a characteristic fea-ture of ARDS (95, 96). Pulmonary hyper-tension contributes to impaired rightventricular performance and cardiac out-put in patients with ARDS, leading to areduction in systemic oxygen delivery.Pharmacologic manipulation of pulmo-nary vascular tone is feasible in patientswith ARDS but will require carefully per-formed clinical trials and close character-ization of the hemodynamic profile.
Recommendations for the use of a PAcatheter in the management of patientswith ARDS or pulmonary edema are: 1)the PA catheter may be useful in selectedpediatric patients with ARDS (class IIb,level of evidence C) (53); and 2) the PAcatheter may be useful in the diagnosisand management of uncertain causes ofpulmonary edema (class IIb, level of evi-dence C) (33–36).
Conclusion
The PA catheter may be useful in themanagement of selected pediatric pa-tients, especially those with pulmonaryarterial hypertension and shock refrac-tory to standard fluid resuscitation andvasoactive agents. Data obtained from thePA catheter can delineate the patient’shemodynamic profile, can be followed toevaluate the response to therapeutic in-terventions, and in certain circumstancesmay improve outcome and/or be of prog-nostic importance.
If a properly trained physician believesthat invasive hemodynamic data are nec-essary for the management of a specificpatient, then the use of the PA catheter isjustified in that patient (42). Once a PAcatheter is in place, one must insist oncorrect measurement, correct interpreta-tion, and correct application of the dataobtained.
REFERENCES
1. Swan HJL, Ganz W, Forrester J, et al: Cath-eterization of the heart in man with use of aflow-directed balloon-tipped catheter. N EnglJ Med 1970; 283:447–451
2. Lodato RF: Use of the pulmonary artery cath-eter. Semin Respir Crit Care Med 1999; 20:29–42
3. Katz RN, Pollack MM, Weibley RE: Pulmo-nary artery catheterization in pediatric in-tensive care. Adv Pediatr 1983; 30:169–190
4. Thompson AE: Pulmonary artery catheter-ization in children. New Horiz 1997;5:244–250
5. Todres ID, Crone RK, Rogers ML, et al:Swan-Ganz catheterization in the criticallyill newborn. Crit Care Med 1979; 7:330–334
6. Yoshizato T, Hagler DJ: Pulmonary arterycatheter placement with two-dimensionalechocardiographic guidance: A technique ap-plicable in critically ill neonates. Mayo ClinProc 1989; 64:387–391
7. Pollack MM, Reed TP, Holbrook PR, et al:Bedside pulmonary artery catheterization inpediatrics. J Pediatr 1980; 96:274–276
8. Weidemann HR, Matthay MA, Matthay RA:Cardiovascular–pulmonary monitoring inthe intensive care unit. Chest 1984; 85:537
9. Perkin RM: Invasive monitoring in the pedi-atric intensive care unit. In: Pediatric Inten-sive Care. Nussbaum E (Ed). New York, Fu-ture Publishing Inc, 1989, pp 255–267
10. Ganz W, Swan HJC: Measurement of bloodflow by thermodilution. Am J Cardiol 1972;29:241–246
11. Raper R, Sibbald WJ: Misled by the wedge?Chest 1986; 89:427
12. Stevens JH, Rattin TA, Mihm FG, et al: Ther-modilution cardiac output measurement.JAMA 1985; 253:2240
13. Borland LM: Allometric determination of the
distance from the central venous pressureport to wedge position of the balloon-topcatheters in the pediatric patients. Crit CareMed 1986; 14:974–976
14. Vincent JL: New developments in pulmonaryartery catheterization. Intensive Care World1986; 3:42–43
15. Carcillo JA, Davis AL, Zaritsky A: Role ofearly fluid resuscitation in pediatric septicshock. JAMA 1991; 26:1242–1245
16. Pollack MM, Fields AI, Ruttimann UE, et al:Sequential cardiopulmonary variables of in-fants and children in septic shock. Crit CareMed 1984; 12:554–559
17. Pollack MM. Fields AI, Ruttimann UE: Dis-tributions of cardiopulmonary variables inpediatric survivors and nonsurvivors of sep-tic shock. Crit Care Med 1985; 13:454–459
18. Carcillo JA, Pollack MM, Ruttimann UE, et al:Sequential physiologic interactions in car-diogenic and septic shock. Crit Care Med1989; 17:12–16
19. Mercier JC, Beaufils F, Hartmann JF, et al:Hemodynamic patterns of meningococcalshock in children. Crit Care Med 1988; 16:27–33
20. Lucking SE, Williams TM, Chaten FC: De-pendence of oxygen consumption on oxygendelivery in children with hyperdynamic sep-tic shock and low oxygen extraction. CritCare Med 1990; 18:1316–1319
21. Mink RB, Pollack MM: Effect of blood trans-fusion on oxygen consumption in pediatricseptic shock. Crit Care Med 1990; 18:1087–1091
22. Reynolds EM, Ryan DP, Sheridan RL, et al:Left ventricular failure complicating severepediatric burn injury. J Pediatr Surg 1994;30:264–269
23. Krafte-Jacobs B, Carver J, Wilkinson JD:Comparison of gastric intramucosal pH andstandard perfusional measurements in pedi-atric septic shock. Chest 1995; 108:220–225
24. Perkin RM, Levin DL, Webb R, et al: Dobut-amine: A hemodynamic evaluation in chil-dren with shock. J Pediatr 1982; 100:977–983
25. Barton P, Garcia J, Koutali A, et al: Hemo-dynamic effects of IV milrinone lactate inpediatric patients with septic shock: A pro-spective, double-blind, randomized, placebo-controlled, interventional study. Chest 1996;109:1302–1312
26. Lindsay CA, Barton P, Lawless S, et al: Phar-macokinetics and pharmacodynamics of mil-rinone lactate in pediatric patients with sep-tic shock. J Pediatr 1998; 132:329–334
27. Irazusta JE, Pretzlaff RK, Rowin ME: Amri-none in pediatric refractory shock: An openlabel pharmacodynamic study. Pediatr CritCare Med 2001; 2:24–28
28. Morray JP, Lynn AM, Mansfield PB: Effects ofpH and CO2 on pulmonary and systemic he-modynamics after surgery in children withcongenital heart disease and pulmonary hy-pertension. J Pediatr 1988; 113:474–479
29. Seear M, Wensky D, MacNab A: Oxygen
S18 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

consumption– oxygen delivery relationshipin children. J Pediatr 1993; 123:208–214
30. Morris K, Beghetti M, Petros A, et al: Com-parison of hyperventilation and inhaled ni-tric oxide for pulmonary hypertension afterrepair of congenital heart disease. Crit CareMed 2000; 28:2974–2978
31. Goodman G, Perkin RM, Anas NG, et al:Pulmonary hypertension in infants withbronchopulmonary dysplasia. J Pediatr 1988;112:67–72
32. Ameling A, Joosten KFM, Berger RMF: Thesemi-elective use of the pulmonary floatationcatheter in children with progressive pulmo-nary hypertension or left ventricular dys-function. Pediatr Crit Care Med 2001;2:211–216
33. Perkin RM, Anas N, Lubinsky P: Myocardialischemic and disparate ventricular functionafter pediatric head injury. Crit Care Med1991; 19:587–588
34. Sibbald WJ, Cunningham DR, Chin DN: Non-cardiac or cardiac pulmonary edema: A prac-tical approach to clinical differentiation incritically ill patients. Chest 1983; 84:452–460
35. Fein AM, Goldberg SK, Walkenstein MD, etal: Is pulmonary artery catheterization nec-essary for the diagnosis of pulmonary edema?Am Rev Respir Dis 1984; 129:1006
36. Ermakov S, Hoyt JW: Pulmonary artery cath-eterization. Crit Care Clin 1992; 8:773–806
37. Pollack MM, Fields AI, Holbrook PR: Cardio-pulmonary parameters during high PEEP inchildren. Crit Care Med 1980; 8:372–376
38. Paulson TE, Spear RM, Silva PO, et al: High-frequency pressure-control ventilation withhigh positive end-expiratory pressure in chil-dren with acute respiratory distress syn-drome. J Pediatr 1996; 129:566–573
39. Williams G, Grouds M, Rhodes A: Pulmonaryartery catheter. Curr Opin Crit Care 2002;8:251–256
40. Harvey S, Harrison DA, Singer M, et al: As-sessment of the clinical effectiveness of pul-monary artery catheters in management ofpatients in intensive care (PAC-MAN): A ran-domized controlled trial. Lancet 2005; 366:472–477
41. Chatterjee K: The Swan-Ganz catheters:Past, present and future: A viewpoint. Circu-lation 2009; 119:147–152
42. Vincent JL, Pinsky MR, Sprung CL, et al: Thepulmonary artery catheter: In medio virtus.Crit Care Med 2008; 36:3093–3096
43. Robin ED: The cult of the Swan-Ganz catheter:Overuse and abuse of pulmonary flow cathe-ters. Ann Intern Med 1985; 103:445–449
44. Guyatt G: A randomized control trial ofright-heart catheterization in critically ill pa-tients. J Intensive Care Med 1991; 6:91–95
45. Trottier SJ, Taylor RW: Physicians’ attitudestoward and knowledge of the pulmonary ar-tery catheter: Society of Critical Care Mem-bership Survey. New Horiz 1997; 5:201–206
46. Connors AF: Potential misuse of the pulmo-nary artery catheter. Semin Respir Crit CareMed 1999; 20:43–51
47. Squara P, Bennett D, Perret C: Pulmonaryartery catheter: Does the problem lie withthe users? Chest 2002; 121:2009–2015
48. Peters SG, Afessa B, Decker PA, et al: In-creased risk associated with pulmonary ar-tery catheterization in the medical intensivecare unit. J Crit Care 2003; 18:166–171
49. Gore JM, Goldberg RJ, Spodick DH, et al: Acommunity wide assessment of the use ofpulmonary artery catheters in patients withacute myocardial infarction. Chest 1987; 92:721–727
50. Zion MM, Balkin J, Rosenmann D, et al: Useof pulmonary artery catheters in patientswith acute myocardial infarction. Chest1990; 98:1331–1335
51. Sandham JD, Hull RD, Brant RF, et al: Arandomized, controlled trial of the use ofpulmonary artery catheters in high-risk sur-gical patients. N Engl J Med 2003; 348:5–14
52. Connors AF, Speroff TS, Dawson NV, et al:The effectiveness of right heart catheteriza-tion in the initial care of critically ill pa-tients. JAMA 1996; 276:889–897
53. Pulmonary Artery Catheter Consensus Con-ference Participants: Pulmonary Artery Cath-eter Consensus Conference: ConsensusStatement. Crit Care Med 1997; 25:910–924
54. Rhodes A, Cusack RJ, Newman PJ, et al: Arandomized, controlled trial of the pulmo-nary artery catheter in critically ill patients.Intensive Care Med 2002; 28:256–264
55. Dalen JE, Bone RC: Is it time to pull thepulmonary artery catheter? JAMA 1996; 276:916–918
56. Abman SH: Pulmonary hypertension in chil-dren: A historical overview. Pediatr Crit CareMed 2010; 11(Suppl):S4–S9
57. Bronicki RA, Baden HP: Pathophysiology ofright ventricular failure in pulmonary hyper-tension. Pediatr Crit Care Med 2010;11(Suppl):S15–S22
58. Mullen MP: Diagnostic strategies for acutepresentation of pulmonary hypertension inchildren: Particular focus on use of echocar-diography, cardiac catheterization, magneticresonance imaging, chest computed tomog-raphy, and lung biopsy. Pediatr Crit CareMed 2010; 11(Suppl):S23–S26
59. Greyson CR: Pathophysiology of right ventric-ular failure. Crit Care Med 2008; 36(Suppl):557–565
60. Zamanian RT, Haddock F, Doyle RL, et al:Management strategies for patients with pul-monary hypertension in the intensive careunit. Crit Care Med 2007; 35:2037–2050
61. Widlitz A, Barst RJ: Pulmonary arterial hy-pertension in children. Eur Respir J 2006;21:155–176
62. Rashid A, Ivy D: Severe paediatric pulmonaryhypertension: New management strategies.Arch Dis Child 2005; 90:92–98
63. Berger S, Konduri GC: Pulmonary hyperten-sion in children: The twenty-first century.Pediatr Clin North Am 2006; 53:964–987
64. McLaughlin VV, Archer SL, Badesch DB, etal: ACCF/AHA 2009 expert consensus docu-
ment on pulmonary hypertension: A reportof the American College of Cardiology TaskForce on Expert Consensus Documents andthe American Heart Association. Circulation2009; 119:2250–2294
65. Linsuwan A, Khawsathit P: Assessment ofpulmonary vasoreactivity in children withpulmonary hypertension. Curr Opin Pediatr2009; 21:00594–599
66. Taylor MB, Laursen PC: Fundamentals ofmanagement of acute post operative pulmo-nary hypertension. Pediatr Crit Care Med2010; 11(Suppl):S27–S29
67. Heerdt PM, Blessios GA, Beach ML, et al:Flow dependency of error in thermodilutionmeasurement of cardiac output during acutetricuspid regurgitation. J Cardiothorac VascAnesth 2001; 15:183–187
68. Olsson B, Pool J, Vandernoten P, et al: Valid-ity and reproducibility of determination ofcardiac output by thermodilution in man.Cardiology 1970; 55:136–148
69. Sharkey SW: Beyond the wedge: Clinicalphysiology and the Swan-Ganz catheter.Am J Med 1987; 83:111–122
70. Carmosino MJ, Friesen RH, Doran A, et al:Perioperative complications in children withpulmonary hypertension undergoing non-cardiac surgery or cardiac catheterization.Anesth Analog 2007; 204:521–527
71. Taylor CJ, Derrick G, McEwen A: Risk ofcardiac catheterization under anesthesia inchildren with pulmonary hypertension. Br JAnaesth 2007; 98:657–661
72. Giglia TM, Humpl T: Preoperative pulmonaryhemodynamics and assessment of operabil-ity: Is there a pulmonary vascular resistancethat precludes cardiac operations? PediatrCrit Care Med 2010; 11(Suppl):557–569
73. Bloss F, Reinhart K: Venous oximetry. Inten-sive Care Med 2005; 31:911–913
74. Spenceley N, Krahn G, Skipper PW, et al:Evaluation of a pediatric central venous oxi-metry catheter in critically ill children. Pe-diatric Crit Care Med 2010; 11:26–30
75. de Oliveira CF, de Oliveira DSF, GottschaldAFC, et al: ACCM/PALS haemodynamicsupport guidelines for paediatric septicshock: An outcome comparison with andwithout monitoring central venous oxygensaturation. Intensive Care Med 2008; 34:1065–1075
76. Ceneviva G, Paschall JA, Maffei F, et al: He-modynamic support in fluid refractory pedi-atric septic shock. Pediatrics 1998; 102:e19
77. Carcillo JA, Fields AI: Task Force CommitteeMembers. Clinical practice parameters forhemodynamic support of pediatric and neo-natal patients in septic shock. Crit Care Med2002; 301:1365–1378
78. Zaritsky A: Hemodynamic patterns in pediat-ric septic shock. Pediatr Emerg Crit Care1998; 11:33–34
79. Brierly J, Carcillo JA, Choong K, et al: Clin-ical practice parameters for hemodynamicsupport of pediatric and neonatal septic
S19Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

shock: 2007 update from the American Col-lege of Critical Care Medicine. Crit Care Med2009; 37:666–688
80. Gattinoni L, Brazzi L, Pelosi P, et al: A trial ofgoal oriented hemodynamic therapy in crit-ically ill patients. N Engl J Med 1994; 333:1025–1032
81. Shoemaker WC: Relation of oxygen transportpatterns to the pathophysiology and therapyof shock states. Intensive Care Med 1987;13:230–243
82. Shoemaker WC, Appel PL, Kram HB, et al:Prospective trial of supranormal values ofsurvivors as therapeutic goals in high-risksurgical patients. Chest 1988; 94:1176–1186
83. Boyd O, Grounds RM, Bennett ED: A ran-domized clinical trial of the effect of deliber-ate perioperative increase of oxygen deliveryon mortality in high-risk surgical patients.JAMA 1993; 270:2699–2707
84. Hayes MA, Timmins AL, Yau EHS, et al:Oxygen transport patterns in patients withsepsis syndrome or septic shock: Influence oftreatment and relationship to outcome. CritCare Med 1997; 25:926–936
85. McKinky BA, Kozar RA, Cocanour CS, et al:Normal versus supranormal oxygen delivery
goals in shock resuscitation: The response isthe same. J Trauma 2002; 53:825–832
86. Bronicki RA, Anas NG: Cardiopulmonary in-teraction. Pediatr Crit Care Med 2009; 10:313–322
87. Tolh I, Leiner T, Mikor A, et al: Hemody-namic and respiratory changes during lungrecruitment and descending optimal positiveend-expiratory pressure filtration in patientswith acute respiratory distress syndrome.Crit Care Med 2007; 35:787–793
88. Lo TM, Jones PA, Freeman JA, et al: The role ofhigh frequency oscillatory ventilation in man-agement of children with severe traumaticbrain injury and concomitant lung pathology.Pediatr Crit Care Med 2008; 9:e38–e42
89. Richard C, Warszawski J, Anguel N, et al:Early use of the pulmonary artery catheterand outcomes in patients with shock andacute respiratory distress syndrome: A ran-domized controlled trial. JAMA 2003; 290:2713–2720
90. Grissom CK, Morris AH, Lanken PN, et al:Association of physical examination with pul-monary artery catheter parameters in acutelung injury. Crit Care Med 2009; 37:2720–2726
91. The National Heart, Lung, and Blood Insti-tute Acute Respiratory Distress Syndrome(ARDS) Clinical Trials Network: Pulmonary-artery versus central venous catheter toguide treatment of acute lung injury. N EnglJ Med 2006; 354:2213–2224
92. Schuster KM, Alouidor R, Barquist ES: Non-ventilatory interventions in the acute respi-ratory distress syndrome. J Intensive CareMed 2008; 23:19–32
93. Raoof S, Goulet K, Esan A, et al: Severehypoxemic respiratory failure. Part 2—Non-ventilatory strategies. Chest 2010; 137:1437–1448
94. The National Heart, Lung, and Blood Insti-tute Acute Respiratory Distress Syndrome(ARDS) Clinical Trials Network: Comparisonof two fluid-management strategies in acutelung injury. N Engl J Med 2006; 354:2264–2275
95. Zapol WM, Snider MT: Pulmonary hyperten-sion in severe acute respiratory failure.N Engl J Med 1977; 296:476–480
96. Moloney D, Evans TW: Pathophysiology andpharmacological treatment of pulmonary hy-pertension in acute respiratory distress syn-drome. Eur Respir J 2003; 21:720–727
S20 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Venous oximetry and the assessment of oxygen transport balance
Ronald A. Bronicki, MD
One of the tenets of criticalcare medicine is to ensureadequate tissue oxygenation.This assessment must be
timely and accurate to optimize out-comes. This determination is often basedon clinical parameters such as the phys-ical examination and standard hemody-namic parameters, including blood pres-sure, central venous pressure, and urineoutput. However, studies have demon-strated significant discordance betweenassessments based on these parametersand those based on measurements of car-diac output (CO) and venous oximetry(1–3). The routine use of central venouscatheters readily enables the clinician toassess oxygen extraction, oxygen trans-port balance, and the adequacy of tissueoxygenation.
To accurately interpret and appreciatethe use and limitations of venous oxime-try requires an understanding of the de-terminants of tissue oxygenation; the re-lationship between oxygen requirementsand oxygen delivery or oxygen transportbalance; and the compensatory circula-tory responses to alterations in oxygentransport balance. These principles aswell as the evidence supporting the use ofvenous oximetry are reviewed.
Physiology of TissueOxygenation and OxygenTransport Balance
According to the Fick equation, totalbody oxygen consumption (VO2) is equalto the product of CO and the difference inarterial–venous oxygen content (CaO2 �CvO2) or the volume of oxygen extractedper minute (Table 1). Because oxygen ispoorly soluble in water, the amount ofoxygen dissolved in blood is minimal andinconsequential except in cases of severeanemia. By ignoring the amount of oxy-gen dissolved in blood, the Fick equationmay be simplified to: SaO2 � SmvO2 �VO2/DO2, where SaO2 is the arterial oxygensaturation; SmvO2 is the mixed venousoxygen saturation, which is obtainedfrom the pulmonary artery and is theweighted average of venous return fromall viscera; and DO2 is oxygen delivery, theproduct of CO and arterial oxygen con-tent. SaO2 � SmvO2 is the percent oxygenextraction; however, in the presence ofarterial hypoxemia, oxygen extraction isassessed by calculating the oxygen extrac-tion ratio (OER) (Table 2A).
By measuring oxygen extraction, therelationship between oxygen demand andDO2 or oxygen transport balance can beassessed and the adequacy of tissue oxy-genation determined (Table 1). If oxygenrequirements were to remain constant, asDO2 decreases, oxygen extraction in-creases to maintain adequate tissue oxy-genation and VO2 remains unchanged(Fig. 1). Below a given DO2, oxygen ex-traction continues to increase but oxygendemands exceed oxygen availability. Atthis point VO2 falls, anaerobic metabolismensues, and lactate begins to accumulate(Table 2B). This represents the critical
DO2, which is the same regardless ofwhether the decrease in DO2 resultedfrom anemia, hypoxemia, and/or low CO(4). The corresponding percent oxygenextraction represents the critical OER. Ifoxygen requirements were to change, thecritical DO2 would change in parallel;however, the indicator of the adequacy oftissue oxygenation, the critical OER, re-mains constant between 50% and 60%(Fig. 2) (5–7).
For most viscera, flow is tightly cou-pled to metabolism. Local metabolic reg-ulation of vasomotor tone provides thehomeostatic mechanism by which meta-bolic demand influences perfusion. As aresult, regional and global OERs remainfairly constant despite modest changes inthe determinants of oxygen transport bal-ance (Table 3). Increases in oxygen re-quirements or decreases in oxygen con-tent resulting from hypoxemia or anemiaare compensated for by increases in bloodflow and the OER remains normal (8–11). The OER increases appreciably withsignificant increases in oxygen require-ments or decreases in oxygen content andwhen CO is limited. The primary com-pensatory mechanism to maintain tissueoxygenation in a low CO state is an in-crease in oxygen extraction. Thus, as longas the OER is not significantly elevated,DO2 is adequate and aerobic metabolismis maintained. The exception to this oc-curs in pathologic states characterized byimpaired oxygen use such as cyanide poi-soning. In this condition, serum lactatelevels are significantly elevated despite anelevated DO2 and narrowed OER.
Like with cyanide poisoning, some pa-tients in septic shock also appear to haveimpaired oxygen utilization. In these pa-
From the Children’s Hospital of Orange County, Or-ange, CA; and David Geffen School of Medicine at theUniversity of California Los Angeles, Los Angeles, CA.
The author has not disclosed any potential conflictof interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e3182211667
Objective: To review the principles of venous oximetry; thephysiology of oxygen transport balance; clinical studies on ve-nous oximetry; and the assignment of a classification of recom-mendation and level of evidence.
Data Source: A MEDLINE-based literature source.Conclusion: One of the tenets of critical care medicine is to
provide a timely and accurate assessment of tissue oxygenation.
In conjunction with other monitoring modalities, the routine de-ployment of central venous catheters readily enables the clinicianto complete this task. (Pediatr Crit Care Med 2011; 12[Suppl.]:S21–S26)
KEY WORDS: oxygen delivery; oxygen consumption; oxygen ex-traction ratio; oxygen transport balance; venous oximetry; shock
S21Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

tients, serum lactate levels are elevateddespite the fact that the OER is less thancritical. Furthermore, increasing DO2
does not increase measured VO2 (12).That said, it is unclear if the lactic acido-sis is the result of impaired oxygen utili-zation because the OER increases as DO2
decreases; the critical DO2 and criticalOER are the same as those seen in criti-cally ill nonseptic patients; and as theOER rises above critical, serum lactatelevels rise even further (13–16). Furtherconfounding the discussion, serum lac-tate levels may be elevated as a result ofimpaired clearance (17). In any case, thelactic acidosis seen in patients with septicshock in conjunction with an OER lessthan critical is not responsive to an in-crease in DO2.
The Oxygen–HemoglobinDissociation Curve
The shape and position of the oxygen–hemoglobin dissociation curve relates thepartial pressure of oxygen to the percentoxygen bound to hemoglobin and in do-ing so graphically depicts the affinity ofoxygen for hemoglobin. The P50 is thepartial pressure of oxygen at which 50%
of hemoglobin is saturated. A shift in theoxygen– hemoglobin dissociation curveto the right, or an increased P50, repre-sents a decrease in the affinity of oxygenfor hemoglobin, whereas a shift to the leftis reflective of an increase in affinity ofoxygen for hemoglobin. The relevance ofthe oxygen– hemoglobin dissociationcurve to a review of venous oximetry isthat in critical illness, the affinity of ox-ygen for hemoglobin is frequently al-tered, which may affect the loading andunloading of oxygen and the interpreta-tion of venous oximetry.
A decrease in the affinity of oxygen forhemoglobin is thought to be teleologicalin shock because it increases the effi-ciency of oxygen extraction. If this weretrue, a shift in the oxygen–hemoglobin dis-sociation curve to the right would increaseand a shift to the left would decrease thecritical OER. However, this does not appear
to be the case. Regardless of the P50, theOER increases in proportion to decreases inCO/DO2. Whether the P50 is reduced (18) orincreased (19), the efficiency of oxygenextraction and the critical OER remainunchanged. At the critical OER, the ve-nous partial pressure of oxygen will belowest in those with a reduced P50, in-termediate in those with a normal P50,and highest in those with an increasedP50. However, the critical OER remainsthe same across all groups.
Compensatory Mechanisms toMaintain Tissue Oxygenation
As CO and DO2 decrease and/or VO2
increases, three separate but interrelatedprocesses attempt to maintain oxygentransport balance: CO is augmented,blood flow is redistributed between or-gans, and microcirculatory changes en-
Figure 1. The relationship between oxygen delivery (DO2), oxygen consumption (VO2), and oxygen (O2)extraction. Initially, as DO2 decreases, VO2 remains constant as a result of an increase in O2 extraction(i.e., VO2 is independent of DO2). As DO2 decreases further, O2 extraction increases further but notenough to maintain a constant VO2 (i.e., VO2 becomes dependent on DO2). Without a change in O2
demand, the critical DO2 is defined when VO2 begins to fall.
Figure 2. The curvilinear relationship between cardiac index and oxygen extraction as oxygenconsumption (VO2) varies. The critical oxygen extraction ratio remains the same; however, the criticaloxygen delivery increases as O2 demand increases.
Table 1. Oxygen transport balance
Fick equation:VO2 � CO � CaO2 � CvO2
By ignoring the amount of oxygen dissolved inblood, the Fick equation may be simplified to:
SaO2 � SmvO2 � VO2/DO2 � oxygentransport balance
VO2, oxygen consumption (cc/min); CO, car-diac output (L/min); CaO2, arterial O2 content (ccO2/dL); CvO2, venous O2 content (cc O2/dL); SaO2,arterial O2 saturation; SmvO2, mixed venous O2
saturation; DO2, oxygen delivery (CO � CaO2;O2/min).
Table 2. Oxygen extraction ratioa
A. Oxygen Extraction Ratio (OER)
OER �SaO2 � SmvO2
SAO2
SaO2, arterial O2 saturation; SmvO2, mixed venousO2 saturation
B. Oxygen Extraction Ratios
25% Normal30% to 40% Increased40% to 50% Impending shock�50% to 60% Shock, lactic acidosis
aBased on mixed venous O2 saturation.
S22 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

hance tissue extraction of oxygen. As DO2
and CO become limited, cardiopulmo-nary receptors, arterial baroreceptors,and chemoreceptors are stimulated. Thisleads to activation of neurohormonal sys-tems and an increase in circulating levels ofcatecholamines, angiotensin II, aldoste-rone, and vasopressin; direct adrenergicstimulation of the myocardium also occurs.These vasoactive substances cause veno-constriction, thereby reducing venous ca-pacitance, and stimulate fluid retention,both of which serve to increase venous re-turn and ventricular filling; additionally,they increase heart rate, enhance myocar-dial function, and increase arterial vasculartone. The net result is an increase in CO,DO2, and arterial pressure.
When CO is limited, the redistributionof blood flow between organs represents anadditional mechanism by which to opti-mize DO2. Less vital organs (such as themesentery and dermis) and organs withconsiderable flow reserve (such as the kid-neys) experience an increase in vascularresistance and therefore a reduction in per-fusion. Vital organs such as the brain, myo-cardium, and diaphragm do not experiencean increase in vascular resistance and per-fusion is maintained. This represents animportant compensatory mechanism, be-cause these vital organs have high restingoxygen extraction, necessitating a relatively
large percentage of CO under normal con-ditions, and an increase in flow as oxygenrequirements increase.
Finally, although there may be altera-tions in vascular resistance that reduceblood flow, all organs are capable of mi-crocirculatory adjustments that lead tovascular recruitment and a compensatoryincrease in oxygen extraction. The localaccumulation of adenosine, a byproductof adenosine-5�-triphosphate utilization,and a decrease in tissue oxygen tension,for example, have been shown to mediatethese changes. Vascular recruitment in-creases capillary density. As a result, thediffusion distance for oxygen decreasesand the capillary surface area available forgas exchange increases. In addition, thecross-sectional area of the individual ves-sel and of the vascular bed increases; be-cause the linear velocity of blood is in-versely related to the cross-sectional area,red blood cell velocity decreases and itstransit time increases, increasing oxygendiffusion times and oxygen extraction.
Regional Oxygen TransportBalance
An understanding of regional oxygentransport balance enables the clinician toaccurately interpret venous oximetryfrom different sites under normal condi-tions and in limited CO states. Cerebralblood flow is tightly coupled to cerebralmetabolism providing a fairly constantcerebral OER (20). The exception to thisoccurs when cerebral blood flow is lim-ited, in which case the cerebral OER in-creases, and when changes in the PaCO2
occur. Irrespective of cerebral metabolicdemands and systemic hemodynamics, ce-rebral blood flow changes in parallel withPaCO2. The normal cerebral OER is 35%(jugular bulb) and the critical cerebralOER (corresponding to the onset of neu-rologic deficits and a rise in brain lactatelevels) is similar to the global criticalOER at approximately 50% (21). How-ever, as CO becomes limited, the globalOER increases first and to a greater ex-tent than does the cerebral OER.
Total blood flow to the gastrointesti-nal system is approximately 20% to 25%of CO in the unfed sate and may increaseby as much as 200% above baseline levelswith ingestion of nutrients (22). The nor-mal splanchnic OER is approximately25% to 35% and the critical OER is sim-ilar to the global critical OER at roughly50% to 60% (23). However, as CO falls,the splanchnic OER increases first and
becomes critical sooner than does theglobal OER (23).
The kidneys are second only to the heartin terms of VO2. The vast majority of renalVO2 occurs with the active resorption offiltrate and because renal sodium transportis coupled to renal blood flow, changes inrenal VO2 are met by correspondingchanges in renal oxygen delivery. This phe-nomenon coupled with the fact that thekidneys receive a very high blood flow (ap-proximately 20% of CO) produces a verylow OER of approximately 10% to 15%(24). As a result, the renal OER increasesappreciably only with significant decreasesin renal DO2 (25).
These differences in regional oxygentransport balance are responsible for theranges of venous oximetry obtained fromdifferent sites under normal conditions andin low CO states. Under normal conditions,venous saturations range from 80% to 85%in the inferior vena cava (IVC), 70% to 75%in the superior vena cava (SVC), 65% to70% in the jugular vein, and a normalSmvO2 is 75% (26). As CO decreases, IVCsaturations fall first, which is accompaniedby a less severe drop in SmvO2. As CO fallsfurther, SVC and jugular saturations beginto decrease (27, 28).
Advantages and Limitations ofVenous Oximetry
It is not until the critical OER isreached and the production of lactate ex-ceeds its clearance that the serum lactatelevel begins to rise (Table 2B). Therefore,venous oximetry is more sensitive at de-tecting impaired oxygen transport bal-ance and impending tissue hypoxia thanan elevated serum lactate level. Oxygendemand is an important determinant ofoxygen transport balance; however, it isimpractical to measure and it varies con-siderably between and within diseasestates (Table 4). Thus, a determination ofCO and DO2 does not provide an indica-tion of whether they are adequate to meetmetabolic demand. Venous oximetry as-sesses oxygen transport balance and theadequacy of DO2. Similarly, changes inoxygen extraction do not necessarily re-flect changes in CO and DO2 because ox-ygen demand may vary over time.
The relationship between CO and ve-nous oxygen saturations is curvilinear(Fig. 2). Thus, for a given VO2, venousoximetry is relatively insensitive at de-tecting changes in CO as it falls fromnormal values. It is when CO becomeslow that further decreases produce a
Table 3. Compensatory circulatory responses tochanges in O2 transport balance
Increased metabolismVO21 3 CO/DO21 3 OER normalVO211 3 CO/DO211, � OER13 O2
demands metHypoxic or anemic hypoxia
CaO2 23 CO13 DO2 maintained, OERnormal
CaO2 223 CO11, DO21 � OER13 O2
demands metStagnant hypoxia
CO2 3 OER13 O2 demands metCO223 OER113 VO2 falls
Histotoxic hypoxiaVO223 CO/DO213 OER22, lactic acidosis
OER, oxygen extraction ratio; VO2, oxygenconsumption; CO, cardiac output; CaO2, arterialoxygen content; DO2, oxygen delivery.
Table 4. Factors responsible for increasing O2
requirements
Catecholamines, endogenous and exogenousSystemic inflammatory responseFeverConsciousness, pain and anxietySpontaneous respirationEnteral nutrition
S23Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

large increase in oxygen extraction. Sys-temic hemodynamic parameters (e.g.,CO) and global indicators of oxygentransport balance, such as SmvO2 and se-rum lactate levels, do not necessarily re-flect the adequacy of regional tissue oxy-genation. This is exemplified in thecomparison of systemic and splanchnicindicators of oxygen transport balance inlow CO states, as discussed previously(29, 30).
Central Venous Oximetry
Mixed venous oximetry is often notavailable. Placement of a pulmonary ar-terial catheter is difficult in neonates andinfants. Pulmonary artery saturations arerendered useless in the presence of left-to-right cardiac shunting. Alternativesites for monitoring venous oxygen satu-rations include the right atrium (RA), solong as there is no left-to-right atrialshunt, IVC–RA junction, and the SVC.Right atrial saturations are close to andtrack changes in SmVO2; however, theymay vary some from SmvO2 if inadequatemixing occurs (10, 28, 31, 32). IVC satu-rations should be obtained from theIVC–RA junction to optimize mixing ofvenous return from abdominal viscera. Inaddition to giving consideration to wherethe samples are obtained from, centralvenous saturations should be interpretedin their clinical context, because thesevalues vary considerably from site to siteunder normal conditions and as CO andregional oxygen transport balance are al-tered, as described previously.
Clinical Studies
Venous oximetry has been studied ex-tensively in severe sepsis and septic shockwith the seminal study published by Riv-ers and colleagues in 2001 (3). On pre-sentation to the emergency department,adults with severe sepsis and septic shockwere eligible for enrollment if their sys-tolic blood pressure was �90 mm Hgdespite 20–30 mL/kg of fluid or if theirserum lactate level was �4 mmol/L (n �263). Patients were randomized to re-ceive either 6 hrs of standard therapy(interventions based on central venouspressure, blood pressure, and urine out-put) or “early goal-directed therapy”(EGDT), which included the targeting ofa “central venous oxygen saturation”(ScvO2; SVC saturations) of �70%. Thegroup randomized to EGDT had signifi-cantly less severe organ dysfunction and
improved survival with an inhospitalmortality of 30.5% (vs. 46.5%, p � .009)and 28-day mortality of 33.3% (vs. 49.2%,p � .01).
The author concluded that the signif-icant impact on morbidity and mortalityin the EGDT group was the result of anearly and accurate diagnosis of the sever-ity of illness and the implementation of atimely and aggressive resuscitation. Thisapproach has been shown to improve out-comes in other critical illness, includingtrauma, acute myocardial infarction, andischemic stroke (33–35). At the core ofthis approach is an appreciation of thefact that estimations of CO and tissueoxygenation based on the physical exam-ination and standard clinical parameters(e.g., central venous pressure, blood pres-sure, and urine output) are often discor-dant from measured values, whereas tar-geting a parameter such as SvO2
represents a more definitive resuscitationstrategy (1–3). These notions are sup-ported by the fact that during the initial 6hrs of therapy, the ScvO2 was significantlyhigher and a ScvO2 of �70% was achievedin significantly more patients in theEGDT group than in the standard prac-tice group, and those receiving EGDT re-ceived significantly more fluid, red bloodcell transfusions, and inotropic support.Furthermore, although the EGDT grouphad a significantly higher mean bloodpressure during the initial 6 hrs, all pa-tients in both groups reached the goalmean blood pressure and there was nodifference between groups for heart rateor central venous pressure.
Several studies since the original reportby Rivers and colleagues have evaluated theimpact of EGDT on outcomes in adultswith severe sepsis and septic shock. Thesestudies differed in that they relied on his-torical controls and their protocols werenot limited to optimizing hemodynamicsbut included additional therapies such asantibiotics, which were bundled into theresuscitation protocols (36). Eight single-center studies (37–43) and one nationalstudy (44) demonstrated a significant re-duction in mortality following implemen-tation of EGDT, whereas two inadequatelypowered studies did not demonstrate im-proved outcomes (45, 46). In the study byCastellanos-Ortega and colleagues, the onlysingle intervention with impact on mortal-ity was the achievement of a ScvO2 of�70% (43). A study by Rivers et al (47) alsofound the ScvO2 component of the bundleto have the greatest impact on survival ofany bundle element.
A study similar to that conducted byRivers and colleagues was carried out byde Oliveira and colleagues in childrenwith severe sepsis (48). Patients were re-cruited from the emergency department,inpatient unit, and pediatric intensivecare unit (n � 102). Eligibility criteriawere severe sepsis or fluid-refractoryshock despite 40 mL/kg of fluid. Severesepsis was defined as evidence of infectionand sepsis inflammatory response syn-drome criteria and at least one of thefollowing: altered mental status, hypox-emia, increased serum lactate level, oli-guria, or hypotension. The duration ofthe resuscitation protocols was 72 hrsand the intervention group targeted aSvO2 of �70%, which was obtained fromthe RA, or SVC–RA, or IVC–RA junction.Those patients randomized to the SvO2
group had significantly less mortality at28 days (11.8 vs. 39.2%, p � .002) andless organ dysfunction than the grouptargeting standard hemodynamic param-eters alone. As was the case in the studyby Rivers and colleagues, during the ini-tial 6 hrs, the group targeting SvO2 re-ceived significantly more fluid, red bloodcell transfusions, and vasoactive supportand were much more likely to reach aSvO2 �70% (37.9 vs. 12.5%, p � .02).Furthermore, there was no difference inheart rate, mean blood pressure, or cen-tral venous pressure between groups.
Venous oximetry has not been studiedextensively in cardiac surgical patients. Aprospective randomized study was con-ducted by Polonen and colleagues (49) of403 adult patients undergoing cardiacsurgery. The protocol-driven group thattargeted a SmvO2 of �70% had signifi-cantly reduced hospital length of stay andless postoperative organ dysfunction thanthe control group. Two additional smallprospective randomized studies in adultsundergoing cardiac surgery found a de-crease in length of stay in their respectivegroups that targeted SvO2 (50, 51).
Data supporting the use of venous oxi-metry in pediatric cardiac patients is alsolimited. Tweddell and colleagues (52)performed a retrospective analysis of out-comes for 115 consecutive patients un-dergoing the Norwood procedure. From1992 to 1996, the survival rate for theNorwood procedure at their institutionwas 53%. Commensurate with the imple-mentation of new treatment strategies in1996, the survival rate increased to 93%from 1996 to 2001. Multivariate analysisidentified continuous SsvcO2 monitoring
S24 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

as a significant factor responsible for im-proved survival.
In addition to the prospective random-ized studies in severe sepsis conducted byRivers and colleagues and by de Oliveiraand colleagues, a study by Donati andassociates (53) randomized adult patients(n � 135) undergoing major abdominalsurgery to receive either goal-directedtherapy, which targeted ScvO2 duringsurgery up until postoperative day 1, orstandard care. Although patients in bothgroup received similar amounts of fluidand packed red blood cells during thestudy, those in the goal-directed groupreceived a greater amount of each duringsurgery as well as significantly more ino-tropic support during and after surgery.The goal-directed group had significantlyhigher ScvO2 and lower serum lactate lev-els at the conclusion of surgery and de-veloped significantly less organ failureand had a greater reduction in hospitallength of stay.
Conclusion
One of the tenets of critical care med-icine is to provide a timely and accurateassessment of tissue oxygenation. In con-junction with other monitoring modali-ties, the routine deployment of centralvenous catheters readily enables the cli-nician to complete this task.
Classification ofrecommendations and level ofevidence
Class I and level of evidence: B. ScvO2
should be monitored in critically ill pedi-atric patients and a ScvO2 of �70%should be targeted. In patients with arte-rial hypoxemia, a normal oxygen extrac-tion ratio should be targeted.
REFERENCES
1. Tibby SM, Hetherill M, Marsh MJ, et al: Cli-nicians’ abilities to estimate cardiac index inventilated children and infants. Arch DisChild 1997; 77:516–518
2. Connors AF, McCaffree DR, Gray BA: Evalu-ation of right heart catheterization in thecritically ill patient without acute myocardialinfarction. N Engl J Med 1983; 308:263–267
3. Rivers E, Nguyen B, Havstad S, et al: Earlygoal-directed therapy in the treatment of se-vere sepsis and septic shock. N Engl J Med2001; 345:1368–1377
4. Cain SM: Oxygen delivery and uptake in dogsduring anemic and hypoxic hypoxia. J ApplPhysiol 1977; 42:228–234
5. Dantzker DR, Foresman B, Gutierrez G: Ox-
ygen supply and utilization relationships. AmRev Respir Dis 1991; 143:675–679
6. Baigorri F, Russell JA: Oxygen delivery incritical illness. Crit Care Clin 1996; 12:971–994
7. Ermakov S, Hoyt JW: Pulmonary artery cath-eterization. Crit Care Clin 1992; 8:773–806
8. Ronco JJ, Phang T, Walley KR, et al: Oxygenconsumption is independent of changes inoxygen delivery in severe adult respiratorydistress syndrome. Am Rev Respir Dis 1991;143:1267–1273
9. Woodson RD, Wills RE, Lenfant C: Effect ofacute and established anemia on O2 trans-port at rest, submaximal and maximal work.J Appl Physiol 1978; 44:36–43
10. Van Der Linden P, Gilbart E, Paques P, et al:Influence of hematocrit on tissue O2 extrac-tion capabilities during acute hemorrhage.Am J Physiol 1993; 264:H1942–H1947
11. Vincent J-L: Determination of oxygen deliv-ery and consumption versus cardiac indexand oxygen extraction ratio. Crit Care Clin1996; 12:995–1006
12. Phang PT, Cunningham KF, Ronco JJ, et al:Mathematical coupling explains dependenceof oxygen consumption on oxygen delivery inARDS. Am J Respir Crit Care Med 1994;150:318–323
13. Ronco JJ, Fenwick JC, Tweeddale MG, et al:Identification of the critical oxygen deliveryfor anaerobic metabolism in critically ill sep-tic and nonseptic humans. JAMA 1993; 270:1724–1730
14. Wysocki M, Besbes M, Roupie E, et al: Mod-ification of oxygen extraction ratio by changein oxygen transport in septic shock. Chest1992; 102:221–226
15. Annat G, Viale J-P, Percival C, et al: Oxygendelivery and uptake in the adult respiratorydistress syndrome. Am Rev Respir Dis 1986;133:999–1001
16. Ronco JJ, Fenwick JC, Wiggs BR, et al: Oxy-gen consumption is independent of increasesin oxygen delivery by dobutamine in septicpatients who have normal or increasedplasma lactate. Am Rev Respir Dis 1993; 147:25–31
17. Levraut J, Ciebiera J-P, Chave S, et al: Mildhyperlactatemia in stable septic patients isdue to impaired lactate clearance rather thanoverproduction. Am J Respir Crit Care Med1998; 157:1021–1026
18. Schumaker PT, Long RG, Wood LDH: Tissueoxygen extraction during hypovolemia: Roleof hemoglobin P50. J Appl Physiol 1987; 62:1801–1807
19. Curtis SE, Walker TA, Bradley WE, et al:Raising P50 increases tissue PO2 in canineskeletal muscle but does not affect critical O2
extraction ratio. J Appl Physiol 1997; 83:1681–1689
20. Feldman Z, Robertson CS: Monitoring of ce-rebral hemodynamics with jugular bulbcatheters. Crit Care Clin 1997; 13:51–77
21. Schnell RM, Cole DJ: Cerebral monitoring:jugular venous oximetry. Anesth Analg 2000;90:599–566
22. Matheson PJ, Wilson MA, Garrison RN, et al:Regulation of intestinal blood flow. J SurgRes 2000; 93:182–196
23. Nelson DP, King CE, Dodd SL, et al: Sys-temic and intestinal limits of O2 extraction inthe dog. J Appl Physiol 1987; 63:387–394
24. O’Connor PM: Renal oxygen delivery: Match-ing delivery to metabolic demand. Clin ExpPharmacol Physiol 2006; 33:961–967
25. Ciocca RG, Wilkerson DK, Conway RS, et al:Increased oxygen extraction as adaptation toacute renal ischemia. J Invest Surg 1994;519–526
26. Barratt-Boyes BG, Wood EH: The oxygen sat-uration of blood in the venae cavae, right-heart chambers, and pulmonary vessels ofhealthy subjects. J Lab Clin Med 1957; 50:93–106
27. Scheinman MM, Brown MA, Rapaport E:Critical assessment of use of central venousoxygen saturation as mirror of mixed venousoxygen in severely ill cardiac patients. Circu-lation 1969; XL:165–172
28. Lee J, Wright F, Barber R, et al: Centralvenous oxygen saturation in shock: A studyin man. Anesthesiology 1972; 36:472–478
29. Dahn MS, Lange MP, Jacobs LA, et al: Centralmixed and splanchnic venous oxygen satura-tion monitoring. Intensive Care Med 1988;14:373–378
30. Landow L, Phillips DA, Heard SO, et al: Gas-tric tonometry and venous oximetry in car-diac surgery patients. Crit Care Med 1991;19:1226–1233
31. Davies GG, Mendenhall J, Symreng T: Mea-surements of right atrial oxygen saturationby fiberoptic oximetry accurately reflectsmixed venous oxygen saturation in swine.J Clin Monit 1988; 4:99–102
32. Perez AC, Eulmesekian PG, Minces PG, et al:Adequate agreement between venous oxygensaturation in right atrium and pulmonaryartery in critically ill children. Pediatr CritCare Med 2009; 10:76–79
33. Mullins RJ, Mann NC: Population-based re-search assessing the effectiveness of traumasystems. J Trauma 1999; 47:S59–S66
34. Hollenberg SM: Top ten list in myocardialinfarction. Chest 2000; 118:1477–1479
35. Adams HP, del Zoppo G, Alberts MJ, et al:Guidelines for the early management ofadults with ischemic stroke. Circulation2007; 115:478–534
36. Levy MM, Dellinger RP, Townsend SR, et al:The surviving sepsis campaign: Results of aninternational guideline-based performanceimprovement program targeting severe sep-sis. Crit Care Med 2010; 38:367–374
37. Micek ST, Roubinian N, Heuring T, et al:Before–after study of a standardized hospitalorder set for the management of septicshock. Crit Care Med 2006; 34:2707–2713
38. Jones AE, Focht A, Horton JM, et al: Prospec-tive external validation of the clinical effec-tiveness of an emergency department-basedearly goal-directed therapy protocol for se-vere sepsis and septic shock. Chest 2007;132:425–432
S25Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

39. Nguyen HB, Corbett SW, Steele R, et al:Implementation of a bundle of quality indi-cators for the early management of severesepsis and septic shock is associated withdecreased mortality. Crit Care Med 2007; 35:1105–1112
40. Kortgen A, Niederprum P, Bauer M: Imple-mentation of an evidence-based ‘standard op-erating procedure’ and outcome in septicshock. Crit Care Med 2006; 34:943–949
41. El Solh AA, Akinnusi ME, Alsawalha LN, et al:Outcome of septic shock in older adults afterimplementation of the sepsis ‘bundle.’ J AmGeriatr Soc 2008; 56:272–278
42. Sebat F, Musthafa AA, Johnson D, et al: Effectof a rapid response system for patients inshock on time to treatment and mortalityduring 5 years. Crit Care Med 2007; 35:2568–2575
43. Castellanos-Ortega A, Suberviola B, Garcia-Astudillo LA, et al: Impact of the survivingsepsis campaign protocols on hospital lengthof stay and mortality in septic shock patients:Results of a three-year follow-up quasi-experimental study. Crit Care Med 2010; 38:1036–1043
44. Ferrer R, Artigas A, Levy MM, et al: Improve-ment in process of care and outcome after amulticenter severe sepsis educational pro-gram in Spain. JAMA 2008; 299:2294–2303
45. Trzeciak S, Dellinger RP, Abate NL, et al:Translating research to clinical practice. A1-year experience with implementing earlygoal-directed therapy for septic shock in theemergency department. Chest 2006; 129:225–232
46. Shapiro NI, Howell MD, Talmor D, et al:Implementation and outcomes of the multi-ple urgent sepsis therapies protocol. CritCare Med 2006; 34:1025–1032
47. Rivers EP, Coba V, Whitmall M: Early goal-directed therapy in severe sepsis and septicshock: A contemporary review of the litera-ture. Curr Opin Anesthesiol 2008; 21:128–140
48. de Oliveira CF, de Oliveira DSF, GottschaldAFC, et al: ACCM/PALS haemodynamic sup-port guideline for paediatric septic shock: Anoutcomes comparison with and withoutmonitoring central venous oxygen satura-tion. Intensive Care Med 2008; 34:1065–1075
49. Polonen P, Ruokonen E, Hippelainen M, et
al: A prospective, randomized study of goal-oriented hemodynamic therapy in cardiacsurgical patients. Anesth Analg 2000; 90:1052–1059
50. Smetkin AA, Kirov MY, Kuzkov VV, et al:Single transpulmonary thermodilution andcontinuous monitoring of central venous ox-ygen saturation during off-pump coronarysurgery. Acta Anaesthesiol Scand 2009; 53:505–514
51. Kapoor PM, Kakani M, Chowdhury U, et al:Early goal-directed therapy in moderate tohigh-risk cardiac surgery patients. Ann Car-diac Anaesth 2008; 11:27–34
52. Tweddell JS, Hoffman GM, Mussatto KA, etal: Improved survival of patients undergoingpalliation of hypoplastic left heart syndrome:lessons learned from 115 consecutive pa-tients. Circulation 2002; 106(Suppl I):I-82–I-89
53. Donati A, Loggi S, Preiser J-C, et al: Goal-directed intraoperative therapy reducesmorbidity and length of hospital stay inhigh-risk surgical patients. Chest 2007;132:1817–1824
S26 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Near-infrared spectroscopy as a hemodynamic monitor in criticalillness
Nancy S. Ghanayem, MD; Gil Wernovsky, MD; George M. Hoffman, MD
Conventional hemodynamicmonitoring (typically measuredcontinuously such as bloodpressure or heart rate) and lab-
oratory evidence of anaerobic metabolismor organ dysfunction (typically measuredintermittently such as acid-base status orserum lactate levels) are often relatively lateindicators of shock, resulting in delayedrecognition of serious illness and poten-tially suboptimal outcomes (1–12). A con-tinuous, noninvasive indicator of thechanges in regional circulation that occur
early in developing shock states would fill agap in standard evaluation and treatment ofthese circulatory abnormalities (13–16). Inpatients with the potential for (or with es-tablished) shock and critical illness, the ad-dition of near-infrared spectroscopy (NIRS)monitoring to traditional hemodynamicand electrophysiological monitoring helpscharacterize regional and global circulatoryfunction with growing evidence for im-proved outcomes.
NIRS technology
Near-infrared spectroscopy uses a mod-ified Beer-Lambert law for measurement ofconcentration of a substance according tothe absorption and scatter of light. Currentclinically useful NIRS devices provide anoninvasive assessment of tissue oxygen-ation through quantitative assessment ofthe color of hemoglobin in blood. Unlikepulse oximetry, NIRS devices do not lookfor an arterial pulsatile signal, but for theaverage or nonpulsatile optical component,which is highly related to capillary–venoushemoglobin saturation (rSO2). An opticalwindow of 700–900 nm allows light to pass
through skin or bone into underlying tis-sue; the differential absorption of at leasttwo light wavelengths of light, and a dual-detector system that can reduce by subtrac-tion the effects of shallow signals, allows aNIRS device to continuously and noninva-sively estimate the hemoglobin–oxygensaturation within tissues deep to the sen-sor. The depth of the optical field is approx-imately half the source-detector distance,which is 4 cm in the most widely useddevice (Invos; Somanetics Inc, Troy, MI).This source-detector distance and the sub-traction algorithm allow the device to esti-mate rSO2 in a tissue sample approximately1 cm3 centimeter in volume and approxi-mately 2–3 cm beneath the sensor. Thisvenous-weighted measurement provides anestimation of the regional oxygen supply–demand relationship. Continuous, real-time changes in rSO2 reflect changes eitherin metabolic demand or in supply in thesampled region, a function of systemic car-diac output, arterial oxygen content, andtotal and regional resistance.
Near-infrared spectroscopy has beenextensively studied in animal and human
From the Division Critical Care in Department ofPediatrics (NSG, GMH) and the Department of Anes-thesiology (GMH), Medical College of Wisconsin, Chil-dren’s Hospital of Wisconsin, Milwaukee, WI; and theDivision of Pediatric Cardiology (GW), The Children’sHospital of Philadelphia, University of PennsylvaniaSchool of Medicine, Philadelphia, PA.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e318221173a
Background: Near-infrared spectroscopy has moved from aresearch tool to a widely used clinical monitor in the critically illpediatric patient over the last decade. The physiological andclinical evidence supporting this technology in practice is re-viewed here.
Methodology: A search of MEDLINE and PubMed was con-ducted to find validation studies, controlled trials, and otherreports of near-infrared spectroscopy use in children and adultsin the clinical setting. Guidelines published by the American HeartAssociation, the American Academy of Pediatrics, and the Inter-national Liaison Committee on Resuscitation were reviewed in-cluding further review of references cited.
Results: The biophysical properties of near-infrared spectros-copy devices allow measurement of capillary–venous oxyhemo-globin saturation in tissues a few centimeters beneath the surfacesensor with validated accuracy in neonates, infants, and smallpatients. The biologic basis for the relationship of capillary–venous oxyhemoglobin saturation to cerebral injury has beendescribed in animal and human studies. Normal ranges for cere-bral and somatic capillary–venous oxyhemoglobin saturation
have been described for normal newborns and infants and chil-dren with congenital heart disease and other disease states. Thecapillary–venous oxyhemoglobin saturation from both cerebraland somatic regions has been used to estimate mixed venoussaturation and to predict biochemical shock, multiorgan dysfunc-tion, and mortality in different populations. The relationship ofcerebral capillary–venous oxyhemoglobin saturation to neuroim-aging and functional assessment of outcome is limited but ongo-ing. Although there are numerous conflicting reports in smallpopulations, expert opinion would suggest that special use mayexist for near-infrared spectroscopy in patients with complexcirculatory anatomy, with extremes of physiology, and in whomextended noninvasive monitoring is useful.
Conclusions: Class II, level B evidence supports the conclusionthat near-infrared spectroscopy offers a favorable risk–benefitprofile and can be effective and beneficial as a hemodynamicmonitor for the care of critically patients. (Pediatr Crit Care Med2011; 12[Suppl.]:S27–S32)
KEY WORDS: NIRS; spectroscopy; hemodynamic monitoring; he-moglobin saturation; electrophysiologic monitoring
S27Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
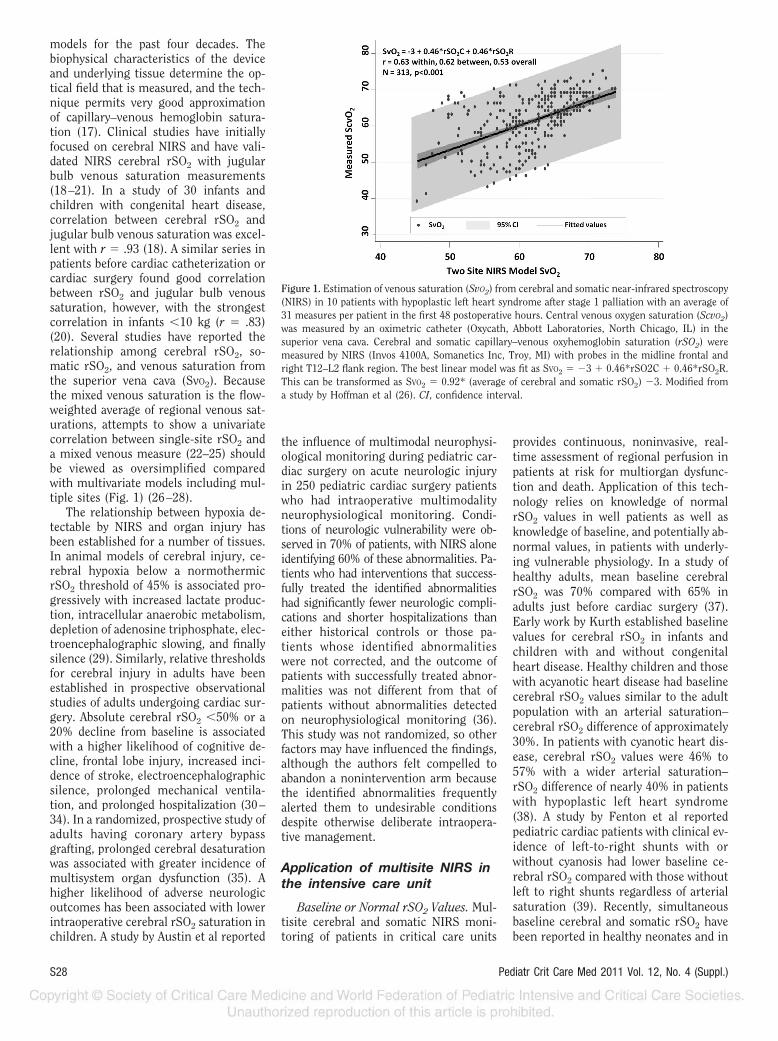
models for the past four decades. Thebiophysical characteristics of the deviceand underlying tissue determine the op-tical field that is measured, and the tech-nique permits very good approximationof capillary–venous hemoglobin satura-tion (17). Clinical studies have initiallyfocused on cerebral NIRS and have vali-dated NIRS cerebral rSO2 with jugularbulb venous saturation measurements(18–21). In a study of 30 infants andchildren with congenital heart disease,correlation between cerebral rSO2 andjugular bulb venous saturation was excel-lent with r � .93 (18). A similar series inpatients before cardiac catheterization orcardiac surgery found good correlationbetween rSO2 and jugular bulb venoussaturation, however, with the strongestcorrelation in infants �10 kg (r � .83)(20). Several studies have reported therelationship among cerebral rSO2, so-matic rSO2, and venous saturation fromthe superior vena cava (SvO2). Becausethe mixed venous saturation is the flow-weighted average of regional venous sat-urations, attempts to show a univariatecorrelation between single-site rSO2 anda mixed venous measure (22–25) shouldbe viewed as oversimplified comparedwith multivariate models including mul-tiple sites (Fig. 1) (26–28).
The relationship between hypoxia de-tectable by NIRS and organ injury hasbeen established for a number of tissues.In animal models of cerebral injury, ce-rebral hypoxia below a normothermicrSO2 threshold of 45% is associated pro-gressively with increased lactate produc-tion, intracellular anaerobic metabolism,depletion of adenosine triphosphate, elec-troencephalographic slowing, and finallysilence (29). Similarly, relative thresholdsfor cerebral injury in adults have beenestablished in prospective observationalstudies of adults undergoing cardiac sur-gery. Absolute cerebral rSO2 �50% or a20% decline from baseline is associatedwith a higher likelihood of cognitive de-cline, frontal lobe injury, increased inci-dence of stroke, electroencephalographicsilence, prolonged mechanical ventila-tion, and prolonged hospitalization (30–34). In a randomized, prospective study ofadults having coronary artery bypassgrafting, prolonged cerebral desaturationwas associated with greater incidence ofmultisystem organ dysfunction (35). Ahigher likelihood of adverse neurologicoutcomes has been associated with lowerintraoperative cerebral rSO2 saturation inchildren. A study by Austin et al reported
the influence of multimodal neurophysi-ological monitoring during pediatric car-diac surgery on acute neurologic injuryin 250 pediatric cardiac surgery patientswho had intraoperative multimodalityneurophysiological monitoring. Condi-tions of neurologic vulnerability were ob-served in 70% of patients, with NIRS aloneidentifying 60% of these abnormalities. Pa-tients who had interventions that success-fully treated the identified abnormalitieshad significantly fewer neurologic compli-cations and shorter hospitalizations thaneither historical controls or those pa-tients whose identified abnormalitieswere not corrected, and the outcome ofpatients with successfully treated abnor-malities was not different from that ofpatients without abnormalities detectedon neurophysiological monitoring (36).This study was not randomized, so otherfactors may have influenced the findings,although the authors felt compelled toabandon a nonintervention arm becausethe identified abnormalities frequentlyalerted them to undesirable conditionsdespite otherwise deliberate intraopera-tive management.
Application of multisite NIRS inthe intensive care unit
Baseline or Normal rSO2 Values. Mul-tisite cerebral and somatic NIRS moni-toring of patients in critical care units
provides continuous, noninvasive, real-time assessment of regional perfusion inpatients at risk for multiorgan dysfunc-tion and death. Application of this tech-nology relies on knowledge of normalrSO2 values in well patients as well asknowledge of baseline, and potentially ab-normal values, in patients with underly-ing vulnerable physiology. In a study ofhealthy adults, mean baseline cerebralrSO2 was 70% compared with 65% inadults just before cardiac surgery (37).Early work by Kurth established baselinevalues for cerebral rSO2 in infants andchildren with and without congenitalheart disease. Healthy children and thosewith acyanotic heart disease had baselinecerebral rSO2 values similar to the adultpopulation with an arterial saturation–cerebral rSO2 difference of approximately30%. In patients with cyanotic heart dis-ease, cerebral rSO2 values were 46% to57% with a wider arterial saturation–rSO2 difference of nearly 40% in patientswith hypoplastic left heart syndrome(38). A study by Fenton et al reportedpediatric cardiac patients with clinical ev-idence of left-to-right shunts with orwithout cyanosis had lower baseline ce-rebral rSO2 compared with those withoutleft to right shunts regardless of arterialsaturation (39). Recently, simultaneousbaseline cerebral and somatic rSO2 havebeen reported in healthy neonates and in
Figure 1. Estimation of venous saturation (SvO2) from cerebral and somatic near-infrared spectroscopy(NIRS) in 10 patients with hypoplastic left heart syndrome after stage 1 palliation with an average of31 measures per patient in the first 48 postoperative hours. Central venous oxygen saturation (ScvO2)was measured by an oximetric catheter (Oxycath, Abbott Laboratories, North Chicago, IL) in thesuperior vena cava. Cerebral and somatic capillary–venous oxyhemoglobin saturation (rSO2) weremeasured by NIRS (Invos 4100A, Somanetics Inc, Troy, MI) with probes in the midline frontal andright T12–L2 flank region. The best linear model was fit as SVO2 � �3 � 0.46*rSO2C � 0.46*rSO2R.This can be transformed as SVO2 � 0.92* (average of cerebral and somatic rSO2) �3. Modified froma study by Hoffman et al (26). CI, confidence interval.
S28 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

neonates before stage 1 palliation for hy-poplastic left heart syndrome. A study byBernal et al reported resting and post-prandial cerebral and somatic rSO2 val-ues in healthy neonates with normal ar-terial saturation. The at-rest averagecerebral rSO2 was 78% with a somaticrSO2 of 88% demonstrating higher oxy-gen extraction across the cerebral bedcompared with the somatic bed. Changesin cerebral and somatic tissue oxygen-ation during feeding in healthy neonateswas not significant as would be expectedwith good physiological reserve (40). In aseries of 45 neonates with hypoplastic leftheart syndrome before stage 1 palliation,mean arterial saturation was 92% withmean cerebral rSO2 of 68% and mean so-matic rSO2 of 70% demonstrating similarextraction across somatic and cerebral vas-cular beds as would be expected with rela-tively limited systemic perfusion (41).
Critical illness in patients withstructural heart disease
Use of NIRS for monitoring and man-agement of critical illness in intensivecare units has predominated in infantsand children. Several prospective obser-vational studies of infants and childrenwith congenital heart disease requiringsurgery have evaluated the relationship ofmultisite NIRS and SvO2 or indicators ofanaerobic metabolism (Fig. 1) (26–28,42–44). In a series of 20 infants and chil-dren, dorsal lateral flank and anterior ab-dominal rSO2 exhibited a strong correla-tion with SvO2 and lactate within 48 hrsof surgery (23). In a similar study of 23infants, cerebral, splanchnic, renal, andmuscle rSO2 values were recorded every30 secs and correlated to lactate measure-ments during the first 24 hrs after sur-gery. rSO2 from each site was associatedwith elevated lactate with the strongestinverse relationship between cerebralrSO2 and lactate. In this series, averagedtwo-site (cerebral and renal) rSO2 �65%in acyanotic children predicted serumlactate �3 mmol/L with 95% sensitivityand 83% specificity (44). In a series of 30neonates with hypoplastic left heart syn-drome, 48 hrs of postoperative physiolog-ical data including cerebral and somaticrSO2 were used to detect the distributionof systemic perfusion during periods oflow cardiac output defined by low SvO2
and metabolic acidosis. Actual cerebraland somatic rSO2 were loosely relatedwith SvO2 but more closely related whenconsidering both rSO2 in a multilinear
relationship. A somatic rSO2– cerebralrSO2 difference of �10, indicating redis-tribution of perfusion away from somaticregions, predicted anaerobic metabolism(42). In a series of 79 patients who un-derwent stage 1 palliation, somatic rSO2
�60%, and an progressive somatic isch-emia indicated by a somatic– cerebralrSO2 difference approaching zero pre-dicted biochemical shock, complications,and longer intensive care unit length ofstay (Fig. 2) (43).
The relatively recent application ofNIRS monitoring precludes evaluation ofits predictive validity for important lon-ger-term outcomes, particularly for thecentral nervous system. There are in-creasing reports of a favorable associationof improved rSO2 values with improvedneurodevelopmental measurements ininfants and preschool-aged children;however, studies in this age group havevery limited correlation with importantneurodevelopmental outcomes in school-aged children and adolescents. Long-term functional outcome studies thatdemonstrate a relationship to any mea-sured physiological parameter, includingcerebral rSO2, arterial blood pressure, orarterial saturation, remain absent fromthe literature.
Few studies have correlated low rSO2
to magnetic resonance imaging abnor-malities and early childhood developmen-tal outcomes, and the results have beenequivocal. Specifically, in a prospectiveobservational assessment of infants withcongenital heart disease after cardiac sur-gery, Dent et al reported new or worsened
postoperative magnetic resonance imag-ing lesions in 73% study subjects, typi-cally abnormalities of the white matter.These new or worsened lesions were cor-related with a prolonged cerebral rSO2
decline (rSO2 �45% for �180 mins) (45).In a prospective series, Andropoulos andcolleagues reported results in a cohort ofneonates with complex congenital heartdisease (with either one or two ventricles)requiring surgery shortly after birth. Thepatients had intraoperative and postoper-ative cerebral NIRS monitoring and tar-geted interventions to maintain cerebralrSO2 �50%. The investigators found newpostoperative magnetic resonance imag-ing lesions in 36% of the cohort. In con-trast to the report by Dent et al, this studydid not identify an association betweennew magnetic resonance imaging find-ings and cerebral rSO2, although rSO2
was maintained �45% for 96% of themonitored period (46). Most recently, astudy by Kussman et al reported an in-traoperative prospective study of 104 in-fants who underwent biventricular repairwithout aortic arch obstruction with 1-yrdevelopment assessment and magneticresonance imaging. Lower PsychomotorDevelopment Index (Bayley Scale) scoreswere associated with lower rSO2 60 minsafter separation from cardiopulmonarybypass (Fig. 3). The study was limited tomeasuring values in the operating room,thus not measuring the continued vul-nerability of the central nervous systemin the intensive care unit (47).
In addition to identification of globaland organ-specific hypoxic–ischemic
Figure 2. Predicted probability of complications, biochemical shock, and mortality in 79 neonates withhypoplastic left heart syndrome. A somatic-cerebral capillary—venous oxyhemoglobin saturation(rSO2) difference �10 during first 48 postoperative hours after stage 1 palliation is associated with anincrease risk of biochemical shock and postoperative complications. A somatic–cerebral rSO2 differ-ence of zero or less is associated with an increased risk of mortality. Modified from a study by Hoffmanet al (43). CI, confidence interval.
S29Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

states, NIRS can be used to trend theseconditions noninvasively in less intenseenvironments or before invasive or labo-ratory measures can be obtained (41, 48,49). In conditions of limited global oxy-gen delivery, optimizing the distributionof cardiac output is a critical goal thatcan be achieved with the regional mea-sures provided by NIRS. For example,NIRS can guide changes in cerebral rSO2
and systemic perfusion with changes in thefraction of inspired oxygen and changes incarbon dioxide (50, 51). Consequently,changes in pulmonary and system flowscan be approximated by trending systemicand pulmonary arteriovenous differenceswith SvO2 or noninvasively with NIRS.The patient with a single ventricle in ashock or cardiac arrest state may partic-ularly benefit from information obtainedfrom NIRS (52, 53). In this subset ofpatients, optimization of the pulmonaryto systemic flow ratio (minimizing “steal”of systemic cardiac output into the pul-monary circulation) can be critical toavoid end-organ injury and treatment canbe guided more easily with the informa-tion derived from venous-side measuresprovided by NIRS monitoring.
Critical illness in patientswithout structural heart disease
Application of NIRS has expanded be-yond perioperative cardiac care to areasof neurovascular disease, plastic and vas-cular surgery, general surgery, emer-gency medicine, sports medicine, sleepdisorders, and neonatology. Many studiesin adults have used a superficial muscle
(thenar eminence) and a shallow-detect-ing NIRS measure (Inspectra; Hutchin-son Technology, Hutchinson, MN) inidentifying perfusion derangements in-curred from traumatic injury, sepsis, anddehydration. Low shallow-detecting NIRSmeasure in early traumatic injury hasbeen linked to increased risk of multior-gan dysfunction syndrome and mortality(54–57). Additionally, good correlationbetween acute blood loss and NIRS hasbeen reported (58, 59). In septic shock,low shallow-detecting NIRS measureidentifies patients at increased risk ofmortality (60, 61) and is significantly re-lated to anaerobic metabolism, venousoximetry, and reperfusion derangements(62–65).
Reports of NIRS effectiveness in de-tecting and managing perfusion abnor-malities in pediatric patients without car-diac disease are limited. Few studies haveevaluated regional perfusion during ap-neic or hypoxic events in preterm neo-nates. Fortune applied NIRS-derived ce-rebral and mesenteric rSO2 in 39neonates to evaluate the risk of develop-ing necrotizing enterocolitis. NIRS val-ues were expressed as absolute rSO2 foreach site and as a somatic/cerebral ratio.When the ratio was �0.75, indicating se-verely increased somatic oxygen extrac-tion, there was an eight times greater riskof developing necrotizing enterocolitiswith 90% sensitivity. The somatic/cerebral ratio was more predictive of ne-crotizing enterocolitis than the mesen-teric signal alone (66). In children withacute dehydration, a study by Hansonused cerebral and somatic (flank, renal,
or muscle rSO2) NIRS to assess changesin perfusion with rehydration. In chil-dren with moderate dehydration, cerebralrSO2 was preserved and unchanged withrehydration, whereas somatic rSO2 in-creased significantly from 79% to 87%(p � .001) with concomitant decrease insomatic regional oxygen extraction (19%to 11%, p � .001). Most significant ob-servations were seen in patients who were�15 kg and in patients who received ahigher volume of rehydration (49). Al-though increasingly used, no studieshave reported the effectiveness of NIRStechnology for triage or management ofpediatric patients with isolated sepsis orseptic shock syndrome.
Recommendations
Over the last decade, there have beenapproximately 400 reports from humanstudies (approximately 100 in children)that include use of NIRS; however, not allthese studies assess its effectiveness as ahemodynamic monitor. The most exten-sive reports in pediatrics investigate theuse of NIRS as a perioperative cerebralmonitor during cardiac surgery. A singlerandomized controlled study in adultsundergoing coronary artery bypass graft-ing has demonstrated improved outcomewith NIRS-driven intervention. Manyprospective observational studies, with asubset of randomized studies, validateNIRS rSO2 in relationship to venous oxi-metry and anaerobic metabolism withsome studies that link NIRS-derived rSO2
to intermediate patient outcomes,whereas others show little effect. There
Figure 3. Perioperative periods of diminished cerebral capillary–venous oxyhemoglobin saturation (rSO2) associated with neurologic findings in infantsundergoing reparative cardiac surgery. Lower cerebral rSO2 in the 60 mins after separation from cardiopulmonary bypass (CPB) is associated with thePsychomotor Development Index (Bayley Scale) at age 1 yr (A) and brain hemosiderin on magnetic resonance imaging (B). Modified with permission froma study by Kussman et al (47).
S30 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

are two principle questions that need tobe answered in the coming years as NIRSis adopted with increasing frequency ingeneral pediatric and cardiac intensivecare units. The first is the uncertaintyabout critical thresholds—both absolutevalues and duration—that should beavoided to minimize the risk of secondaryorgan dysfunction in a low-output/delivery state. The second is that futurestudies must be performed to assess thebenefit—and risk—of management strat-egies targeted to improve NIRS rSO2 val-ues. Management protocols that includetransfusions, increased sedation, andchanges in mechanical ventilation mustbe carefully designed to assess the rela-tive risks (short-term) of the treatmentstrategies to the potential benefits of im-proved long-term outcomes. We shouldcontinue to evaluate the relationship tooutcome of all monitoring modalities—NIRS, pulse oximetry, blood pressure,capnography—to use the technologiesonly where they add value, recognizingthe potential to harm by inappropriateintervention or nonintervention. Futurestudies might use both the pressure andoxygenation dimension to better charac-terize circulatory status and identify riskconditions.
The current evidence of NIRS moni-toring in human studies over the pastdecade is consistent with class II recom-mendations according to the AmericanHeart Association and the American Col-lege of Cardiology Task Force on PracticeGuidelines. The lack of randomized,blinded, interventional trials that studythe impact of NIRS as a hemodynamicmonitor along with some studies report-ing equivocal outcomes associated withNIRS classifies the evidence at level B.Specifically, NIRS appears to have a fa-vorable risk–benefit profile and can beeffective and beneficial as a hemodynamicmonitor for the care of critically patients.
REFERENCES
1. Shoemaker WC: Relationship of oxygentransport to the pathophysiology and therapyof shock states. Intensive Care Med 1987;13:230–243
2. Schlag G, Redl H, Hallstrom S: The cell inshock: The origin of multiple organ failure.Resuscitation 1991; 21:137–180
3. Proix F, Gauthoer M, Nadeau D, et al: Timingand predictors of death in pediatric patientswith multiple organ system failure. Crit CareMed 1994; 22:1025–1031
4. Hatherill M, Waggie Z, Purves L, et al: Mor-tality and the nature of metabolic acidosis in
children with shock. Intensive Care Med2003; 29:286–291
5. Tantalean J, Leon R, Santos A, et al: Multipleorgan dysfunction syndrome in children. Pe-diatr Crit Care Med 2003; 4:181–185
6. Rhodes A, Bennett ED: Earl goal-directedtherapy: An evidence-based review. Crit CareMed 2004; 32:S448–S450
7. Yu M, Burchell S, Hasaniya NW, et al: Rela-tionship of mortality to increasing oxygendelivery in patients � or �50 years of age: Aprospective, randomized trial. Crit Care Med1998; 26:1011–1019
8. Alia I, Esteban A, Gordo F, et al: A random-ized and controlled trial of the effect of treat-ment aimed at maximizing oxygen deliveryin patients with severe sepsis or septic shock.Chest 1999; 115:453–461
9. Rivers E, Nguyen B, Havstad S, et al: Earlygoal-directed therapy in the treatment of se-vere sepsis and septic shock. N Engl J Med2001; 345:1368–1377
10. Rivers EP, Ander DS, Powell D: Central ve-nous oxygen saturation monitoring in thecritically ill patient. Curr Opin Crit Care2001; 7:204–211
11. Han YY, Carcillo JA, Dragotta MA: Early re-versal of pediatric–neonatal septic shock bycommunity physicians associated with im-proved outcomes. Pediatrics 2003; 112:793–799
12. Tibby SM, Murdoch AJ: Monitoring cardiacfunction in intensive care. Arch Dis Child2003; 88:46–52
13. Haljamae H: Pathophysiology of shock. ActaAnaesthesiol Scand Suppl 1993; 98:3–6
14. Dyess DI, Powell RW, Swafford AN: Redistri-bution of organ flow after hemorrhage andresuscitation in full-term piglets. J PediatrSurg 1994; 29:1097–1102
15. Reilly PM, Wilkongs KB, Fuh KC, et al: Themesenteric hemodynamic response to circu-latory shock: An overview. Shock 2001; 15:329–343
16. Ceppa EP, Fuh KC, Bulkley G: Mesenterichemodynamic response to circulatory shock.Curr Opin Crit Care 2003; 9:127–132
17. Boushel R, Langberg H, Olesen J, et al: Mon-itoring tissue oxygen availability with nearinfrared spectroscopy (NIRS) in health anddisease. Scand J Med Sci Sports 2001; 11:213–222
18. Abdul-Khaliq H, Troitzsch D, Berger F, et al:Regional transcranial oximetry with near in-frared spectroscopy (NIRS) in comparisonwith measuring oxygen saturation in the jug-ular bulb in infants and children for moni-toring cerebral oxygenation [in German].Biomed Tech (Berl) 2000; 45:328–332
19. Watzman HM, Kurth DM, Montenegro LM,et al: Arterial and venous contributions tonear infrared cerebral oximetry. Anesthesiol-ogy 2000; 93:947–953
20. Nagdyman N, Fleck T, Schubert S, et al:Comparison between cerebral tissue oxygen-ation index by near-infrared spectroscopyand venous jugular bulb saturation in chil-dren. Intensive Care Med 2005; 31:846–850
21. Nagdyman N, Ewert P, Peters B, et al: Com-parison of different near-infrared spectro-scopic cerebral oxygenation indices with cen-tral venous and jugular venous oxygenationsaturation in children. Paediatr Anaesth2008; 18:160–166
22. Bhutta AT, Ford JW, Parker JG, et al: Non-invasive cerebral oximeter as a surrogate formixed venous saturation in children. PediatrCardiol 2007; 28:34–41
23. Kaufman J, Almodovar MC, Zuk J, et al: Cor-relation of abdominal site near-infrared spec-troscopy with gastric tonometry in infantsfollowing surgery for congenital heart dis-ease. Pediatr Crit Care Med 2008; 9:62–68
24. Ranucci M, Isgro G, De la Torre, et al: Near-infrared spectroscopy correlates with contin-uous superior vena cava oxygen saturation inpediatric cardiac surgery patients. PaedritrAnaesth 2008; 18:1163–1169
25. Tortoriello TA, Stayer SA, Mott AR, et al: Anoninvasive estimation of mixed venous ox-ygen saturation using near-infrared spectros-copy by cerebral oximetry in pediatric car-diac surgery patients. Paediatr Anaesth 2005;15:495–503
26. Hoffman GM, Ghanayem NS, Tweddell JS:Noninvasive assessment of cardiac output.Semin Thorac Cardiovasc Surg Pediatr CardSurg Annu 2005(8):12–21
27. Li J, Van Arsdell GS, Zhang G, et al: Assess-ment of the relationship between cerebraland splanchnic oxygen saturations measuredby near-infrared spectroscopy and directmeasurements of systemic haemodynamicvariables and oxygen transport after the Nor-wood procedure. Heart 2006; 92:1678–1685
28. McQuillen PS, Nishimoto MS, Bottrel CL, etal: Regional and central venous oxygen sat-uration monitoring following pediatric car-diac surgery: Concordance and associationwith clinical variables. Pediatr Crit Care Med2007; 8:156–160
29. Kurth CD, Levy WJ, McCann J: Near-infraredspectroscopy cerebral oxygen saturationthresholds for hypoxia-ischemia in piglets.J Cereb Blood Flow Metab 2002; 22:335–341
30. Levy WJ, Levin S, Chance B: Near-infraredmeasurement of cerebral oxygenation. Cor-relation with electroencephalographic isch-emia during ventricular fibrillation Anesthe-siology 1995; 83:738–746
31. Edmonds HL, Ganzel BL, Austin EH 3rd:Cerebral oximetry for cardiac and vascularsurgery. Semin Cardiothorac Vasc Anesth2004; 8:147–166
32. Goldman S, Sutter F, Ferdinand F, et al: Opti-mizing intraoperative cerebral oxygen deliveryusing noninvasive cerebral oximetry decreasesthe incidence of stroke for cardiac surgical pa-tients. Heart Surg Forum 2004; 7:E376–E381
33. Murkin JM, Adams S, Schaefer B, et al: Mon-itoring cerebral oxygen saturation signifi-cantly decreases major organ morbidity inCABG patients: A randomized blinded study.Heart Surg Forum 2004; 7:515
34. Slater JP, Guarino T, Stack J, et al: Cerebraloxygen desaturation predicts cognitive de-
S31Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

cline and longer hospital stay after cardiacsurgery. Ann Thorac Surg 2009; 87:36–44
35. Murkin JM, Adams SJ, Novick RJ, et al: Mon-itoring brain oxygen saturation during coro-nary bypass surgery: A randomized, prospec-tive study. Anesth Analg 2007; 104:51–58
36. Austin EH, Edmonds H, Seremet V, et al:Benefit of neurophysiologic monitoring forpediatric cardiac surgery. J Thorac Cardio-vasc Surg 1997; 114:707–717
37. Kim MB, Ward DS, Cartwright CR, et al:Estimation of jugular venous O2 saturationfrom cerebral oximetry or arterial O2 satura-tion during isocapnic hypoxia. J Clin Monit2000; 16:191–199
38. Kurth DM, Steven JL, Montenegro LM, et al:Cerebral oxygen saturation before congenitalheart surgery. Ann Thorac Surg 2001; 72:187–192
39. Fenton KN, Freeman K, Glogowski K, et al:The significance of baseline cerebral oxygensaturation in children undergoing congenitalheart surgery. Am J Surg 2005; 190:260–263
40. Bernal NP, Hoffman GM, Ghanayem NS, etal: Cerebral and somatic near-infrared spec-troscopy in normal newborns. J Pediatr Surg2010; 45:1306–1310
41. Johnson BA, Hoffman GM, Tweddell JS, et al:Near-infrared spectroscopy in neonates be-fore palliation of hypoplastic left heart syn-drome. Ann Thorac Surg 2009; 87:571–577;discussion 577–579
42. Hoffman GM, Ghanayem NS, Stuth EA, et al:NIRS-derived somatic and cerebral saturationdifference provides non-invasive real-time he-modynamic assessment of cardiogenic shockand risk of anaerobic metabolism. Anesthesiol-ogy 2004; 102:A1448. Available at: http://www.asaabstracts.com/strands/asaabstracts/abstract.htm?year�2004&index�16&absnum�2206. Accessed May 12, 2011
43. Hoffman GM, Ghanayem NS, Mussatto KA, etal. Postoperative two-site NIRS predicts com-plications and mortality after stage 1 pallia-tion of HLHS. Anesthesiology 2007;107:A234. Available at: http://www.asaabstracts.com/strands/asaabstracts/abstract.htm?year�2007&index�16&absnum�1585. Accessed May12, 2011
44. Chakravarti SB, Mittnacht AJ, Katz JC, et al:Multisite near-infrared spectroscopy predictselevated blood lactate levels in children aftercardiac surgery. J Cardiothorac Vasc Anesth2009; 23:663–667
45. Dent CL, Spaeth JP, Jones BV, et al: Brainmagnetic resonance imaging abnormalitiesafter the Norwood procedure using regional
cerebral perfusion. J Thorac Cardiovasc Surg2006; 131:190–197
46. Andropoulos DB, Hunter JV, Nelson DP, etal: Brain immaturity is associated with braininjury before and after neonatal cardiac sur-gery with high-flow bypass and cerebral ox-ygenation monitoring. J Thorac CardiovascSurg 2010; 139:543–556
47. Kussman BD, Wypij D, Laussen PC, et al:Relationship of intraoperative cerebral oxy-gen saturation to neurodevelopmental out-come and brain magnetic resonance imagingat 1 year of age in infants undergoing biven-tricular repair. Circulation 2010; 122:245–254
48. Hoffman GM, Ghanayem NS, Berens RJ, et al:Reduction in critical indicators of shock byroutine use of two-site NIRS in pediatric ICUpatients. Anesthesiology 2006; 105: A803.Available at: http://www.asaabstracts.com/strands/asaabstracts/abstract.htm?year�2006&index�6&absnum�1239. AccessedMay 12, 2011
49. Hanson SJ, Berens RJ, Hoffman GM, et al:Effect of volume resuscitation on regionalperfusion in dehydrated pediatric patients asmeasured by two-site near-infrared spectros-copy. Pediatr Emerg Care 2009; 25:150–153
50. Tabbutt S, Ramamoorthy C, Montenegro LM,et al: Impact of inspired gas mixtures onpreoperative infants with hypoplastic leftheart syndrome during controlled ventila-tion. Circulation 2001; 104(Suppl 1):I159–164
51. Ramamoorthy C, Tabbutt S, Kurth CD, et al:Effects of inspired hypoxic and hypercapnicgas mixtures on cerebral oxygen saturationin neonates with univentricular heart de-fects. Anesthesiology 2002; 96:283–288
52. Kleinman ME, de Caen AR, Chameides L, etal: Part 10: Pediatric basic and advanced lifesupport: 2010 International Consensus onCardiopulmonary Resuscitation and Emer-gency Cardiovascular Care Science WithTreatment Recommendations. Circulation2010; 122(Suppl 2):S466–S515
53. Tibby S, Hoffman GM: Peds-059b. Worksheetfor Evidence-Based Review of Science forEmergency Cardiac Care. International Liai-son Committee on Resuscitation. Availableat: http://circ.ahajournals.org/site/C2010/Peds-059.pdf. Accessed May 12, 2011
54. Cohn SM, Nathens AB, Moore FA, et al: Tis-sue oxygen saturation predicts the develop-ment of organ dysfunction during traumaticshock resuscitation. J Trauma 2007; 62:44–54; discussion 54–55
55. Moore FA, Nelson T, McKinley BA, et al:
Massive transfusion in trauma patients: Tis-sue hemoglobin oxygen saturation predictspoor outcome. J Trauma 2008; 64:1010–1023
56. Beilman GJ, Blondett CJ, Nelson TR, et al:Early hypothermia in severely injuredtrauma patients is a significant risk factor formultiple organ dysfunction syndrome butnot mortality. Ann Surg 2009; 249:845–850
57. Sagraves SG, Newell MA, Bard MR, et al:Tissue oxygenation monitoring in the field: Anew EMS vital sign. J Trauma 2009; 67:441–443, discussion 443–444
58. Torello F, Cowley RD, Thorniley MS, et al:Regional tissue oxygenation during hemor-rhage: Can near infrared spectroscopy beused to monitor blood loss? Shock 2002;18:440–444
59. Beekley AC, Martin MJ, Nelson T, et al: Con-tinuous noninvasive tissue oximetry in theearly evaluation of the combat casualty: Aprospective study. J Trauma 2010; 69(Suppl1):S14–S25
60. Creteur J, Carollo T, Soldati G, et al: Theprognostic value of muscle StO2 in septicpatients. Intensive Care Med 2007; 33:1549–1556
61. Leone M, Blidi S, Antonini F, et al: Oxygentissue saturation is lower in nonsurvivorsthan in survivors after early resuscitation ofseptic shock. Anesthesiology 2009; 111:366–371
62. Mulier KE, Skarda DE, Taylor JH, et al: Near-infrared spectroscopy in patients with severesepsis: Correlation with invasive hemody-namic measurements. Surg Infect 2008;9:515–519
63. Payen D, Luengo C, Heyer L, et al: Is thenartissue hemoglobin oxygen saturation in sep-tic shock related to macrohemodynamicvariables and outcome? Crit Care 2009;13(Suppl 5):S6
64. Nanas S, Gerovasili V, Renieris P, et al: Non-invasive assessment of the microcirculationin critically ill patients. Anaesth IntensiveCare 2009; 37:733–739
65. Mozina H, Podbregar M: Near-infrared spec-troscopy during stagnant ischemia estimatescentral venous oxygen saturation and mixedvenous oxygen saturation discrepancy in pa-tients with severe left heart failure and addi-tional sepsis/septic shock. Crit Care 2010;14:R42
66. Fortune PM, Wagstaff M, Petros AJ: Cerebro-splanchnic oxygenation ratio (CSOR) usingnear infrared spectroscopy may be able topredict splanchnic ischaemia in neonates.Intensive Care Med 2001; 27:1401–1407
S32 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Biomonitors of cardiac injury and performance: B-type natriureticpeptide and troponin as monitors of hemodynamics and oxygentransport balance
Michelle Domico, MD; Paul A. Checchia, MD, FCCM, FACC
A biomonitor is defined in ecol-ogy as any organism that pro-vides quantitative informationon the quality of its environ-
ment. It is tempting to think thatbiomonitors could be used to monitor thehemodynamic environment of the patientin a critical care setting. The use of se-rum measurements of organ injury ordysfunction is utilized in a variety of sce-narios in medicine. Biomarkers specificto the cardiovascular system have in-cluded cardiac troponin and natriureticpeptides. While these measures have beenutilized as markers of injury and dysfunc-tion, it has yet to be determined if theycan be utilized as a monitoring strategy
that can guide management decisions ina pediatric critical care setting.
Process
MEDLINE, Embase, PubMed, and Co-chrane Database searches were con-ducted to find controlled trials regardingthe use of heart rate, noninvasive andinvasive pressure, end-tidal CO2, andpulse oximetry monitoring. Adult and pe-diatric data were considered. Guidelinespublished by the Society for Critical CareMedicine, the American Heart Associa-tion, the American Academy of Pediatrics,and the International Liaison Committeeon Resuscitation were reviewed, includ-ing further review of references cited.
B-Type Natriuretic Peptide
Over the last decade, B-type natri-uretic peptide (BNP) has generated inter-est as a promising biomarker in the eval-uation, management, and treatment ofadults and children with a variety of car-diac diseases. The role of BNP and itscleaved inactive metabolite, amino-terminal pro-BNP (NT-proBNP), has beenwell studied in adults with congestiveheart failure (CHF). The utility of BNP inthe pediatric population and in criticalcare units is less well defined. This review
of the evidence will serve as a guideline toaugment understanding and interpreta-tion of BNP levels for practitioners ofpediatric cardiac intensive care.
In 1988, BNP was first identified in theextracts of porcine brain and originallytermed brain natriuretic peptide (1).Subsequent investigations have demon-strated that BNP is a neurohormone se-creted predominantly by ventricularmyocytes. BNP is synthesized as a largerprecursor prohormone (proBNP) of 108amino acids, which is cleaved into thebiologically active BNP (32 amino acids)and an inactive NT-proBNP peptide (76amino acids) (Fig. 1). The regulation ofBNP synthesis and secretion takes placeat the transcriptional level on chromo-some 1. The main impetus for BNP se-cretion is increased ventricular end-diastolic pressure and ventricular walltension (2).
BNP is a member of the natriureticpeptide family, which includes atrial na-triuretic peptide, BNP, C-type natriureticpeptide, and Dendroaspis natriuretic pep-tide (2, 3). BNP has similar physiologicactivity to atrial natriuretic peptide andexerts its actions through natriureticpeptide receptors A and B, ultimately in-creasing intracellular levels of cyclicguanosine monophosphate. BNP binds
From the Children’s Hospital of Orange County(MD), Orange, CA, David Geffen School of Medicine atthe University of California, Los Angeles, CA; and St.Louis Children’s Hospital (PAC), Washington UniversitySchool of Medicine, St. Louis, MO.
Dr. Checchia has received honoraria from MedIm-mune and Edwards Lifesciences, and grants fromIkaria. Dr. Domico has not disclosed any potentialconflicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e318221178d
Serum biomarkers, such as B-type natriuretic peptide andtroponin, are frequently measured in the cardiac intensive careunit. A review of the evidence supporting monitoring of thesebiomarkers is presented.
Design: A search of MEDLINE, PubMed, and the CochraneDatabase was conducted to find literature regarding the use ofB-type natriuretic peptide and troponin in the cardiac intensivecare setting. Adult and pediatric data were considered.
Results and Conclusion: Both B-type natriuretic peptide andtroponin have demonstrated utility in the intensive care settingbut there is no conclusive evidence at this time that eitherbiomarker can be used to guide inpatient management ofchildren with cardiac disease. Although B-type natriuretic pep-
tide and troponin concentrations can alert clinicians to myo-cardial stress, injury, or hemodynamic alterations, the levelscan also be elevated in a variety of clinical scenarios, includingsepsis. Observational studies have demonstrated that periop-erative measurement of these biomarkers can predict postop-erative mortality and complications.
Recommendation and Level of Evidence: (class IIb, level ofevidence B): The use of B-type natriuretic peptide and/or troponinmeasurements in the evaluation of hemodynamics and postoper-ative outcome in pediatric cardiac patients may be beneficial.(Pediatr Crit Care Med 2011; 12[Suppl.]:S33–S42)
KEY WORDS: B-type natriuretic peptide; biomarkers; cardiacdisease; hemodynamics; troponin
S33Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
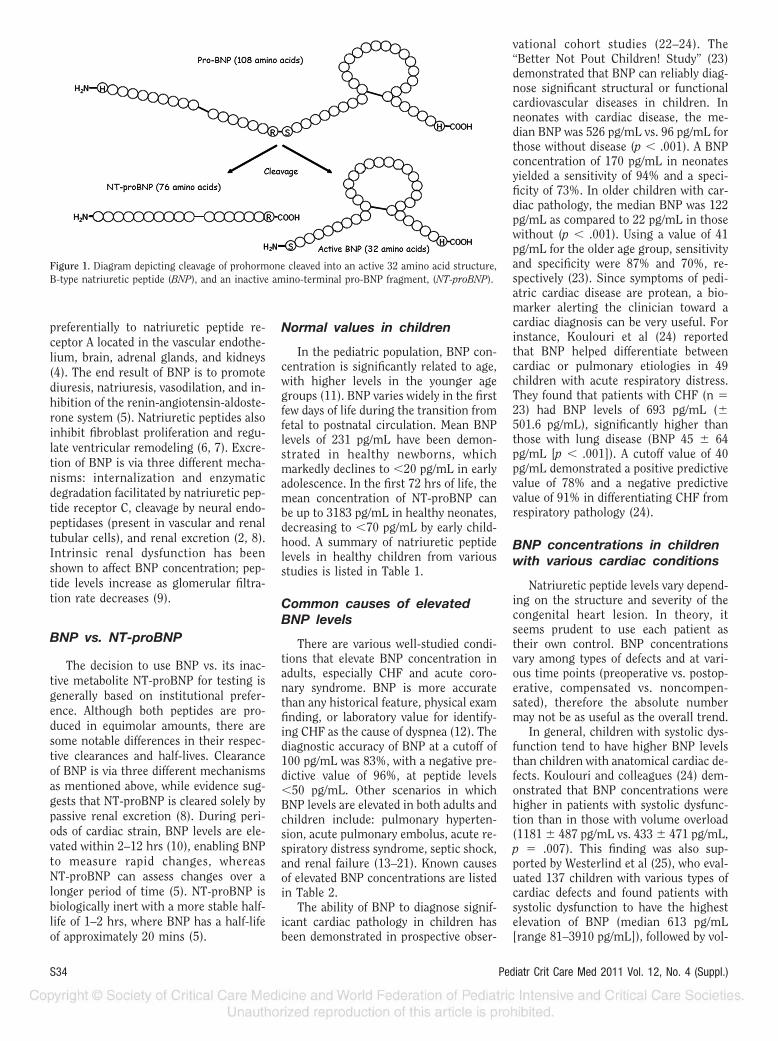
preferentially to natriuretic peptide re-ceptor A located in the vascular endothe-lium, brain, adrenal glands, and kidneys(4). The end result of BNP is to promotediuresis, natriuresis, vasodilation, and in-hibition of the renin-angiotensin-aldoste-rone system (5). Natriuretic peptides alsoinhibit fibroblast proliferation and regu-late ventricular remodeling (6, 7). Excre-tion of BNP is via three different mecha-nisms: internalization and enzymaticdegradation facilitated by natriuretic pep-tide receptor C, cleavage by neural endo-peptidases (present in vascular and renaltubular cells), and renal excretion (2, 8).Intrinsic renal dysfunction has beenshown to affect BNP concentration; pep-tide levels increase as glomerular filtra-tion rate decreases (9).
BNP vs. NT-proBNP
The decision to use BNP vs. its inac-tive metabolite NT-proBNP for testing isgenerally based on institutional prefer-ence. Although both peptides are pro-duced in equimolar amounts, there aresome notable differences in their respec-tive clearances and half-lives. Clearanceof BNP is via three different mechanismsas mentioned above, while evidence sug-gests that NT-proBNP is cleared solely bypassive renal excretion (8). During peri-ods of cardiac strain, BNP levels are ele-vated within 2–12 hrs (10), enabling BNPto measure rapid changes, whereasNT-proBNP can assess changes over alonger period of time (5). NT-proBNP isbiologically inert with a more stable half-life of 1–2 hrs, where BNP has a half-lifeof approximately 20 mins (5).
Normal values in children
In the pediatric population, BNP con-centration is significantly related to age,with higher levels in the younger agegroups (11). BNP varies widely in the firstfew days of life during the transition fromfetal to postnatal circulation. Mean BNPlevels of 231 pg/mL have been demon-strated in healthy newborns, whichmarkedly declines to �20 pg/mL in earlyadolescence. In the first 72 hrs of life, themean concentration of NT-proBNP canbe up to 3183 pg/mL in healthy neonates,decreasing to �70 pg/mL by early child-hood. A summary of natriuretic peptidelevels in healthy children from variousstudies is listed in Table 1.
Common causes of elevatedBNP levels
There are various well-studied condi-tions that elevate BNP concentration inadults, especially CHF and acute coro-nary syndrome. BNP is more accuratethan any historical feature, physical examfinding, or laboratory value for identify-ing CHF as the cause of dyspnea (12). Thediagnostic accuracy of BNP at a cutoff of100 pg/mL was 83%, with a negative pre-dictive value of 96%, at peptide levels�50 pg/mL. Other scenarios in whichBNP levels are elevated in both adults andchildren include: pulmonary hyperten-sion, acute pulmonary embolus, acute re-spiratory distress syndrome, septic shock,and renal failure (13–21). Known causesof elevated BNP concentrations are listedin Table 2.
The ability of BNP to diagnose signif-icant cardiac pathology in children hasbeen demonstrated in prospective obser-
vational cohort studies (22–24). The“Better Not Pout Children! Study” (23)demonstrated that BNP can reliably diag-nose significant structural or functionalcardiovascular diseases in children. Inneonates with cardiac disease, the me-dian BNP was 526 pg/mL vs. 96 pg/mL forthose without disease (p � .001). A BNPconcentration of 170 pg/mL in neonatesyielded a sensitivity of 94% and a speci-ficity of 73%. In older children with car-diac pathology, the median BNP was 122pg/mL as compared to 22 pg/mL in thosewithout (p � .001). Using a value of 41pg/mL for the older age group, sensitivityand specificity were 87% and 70%, re-spectively (23). Since symptoms of pedi-atric cardiac disease are protean, a bio-marker alerting the clinician toward acardiac diagnosis can be very useful. Forinstance, Koulouri et al (24) reportedthat BNP helped differentiate betweencardiac or pulmonary etiologies in 49children with acute respiratory distress.They found that patients with CHF (n �23) had BNP levels of 693 pg/mL (�501.6 pg/mL), significantly higher thanthose with lung disease (BNP 45 � 64pg/mL [p � .001]). A cutoff value of 40pg/mL demonstrated a positive predictivevalue of 78% and a negative predictivevalue of 91% in differentiating CHF fromrespiratory pathology (24).
BNP concentrations in childrenwith various cardiac conditions
Natriuretic peptide levels vary depend-ing on the structure and severity of thecongenital heart lesion. In theory, itseems prudent to use each patient astheir own control. BNP concentrationsvary among types of defects and at vari-ous time points (preoperative vs. postop-erative, compensated vs. noncompen-sated), therefore the absolute numbermay not be as useful as the overall trend.
In general, children with systolic dys-function tend to have higher BNP levelsthan children with anatomical cardiac de-fects. Koulouri and colleagues (24) dem-onstrated that BNP concentrations werehigher in patients with systolic dysfunc-tion than in those with volume overload(1181 � 487 pg/mL vs. 433 � 471 pg/mL,p � .007). This finding was also sup-ported by Westerlind et al (25), who eval-uated 137 children with various types ofcardiac defects and found patients withsystolic dysfunction to have the highestelevation of BNP (median 613 pg/mL[range 81–3910 pg/mL]), followed by vol-
Figure 1. Diagram depicting cleavage of prohormone cleaved into an active 32 amino acid structure,B-type natriuretic peptide (BNP), and an inactive amino-terminal pro-BNP fragment, (NT-proBNP).
S34 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

ume overload lesions (i.e., ventricularseptal defect, atrial septal defect, or pat-ent ductus arterious [PDA]), with medianBNP concentration of 29 pg/mL (range 5-352 pg/mL). Children with pressure over-load lesions (i.e., aortic or pulmonic ste-nosis) had only slightly higher elevationsthan controls (median 17 pg/mL [range0–315 pg/mL] vs. 4 pg/mL [range 0–17pg/mL]) (25). BNP levels are higher whenthe volume overload is at the level of theventricles (dilated cardiomyopathy pa-tients) as compared to the atria (mitralstenosis patients), with levels of 333 �405 pg/mL vs. 147 � 54 pg/mL, respec-tively (p � .01) (26). Diastolic dysfunc-tion also produces elevated BNP levels,but not to the same degree as systolicdysfunction (27–29). Perhaps the ventric-ular hypertrophy that accompanies dia-stolic dysfunction does not permit the“stretch stimulus for BNP,” only the“strain.”
NT-proBNP levels follow similartrends as BNP. Eerola et al (30) examinedserum NT-proBNP levels in 128 childrenwith different types of loading conditions,including atrial septal defect (right-sidedvolume load lesion), PDA (left-sided over-load), coarctation of the aorta (pressureload), and children with Mulibrey nanism(restrictive cardiomyopathy). The highestlevels of NT-proBNP were seen in chil-dren with Mulibrey nanism (mean 280pg/mL, range 18–9170 pg/mL), followedby left-sided overload lesion (PDA), pro-ducing levels ranging from 31 to 6027pg/mL (mean 154 pg/mL). NT-proBNPconcentrations were lower in right-sidedvolume load lesion (mean 90 pg/mL,range 5– 458 pg/mL). Interestingly, inthis particular study, patients with left-sided pressure load (coarctation of theaorta) did not have a statistically signifi-cant elevation of NT-proBNP as comparedto controls (mean 50 pg/mL [range
4–167 pg/mL] vs. mean 57 pg/mL [range14–157 pg/mL], respectively) (30).
Plasma BNP and pulmonary-to-systemic blood flow ratio
Since BNP is elevated in volume over-load lesions, it is logical to questionwhether levels reflect the degree of high-output heart failure, i.e., pulmonary-to-systemic blood flow ratio (Qp/Qs). Kuniiand colleagues (31) explored this possi-bility in 154 children with volume-loadedlesions. Serum BNP correlated signifi-cantly with Qp/Qs values measured in thecatheterization lab in 91 children with aventricular septal defect (r � .75, p �.0001), in 29 with a PDA (r � 089, p �.0001), and in patients with an atrial sep-tal defect (r � .69, p � .001). A cutoffBNP level of 40 pg/mL corresponded to aQp/Qs of 2:1, with a sensitivity of 88%and specificity of 76% (31). This findingwas corroborated by Suda et al (32), dem-onstrating a significant positive correla-tion between BNP levels and Qp/Qs (r �.65) in 59 children with a ventricularseptal defect.
The single-ventricle patient andBNP
Lechner and associates (33) studied 78single-ventricle patients with a bidirec-tional cavopulmonary anastomosis to ob-tain “baseline” NT-proBNP concentra-tions. Thirty-one of those children hadCHF (based on the New York University
Table 1. Values of B-type natriuretic peptide (BNP) and amino-terminal pro BNP (NT-proBNP) in healthy neonatal and pediatric populations
StudyNumber of
Patients (Age Range) Cardiac Peptide Results
Walsh et al 2008 34 (1–36 months) BNP 105 � 78 pg/mL rangeMaher et al 2008 70 (3 days–6 years) BNP 17.4 pg/mL (mean); 5–174 pg/mL rangeZhang et al 2006 190 (1–16 years) BNP 51.9 � 46.3 pg/mL rangeKoch et al 2006 195 (0 days–17 years) BNP 231 pg/mL (mean): 0–1 days
48.6 pg/mL (mean): 2–6 days8.3 pg/mL (females), 8.5 pg/mL (males) mean: �10 years12.1 pg/mL (females), 5.1 pg/mL (males) mean: �10 years
Koch et al 2006 46 (0.4–17 years) NT-proBNP 35.5 pg/mL (median); 10–289 pg/mL rangeEerola et al 2009 64 (0.6–15 years) NT-proBNP 57 pg/mL (mean); 14–157 pg/mL rangea
Mir et al 2006 332 (0–19 years) NT-proBNP 202 pg/mL (mean): 0–9 yearsa
151 pg/mL (mean): 10–14 yearsa
98 pg/mL (mean): 15–19 yearsa
Nir et alb 2009 690 (0–18 years) NT-proBNP 3,183 pg/mL (mean); 260–13,224 pg/mL range: 0–2 days2,210 pg/mL (mean); 28–7,250 pg/mL range: 3–11 days141 pg/mL (mean); 5–1,121 pg/mL range: �1–12 months129 pg/mL (mean); 31–675 pg/mL range: �1–2 years70 pg/mL (mean); 5–391 pg/mL range: �2–6 years52 pg/mL (mean); 5–391 pg/mL range: �6–14 years34 pg/mL (mean); 5–363 pg/mL range: �14–18 years
aconverted from fmol/mL to pg/mL; bpooled data from four separate studies.
Table 2. Known causes of elevated serum B-type natriuretic peptide concentration
Cardiac Etiology Noncardiac Etiology
Congestive heart failure Sepsis/septic shockAcute coronary syndrome Pulmonary embolusCardiomyopathy Pulmonary hypertensionMyocarditis Acute respiratory distress syndromeCongenital heart disease PneumoniaKawasaki disease Chronic obstructive pulmonary disease with
cor pulmonaleAtrial fibrillation/flutter Sleep apneaDiastolic dysfunction/restrictive physiology Renal failureAnthracycline toxicity HyperthyroidismAcute rejection in transplanted hearts Dexamethasone administration
Anemia
S35Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Pediatric Heart Failure Index score), andall had significantly elevated NT-proBNPlevels (median 670 pg/mL, range 290-39,763 pg/mL) vs. bidirectional cavopul-monary anastomosis patients withoutCHF (median 171 pg/mL, range 32–355pg/mL) (33). It has been postulated thatafter bidirectional cavopulmonary anas-tomosis, children with univentricular de-fects and without signs of heart failurehave intrinsic dysfunction in the natri-uretic peptide system, since their BNPconcentrations are nearly equivalent tohealthy children. Natriuretic peptide sys-tem dysfunction in patients with a singleventricle may be related to hypoplasticventricular development (34); however,when in failure, univentricular patientsare able to increase BNP synthesis andsecretion. Evidence for this was providedby Nozohoor and colleagues (35), whoreported that a doubling of plasma BNPwas associated with an odds ratio forheart failure of 2.17 (95% confidence in-terval 1.10 to 4.3, p � .026) in patientswith a single ventricle. Law et al (36) alsodemonstrated elevated BNP concentra-tions (mean 714 � 912 pg/mL) in single-ventricle patients with symptomaticheart failure (n � 18) as compared tothose (n � 8) with no heart failure (mean22 � 12 pg/mL, p � .001).
BNP as a surrogate markerfor other hemodynamicmeasurements
Several pediatric studies mirror theadult experience and report an inversecorrelation between BNP levels and leftventricular ejection fraction in a varietyof clinical scenarios (18, 21, 37–41). Cir-culating levels of BNP have also beenshown to correlate with mean pulmonaryarterial pressure and pulmonary vascularresistance (13, 32, 42). Overall, there areno adequate data to support the utility ofBNP as a surrogate marker for hemody-namic measurements, with the exceptionof ejection fraction as measured by echo-cardiography.
The utility of plasma BNP levelsin the perioperative setting
There is strong evidence (level 1 A) inthe adult population supporting elevatedpreoperative BNP or NT-proBNP mea-surement as an independent predictor ofmortality and major adverse cardiovascu-lar events following vascular and noncar-diac surgery (43–45). Preoperative natri-
uretic peptide levels provide powerfulinformation, predicting adverse out-comes and mortality in adult patientswith acute coronary syndrome, cardio-genic shock, critical illness, and after cor-onary artery bypass grafting (46 –50).There are also adult data demonstratingthat a high predischarge BNP concentra-tion (�700 pg/mL) is a strong, indepen-dent predictor of death or readmissionafter decompensated CHF (51).
Although the pediatric literature isnot as robust, preoperative NT-proBNPlevels correlate with postoperative ino-trope score, duration of mechanical ven-tilation, and duration of intensive careunit (ICU) stay, hence showing promiseas a prognostic predictor for children un-dergoing cardiac surgery (52–54). Newevidence suggests that the biological ac-tivity of the natriuretic hormone systemmay be transiently decreased followingcardiopulmonary bypass, but the mecha-nism is unknown (55). Nonetheless, post-operative BNP concentrations are usefulafter cardiopulmonary bypass; correlat-ing with duration of cardiopulmonary by-pass, postoperative inotrope score, pres-ence of low cardiac output syndrome,cardiac index, duration of mechanicalventilation, and hospital length of stay inneonates and children with a variety ofcongenital heart defects (11, 55–64).
BNP in the periextubationperiod
Cardiopulmonary interactions are ofvital importance in the cardiac ICU. Pos-itive pressure ventilation is highly bene-ficial to a compromised systemic ventri-cle. Conversion from positive pressureventilation to negative pressure ventila-tion following extubation increases after-load on the left ventricle (65) and may bea difficult transition for cardiac patients.A few small studies suggest that BNP maybe a useful adjunct to predict success ofextubation in patients with possible car-diovascular instability. Chien and col-leagues (66) evaluated BNP concentra-tion along with a spontaneous breathingtrial in adults recovering from acute re-spiratory failure and concluded that mea-suring the percentage change in BNPmay improve weaning outcome. Berryand associates (63) noted that BNP levelsincreased within 48 hrs of extubation in12 of 13 patients after the Norwood pro-cedure. This could be a reflection of thecardiopulmonary stress extubation elicitson the systemic ventricle. Further studies
are needed to identify the utility of BNPas an adjunctive marker to determine ex-tubation readiness.
Therapy targeted to BNPconcentration
Natriuretic peptide-guided therapyhas been shown to significantly reduceall-cause mortality in patients with CHFas compared to usual care in both theoutpatient and inpatient setting (67–69).A BNP level of �300 pg/mL in pediatricoutpatients with chronic left ventricularheart failure increased the risk of havingan adverse cardiovascular event (such ascardiac death or cardiac-related hospital-ization) within 90 days (adjusted hazardratio 63.6; p � .0001) (40). Unfortu-nately, there are no data to suggest thatBNP-guided therapy can alter outcome inchildren with anatomical cardiac defects.Unlike adults, the pathophysiology in thepediatric cardiac ICU is diverse, includingsystolic dysfunction, diastolic dysfunc-tion, and volume or pressure overload ofeither ventricle and/or atria.
Limitations
The use of BNP measurements arehandicapped by a wide variety of clinicalscenarios in which natriuretic peptidelevels can be elevated, including cardiacpathology, lung disease, and septic shock.Therefore, increased BNP concentrationsshould be interpreted with caution andpractitioners should consider the clinicalsituation in total, rather than focus solelyon cardiac pathology.
Conclusion for BNP
BNP is a useful adjunctive biomarkerin children with cardiac pathology. Thisbiomarker can be elevated in several con-ditions, such as systolic dysfunction, dia-stolic dysfunction, and various congenitalheart defects causing volume and/or pres-sure load on the heart. There is evidenceto support that BNP concentrations par-allel Qp/Qs measurements and inverselycorrelate with ejection fraction. A recentapplication for natriuretic peptides ismeasurement in the perioperative periodto prognosticate morbidity and mortalityin cardiac surgical patients. Further stud-ies are required in children to define therole of natriuretic peptides in the periop-erative setting. Current pediatric evi-dence suggests that BNP levels are re-lated to postoperative complications,
S36 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

such as prolonged duration of mechani-cal ventilation and hospital length of stay.Future studies in the cardiac ICU evalu-ating preoperative, postoperative, andpredischarge BNP levels while trendingthese values in an individual patient mayhelp prognosticate outcome. This neuro-hormone may prove to be invaluable as adiagnostic tool and therapeutic agent inthe future of pediatric cardiac intensivecare.
Cardiac Troponin
The myocardial sarcomere is com-posed of the contractile proteins myosin,tropomyosin, and the troponin complex.The cardiac troponin (cTn) complex ismade up of three distinct subtypes: tro-ponin C, troponin I, and troponin T. To-gether, this complex controls the inter-action of the thick and thin filamentsand, ultimately, muscular contraction.Specifically, calcium binds to the tro-ponin C subunit, resulting in a confor-mational change allowing actin-myosincross-bridge formation. The utility of tro-ponin as a marker of myocardial injurystems from its origin specifically fromcardiac muscles. While the troponincomplex is found throughout all musclecells, the I and T subunits found in thecardiac myocyte are immunologically dis-tinct from their skeletal muscle forms.The N-terminus amino chain is uniquein the cardiac subunits and has resulted inthe development of monoclonal antibod-ies as markers in the serum of patients(70–73). The sensitivity and specificity ofboth the I and T isoforms are similarexcept for their detectable half-lives (74).
Troponin in cardiac injury
Cardiac troponin I (cTnI) and cardiactroponin T (cTnT) are released as a resultof myocardial cell injury and are highlysensitive and specific markers of myocar-dial damage (75). As early as 1981, studiessuggested that troponin subunits are re-leased from the endocardium of the in-farcted region relatively early (4 hrs aftercoronary artery occlusion) in patientswith myocardial infarction (76). Thisfinding prompted some studies to suggestthe use of cTn as a clinically importantmarker of cardiac injury and infarction(77–81). cTn measurements are superiorto that of creatine kinase MB, with highersensitivity and specificity (70, 77). Severalstudies in the adult patient populationhave shown that cTnI and cTnT are the
most diagnostically sensitive and specificbiomarkers of myocardial injury (82–84).Based on this sensitivity and specificityprofile, cTn is recommended for the di-agnosis of acute myocardial infarction bythe National Academy of Clinical Bio-chemistry Laboratory Medicine PracticeGuidelines, and the International Com-mittee of Experts in Epidemiology, Pa-thology, Clinical, and Laboratory Medi-cine (85–87). Serial sampling, includinga baseline sample and follow-up examina-tion 8 to 12 hrs after symptom onset, isrecommended (88). Although cTnI iscleared more quickly from the circulationthan cTnT, both isoforms remain ele-vated in the serum for several days afterinjury, allowing for diagnostic confirma-tion even in patients presenting with de-layed symptoms. For similar reasons, itsutility as a monitor of ongoing cardiacinjury is limited.
Troponin in pediatrics
There are specific issues related to theuse of troponin measurements in the pe-diatric population. The fetal heart con-tains two cTnI isoforms: the adult cTnIand an isoform similar to one found inadult slow-twitch skeletal muscle. Thelatter, which is predominant in the fetus,is replaced with maturation, so at term,only the adult cTnI is detectable (89).Troponin concentrations in normal chil-dren are higher in the first year of life,being highest after birth, and graduallydecreasing to adult concentrations to-ward the end of the first year (90, 91).These ranges appear to require at leastone standard deviation above the normalreference range, depending on specificassay characteristics. Additionally, tro-ponin measurements in the perinatal pe-riod and in premature infants may belimited by these issues (92–97). Thesefactors reinforce the recommendation forserial measurements in the neonatal pe-riod.
Troponin in nonischemiccardiac conditions
Critically ill patients may have ele-vated cTn levels in various nonacute cor-onary syndrome disorders (98–104). Sev-eral studies have demonstrated that thepresence of elevated troponin levels incritically ill septic patients predicts thepresence of myocardial dysfunction andan increased mortality rate (105, 106). Ina study of 37 consecutive patients with
septic shock (107), the 16 (43%) patientswith elevated serum cTnI had a signifi-cantly lower ejection fraction and signif-icantly higher mortality than the others.Preexisting coronary artery disease anddemand ischemia could account for cTnrelease in sepsis. However, it has beenshown that cTn release can also occur inpatients in whom significant coronary ar-tery disease has been excluded with sen-sitive methods (98).
Babuin et al (100) evaluated the short-term and long-term prognostic value ofmeasurement cTnT levels in 1,657 med-ical ICU patients. Admission (within 6hrs) cTnT measurement of at least 0.01�g/L was considered elevated. PositivecTnT levels were available in 929 (56.1%)patients, of which 570 (61.4%) had ele-vated levels. During hospitalization,12.5% of patients with negative cTnTdied, compared with 29.5% with elevatedcTnT. Mortality rate at 30 days was 13.7%in patients with negative, compared with34.6% in patients with positive, cTnT.The expected probability of mortality at1-yr, 2-yr, and 3-yr follow-up was higherin patients with elevated cTnT. After ad-justment for severity of illness using theAcute Physiology and Chronic HealthEvaluation III prognostic system, positivecTnT levels were independently associ-ated with in-hospital, and short- andlong-term mortality. Interestingly, theprognostic value of cTnT elevations wassimilar (or even slightly better) in pa-tients with noncardiovascular etiologiesof their acute illness and in patients whowere less ill according to Acute Physiol-ogy and Chronic Health Evaluation III.Elevated cTnT was associated with short-term and long-term mortality, indicatingthat even after successful treatment anddischarge, there still may be opportuni-ties to improve outcomes if mechanismsresponsible for the cardiac injury areidentified. These data further supportpublished studies that underlined theprognostic impact of elevated cTn in dif-ferent settings of critically ill patients(108–112). In another study of 46 pa-tients with septic shock, increasedplasma concentrations of cTnI and cTnTwere found in 50% and 36% of patients,respectively (113). Left ventricular func-tional assessment revealed that both cTnIand cTnT were exclusively associatedwith left ventricular dysfunction (p �.0001).
However, the usefulness of elevatedtroponin levels in identifying septic pa-tients with myocardial dysfunction is lim-
S37Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

ited, since many other conditions com-monly observed within the ICU, such asacute coronary syndrome, acute kidneyinjury, and pulmonary embolism, are alsoassociated with an increase in troponinlevels (75). As such, there is no evidenceto support the use of inotropes in patientswith elevated troponin levels in an effortto enhance myocardial performance. In-deed, this approach may be harmful(114). Nevertheless, an elevated troponinlevel in the critically ill is associated withan adverse prognosis irrespective of theunderlying cause (98, 108, 115, 116).
Fenton et al (101) demonstrated in-creased cTnI in children with septicshock admitted to a pediatric ICU, a find-ing similar to studies in adults (105, 106,117). Other pediatric data have shownthat children with meningococcal septicshock had a significant increase in cTnI(118). In another series of children withmeningococcal sepsis, Thiru and col-leagues (119) found that cTnI was in-creased at admission to a degree similarto that we have found in septic shock(24% at admission, 62% within the first 2days of illness), but ischemic heart dis-ease was not excluded in these children.Additionally, troponin elevation has beendemonstrated in children with a septic-like picture associated with respiratorysyncytial virus infection (120, 121).
Troponin and renal disease
In apparently asymptomatic, stable di-alysis patients, multivessel coronary ar-tery disease diagnosed by angiography ismore prevalent with progressively greaterquartiles of troponin (122), and it is astrong predictor of death and cardiovas-cular events. It is unlikely that elevatedserum troponin is the result of decreasedclearance by the failing kidney. Free tro-ponin T and bound troponin T are rela-tively large molecules (37 and 77 kDa,respectively), similar in molecular weightto albumin (60 kDa), making it improb-able that the kidney would be responsiblefor their clearance. Creatine kinase andits isoforms are of similar size and aremainly cleared by the reticuloendothelialsystem (123), whereas myoglobin issmaller (18 kDa) and cleared by the kid-ney (124). Indeed, in asymptomatic he-modialysis patients, troponin T rises inparallel with left ventricular mass andmirrors declining left ventricular systolicfunction (125). These relationships prob-ably reflect subtle myocardial cell isch-emia brought about by perfusion mis-
match. It is possible that smaller,immunoreactive troponin fragments arecleared by the kidney, but this remains tobe clarified. Improvement in renal func-tion after renal transplant does not ap-pear to alter the occurrence of elevatedserum troponin (126). Even if the kidneyswere partially responsible for troponinclearance, it does not explain why tro-ponin is released from the heart. Duringmyocardial necrosis, the elimination rateand apparent half-life of serum cTnI isnot significantly different in patients withnormal renal function or end-stage renaldisease (127). Additionally, preliminaryresults from Western blot analysis fail toimplicate renal tissue as the source ofserum cTnT in patients with renal failure(128). Notably, it has been repeatedlyconfirmed that troponin T is a powerfuldeath predictor, and a recent meta-analysis has nicely shown that high tro-ponin T (�0.1 ng/mL) conveys a 2.6times higher risk of death in asymptom-atic dialysis patients (129).
Troponin in perioperativecardiac patients
Increased cTn has been reported tooccur after virtually every open-heartsurgery (70, 130, 131). However, releaseof cTn in the postoperative cardiac set-ting may not only reflect acute myocar-dial infarction related to coronary syn-dromes, but could also result frommyocardial cell injury attributable to in-complete myocardial protection, reperfu-sion injury, unavoidable surgical trauma,intramyocardial vessel manipulation, anddefibrillation (132, 133). Previous studiesdemonstrated that all children with intra-cardiac surgery showed a postoperativeincrease in cTnT. Children with extracar-diac surgery of the great vessels showedno postoperative increase of cTnT (134).Increases in creatine kinase MB and cTnThave been reported to be about five timesgreater than those previously reported inadult patients (135).
The association between increasedpostoperative troponin release and clini-cal postoperative outcomes is controver-sial (136–140). Nesher et al (139) foundthat moderate elevations in troponin arecommon after cardiac operations inadults, and specifically, a cTnT level ex-ceeding eight times the upper limit ofnormal (�0.8 �g/L) was found to be anindependent predictor of increased majoradverse cardiac events. Mildh et al (141),using a forward stepwise logistic regres-
sion, showed that troponin T measuredon the first postoperative day was astrong independent predictor of death at30 days. Levels of troponin T �5.9 �/L onthe first postoperative day predicteddeath, as did an admission lactate level�5.2 mmol/L. No other variable, includ-ing postoperative creatine kinase MBconcentration, age, diagnosis, surgicalprocedure, presence of cyanosis, chromo-somal anomaly or ventriculotomy, dura-tion of cardiopulmonary bypass, or aorticcross-clamp, had any independent effecton 30-day survival. Additionally, Lip-shultz et al (142) demonstrated an asso-ciation between a score of increasing sur-gical severity and the mean level ofpostoperative cTnT. Postoperative cTnTlevels were significantly elevated in chil-dren who completed cardiovascular sur-gery with an open chest compared withthose with a closed chest. In addition,cTnT levels before cardiovascular surgerypredicted postoperative survival. Finally,perioperative troponin measurementshave been used as a gauge of therapeuticsuccess with a variety of intraoperativeprotocols (142–148).
Recommendation and Level ofEvidence
Class IIb, level of evidence B
The use of BNP and/or troponin mea-surements in the evaluation of hemody-namics in pediatric patients may be con-sidered and may be beneficial.
REFERENCES
1. Sudoh T, Kangawa K, Minamino N, et al: Anew natriuretic peptide in porcine brain.Nature 1988; 332:78–81
2. Levin ER, Gardner DG, Samson WK: Natri-uretic peptides. N Engl J Med 1998; 339:321–328
3. Costello JM, Goodman DM, Green TP: Areview of the natriuretic hormone system’sdiagnostic and therapeutic potential in crit-ically ill children. Pediatr Crit Care Med2006; 7:308–318
4. Suga S, Nakao K, Hosoda K, et al: Receptorselectivity of natriuretic peptide family,atrial natriuretic peptide, brain natriureticpeptide, and C-type natriuretic peptide. En-docrinology 1992; 130:229–239
5. Godkar D, Bachu K, Dave B, et al: B-typenatriuretic peptide (BNP) and proBNP: Roleof emerging markers to guide therapy anddetermine prognosis in cardiovascular dis-orders. Am J Ther 2008; 15:150–156
6. Munzel T, Feil R, Mulsch A, et al: Physi-ology and pathophysiology of vascular sig-
S38 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

naling controlled by guanosine 3�,5�-cyclic monophosphate-dependent proteinkinase [corrected]. Circulation 2003; 108:2172–2183
7. Magga J, Puhakka M, Hietakorpi S, et al:Atrial natriuretic peptide, B-type natriureticpeptide, and serum collagen markers afteracute myocardial infarction. J Appl Physiol2004; 96:1306–1311
8. Hall C: Essential biochemistry and physiol-ogy of (NT-pro)BNP. Eur J Heart Fail 2004;6:257–260
9. Wiley CL, Switzer SP, Berg RL, et al: Asso-ciation of B-type natriuretic Peptide levelswith estimated glomerular filtration rateand congestive heart failure. Clin Med Res2010; 8:7–12
10. Rodseth RN: B type natriuretic peptide–adiagnostic breakthrough in peri-operativecardiac risk assessment? Anaesthesia 2009;64:165–178
11. Mir TS, Flato M, Falkenberg J, et al: Plasmaconcentrations of N-terminal brain natri-uretic peptide in healthy children, adoles-cents, and young adults: Effect of age andgender. Pediatr Cardiol 2006; 27:73–77
12. Maisel A: Algorithms for using B-type natri-uretic peptide levels in the diagnosis andmanagement of congestive heart failure.Crit Pathw Cardiol 2002; 1:67–73
13. Casserly B, Klinger JR: Brain natriureticpeptide in pulmonary arterial hypertension:Biomarker and potential therapeutic agent.Drug Des Devel Ther 2009; 3:269–287
14. Cavallazzi R, Nair A, Vasu T, et al: Natri-uretic peptides in acute pulmonary embo-lism: A systematic review. Intensive CareMed 2008; 34:2147–2156
15. Post F, Weilemann LS, Messow CM, et al:B-type natriuretic peptide as a marker forsepsis-induced myocardial depression in in-tensive care patients. Crit Care Med 2008;36:3030–3037
16. Kandil E, Burack J, Sawas A, et al: B-typenatriuretic peptide: A biomarker for the di-agnosis and risk stratification of patientswith septic shock. Arch Surg 2008; 143:242–246
17. Reel B, Oishi PE, Hsu JH, et al: Early ele-vations in B-type natriuretic peptide levelsare associated with poor clinical outcomesin pediatric acute lung injury. Pediatr Pul-monol 2009; 44:1118–1124
18. Domico M, Liao P, Anas N, et al: Elevationof brain natriuretic peptide levels in chil-dren with septic shock. Pediatr Crit CareMed 2008; 9:478–483
19. Austin WJ, Bhalla V, Hernandez-Arce I, etal: Correlation and prognostic utility of B-type natriuretic peptide and its amino-terminal fragment in patients with chronickidney disease. Am J Clin Pathol 2006; 126:506–512
20. Kawamura T, Wago M, Kawaguchi H, et al:Plasma brain natriuretic peptide concentra-tions in patients with Kawasaki disease. Pe-diatr Int 2000; 42:241–248
21. Hayakawa H, Komada Y, Hirayama M, et al:
Plasma levels of natriuretic peptides in re-lation to doxorubicin-induced cardiotoxic-ity and cardiac function in children withcancer. Med Pediatr Oncol 2001; 37:4–9
22. Maher KO, Reed H, Cuadrado A, et al: B-type natriuretic peptide in the emergencydiagnosis of critical heart disease in chil-dren. Pediatrics 2008; 121:e1484–e1488
23. Law YM, Hoyer AW, Reller MD, et al: Accu-racy of plasma B-type natriuretic peptide todiagnose significant cardiovascular diseasein children: The Better Not Pout Children!Study. J Am Coll Cardiol 2009; 54:1467–1475
24. Koulouri S, Acherman RJ, Wong PC, et al:Utility of B-type natriuretic peptide in dif-ferentiating congestive heart failure fromlung disease in pediatric patients with re-spiratory distress. Pediatr Cardiol 2004; 25:341–346
25. Westerlind A, Wåhlander H, Berggren H, etal: Plasma levels of natriuretic peptide typeB and A in children with heart disease withdifferent types of cardiac load or systolicdysfunction. Clin Physiol Funct Imaging2008; 28:277–284
26. Yoshimura M, Yasue H, Okumura K, et al:Different secretion patterns of atrial natri-uretic peptide and brain natriuretic peptidein patients with congestive heart failure.Circulation 1993; 87:464–469
27. Krishnaswamy P, Lubien E, Clopton P, et al:Utility of B-natriuretic peptide levels inidentifying patients with left ventricularsystolic or diastolic dysfunction. Am J Med2001; 111:274–279
28. Lukowicz TV, Fischer M, Hense HW, et al:BNP as a marker of diastolic dysfunction inthe general population: Importance of leftventricular hypertrophy. Eur J Heart Fail2005; 7:525–531
29. Grewal J, McKelvie R, Lonn E, et al: BNPand NT-proBNP predict echocardiographicseverity of diastolic dysfunction. EurJ Heart Fail 2008; 10:252–259
30. Eerola A, Jokinen E, Pihkala JI: Serum lev-els of natriuretic peptides in children withvarious types of loading conditions. ScandCardiovasc J 2009; 43:187–193
31. Kunii Y, Kamada M, Ohtsuki S, et al:Plasma brain natriuretic peptide and theevaluation of volume overload in infantsand children with congenital heart disease.Acta Med Okayama 2003; 57:191–197
32. Suda K, Matsumura M, Matsumoto M: Clin-ical implication of plasma natriuretic pep-tides in children with ventricular septal de-fect. Pediatr Int 2003; 45:249–254
33. Lechner E, Schreier-Lechner EM, Hofer A,et al: Aminoterminal brain-type natriureticpeptide levels correlate with heart failure inpatients with bidirectional Glenn anasto-mosis and with morbidity after the Fontanoperation. J Thorac Cardiovasc Surg 2009;138:560–564
34. Sun LS, Dominguez C, Mallavaram NA, etal: Dysfunction of atrial and B-type natri-uretic peptides in congenital univentricular
defects. J Thorac Cardiovasc Surg 2005;129:1104–1110
35. Nozohoor S, Nilsson J, Luhrs C, et al: B-type natriuretic peptide as a predictor ofpostoperative heart failure after aortic valvereplacement. J Cardiothorac Vasc Anesth2009; 23:161–165
36. Law YM, Ettedgui J, Beerman L, et al: Com-parison of plasma B-type natriuretic peptidelevels in single ventricle patients with sys-temic ventricle heart failure versus isolatedcavopulmonary failure. Am J Cardiol 2006;98:520–524
37. Koch A, Zink S, Singer H: B-type natri-uretic peptide in paediatric patients withcongenital heart disease. Eur Heart J 2006;27:861–866
38. Koch AM, Rauh M, Zink S, et al: Decreasingratio of plasma N-terminal pro-B-type na-triuretic peptide and B-type natriuretic pep-tide according to age. Acta Paediatr 2006;95:805–809
39. Mir TS, Marohn S, Laer S, et al: Plasmaconcentrations of N-terminal pro-brain na-triuretic peptide in control children fromthe neonatal to adolescent period and inchildren with congestive heart failure. Pe-diatrics 2002; 110:e76
40. Price JF, Thomas AK, Grenier M, et al: B-type natriuretic peptide predicts adversecardiovascular events in pediatric outpa-tients with chronic left ventricular systolicdysfunction. Circulation 2006; 114:1063–1069
41. Mangat J, Carter C, Riley G, et al: The clin-ical utility of brain natriuretic peptide inpaediatric left ventricular failure. EurJ Heart Fail 2009; 11:48–52
42. Cowley CG, Bradley JD, Shaddy RE: B-typenatriuretic peptide levels in congenitalheart disease. Pediatr Cardiol 2004; 25:336–340
43. Karthikeyan G, Moncur RA, Levine O, et al:Is a pre-operative brain natriuretic peptideor N-terminal pro-B-type natriuretic pep-tide measurement an independent predictorof adverse cardiovascular outcomes within30 days of noncardiac surgery? A systematicreview and meta-analysis of observationalstudies. J Am Coll Cardiol 2009; 54:1599–1606
44. Ryding AD, Kumar S, Worthington AM, etal: Prognostic value of brain natriureticpeptide in noncardiac surgery: A meta-analysis. Anesthesiology 2009; 111:311–319
45. Rodseth RN, Padayachee L, Biccard BM: Ameta-analysis of the utility of pre-operativebrain natriuretic peptide in predicting earlyand intermediate-term mortality and majoradverse cardiac events in vascular surgicalpatients. Anaesthesia 2008; 63:1226–1233
46. Fox AA, Muehlschlegel JD, Body SC, et al:Comparison of the utility of preoperativeversus postoperative B-type natriuretic pep-tide for predicting hospital length of stayand mortality after primary coronary arterybypass grafting. Anesthesiology 2010; 112:842–851
S39Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

47. Cuthbertson BH, McKeown A, Croal BL, etal: Utility of B-type natriuretic peptide inpredicting the level of peri- and postopera-tive cardiovascular support required aftercoronary artery bypass grafting. Crit CareMed 2005; 33:437–442
48. de Lemos JA, Morrow DA, Bentley JH, et al:The prognostic value of B-type natriureticpeptide in patients with acute coronary syn-dromes. N Engl J Med 2001; 345:1014–1021
49. Jarai R, Fellner B, Haoula D, et al: Earlyassessment of outcome in cardiogenicshock: Relevance of plasma N-terminal pro-B-type natriuretic peptide and interleukin-6levels. Crit Care Med 2009; 37:1837–1844
50. Almog Y, Novack V, Megralishvili R, et al:Plasma level of N terminal pro-brain natri-uretic peptide as a prognostic marker incritically ill patients. Anesth Analg 2006;102:1809–1815
51. Logeart D, Thabut G, Jourdain P, et al:Predischarge B-type natriuretic peptide as-say for identifying patients at high risk ofre-admission after decompensated heartfailure. J Am Coll Cardiol 2004; 43:635–641
52. Walsh R, Boyer C, LaCorte J, et al: N-termi-nal B-type natriuretic peptide levels in pe-diatric patients with congestive heart fail-ure undergoing cardiac surgery. J ThoracCardiovasc Surg 2008; 135:98–105
53. Tissieres P, da Cruz E, Habre W, et al: Valueof brain natriuretic peptide in the perioper-ative follow-up of children with valvular dis-ease. Intensive Care Med 2008; 34:1109–1113
54. Gessler P, Knirsch W, Schmitt B, et al:Prognostic value of plasma N-terminal pro-brain natriuretic peptide in children withcongenital heart defects and open-heartsurgery. J Pediatr 2006; 148:372–376
55. Costello JM, Backer CL, Checchia PA, et al:Effect of cardiopulmonary bypass and sur-gical intervention on the natriuretic hor-mone system in children. J Thorac Cardio-vasc Surg 2005; 130:822–829
56. Koch A, Kitzsteiner T, Zink S, et al: Impactof cardiac surgery on plasma levels of B-type natriuretic peptide in children withcongenital heart disease. Int J Cardiol 2007;114:339–344
57. Hsu JH, Keller RL, Chikovani O, et al: B-type natriuretic peptide levels predict out-come after neonatal cardiac surgery. J Tho-rac Cardiovasc Surg 2007; 134:939–945
58. Hsu JH, Oishi PE, Keller RL, et al: Periop-erative B-type natriuretic peptide levels pre-dict outcome after bidirectional cavopulmo-nary anastomosis and total cavopulmonaryconnection. J Thorac Cardiovasc Surg2008; 135:746–753
59. Mir TS, Haun C, Lilje C, et al: Utility ofN-terminal brain natriuretic peptide plasmaconcentrations in comparison to lactate andtroponin in children with congenital heartdisease following open-heart surgery. Pedi-atr Cardiol 2006; 27:209–216
60. Shih CY, Sapru A, Oishi P, et al: Alterationsin plasma B-type natriuretic peptide levels
after repair of congenital heart defects: Apotential perioperative marker. J ThoracCardiovasc Surg 2006; 131:632–638
61. Breuer T, Sapi E, Skoumal R, et al: N-ter-minal probrain natriuretic peptide level in-versely correlates with cardiac index afterarterial switch operation in neonates. Pae-diatr Anaesth 2007; 17:782–788
62. Cannesson M, Bionda C, Gostoli B, et al:Time course and prognostic value of plasmaB-type natriuretic peptide concentration inneonates undergoing the arterial switch op-eration. Anesth Analg 2007; 104:1059–1065, tables of contents
63. Berry JG, Askovich B, Shaddy RE, et al:Prognostic value of B-type natriuretic pep-tide in surgical palliation of children withsingle-ventricle congenital heart disease.Pediatr Cardiol 2008; 29:70–75
64. Carmona F, Manso PH, Vicente WV, et al:Risk stratification in neonates and infantssubmitted to cardiac surgery with cardio-pulmonary bypass: A multimarker approachcombining inflammatory mediators, N-ter-minal pro-B-type natriuretic peptide andtroponin I. Cytokine 2008; 42:317–324
65. Bronicki RA, Anas NG: Cardiopulmonary in-teraction. Pediatr Crit Care Med 2009; 10:313–322
66. Chien JY, Lin MS, Huang YC, et al: Changesin B-type natriuretic peptide improve wean-ing outcome predicted by spontaneousbreathing trial. Crit Care Med 2008; 36:1421–1426
67. Porapakkham P, Porapakkham P, ZimmetH, et al: B-type natriuretic peptide-guidedheart failure therapy: A meta-analysis. ArchIntern Med 2010; 170:507–514
68. Felker GM, Hasselblad V, Hernandez AF, etal: Biomarker-guided therapy in chronicheart failure: A meta-analysis of random-ized controlled trials. Am Heart J 2009;158:422–430
69. Valle R, Aspromonte N, Giovinazzo P, et al:B-type natriuretic Peptide-guided treat-ment for predicting outcome in patientshospitalized in sub-intensive care unit withacute heart failure. J Card Fail 2008; 14:219–224
70. Adams JE 3rd, Bodor GS, Davila-Roman VG,et al: Cardiac troponin I. A marker withhigh specificity for cardiac injury. Circula-tion 1993; 88:101–106
71. Cummins B, Auckland ML, Cummins P:Cardiac-specific troponin-I radioimmuno-assay in the diagnosis of acute myocardialinfarction. Am Heart J 1987; 113:1333–1344
72. Larue C, Defacque-Lacquement H, CalzolariC, et al: New monoclonal antibodies asprobes for human cardiac troponin I:Epitopic analysis with synthetic peptides.Mol Immunol 1992; 29:271–278
73. Wilkinson JM, Grand RJ: The amino-acidsequence of chicken fast-skeletal-muscletroponin I. Eur J Biochem 1978; 82:493–501
74. Heidenreich PA, Alloggiamento T, Melsop
K, et al: The prognostic value of troponin inpatients with non-ST elevation acute coro-nary syndromes: A meta-analysis. J Am CollCardiol 2001; 38:478–485
75. Wong CK, White HD: Implications of thenew definition of myocardial infarction.Postgrad Med J 2005; 81:552–555
76. Toyo-Oka T, Ross J Jr: Ca2� sensitivitychange and troponin loss in cardiac naturalactomyosin after coronary occlusion. Am JPhysiol 1981; 240:H704–H708
77. Chiu A, Chan WK, Cheng SH, et al: Tro-ponin-I, myoglobin, and mass concentra-tion of creatine kinase-MB in acute myocar-dial infarction. QJM 1999; 92:711–718
78. Ellis AK: Serum protein measurements andthe diagnosis of acute myocardial infarc-tion. Circulation 1991; 83:1107–1109
79. Katus HA, Remppis A, Neumann FJ, et al:Diagnostic efficiency of troponin T mea-surements in acute myocardial infarction.Circulation 1991; 83:902–912
80. Mair J, Artner-Dworzak E, Lechleitner P, etal: Cardiac troponin T in diagnosis of acutemyocardial infarction. Clin Chem 1991; 37:845–852
81. Mair J, Wieser C, Seibt I, et al: Troponin Tto diagnose myocardial infarction in bypasssurgery. Lancet 1991; 337:434–435
82. Kavsak PA, Wang X, Ko DT, et al: Short- andlong-term risk stratification using a next-generation, high-sensitivity research car-diac troponin I (hs-cTnI) assay in an emer-gency department chest pain population.Clin Chem 2009; 55:1809–1815
83. Keller T, Zeller T, Peetz D, et al: Sensitivetroponin I assay in early diagnosis of acutemyocardial infarction. N Engl J Med 2009;361:868–877
84. Reichlin T, Hochholzer W, Bassetti S, et al:Early diagnosis of myocardial infarctionwith sensitive cardiac troponin assays.N Engl J Med 2009; 361:858–867
85. Alpert JS, Thygesen K, Antman E, et al:Myocardial infarction redefined–a consen-sus document of The Joint European Soci-ety of Cardiology/American College of Car-diology Committee for the redefinition ofmyocardial infarction. J Am Coll Cardiol2000; 36:959–969
86. Jaffe AS, Ravkilde J, Roberts R, et al: It’stime for a change to a troponin standard.Circulation 2000; 102:1216–1220
87. Morrow DA, Cannon CP, Jesse RL, et al:National Academy of Clinical BiochemistryLaboratory Medicine Practice Guidelines:Clinical characteristics and utilization ofbiochemical markers in acute coronary syn-dromes. Circulation 2007; 115:e356–e375
88. Evaluation of a bedside whole-blood rapidtroponin T assay in the emergency depart-ment. Rapid Evaluation by Assay of Car-diac Troponin T (REACTT) InvestigatorsStudy Group. Acad Emerg Med 1997;4:1018 –1024
89. Sasse S, Brand NJ, Kyprianou P, et al: Tro-ponin I gene expression during human car-
S40 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

diac development and in end-stage heartfailure. Circ Res 1993; 72:932–938
90. Hirsch R, Landt Y, Porter S, et al: Cardiactroponin I in pediatrics: Normal values andpotential use in the assessment of cardiacinjury. J Pediatr 1997; 130:872–877
91. Towbin JA, Gajarski RJ: Cardiac troponin I:A new diagnostic gold standard of cardiacinjury in children? J Pediatr 1997; 130:853–855
92. Kanaan UB, Chiang VW: Cardiac troponinsin pediatrics. Pediatr Emerg Care 2004; 20:323–329
93. McAuliffe F, Mears K, Fleming S, et al: Fetalcardiac troponin I in relation to intrapar-tum events and umbilical artery pH. Am JPerinatol 2004; 21:147–152
94. Quivers ES, Murthy JN, Soldin SJ: The ef-fect of gestational age, birth weight, anddisease on troponin I and creatine kinaseMB in the first year of life. Clin Biochem1999; 32:419–421
95. Soldin SJ, Murthy JN, Agarwalla PK, et al:Pediatric reference ranges for creatine ki-nase, CKMB, Troponin I, iron, and cortisol.Clin Biochem 1999; 32:77–80
96. Trevisanuto D, Pitton M, Altinier S, et al:Cardiac troponin I, cardiac troponin T andcreatine kinase MB concentrations in um-bilical cord blood of healthy term neonates.Acta Paediatr 2003; 92:1463–1467
97. Turker G, Babaoglu K, Gokalp AS, et al:Cord blood cardiac troponin I as an earlypredictor of short-term outcome in perina-tal hypoxia. Biol Neonate 2004; 86:131–137
98. Ammann P, Maggiorini M, Bertel O, et al:Troponin as a risk factor for mortality incritically ill patients without acute coronarysyndromes. J Am Coll Cardiol 2003; 41:2004–2009
99. Babuin L, Jaffe AS: Troponin: The bio-marker of choice for the detection of car-diac injury. CMAJ 2005; 173:1191–1202
100. Babuin L, Vasile VC, Rio Perez JA, et al:Elevated cardiac troponin is an independentrisk factor for short- and long-term mortal-ity in medical intensive care unit patients.Crit Care Med 2008; 36:759–765
101. Fenton KE, Sable CA, Bell MJ, et al: In-creases in serum levels of troponin I areassociated with cardiac dysfunction and dis-ease severity in pediatric patients with sep-tic shock. Pediatr Crit Care Med 2004;5:533–538
102. John J, Woodward DB, Wang Y, et al: Tro-ponin-I as a prognosticator of mortality insevere sepsis patients. J Crit Care 2010;25:270–275
103. Roongsritong C, Warraich I, Bradley C:Common causes of troponin elevations inthe absence of acute myocardial infarction:Incidence and clinical significance. Chest2004; 125:1877–1884
104. Checchia PA, Moynihan JA, Brown L: Car-diac troponin I as a predictor of mortalityfor pediatric submersion injuries requiringout-of-hospital cardiopulmonary resuscita-tion. Pediatr Emerg Care 2006; 22:222–225
105. Ammann P, Fehr T, Minder EI, et al: Ele-vation of troponin I in sepsis and septicshock. Intensive Care Med 2001; 27:965–969
106. Arlati S, Brenna S, Prencipe L, et al: Myo-cardial necrosis in ICU patients with acutenon-cardiac disease: A prospective study.Intensive Care Med 2000; 26:31–37
107. Mehta NJ, Khan IA, Gupta V, et al: Cardiactroponin I predicts myocardial dysfunctionand adverse outcome in septic shock. IntJ Cardiol 2004; 95:13–17
108. King DA, Codish S, Novack V, et al: The roleof cardiac troponin I as a prognosticator incritically ill medical patients: A prospectiveobservational cohort study. Crit Care 2005;9:R390–R395
109. Landesberg G, Vesselov Y, Einav S, et al:Myocardial ischemia, cardiac troponin, andlong-term survival of high-cardiac risk crit-ically ill intensive care unit patients. CritCare Med 2005; 33:1281–1287
110. Lim W, Qushmaq I, Cook DJ, et al: Elevatedtroponin and myocardial infarction in theintensive care unit: A prospective study.Crit Care 2005; 9:R636–R644
111. Quenot JP, Le Teuff G, Quantin C, et al:Myocardial injury in critically ill patients:Relation to increased cardiac troponin I andhospital mortality. Chest 2005; 128:2758–2764
112. Wu TT, Yuan A, Chen CY, et al: Cardiactroponin I levels are a risk factor for mor-tality and multiple organ failure in noncar-diac critically ill patients and have an addi-tive effect to the APACHE II score inoutcome prediction. Shock 2004; 22:95–101
113. ver Elst KM, Spapen HD, Nguyen DN, et al:Cardiac troponins I and T are biologicalmarkers of left ventricular dysfunction inseptic shock. Clin Chem 2000; 46:650–657
114. Vieillard-Baron A, Caille V, Charron C, et al:Actual incidence of global left ventricularhypokinesia in adult septic shock. Crit CareMed 2008; 36:1701–1706
115. Guest TM, Ramanathan AV, Tuteur PG, etal: Myocardial injury in critically ill pa-tients. A frequently unrecognized complica-tion. JAMA 1995; 273:1945–1949
116. Kollef MH, Ladenson JH, Eisenberg PR:Clinically recognized cardiac dysfunction:An independent determinant of mortalityamong critically ill patients. Is there a rolefor serial measurement of cardiac troponinI? Chest 1997; 111:1340–1347
117. Turner A, Tsamitros M, Bellomo R: Myocar-dial cell injury in septic shock. Crit CareMed 1999; 27:1775–1780
118. Briassoulis G, Narlioglou M, Zavras N, et al:Myocardial injury in meningococcus-induced purpura fulminans in children. In-tensive Care Med 2001; 27:1073–1082
119. Thiru Y, Pathan N, Bignall S, et al: A myo-cardial cytotoxic process is involved in thecardiac dysfunction of meningococcal sep-tic shock. Crit Care Med 2000; 28:2979–2983
120. Moynihan JA, Brown L, Sehra R, et al: Car-diac troponin I as a predictor of respiratoryfailure in children hospitalized with respi-ratory syncytial virus (RSV) infections: Apilot study. Am J Emerg Med 2003; 21:479–482
121. Checchia PA, Appel HJ, Kahn S, et al: Myo-cardial injury in children with respiratorysyncytial virus infection. Pediatr Crit CareMed 2000; 1:146–150
122. deFilippi C, Wasserman S, Rosanio S, et al:Cardiac troponin T and C-reactive proteinfor predicting prognosis, coronary athero-sclerosis, and cardiomyopathy in patientsundergoing long-term hemodialysis. JAMA2003; 290:353–359
123. Clark GL, Robison AK, Gnepp DR, et al:Effects of lymphatic transport of enzyme onplasma creatine kinase time-activity curvesafter myocardial infarction in dogs. Circ Res1978; 43:162–169
124. Klocke FJ, Copley DP, Krawczyk JA, et al:Rapid renal clearance of immunoreactivecanine plasma myoglobin. Circulation1982; 65:1522–1528
125. Mallamaci F, Zoccali C, Parlongo S, et al:Troponin is related to left ventricular massand predicts all-cause and cardiovascularmortality in hemodialysis patients. Am JKidney Dis 2002; 40:68–75
126. Fredericks S, Chang R, Gregson H, et al:Circulating cardiac troponin-T in patientsbefore and after renal transplantation. ClinChim Acta 2001; 310:199–203
127. Ellis K, Dreisbach AW, Lertora JL: Plasmaelimination of cardiac troponin I in end-stage renal disease. South Med J 2001; 94:993–996
128. Davis GK, Labugger R, Van Eyk JE, et al:Cardiac troponin T is not detected in West-ern blots of diseased renal tissue. ClinChem 2001; 47:782–783
129. Khan NA, Hemmelgarn BR, Tonelli M, et al:Prognostic value of troponin T and I amongasymptomatic patients with end-stage renaldisease: A meta-analysis. Circulation 2005;112:3088–3096
130. Adams JE 3rd, Schechtman KB, Landt Y, etal: Comparable detection of acute myocar-dial infarction by creatine kinase MB isoen-zyme and cardiac troponin I. Clin Chem1994; 40:1291–1295
131. Bonnefoy E, Filley S, Kirkorian G, et al:Troponin I, troponin T, or creatine ki-nase-MB to detect perioperative myocardialdamage after coronary artery bypass sur-gery. Chest 1998; 114:482–486
132. Pichon H, Chocron S, Alwan K, et al: Crys-talloid versus cold blood cardioplegia andcardiac troponin I release. Circulation1997; 96:316–320
133. Swaanenburg JC, Loef BG, Volmer M, et al:Creatine kinase MB, troponin I, and tro-ponin T release patterns after coronary ar-tery bypass grafting with or without cardio-pulmonary bypass and after aortic andmitral valve surgery. Clin Chem 2001; 47:584–587
S41Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

134. Immer FF, Stocker F, Seiler AM, et al: Tro-ponin-T: Improved diagnostic assessment ofmyocardial damage in childhood. Acta Pae-diatr 1997; 86:1321–1327
135. Taggart DP, Hadjinikolas L, Wong K, et al:Vulnerability of paediatric myocardium tocardiac surgery. Heart 1996; 76:214–217
136. Fellahi JL, Gue X, Richomme X, et al:Short- and long-term prognostic value ofpostoperative cardiac troponin I concentra-tion in patients undergoing coronary arterybypass grafting. Anesthesiology 2003; 99:270–274
137. Greenson N, Macoviak J, Krishnaswamy P,et al: Usefulness of cardiac troponin I inpatients undergoing open heart surgery.Am Heart J 2001; 141:447–455
138. Koh TW, Hooper J, Kemp M, et al: Intraop-erative release of troponin T in coronaryvenous and arterial blood and its relation torecovery of left ventricular function and ox-idative metabolism following coronary ar-tery surgery. Heart 1998; 80:341–348
139. Nesher N, Alghamdi AA, Singh SK, et al:Troponin after cardiac surgery: A predictoror a phenomenon? Ann Thorac Surg 2008;85:1348–1354
140. Paparella D, Cappabianca G, Visicchio G, etal: Cardiac troponin I release after coronaryartery bypass grafting operation: Effects onoperative and midterm survival. Ann Tho-rac Surg 2005; 80:1758–1764
141. Mildh LH, Pettila V, Sairanen HI, et al:Cardiac troponin T levels for risk stratifica-tion in pediatric open heart surgery. AnnThorac Surg 2006; 82:1643–1648
142. Lipshultz SE, Rifai N, Sallan SE, et al: Pre-dictive value of cardiac troponin T in pedi-atric patients at risk for myocardial injury.Circulation 1997; 96:2641–2648
143. Checchia PA, Backer CL, Bronicki RA, et al:Dexamethasone reduces postoperative tro-ponin levels in children undergoing cardio-pulmonary bypass. Crit Care Med 2003; 31:1742–1745
144. Checchia PA, Bronicki RA, Costello JM, et
al: Steroid use before pediatric cardiac op-erations using cardiopulmonary bypass: Aninternational survey of 36 centers. PediatrCrit Care Med 2005; 6:441–444
145. Maddali MM, Valliattu J, Al Delamie T, et al:Arterial switch operation: Troponin T doesnot predict ventilation requirements. AsianCardiovasc Thorac Ann 2008; 16:274–277
146. Malagon I, Hogenbirk K, van Pelt J, et al:Effect of dexamethasone on postoperativecardiac troponin T production in pediatriccardiac surgery. Intensive Care Med 2005;31:1420–1426
147. Malagon I, Hogenbirk K, van Pelt J, et al:Effect of three different anaesthetic agentson the postoperative production of cardiactroponin T in paediatric cardiac surgery.Br J Anaesth 2005; 94:805–809
148. Nagy ZL, Collins M, Sharpe T, et al: Effect oftwo different bypass techniques on the se-rum troponin-T levels in newborns andchildren: Does pH-Stat provide better pro-tection? Circulation 2003; 108:577–582
S42 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Lactate and acid base as a hemodynamic monitor and markers ofcellular perfusion
Meredith Allen, MB, BS, FRACP, FRCPCH, PhD
Clinical and hemodynamic pa-rameters such as heart rate,blood pressure, toe-core tem-perature difference, urine
output, and central venous pressure areunreliable or late signs of inadequate tis-sue perfusion and hence their use is lim-ited in guiding timely therapy. An idealbiomarker would identify states of dimin-ished cardiac output/oxygen delivery be-fore hemodynamic instability, facilitatingearly therapeutic intervention and im-proving patient outcome.
The intra- and postoperative monitor-ing of lactate, acid-base, and mixed ve-nous oxygenation (SvO2) have been advo-cated in pediatric cardiac critical care assurrogate markers of cardiac output, ox-ygen delivery, and cellular perfusion.
Many clinicians use lactate and base ex-cess routinely as markers of tissue perfu-sion and to assess the effectiveness oftheir intervention. This review discussesthe strengths and weaknesses of usingthese measurements in pediatric cardiaccritical care.
Lactate Shuttle
Lactate (2-hydroxypropanoic acid) wasfirst discovered in 1780 (1) in samples ofsour milk—“lactic”—and first isolatedfrom the blood of two women who diedfrom puerperal fever in 1843 (2).
An intermediary of carbohydrate me-tabolism, lactate is formed from pyruvateby lactate dehydrogenase in the final stepof glycolysis (Fig. 1). Under normal aer-obic conditions, lactate is constantly be-ing produced and consumed (metabo-lized) by cells in the body. The majority oflactate produced (70% to 75%) is con-verted back to pyruvate by oxidation (Fig.2) in the mitochondria with a smallerpercentage (20%) providing the predom-inant precursor for glyconeogenesis. Theproduction (glycolysis), exchange (oxida-tion), and use (gluconeogenesis) of lac-tate within or between cells is known as
the lactate shuttle and believed to repre-sent a form of cell–cell signaling (3).
Normal circulating lactate levels inthe body are �1.5 mmol/L and �2mmol/L in critical illness. It is normallyproduced in skeletal muscle (fast-glyco-lytic type IIB fibers), brain, renal me-dulla, and red blood cells and metabo-lized by the liver (50%), renal cortex(20%), skeletal muscle (slow-oxidativetype I fibers), heart, and brain (4). At veryhigh levels, lactate is actively excreted bythe kidney.
Critical Illness
During critical illness, plasma lactatelevels can be increased by a number ofmechanisms; only some of these repre-sent cellular hypoperfusion (Table 1). Thedistinction between hypoxic or nonhy-poxic production of lactate is critical forthe correct interpretation of lactate val-ues and selection of appropriate ther-apy. Although initially thought to beexclusively the result of tissue hypoxia,hyperlactemia in critical illness mayalso result from reduced lactate clear-ance relative to production during crit-ical illness or accelerated aerobic glyco-
From Paediatric Intensive Care and the SPRinTProgram, Royal Brompton Hospital, London, UK.
The author has not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e3182211aed
Background: The intra- and postoperative monitoring of lac-tate and acid-base has been advocated in pediatric cardiac crit-ical care as surrogate markers of cardiac output, oxygen delivery,and cellular perfusion. Many clinicians use lactate and baseexcess routinely as markers of tissue perfusion and to assess theeffectiveness of their intervention. This review discusses thestrengths and weaknesses of using these measurements in pe-diatric cardiac critical care.
Methodology: A search of MEDLINE, EMBASE, PubMed, and theCochrane Database was conducted to find controlled trials oflactate and base excess. Adult and pediatric data were consid-ered. Guidelines published by the Society of Critical Care Medi-cine, the American Heart Association, the American Academy ofPediatrics, and the International Liaison Committee on Resusci-tation were reviewed including further review of references cited.
Results and Conclusions: Many factors other than tissue hyp-oxia may contribute to hyperlactemia in critical illness. Althoughthe presence of hyperlactemia on admission appears to be asso-
ciated with intensive care unit mortality and morbidity in someretrospective analyses, significant overlap between survivors andnonsurvivors means that nonsurvivors cannot be predicted fromadmission lactate measurement. Persistently elevated postoper-ative lactate is associated with increased morbidity and mortalityin the pediatric cardiac population. To date there is no random-ized control trial of goal-directed therapy in adult or pediatriccardiac care that includes normalization of lactate as a target.Overall equivalent time measurements of base excess, anion gap,and pH have a low predictive value for morbidity and mortality inchildren after cardiac surgery. Lactate is one of a cluster ofmarkers of cellular perfusion and oxygen delivery. Alone, as asingle measurement, it has minimal predictive value and is non-discriminatory for survival. (Pediatr Crit Care Med 2011;12[Suppl.]:S43–S49)
KEY WORDS: lactate; base excess; biomarkers; cardiac output;cell perfusion; oxygenation
S43Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

lysis that exceeds the oxidative capacityof mitochondria (e.g., cytokine or cate-cholamine-driven) (5, 6).
Lactate after cardiopulmonarybypass and cardiac surgery
Although lactate is normally extractedfrom the circulation by the myocardiumas a cellular fuel (7, 8), in the setting ofsurgical trauma, lactate extraction de-creases (9) and production is increased asa result of anaerobic glycolysis.
Lactate release from the infant myo-cardium has been shown to be greaterafter crystalloid cardioplegia comparedwith blood cardioplegia (10).
Studies show a delay of 30–40 minsbetween release of a cross-clamp/reperfu-
sion and reduction in lactate release byheart muscle into the coronary sinus,suggesting that, after ischemia, anaerobiccellular metabolism within the myocar-dium continues for some time (10).
With restoration of blood flow, a“washout” of lactate from regional tissueshas been shown to occur in animal andhuman models, especially from the coro-nary and renal circulations (11, 12). Aparadoxic increase in blood lactate con-centration after the release of the aorticcross-clamp or completion of surgerymay reflect improvement rather than de-terioration of cellular perfusion; however,high or sustained levels of lactate shouldnot be accredited to washout.
Pulmonary lactate levels rise signifi-cantly after exposure to surgical traumaand cardiopulmonary bypass and may con-tribute significantly to circulating lactatelevels up to 6 hrs postoperatively (13,14).Although pulmonary lactate levels have notbeen shown to correlate with cardiopulmo-nary bypass time, a statistically significantcorrelation has been shown between pul-monary lactate release and postoperativealveolar–arterial oxygen gradient (13).
Lactate and cellular hypoxia
Under hypoxic conditions or if the rateof cellular glycolysis exceeds the mito-
chondrial capacity, pyruvate is convertedto lactate in the cytosol (through lactatedehydrogenase) to regenerate NAD� andsupport continued adenosine-5�-triphos-phate regeneration from glycolysis. Al-though less energy-efficient than mito-chondrial respiration, this adaptiveprocess maintains cellular energy (Fig.3). The metabolic acidosis observed withthis process is caused by the increasedcellular reliance on nonmitochondrialadenosine-5�-triphosphate turnover.
An increase in circulating lactate in crit-ically ill patients in the setting of supplydependency may be viewed as a positivefeature indicating the presence of function-ing adaptive metabolic pathways. Withtimely correction of cellular perfusion,there is restoration of mitochondrial respi-ration and minimal cell death is seen inaffected organs. However, if cellular hyp-oxia persists, apoptosis and necrosis occurand organ failure emerges (15, 16). Withcell death, lactate production may ceaseand plasma lactate levels may fall (providedclearance is not impaired).
High circulating levels of lactate canbe divided into two groups according tothe following etiology: 1) type A: in-creased lactate secondary to reduced cel-lular perfusion/hypoxia. Lactate produc-tion is in excess of pyruvate and lactate:pyruvate ratio increases; and 2) type B:conditions that increase the amount oflactate in the blood unrelated to a de-creased availability of oxygen. Pyruvatesynthesis increases in proportion to lac-tate and ratio remains normal (10:1). Incardiac critical care, hyperlactemia maybe the result of a combination of bothtype A and type B etiologies.
Prognostic Significance of EarlyPostoperative Lactate
Protagonists of lactate measurement incritical illness have suggested that lactatelevels reflect the degree of global tissueanoxia, thus acting as a marker of organdamage and eventual outcome. There aremany studies that show an association be-tween plasma lactate levels and subsequentmortality/morbidity in critically ill adults,children, and neonates (16–27). Many ofthese are in the pediatric cardiac popula-tion (20, 23, 28–36).
For lactate to have a practical use dur-ing the early postoperative period, it hasto have a high predictive value. The pos-itive predictive value of a high admissionlactate for postoperative mortality is sup-ported by some single-center retrospec-
Figure 1. Lactate oxidation. Lactate is convertedto pyruvate in the presence of cytosolic or mito-chondrial lactate dehydrogenase by oxidation.
Figure 2. Cellular respiration. Glycolysis is the first part of aerobic (and anaerobic) respiration andtakes part in the cytosol. Lactate is formed from pyruvate in the final step of glycolysis. Thepredominant monocarboxylate entering the mitochondrial intermembrane space is lactate. Entry oflactate and pyruvate into the mitochondrial matrix is facilitated by monocarboxylate transporters.Lactate is then oxidized to pyruvate through mitochondrial lactic dehydrogenase. In the presence ofoxygen, pyruvate enters the Krebs cycle to generate cellular energy by mitochondrial respiration.
S44 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

tive studies (19, 28, 32–35) but not ob-served in others (20, 31, 36, 37). Althoughlow lactate levels are highly predictive ofsurvival (97%), high lactate levels have onlya modest and variable predictive value fornonsurvival (43%) (20).
The limitations of lactate as a predictorreflects the fact that hyperlactemia earlyafter cardiopulmonary bypass may repre-sent intraoperative factors, early postoper-ative tissue oxygen debt, impaired lactateclearance, or a combination of these. Re-duced cardiopulmonary bypass flow (�100mL/kg/min�1) and oxygen delivery (38),duration of bypass and circulatory arrest,temperature, hematocrit during and aftersurgery, and host systemic inflammatoryresponse have all been shown to affect post-operative lactate (20, 30, 31, 39). In addi-tion, increased catecholamines (intrinsicand extrinsic) may increase glycolysis withincreased lactate production beyond the ca-pacity of pyruvate dehydrogenase, indepen-dent of the adequacy of cellular perfusion(type B).
Figure 3. Aerobic vs. anaerobic metabolism. Under hypoxic conditions or if the rate of cellularglycolysis exceeds mitochondrial capacity (e.g., catecholamine/cytokine driven), pyruvate is convertedto lactate via cytosolic lactate dehydrogenase. This regeneration of NAD� enables continued (but lessefficient) adenosine-5-�-triphosphate generation from glycolysis.
Table 1. Mechanism of increased plasma lactate levels in critical illness
Inhibition of mitochondrialrespiration
Anaerobic Hypoxia—systemic (66), regional (67), or microcirculatoryLactate is produced from pyruvate by cells functioning in reduced oxygen conditions provided
cells are supplied with sufficient glucoseInhibition of mitochondrial
respirationAerobic Impaired activity of pyruvate dehydrogenase is seen with sepsis (12, 68–71), thiamine deficiency
(72)Drugs that induce mitochondrial cytopathy or inhibit oxidative phosphorylation
White blood cell production Anaerobic (butnot hypoxic)
White blood cells, when activated by endotoxin, produce large amounts of lactate by anaerobicglycolysis (81)
Although generated by anaerobic metabolism, this increase in lactate is not the result ofhypoxia
In inflammatory processes 3 large amounts of lactate may be produced without tissue hypoxia2 Lactate clearance Aerobic Liver dysfunction (74)
Maturation of liver enzymes may in part explain high lactate concentrations seen in perinatalstudies (72)
Blood lactate levels are normal in very severely impaired liver patients; therefore, productionmust be high in addition to impaired clearance
Cytokine-mediated cellularuptake of glucose
Aerobic Cytokines increase in aerobic glycolysis resulting in levels of pyruvate that exceed the oxidativecapacity of mitochondria (pyruvate dehydrogenase capacity) (75)
1Pyruvate concentration drives lactate production and lactate:pyruvate ratio remains normalCatecholamine stimulated Aerobic Epinephrine increases glycogenolysis, glycolysis and stimulates Na�K�adenosine triphosphatase
membrane ion pump (76,77)Epinephrine has been shown to increase plasma lactate levels under fully aerobic conditions
in healthy control subjects at rest and during exercise (78,79)�oradrenaline does not have these effects (80)
Hyperglycemia Aerobic Hyperglycemia results in increased production of pyruvate through aerobic glycolysis thatexceeds the oxidative capacity of mitochondria (pyruvate dehydrogenase capacity)
Lung production Aerobic Lung has been shown to be an important source of lactate in pulmonary and extrapulmonarydisease (12 � 14,81,82)
Probably reflects a response to inflammatory mediatorsAlkalosis Aerobic Alkalosis increases cellular lactate efflux via the cell membrane H�- linked carrier
mechanism (83)Drugs Nucleoside reverse transcriptase inhibitors
MethanolBiguanides (e.g., metformin)CyanideEthylene-glycol
Incorrect whole bloodprocessing
— Blood not kept on ice or measured immediately may be falsely elevated by in vitro red blood celllactate production
S45Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
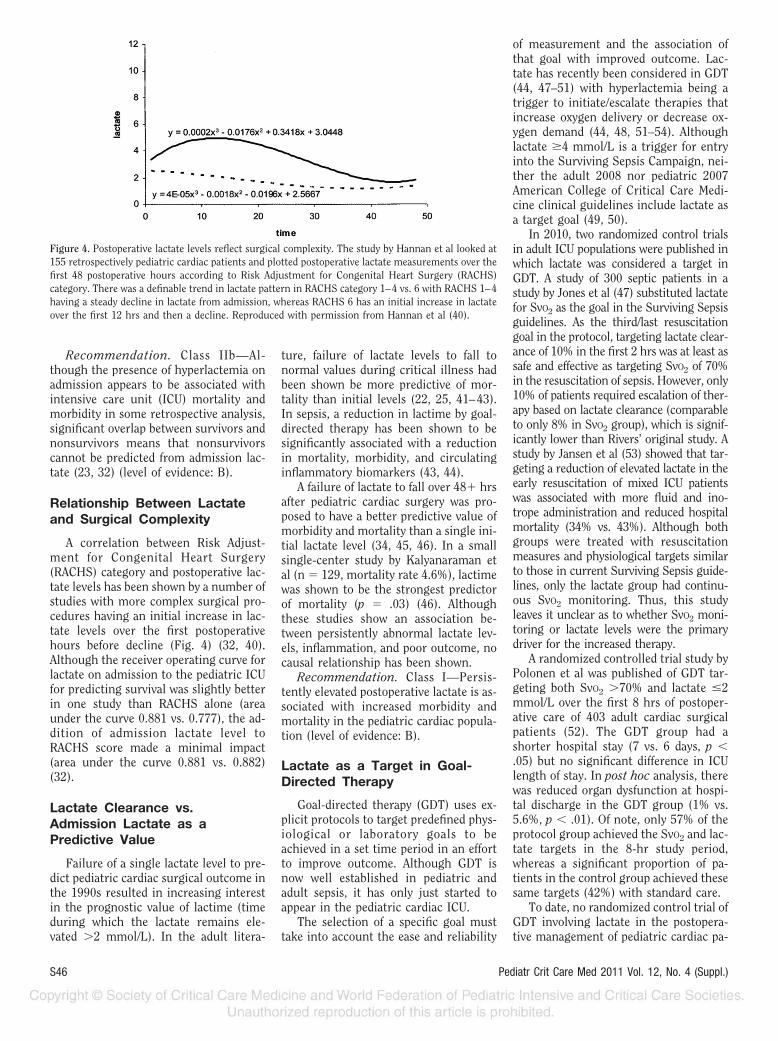
Recommendation. Class IIb—Al-though the presence of hyperlactemia onadmission appears to be associated withintensive care unit (ICU) mortality andmorbidity in some retrospective analysis,significant overlap between survivors andnonsurvivors means that nonsurvivorscannot be predicted from admission lac-tate (23, 32) (level of evidence: B).
Relationship Between Lactateand Surgical Complexity
A correlation between Risk Adjust-ment for Congenital Heart Surgery(RACHS) category and postoperative lac-tate levels has been shown by a number ofstudies with more complex surgical pro-cedures having an initial increase in lac-tate levels over the first postoperativehours before decline (Fig. 4) (32, 40).Although the receiver operating curve forlactate on admission to the pediatric ICUfor predicting survival was slightly betterin one study than RACHS alone (areaunder the curve 0.881 vs. 0.777), the ad-dition of admission lactate level toRACHS score made a minimal impact(area under the curve 0.881 vs. 0.882)(32).
Lactate Clearance vs.Admission Lactate as aPredictive Value
Failure of a single lactate level to pre-dict pediatric cardiac surgical outcome inthe 1990s resulted in increasing interestin the prognostic value of lactime (timeduring which the lactate remains ele-vated �2 mmol/L). In the adult litera-
ture, failure of lactate levels to fall tonormal values during critical illness hadbeen shown be more predictive of mor-tality than initial levels (22, 25, 41–43).In sepsis, a reduction in lactime by goal-directed therapy has been shown to besignificantly associated with a reductionin mortality, morbidity, and circulatinginflammatory biomarkers (43, 44).
A failure of lactate to fall over 48� hrsafter pediatric cardiac surgery was pro-posed to have a better predictive value ofmorbidity and mortality than a single ini-tial lactate level (34, 45, 46). In a smallsingle-center study by Kalyanaraman etal (n � 129, mortality rate 4.6%), lactimewas shown to be the strongest predictorof mortality (p � .03) (46). Althoughthese studies show an association be-tween persistently abnormal lactate lev-els, inflammation, and poor outcome, nocausal relationship has been shown.
Recommendation. Class I—Persis-tently elevated postoperative lactate is as-sociated with increased morbidity andmortality in the pediatric cardiac popula-tion (level of evidence: B).
Lactate as a Target in Goal-Directed Therapy
Goal-directed therapy (GDT) uses ex-plicit protocols to target predefined phys-iological or laboratory goals to beachieved in a set time period in an effortto improve outcome. Although GDT isnow well established in pediatric andadult sepsis, it has only just started toappear in the pediatric cardiac ICU.
The selection of a specific goal musttake into account the ease and reliability
of measurement and the association ofthat goal with improved outcome. Lac-tate has recently been considered in GDT(44, 47–51) with hyperlactemia being atrigger to initiate/escalate therapies thatincrease oxygen delivery or decrease ox-ygen demand (44, 48, 51–54). Althoughlactate �4 mmol/L is a trigger for entryinto the Surviving Sepsis Campaign, nei-ther the adult 2008 nor pediatric 2007American College of Critical Care Medi-cine clinical guidelines include lactate asa target goal (49, 50).
In 2010, two randomized control trialsin adult ICU populations were published inwhich lactate was considered a target inGDT. A study of 300 septic patients in astudy by Jones et al (47) substituted lactatefor SvO2 as the goal in the Surviving Sepsisguidelines. As the third/last resuscitationgoal in the protocol, targeting lactate clear-ance of 10% in the first 2 hrs was at least assafe and effective as targeting SvO2 of 70%in the resuscitation of sepsis. However, only10% of patients required escalation of ther-apy based on lactate clearance (comparableto only 8% in SvO2 group), which is signif-icantly lower than Rivers’ original study. Astudy by Jansen et al (53) showed that tar-geting a reduction of elevated lactate in theearly resuscitation of mixed ICU patientswas associated with more fluid and ino-trope administration and reduced hospitalmortality (34% vs. 43%). Although bothgroups were treated with resuscitationmeasures and physiological targets similarto those in current Surviving Sepsis guide-lines, only the lactate group had continu-ous SvO2 monitoring. Thus, this studyleaves it unclear as to whether SvO2 moni-toring or lactate levels were the primarydriver for the increased therapy.
A randomized controlled trial study byPolonen et al was published of GDT tar-geting both SvO2 �70% and lactate �2mmol/L over the first 8 hrs of postoper-ative care of 403 adult cardiac surgicalpatients (52). The GDT group had ashorter hospital stay (7 vs. 6 days, p �.05) but no significant difference in ICUlength of stay. In post hoc analysis, therewas reduced organ dysfunction at hospi-tal discharge in the GDT group (1% vs.5.6%, p � .01). Of note, only 57% of theprotocol group achieved the SvO2 and lac-tate targets in the 8-hr study period,whereas a significant proportion of pa-tients in the control group achieved thesesame targets (42%) with standard care.
To date, no randomized control trial ofGDT involving lactate in the postopera-tive management of pediatric cardiac pa-
Figure 4. Postoperative lactate levels reflect surgical complexity. The study by Hannan et al looked at155 retrospectively pediatric cardiac patients and plotted postoperative lactate measurements over thefirst 48 postoperative hours according to Risk Adjustment for Congenital Heart Surgery (RACHS)category. There was a definable trend in lactate pattern in RACHS category 1–4 vs. 6 with RACHS 1–4having a steady decline in lactate from admission, whereas RACHS 6 has an initial increase in lactateover the first 12 hrs and then a decline. Reproduced with permission from Hannan et al (40).
S46 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

tients has been undertaken. This may bein part because monitoring of postopera-tive lactate has become embedded in ourdaily practice without prospective proofof clear benefit. A study by Rossi et al in(48) 2005 compared the outcome of 710pediatric cardiac patients (RACHS 1–6)managed with GDT involving lactateagainst a historical cohort (1995�2001).In the GDT group, blood lactate was mea-sured hourly for the first 4–6 hrs in ne-onates and 4 hourly in older children.Escalation of therapy was indicated forpersistently abnormal or rising lactatelevels. Overall mortality was significantlydifferent in the GDT cohort comparedwith historical controls (1.8 vs. 3.7%, p �.02) with the greatest difference seen inthe neonatal group (3.75 vs. 15%, p �.001) and RACHS 4–6 category patients(p � .006). However clinical extrapola-tion from this study should be limited asa result of the use of historical controlsand lack of explicit treatment protocol.
Recommendation. Class IIb—To date,there is no randomized control trial ofGDT in adult or pediatric cardiac carethat includes normalization of lactate as atarget. There are limited data using a his-torical cohort for control that suggest es-calation of ICU therapy in the setting ofpersistently abnormal or rising lactate im-proves mortality in pediatric cardiac criticalcare patients (level of evidence: B).
Relationship Among Lactate,pH, and Base Excess in CriticalIllness
In critical care, plasma lactate, baseexcess, and pH often do not appear to belinked (55, 57–62). Metabolic acidosis isassociated with differing mortality ratesin critical care depending on the etiology(57, 63). Base excess (BE) is a calculatedvalue that estimates the metabolic com-ponent of the blood pH. BE and anion gapreflect lactate levels only in pure lacticacidosis. Renal failure, pre-existing acid-base disorders, decreased albumin levels,and intraoperative administration of bi-carbonate or any other base may alter thespecificity and sensitivity of BE (28). Sig-nificant hyperlactemia and tissue hypo-perfusion can exist despite lack of acido-sis (17, 18). Similarly, many studies haveshown that lactate is responsible for onlya minor component of the metabolic ac-idosis in some critically ill patients (60,64, 65). The weak correlation betweenhyperlactemia and metabolic acidosis
(BE) can, in part, be explained using theStewart’s acid-base classification.
Stewart’s acid-baseclassification
Stewart showed that three indepen-dent variables control pH: strong ion dif-ference, the partial pressure of carbondioxide in blood, and the sum of the weakacids and proteins in the plasma. A raisedvalue for strong ion difference is definedas �3 mEq/L. Lactate is an unmeasuredanion (UMA) in the Stewart equation. Anincreased lactate level reduces strong iondifference, which has an acidifying effect.However, in Stewart’s model, raised lac-tate alone does not necessarily result inmetabolic acidosis because other simul-taneous alterations in UMA, weak acidsand proteins (particularly albumin), orpartial pressure of carbon dioxide inblood can all influence pH (60, 64).
Some authors have looked at UMA andstrong ion difference as alternative mark-ers to lactate as outcome predictors. Con-sidering lactate is an UMA, it is not sur-prising that studies have shown that UMAmake a significant contribution to acido-sis immediately after pediatric cardiacsurgery or that UMA increase with surgi-cal complexity (RACHS) and higher post-operative levels have an association withincreased risk of major adverse eventsand patient death (UMA �6 mEq/L; rela-tive risk of mean absolute error, 2.13[95% confidence interval {CI}, 1.3–3.4])(37, 65). Like lactate, the majority of pa-tients with elevated UMA had uneventfulpostoperative courses and no level ofUMA has been identified above which thepredictive ability is useful. A study byDurwood et al found that admissionstrong ion difference �3.2 mEq/L wasmarginally superior to lactate �3mmol/L or BE �5 mEq/L as a mortalitypredictor (receiver operating curve, 0.85;[95% CI, 0.74–0.95] vs. 0.71 [95% CI,0.44–0.98] and 0.73 [95% CI, 0.43–1],respectively) (64).
Recommendation. Class III—Overallequivalent time measurements of BE, an-ion gap, and pH have a low predictivevalue for morbidity and mortality in chil-dren after cardiac surgery (19, 29) (levelof evidence: B).
CONCLUSION
In pediatric cardiac care, mortality ap-pears to be more closely related to thenature rather than the magnitude (BE) of
a metabolic acidosis. Although hyper-lactemia has been frequently associatedwith metabolic acidosis, this relationshipis not causal. Many factors other thantissue hypoxia may contribute to hyper-lactemia in critical illness. Failing to rec-ognize the correct etiology of hyper-lactemia may result in initiation/escalation of therapies, which mayworsen the hyperlactemia. The presenceor absence of coexisting metabolic acido-sis is important in distinguishing aerobicfrom anaerobic hyperlactemia (39, 65).
Early recognition of hypoxic hyper-lactemia is essential and interventionsdesigned to improve tissue oxygenation(GDT) have been shown to both reducelactime as well as improve morbidity,mortality, and inflammatory biomarkers.Although it might be hypothesized thatreducing duration of hyperlactemia im-proves outcome through minimizingtime of tissue oxygen debt and therebyreduce apoptosis and tissue necrosis, thiscausal relationship has never beenshown.
Perhaps it is too much to ask a singleisolated biochemical measurement topredict the course of a complex criticallyill patient. Lactate is one of a cluster ofmarkers of cellular perfusion and oxygendelivery. Alone, as a single measurement,it has minimal predictive value and isnondiscriminatory for survival.
REFERENCES
1. Robergs RA, Ghiasvand F, Parker D: Bio-chemistry of exercise-induced metabolic ac-idosis. Am J Physiol Regul Integr CompPhysiol 2004; 287:R502–R516
2. Kompanje EJ, Jansen TC, van der HB, et al:The first demonstration of lactic acid in hu-man blood in shock by Johann JosephScherer (1814–1869) in January 1843. Inten-sive Care Med 2007; 33:1967–1971
3. Brooks GA: Cell–cell and intracellular lactateshuttles. J Physiol 2009; 587:5591–5600
4. Bellomo R: Bench-to-bedside review: Lactateand the kidney. Crit Care 2002; 6:322–326
5. Levraut J, Ciebiera JP, Chave S, et al: Mildhyperlactaemia in stable septic patients isdue to impaired lactate clearance rather thanoverproduction. Am J Respir Crit Care Med1998; 157:1021–1026
6. Levraut J, Ichai C, Petit I, et al: Low exoge-nous lactate clearance as an early predictorof mortality in normolactatemic critically illseptic patients. Crit Care Med 2003; 31:705–710
7. Carlsten A, Hallgren B, Jagenburg R, et al:Myocardial metabolism of glucose, lacticacid, amino acids and fatty acids in healthyhuman individuals at rest and at different
S47Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

work loads. Scand J Clin Lab Invest 1961;13:418–428
8. Amark K, Ekroth R, Nilsson K, et al: Myocar-dial substrates in children with congenitalheart disease: Relationship to substrate sup-ply, age, growth and desaturation. Acta Pae-diatr 2007; 96:1677–1680
9. Svensson S, Svedjeholm R, Ekroth R, et al:Trauma metabolism and the heart. Uptake ofsubstrates and effects of insulin early aftercardiac operations. J Thorac CardiovascSurg 1990; 99:1063–1073
10. Amark K, Berggren H, Bjork K, et al: Bloodcardioplegia provides superior protection ininfant cardiac surgery. Ann Thorac Surg2005; 80:989–994
11. Leavy JA, Weil MH, Rackow EC: ‘Lactatewashout’ following circulatory arrest. JAMA1988; 260:662–664
12. De BD: Lactic acidosis. Intensive Care Med2003; 29:699–702
13. Gasparovic H, Plestina S, Sutlic Z, et al:Pulmonary lactate release following cardio-pulmonary bypass. Eur J Cardiothorac Surg2007; 32:882–887
14. Bendjelid K, Treggiari MM, Romand JA:Transpulmonary lactate gradient after hypo-thermic cardiopulmonary bypass. IntensiveCare Med 2004; 30:817–821
15. Azevedo LC: Mitochondrial dysfunction dur-ing sepsis. Endocr Metab Immune DisordDrug Targets 2010; 10:214–223
16. Feinman R, Deitch EA, Watkins AC, et al:HIF-1 mediates pathogenic inflammatory re-sponses to intestinal ischaemia–reperfusioninjury. Am J Physiol Gastrointest LiverPhysiol 2010; 299:G833–843
17. Jeng JC, Jablonski K, Bridgeman A, et al:Serum lactate, not base deficit, rapidly pre-dicts survival after major burns. Burns 2002;28:161–166
18. Husain FA, Martin MJ, Mullenix PS, et al:Serum lactate and base deficit as predictorsof mortality and morbidity. Am J Surg 2003;185:485–491
19. Siegel LB, Dalton HJ, Hertzog JH, et al: Ini-tial postoperative serum lactate levels predictsurvival in children after open heart surgery.Intensive Care Med 1996; 22:1418–1423
20. Cheung PY, Chui N, Joffe AR, et al: Postop-erative lactate concentrations predict theoutcome of infants aged 6 weeks or less afterintracardiac surgery: A cohort follow-up to18 months. J Thorac Cardiovasc Surg 2005;130:837–843
21. Crowl AC, Young JS, Kahler DM, et al: Occulthypoperfusion is associated with increasedmorbidity in patients undergoing early fe-mur fracture fixation. J Trauma 2000; 48:260–267
22. McNelis J, Marini CP, Jurkiewicz A, et al:Prolonged lactate clearance is associatedwith increased mortality in the surgical in-tensive care unit. Am J Surg 2001; 182:481–485
23. Hatherill M, McIntyre AG, Wattie M, et al:Early hyperlactataemia in critically ill chil-dren. Intensive Care Med 2000; 26:314–318
24. Hatherill M, Waggie Z, Purves L, et al: Mor-tality and the nature of metabolic acidosis inchildren with shock. Intensive Care Medicine2003; 29:286–291
25. Bakker J, Gris P, Coffernils M, et al: Serialblood lactate levels can predict the develop-ment of multiple organ failure following sep-tic shock. Am J Surg 1996; 171:221–226
26. Howell MD, Donnino M, Clardy P, et al: Oc-cult hypoperfusion and mortality in patientswith suspected infection. Intensive Care Med2007; 33:1892–1899
27. Lavery RF, Livingston DH, Tortella BJ, et al:The utility of venous lactate to triage injuredpatients in the trauma center. J Am Coll Surg2000; 190:656–664
28. Duke T, Butt W, South M, et al: Early mark-ers of major adverse events in children aftercardiac operations. J Thorac CardiovascSurg 1997; 114:1042–1052
29. Basaran M, Sever K, Kafali E, et al: Serumlactate level has prognostic significance afterpediatric cardiac surgery. J CardiothoracVasc Anesth 2006; 20:43–47
30. Hamamoto M, Uemura H, Imanaka H, et al:Relevance of the measurement of the con-centration of lactate in the serum subse-quent to the Fontan procedure in small chil-dren. Cardiol Young 2006; 16:275–280
31. Munoz R, Laussen PC, Palacio G, et al:Changes in whole blood lactate levels duringcardiopulmonary bypass for surgery for con-genital cardiac disease: An early indicator ofmorbidity and mortality. J Thorac Cardio-vasc Surg 2000; 119:155–162
32. Molina HV, Gonen Y, Vardi A, et al: Bloodlactate levels differ significantly between sur-viving and nonsurviving patients within thesame risk-adjusted classification for congen-ital heart surgery (RACHS-1) group after pe-diatric cardiac surgery. Pediatr Cardiol 2010;31:952–960
33. Shemie SD: Serum lactate predicts postoper-ative complications after pediatric cardiacsurgery. Pediatr Res 1996; 39:54
34. Charpie JR, Dekeon MK, Goldberg CS, et al:Serial blood lactate measurements predictearly outcome after neonatal repair or palli-ation for complex congenital heart disease.J Thorac Cardiovasc Surg 2000; 120:73–80
35. Cheifetz IM, Kern FH, Schulman SR, et al:Serum lactates correlate with mortality afteroperations for complex congenital heart dis-ease. Ann Thorac Surg 1997; 64:735–738
36. Hatherill M, Sajjanhar T, Tibby SM, et al:Serum lactate as a predictor of mortalityafter paediatric cardiac surgery. Arch DisChild 1997; 77:235–238
37. Murray D, Grant D, Murali N, et al: Unmea-sured anions in children after cardiac sur-gery. J Thorac Cardiovasc Surg 2007; 133:235–240
38. Abraham BP, Prodhan P, Jaquiss RD, et al:Cardiopulmonary bypass flow rate: A risk fac-tor for hyperlactatemia after surgical repairof secundum atrial septal defect in children.J Thorac Cardiovasc Surg 2010; 139:170–173
39. Ranucci M, De TB, Isgro G, et al: Hyperlac-tatemia during cardiopulmonary bypass: De-terminants and impact on postoperative out-come. Crit Care 2006; 10:R167
40. Hannan RL, Ybarra MA, White JA, et al: Pat-terns of lactate values after congenital heartsurgery and timing of cardiopulmonary sup-port. Ann Thorac Surg 2005; 80:1468–1473
41. Meregalli A, Oliveira RP, Friedman G: Occulthypoperfusion is associated with increasedmortality in hemodynamically stable, high-risk, surgical patients. Crit Care 2004;8:R60–R65
42. Vincent JL, Dufaye P, Berre J, et al: Seriallactate determinations during circulatoryshock. Crit Care Med 1983; 11:449–451
43. Nguyen HB, Loomba M, Yang JJ, et al: Earlylactate clearance is associated with biomark-ers of inflammation, coagulation, apoptosis,organ dysfunction and mortality in severesepsis and septic shock. J Inflamm (Lond)2010; 7:6
44. Rivers E, Nguyen B, Havstad S, et al: Earlygoal-directed therapy in the treatment of se-vere sepsis and septic shock. N Engl J Med2001; 345:1368–1377
45. Robertson CM, Joffe AR, Sauve RS, et al:Outcomes from an interprovincial programof newborn open heart surgery. J Pediatr2004; 144:86–92
46. Kalyanaraman M, DeCampli WM, CampbellAI, et al: Serial blood lactate levels as a pre-dictor of mortality in children after cardio-pulmonary bypass surgery. Pediatr Crit CareMed 2008; 9:285–288
47. Jones AE, Shapiro NI, Trzeciak S, et al: Lac-tate clearance vs central venous oxygen sat-uration as goals of early sepsis therapy: Arandomized clinical trial. JAMA 2010; 303:739–746
48. Rossi AF, Khan DM, Hannan R, et al: Goal-directed medical therapy and point-of-caretesting improve outcomes after congenitalheart surgery. Intensive Care Med 2005; 31:98–104
49. Dellinger RP, Levy MM, Carlet JM, et al:Surviving Sepsis Campaign: Internationalguidelines for management of severe sepsisand septic shock: 2008. Crit Care Med 2008;36:296–327
50. Brierley J, Carcillo JA, Choong K, et al: Clin-ical practice parameters for hemodynamicsupport of pediatric and neonatal septicshock: 2007 update from the American Col-lege of Critical Care Medicine. Crit Care Med2009; 37:666–688
51. Blow O, Magliore L, Claridge JA, et al: Thegolden hour and the silver day: Detectionand correction of occult hypoperfusionwithin 24 hours improves outcome from ma-jor trauma. J Trauma 1999; 47:964–969
52. Polonen P, Ruokonen E, Hippelainen M, etal: A prospective, randomized study of goal-oriented hemodynamic therapy in cardiacsurgical patients. Anesth Analg 2000; 90:1052–1059
53. Jansen TC, van Bommel J, SchoonderbeekFJ, et al: Early lactate-guided therapy in in-
S48 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

tensive care unit patients. Am J Respir CritCare Med 2010; 182:752–761
54. Kern JW, Shoemaker WC: Meta-analysis ofhemodynamic optimization in high-risk pa-tients. Crit Care Med 2002; 30:1686–1692
55. Aduen J, Bernstein WK, Miller J, et al: Rela-tionship between blood lactate concentra-tions and ionized calcium, glucose, and acid-base status in critically ill and noncriticallyill patients. Crit Care Med 1995; 23:245–252
56. Brill SA, Stewart TR, Brundage SI, et al: Basedeficit does not predict mortality when sec-ondary to hyperchloremic acidosis. Shock2002; 17:459–462
57. Balasubramanyan N, Havens PL, HoffmanGM: Unmeasured anions identified by theFencl-Stewart method predict mortality bet-ter than base excess, anion gap, and lactate inpatients in the pediatric intensive care unit.Crit Care Med 1999; 27:1577–1581
58. Martin MJ, FitzSullivan E, Salim A, et al:Discordance between lactate and base deficitin the surgical intensive care unit: Whichone do you trust? Am J Surg 2006; 191:625–630
59. Maciel AT, Park M: Unmeasured anions ac-count for most of the metabolic acidosis inpatients with hyperlactatemia. Clinics (SaoPaulo) 2007; 62:55–62
60. Deshpande SA, Platt MP: Association be-tween blood lactate and acid-base status andmortality in ventilated babies. Arch Dis ChildFetal Neonatal Ed 1997; 76:F15–F20
61. Rocktaeschel J, Morimatsu H, Uchino S, etal: Unmeasured anions in critically ill pa-tients: Can they predict mortality? Crit CareMed 2003; 31:2131–2136
62. Gunnerson KJ, Saul M, He S, et al: Lactateversus non-lactate metabolic acidosis: A ret-rospective outcome evaluation of critically illpatients. Crit Care 2006; 10:R22
63. Murray DM, Olhsson V, Fraser JI: Definingacidosis in postoperative cardiac patients us-
ing Stewart’s method of strong ion differ-ence. Pediatr Crit Care Med 2004; 5:240–245
64. Durward A, Tibby SM, Skellett S, et al: Thestrong ion gap predicts mortality in childrenfollowing cardiopulmonary bypass surgery.Pediatr Crit Care Med 2005; 6:281–285
65. Handy J: The origin and interpretation ofhyperlactataemia during low oxygen deliverystates. Crit Care 2007; 11:104
66. Ronco JJ, Fenwick JC, Tweeddale MG, et al:Identification of the critical oxygen deliveryfor anaerobic metabolism in critically ill sep-tic and nonseptic humans. JAMA 1993; 270:1724–1730
67. Astiz ME, Rackow EC, Kaufman B, et al:Relationship of oxygen delivery and mixedvenous oxygenation to lactic acidosis in pa-tients with sepsis and acute myocardial in-farction. Crit Care Med 1988; 16:655–658
68. Brealey D, Brand M, Hargreaves I, et al: As-sociation between mitochondrial dysfunctionand severity and outcome of septic shock.Lancet 2002; 360:219–223
69. Exline MC, Crouser ED: Mitochondrialmechanisms of sepsis-induced organ failure.Front Biosci 2008; 13:5030–5041
70. Crouser ED, Julian MW, Blaho DV, et al:Endotoxin-induced mitochondrial damagecorrelates with impaired respiratory activity.Crit Care Med 2002; 30:276–284
71. Fredriksson K, Hammarqvist F, Strigard K,et al: Derangements in mitochondrial metab-olism in intercostal and leg muscle of criti-cally ill patients with sepsis-induced multipleorgan failure. Am J Physiol EndocrinolMetab 2006; 291:E1044–E1050
72. Madl C, Kranz A, Liebisch B, et al: Lacticacidosis in thiamine deficiency. Clin Nutr1993; 12:108–111
73. Mustafa I, Roth H, Hanafiah A, et al: Effect ofcardiopulmonary bypass on lactate metabo-lism. Intensive Care Med 2003; 29:1279–1285
74. Saugstad OD: Is lactate a reliable indicator oftissue hypoxia in the neonatal period? ActaPaediatr 2002; 91:17–19
75. Haji-Michael PG, Ladriere L, Sener A, et al:Leukocyte glycolysis and lactate output inanimal sepsis and ex vivo human blood.Metabolism 1999; 48:779–785
76. Levy B, Mansart A, Bollaert PE, et al: Effectsof epinephrine and norepinephrine on hemo-dynamics, oxidative metabolism, and organenergetics in endotoxemic rats. IntensiveCare Med 2003; 29:292–300
77. Levy B, Gibot S, Franck P, et al: Relationbetween muscle Na�K� ATPase activity andraised lactate concentrations in septic shock:A prospective study. Lancet 2005; 365:871–875
78. Mazzeo RS, Marshall P: Influence of plasmacatecholamines on the lactate threshold dur-ing graded exercise. J Appl Physiol 1989;67:1319–1322
79. Clutter WE, Bier DM, Shah SD, et al: Epi-nephrine plasma metabolic clearance ratesand physiologic thresholds for metabolic andhemodynamic actions in man. J Clin Invest1980; 66:94–101
80. Ensinger H, Geisser W, Brinkmann A, et al:Metabolic effects of norepinephrine and do-butamine in healthy volunteers. Shock 2002;18:495–500
81. De BD, Creteur J, Zhang H, et al: Lactateproduction by the lungs in acute lung injury.Am J Respir Crit Care Med 1997; 156:1099–1104
82. Routsi C, Bardouniotou H, Ivoria-IoannidouV, et al: Pulmonary lactate release in patientswith acute lung injury is not attributable tolung tissue hypoxia. Crit Care Med 1999;27:2469–2473
83. Druml W, Grimm G, Laggner AN, et al: Lac-tic acid kinetics in respiratory alkalosis. CritCare Med 1991; 19:1120–1124
S49Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Echocardiography as a hemodynamic monitor in critically illchildren
Darren Klugman, MD, MMS; John T. Berger, MD
Echocardiography is a modalityoften utilized for the assess-ment of myocardial functionin the pediatric intensive care
unit (ICU) due to its widespread availabil-ity, ability to be performed at the bedside,and its noninvasiveness. Further, simpleassessments of pericardial fluid and myo-cardial function can be performed bynoncardiologists (1). While echocardiog-raphy provides excellent informationabout valvar and other structural abnor-malities in children with acquired or con-genital heart disease (CHD), and has be-come the diagnostic test of choice inpediatric cardiology, its use for the ongo-ing assessment of cardiac function hasless utility. In the pediatric or cardiacICU, many of the factors influencing car-diac performance are dynamic and thusnot tracked well by intermittent echocar-diograms. Other limitations include theneed for echocardiographic expertise toanswer complex questions relating tostructure and function, inadequate
acoustic windows, and misinterpretation.Despite its limitations as a real-timemonitor, echocardiography remains animportant tool to diagnose the presenceand etiologies of myocardial dysfunctionin critically ill children. The purpose ofthis manuscript is to examine the scien-tific evidence for the use of echocardiog-raphy as a hemodynamic monitoring toolin pediatric critical care.
Two-DimensionalEchocardiography
Many standard two-dimensional echo-cardiography (2DE) techniques are usedto assess ventricular function. The termventricular function is often used inter-changeably to describe both contractilityand global myocardial performance; how-ever, these two terms are not synony-mous. Contractility is the shortening ofsarcomeres, a load-independent measureof myocardial performance, and is onlyindirectly assessed by echocardiography.Global myocardial performance is influ-enced by preload, afterload, heart rate,and contractility. While 2DE can over orunderestimate contractility due to fre-quent changes in a patient’s preload, af-terload, heart rate, and contractility, 2DEcan be useful as a diagnostic tool to assessetiologies of cardiac dysfunction, such ashypovolemia, pulmonary hypertension,and structural heart disease (2, 3) (Table1). The most frequently used parametersto assess systolic function are the ejectionphase indices fractional shortening (FS)and ejection fraction (EF).
FS and EF
FS and EF are two echocardiographicmeasures of stroke volume. FS is deter-mined using the parasternal short-axisview and is calculated using the end-diastolic dimension (EDD) and end-systolic dimension of the ventricle withthe equation: FS � (EDD � end-systolicdimension)/EDD. Measurements aremade using M-mode along a line from theintraventricular septum to the inferolat-eral wall at the level of the papillary mus-cles. The advantages of this techniqueinclude the interobserver reliability andease of performance. Since the measure-ment is made along a single line, regionalabnormalities, such as septal dyskinesisand arrhythmias, will greatly affect themeasurement. Loading conditions, i.e.,preload and afterload, will also affect FS.Increased preload will increase the EDD,falsely elevating FS, while increased af-terload will alter systolic dimensions andtherefore result in a decreased FS. Aspreload increases, the EDD will increaseand potentially increase the FS; however,this does not reflect any positive or neg-ative alteration in intrinsic myocardialfunction. Further, an increase in after-load may cause early closure of the aorticvalve, thus altering end-systolic dimen-sion and falsely decreasing the EF.
Echocardiographic assessment in sep-tic shock has demonstrated myocardialdysfunction (2, 4, 5) similar to that whichhas been shown with more invasive mea-sures (6), and may be useful in patientswith septic shock whose management of-
From the Department of Critical Care Medicine andCardiology, Children’s National Medical Center, Wash-ington, DC; and Department of Pediatrics, The GeorgeWashington University School of Medicine, Washing-ton, DC.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e3182211c17
Echocardiography is a widely used modality to assess myo-cardial structure and function in pediatric intensive care settings.While the use of echocardiography for diagnostic purposes re-mains important, its use as a hemodynamic monitoring tool hasnot been well established. The benefits of echocardiography arein its widespread availability, relative ease of use, and importancein diagnosing structural disease and simple changes in myocar-dial function. However, echocardiography in pediatric critical careis limited in its use because it requires the acquisition of quality
images and the accurate interpretation of the study. To date, theliterature on echocardiography in pediatric critical care is limited.The purpose of this review is to examine the scientific evidencefor the usefulness of echocardiography as a hemodynamic mon-itoring tool in pediatric critical care. (Pediatr Crit Care Med 2011;12[Suppl.]:S50–S54)
KEY WORDS: cardiac function; Doppler imaging; echocardiogra-phy; hemodynamic monitoring
S50 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

ten includes manipulation of preloadand afterload. FS has also been shownto correlate well with alterations inventricular function related to varia-tions in preload following the arterialswitch operation (7, 8).
EF is an echocardiographic determi-nation of stroke volume and can be per-formed using 2DE, M-mode, or three-dimensional echocardiography (3DE).The standard echocardiographic view uti-lized for determination of EF is per-formed in the apical four- or two-chambered view. The recommendedmethod for this calculation is the Simp-son or modified Simpson method (9),which divides the left ventricle into cyl-inders, or disks, and uses the radius andlength of the multiple disks measured tocalculate a left ventricle volume. Mea-surements are derived by tracing the leftventricular endomyocardial surface atend diastole and end systole. Limitationsof this method include: dependence on anelliptical or bullet-shaped chamber (lim-iting its use to assessments of the leftventricle only), optimal delineation of theendocardial-blood interface, and poten-tial foreshortening of the left ventriclelength. Further, in children with highheart rates, the echocardiogram may notcapture the true ends of the cardiac cycle.Despite these limitations, images for EFare easy to acquire and EF accounts forregional wall motion abnormalities.
The clinical utility of EF in pediatricshas been established in multiple studies.EF has been used to assess ventricularfunction immediately following cardio-pulmonary bypass, and has correlatedwell with invasive measures of functionlongitudinally (10–13). In addition, EFhas been shown to correlate with cellularmarkers of myocardial injury in childrenwith septic shock (5).
Due to ease of image acquisition andwide availability, EF and FS should becalculated when assessing baseline leftventricular function (9). However, be-cause of dependence on loading condi-tions, influence of ventricular geometry,
and reliance on angle of acquisition,these measurements should not be usedas absolute values. Rather, FS and EFshould be interpreted with respect to theclinical condition of the patient and arebest used to follow physiologic changesover time.
Velocity of circumferential fibershortening
Velocity of circumferential fiber short-ening (VCF) is measured during systolicejection, the only time fiber shorteningoccurs during the cardiac cycle, using theformula: VCF � %FS/ejection time.When corrected for heart rate, the vari-able is termed VCFc, and is preload inde-pendent (14). Small single-center studieshave investigated changes in VCFc inchildren following repair of CHD andhave demonstrated decreases in VCFc,which likely reflect known myocardial de-pression following cardiopulmonary by-pass (7, 8). Further, in pediatric septicshock, VCFc has been shown to reflectalterations in cellular dysfunction (5) andloading conditions (2, 15).
VCFc is easily performed on standardechocardiographic images and is preloadindependent, making it preferable to EFand FS in the critical care setting.
Tissue Doppler Imaging
Tissue Doppler imaging (TDI) allowsfor a quantitative assessment of regionaland global myocardial function by detect-ing regional changes in myocardial defor-mation based on tissue velocities (16).Myocardial deformation is described bystrain and strain rate. Strain representsthe percent change in the length of asegment of myocardium, and strain rate,the speed at which it occurs. Myocardialdeformation has been shown to correlatewell with global and regional ventricularcontractility in animals (17, 18) and hu-mans (19). TDI is also extremely valuablein assessing diastolic function. Becausethe myocardium shortens most in a lon-gitudinal plane, TDI is optimally acquiredfrom the apical two- or four-chamberview. During the cardiac cycle, the atrio-ventricular valve moves toward and awayfrom the apex during systole and diastole,respectively, and there is limited lateralmotion of the ventricular myocardium,making these views ideal to assess longi-tudinal annular velocities of the atrioven-tricular valve. Two methods of TDI areavailable: pulsed-wave TDI and colorDoppler myocardial imaging. Pulsed-wave Doppler interrogation is performedof the myocardium rather than on bloodflow. The ultrasound beam is aligned par-
Figure 1. Pulsed tissue Doppler mitral annulus. This typical tracing of the mitral annular velocityshows the measurements that can be obtained. Ea represents mitral velocity in early diastole and Aais the mitral velocity during atrial contraction. The S wave is the mitral velocity during early systole.Its presence above the baseline indicates its reflection into the left atrium during ventricular systole.Isovolumic relaxation (IR) and contraction (IC) times are also shown. IR is from the end of the S waveto the onset of the Ea wave, and IC is from the end of atrial contraction to the onset of systolic velocity.
Table 1. Diagnoses identifiable withechocardiography
HypovolemiaInfarctsDilated Cardiomyopathy/MyocarditisPericardial DiseasePulmonary Hypertension/Acute Right Heart
FailureStructural/Congenital Disease
S51Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

allel to the myocardium, and a Dopplerinterrogation of a small segment of myo-cardium or atrioventricular valve annu-lus is obtained. A velocity waveform isgenerated, which is the peak instanta-neous velocity of that segment through-out the cardiac cycle (Fig. 1). While thespatial resolution of this modality is poor,the temporal resolution is high, allowingfor the evaluation of brief events, such asisovolumic contraction during systoleand isovolumic relaxation during dias-tole.
In children, TDI is useful because it isindependent of ventricular geometry andis easily obtained with limited training.However, like all Doppler techniques, TDIis highly dependent on the angle of in-sonation. TDI has been shown to accu-rately detect transient changes in rightand left ventricular function in childrenundergoing percutaneous device closureof atrial septal defects (20). Further, in aheterogeneous group of children follow-ing cardiopulmonary bypass, TDI accu-rately reflects alterations in myocardial
performance across a range of congenitalheart defects (21). Others have shownthat postoperative changes in TDI-derived indices correlate with myocardialinjury and duration of postoperative ven-tilator days (22). In a single-center trial,TDI was shown to be useful to followventricular parameters in patients withsingle right ventricles through the firsttwo stages of palliation (23). Longitudinalassessment of changes in ventricular sys-tolic and diastolic performance is alsopossible with TDI, as shown in studies ofpatients with repaired tetralogy of Fallot(24,25), transposition of the great vessels(26), and palliated single ventricles (27).TDI has also been shown to demonstratesignificant changes in myocardial func-tion in the immediate post-transplant pe-riod (28) and has demonstrated utility indetecting early graft failure (29). In thepostoperative and post-transplant period,TDI is a reliable tool to assess myocardialfunction, and can be used to trend alter-ations in myocardial function.
Two-dimensional strainechocardiography
During the cardiac cycle, the heartcontracts and relaxes in multiple planes,and also has a subtle twisting motion.Two-dimensional strain echocardiogra-phy (2DSE) tracks myocardial movementin these planes throughout the cardiaccycle. Tracings of the ventricular endo-cardial and epicardial surface in the api-cal four-chamber and short-axis views al-low for tracking alterations in velocityand deformation of single myocardialpoints on the endocardial surface to at-tain data on strain and strain rate com-parable to TDI (30, 31) (Fig. 2). 2DSE’sadvantages over TDI include angle inde-pendence, shorter postprocessing time,better reproducibility, and technical ease.Disadvantages of 2DSE compared to TDIinclude lower temporal resolution athigher heart rates and undersampling inpatients with poor acoustic windows.2DSE has been validated against mag-netic resonance imaging as a measure of
Figure 2. Two-dimensional strain echocardiography (2SDE). This tracing of 2DSE shows the ability to track alterations in myocardial strain. Global andregional measurements of strain are calculated and differentiated by color coding.
S52 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

myocardial function in human and ani-mal models (32, 33), and is superior toTDI inasmuch as it is unaffected by angleof acquisition.
Investigations of myocardial functionin the intensive care setting using 2DSEare limited. The need for manual postac-quisition data processing, technical diffi-culties of data acquisition, and variabilityin data between vendor packages havelimited the use of this method for real-time assessment of cardiac function (34).As a result, further research is needed tomake 2DSE a useful diagnostic tool in thepediatric critical care setting.
3DE
3DE allows acquisition of images in apyramidal set, which allows for multi-plane acquisition. Multiple plane imageacquisition provides significant improve-ment in resolution, which is particularadvantageous in patients with CHD: im-proved quantification of left and rightventricular mass/volumes (35, 36), valveassessment (37, 38), and guidance of sur-gical and catheter-based procedures. Fur-thermore, magnetic resonance imagingis superior to standard 2DE for the as-sessment of the right ventricle in patientswith CHD disease (39), and 3DE corre-lates well with magnetic resonance imag-ing assessment of right ventricular vol-umes and function (40–42). Images canbe processed in real time (43) or pro-cessed postacquisition.
Currently, there is limited research onthe utility of 3DE to assess cardiac outputin the pediatric ICU in children with orwithout congenital or acquired heart dis-ease. However, there are multiple studiesdemonstrating the utility of 3DE for thelongitudinal assessment of children withCHD (40, 42, 44). In a single-center trialof transesophageal 3DE in a CHD center,Baker et al (45) demonstrated the feasi-bility and utility of 3DE in the catheter-ization laboratory, the ICU, and operatingroom.
3DE is particularly useful in pediatricsfor the assessment of valve structure andfunction, and right and left ventricularvolumes and indices. Recent studies ofthe use of real-time 3DE in the cardiaccatheterization lab and operating roomsupport its continued use in these clinicalsettings. Additional research is needed inthe critical care setting to advance theuse of 3DE for children with and withoutheart disease.
Conclusion
The role of echocardiography in theICU is invaluable. Echocardiography isnoninvasive, portable, and widely avail-able as a diagnostic tool, particularly toassess structural/mechanical causes of al-terations in cardiac function and cardiacoutput. As a result, the echocardio-graphic assessment of myocardial func-tion in the ICU should remain a mainstayof clinical practice. The strength of echo-cardiography lies in its qualitative ratherthan quantitative assessment of the myo-cardium. When assessing cardiac func-tion in the ICU, one must answer threefundamental questions: 1) What is thecardiac function? 2) Is the cardiac func-tion normal for this clinical scenario?3) If the cardiac function is abnormal,why? Echocardiography is a very effectivetool to assist in answering the third ques-tion of why the cardiac function is abnor-mal; however, it only intermittently an-swers the question of cardiac function,thus limiting its utility as a hemody-namic monitor. For example, echocardi-ography is irreplaceable in the care ofchildren with CHD as a diagnostic toolbefore the surgical repair and to assessalterations in postoperative cardiac func-tion, which may result following thesurgical intervention. Further, in thehemodynamically unstable child, echo-cardiography can often provide assess-ment of preload and systolic functionnecessary to make informed manage-ment decisions.
The current evidence of echocardiog-raphy as a hemodynamic monitoring de-vice in critically ill children is consistentwith class II recommendations accordingthe American Heart Association and theAmerican College of Cardiology TaskForce on Practice Guidelines. The totalbody of evidence in pediatrics for the useof echocardiography as a hemodynamicmonitor has not been widely studied,with randomized controlled trials placingthe level of evidence at C. There are,however, notable exceptions when echo-cardiography must be performed: the di-agnosis of CHD, the hemodynamicallyunstable child without definitive etiologyor unresponsive to routine resuscitation,the postoperative patient with CHD andsuspected residual/new intracardiacshunts or hemodynamic instability, andthe child with suspected new structuralheart disease (i.e., tamponade, myocar-dial infarction, and cardiomyopathy).Newer modalities such as 3DE and 2DSE
remain limited in their use in the ICU,and additional research is needed toprove the viability of these modalities.
REFERENCES
1. Spurney CF, Sable CA, Berger JT, et al: Use ofa hand-carried ultrasound device by criticalcare physicians for the diagnosis of pericar-dial effusions, decreased cardiac function,and left ventricular enlargement in pediatricpatients. J Am Soc Echocardiogr 2005; 18:313–319
2. Feltes TF, Pignatelli R, Kleinert S, et al:Quantitated left ventricular systolic mechan-ics in children with septic shock utilizingnoninvasive wall-stress analysis. Crit CareMed 1994; 22:1647–1658
3. Rychik J, Jacobs ML, Norwood WI Jr: Acutechanges in left ventricular geometry aftervolume reduction operation. Ann ThoracSurg 1995; 60:1267–1273; discussion 1274
4. Knoester H, Sol JJ, Ramsodit P, et al: Cardiacfunction in pediatric septic shock survivors.Arch Pediatr Adolesc Med 2008; 162:1164–1168
5. Fenton KE, Sable CA, Bell MJ, et al: Increasesin serum levels of troponin I are associatedwith cardiac dysfunction and disease severityin pediatric patients with septic shock. Pedi-atr Crit Care Med 2004; 5:533–538
6. Pollack MM, Fields AI, Ruttimann UE: Dis-tributions of cardiopulmonary variables inpediatric survivors and nonsurvivors of sep-tic shock. Crit Care Med 1985; 13:454–459
7. Bryant RM, Shirley RL, Ott DA, et al: Leftventricular performance following the arte-rial switch operation: Use of noninvasive wallstress analysis in the postoperative period.Crit Care Med 1998; 26:926–932
8. Colan SD, Boutin C, Castaneda AR, et al:Status of the left ventricle after arterialswitch operation for transposition of thegreat arteries. Hemodynamic and echocar-diographic evaluation. J Thorac CardiovascSurg 1995; 109:311–321
9. Lopez L, Colan SD, Frommelt PC, et al: Rec-ommendations for quantification methodsduring the performance of a pediatric echo-cardiogram: A report from the Pediatric Mea-surements Writing Group of the AmericanSociety of Echocardiography Pediatric andCongenital Heart Disease Council. J Am SocEchocardiogr 2010; 23:465– 495; quiz576–577
10. Di Donato RM, Wernovsky G, Walsh EP, et al:Results of the arterial switch operation fortransposition of the great arteries with ven-tricular septal defect. Surgical consider-ations and midterm follow-up data. Circula-tion 1989; 80:1689–1705
11. Elkins RC, Knott-Craig CJ, Ahn JH, et al:Ventricular function after the arterial switchoperation for transposition of the great ar-teries. Ann Thorac Surg 1994; 57:826–831
12. Okuda H, Nakazawa M, Imai Y, et al: Com-parison of ventricular function after Senning
S53Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

and Jatene procedures for complete transpo-sition of the great arteries. Am J Cardiol1985; 55:530–534
13. Colan SD, Trowitzsch E, Wernovsky G, et al:Myocardial performance after arterial switchoperation for transposition of the great ar-teries with intact ventricular septum. Circu-lation 1988; 78:132–141
14. Colan SD, Borow KM, Neumann A: Left ven-tricular end-systolic wall stress-velocity offiber shortening relation: A load-independentindex of myocardial contractility. J Am CollCardiol 1984; 4:715–724
15. Courand JA, Marshall J, Chang Y, et al: Clin-ical applications of wall-stress analysis in thepediatric intensive care unit. Crit Care Med2001; 29:526–533
16. Sutherland GR, Di Salvo G, Claus P, et al:Strain and strain rate imaging: A new clinicalapproach to quantifying regional myocardialfunction. J Am Soc Echocardiogr 2004; 17:788–802
17. Gorcsan J 3rd, Strum DP, Mandarino WA, etal: Quantitative assessment of alterations inregional left ventricular contractility withcolor-coded tissue Doppler echocardiogra-phy. Comparison with sonomicrometry andpressure-volume relations. Circulation 1997;95:2423–2433
18. Greenberg NL, Firstenberg MS, Castro PL, etal: Doppler-derived myocardial systolic strainrate is a strong index of left ventricular con-tractility. Circulation 2002; 105:99–105
19. Herbots L, Maes F, D’hooge J, et al: Quanti-fying myocardial deformation throughoutthe cardiac cycle: A comparison of ultra-sound strain rate, grey-scale M-mode andmagnetic resonance imaging. UltrasoundMed Biol 2004; 30:591–598
20. Pauliks LB, Chan KC, Chang D, et al: Re-gional myocardial velocities and isovolumiccontraction acceleration before and after de-vice closure of atrial septal defects: A colortissue Doppler study. Am Heart J 2005; 150:294–301
21. Cheung MM, Smallhorn JF, Vogel M, et al:Disruption of the ventricular myocardialforce-frequency relationship after cardiacsurgery in children: Noninvasive assessmentby means of tissue Doppler imaging. J Tho-rac Cardiovasc Surg 2006; 131:625–631
22. Vassalos A, Lilley S, Young D, et al: TissueDoppler imaging following paediatric cardiacsurgery: Early patterns of change and rela-tionship to outcome. Interact CardiovascThorac Surg 2009; 9:173–177
23. Frommelt PC, Sheridan DC, Mussatto KA, etal: Effect of shunt type on echocardiographicindices after initial palliations for hypoplasticleft heart syndrome: Blalock-Taussig shuntversus right ventricle-pulmonary artery con-duit. J Am Soc Echocardiogr 2007; 20:1364–1373
24. Vogel M, Sponring J, Cullen S, et al: Regionalwall motion and abnormalities of electricaldepolarization and repolarization in patientsafter surgical repair of tetralogy of Fallot.Circulation 2001; 103:1669–1673
25. Harada K, Toyono M, Yamamoto F: Assess-ment of right ventricular function duringexercise with quantitative Doppler tissue im-aging in children late after repair of tetralogyof Fallot. J Am Soc Echocardiogr 2004; 17:863–869
26. Vogel M, Derrick G, White PA, et al: Systemicventricular function in patients with trans-position of the great arteries after atrial re-pair: A tissue Doppler and conductance cath-eter study. J Am Coll Cardiol 2004; 43:100–106
27. Hershenson JA, Zaidi AN, Texter KM, et al:Differences in tissue Doppler imaging be-tween single ventricles after the fontan op-eration and normal controls. Am J Cardiol2010; 106:99–103
28. Mahle WT, Cardis BM, Ketchum D, et al:Reduction in initial ventricular systolic anddiastolic velocities after heart transplanta-tion in children: Improvement over timeidentified by tissue Doppler imaging. J HeartLung Transplant 2006; 25:1290–1296
29. Fyfe DA, Ketchum D, Lewis R, et al: TissueDoppler imaging detects severely abnormalmyocardial velocities that identify childrenwith pre-terminal cardiac graft failure afterheart transplantation. J Heart Lung Trans-plant 2006; 25:510–517
30. D’hooge J, Heimdal A, Jamal F, et al: Re-gional strain and strain rate measurementsby cardiac ultrasound: Principles, implemen-tation and limitations. Eur J Echocardiogr2000; 1:154–170
31. Helle-Valle T, Crosby J, Edvardsen T, et al:New noninvasive method for assessment ofleft ventricular rotation: Speckle trackingechocardiography. Circulation 2005; 112:3149–3156
32. Amundsen BH, Helle-Valle T, Edvardsen T, etal: Noninvasive myocardial strain measure-ment by speckle tracking echocardiography:Validation against sonomicrometry andtagged magnetic resonance imaging. J AmColl Cardiol 2006; 47:789–793
33. Marwick TH, Leano RL, Brown J, et al: Myo-cardial strain measurement with 2-dimen-sional speckle-tracking echocardiography:Definition of normal range. JACC CardiovascImaging 2009; 2:80–84
34. Friedberg MK, Mertens L: Tissue velocities,strain, and strain rate for echocardiographicassessment of ventricular function in con-genital heart disease. Eur J Echocardiogr2009; 10:585–593
35. Lu X, Xie M, Tomberlin D, et al: How accu-rately, reproducibly, and efficiently can wemeasure left ventricular indices using M-
mode, 2-dimensional, and 3-dimensionalechocardiography in children? Am Heart J2008; 155:946–953
36. Bu L, Munns S, Zhang H, et al: Rapid fullvolume data acquisition by real-time 3-di-mensional echocardiography for assessmentof left ventricular indexes in children: A val-idation study compared with magnetic reso-nance imaging. J Am Soc Echocardiogr2005; 18:299–305
37. Lang RM, Mor-Avi V, Sugeng L, et al: Three-dimensional echocardiography: The benefitsof the additional dimension. J Am Coll Car-diol 2006; 48:2053–2069
38. Hlavacek AM, Crawford FA Jr, Chessa KS, etal: Real-time three-dimensional echocardi-ography is useful in the evaluation of pa-tients with atrioventricular septal defects.Echocardiography 2006; 23:225–231
39. Helbing WA, Bosch HG, Maliepaard C, et al:Comparison of echocardiographic methodswith magnetic resonance imaging for assess-ment of right ventricular function in chil-dren. Am J Cardiol 1995; 76:589–594
40. van der Zwaan HB, Helbing WA, McGhie JS,et al: Clinical value of real-time three-dimensional echocardiography for right ven-tricular quantification in congenital heartdisease: Validation with cardiac magneticresonance imaging. J Am Soc Echocardiogr2010; 23:134–140
41. Lu X, Nadvoretskiy V, Bu L, et al: Accuracyand reproducibility of real-time three-dimensional echocardiography for assess-ment of right ventricular volumes and ejec-tion fraction in children. J Am SocEchocardiogr 2008; 21:84–89
42. Khoo NS, Young A, Occleshaw C, et al: As-sessments of right ventricular volume andfunction using three-dimensional echocardi-ography in older children and adults withcongenital heart disease: Comparison withcardiac magnetic resonance imaging. J AmSoc Echocardiogr 2009; 22:1279–1288
43. De Castro S, Caselli S, Papetti F, et al: Fea-sibility and clinical impact of live three-dimensional echocardiography in the man-agement of congenital heart disease.Echocardiography 2006; 23:553–561
44. Riehle TJ, Mahle WT, Parks WJ, et al: Real-time three-dimensional echocardiographicacquisition and quantification of left ventric-ular indices in children and young adultswith congenital heart disease: Comparisonwith magnetic resonance imaging. J Am SocEchocardiogr 2008; 21:78–83
45. Baker GH, Shirali G, Ringewald JM, et al:Usefulness of live three-dimensional trans-esophageal echocardiography in a congenitalheart disease center. Am J Cardiol 2009; 103:1025–1028
S54 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Emerging technologies
Avihu Z. Gazit, MD; David S. Cooper, MD
T he primary goal of hemody-namic monitoring in criticallyill patients is to assess the ad-equacy of systemic perfusion.
Since the introduction of the balloonfloatation-assisted pulmonary arterycatheter (PAC) in the 1970s, hemody-namic monitoring has been consideredpart of the standard of care in managingpatients with shock and/or acute lunginjury (1). Recent studies, however, ques-tion the PAC’s outcome benefit (2, 3),particularly in pediatric patients. The im-plications of these outcome studies arenot clear, but question whether alterna-tive hemodynamic monitoring strategiesavailable today can replace the PAC.
The commercially available hemody-namic monitoring systems can be dividedinto three categories: 1) calibration-dependent pulse contour analysis devices(1) such as the Pulse Contour Cardiac Out-put (PiCCO, Pulsion, Munich, Germany)and LiDCO (LiDCO, Cambridge, UK) sys-tems; 2) noncalibrated pulse contour anal-ysis devices (2) such as the FloTrac system(FloTrac/Vigileo, Edwards Life Sciences, Ir-vine, CA), Pressure Recording AnalyticalMethod (PRAM, Vytech Health, Padova, It-
aly), and LiDCOrapid (LiDCO, Cambridge,UK); and 3) alternative techniques (3) suchas Doppler ultrasound methods, pulse dyedensitometry, bioimpedance cardiography,and partial CO2 rebreathing.
In general, the method described byBland and Altman (4) seems to be themost appropriate when comparing mea-surements obtained by one methodagainst another method whose accuracyis questionable. This method uses themean of the two methods as the yard-stick, and reports accuracy in terms ofthe mean difference (bias) between thetwo methods �2 standard deviations; thelatter, also termed the limits of agree-ment, is an indicator of precision. Critch-ley and Critchley (5) recommend thatlimits of agreement between the new andreference technique of up to �30%should be accepted.
The purpose of this review is to assessthe theoretical basis of these strategiesand their possible benefit in guiding thetherapy of critically ill children.
Calibration-Dependent PulseContour Analysis Devices
PiCCO
This device utilizes a standard centralvenous catheter as well as a proprietarythermistor-tipped arterial catheter to as-sess a variety of hemodynamic parame-ters via transpulmonary thermodilution.A 3F or 4F arterial catheter is availablefor cannulation of the femoral artery inchildren. To compensate for interindi-vidual differences in compliance and re-sistance of the arterial vessel system, andto track changes of these variables as aresult of changing clinical conditions,
manual calibrations are necessary. Thetemperature-time curves obtained duringtranspulmonary thermodilution mea-surements are broader and lower in mag-nitude than when obtained via a PAC.Thus these measurements are more vul-nerable to errors caused by baseline driftand miscorrections for indicator recircu-lation. The transpulmonary technique isless vulnerable to errors caused by respi-ratory variation in blood temperature. Ahigh degree of correlation between trans-pulmonary thermodilution measure-ments of cardiac output (CO) and thedirect Fick principle has been establishedin critically ill children (6, 7). However,Bein and colleagues (8) observed largedifferences between the arterial wave-form-based CO and reference methodsduring hemorrhage, shock, and vasodila-tation. It has become more and moreevident that frequent recalibration is nec-essary in these patients to obtain reason-able accuracy (8, 9).
Indicator dilution methods (includingthermodilution) can be used not only tomeasure flow but also to measure thevolume through which flow is measured.The distribution volume for the indicatoris the product of the CO multiplied by themean transit time for the indicator. Adetailed discussion of the measurementsof intrathoracic thermal volumes can befound elsewhere (10). PiCCO measuresboth static and dynamic hemodynamicvariables. Based on recent studies,changes in intrathoracic blood volumeand global end-diastolic volume reflectboth changes in volume status and theresulting alteration in CO. Lichtwarck-Aschoff and colleagues (11) demonstratedin a group of ventilated patients withacute respiratory failure a better correla-
From the Divisions of Critical Care and Cardiology(AZG), Department of Pediatrics, St. Louis Children’sHospital, Washington University, St. Louis, MO; andThe Congenital Heart Institute of Florida, Divisions ofCritical Care and Cardiology (DSC), All Children’s Hos-pital, University of South Florida College of Medicine,St. Petersburg, FL.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2011 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/PCC.0b013e3182211c2b
Hemodynamic monitoring in critically ill patients has beenconsidered part of the standard of care in managing patients withshock and/or acute lung injury, but outcome benefit, particularlyin pediatric patients, has been questioned. There is difficulty invalidating the reliability of monitoring devices, especially sincethis validation requires comparison to the pulmonary artery cath-
eter, which has its own problems as a measurement tool. Inter-pretation of the available evidence reveals advantages and dis-advantages of the available hemodynamic monitoring devices.(Pediatr Crit Care Med 2011; 12[Suppl.]:S55–S61)
KEY WORDS: cardiac output; circulation; hemodynamics; moni-toring
S55Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

tion between changes in intrathoracicblood volume index and cardiac index(CI) than between changes in either cen-tral venous pressure or pulmonary arteryocclusion pressure and CI. Lopez-Herceand colleagues (12) evaluated the re-sponse to acute hypovolemia, rapid bloodvolume expansion, and epinephrine ad-ministration in an infant animal modeland showed that intrathoracic blood vol-ume index and global end-diastolic vol-ume index were more sensitive tochanges in blood volume than centralvenous pressure or pulmonary artery oc-clusion pressure.
A prospective, multicenter, multina-tional study performed by Uchino andcolleagues (13) in 331 critically ill adultpatients monitored by PAC or PiCCO,showed that the choice of monitoring didnot influence major outcomes. The use ofPiCCO, however, was associated with agreater fluid balance and fewer ventila-tor-free days. A recent meta-analysis per-formed by Marik and colleagues (14) re-vealed that dynamic PiCCO variables,such as the pulse pressure variability andstroke volume variability, have bettercorrelation with fluid responsiveness indifferent adult patient populations. Thismeta-analysis revealed that the diagnos-tic accuracy of the pulse pressure vari-ability (directly measured) was signifi-cantly greater (p � .001) than that forstroke volume variability (calculated).These data suggest that the pulse pres-sure variability may be the preferred ar-terial waveform-derived variable for as-sessment of volume status.
The PiCCO method may give incorrectthermodilution measurements in patientswith intracardiac shunts, aortic aneurysm,aortic stenosis, pneumonectomy, macrolung embolism, and extracorporeal circula-tion (if blood is either extracted from orinfused back into the cardiopulmonary cir-culation). It is therefore of limited use inthe perioperative care of children withcomplex congenital heart defects, butmay be useful in children with normalcardiac anatomy who present with car-diogenic shock, or in the postoperativecare of children after heart transplanta-tion or biventricular repair.
LiDCO
Lithium dilution CO is a minimallyinvasive indicator dilution technique. Itwas primarily developed as a simple cali-bration for the PulseCO (LiDCO, London,UK) continuous arterial waveform analy-
sis monitor. The technique requires astandard arterial catheter and central orperipheral venous access (15). A smallintravenous dose (0.002–0.004 mmol/kg)of isotonic lithium chloride solution (150mM) is injected. The resulting lithiumconcentration-time curve is recorded bythe flow of blood (4 mL/min) through aspecial disposable sensor that is attachedto the patient’s arterial catheter. The COis calculated from the lithium dose andthe area under the curve before recircu-lation (16). The advantages of lithium areits safety profile related to the minutedose required to achieve an adequatereading, no significant first-pass metabo-lism, and rapid distribution (17, 18).
PulseCO system
The PulseCO Hemodynamic Monitor(LiDCO, London, UK) was developed inconjunction with LiDCO to give a beat-to-beat estimate of stroke volume and COderived from the arterial pressure wave-form. The proprietary algorithm of thePulseCO is based on pulse power analysisrather than on the shape of the arterialwaveform or the area under the curve forcalculating CO. The assumption is thatthe pulse power is proportional to thestroke volume. Rhodes (19) published adetailed description of the underlying al-gorithm. The lithium dilution techniqueis of sufficient accuracy when there isconstant blood flow, homogeneous mix-ing of blood, and when there is no indi-cator loss due to abnormal shunt betweenthe site of injection and the detection site(20). The recalibration interval recom-mended by the manufacturer is 8 hrs;however, recent data suggest calibrationwhenever major hemodynamic changesoccur (21). A recent study by Costa andcolleagues (22) examined the level ofagreement between intermittent COmonitoring by the lithium dilution tech-nique, continuous CO monitoring usingthe arterial pressure waveform, and inter-mittent thermodilution using the PAC.This work revealed technical limitationsrelated to the calibration of the LiDCOsystem, including the need for accuratemeasurements of serum sodium and he-moglobin concentration, limited numberof calibrations based on a maximum dailylithium dose of 3 mM, and inability tocalibrate within 15 to 30 mins of neuro-muscular blockade administration due tothe reaction with the lithium sensor. Theconclusion of the study was that, in pa-tients with hyperdynamic circulation, in-
termittent and continuous CO values de-termined using the LiDCO systemshowed good agreement with those ob-tained by intermittent PAC thermodilu-tion (22).
Noncalibrated Pulse ContourAnalysis Devices
FloTrac/Vigileo
This system consists of a sensor (Flo-Trac, Edwards) and a processing/displayunit (Vigileo, Edwards). The latter appliesa proprietary algorithm to the digitizedarterial wave, and reports CO and otherhemodynamic parameters. If a central ve-nous pressure catheter has been placed,its signal can be interfaced with the Vigi-leo, allowing for the calculation of in-dexed systemic vascular resistance. Whenused with a central venous oximetry cath-eter, the Vigileo also provides continuouscentral venous oxygen saturation. The di-rect proportionality between arterial pul-satility and the stroke volume in conjunc-tion with heart rate is used to calculateCO. Individual demographic data includ-ing height, weight, age, and sex are usedto correct for interindividual differencesin arterial compliance based on themodel proposed by Langewouters andcolleagues (23). A recent meta-analysis(24) showed overestimation of CO by Flo-Trac/Vigileo in the setting of significantaortic regurgitation. Of note, studies in-volving rapidly changing hemodynamicprofiles and continuous thermodilutionwere not included in the meta-analysis.Other single-center studies showed un-derestimation of CO by this device inhigh-output, vasodilatory states (25, 26).
PRAM
Different from the FloTrac/Vigileo sys-tem, the evaluation of CO by Most-Care(powered by PRAM; Vytech Health, Pa-dova, Italy) does not require anthropo-metric data. It is based on the morpho-logic analysis of both the pulsatile andcontinuous components of the arterialpressure waveform. The concept behindPRAM is based on the physics theory ofperturbations (27). Another importantcharacteristic of the PRAM methodologyis the 1000 Hz sampling frequency, dif-ferent from other pulse contour analysistechnologies that usually use a samplingfrequency of 100 Hz. A detailed descrip-tion of the method is published elsewhere(28). This morphology-based analysis
S56 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

makes the system susceptible to sourcesof error, as may be seen in stenosis of thearterial tree, for example. Furthermore,dampened waveforms and inadequatepulse detection associated with severe ar-rhythmias or catheter obstruction/dis-lodgment may influence the precision ofthe waveform analysis (29). Although thistechnology is considered accurate in con-ditions of hemodynamic stability (30, 31),its accuracy is still questionable whenprofound hemodynamic changes occur. Arecent study by Romagnoli and col-leagues (32), performed in a swine model,investigated the reliability of Most-Carein conditions of hemodynamic instabil-ity in comparison with PAC thermodilu-tion and transesophageal echocardiogra-phy. The study showed that Most-Carewas less accurate during the low strokevolume states; however, it was not influ-enced by variations in vascular tone.Since only a few validation studies havebeen published so far, a conclusive ap-praisal cannot yet be made.
LiDCOrapid
LiDCOrapid (LiDCO, Cambridge, UK)was recently launched. It applies theknown LiDCO pulse power analysis algo-rithm without the need for calibration bylithium chloride. No scientific evidenceexists so far.
Alternative Techniques
Doppler ultrasound methods
The concepts behind hemodynamicevaluation via transesophageal Dopplermonitoring were first introduced by Sideand Gosling (33), and later refined bySinger and colleagues (34). The tech-nique of probe insertion is straightfor-ward, with low inter- and intra-observervariability, and most operators becomeproficient after 10–12 probe insertions(35, 36). Recommended absolute contra-indications include recent esophagealsurgery or the presence of congenital oracquired esophageal abnormalities.
The accuracy of velocity measurementrequires a good alignment between theDoppler “beam” and blood flow, andknowledge of the angle between the ul-trasound beam and the blood flow vector(angle of insonation). Proper alignmentof the probe is best assessed subjectivelyby optimizing the quality of the obtainedsignal with the aid of the visual display ofthe instantaneous velocity waveform and
the Doppler sound. The area under eachwaveform (the integral of velocity duringthe ejection time) is called the “strokedistance,” i.e., the distance traveled byblood in the descending aorta duringeach systole. Stroke volume (cm3) is theproduct of stroke distance (cm) multi-plied by the cross-sectional area of theaortic lumen (cm2). The validity of thiscomputation requires a “flat” descendingaorta velocity profile (i.e., the velocityshould be the same at any given pointacross the aortic lumen), and cross-sectional area should be constant duringsystole. Whereas flow in the descendingaorta may be somewhat parabolic, withfaster flow at the center of the vesselcompared to the periphery (37), the dif-ferences in the absence of aortic pathol-ogy that would create turbulent flow areunlikely to be significant (38). Bedsidemeasurement of the cross-sectional areaof the descending aorta can only be per-formed by using transesophageal echo-cardiography. This technique is not avail-able everywhere, and the manufacturersof the transesophageal Doppler probehave incorporated a nomogram to esti-mate the cross-sectional area of the de-scending aorta based on the patient’s age,weight, and height. Because blood flow inthe descending aorta is only a fraction oftotal CO, a constant proportion of theblood flow between the descending aorta(approximately 70%) and the coronaryand brachiocephalic arteries (approxi-mately 30%) needs to be assumed to es-timate stroke volume and CO; however,the partition of blood flow between ce-phalic and caudal territories may alsovary according to hemodynamic condi-tions, reflex activation, or metabolic ac-tivity within different organs. Therefore,the assigned constant ratio of 70%:30%may become inaccurate under a variety ofpathophysiologic conditions (39, 40). Theextent to which this partition of CO isaltered by or during critical illness hasnot been studied.
CO as measured by the esophagealDoppler technique has been comparedwith CO obtained by thermodilution inmultiple clinical settings, including theoperating room and the medical/surgicalintensive care unit. Dark and Singer (41)published a meta-analysis of validity stud-ies comparing CO measurements ob-tained from the esophageal Doppler mon-itor (EDM, trademarked Cardio Q,previously ODM), the echo-esophagealDoppler (Echo-ED, trademarked He-moSonic100, previously Dynemo 3000),
and the PAC between 1989 and 2003. Theauthors concluded that EDM has mini-mal bias when estimating absolute valuesof CO, but limited clinical agreementwith PAC thermodilution estimates. Inaddition, EDM has high validity (no biasand high clinical agreement) for moni-toring changes in CO during the manage-ment of critically ill patients in both theoperating room and intensive care unit.There were an insufficient number ofstudies to assess the validity of Echo-EDin estimating cardiac output.
Pulse dye densitometry
A recently developed and clinically in-troduced device (DDG2001 analyzer; Ni-hon Kohden, Tokyo, Japan) allows COmeasurement based on transcutaneousindocyanine green (ICG) concentrationcurves obtained after bolus venous injec-tion (42, 43). ICG distributes exclusivelyin the intravascular space via binding to�1-lipoproteins. Its concentration in thearterial blood after passage through thepulmonary circulation can be detectedvia a fingertip sensor that emits lightwith wavelengths of 805 and 890 nm. Theratio of ICG concentration measured atthese two wavelengths is used to calcu-late the ICG concentration-time curve.CO is calculated from the observed dyedilution curve according to the Stewart-Hamilton principle. Besides CO, this sys-tem has been suggested to allow mea-surement of total blood volume andcentral blood volume. Since appropriatesignal detection is mandatory, poor pe-ripheral circulation, movement artifacts,or ambient light influences are inherentlimitations of this technique. The ICGdye is nontoxic, except for rare cases ofanaphylaxis and allergic reactions. It isexclusively cleared by the liver withoutundergoing either intrahepatic or en-terohepatic metabolism. Usually, theICG concentration decreases to 1% ofthe initial concentration after 20 mins,enabling a new measurement. The ma-jority of recently published validationstudies reported only moderate agree-ment with intermittent thermodilutionmeasurements (44 – 46).
Thoracic electricalbioimpedance
The methodology for calculating COfrom changes in electrical impedanceover the thoracic area has improved overthe last decade. The initial impedance
S57Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

measurements used the Kubicek equa-tion (47). Bernstein (48) proposed a mod-ified stroke volume equation for thoracicbioimpedance. It was based on the theorythat the base thoracic impedance, whichdepends on the thoracic morphology andgas/fluid distribution, shows pulsatilevariations during the heart cycle. It wasassumed that these changes were causedby systolic dilation of the aorta and itsmajor branches. The different bioimped-ance techniques and their agreementwith invasive thermodilution techniquesare discussed below.
Cylinder- and Cone-based Bioimped-ance Algorithms. The thoracic electricalbioimpedance technique involves theanalysis of intrabeat variations in trans-thoracic voltage in response to appliedhigh-frequency transthoracic currents. Arecent study by de Waal and colleagues(49) assessed three common cylinder-and cone-based bioimpedance algorithmsin comparison with the thermodilutiontechnique during the perioperative pe-riod in coronary artery bypass graft pa-tients. This study revealed significant de-viations between bioimpedance andthermodilution stroke volume index.Bernstein and Osypka (50) substantiallymodified the basic equation to improvethe reliability of impedance measure-ments, so that the maximum rate ofchange of impedance is related to thepeak aortic blood acceleration. Thismethod is called electrical velocimetry.
Electrical Velocimetry Technique.This new bioimpedance cardiographytechnique interprets the changes in tho-racic electrical bioimpedance as theohmic equivalent of the mean aorticblood flow acceleration. The impedancerecordings and calculations of CO, strokevolume, and CI are obtained with a newcardiovascular monitor (Aesculon Elec-trical Velocimetry, Osypka MedicalGmbh, Berlin, Germany) that transformsthe ohmic equivalent of the mean aorticblood flow acceleration into an equivalentof mean aortic blood flow velocity. Acomparison of this new method with in-vasive thermodilution methods (PAC orPiCCO) in 50 critically ill adult patientsrevealed a very small bias and acceptablelimits of agreement (�30%) (51).
Bioreactance Technology. Thismethod, applied in the NICCOM system(Cheetah Medical, Indianapolis, IN), in-volves the analysis of intrabeat variationsin voltage phase shifts in response tohigh-frequency transthoracic currents. Arecent multicenter study (52) used this
device to test the accuracy of bioreac-tance-based CO measurement in the car-diac catheterization laboratory and inmedical and cardiac intensive care unitscompared to thermodilution. The studyshowed that this device has acceptableaccuracy in these varied and challengingclinical environments.
Partial CO2 Rebreathing. The nonin-vasive cardiac output (NICO) monitor(Respironics Novametrix, Wallingford,CT) estimates CO by applying the CO2
version of the Fick equation. Fick postu-lated that oxygen uptake in the lungs isentirely transferred to the blood. There-fore, CO can be calculated as the ratiobetween oxygen consumption and arte-riovenous oxygen difference. The Fickprinciple allows substitution with a mul-tiple of substitutes for oxygen consump-tion, including CO2 clearance, and can berepresented mathematically: Q � VCO2/(CvCO2-CaCO2); where Q is the CO (mL/min), VCO2 is the CO2 elimination; andCvCO2 and CaCO2 are the venous andarterial CO2 contents (mL/100 mL blood),respectively (53). VCO2 can be calculatedby the difference in CO2 content betweenexpired and inspired gases. The Fickequation can then be further modified byuse of a partial CO2 rebreathing tech-nique. This involves a transitory inter-ruption of CO2 elimination by the addi-tion of dead space to the ventilatorycircuit, which leads to a progressive in-crease in end-tidal CO2 that approximatesthe mixed venous partial CO2 value (54–57). The change in VCO2 is then calcu-lated by comparing normal and rebreath-ing values. The change in CaCO2 contentcan then be approximated by the changein end-tidal CO2 multiplied by the slopeof the CO2 dissociation curve, which islinear between 15 and 70 mm Hg of par-tial pressure of CO2 (57, 58). Becauseintrapulmonary shunts can affect esti-mates of CO with this technique, an ar-terial blood sample is required to enterarterial oxygen tension values for shuntestimation.
The NICO monitor is characterized asminimally invasive for intubated, me-chanically ventilated patients and is easyto setup with operator-independent per-formance. Older versions of the monitorwere found to have moderate accuracybased on most validation studies (59–63). This was attributed to inadequaterebreathing time, recirculation, the dif-ference in CO2 between alveolus andproximal airway, as well as the differencebetween arterial and alveolar CO2 (64).
Recent validation studies using newersoftware demonstrated better results.Gueret and colleagues (65) looked at theuse of NICO for monitoring patients un-dergoing repeat total hip replacement.They reported that the bias � precision ofthe NICO monitor with version 4.2 soft-ware against continuous CO monitoringwas �0.3 � 1.1 L/min. The bias wassmaller when mean CO was below 3L/min. A recent study by Kotake and col-leagues (66) investigated the accuracy ofthe NICO monitor with versions 4.2 and 5in patients undergoing elective aortic re-construction. Similar to Gueret and col-leagues, this study revealed a smallerbias � precision compared to the previ-ous NICO software version, however, thelevel of agreement with the measure-ments obtained with the PAC failed tomeet the criteria set by Critchley andCritchley (5). In pediatric patients, vali-dation studies are scarce and not suffi-cient to make decisions in regards to im-plementation of the NICO monitor inclinical practice. Levy and colleagues (67)concluded that NICO is clinically accept-able in children with a body surface areaof �0.6 m2 and a tidal volume �300 mL,whereas discrepancies with thermodilu-tion were more important in smaller pa-tients. Botte and colleagues (68) evalu-ated 21 mechanically ventilated children,weighing �15 kg, in stable respiratoryand hemodynamic conditions. CO valuesobtained with this technique were inagreement with those obtained withDoppler echocardiography. AlthoughNICO evaluation has yet to be completedin children in unstable respiratory andhemodynamic conditions, this wouldseem to be a reasonable endeavor for fu-ture investigations.
Discussion
Maintenance of adequate oxygen deliv-ery in critically ill children is the maingoal of the pediatric intensivist. Unfortu-nately, physical examination findings andbasic bedside monitoring devices do notalways provide sufficient data to aid inmeeting this goal. The PAC is still con-sidered the de facto gold standard forhemodynamic monitoring; however, itsinvasive nature is associated with signif-icant complications, and its appropriateplacement, which is crucial to the ade-quacy of hemodynamic data derived fromit, is operator dependent and requires sig-nificant experience and expertise, partic-ularly in pediatric patients. To fill this
S58 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

monitoring “gap,” several devices weredeveloped and introduced into the clini-cal arena over the course of the last 2decades. These devices are minimally in-vasive and allow continuous and inter-mittent hemodynamic measurements. Ingeneral, their use is not complicated anddoes not require significant training orexpertise. The main problem we face asintensivists is the difficulty to validate thereliability of these devices, especiallysince this validation requires comparisonto the PAC, which by itself is problematicas a measurement tool. Elaborate andsomewhat artificial statistical methodswere devised by Bland and Altman (4) andmodified by Critchley and Critchley (5) tooptimize this validation process, and in-deed, these are the tools that we cur-rently use. Another significant problem isthe lack of large-scale randomized valida-tion studies in adults and especially in chil-dren. This obstacle is tackled by the use ofmeta-analysis studies, which, in spite of themeticulous nature of their preparation, in-troduce more confounding factors to thealready hazy picture. Interpretation of theevidence available to us points toward ad-vantages and disadvantages of the availablehemodynamic monitoring devices, and wehereby summarize our recommendationsfor the use of these devices in the criticalcare environment.
PiCCO. The use of this monitor inchildren is overall simple and, based onour experience, requires minimal train-ing. In hemodynamically unstable pa-tients it requires frequent recalibrationsto obtain reasonable accuracy (9). Thedata in children are minimal but suggestgood correlation of PiCCO CI measure-ments and calculations based on the Fickprinciple (6, 7). Both the dynamic andstatic variables measured by the PiCCOwere shown to have good correlation withCI and fluid responsiveness, respectively(69). PiCCO monitoring is inaccurate inchildren with intracardiac shunts, limit-ing its utility in congenital heart disease.
LiDCO/PulseCO. The use of this sys-tem is problematic due to the complexityof its calibration. The available data sup-port its use in patients with hyperdy-namic circulation; however, its validity inpatients with low CO has not been stud-ied. Overall it appears that more data arerequired before use of this system in crit-ically ill children.
FloTrac/Vigileo. The agreement of thesecond-generation operating system ofthis device (1.07 and higher) with COmeasurements of other devices was found
to be adequate. The evidence for the useof this technology in the pediatric inten-sive care unit is lacking.
PRAM. This system’s accuracy is un-clear in unstable clinical states (32).
LiDCOrapid. This is a new system. Noscientific evidence exists so far that wouldallow us to make any recommendations.
EDM (trademarked Cardio Q, previ-ously ODM) and Echo-ED (trademarkedHemoSonic100, previously Dynemo3000).Insertion and alignment of the probe issimple and requires minimal training toachieve proficiency (35, 36). The currentevidence (41) reveals that EDM has min-imal bias when estimating absolute val-ues of CO, but limited clinical agreementwith PAC thermodilution estimates. Ithas high validity (no bias and high clini-cal agreement) for monitoring changes inCO during the management of criticallyill patients in both operating rooms andintensive care units. There were an insuf-ficient number of studies to assess thevalidity of Echo-ED in estimating cardiacoutput.
Pulse Dye Densitometry (DDG2001Analyzer; Nihon Kohden, Tokyo, Japan).Current evidence is limited and revealsonly moderate agreement with the in-termittent thermodilution technique(44 – 46).
Cylinder- and Cone-based Bioimped-ance Algorithms. Evidence suggests it isnot acceptable as a hemodynamic moni-toring technique.
Electrical Velocimetry Technique(Aesculon Electrical Velocimetry, OsypkaMedical Gmbh, Berlin, Germany). Lim-ited data (51) reveal small bias and ac-ceptable limits of agreement comparingthe measurements obtained by this tech-nique and measurements obtained bythermodilution (PAC or PiCCO).
Bioreactance Technology (NICCOMSystem; Cheetah Medical, Indianapolis,IN). New technology. Limited data (61)reveal acceptable measurement accuracyin the cardiac catheterization laboratoryand intensive care unit compared to ther-modilution.
Partial CO2 Rebreathing (NICO; Re-spironics Novametrix, Wallingford, CT).This monitor is easy to setup with oper-ator-independent performance. However,its use is limited to sedated and mechani-cally ventilated patients, and the level ofagreement of CO measurements obtainedby the newer software versions of this mon-itor (4.2 and 5) compared to thermodilu-tion measurements fail to meet the accept-
able criteria. Validation studies in childrenare currently insufficient (67, 68).
Conclusion
Minimally invasive hemodynamicmonitoring devices are commerciallyavailable but their role in the evaluationof systemic perfusion in critically illchildren is not well established. Large-scale validation studies are required toexamine their applicability in pediatricpatients.
REFERENCES
1. Williams G, Grounds M, Rhodes A: Pulmo-nary artery catheter. Curr Opin Crit Care2002; 8:251–256
2. Harvey S, Young D, Brampton W, et al: Pul-monary artery catheters for adult patients inintensive care. Cochrane Database Syst Rev2006; 3:CD003-CD408
3. National Heart, Lung, and Blood InstituteAcute Respiratory Distress Syndrome (ARDS)Clinical Trials Network, Wheeler AP, BernardGR, et al: Pulmonary-artery versus centralvenous catheter to guide treatment of acutelung injury. N Engl J Med 2006; 354:2213–2224
4. Bland JM, Altman DG: Statistical methodfor assessing agreement between twomethods of clinical measurement. Lancet1986; 1:307–310
5. Critchley LA, Critchley JA: A meta-analysis ofstudies using bias and precision statistics tocompare cardiac output measurement tech-niques. J Clin Monit Comput 1999; 15:85–91
6. Pauli C, Fakler U, Genz T, et al: Cardiacoutput determination in children: Equiva-lence of the transpulmonary thermodilutionmethod to the direct Fick principle. Inten-sive Care Med 2002; 28:947–952
7. Tibby SM, Hatherill M, Marsh MJ, et al: Clin-ical validation of cardiac output measure-ments using femoral artery thermodilutionwith direct Fick in ventilated children andinfants. Intensive Care Med 1997; 23:987–991
8. Bein B, Meybohm P, Cavus E, et al: Thereliability of pulse contour-derived cardiacoutput during hemorrhage and after vaso-pressor administration. Anesth Analg 2007;105:107–113
9. Hamzaoui O, Monnet X, Richard C, et al:Effects of changes in vascular tone on theagreement between pulse contour and trans-pulmonary thermodilution cardiac outputmeasurements within an up to 6-hour cali-bration-free period. Crit Care Med 2008; 36:434–440
10. Isakow W, Schuster DP: Extravascular lungwater measurements and hemodynamicmonitoring in the critically ill: Bedside alter-natives to the pulmonary artery catheter.Am J Physiol Lung Cell Mol Physiol 2006;291:L1118–L1131
S59Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)
11. Lichtwarck-Aschoff M, Zeravik J, Pfeiffer UJ:Intrathoracic blood volume accurately re-flects circulatory volume status in criticallyill patients with mechanical ventilation. In-tensive Care Med 1992; 18:142–147
12. Lopez-Herce J, Ruperez M, Sanchez C, et al:Haemodynamic response to acute hypovolae-mia, rapid blood volume expansion andadrenaline administration in an infant ani-mal model. Resuscitation 2006; 68:259–265
13. Uchino S, Bellomo R, Morimatsu H, et al:Pulmonary artery catheter versus pulse con-tour analysis: a prospective epidemiologicalstudy. Crit Care 2006; 10:R174
14. Marik PE, Cavallazzi R, Vasu T, et al: Dy-namic changes in arterial waveform derivedvariables and fluid responsiveness in me-chanically ventilated patients: A systematicreview of the literature. Crit Care Med 2009;37:2642–2647
15. Jonas MM, Kelly FE, Linton RA, et al: Acomparison of lithium dilution cardiac out-put measurement using central and antecu-bital venous injection of lithium chloride.J Clin Monit Comput 1999; 15:525–528
16. Band DM, Linton RA, O’Brien TK, et al: Theshape of indicator dilution curves used forcardiac output measurement in man.J Physiol 1997; 498:225–229
17. Hatfield CL, McDonell WN, Lemke KA, et al:Pharmacokinetics and toxic effects of lithiumchloride after intravenous administration inconscious horses. Am J Vet Res 2001; 62:1387–1392
18. Jonas MM, Linton RA, O’Brien TK, et al: Thepharmacokinetics of intravenous lithiumchloride in patients and normal volunteers.J Trace Microprobe Tech 2001; 19:313–320
19. Rhodes A, Sunderland R: Arterial pulse pres-sure analysis: The LiDCOplus system. Updatein intensive care and emergency medicine.In: Functional Hemodynamic monitoring.Pinsky MR, Payen D (Eds). Heidelberg:Springer, 2004, pp 183–192
20. Christiansen C, Hostrup A, Tønnesen E, et al:Hemodynamic monitoring with the lithiumdilution cardiac output system. Ugeskr Lae-ger 2008; 170:522–524
21. Cecconi M, Dawson D, Grounds RM, et al:Lithium dilution cardiac output measure-ment in the critically ill patient: Determina-tion of precision of the technique. IntensiveCare Med 2009; 35:498–504
22. Costa MG, Della Rocca G, Chiarandini P, etal: Continuous and intermittent cardiac out-put measurement in hyperdynamic condi-tions: Pulmonary artery catheter vs. lithiumdilution technique. Intensive Care Med 2008;34:257–263
23. Langewouters GJ, Wesseling KH, GoedhardWJ: The pressure dependent dynamic elastic-ity of 35 thoracic and 16 abdominal humanaortas in vitro described by a five componentmodel. J Biomech 1985; 18:613–620
24. Mayer J, Boldt J, Poland R, et al: Continuousarterial pressure waveform-based cardiacoutput using the FloTrac/Vigileo: A review
and meta-analysis. J Cardiothorac VascAnesth 2009; 23:401–406
25. Biais M, Nouette-Gaulain K, Cottenceau V, etal: Cardiac output measurement in patientsundergoing liver transplantation: Pulmonaryartery catheter versus uncalibrated arterialpressure waveform analysis. Anesth Analg2008; 106:1480–1486
26. Biancofiore G, Critchley LA, Lee A, et al:Evaluation of an uncalibrated arterial pulsecontour cardiac output monitoring system incirrhotic patients undergoing liver surgery.Br J Anaesth 2009; 102:47–54
27. Messiah A: Change of representation and per-turbation treatment of a part of the Hamil-tonian. In: Quantum Mechanics, Vol 2. Am-sterdam, North-Holland Physics, 1985, pp.722–760
28. Scolletta S, Romano SM, Biagioli B, et al:Pressure recording analytical method(PRAM) for measurement of cardiac outputduring various haemodynamic states. Br JAnaesth 2005; 95:159–165
29. van Lieshout JJ, Wesseling KH: Continuouscardiac output by pulse contour analysis?Br J Anaesth 2001; 86:467–469
30. Calamandrei M, Mirabile L, Muschetta S, etal: Assessment of cardiac output in children:A comparison between the pressure record-ing analytical method and Doppler echocar-diography. Pediatr Crit Care Med 2008;9:310–312
31. Romano SM, Pistolesi M: Assessment of cardiacoutput from systemic arterial pressure in hu-mans. Crit Care Med 2002; 30:1834–1841
32. Romagnoli S, Romano SM, Bevilacqua S, etal: Cardiac output by arterial pulse contour:Reliability under hemodynamic derange-ments. Interact Cardiovasc Thorac Surg2009; 8:642–646
33. Side CD, Gosling RG: Non-surgical assess-ment of cardiac function. Nature 1971; 232:335–336
34. Singer M, Clarke J, Bennett ED: Continuoushemodynamic monitoring by esophagealDoppler. Crit Care Med 1989; 17:447–452
35. Valtier B, Cholley BP, Belot JP, et al. Noninva-sive monitoring of cardiac output in criticallyill patients using transesophageal Doppler.Am J Respir Crit Care Med 1998; 158:77–83
36. Lefrant JY, Bruelle P, Aya AG, et al. Trainingis required to improve the reliability ofesophageal Doppler to measure cardiac out-put in critically ill patients. Intensive CareMed 1998; 24:347–352
37. Farthing S, Peronneau P: Flow in the tho-racic aorta. Cardiovasc Res 1979; 13:607–620
38. Singer M: ODM/CardioQ esophageal Dopplertechnology. Crit Care Med 2003; 31:1888–1889; author reply 1889
39. Mark JB, Steinbrook RA, Gugino LD, et al.Continuous noninvasive monitoring of car-diac output with esophageal Doppler ultra-sound during cardiac surgery. Anesth Analg1986; 65:1013–1020
40. Perrino AC Jr, Fleming J, LaMantia KR:Transesophageal Doppler cardiac output
monitoring: performance during aortic re-constructive surgery. Anesth Analg 1991; 73:705–710
41. Dark PM, Singer M: The validity of trans-esophageal Doppler ultrasonography as ameasure of cardiac output in critically illadults. Intensive Care Med 2004; 30:2060–2066
42. He YL, Tanigami H, Ueyama H, et al: Mea-surement of blood volume using indocyaninegreen measured with pulse-spectrophotome-try: Its reproducibility and reliability. CritCare Med 1998; 26:1446–1451
43. Iijima T, Aoyagi T, Iwao Y, et al: Cardiacoutput and circulating blood volume analysisby pulse dye-densitometry. J Clin Monit1997; 13:81–89
44. Baulig W, Bernhard EO, Bettex D, et al: Car-diac output measurement by pulse dye den-sitometry in cardiac surgery. Anaesthesia2005; 60:968–973
45. Hofer CK, Buhlmann S, Klaghofer R, et al:Pulsed dye densitometry with two differentsensor types for cardiac output measurementafter cardiac surgery: A comparison with thethermodilution technique. Acta AnaesthesiolScand 2004; 48:653–657
46. Sakka SG, Reinhart K, Wegscheider K, et al:Comparison of cardiac output and circula-tory blood volumes by transpulmonarythermo-dye dilution and transcutaneous in-docyanine green measurement in criticallyill patients. Chest 2002; 121:559–565
47. Kubicek WG, Karnegis JN, Patterson RP, etal: Development and evaluation of an imped-ance cardiac output system. Aerosp Med1966; 37:1208–1212
48. Bernstein DP: A new stroke volume equationfor thoracic electrical bioimpedance: Theoryand rationale. Crit Care Med 1986; 14:904–909
49. de Waal EE, Konings MK, Kalkman CJ, et al:Assessment of stroke volume index withthree different bioimpedance algorithms:Lack of agreement compared to thermodilu-tion. Intensive Care Med 2008; 34:735–739
50. Bernstein DP, Osypka MJ: Apparatus andmethod for determining an approximation ofthe stroke volume and the cardiac output ofthe heart. 2001, US Patent no: 6511438 B2
51. Zoremba N, Bickenbach J, Krauss B, et al:Comparison of electrical velocimetry andthermodilution techniques for the measure-ment of cardiac output. Acta AnaesthesiolScand 2007; 51:1314–1319
52. Raval NY, Squara P, Cleman M, et al: Multi-center evaluation of noninvasive cardiac out-put measurement by bioreactance technique.J Clin Monit Comput 2008; 22:113–119
53. Michael JB: Partial CO2 rebreathing cardiacoutput-operating principles of the NICOTMsystem. J Clin Monit Comput 1999; 15:387–401
54. Chaney JC, Derdak S: Minimally invasive he-modynamic monitoring for the intensivist:Current and emerging technology. Crit CareMed 2002; 30:2338–2345
55. de Abreu MG, Quintel M, Ragaller M, et al:
S60 Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)

Partial carbon dioxide rebreathing: A reliabletechnique for noninvasive measurement ofnonshunted pulmonary capillary blood flow.Crit Care Med 1997; 25:675–683
56. de Abreu MG, Geiger S, Winkler T, et al:Evaluation of a new device for noninvasivemeasurement of nonshunted pulmonary cap-illary blood flow in patients with acute lunginjury. Intensive Care Med 2002; 28:318–323
57. Heigenhauser GJ, Jones NL: Measurement ofcardiac output by carbon dioxide rebreathingmethods. Clin Chest Med 1989; 10:255–264
58. Cholley BP, Payen D: Noninvasive techniquesfor measurements of cardiac output. CurrOpin Crit Care 2005; 11:424–429
59. van Heerden PV, Baker S, Lim SI, et al: Clinicalevaluation of the non-invasive cardiac output(NICO) monitor in the intensive care unit. An-aesth Intensive Care 2000; 28:427–430
60. Nilsson LB, Eldrup N, Berthelsen PG: Lack ofagreement between thermodilution and car-bon dioxide-rebreathing cardiac output. ActaAnaesthesiol Scand 2001; 45:680–685
61. Odenstedt H, Stenqvist O, Lundin S: Clinicalevaluation of a partial CO2 rebreathing tech-nique for cardiac output monitoring in crit-ically ill patients. Acta Anaesthesiol Scand2002; 46:152–159
62. Kotake Y, Moriyama K, Innami Y, et al: Per-formance of noninvasive partial CO2 re-breathing cardiac output and continuousthermodilution cardiac output in patientsundergoing aortic reconstruction surgery.Anesthesiology 2003; 99:283–288
63. Tachibana K, Imanaka H, Takeuchi M, et al:Noninvasive cardiac output measurementusing partial carbon dioxide rebreathing isless accurate at settings of reduced minuteventilation and when spontaneous breathingis present. Anesthesiology 2003; 98:830–837
64. Yem JS, Tang Y, Turner MJ, et al: Sources oferror in noninvasive pulmonary blood flowmeasurements by partial rebreathing: Acomputer model study. Anesthesiology 2003;98:881–887
65. Gueret G, Kiss G, Khaldi S, et al: Comparison
of cardiac output measurements betweenNICO and the pulmonary artery catheter dur-ing repeat surgery for total hip replacement.Eur J Anaesthesiol 2007; 24:1028–1033
66. Kotake Y, Yamada T, Nagata H, et al: Im-proved accuracy of cardiac output estimationby the partial CO2 rebreathing method.J Clin Monit Comput 2009; 23:149–155
67. Levy RJ, Chiavacci RM, Nicolson SC, et al: Anevaluation of a noninvasive cardiac outputmeasurement using partial carbon dioxiderebreathing in children. Anesth Analg 2004;99:1642–1647, table of contents
68. Botte A, Leclerc F, Riou Y, et al: Evaluationof a noninvasive cardiac output monitor inmechanically ventilated children. PediatrCrit Care Med 2006; 7:231–236
69. Buhre W, Weyland A, Buhre K, et al: Effectsof the sitting position on the distribution ofblood volume in patients undergoing neuro-surgical procedures. Br J Anaesth 2000; 84:354–357
S61Pediatr Crit Care Med 2011 Vol. 12, No. 4 (Suppl.)