Hemodynamics 2011 (1)

of 13
Transcript of Hemodynamics 2011 (1)
-
7/31/2019 Hemodynamics 2011 (1)
1/13
2011 Hemodynamics Page 1 of 13 RJ Barsotti, Ph.D.
Hemodynamics
IntroductionThe cardiovascular system consists of a muscular pump, the heart that propels blood through acomplex network of branched blood vessels, delivering nutrients to and removing wastes from
each organ and transporting hormones and other messengers between various regions of thebody. Hemodynamics considers the physical forces involved in moving blood through thecirculation. In this section, we consider the forces that the heart must overcome to get this bloodsupply where it is needed, and how the body uses these forces to redistribute the supply as localdemands change.
The heart pumps a given volume of blood into the aorta each minute (the cardiac output). Thepercentage of the cardiac output that any given organ receives depends upon the resistance thatthe organ offers to the flow of blood. Cardiac and vascular function is regulated on a beat to beatbasis by the interaction of the autonomic nervous system and local factors within tissues.
A fluid is a material that flows and that the shape of its containment vessel. It is a substance thatdeforms easily when a shearing force is applied and does NOT return to its original form whenthe force is removed like a solid would. Thus, in liquids, there are no elastic forces that restorethe original unstressed shape. We also know or should know that liquids are NOT easilycompressed. In addition liquids flow downhill in a gravitational field
Hemodynamics considers the physical forces involved in moving the blood through thecirculation. The cardiac pump adds energy to the circulation which we measure as pressure.This pressure is dissipated through the circulatory system in overcoming the resistance to bloodflow offered by the blood itself and the blood vessels.
PressureForce in a liquid system is manifested as pressure. In the cardiovascular system, the effects ofpressure may be observed in two major ways: first, the pressure differences that moves bloodthrough blood vessels; and second, the pressure in a liquid at rest can distend arteries and veins.
Blood pressure is given in terms of the height of a liquid in a tube, i.e. in units of the height of aliquid of known density. If we apply pressure to one side of a column of fluid in a U-shaped tube,the fluid height in the other column will increase (see Figure 1a). The pressure we apply ismeasured as the height of the column of fluid. Arterial pressure is usually expressed inmillimeters of mercury (mm Hg). Mercury was chosen for its relatively high density, making itpossible to measure arterial pressure using a relatively short tube. This is the same principle used
in a sphygmomanometer to measure blood pressure. However, usually pressure is expressed asforce per unit area, and the appropriate basic unit is dyne/cm2.
-
7/31/2019 Hemodynamics 2011 (1)
2/13
2011 Hemodynamics Page 2 of 13 RJ Barsotti, Ph.D.
Figure 1a Measurement of Pressure
P1
Measured pressure is the heightof the column (P2-P1). If the fluid
column is mercury, pressure is mm Hg.If the fluid column is water, pressure iscm H2O.
P2
Apply pressure
The pressure at a given depth in a liquid is equal in all directions , also known as PascalsPrinciple . The shape of the vessel holding the liquid does not alter this. The pressure (P) belowthe surface of the liquid increases with depth such that P = h g, where is the density of thefluid (g/cm
3), g is gravitational acceleration (980 cm/sec
2), and h is the height of the fluid column
(cm). This hydrostatic pressure is caused by the force of gravity on the fluid (see Figure 1b).Thus when a person is standing, blood pressure is greater in the vessels of the legs than in the
analogous vessels of the arms because hydrostatic pressure is added to the hemodynamic
pressure (the pressure generated by the contraction of the heart and stored in the elastic
walls of the blood vessels).
Figure 1b Gravity acts on columns of fluid such that pressures increases with depth
P1
P2
P2
P1
P3
P2
P3
Pressures in the same
horizontal plane are equal
Pressures increase with
depth or the height of thecolumn
-
7/31/2019 Hemodynamics 2011 (1)
3/13
2011 Hemodynamics Page 3 of 13 RJ Barsotti, Ph.D.
Gravity also acts on columns of blood within the cardiovascular system. In the individual lyingdown, the mean pressure in the root of the aorta might be 100 mm Hg. Mean pressure in a largeartery in the foot might be 95 mm Hg because the large vessels offer little resistance to the flowof blood. Similarly the average pressure within a large artery in the head might also be 95 mmHg.
When theindividual stands,the pressure atthe root of theaorta will still be100 mm Hgbecause themeasurement isclose to thesource of thepressure, the leftventricle.However, abovethe level of theheart, e.g. at thecerebral artery,gravity acts onthe column ofblood to decreasethe bloodpressure in the
cerebral artery by minus gh1. Pressure in the cerebral artery might now be approximately 50mm Hg. Conversely, below the level of the heart, gravity acts on the column of blood to increase
the blood pressure by plus gh2. Pressure in a large artery in the foot might be approximately
180 mm Hg. Arteries and veins are elastic. Under the increased transmural pressure theydilate. This elasticity, especially in the pulmonary artery, serves as a damper in which much ofthe blood ejected by the heart in taken by the increased volume of the artery. Thus blood flowthrough the lung capillaries is less pulsatile.
Fluid filtration from the capillary (described in detail in later lectures) into the interstitial spacewill also increase as the capillary pressure increases. Thus, in the standing individual blood andextracellular fluid pools in the dependent limbs. This will decrease the amount of blood
returning to the heart (the venous return). This, in turn, will decrease the amount of blood
pumped by the heart (the cardiac output). The perfusion pressure of blood to the brain will bereduced as the cardiac output is reduced. Cerebral blood flow will decline. If the situationpersists and cerebral blood flow becomes inadequate, you will lose consciousness. Obviouslythere are mechanisms to maintain venous return, cardiac output, and cerebral blood flow, and youwill hear about these in subsequent lectures.
-
7/31/2019 Hemodynamics 2011 (1)
4/13
2011 Hemodynamics Page 4 of 13 RJ Barsotti, Ph.D.
To understand the relationship between blood pressure, blood flow and the resistance to bloodflow, we need to first consider the pressure relationships within the blood vessel. Within the
vessel here is an intraluminal pressure tending to distend the vessel in all directions. The
pressure in the space outside the vessel is the extraluminal pressure tending to collapse the
vessel. The pressure gradient ( P) is the pressure difference across the vessel wall, i.e. the
pressure inside (Pi) minus the pressure outside (Po). This is the transmural pressure.
Transmural Pressure orPtm = (PiPo)
Compliance
The degree to which an elastic vessel dilates when its filled with fluid is determined by thetransmural pressure and its compliance (C)
C = V / Ptm
where V is the change in volume and Ptmis the change in transmural pressure. The morecompliant the vessel, the greater the change in its volume for a given change in transmuralpressure. The less compliant or stiffer a vessel, as occurs with aging, the greater the change intransmural pressure for a given change in volume.
Law of Laplace
In a hollow cylinder the tension in the wall (T) equals the product of the pressure across the wall(P) and the radius (r):
T P r
This relationship was derived by Bernoulli, but is usually known asLaplace's law. It tells us that,for a given pressure, the tension in the wall increases in direct proportion to radius. For the wallto withstand the tension, the thickness must be appropriate. This is the reason a large artery musthave a thicker wall than a small artery.
IntraluminalPressure (Pi)
Extraluminalpressure (Po)
-
7/31/2019 Hemodynamics 2011 (1)
5/13
2011 Hemodynamics Page 5 of 13 RJ Barsotti, Ph.D.
A vein, which withstands much lower blood pressure, has a thinner wall. Again, a smaller veincan withstand the venous pressure with a thinner wall than a larger vein. A capillary has a higherblood pressure than the veins, but nevertheless, because of its very small radius, a wall consistingof a single layer of cells has sufficient strength. Thus, the radius of the capillary, which is aprerequisite for a capillary wall thin enough to permit rapid exchange of material between the
blood and the tissues.
Interrelationship among pressure, flow, and resistanceBlood moves within the cardiovascular system from regions of higher energy or pressure toregions of lower energy or pressure. Pressure is high at the ventricular exits, e.g. at the aorta andis low as the blood returns to the atria.
Blood flow through a blood vessel is determined by two factors: (1)pressure difference of theblood between the two ends of the vessel, also sometimes called "pressure gradient" along thevessel, which is the force that pushes the blood through the vessel, and (2) the impediment toblood flow through the vessel, which is called vascular resistance. The figure belowdemonstrates these relationships, showing a blood vessel segment located anywhere in thecirculatory system:
P1 represents the pressure at the origin of the vessel; at the other end, the pressure is P2.
Resistance occurs as a result of friction between the flowing blood and the intravascularendothelium all along the inside of the vessel. The flow through the vessel can be calculated bythe following formula, which is analogous to Ohm's Law (V=IR):
F = P/ R
in which F is blood flow, P is the pressure difference (P1 - P2) between the two ends of thevessel, and R is the resistance. This formula states, in effect, that the blood flow is directlyproportional to the pressure difference but inversely proportional to the resistance.
Note that it is the difference in pressure between the two ends of the vessel, NOT the absolute
pressure in the vessel that determines rate of flow. For example, if the pressure at both ends of avessel is 100 mm Hg and yet no difference exists between the two ends, there will be no flowdespite the presence of 100 mm Hg pressure.
The equation expresses the most important of all the relations you need to understand tocomprehend the hemodynamics of the circulation. Because of the extreme importance of thisformula, you should also become familiar with its other algebraic forms:
-
7/31/2019 Hemodynamics 2011 (1)
6/13
2011 Hemodynamics Page 6 of 13 RJ Barsotti, Ph.D.
P = F x R
R = P / F
Pressure declines as the blood moves through the arteries, arterioles, capillaries and veins due toresistance to flow offered by the vascular structures and blood viscosity. The major sites ofresistance in the vascular system are the arterioles.
Blood leaves the heart via the aorta, which has an internal diameter of about an inch (2.5 cm). Itis then distributed throughout the body by arteries with diameters of around 0.4 cm. On arrivingto the tissues, these arteries branch into smaller arterioles (
-
7/31/2019 Hemodynamics 2011 (1)
7/13
2011 Hemodynamics Page 7 of 13 RJ Barsotti, Ph.D.
Summarizing:
Fa = Fb = Fc or va Aa = vb Ab = vc Aca b c
Flow (ml/sec) 10 10 10Area (cm
2) 10 2 1
Velocity (cm/sec) 1 5 10
The body solves this problem by having a branched network of blood vessels in which thecharacteristic branching pattern is that the total cross-sectional area of the branches is larger thanthat of the parent truck. This means that the total cross-sectional area of the cardiovascular
system increases as theaorta branches to arteries,arterioles and capillaries.Correspondingly, theaverage blood flow
velocity in the smallvessels is less than in largearteries or veins. Theadjacent figure illustratesthe relationships amongblood pressure, velocityand cross-sectional area ofthe blood vessels of the
systemic circulation. The
important features are
the inverse relationship
between velocity and
cross-sectional area, the
major pressure drop
across small arteries
(SA) and arterioles
(ART), and both the maximal cross-sectional area and minimal flow velocity in the
capillaries (CAP).
-
7/31/2019 Hemodynamics 2011 (1)
8/13
2011 Hemodynamics Page 8 of 13 RJ Barsotti, Ph.D.
Poiseuille's LawWe need to examine the principles that govern blood flow in more detail. These are nicelysummarized by Poiseuille's Law that describes the relationship between pressure, resistance andfluid flow through rigid tubes:
F = P r4
8L
where F again represents blood flow, P the pressure gradient across the vessel, r vessel radius,
L vessel length, and (the Greek letter eta) the viscosity of blood.
Thus flow or resistance (R = P/F or 8L / r4) can be altered by changing vessel geometry L or
r or blood viscosity . Blood viscosity can be altered by changing hematocrit or temperature.Increases in hematocrit and decreases in temperature increase the viscosity of the blood and theresistance to blood flow. Changes in vessel length are not very important in determining
resistance to flow. Changes in radius are the major mechanism for regulating blood flow!
Vessel radius can be altered by active or passive changes in wall tension. Note that a small
change in vessel radius produces asubstantialchange in flow. Raising radius to the 4th
power means that a doubling of radius produces a 16-fold increase in flow.
In future lectures, we will discuss this in more detail, but a close examination of themicrocirculation reveals that the arterioles have a thick coat of smooth muscle. When thesemuscles contract, in response to local or neural factors, they cause the arterioles to narrow andflow to the capillaries is reduced greatly. Conversely, relaxation of these muscles causes thearterioles to dilate, thereby allowing increased blood flow to the capillaries.
The more viscous a fluid, the greater its resistance to flow. Viscosity is usually measured in
poise (after Poiseuille, or dyne sec/cm2). Water has a viscosity of 0.01 poise (one centipoise or
1cp), and this provides an easy standard against which other fluids are measured: relativeviscosity. Blood is a complex fluid, and the presence of plasma proteins alone increases itsviscosity by about 20% over that of water. Blood also contains cells, causing relative viscosity toincrease steeply with hematocrit (the concentration of red cells in blood). The relative viscosityof blood is 3.5 to 5.5.
There are several conditions that increase blood viscosity and make the heart work harder. Forexample:
Life at high altitudes increases the hematocrit to compensate for the reducedavailability of oxygen,
Polycythemia vera is a disease that causes overproduction of red blood cells, thereby
increasing hematocrit and blood viscosity, Sickle-Cell Anemia reduces the pliability of red blood cells and makes them harder to
push through smaller vessels. This also increases its apparent viscosity.
-
7/31/2019 Hemodynamics 2011 (1)
9/13
2011 Hemodynamics Page 9 of 13 RJ Barsotti, Ph.D.
Series and Parallel ResistancesThe resistance of a system of tubesarranged in series will be the total of theindividual resistances. The addition of
another resistor in series will alwaysincrease the total network resistance.Thus the combined resistance of vascularbeds that are plumbed in series is equal tothe sum of these resistances:
Rtotal = R1 + R2 + R3+
if the resistances of each component were equal R1 = R2 = R3 then: Rtotal = 3RThe addition of another component will increase Rtotal to 4R
In contrast, the resistance of a system of tubes arranged in parallel will be proportional to the
reciprocal of the resistances. The addition of another component in parallel will always
decrease the total network resistance. In a parallel system, the total resistance is less than
that of the individual components. The combined resistance of vascular beds that are plumbedin parallel is calculated as:
1 = 1 + 1 + 1 + Rtotal R1 R2 R3
if the resistances were equal R1 = R2 = R3 then: 1/Rtotal = 3/R or Rtotal = R/3
The addition of another component will decrease Rtotal to R/4
When dealing with parallel vascular arrangements it is more convenient to use conductancewhich is the reciprocal of resistance orC = 1/ R. So the above equation becomes
Ctotal = C1 + C2 + C3+
or the total conductance is the sum of the individual conductances. So, the addition of another
conduit increases flow and decreases resistance! This accounts in part for the lower resistancethrough the set capillaries than through the set of arterioles in the systemic circulation, despitethe smaller caliber of the individual capillaries than of the individual arterioles. The number ofparallel capillaries far exceeds the number of parallel arterioles (the cross-sectional area ofcapillaries bed is much greater than of the arteriole bed). The much greater number of systemic
capillaries than of systemic arterioles accounts for the lower resistance to flow through thecapillaries than the arterioles.
-
7/31/2019 Hemodynamics 2011 (1)
10/13
2011 Hemodynamics Page 10 of 13 RJ Barsotti, Ph.D.
Total Peripheral ResistanceThe sum of all the vascular resistances that lie between the aorta and the vena cava is referred to
as systemic vascular resistance (SVR) or total peripheral resistance (TPR).
How do we calculate SVR or TPR?We know that flow F = P / R
F is this case is better known as cardiac output or CO - about 5 L/min in an average resting
person. P is the pressure gradient that drives flow - the difference between aortic pressure andpressure in the right atrium - about 5 mm Hg). Aortic pressure fluctuates greatly between systole
and diastole, so a better and more common measure is Mean Arterial Pressure or MAP - about95 mm Hg in a normal person. Thus,
TPR = MAP - CVP = 95mmHg5mmHg = 18 mm Hg/L/minCO 5 L/min
A digression on arterial blood pressures: the aortic pressure curve shown below defines
systolic and diastolic bloodpressures. The difference between
the two is known as pulse pressure.Pulse pressure is largely determinedby heart stroke volume and by thecompliance of the arterial tree.
Thus, as the arteries harden with age (for example), the heart has to generate increasedpressures to ensure that the required stroke volume is ejected into the vasculature. From theaortic pressure trace over time, the shape of the pressure trace yields a mean arterial pressurevalue MAP that is less than the arithmetic average of the systolic and diastolic pressures asshown above. At normal resting heart rates, MAP can be approximated from the diastolic
blood pressure (Pdias) plus one third of pulse pressure (Psys - Pdias) orMAP = Pdias + (Psys - Pdias)
3
MAP = 85mmHg + (115mmHg85mmHg) = 95 mm Hg3mmHg
Viscosity, laminar flow, turbulent flow, and noiseWhen a fluid such as water or blood moves through a tube, it experiences drag caused by frictionbetween the fluid and the walls of the tube. This causes a layer of slower-moving fluid to formagainst the wall of the tube, which in turn exerts drag on the fluid closer to the center. This
causes another slowed layer to form which exerts its own drag - and so on toward the center ofthe tube. The net result is that fluid movement in tubes occurs in concentric layers, with fastestflow at the center and slowest flow up against the walls of the tube. This is referred to as laminaror streamlineflow. Fluid with viscosity independent of tube size or velocity of flow is said to be
"Newtonian." Blood is a non-Newtonian fluid and shows anomalous viscosity. In small tubes(< 0.3 mm in diameter) the viscosity of blood decreases.
-
7/31/2019 Hemodynamics 2011 (1)
11/13
2011 Hemodynamics Page 11 of 13 RJ Barsotti, Ph.D.
Laminar flow (B inadjacent Figure) isactually very efficient
and obeys Poiseuilles
law for as long as it ismaintained. As bloodvelocity increases,however, this flowpattern becomesincreasingly unstableand can become
turbulent (C in
adjacent Figure). Thismight occur when blood
is forced through a constriction for example, because velocity has to increase to maintain flow (F= v A).
Turbulent flow is less efficient than laminar flow because it contains cross-currents and eddiesand the fluid particles move from one region of the tube to another in an irregular fashion. Thismeans that a correspondingly greater pressure gradient is required to push turbulent bloodthrough a vessel, and it no longer conforms to Poiseuilles law.
The transition from laminar to turbulent flow is determined by several factors in addition to
velocity. These are combined into the non-dimensional Reynolds number (NR):
NR = v d
where v is mean velocity, d is vessel diameter, (rho) is blood density and is viscosity. Thus,turbulence is more likely where flow velocities are high and vessel diameter is large, or whenblood viscosity drops or density increases significantly. Generally, flow becomes turbulent when
NR exceeds 2000. Consider the Reynolds number as a threshold. Values greater than 2000indicate that flow is turbulent.
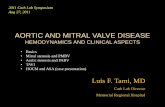
Turbulent flow is fairly uncommon in a healthy cardiovascular system. Usually, it only occurswhere blood is being forced at high velocity into large-diameter vessels, such as from the leftventricle into the aorta. There are three examples where this turbulence is noteworthy, however.When blood flow becomes turbulent, it sets up vibrations in walls of the vessel. These vibrations
travel to the body surface where they can be detected as murmurs using a stethoscope:
Congenital and pathological changes in the heart valves may prevent them fromopening normally. The heart responds by pumping at increased pressure to maintainadequate flow to the body, causing blood to be forced at high velocity through therestricted opening. The resultant turbulence generates characteristic murmurs that areuseful in diagnosing the condition.
A, Two fluids (one dyed red, and the other clear) before flow begins; B,the same fluids 1 second after flow begins; C, turbulent flow, withelements of the fluid moving in a disorderly pattern.
-
7/31/2019 Hemodynamics 2011 (1)
12/13
2011 Hemodynamics Page 12 of 13 RJ Barsotti, Ph.D.
Pregnancy causes a substantial increase in blood volume and cardiac output tosupport the developing fetus. Red blood cell production lags behind this increase,however, causing the hematocrit to fall. This, together with an increase in blood
velocity associated with increased cardiac output, causes the mothers (healthy) heartto generate murmurs, even without a structural change in the heart.
Partial occlusion of the brachial artery with a pressure cuff causes murmurs thatreflect blood spurting at high velocity through the constriction. These murmurs(Korotkoff sounds) can be heard with a stethoscope placed downstream ofthe cuff,providing a convenient way of approximating systolic and diastolic blood pressures.
Note especially that another of the important factors in Poiseuille's equation is the viscosity of theblood. The greater the viscosity, the less the flow in a vessel if all other factors are constant.
Furthermore, the viscosity of normal blood is about three times as great as the viscosity of
water. But what makes the blood so viscous? It is mainly the large numbers of suspended redcells in the blood, each of which exerts frictional drag against adjacent cells and against the wall
of the blood vessel. The percentage of the blood that is cells is called the hematocrit. Thus, if aperson has a hematocrit of 40, this means that 40 per cent of the blood volume is cells and theremainder is plasma. The hematocrit of men averages about 42, while that of women averagesabout 38. These values vary tremendously, depending on whether the person has anemia, on thedegree of bodily activity, and on the altitude at which the person resides.
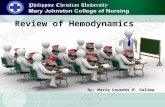
The viscosity of blood increasesdrastically as the hematocritincreases, as shown in the Figure.below. The viscosity of wholeblood at normal hematocrit is about3; this means that three times asmuch pressure is required to forcewhole blood as to force waterthrough the same blood vessel.When the hematocrit rises to 60 or70, which it often does inpolycythemia, the blood viscositycan become as great as 10 timesthat of water, and its flow throughblood vessels is greatly retarded.
-
7/31/2019 Hemodynamics 2011 (1)
13/13
2011 Hemodynamics Page 13 of 13 RJ Barsotti, Ph.D.
Effects of Pressure on Vascular Resistance and Tissue Blood Flow
From the discussion thus far, onemight expect an increase in arterialpressure to cause a proportionateincrease in blood flow through thevarious tissues of the body.However, the effect of pressure onblood flow is greater than onewould expect, as shown by theupward curving lines in the Figure.The reason for this is that anincrease in arterial pressure notonly increases the force that pushesblood through the vessels but alsodistends the vessels at the same
time, which decreases vascular resistance. Thus, greater pressure increases the flow in both ofthese ways. Therefore, for most tissues, blood flow at 100 mm Hg arterial pressure is usually fourto six times as great as blood flow at 50 mm Hg instead of two times as would be true if therewere no effect of increasing pressure to increase vascular diameter.
Note also in the Figure that the large changes in blood flow that can be caused by either increasedor decreased sympathetic nerve stimulation of the peripheral blood vessels. Thus, as shown in thefigure, inhibition ofsympathetic activity greatly dilates the vessels and can increase the blood
flow twofold or more. Conversely, very strong sympathetic stimulation can constrictthe vesselsso much that blood flow occasionally decreases to as low as zero for a few seconds despite higharterial pressure.