How to build relationships with journalists and get media exposure

Estimating the Exposure–Response Relationships between Particulate Matter and Mortality within the APHEA Multicity Project
CitationSamoli, Evangelia, Antonis Analitis, Giota Touloumi, Joel Schwartz, Hugh R. Anderson, Jordi Sunyer, Luigi Bisanti, et al. 2005. Estimating the Exposureâ Response Relationships between Particulate Matter and Mortality within the APHEA Multicity Project. Environmental Health Perspectives 113(1): 88-95.
Published Versiondoi:10.1289/ehp.7387
Permanent linkhttp://nrs.harvard.edu/urn-3:HUL.InstRepos:4874506
Terms of UseThis article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA
Share Your StoryThe Harvard community has made this article openly available.Please share how this access benefits you. Submit a story .
Accessibility

88 VOLUME 113 | NUMBER 1 | January 2005 • Environmental Health Perspectives
Research | Article
Many epidemiologic studies in recent years havedocumented adverse effects of ambient particu-late matter (PM) concentrations on mortality(Katsouyanni et al. 2001; Pope et al. 1995;Samet et al. 2000). The indications of adversehealth effects even at below-guideline levels haveled to revisions of air quality guidelines andstandards and scheduled dates for regular revi-sions in the future [Commission of EuropeanCommunities 1999; U.S. EnvironmentalProtection Agency (EPA) 1996; World HealthOrganization (WHO) 2000]. Most of thesestudies have assumed linear associations betweenair pollution and daily deaths, although in caseswhere concentrations reached high levels, loga-rithmic transformations have frequently beenused (Touloumi et al. 1994). However, theshape of the exposure–response relationship iscrucial for public health assessment, and therehas been growing demand for providing the rel-evant curves. Whether or not there is a thresh-old makes a large difference to the estimateof attributable deaths, and the shape of theexposure–response association is important forpredicting the benefits of policies reducingexposure.
Recently, multicity national or interna-tional programs have provided results basedon data from many cities (Katsouyanni et al.2001; Samet et al. 2000). Combined evidence
was obtained using hierarchical models imple-mented in two stages. In the first stage, datafrom each city were analyzed separately,whereas in the second stage, the city-specific airpollution estimates were regressed on city-spe-cific covariates to obtain overall estimates andto explore sources of possible heterogeneity.
In the United States, several multicitystudies have explored the exposure–responseassociation between particulate air pollutionand mortality (Daniels et al. 2000; Dominiciet al. 2002a; Schwartz and Zanobetti 2000).A linear association without threshold wasseen. Particulate characteristics differ consid-erably between Europe and the United States,and the high penetration of diesel engines inEurope makes mobile sources a much moreimportant source of urban particles there.Schwartz et al. (2001) confirmed that theexposure–response relation between airborneparticles and total daily deaths is essentiallylinear, at least at low to moderate concentra-tions in eight cities in Spain. Similarly, Rossiet al. (1999) found that in Milan, Italy, theassociation for all causes and cause-specificdeaths was almost identical to that noted bySchwartz et al. (2001).
One key limitation of these Europeanstudies (Rossi et al. 1999; Schwartz et al.2001) has been the use of data from a single
or a few locations. We address this limitationby presenting the results of analyses examiningthe exposure–response relationship betweendaily deaths and airborne particles within theAPHEA-2 (Air Pollution and Health—AEuropean Approach) project (Short-TermEffects of Air Pollution on Health: A Euro-pean Approach to Methodology, Exposure–Response Assessment and Evaluation of PublicHealth Significance) that uses an extensiveEuropean database from 30 cities. This data-base also allows a comprehensive and struc-tured approach at the second stage of theanalysis, in which we explore the role of effectmodifiers in explaining the heterogeneity in theshape of the exposure–response relation of airpollution and mortality across cities.
Materials and Methods
Data. The APHEA-2 project was a multicenterstudy including 30 cities across Europe andassociated regions (i.e., Istanbul, Turkey, andTel Aviv, Israel) that studied health effects of airpollution. Data were collected on daily countsof all-cause mortality (excluding deaths fromexternal causes) [International Classification ofDiseases, 9th Revision (ICD-9; WHO 2002)codes > 800], cardiovascular mortality (ICD-9390–459), and respiratory mortality (ICD-9460–519). The data covered at least 3 consecu-tive years for each city within the years1990–1997. Details about the data have beenpublished elsewhere (Katsouyanni et al. 2001).
Daily air pollution measurements wereprovided by the monitoring networks estab-lished in each town participating in theAPHEA-2 project. A monitor was included ifcertain completeness criteria were fulfilled
Address correspondence to E. Samoli, Departmentof Hygiene and Epidemiology, University of AthensMedical School, 75 Mikras Asias St., 115 27 Athens,Greece. Telephone: 30-210-7462085. Fax: 30-210-7462205. E-mail: [email protected]
This work was funded by Environment andClimate Programme contracts ENV4-CT97-0534and QLK4-CT-2001-30055 from the EuropeanCommission.
The authors declare they have no competingfinancial interests.
Received 5 July 2004; accepted 21 October 2004.
Estimating the Exposure–Response Relationships between ParticulateMatter and Mortality within the APHEA Multicity Project
Evangelia Samoli,1 Antonis Analitis,1 Giota Touloumi,1 Joel Schwartz,2 Hugh R. Anderson,3 Jordi Sunyer,4
Luigi Bisanti,5 Denis Zmirou,6 Judith M. Vonk,7 Juha Pekkanen,8 Pat Goodman,9 Anna Paldy,10
Christian Schindler,11 and Klea Katsouyanni1
1Department of Hygiene and Epidemiology, University of Athens, Athens, Greece; 2Harvard School of Public Health, Boston,Massachusetts, USA; 3Community Health Sciences, St. George’s Hospital Medical School, University of London, London, UnitedKingdom; 4Institut Municipal Investigacio Medica (IMIM), Barcelona, Spain; 5Azienda Sanitaria Locale della Città di Milano, Milano, Italy;6INSERM U420, Nancy, France; 7Department of Epidemiology and Statistics, University of Groningen, Groningen, the Netherlands;8National Public Health Institute, Unit of Environmental Epidemiology, Kuopio, Finland; 9Dublin Institute of Technology, Dublin, Ireland;10National Institute of Environmental Health, Budapest, Hungary; 11University of Basel, Institut fur Sozial-und Praventivmedizin, Basel,Switzerland
Several studies have reported significant health effects of air pollution even at low levels of airpollutants, but in most of theses studies linear nonthreshold relations were assumed. We investi-gated the exposure–response association between ambient particles and mortality in the 22 Europeancities participating in the APHEA (Air Pollution and Health—A European Approach) project, whichis the largest available European database. We estimated the exposure–response curves using regres-sion spline models with two knots and then combined the individual city estimates of the spline toget an overall exposure–response relationship. To further explore the heterogeneity in the observedcity-specific exposure–response associations, we investigated several city descriptive variables aspotential effect modifiers that could alter the shape of the curve. We conclude that the associationbetween ambient particles and mortality in the cities included in the present analysis, and in therange of the pollutant common in all analyzed cities, could be adequately estimated using the linearmodel. Our results confirm those previously reported in Europe and the United States. The hetero-geneity found in the different city-specific relations reflects real effect modification, which can beexplained partly by factors characterizing the air pollution mix, climate, and the health of the popula-tion. Key words: air pollution, exposure–response, heterogeneity, hierarchical modeling, mortality,splines. Environ Health Perspect 113:88–95 (2005). doi:10.1289/ehp.7387 available viahttp://dx.doi.org/ [Online 21 October 2004]

(Katsouyanni et al. 1996). Time-series data ondaily temperature (degrees centigrade, dailymean) and relative humidity (percent) wereused to control for the potential confoundingeffects of weather. External information oninfluenza epidemics or other unusual events(e.g., heat waves, strikes) was also collected, ifavailable (Katsouyanni et al. 2001).
In the present study we used the average oflags of 0 and 1 day for black smoke (BS) andPM < 10 µm in aerodynamic diameter (PM10)for all cities, because there is evidence that theaverage of 2 days’ pollution correlates betterwith mortality than a single day’s exposure(Schwartz 2000a).
Table 1 presents descriptive characteristicsof the analyzed cities. The Netherlands is con-sidered one urban area because of its relativelysmall size and dense population. Together, all30 areas have a population of > 60 millionpeople. The mean daily total number ofdeaths ranged from 6 (in Erfurt and Geneva)to 342 in the Netherlands. For respiratorymortality, daily rates ranged from 0 to 29. Themedian levels of BS and PM10 concentrationsranged from 9 to 63 µg/m3 and from 14 to65 µg/m3, respectively. BS levels representconcentrations of black particles with an aero-dynamic diameter < 4.5 µm (Department ofHealth 1995). These measurements have a
long history in Europe, and although stan-dards for BS have been replaced recently bythose for PM10 (Commission of EuropeanCommunities 1999), the results are displayedhere both for continuity and because there isevidence that BS exposure is more relevant tohealth effects than is PM10 (Bremner et al.1999; Brunekreef et al. 1997). BS is a bettermarker of primary combustion products andsmall particles (Reponen et al. 1996). Becausedomestic or industrial burning of coal is mini-mal in most of the cities studied, BS is morespecific for traffic-related particles than PM10and provides a means of addressing the ques-tion of particle composition.
The analysis was restricted to days withPM10 levels < 200 µg/m3 and days with BS< 150 µg/m3 because these few extreme valuescould influence disproportionally the results.Besides, air pollution mixes in the high con-centration range are likely to contain smallerfractions of the pollutants under investigation(primarily combustion particles). For example,Tel Aviv has the highest concentration of PM10,but the extreme values of the distribution are infact due to desert dust. Restricting analyses todays below these levels excluded < 2% of theavailable days in each city for PM10, and < 3%for BS, except for Athens, for which 3.8% of thedays were excluded in the BS analysis.
Methods. We used a hierarchic modelingapproach. First, we fit regression models ineach city separately to control for potentialconfounders. We used the results of the indi-vidual city analysis in a second-stage analysisto provide overall estimates and to investigatepotential effect modifiers.
Individual city analysis. We investigatedthe pollution–mortality associations for eachcity using Poisson regression models allowingfor overdispersion. The city-specific model isof the form
[1]
where E[Ytc] is the expected value of the
Poisson distributed variable Ytc indicating
the count of the health outcome on day t atcity c with var(Yt
c) = ϕE[Ytc], ϕ being the
overdispersion parameter; xitc is the value of
the xi meteorologic ovariate on day t at city c;Pt
c is the air pollution level on day t at city c;f c is the function defining the exposure–response relation between the pollutant andthe health outcome; and βo
c represents the
log
,
E Y f P
s time k
s
tc
oc c
tc
ctc
ic
i
⎡⎣ ⎤⎦ = + ( )+ ( )+ ∑
β
xx k
othersitc
i,
,
( )+ [ ]
Article | Ambient-particles–mortality exposure–response relation
Environmental Health Perspectives • VOLUME 113 | NUMBER 1 | January 2005 89
Table 1. City descriptive data on the study period, population, exposure (PM10 and BS), outcome (daily number of deaths), and selected effect modifiers (region,mean temperature, mean NO2 over 24 hr, and directly standardized mortality rate).
PM10 (µg/m3) BS (µg/m3)Study period Population No. of deaths per day percentile percentile Geographic Mean NO2
City (month/year) (× 1,000) Total CVD Respiratory 50th 90th 50th 90th region temperature (24-hr) SDR
Athens 1/92–12/96 3,073 73 64 5 40a 59 64 122 South 18 74 784Barcelona 1/91–12/96 1,644 40 32 4 60 95 39 64 South 16 69 740Basel 1/90–12/95 360 9 8 1 28a 55 West 11 38 678Bilbao 4/92–3/96 667 15 11 1 23 39 South 15 49 711Birmingham 1/92–12/96 2,300 61 50 9 21 40 11 22 West 10 46 895Budapest 1/92–12/95 1,931 80 57 3 40a 52 East 11 76 1,136Cracow 1/90–12/96 746 18 13 0 54a 86 36 101 East 8 44 1,009Dublin 1/90–12/96 482 13 10 2 10 26 West 10 — 940Erfurt 1/91–12/95 216 6 — — 48 98 West 9 40 972Geneva 1/90–12/95 317 6 4 0 33a 71 West 10 45 608Helsinki 1/93–12/96 828 18 14 2 23a 49 West 6 33 915Ljubljana 1/92–12/96 322 7 5 0 13 42 East 11 46 823Lodz 1/90–12/96 828 30 20 1 30 77 East 8 39 1,231London 1/92–12/96 6,905 169 139 29 25 46 11 22 West 12 61 851Lyon 1/93–12/97 416 9 7 1 39 63 West 12 63 579Madrid 1/92–12/95 3,012 61 46 6 33 59 South 15 70 636Marseille 1/90–12/95 855 22 18 2 34 56 West 16 71 666Milan 1/90–12/96 1,343 29 23 2 47a 88 West 14 94 632Netherlands 1/90–9/95 15,400 342 140 29 34 67 63 122 West 10 43 757Paris 1/92–12/96 6,700 124 91 9 22 46 21 45 West 12 53 644Poznan 1/90–12/96 582 17 12 1 23 76 East 9 47 1,106Prague 2/92–12/95 1,213 38 30 1 66 124 East 10 58 984Rome 1/92–12/96 2,775 56 44 3 57a 81 South 17 88 585Stockholm 1/94–12/96 1,126 30 25 3 14 27 West 8 26 666Tel Aviv 1/93–12/96 1,141 27 22 2 43 75 South 20 70 430Teplice 1/90–12/97 625 18 13 1 42 83 East 9 32 1,173Torino 1/90–12/96 926 21 17 1 65a 129 West 14 76 724Valencia 1/94–12/96 753 16 14 2 40 70 South 19 66 820Wroclaw 1/90–12/96 643 15 10 1 33 97 East 9 27 970Zurich 1/90–12/95 540 13 10 1 28a 54 West 11 40 666
Abbreviations: —, no data; CVD, cardiovascular deaths; SDR, directly standardized mortality rate. Mean temperature in degrees centigrade.aPM10 were estimated using a regression model relating collocated PM10 measurements to the BS or total suspended particles.

baseline mortality in city c. The smooth func-tions s capture the nonlinear relationship withcovariates and can be defined as a linear com-bination of a set of functions {bj} with conve-nient properties; that is, s = Σjajbj (Wood andAugustin 2002). Then k is the number ofthese basis functions {bj}. We also includeddummy variables for the day of the weekeffect, holidays, and influenza epidemics.
In the last decade, the use of generalizedadditive models (GAM), which allow non-parametric smooth functions to control forpossible confounders, was a standard approachon air pollution time series analysis. Recently,Dominici et al. (2002b) identified that theapplication of GAM models in the S-Plus soft-ware (MathSoft, Inc., Cambridge, MA, USA)with the default convergence criteria leads tobiased parameters’ estimates, whereas Ramsayet al. (2003) found in addition that this func-tion underestimated the parameters’ variances.In response to these findings, we used thepenalized regression splines as smoothingfunctions, as implemented by Wood (2000) inR, a public-domain implementation of theS language on which S-Plus is based.
We followed the general methodologicguidelines developed within the framework ofthe APHEA-2 project, described in detailelsewhere (Touloumi et al. 2004). The basicdifference from the APHEA-2 methodologyis the use of penalized regression splinesinstead of the nonparametric function loess assmoothing functions to control for possibleconfounding. According to the APHEA-2methodology, these smooth functions of timeserve as a proxy for any time-dependent out-come predictors with long-term trends andseasonal patterns not explicitly included inthe model. Hence, we remove long-termtrends and seasonal patterns from the data toguard against this confounding by omittedvariables. Weather variables, which we believeare causally connected to deaths, were alsoincluded. In particular, same-day temperatureand humidity and a lagged value of thesemeteorologic variables were also included in
the models. We used thin-plate regressionsplines as basis functions for the penalizedregression splines (Wood 2003). In the case ofpenalized regression splines, as implemented byWood (2000), k in Equation 1 denotes thenumber of basis functions used for the corre-sponding variable fit. The choice of a smallnumber of basis functions can have a substan-tial effect on the final model, because it placesan upper bound on how variable the solutioncan be. Given our experiences from the previ-ous analyses of the APHEA-2 data, we chosethe number of basis functions (k) to be 40 forthe time variable and 10 for the weather vari-ables. We then chose the smoothing parame-ters that minimized the absolute value of thesum of partial autocorrelations (PACs) of theresiduals from lags 3 to 30 days. The choice oflags was based on the fact that in mortalityhealth outcomes there was usually strongremaining PAC in the first two lags of theresiduals, which could influence the sum dis-proportionally. To account for serial correla-tion in the cases that it remained in the finalmodel residuals, we added autoregressive termsinto the model, based on the methodologydescribed by Brumback et al. (2000). In thespecial case of the small cities (and especially incause-specific mortality), where the above crite-rion may lead to almost linear fit for the sea-sonality, we allowed more degrees of freedomfor time provided that this imposed only aminor burden in the sum of the residual PACs.When such a case occurred, we allowed asminimum 1 degree of freedom per year.
Day of the week effects, holidays, and epi-demics were controlled for by using dummyvariables. We used the APHEA-2 method forinfluenza control, including a dummy vari-able taking the value of one when the 7-daymoving average of the respiratory mortalitywas greater than the 90th percentile of itscity-specific distribution. Because influenzacontrol as described was based on the distrib-ution of respiratory mortality, we includedthe influenza dummy variable only when weanalyzed total and cardiovascular mortality.
Based on previously published results (Bragaand Zanobetti 2000; Touloumi et al., Inpress), there is no indication that omittingcontrol for influenza when we analyzed respi-ratory mortality would influence the associa-tion between air pollution and mortality. It isunclear why the specific time within a winterthat an epidemic occurs in a particular cityshould have much to do with air pollutionlevels and hence confound the relation underinvestigation.
Regression cubic splines were used to esti-mate the exposure–response relationship foreach city (Samoli et al. 2003), defined by thefunction f in Equation 1. The regression cubicspline function of a variable P is (Durrlemanand Simon 1989)
[2]
where k is the number of knots, and using the+ notation of Smith (1979),
[3]
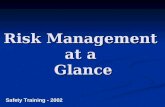
For each health outcome, the knots were pre-specified and were the same for each city. Thishad the advantage that similar terms werepooled in the second stage of the analysis. Thenumber and location of the knots were deter-mined according to exploratory graphicalanalysis results. Three distinct patterns weredominant across cities in each case—that is,linear and two parabolas. Figure 1 shows thepatterns of the particles–total-mortality expo-sure–response relations in London, England,Athens, Greece, and Cracow, Poland, thelargest cities in each of the three distinct geo-graphic areas (western, southern, and easternEuropean cities). When exploring thePM10–mortality relationship we decided touse a cubic spline with two knots at 30 and50 µg/m3, for all mortality outcomes, to suffi-ciently capture the association in our data.When exploring the relation of BS with mor-tality we used a regression cubic spline withtwo knots at 40 and 70 µg/m3 in the case oftotal mortality, at 30 and 60 µg/m3 for cardio-vascular mortality and at 20 and 50 µg/m3 forrespiratory mortality.
To further explore indications of potentialthreshold levels, we fitted threshold models byapplying piecewise linear models. We also fit-ted models with a linear association betweenthe pollutant and mortality to compare thegoodness of fit of the different approaches.
Second-stage analysis. In the second stagewe regressed the city-specific air pollutioneffect estimates produced form the first stageof the analysis (βc) on city-specific covariates(Zc) to obtain the overall exposure–response
P PP P P P
i
i i–
– ,
,.( ) =
>⎧⎨⎪
⎩⎪
⎫⎬⎪
⎭⎪+
0 otherwise
f P P P Pjj
ji i
i
k
( ) = +∑ ( )∑=
+=
β β00
3
33
1– ,
Article | Samoli et al.
90 VOLUME 113 | NUMBER 1 | January 2005 • Environmental Health Perspectives
Figure 1. Exposure–response curves of PM10 (A) and BS (B) with total mortality in London, Athens, and Cracow.
20
15
10
5
0
–5
20
15
10
5
0
–5
0 50 100 150 200 0 50 100 150 200
Perc
ent i
ncre
ase
in d
eath
s
Perc
ent i
ncre
ase
in d
eath
s
Lag 0–1 particles (µg/m3) Lag 0–1 particles (µg/m3)
LondonAthensCracow
BA

curve and to explore potential heterogeneityin the city-specific curves (Samoli et al. 2003).For the linear model, βc is the log-relative ratein city c, whereas for the spline model, βc isthe vector of the regression coefficients corre-sponding to the spline function.
For the spline method, we fitted multivari-ate second stage regression models based onthe method described by Berkey et al. (1998).More specifically, the models are of the form
βc = Zcα + δc + εc, [4]
where βc is the (5 × 1) vector of the five splineestimates in each city c (the intercept term inEquation 2 was ignored because only relativerisks are considered); Zc is a 5 × 5p matrix,where p is the number of city level covariatesfor city c (including the intercept); α is thevector of regression coefficients to be esti-mated; δc is a vector of five random effectsassociated with city c representing, for eachspline estimate, the city’s deviation from theoverall model; and εc (assumed independentfrom δc) is the vector of sampling errorswithin each city.
The 5 × 5 matrix cov(δc) = D representsthe within-city covariances of the randomeffects capturing determinants of the city-specific regression coefficients other thansampling error and the city-level covariatesconsidered. It is assumed that δc follows themultivariate normal distribution (MVN) withmean 0 and variance-covariance matrix D—that is, δc ~ MVN (0, D), and εc ~ MVN (0,Sc), βc ~ MVN (Zcα, D + Sc) where Sc is thecovariance matrix of the five regression coeffi-cients of the spline function in city c that isestimated in the first stage of the analysis.When D ≈ 0 we get the corresponding fixedeffects estimates, whereas when D ≠ 0 we getthe random effects estimates.
The iterative generalized least squaresmethod was applied to estimate model para-meters. The parameters of the between-citycovariance matrix D are estimated by maxi-mum likelihood (Berkey et al. 1998). Weapplied an overall chi-square test to examineheterogeneity (Touloumi et al. 2004).
When assuming a linear exposure–responserelation model, Equation 4 collapses to a uni-variate one that expresses the usual meta-regres-sion. In this case D denotes the between-cityvariance in the effects estimates and can be esti-mated from the data using the maximum likeli-hood method described by Berkey et al. (1995).
After obtaining an overall curve that drawsinformation from all cities, we also comparedthe two types of models: the linear and thecubic regression spline, within each city andover all cities to determine which best fits thedata. We used the Akaike information criterion(AIC) (Akaike 1973) to compare the cubicspline to the linear exposure–response model
without threshold representing the standardapproach in time series analyses estimatingeffects of air pollution on mortality or morbid-ity. For an overall comparison of the differentmodels, we computed the sum of the city-specific AIC values.
As an alternative way to compare the twoapproaches—the linear and spline models—wecomputed the difference between the deviancesof the fitted models. This difference follows achi-square distribution with degrees of freedomthe difference in the degrees of freedom of thefitted models. For an overall comparison of thedifferent models, we computed the sum of thecity-specific differences in deviance, whichagain follows the chi-square distribution withdegrees of freedom the sum of the city-specificdifference in the degrees of freedom.
Results
There was significant heterogeneity for allpollutant–mortality relationships under inves-tigation. Although the observed heterogeneitywas either explained or substantially reducedwhen we investigated the effect modificationpatterns, all results presented are from the ran-dom effects models for consistency reasons.When there was no significant heterogeneityleft, results from the fixed-effects models werealmost identical to those obtained under therandom effects models.
Figure 2 shows the estimated overallexposure–response curves between PM10 andtotal, cardiovascular, and respiratory mortalityand their 95% confidence intervals (CIs). Notall cities have values for the pollutant at bothends of the distribution, which is obvious fromthe wide CIs in the end points of the data.Excluding Stockholm, Sweden, from the analy-sis, which is the city with the lowest values, theresulting curves were almost identical. Withinthe range of 36 to 83 µg/m3—that is, thecommon range of the pollutant levels across theanalyzed cities—the combined exposure–response curves could be adequately approxi-mated by a linear association. Although allthree curves are similar in that range, a steeperslope is indicated for cardiovascular mortality.Overall, for total and cardiovascular mortality,
the spline curves are roughly linear, consistentwith the absence of a threshold. The curve forrespiratory mortality suggests that a thresholdmodel might be reasonable. The downwardcurve for the exposure–response relationshipbetween respiratory mortality and PM10 in thelower end of the distribution of the pollutant isalso evident in most of the city-specific expo-sure–response curves. In the case of total or car-diovascular mortality, this shape is evident inonly about five (out of the 22) cities, whereas alinear or logarithmic shape is evident in abouthalf of the analyzed cities. Based on the esti-mated overall exposure–response curves, anincrease from 50 to 60 µg/m3 is associated withan increase of about 0.4% in total deaths andwith increases of about 0.5% in both cardiovas-cular and respiratory deaths. These are consis-tent with the results from regressions assuminga linear relation giving an estimated increase ofabout 0.5% for total mortality and 0.7% forcardiovascular and respiratory mortality, for a10-µg/m3 increment in PM10.
Figure 3 shows the estimated combinedoverall exposure–response curves between BSand total, cardiovascular, and respiratory mor-tality along with their 95% CIs. As with PM10,the spline curves are roughly linear, consistentwith the absence of a threshold. In the case ofBS, though, the association is steeper betweenrespiratory mortality and the pollutant. This isconsistent also with the results assuming alinear association, which indicate a higherincrease for respiratory mortality. The bump inthe exposure–response relation between respi-ratory mortality and PM10 is not so apparentin the case of BS. Nevertheless, in the lowerend of the distribution of the pollutant thisassociation shows a small curvature notobserved with the other two outcomes; hence,there is suggestion of a possible threshold.
We examined the hypothesis of linearityin the pollutant–mortality relation more for-mally by comparing the AIC values obtainedunder the linear and the spline models. In allcases, both models gave very similar AIC val-ues. Overall the linear model gave a slightlybetter fit, because the AIC was lower by about0.1% in all pollutant–mortality combinations.
Article | Ambient-particles–mortality exposure–response relation
Environmental Health Perspectives • VOLUME 113 | NUMBER 1 | January 2005 91
Figure 2. Exposure–response curves and 95% CIsof PM10 and total, cardiovascular, and respiratorymortality.
Figure 3. Exposure–response curves and 95% CIsof BS and total, cardiovascular, and respiratorymortality.
20
15
10
5
0
–5
0 50 100 150 200
Perc
ent i
ncre
ase
in d
eath
s
PM10 (µg/m3)
TotalCardiovascularRespiratory
20
15
10
5
0
–5
0 50 100 150
Perc
ent i
ncre
ase
in d
eath
s
BS (µg/m3)
TotalCardiovascularRespiratory

On the other hand, the deviance under thespline model was smaller. In all pollutant–mortality relations, apart from respiratorymortality and BS for which no significantdepartures from linearity were observed, theoverall difference in the deviance between thelinear and the spline models was statisticallysignificant, whereas the great majority of thecity-specific differences in the deviance ofthe two models was not statistically significantand in accordance with the findings fromthe AIC.
We further tested the sensitivity of theresults to the number and location of theknots of the spline specification. We re-ran theanalysis by specifying one knot at 40 µg/m3,and the results were largely similar to the onespresented.
To further explore the indication of athreshold, especially in the case of the associa-tion between PM10 and respiratory mortality,we applied threshold models with a thresholdlevel at 20 µg/m3, because this was indicatedby the pooled spline curves. The model com-parisons between the linear and the thresholdmodels, based on both the AIC and the differ-ence in the deviance, always chose the linearexposure–response model.
To contribute to the ongoing discussionon whether there is a threshold below currentlimit values (40 or 50 µg/m3), we also fittedthreshold models after excluding data at con-centrations > 50 µg/m3. We tried two thresh-old models defining the threshold level at 20and 10 µg/m3 because those were indicatedby our spline analysis. In any case, the linearmodels gave a better fit.
We investigated the observed heterogene-ity by taking into account the potential effectmodifiers through second stage regressionmodels. Potential effect modifiers used in theAPHEA-2 analysis included variables describ-ing the air pollution level and mix in eachcity, the health status of the population, thegeographic area, and the climatic conditions(Katsouyanni et al. 2001). We present herethe exposure–response curves as shaped by themost important effect modifier from each ofthe above four distinct categories describedabove. Namely, we present the associations asthey are shaped by the geographic region, thetemperature levels, the mean level of nitrogendioxide (24 hr), and the age-standardizedannual mortality rate per 100,000. All thereported effect modifiers were statistically sig-nificant apart from the effect of NO2 on theassociation between respiratory mortality andBS. The mean temperature levels in the citiesincluded in the analysis ranged from 6°Cin Helsinki, Finland, to 20°C in Tel Aviv,the mean level of NO2 (24 hr) ranged from26 µg/m3 in Stockholm to 94 µg/m3 in Milan,Italy, and the standardized mortality rateranged from 430 in Tel Aviv to 1,231 in Lodz,
Poland (Table 1). The temperature levelsdiffered significantly among the three geo-graphic areas, whereas the standardized mor-tality rate differed between the eastern andother cities and the mean NO2 24 hr levelsdiffered between the southern and other cities.The highest correlations (Spearman r = 0.86)were observed between temperature and meanNO2 24-hr levels in the cities that providedBS data.
Each of the presented effect modifiersexplained in most cases > 20% of the observedheterogeneity. We present the exposure–response curves as observed in the threedistinct geographic regions included in theanalysis (western cities, southern cities, andcentral-eastern European cities). We also pre-sent the exposure–response curves as shapedfor cities with corresponding levels of the pre-sented effect modifier equal to the 25th andthe 75th percentile of the distribution of therelevant effect modifier.
Figure 4 shows the resulting exposure–response curves (and 95% CIs) for PM10 andtotal mortality. The exposure–response curvesfor the western and southern cities are similar,although the latter is steeper. The correspond-ing curve for the eastern cities is very steep inthe lower end of the pollutant distribution—that is, at levels < 30 µg/m3. However, the min-imum value for the pollutant in those areas is10 µg/m3, so in fact the part of the curve belowthat point is an extrapolation, whereas between10 and 30 µg/m3 only a small proportion of thetotal data contribute to the estimation, makingestimates unstable. The remaining effect modi-fication patterns indicate that the effect of the
pollutant on mortality is greater in areas withhigher temperature and mean NO2 (24-hr)levels, and lower standardized mortality rate.These results are in agreement with thoseobserved when a linear association of PM10 andtotal mortality is assumed (APHEA, unpub-lished data; Katsouyanni et al. 2001).
When we investigated the heterogeneity ofthe relation between PM10 and respiratorymortality by geographic region, as in totalmortality, the exposure–response curves forthe western and southern cities were similar,although the latter was steeper. The corre-sponding curve for the eastern cities had thesteepest slope. However, the whole curve waspoorly estimated, because of the small counts.The remaining effect modification patternswere not so clear, with lines crossing over therange of the relevant effect modifier. The curvecorresponding to the 25th percentile of theNO2 (24-hr) distribution is steeper from thelevel of 50 µg/m3 until the level of approxi-mately 150 µg/m3, whereas in the range from20 to 50 µg/m3 the slope of the curve corre-sponding to the 75th percentile is steeper. Thecurves corresponding to the effect modificationby temperature levels are similar, although, asbefore, in the lower level of the pollutant distri-bution the slope corresponding to higher tem-perature is steeper, and in the higher level ofthe pollutant the slope corresponding to lowertemperature is steeper. The effect modificationpattern of the standardized mortality rate indi-cates a steeper slope for higher ratios, except forthe range of the pollutant from about 20 to50 µg/m3, where the slope corresponding tolower ratios is steeper.
Article | Samoli et al.
92 VOLUME 113 | NUMBER 1 | January 2005 • Environmental Health Perspectives
Figure 4. Exposure–response curves and their 95% CIs of PM10 and total mortality in different geographicareas (A), and in the 25th and 75th percentiles of the distribution of temperature (B), standardized mortalityrate (C), and mean NO2 24-hr levels (D).
25
20
15
10
5
0
–5
0 50 100 150
Perc
ent i
ncre
ase
in d
eath
s
PM10 (µg/m3)
25
20
15
10
5
0
–5Perc
ent i
ncre
ase
in d
eath
s
Perc
ent i
ncre
ase
in d
eath
sPe
rcen
t inc
reas
e in
dea
ths
200 0 50 100 150 200
0 50 100 150 200 0 50 100 150 200
PM10 (µg/m3)
PM10 (µg/m3) PM10 (µg/m3)
BA
DC
WesternSouthernEastern
25th percentile75th percentile
25th percentile75th percentile
25th percentile75th percentile
25
20
15
10
5
0
–5
25
20
15
10
5
0
–5

Figure 5 shows the resulting exposure–response curves (and 95% CIs) for BS andtotal mortality. The effect modification pat-terns for BS are more linear than the onesobserved for PM10. Apart from the edges, theexposure–response curves for the western andeastern cities are similar, although the latter isslightly steeper. The corresponding curve forthe southern cities indicates the strongesteffect of the pollutant on mortality. The othereffect modification patterns indicate that theeffect of the pollutant on mortality is greater inareas with higher temperature levels and meanNO2 (24-hr) levels and lower standardizedmortality rates. These results are in agreementwith those observed when a linear associationof BS and total mortality is assumed (APHEA,unpublished data; Katsouyanni et al. 2001).
When we investigated the heterogeneity inthe BS–respiratory mortality association, thecurvature observed in the lower end of theoverall exposure–response curve of PM10 andBS with respiratory mortality (Figure 1) wasalso apparent in about half of the relationshipsas those were shaped by the different effectmodifiers. As was the case with PM10, theexposure–response curve for the eastern citieshad the steepest slope. However, also southerncities had, on average, a substantially steeperslope than the western cities, where in fact norelation was observed. The remaining effectmodification patterns were not so clear. Thecurve corresponding to the 25th percentile ofthe NO2 (24-hr) distribution was steeper up toapproximately 30 µg/m3, and above that theslope of the curve corresponding to the 75thpercentile was steeper. Similarly, the curves
corresponding to the effect modification bytemperature levels indicated that in the lowerlevel of the pollutant distribution the slope cor-responding to lower temperature was steeperand in the higher level of the pollutant theslope corresponding to higher temperature wassteeper. The effect modification pattern of thestandardized mortality rate indicated a steeperslope for higher rates.
Discussion
In recent years there has been growingdemand from policy makers for better under-standing of the exposure–response relationshipbetween air pollution and various adversehealth effects, including mortality. Most of therelevant studies in Europe were carried outwithin a small number of locations and conse-quently have limited statistical power to pro-vide evidence in support of a particular model.We used the most extensive database availablein Europe until today (Katsouyanni et al.2001) to investigate the exposure–responserelation between ambient particle concentra-tions and the daily number of deaths. By useof multiple locations, power is gained andgeneralizability is enhanced.
We used cubic splines to estimate nonlin-ear relations of particulate air pollution withmortality. Our results (Figures 2 and 3) indi-cate that the spline curves for both PM10 andBS with total and cardiovascular mortality areroughly linear, consistent with the absence ofa threshold. The curve for respiratory mortal-ity suggests that there is some evidence fordeviation from linearity in the lowest levels ofthe pollutants distribution.
There was significant heterogeneity in allassociations under investigation. However, thechi-square test applied for the investigation ofheterogeneity has very high power when manystudies are included in the meta-analysis, andespecially when these studies are large, as inour case (Higgins et al. 2003). Formal com-parison between spline and linear modelsbased on the AIC indicated that the linearmodels fit better. The result under the chi-square test indicating that in most of the pol-lutant–mortality associations the deviance ofthe spline models is significantly smaller maybe an artifact due to the sensitivity of the chi-square test. This claim is supported by thecity-specific results, where the conclusionsderived from the AIC and the chi-square testsare in agreement. In the great majority of thecities analyzed, the linear and spline modelsgave very similar fit; hence, the sensitivity ofthe overall chi-square test picks up the differ-ence in the few other cities. Another possibleexplanation is that the spline model capturesthe logarithmic shape of the relation in thehigher end of the pollutant’s distribution bet-ter, because fitting a logarithmic associationwith the pollutant gave the best fit.
It is well understood that the measuredparticle indicators represent a mixture, withvarying chemical and physical characteristics,reflected on different toxicity of parts of thismixture. Similarly, the populations studied inour analysis consist of subgroups with differ-ent sensitivity to PM exposure. It is likely thatthe exposure profile and sensitivity of eachsubgroup (indeed, of each individual) result invarious thresholds of effects that cannot beidentified with this methodology. The linearcurve resulting from our analysis may be seenas a composition of these postulated “partial”curves and may be used effectively for the pro-tection of the whole population. Clearly, moreresearch is needed to identify the most danger-ous components of the PM mixture and themost sensitive population subgroups. On theother hand, the biologic mechanisms underly-ing the PM–health outcome associations arenot yet completely clear.
The curvature of the exposure–responserelationship between ambient particles andrespiratory mortality in the lower levels of thepollutants, not so strongly observed for totaland cardiovascular mortality, suggests thatthere may be different mechanisms underly-ing the association of particulate pollutionexposure to different mortality health out-comes. Goodman et al. (2004) reported adifferent time response for cardiovascularmortality compared with respiratory mortal-ity, where cardiovascular mortality occurswithin the first few days of exposure, whereasrespiratory mortality showed a lag of up to2 weeks. This observed curvature couldalso be caused by the composition of the air
Article | Ambient-particles–mortality exposure–response relation
Environmental Health Perspectives • VOLUME 113 | NUMBER 1 | January 2005 93
Figure 5. Exposure–response curves and their 95% CIs of BS and total mortality in different geographicareas (A), and in the 25th and 75th percentiles of the distribution of temperature (B), standardized mortalityrate (C), and mean NO2 24-hr levels (D).
25
20
15
10
5
0
–5
0 50 100 150
Perc
ent i
ncre
ase
in d
eath
s
BS (µg/m3)
25
20
15
10
5
0
–5
25
20
15
10
5
0
–5
25
20
15
10
5
0
–5Perc
ent i
ncre
ase
in d
eath
s
Perc
ent i
ncre
ase
in d
eath
sPe
rcen
t inc
reas
e in
dea
ths
BA
DC
BS (µg/m3)
BS (µg/m3) BS (µg/m3)
WesternSouthernEastern
25th percentile75th percentile
25th percentile75th percentile
25th percentile75th percentile
0 50 100 150
0 50 100 1500 50 100 150

pollution mix at the low concentrations. Thisrationale is based on the fact that PM10measurements represent all particles withaerodynamic diameter < 10 µm, a mixture ofprimary and secondary particles from differ-ent sources with varying characteristics andlevels of toxicity. Unfortunately, the presentstudy does not have enough information tosufficiently investigate this possibility.
Nevertheless, in the range of the pollutantscommon to all the cities included in the analy-ses, all associations were approximately linear.The above results are consistent with thosereported in previous studies in Europe (Rossiet al. 1999; Schwartz et al. 2001) and in theUnited States (Daniels et al. 2000; Dominiciet al. 2002a; Schwartz and Zanobetti 2000).The slope of the association between ambientparticles and total or cardiovascular mortality ishigher for levels < 50 µg/m3 (and > 10 µg/m3
where there is enough information). This isconsistent from the results from 10 U.S. citiesanalyzed by Schwartz (2000b).
Formal comparison between thresholdand linear models, based either on the AIC oron the deviance chi-square test, showed thatlinear models would on average fit better thanthe threshold ones.
We investigated several factors that poten-tially influence the exposure–response rela-tions and might provide some explanations forthe different shapes observed in different loca-tions. Specifically, in the range of the pollu-tants common in all analyzed cities, theexposure–response curves between ambientparticles and total or cardiovascular mortalitywere steeper in southern European cities. Theassociation between particles and total andcardiovascular mortality was steeper in loca-tions with hotter climates, higher mean NO2(24-hr) levels, and lower standardized mortal-ity rates. The effect of NO2 suggests that par-ticles originating from vehicle exhausts aremore toxic than those from other sources. Apossible explanation for the temperature effecton the exposure–response association may bethat in warmer countries, outdoor fixed-siteair pollution measurements may represent theaverage population exposure better than themeasurements in colder climates, because peo-ple tend to keep their windows open andspend more time outdoors in warmer climates.Finally, in this study a large age-standardizedmortality rate was related to a smaller propor-tion of elderly persons and probably to thepresence of competing risks for the same dis-ease entities. It is therefore related to a smallerproportion of people belonging to vulnerablegroups who are more susceptible to air pollu-tion effects. The above-reported effect modifi-cation patterns are in accordance with thecorresponding ones when a linear pollutant–mortality association was assumed (APHEA,unpublished data; Katsouyanni et al. 2001).
When we investigated the relation withrespiratory mortality, the exposure–responsecurves were steeper in Eastern European cities.The effect modification patterns betweenambient particles and respiratory mortality areless clear and need further investigation. In therange of the pollutants common in all ana-lyzed cities, the exposure–response curves aresteeper in eastern European cities. Also, incities with higher standardized mortality rates,the slopes were steeper. These findings supple-ment each other, because in the cities includedin our analysis, all eastern cities had high stan-dardized mortality rates. The effect on the par-ticles–respiratory mortality association of theremaining potential effect modifiers investi-gated is analogous to the ones observed in thecases of total and cardiovascular mortality.Namely, in the range of the pollutants mostcommonly observed, cities with highertemperatures and mean NO2 (24-hr) levelspresent steeper slopes.
In conclusion, the association betweenambient particles and mortality in the citiesincluded in the present analysis could be ade-quately estimated using the linear model.Our results confirm those previously reportedfrom Europe and the United States. The het-erogeneity found in the different city-specificrelations reflects real effect modification,which can be explained partly by factors char-acterizing the air pollution mix, climate, andthe health of the population. Hence, measuresthat focus on lowering air pollution concentra-tions have greater public health benefits thanthose that focus on a few days with the highestconcentrations (Clancy et al. 2002). The ten-dency for a curvature at levels < 20 µg/m3, iftrue, is likely to reflect differences in the mix-ture and toxicity at different levels. Furtherstudy focusing on the composition of particlesis needed to further our understanding of theetiologic mechanism through which particlesaffect mortality and particularly respiratorymortality.
REFERENCES
Akaike H. 1973. Information theory and an extension of themaximum likelihood principal. In: Second InternationalSymposium on Information Theory, Tsahkadsor, Armenia,USSR, September 2–8, 1971 (Petrov BN, Csáki F, eds).Budapest:Akadémiai Kiadó, 267–281.
Berkey CS, Hoaglin DC, Antczak-Bouckoms A, Mosteller F,Colditz GA. 1998. Meta-analysis of multiple outcomes byregression with random effects. Stat Med 17:2537–2550.
Berkey CS, Hoaglin DC, Mosteller F, Colditz GA. 1995. A random-effects regression model for meta-analysis. Stat Med14:395–411.
Braga A, Zanobetti A. 2000. Do respiratory epidemics confoundthe association between air pollution and daily deaths?Eur Respir J 16:723–726.
Bremner SA, Anderson HR, Atkinson RW, McMichael AJ,Bland JM, Strachan DP, et al. 1999. Short-term associa-tions between outdoor air pollution and mortality inLondon 1992–94. Occup Environ Med 56:237–244.
Brumback BA, Ryan LM, Schwartz JD, Neas LM, Stark PC,Burge HA. 2000. Transitional regression models, withapplication to environmental time series. JASA 95:16–27.
Brunekreef B, Janssen NA, de Hartog J, Harssema H, Knape M,Van Vliet P. 1997. Air pollution from truck traffic and lungfunction in children living near motorways. Epidemiology8:298–303.
Clancy L, Goodman P, Sinclair H, Dockery DW. 2002. Effect ofair-pollution control on death rates in Dublin, Ireland: anintervention study. Lancet 360(9341):1210–1214.
Commission of the European Communities. 1999. CouncilDirective 1999/30/EC Relating to Limit Values for SulphurDioxide, Oxides of Nitrogen, Particulate Matter and Leadin Ambient Air. Official J Eur Communities 163:41–60.
Daniels MJ, Dominici F, Samet JM, Zeger SL. 2000. Estimatingparticulate matter-mortality dose-response curves andthreshold levels: an analysis of daily time-series for the20 largest US cities. Am J Epidemiol 152(5):397–405.
Department of Health. 1995. Committee on the Medical Effectsof Air Pollution: Non-Biological Particles and Health.London:Her Majesty’s Stationery Office.
Dominici F, Daniels M, Zeger SL, Samet JM. 2002a. Air pollutionand mortality: estimating regional and national dose-response relationships. J Am Stat Assoc 97:100–111.
Dominici F, McDermott A, Zeger S, Samet J. 2002b. On the useof generalized additive models in time-series studies of airpollution and health. Am J Epidemiol 156:193–203.
Durrleman S, Simon R. 1989. Flexible regression models withcubic splines. Stat Med 8:551–561.
Goodman PG, Dockery DW, Clancy L. 2004. Cause-specificmortality and the extended effects of particulate pollutionand temperature exposure. Environ Health Perspect112:179–185.
Higgins J, Thompson S, Deeks J, Altman D. 2003. Measuringinconsistency in meta-analyses. Br Med J 327:557–560.
Katsouyanni K, Schwartz J, Spix C, Touloumi G, Zmirou D,Zanobetti A, et al. 1996. Short-term effects of air pollutionon health: a European approach using epidemiologic time-series data: the APHEA protocol. J Epidemiol CommunityHealth 50(suppl 1):S12–S18.
Katsouyanni K, Touloumi G, Samoli E, Gryparis A, Le Tertre A,Monopolis Y, et al. 2001. Confounding and effect modifica-tion in the short-term effects of ambient particles on totalmortality: results from 29 European cities within theAPHEA2 project. Epidemiology 12:521–531.
Pope CA III, Dockery DW, Schwartz J. 1995. Review of epi-demiological evidence of health effects of particulate airpollution. Inhal Toxicol 7:1–18.
Ramsay T, Burnett R, Krewski D. 2003. The effect of concurvityin generalized additive models linking mortality and ambi-ent air pollution. Epidemiology 14(1):18–23.
Reponen A, Ruuskanen J, Mirme A, Parjala E, Hoek G, Roemer W,et al. 1996. Comparison of five methods for measuring partic-ulate matter concentrations in cold winter climate. AtmosEnvironment 30:3873–3879.
Rossi G, Vigotti MA, Zanobetti A, Repetto F, Gianelle V,Schwartz J. 1999. Air pollution and cause-specificmortality in Milan, Italy, 1980–1989. Arch Environ Health54(3):158–164.
Samet JM, Dominici F, Curriero F, Coursac I, Zeger SL. 2000.Particulate air pollution and mortality: findings from 20 U.S.cities. N Engl J Med 343:1742–1757.
Samoli E, Touloumi G, Zanobetti A, Le Tertre A, Shindler C,Atkinson R, et al. 2003. Investigating the dose-responserelation between air pollution and total mortality inthe APHEA-2 multicity project. Occup Environ Med60:977–982.
Schwartz J. 2000a. The distributed lag between air pollutionand daily deaths. Epidemiology 11:320–326.
Schwartz J. 2000b. Assessing confounding, effect modifi-cation, and thresholds in the association between ambi-ent particles and daily deaths. Environ Health Perspect108:563–568.
Schwartz J, Ballester F, Saez M, Perez-Hoyos S, Bellido J,Cambra K, et al. 2001. The concentration–response relationbetween air pollution and daily deaths. Environ HealthPerspect 109:1001–1006.
Schwartz J, Zanobetti A. 2000. Using meta-smoothing to esti-mate dose-response trends across multiplie studies, withapplication to air pollution and daily death. Epidemiology11(6):666–672.
Smith PL. 1979. Splines as a useful and convenient statisticaltool. Am Stat 33:57–62.
Touloumi G, Atkinson R, Le Tetre A, Samoli E, Schwartz J,Schndler C, et al. 2004. Analysis of health outcome timeseries data in epidemiological studies. Environmetrics15:101–117.
Article | Samoli et al.
94 VOLUME 113 | NUMBER 1 | January 2005 • Environmental Health Perspectives

Article | Ambient-particles–mortality exposure–response relation
Environmental Health Perspectives • VOLUME 113 | NUMBER 1 | January 2005 95
Touloumi G, Pocock SJ, Katsouyanni K, Trichopoulos D. 1994.Short-term effects of air-pollution on daily mortality inAthens time-series analysis. Int J Epidemiol 23(5):957–967.
Touloumi G, Samoli E, Quenel P, Paldy A, Anderson HR, Zmirou D,et al. In press. Short-term effects of air pollution on totaland cardiovascular mortality: the confounding effects ofinfluenza epidemics. Epidemiology.
U.S. EPA. 1996. Review of the National Ambient Air QualityStandards for Particulate Matter: Policy Assessment of
Scientific and Technical Information. WAWPS Staff Paper.EPA-45/R-1996:96-013. Research Triangle Park, NC:U.S.Environmental Protection Agency, Office of Air QualityPlanning and Standards.
WHO. 2000. Air Quality Guidelines for Europe. 2nd ed.WHO Regional Publications European Series No 91.Copenhagen:World Health Organization.
WHO. 2002. International Classification of Diseases, 9thRevision. ICD-9-CM. Geneva:World Health Organization.
Wood SN. 2000. Modelling and smoothing parameter estima-tion with multiple quadratic penalties. J R Stat Soc Ser B62(1):413–428.
Wood SN. 2003. Thin plate resgression splines. J R Stat SocSer B 65(1):95–114
Wood SN, Augustin NH. 2002. GAMs with integrated modelselection using penalized regression splines and applica-tions to environmental modelling. Ecol Model 157:157–177.