Electrolyte Abnormalities in the Hospital: Diagnosis and ......Initial evaluation of Hyponatremia...
63
Electrolyte Abnormalities in the Hospital: Diagnosis and Management Matthew Rivara, MD, FASN Assistant Professor of Medicine Division of Nephrology University of Washington
Transcript of Electrolyte Abnormalities in the Hospital: Diagnosis and ......Initial evaluation of Hyponatremia...

ElectrolyteAbnormalitiesintheHospital:Diagnosisand
Management
MatthewRivara,MD,FASNAssistantProfessorofMedicine
DivisionofNephrologyUniversityofWashington

Objectives
Useacase-basedapproachtodiscussworkupandmanagementof…
1. Sodiumandwaterdisordersinhospitalizedpatients▫ Focusonhyponatremia
2. Potassiumdisordersinhospitalizedpatients▫ Focusonhypokalemia

HypokalemiaCase6–Ayoungwomanwithheartfailure
Case1:bodyfluid
compartments
Hyponatremia/HypernatremiaCase2:RavereviewsCase3:Acaseofiatrogenesis?Case4:Howmuchcanyoudrink?Case5:The“un-watered”patient
Summary & Take home points
Outline

Case1:BodyfluidcompartmentsA20yearoldmanpresentstothehospitalafterexperiencingagrandmalseizure.Examandvitalsondayofadmissionarenormal(PNawas140mEq/L).• Experiencesarecurrentwitnessedseizurex3minutes• Blooddrawnimmediatelyà+aniongapmetabolicacidosis,returnedtonormalinlessthan1hour.• PNawas154mEq/L,butfellbackdownto140mEq/Loverashortperiodoftime.• Noincreaseinurineoutput,orfreewateradministrationduringthistime
Question:WhatisthebasisoftheacuteriseinPNa?

Bodyfluidcompartments• Totalbodywater≈50-60%oftotalbodymass▫ 2/3inICFand1/3inECF▫ ECF:75%interstitial,25%plasmavolume
TBW = 40L (60% body weight of 70 kg person)
Intracellular fluid volume =
25L, 40% body weight
Extracellular fluid volume =
15L, 20% body weight
Inte
rsti
tia
l fl
uid
vo
lum
e =
12L
(80
% o
f E
CF
)
Pla
sma
vo
lum
e =
3L
(20
% o
f E
CF
)
2/3 1/3

Determinantsofvolumeofcells• ContentofNaintheECFisthemajordeterminantofitsvolume.
• ConcentrationofNaintheECFcompartmentisthemostimportantfactorinICFvolume(exceptwhencellshaveothereffectiveosmoles).
• MajorintracellularfactorresponsibleforaccumulationofwaterincellsisretentionofK
K+
K+ K+
K+
K+ K+
Na+
Na+
Na+
ICF ECF

ChangesinvolumesofbodyfluidswithIVfluids
K+
K+
K+
K+
Na+
Na+
ICF ECF Gain of pure water
K+ K+
K+ K+
Na+
Na+
ICF ECF ICF ECF
Na+
Na+
Gain of Isotonic Saline
K+
K+
K+
K+
Na+
Na+

BacktoCase1…
• Case:A20yearoldmanpresentstothehospitalafterexperiencingagrandmalseizure.Examandvitalsondayofadmissionarenormal(SNawas140mEq/L).Severalhourslaterheexperiencesawitnessedgrandmalseizure.SurprisinglyhoweverhisSNawas154mEq/L,butfellbackdownto140mEq/Loverashortperiodoftime
• Question:WhatisthebasisoftheacuteriseinhisSNa?

Answer
• Transienttranscellularshiftinwaterduetosuddenandmassiveincreaseineffectiveosmolesinskeletalmusclecells(pullsH2Oin)
Muscle Cell
H2O
Glycogen + ADP + Pi à ATP + 2H+ +
Na+/H2O
Na+/H2O
2 Lactate-

Case2:Ravereviews• A19y/omanwithhistoryofanorexianervosapresentstotheERwithcomplaintofweaknessandlethargy.PriortoadmissionwasataravewherehetookMDMA(Ecstasy/Molly)anddrankalargeamountofwatertoavoiddehydrationfromsweating.
• IntheED,hehadagrandmalseizurex3minutes.BloodwasdrawnimmediatelyaftertheseizureandSNawas130mEq/L.Uosm700mOsm/kg.
• AdmittedtoMedicineànextAM,SNawas120meq/L

Questions
• Is thisacutehyponatremia?• WhydidhehaveaseizureiftheSNawas130mEq/L?AndwhywasSNathenextmorninglower?
• Whatrolemayanorexianervosaplayintheclinicalpicture?
• Howdoyoumanage?
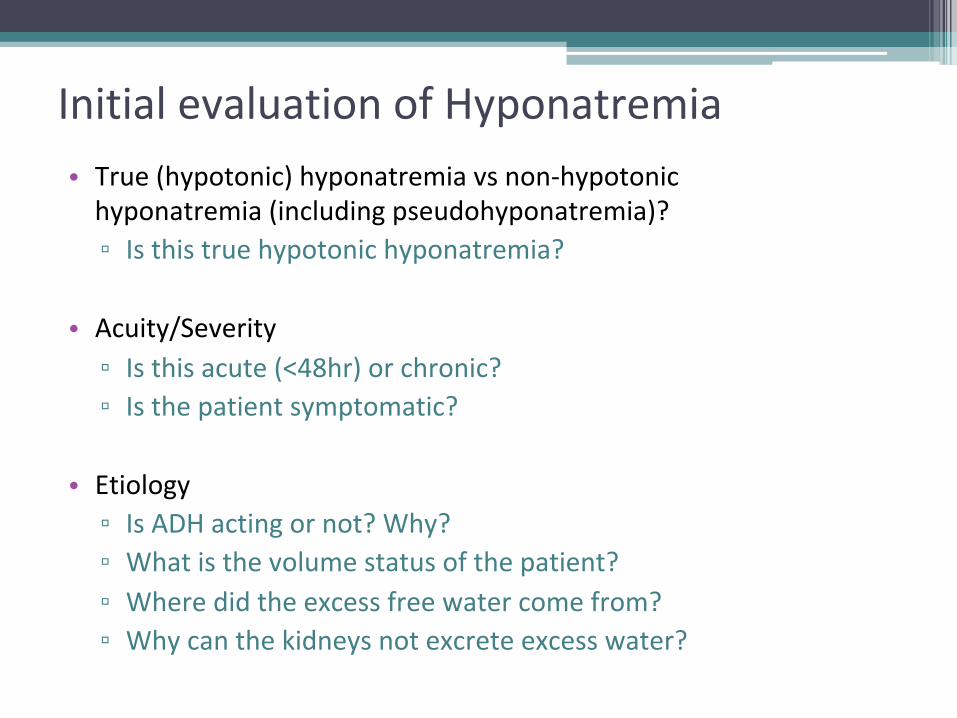
InitialevaluationofHyponatremia• True(hypotonic)hyponatremiavsnon-hypotonichyponatremia(includingpseudohyponatremia)?▫ Isthistruehypotonichyponatremia?
• Acuity/Severity▫ Isthisacute(<48hr)orchronic?▫ Isthepatientsymptomatic?
• Etiology▫ IsADHactingornot?Why?▫ Whatisthevolumestatusofthepatient?▫ Wheredidtheexcessfreewatercomefrom?▫ Whycanthekidneysnotexcreteexcesswater?

Non-hypotonichyponatremia• Hypertonicorisotonichyponatremia▫ Hyperglycemia� Dilutionalhyponatremia,noriskofcerebraledema� Cancalculate“corrected”serumsodium(predictedserumsodiumw/correctionofhyperglycemia)� 2mEq/Lforeach100mg/dLincreaseinglucose
▫ Rareothercauses� IVIGorsurgicalirrigantsolutions(glycineorsorbitol)
• Pseudohyponatremia(laboratoryartifact)▫ Hypertriglyceridemia(lessrelevantinmodernera)▫ Monoclonalgammopathy

InitialevaluationofHyponatremia• True(hypotonic)hyponatremiavsnon-hypotonichyponatremia(includingpseudohyponatremia)?▫ Notnecessarytotestforineverycase,buttor/o,checkserumosm
• Acuity/Severity▫ Isthisacute(<48hr)orchronic?▫ Isthepatientsymptomatic?
• Etiology▫ IsADHactingornot?Why?▫ Whatisthevolumestatusofthepatient?▫ Wheredidtheexcessfreewatercomefrom?▫ Whycanthekidneysnotexcreteexcesswater?

SymptomsofHyponatremiaIncreasing severity of
hyponatremia and rate of
[Na+] decline
Verbalis JG et al. Am J Physiol. 1986;250(3 pt 2):R444-R451. Slide credit: M. Rosner
Hyponatremic brain

Normalbrain
(normalosmolality)
Watergain(low
osmolality)
Lossofsodium,K+andCl–
(lowosmolality)
Lossoforganic
osmolytes(low
osmolality)
RateofHyponatremia:EffectsonCellularVolume
16
AdrogueHJetal.NEnglJMed.2000;342:1581-589.
Immediateeffectofhypotonicstate
RapidadaptationSlowadaptation
Propertherapy
Water
Understandingthecellularadaptationsiscriticalinthepropertreatmentofacutev.chronichyponatremia
Slide credit: M. Rosner

InitialevaluationofHyponatremia• True(hypotonic)hyponatremiavsnon-hypotonichyponatremia(includingpseudohyponatremia)?▫ Notnecessarytotestforineverycase,buttor/o,checkserumosm
• Acuity/Severity▫ Isthisacute(<48hr)orchronic?▫ Isthepatientsymptomatic?
• Etiology▫ IsADHactingornot?Why?▫ Whatisthevolumestatusofthepatient?▫ Wheredidtheexcessfreewatercomefrom?▫ Whycanthekidneysnotexcreteexcesswater?

Low EABV Edematous states (CHF, cirrhosis, nephrotic syndrome) Adrenal insufficiency (high CRH)
Stress, pain, nausea, drugs, carcinomas, pulmonary disorders, CNS disorders
Bhardwaj, Ann Neurol. 2006
Vasopressin(ADH)

InterpretingUrineOsmolarity
• ADH“on”or“off”?▫ [TestserumADHlevels]▫ Urineosmolarity?� ADH“on”àUosms>300� ADHappropriately“off”àUosms50-150
Collectingductepithelialcell
ADH
V2 receptor
H2O
Urinary space
H2O
H2O
Aquaporin 2
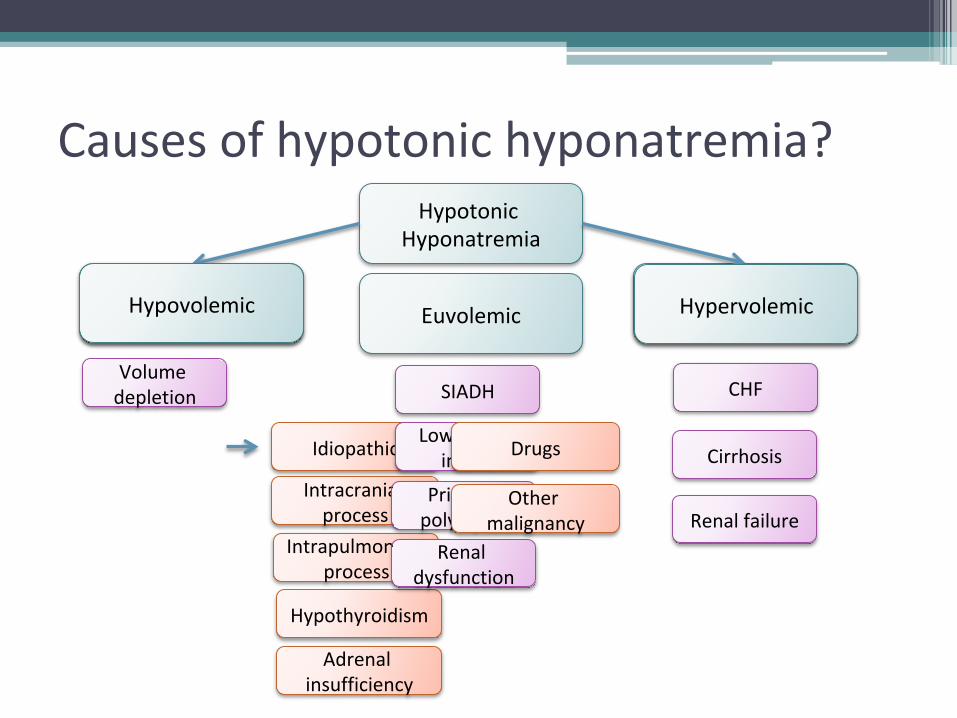
Causesofhypotonichyponatremia?Hypotonic
Hyponatremia
ADH“active”
Volumedepletion
ADH“inactive”
SIADH CHF
CirrhosisIdiopathic
Intracranialprocess
Intrapulmonaryprocess
Hypothyroidism
Adrenalinsufficiency
Lowsoluteintake
PrimarypolydipsiaRenal
dysfunction
Drugs
Othermalignancy
Hypovolemic HypervolemicEuvolemic
Renalfailure

SIADHversuslowEABV?
• History?• Physicalexamination?▫ Vitals,orthostatics,JVP,etc▫ Advancedexam:IVCcollapsibility,bedsideTTE• LabTests?▫ Urinesodium� Low(<20meq/L)àvolumedepletion� Notlow(>40meq/L)àSIADH▫ Serumuricacid� <4mg/dlàconsistentwithSIADH

Iliternormalsaline(350mosm/L)
SIADH w/ urine osm 400 mosm/L
875mlurine125mlfreewater
SIADH w/ urine osm 900 mosm/L
390mlurine
610mlfreewater
Iliternormalsaline(350mosm/L)
+
+
OtherdiagnosticmaneuversforSIADHversuslowEABV?
What about just giving IV fluids?

Case2again• A19y/omanwithhistoryofanorexianervosapresentswithweakness,lethargy,andinabilitytoconcentrate.PriortoadmissionwasataravewherehetookMDMAanddranklotsofwater.
• IntheED,hehadagrandmalseizure.Afterward,SNawas130mEq/LandUosmwas700mOsm/kg.
• Vitals:Ht5’7”andwt105Lbs(45kg).Afebrile.HR80BP110/70
• Exam:Post-ictal,diaphoretic.Ralesonchestexam

Answerstocase2• Isthisacutehyponatremia?▫ YES!Why?▫ Ingestionoflargevolumeofwater▫ IngestionofEcstasy,adrugthatleadstosecretion/releaseofvasopressin,andthusSIADH
• WhydidhehaveSz?▫ Acutehyponatremia▫ SNafromvenoussampleafterSzoverestimatespriorSNa.NumberofosmolesincreasedinmusclecellduringSz
• What’stheroleofanorexianervosa?▫ Lowmusclemass(50%ofTBW).▫ SmallerpositivewaterbalancecausesgreaterfallinhisSNa.
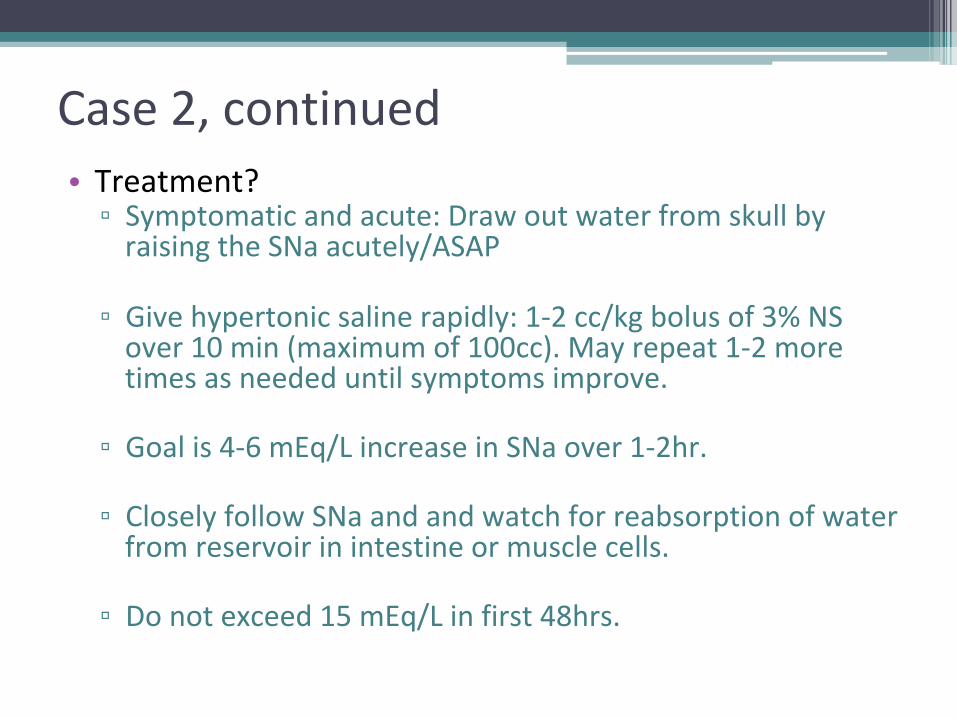
Case2,continued• Treatment?▫ Symptomaticandacute:DrawoutwaterfromskullbyraisingtheSNaacutely/ASAP
▫ Givehypertonicsalinerapidly:1-2cc/kgbolusof3%NSover10min(maximumof100cc).Mayrepeat1-2moretimesasneededuntilsymptomsimprove.
▫ Goalis4-6mEq/LincreaseinSNaover1-2hr.
▫ CloselyfollowSNaandandwatchforreabsorptionofwaterfromreservoirinintestineormusclecells.
▫ Donotexceed15mEq/Linfirst48hrs.
Case3–Acaseofiatrogenesis?
• 80yearoldwomenishospitalizedfor1wkhistoryofprogressiveweakness,nauseaandanorexia.Hasbecomebedriddenandconfusedduringpast3days.Shehashypertensionmanagedwithenalaprilandchlorthalidoneinitiated3weeksago.OnadmissionSNawas110mEq/L,Kof3
• PhysicalExam:T37.3C,BP110/65,HR95andRR14.Wt47kg.BMI20.Cardiacandpulmonaryexamsnormal.Nofocaldeficitsonneuroexam.Noedema,ascites.

LabstudiesParameter Admission
PlasmaAdmissionUrine
Na(mEq/L) 110 30
K(mEq/L) 3
Cl(mEq/L) 72 30
HCO3(mEq/L) 30
Cr 1
BUN 9
Glucose 90
Osmolality 231 500
Whatisthecauseofthispatient’s
hyponatremia?

Thiazide-inducedhyponatremia• Increasedincidenceinwomenandelderlypatients
• Pathogenesisunclear,butpotentialcauses:▫ VolumelossàADH-inducedwaterretention▫ ?Increasedthirstduetoxerostomia▫ ?IncreasedADHrelease

Returningtothelabs…
Parameter AdmissionPlasma
AdmissionUrine
10hrPlasma
10hrUrine
Na(mEq/L) 110 30 121 25K(mEq/L) 3 2.7Cl(mEq/L) 72 30HCO3(mEq/L) 30Cr 1BUN 9Osmolality 231 500 252 180UrineOutput 400cc/hr
InEDgiven80ccof3%salineandmentationrapidlyimproves.Afteradmission,someadditionalisotonicfluidisgiven.10hourslater…

Sonowwhat?
• Whichofthefollowingisthemostappropriatetreatmentforthispatient?
(A) 0.9%Saline
(B) 5%Dextroseinwater+KCl
(C) Fluidrestriction+KCl
(D) Tolvaptan

Answer
• 5%Dextroseinwater+KCltodropSNabacktogoalrateofrise
• Whatisthegoalratetoavoidavoidosmoticdemyelination(ODS)?▫ Chronic(>48hr):0.5mEq/Lperhour,≤10mEqinfirst24hr(6-8inthosewithRFforODS)and≤18infirst48hr.
▫ Acute(<48hr)symptomatic:1-2mEq/Lperhour,correctingby4-6mEq/Land/orcorrectionofsymptoms.

OsmoticDemyelinationSyndrome(ODS)
Symptoms seen 2-6 days after correction: • Dysarthria (CPM) • Dysphagia (CPM) • Ataxia, dystonia • “Locked in” state • Acute flaccid paralysis • Coma

Case4:Howmuchcanyoudrink?• 45yearoldmanwithschizophrenia,wellmanagedonanti-psychotics,intermittentlyunhoused,alsowithalcoholusedisorder,presentstotheHMCemergencydepartmentwithrightlegswelling,erythema,pain.Diagnosedclinicallywithcellulitis.
• Onarrival,vitalsignsarestable.Notorthostatic.

Parameter ValuePlasmavaluesNa(mEq/L) 116K(mEq/L) 3.5Cl(mEq/L) 88Bicarb(mEq/L) 26Creatinine(mEq/dL) 0.8BUN(mEq/dL) 9Glucose(mEq/dL) 119Osmolality(mOsm/kg) 246Bloodalcohol UndetectableUrineOsmolality(mOsm/kg) 75Na(mEq/L) 7
Questions
• Is thisacutehyponatremia?• Whatarethepossibleetiologiesforhishyponatremia?
• Howdoyoumanage?

InitialevaluationofHyponatremia• Truehyponatremiavsnon-hypotonichyponatremia?▫ Truehyponatremia(lowserumosms)
• Severity/chronicity?▫ Moderatetosevere,likelychronicgivenasymptomatic
• Etiology▫ IsADHactingornot?
� No!(Howdoyouknow)▫ Whatisthevolumestatusofthepatient?
� Euvolemic▫ Wheredidtheexcessfreewatercomefrom?
� Beer+water▫ Whycanthekidneysnotexcretetheexcesswater?
� Lowsoluteintakew/highwaterintakelikely

Primarypolydipsiavs.Lowsoluteintake• Key:Hyponatremiaensueswhenwaterintakeexceedsmaximumurineoutput
• NormalAmericandiet(perday):
÷=8to12litersurine/day
• Lowsoluteintake(“tea-and-toast”or“beerpotomania”)
÷=2.6litersurine/day
600-900mosms
75mOsmsperliter
200mosms
75mOsmsperliter

Case5:The“un-watered”patient• 61y/ofemalewithh/obipolardisorderandpasth/olithiumusetransferredfromAlaskawithintractableseizures.WorkupdemonstratedneuronalK+channelAb.PatientadmittedtoICU,startedonpulsesteroids,wasNPOduetoAMS.Alsoonkeppraanddepakote.
• Vitals:T36.1HR65BP110/68RR1296%RA.Wt50kg
• Exam:▫ GEN:Somnolent.▫ Neuro:Followingsimplecommands.Intactgag.Facesymmetric.▫ Ext:Noedema
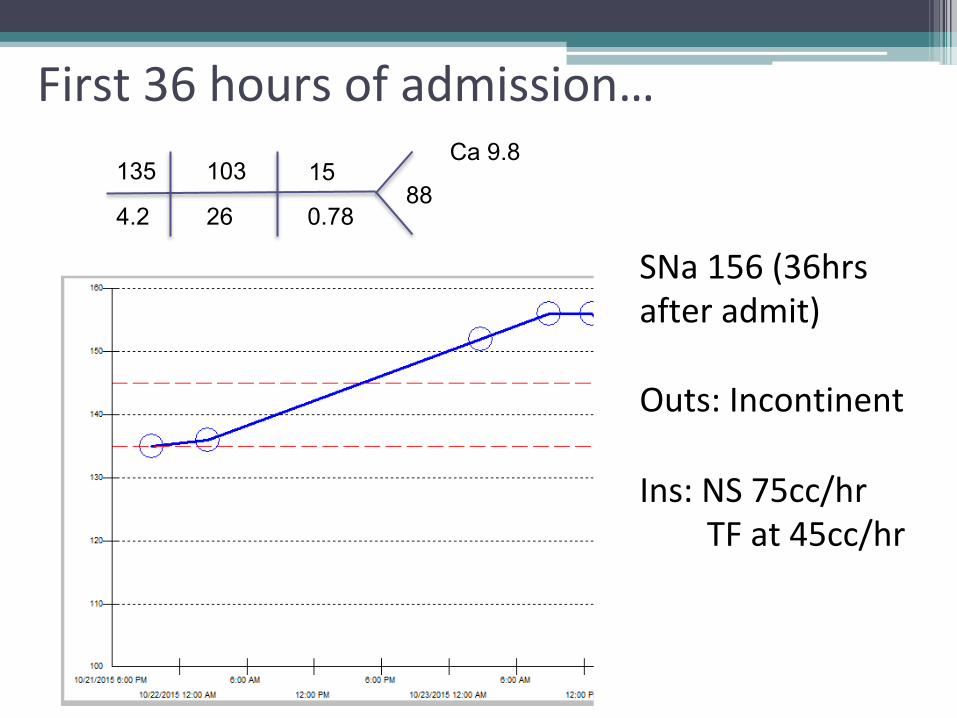
First36hoursofadmission…135
4.2
103
26
15
0.78 88
Ca 9.8
SNa156(36hrsafteradmit)Outs:IncontinentIns:NS75cc/hrTFat45cc/hr

HypernatremiaQuestion:Whatarethemajorcausesofhypernatremiainhospitalizedpatients?
• Primarywaterdeficit▫ Reducedwaterintakeordefectivethirstmechanism▫ Increasedwaterloss
� Renalloss:Central/nephrogenicDI,osmoticdiuresis� GIloss:Vomiting,Nasogastricsuction,osmoticdiarrhea� Insensiblelosses:Respiratory,skin▫ Shiftofwaterintocells:Seizures
• PrimarygainofNa+▫ Infusionofhypertonicfluidinoliguricpatients

Factorstoassessthepatientwithhypernatremia• Thirst(History):Whyispatientnotcompensating?
• Whatissourceofwaterloss?(urinevolume?)� HighinsensiblewaterlossorGIloss(NGTsuction,diarrhea)
� Polyuria?Urineflowrateandeffectiveosmolality:� Osmoticdiuresis:Uosm400-500mOsm/kg� Waterdiuresis:Uosm<150mOsm/kg(LowADH)

Uosm >400-500mOsm/kg
>3L/day
Tumors (pituitary)Post-surgery, TBIInfiltration (sarcoid)
Renal interstitial dz & Drugs (Li mostly)

Case5-Subsequentmanagement
• FoleycatheterplacedwithUOP175cc/hr
• SNa=156
• Urineosm:140mosm/kg
• Totalbodyfreewaterdeficit:TBWx([SNa/140]–1)▫ 25Lx([156/140]–1)=2.9L
• Treatment:D5Wat250cc/hrandFWB300Q6hr.

ChangesinSNaandUNa
SNa
UNa
Mentation improve, but UOP now increased to 250-300cc/hr
UK

Questions
• IsthispartialorcompletenephrogenicDI?Whatdoyoudo?
• WhataretreatmentsforLithiuminducedNephrogenicDI?A. Stoplithium(ifpossible,butwithcaution)B. AmilorideC. NSAIDs
Response to DDAVP? 4mcg IV DDAVP: Uosm 100->125 2hr after DDAVP.
• Started on indomethacin with drop in urine output from 250-350cc/hr to 60-125cc/hr
Case6:Ayoungwomanwithheartfailure• A32yearoldwomanwithnoPMHpresentstourgentcarewithabdominalpainx4months,foundtohaveBPof240/180.• Deniesheadaches,visualchanges,chestpain• OnROS,endorses2weeksoflegswelling
• PhysicalExam:T37.3C,BP240/183,HR87.Cardiacexamwith+S3,displacedPMIlaterally,1+LEedema,lungswithcracklesatbases

Case6,continued
• InitiallabsintheEDàK2.4,HCO336,Cr1.2,andBNP3000.EKGconcerningforLVH.
• ShewasgivenIVLabetolol30mg,POAmlodipine10mg,andPOLisinopril10mgwithimprovementinherBPsto188/140.
• TTE:NormalLVsize,withconcentricLVHandmoderatelyreducedsystolicfunctionandglobalhypokinesis(LVEF30%).

Case6questions
Whatisthedifferentialdiagnosisforthispatient’shypokalemiawithmetabolicalkalosisinthesettingofseverehypertension?1. Primaryhyperaldosteronism2. Renalarterystenosisleadingtosecondary
hyperaldosteronism3. Otherrareconditionsa) Inheritedmonogenicdisordersb) Apparentmineralocorticoidexcess

Hyperaldosteronism• Estimatedtoberesponsiblefor20%ofsevere/resistantHTNinadults• Includesboth▫ Bilateraladrenalhyperplasia(60%)▫ Aldo-producingadenomas(40%)
• Clinicalfeatures▫ HTN▫ Hypokalemia(only~30%)▫ Metabolicalkalosis(only10-35%)

ScreeningforHyperaldosteronism• Labtest:Serumaldosteroneandplasmareninactivity(PRA)▫ Ideally8am,OFFMRAs,Oktobeonotherdrugs� ThoughACEI/ARBcanraisePRA,B-blockersdecreasePRA▫ Definition:� Aldosterone/PRA>20,AND� Serumaldosterone>15ng/dL
• IscreeneveryonewithresistantHTNorwithHTN+spontaneous(orminimallyprovoked)hypokalemiaormetabolicalkalosis

“CaseConfirmation”forhyperaldo• Neededinmostcases▫ Exception:HTN,spontaneoushypokalemia,undetectablePRA,PAC>20ng/dL
• Bestchoiceforinpatients:▫ Salineinfusiontest:2LNSover4hours,thencheckserumaldosteroneà+testis>12ng/dL
• NeedtocontrolserumpotassiumandBPprior

Hyperaldosteronismconfirmed–Nextstep?

Hyperaldo–Nextstep?
• Adrenalvenoussamplingbyhighvolumeinterventionalradiologistorvascularsurgeon
• Exception:Patients<35yearsofagewithcompletelysuppressedPRAandPAC>20ng/dL

Hyperaldo–NextStep?

Renalarterystenosis• Prevalence10%-30%insevereorrefractoryHTN

Renalarterystenosis• Clinicalclues:▫ Diffusevasculopathy(CAD,CVD,PVD)▫ Youngwomen(FMD)▫ Systolic+diastolicabdominalbruit(specific,notsensitive)▫ Isolatedsystolicbruit(sensitive,lessspecific)▫ Headaches,tinnitus,neckpain(FMD)▫ RiseincreatininewithACEI/ARB(oranyanti-HTNtherapy)
• Key:knowwhatyouwilldowithresultsoftestingbeforeyouproceed
Renalarterystenosis–cont.
• Diagnosis:centerdependent▫ Renalarteryduplex–onlyifyouhavegoodvascularlab,butgivesyousomefunctionalresults▫ CTAorMRAoftheabdomen• Therapy:▫ FMD-renalarteryangioplasty(withoutstenting)� Diseasecanrecur,buttypically>5-10yearslater� Recommendedtoscreenothervascularbeds� AllpatientsneedASA▫ Atherosclerosis–medicalmanagement(CORALandASTRALtrials)

Monogeniccauses• Rare,butinterestinganddemonstratepathophysiology
• Diseasesofdistaltubuleorcollectingduct
• Theseareoftenassociatedwithhypokalemiaandmetabolicalkalosis(mimicprimaryhyperaldo)
• 3mostcommon(stillrare): ▫ Liddlesyndrome▫ Apparentmineralocorticoidexcess(AME)▫ Glucocorticoidremedialhyperaldosteronism

Bloodpressurehigh
Checkplasmaaldosteroneand
reninlevels
HighreninHighaldosterone
LowreninHighaldosterone
LowreninLowaldosterone
Reninoma
Renalarterystenosis
Primaryhyperaldo(Conn’ssyndrome
GlucocorticoidRemedial
Aldosteronism
Licoriceingestion
AME
Liddle’ssyndrome
Evaluationofhypokalemia+metabolicalkalosis…

Backtoourpatient…
• Aldosteroneandrenintestingshowed:▫ Aldosterone:4ng/dL▫ PRA<0.1ng/mL/hr
• CTAabdomenshowednorenalarterystenosis
• StartedonHFtreatmentàcarvedilol,Lisinopril,loopdiuretic
• PersistentBP>180/100
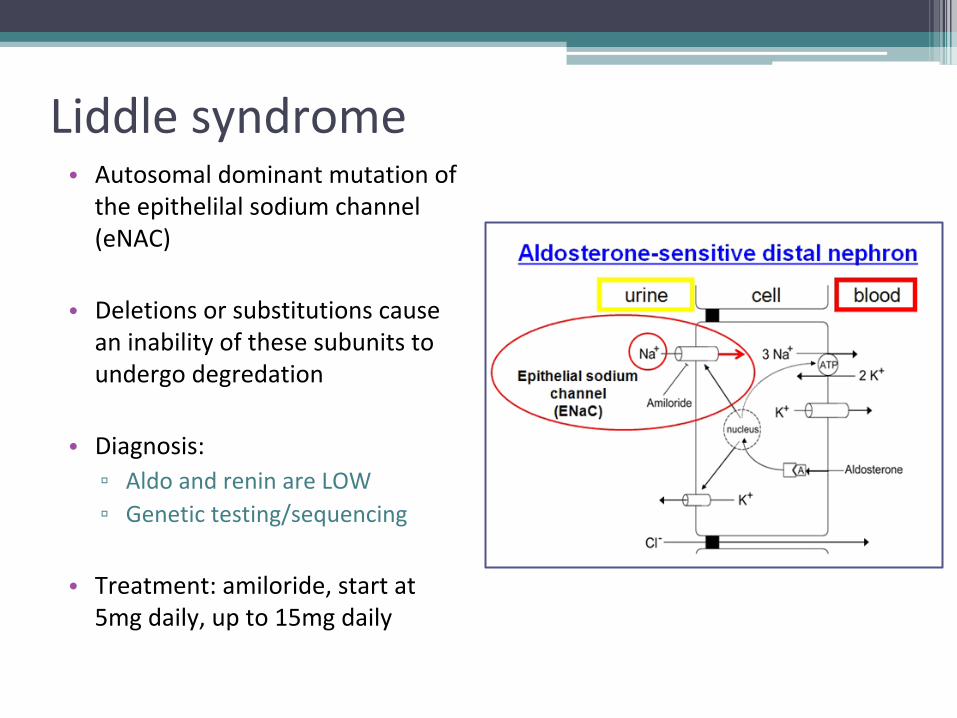
Liddlesyndrome• Autosomaldominantmutationoftheepithelilalsodiumchannel(eNAC)
• Deletionsorsubstitutionscauseaninabilityofthesesubunitstoundergodegredation
• Diagnosis:▫ AldoandreninareLOW▫ Genetictesting/sequencing
• Treatment:amiloride,startat5mgdaily,upto15mgdaily

Summary&Takehomepoints1. Hyponatremiaandhyponatremiaarereallydisorders
ofWATERimbalancebetweenfluidcompartments
2. CriticalchallengeinevaluationofhyponatremiaisdistinguishinglowEABVversusSIADH
3. Hypernatremiainahospitalizedpatientisnearlyalwaysduetoinadequatefreewateradministration
4. Ininpatientswithhypokalemiaandhypertension,thinkaboutaldosterone

• Acknowledgements:▫ YoshioHall,MD,MS▫ BobRoshanravan,MD,MS
Questions?