The Manager's Pocket Guide to Team Sponsorship (Manager's Pocket Guide Series)
Upload
atif-gazaliCategory
view
38download
1description

in the hospital setting
• Recognition
• Evaluation
• Consequences
• Management
Fundamentals of

V IS I T
2 3
Table of contents
Chapter 1: Recognition 4
• Definition .................................................4
• Prevalence ................................................5
• Etiologies ..................................................6
• Signs, symptoms, and complications ......7
Chapter 2: Evaluation 10
• Classification ..........................................10
• Prognostic markers ................................11
• Acute vs chronic .....................................12
• Levels of severity ...................................12
• Misdiagnosis ...........................................13
Chapter 3: Consequences 14
• Potential effect on the brain ...............14
• Impact on selected outcomes ...............15
• In-hospital mortality ..............................16
• Risk of mortality ....................................17
• Impact on hospital costs .......................18
Chapter 4: Management 20
• Considerations .......................................20
• Rate of correction..................................20
• Management strategy for correction .........................................21
Introduction
Hyponatremia is the most common electrolyte disorder in
hospitalized patients.1 Hyponatremia can be a serious threat.1
One study found that mild, or even asymptomatic, hyponatremia
may be associated with increased morbidity and the risk of
mortality.1,2 While the symptoms of hyponatremia are not
always severe, the danger may be real.1
Hyponatremia can produce a range of symptoms involving
almost all of the body systems.2 The effects on the central
nervous system (CNS) can be significant and potentially lethal.2
Hyponatremia also impacts hospital economics as it has been
shown to induce longer, more costly hospital stays.3
Although there are many scientific articles on hyponatremia,
this pocket guide is designed to bring you the broad
fundamentals. From the definition of hyponatremia to
its relationship with mortality to its estimated burden on
the national healthcare system, you will find important
information in one concise resource.

V IS I T
4 5
0
10
20
30
40
Pa
tie
nts
wit
h h
yp
on
atr
em
ia,
%
Hyponatremia during the hospital stay1
Hospital-acquired hyponatremia
0
10
20
30
40
Hyponatremia upon admission6
Acute care hospital patients
Serum sodium level upon admission was <136 mEq/L
Serum sodium level upon admission was <126 mEq/L
Pa
tie
nts
wit
h h
yp
on
atr
em
ia,
%
Prevalence in the hospitalApproximately 25% of acute care patients had hyponatremia ([Na+] <136 mEq/L) upon admission to the hospital6
• Analyzed in a large study of more than 100,000 patients conducted at an Asian hospital6
• A more severe level of hyponatremia (defined in this study as [Na+] <126 mEq/L) was seen in 2.6% of hospitalized patients6
In a separate study, it was shown that 38.2% of patients acquired hyponatremia during their hospital stay1
• Determined in a retrospective analysis of 53,236 hospitalizations represented by 7 years of discharge records1
— Hospital-acquired hyponatremia developed in 10,662 of 27,897 hospitalizations for which the initial serum sodium level was within 138-142 mEq/L and length of stay was longer than 1 day1
Chapter 1: Recognition
Defining hyponatremia• Hyponatremia, defined as a serum sodium level of <135 mEq/L,
indicates a relative excess of total body water to sodium4
• Most common electrolyte disorder in the hospital1
Types of hyponatremia2,5
Dilutional• Hypervolemic — Total body sodium increased
— Total body water increased
— Edema
• Euvolemic — Total body sodium unchanged
— Total body water increased
— No edema
Depletional• Hypovolemic — Total body sodium and water reduced

V IS I T
6 7
Etiologies of hyponatremia
Hypervolemic5,7
• Congestive heart failure
• Cirrhosis
• Nephrotic syndrome
• Acute/chronic renal failure
Euvolemic5,7-9
• Adrenal insufficiency
• Hypothyroidism
• Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
— Drugs (antidepressants, antipsychotics, barbiturates, nicotine, NSAIDs, morphine, vincristine)
— Physical/emotional stress
— Malignancies
— Pulmonary disease
— CNS disorders
— Idiopathic
Hypovolemic5
• Diuretic excess
• Mineralocorticoid deficiency
• Salt-losing nephritis
• Osmotic diuresis
• Ketonuria
• Bicarbonaturia
• Vomiting or diarrhea (extrarenal origin)
• Third-spacing (ie, burns, pancreatitis)
• Seizures
• Coma
• Permanent brain damage
• Respiratory arrest
• Brain-stem herniation
• Death
• Headache
• Nausea
• Vomiting
• Muscle cramps
• Lethargy
• Restlessness
• Disorientation
• Depressed reflexes
Signs and symptoms of hyponatremia14,15
Complications of severe and rapidly evolving hyponatremia14,15
Signs, symptoms, and complications The symptoms of hyponatremia may not always be clear10
• The symptoms of hyponatremia may overlap with the symptoms of other disorders or diseases11-13
— While hyponatremia can affect a wide range of body systems, the most severe consequences involve the CNS2

V IS I T
8 9
21.3%
5.3%
0
5
10
15
20
25
Patients admitted for falls16
Hyponatremic patients126 ± 5 mEq/L
(n=122)
Adjusted OR 67.4,95% CI 7.5-607.4, P<0.001
Mean serum [Na+]:No. of patients:
Control patients139 ± 2 mEq/L
(n=244)
Pat
ient
s ad
mitt
ed w
ith f
alls
, %
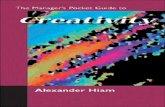
Incidence of falls among 122 patients (mean age 72 ± 13 years) with asymptomatic chronic hyponatremia (mean serum sodium concentration [SNa] 126 ± 5 mEq/L) compared with 244 matched controls (mean age 71 ± 12 years). Adapted from Renneboog B et al. Am J Med. 2006;119(1):71.e1-71.e8.16
Mild hyponatremia is not always “asymptomatic”16
Irregular gait16
• Unsteadiness of gait was shown to be significantly greater in patients with hyponatremia (n=12) as compared with patients who were normonatremic16
• Assessed in a study (N=122, approximate mean serum Na 126 mEq/L) of mild, chronic hyponatremia conducted in a Brussels, Belgium, hospital over the course of 3 years16
High incidence of falls16
• In this same study, falls were demonstrated to be a common symptom in mild chronic hyponatremia16
• Patients with chronic “asymptomatic” hyponatremia were admitted for falls significantly more frequently than patients with normal sodium levels16
140
120
100
80
60
40
20
0
-20
-40
-60
-80
-100
-120
-500 -400 -300 -200 -100 100 200
[Na+]=124 mEq/L
Irregular gait with mild asymptomatic hyponatremia16
Evolution of the “total traveled way” (TTW) by the center of pressure in the dynamic test to walk on the platform 3 stereotyped steps “in tandem,” eyes open, in patient C with mild asymptomatic hyponatremia. Patient is walking from right to left. Irregular path of the center of pressure observed in the hyponatremia condition (arrow).Adapted with permission from Renneboog B et al. Am J Med. 2006;119(1):71.e1-71.e8.16

V IS I T
10 11
Classifying hyponatremia
Plasma osmolality
Hypotonichyponatremia
Euvolemic hyponatremia
SIADH Endocrinopathies • Hypothyroidism • Glucocorticoid deficiency
Excess water intake Impaired renal concentrating ability
Serum sodium <135 mEq/L
Hypovolemichyponatremia
Hypervolemichyponatremia
>295 mOsm/kg<280 mOsm/kg280-295 mOsm/kg
>100 mOsm/kg<100 mOsm/kg
Isotonichyponatremia
Hypertonichyponatremia
Urine osmolality
Extracellular fluid
Urine sodium
>20 mEq/L
Renalfailure
>20 mEq/L <10 mEq/L
Urine sodium
Renalsolute loss
Extrarenalsolute loss
>20 mEq/L <10 mEq/L
Urine sodium
Edematousdisorders • Heart failure • Cirrhosis • Nephrotic syndrome
Hyponatremia classification algorithm5
Adapted from Douglas I. Clev Clin J Med. 2006;73(3):S4-S12.5
Chapter 2: Evaluation
Prognostic markers • Laboratory measurements can be used in the differentiation
of hyponatremia17
* Compared with serum osmolality. Adapted from Hoorn EJ et al. Nephron Physiol. 2008;108(3):46-59.17
Diagnostic indicators17
Laboratory Disease/ measurement disorder
Serum osmolality: high Hyperglycemia, glycine solutions
Serum osmolality: normal Pseudohyponatremia
Serum osmolality: low Hypotonic hyponatremia
Urine osmolality: high* Vasopressin-dependent cause of hyponatremia
Urine osmolality: low* Vasopressin-independent cause of hyponatremia
Urine sodium: low Heart/liver failure, polydipsia, nonrenal sodium loss, volume depletion
Urine sodium: high Diuretics, cerebral and renal salt wasting, SIADH, primary adrenal insufficiency, hypopituitarism
Serum potassium: low Diuretic use, vomiting, diarrhea
Serum potassium: high Primary adrenal insufficiency, renal failure

V IS I T
12 13
Acute vs chronic• Hyponatremia can be further classified as acute or chronic,
defined as duration of onset of <48 hours or ≥48 hours2,5
Serum sodium falls rapidly over a period of
<48 hours
Serum sodium falls slowly over a period of
≥48 hours
Acute Chronic
Hyponatremia
Classification by rate of declining serum sodium2
• The distinction of acute vs chronic significantly influences the severity of CNS manifestations and potential complications2
• Patients with acute hyponatremia (serum sodium <120 mEq/L) are at risk of irreversible neurologic damage when the rate of serum sodium decrease exceeds 0.5 mEq/L/h18
Levels of severity
Mild to severe hyponatremia18,19*
MildModerateSevere
130-135 mEq/L
120-130 mEq/L
<120 mEq/L
• Mild hyponatremia can often be asymptomatic19
• While lower serum sodium levels can lead to more severe consequences of hyponatremia, mounting evidence has found that even mild hyponatremia can be associated with increased morbidity and mortality1,14,16
Misdiagnosis As the cause of hyponatremia is often unclear, the differential diagnosis of hyponatremia may be complex20
• Assessed in a study analyzing a diagnostic algorithm for hyponatremia in 121 patients presenting with serum sodium <130 mEq/L20
• In this study common causes of misdiagnosis:
— Effect of diuretics on clinical presentation and laboratory measurements20
— Use of extracellular volume status as the determining diagnostic factor20
• Hyponatremia and inadequate therapy may substantially raise morbidity, mortality, and healthcare expenditure; therefore, a careful diagnostic approach to patients with hyponatremia is considered essential20
Rate of misdiagnosis20:Patients on diuretics
20
0 5 10 15 20 25Percentage of patients misdiagnosed
Rate of misdiagnosis20:Extracellular fluid volume
5
0 5 10 15 20 25Percentage of patients misdiagnosed
* Serum Na values defining hyponatremia and its severity may vary across institutional laboratories

V IS I T
14 15
In-hospital mortality
19,030
1151
621
65Admission [Na+] <138 mEq/L and further drop
Admission [Na+] <138 mEq/L and no further drop
Disposition‡
Adjusted odds ratio†
Adjusted relative prolongationDisposition = discharge to short- or long-term care facility.†Adjustments for age, sex, race, admission service, and Deyo-Charlson Comorbidity Index score.‡Hospitalizations resulting in death were excluded from analyses of disposition and length of stay.§Adjusted relative prolongation (95% CI).
0 1
§
§
2 3
Admissions(n)
Impact of hyponatremia* on selected outcomes1
In-hospitaldeaths (n)
18,409
1086
6744
569Admission [Na+] <138 mEq/L and further drop
Admission [Na+] <138 mEq/L and no further drop
Admissions(n)
18,409
1086Admission [Na+] <138 mEq/L and further drop
Admission [Na+] <138 mEq/L and no further drop
Admissions(n)
Discharged tofacilities (n)
Increased length of stay‡
* Community-acquired hyponatremia or hospital-aggravated hyponatremia.Adapted from Wald R et al. Arch Intern Med. 2010;170(3):294-302.1
Impact of hyponatremia on selected outcomes One study showed that hospital-acquired hyponatremia (n=10,662 hospitalizations)was associated with twice the incidence of in-hospital mortality (2.9% vs 1.4%) compared with a group without hospital-acquired hyponatremia1
• Analyzed in a retrospective analysis of 53,236 hospitalizations* represented by 7 years of discharge records1
Chapter 3: Consequences
Potential effect on the brainThe brain reveals most of the clinical effects associated with hyponatremia21
• Patients exhibiting symptoms of hyponatremia usually have cerebral edema22
• If the brain has not adapted sufficiently to the swelling, the resulting pressure on the skull can cause a decrease in cerebral blood flow and pressure necrosis22
• Unrestrained brain swelling will often lead to death or permanent brain damage23
Adapted from Gross P. Kidney Int. 2001;60(6):2417-2427.24
Cerebral edema in acute, severe hyponatremia24
AXIAL COMPUTER
TOMOGRAPHIC (CT) SCAN OF
THE BRAIN SHOWING CEREBRAL
EDEMA

V IS I T
16 17
Risk of mortality may continue4
In a separate study, postdischarge mortality was nearly double in hyponatremic patients vs normonatremic patients at 1 year4
• Determined by a 3-year cohort analysis of 98,411 admissions4*
• The study demonstrated that even mild hyponatremia carried a significantly increased risk of death in-hospital, at 1 year, and at 5 years following discharge4
• Resolution of hyponatremia during hospitalization attenuated an increased mortality risk conferred by hyponatremia10
Patients with hyponatremia had higher mortality rates than patients with
normal serum sodium concentrations4
Normonatremic patients
Hyponatremic patients
Serum sodium level (mEq/L) 135-144 <135
Mean age (years) 63.1 67.0
Crude in-hospital mortality (%) 2.4 5.4
Crude 1-year mortality (%) 11.7 21.4
Crude 5-year mortality (%) 42.3 54.8
*Patients’ serum sodium was <135 mEq/L. The study assessed the risk of mortality at 2 academic teaching hospitals in Boston, Massachusetts. Adapted from Waikar SS et al. Am J Med. 2009;122(9):857-865.4
In-hospital mortalityOne study showed that the risk for mortality began to rise at serum sodium <138 mEq/L25 • Assessed by the OPTIMIZE-HF registry, which evaluated the
risk of mortality in heart failure patients (N=48,612) with hyponatremia at the time of admission25
— Risk of mortality was more than double in the serum sodium range of 132-135 mEq/L compared to the normal serum sodium range25
— The overall mortality rate was 3.8% in the study25
In-h
ospi
tal m
orta
lity
rate
Admission serum sodium, mEq/L
0.08
0.07
0.06
0.05
0.04
0.03
0.02
0.01
125126 127 129128 130 131132133134 135136 137138 139 140 141142143144 145146 147
Restrictive cubic spline transformation plot with 95% confidence intervals is shown.Adapted from Gheorghiade M et al. Eur Heart J. 2007;28(8):980-988.
Relationship between admission serum sodium levels and
in-hospital mortality25
• Any level of hyponatremia can be associated with potentially adverse outcomes1
Adapted from Gheorghiade M et al. Eur Heart J. 2007;28(8):980-988.25

V IS I T
18 19
One study estimated the potential burden of hyponatremia on the national healthcare system3
• On a national level, the estimated economic burden of hyponatremia for hospitals included3
— 1.4 million additional bed days
— $1.1 billion in additional costs
• Hospitals will likely bear the responsibility for these costs, which under most reimbursement programs are unable to bill patients or payers for these extended hospital stays3
• Higher treatment costs are associated with patients requiring ICU care, especially among those with moderate to severe hyponatremia3
In a separate study, the presence of various levels of hyponatremia was associated with longer lengths of stay compared with the absence of hyponatremia3
• This data analysis of more than 50,000 hospitalizations over a 7-year period further implicated the potential financial impact of hyponatremia1
Impact on hospital costsIn one study, patients with hyponatremia incurred ~$1400 to nearly $3000 more per hospital visit3
• Analyzed in a retrospective cohort study, patients (N=9620) with moderate to severe (n=547) or mild to moderate (n=1500) hyponatremia had longer hospital stays vs patients in the normal range (n=7573)3
• Increased median LOS by 2 to 3 days3
• Incurred extra costs per visit by severity of hyponatremia:
— Approximately $1400 for mild to moderate hyponatremic patients3
— Nearly $3000 for moderate to severe hyponatremic patients3
• Based on an annual admission of approximately 55,000 patients in this study, it was estimated that because of hyponatremia the hospital accrued an additional3
— $2.15 million in hospital costs3
— Over 3400 additional bed days3
Hyponatremia n Hospital LOS, Percent admitted Total cost, status median days* to ICU* USD*
Moderate to severe (≤129 mEq/L)
547 8 32 $19,519
Mild to moderate (130-134 mEq/L)
1500 8 26 $18,054
Normal serum sodium (135-145 mEq/L)
7573 6 22 $17,085
Average in-hospital hyponatremia levels and associated cost in
the hospital setting3
Hospital LOS, ICU admission rate, and total cost per admission by hyponatremia status adjusted
for clinical and demographic variables
*P<0.001 for Cuzick’s test for trend.Abbreviations: ICU, intensive care unit; LOS, length of stay.
Adapted from Callahan MA et al. Postgrad Med. 2009;121(2):186-191.3

V IS I T
20 21
The risk of overly rapid correction5,28
• Too rapid correction of serum sodium levels may lead to osmotic demyelination, which can result in adverse neurologic outcomes or death5,28
Understanding the physiology for correcting hyponatremiaPlasma sodium is the balance of exchangeable sodium and potassium divided by total body water.29,30 This simplified equation illustrates two approaches to potentially correct hyponatremia:• Increase the numerator by adding sodium29,30
• Decrease the denominator by subtracting water29,30
Key: [Na+]: plasma sodium concentration Nae: total exchangeable sodium Ke: total exchangeable potassium TBW: total body water
[Na+] =TBW
Nae + Ke
Considerations in treating hyponatremiaThe rate of decline in serum sodium concentration5
• The rapidity of onset of hyponatremia determines whether the imbalance is chronic or acute5
• As there are risks associated with all forms of hyponatremia, once identified, patient monitoring and careful management are critical1
Dilutional hyponatremia5
• Mild hyponatremia may require less aggressive therapies (e.g., fluid restriction)26
• Moderate hyponatremia may require specific therapy (e.g., aquaretic drugs)
• Severe symptomatic hyponatremia, with apparent neurologic signs, will require more immediate attention (e.g., hypertonic saline)5,26
Depletional hyponatremia5
• Isotonic saline is typically the mainstay of treatment17
• If appropriate, discontinuation of diuretic can be considered17
Rates of serum sodium correctionIncreasing serum sodium levels It has been shown that osmotic demyelination syndrome (ODS) can occur when hyponatremia is overcorrected, e.g., serum sodium levels are increased ≥10 – 12 mEq/L in 24 hours and/or ≥18 mEq/L in 48 hours.5,27
The treatment goal for improving serum sodium levels should be sufficient to keep patients safe from hyponatremia-associated complications while avoiding injury due to overcorrection.5,27
Chapter 4: Management
Adapted from Rose BD. Am J Med. 1986;81(6):1033-1040 and Edelman IS et al. J Clin Invest. 1958;37(9):1236-1256.29,30

V IS I T
22 23
Notes:Notes:

©2012 Otsuka America Pharmaceutical, Inc. December 2012 0712W-5845I
References: 1. Wald R, Jaber BL, Price LL, Upadhyay A, Madias NE. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170(3):294-302. 2. Adrogué HJ. Consequences of inadequate management of hyponatremia. Am J Nephrol. 2005;25(3):240-249. 3. Callahan MA, Do HT, Caplan DW, Yoon-Flannery K. Economic impact of hyponatremia in hospitalized patients: a retrospective cohort study. Postgrad Med. 2009;121(2):186-191. 4. Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009;122(9):857-865. 5. Douglas I. Hyponatremia: why it matters, how it presents, how we can manage it. Cleve Clin J Med. 2006;73(suppl 3):S4-S12. 6. Hawkins RC. Age and gender as risk factors for hyponatremia and hypernatremia. Clin Chim Acta. 2003;337(1-2):169-172. 7. Widdess-Walsh P, Sabharwal V, Demirjian S, DeGeorgia M. Neurologic effects of hyponatremia and its treatment. Cleve Clin J Med. 2007;74(5):377-383. 8. Kumar S, Berl T. Sodium. Lancet. 1998;352(9123):220-228. 9. Verbalis JG, Goldsmith SR, Greenberg A, et al. Hyponatremia treatment guidelines 2007: expert panel recommendations. Am J Med. 2007;120(suppl 11A):S1-S21. 10. Hoorn EJ, van der Lubbe N, Zietse R. SIADH and hyponatraemia: why does it matter? NDT Plus. 2009;2(suppl 3):iii5-iii11. 11. National Digestive Diseases Information Clearinghouse (NDDIC)Web site. What I need to know about cirrhosis of the liver. http://digestive.niddk.nih.gov/ddiseases/pubs/cirrhosis_ ez/index.htm. Accessed August 3, 2010. 12. National Heart, Lung, and Blood Institute, National Institutes of Health Web site. What are the signs and symptoms of heart failure? http://www.nhlbi.nih.gov/health/dci/Diseases/Hf/HF_SignsAndSymptoms.html. Accessed August 3, 2010. 13. Robertson GL. Regulation of arginine vasopressin in the syndrome of inappropriate antidiuresis. Am J Med. 2006;119(7A)(suppl 1):S36-S42. 14. Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000;342(21):1581-1589. 15. Mayo Clinic Web site. Hyponatremia: symptoms. http://www.mayoclinic.com/health/hyponatremia/DS00974/DSECTION=symptoms. Accessed December 21, 2010. 16. Renneboog B, Musch W, Vandemergel X, Manto MU, Decaux G. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. 2006;119:71.e1-71.e8. doi:10.1016/j.amjmed.2005.09.026. 17. Hoorn EJ, Zietse R. Hyponatremia revisited: translating physiology to practice. Nephron Physiol. 2008;108(3):46-59. 18. Ghali JK. Mechanisms, risks, and new treatment options for hyponatremia. Cardiology. 2008;111(3):147-157. 19. Bagshaw SM, Townsend DR, McDermid RC. Disorders of sodium and water balance in hospitalized patients. Can J Anesth. 2009;56(2):151-167. 20. Fenske W, Maier SK, Blechschmidt A, Allolio B, Störk S. Utility and limitations of the traditional diagnostic approach to hyponatremia: a diagnostic study. Am J Med. 2010;123(7):652-657. 21. Sterns RH, Silver SM. Brain volume regulation in response to hypo-osmolality and its correction. Am J Med. 2006;119(7A)(suppl 1):S12-S16. 22. Arieff AI. Management of hyponatraemia. BMJ. 1993;307(6899):305-308. 23. Ayus JC, Achinger SG, Arieff A. Brain cell volume regulation in hyponatremia: role of sex, age, vasopressin, and hypoxia. Am J Physiol Renal Physiol. 2008;295(3):F619-F624. 24. Gross P. Treatment of severe hyponatremia. Kidney Int. 2001;60(6):2417-2427. 25. Gheorghiade M, Abraham WT, Albert NM, et al; OPTIMIZE-HF Investigators and Coordinators. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur Heart J. 2007;28(8):980-988. 26. Fraser CL, Arieff AI. Epidemiology, pathophysiology, and management of hyponatremic encephalopathy. Am J Med. 1997;102(1):67-77. 27. Sterns H, Nigwekar SU, Hix JK. The treatment of hyponatremia. Semin Nephrol. 2009;29(3):282-299. 28. Sterns RH, Riggs JE, Schochet SS. Osmotic demyelination syndrome following correction of hyponatremia. N Engl J Med. 1986;314(24):1535-1542. 29. Rose BD. New approach to disturbances in the plasma sodium concentration. Am J Med. 1986;81(6):1033-1040. 30. Edelman IS, Leibman J, O’Meara MP, et al. Interrelations between serum sodium concentration, serum osmolality and total exchangeable sodium, total exchangeable potassium and total body water. J Clin Invest. 1958;37(9):1236-1256.
V IS I T
Connect with important updates about:
Hyponatremia: The most common electrolyte disorder in hospitalized patients1
Effects on the brain: The brain reveals most of the clinical effects associated with hyponatremia21
Risk of mortality: Mortality is significantly higher among hospitalized patients with hyponatremia25
Impact on the hospital: Hyponatremia can induce longer, more costly hospital stays3