RESEARCH ARTICLE ...Holliday-Segar method has been the risk of iatrogenic hyponatremia with...
9
RESEARCH ARTICLE Outcomes of a Clinical Pathway to Standardize Use of Maintenance Intravenous Fluids Sahar N. Rooholamini, MD, MPH, a Holly Clifton, MPH, b Wren Haaland, MPH, c Caitlin McGrath, MD, a Surabhi B. Vora, MD, MPH, a,b Claudia S. Crowell, MD, MPH, a,b Holly Romero, MD, d Jeffrey Foti, MD a,b ABSTRACT OBJECTIVES: Improper use of maintenance intravenous fluids (IVFs) may cause serious hospital- acquired harm. We created an evidence-based clinical pathway to guide providers on the indications for IVF, its preferred composition, and appropriate clinical monitoring. METHODS: Pathway implementation was supported by the creation of an electronic order set (PowerPlan) and hospital-wide education. Outcomes were measured among pathway-eligible patients for the years before (July 1, 2014–June 30, 2015) and after (July 1, 2015–June 30, 2016) implementation. An interrupted time series analysis was used to evaluate monthly trends related to IVF use, including the following: median duration, proportions of isotonic and hypotonic IVF, adherence to monitoring recommendations, incidence of associated severe dysnatremia, potassium- containing IVF use in the emergency department, and costs. RESULTS: There were 11 602 pathway-eligible encounters (10 287 patients) across the study. Median IVF infusion hours did not change. Isotonic maintenance IVF use increased significantly from 9.3% to 50.6%, whereas the use of any hypotonic fluid decreased from 94.2% to 56.6%. There were significant increases in daily weight measurement and recommended serum sodium testing. Cases of dysnatremia increased from 2 to 4 among pathway-eligible patients and were mostly associated with hypotonic IVF use. Patients in the emergency department had a significant increase in the number of potassium-containing IVF bags (52.9% to 75.3%). Total hospitalization and laboratory test costs did not change significantly. CONCLUSIONS: This is the first report of outcomes of a clinical pathway to standardize IVF use. Implementation was feasible in both medical and surgical units, with sustained improvements for 1 year. Future improvement work includes increasing PowerPlan use and developing clinical assessment tools. a Department of Pediatrics, Division of General Pediatrics and Hospital Medicine, University of Washington, Seattle, Washington; b Clinical Effectiveness Program, Seattle Children’ s Hospital, Seattle, Washington; c Center for Child Health, Behavior and Development, Seattle Children’ s Research Institute, Seattle, Washington; and d Department of Pediatrics, Hawaii Permanente Medical Group, Wailuku, Hawaii www.hospitalpediatrics.org DOI:https://doi.org/10.1542/hpeds.2017-0099 Copyright © 2017 by the American Academy of Pediatrics Address correspondence to Sahar N. Rooholamini, MD, MPH, Department of Pediatrics, Division of General Pediatrics and Hospital Medicine, Seattle Children’ s Hospital, M/S FA.2.115, PO Box 5371, Seattle, WA 98105. E-mail: [email protected] HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671). FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: Supported by an internal grant from Seattle Children’ s Hospital Clinical Effectiveness Program. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. Dr Rooholamini conceptualized and designed the study and drafted and revised the manuscript; Ms Clifton and Ms Haaland collected, cleaned, and analyzed data and reviewed and revised the manuscript; Drs McGrath, Vora, Crowell, Romero, and Foti refined study design and outcome measures and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. HOSPITAL PEDIATRICS Volume 7, Issue 12, December 2017 703 by guest on February 19, 2020 http://hosppeds.aappublications.org/ Downloaded from
Transcript of RESEARCH ARTICLE ...Holliday-Segar method has been the risk of iatrogenic hyponatremia with...

RESEARCH ARTICLE
Outcomes of a Clinical Pathway to Standardize Useof Maintenance Intravenous FluidsSahar N. Rooholamini, MD, MPH,a Holly Clifton, MPH,b Wren Haaland, MPH,c Caitlin McGrath, MD,a Surabhi B. Vora, MD, MPH,a,b Claudia S. Crowell, MD, MPH,a,b
Holly Romero, MD,d Jeffrey Foti, MDa,b
A B S T R A C T OBJECTIVES: Improper use of maintenance intravenous fluids (IVFs) may cause serious hospital-acquired harm. We created an evidence-based clinical pathway to guide providers on the indicationsfor IVF, its preferred composition, and appropriate clinical monitoring.
METHODS: Pathway implementation was supported by the creation of an electronic order set(PowerPlan) and hospital-wide education. Outcomes were measured among pathway-eligiblepatients for the years before (July 1, 2014–June 30, 2015) and after (July 1, 2015–June 30, 2016)implementation. An interrupted time series analysis was used to evaluate monthly trends related toIVF use, including the following: median duration, proportions of isotonic and hypotonic IVF,adherence to monitoring recommendations, incidence of associated severe dysnatremia, potassium-containing IVF use in the emergency department, and costs.
RESULTS: There were 11 602 pathway-eligible encounters (10 287 patients) across the study. MedianIVF infusion hours did not change. Isotonic maintenance IVF use increased significantly from 9.3%to 50.6%, whereas the use of any hypotonic fluid decreased from 94.2% to 56.6%. There weresignificant increases in daily weight measurement and recommended serum sodium testing. Casesof dysnatremia increased from 2 to 4 among pathway-eligible patients and were mostly associatedwith hypotonic IVF use. Patients in the emergency department had a significant increase in thenumber of potassium-containing IVF bags (52.9% to 75.3%). Total hospitalization and laboratory testcosts did not change significantly.
CONCLUSIONS: This is the first report of outcomes of a clinical pathway to standardize IVF use.Implementation was feasible in both medical and surgical units, with sustained improvements for1 year. Future improvement work includes increasing PowerPlan use and developing clinicalassessment tools.
aDepartment ofPediatrics, Division of
General Pediatrics andHospital Medicine,
University of Washington,Seattle, Washington;
bClinical EffectivenessProgram, Seattle
Children’s Hospital,Seattle, Washington;
cCenter for Child Health,Behavior and
Development, SeattleChildren’s Research
Institute, Seattle,Washington; anddDepartment of
Pediatrics, HawaiiPermanente Medical
Group, Wailuku, Hawaii
www.hospitalpediatrics.orgDOI:https://doi.org/10.1542/hpeds.2017-0099Copyright © 2017 by the American Academy of Pediatrics
Address correspondence to Sahar N. Rooholamini, MD, MPH, Department of Pediatrics, Division of General Pediatrics and HospitalMedicine, Seattle Children’s Hospital, M/S FA.2.115, PO Box 5371, Seattle, WA 98105. E-mail: [email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671).
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by an internal grant from Seattle Children’s Hospital Clinical Effectiveness Program.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Dr Rooholamini conceptualized and designed the study and drafted and revised the manuscript; Ms Clifton and Ms Haaland collected,cleaned, and analyzed data and reviewed and revised the manuscript; Drs McGrath, Vora, Crowell, Romero, and Foti refined study designand outcome measures and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted andagree to be accountable for all aspects of the work.
HOSPITAL PEDIATRICS Volume 7, Issue 12, December 2017 703
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

In the past decade, the standard approachto pediatric maintenance intravenous fluid(IVF) therapy has shifted. For generations,the Holliday-Segar method (published in1957 and based on studies of the caloricexpenditure of previously healthyhospitalized infants) has been the standardfor the composition and rate of IVF inpediatric patients of all ages despite theauthors’ disclaimers that their calculationsmay not be generalizable.1 The mostprominent concern raised about theHolliday-Segar method has been the risk ofiatrogenic hyponatremia with hypotonicIVF,2–8 which can have devastating clinicalconsequences, including seizures, cerebraledema, and death. This risk is exacerbatedin inpatients who commonly have 1 or morenonosmotic risk factors for increasedantidiuretic hormone (ADH) secretion,including but not limited to the following:nausea, vomiting, uncontrolled pain, recentsurgery, and acute respiratory and centralnervous system disorders. Authors of aCochrane Collaboration systematic reviewand meta-analysis9 concluded that isotonicIVF decreased the risk of hyponatremia by52% compared with hypotonic IVF usingdata from 10 studies (pooled risk ratio 50.48; 95% confidence interval [CI]: 0.38 to 0.60).
One clinical pathway related to IVFmanagement in children has beenpreviously described.10 To our knowledge, noarticle regarding the clinical outcomes ofsuch a pathway has been published. Inaddition, we are unaware of any analysesrelated to the costs associated withpathway-guided IVF use.
We designed and implemented a clinicalstandard work (CSW) pathway to guidemaintenance IVF use at our children’shospital. Our specific aims with this studywere to evaluate the pathway’s impact onthe following: overall IVF use, use of isotonicand hypotonic IVF and potassium-containingIVF in the emergency department (ED),weight and laboratory monitoring, andincidence of severe dysnatremia.
METHODSSetting and Context
There were 3 sentinel events at our tertiary,370-bed, university-affiliated children’shospital and regional referral center that
sparked an initiative to standardize use ofmaintenance IVF. A child with acutegastroenteritis who received more than themaintenance rate of hypotonic IVFdeveloped severe iatrogenic hyponatremiaand cerebral edema. Two other patientsdied of unrecognized hypernatremicdehydration because of inappropriate fluidrestriction and inadequate clinical andlaboratory monitoring. After these events,hospital leadership requested that astandardized approach be created toaddress inconsistencies and potential high-risk practices around IVF use. We formed amultidisciplinary team to design, implement,and monitor the maintenance IVF pathway.This team was led by faculty from generalpediatrics and hospital medicine andincluded physician and nursingrepresentation from emergency medicine,nephrology, and general surgery. The teamwas supported by a centralized clinicaleffectiveness group, which included amedical librarian, informatician, consultant,project manager, and data analyst.
Interventions
Literature Review
The standardized planning andimplementation of our hospital’s CSWpathways has been previously described.11
A systematic literature search from 2004to 2014 was undertaken using the searchterms and selection process referenced inour publicly available pathway.12
Evidence Synthesis and PathwayCreation
As evidence was synthesized, specificrecommendations were developed(Supplemental Fig 4), and a pathwayframework was created with phases for IVFinitiation and monitoring. When evidencecould not sufficiently address clinicalquestions, team members polled theirrespective colleagues and reported back tothe group, with final decisions made using aLikert scale–based consensus tool.
Using standard processes and templatesdeveloped by our hospital’s ClinicalEffectiveness team, we developed a clinicalalgorithm12 with an associated web-basedtraining module. Presentations were givento our hospital’s Clinical Standards
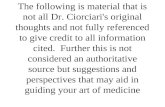
Committee, Executive Nursing Leadership,and the Medical Director of Laboratories toestablish wide-ranging awareness andsupport for our work. Key drivers wereidentified for each aim; an example for theuse of potassium-containing IVF in the ED isincluded in Fig 1.
Pathway Implementation andLogistical Support
A maintenance IVF PowerPlan (CernerMillennium; Cerner Corporation, London,UK) was created and embedded into allPowerPlans that previously contained IVForders. The PowerPlan can also be orderedon its own. Informaticians assisted with thedevelopment of a weight change calculatorthat displays on the “patient summary”page of the electronic medical record andindicates both the absolute and relative(percentage) change between the last2 consecutive measured weights. Thisallows for rapid identification of significantweight and/or fluid status changes inpatients, defined as a difference of$3% and chosen based on conventionaldehydration classification schemes andto ensure early identification of weightchanges.
Patients are pathway eligible if they areeuvolemic and require maintenance IVfluids on the basis of clinical judgment andare ineligible if they are any of the following:hypovolemic, hypervolemic, critically ill, onparenteral nutrition or a ketogenic diet,severely dysnatremic before IVF initiation(serum sodium$150 mEq/L or#130 mEq/L),,40 weeks postmenstrual age, diabetic, oradmitted to critical care or certainsubspecialty services (nephrology,neurosurgery, cardiology, biochemicalgenetics, oncology, or organ and/or stem celltransplant). “Maintenance” is defined in ourpathway as requiring $75% of fluid needsvia IVF as calculated by the “4-2-1” rule, anhourly approximation of fluid requirements.1
Providers are guided to select IVFcomposition on the basis of the presence orabsence of increased ADH secretion riskfactors.12 These include the following:uncontrolled pain, uncontrolled nauseaand/or vomiting, recent surgery, acutecentral nervous system disorders, andacute pulmonary diseases, particularly
704 ROOHOLAMINI et al
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

pneumonia. Our pathway encouragesclinicians to use their judgment indetermining eligibility for the pathwayand subsequent IVF choice.
Pathway implementation occurred on July 1,2015. Pathway details were communicatedthrough hospital-wide announcements andpresentations at faculty meetings andteaching conferences.
Before pathway development, standardpractice in our ED had been to use onlynon–potassium-containing IVF. This often ledto IVF bags being wasted when potassium-containing IVF were subsequently orderedafter admission. Our literature review didnot reveal much evidence on this topic;however, given our pathway’s exclusioncriteria, we were confident that patientswith contraindications to potassium wouldbe excluded from the pathway. To supportthe recommendation that maintenance IVFshould include potassium for eligiblepatients, IVF bags in the ED were restockedso that maintenance IVF bags withoutpotassium chloride were removed fromautomated dispensing cabinets.
Education
A web-based training module was requiredtraining for a subset of faculty in generalpediatrics, hospital medicine, andemergency medicine. Surgical andmedical residents were encouraged (butnot required) to complete the training.
Pathway descriptions were included innursing bulletins and reviewed at dailynursing huddles for 2 months afterimplementation.
Measures
Aim statements were formulated beforepathway implementation to inform theprocess metrics that are reviewed atquarterly improvement meetings.
Objective 1
Our first objective was to determine ifpathway implementation significantlyreduces the overall use of IVF amongpathway-eligible medical and surgicalpatients.
Aim Statement
Our aim was to decrease IVF use amongpathway-eligible patients by 10%.
Outcomes
Duration of IVF was measured by thenumber of hours of IVF infusion at any rate.5 mL/h, as recorded by nurses. This cutoffrate was used on the basis of institutionalpolicy for standard “to keep open” IVF rates.To assess for potential confounding by ICUstay, the proportion of pathway-eligiblepatient encounters with any time in the ICUand the mean length of ICU stay in dayswere compared pre- and post-pathwayimplementation. Each patient’s medicalcomplexity was categorized by using thePediatric Medical Complexity Algorithm.13
Objective 2
Our second objective was to assess whetherpathway implementation significantlychanges the frequency with which hypotonic(0.45% sodium chloride and 0.225% sodiumchloride) and isotonic (0.9% sodiumchloride) IVF are prescribed by providersand any resultant changes in the incidenceof severe hyponatremia and hypernatremia.
Aim Statement
Our aim was to increase the use of isotonicfluids by 20%, with an equivalent decreasein use of hypotonic fluids.
Outcomes
The proportions of hypotonic and isotonicIVF orders were analyzed before and afterimplementation in pathway-eligible patients.This analysis was independent of thedextrose content of IVF because dextrose israpidly used by cells and does notsignificantly contribute to intravascularosmolality compared with sodium andchloride. A chart review of pathway-eligiblepatients with severe hyponatremia andhypernatremia (sodium #130 or$150 mEq/L, respectively) was performedto better understand the clinicalcharacteristics and potential risk factorsassociated with these electrolytedisturbances. The overall dysnatremia ratefor this subgroup was calculated as follows:IVF-associated dysnatremia divided by allpathway-eligible patients on IVF.
FIGURE 1 Sample key driver diagram.
HOSPITAL PEDIATRICS Volume 7, Issue 12, December 2017 705
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

Objective 3
Our third objective was to assess whetherpathway implementation reduces waste andvariability in maintenance IVF use byincreasing the percentage of potassium-containing IVF bags ordered in the ED.
Aim Statement
Our aim was to have 80% of pathwaypatients receiving IVF in the ED to receivepotassium-containing fluids at initiation.
Outcomes
The proportions of potassium-containingand potassium-free IVF bags were analyzedbefore and after implementation inpathway-eligible patients.
Objective 4
Our fourth objective was to determine ifpathway implementation significantlyimproves appropriate clinical andlaboratory monitoring for patients whoremain on maintenance IVF.
Aim Statement
Our aim was that among patients on ourpathway receiving maintenance IVF, 50%would have (1) daily weight measurementand (2) serum sodium checked within36 hours of IVF initiation.
Outcomes
To measure adherence to therecommendation for daily weightmeasurements, we measured the number ofpatients on our pathway with a weightrecorded per calendar day (numerator)divided by the total number of pathwayeligible days (denominator). This calculationwas then compared pre- and post-pathwayimplementation. To exclude patient weightsand laboratory values obtained onadmission, we only included pathway-eligiblepatients who had been on IVF for$12 hours.Additionally, a serum sodium result had tohave been obtained ,36 hours after first IVbag administration. This 36-hour markreflects the PowerPlan, in which a serumsodium test is ordered for the subsequentcalendar day after IVF initiation.
All data came from medical records forpatients admitted during the time periods ofinterest; laboratory and medicationadministration data were obtained from
Cerner and hospital administrative datafrom Epic Hyperspace.
Analysis
Outcomes were measured for the yearbefore (July 1, 2014–June 30, 2015) and theyear immediately after (July 1, 2015–June30, 2016) pathway implementation.Population characteristics in both periodswere compared by using t tests for themean of continuous variables, x2 tests forcategorical variables, and Wilcoxon ranktests for median of continuous variableswhen appropriate. An interrupted timeseries analysis was used to evaluate trendsover time and compare pre- and post-pathway outcomes. Rates for each outcomewere calculated per month. A linearregression was estimated for each timeperiod, and Wald tests were used tocompare slope parameters across periodsand intercept parameters across periods.
Costs were adjusted for inflation to2016 dollars using the medical servicescomponent of the consumer price index andwinsorized at the 99th percentile. Differenceestimates for costs were calculated byusing bootstrapped t tests with1000 replicates. Bias-corrected 95% CIsare reported.
All statistical analyses were conducted byusing Stata version 12.0 (StataCorp LP,College Station, TX).
Ethics
The hospital institutional review boardapproved this research project.
RESULTS
In the year before pathway implementation,there were 6030 pathway-eligibleencounters representing 5324 distinctpatients. In the year after pathwayimplementation, 5572 encounters and4963 distinct patients were pathwayeligible. Pre-implementation, 68% of alladmitted patients were pathway eligiblecompared with 63% post-implementation.The PowerPlan was used for 62% of alleligible encounters, totaling 3249 patientsin the post-implementation period. Therewere no statistically significant differencesin demographic characteristics, meanlength of hospital stay, ICU admissionrates, or medical complexity (Table 1)between the 2 study populations.
Pathway outcomes are summarized inTable 2 and described in detail below.
IVF Use and Monitoring
The median hours of IVF infusion inpathway-eligible patients was identicalbetween study periods. The use of isotonicmaintenance IVF increased significantly(9.3% to 50.6%; difference: 41.3%; 95% CI:39.8% to 42.8%), whereas the use of anyhypotonic fluid decreased significantly(94.2% to 56.6%; difference: 237.6%; 95% CI:239.0 to 236.2%), as shown in Fig 2. Theuse of 0.225% saline (1/4 normal saline[NS]) accounted for a small percentage ofIVF across study periods: 4% of eligibleencounters in the pre-implementationperiod compared with 0.3% post-implementation.
TABLE 1 Comparison of Pre- and Post-pathway Implementation Populations
Characteristic Pre-implementation Post-implementation P
Pathway-eligible encounters 6030 5572 —
No. distinct patients 5324 4963 —
Age, mean (SD) 7.9 (6.2) 8.0 (6.1) .24
Female, n (%) 2885 (47.8) 2645 (47.5) .69
Inpatient LOS, d, mean (SD) 3.4 (11.6) 3.2 (7.5) .34
ICU admission, n (%) 451 (7.5) 391 (7.0) .34
ICU LOS, d, median 1.6 1.6 .86
PMCA, n (%) — — .08
Without chronic disease 2060 (34.2) 1820 (32.7) —
Noncomplex chronic 1514 (25.1) 1493 (26.8) —
Complex chronic 2454 (40.7) 2258 (40.5) —
LOS, length of stay; PMCA, Pediatric Medical Complexity Algorithm; —, not applicable.
706 ROOHOLAMINI et al
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

Compared with the pre-implementationperiod, during the post-implementationperiod there were significant increases inthe number of potassium-containing bagsadministered in the ED (52.9% to 75.3%;difference: 22.5%; 95% CI: 19.4% to 25.6%;Fig 3) and the proportion of patients whohad serum sodium monitoring within36 hours of IVF initiation and a daily weightmeasurement.
Severe Iatrogenic Hyponatremiaand Hypernatremia
Chart reviews of pathway-eligible patientswith severe dysnatremia in the pre- and post-implementation periods revealed an increasein IVF-associated dysnatremia from 2 to4 cases, respectively (Supplemental Table 3).No patients in the study required ICU transferas a result of their dysnatremia.
Costs
The mean total costs of hospitalization didnot significantly increase from pre- to post-pathway implementation (from $18 880 perencounter to $19 581 per encounter;difference: 1$701; 95% CI: 2$108 to $1409).The mean costs of IVF per account increasedsignificantly by $14. Mean electrolyte andserum sodium laboratory test costs peraccount were not significantly different.
DISCUSSION
To our knowledge, this is the first study of aclinical pathway in which an evidence-based
approach to maintenance IVF therapy inmedical and surgical pediatric patients isstandardized. With our pathway, we havesucceeded in changing and sustainingprescribing practices of clinicians awayfrom hypotonic IVF and toward monitoreduse of isotonic IVF when there are concernsfor increased ADH secretion. Although thereare potential risks and harms associatedwith the use of IVF of any composition, thesafety of isotonic fluids to meetmaintenance hydration needs withsignificantly less risk for iatrogenichyponatremia is supported by a growingbody of evidence.2–4,8,9 Our CSW pathwaydemonstrates how evidence can beoperationalized and is not a substitute forclinical research.
Systematic changes to promote consistentuse of maintenance IVF between ED andacute care units led to a 22.5% increase inuse of recommended potassium-containingIVF in the ED. We continue to see thesechanges sustained .1 year after pathwayimplementation, largely because the supplyin ED dispensing cabinets was changed toensure that recommended IVF bags arereadily available. There have been noreports of pathway-associatedhyperkalemia since implementation.
The median duration of IVF use, includinginfusion hours in the ED before admission,did not change pre- and post-
implementation. There are no nationalbenchmarks for IVF use to provide a point ofcomparison; however, future pathwayefforts will reinforce appropriate IVF useonly when enteral routes of hydration arenot possible and prompt IVF discontinuationwhen feasible. Our post-implementationplan-do-study-act work includes discussionswith pharmacy leaders to incorporatequestions about IVF use as part of theirstandard work to encourage a paradigmshift to view IVF as a medication withserious risks.
During the creation and implementation ofthis pathway, our biggest challenge wasformulating feasible recommendations forweight and sodium monitoring.Collaboration with nursing leadership to (1)provide ongoing education about thepathway’s monitoring recommendationsand (2) address practical constraints (eg,availability of scales on every unit) has beenessential in maintaining the gains inadherence to these recommendations.
The most controversial recommendation ofour pathway has been serum sodiummonitoring, the value of which has beenquestioned given the overall low incidenceof severe iatrogenic dysnatremia in ourpopulation and the associated pain, anxiety,and costs of this test. This recommendationwas based on our literature review and datashowing that the incidence of iatrogenic
TABLE 2 Outcomes Pre- and Post-pathway Implementation Among Pathway-Eligible Patients
Outcome Measure Pre-implementation Post-implementation Difference (95% CI) P
IVF infusion, h, median 18.0 18.0 — .19
IVF composition usage, n (%)
Isotonic (NS) 560 (9.3) 2819 (50.6) 41.3 (39.8 to 42.8) ,.001
Hypotonic (any) 5679 (94.2) 3155 (56.6) 237.6 (239.0 to 236.2) ,.001
1/2 NS 5494 (91.1) 3145 (56.4) 234.7 (236.1 to 233.2) ,.001
1/4 NS 264 (4.4) 15 (0.3) 24.1 (24.7 to 23.6) ,.001
ED IVF encounters with K-containing IVF, n (%) 965 (52.9) 1204 (75.3) 22.5 (19.4 to 25.6) ,.001
Eligible patients with sodium level check, n (%) 362 (18.4) 537 (30.5) 12.1 (9.4 to 14.8) ,.001
% of eligible d with wt collected, mean (SD) 47.9 (43.5) 55.6 (42.9) 7.8 (4.8 to 10.7) ,.001
Instances of dysnatremia 2 4 — —
Total costs (2016 $), mean (SD) 18879.8 (21002.1) 19580.6 (20789.9) 700.8 (2108.0 to 1409.1) .07
Fluid costs (2016 $), mean (SD) 99.5 (106.4) 113.6 (121.4) 14.1 (10.1 to 18.1) ,.001
Electrolyte laboratory test costs (2016 $), mean (SD) 62.0 (86.1) 58.6 (71.8) 23.4 (28.1 to 2.0) .20
Serum sodium laboratory test costs (2016 $), mean (SD) 15.9 (9.1) 15.6 (6.8) 20.3 (23.3 to 2.3) .85
Differences represent differences in rates where rates are shown. Otherwise, it is the difference in means. Differences, 95% CIs, and P values are estimated using ttests or rank-sum tests for comparison of medians. K, potassium; —, not applicable.
HOSPITAL PEDIATRICS Volume 7, Issue 12, December 2017 707
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

hyponatremia is highest among patients onIVF in the first 24 hours after initiation4 aswell as discussions with multidisciplinarystakeholders. Our chart review of pathway-eligible patients revealed an increase insevere IVF-related dysnatremia betweenpre- and post-implementation periods(Supplemental Table 3), which could beattributed to greater detection after
pathway implementation. Of the total6 cases of severe dysnatremia across studyperiods, 4 occurred in patients withhyponatremia who had received hypotonicfluids. Two patients in the post-implementation period had hypernatremia;1 patient presented with acute illness andmild hypernatremia (149 mEq/L) thatworsened with isotonic IVF, and a second,
medically complex patient hadhypernatremia while receiving hypotonic IVFin the setting of missed enteral feedingsand possible dehydration. These results areconsistent with the pathophysiologic basisfor our pathway recommendations andunderscore the need for careful clinicalassessment for increased ADH secretionrisk factors for each patient.
We found that for every 2589 patientencounters, 1 instance of severe IVF-relateddysnatremia occurred. This number neededto harm does not capture less severedysnatremias and should be interpretedcautiously, especially because we identifiedcases retrospectively via electronic medicalrecord. In randomized controlled trials inwhich researchers compared isotonic andhypotonic IVF, real-time standardized clinicalassessment tools have been used to evaluateadverse effects such as hypertension andedema.3,4 A future area of intervention is toidentify those at greatest risk of dysnatremiawith such a tool and target serum sodiumtesting to these patients.
The financial costs of IVF increasedsignificantly between pre- and post-pathwayperiods, although the absolute difference($14; 95% CI: $10 to $18) was unlikely to havehad clinical significance. Total hospitalizationand laboratory test costs did not increasesignificantly between study periods,indicating that our pathway was notassociated with significant cost increases.
Our study has additional limitations. Wehave had ∼60% PowerPlan usage despiteefforts up front to embed it into all majormedical and surgical plans. This may be theresult of providers ordering maintenanceIVF after admission orders have alreadybeen placed, thus bypassing the fullPowerPlan that includes IVF compositionand monitoring recommendations. Wecurrently rely on reporting and feedback byproviders to identify plans that do notcontain our PowerPlan, and this has causeda lag in addressing gaps in use. There isalso a difference between medical andsurgical units in PowerPlan use (53% on themedical unit and 78% on the surgical unit),which we are addressing as a targeted areafor improvement. The generalizability of ourresults is limited because our pathway was
FIGURE 2 Percent of encounters with isotonic or hypotonic IVF use. Arrow indicates pathwayimplementation.
FIGURE 3 Percent of ED patients on IVF with appropriate potassium-containing IVF. Arrowindicates pathway implementation.
708 ROOHOLAMINI et al
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

implemented and studied at a single,freestanding tertiary-care children’shospital with a culture of patient safety andstandardized pathways. Finally, thesuccesses of this pathway work should beassessed for their value. We plan to conducta formal value analysis for serum sodiumtesting using a previously published tool.14
CONCLUSIONS
The implementation of our clinical pathwayhas led to sustained changes in IVF-prescribing practices and improvedconsistency of IVF use between the ED andacute care units, adherence to weight andserum sodium monitoringrecommendations, and evidence-based useof isotonic IVF.
Acknowledgments
We thank Ashley Van Drunen, KateDrummond, Susan Klawansky, ElaineBeardsley, Ari Pollack, Russ Migita, andMichael Leu of the Maintenance IVF PathwayTeam, whose efforts made this workpossible. We thank Mark Del Beccaro andCara Bailey (sponsors), Darren Migita(Medical Director), and Kathy Mullin(Director) of Clinical Effectiveness fortheir support.
REFERENCES
1. Holliday MA, Segar WE. The maintenanceneed for water in parenteral fluidtherapy. Pediatrics. 1957;19(5):823–832
2. Moritz ML, Ayus JC. Maintenanceintravenous fluids in acutely III patients.N Engl J Med. 2015;373(14):1350–1360
3. Friedman JN, Beck CE, DeGroot J, GearyDF, Sklansky DJ, Freedman SB.Comparison of isotonic and hypotonicintravenous maintenance fluids: arandomized clinical trial. JAMA Pediatr.2015;169(5):445–451
4. McNab S, Duke T, South M, et al.140 mmol/L of sodium versus 77 mmol/Lof sodium in maintenance intravenousfluid therapy for children in hospital(PIMS): a randomised controlled double-blind trial. Lancet. 2015;385(9974):1190–1197
5. Choong K, Kho ME, Menon K, Bohn D.Hypotonic versus isotonic saline inhospitalised children: a systematic review.Arch Dis Child. 2006;91(10):828–835
6. Neville KA, Verge CF, Rosenberg AR,O’Meara MW, Walker JL. Isotonic is betterthan hypotonic saline for intravenousrehydration of children withgastroenteritis: a prospectiverandomised study. Arch Dis Child.2006;91(3):226–232
7. Foster BA, Tom D, Hill V. Hypotonic versusisotonic fluids in hospitalized children: asystematic review and meta-analysis.J Pediatr. 2014;165(1):163–169.e2
8. Wang J, Xu E, Xiao Y. Isotonic versushypotonic maintenance IV fluids inhospitalized children: a meta-analysis.Pediatrics. 2014;133(1):105–113
9. McNab S, Ware RS, Neville KA, et al.Isotonic versus hypotonic solutions formaintenance intravenous fluid
administration in children. CochraneDatabase Syst Rev. 2014;(12):CD009457
10. Edelson JB, Orenstein EW, Zaoutis LB,Copelovitch L. Intravenous fluidmanagement in the pediatric hospitalsetting: is isotonic fluid the rightapproach for all patients? Curr TreatOptions Pediatr. 2015;1(1):90–99
11. Koves IH, Leu MG, Spencer S, et al;Diabetic Ketoacidosis GuidelineDevelopment Workgroup. Improving carefor pediatric diabetic ketoacidosis.Pediatrics. 2014;134(3). Available at:www.pediatrics.org/cgi/content/full/134/3/e848
12. Seattle Children’s Hospital, Romero H,Rooholamini S, Drummond K, Foti J, VanDrunen A. Maintenance IV fluidmanagement pathway. 2015. Available at:www.seattlechildrens.org/pdf/maintenance-IV-fluid-management-pathway.pdf. Accessed September 28,2017
13. Simon TD, Cawthon ML, Stanford S, et al;Center of Excellence on Quality of CareMeasures for Children with ComplexNeeds (COE4CCN) Medical ComplexityWorking Group. Pediatric medicalcomplexity algorithm: a new method tostratify children by medical complexity.Pediatrics. 2014;133(6). Available at:www.pediatrics.org/cgi/content/full/133/6/e1647
14. Leu MG, Austin E, Foti JL, et al. Aframework for evaluating value of newclinical recommendations. Hosp Pediatr.2016;6(10):578–586
HOSPITAL PEDIATRICS Volume 7, Issue 12, December 2017 709
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

DOI: 10.1542/hpeds.2017-0099 originally published online November 21, 2017; 2017;7;703Hospital Pediatrics
Vora, Claudia S. Crowell, Holly Romero and Jeffrey FotiSahar N. Rooholamini, Holly Clifton, Wren Haaland, Caitlin McGrath, Surabhi B.
FluidsOutcomes of a Clinical Pathway to Standardize Use of Maintenance Intravenous
ServicesUpdated Information &
http://hosppeds.aappublications.org/content/7/12/703including high resolution figures, can be found at:
Supplementary Material
2017-0099.DCSupplementalhttp://hosppeds.aappublications.org/content/suppl/2017/11/17/hpeds.Supplementary material can be found at:
Referenceshttp://hosppeds.aappublications.org/content/7/12/703.full#ref-list-1This article cites 10 articles, 5 of which you can access for free at:
Subspecialty Collections
provement_subhttp://classic.hosppeds.aappublications.org/cgi/collection/quality_imQuality Improvementedicine_subhttp://classic.hosppeds.aappublications.org/cgi/collection/hospital_mHospital Medicineion:practice_management_subhttp://classic.hosppeds.aappublications.org/cgi/collection/administratAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.hosppeds.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from

DOI: 10.1542/hpeds.2017-0099 originally published online November 21, 2017; 2017;7;703Hospital Pediatrics
Vora, Claudia S. Crowell, Holly Romero and Jeffrey FotiSahar N. Rooholamini, Holly Clifton, Wren Haaland, Caitlin McGrath, Surabhi B.
FluidsOutcomes of a Clinical Pathway to Standardize Use of Maintenance Intravenous
http://hosppeds.aappublications.org/content/7/12/703located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 2154-1663. Illinois, 60143. Copyright © 2017 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 2012. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on February 19, 2020http://hosppeds.aappublications.org/Downloaded from