edition may and june 2013 - fcm.unicamp.br · Figure 1 – Non contrast abdominal CT scan, coronal...
15
may and june 2013 edition
Transcript of edition may and june 2013 - fcm.unicamp.br · Figure 1 – Non contrast abdominal CT scan, coronal...

may and june 2013 edition

Dr. Carlos D'Ancona
We are making profound modifications in the structure of Urovirt. This year, 2013, the journal will become bimestrial. Do not miss reading the clinical case which presents the case of a young patient with cystine stones with interesting comments by Dr. Liliam Montero and Dr. Manoj Monga. In the section of image learning videos were presented about the localization and dissection of intra-abdominal testis. With the increase of endourological procedures a greater interest has developed in ureterorenolithotrisy and an increased number of complications have been observed. This is presented in News Technologies, a classification of ureteral lesions. In Urologic News, we are advertising the new course of Good Morning Urology which will be presented on June 12, 2013 at The Royal Palm Hotel. The scientific activities performed were Urodynamic without mystery and the abstract of the Ph.D. thesis is included for you to read. Enjoy your reading.

Dr. Guido Barbagli Dr. Manoj Monga Dr. Mark Soloway
editorialboardeditorialboard
Dr. Guido Barbagli Dr. Manoj Monga Dr. Mark Soloway
Dr. Carlos D'Ancona Dr. Paulo Palma Dr. Daniel Carlos Silva
Co-editors:
Dr. Cassio Riccetto Dr. Ricardo Miyaoka Dr. Ricardo Souza
Radiology - Editorial Committee
Dr. Adilson Prando Dr. Athanese Billis
Editorial Committee
Dr. Guido Barbagli Dr. Manoj Monga Dr. Mario João Gomes Dr. Matthias Oelke Dr. Mark Soloway
Editors: Associated Editor:
Pathology - Editorial Committee
Dr. Carlos D'Ancona Dr. Paulo Palma Dr. Daniel Carlos Silva
Co-editors:
Dr. Cassio Riccetto Dr. Ricardo Miyaoka Dr. Ricardo Souza
Radiology - Editorial Committee
Dr. Adilson Prando Dr. Athanese Billis
Editorial Committee
Dr. Guido Barbagli Dr. Manoj Monga Dr. Mario João Gomes Dr. Matthias Oelke Dr. Mark Soloway
Editors: Associated Editor:
Pathology - Editorial Committee

CYSTINE CALCULI: MULTIDISCIPLINARY CHALLENGE
edition: may and june 2013
Elaine Bronzatto, Daniel Silva
Division of Urology - UNICAMP
clinicalCASE

CLINICAL BACKGROUND
CLINICAL WORKUP
Eighteen year-old male is under treatment for recurrent stone disease since 10 years of age. He underwent several surgical interventions including percutaneous nephrolithotomy on left side, open pielolithotomy on left side and repeated extracorporeal shockwave lithotripsy (ESWL) session bilaterally.
Laboratorial : cystinuria, hypomagnesuria and hypophosphaturia
2. Abdominal CT scan (figure 1)
Figure 1 – Non contrast abdominal CT scan, coronal and sagital cuts, showing a grade II staghorn calculi on right side and multiple calculi in inferior calyx on left side (arrows).
Right percutaneous nephrolithotomy was performed (figure 2)
MANAGEMENT
F igure 2 – Percutaneous nephrolithotomy. A) Patient in ventral position with marking (left posterior axilary line, 12th rib edge). B) Access to collecting system and placement of guidewire down the ureter. C) Final aspect: residual fragments and double J catheter.
FOLLOW UPPatient was kept under hypossodic diet, with red meat restriction and fluid intake over 2 liters/day. Potassium citrate 2g/ day; magnesium oxide 100mg/ day; pyridoxine 40 mg/day; captopryl 50 mg/day.
clinicalCASEedition: may and juneElaine Bronzatto, Daniel SilvaDivision of Urology - UNICAMP

Manoj MongaCleveland Clinic
Manoj MongaCleveland Clinic
O tratamento desse paciente é um desafio – calculo coraliforme bilateral (parcial no lado esquerdo). Estou de acordo com a indicação de nefrolitotripsia percutânea. Eu gostaria de puncionar o cálice superior, risco um pouco maior mas com melhor resultado em cálculos grandes, especialmente em associado com nefroscopio flexível (1). A punção é feita em expiração forçada, utilizando orientação endoscópica para ter uma punção acurada de onde introduzir a agulha (2). Nesse ponto os cálculos residuais no rim direito podem ser tratados com ureteroscopia flexível.
O calculo do lado esquerdo, seria melhora acesso percutâneo através do cálice superior. Eu prefiro o cálice superior em todos os casos com configuração ramificada porque possibilita maior acesso com nefroscopio rígido para tratamento de cálculos grandes com litotridor ultrassônico. O paciente deverá fazer avaliação quantitativa de cistina em urina de 24 horas, devendo ser considerado tratamento com Thiola (alfa-mercatopropionil-glicina).
References:1. Wong C, Leveillee RJ. Single upper-pole percutaneous access for treatment of > or = 5-cm complex branched staghorn calculi: is shockwave lithotripsy necessary? J Endourol. 2002 Sep;16(7):477-81.2. Isac W, Rizkala E, Liu X, Noble M, Monga M. Endoscopic-guided Versus Fluoroscopic-guided Renal Access for Percutaneous Nephrolithotomy: A Comparative Analysis. Urology. 2013 Feb;81(2):251-6. doi: 10.1016/j.urology.2012.10.004.
COMMENTARY
clinicalCASEedition: may and juneElaine Bronzatto, Daniel SilvaDivision of Urology - UNICAMP

COMMENTARY
Lillian Moneiro PereiraClinica do Rim e Hipertensão de Campinas
Cystinuria is an inherited autosomal recessive disease in which cystine transportation through renal proximal tubules is deficient which in turn leads to urinary over saturation. Cystine calculi occur in 1 to 2% of patients with stone disease (and can reach 5% in pediatric population). It must be suspected whenever stone is formed in early infant age or teenage and when staghorn calculi is diagnosed. Lack of adequate response to extracorporeal shockwave lithotripsy may also rise suspicion of cystine calculi since these are extremely resistant (although less opaque than calcium oxalate stones).
Diagnosis is based upon calculi chemical analysis or through visualization of hexagonal crystals which are known to be pathognomonic in urinalysis (up to 25% of cases), especially when family history is positive.
In the absence of identifiable calculi or crystals, work up begins with a qualitative urinalysis of cystine (reference value:negative) – positive value indicates a urinary concentration of at least 75 mg/ml. Whenever one finds a positive result, a quantitative analysis is mandatory in a 24 hours urine colection specimen. A normal value should be lower than 50 mg/1,73m2/day. In cystinuria cases, excretion is usually higher than 400 mg/1,73m2/day. In the present case, urine excretion was 1485 mg/day and pharmacological treatment was affected.
The basis of treatment relies on keeping a cystine urinary concentration lower than solubility level, which is 243 mg/L on average under a pH higher than 7. As such, in the current case a minimal urinary volume of 6 liters would be necessary to avoid supersaturation and crystal formation. Besides, this volume would be needed throughout daytime and night time. Maintanance of such high urine volume is not achievable and therefore complementary pharmacological therapy was needed.
Sodium diet restriction (<100 mEq/day): diminishes cystine excretionProtein diet restriction (0,8–1 g/kg/day): diminishes cystine productionUrine alkalinization: enhances cystine solubility in a pH higher than 7 or 7,5; we preferentially usepotassium citrate (upto 3 to 4 mEq/kg/day in 4 separate intakes). Sodium bicarbonate should be avoided as a sodium overload nmay occur leading to higher cystine excretion (except for hyperkalemia cases). In selected cases, acetazolamide may be associated. Metabolic acidosis, however, must be monitored.Drugs containing thiol: contain sulphydryl groups that reduce disulphide bonds to protein molecules which composes cystine crystals enhancing their solubility. Main examples in this category are:
D-penicilamine: high severe side effects rate including aplastic anemia
Tiopronin: fair results in some clinical cases, but similar poor safety profile as D-penicilamina
Captopryl: disulphide bonds captopryl-cystein are more soluble than cystine; however, the recommended therapeutic dose may reach 150 mg/day, leading to intolerable hypotensive side effect. Dose must be titrated to a maximum clinically acceptable level.
Periodical monitoring of cystine daily excretion is recommended.Although several pharmacological agents are available for clinical treatment of cystinuria, many patients maintain calculi formation and demand multiple surgical interventions.
Multiple interventions and repeated inefficient ESWL sessions may explain the progressive decrease in renal function in many of these patients, although kidney transplant is rarely needed. If this is the case, however, disease does not recur since the graft normally performs cystine transportation.
Still in experimental phase, the ester dimetil L-cystine inhibits crystal formation and may be an important addition to the therapeutic armamentarium against this devastating disease.
clinicalCASEedition: may and juneElaine Bronzatto, Daniel SilvaDivision of Urology - UNICAMP

References:
Palacin, M, Goodyer, P et al. Cystinuria. In: The Metabolic and Molecular Basis of Inherited Disease, 8th Ed, Scriver, CR, Beaudet, AL, Sly, WS, Valle, D (Eds), McGraw-Hill, New York 2001. p.4909
Mattoo A, Goldfarb DS. Cystinuria. Semin Nephrol 2008; 28:181.
Tiselius HG. New horizons in the management of patients with cystinuria. Curr Opin Urol 2010; 20:169.
Copelovitch L. Urolithiasis in children. Pediatr Clin North Am 2012 Aug; 59 (4): 881-96
clinicalCASEedition: may and juneElaine Bronzatto, Daniel SilvaDivision of Urology - UNICAMP

editon: may and june 2013
Wilmar Azal Neto, Tomas Moretti, Antonio Gugliota, Daniel Silva
Division of Urology - Unicamp
NON PALPABLE TESTIS: DIAGNOSIS AND MANAGEMENT
learningby image

learningby imageediton: may and june 2013Wilmar Azal Neto, Tomas Moretti, Antonio Gugliota, Daniel SilvaDivision of Urology - Unicamp
CLINICAL BACKGROUND
PHYSICAL EXAM
MANAGEMENT
Eight years-old male presents with an absent right testicle in scrotum since he was born, with no further complains or associated diseases.
Topic left testis. Non palpable right testis (scrotum, inguinal region, perineum).
Patient underwent diagnostic abdominal laparoscopy (Figure 1 and Vídeo 1)
Figure 1 -
A) Trocars positioning for laparoscopic approach B) Intraoperative view, right testicle is visualized near internal ring (red arrow) and vas deferens (yellow arrow). Spermatic cord dissection was performed laparoscopically, followed by right inguinotomy and right orchidopexy in inguinal canal.
Patient was discharged in the first post operative day. One week follow up was uneventful. A novel surgical approach to deliver the right testis to the scrotum is programmed in 6 months.
Follow up
Comment
Non palpable testis incidence in newborns is estimated to be 1 to 4%. Testis may be either cryptorchidic or ectopic. The exact cause is unknown, but assumed risk factors include low birth weight, low gestational age and genetic alterations.
Eighty per cent of crytorchidic testis are palpable somewhere else other than the scrotum and in 60% of cases testis abscence is unilateral. Abdominal laparoscopic exploration is the gold standard and should be performed within 6 months to 1 year of age. Hormonal therapy is controversial and questioned by many authors.
Whenever a sole testicle is found, as in the presented case, the distance separating the testis from the inner ring will determine the best approach.
Technical oiptions are laparoscopic orchidopexia or Fowler Stephens technique in one or two-stage fashion (Distances over 2,5cm between testis and inner ring are more susceptible to need a two-stage approach). In long term follow up, esthetical issues are avoided with testis preservation; there is a 25% chance of sperm count reduction. Malignancy risk may be diminished by 2 to 3 times.
Videolaparoscopia - Criptorquidia http://www.youtube.com/urovirt

edition: may and june 2013
Olivier Traxer e Alexandre Thomas
Department od Urology Academic Hospital of Tenon, University Pierre and
Marie Curie, Paris, France, and University Hospital of Liège, Liège, Belgium
J Urol 2013 Feb;189(2):580-4.
PROSPECTIVE EVALUATION AND CLASSIFICATION OF URETERAL WALL INJURIES RESULTING FROM INSERTION OF A URETERAL ACCESS SHEATH DURING RETROGRADE INTRARENAL SURGERY
newTECHNOLOGIES
edition: may and june 2013Olivier Traxer e Alexandre ThomasDepartment od Urology Academic Hospital of Tenon, University Pierre and Marie Curie, Paris, France, and University Hospital of Liège, Liège, Belgium J Urol 2013 Feb;189(2):580-4.
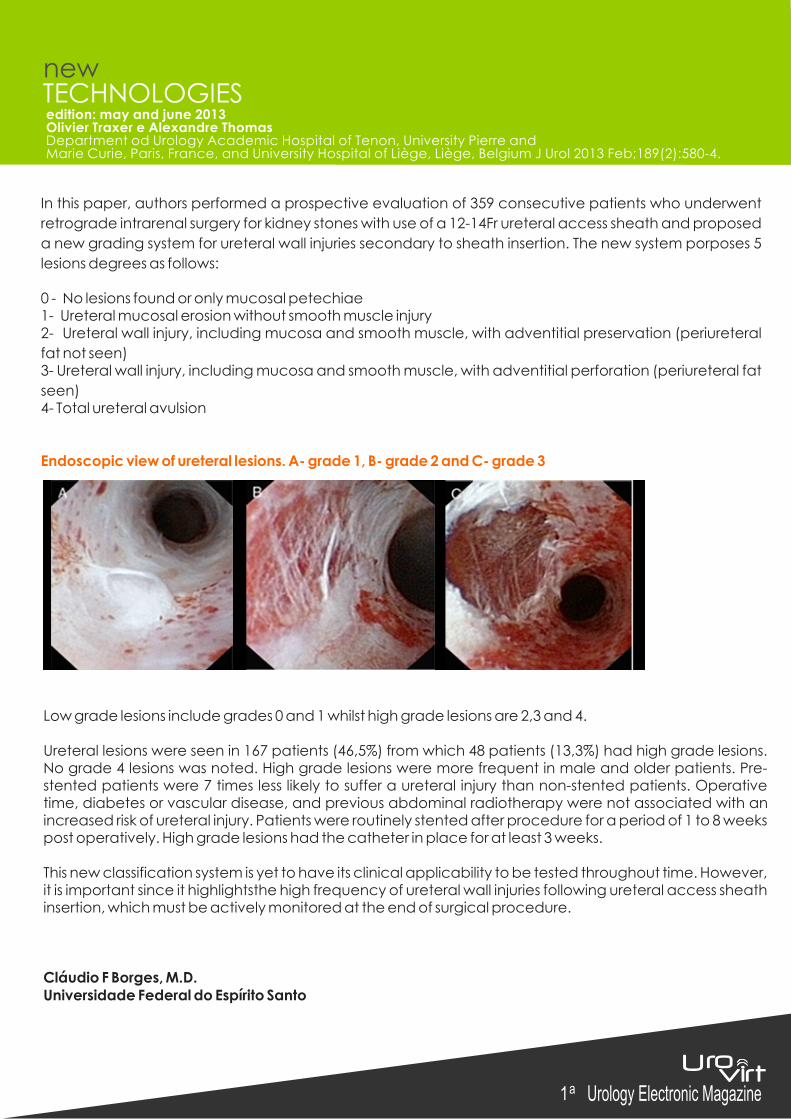
In this paper, authors performed a prospective evaluation of 359 consecutive patients who underwent
retrograde intrarenal surgery for kidney stones with use of a 12-14Fr ureteral access sheath and proposed
a new grading system for ureteral wall injuries secondary to sheath insertion. The new system porposes 5
lesions degrees as follows:
0 - No lesions found or only mucosal petechiae1- Ureteral mucosal erosion without smooth muscle injury2- Ureteral wall injury, including mucosa and smooth muscle, with adventitial preservation (periureteral
fat not seen)3- Ureteral wall injury, including mucosa and smooth muscle, with adventitial perforation (periureteral fat
seen)4- Total ureteral avulsion
Endoscopic view of ureteral lesions. A- grade 1, B- grade 2 and C- grade 3
Low grade lesions include grades 0 and 1 whilst high grade lesions are 2,3 and 4.
Ureteral lesions were seen in 167 patients (46,5%) from which 48 patients (13,3%) had high grade lesions. No grade 4 lesions was noted. High grade lesions were more frequent in male and older patients. Pre-stented patients were 7 times less likely to suffer a ureteral injury than non-stented patients. Operative time, diabetes or vascular disease, and previous abdominal radiotherapy were not associated with an increased risk of ureteral injury. Patients were routinely stented after procedure for a period of 1 to 8 weeks post operatively. High grade lesions had the catheter in place for at least 3 weeks.
This new classification system is yet to have its clinical applicability to be tested throughout time. However, it is important since it highlightsthe high frequency of ureteral wall injuries following ureteral access sheath insertion, which must be actively monitored at the end of surgical procedure.
Cláudio F Borges, M.D.Universidade Federal do Espírito Santo
newTECHNOLOGIES

urology NEWS
edition: may and june 2013
V Curso Urodinâmica Sem MistérioEscola de Urodinâmica da UNICAMP
Nos dias 22 e 23 de Março ocorreu o 5o curso “Urodinâmica Sem Mistério”, sob a coordenação do Prof. Carlos D’Ancona e com o apoio da Dynamed, nas dependências da Casa do Professor Visitante (CPV) e Núcleo de Cirurgia Experimental, no campus da UNICAMP. Foram apresentados os mais variados temas em urodinâmica, desde orientações básicas de sondagem, preparo e calibragem do aparelho, até o aprendizado de interpretação de gráficos de alta complexidade, videourodinâmica e identificação de artefatos nos traçados. O já tradicional curso repetiu o sucesso de anos anteriores, tendo suas vagas esgotadas e contando com participação de estrangeiros e de diversos estados do Brasil. A integração social ficou por conta de um jantar de confraternização e do tradicional almoço do sábado.

Defesa de DoutoradoMARIA CAROLINA PERISINOTTO
No dia 26 de fevereiro de 2013, Maria Carolina Perisinotto defendeu Tese de Doutorado, sob orientação do Prof. Carlos Arturo Levi D’Ancona, com estudo sobre “Efeitos da Eletroestimulação do Nervo Tibial Posterior nos Sintomas do Trato Urinário Inferior e Impacto na Qualidade de Vida em Pacientes com Doença de Parkinson” tendo sido aprovada por unanimidade .
RESUMO
Introdução:A doença de Parkinson é uma doença neurológica degenerativa de causa desconhecida que leva a alterações motoras em decorrência da diminuição dos neurotransmissores de dopamina na substância nigraestriatal. Distúrbios miccionais acometem de 37% a 70% dos pacientes com esta doença. A eletroestimulação do nervo tibial posterior é uma opção no tratamento dos sintomas do trato urinário inferior.
Objetivo:Avaliar a eficácia da referida eletroestimulação na sintomatologia do trato urinário inferior em pacientes com doença de Parkinson.
Métodos:A metodologia utilizada foi o estudo controlado randomizado, pela qual foram 96 pacientes com diagnóstico de doença de Parkinson com queixas de sintomas do trato urinário inferior, os quais foram alocados em dois grupos: grupo tratamento e grupo sham. Todos os pacientes foram avaliados através de escalas específicas para a doença de Parkinson, como a Unified Parkinson's Diseases Rating Scale, nos quais preencheram os questionários de qualidade de vida, de incontinência urinária e de bexiga hiperativa, através dos quais foi realizado o estudo urodinâmico. Todas as avaliações foram realizadas pré e pós-tratamento e a técnica utilizada foi a eletroestimulação do nervo tibial posterior durante dez sessões, duas vezes por semana com duração de 30 minutos cada sessão. O grupo de tratamento realizou esta eletroestimulação e o outro grupo, o procedimento sham.
Resultados:Os resultados obtidos ao final do tratamento foi que o grupo de tratamento relatou melhora significativa nos sintomas urinários de urgência e noctúria em comparação ao grupo sham. Urgência (p=0,0047), entre os grupos (100,0% grupo de tratamento, 12,5% grupo sham) e noctúria no grupo de tratamento entre os tempos pré e pós (p=0,0156) (4,0 pré – 2,0 pós). Na análise da qualidade de vida, ocorreu uma melhora significativa no score total do questionário International Consultation on Incontinence Questionnaire no grupo de tratamento entre os tempos pré e pós (p=0,0191) (7,0 pré – 4,0 pós), e n o q u e s t i o n á r i o O v e r a c t i v e B l a d d e r Questionnaire no mesmo grupo entre os tempos (p=0,0144) (29,0 pré – 21,5 pós). No estudo urodinâmico, houve melhora significativa no grupo de tratamento entre o tempo pré e pós no primeiro desejo (mediana 150 pré -185 ml pós) (p=0.0056) e volume urgência (mediana 200 pré -285 ml pós) (p= 0.0014).
Conclusão:O tratamento com a eletroestimulação do nervo tibial posterior se mostrou uma técnica capaz de melhoras na sintomatologia do trato urinário inferior em pacientes com doença de Parkinson, tais como a redução da urgência e da noctúria,
urology NEWS
edition: may and june 2013

may and june 2013 edition
www.urovirt.org.br
Realization:Sponsors:









![[PPT]Sagital View of the eye · Web view2017/10/31 · Gambaranklinik: - Gejalasubyektif : visushilang-timbul (amourosisfugaks) - Gejalaobyektif : Pupil refleks , anisokoria Funduskopi:](https://static.fdocuments.in/doc/165x107/5ac3152a7f8b9a57528bb29a/pptsagital-view-of-the-eye-view20171031gambaranklinik-gejalasubyektif-visushilang-timbul.jpg)