Eating disorders mothers and their children: a systematic ... · eating behaviours, and might...
19
REVIEW ARTICLE Eating disorders mothers and their children: a systematic review of the literature Maria Giulia Martini 1,2 & Manuela Barona-Martinez 1 & Nadia Micali 1,3,4 Received: 30 July 2019 /Accepted: 7 January 2020 # The Author(s) 2020 Abstract To provide an overview of the impact of maternal eating disorders (ED) on child development in a number of domains including feeding and eating behaviour, neuropsychological profile and cognitive development, psychopathology and temperament. PubMed, Embase and PsychInfo were searched for studies exploring the impact of maternal ED on children between January 1980 and September 2018. Initial search yielded 569 studies. After exclusion, 32 studies were reviewed. Overall, available evidence shows that children of mothers with ED are at increased risk of disturbances in several domains. They exhibit more difficulties in feeding and eating behaviours, display more psychopathological and socio-emotional difficulties, and they are more likely to be described as having a difficult temperament. Maternal ED have an impact on child psychological, cognitive and eating behaviours, and might affect the development of ED in the offspring. Future research should focus on resilience and on which protective factors might lead to positive outcomes. These factors can be then used as therapeutic and preventative targets. Keywords Eating disorder . Intergenerational effect . Children . Mothers Introduction Eating disorders (ED) are mental health disorders characterised by severe disturbances in eating behaviour that significantly impact an individual’ s emotional, psychosocial and physical well-being (Bannatyne et al. 2018). Current diagnostic classifi- cations of ED include anorexia nervosa (AN), bulimia nervosa (BN) and binge-eating disorder (BED) as full threshold ED. ED typically affect women of reproductive age (Easter et al. 2014). Early childhood is a crucial time for the development of the mother–child relationship. It is during this time that children develop psychosocially, engage in social learning and express their temperament—which is a biological tendency within each child but it is shaped by complex interactions between genetic, biological and environmental factors (Shiner et al. 2012). Risk for developmental problems in children of women with psychiatric disorder has been well documented in litera- ture and several aspects of children’ s development can be affected, including their physical, cognitive, social, emotional and behavioural development (Ramchandani and Stein 2003). Fewer studies are available regarding the impact of ED on child development. However, the literature available suggests that children of mothers with ED have an increased risk for negative develop- mental outcomes, including cognitive, social and emotional disturbances (Patel et al. 2002). Research has shown that chil- dren of mothers with ED are more likely to develop an emo- tional disorder at the age of 7 and 10 (Micali et al. 2014a), they are more likely to show neurobehavioural dysregulation early after birth and poorer language and motor development at 1 year (Barona et al. 2017). Furthermore, there is evidence that children of mothers with ED are more likely to develop ED themselves (Kothari et al. 2013). Family and twin studies have consistently demonstrated that ED have a strong genetic component (Mazzeo et al. * Maria Giulia Martini [email protected]; [email protected] 1 Behavioural and Brain Sciences Unit, Institute of Child Health, University College London, 4th Floor, 30 Guilford Street, London WC1N 1EH, UK 2 South London and Maudsley, NHS Foundation Trust, London, UK 3 Department of Psychiatry, University of Geneva, Geneva, Switzerland 4 Child and Adolescent Psychiatry Division, Department of Child and Adolescent Health, University Hospital Geneva, Geneva, Switzerland Archives of Women's Mental Health https://doi.org/10.1007/s00737-020-01019-x /Published online: 14 January 2020 (2020) 23:449–467
Transcript of Eating disorders mothers and their children: a systematic ... · eating behaviours, and might...

REVIEW ARTICLE
Eating disorders mothers and their children: a systematicreview of the literature
Maria Giulia Martini1,2 & Manuela Barona-Martinez1 & Nadia Micali1,3,4
Received: 30 July 2019 /Accepted: 7 January 2020# The Author(s) 2020
AbstractTo provide an overview of the impact of maternal eating disorders (ED) on child development in a number of domains includingfeeding and eating behaviour, neuropsychological profile and cognitive development, psychopathology and temperament.PubMed, Embase and PsychInfo were searched for studies exploring the impact of maternal ED on children between January1980 and September 2018. Initial search yielded 569 studies. After exclusion, 32 studies were reviewed. Overall, availableevidence shows that children of mothers with ED are at increased risk of disturbances in several domains. They exhibit moredifficulties in feeding and eating behaviours, display more psychopathological and socio-emotional difficulties, and they aremore likely to be described as having a difficult temperament. Maternal ED have an impact on child psychological, cognitive andeating behaviours, and might affect the development of ED in the offspring. Future research should focus on resilience and onwhich protective factors might lead to positive outcomes. These factors can be then used as therapeutic and preventative targets.
Keywords Eating disorder . Intergenerational effect . Children .Mothers
Introduction
Eating disorders (ED) are mental health disorders characterisedby severe disturbances in eating behaviour that significantlyimpact an individual’s emotional, psychosocial and physicalwell-being (Bannatyne et al. 2018). Current diagnostic classifi-cations of ED include anorexia nervosa (AN), bulimia nervosa(BN) and binge-eating disorder (BED) as full threshold ED. EDtypically affect women of reproductive age (Easter et al. 2014).
Early childhood is a crucial time for the development of themother–child relationship. It is during this time that children
develop psychosocially, engage in social learning and expresstheir temperament—which is a biological tendency within eachchild but it is shaped by complex interactions between genetic,biological and environmental factors (Shiner et al. 2012).
Risk for developmental problems in children of womenwith psychiatric disorder has been well documented in litera-ture and several aspects of children’s development can beaffected, including their physical, cognitive, social, emotionaland behavioural development (Ramchandani and Stein 2003).Fewer studies are available regarding the impact of ED onchild development.
However, the literature available suggests that children ofmothers with ED have an increased risk for negative develop-mental outcomes, including cognitive, social and emotionaldisturbances (Patel et al. 2002). Research has shown that chil-dren of mothers with ED are more likely to develop an emo-tional disorder at the age of 7 and 10 (Micali et al. 2014a), theyare more likely to show neurobehavioural dysregulation earlyafter birth and poorer language and motor development at1 year (Barona et al. 2017).
Furthermore, there is evidence that children of motherswith ED are more likely to develop ED themselves (Kothariet al. 2013).
Family and twin studies have consistently demonstratedthat ED have a strong genetic component (Mazzeo et al.
* Maria Giulia [email protected]; [email protected]
1 Behavioural and Brain Sciences Unit, Institute of Child Health,University College London, 4th Floor, 30 Guilford Street,London WC1N 1EH, UK
2 South London and Maudsley, NHS Foundation Trust, London, UK3 Department of Psychiatry, University of Geneva,
Geneva, Switzerland4 Child and Adolescent Psychiatry Division, Department of Child and
Adolescent Health, University Hospital Geneva,Geneva, Switzerland
Archives of Women's Mental Healthhttps://doi.org/10.1007/s00737-020-01019-x
/Published online: 14 January 2020
(2020) 23:449–467

2005); however, the environment is likely to play a crucial rolein the expression of underlying genetic predispositions.
In 2005, Bulik et al. (2005) proposed a cycle of risk modelfor the development of AN, whereby the maternal effect ofAN on their children via perinatal complications ishypothesised as being influenced by environmental factors,genetic factors and environmental factors that are highly in-fluenced by maternal genotype (i.e. pregnancy nutrition,weight gain in utero, appearance focus and restrictive eatingduring childhood/adolescence). In 2009, Micali and Treasuresuggested a risk model for the impact of maternal ED on childdevelopment that embraces all ED focusing on in utero mech-anisms. In particular, the model explained the effect of a ma-ternal ED in pregnancy on the foetus via nutritional factors(including protein deficiency, low folate and low iron intake)and comorbid psychopathology (i.e. comorbid anxiety anddepression and in turn via increased glucocorticoids andcorticotrophin-releasing hormone) which both could lead toobstetric complications (Micali and Treasure 2009). The in-fluence of parental ED on child phenotype might likely be theresult of a complex interplay between genetic (maternal andchild) and environmental factors.
Understanding the mechanisms leading from maternal EDto adverse child development could help to determine bothrisk and protective factors that could be potentially targetedfor intervention.
To date, only one recent systematic review has been pub-lished on this topic in the last several years and the authors didfocus only on the most recent findings (2015 onwards) (Watsonet al. 2018). Previous reviews focusing on children of motherswith ED include (Patel et al. 2002) and (Park et al. 2003). Nosystematic reviews have been carried out so far covering theperiod between 2003 and 2015 and many relevant population-based studies have been carried out over this period.
The purpose of our paper is to provide an overview of theimpact of maternal ED on child development. Particularly, thisreview will focus on effects on developmental aspects, acrossthe spectrum of feeding and eating behaviour, neuropsycho-logical profile and cognitive development, psychopathologyand temperament.
Methods and materials
Data source
A systematic and comprehensive search of databases, includ-ing PsychInfo, Embase and Medline, was carried out for stud-ies published between January 1980 and September 2018. Thesearch was performed using the following mesh terms andkeywords: (‘maternal eating disorders’ or ‘maternal anorexianervosa’ or ‘maternal bulimia nervosa’ or ‘maternal bingeeating disorder’ or ‘mothers with eating disorders’ or ‘mothers
with anorexia nervosa’ or ‘mothers with bulimia nervosa’ or‘mothers with binge eating disorder’) and (‘child develop-ment’ or ‘child language development’ or ‘child feeding’ or‘child cognitive development’ or ‘child temperament’ or‘child psychopathology’).
Study selection
Inclusion criteria for the studies included (1) exposure(mothers) diagnosed with any ED (i.e. AN, BN and BED)either active or past, (2) the outcome was a measure of childdevelopment assessed from birth up until 12 years of age, (3)studies published in English and (4) primary studies.
Exclusion criteria for the studies included the following:studies were excluded if the aims were to investigate childeating pathology. Papers were also excluded if an interventionwas assessed such as video-feedback interactional treatment.
Quality assessment and data extraction
Two authors (M.G.M. and M.B.) independently screened, ex-tracted and cross-checked the data based on a priori exclusionand inclusion criteria. The quality of the final studies was alsoindependently checked by both authors using the Newcastle–Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses (Table 1). The abovescale includes case–control and cohort studies.
For each study, the following data were extracted whenavailable: demographic information, including participantcharacteristics (sample size ad mean age), ED type (AN,BN, BED), ED status (actual vs. recovered); measures usedto certain exposure and outcome. The identified studies inves-tigated a number of different child outcomes. After discussionbetween authors (M.B., M.G.M., N.M.), four domains werediscussed: feeding/eating, neuropsychological profile/cognitive development, psychopathology and temperament.However, a range of studies investigated more than one out-come and were included in more than one domain (Table 1).
Results
Search findings
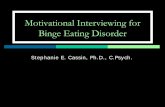
A PRISMA flow diagram presents all phases of the review(Fig. 1) (Moher et al. 2009).
Most studies used case–control (n = 17) and cohort design(n = 16) and one early study used an uncontrolled design. Themajority of studies were published within the last decade (n =25) with 59% published within the last 5 years (2013–2018).
Studies included measured various aspects of child devel-opment: feeding/eating (n = 17), cognitive development/neuropsychological profile (n = 6), psychopathology (n = 12)
M. G. Martini et al.450

Table1
Studiesexploringtheim
pactof
maternalE
atingDisorder(ED)on
child
developm
ent
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
FEEDIN
G/EATIN
G1 Feeding/Eating
Steinetal.1994
Case–control
Totaln
=58
mothers
Cases
recruitedfrom
community
n=34;m
eanage28.3
12EDNOS,
6BNand16
subthreshold
Health
ycontrolsrecruitedfrom
community
n=24;m
eanage29.0
Exposure:MaternalE
D(Clinical
InterviewthroughEating
DisorderExamination—
EDE)
Outcome:infant
developm
ent:
BayleyScales
feedingand
grow
th:T
annerand
Whitehouse’sspecification
▪Negativeexpressedem
otionwas
morefrequent
amongthecase
motherscomparedto
controls
during
mealtimes
butn
otduring
play
▪Motherswith
EDwerelessfacilitatingduring
both
mealtimes
andplay,had
significantly
more
conflictw
ithinfants
▪Caseinfantswereratedas
less
happythan
the
controlsduring
both
mealtimeandplay
9/9
2 Feeding/Eating/Temperament
Evans
andleGrange1995
Case–control
Totaln
=20
Cases,A
NandBN
N=10,m
eanage=36.0(7.02)
Health
ycontrols
N=10,m
eanage=35.4(4.12)
Exposure:MaternalE
D(Clinical
InterviewDSM
III-RAPA
)Outcome:body
shape
questio
nnaire;sem
i-structured
interviewon
feeding
anddevelopm
ent
▪Positive
correlationfoundinbothcase
andcontrol
groups
betweenmothers’satisfactionwith
their
body
size
andtheirchild
ren’ssatisfactionwith
theirow
nweightand
shape
▪Mothersintheclinicalgroupreported
experiencing
emotionalp
roblem
swhenbreastfeedingtheir
child
ren
▪Infantsin
theclinicalgroupwereschedulefed—
thisrigidadherencecaused
someconfusionand
anxietyformotherswhentheirinfantsdisplayed
signsofhungeroutsidetherecommendedfeeding
times
▪Halfthechild
renof
EDmothersweredescribedas
displaying
difficultiessuch
ashyperactivity,
avoidant
behaviour,enuresis,insecure
attachment,depression,fears,personality
problems,stuttering,violent
temperamentand
oppositio
nald
efiant
behaviour
8/9
3 Feeding/Eating/Temperament
Agras
etal.1999
Case–control
Totaln
=194
Cases
N=41,m
eanage=32.1(4.4)
AN=2,BN=17,B
ED=22
Health
ycontrols
N=153,meanage32.9(3.8)
Exposure:maternalE
D(Clinical
InterviewDSM
III-R+Eating
DisorderInventory—
EDI)
Outcome:Infant
FeedingReport
(IFR
);Su
ckom
eter;C
hildren’s
Behaviour
Questionnaire
▪Fem
aleinfantsof
EDmotherssucked
morerapidly
than
otherinfants,butn
odifferencesin
caloric
intake
atthesefeedings
▪EDmothersbottlefedtheirdaughtersforamean
timeof
33.2
monthscomparedwith
infantsof
NEDmotherswith
23.6
months
▪EDmothersconsidered
theirfemalechild
rento
have
moredifficulty
inweaning
from
thebottle
(but
notfrom
thebreast)
than
NEDmothers
▪Infantsof
EDmotherswerereported
todawdle
morewhileeatin
gcomparedto
child
renof
NED
group
▪EDmothersreported
theirdaughtersas
vomiting
morefrequently
than
theirsons
(opposite
effect
forNEDmothers)
▪EDmothersreported
higher
concernfortheir
daughter’sweightthanNEDmothers
8/9
Eating disorders mothers and their children: a systematic review of the literature 451

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
▪Significant
maineffectfortheEDgroupforusing
food
asnon-nutritive
purposes
▪Significanteffectof
EDmothersreportingthey
fed
theirchildrenon
alessregularschedulethan
NED
mothers
▪Childrenof
motherswith
EDreported
asdemonstratingmorenegativ
eaffect(sadness,
crying,irritability)
than
childrenof
NEDmothers
4 Feeding/Eating
Steinetal.1999
Case–control
Totaln
=58
Cases
N=34,m
eanage=28.3
Health
ycontrols
N=24,m
eanage=29
Exposure:maternalE
D(Clinical
InterviewDSM
IIIR)
Outcome:Five-Point
Conflict/H
armonyScale
▪The
mostfrequentantecedenttoconflictw
asthe
mother’sconcernaboutthe
mannerof
eating;
disagreemento
verwho
fedtheinfant
andfood
refusal
▪Mothersin
theclinicalgrouponly
acknow
ledged
theinfant’ssignalsinathirdof
casescomparedto
over
ahalfin
theNEDmothersgroup
5/9
5 Feeding/Eating
Temperament
Waugh
andBulik
1999
Case–control
Totaln
=20
mothers
N=10,m
eanage30.1(3.1)
PastAN=6,pastBN=7
Health
ycontrolsrecruitedfrom
community
n=10,m
eanage30.8(3.6)
Exposure:maternalE
D(Clinical
InterviewDSM
III-R)
Outcome:To
ddlerTemperament
Scale(TTS);M
ealtime
Observatio
nSchedule(M
OS);
Food
Diary
▪Childrenof
wom
enwith
eatingdisordershad
significantly
lowerbirthweightsandlengthsthan
controlchildren
▪Nodifferencesobserved
inchildhood
temperament
ormothers’satisfactionwith
child
ren’s
appearance
▪Motherswith
EDmadesignificantly
fewerpositive
eatingcomments
8/9
6 Feeding/Eating
WhelanandCooper2000
Case–control
Totaln
=128mothers
Clin
icalgroup(any
EDdisorder)
Childrensplit
inthreegroups:
▪Clin
ical—feedingproblems
(1):42
▪Clin
ical—disturbedcomparisons
(2):79
▪Control:2
9
Exposure:maternalcurrentandpast
affectivedisorder
andcurrent
andpastED(EatingDisorder
Examination—
EDE+Clin
ical
InterviewDSM
IV)
Outcome:Sh
yness;Preschool
Behaviour
Checklist(PB
CL);
Behaviour
Screening
Questionnaire
(BSQ
);Feeding
ProblemsandEatingDisorders
InterviewSchedule
▪Childrenin
thefeedingproblem
groupwererated
assignificantly
moredisturbedthan
thecontrol
group(feeding
disturbances
such
asrefusal,
faddinessandspitting)
▪Severity
ofchild
disturbancewas
notrelated
tothe
relatio
nshipbetweenfeedingproblemsand
maternalE
D
8/9
7 Feeding/Eating
BlissettandMeyer
2006
Case–control
Totaln
=114mothers
and114child
ren
Meanmaternalage
33(5.5)
Meanchild
age29
months(13.77)
Exposure:MaternalE
D(Eating
DisorderInventory2—
EDE-2
questio
nnaire)
Outcome:Child
Feeding
Assessm
entQ
uestionnaire
(CFA
Q);Young
Schema
Questionnaire
▪Eatingpsychopathologydidnotexplain
mealtime
negativ
ityin
boys
▪Eatingpsychopathologyfailedtoexplainmealtime
negativ
ityin
girls
Food
refusal
▪Eatingpsychopathologyfailedto
explainfood
refusalinboys
Eatingpsychopathologyaddedsignificantly
tothe
variance
explainedin
food
refusalo
fgirls
6/9
8 Feeding/Eating
Cohort
Totaln
=12,050
ALSPAC
Exposure:MaternalE
D(self-report)
▪Motherswith
ahistoryof
EDweremorelik
elyto
startbreastfeeding
than
controls(83%
with
76%)
7/9
M. G. Martini et al.452

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
Micalietal.2009
Cases
N=441,AN=247andBN=194
Meanage,AN=29.1(5.0),
BN=28.3(4.6)
Health
ycontrols
N=10,461,m
eanage=28.2(4.8)
Outcome:feedingquestio
nnaires;
health
records
▪Alsoless
likelyto
stop
breastfeedingduring
the
firsty
earof
infant
life
▪Those
with
BNweremorelikelytocontinue
breast
feeding
Infant
feeding
▪ANmothersreported
moreearlyonsetp
ersistent
feedingdifficultiesin
alld
omains
except
refusal
totake
solid
s▪Infantsof
motherswith
BNdiffered
intherateof
refusaltotake
solid
sfrom
thoseANmothersin
theratesof
beingunsatisfied/hungryafterfeeding
9 Psychopathology/
Feeding/Eating
Reba-Harrelson
etal.2010
Cohort
Totaln
=13,006
MoB
a(N
orwegianmothersand
child
cohortstudy)
Cases
N=479,BED=634,BN=98,
AN=17
Health
ycontrols
N=12,257
Exposure:maternalE
D(self-report)
Outcome:Child
Feeding
Questionnaire;C
hild
Behaviour
Checklist(CBCL);Infant
ToddlerSo
cialEmotional
Assessm
ent(ITSE
A)
▪Motherswith
BNandBEDreported
higher
levels
ofdisordered
eatin
gbehavioursin
theirchild
ren
than
controls
▪Theyalso
reported
higher
levelsof
anxiety
symptom
sin
theirchildren
▪Motherswith
BNreported
higher
levelsof
OCD
symptom
sin
theirchildren
▪Maternally
reported
restrictivefeedingwas
significantly
associated
with
child
disordered
eatin
gdifficulties
8/9
10 Feeding/Temperament
Micalietal.2011
Cohort
Totaln
=10,902
ALSPAC
Cases
N=441,AN=166,BN=194,AN
+BN=81;m
eanage=28.7
(4.8)
Health
ycontrols
n=10,461;m
eanage=28.2(4.8)
Exposure:maternalE
D(self-report),maternal
depression,m
aternalanxiety
Outcome:maternalreports;C
arey
Infant
TemperamentS
cale;
DenverDevelopmentalS
cale
▪Maternallifetim
eEDpredictedfeedingdifficulties
at1month
and6months
▪EDsymptom
sin
pregnancyfoundto
predict
feedingdifficultiesat1month
▪Child‘difficult’
temperamentscorewas
associated
with
latefeedingdifficulties
8/9
11 Feeding/Eating
Easteretal.2013
Cohort
Totaln
=9423
ALSPAC
Cases
N=387,AN=140,mean
age=29.7(5.2),BN=170,
meanage=28.3(4.6),
AN+BN=71,m
eanage=29.6
(4.6)
Health
ycontrols
N=9037,m
eanage=28.8(4.8)
Exposure:maternalE
D(self-reported)
Outcome:Fo
odFrequency
Questionnaire
(FFQ
s);
nutritionalintake
▪Childrenofmotherswith
all3
EDgroups
(AN,B
NandAN+BN)hadhigher
scores
onthehealth
conscious/vegetarian
dietarypattern
across
all4
timepoints:3
,4,7
and9years*
▪Differences
persistedin
maternalA
NandBN
groups
afteradjustments—child
renscored
lower
onthetraditionaldietarypattern
across
all4
time
points
▪Trendsshow
edhigher
energy
intake
ofchild
ren
with
motherswith
BNandAN+BN
▪Childrenwith
motherswith
BNhadhigher
starch
intake
8/9
12 Feeding/Eating
Hoffm
anetal.2014
Cohort
Totaln
=50
Recruitedfrom
community
Cases
Exposure:maternalE
D(clin
ical
interviewSC
ID-I)
Outcome:anthropometric
data/in
fant
feedingstyle
▪Motherswith
historiesof
eatingdisordersscored
significantly
loweron
therestrictivefeedingstyle
subscalethan
controlm
others
7/9
Eating disorders mothers and their children: a systematic review of the literature 453

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
N=25;A
N=13;B
N=13;
EDNOS=2,meanage=32.7
(4.61)
Health
ycontrols=25,m
eanage
29.68(1.99)
questio
nnaire/Toddler
Diet
Questionnaire/EDE-Q
/BDI/BAI
▪Nosignificantdifferences
betweengroups
inchild
diet(i.e.durationof
breastfeeding,ageatsolid
food
introduction,daily
numberof
snacks
and
mealsetc)
▪Motherswith
eatin
gdisorder
historiesweremore
likelyto
reporttaking
arestrictivespecial
approach
tofeedingsuch
aslim
iting
processed
foodsor
feedingorganicfoodsonly
13 Feeding/Eating
deBarse
etal.2015
Cohort
Totaln
=4851
GenerationRstudy
Cases
N=415,meanage=30.8(5.0)
AN=121,BN=189,
AN+BN=105
Health
ycontrols
N=4436,m
eanage=30.8(4.8)
Exposure:maternalE
D(self-report
questio
nnaire)
Outcome:Child
Feeding
Questionnaire
(CFQ
);Child
EatingBehaviour
Questionnaire
(CEBQ);Children’sbody
mass
index
▪Motherswith
ahistoryof
EDused
lesspressureto
eatthanmotherswith
out
▪Motherswith
ahistoryof
ANwerelik
elyto
use
lowlevelsof
pressure
toeat
▪Childrenof
motherswith
anEDhadhigher
levels
ofem
otionalo
vereatingthan
controls—thiswas
strongestw
ithmotherswith
ahistoryof
AN
8/9
14 Feeding/Eating
Torgersenetal.2015
Cohort
Totaln
=49,045,m
eanage=29.6
(4.6)
MoB
a(N
orwegianmothersand
child
cohortstudy)
Cases
N=3013
AN=44,B
N=436,BED=2475,
EDNOS–
P=58
Health
ycontrols
N=46,032
Exposure:maternalE
D(Self-reported)questio
nnaire
Outcome:InfantDietQ
uestionnaire
4
▪Percentages
ofmothersbreastfeedingat6months:
BN(79%
),BED(76%
),EDNOS-P(59%
),AN
(58%
),no-ED(82%
)▪Infantsof
motherswith
BNhadsignificantly
lower
odds
ofbeingin
thehomem
adetraditional
food
classthan
thecommercial
jarred
baby
food
class
▪Infantsof
motherswith
BEDweresignificantly
lesslik
elytobe
inthehomem
adevegetarian
food
classthan
thecommercial
jarred
baby
food
7/9
15 Feeding/Eating
Saltzman
etal.2016
Case–control
Totaln
=260
Cases
N=36
motherswith
BED
Health
ycontrols
N=224
Exposure:frequencyof
BED
behavioursthroughself-report
questio
nnaire
EatingDisorder
Diagnostic
Scale(EDDS)
Exposure:Children’sNegative
Emotions
Scale;Com
prehensive
FeedingPractices
Questionnaire;
Child
BMI
▪MaternalB
EDpredicteduseof
more
nonresponsivefeedingpractices
(e.g.E
motion
Regulation,Restrictio
nforHealth
,Pressureto
Eat,and
Food
asRew
ard)
▪MaternalB
EDwas
associated
with
greateruseof
distress
responses,which
indirectly
predicted
higher
child
BMIpercentilethroughFo
odas
Rew
ardfeedingpractices
5/9
16 Feeding/Eating
Nguyenetal.2017
Cohort
Totaln
=6196
GenerationRstudy
Cases
N=591
Health
ycontrols
N=5605
Exposure:self-reportq
uestionnaire
Outcome:Fo
odFrequency
Questionnaire
(FFQ
),breastfeedingduration
▪Motherswith
ahistoryof
EDsseem
slightly
less
likelyto
initiatebreastfeeding,although
nolonger
statistically
significantafter
adjustment
▪Atthe
ageof
1year,infantsof
motherswith
ahistoryof
EDshadahigher
dietquality
7/9
17 Feeding/Eating
Martinietal.2018
Case–control
Totaln
=99
Cases
N=53;p
astE
D28,m
ean
age=33.3(5.5);currentE
D25,
meanage=29.0(5.4)
Exposure:clinicalinterview
(SCID
-I)
Outcome:
Infant
FeedingQuestionnaire
(IFQ
)/ParentalModellin
gof
▪Wom
enwith
P-EDandC-EDreported
higher
concerns
abouttheirinfant
being/becoming
overweightcom
paredwith
HC,respectively,at
8weeks
and6monthsand6monthsonly
post
partum
8/9
M. G. Martini et al.454

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
Health
ycontrols
N=46,m
eanage=34.0(3.8)
EatingBehaviours
Scale(PARM)
▪Wom
enwith
P-EDshow
edless
awarenessof
infanthungerandsatietycues
comparedwith
HC
at8weeks
COGNITIV
EDEVELOPM
ENT/NEUROPS
YCHOLOGICALPR
OFILE
1 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
Kotharietal.2014
Cohort
Different
samplesizesweretaken
into
account
Totaln
=982/852
Health
ycontrols:9
37/819
Cases
AN=14;B
N=18;A
N+BN=13
AN=11;B
N=12;A
Nand
BN=10
Exposure:self-reportq
uestionnaire
Outcome:GriffithsDevelopment
Scales;W
echslerPreschooland
Prim
aryScaleof
Intelligence–Revised
Griffithsdevelopm
entscales
▪Childrenof
wom
enwith
alifetim
eof
ANshow
edlower
scores
onthedevelopm
ento
flocomotor
andpersonal–socialdevelopmentthanchildrenof
unexposedmothers
WechslerPreschooland
Prim
aryScaleof
Intelligence–Revised
▪Childrenof
wom
enwith
alifetim
eof
ANshow
edlower
scores
onperformance
subtestsof
geom
etricdesign
andblockdesign
▪Theyalso
show
edlower
scores
onvernaltestsof
comprehension
andsimilarities
Theyalso
show
edlower
verbalIQ
scores
incomparisonto
thecontrols
7/9
2 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
Kotharietal.2013
Cohort
Totaln
=11,088
Cases=446
Meanage=29.17(4.49)
AN=194,BN=171and
AN+BN=81
Health
ycontrols
N=10,642,
meanage=29.10(4.5)
Exposure:maternalE
D(self-report)
questio
nnaire
Outcome:WechslerIntelligence
ScaleforChildren(W
ISC-III);
TestsforEverydayAttentionfor
Children;
CountingSp
anTask;
Stop-SignalP
aradigm
Intelligenceandglobalcognition
▪Childrenof
ANmothersshow
edhigher
full-scale
IQandperformance
IQthan
comparedwith
NED
mothers
▪Childrenof
ANmothersshow
edhigh
picture
arrangem
entscoreson
theWISCsubtestw
hereas
child
renof
BNmothersshow
edlowobject
assemblyscores
Working
mem
ory(W
M)
▪Childrenof
ANmothersshow
edslightly
better
WM
span
scores
afteradjustments
▪Childrenof
AN+BNmothersshow
edbetter
globalWM
scores
7/9
3 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
Koubaaetal.2013
Cohort
Totaln
=112
Cases
N=47;A
N=24;B
N=20;
EDNOS=3,
meanage=29.3(4.6)
Health
ycontrols=65,
meanage30
(3.7)
Exposure:maternalE
D(clin
icalinterview)
Outcome:anthropometric
measurement/M
aternal
Adjustm
entand
Maternal
Attitude
Questionnaire
(MAMA)/Five
toFifteen(FTF)
▪Childrenborn
tomotherswith
EDhadalower
birthweightb
utdisplayedan
earlycatch-up
inweight
▪The
averagehead
circum
ferencewas
foundto
bedelayedup
toatleast1
8monthsof
age
▪Childrenof
motherswith
ANor
BNhad
significantly
higher
FTFscores
than
controls
reflectin
gdifficultiesinlanguage
andsocialskills
8/9
4 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
Kotharietal.2015
Cohort
Totaln
=1128
Cases
N=266
AN–R
=58
AN–B
P=66
BED=72
Exposure:clinical
interview(SCID
)Outcome:So
cialCom
munication
DisordersChecklist(SC
DC);
Diagnostic
Analysisof
Non-VerbalA
ccuracy
Socialcognition
▪Childrenof
wom
enwith
abingingphenotypehad
higher
odds
ofapoor
socialcommunication
▪Those
with
abingingandpurgingphenotypehad
child
renwith
higher
odds
ofhaving
poor
social
communication
8/9
Eating disorders mothers and their children: a systematic review of the literature 455

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
Purge=70
Health
ycontrols
N=862
(DANVA);EmotionalT
riangles
Task
DANVA
▪Childrenof
motherswith
abingingandpurging
phenotypehadlowerodds
ofmakingerrorswhen
recognisingem
otionalfrom
high-intensity
faces
andlower
odds
ofmisattributingfacesas
sad***
Emotionaltriangle
Binging
andpurgingphenotypemothers’infants’
show
edpoorer
recognition
offear
5 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
Sadeh-Sh
arvitetal.2016a
Case–control
Totaln
=58
Cases
N=29;A
N=14,B
N=13,
EDNOS=2,
meanage31
(4.20)
Health
ycontrols
N=29,m
eanage=33.1(4.64)
Exposure:self-reported
questio
nnaire
(EDI-2)
Outcome:BayleyScales
ofInfant
Development(BSID)
▪The
child
renof
motherswith
eating
disordersshow
eddelayedmentaland
psychomotor
developm
ent
▪Severity
ofmaternaleatingdisordersymptom
sem
ergedas
asignificantp
redictor
ofchild
developm
ent,buto
ther
maternal
psychopathologydidnot
7/9
6 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
Baronaetal.2017
Case–control
Totaln
=65
Cases
N=37;activeED=18,m
eanage
30.17(5.74);pastE
D=19,m
ean
age34.47(3.96)
Health
ycontrols
N=28,m
eanage=34.00(3.34)
Exposure:clinical
interview(SCID
-I)
Outcome:Brazelto
nNeonatal
BehaviouralAssessm
entS
cale
(NBAS)/BayleyScales
ofInfant
andTo
ddlerDevelopment
(BSID-III)
•Exposed
childrenhadpoorer
neurobehaviour
atbirthandworse
language
andmotor
developm
ent
at1year
8/9
PSYCHOPA
THOLOGY
1 Feeding/Eating/
Psychopathology
Evans
andleGrange1995*
Case–control
Totaln
=20
Cases,A
NandBN
N=10,m
eanage=36.0(7.02)
Health
ycontrols
N=10,m
eanage=35.4(4.12)
Exposure:maternalE
D(clinicalinterview?)
Outcome:BodySh
ape
Questionnaire;sem
i-structured
interviewon
feedingand
developm
ent
▪Positive
correlationfoundinbothcase
andcontrol
groups
betweenmothers’satisfactionwith
their
body
size
andtheirchild
ren’ssatisfactionwith
theirow
nweightand
shape
▪Mothersintheclinicalgroupreported
experiencing
emotionalp
roblem
swhenbreastfeedingtheir
child
ren
▪Infantsin
theclinicalgroupwereschedulefed—
thisrigidadherencecaused
someconfusionand
anxietyformotherswhentheirinfantsdisplayed
signsofhungeroutsidetherecommendedfeeding
times
▪Halfthechild
renof
EDmothersweredescribedas
displaying
difficultiessuch
ashyperactivity,
avoidant
behaviour,enuresis,insecure
attachment,depression,fears,personality
problems,stuttering,violent
temperamentand
oppositio
nald
efiant
behaviour
8/9
2 Psychopathology
Barbinetal.2002
Case–control
Totaln
=65,m
eanage=33.2(3.1)
Cases:N
=44
EDgroup(N
=22),depressed
group(N
=20)
Exposure:maternalE
D(self-report
questio
nnaire)
Outcome:Child
Behaviour
Checklist(CBCL);Children’s
▪Nodifferencesin
term
sof
psychological
adjustmentinchild
renof
motherswith
EDand
controls.E
Dmothersreported
higher
numberof
problemsduring
pregnancyandchild
birth
8/9
M. G. Martini et al.456

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
Health
ycontrols
N=23
EatingBehaviour
inventory
(CEBI);P
arentC
hild
RelationshipInventory(PCRI)
▪Childrenof
motherswith
depression
had
significantly
greaterpsychologicalp
roblem
scomparedwith
child
renof
motherswith
EDand
controls
3 Psychopathology/
Feeding/Eating
Reba-Harrelson
etal.2010*
Cohort
Totaln
=13,006
Cases
N=479,BED=634,BN=98,
AN=17
Health
ycontrols
N=12,257
Exposure:maternalE
D(self-reported)
Outcome:Child
Feeding
Questionnaire;C
hild
Behaviour
Checklist(CBCL);Infant
ToddlerSo
cialEmotional
Assessm
ent(ITSE
A)
▪Motherswith
BNandBEDreported
higher
levels
ofdisordered
eatin
gbehavioursin
theirchild
ren
than
controls
▪Theyalso
reported
higher
levelsof
anxiety
symptom
sin
theirchildren
▪Motherswith
BNreported
higherlevelsof
anxiety
andOCDsymptom
sin
theirchildren
▪Maternally
reported
restrictivefeedingwas
significantly
associated
with
child
disordered
eatin
gdifficulties
8/9
4 Psychopathology
Cim
inoetal.2013
Case–control
Totaln
=64,
meanage=33.2(3.1)
Cases
N=31;A
N=16,B
N=15
Health
ycontrol
N=33
Exposure:maternalE
D(clin
icalinterviewSC
ID-I)
Outcome:
Symptom
Checklist-90–R
evised
(SCL-90-R)
Child
Behaviour
Checklist(CBCL)
Children’slongitu
dinalp
rofiles
▪Emotional-adaptiv
eprofilesweresignificantly
higher
inchildrenin
theexposedgroupon
all
CBCLdimensionsacross
allthree
assessment
timepoints
Powerof
maternalE
Dson
thechild
’spsychological
profile
▪Mother’spsychoticism
scorewas
relatedto
the
child
’sanxiety/depression
andT1andT2
8/9
5 Psychopathology
Micalietal.2014a
Cohort
Totaln
=9443
Cases
AN=126,BN=156and
AN+BN=62
Health
ycontrols
N=9099
ALSPAC
Exposure:self-reported
questio
nnaire
(EDE-Q
)Outcome:Developmentand
Well-beingAssessm
ent
(DAWBA);Strengths
andDifficulties
Questionnaire
(SDQ)
MaternalE
Dandoffspringpsychopathology
atage7
▪MaternalE
Dpredictedem
otionald
isorders,
particularly
astrong
associationbetween
maternalA
NandAN+BNforoffspring
emotionald
isorders
MaternalE
Dandoffspring
psychopathologyatage10
▪MaternalE
DpredictedoffspringDSM
-IVor
ICD-10disorder
▪MaternalA
NandAN+BNstrong
associated
with
emotionaland
anxietydisorders**
7/9
6 Psychopathology
Micalietal.2014b
Cohort
Totaln
=8622
Cases
N=351,
AN:n
=193,
meanage=29.5(4.9)
BN:n
=158,
meanage=28.4(4.3)
AN+BN=81
Health
ycontrols
N=8271,m
eanage=28.7(4.6)
Exposure:self-reported
questio
nnaire
Outcome:StrengthsandDifficulties
Questionnaire
(SDQ);Carey
Infant
TemperamentS
cale;
DenverDevelopmentalS
cale;
LifeEventsQuestionnaire;
obstetricrecords
Childhood
psychopathology
▪Genderwas
predictiv
eof
having
conduct
problems,hyperactivity
/inattentionbutn
otof
emotionalp
roblem
s▪Childrenof
wom
enwith
AN(bothgenders)and
boys
ofwom
enwith
BNweremorelikelytohave
emotionalp
roblem
s▪Childrenof
wom
enwith
BNweremorelik
elyto
presentw
ithconductp
roblem
s
7/9
Eating disorders mothers and their children: a systematic review of the literature 457

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
ALSPAC
▪Girlsof
ANmothersweremorelik
elyto
have
emotional,conductand
hyperactivity
problems
▪Girlsof
BNmothersweremorelik
elyto
have
hyperactivity
/inattentionproblems
▪Boysof
ANmothersweretwiceas
likelyto
have
emotionalproblem
swhereas
boys
ofBNmothers
weretwiceas
likelyto
have
emotionaland
conductp
roblem
s7 Psychopathology
Cim
inoetal.2015
Case–control
TotalN
=251families,m
ean
age=33.2(3.1)
Anxiety
disorder
(N=42)
Depressivedisorder
(N=39)
Eatingdisorder(N
=44)
Health
ycontrol
N=126
Exposure:MaternalE
D(clinical
interviewSC
ID-I)
Outcome:symptom
schecklist9
0(SCL-90-R);The
Child
Behaviour
Checklist(CBCL)
▪Children’sexternalisingproblemstended
toincrease
over
timeonly
inthegroups
ofmothers
with
anED
▪Interpersonalsensitivity
andpsychoticism
significantly
predictedexternalizingproblems
8/9
8 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
and
Temperament
Baronaetal.2016*
Cohort
Totaln
=48,403
Cases
N=2197;A
N=906;
BN=931;
AN+BN=360
Health
ycontrols
N=46,206,
meanage=29.4(4.16)
DNBC
Exposure:self-reportq
uestionnaire
Outcome:Developmental
MilestoneInterview;C
hild
Temperament;Looking
after
Child;S
DQ
▪Girlsof
wom
enwith
lifetim
eANhadhigherodds
ofhaving
emotionalp
roblem
s▪Girlsof
wom
enwith
lifetim
eBNof
having
conductp
roblem
scomparedwith
childrenof
healthywom
en▪Boysof
wom
enwith
lifetim
eANhadhigherodd
oftotal,em
otionaland
conductp
roblem
s▪B
oysof
wom
enwith
lifetim
eBNhadhigherodds
oftotal,conduct,hyperactivity
andpeer
difficultiescomparedto
childrenof
wom
enwith
outanED
▪Boysof
wom
enwith
lifetim
eANandBNhad
higherodds
oftotal,em
otionaland
peerproblems
comparedto
child
renof
healthywom
en
8/9
9 Psychopathology
Cim
inoetal.2016
Case–control
Totaln
=408parents
Cases
Bothparentswith
BEDN=102,
child
ren=51
Onlymotherswith
BEDN=104,
child
ren=52
Onlyfatherswith
BEDN=100,
child
ren=50
Health
ycontrols
N=102parents,child
renN=51
Exposure:maternalE
D(clin
ical
interviewthroughDSM
-5criteria)
Outcome:ScalefortheAssessm
ent
ofFeedingInteractions
(SVIA
)/Child
Behaviour
Checklist
(CBCL)
▪The
groups
with
oneor
both
parentsdiagnosed
with
BEDshow
edhigherscoreson
theSV
IAand
ontheCBCLinternalisingandexternalising
scales,indicatingpoorer
adult–child
feeding
interactions
andhigher
emotional–behavioural
difficulties
▪Adirectinfluenceof
parentalpsychiatricdiagnosis
onthequality
ofmother–infant
andfather–infant
interactions
was
also
found,both
atT1andT2
8/9
10 Psychopathology
Sadeh-Sh
arvitetal.2016b
Case–control
Totaln
=notspecified
Cases
N=29;A
N=14;B
N=13;
EDNOS=2,meanage=31
(4.20)
Health
ycontrols
Exposure:self-reportq
uestionnaire
(EDI-2)
Outcome:CBCL/2–3;v
ideo
recordingof
mother/child
interaction
▪Motherswith
eatingdisorderswerelesssensitive
totheirchildren,triedto
controltheirchildren’s
behavioursmore,andwereless
happyduring
mother–child
interactions
▪The
child
renin
thematernaleatingdisordergroup
wereratedas
lessresponsive
totheirmothersand
8/9
M. G. Martini et al.458

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
N=notspecified,
meanage,33.1(4.64)
theirmothersalso
reported
morebehavioural
problemsthan
thosein
thecontrolg
roup
11 Psychopathology
Cim
inoetal.2018
Case–control
Totaln
=150families
Cases
F+/M
+N=50
M−/F+
N=50
F+/M
−N=50
Health
ycontrols
N=50
Exposure:maternalE
D,clin
ical
interview(SCID
-I)
Outcome:Italianadaptio
nof
FeedingScale(SVIA
)/CBCL
▪Childrenwith
both
parentswith
BEDshow
edthe
highestaffective,anxiety,oppositio
nal/defiant
andautism
spectrum
problems,butn
oinfluence
ofpaternaldiagnosiswasfoundon
theoffspring’s
psychopathology
▪MaternalB
EDhadan
influenceon
children’s
affectiveandautism
spectrum
problems
▪Diagnosisof
BEDinbothparentshadan
effecton
infants’affectiveproblems
▪PaternalB
EDhadan
effecton
oppositio
nal/d
efiant
problemsthroughthequality
offather–infant
interactions
▪MaternalB
EDhadan
effecton
theoffspring’s
affectiveandanxietyproblemsthroughthe
mediatio
nof
mother–infant
interactions
7/9
TEMPE
RAMENT
1 Feeding/Eating/Temperament
Agras
etal.1999*
Case–control
Totaln
=194
Cases
N=41,m
eanage=32.1(4.4)
AN=2,BN=17,B
ED=22
Health
ycontrols
N=153,meanage32.9(3.8)
Exposure:maternalE
D(clin
ical
interviewDSM
III-R+Eating
DisorderInventory—
EDI)
Outcome:Infant
FeedingReport
(IFR
);Su
ckom
eter;C
hildren’s
Behaviour
Questionnaire
▪Fem
aleinfantsof
EDmotherssucked
morerapidly
than
otherinfantsbutn
odifferencesin
caloric
intake
atthesefeedings
▪EDmothersbottlefedtheirdaughtersforamean
timeof
33.2
monthscomparedwith
infantsof
NEDmotherswith
23.6
months
▪EDmothersconsidered
theirfemalechild
rento
have
moredifficulty
inweaning
from
thebottle
(but
notfrom
thebreast)than
NEDmothers
▪Infantsof
EDmotherswerereported
todawdle
morewhileeatin
gcomparedto
child
renof
NED
group
▪EDmothersreported
theirdaughtersas
vomiting
morefrequently
than
theirsons
(opposite
effect
forNEDmothers)
▪EDmothersreported
higher
concernfortheir
daughter’sweightthanNEDmothers
▪Significant
maineffectfortheEDgroupforusing
food
asnon-nutritive
purposes
▪Significanteffectof
EDmothersreportingthey
fed
theirchildrenon
alessregularschedulethan
NED
mothers
▪Childrenof
motherswith
EDreported
asdemonstratin
gmorenegativeaffect
(sadness,crying,irritability)
than
childrenof
NEDmothers
8/9
Eating disorders mothers and their children: a systematic review of the literature 459

Tab
le1
(contin
ued)
Authors
Study,design
Participants:n
,age
(SD),
diagnosesandrecruitm
ent
Measures
(exposureandoutcom
e)Results
NOSratin
g
2 Feeding/Eating/Temperament
Waugh
andBulik
1999*
Case–control
Totaln
=20
mothers
N=10,m
eanage30.1(3.1)
PastAN=6,PastBN=7
Health
ycontrolsrecruitedfrom
community
n=10,m
eanage30.8(3.6)
Exposure:maternalE
D(clin
icalinterview)
Outcome:To
ddlerTemperament
Scale(TTS);M
ealtime
Observatio
nSchedule(M
OS);
Food
Diary
▪Childrenof
wom
enwith
eatingdisordershad
significantly
lowerbirthweightsandlengthsthan
controlchildren
▪Nodifferencesobserved
inchildhood
temperament
ormothers’satisfactionwith
child
ren’s
appearance
▪Motherswith
EDmadesignificantly
fewerpositive
eatingcomments
8/9
3 Cognitiv
edevelopm
ent/
Neuropsychologicalp
rofile
and
Temperament
Baronaetal.2016*
Cohort
Totaln
=48,403
Cases
N=2197;A
N=906;
BN=931;
AN+BN=360
Health
ycontrols
N=46,206,
meanage=29.4(4.16)
Exposure:self-reportq
uestionnaire
Outcome:Developmental
MilestoneInterview;C
hild
Temperament;Looking
after
Child;S
DQ
▪Girlsof
wom
enwith
lifetim
eANhadhigherodds
ofhaving
emotionalp
roblem
s▪Girlsof
wom
enwith
lifetim
eBNof
having
conductp
roblem
scomparedwith
childrenof
healthywom
en▪B
oysof
wom
enwith
lifetim
eANhadhigherodds
oftotal,em
otionaland
conductp
roblem
s▪B
oysof
wom
enwith
lifetim
eBNhadhigherodds
oftotal,conduct,hyperactivity
andpeer
difficultiescomparedto
childrenof
wom
enwith
outanED
▪Boysof
wom
enwith
lifetim
eANandBNhad
higherodds
oftotal,em
otionaland
peerproblems
comparedto
child
renof
healthywom
en
8/9
4 Temperament
Zerwas
etal.2012
Cohort
Totaln
=48,964
Cases
N=3013,
AN:n
=44
meanage=26.5(4.7)
BN:n
=436mean
age=29.6(4.7)
BED:n
=2475,
meanage=30.1(4.6)
EDNOS:
n=58
meanage=27.8(5.2)
Health
ycontrols
N=45,964
Exposure:maternalE
D(self-report
questio
nnaire)
Outcome:Fu
ssy/Difficult
Subscale–InfantC
haracteristics
Questionnaire
▪Motherswith
anEDhadgreaterodds
ofreporting
moredifficultinfanttem
peramentratings
▪Wom
enwith
ANandEDNOS-Pwere2.3–2.8
times
morelikelyto
ratetheirchild
ren’s
temperamentasdifficult
9/9
AN,anorexianervosa;BED,binge-eatingdisorder;B
N,bulim
ianervosa;ED,eatingdisorder;S
CID
,StructuredClin
icalInterviewforDSM-IV
*Studies
fitting
morethan
onedomain
M. G. Martini et al.460

and infant temperament (n = 4). Five studies fit more than onedomain.
Characteristics of the 34 articles included in the systematicreview are shown in Table 1.
Quality assessment
The research design and content of studies was well executedwith over 90% rated as strong. The four studies rated as mod-erate were due to (1) poor representativeness of cases, poorlydefined controls and ascertainment of exposure; (2) lack ofcomparability of cases and controls on the basis of design oranalysis (Blissett and Meyer 2006); (3) one study being un-controlled (Hodes et al. 1997); and (4) no description of con-trol group, no mention of history of outcome (Saltzman et al.2016). It is worth noting that sample size was not accountedfor as some studies rated as strong included small sample sizesof less than 10 (Evans and le Grange 1995). Therefore, astrong and positive overall assessment should be interpretedwith caution.
Study results
Feeding outcomes (n = 17)
Given its relevance, the impact of maternal ED on children’sfeeding and mealtimes is an area that has received consider-able attention. Feeding the infant is a crucial task of parentingnot only because it can absorb considerable part of the day inthe early stages of life but also because it is one of the mostimportant means of communication between mother and child(Silva et al. 2016).
Review of the present studies showed that mothers with EDmight exhibit problems in feeding behaviours with their off-spring starting from breast feeding. A number of population-based studies investigated the impact of ED on breast feeding,yielding discrepant findings (Micali et al. 2011, 2009). A largepopulation-based study showed that women with a history ofED were more likely to start breast feeding and less likely tostop during the first year of the infant life. More specifically,mothers with BN were more likely to continue breast feedingand these differences persisted even after adjusting for
Records iden�fied through database searching
Medline 564
Psycinfo 33
Embase 10
Records iden�fied when duplicates removed 569
Titles and abstracts screened 569
Full Text ar�cles screened for eligibility 69
Full text ar�cles mee�ng inclusion criteria 33
28 Duplicates removed
Full text ar�cles excluded 21
Reasons:
-Inves�gated Ea�ng problems in mothers with ED 14
-Inves�gated child weight or growth 2
-Interven�ons were assessed 3
-Inves�gated birth or perinatal outcomes 16
-Uncontrolled study 1
Fig. 1 PRISMA flow diagram showing study selection process
Eating disorders mothers and their children: a systematic review of the literature 461

confounding factors (Micali et al. 2009). A similar studyfound that women with ED started breast feeding their infantsas often as controls; however, they were more likely to inter-rupt early (Torgersen et al. 2010). Conversely, Nguyen andcolleagues found that mothers with a history of ED wereslightly less likely to initiate breast feeding, although no lon-ger significant after adjustment (socio-demographics, bodymass index (BMI), maternal psychiatric symptoms) (Nguyenet al. 2017).
Although feeding difficulties are common in early stages ofthe infant’s life, mothers with AN reported increased feedingproblems including exhaustion during feeding, slow feedingand no established feeding routine (Micali et al. 2011, 2009).On the other hand, infants of women with BN had higherlevels of refusal to take solids in comparison to controls(Micali et al. 2009). Blisset and Meyer found similar resultswith some gender specificity, showing that maternal eatingpsychopathology predicted food refusal in girls but not boys.Symptoms of low maternal depression combined with highbulimic scores were significantly associated with food refusalin girls (Blissett and Meyer 2006). Conversely, Whelan andCooper did not find the gender of the child to be related tomaternal ED history, nor did it moderate the relationship be-tween feeding difficulties and maternal ED (Whelan andCooper 2000).
There is a well-known relationship between specific par-enting styles in women with EDs and feeding problems intheir offspring. An early study found that negative expressedemotions and more intrusive behaviours were more frequentamong mothers with ED compared to controls during bothmealtime and play (Stein et al. 1994). Mealtime interactionin offspring (ages 1–4) and mothers with ED compared tocontrols was also investigated by Waugh and Bulik (1999)who found that control mothers made more positive eatingcomments while mothers with ED tended to be more negative.
Differences between ED diagnoses and their impact oninfant feeding problems are worth noting. Saltzman and col-leagues found that maternal BED predicted use of more non-responsive feeding practices (i.e. emotion regulation, restric-tion for health, pressure to eat and food as reward), indirectlythrough more distress responses to children’s negative emo-tions. Maternal BED was associated with greater use of dis-tress responses, which indirectly predicted higher child BMIpercentile through food as reward feeding practices (Saltzmanet al. 2016). Also, mothers with BN or BED were more likelyto report higher levels of restrictive feeding styles compared tocontrols (Reba-Harrelson et al. 2010), and mothers with ahistory of AN were more likely to use less pressuring feedingstrategies compared to controls (de Barse et al. 2015).
Maternal ED can also influence nutritional intake, dietarypatterns and diet quality in infants.
Easter and colleagues found that children of mothers withED reported higher scores on the ‘health conscious/
vegetarian’ dietary pattern (diet high in vegetarian foods, nuts,salad, rice, pasta and fruits) across all four time periods (ages3, 4, 7 and 9) when compared with controls (Easter et al.2013). Furthermore, they showed less adherence to the ‘tradi-tional’ dietary pattern across all four time points. Energy in-take was higher in the BN and AN +BN group, and this intakeincreased significantly over time for children of mothers withBN (Easter et al. 2013). In another study, Torgersen et al.(2015) found that mothers with BN and BED were less likelyto use ‘homemade traditional food’ than ‘commercial jarredbaby food’ when compared with mothers without ED; how-ever, in women with BED, the associations were significantonly before controlling for relevant confounders (Torgersenet al. 2015). Nguyen and colleagues found that children ofmothers with life-time ED had higher diet quality at 1 year(Nguyen et al. 2017). Mothers with histories of ED may alsobe more likely to take ‘special approaches’ to feeding theirchildren, such as limiting the amount of processed foods oreliminating other types or classes of foods (Hoffman et al.2014).
Body image distortion, core symptoms of both AN and BNcan also have an impact on feeding practices. In a recent studyconducted by our team, we found that women with both pastand current ED reported higher concerns about their infantbeing/becoming overweight compared with controls, respec-tively, at 8 weeks and 6months and 6 months only postnatally.Also, women with past ED showed less awareness of infanthunger and satiety cues compared with HC at 8 weeks(Martini et al. 2018).
Cognitive development and neuropsychological profile (n =6)
There is a growing evidence to suggest that ED arecharacterised by a specific neurocognitive profile includingalterations in attention, visuospatial ability, memory, socialcognition and executive functions, encompassing set shiftingand central coherence (Giombini et al. 2018; Lang et al. 2014;Westwood et al. 2016). These profiles observed during activeillness were thought to be a complex interplay between riskand protective factors, given the genetic profile and the driveto high educational achievement and perfectionism, commonfeatures of ED profile (Bardone-Cone et al. 2010). Also, thesemight be intermediate phenotypes, an early risk marker thatare thought to lie between genetic/biological risk and actualphenotypical manifestations (Micali and Dahlgren 2016).
Research on neuropsychological profiles in children ofwomen with ED aimed mainly at understanding both the im-pact of maternal ED on their children and to obtain a betterunderstanding of intermediate endophenotypes of ED.
In the study carried out by Kothari et al. (2013), the inves-tigation of neuropsychological profiles showed that childrenof mothers with AN had high full-scale and performance IQ,
M. G. Martini et al.462

increased working memory (WM) capacity, better visuospa-tial functioning and decreased attentional control when com-pared to controls (Kothari et al. 2013). Another study investi-gating the early cognitive development (18 months and4 years) in a sub-set of these children showed that childrenof women with lifetime AN had difficulties with social under-standing, poorer motor skills, planning and abstract reasoning(Kothari et al. 2014). In a recent longitudinal study of childrenof mothers with ED, we recently found that infants of motherswith ED had poorer language and motor development com-pared to control mothers. Interestingly, after studying differ-ential outcomes based on active versus past ED, we found thatchild cognitive difficulties were associated both with maternalactive ED and past ED (Barona et al. 2017). Overall, thesefindings highlight early developmental difficulties in motorand cognitive development in offspring of ED mothers.
The study of later cognitive characteristics suggests a morespecific pattern of strengths and difficulties across several do-mains of cognition, for example, higher IQ, better visuospatialperformance and WM in children of mothers with lifetimeAN, and poorer visuospatial functioning in children ofmothers with lifetime BN (Barona et al. 2017).
Only one study to date has investigated social cognition inchildren of mothers with ED in mid-childhood and early ado-lescence, with some evidence of differences between at-riskoffspring and controls. In particular, differential facial emotionprocessing, poorer recognition of fear, and higher scores onthe social communication disorders checklist were present inchildren of mothers with binge eating and purging behaviours,the latter also present in children of mothers with lifetimeBED (Kothari et al. 2015).
Finally, in a small longitudinal cohort study, Koubaa andcolleagues found that children born to mothers with AN or BNhad significantly higher Five to Fifteen (validated parent ques-tionnaire assessing neurocognitive development) scores thancontrols reflecting difficulties in language and social skills(Koubaa et al. 2013).
Psychopathology (N = 12)
There is strong evidence that parental mental illness is associ-ated with psychopathology in offspring, establishing that chil-dren of parents with psychiatric disorders are at higher risk ofdeveloping psychopathology themselves (Rasic et al. 2013).Research has also shown that familiar risk is only partlydiagnosis-specific meaning that children might develop thesame parental diagnosis (homotypic transmission) but maybe also at risk for a range of other psychiatric disorders (het-erotypic transmission) (Siegenthaler et al. 2012). However,the effect of maternal ED on their offspring psychopathologyhas received less attention.
Of the studies in this domain, five specifically investigatedpsychological/emotional development (Barbin et al. 2002;
Cimino et al. 2016, 2013, 2015; Sadeh-Sharvit et al. 2016b) andseven explored general psychopathology (Barona et al. 2016;Cimino et al. 2018; Evans and le Grange 1995; Hodes et al.1997; Micali et al. 2014a, 2014b; Reba-Harrelson et al. 2010).
A large longitudinal cohort study identified a higher riskfor emotional and behavioural disorders in offspring of EDmothers at an early age (3.5 years). Specifically, the authorsidentified associations between maternal ED type (AN vs.BN) and child psychopathology (emotional vs. behaviouralproblems), as well as gender differences (Micali et al.2014b). Emotional difficulties were found in both girls andboys of mothers with AN, while more hyperactivity and peerdifficulties were found in both girls and boys of mothers withBN. This study also aimed to understand risk mechanisms andhighlighted a mediating role for maternal anxiety and depres-sion in the postpartum. These findings were confirmed andextended in a later study when the same children were aged7, 10 and 13, where maternal EDs (both AN and BN) stronglypredicted emotional and anxiety disorders (Micali et al.2014a). A recent longitudinal study showed that maternalED was associated with childhood psychopathology in girlsand boys at age 7, both emotional and behavioural problems.Disorder and gender-specific findings across studies point toan effect of maternal lifetime AN on emotional disorders, inparticular anxiety, across ages; while maternal BN seems to beassociated with hyperactivity, conduct and peer problems(Barona et al. 2016).
These findings support those of case–control studies. Intwo longitudinal studies using the Child Behaviour Checklist(CBCL), the authors found that children of mothers with EDreported higher externalising and internalising scores fromthe CBCL compared to controls (Cimino et al. 2015,2018). The emotional-adaptive profiles of children in theclinical group of mothers with ED scored significantly higherin all dimensions of the CBCL (Cimino et al. 2013). Morespecifically, externalising problems increased over time(Cimino et al. 2015).
The same authors carried out other two longitudinal studiesaimed at investigating the emotional and behavioural profileof children of one or both parents with BED and adult–childfeeding interaction (Cimino et al. 2016, 2018). They foundthat the children with one or both parents diagnosed withBED had higher scores on the internalising and externalisingscales, and higher levels of emotional and behavioural diffi-culties (Cimino et al. 2016). Furthermore, children with bothparents with BED showed the highest affective, anxiety, op-positional/defiant, and autism spectrum problems versus chil-dren of families with only one BED diagnosed father.Maternal BED was associated with children’s affective andautism spectrum problems, and diagnosis of BED in bothparents had an effect on infants’ affective problems. PaternalBED had an effect on oppositional/defiant problems throughthe quality of father–infant interactions, and maternal BED
Eating disorders mothers and their children: a systematic review of the literature 463

had an effect on the offspring’s affective and anxiety problemsthrough the mediation of mother–infant interactions (Ciminoet al. 2018).
On the contrary, Barbin et al. did not find any difference interms of psychological adjustment on both subscales ofinternalising and externalising in children of mothers withED compared to healthy controls (Barbin et al. 2002).
In two early small studies, authors found that half ofchildren of mothers with ED displayed psychiatric problemssuch hyperactivity, avoidant behaviour, enuresis, insecureattachment, depression, fears, personality problems,stuttering, violent temperament and oppositional defiant be-haviour (Evans and le Grange 1995) and OCD (Hodes et al.1997), respectively.
The latter association has also been found in a more recentlarge cohort study conducted by Reba-Harrelson and col-leagues. The authors found that children of mothers withbinge BED or BN were significantly more likely to exhibitsymptoms of anxiety compared to children of control groupmothers. Children of mothers with BN were also significant-ly more likely to exhibit obsessive-compulsive symptomsthan children of non-eating-disordered mothers. All thosewith AN, BN or BED were significantly more likely to havechildren who exhibited symptoms of depression (Reba-Harrelson et al. 2010).
Likewise in a small recent study, mothers with ED reportedhigher levels of behavioural problems in their children com-pared to control mothers (Sadeh-Sharvit et al. 2016b).
Temperament (N = 4)
Temperament is defined as early appearing, biologicallyrooted, basic personality dimension (Bates et al. 1995).Although temperament is said to be a biological tendencywithin each child, environmental contexts, especially the so-cial context, interrelate with the genetic tendencies of eachchild (Shiner et al. 2012).
Mothers with EDs have been shown to be more likely todescribe their infant as having a difficult temperament.Compared to womenwith no history or current EDs, they tendto rate their children as having high levels of difficult temper-ament (Zerwas et al. 2012) and perceive them as having great-er negative affect, that is, demonstrating more sadness, irrita-bility and crying compared to controls (Agras et al. 1999). In amore recent large longitudinal study, we found that motherswith ED were more likely to perceive their children as havinga ‘difficult temperament’ characterised by the child being lesshappy and active than other children their age, more restlessand as having more tantrums and as being less cautious andguarded than other children their age (Barona et al. 2016). Onthe contrary in an early study, the authors did not observe anydifference in childhood temperament between children bornfrom ED mothers and controls (Waugh and Bulik 1999).
Discussion
The literature regarding the impact of maternal ED onchild development has expanded in the last decade.Albeit earlier studies focusing on small clinical samples,larger population-based samples have recently increasedour knowledge on the topic.
Overall, the literature suggests that maternal ED im-pact on child cognitive, psychological and feeding andeating development.
Regarding feeding and eating, research shows that childrenof mothers with ED tend to experience more difficulties infeeding their children both in infancy and childhood.Although studies on breast feeding yield mixed results, wom-en with ED often report difficulties with this. Throughouttoddler years, difficulties such as slow feeding, small quanti-ties feeding and not having established feeding routinesemerged as common among ED mothers. Restricting parentalfeeding styles, negative expressed emotions and intrusive be-haviours also appeared to be more frequent in ED motherscompared to controls. The most recent findings (Martiniet al. 2018; Saltzman et al. 2016) are in line with earlier re-search (Stein et al. 1994). To date, it is not possible to disen-tangle the influence of genetic predisposition versus environ-mental factors, though likely both have a role. Future researchinvestigating genotype–environment interface is warranted toprovide further insight.
Although the current literature is less prominent, availablefindings shows that a maternal lifetime history of ED mayhave a negative impact also on children’s cognitive, psycho-logical development and psychopathology.
Interestingly, recent studies have identified shared geneticrisk between ED and other psychiatric disorders, i.e. schizo-phrenia and BED (Solmi et al. 2019) and AN and obsessivecompulsive disorder (OCD) but also other positive geneticcorrelations between AN and schizophrenia and AN and neu-roticism (Duncan et al. 2017; Yilmaz et al. 2018). These find-ings suggest that the genetic risk transmitted will impact onthe behavioural, physiological and medical phenotypesexpressed in children. Therefore, we might assume that chil-dren of AN women have a higher genetic risk of developing awide range of phenotypes and psychiatric disorders such aspsychosis, neuroticism, educational attainment but also lowerBMI and lower risk of diabetes. Less is known on cognitionand neuropsychological characteristics in offspring of EDmothers prior to the onset of psychopathology, and thesemight be an important focus of study in at-risk offspring, help-ing future prevention and early interventions.
Strengths and limitations
This systematic review has several strengths. First, it is thefirst systematic review summarising the existing findings from
M. G. Martini et al.464

1980 until 2018 on the impact of maternal ED on child devel-opment, and its findings can be valuable in deriving futurehypothesis.
Second, the majority of studies relied on community-basedor register-based samples rather than clinical samples; there-fore, selection bias in the original studies is likely to be small.
Moreover, if an association between maternal ED and childdevelopment has been established in population-based stud-ies, which are more likely to include less severe case of ED,our results are liable to be an underestimation of the effect.
However, some limitations should also have to be takeninto account. Some of the studies reviewed above are singlefindings and need replication. Also, the vast majority of thestudies explored mother–child dyad and did not involve thefathers. Although ED have a higher incidence in women thanin men, gender ration is less skewed in BED than BN and AN(Hudson et al. 2007) and paternal ED can also have an impacton child development.
Studies showed a high degree of heterogeneity in the waythe ED diagnosis is established, ranging from self-reportedquestionnaires (used in cohort studies such as ALSPAC(Easter et al. 2013; Micali et al. 2009, 2011, 2014a, 2014b,), DNBC (Barona et al. 2016), Generation R study (de Barseet al. 2015; Nguyen et al. 2017), MoBa (Torgersen et al.2015)) to structured interviews using both the Diagnosticand Statistical Manual (Agras et al. 1999; Cimino et al.2016; Evans and le Grange 1995; Stein 1999; Waugh andBulik 1999; Whelan and Cooper 2000) and SCID I (Baronaet al. 2017; Cimino et al. 2015, 2018; Hoffman et al. 2014;Kothari et al. 2015; Martini et al. 2018).
It is important to point out that parental psychopathologydoes not always impact on child development in a negativeway. This might be due to numerous factors including protec-tive family network, child resilience, early access to mentalhealth services, parenting abilities etc.
Future research should focus on the protective factors thatmoderate the relationship between maternal ED and adversechild outcomes leading to a healthy development of the child.This would shed light into mechanisms that could be poten-tially directed for intervention. For example, further researchcould introduce fathers and explore their roles in the familydynamics and in ameliorating, exacerbating or acting indepen-dently of the possible influence of a mother with ED.
Conclusion
In summary, maternal ED have an impact on child psycholog-ical, cognitive and eating development, and might affect thedevelopment of ED in the offspring. Despite this evidence,little is known on how genetic and environmental factors in-terplay and affect risk. As maternal psychopathology not al-ways negatively affect child development, future research
should focus on resilience and on which protective factorshave impact on positive outcome. These factors can be thenused as therapeutic and preventative targets.
Compliance with ethical standards
Conflict of interest The authors declare that they have no competinginterests.
Ethical approval The article does not contain any studies with humanparticipants performed by any of the authors.
Open Access This article is licensed under a Creative CommonsAttribution 4.0 International License, which permits use, sharing, adap-tation, distribution and reproduction in any medium or format, as long asyou give appropriate credit to the original author(s) and the source, pro-vide a link to the Creative Commons licence, and indicate if changes weremade. The images or other third party material in this article are includedin the article's Creative Commons licence, unless indicated otherwise in acredit line to the material. If material is not included in the article'sCreative Commons licence and your intended use is not permitted bystatutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of thislicence, visit http://creativecommons.org/licenses/by/4.0/.
References
Agras S, Hammer L, McNicholas F (1999) A prospective study of theinfluence of eating-disordered mothers on their children. Int J EatingDisord 25(3):253–262
Bannatyne AJ, Hughes R, Stapleton P, Watt B, MacKenzie-Shalders K(2018) Signs and symptoms of disordered eating in pregnancy: aDelphi consensus study. BMC Pregnancy Childbirth 18(1):1–16.https://doi.org/10.1186/s12884-018-1849-3
Barbin JM, Williamson DA, Stewart TM, Reas DL, Thaw JM (2002)Psychological adjustment in the children of mothers with a historyof eating disorders. Eat Weight Disord 7:32–38
Bardone-Cone AM, Sturm K, Lawson MA, Robinson DP, Smith R(2010) Perfectionism across stages of recovery from eating disor-ders. Int J Eating Disord 43(2):139–148. https://doi.org/10.1002/eat.20674
Barona M, Nybo Andersen AM, Micali N (2016) Childhood psychopa-thology in children of women with eating disorders. Acta PsychiatrScand 134(4):295–304. https://doi.org/10.1111/acps.12616
Barona M, Taborelli E, Corfield F, Pawlby S, Easter A, Schmidt U et al(2017) Neurobehavioural and cognitive development in infants bornto mothers with eating disorders. J Child Psychol Psychiatry AlliedDiscip 58(8):931–938. https://doi.org/10.1111/jcpp.12736
Bates JE, Wachs T, VandenBos G (1995) Trends in research on temper-ament. Psychiatr Serv 46(7):661–663
Blissett J, Meyer C (2006) The mediating role of eating psychopathologyin the relationship between unhealthy core beliefs and feeding diffi-culties in a nonclinical group. Int J Eat Disord 39:763–771. https://doi.org/10.1002/eat
Bulik CM, Reba L, Siega-Riz AM, Reichborn-Kjennerud T (2005)Anorexia nervosa: definition, epidemiology, and cycle of risk. Int JEat Disord 37(SUPPL). https://doi.org/10.1002/eat.20107
Cimino S, Cerniglia L, PacielloM, Sinesi S (2013) A six-year prospectivestudy on children of mothers with eating disorders: the role of pa-ternal psychological profiles. Eur Eat Disord Rev 21:238–246.https://doi.org/10.1002/erv.2218
Eating disorders mothers and their children: a systematic review of the literature 465

Cimino S, Cerniglia L, Paciello M (2015) Mothers with depression, anx-iety or eating disorders: outcomes on their children and the role ofpaternal psychological profiles. Child Psychiatry Hum Dev 46:228–236. https://doi.org/10.1007/s10578-014-0462-6
Cimino S, Cerniglia L, Porreca A, Simonelli A, Ronconi L, Ballarotto G(2016) Mothers and fathers with binge eating disorder and their 18–36 months old children: a longitudinal study on parent–infant inter-actions and offspring’s emotional-behavioral profiles. Front Psychol7:1–12. https://doi.org/10.3389/fpsyg.2016.00580
Cimino S, Cerniglia L, Porreca A, Ballarotto G, Marzilli E, Simonelli A(2018) Impact of parental binge eating disorder: exploring children’semotional/behavioral problems and the quality of parent–child feed-ing interactions. Infant Ment Health J 39(5):552–568. https://doi.org/10.1002/imhj.21732
de Barse LM, Tharner A, Micali N, Jaddoe VVW, Hofman A, VerhulstFC et al (2015) Does maternal history of eating disorders predictmothers’ feeding practices and preschoolers’ emotional eating?Appetite 85:1–7. https://doi.org/10.1016/j.appet.2014.10.031
Duncan L, Yilmaz Z, Walters R, Goldstein J, Anttila V, Bulik-Sullivan Bet al (2017) Genome-wide association study reveals first locus foranorexia nervosa andmetabolic correlations. Am J Psychiatr 174(9):850–858. https://doi.org/10.1176/appi.ajp.2017.16121402.Genome-Wide
Easter A, Howe LD, Tilling K, Schmidt U, Treasure J, Micali N (2014)Growth trajectories in the children of mothers with eating disorders:a longitudinal study. BMJ Open 4(3):1–10. https://doi.org/10.1136/bmjopen-2013-004453
Easter A, Naumann U, Northstone K, Schmidt U, Treasure J, Micali N(2013) A longitudinal investigation of nutrition and dietary patternsin children of mothers with eating disorders. J Pediatr 163(1):173–178.e1. https://doi.org/10.1016/j.jpeds.2012.11.092
Evans J, le Grange D (1995) Body size and parenting in eating disorders:a comparative study of the attitudes of mothers towards their chil-dren. Int J Eating Disord 18(1):39–48
Giombini L, Nesbitt S, Cox H, Foxall A, Sharia T, Easter A, Tchanturia K(2018) Cognitive remediation therapy ( CRT ) in a specialist inpa-tient eating disorder service for children and adolescents : CAN–CRT study protocol for a pilot randomised controlled trial. Eur EatDisord Rev (February):1–9. https://doi.org/10.1002/erv.2592
Hodes M, Timimi S, Robinson P (1997) Children of mothers with eatingdisorders: a preliminary study. Eur Eat Disord Rev 5(1):11–24.https://doi.org/10.1002/(SICI)1099-0968(199703)5:1<11::AID-ERV179>3.0.CO;2-7
Hoffman ER, BentleyME, Hamer RM, Hodges EA,Ward DS, Bulik CM(2014) A comparison of infant and toddler feeding practices ofmothers with and without histories of eating disorders. MaterChild Nutr 10(3):360–372. https://doi.org/10.1111/j.1740-8709.2012.00429.x
Hudson JI, Hiripi E, Pope H, Kessler RC (2007) The prevalence andcorrelates of eating disorders in the National Comorbidity SurveyReplication. Biol Psychiatry 61(3):348–358
Kothari R, Solmi F, Treasure J, Micali N (2013) The neuropsychologicalprofile of children at high risk of developing an eating disorder.Psychol Med 43:1543–1554. ht tps: / /doi .org/10.1017/S0033291712002188
Kothari R, Rosinska M, Treasure J, Micali N (2014) The early cognitivedevelopment of children at high risk of developing an eating disor-der. Eur Eat Disord Rev 22:152–156. https://doi.org/10.1002/erv.2274
Kothari R, Barona M, Treasure J, Micali N (2015) Social cognition inchildren at familial high-risk of developing an eating disorder. FrontBehav Neurosci 9:1–17. https://doi.org/10.3389/fnbeh.2015.00208
Koubaa S, Hallstrom T, Hagenas L, Hirschberg AL (2013) Retarded headgrowth and neurocognitive development in infants of mothers with ahistory of eating disorders: longitudinal cohort study. BJOG 120:1413–1421. https://doi.org/10.1111/1471-0528.12370
Lang K, Lopez C, Stahl D, Tchanturia K, Treasure J, Lang K et al (2014)Central coherence in eating disorders: an updated systematic reviewand meta-analysis. World J Biol Psychiatry:2975. https://doi.org/10.3109/15622975.2014.909606
Martini MG, Taborelli E, Schmidt U, Treasure J, Micali N (2018) Infantfeeding behaviours and attitudes to feeding amongst mothers witheating disorders: a longitudinal study. Eur Eat Disord Rev:1–10.https://doi.org/10.1002/erv.2626
Mazzeo SE, Zucker NL, Gerke CK, Mitchell KS, Bulik CM (2005)Parenting concerns of women with histories of eating disorders.Int J Eat Disord 37(SUPPL):77–79. https://doi.org/10.1002/eat.20121
Micali N, Treasure J (2009) Biological effects of a maternal ED on preg-nancy and foetal development: a review. Eur Eat Disord Rev 17:448–454. https://doi.org/10.1002/erv.963
Micali N, Simonoff E, Treasure J (2009) Infant feeding and weight in thefirst year of life in babies of women with eating disorders. J Pediatr154:55–60. https://doi.org/10.1016/j.jpeds.2008.07.003
Micali N, Simonoff E, Stahl D, Treasure J (2011) Maternal eating disor-ders and infant feeding difficulties: maternal and child mediators in alongitudinal general population study. J Child Psychol Psychiatry52(7):800–807. https://doi.org/10.1111/j.1469-7610.2010.02341.x
Micali N, De Stavola B, Ploubidis GB, Simonoff E, Treasure J (2014a)The effects of maternal eating disorders on offspring childhood andearly adolescent psychiatric disorders. Int J Eat Disord 47(4):385–393. https://doi.org/10.1002/eat.22216
Micali N, Stahl D, Treasure J, Simonoff E (2014b) Childhood psychopa-thology in children of women with eating disorders: understandingrisk mechanisms. J Child Psychol Psychiatry 55(2):124–134. https://doi.org/10.1111/jcpp.12112
Micali N, Dahlgren CL (2016) All that glisters is not an endophenotype:rethinking endophenotypes in anorexia nervosa. Eur Child AdolescPsychiatry 25(11):1149–1150. https://doi.org/10.1007/s00787-016-0910-x
Moher D, Liberati A, Tetzlaff J, AltmanDG, Group, T. P (2009) Preferredreporting items for systematic reviews and meta-analyses: thePRISMA statement. PLoS Med 6(7):1–6. https://doi.org/10.1371/journal.pmed.1000097
NguyenAN, deBarse LM, Tiemeier H, Jaddoe VWV, Franco OH, JansenPW, Voortman T (2017) Maternal history of eating disorders: dietquality during pregnancy and infant feeding. Appetite 109:108–114.https://doi.org/10.1016/j.appet.2016.11.030
Park R, Senior R, Stein A (2003) The offspring of mothers with eatingdisorders. Eur Child Adolesc Psychiatry 12:110–119. https://doi.org/10.1007/s00787-003-1114-8
Patel P, Wheatcroft R, Park R, Stein A (2002) The children of motherswith eating disorders. Clin Child Fam Psychol Rev 5(1):1–19
Ramchandani P, Stein A (2003) The impact of parental psychiatric disor-der on children. BMJ 327(August):242–243
Rasic D, Hajek T, Alda M, Uher R (2013) Risk of mental illness inoffspring of parents with schizophrenia, bipolar disorder and majordepressive disorder: a meta-analysis of family high-risk studies.Compr Psychiatry 54:e34–e40. https://doi.org/10.1016/j.comppsych.2013.07.057
Reba-Harrelson L, Von Holle A, Hamer RM, Torgersen L, Reichborn-Kjennerud T, Bulik CM (2010) Patterns of maternal feeding andchild eating associated with eating disorders in the Norwegian moth-er and child cohort study (MoBa). Eat Behav 11(1):54–61
Sadeh-Sharvit, S., Levy-Shiff, R., & Lock, J. D. (2016a). Maternal eatingdisorder history and toddlers' neurodevelopmental outcomes: Abrief report. Eating Disorders. 24(2):198-205. https://doi.org/10.1080/10640266.2015.1064280
Sadeh-Sharvit S, Levy-Shiff R, Arnow KD, Lock JD (2016b) The inter-actions of mothers with eating disorders with their toddlers: identi-fying broader risk factors. Attach Hum Dev 18(4):418–428. https://doi.org/10.1080/14616734.2016.1164201
M. G. Martini et al.466

Saltzman JA, Pineros-Leano M, Liechty JM, Bost KK, Fiese BH,Harrison K et al (2016) Eating, feeding, and feeling: emotional re-sponsiveness mediates longitudinal associations between maternalbinge eating, feeding practices, and child weight. Int J Behav NutrPhys Act 13(1):1–14. https://doi.org/10.1186/s12966-016-0415-5
Shiner RL, Buss KA, Mcclowry SG, Putnam SP, Saudino KJ, Zentner M(2012) What is temperament now? Assessing progress temperamentresearch on the twenty-fifth anniversary of Goldsmith et al. ChildDev Perspect 6(4):436–444. https://doi.org/10.1111/j.1750-8606.2012.00254.x
Siegenthaler E, Munder T, Egger M (2012) Effect of preventive interven-tions in mentally ill parents on the mental health of the offspring:systematic review and meta-analysis. JAAC 51(1):8–17. https://doi.org/10.1016/j.jaac.2011.10.018
Silva, G., Costa, K., & Giugliani, E. (2016). Infant feeding: Beyond thenutritional aspects. Jornal de Pediatria (Rio J) 92(3):S2-S7. https://doi.org/10.1016/j.jped.2016.02.006
Solmi F, Mascarell MC, Zammit S, Kirkbride JB, Lewis G (2019)Polygenic risk for schizophrenia, disordered eating behaviours andbody mass index in adolescents. Br J Psychiatry 3(December 1992):1–6. https://doi.org/10.1192/bjp.2019.39
Stein A,Woolley H, Cooper S, Fairburn C (1994) An observational studyof mothers with eating disorders and their infants. J Child PsycholPsychiatry Allied Discip 35(4):733–748
Stein A,Woolley H,McPherson K (1999) Conflict between mothers witheating disorders and their infants during mealtimes. Br J Psychiatry175:455
Torgersen L, Ystrom E, Haugen M, Meltzer HM, Von Holle A, Berg CKet al (2010) Breastfeeding practice in mothers with eating disorders.Mater Child Nutr 6(3):243–252. https://doi.org/10.1111/j.1740-8709.2009.00208.x
Torgersen L, YstromE, Siega-Riz AM, Berg CK, Zerwas SC, Reichborn-Kjennerud T, Bulik CM (2015) Maternal eating disorder and infantdiet. A latent class analysis based on the Norwegian mother andchild cohort study (MoBa). Appetite 84:291–298. https://doi.org/10.1016/j.appet.2014.10.009
Watson HJ, O’Brien A, Sadeh-Sharvit S (2018) Children of parents witheating disorders. Curr Psychiatry Rep 20(11):101. https://doi.org/10.1007/s11920-018-0970-3
Waugh E, Bulik CM (1999) Offspring of women with eating disorders.Int J Eating Disord 25(2):123–133
Westwood H, Stahl D, Mandy W, Tchanturia K (2016) The set-shiftingprofiles of anorexia nervosa and autism spectrum disorder using theWisconsin card sorting test: a systematic review and meta-analysis.Psychol Med 46:1809–1827. ht tps: / /doi .org/10.1017/S0033291716000581
Whelan E, Cooper PJ (2000) The association between childhood feedingproblems and maternal eating disorder: a community study. PsycholMed 30:69–77
Yilmaz Z, HalvorsenM, Bryois J, et al. (2018). EatingDisordersWorkingGroup of the Psychiatric Genomics Consortium, TouretteSyndrome/Obsessive–Compulsive Disorder Working Group of thePsychiatric Genomics Consortium. Examination of the shared ge-netic basis of anorexia nervosa and obsessive-compulsive disorder.Mol Psychiatry. https://doi.org/10.1038/s41380-018-0115-4
Zerwas S, VonHolle A, Torgersen L, Reichborn-kjennerud T, StoltenbergC, Bulik CM (2012) Maternal eating disorders and infant tempera-ment: findings from the Norwegian mother and child cohort study.Int J Eat Disord 45:546–555. https://doi.org/10.1002/eat.20983
Publisher’s note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.
Eating disorders mothers and their children: a systematic review of the literature 467