Coping with loss and changing eating behaviours following bariatric surgery AUGIS September 2010.
13
Coping with loss and changing eating behaviours following bariatric surgery AUGIS September 2010
-
Upload
loraine-powers -
Category
Documents
-
view
222 -
download
0
Transcript of Coping with loss and changing eating behaviours following bariatric surgery AUGIS September 2010.

Coping with loss and changing eating behaviours following bariatric surgery
AUGIS September 2010

Surgery is No Panacea It is well documented that there are certain variables which
determine the results of bariatric surgery. In fact some go as far as to say that it is one’s ability to maintain changes that leads to permanent weight loss after surgery rather than the quality of the procedure. (Niego 2007).
By determining which variables effect the weight loss outcomes we can work towards supporting individuals who have undergone surgery to enable them to achieve their weight loss goals.
If we can establish how the individual deal with changing their behaviours we can tailor our practise to meet their needs (Canetti 2009).

Model of change
The Transtheoretical Model, Prochaska and DiClemente (1983)
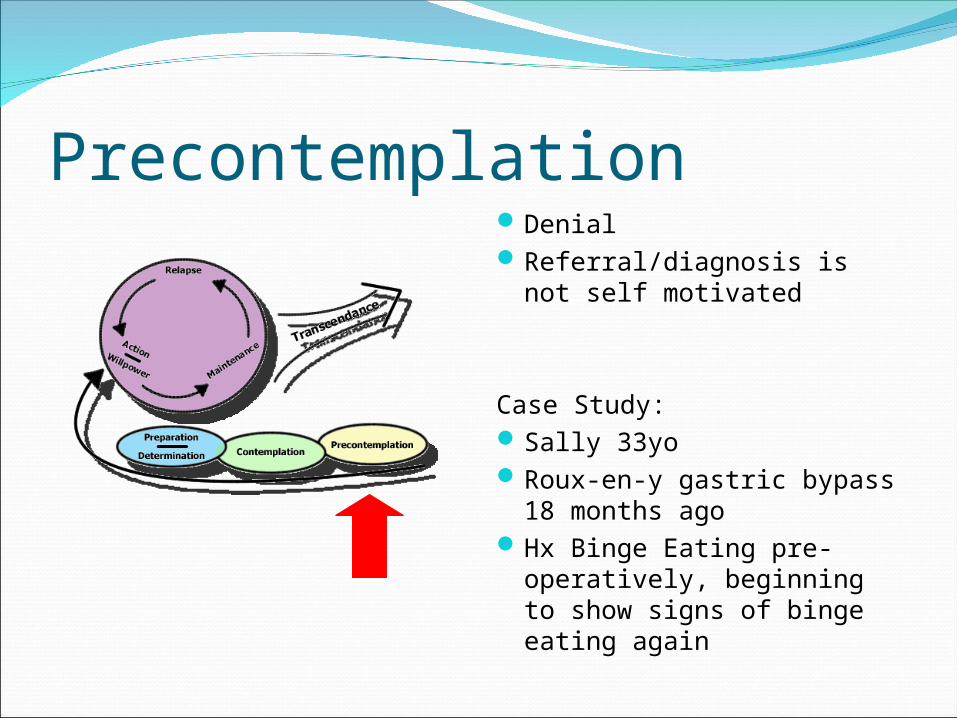
Precontemplation Denial
Referral/diagnosis is not self motivated
Case Study:Sally 33yoRoux-en-y gastric bypass
18 months agoHx Binge Eating pre-
operatively, beginning to show signs of binge eating again

Definitions of Binge EatingA binge occurs when a food addict consumes a greater
than average amount of food in a specific amount of time. (Greater than average will vary from person to person)
A disorder characterised by repeated episodes of excessive eating (over longer than 6 months) such that the binging does not stop until the person is uncomfortably full.
Binge eating disorder is characterised by a loss of control over eating behaviours. The binge eater consumes unnaturally large amounts of food in a short time period.

ContemplationSelf initiated referralStarting to considered
there is an issueEvent/incidentPotential to stop here and
relapseRecognising lack of control
Barriers: socioeconomics, culture, education, understanding.
Consider- is individual aware that effort is needed? Consider health beliefs.
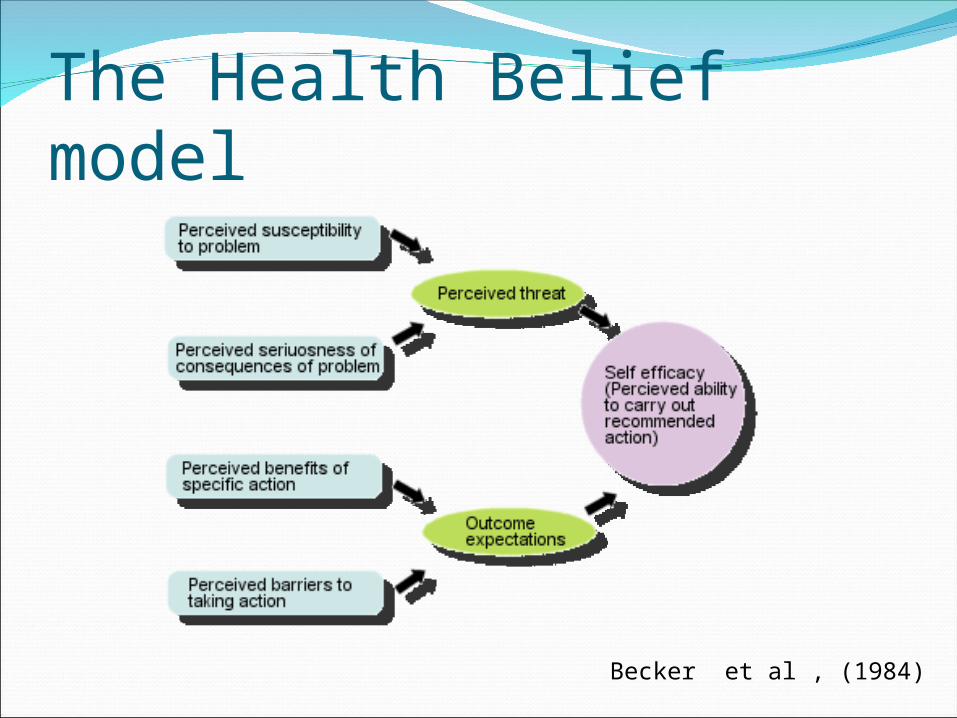
The Health Belief model
Becker et al , (1984)

PreparationWhat to do about it?Forming plansSeek professional help,
WW/SW, fad diets, counselling, CBT, hypnosis
Has self awareness- does the individual have ability to change awareness into action?
Starting to feel in control

ActionStart making changesMotivatedFeels in controlStarting to see results
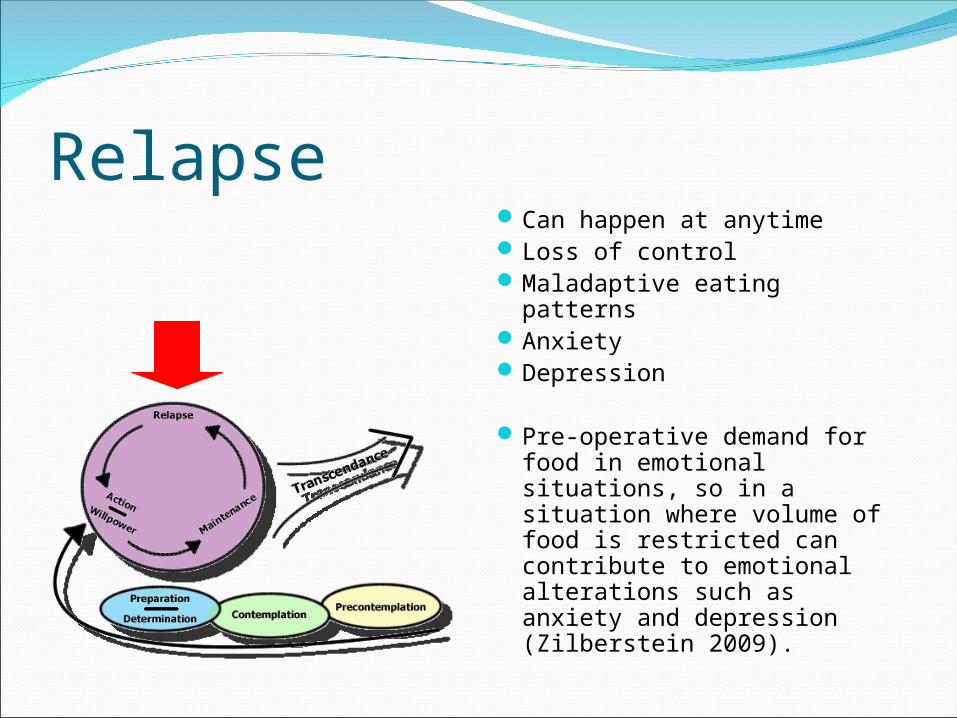
RelapseCan happen at anytimeLoss of controlMaladaptive eating patternsAnxietyDepression
Pre-operative demand for food in emotional situations, so in a situation where volume of food is restricted can contribute to emotional alterations such as anxiety and depression (Zilberstein 2009).

Weight regain Related to inability to change habits rather than surgery.
“I Expected that it would become easier to choose what to eat; that I would be able to choose the sandwich instead of the chocolate… I thought that I would be able to manage it easily…”
(Zijlstra et al 2008)“I know I should be eating those tiny meals but my brain actually wants to eat more- I miss big meals…”
Sally 2010
Consider contemplation and health beliefs;When interviewing individuals who have undergone WLS yes/no answers
46% feel they could loose weight if they change eating behaviours (54% don’t!)
17% feel exercise will help them to loose weight, 83% don’t.(Pinto 2009)
These statistics illustrate sensations of lack of control and self efficacy.

Implication for practiceTo improve treatment we must identify
variables which predict weight loss outcomes.
Model of change helps provide a theoretical insight into the change process and may help to facilitate customised programmes so individuals with disordered eating are not necessarily discounted for surgery (Gorin and Raftopoulos 2008).
ReferencesCanetti L et al. Psychosocial Preditors of Weight Loss and Psychological Adjustment
Following Bariatric Surgery and a Weight Loss Programme: The Mediating Role of Emotional Eating. International Journal of Eating Disorders. 2009. 42:2 109-117
Chesler B, et al. Implications of Emotional Eating Beliefs and Reactance to Dietary Advice for the Treatment of Emotional Eating and Outcome Following Roux-en-y Gastric Bypass: A Case Report. Clinical Case Studies. 2009 8:277-295
Gorin A, Raftopoulos. Effect of Mood and Eating Disorders on the Short Term Outcome of Laparoscopic Roux-en-y Gastric Bypass. Obesity Surgery. 2008. 19:1685-1690
Janz N, Becker M. The health Belief model: A Decade Later. Health Education Quarterly. 1984. 11: 1-47
Madan A, Beech B, Tichansky D. Eating patterns in Patients undergoing Bariatric Surgery. Conference Abstract. 2009.
Niego S et al. Binge Eating in the Bariatric Surgery Population: A Review of the Literature. International Journal of Eating Disorders. 2007. 40:4 349- 359.
Pinto L et al. Study of Factors Related to the Regaining of Weight in Patients Submitted to Bariatric Surgery. Conference Abstract 2009
Rusch M, Andris D. maladaptive eating Patterns after weight loss surgery. Nutrition in Clinical Practise. 2007. 22:41-44.
Zilberstein B et al. Compulsive Behaviour After Bariatric Surgery. Conference Abstract. 2009
Zjlstra H et al. Patient’s Explanations for Unsuccessful Weight Loss After Laparoscopic Adjustable Gastric Banding. Patient Education and Counselling. 2009. 75 108-113.