Early Implementers Workshop 23rd March 2016
163
www.england.nhs.uk 23 rd March 2016 10.30am – 3.30pm WELCOME! LtC Year of Care Commissioning EIS and LTC Community of Practice Workshop
-
Upload
nhs-improving-quality -
Category
Healthcare
-
view
558 -
download
1
Transcript of Early Implementers Workshop 23rd March 2016

www.england.nhs.uk
23rd March 201610.30am – 3.30pm
WELCOME!
LtC Year of Care CommissioningEIS and LTC Community of
Practice Workshop

www.england.nhs.uk
• National context• Integrated intelligence – Kent• Use of the linked data - Leeds• Health 1000 – BHR• LTC animations
Introductions and outline of today:

www.england.nhs.uk
• To understand national context and thinking around LTC care
for the future
• To hear and learn from LTC YoC Commissioning Programme
EIS around key achievements as at end national programme
• To develop local thinking for 1617 and beyond
• To network and share knowledge
• To contribute to the development of the LTC framework
animations card game
Learning Outcomes:

www.england.nhs.uk
National Update
Julie Renfrew

www.england.nhs.uk
• 4 year national programme 2012 to 2016
• Lots of learning shared
• NOT the end of the work
• Close of the proof of concept stage - transition now
to mainstreaming.
• EIS plans / work in 15/16 to embed YOC
Commissioning outputs into operational processes
Long Term Conditions Year of Care Commissioning Programme

www.england.nhs.uk
LTC Framework
Commitment to Carers
Frailty
Health AgeingGuide
Fire Service as an asset
Care Homes Quick Guides
Care & Support Planning
Navigating Health& Social Care
Self Care
Ambitions for End of Life Care
Our Declaration
Delivery Models
Planning for Change:• Capitated Budget• Contracting• Simulation Modelling
Patient and Service Selection
Planning for Change:Workforce
Whole Population Analysis;Understanding your population
LTC Dashboard LTC Toolkit

www.england.nhs.uk
Long term conditions resources
Simulation modelUnbundling recovery simulation model

www.england.nhs.uk
7
Using behavioural change to open
minds
o Make a declaration at www.engage.england.nhs.uk/survey/ltc-declaration
o Tell your teams about our worko Encourage them to make a declarationo Ask them to feed back thoughts and
ideaso Use our hashtag – #A4PCC – when
you see work that is relevant to person-centred care for people with LTCs
o Let us know of any events, activities or social media opportunities that we can join forces with you
#A4PCC – Action for Person-Centred Care
Person with long term
condition

www.england.nhs.uk
National Context and Perspective for 2016/17
Jacquie WhiteNHSE

www.england.nhs.uk
LTC care for the future: Person Centred Co-ordinated CareJacquie White
Deputy Director - Long Term Conditions, Older People and End of Life Care Clinical Policy & Strategy TeamNHS England
23rd March 2016

www.england.nhs.uk
Opening thought
The good physician treats the disease; the great physician treats the patient who has the disease.
William Osler - 1800s
11

www.england.nhs.uk
What’s the diagnosis?

www.england.nhs.uk 13
1mPeople with frailty
10mPeople have two
or more LTCs
0.5mAt end of life
16mPeople have one
LTC
Long term conditions: some facts

www.england.nhs.uk 14
0.01%average no. hours
per year spent with health
professional 33%70%health budget
spent on LTCs
3.2%of people with LTCs
have a care plan
Long term conditions: some facts
of GP consultations are with people with multi
LTCs

www.england.nhs.uk 15
50 50
96 4
50% of total emergency beds days for over 75s
4% over 65s in care home with 14% total emergency admissions for over 65s
2570 25% of hospital beds occupied by someone dying
Three-fold increase in cost of health care with frailty
Long term conditions: some facts

www.england.nhs.uk
Long term conditions: some facts
16
1 in 9
Nearly 1 in 2(46%)
said they had fallen ill but just had to continue caring
£1bn in Carer’s Allowance goes unclaimed each year
said the person they cared for had emergency admission or social services while the carer recovered from illness

www.england.nhs.uk
People living longer but not always well
The larger the number of co-morbidities a patient has, the lower their quality of life
Increasing evidence on over-treatment and harm
Social isolation/loneliness a risk factor for mortality in over 75s and should be supported as a co-morbidity
And…
01/05/2023

www.england.nhs.uk
Wellbeing is about more than just medically managing a condition
It’s about thriving not just survivingIt’s an ethical, social and financial issueShared decision-making is key We need to take support people to self-
care, feel in control No one knows more about their
condition than the patient
Navigating health and care: Living independently with long term conditions, an ethnographic evaluation • http://
www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions-and-integrated-care/navigating-health-and-care.aspx
18
Why does it matter to people with LTCs?

www.england.nhs.uk
• More activated patients have 8% lower costs in the base year and 21% lower costs in the following year than less activated patients
• Health coaching can yield a 63% cost saving from reduced clinical time, giving a potential annual saving of £12,438 per FTE from a training cost of £400
• Coaching and care co-ordination has shown to reduce emergency admissions by 24%
• Social prescribing can reduce emergency admissions by 11%• Timely physiotherapy for people with MSK conditions can save £1.50 for every
£1 invested• Community-based neurological care models could save the NHS £369,286 per
patient over 10 years• Improved medication adherence for instance in 6000 adults in the UK with Cystic
Fibrosis, could save more than £100 million over a 5-year timescale• Proactive case finding, frailty assessment, care planning and targeted
intervention could prevent between 20% and 30% of hospital admissions in over 85’s
• Areas that have implemented EPaCCs* see an increase in home deaths and annual savings of £35,910 per 200,000 population
*Electronic Palliative Care Co-ordination system19
Benefits to all

www.england.nhs.uk
The “treatment”

www.england.nhs.uk
Person centred coordinated care“My care is planned with people who work together to understand me and my carer(s), put me in control, co-ordinate and deliver services to achieve my best outcomes”
Goal:
Improve quality of life and experience of end of life care for people with Long Term Conditions and their carers through:
21

www.england.nhs.uk
Framing delivery….LTC Framework:
Empowered patient and carersProfessional collaborationBest Practice (clinical and organisational)Commissioning
Delivering Person Centred Co-ordinated Care Cf: ‘Roadmap for Strengthening people-centred health systems in the WHO European Region: A Framework for Action towards Coordinated/Integrated Health Services Delivery (CIHSD)’ (WHO 2013)

www.england.nhs.uk
The Framework
23
Organisational & Clinical Processes
Informed and engaged patients and carers
Health & Care Professionals committed to
partnership working
Commissioning
• Information and technology
• Case finding & risk stratification
• Guidelines, evidence and national audits
• Self Management• Patient activation• Health literacy• Group and Peer
Support• Care Planning• Carer support• 3rd sector support• Community
mobilisation
• Integration of services
• Multi Disciplinary Teams
• Health coaching• Clinical activation• Workforce
development• Care Co-ordination
• Place based approach to needs assessment and planning
• Joint Commissioning • Joint funding (BCF,
shared risk and reward)
• Metrics and Evaluation
• Service User and Public Involvement
Key factors needed to deliver Person Centred Coordinated Care and that are being supported nationally:

www.england.nhs.uk
The “review”
24

www.england.nhs.uk
The LTC Year of Care journeyNational
initiatives (pre 2012
)
Health &
Social Care Act
(2012)
National
Collaboration for integrated care
(2013)
Person
centred co-
ordinated care: LTC
framework (2013
)
Five year forwa
rd view 5YFV (201
4)
Post
election (2015)
Integration
pilots, Community
Matrons, Self management, Techno
logy, PHB, LTC Year
of Care
Commissioni
ng Programme
“Duty”, New
organisations, roles and
responsibilitie
s – Local, Nation
al
National
support –
Narrative,
definition,
Better care fund,
Integration
pioneers
Permissive
framework for
local implementatio
n – House
of Care
Clarity of
vision, prioriti
es, new
national
programmes: “new
models of
care”, “integrated
personal
commissionin
g”
LTCs embedded in
all programmes, Self-care
priority, STPs
25
LTC Year
of Care: Development year and site
selection
LTC Year
of Care:
1st year – experimentation to define scope
LTC Year
of Care:
2nd year –techni
cal phase (data and
analysis)
LTC Year
of Care:
2nd year –techni
cal phase (data and
analysis
LTC Year
of Care:
3rd year – development
of curren
cies and new
delivery
models
LTC Year
of Care:
4th year – implement
currencies,
testing deliver
y models and
capitated
budgets.

www.england.nhs.uk 26
Celebrating success

www.england.nhs.uk
Sharing the LTC YoC learning
27
1. Handbook and case studies:• Leadership and engagement• Co-production• Whole population diagnostic• Patient & Service Selection• Delivery Models• Defining and managing a budget• Contracting and performance monitoring

www.england.nhs.uk 28
2. Communication and promotion:• Nationally & Internationally• Presentations, articles, social media
3. Supporting other programmes/initiatives:• STPs, Vanguards, IPCs, Maternity review etc
4. EIS roles:• Local sharing and input into wider plans• 6 – 12 months f/u• What else?

www.england.nhs.uk
Continuing to implement and push the boundaries
29

www.england.nhs.uk
And finally - the world we operate in…
30
I can't change the direction of the wind, but I can adjust my sails to
always reach my destination.
Jimmy Dean

www.england.nhs.uk
@jaqwhite1#A4PCC
www.england.nhs.uk/resources/resources-for-ccgs/out-frwrk/dom-2/
31
Thank you

www.england.nhs.uk
Working in partnership across Kent developing integrated intelligence
Kent LTC YOC Commissioning EIS

Year of Care Early Implementer Workshop23rd March 2016
Kent Long Term Conditions Year of Care Commissioning Programme

Content
1. Public Health leading the informatics dimension using their statutory powers – Abraham George
2. The Kent approach to linking data, and identifying YOC patients– Pete Gough
3. The programme structure – for post Year of Care – Abraham George
4. Data Quality Improvement – Tom Bourne
5. Using the linked dataset for Matched Cohort studies – e.g. Home Safety Visits – Abraham George, James Finch (Kent Fire and Rescue)

1. Using Public Health Powers
Abraham George, Consultant in Public Health

Context - Local Profile of Kent
• >1.5 million population www.kpho.org.uk • Health and care service planning at multiple levels • Public Health Intelligence works closely with local data
warehouse team that collates and link data from >100 health and care providers
• Kent LTC YOC programme – Year 4 out of 4• 1 of 5 national early implementer sites• Part of national Integration initiatives eg. Pioneer, Vanguard,
Integrated Personal Commissioning etc.• Kent whole population dataset analyses examining impact of
multi-morbidity on health and care service activity and costs.

Public Health Statutory Powers• Health and Social Care Act 2012 - Councils have a statutory responsibility for improving the
health of their citizens and for providing local public health services • Includes a duty to take appropriate steps to improve the public health of people in our area -
include carrying out research, providing information, advice and facilities for the prevention and treatment of illness and providing incentives to encourage the adoption of healthy lifestyles. We also seek to minimise health risks to individuals arising from poor accommodation, environment or other factors.
• Public Health has a statutory right to access and use your confidential information, but only does so when absolutely necessary e.g.
– Organising the National Child Measurement Programme;– Organising the NHS Health Check Programme;– Organising and supporting the 0-5 health service and school nursing services;
• Statistics and intelligence are gathered about health and social care in order to meet our statutory duties to produce:
– Director of Public Health’s Annual Report;– Joint Strategic Needs Assessment; (Care Act 2014)– Health and Wellbeing Strategy;
• We have a statutory responsibility to assess risks to public health arising from inequalities in health care provision, poor quality or inappropriate housing, lifestyles, education and employment, communicable diseases, chemicals, poisons, radiation and environmental health hazards.
• Public Health are also supporting CCG’s with regard to Section 3 NHS Act 2006 Under section 3(1), a CCG must arrange for the provision of certain specified health services to such extent as it considers necessary to meet the reasonable requirements of the persons for whom it has responsibility.

Why public health?
• Statutory powers• Located in council• Central position covering all CCG areas• Informatics expertise• Health intelligence expertise• JSNA

Legal ways to link data
Four choices for sharing confidential data about groups and populations:
• Consent (will generally need to be explicit rather than implied)
• HSCIC power • Support under s251 Regulations• Anonymised/pseudonymised data
39

Pseudonymisation Options
Option 1: Pseudonymisation at Source (no re-identification);Option 2: Pseudonymisation at Source (variation using Public and Private Key);Option 3: Pseudonymisation on Landing;Option 4: Full Consent;Option 5: Section 251 application to the CAG;Option 6: Department of Health issued directions to HSCIC (and therefore DSCROs);Option 7: A mix of the above (e.g. Southend-on-Sea).

Key Challenges1. Information Governance
– Current approach to data sharing has been difficult – different expert opinions on how to share / link data
2. Data quality and accessibility– Good support from provider organisations– Quality / completeness of data variables across
different organisations
3. Commissioner buy-in

Key Successes 1. Establishment of partnerships 2. Range of analytical projects to support commissioners
respond to national direction on payment systems3. Enhanced data quality discussions with providers
(prompted by analysis of linked dataset)4. Generation of research and development opportunities
with academia (PSSRU & Farr institute) 5. Raising awareness of informatics within local authority 6. Exploring new applications of linked datasets (e.g.
systems modelling)

2. The Kent approach to linking data, and identifying YOC patients
Pete Gough, HISbi manager

Defining MethodologyIdentify Year of Care Patient Cohort
Risk Strat Band 1 or 2 (top 5% of popn)Rising Risk score –
Rapid – 3 consecutive rises (15 points overall)Gradual – 4 rises in 6 months
Age 18 or over2 or more of QOF LTCs (from GP data)Remain in for minimum 6 monthsFlagged as B,C,D,E depending on number of LTCs

Defining MethodologyHow to create main dataset
Key is to link data at a patient levelNeed common identifier – NHS NumberAlso need to keep data pseudonymousTHIS WAS A PROBLEM!!!!A REAL PROBLEMTook 6 months to solve

Defining MethodologySolution:
Need method for organisations to flow data into dataset pseudonymised but flag as YoCSQL Hashing Tool – via SQL Server directly or via excel add inTwo numbers never exist in same place – pseudonymisation happens in transit

Defining MethodologyNow have a way of linking all datasets by patient without knowing who they were or being able to link to any other dataset
There was much rejoicing


3. Programme structure for post–Year of Care
Abraham George, Consultant in Public Health

Implementing Integrated Payments
LinkedDataset
HISbiProviders
Change Management, Engagement, Governance
Programme Management
Data Quality
PH
InformaticsAnalysis
PH
Model of Care
ImplementPayment
Arrangements
Contracts
Design ofPayment System

Flow of data into the Kent Integrated DatasetGP practice Mental
healthOut of hours
Acute hospital
HospiceAdult social care
Ambulance service
KENT INTEGRATED DATASET
Kent County Council Public Health and HISBI data warehouse
Community health
Public health
KID minimum dataset: data on activity, cost, service/treatment received, staffing, commissioning and providing organisation, patient diagnosis, demographics and location.
Datasets linked on a common patient identifier (NHS number) and pseudonymised
Arrangements are in progress to link to data covering other services, including: Health and social care services: Children’s social care, child and adolescent mental health, improving access to psychological therapies, and non-SUS-reported acute care. Non-health and social care services: District council, HM Prisons, Fire and Rescue, Probation, and Education.

C
KENT INTEGRATED DATASET
Ongoing data quality improvement efforts, to ensure data is of sufficient quality to support new payment systems and decisions on service reconfiguration
1. CAPITATED BUDGETS 2. SYSTEM MODELLING 3. EVALUATION
1. Select Cohort/ population
2. Select services
3. Set the price
4. Financial risk mitigation5. Payment cash flows6. Gain/loss agreements7. Quality/outcome measures
1. Generating evidence-based assumptions to support systems modelling
2. Quality assuring and refining existing models
Activity
Finance
Staffing Estates
Quality and safety
Contract model
1. Evaluation of commissioned services.
2. Attempts to identify the economy, efficiency and effectiveness of individual services.
3. Assessing the relative benefit of services compared to one another.
Utility of the Kent Integrated Dataset

4. Data Quality Improvement
Tom Bourne, Senior Analyst

C
KENT INTEGRATED DATASET
Ongoing data quality improvement efforts, to ensure data is of sufficient quality to support new payment systems and decisions on service reconfiguration
1. CAPITATED BUDGETS 2. SYSTEM MODELLING 3. EVALUATION
1. Select Cohort/ population
2. Select services
3. Set the price
4. Financial risk mitigation5. Payment cash flows6. Gain/loss agreements7. Quality/outcome measures
1. Generating evidence-based assumptions to support systems modelling
2. Quality assuring and refining existing models
Activity
Finance
Staffing Estates
Quality and safety
Contract model
1. Evaluation of commissioned services.
2. Attempts to identify the economy, efficiency and effectiveness of individual services.
3. Assessing the relative benefit of services compared to one another.
Utility of the Kent Integrated Dataset

Why invest resource in data quality?
• The Kent Integrated Dataset (the KID) will serve at least 3 important purposes:
1. To generate budgets for integrated care services
2. To evaluate complex care models (and interventions)
3. To generate assumptions to support systems modelling
• Whether service providers, commissioners, and finance managers will accept the KID’s evidence will depend on the assurances we can give on data quality.
• Or, put more positively, data quality can give service providers the confidence to change services or payment systems for the benefit of patients
Context

Data quality efforts
Recording and prioritising
gaps
1. Formal data reconciliation exercise
with East Kent Federation of CCGs
2. Data quality clauses in CCG commissioning
contracts (working with CSU)
3. Informal data quality discussions with providers via Kent Wide Finance and
Informatics Group (supported by data quality
dashboard)
4. Working with University of Kent to establish
whether the cost and activity data we hold is of
sufficient quality to support new payment models5. Compiling a
comprehensive data dictionary
Data quality improvement plan

Data quality efforts
Recording and prioritising
gaps
1. Formal data reconciliation exercise
with East Kent Federation of CCGs
2. Data quality clauses in CCG commissioning
contracts (working with CSU)
3. Informal data quality discussions with providers via Kent Wide Finance and
Informatics Group (supported by data quality
dashboard)
4. Working with University of Kent to establish
whether the cost and activity data we hold is of
sufficient quality to support new payment models5. Compiling a
comprehensive data dictionary
Data quality improvement plan
Q, Do we have sufficient cost and activity data to support the development of new payment systems?

Data reconciliation templates

Data quality efforts
Recording and prioritising
gaps
1. Formal data reconciliation exercise
with East Kent Federation of CCGs
2. Data quality clauses in CCG commissioning
contracts (working with CSU)
3. Informal data quality discussions with providers via Kent Wide Finance and
Informatics Group (supported by data quality
dashboard)
4. Working with University of Kent to establish
whether the cost and activity data we hold is of
sufficient quality to support new payment models5. Compiling a
comprehensive data dictionary
Data quality improvement plan
Q, Is the quality of our data stable over time?

Data quality dashboard1. This first version of the dashboard concentrates on the completeness and longitudinal stability of the key data
fields and aims to introduce an element of competition around compliance by providers and CCGs.
2. We are now discussing ‘fatal quality thresholds’. On stability, this could be set at 5%, meaning that if in one month we received a dataset with only 94% of the number of records received from a data provider in the previous month, then this would be flagged for further discussion.

Data quality efforts
Recording and prioritising
gaps
1. Formal data reconciliation exercise
with East Kent Federation of CCGs
2. Data quality clauses in CCG commissioning
contracts (working with CSU)
3. Informal data quality discussions with providers via Kent Wide Finance and
Informatics Group (supported by data quality
dashboard)
4. Working with University of Kent to establish
whether the cost and activity data we hold is of
sufficient quality to support new payment models5. Compiling a
comprehensive data dictionary
Data quality improvement plan
Q, Do we have sufficient data to support new payment models?

PSSRU work- regression model to identify drivers of average total cost
Multi-morbidity
Age
Sex
Risk score(& previous use)
Controlling for practice led variation
Average Total Cost (ATC)
PredictorsExplaining up to a third of the
variation in ATC
Q, Can we use these drivers to segment the population into cohorts to build tariffs?
£1,014 across all population
£1,708 across just service users

PSSRU work - quantify likely uncertainty/tolerance
£1,500- 1SD- £200
+ 1SD + £200
Q, Will average costs produced from the dataset be sound predictors of future prices to support risk sharing decisions?

Data quality efforts
Recording and prioritising
gaps
1. Formal data reconciliation exercise
with East Kent Federation of CCGs
2. Data quality clauses in CCG commissioning
contracts (working with CSU)
3. Informal data quality discussions with providers via Kent Wide Finance and
Informatics Group (supported by data quality
dashboard)
4. Working with University of Kent to establish
whether the cost and activity data we hold is of
sufficient quality to support new payment models5. Compiling a
comprehensive data dictionary
Data quality improvement plan
Q, What have we learnt to date?

GP practices: need to focus efforts on West of the county (and better understand any bias introduced by ‘patchy’ coverage)
14 of 19 flowing
15 of 17 flowing
18 of 21 flowing
19 of 29 flowing
34 of 34 flowing
20 of 61 flowing
8 of 14 flowing
Also need better assurance over the quality of GP read coding, which we are using to define LTCs

High cost
drugs
GP prescri
bing data
Maternity
(non-deliver
y)
Pathology
Sexual health
For some we have been able to develop a plan to bring in
Some we are unlikely to ever get
For some datasets, the impact is large, and the ‘fix’ complicated, so we will need to develop temporary mitigation strategies and communicate approximate nature
There are several healthcare activities, accounting for significant chunks of expenditure, on which we are not yet capturing data
However, we are reasonably confident we can ‘account’ for this expenditure (known unknown) and must now prioritise sourcing this data and bringing it into our dataset.

Data quality efforts
Recording and prioritising
gaps
1. Formal data reconciliation exercise
with East Kent Federation of CCGs
2. Data quality clauses in CCG commissioning
contracts (working with CSU)
3. Informal data quality discussions with providers via Kent Wide Finance and
Informatics Group (supported by data quality
dashboard)
4. Working with University of Kent to establish
whether the cost and activity data we hold is of
sufficient quality to support new payment models5. Compiling a
comprehensive data dictionary
Data quality improvement plan

Data quality improvement planQuality dimension Research ready? (1-10)Accuracy 5
Timeliness and punctuality 10
Accessibility and clarity 2
Comparability: geographic 6Comparability: other units of healthcare 7
Comparability: over time 7Coherence Yet to be scoredRelevance 6Additional: External comparison Yet to be scored
Additional: Uniqueness 7Additional: Engagement of data providers 9
Additional: Engagemenf of data users 5 (and rising)

5. Matched Cohort Studies
Gerrard Abi-Aad and James Finch

Matched cohort analysis of Kent Fire and Rescue Home Safety Visit Data
Gerrard Abi-Aad, Head of Health Intelligence, Kent County Council
Version: 01Last updated: March 2016

71
Background
Increased interest in exploring the ‘hidden’ benefits of public services – fiscal constraints coupled with a recognition of the need for improved cross sectoral joint action. Kent Integrated Dataset – enhanced opportunity to evaluate ‘hidden impacts’ through data linkage techniques and advanced analytics

72
Identification of the final ‘Intervention’ cohort
KFRS – HSV data
Kent Patient Master Index (March 2015)
Individuals requesting and receiving a HSV(30,601, 01 April 2012 to 31 March 2015)
Initial NHS number
matching
11,377 / 30,089 (37.8%)
2nd stage matching to identify householders
Final intervention cohort HSV (requesters
+ ‘presumed’ occupants) 27,021* (15,644 +
11,377)*165 patients were removed due to further data quality
issues resulting in a final cohort of 26,856

73
Identification of the final ‘Control’ cohort
Presentation title, Month Year
Age
Index of Multiple Deprivation (LSOA)
Gender
A&E attendance date (01 April 2012 to 31 March 2015
SUS – A&E (Kent residents only)
(>500,000 cases)

74
Findings_1Of the 26,856 KFRS subjects identified, 7,478 (28%) were found to have attended A&E during the period 01 April 2012 to 30 September 2015. Of these, 4859 (65%) attended once only whereas 2,619 (35%) attended on two or more occasions. In total the 7,478 KFRS subjects ‘generated’ a total of 12,178 A&E attendances. The subject to attendance ratio for this group was 1.63 attendances per person on average.
Presentation title, Month Year

75
Findings_2The 7,478 subjects included in the analysis were case matched to 9,588 (128.2%) ‘control’ subjects in the A&E attendance dataset. Of these, 8,874 (93%) attended once only whereas 714 (7.4%) attended on two or more occasions. In total the 9,588 control subjects ‘generated’ a total of 10,443 A&E attendances. The subject to attendance ratio for this group was 1.1.
Presentation title, Month Year

76
Findings_3
Non parametric tests were used to assess whether or not the proportional distribution in A&E attendances differed between the control and the intervention groups. A two-way analysis of variance by ranks revealed no significant differences between both groups (p=.180).
Presentation title, Month Year

77
ConclusionsThe apparent lack of association between HSV and reduction in A&E utilisation is not necessarily indicative of absence of impact.Requirement for a more nuanced case control matching framework required but perhaps not possible? (A&E attendance for effects of inhalation?)Absence of a dynamic PMI may have introduced systematic bias (difficult to determine the scope of any potential bias)Perhaps most significantly, the high initial miss-match rate (62.2%) may have introduced further unhelpful bias which impeded a more accurate case control selection process. It has not been possible to assess the underlying reasons for the high miss-match rate?
Presentation title, Month Year

78
Kent Public Health Observatory

79
Thank you!
Presentation title, Month Year
Http://www.kpho.org.uk/

www.england.nhs.uk
Working in partnership across Kent developing integrated intelligence
Questions and discussion

www.england.nhs.uk
Developing integrated data to support service redsign
Leeds LTC YOC Commissioning EIS

Developing integrated data to support service redesign
decision making
Alison Phiri - Business Intelligence ManagerMohini Chauhan - YoC Commissioning Manager

• Developing the data setWhat?
• Review of current Information Assets
• Gap analysis
• Developed Leeds Data Model
• Tailored Leeds Data Model for specific purposes.

What?
Leeds Integrated Health & Social
Care Data Model
Datasets linked on a common patient identifier
GP Practice Data Notional costs assigned
Community Dataset Notional costs assigned
Mental Health Data Cost per unit assigned
Inpatient Data
Adult Social Care Data No costs assigned
Outpatient Data
A&E Data
Year of Care Combined Dataset
ACG Grouper
Linked data processed through
the ACG Grouper to create risk scores
Input Dataset
Used for production of
capitated budgets
Output Dataset
Used for cohort
identification
To be defined
Dataset for shadow
monitoring
Key:

• How did we use the dataset?
So what?
• Cohort identification – pivot table hell!
• Created a tool that enabled us to get the best out of the data

• Introduction to data packs
• Data packs were developed to create an impact and so they could be easily distributed to stakeholders across the system.
• Inspiration taken from commissioning for value data packs.
• A visual and engaging way of presenting data.
• The data packs do not provide the answers to which cohorts should be selected. Their purpose is to generate discussion and to support stakeholders to make a more informed decision around which cohorts they would like to focus on.
Now What?


CASE MANAGEMENT
DISEASE MANAGEMENT
SUPPORTED SELF CARE
POPULATION WIDE PREVENTION
Which populations do we want to target?
Reducing unplanned admissions?
Reducing total costs?
Health outcomes/potential years of life lost (PYLL)?
Multimorbidity?
Age?
Risk of high healthcare utilisation?
Focus on now or the future?
Frailty?

Prevalence of CHD, COPD and Diabetes is higher than the rest of the city Around 40% of the NHS
Leeds South and East CCG population has one or more
LTC
Emergency readmissions are significantly higher than the national averageThe biggest cause of years of life lost is due to cardiovascular disease cancer and respiratory disease
More people have mental health problems than in the rest of the city, above the national average
Health related
quality of life for people
with LTC’s is
significantly lower than the national average
25% of the CCG population have an existing
health problem, which is above the England average
More people are living with 2 or 3 LTC’s, compared to the rest of the city By 18/19 PYLL
to be improved by 26.6%
Please note: the data on this slide was taken from a number of sources including; public health profiles, the LSE CCG 2 year plan, NHS England commissioning for value packs and the NHS England long term condition dashboard.
NHS Leeds South and East CCG

Whole population dataset
Analysis of Leeds city wide data involved testing the following methodologies to understand utilisation of healthcare services, over a two year period:
a. Patients who had three or more A&E attendancesb. All patients aged 85 and over c. All patients with a Frailty Index of seven or more d. All patients with 4 or more long-term conditions e. All patients in the top 2% by risk of unplanned hospitalisation in
the next 12 months (based on the Kings Fund’s Combined Predictive Model algorithm).
The analysis demonstrated an increased use of healthcare services over the subsequent two years when moving from (a) to (e) and points towards a multimorbidity model.

18-34 35-44 45-54 55-64 65-74 75-84 85+0
2000
4000
6000
8000
10000
12000
14000
16000
18000
Number of LTC’s, by age, for people with at least one LTC*
13+
12
11
10
9
87
6
5
4
3
2
1
Age category
Num
ber o
f pat
ient
s
*NHS Leeds South and East CCG

GP
Community
Mental Health
Outpatients
A&E
Inpatients
£0 £5,000,000 £10,000,000 £15,000,000 £20,000,000 £25,000,000 £30,000,000 £35,000,000 £40,000,000 £45,000,000 £50,000,000
£12,297,218
£11,947,166
£6,591,526
£12,381,539
£2,439,706
£43,220,633
Total costs of services, for people with at least one LTC*
Total costs (£)
Serv
ice
area 14%
13%
7%
14%3%
49%
% total costs of services
GP
Community
Mental Health
Outpatients
A&E
Inpatients
*NHS Leeds North CCG

1 2 3 4 5 6 7 8 9 10 11 12 13+ -
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
Total costs of services, by number of LTC’s, for people with at least one LTC*
Inpatient
A&E
Outpatient
Mental Health
Community
GP
Number of LTC/s
Tota
l cos
ts (£
)
*NHS Leeds South and East CCG

1 2 3 4 5 6 7 8 9 10 11 12 13+ -
2,000.00
4,000.00
6,000.00
8,000.00
10,000.00
12,000.00
14,000.00 Average costs of services, by number of LTC’s, for people with at least one LTC*
Inpatient
A&E
Outpatient
Mental Health
Community
GP
Number of LTC/s
Aver
age
cost
s (£
)
*NHS Leeds South and East CCG

Patterns of multimorbidity*
*NHS Leeds West CCG

Ischemic heart diseaseCOPD
Depression(+any other conditions)
1028 people affected of which 47%
are male
Average costs per person, over a one year period £5,399
8.6 average number of LTC’s per person
Total costs, over a one year period £5,550,474
GP costs £439,814
Inpatient costs £3,277,790
A&E costs£199,067
Outpatient costs £438,993
Mental Health costs£155,436
Community costs£1,039,082
*NHS Leeds South and East CCG

18-34 35-44 45-54 55-64 65-69 70-74 75-79 80-84 85+0
50
100
150
200
250
0
10
65
205
153 152
182
150
111
Age split of patients who have IHD, COPD and depression (+any other conditions)*
Age category
Num
ber o
f pat
ient
s
*NHS Leeds South and East CCG

1 2 3 4 5 6 7 8 9 10 11 12 13 14 150
50
100
150
200
250
0 0 1
11
36
119
171
203
153
121112
51
37
103
Numbers of multiple LTC’s for patients with IHD, COPD and depression (+any
other conditions)*
Number of long term conditions
Num
ber o
f pat
ient
s
*NHS Leeds South and East CCG

NHS Leeds South and East CCG

Beeston Chapeltown Kippax Middleton Seacroft0
5000
10000
15000
20000
25000
12472
22856
14955
21171
14757
Neighbourhood teams
Num
ber o
f pat
ient
s
Neighbourhood team breakdown, for patients with at least one LTC*
*NHS Leeds South and East CCG

Leed
s C
ity M
edic
al P
ract
ice
City
Vie
w M
edic
al P
ract
ice
Oak
ley
Med
ical
Pra
ctic
eB
eest
on V
illag
e S
urge
ryS
hafto
n La
ne S
urge
ryC
ottin
gley
Com
mun
ity C
entre
Sha
ftesb
ury
Med
ical
Cen
treLa
ybou
rn &
Par
tner
s Th
e M
edic
al P
ract
ice
Bel
lbro
oke
Sur
gery
Eas
t Par
k M
edic
al C
entre
Gar
den
Sur
gery
Linc
oln
Gre
en M
edic
al P
ract
ice
The
Pra
ctic
e at
Har
ehill
s C
orne
rR
ound
hay
Roa
d S
urge
ryTh
e S
urge
ryY
ork
Stre
etTh
e R
ichm
ond
Med
ical
Cen
treS
hake
spea
re C
omm
unity
Pra
ctic
eA
shto
n V
iew
Con
way
Med
ical
Cen
treG
arfo
rth M
edic
al P
ract
ice
Gib
son
Lane
Pra
ctic
eN
ova
Sco
tiaK
ippa
x H
all
Moo
rfiel
d H
ouse
Rad
shan
Med
ical
Cen
treS
will
ingt
on C
linic
Ling
wel
l Cro
ft S
urge
ryO
ulto
n S
urge
ryLo
fthou
se S
urge
ryN
ew C
ross
Sur
gery
The
Arth
ingt
on M
edic
al C
entre
Whi
tfiel
d P
ract
ice
Mid
dlet
on P
ark
Sur
gery
Hun
slet
Hea
lth C
entre
Col
ton
Mill
Med
ical
Cen
treW
indm
ill H
ealth
Cen
treM
anst
on S
urge
ryP
ark
Edg
e S
urge
ryA
shfie
ld M
edic
al C
entre
The
Fam
ily D
octo
rW
hinm
oor S
urge
ry
Beeston Chapeltown Kippax Middleton Seacroft
0
1000
2000
3000
4000
5000
6000
7000
GP breakdown, by neighbourhood team, for patients with at least one LTC
Neighbourhood team
Num
ber o
f pat
ient
s
*NHS Leeds South and East CCG

102
Coronary heart disease (n= 1801)
Hypertension (n=8267)
Heart failure (n= 1122)
Stroke/ TIA (n= 1009)
Diabetes (n= 2314)
COPD (n= 1283)
Depression (n=8646)
Dementia (n= 399)
1632
1001
789
1766
791
2702
326
533
1001
204
361
277
404
120
279
789
204
242
160
391
143
520
1766
361
242
236
746
86
329
791
277
160
236
510
64
591
2702
404
391
746
510
194
138
326
120
143
86
64
194
1632
533
279
520
329
591
138
Coronary heart disease
Hypertension
Heart failure
Stroke/ TIA
Diabetes
COPD
Depression
Dementia
Multimorbidity analysis at NT level

COPDHypertention
Lipid Metabolism Disorders
Cardiac Arrhythmia
Ischemic Heart Disease
Heart Failure
Peripheral Vascular Disease
Renal Failure
Cerebrovascular Disease
Osteoporosis
Rheumatoid ArthritisEpilepsy
Parkinsons
Multiple Sclerosis
Hypothroidism
Chronic Pancreatitis
Chronic Liver Disease
Cancer
Depression
Bipolar Disorder
Schizophrenia
Dementia and Delirium
-
5,000
10,000
Prevalence of other conditions for pa-tients who have Diabetes (n=10654)*
*NHS Leeds North CCG


I visited my GP 35 times, in the past year
My name is Bob. I suffer from COPD, IHD,
rheumatoid arthritis, high blood pressure, high cholesterol and
depression
The total cost for my healthcare, over the
year, was around £9500
I was admitted to hospital 8 times, which
cost £6000
I was seen by a number of health professionals
and visited the outpatient clinic 19 times
I am between 45-54 years old

Having a care plan will help me feel more
supported to manage my condition
I want to feel more empowered to
manage my condition
Where can I find out about self help courses for people who have long-term conditions?
I want to find out more about my condition. Where are the
best places to do this?
Are there any lifestyle changes I should make to
help my health?
What do our service users say?How do I meet other people
who have the same condition as me? Is there a
local or national support group?I feel I cannot manage my
condition due to lack of information and support
How can I make my condition easier on my family and
friends?



Developing integrated data to support service redesign decision making
Questions and discussion

Health 1000:A local complex care organisation
BHR LTC YOC Commissioning EIS

My services selected by Me
• Introduction
• Technology developed to facilitate “YoC research and Health 1000 provision”
• YoC Research & Cohorts
• Implementation of a Person Centred Provider organisation
• Current Situation – Health 1000 Limited.
Establishing a Complex Care Organisation in East London
Presenter : Rob MeakerDate : 23rd March 2016

Background on the pilot site area in East London
Introduction

East Of England
LAS Station
Central London
Cluster 1
Cluster 2
Cluster 3
Cluster 4
Cluster5
Cluster4
Cluster6
Cluste
r3
Cluster2
Cluster 1
Cluster 1
Cluster 2
Cluster 3
Cluster 4
Cluster 6
Walk In Centre
Cluster 5
Hospital
Geography of the boroughs and key health infrastructure
Borough Population 770,000
Emerging GP federations
Redbridge federation
Havering federation
Barking & Dagenham federation
Introduction

Alignment between YoC and the vision for health and social care in BHR
Introduction

2008 – Polysystems & Person Centred Care
2009 – Risk Stratification
2010 – Integrated data
2011 – LTC management, & The Year of Care
2012 – Integrated Case Management
2013 – Rapid Response & Community Treatment Teams
2014– Complex Primary Care Practice establishment
2015– became operational.
Timeline for person centred care & complex care organsiation
Introduction

Operational January 2015, Core Staff Recruited, Patients No increasing

Ben and Eileen have been married for 59 years. They have four children, nine grandchildren and eighteen great-grandchildren and they also spent fifteen years fostering teenagers. Now, their focus is on enjoying life and their family.Eileen was diagnosed with osteoporosis in 1986, and has had resulting problems with her knees and joints. She overcame breast cancer and she also had a heart attack in 2012. Her husband, Ben, was diagnosed with prostate cancer last year and has a collapsed vertebrae in his back. They had been registered at their previous GP practice for 40 years when they received the call from Health 1000. Staff at the new practice explained that there would be specialists on hand, that they would be able to get an appointment whenever was convenient for them and that they could be looked after in their own home if need be. At first, they weren’t sure if they were doing the right thing by moving practice, but the support they’ve received since joining Health 1000 has left them confident that they’ve made the right decision. For Eileen, the biggest difference is that someone is always on the other end of the phone to help. When calling the practice, she can get straight through to their key worker who is already aware of all their problems and the medication they take. She said: “They’re always informative and eager to help. It feels like they know you personally and they’re interested in your welfare. It makes you feel more confident. We haven’t been with Health 1000 very long, but we’ve seen a big improvement.” The emotional support that they receive from Health 1000 is as important as the physical care. A while ago, Eileen was worried about her husband’s health. She called the practice and spoke to their doctor, who offered to come out to their home and give him a check-up that same day. She said: “Just offering to get someone to come and see you makes you feel so much better. You might not need it, but you know it’s there. They can make you feel better in yourself just by being there, and you know that they’re taking a real interest. That’s the most important thing.”
Patient case study - Health 1000
Ben and Eileen Eaton
Introduction

Before joining Health 1000, Maurice had been registered with the same GP practice in Barking his entire life. Maurice keeps busy and doesn’t like to take up too much of his doctor’s time, but he has a number of health problems and his GP suggested that he join Health 1000, as doctors there would be able to treat him in a way that would work better for him. Asked for his views on how he’s been treated since joining Health 1000, Maurice said: “I find I’m getting more attention here than at my old practice. Before I was just a number, but here I feel like they really listen to me. It gives me confidence.”Maurice finds it easier to get an appointment to see his doctor: “At my old practice, I might have had to wait two weeks to see my doctor. But pain doesn’t wait a fortnight! You want to get treatment for it there and then. Now I know I can call up in the morning, come down to Health 1000 and see someone.”He also knows that if the doctor has any concerns or if he needs an X-ray, they can send him on to the relevant department straight away, and it’s quicker and easier for him to collect his prescriptions.For Maurice, one of the best things about Health 1000 is the people that work there: “So far I’m impressed. They listen. Without a doubt I would recommend the practice to other people.”
Patient case study - Health 1000
Maurice Wilson
Introduction

The graphic below captures the experience of two patients using Health 1000

Play Video 540
Patient Story Part 1
https://youtu.be/x5ThfJ3dvxU

The Year of Care Pilot
Data Analysis and Cohort selection
Data Analysis and cohort selection

Infrastructure for effective data analysis has been a challenge
Hospital Data
GPData
Infrastructure is key
•Link data•Commission a data platform
Platform should provide
•Risk stratification•Case Management•Activity level data•Costed datasets•Fast user defined analysis•Not SQL•Automated reporting•Snova technology•ITK standard interfaces
Community data
Social Care data

Cohort selection
Data Analysis
Case Management
3949 individuals
Care ManagementSupported self care
40,248 individuals
Self CarePrevention and wellbeing promotion
162,163 individuals
RELATIVE RISK 2-20%Emergency admits = 7129 A&E visits = 26,756Total Cost= £47 million
RELATIVE RISK 0-1%Emergency admits = 3931A&E visits = 7158Total Cost = £16 million
RELATIVE RISK 21-100%Emergency admits = 1512 A&E visits = 23,586Total Cost= £22 million
Case ManagementImproving outcomes for patients with complex health and social care needs
Care ManagementIncreasing the ‘value of care’ provided to patients with long term conditions
Self CareEmpowering patients, carers & families to make informed decisions about their care treatment & providing choice in primary care to meet these needs

BHR
Kirklee
s
Lambeth
Leeds
North St
affs
South Es
sex0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Average cost of care for complex patients 1 % risk
Average cost per patientAverage
BHR
Kirklee
s
Lambeth
Leeds
North St
affs
South Es
sex
West Ham
ps0
2,0004,0006,0008,000
10,00012,00014,00016,00018,000
Average cost of care for patients 10 %
Average cost per patientAverage
BHR Total
Kirklee
s Total
Lambeth
Total
Leeds T
otal
North St
affs T
otal
South Es
sex To
tal
West Ham
ps0
5000
10000
15000
20000
25000
30000
Combined average for patient care
Average cost per patientAverage
Data Analysis

ICM increased community spend during YOC pilot
Data Analysis

Moved towards – comorbidities based on Scottish multimorbidity report 2008
Data Analysis

DiabetesDementiaStroke
COPD
HypertensionCVDHeart Failure Depression
Patient cohort for the service 5 or more long term conditions.2000 patients eligible across BHRCCGs and aim to recruit 1000
Patient cohortRow Labels Cohort Hypertension CHD Diabetes Stroke Depression COPD Heart Failure DementiaLTC 5+ 100 99 96 80 70 80 69 75 36Scottish modified LTC 4+ 1924 1816 1559 1421 863 793 783 679 303Grand Total 2024 1915 1655 1501 933 873 852 754 339
The selected cohort criteria, excludes CHC patients

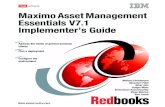
The number of patients in the complex care cohort by the annual number of primary care contacts - 2013/14 data only, Barking & Dagenham CCG cohort only
This illustrates a relatively normal distribution of patients receiving primary care contacts around the mean of 51 contacts per year , but still there was one patient with 186 contacts in 2013/14 . The relatively normal distribution of numbers around the mean is represented by a skewness value of close to 1

Activity Cost (£thousand)
2012/13 2013/14 2014/15 2012/13 2013/14 2014/15
Primary Care Contact85,311 91,416 91,288 3,839 4,114 4,108
Pharmacy272,793 271,471 274,340 4,804 4,781 4,831
Acute care A&E2,341 2,342 1,936 277 291 244
Outpatient11,523 11,077 11,320 1,219 1,502 1,546
Daycase1,130 925 572 858 740 439
Elective162 131 128 579 392 353
NEL short-stay443 435 336 497 461 336
NEL long-stay959 985 768 3,174 3,178 2,538
Community care Face-to-Face12,052 20,654 24,936 2,210 3,814 4,396
Telephone1,032 1,859 2,244 55 96 109
Total17,511 19,368 18,899
Total annual number of events and total annual cost for all patients in the complex care cohort - all CCGs
Activity and cost for the cohort

Variation in activity between patients
The averages in the previous slide hide a great deal of variation. Thus if we take one example, patient's in the complex care cohorts on average visit A&E once a year but over 50% of patients did not visit A&E at all during 2013/14, and one patient visited 41 times .
Perhaps the most striking feature of the data is that large percentages of patient in the complex care cohorts didn't require acute inpatient care at all in 2013/14.

The trend in adjusted cost for all patient in the complex care cohort by service type
• Costs have more than doubled in 7 years
• 0ver 50% of costs are primary care
• Acute care accounts for 29% of cost and reducing
• £10k average cost per patient but escalates dramatically in last year of life
The costs have increased for these patients over the 7 years, presumably as more of the patients in the cohorts need services and/or patients in the cohorts need greater volumes of services
The greatest cost increases over the period for patients in the cohorts were primary care and community care. In percentage terms, the cost of acute care has decreased over the period.

The Implementation of a Complex Care organisation
Implementation
Legal & governance issues , Clinical design, Financial model, location and Patient recruitment

• Establishing the financial arrangements for the service as set up, then BAU and capitated budget moving forward
• CQC registration• Insurances wider provision of services• GPs and the Provider list and having a non GP as the clinical lead• CCG membership • Receiving records from practices- system challenges• Legal requirements for the Limited Company,• The APMS contract• Recruiting clinical teams for a time limited project and people leaving• GPs and the Provider list and having a non GP as the clinical lead
Challenges setting up the organisation

• Early Implementer site for YOC
• Advanced data sets from primary care, acute community and social care
• PMCF Bid to include testing of capitated budget being developed to one provider in early 2014
• PMCF Bid to include testing of capitated budget being developed to one provider in early 2014
• PMCF bid approved may 2014
May 2014
• Started work on project
May 2014
June-September 2014
• academic development of the service model and staffing requirements with UCLP
• Set up of the legal entity to operate the service
• Source premises• Source clinical leadership
October-January 2014
• Commence recruitment of staff
• Training • Premises set up• Legal entity formed• APMS discussions started• Engagement with practices • January 16th APMS
contract signed• January 19th first patient
registered
Complex Care organisation timeline

Governance
Community Trust
Private Provider
Voluntary Sector
GP Federation
Acute Trust

ROLE WTE at start up
Start up Cover provided WTE by month 3
MD and Geriatrician (50:50 role)
1.0 20 hours direct patient care plus 17.5 hours management plus on call support as required
1.0
HCS Key workers 5.0 73.5 hours per week 8am to 18.30pm Monday to Sunday. This is a dual function role covering reception and health care support and requires two members of staff to be on duty during 08.00 to 18.30pm Monday to Friday
6.0
GPs 3.0 52 hours per week 08am to 18.30pm Monday to Friday plusOn call for 5 hours per week Monday to Friday 6.30 to 8pm and 24 hours on Saturday and Sunday from 8am to 8pmA total of 81 hours per week
3.0
Practice Manager 1.0 37.5 hours per week as required to cover 7 days per week on rota
0.5
Nurse 1.0 37.5 hours per week during 8am to 6.30pm 0OT 0.5 18.5 hours per week during 8am to 6.30pm 3.0Physiotherapist 0.5 18.5 hours per week during 8am to 6.30pm 2.0Pharmacist 0.5 18 hours per week Monday to Friday as required 1Community Nurse 0.0 Not applicable 4.0
Mental health Nurse 0 Not applicable 0.5
Social Worker 1.0 Seconded from Local Authority
Complex Care organisation staffing model

Operation process for the clinical model

Key Features of the clinical model
• GP lead model of chronic disease management with proactive case management of medical and social care
• Tele-monitoring• Patient and carer education and enhanced self-management• Promotion of independence and personal responsibility• Shared care record with agreed care plan• Quality improvement embedded in culture• Key worker skills and competencies developed

Age UK care navigator pilot

Financial modelling
31/01/2015 28/02/2015 31/03/2015 30/04/201531/05/201
530/06/201
5 31/07/201531/08/201
5 30/09/201531/10/201
5
2 12 55 175 295 415 535 655 775 895
Costs Clinical Staff B £53,131 £53,131 £53,131 £53,131 £54,417 £65,585 £65,585 £76,754 £83,495 £87,923 Operational £17,634 £17,684 £17,899 £18,499 £19,099 £19,699 £20,299 £20,899 £21,499 £22,099 Per Patient Per Month Pharmacy £67 £133 £799 £3,663 £11,654 £19,645 £27,637 £35,628 £43,619 £51,610 £59,602Acute £174 £349 £2,093 £9,592 £30,519 £51,446 £72,373 £93,300 £114,227 £135,154 £156,081Community £175 £350 £2,098 £9,616 £30,596 £51,576 £72,556 £93,536 £114,516 £135,496 £156,476Social Care £83 £167 £1,000 £4,583 £14,583 £24,583 £34,583 £44,583 £54,583 £64,583 £74,583Out of Hours £34 £68 £405 £1,856 £5,906 £9,956 £14,006 £18,056 £22,106 £26,156 £30,206 £70,765 £70,815 £71,030 £71,630 £73,516 £85,284 £85,884 £97,653 £104,995 £110,022
Total Costs £71,831 £77,210 £100,340 £164,888 £230,722 £306,439 £370,987 £446,704 £517,994 £586,969Revenue Year of Care Payment £707 £1,414 £8,486 £38,892 £123,747 £208,602 £293,457 £378,312 £463,167 £548,022 £632,877APMS Revenue £80
Total Revenue £1,414 £8,486 £38,892 £123,747 £208,602 £293,457 £378,312 £463,167 £548,022 £632,877
Revenue > Cost???? YES YES YES YES
Total Spend Jan to Apr £433,846Total Available £900,000Total Remaining £466,154Total Spend to Breakeven £230,430
IN BUDGET
Total Additional Funding Requirement -£235,724
Point of transition where operating costs are lower than revenue and the organisation breaks even

Financial modellingApr-15 May-15 Jun-15 Jul-15 Aug-15
Description ParametersStaff Costs B Total Costs £164,888 £230,722 £306,439 £370,987 £446,704
Sensitivity Total Revenue Original £124,914 £210,569 £296,224 £381,879 £467,5341 Flex Capitated Revenue Increase by 25% Total Increased Revenue £156,142 £263,211 £370,280 £477,349 £584,417
Decrease by -25% Total Decreased Revenue £93,685 £157,927 £222,168 £286,409 £350,650Apr-15 May-15 Jun-15 Jul-15 Aug-15
DescriptionSensitivity Total Costs (Staff Costs UCLP) £182,320 £250,007 £326,858 £416,858 £482,692
2 Choose Staff Costs Total Costs (Staff Costs Health 1000) £164,888 £230,722 £306,439 £370,987 £446,704Total Revenue £124,914 £210,569 £296,224 £381,879 £467,534
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15£100,000
£300,000
£500,000
£700,000
£900,000
£1,100,000
Total Costs Total Revenue Original Total Increased Revenue Total Decreased Revenue
Tota
l Mon
thly
Cos
ts/R
even
ues (
£)
Effect of changing Capitated Revenue Payment Only

StaffNEW PATIENT (mins - once off) MD Geriatrician GP Nurse Therapist Social Worker Key Worker Source - see Health 1000 Staff email (hidden tab)
could either be any of five individuals doing this work so one fifth of total time assigned to each.
Initial Visit 14 14 14 14 14 70Assessment 24 28 24 24 24 72 various options of mix of staff undertaking workAdmin 60Care Planning 10 40 10 10 10 10TOTAL TIME A NEW PATIENT 48 82 48 48 48 212 minutes EXISTING PATIENT (mins per month) MD Geriatrician GP Nurse Therapist Social Worker Key Worker check 4 reviewsReviews 5.83 5.83 5.83 5.83 0.00 23.33 quarterly review of 70 mins by one professional 560 560Reactive 11.88 11.88 11.88 60 mins per day for 50 patients by 1 of 3 professionals TOTAL TIME EXISTING PATIENT 5.83 17.71 17.71 17.71 0.00 23.33
WTE 40 hours per week for 48 weeks
1920
WTE NEW 0.0004 0.0007 0.0004 0.0004 0.0004 0.0018 WTE 160 hours per month 160
WTE EXISTING 0.001 0.002 0.002 0.002 0.000 0.002minutes in hour 60
WITH UTILISATION MD Geriatrician GP Nurse Therapist Social Worker Key Worker UtilisationWTE NEW 0.0005 0.0008 0.0005 0.0005 0.0005 0.0022 85%WTE EXISTING 0.0007 0.0022 0.0022 0.0022 0.0000 0.0029
check for 1000 patients1000 0.71 2.17 2.17 2.17 0.00 2.86
Financial modelling – Staffing model calculations option B
Patient number VS Staff Costs
4/1/2015
5/1/2015
6/1/2015
7/1/2015
8/1/2015
9/1/2015
10/1/2015
11/1/2015
12/1/2015
1/1/2016
£0£20,000£40,000£60,000£80,000
£100,000£120,000£140,000£160,000
0
200
400
600
800
1000
1200
Staff UCLP Staff Health 1000 Patient Numbers
Staff
Cos
t
Patie
nt N
umbe
rs

1-Jan-15 1-Feb-15 1-Mar-15 1-Apr-15 1-May-15 1-Jun-15 1-Jul-15 1-Aug-15 1-Sep-15 1-Oct-15 1-Nov-15 1-Dec-150
200
400
600
800
1000
1200
Num
ber o
f reg
ister
ed p
atien
ts
Patient recruitment

Play Video 540
Patient Story Part 2

Outcomes per £ Spent
COM
SPREM
S
PROMS
Evaluation – Independent evaluation by the Nuffield Trust

BHRQuestions and Discussion


May 2013
• Early Implementer site for YOC
• Advanced data sets from primary care, acute community and social care
• PMCF Bid to include testing of capitated budget being developed to one provider in early 2014
• PMCF Bid to include testing of capitated budget being developed to one provider in early 2014
• PMCF bid approved may 2014
May 2014
• Started work on ACO roll out
May 2014
June-September 2014
• academic development of the service model and staffing requirements with UCLP
• Set up of the legal entity to operate the service
• Source premises• Source clinical leadership
October-January 2014
• Commence recruitment of staff
• Training • Premises set up• Legal entity formed• APMS discussions started• Engagement with practices • January 16th APMS
contract signed• January 19th first patient
registered
Year of Care Timeline


Outline governance structure
Direct reporting linesInformation flow
Programme Management BoardChair (independent)
NEDs (providers, CCGs, Programme Clinical Lead)
Executive Lead (MD)Other Executive (COO)
Complex Primary Care Practice
NHS EnglandCCGs
Local AuthoritiesContractual
Clinical Staffing(via providers)
Support ServicesHR
Finance IT
Other
Owners
(‘members’)
Regulators etcCQC
MonitorNHSLA
TDA
2

Differences in hospital service use between cases and controls (see table 5, page 25)
-10
0
10
20
30
40 Extra service use among the control group
n = 146 n = 126 n = 146n = 151

Estimated cost differences in acute sector based on projected changes in hospital activity.
-£100
-£50
£0
£50
£100
£150
£200
£250
Outpatients A&E Elective inpatientvisit
Emergencyinpatient visitCo
st d
iffer
ence
per
per
son
-m
onth
Low High Projected

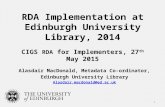
The impact of the number of patients recruited to the service and plausible scenarios for which costs balance.
£0
£25,000
£50,000
£75,000
£100,000
£125,000
£150,000
£175,000
£200,000
£225,000
£250,000
0 100 200 300 400 500 600 700
Health1000 Total running cost Lower bound Upper bound Projected Health1000 staff cost
Upper bound costdifferences
Lower bound cost differences
Operational cost
Total running cost (including staff costs) of delivering service at Health1000practice
Projected costdifference estimates
Staff cost
+

Implications of relaxing eligibility criteria
Lower service use => Recruitment of more patients to achieve acceptable statistical powere.g. with a 15% reduction
It will affect the balance between fewer costs saved per patient and lower cost of providing primary care services via Health 1000
Numbers needed to achieve 80% power
Recruited under existing criteria
300
Existing criteria
600
Opening up to three conditions
800

A&E atten
dances
Outpatient visit
s
Electi
ve admissions
Emerg
ency admiss
ions
Primary
care co
ntacts
-60%
-50%
-40%
-30%
-20%
-10%
0%
% difference in use over 2014
Health service use for people with three conditions compared with those currently eligible for Health 1000

The Next Steps
Implementing The Learning From Health 1000 across the Wider
Health and Social Care Economy


Per capita costing

Health 1000: A local complex care organisation
Questions and discussion

www.england.nhs.uk
LTC Framework postcards game
Susie Peachey

www.england.nhs.uk
• Helping us to test and develop it
• Each group should have:• Picture of the LTC Framework • Set of 30 cards
• Aim is to match the illustrations to a section of the Framework
• THERE IS NO DEFINITIVE CORRECT ANSWER• It is the discussions that are as important as the
final result
The LTC framework postcard game

www.england.nhs.uk
Summary of the day and key messages
Bev Matthews

www.england.nhs.uk
23rd March 2016
CLOSE
LtC Year of Care CommissioningEIS and LTC Community of Practice
Workshop