Double fixation of displaced patella fractures using bioabsorbable cannulated lag screws and braided...
5
Double fixation of displaced patella fractures using bioabsorbable cannulated lag screws and braided polyester suture tension bands § Li Qi a,1 , Cao Chang b , Tang Xin a , Pei Fu Xing a , Yang Tianfu a , Zhong Gang a , Li Jian a, * a Department of Orthopaedic Surgery, West China Hospital, Sichuan University, Chengdu 610041, China b Department of Reconstruction Surgery, West China Hospital, Sichuan University, Chengdu 610041, China Introduction Patella fractures are relatively uncommon and only account for 0.5–1.5% of all bone fractures. 3,7 Due to the patella’s importance as regards the extensor mechanism, efforts should to be made to preserve the patella. The goal of the therapy is the anatomical reduction of both the fracture and the articular surface in addition to the stable fixation of the fracture, which allows early rehabilitation of the knee. Surgical treatment becomes necessary when the fracture displacement exceeds 3 mm or the articular incongruity exceeds 2 mm. 14 The tension band technique is most often used for patella fractures, and has been shown to produce satisfactory out- comes. 25,30 Metal implants, such as stainless steel wires, K-wires and screws have generally been used for this method of fixation. However, numerous complications including postoperative pain, K-wire migration and other complications related to the use of metal implants are fairly common, 14,18,27,28 and revision surgery to remove the implants becomes necessary. According to Hung et al. 18 the incidence of complications related to the use of wire loops was 47%, and 15% had required wire removal. Moreover, far more serious complications, such as intra-articular migration of the broken wire, have also been reported. 11 In recent years, non-metallic implants have become available for use in fracture fixation. Some authors have evaluated new fixation techniques for fractures of the patella or olecranon using various materials, such as braided polyester sutures and biode- gradable screws, via biomechanical studies and randomised clinical trials. 10,14,16,17,20,21,27 Such studies have discovered that Injury, Int. J. Care Injured 42 (2011) 1116–1120 ARTICLE INFO Article history: Received 22 July 2010 Received in revised form 5 January 2011 Accepted 24 January 2011 Keywords: Bioabsorbable cannulated lag screws Braided polyester suture Tension band Patella fracture Double fixation SUMMARY Purpose: To evaluate the effectiveness and safety of a new double fixation technique for displaced patellar fractures using bioabsorbable cannulated lag screws and braided polyester suture tension bands. Methods: Fifteen patients (mean age of 46.2 years) with displaced transverse or comminuted patella fractures were enrolled in this prospective study. All of the patients were treated via the open reduction internal fixation (ORIF) procedure using bioabsorbable cannulated lag screws and braided polyester suture tension bands. The patients were followed post-surgery to evaluate (1) the time required for radiographic bone union, (2) the knee joint range of motion at the time of radiographic bone union, (3) the degree of pain assessed using the visual analogue scale (VAS), (4) the function of the knee using the Lysholm score and (5) the presence of any additional complications from the surgery. Results: All of the patients were followed post-treatment for more than 1 year (range, 12–19 months; mean post-treatment follow up time, 14 months). The bone union of the fractures as seen radiographically occurred approximately 3 months from surgery in all cases without implant failure or redisplacement of the fractured site. The mean knee joint range of motion was from 0 to 134.68, and the mean VAS score was 0.7 at the time of bone union. The mean Lysholm scores at the time of bone union and 12 months post-surgery were 86.7 and 95.7, respectively. No postoperative complications, such as infection, dislocation or breakage of the implants, were observed. Moreover, all of the patients returned to their previous activity level. Conclusion: This new double fixation technique using bioabsorbable cannulated lag screws and braided polyester suture tension bands resulted in satisfactory outcomes for patella fractures without any obvious complications. ß 2011 Elsevier Ltd. All rights reserved. § This research was supported by Department of Orthopaedic Surgery, West China Hospital, Si Chuan University. Research was performed at Department of Orthopaedic Surgery, West China Hospital, Si Chuan University. * Corresponding author. Tel.: +86 13908016178; fax: +86 028 85423438. E-mail addresses: [email protected] (L. Qi), [email protected] (L. Jian). 1 Tel.: +86 13880765013; fax: +86 028 85423438. Contents lists available at ScienceDirect Injury journal homepage: www.elsevier.com/locate/injury 0020–1383/$ – see front matter ß 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.injury.2011.01.025
Transcript of Double fixation of displaced patella fractures using bioabsorbable cannulated lag screws and braided...

Injury, Int. J. Care Injured 42 (2011) 1116–1120
Contents lists available at ScienceDirect
Injury
journa l homepage: www.e lsevier .com/ locate / in jury
Double fixation of displaced patella fractures using bioabsorbable cannulatedlag screws and braided polyester suture tension bands§
Li Qi a,1, Cao Chang b, Tang Xin a, Pei Fu Xing a, Yang Tianfu a, Zhong Gang a, Li Jian a,*a Department of Orthopaedic Surgery, West China Hospital, Sichuan University, Chengdu 610041, Chinab Department of Reconstruction Surgery, West China Hospital, Sichuan University, Chengdu 610041, China
A R T I C L E I N F O
Article history:
Received 22 July 2010
Received in revised form 5 January 2011
Accepted 24 January 2011
Keywords:
Bioabsorbable cannulated lag screws
Braided polyester suture
Tension band
Patella fracture
Double fixation
S U M M A R Y
Purpose: To evaluate the effectiveness and safety of a new double fixation technique for displaced
patellar fractures using bioabsorbable cannulated lag screws and braided polyester suture tension
bands.
Methods: Fifteen patients (mean age of 46.2 years) with displaced transverse or comminuted patella
fractures were enrolled in this prospective study. All of the patients were treated via the open reduction
internal fixation (ORIF) procedure using bioabsorbable cannulated lag screws and braided polyester
suture tension bands. The patients were followed post-surgery to evaluate (1) the time required for
radiographic bone union, (2) the knee joint range of motion at the time of radiographic bone union, (3)
the degree of pain assessed using the visual analogue scale (VAS), (4) the function of the knee using the
Lysholm score and (5) the presence of any additional complications from the surgery.
Results: All of the patients were followed post-treatment for more than 1 year (range, 12–19 months;
mean post-treatment follow up time, 14 months). The bone union of the fractures as seen
radiographically occurred approximately 3 months from surgery in all cases without implant failure
or redisplacement of the fractured site. The mean knee joint range of motion was from 0 to 134.68, and
the mean VAS score was 0.7 at the time of bone union. The mean Lysholm scores at the time of bone
union and 12 months post-surgery were 86.7 and 95.7, respectively. No postoperative complications,
such as infection, dislocation or breakage of the implants, were observed. Moreover, all of the patients
returned to their previous activity level.
Conclusion: This new double fixation technique using bioabsorbable cannulated lag screws and braided
polyester suture tension bands resulted in satisfactory outcomes for patella fractures without any
obvious complications.
� 2011 Elsevier Ltd. All rights reserved.
Introduction
Patella fractures are relatively uncommon and only account for0.5–1.5% of all bone fractures.3,7 Due to the patella’s importance asregards the extensor mechanism, efforts should to be made topreserve the patella. The goal of the therapy is the anatomicalreduction of both the fracture and the articular surface in additionto the stable fixation of the fracture, which allows earlyrehabilitation of the knee. Surgical treatment becomes necessarywhen the fracture displacement exceeds 3 mm or the articularincongruity exceeds 2 mm.14
§ This research was supported by Department of Orthopaedic Surgery, West
China Hospital, Si Chuan University. Research was performed at Department of
Orthopaedic Surgery, West China Hospital, Si Chuan University.
* Corresponding author. Tel.: +86 13908016178; fax: +86 028 85423438.
E-mail addresses: [email protected] (L. Qi), [email protected] (L. Jian).1 Tel.: +86 13880765013; fax: +86 028 85423438.
0020–1383/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2011.01.025
The tension band technique is most often used for patellafractures, and has been shown to produce satisfactory out-comes.25,30 Metal implants, such as stainless steel wires, K-wiresand screws have generally been used for this method of fixation.However, numerous complications including postoperative pain,K-wire migration and other complications related to the use ofmetal implants are fairly common,14,18,27,28 and revision surgery toremove the implants becomes necessary. According to Hung etal.18 the incidence of complications related to the use of wire loopswas 47%, and 15% had required wire removal. Moreover, far moreserious complications, such as intra-articular migration of thebroken wire, have also been reported.11
In recent years, non-metallic implants have become availablefor use in fracture fixation. Some authors have evaluated newfixation techniques for fractures of the patella or olecranon usingvarious materials, such as braided polyester sutures and biode-gradable screws, via biomechanical studies and randomisedclinical trials.10,14,16,17,20,21,27 Such studies have discovered that

[()TD$FIG]
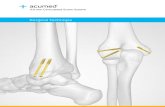
Fig. 1. Drill hole within the central part in the sagittal plane of the patella.
[()TD$FIG]
Fig. 2. Schematic diagram showing the technique of patella fracture fixation used in
this study.
L. Qi et al. / Injury, Int. J. Care Injured 42 (2011) 1116–1120 1117
when compared with metal implants, bioabsorbable implantsdemonstrated comparable results for patella and olecranonfracture fixation and were notably characterised by less postoper-ative pain. However, the combined use of bioabsorbable cannu-lated lag screws and braided polyester suture tension bands wasseldom reported.
We speculated that bioabsorbable screws and braided polyestersutures might be a useful alternative to the use of stainless steelwires, K-wires and metal screws that have been traditionally usedin surgeries to repair patella fractures, due to the potential forreducing the rate of postoperative complications and avoidingadditional operations to remove the implants. Thus, we developeda new double technique for patella fracture fixation usingbioabsorbable cannulated lag screws and braided polyester suturetension bands. The goal of this study was to evaluate theeffectiveness and safety of this new technique for the treatmentof patella fractures.
Materials and methods
Patients
Nine male and six female patients with displaced transverse orcomminuted patella fractures with adequate bone composition toaccommodate screws were enrolled in this prospective study.Individuals with severe comminuted patella fractures were noteligible because the lag screws cannot be used without adequatebone composition (i.e., in cases involving severe comminutedpatella fractures). The patients’ ages ranged from 26 to 67 years(mean 46.2 years). All of the patients were treated by the ORIFprocedure using bioabsorbable cannulated lag screws and braidedpolyester suture tension bands between September 2008 and June2009, after consent was obtained from all patients, and approvalwas obtained from the ethics committee of the authors’ institution.The patients were then followed up after the surgery to evaluatethe time required for radiographic bone union, the knee joint rangeof motion at the time of radiographic bone union, the degree ofpain assessed using the visual analogue scale (VAS), the function ofknee using the Lysholm score and the presence of any additionalcomplications from the surgery.
Materials
Two No. 5 Ethibond (Ethicon, Somerville, NJ, USA) braidedpolyester sutures and two bioabsorbable cannulated lag screwswith a 4.5-mm diameter (Conmed Linvatec, Largo, FL, USA) wereused for each procedure.
Surgical technique
Under lumbar anaesthesia, a median longitudinal or transverseskin incision approximately 7 cm in length was made above thepatella. After debriding the clot, the fracture was carefully reducedto ensure that the articular surface of the patella was smooth. Theanatomical reduction position of the fractured patella wasmaintained using bone reduction forceps prior to drilling twolongitudinal parallel holes (3.5 mm in diameter) within the centralportion of the patella in the sagittal plane from a distal to proximaldirection (Fig. 1). The distal portions of the drill holes wereoverdrilled to ensure that the screws act as lag screws that couldoffer compression across the fracture line. The length of each screwwas 1–2 mm shorter than the length of the drill hole. Twobioabsorbable cannulated lag screws were subsequently screwedinto the drill holes from a distal to proximal direction, and thefracture was fixed via compression burying the heads of the screwsinto the distal cortical bone.
Two No. 5 Ethibond braided polyester sutures were then passedthrough the cannulated screws and were subsequently crossedover the front of the patella forming a horizontally oriented figureeight on the anterior surface of the patella beneath the fascia. Thesuture was initially tied with a sliding knot centred on the distalpole of the patella after which the suture loop was tightened withsufficient pressure to achieve a stable and firm osteosynthesis.Finally, the knot was tied a minimum of three times to secure thefractured patella (Fig. 2). For comminuted patella fractures, acircular suture surrounding the patella should be positioned usinga loop of No. 5 Ethibond braided polyester suture to improve thefixation.
The knee was gently flexed, and then the position of reducedfragments and the stability of the fixation were checked. At thispoint, any incisions or tears observed in the retinacula wererepaired. Prior to wound closure, the full range of knee motionshould be assessed an additional two to three times to ensure thatthere is no restriction in knee motion.
Radiographs and a photograph of the operated site are shown inFig. 3.
Postoperative management
Both active and passive knee motion exercises began 1 day afterthe surgery, when knee flexion was less than 908. At this time,isometric exercises involving the quadriceps were initiated. On

[()TD$FIG]
Fig. 3. Radiographs and a photograph of the operated site. (a) Preoperative lateral radiograph; (b) two Kirschner wires (2 mm in diameter) drilled from a distal to proximal
direction longitudinally as guide wires; (c) after the distal portions of the drill holes were overdrilled, bioabsorbable cannulated screw was screwed into the drill holes from a
distal to proximal direction; (d) photograph after fixation showed that the suture was placed beneath the fascia and in intimate contact with the bone surface; (e) C-arm
lateral radiograph immediately after fixation; (f) radiograph 12 months after surgery.
L. Qi et al. / Injury, Int. J. Care Injured 42 (2011) 1116–11201118
postoperative day 2 or 3, partial or full weight-bearing exerciseswere started under the protection of a hinge brace, while walkingexercises involving the use of crutches also began at this time and
lasted for a period of 4 weeks. Beginning in the fourthpostoperative week, normal daily activities for the participantswere permitted. Approximately 3 months after the surgery, non-

Table 1Clinical features of the 15 patients.
Case Age/sex
(years)
Fracture
type
Follow-up
period
(months)
Time to bone
union
(months)
ROM at
bone union
(extension/flexion)
VAS score
(bone union/12
months after surgery)
Lysholm score
(bone union/12
months after surgery)
Complications
(12 months
after surgery)
1 26/F Transverse 15 2.5 0/135 0/0 90/100 None
2 67/F Comminuted 13 3 0/130 1/1 82/91 None
3 34/M Transverse 16 3.5 0/140 1/0 89/99 None
4 33/M Transverse 15 3.5 0/135 0/0 95/100 None
5 55/M Transverse 13 3 0/135 0/0 89/99 None
6 40/F Comminuted 15 3 0/120 3/1 80/90 None
7 35/M Transverse 14 2.5 0/140 0/0 85/99 None
8 47/M Transverse 12 2.5 0/135 1/0 85/94 None
9 52/F Transverse 17 3 0/140 0/0 90/94 None
10 58/M Comminuted 13 3 0/130 2/1 85/95 None
11 38/M Transverse 14 3 0/140 0/0 90/100 None
12 62/F Transverse 16 3.5 0/130 1/1 85/91 None
13 43/F Transverse 15 2.5 0/140 0/0 89/99 None
14 48/M Transverse 19 3 0/135 1/0 86/94 None
15 55/M Transverse 17 3 0/135 0/0 83/91 None
Average 46.2 14 2.96 0/134.6 0.7/0.3 86.7/95.7
L. Qi et al. / Injury, Int. J. Care Injured 42 (2011) 1116–1120 1119
confrontational sports activities were permitted, provided thepatient’s clinical indicators were satisfactory and that there wasradiographic evidence of bone healing.
Results
All of the patients were followed for more than 1 year post-treatment (range, 12–19 months; mean post-treatment follow uptime of 14 months), and the clinical characteristics of all patientsare shown in Table 1.
Time of radiographic bone union
The bone fracture union occurred at approximately 3 monthspost-surgery in all cases not involving implants failure orredisplacement of the fractured site.
Range of motion
At the time of bone union, the mean knee joint range of motionwas 0–134.68. However, one obese female patient with acomminuted patella fracture had a range of knee motion of 0–1208 at the time of bone union due to slow progress made duringrehabilitation. However, this patient had a normal range of kneemotion and satisfactory knee function at 6 months post-surgery.
VAS score
The mean VAS score of all patients was 0.7 at the time of boneunion. The pain was most often reported to be located on the frontknee and was caused by excessive activity. Notably, no patientcomplained of pain due to irritation from the implants.
Function of knee (Lysholm score)
The mean Lysholm scores at the time of bone union and 12months after surgery were 86.7 and 95.7, respectively. All of thepatients eventually returned to their preoperative activity level.
Complications
No postoperative complications, such as infection, dislocationor breakage of the implants were observed up through the finalfollow-up examination.
Discussion
The modified tension band wire technique suggested by theAbreitsgemeinshaft fur Osteosynthese (AO) appears to be the mostwidely accepted approach used for practically all types of patellafractures.2,18,30 For this technique, compression of the fracture siteis obtained only by the presence of a figure-eight tension band wirelocated in front of the patella, especially during knee flexion.However, this tension wire system probably does not offersufficient compression and may lead to fracture displacementduring full knee extension or due to soft-tissue atrophy within afew weeks after surgery.7,8,12,18,23 Generally, 25–42% of thepatients who underwent the modified tension band wiretechnique have suboptimal results due to wire migration, failureof fixation and postoperative pain because of to implantirritation.2,3,8,14,18,22
Alternatively, metal cannulated lag screws with or without atension band wire placed through the screws have been introducedin some instances.1,7 According to previous reports, combiningmetal cannulated lag screws with a tension band wire couldprovide superior fixation strength and greater stability along witha decreased risk of fracture dislocation than each individualmethod. The lag screws and tension bands may offer compressionof the fracture site both during knee extension and flexion, as wellas during times of higher load-bearing capacity.4,7,30 Thistechnique is mostly applicable to transverse and comminutedpatella fractures with adequate bone composition for screws,whereas patients with severe comminuted patella fractures werenot eligible, as in our study.
Previous studies9,20 have shown that postoperative symptomsrelated to patella fracture implants decreased in severity with theuse of non-metallic implants. In recent years, a significant amountof research has been conducted on the use of braided polyestersutures with high tensile strength in patella fracture fixationprocedures, suggesting their use as an alternative to metalwires.14,16,17,24,27 These braided polyester sutures have severaladvantages both in vitro and in vivo. First, in vitro studies haveshown that braided polyester sutures have higher stiffness andtensile strength than other non-absorbable or absorbablesutures.13 Second, braided polyester sutures demonstrate minimaltissue reaction and have been shown to be safe for clinical use.Moreover, braided polyester sutures can maintain their mechani-cal characteristics in vivo.5,15 The examination of various sutureconfigurations performed by Patel et al.27 determined that theaverage fracture gap size of the suture Lotke technique with two

L. Qi et al. / Injury, Int. J. Care Injured 42 (2011) 1116–11201120
loops of No. 5 Ethibond was comparable to the wire Lotketechnique in that no failures of fixation occurred. Thus, we usedtwo loops of No. 5 Ethibond in our study.
Metal cannulated lag screws with a tension band wire and theLotke technique with suture were both proved to be stable fixationtechniques for patella fractures.23,27 The technique reported hereinoriginated from them and can avoid additional surgeries forimplant problems. Biodegradable screws and braided polyestersutures have been widely used for fracture fixation of theolecranon and the malleoli, as evidenced by biomechanical studiesand clinical trials with positive results. The tension band used inour technique is more like a horizontally oriented figure-eighttension band, which was found to be stronger than the verticallyoriented bands.19 In addition, the compression provided by the lagscrews could offer greater stability than the Lotke technique thatonly uses a suture, thus allowing for an earlier start torehabilitation of the knee joint, as indicated in our study. Forpatients with comminuted patella fractures, the rehabilitation ofthe knee function may also be delayed, but with good resultsfollowing progressed training.
Several technical points of this technique merit discussion.First, one pole of the drill holes was overdrilled to allow the screwsto act as lag screws that could offer compression of the fracturesite. The screws should be screwed into the drill holes gently toprevent them from being broken. Second, it is important to placethe suture in close contact with the bone surface to achieve securefixation and to avoid suture loosening after soft-tissue atrophy.6
Studies have shown that when using the tension band technique,the wire or suture tension band that is adjacent to the bone surfacehas to be more stable than that turned over the soft tissue.26 Toensure that the suture is in close contact with the bone, the sutureshould be passed under the soft tissue such that it directly contactsthe bone, even when no intervening soft tissue is present at theproximal and distal poles of the patella, a manoeuvre that could notbe achieved easily using metal wire. Moreover, to achieve propersuture and bone contact, the heads of the screws should be buriedwithin the cortical bone, and the length of the screw should be 1–2 mm shorter than the length of the drill holes, which can also helpavoid skin and soft tissue irritation from the screws. Third, thetension band suture loop should be gradually tightened until thefragments are in close contact. Thus, the sliding knot technique isrecommended because the tightening process of the loop can becontrolled.13 The knots should be buried in the soft tissue to reducesymptoms caused by them.9 Fourth, knee flexion should berepeated several times after fracture fixation is completed, butbefore wound closure to check the stability of the fixation and toensure that there is no restriction in the knee’s motion. Because agap of <2 mm may influence bone union,29 this step can helpmedical staff vary the rehabilitation programme for each patient.
In this study, a new double fixation technique using bioabsorb-able cannulated lag screws and braided polyester suture tensionbands for patella fracture fixation was devised and was shown tobe safe and to produce satisfactory clinical results. The mostimportant benefits of this technique include a reduction ofcomplications due to the lack of metal implants and the abilityto perform a single operation without the need for additionalsurgeries to remove the implants. On the other hand, a limitation ofthis technique is its relatively narrow application to patellafractures with adequate bone composition to accommodatescrews.
Conclusions
This new double fixation technique using bioabsorbablecannulated lag screws and braided polyester suture tension bandswas shown to be safe and resulted in satisfactory outcomes for
patients with patella fractures without obvious complications. Theapplications include procedures involving transverse patellafractures and comminuted patella fractures with adequate bonecomposition to accommodate screws.
References
1. Berg EE. Open reduction internal fixation of displaced transverse patella frac-tures with figure-eight wiring through parallel cannulated compression screws.J Orthop Trauma 1997;11:573–6.
2. Bostman O, Kiviluoto O, Nirhamo J. Comminuted displaced fractures of thepatella. Injury 1981;13:196–202.
3. Bostman O, Kiviluoto O, Santavirta S, et al. Fractures of the patella treated byoperation. Arch Orthop Trauma Surg 1983;102:78–81.
4. Burvant JG, Thomas KA, Alexander R, Harris MB. Evaluation of methods ofinternal fixation of transverse patella fractures: a biomechanical study. J OrthopTrauma 1994;8:147–53.
5. Campbell EJ, Bailey JV. Mechanical properties of suture materials in vitro andafter in vivo implantation in horses. Vet Surg 1992;21:355–61.
6. Carpenter JE, Kasman R, Matthews LS. Fractures of the patella. J Bone Joint Surg A1993;75:1550–61.
7. Carpenter JE, Kasman RA, Patel N, Lee ML. Biomechanical evaluation of currentpatella fracture fixation techniques. J Orthop Trauma 1997;11:351–6.
8. Catalano JB, Iannacone WM, Marczyk S, Dalsey RM, Deutsch LS, Born CT, DelongWG. Open fractures of the patella: long-term functional outcome. J Trauma1995;39:439–44.
9. Chatakondu SC, Abhaykumar S, Elliott DS. The use of nonabsorbable suture inthe fixation of patellar fractures: a preliminary report. Injury 1998;29:23–7.
10. Chen A, Hou C, Bao J, Guo S. Comparison of biodegradable and metallic tension-band fixation for patella fractures 38 patients followed for 2 years. Acta OrthopScand 1998;69:39–42.
11. Chen YJ, Wu CC, Hsu RW, Shih CH. The intra-articular migration of the brokenwire: a rare complication of circumferential wiring in patellar fractures. ChangKeng I Hsueh 1994;17:276–9.
12. Fortis AP, Milis Z, Kostopoulos V, Tsantzalis S, Kormas P, Tzinieris N, BoudourisT. Experimental investigation of the tension band in fractures of the patella.Injury 2002;33:489–93.
13. Gerber C, Schneeberger AG, Beck M, Schlegel U. Mechanical strength of repairsof the rotator cuff. J Bone Joint Surg B 1994;76:371–80.
14. Gosal HS, Singh P, Field RE. Clinical experience of patellar fracture fixation usingmetal wire or non-absorbable polyester – a study of 37 cases. Injury2001;32:129–35.
15. Greenwald D, Shumway S, Albear P, Gottlieb L. Mechanical comparison of 10suture materials before and after in vivo incubation. J Surg Res 1994;56:372–7.
16. Harrell RM, Tong J, Weinhold PS, Dahners LE. Comparison of the mechanicalproperties of tension band materials and suture techniques. J Orthop Trauma2003;17:119–22.
17. Hughes SCA, Stott PM, Hearnden AJ, Ripley LG. A new and effective tension bandbraided polyester suture technique for transverse patellar fracture fixation.Injury 2007;38:212–22.
18. Hung LK, Chan KM, Chow YN, Leung PC. Fractured patella: operative treatmentusing the tension band principle. Injury 1985;16:343–7.
19. John J, Wagner WW, Kuiper JH. Tension-band wiring of transverse fractures ofpatella. The effect of site of wire twists and orientation of stainless steel wireloop: a biomechanical investigation. Int Orthop 2007;31:703–7.
20. Juutilainen T, Patiala H, Rokkanen P, Tormala P. Biodegradable wire fixation inolecranon and patella fractures combined with biodegradable screws or plugsand compared with metallic fixation. Arch Orthop Trauma Surg 1995;114:319–23.
21. Lalonde JA, Rabalais RD, Mansour A, et al. New tension band material for fixationof transverse olecranon fractures: a biomechanical study. Orthopedics 2005;28:1191–4.
22. Levack B, Flannagan JP, Hobbs S. Results of surgical treatment of patellarfractures. J Bone Joint Surg Brit 1985;67:416–9.
23. Lotke PA, Ecker ML. Transverse fractures of the patella. Clin Orthop Relat Res1981;158:180–4.
24. McGreal G, Reidy D, Joy A, Mahalingam K, Cashman WF. The biomechanicalevaluation of polyester as a tension band for the internal fixation of patellarfractures. J Med Eng Technol 1999;23:53–6.
25. Muller ME, Allgower M, Schneider R, Willeneger H. Manual of internal fixation:
techniques recommended by the AO group. Berlin: Springer; 1979. p. 248–253.26. Onder B, Metin M, Berivan C. Anatomical and biomechanical evaluation of the
tension band technique in patellar fractures. Int Orthop 2009;33:1113–7.27. Patel VR, Parks BG, Wang Y, Ebert FR, Jinnah RH. Fixation of patella fractures
with braided polyester suture: a biomechanical study. Injury 2000;31:1–6.28. Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the
operative treatment of patella fractures. J Orthop Trauma 1997;11:183–7.29. Tadahiko Y, Umeo N, Koji R, et al. Tension band fixation for treatment of patellar
fracture: novel technique using a braided polyblend sutures and ring pins.Injury 2009;40:713–71.
30. Weber MJ, Janecki CJ, McLeod P, Nelson CL, Thompson JA. Efficacy of variousforms of fixation of transverse fractures of the patella. J Bone Joint Surg Am1980;62:215–20.