do Sense of Coherence Ansiedad y Sitnomas Depresivos
12
Comparing sense of coherence, depressive symptoms and anxiety, and their relationships with health in a population-based study * Hanna Konttinen a, * , Ari Haukkala a , Antti Uutela b a Department of Social Psychology, University of Helsinki, Unioninkatu 37, P.O. Box 54, 00014 Helsinki, Finland b National Public Health Institute, Finland Available online 11 March 2008 Abstract The strong negative correlatio ns observed between the sense of coherenc e (SOC) scale and measures of depressio n and anxiety raise the question of whether the SOC scale inversely measures the other constructs. The main aim of the present study was to examine the discriminant validity of the three measures by comparing their associations with health indicators and behaviours. The participants were 25 to 74-year-old Finnish men ( n ¼ 2351) and women ( n ¼ 2291) from the National Cardiovascular Risk Factor Survey conducted in 1997. The SOC scale had high inverse correlations with both depression ( r ¼À0.62 among both men and women) and anxiety measures ( r ¼À0.57 among the men and r ¼ À0.54 among the women). Although confirmatory factor analyses suggested that it was possible to differentiate between SOC, cognitive depressive symptoms and anxiety, the estimated correlations were even higher than those mentioned above. Education was related only to SOC, but the associations of SOC, cognitive depressive symptoms and anxiety with self-reported and clinically measured health indicators (body mass index, blood pressure, chole sterol) and health behaviours were almost identica l. The variation in the lowest SOC tertile was more strongly associated with health variables than in the highest tertile. To conclude, the size of the overlap between the SOC and depression scal es was the same as between d epre ssio n and anxiety mea sure s. Thi s indi cate s that f utur e stud ies should examine the disc rimin ant validity of different psychosocial scales more closely, and should compare them in health research in order to bring parallel concepts into the same scientific discussion. Ó 2008 Elsevier Ltd. All rights reserved. Keywords: Finland; Sense of coherence; Depression; Anxiety; Health; Psychological measurement; Discriminant validity; Mental health Introduction Per sonalit y and emotional fac tors have long bee n suggested to have an influence on phy sical hea lth. Res earch eff orts have bee n dire cted to the nega ti ve emotions (e.g., hostility , depress ion, anxiet y) hypothe- sized to affect disease onset and development ( Suls & Bunde, 2005), as well as, positive psychosocial vari- ables (e.g., optimism, social support, sense of coher- ence ) that are assume d to mainta in and enhance health. The tendency among researchers has been to evaluate the independ ent effects of differe nt psychoso - cial factors on physical health, while ignoring possible ove rlap among variabl es (Kapl an, 1995 ). Sense of coherence (SOC) attracted a lot of attention after the devel opment of a quantitative scal e to me asure it. * Support to conduct this research was provided by the Signe and Ane Gyllenberg Foundation. * Corresponding author. Tel.: þ358 919124878. E-mai l address es: hanna.konttinen@helsinki.fi (H. Kon ttine n), ari.haukkala@helsinki.fi ( A. Ha ukka la ), antti.uutela@ktl.fi (A. Uutela). 0277-9 536/$ - see front matte r Ó 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.socscimed.2008.01.053 Socia l Science & Medicine 66 (2008) 2401e2412 www.elsevier.com/locate/socscimed
-
Upload
hamletquiron -
Category
Documents
-
view
220 -
download
0
Transcript of do Sense of Coherence Ansiedad y Sitnomas Depresivos

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 1/12
Comparing sense of coherence, depressive symptoms and anxiety,and their relationships with health in a population-based study*
Hanna Konttinen a,*, Ari Haukkala a, Antti Uutela b
a Department of Social Psychology, University of Helsinki, Unioninkatu 37, P.O. Box 54, 00014 Helsinki, Finland b National Public Health Institute, Finland
Available online 11 March 2008
Abstract
The strong negative correlations observed between the sense of coherence (SOC) scale and measures of depression and anxiety
raise the question of whether the SOC scale inversely measures the other constructs. The main aim of the present study was to
examine the discriminant validity of the three measures by comparing their associations with health indicators and behaviours.
The participants were 25 to 74-year-old Finnish men (n¼ 2351) and women (n¼ 2291) from the National Cardiovascular Risk
Factor Survey conducted in 1997. The SOC scale had high inverse correlations with both depression ( r ¼À0.62 among both
men and women) and anxiety measures (r ¼À0.57 among the men and r ¼À0.54 among the women). Although confirmatory
factor analyses suggested that it was possible to differentiate between SOC, cognitive depressive symptoms and anxiety, the
estimated correlations were even higher than those mentioned above. Education was related only to SOC, but the associations
of SOC, cognitive depressive symptoms and anxiety with self-reported and clinically measured health indicators (body mass index,
blood pressure, cholesterol) and health behaviours were almost identical. The variation in the lowest SOC tertile was more stronglyassociated with health variables than in the highest tertile. To conclude, the size of the overlap between the SOC and depression
scales was the same as between depression and anxiety measures. This indicates that future studies should examine the discriminant
validity of different psychosocial scales more closely, and should compare them in health research in order to bring parallel
concepts into the same scientific discussion.
Ó 2008 Elsevier Ltd. All rights reserved.
Keywords: Finland; Sense of coherence; Depression; Anxiety; Health; Psychological measurement; Discriminant validity; Mental health
Introduction
Personality and emotional factors have long been
suggested to have an influence on physical health.
Research efforts have been directed to the negative
emotions (e.g., hostility, depression, anxiety) hypothe-
sized to affect disease onset and development (Suls &Bunde, 2005), as well as, positive psychosocial vari-
ables (e.g., optimism, social support, sense of coher-
ence) that are assumed to maintain and enhance
health. The tendency among researchers has been to
evaluate the independent effects of different psychoso-
cial factors on physical health, while ignoring possible
overlap among variables (Kaplan, 1995). Sense of
coherence (SOC) attracted a lot of attention after the
development of a quantitative scale to measure it.
* Support to conduct this research was provided by the Signe and
Ane Gyllenberg Foundation.
* Corresponding author. Tel.: þ358 919124878.
E-mail addresses: [email protected] (H. Konttinen),
[email protected] (A. Haukkala), [email protected]
(A. Uutela).
0277-9536/$ - see front matter Ó 2008 Elsevier Ltd. All rights reserved.
doi:10.1016/j.socscimed.2008.01.053
Social Science & Medicine 66 (2008) 2401e2412www.elsevier.com/locate/socscimed

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 2/12
Nevertheless, researchers such as Geyer (1997) have
criticized the ambiguity of the scale and its lack of dis-
criminant validity in relation to the measures of depres-
sion and anxiety.
The sense of coherence construct
Antonovsky (1979, 1987, 1993) proposed a saluto-
genic orientation focusing on factors that protected
individuals’ health. He defined the central concept,
SOC, as an orientation towards life that characterises
the extent to which an individual appraises internal
and external environments as (1) comprehensible, (2)
manageable and (3) meaningful. Antonovsky (1987)
developed these three interrelated dimensions and the
SOC questionnaire on the basis of interviews with
persons who had experienced severe trauma. He
maintained that SOC has much in common with thepsychological constructs of hardiness (Kobasa, 1982),
locus of control (Rotter, 1966) and self-efficacy
(Bandura, 1977).
The SOC scale exists in two forms: the original
29-item questionnaire and the shortened version
including 13 items from the full form. Antonovsky
(1987, p. 87, 1993) designed each item to represent
one of the three dimensions, but he emphasized that
the scale measured the SOC construct unidimension-
ally. The structure of the SOC measure has since
been investigated using both exploratory and confirma-tory factor analysis, but with inconsistent results. Some
studies employing exploratory factor analyses have
supported the one-factor structure proposed by
Antonovsky (e.g., Frenz, Carey, & Jorgensen, 1993),
but other results have also been obtained (e.g., Sandell,
Blomberg, & Lazar, 1998). Furthermore, a confirma-
tory factor analysis study on the 13-item SOC
questionnaire conducted among Finnish working-aged
people found support for the three-factor model (Feldt
et al., 2006). Klepp, Mastekaasa, Sorensen, Sandanger,
and Kleiner (2007), on the other hand, preferred the
one-factor solution for a brief nine-item SOC scale
because the factors in the two- and three-factor models
were very strongly correlated, and the factor scores had
similar correlations with measures of psychological
well-being, depression and anxiety.
The SOC theory hypothesizes that an individual
with a strong SOC maintains and enhances health
through effective and flexible coping with stressors,
such as by adopting health-enhancing and avoiding
unhealthy behaviours (Antonovsky, 1987). An individ-
ual with a strong SOC is also more likely to perceive
internal and social environments as non-stressful.
SOC reduces the health-damaging effects of stress by
lowering the probability of adverse physiological
reactions and negative emotions associated with stress
perceptions. Antonovsky (1987) emphasized that the
consequences of stressors may be negative, neutral or
positive, depending on their nature and the adequacy
of coping. It is also possible that persistent or serious
health problems may influence the development of
SOC.
Numerous cross-sectional studies have found SOC
to be positively associated with physical and psycho-
logical health (Flannery & Flannery, 1990; Larsson
& Kallenberg, 1996; Lundberg, 1997; Pallant & Lae,
2002; Suominen, Blomberg, Helenius, & Koskenvuo,
1999), and health behaviours (e.g., alcohol problems
and physical activity) (Kuuppelomaki & Utriainen,
2003; Midanik, Soghikian, Ransom, & Polen, 1992).
There have been a few longitudinal studies investigat-ing whether SOC predicts health outcomes (e.g., all-
cause mortality and subjective state of health). Most
of these have supported its predictability (Suominen,
Helenius, Blomberg, Uutela, & Koskenvuo, 2001;
Surtees, Wainwright, Luben, Khaw, & Day, 2003),
but inconsistent results have also been reported.
Kivimaki, Feldt, Vahtera, and Nurmi (2000) found in
their study of municipal employees that SOC predicted
sickness absence only among the women. Other
research among people with chronic illness reported
reciprocal causation between SOC and domains of health (Veenstra, Moum, & Roysamb, 2005). Overall,
the SOC relationship with psychological well-being
seems to be stronger and more direct than that with
physical health (Eriksson & Lindstrom, 2006).
Depressive symptoms and anxiety
The conceptual and empirical relationship between
depression and anxiety has been studied extensively,
and the evidence suggests that it is difficult to differen-
tiate these two constructs empirically. The emotion of
fear has a central role in anxiety, which involves
feelings of worry, apprehension and dread (Watson &
Kendall, 1989). The essential characteristic of depres-
sion is sadness, with associated feelings of sorrow,
hopelessness and gloom. Self-reported depression and
anxiety have been highly correlated (typically between
0.45 and 0.75) in both psychiatric and non-psychiatric
samples (Clark & Watson, 1991). Considerable co-
morbidity has also been observed (Mineka, Watson,
& Clark, 1998).
The strong relationship between depression and
anxiety may reflect problems with existing scales
2402 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 3/12
and constructs. There is an overlap in many of the
symptoms that define both syndromes, and many
self-report scales also contain items that actually
measure the other construct (Gotlib & Cane,
1989). Thus, Clark and Watson (1991) proposed a tri-
partite model of depression and anxiety: general
distress or negative affect is common to both, while
manifestations of low positive affect are specific to
depression, and symptoms of somatic arousal signify
anxiety.
The two best-known theories of depression are
perhaps Beck’s (1967, 1987) cognitive theory and
Abramson, Metalsky, and Alloy’s (1989) hopelessness
theory. They both posit that cognitive vulnerability and
negative life stress together precipitate depression.
According to Beck (1987), dysfunctional attitudes
involving feelings of loss, inadequacy, failure and
worthlessness constitute cognitive vulnerability todepression, whereas in the view of Abramson et al.
(1989), cognitive depression diathesis encompasses
the general tendency to attribute negative events to sta-
ble and global causes, to infer negative consequences,
and/or to infer negative characteristics about the self.
In addition, Beck (1987) postulates that all depressed
people show a cognitive triad: automatic thoughts
reflecting negative views of the self, the world and
the future. It is suggested that the degree of this
negative thinking is directly related to the severity of
other depressive symptoms.The SOC construct could be integrated as a protec-
tive/risk factor into vulnerability-stress models of
depression. Individuals with a strong SOC should be
better able to maintain their emotional well-being in
stressful situations, whereas those with a weak SOC
share some of the cognitive vulnerability factors men-
tioned in Abramson et al.’s (1989) and Beck’s (1967)
theories. All this raises a question concerning vulnera-
bility and protective factors in general: do they form
different dimensions or are they merely opposite ends
of a continuum? Antonovsky (1987) considered risk
and protective factors qualitatively different. The
SOC construct also shares similarities with cognitive
and emotional features of depression, which raises
the question of whether a weak SOC represents depres-
sion. Overall, SOC describes individuals’ cognitive
and emotional functioning on a more general level
than theories of depression. In addition, the SOC
theory is more oriented towards societal determinants
(e.g., education) of health than depression theories.
There is evidence that people in higher socio-economic
positions have a stronger SOC (Lundberg & Nystrom
Peck, 1994).
The relationship of SOC with depressive
symptoms and anxiety
High negative associations have been consistently
observed between the SOC scale and measures of
depressive symptoms and anxiety. In studies published
between 1992 and 2003, the correlation coefficients
between the scale and different measures of anxiety
and depression varied from À0.29 to À0.82 and
from À0.34 to À0.90, respectively (Eriksson & Lind-
strom, 2005). Gruszczynska (2006) calculated the
mean weighted SOC correlations on the basis of 17
studies: À0.70 for anxiety and À0.65 for depression.
The size of these correlations raises doubts about the
construct validity of the SOC questionnaire. Thus, it
has been proposed that rather than being a measure
of resilience, the scale measures inversely negative
affectivity/neuroticism (Frenz et al., 1993; Strumpfer,Gouws, & Viviers, 1998; Watson & Clark, 1984).
There are a few studies that have investigated the
relationships between SOC, anxiety, and depression.
When confirmatory factor analysis was used, the 29-
item SOC scale loaded on the same latent variable as
the measures of trait anxiety, neuroticism, optimism,
depression and self-efficacy (Gruszczynska, 2006),
and also on both the health-proneness and negative-
affect factors (Kravetz, Drory, & Florian, 1993). Feldt,
Metsapelto, Kinnunen, and Pulkkinen (2007) found
that a high SOC (measured on the 13-item question-naire) was strongly associated (r ¼À0.86) with
reversed neuroticism in their confirmatory model.
Korotkov (1993) concluded from his four-week
prospective study that the 13-item SOC instrument
lacked face, construct and predictive validity, and
that most of the items measured emotionality (neurot-
icism) rather than SOC. Meanwhile, Breslin, Hepburn,
Ibrahim, and Cole (2006) recently analysed the longi-
tudinal relationship between psychological stress and
the 13-item SOC scale, and found that the stable
components of distress and SOC were strongly inter-
correlated (r ¼ 0.86). On the other hand, Strumpfer
et al. (1998) conceptualised the low end of negative af-
fectivity as emotional stability, and interpreted the
strong negative associations between both versions of
the SOC instrument and the negative-affectivity scales
as supporting the validity of the instrument. However,
the SOC measures were more strongly associated
with negative than with positive emotionality.
In sum, the few previous studies focusing on the
relationship between the SOC scale and measures of
negative emotions have yielded inconclusive results.
SOC, depressive symptoms and anxiety have all been
2403 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 4/12
related to various health indicators and behaviours, but
to our knowledge their associations with health-related
variables have not been compared in any previous
study. The purpose of the present study therefore was
to investigate the discriminant validity of the SOC,
depression and anxiety scales in a population-based
sample. In more specific terms: (1) first, we examined
the strength of the correlations between the measures
of SOC, depressive symptoms and anxiety, and con-
firmed these with a confirmatory model that takes mea-
surement error into account. (2) Our main aim was to
assess the discriminant validity between SOC, depres-
sion and anxiety scales by comparing their associations
with subjective and objective (body mass index, blood
pressure, total cholesterol) health indicators, health
behaviours and sociodemographic factors. If the SOC
scale and the measures of depressive symptoms and
anxiety are distinct measures, they should also bedifferentially related to other variables. (3) Finally,
we wished to find out whether variation in the SOC
was more strongly related to health variables at the
high or low end of the distribution. The questionnaire
produces variation among individuals with a weak
and a strong SOC. Most depression inventories, on
the other hand, do not account for variation among
the non-depressed as they assess only the intensity of
depressive symptoms. Antonovsky specifically hypoth-
esized that a strong SOC, and not just the absence of
weak SOC, protected health. If variation at the highend were associated with health measures, then this
would give the SOC scale an advantage over depres-
sion measures.
Methods
Participants
The participants comprised a random sub-sample of
the national cardiovascular risk factor survey (FIN-
RISK) conducted in Finland in 1997 (Vartiainen
et al., 2000). FINRISK 97 covered a random sample
of 11,500 people aged 25e74 drawn from the Finnish
population registers in five areas, (1) North Karelia
Province, (2) Kuopio Province, (3) South-Western
Finland, (4) the cities of Helsinki and Vantaa in the
capital area, and (5) the northern province of Oulu.
The sample was stratified according to gender,
10-year age groups, and area. In the age bracket
25e64 years there were 250 men and 250 women in
each 10-year age group in each region. In addition,
the sample included 500 men and 250 women aged
65e
74 from North Karelia Province and from the
Helsinki metropolitan area, respectively. Two-thirds
of these participants were randomly assigned to the
present study of psychosocial factors (n¼ 7103).
The participants received by mail a self-adminis-
tered health questionnaire including questions on soci-
odemographic factors (gender, education and income),
health behaviours (smoking and alcohol consumption),
and health (self-rated health, visits to a physician,
somatic and psychological symptoms). They were
asked to fill in the questionnaire at home, and to return
it to the health centre when they came for a medical
examination in which their weight, height and blood
pressure were measured, and blood samples were
taken. A self-administered psychosocial questionnaire
was then given to a sub-sample of these participants,
to be answered afterwards at home. This comprised
a 13-item SOC questionnaire followed by a 21-item
depression inventory and a six-item anxiety inventory.All three scales were separated by a number of other
items. Only the respondents who participated in all
three phases were included in the present study. The
final response rate was 67% (men, n¼ 2351; women,
n¼ 2291).
Measures
Sense of coherence (SOC)
We used a Finnish-language version of Antonov-
sky’s (1987) 13-item orientation to life questionnaireconsisting of four meaningfulness, five comprehensi-
bility, and four manageability items to measure SOC
(for the items and their order in the questionnaire,
see Fig. 1). The respondents were asked to indicate
the number that expressed their feeling best on
a seven-point scale with two anchoring phrases (e.g.,
1¼ very often, 7¼ very seldom or never). As recom-
mended initially by Antonovsky (1993) and recently
by Feldt et al. (2006), one total SOC score was calcu-
lated from the ratings of the 13 questions. The SOC
scores varied from 16 to 91, the higher scores reflecting
stronger SOC. The scale was internally consistent on
the basis of the Cronbach’s alpha criterion (0.86).
Confirmatory factor analysis (with maximum likeli-
hood estimation) was used to compare the applicability
of a one-factor and a correlated three-factor model of
the SOC items to the present data. An adequate fit
was obtained for both models after four error-term
covariances in the one-factor and one error-term
covariance in the three-factor solution were released:
c2 (61)¼ 838.20, p< 0.001; comparison fit index
(CFI)¼ 0.95; root mean square error of approximation
(RMSEA)¼ 0.06 (CI 90%: 0.05e
0.06); Akaike’s
2404 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 5/12
information criterion (AIC)¼ 898.20 for the one-factor
model, and c2 (61)¼ 1006.32, p< 0.001; CFI¼ 0.94;
RMSEA¼ 0.06 (CI 90%: 0.06e0.06); AIC¼ 1066.32
for the three-factor model. The factors were highly
correlated in the three-factor solution (r coÂma¼ 0.94;
r maÂme¼ 0.86; r coÂme¼ 0.76). The three-factor model
could be considered slightly better than the one-factor
model in which we had to release several error-term
covariances based on the largest modification indexes.
However, we decided to use the one-factor solution in
the later confirmatory model because the correlations
between the factors were so high (see also Klepp
et al., 2007).
Depressive symptoms
Depressive symptoms were measured on the Finnish
version of the Beck depression inventory (BDI) (Beck,
Ward, Mendelson, Mock, & Erbaugh, 1961; Raitasalo,
1977). The BDI is a self-administered 21-item ques-
tionnaire covering the intensity of depressive symp-
toms. Each item includes four or five self-evaluative
statements, which carry a numerical value from 1 to
3 reflecting the intensity of the symptom. The respon-
dents were asked to choose for each item one statement
or more that best described their current situation. If
they had selected more than one option, which was
rare, the one indicating the highest level of depression
Depression
Pessimism
Punish-
ment
Self hate
Self-
accusations
Self-punitive
wishes
Crying
Irritability
Unsatis-
faction
Guilty
Indeci-
siveness
Mood
Failure
Social
withdrawal
.73
.64
.59
.61
.66
.51
.63
.55
.52
.49
.26
.50
.59
.35
.41
.40
.37
.43
.26
.54
.30
.28
.24
.07
.25
.34
Sense of
coherence
2 CO
6 CO
7 ME
8 CO
9 CO
10 MA
11 CO
4 ME
5 MA
13 MA
1 ME
3 MA
12 ME
.21
.15
.18
.29
.28
.36
.27
.53
.47
.14
.46
.51
Anxiety
Worried CalmContent Relaxed Upset Tense
.30
.46
.39
.42
.54
.52
.60
.52
.73
.69
.55
.37
.68
.71
.37
.20
.49
-.75
.76-.65
.60 .75 .76 .55 .71 .80
.36 .56 .58 .31 .51 .64
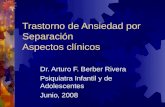
Fig. 1. The first-order correlated three-factor model of the SOC (sense of coherence) scale, BDI-13 (Beck depression inventory without the eight
somatic symptoms) and STAI (state anxiety inventory) with standardized parameter estimates (note: ME¼meaningfulness item;
CO¼ comprehensibility item; MA¼manageability item). The SOC items: 1 (ME) Do you have the feeling that you don’t really care what
goes on around you?; 2 (CO) Has it happened in the past that you were surprised by the behaviour of people whom you thought you knew
well?; 3 (MA) Has it happened that people whom you counted on disappointed you?; 4 (ME) Until now your life has had: no clear goals or
purpose at all e very clear goals and purpose; 5 (MA) Do you have the feeling that you’re being treated unfairly?; 6 (CO) Do you have the feeling
that you are in an unfamiliar situation and don’t know what to do?; 7 (ME) Doing the things you do every day is: a source of deep pleasure and
satisfactione a source of pain and boredom; 8 (CO) Do you have very mixed-up feelings and ideas?; 9 (CO) Does it happen that you have feelings
inside you would rather not feel?; 10 (MA) Many people e even those with a strong character e sometimes feel like sad sacks (losers) in certain
situations. How often have you felt this way in the past?; 11 (CO) When something happened, have you generally found that: you overestimated or
underestimated its importance e you saw things in the right proportion; 12 (ME) How often do you have the feeling that there’s little meaning in
the things you do in your daily life?; 13 (MA) How often do you have feelings that you’re not sure you can keep under control?
2405 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 6/12
was coded on the data. We derived the BDI score by
summing up the ratings given to each of the 21 items.
It varied from 0 to 61 and showed good internal
consistency (Cronbach’s alpha¼ 0.87).
BDI covers eight somatic symptoms (distortion of
body image, work inhibition, sleep disturbance,
fatigability, loss of appetite, weight loss, somatic pre-
occupation and loss of libido) and 13 psychological
symptoms. A measure of depressive symptoms includ-
ing only these 13 psychological symptoms (referred to
as BDI-13 or cognitive depressive symptoms) was also
included as somatic symptoms could also indicate age-
ing and physical health problems.
Anxiety
The six-item short form of the state scale of the
Spielberger State-Trait Anxiety Inventory (STAI)
(Marteau & Bekker, 1992) was used to measure stateanxiety: this has been found comparable to the full
form. The participants were asked to rate the six items
(e.g., ‘‘I am tense’’) from 1 (not at all) to 4 (very
much) according to how they felt at that moment.
The ratings given to each item were summed so that
higher STAI scores reflected higher anxiety. The short
form of the STAI was internally consistent (Cronba-
ch’s a¼ 0.85) and its range was from 6 to 24 in
this sample.
Self-rated healthThe question, What is your opinion about your cur-
rent health condition (1¼ very bad; 5¼ very good)?
was used to assess self-rated health.
Visits to a physician
Visits to a physician were covered by the question,
How many times have you visited a doctor during the
past year (12 months)?
Somatic and psychological symptoms
The participants were asked to indicate (from
1¼ often to 3¼ never) how often they had somatic
or psychological symptoms in the previous 30 days.
Somatic symptoms included tachycardia, trembling of
the hands, an irregular heart rate, dizziness, headache,
and sweaty palms, while psychological symptoms in-
cluded feeling confused when having to do something
quickly, feeling tense and nervous, having frightening
thoughts, feeling exhausted and overstrained, having
nightmares, depressiveness, and sleeplessness. The
mean scores of the ratings of the seven psychological
and six somatic symptoms were calculated separately
(Cronbach’s a¼ 0.81 and 0.67, respectively). The
scores varied from 1 to 3, the higher ones indicating
more symptoms.
Smoking status
Participants who reported that they had been
smoking regularly (more than once a day) for at least
a year, and had been doing so during the preceding
month, were classified as current smokers, and were
compared to former and never smokers in the analyses.
Alcohol consumption
Alcohol consumption was assessed by means of
a self-report questionnaire inquiring into the usual
quantity and frequency of consuming various bever-
ages (Poikolainen, Poldkletnova, & Alho, 2002). The
average weekly alcohol consumption (grams of pure
alcohol per week) was estimated based on this
information.
Body mass index (BMI)
Body mass index was calculated as weight in
kilograms (measured to the nearest 100 g in light
clothing) divided by the square of height in meters
(measured to the nearest 0.5 cm).
Blood pressure
Blood pressure was measured twice after 5 min of
rest in a sitting position and the average systolic value
was used in the analyses.
Cholesterol
An enzymatic method was used to analyse the
serum total cholesterol value from serum samples.
Education
Education was assessed on a continuous scale based
on the self-reported number of years of schooling.
Income
Income was measured in terms of the self-reported
household gross income during the previous 12 months,
the response alternatives ranging from (1) less than
40,000 to (9) more than 320,000 Finnish marks (the
Finnish currency is now the euro, one euro correspond-
ing to 5.95 Finnish marks).
Statistical methods
Pearson correlation coefficients were used in
assessing the associations between the SOC, depressive
symptoms, anxiety and sociodemographic variables
(years of education were age-adjusted), and the
2406 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 7/12
relationships between the SOC scale, BDI-13 and
STAI were further examined by means of confirmatory
factor analyses (with maximum likelihood estimation).
Correlations with health and health-behaviour indica-
tors were controlled for age. We used a method for
testing the significance of the difference between the
dependent correlation coefficients in order to deter-
mine whether the SOC scale correlated with the health
indicators and behaviours to a significantly different
degree than BDI, BDI-13 or STAI (Cohen & Cohen,
1983). Finally, we tested equality of the strength of
the correlations among the SOC and various health-
related variables between the lowest and the highest
SOC tertiles (Cohen & Cohen, 1983). All the analyses
except the factor analyses were conducted separately
for men and women because this study included
variables (depressive symptoms and health-related
measures) that normally feature gender differences.Cases with missing values were excluded. Amos 7
and SPSS 15.0 were used.
Results
Table 1 presents the descriptive statistics for SOC,
depressive symptoms, anxiety and sociodemographic
factors, and the Pearson correlations between these
variables separately for men and women. Correlation
coefficients of less than 0.10 were not considered note-
worthy, although they became statistically significantdue to the large sample size.
The mean age was 51.3 years (SD¼ 13.8) for the
2065 men and 47.1 years (SD¼ 12.7) for the 2002
women (Table 1). The SOC mean score was 65.6
(SD¼ 11.8) among men and 64.8 (SD¼ 11.8) among
women, and was significantly higher for men ( p¼
0.006, h2¼ 0.002). The males (8.0, SD¼ 7.3) had
a significantly lower BDI mean score than females
(8.7, SD¼ 7.5) ( p¼ 0.001, h2¼ 0.003). A similar
phenomenon was observed when the eight somatic
symptoms of the BDI were excluded. In contrast, the
male and female STAI mean scores did not differ
(for the males: 10.4, SD¼ 3.0; for the females: 10.4,
SD¼ 3.1).
As Table 1 shows, SOC, depressive symptoms and
anxiety were highly associated in both genders. The
correlation between SOC and BDI was r ¼À0.62 for
all of the participants, and corresponding results were
found for BDI and STAI (r ¼ 0.64 in males and r ¼
0.65 in females). The association between SOC and
STAI (r ¼À0.57 for men and r ¼À0.53 for women)
was significantly lower than that between SOC and
BDI in both genders ( p< 0.01). The exclusion of the
eight somatic symptoms from the BDI did not affect
these correlations.
Confirmatory analysis was also used to investigate
the relations between SOC, cognitive depressive
symptoms and anxiety. A model was specified in
which cognitive and affective BDI items loaded on
the depression factor, the SOC items on the SOC fac-
tor, and the STAI items on the anxiety factor. These
three latent variables were specified to correlate. This
model did not fit the data adequately based on the fit
indexes: c2 (461)¼ 6345.43, p< 0.001; SRMR¼
0.04; CFI¼ 0.88; RMSEA¼ 0.06 (CI 90%: 0.05e0.06);
AIC¼ 6479.43. After three error-term covariances
between the SOC items were released on the basis of
the largest modification indexes, the model provided
a satisfactory fit with the data: SRMR¼ 0.04;
CFI¼ 0.91; RMSEA¼ 0.05 (CI 90%: 0.05e0.05);
AIC¼ 4712.18. The chi-square value was still signifi-cant (c2 (458)¼ 4572.18, p< 0.001), but the above-
mentioned fit indexes suggested that this was due to
the large sample size. As Fig. 1 indicates, the depres-
sion factor correlated highly with both the SOC and
anxiety factors (r ¼À0.75 and 0.76, respectively),
but it is possible to separate these constructs. The in-
ter-correlation of the SOC and anxiety factors was
also strong (r ¼À0.65).
The associations of SOC, depressive symptoms
and anxiety with sociodemographic factors were
somewhat different (Table 1). Age was related todepressive symptoms: the older men and women
were more depressed. However, this association
disappeared when the eight somatic symptoms of
the BDI were excluded. The younger participants
showed more anxiety, but these correlations were
weak (r ¼À0.07 among males and r ¼À0.06 among
females). Years of education were age-adjusted
because of the rapid rise in the level of education
in recent decades (r educationÂage¼À0.45 for the men
and r educationÂage¼À0.50 for the women, respec-
tively). Education was related to SOC, but not to
BDI, BDI-13 or STAI, after controlling for age:
more educated men and women had higher SOC
scores (Table 1). In contrast, income was associated
with SOC and depressive symptoms: SOC increased
and depression decreased as the income level rose.
We further investigated the discriminant validity of
the SOC scale by comparing the associations of SOC,
depressive symptoms and anxiety with health indica-
tors and health behaviours. Higher SOC scores and
lower depression and anxiety scores were related to
better self-rated health, fewer visits to a doctor, and
less somatic and psychological symptoms in both
2407 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 8/12
genders (Table 2). There were some differences be-
tween the males and females: SOC, depressive symp-
toms and anxiety were all related to smoking and
alcohol consumption among the men, but no such asso-
ciations emerged among the women. However, SOC,
BDI, BDI-13 and STAI showed no associations with
BMI, systolic blood pressure or total cholesterol levels
in either gender. These results suggest that SOC, de-
pressive symptoms and anxiety have inverse but other-
wise comparable relations with health indicators and
behaviours.
A comparison of the magnitude of the correlations
listed in Table 2 showed that BDI had significantly
higher correlations with self-rated health, psychologi-
cal and somatic symptoms, and visits to a physician
than the SOC scale ( p< 0.01). However, this differ-
ence remained significant only for psychological
symptoms among males when the eight somaticsymptoms were excluded. Comparisons between the
SOC scale and STAI indicated that these variables
were associated with all health indicators and health
behaviours to the same degree in both genders. Thus,
of the 54 comparisons of correlation coefficients, 45
indicated relationship equality.
The SOC score tertiles were then used to investigate
whether the variation in a low or high SOC was more
strongly associated with health and health-behaviour
variables. As Table 3 shows, SOC was related to self-
rated health and visits to a physician among the menand women whose SOC score fell into the lowest
SOC tertile, but there were no such relations in the high-
est tertile ( p< 0.05). SOC was associated with somatic
and psychological symptoms in both the lowest and
highest tertiles, but the correlations were stronger in
the lowest tertile among the men ( p¼ 0.035 for somatic
and p< 0.001 for psychological symptoms). The
strength of the associations among SOC and alcohol
consumption, smoking, BMI, blood pressure and cho-
lesterol were equal between the lowest and highest
tertiles, but all these correlations were low and most
of them were non-significant.
Discussion
We found strong relationships between the SOC
scale and measures of depressive symptoms and
anxiety in a representative population sample of 25
to 74-year-old Finnish people. These associations
became stronger when we applied structural equation
modelling, which takes measurement error into
account. The main aim of our study was to examine
the discriminant validity between the SOC, depression T a
b l e 1
T h e c o r r e l a t i o n c o e f fi c i e n t s b e t w e e n S O C , d
e p r e s s i v e s y m p t o m s , a n x i e t y a n d t h e s o c i o
d e m o g r a p h i c v a r i a b l e s
M e n ( n ¼
2 0 6 5 )
W o m e n ( n ¼
2 0 0 2 )
S O C
B D I
B D I - 1 3
S T A I
M e a n ( S D )
M i n e M a x
S O C
B D I
B D I - 1 3
S T A I
M e a n (
S D )
M i n e M a x
S O
C
1 . 0 0
6 5 . 6 ( 1 1 . 8 )
1 9 e 9 1
1 . 0 0
6 4 . 8 ( 1 1 . 8 )
1 6 e 9 1
B D I
À 0 . 6 2
1 . 0 0
8 . 0 ( 7 . 3 )
0 e 4 7
À 0 . 6 2
1 . 0 0
8 . 7 ( 7 . 5 )
0 e 4 6
B D I - 1 3
À 0 . 6 3
0 . 9 4
1 . 0 0
4 . 6 ( 5 . 1 )
0 e 3 4
À 0 . 6 2
0 . 9 5
1 . 0 0
5 . 2 ( 5 . 2 )
0 e 3 0
S T
A I
À 0 . 5 7
0 . 6 4
0 . 6 5
1 . 0 0
1 0 . 4 ( 3 . 0 )
6 e 2 4
À 0 . 5 3
0 . 6 5
0 . 6 3
1 . 0 0
1 0 . 4 ( 3 . 1 )
6 e 2 4
A g e ( y e a r s )
0 . 0 3 *
0 . 1 3
À 0 . 0 3 *
À 0 . 0 7
5 1 . 3 ( 1 3 . 8 )
2 5 e 7 4
À 0 . 0 0 *
0 . 1 4
0 . 0 3 *
À 0 . 0 6
4 7 . 1 ( 1 2 . 7 )
2 5 e 7 4
E d u c a t i o n ( y e a r s ) a
0 . 1 2
À 0 . 0 4
À 0 . 0 2 *
À 0 . 0 1 *
1 1 . 9 ( 4 . 1 )
1 e 5 4
0 . 1 1
À 0 . 0 6
À 0 . 0 4
0 . 0 3 *
1 1 . 9 ( 3 . 9 )
1 e 4 0
I n c o m e
0 . 2 0
À 0 . 1 6
À 0 . 1 3
À 0 . 0 9
0 . 1 7
À 0 . 1 6
À 0 . 1 3
À 0 . 0 6
* N
o t s i g n i fi c a n t ( a t t h e p <
0 . 0 5 l e v e l ) .
S O
C ¼
s e n s e o f c o h e r e n c e s c a l e ; B D I ¼
B e c
k d e p r e s s i o n i n v e n t o r y ; B D I - 1 3 ¼
B e c k d e p r e s s i o n i n v e n t o r y w i t h o u t t h e e i g h t s o m a t i c s y m p t o m s ; S T A I ¼
s t a t e a n x i e t y i n v e n t o r y .
a
A d j u s t e d f o r a g e .
2408 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 9/12
and anxiety scales by comparing their relations with
health-related and sociodemographic variables. Educa-
tion was related only to SOC, but the associations of
SOC, cognitive depressive symptoms and anxiety
with health indicators and health behaviours were
practically identical in both genders. Our eventual
aim was to find out whether variation at the high end
of the SOC distribution is related to health measures.
The inter-correlations among the SOC and health
variables were stronger among the respondents in the
lowest than among those in the highest SOC tertile.
The SOC scores had a high negative association with
both depression (r ¼À0.62 for the men and the women)
and anxiety (r ¼À0.57 for the men and À0.53 for the
women), which is consistent with previous findings
(Eriksson & Lindstrom, 2005). Although factor analy-
ses suggested that it was possible to differentiate
between the SOC, cognitive depressive symptoms andanxiety variables, the estimated correlations were
even higher than those mentioned above. The relation-
ship between SOC and depressive symptoms was as
strong as that between depressive symptoms and
anxiety. This was particularly interesting given
evidence from extensive studies on the close relation-
ship between depression and anxiety (Gotlib & Cane,
1989).
A comparison of the SOC and the BDI items
revealed some content overlap. Four meaningfulness
items and one manageability item (numbered 1, 4, 7,10 and 12, see Fig. 1) could be interpreted as reflecting
symptoms measured with the BDI (lack of satisfaction,
social withdrawal, sense of failure, guilty feeling and
self accusations), and two comprehensibility items
(numbered 8 and 9, see Fig. 1) seemed to assess
negative emotional experiences in general. In addition,
two manageability items and one comprehensibility
item (numbered 2, 3 and 5, see Fig. 1) were more likely
to measure interpersonal trust/mistrust than the man-
ageability or comprehensibility dimensions of SOC.
In previous factor-analytic studies, these items have
formed their own factor, which has been interpreted
as reflecting interpersonal trust or mistrust (e.g.,
Sandell et al., 1998). Factor analyses conducted on
the present data also indicated that the structure of
the SOC scale was rather ambiguous. This is no
wonder as half of the items could be interpreted as as-
sessing symptoms of depression or negative emotions.
The relationships of the SOC, depression and
anxiety scales with years of education revealed some
differences between these measures: educational level,
controlled for age, was associated only with SOC.
Household annual income, however, was associated T a
b l e 2
T h e a g e - a d j u s t e d c o r r e l a t i o n c o e f fi c i e n t s b e t w e e n S O C , d e p r e s s i v e s y m p t o m s , a n x i e t y
a n d h e a l t h - r e l a t e d v a r i a b l e s
M e n ( n ¼
1 9 5 4 )
W o m e n ( n ¼
1 9 4 3 )
S O
C
B D I
B D I - 1 3
S T A I
M e a n ( S D )
M i n e M a x
S O C
B D I
B D I - 1 3
S T A I
M e a n ( S D )
M i n e M a x
S e
l f - r a t e d h e a l t h
0 .
3 0
À 0 . 3 8
L 0 . 2
9
L 0 .
3 1
3 . 5 ( 0 . 8 )
1 e 5
0 .
2 6
À 0 . 3 4
L 0 .
2 7
L 0 .
2 8
3 . 7 ( 0 . 8 )
1 e 5
V i s i t s t o a p h y s i c i a n ( t i m e s / p a s t y e a r )
L 0 .
1 3
0 . 2 4
0 .
1 8
0 .
1 8
2 . 7 ( 4 . 2 )
0 e 9 9
L 0 .
1 4
0 . 2 1
0 .
1 6
0 .
1 7
3 . 5 ( 4 . 2 )
0 e 9 2
S o
m a t i c s y m p t o m s a
L 0 .
3 2
0 . 4 1
0 . 3
4
0 .
3 4
1 . 4 ( 0 . 3 )
1 . 0 e 2 . 8
L 0 .
3 2
0 . 4 1
0 .
3 7
0 .
3 3
1 . 5 ( 0 . 3 )
1 . 0 e 3 . 0
P s
y c h o l o g i c a l s y m p t o m s b
L 0 .
5 1
0 . 6 1
0 . 5 6
0 .
5 5
1 . 5 ( 0 . 4 )
1 . 0 e 3 . 0
L 0 .
5 3
0 . 6 0
0 .
5 7
0 .
5 4
1 . 6 ( 0 . 4 )
1 . 0 e 3 . 0
S m
o k i n g s t a t u s c
L 0 .
1 1
0 .
1 4
0 . 1
4
0 .
1 0
L 0 .
0 8
0 .
0 9
0 .
0 8
0 .
0 6
A l c o h o l c o n s u m p t i o n ( a b s . g / w e e k )
L 0 .
1 1
0 .
1 4
0 . 1
3
0 .
0 9
1 0 3 . 2 ( 1 4 9 . 3 )
0 . 0 e 1 5 1 . 5
L 0 .
0 2 *
0 .
0 1 *
0 .
0 3 *
0 .
0 4 *
4 2 . 6 ( 8 2 . 0 )
0 . 0 e 9 3 . 8
B M I ( k g / m
2 )
L 0 .
0 4 *
0 .
0 7
0 . 0
3 *
0 .
0 3 *
2 6 . 9 ( 3 . 8 )
1 4 . 7 e 4 7 . 9
L 0 .
0 6
0 .
0 7
0 .
0 4 *
0 .
0 1 *
2 6 . 1 ( 4 . 8 )
1 5 . 4 e 5 1 . 6
S y
s t o l i c b l o o d p r e s s u r e ( m m H g )
0 .
0 2 *
L 0 .
0 1 *
L 0 .
0 0 *
0 .
0 2 *
1 4 0 . 3 ( 1 9 . 6 )
7 8 . 0 e 2 1 9 . 0
0 .
0 4 *
L 0 .
0 4 *
L 0 .
0 4 *
L 0 .
0 5
1 3 1 . 5 ( 1 9 . 5 )
8 1 . 0 e 2 2 5 . 0
C h o l e s t e r o l ( m m o l / l )
L 0 .
0 2 *
0 .
0 2 *
0 .
0 4 *
0 .
0 2 *
5 . 6 ( 1 . 0 )
2 . 4 - 1 0 . 5
L 0 .
0 5
0 .
0 2 *
0 . 0
3 *
L 0 .
0 1 *
5 . 5 ( 1 . 1 )
2 . 7 e 1 0 . 3
* N
o t s i g n i fi c a n t ( a t t h e p <
0 . 0 5 l e v e l ) .
T h e s t r e n g t h o f t h e c o r r e l a t i o n c o e f fi c i e n t s m a r k e d i n b o l d i s s i m i l a r t o t h e c o e f fi c i e n t s b e
t w e e n S O C a n d d i f f e r e n t h e a l t h - r e l a t e d v a r i a b l e s . S O C ¼
s e n s e o f c o h e r e n c e s c a l e ; B D
I ¼
B e c k d e p r e s s i o n
i n v e n t o r y ; B D I - 1 3 ¼
B e c k d e p r e s s i o n i n v e n t o r y w i t h o u t t h e e i g h t s o m a t i c s y m p t o m s ; S T A I ¼
s t a t e a n x i e t y i n v e n t o r y ; B M I ¼ b o d y m a s s i n d e x .
a
A r a p i d h e a r t r a t e , s h a k i n g h a n d s , a n i r r e
g u l a r h e a r t r a t e , d i z z i n e s s , h e a d a c h e , a n d
s w e a t y h a n d s .
b
F e e l i n g c o n f u s e d w h e n h a v i n g t o d o s o m
e t h i n g q u i c k l y , f e e l i n g t e n s e a n d n e r v o u s , h a v i n g f r i g h t e n i n g t h o u g h t s , f e e l i n g e x h a u s t e d a n d o v e r s t r a i n e d , h a v i n g n i g h t m a r e s , d e p r e s s i v e n e s s , a n d
s l e e p l e s s n e s s .
c
N e v e r / f o r m e r s m o k e r s ¼
1 ; c u r r e n t s m o k
e r s ¼
2 .
2409 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 10/12
with both SOC and depression. In addition, the levels
of both SOC and depressive symptoms varied accord-
ing to gender: women had a significantly lower SOC
mean score and a higher BDI mean score than men.
Age was not related to SOC in these data, although
not all population studies have found SOC to be
independent of age (Larsson & Kallenberg, 1996).
Antonovsky (1987) developed SOC as an explana-tory concept related to health. Hence, the main interest
in this study was to compare the associations of SOC,
depressive symptoms and anxiety with health
indicators and behaviours. Consistent with the results
of previous studies (Eriksson & Lindstrom, 2006;
Friedman & Booth-Kewley, 1987), SOC was positively
and depressive symptoms and anxiety were negatively
associated with various health-related measures. The
full 21-item BDI includes eight somatic symptoms
that, in addition to depression, are directly related to
ageing and physical health (r ageÂBDI¼ 0.13 for the
men and 0.14 for the women). Thus, to avoid possible
bias, the 13-item BDI, which includes only cognitive
and affective symptoms (r ageÂBDI-13¼À0.03 for the
men and 0.03 for the women), is more appropriate in
terms of comparing the relationships of SOC and de-
pressive symptoms with health indicators. The SOC
scale, BDI-13 and STAI were associated to an equal
magnitude with all the subjective and objective health
indicators used in the present study. The only exception
was that BDI-13 had a significantly higher correlation
with psychological symptoms among the men than the
SOC measure. However, this difference was not
sizeable, becoming statistically significant due to the
large sample size (r SOCÂpsychological symptoms¼À0.51
and r BDI-13Âpsychological symptoms¼ 0.56). Furthermore,
the strength of the correlations of the SOC scale,
BDI, BDI-13 and STAI with health behaviours
(smoking and alcohol consumption) was consistent.
We also examined whether variation at the high end
of the SOC was related to health measures, as depres-sion inventories do not extend to the positive end. The
resulting analyses with the SOC tertiles indicated that
the variation at the low end was more strongly associ-
ated with health variables than the variation at the high
end. This is consistent with the findings reported by
Kivimaki et al. (2000): it was only a low and not
a high SOC that predicted health (sickness absence).
These results could be interpreted to imply that a strong
SOC is not necessary for good health, although it may
have a positive impact on other aspects of the quality
of life.
The present study included quite a wide range of
health-related measures: self-reported health indicators
and health behaviours, and clinically measured health
indicators (BMI, systolic blood pressure and total
cholesterol). SOC, depressive symptoms and anxiety
all had the strongest correlations with self-assessed
health variables. It is possible that self-reported health
indicators are confounded by psychological character-
istics and emotional states. For example, people with
depressive symptoms or anxiety may report more phys-
ical symptoms, and may visit a physician more often
because negative mood states result in negative biases
Table 3
The correlation coefficients between SOC and health-related variables by SOC tertiles
Men Women
Low SOCa
(n¼ 626)
Medium SOCb
(n¼ 717)
High SOCc
(n¼ 741)
Low SOCa
(n¼ 708)
Medium SOCb
(n¼ 682)
High SOCc
(n¼ 678)
Self-rated health 0.18*** 0.10** 0.06 0.20***À
0.01 0.00Visits to a physician (times/past year) À0.13** À0.01 À0.01 À0.17*** 0.05 À0.04
Somatic symptoms À0.25*** À0.06 À0.14*** L0.21*** À0.01 L0.13**
Psychological symptoms À0.39*** À0.10* À0.20*** L0.37*** À0.05 L0.31***
Alcohol consumption (abs. g/week) L0.10* À0.04 L0.03 L0.02 0.03 L0.05
Smoking statusdL0.06 À0.05 L0.02 L0.06 À0.05 L0.09*
BMI (kg/m2) L0.01 À0.03 0.01 L0.05 0.02 0.05
Systolic blood pressure (mmHg) 0.08* À0.00 0.04 L0.02 0.03 0.08*
Cholesterol (mmol/l) 0.04 0.02 L0.04 L0.03 À0.01 0.03
*** p< 0.001; ** p< 0.01; * p< 0.05.
The correlation coefficients marked in bold are equal in strength between the lowest and highest tertiles. SOC ¼ sense of coherence scale; BMI¼
body mass index.a Scores 16e60.b Scores 61e71.c Scores 72
e91.
d Never/former smokers¼ 1; current smokers¼ 2.
2410 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 11/12
in the evaluation and categorisation of stimuli (Cohen
& Rodriguez, 1995). In this study, SOC, depression
and anxiety were not related to clinically measured
health variables.
To our knowledge, this is the first study to compare
the relationships of SOC, depressive symptoms and
anxiety with health-related variables in a representative
population sample. A few earlier studies have compared
the associations of SOC and other personality traits with
health variables. The SOC scale has shown stronger cor-
relations with different health and well-being measures
than the self-efficacy, hardiness, locus of control, self-
esteem and optimism scales, for example (Pallant &
Lae, 2002; Smith & Meyers, 1997). Similar associations
found between the SOC, depression and anxiety
measures suggest that SOC has more in common with
them than other positive psychology concepts.
In the present study, we used the 13-item SOCquestionnaire, and it is possible that the heterogeneity
of the SOC construct would be better captured in the
full 29-item questionnaire. Furthermore, the depression
and anxiety inventories we used are not unproblematic
either: it is possible that one common factor, such as
negative emotionality, explains the strong and inverse
relationship of the SOC with depression and anxiety
(Frenz et al., 1993). Indeed, the SOC questionnaire
might measure negative emotionality, and according
to the tripartite model of depression and anxiety (Clark
& Watson, 1991), negative emotions common to bothdepression and anxiety are mainly responsible for the
strong association between the measures of these two
constructs.
In conclusion, our study provides additional
evidence of the overlap between the SOC scale and
measures of depression and anxiety. This is consistent
with the findings reported by Breslin et al. (2006),
Gruszczynska (2006) and Korotkov (1993). It seems
that current psychometric methods are able to separate
highly correlated measures, and these small differences
could have value in some research settings. However,
in view of our almost equal associations with health
indicators and behaviours, it would be useful to bring
these concepts into the same scientific discussion.
This kind of research could have a positive impact in
the application of these constructs to theory-based
health-improvement programmes.
References
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopeless-
ness depression: a theory-based subtype of depression.
Psychological Review, 96 (2), 358e
372.
Antonovsky, A. (1979). Health, stress and coping. San Francisco:
Jossey-Bass.
Antonovsky, A. (1987). Unraveling the mystery of health: How
people manage stress and stay well . San Francisco: Jossey-Bass.
Antonovsky, A. (1993). The structure and properties of the sense of
coherence scale. Social Science & Medicine, 36 (6), 725e733.
Bandura, A. (1977). Self-efficacy: toward a unifying theory of
behavioral change. Psychological Review, 84, 191e
215.
Beck, A. T. (1967). Depression: Causes and treatment . Philadelphia:
University of Pennsylvania Press.
Beck, A. T. (1987). Cognitive models of depression. Journal of
Cognitive Psychotherapy, 1(1), 5e37.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J.
(1961). An inventory for measuring depression. Archives of
General Psychiatry, 4, 561e571.
Breslin, F. C., Hepburn, C. G., Ibrahim, S., & Cole, D. (2006).
Understanding stability and change in psychological distress
and sense of coherence. Journal of Applied Social Psychology,
36 (1), 1e21.
Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety and
depression: psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100(3), 316e336.
Cohen, J., & Cohen, P. (1983). Applied multiple regression/correla-
tion analysis for the behavioral sciences. Hillsdale: Erlbaum.
Cohen, S., & Rodriguez, M. S. (1995). Pathways linking affective
disturbances and physical disorders. Health Psychology, 14(5),
374e380.
Eriksson, M., & Lindstrom, B. (2005). Validity of Antonovsky’s
sense of coherence scale: a systematic review. Journal of
Epidemiology & Community Health, 59(6), 460e466.
Eriksson, M., & Lindstrom, B. (2006). Antonovsky’s sense of
coherence scale and the relation with health: a systematic
review. Journal of Epidemiology & Community Health, 60,
376e381.
Feldt, T., Lintula, H., Suominen, S., Koskenvuo, M., Vahtera, J., &Kivimaki, M. (2006). Structural validity and temporal stability
of the 13-item sense of coherence scale: prospective evidence
from the population-based HeSSup study. Quality of Life
Research, 16 , 483e493.
Feldt, T., Metsapelto, R.-L., Kinnunen, U., & Pulkkinen, L. (2007).
Sense of coherence and five-factor approach to personality.
European Psychologist, 12(3), 165e172.
Flannery, R. B., & Flannery, G. J. (1990). Sense of coherence,
life stress, and psychological distress: a prospective
methodological inquiry. Journal of Clinical Psychology,
46 (4), 415e420.
Frenz, A. W., Carey, M. P., & Jorgensen, R. S. (1993). Psychometric
evaluation of Antonovsky’s sense of coherence scale. Psycholog-
ical Assessment, 5(2), 145e153.
Friedman, H. S., & Booth-Kewley, S. (1987). The ‘disease prone
personality’: a meta-analytic view of the construct. American
Psychologist, 42(6), 539e555.
Geyer, S. (1997). Some conceptual considerations on the sense of
coherence. Social Science & Medicine, 44(12), 1771e1779.
Gotlib, I. H., & Cane, D. B. (1989). Self-report assessment of
depression and anxiety. In: P. C. Kendall, & D. Watson (Eds.),
Anxiety and depression: Distinctive and overlapping features
(pp. 131e169). San Diego: Academic Press.
Gruszczynska, E. (2006). What is measured by the orientation to life
questionnaire? Construct validity of the instrument for the sense
of coherence measurement. Polish Psychological Bulletin, 37 (2),
74e
83.
2411 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412

8/8/2019 do Sense of Coherence Ansiedad y Sitnomas Depresivos
http://slidepdf.com/reader/full/do-sense-of-coherence-ansiedad-y-sitnomas-depresivos 12/12
Kaplan, G. A. (1995). Where do shared pathways lead? Some
reflections on a research agenda. Psychosomatic Medicine, 57 ,
208e212.
Kivimaki, M., Feldt, T., Vahtera, J., & Nurmi, J. (2000). Sense of
coherence and health: evidence from two cross-lagged longitudi-
nal samples. Social Science & Medicine, 50, 583e597.
Klepp, O. M., Mastekaasa, A., Sorensen, T., Sandanger, I., &
Kleiner, R. (2007). International Journal of Methods in Psychiat-
ric Research, 16 (1), 11e22.
Kobasa, S. C. (1982). The hardy personality: toward a social psychol-
ogy of stress and health. In: J. Suls, & G. Sanders (Eds.), Social
psychology of health and illness (pp. 3e33). Hillsdale: Erlbaum.
Korotkov, D. (1993). An assessment of the (short-form) sense of
coherence personality measure: issues of validity and well-being.
Personality and Individual Differences, 14, 575e583.
Kravetz, S., Drory, Y., & Florian, V. (1993). Hardiness and sense of
coherence and their relation to negative affect. European Journal
of Personality, 7 (4), 233e244.
Kuuppelomaki, M., & Utriainen, P. (2003). A 3 year follow-up study
of health care students’ sense of coherence and related smoking,
drinking and physical exercise factors. International Journal of Nursing Studies, 40(4), 383e388.
Larsson, G., & Kallenberg, K. (1996). Sense of coherence, socioeco-
nomic conditions and health. European Journal of Public Health,
6 (3), 175e180.
Lundberg, O. (1997). Childhood conditions, sense of coherence,
social class and adult ill health: exploring their theoretical and
empirical relations. Social Science & Medicine, 44(6), 821e831.
Lundberg, O., & Nystrom Peck, M. (1994). Sense of coherence,
social structure and health. Evidence from a population survey
in Sweden. European Journal of Public Health, 4, 252e257.
Marteau, T. M., & Bekker, H. (1992). The development of a six-item
short-form of the state scale of the Spielberger State-Trait
Anxiety Inventory (STAI). British Journal of Clinical Psychol-
ogy, 31, 301e
306.Midanik, L. T., Soghikian, K., Ransom, L. J., & Polen, M. R. (1992).
Alcohol problems and sense of coherence among older adults.
Social Science & Medicine, 34, 43e48.
Mineka, S., Watson, D., & Clark, L. A. (1998). Comorbidity of
anxiety and unipolar mood disorders. Annual Review of Psychol-
ogy, 49, 377e412.
Pallant, J. F., & Lae, L. (2002). Sense of coherence, well-being, cop-
ing and personality: further evaluation of the sense of coherence
scale. Personality and Individual Differences, 33(1), 39e48.
Poikolainen, K., Poldkletnova, I., & Alho, H. (2002). Accuracy of
quantity-frequency and graduated frequency questionnaires in
measuring alcohol intake: comparison with daily diary and
commonly used laboratory markers. Alcohol & Alcoholism,
37 (6), 573e576.
Raitasalo, R. (1977). Depression and its connections with need for
psychotherapy. Helsinki: Research Institute for Social Security.
Rotter, J. B. (1966). Generalized expectancies for internal versus ex-
ternal control of reinforcement. Psychological Monographs, 80(1).
Sandell, R., Blomberg, J., & Lazar, A. (1998). The factor structure of
Antonovsky’s sense of coherence scale in Swedish clinical and
nonclinical samples. Personality and Individual Differences,
24(5), 701e711.
Smith, T. L., & Meyers, L. S. (1997). The sense of coherence: its
relationship to personality, stress and health measures. Journal
of Social Behavior and Personality, 12(2), 513e526.
Strumpfer, D. J. W., Gouws, J. F., & Viviers, M. R. (1998). Antonov-
sky’s sense of coherence scale related to negative and positive
affectivity. European Journal of Personality, 12(6), 457e480.
Suls, J., & Bunde, J. (2005). Anger, anxiety, and depression as risk
factors for cardiovascular disease: the problems and implications
of overlapping affective dispositions. Psychological Bulletin,
131(2), 260e300.
Suominen, S., Blomberg, H., Helenius, H., & Koskenvuo, M. (1999).Sense of coherence and health e does the association depend on
resistance resources? A study of 3115 adults in Finland. Psychol-
ogy & Health, 14(5), 937e948.
Suominen, S., Helenius, H., Blomberg, H., Uutela, A., &
Koskenvuo, M. (2001). Sense of coherence as a predictor of
subjective state of health: results of 4 years of follow-up of adults.
Journal of Psychosomatic Research, 50(2), 77e86.
Surtees, P., Wainwright, N., Luben, R., Khaw, K. T., & Day, N.
(2003). Sense of coherence and mortality in men and women in
the EPIC-Norfolk United Kingdom prospective cohort study.
American Journal of Epidemiology, 158(12), 1202e1209.
Vartiainen, E., Jousilahti, P., Alfthan, G., Sundvall, J., Pietinen, P., &
Puska, P. (2000). Cardiovascular risk factor changes Finland,
1972e
1997. International Journal of Epidemiology, 29, 49e
56.Veenstra, M., Moum, T., & Roysamb, E. (2005). Relationships
between health domains and sense of coherence: a two-year
cross-lagged study in patients with chronic illness. Quality of
Life Research, 14, 1455e1465.
Watson, D., & Clark, L. A. (1984). Negative affectivity: the disposi-
tion to experience aversive emotional states. Psychological
Bulletin, 96 (3), 465e490.
Watson, D., & Kendall, P. C. (1989). Understanding anxiety and
depression: their relation to negative and positive affective states.
In: P. C. Kendall, & D. Watson (Eds.), Anxiety and depression:
Distinctive and overlapping features (pp. 3e26). San Diego:
Academic Press.
2412 H. Konttinen et al. / Social Science & Medicine 66 (2008) 2401e 2412