Creating & communicating an improvement strategy · 2020-01-31 · Source: McKinsey Performance...
80
Quality Improvement: Tools, Techniques and Considerations Dr Mark Attah GP Partner, Octagon Medical Practice, Cambridgeshire
Transcript of Creating & communicating an improvement strategy · 2020-01-31 · Source: McKinsey Performance...

Quality Improvement:Tools, Techniques and Considerations
Dr Mark AttahGP Partner, Octagon Medical Practice, Cambridgeshire

Learning Outcomes
Learning about Model for Improvement
Understanding and using Driver Diagrams
Understanding and using Process Mapping
Understanding and working on the PDSA cycle
Being able to apply these to a change for improvement
project

A Model of L S Change
Identifying
need for
change
Framing/
reframing
the
issues
Engaging/
connecting
others
Making
pragmatic
change in
multiple
processesAttracting
further interest
After some time Settling inPossible outcomes
1. sustainable norm
2. plateau
3. run out of energy
Living with
results and
consequences
Maybe later
Repeats
many times
in hard to
predict ways
Time delay

Three dimensions of large scale (transformational) change
Depthof change vis-à-vis
current ways of
thinking and doing;
a.k.a cognitive-
behavioural or
paradigm shift
Pervasivenessof change; does it affect whole or
only portion
of the system?
Sizeof system experiencing change; e.g.
geography, numbers of people
Refs: Mohrman A. et. al. Large-Scale
Organizational Change. Jossey-Bass,
1989 and Levy A. Second-order planned
change: definitions and
conceptualizations. Org. Dynamics.
Summer 1986, 15:5-20

What If Bigger Fixes Nothing?

Improvement or transformation?
Improvement Transformation

“Insanity: doing the same thing over and over again and expecting different results”

Your vision of the future and why? (shared purpose)


Aligning our efforts
“Are we going in the same direction in the activity we’re involved in ... like a school of fish?”*
*Focus group participant

Shared Values
A ‘prerequisite’ for successful large scale change

What is purpose?
A purpose statement sets out our burning ambition
- why this change is important to you
- why this solution rather than any other
A vision is the ideal picture in your mind, and in the minds of your people.
“A clear vision helps to empower your purpose. It shows the desired end result and so provides the motivation
to work toward that goal”
Jeff Randleman

A 3-word concept



Why is shared purpose important?

The evidence – globally
“Shared purpose is a common
thread in successful change
programmes. Organisations with
strong shared purpose consistently
outperform those without it”.
What makes change successful in the NHS? - Gifford
et al 2012 (Roffey Park Institute) and Management
Agenda 2013 - Boury et al (Roffey Park Institute)

The evidence
Growing literature demonstrating & discussing the importance of shared values, before & underpinning any other changes (structures, processes, incentives, infrastructure)• eg implementing integrated care
Failure to invest in establishing shared purpose, based on common values, results in wasted effort and disappointing results later

What happens when shared purpose is absent?
- Other factors move into the space and become ‘de facto’ purpose e.g. cost cutting and targets.
- Change efforts go off course or run out of energy.

Getting some balance…

Mental models of change – striking a balanceHow we think about engagement

Start with the end in sight

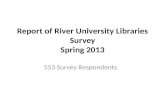
Large scale change usually fails
Source: McKinsey Performance Transformation Survey, 3000 respondents to global, multi-industry survey of company executives
70%
25%
5%

Most transformation efforts fail
30 70
Employee resistance
to change
Management behavior
does not support change
Inadequate resources or budget
Other obstacles
39
33
14
14
Organizational
health factors
% of
efforts
failing to
achieve
target
impact
70% of change programs fail …
… mainly because organizational health gets
in the way
Source: Scott Keller and Colin Price, Beyond Performance: How Great Organizations Build Ultimate Competitive Advantage. 2011

Objectives
DESIRED OUTPUTS AIM
A shared vision for what the
Collaborative wants to achieve
Clarity of WHAT by WHEN
A shared purpose that underpins this
transformation
Clarity of WHY you want to
achieve this chosen change
A shared set of values that underpin
this shared purpose
The ‘WAY’ the collaborative will
work together to deliver this
change
A set of agreed design rules that this
Collaborative will use to drive
development and selection of solutions
Criteria to influence ‘HOW’ we
achieve this change

Define the Problem

QIP vs Audit
“what is the right thing to do?”
vs
“are we doing the right thing in the right way?”

Quality and Improvement
Quality is the degree of excellence in healthcare (Health Foundation Definition)
Quality improvement is better patient experience and outcomes achieved through changing provider behaviour and organisation through using a systematic change method and strategies

Six Dimensions of Quality
Safety - do no harm
Timely - without undue delay; who receive and those who give
Effective - produces desired results
Efficient - avoiding waste, including waste of equipment, supplies, ideas, and energy
Equitable - providing care that does not vary because of gender, ethnicity, disabilities etc. in the patient; or at population level
Patient-centred - providing care that is respectful and responsive; needs, and values; seamless; provided with respect and compassion
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1426185/

• An evidence-based improvement
methodology ensures that our
change will be delivered in a
planned way that follows tried-and
tested methods for assuring
success.
Change Model framework

Model for Improvement

The “Model for Improvement”
What are we trying to
accomplish?
How will we know
that a change is an
improvement?
What changes can
we make that will
result in an
improvement?
Plan
DoStudy
Act

What are we trying to accomplish?
How will we know that change is an improvement?
What change can we make that will result in improvement?
aims
measurements
change ideas
testing ideas before implementing changes
Langley, G., Nolan, K., and Nolan, T., 1994. The Foundation of Improvement, Quality Progress, June 1994

Langley, G., Nolan, K., and Nolan, T., 1994. The Foundation of Improvement, Quality Progress, June 1994
• Carry out the plan
• Collect the data
• Analysis
• Complete the analysis
• Compare with predictions
• Summarise
• Set objectives
• Questions
• Who, where and when
• Collect data to answer questions
• What changes are to be made to the next cycle?
• Can the change be implemented? Act Plan
DoStudy

Meeting rooms
Real world
Approve
Design Design Design Design
Implement !
Spending more time on the WHAT than the HOW!
Courtesy of Patient Safety First
© NHS Institute for Innovation and Improvement 2010. All rights reserved.

Meeting rooms
Real world
Courtesy of Patient Safety First
Implement
Approve
Test & refine
Test & refine
Test & refine
Design
Measurement
Which is typical of your organisation?
© NHS Institute for Innovation and Improvement 2010. All rights reserved.

Traditional Approach to Activities
Suggested Approach
P D
P D S A
S A
Time
PDSA Cycle
Which is typical of your organisation?
Time saved
© NHS Institute for Innovation and Improvement 2010. All rights reserved. 37

Driver Diagrams
Used to plan improvement project activity
Provide a way of systematically laying out aspects of an improvement project
Three columns:
• Aim/Outcome: What needs to be achieved
• Primary Drivers: Set of factors that must be addressed to achieve the aim
• Secondary Drivers: Specific areas where we plan changes.

What are we trying to accomplish?
How will we know that change is an improvement?
What change can we make that will result in improvement?
The Model for Improvement
Langley, G., Nolan, K., and Nolan, T., 1994. The Foundation of Improvement, Quality Progress, June 1994

Plan-Do-Study-Act
disciplined framework ensures every part is done every time
facilitates rapid prototyping and rolling out of new ideas

5127


Using a driver diagram
A method or tool or process for use by individuals or teams to generate and organise strategy

Driver Diagrams
AIM –an improved system
Primary driver 1
Primary driver 2
Secondary driver 1
Secondary driver 2
Secondary driver 3
Secondary driver 4
Secondary driver 5
CHANGE 1
CHANGE 2
CHANGE 3
CHANGE 4
CHANGE 5
CHANGE 6
CHANGE 7
AIM PRIMARYDRIVERS
SECONDARYDRIVERS
CHANGES TO TEST
CauseEffect
Drives


Photo: Jim Pennucci

Overwhelming?



Avoid silver bullet thinking

Avoid silver bullet thinking
We have a major problem with access in
our surgeryThe solution is
obvious. I’ve looked at the evidence and we need to bring in telephone triage.

Avoid silver bullet thinking – The multiple drivers of GP access
AIM PRIMARYDRIVERS
SECONDARYDRIVERS
CHANGE TO TEST
Improveaccess
Doctors (capacity)
Demand
Dealing (efficiency)
Appt system
Supply of GP time
Organisation of GP time
Pt help-seeking
Deflecting demand
Creating our own workload
Planning care
Appt system project
GP rota change project
Community education
Waiting room TV
PILS & CDs & DVDs
Feel better faster
Student sick notes
Reception signposting
Test results
Consulting skills
Longer appts
Guaranteed interpreters
Dealing w failed referrals
Chronic disease pathways
Review periods
More TelC’s
Email appts
Continuity
Telephone triage

Driver DiagramsWeight loss example
2 stone weight
loss in 12 months

Pedometer
Gym work out 3
days
Squash weekends
No pub weekdays
Take packed
lunch
Low fat meals
Buy only 1
sandwich
Water bottle for
work bag
Fruit for dessert
Put away large
wine glasses
Put cycling days
in diary
Cycling kit out
night before
Get rid of Oyster
card
Take stairs2 stone weight
loss in 6/12
Look for patterns

Pedometer
Gym work out 3
days
Squash weekends
No pub weekdays
Take packed
lunch
Low fat mealsBuy only 1
sandwich
Water bottle for
work bag
Fruit for dessertPut away large
wine glasses
Put cycling days
in diary
Cycling kit out
night before
Get rid of Oyster
card
Take stairs
Be more active during
the dayDo sport
Drink less alcohol
Substitute lower calorie
foods
Eat less
Marshall the mass of ideas
2 stone weight
loss in 6/12

Pedometer
Gym work out 3
days
Squash weekends
No pub weekdays
Take packed
lunch
Low fat meals
Buy only 1
sandwich
Water bottle for
work bag
Fruit for dessert
Put away large
wine glasses
Put cycling days
in diary
Cycling kit out
night before
Get rid of Oyster
card
Be more active
during the day
Do sport
Drink less alcohol
Substitute lower
calorie foods
Eat lessReduce
calories in
Increase
calories out
Take stairs
2 stone weight loss
in 6/12
Marshall the mass of ideas

Driver Diagrams
Benefits ...
• build complex strategy
• immediate
• visual
Different scenarios ...
1. Share learning
2. Help generate change ideas
3. Marshall a mass of change ideas
4. Survive failure / the unexpected
• avoid “silver bullet”thinking
• highlight overlooked ideas

20 % REDUCTION IN ADMISSIONS
FOR THE OVER 70s
Reduce attendanceat A&E
Reduce conversion to admission
Utilise alternative options
Clinician education
Increase efficiency / streamlining
Best practice clinical management
Data focused plans
Patient education
SPA inreach to A&E / MAU
Utilise SPA
Make more use of paramedics
Work with third sector
Social services input
Better population health
Link to HWB priorities
Proactive mental health care
Optimise LTC management
Rapid discharge options from A&E
Home discharge
Non-home discharge
All GP referrals to be triaged by SPA
Medical team support on phone for paramedics
Extended scope paramedic roles
Increase community hospital beds
Social worker on call in A&E
Funding for volunteer home visitor training
Engagement meeting with local charitiesCauseEffect

Process Mapping
• Views the system from patient perspective, following their journey
• Help staff understand the complexity of processes
• Diagnostic and used as a basis for redesign, actively involving staff in the process

Process mapping
Helps understand process
Identify critical steps
Consider safety of these steps
Identify redundant steps
Failure mode and effects analysis

Process Map - Example
Go to sleep
Alarm goes off
Groan heavily
Get up!
No
Yes

Process Mapping-2 Stages
• Stage 1
Understand what actually happens to the Patient. Where it happens and who is involved.
• Stage 2
Use the map to identify steps that could be changed.

Using the map
• Look for bottle necks/constraints (Queues)
• Any delays? (eg. Wait for clinician/consent/results/parking)
• Repetition (eg.Patient identity check)
• Unnecessary travel/movement in the department. (eg. Patient or notes)
• Unnecessary steps?
• Inefficient order of events?

Process Mapping-What do you need
• Your aim
• The right people (not just clinicians)
• Time
• Paper (flip chart/backing paper)
• Coloured pens
• Post its
• Facilitator

Process Mapping
• What are you trying to achieve?
Describe your aim. For example-To reduce the time Patients spend waiting in out patients.
• Who do you need at the meeting?
• Do you need to walk the journey yourself?
• Do you need to plot the timings/experiences of a series of cases?

Process mapping
Define the boundaries
Start with …..
Stop with ……
Realise I
have a flat
tyre
Drive away
with tyre fixed

Telephone request for
prescription
Is prescription
on repeat?
prescription
Have they
had it
regularly?
Add to special
request list for
next day
prescription
Don’t print
prescription
Add to special
request list for
next day
GP prints
prescription
GP decides if
issues
prescription
Prescription
returned to
front desk for
collection
Prescription
destroyed and
removed from
System
Returned to
prescribing
team – not
signed and
score through it
No
Yes
Yes
Yes
No
No
GP agrees
to prescribe
YesNo
Message to
prescribing
team – not
being
prescribed
Prescribing
team contact
patient to
inform them

Look at the whole process, not just the individual steps.

Process Mapping-What do you need
• Your aim
• The right people (not just clinicians)
• Time
• Paper (flip chart/backing paper)
• Coloured pens
• Post its
• Facilitator

Measurement for Improvement
“You can’t fatten a cow by weighing it” (Palestinian Proverb)
•Improvement is not about measurement, but…
•How do we know if a change is an improvement?
•“if you can’t measure it, you can’t improve it”

The traditions of measurement
• e.g. A-B comparison, average, huge dataset
Research
• e.g. one-to-many benchmarking comparison, average, large dataset
Judgement
• e.g. continual analysis of single changing process over time
Improvement

What mind sets are at play here?
Mind sets
Research
Improvement
Judgement

Research Judgement Improvement
GoalNew knowledge (not its applicability)
ComparisonReward / punishmentSpur for change
Process understanding
Evaluating a change
Hypothesis Fixed None Multiple and flexible
Measures Many Very few Few
Time period Long, past Long/medium, past Short, current
Sample Large Large Small
Risks in improvement
settings
Ignores time based variation
Over-engineers data collection
Ignores time based variation
Over-reaction to natural variation
Incorrectly perceived as ‘inferior statistics’
Measurement mindsets
Based on L Solberg, G Mosser and S McDonald (1997) The Three Faces of Performance Measurement: Improvement,
Accountability and Research, Journal on Quality Improvement, 23 (3): 135 - 147.

What does this data tell us?
Patients treated in April
600
550
610
540
560
570
580
590
2010 2011

What does this data tell us?
Patients treated
650
600
550
500
450
400
350
300April 2010 April 2011

Plotting the dots - example Run ChartNumber of calls to outreach team (weekly)
November 2010 to June 2011
0
No o
f C
alls
180
160
140
120
100
80
60
40
20
1st Nov 15th Nov 29th Nov 13th Dec 27th Dec 10th Jan 24th Jan 7th Feb 21st Feb 6th Mar 20th Mar 3rd Apr 17th Apr 1st May
Week
Calls per week Median

Statistical Process Control
(SPC) Charts:
No o
f A
dm
issio
ns
0
200
150
100
50
250
Performance Report – Number of Admissions
Week
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
No Admissions Mean Lower Limit (66.5) Upper Limit (222.4)
77