HBV: What is in the Pipeline? - Virology...
37
Shyam Kottilil MD, Ph.D. Institute of Human Virology University of Maryland Baltimore MD HBV: What is in the Pipeline?
Transcript of HBV: What is in the Pipeline? - Virology...

Shyam Kottilil MD, Ph.D.Institute of Human Virology
University of MarylandBaltimore MD
HBV: What is in the Pipeline?

Disclosures
No conflict of interest to disclose

Unlabeled/Unapproved Use
New agents/drugs that are not yet FDA approved will be discussed

Adapted from Rehermann B and Mascimbeni M Nat Rev Immunol 5: 1573, 2005
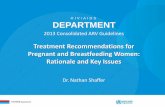
Persistence of Hepatitis B
100
50
0Incr
ease
(% o
f max
imum
)
0 1 2 3 4 5 6 7 8Time After Infection (months)
SerumALT Activity
SerumHBVDNA
Outcome: Clinical Recovery
IncubationPhase
Acute Disease,Clinical Symptoms
Recovery,Protective Immunity
HBcAg-specific antibodies
100
50
0Incr
ease
(% o
f max
imum
)0 10 20 21 30 31 4041 50
Time After Infection (years)
SerumALT Activity
SerumHBV DNA
Immuno-tolerance
ImmunoactivePhase
Low Replicative
Phase
High Replicative
Phase
Outcome: Chronic Hepatitis
HBeAg-specific antibodiesSerum HBeAg
Serum HBsAg HBsAg-specific antibodies
HBcAg-specific antibodies
HBeAg-specific antibodiesSerum HBeAg
Serum HBsAg

Current HBV Treatment
Nucleos(t)ides
Entecavir
N
NN
NNH2
OPOHO
HO
N
NN
NNH2
OPO
HOHO
CH3
AdefovirTenofovir
HO
NH
NN
NO
NH2
OH
Interferons
O
S
N
N
NH2
OOH
Lamivudine
O
HN
N
O
OOH
CH3
OH
Telbivudine
Pegylated Interferon alfa 2a
Pegylated Interferon alfa 2b

Efficacy of HBV Agents After One Year of Therapy
Data from 2012 EASL HBV Management Guidelines
100
80
60
40
20
0
ALT
Nor
mal
izat
ion
(% p
atie
nts
at 1
yea
r)
Tenofovir Entecavir Telbivudine Lamivudine Adefovir PEG-IFN-2a
HBeAg+
HBeAg–

Effects of Treatment on Fibrosis
74% of Patients with Cirrhosis at Baseline Were No Longer Cirrhotic at Year 5
Baseline Ishak Fibrosis Score
No ImprovementImprovement
P <0.001: Jonckheere-Terpstra trend test
Marcellin, P et al. Lancet 2013; 381(9865):468-75
100
90
80
70
60
50
403020
10
0
Perc
enta
ge o
f Pat
ient
s
1 2 3 4 5 6
n=10 n=126 n=79 n=37 n=19 n=77

Efficacy of HBV Agents After One Year of Therapy: HBsAg Loss
Data from 2012 EASL HBV Management Guidelines
100
80
60
40
20
0
HB
sAg
Loss
(% p
atie
nts
at 1
yea
r)
Tenofovir Entecavir Telbivudine Lamivudine Adefovir PEG-IFN-2a
HBeAg+
HBeAg–

Nucleoside analog therapy has little effect on HBsAg levels, HBsAg loss and depletion of cccDNA
Emergence of resistance is a potential problem with long term nucleoside analog therapy
Long term adverse events may occur with continued use of nucleoside analogs
Pitfalls of Current Therapy

Absence of plasma HBV DNA after stopping antiviral therapy
Loss of HBsAg with or without HBsAg seroconversion
Goals for Eradication

Target the Virus Target the Hostand/or
• Viral proteins or nucleic acids• Host proteins necessary for viral
replication• Innate or adaptive immune system
Novel Strategies to Eradicate HBV

Target the Virus
• Viral proteins or nucleic acids
Novel Strategies to Eradicate HBV

Entry of HBVinto cell
HBV Life Cycle, Potential Targets
Repair
Transcription
TranslationCore assembly
and RNA packaging
Recycling
HBV
Core particleminus strand
synthesis
Core particleplus strandsynthesis
Vesicular transport
to cellmembrane
cccDNA
HBsAg
HBeAg

Entry of HBVinto cell
Targeting HBV Entry
Repair
Transcription
TranslationCore assembly
and RNA packaging
Recycling
HBV
Core particleminus strand
synthesis
Core particleplus strandsynthesis
Vesicular transport
to cellmembrane
1
cccDNA
HBsAg
HBeAg

Inhibition of Viral Entry: Myrcludex B
Myrcludex B prevents de novo infection preclinicallyKey Issues: Will it have an impact on chronic infection, or HBsAg loss?
uPA-SCID HBV Mice
Lütgehetmann M, et al. Hepatology 2012; 55:685-694
7
6
5
4Log
Vire
mia
[cop
ies/
ml]
HBV HBVControl Treated
50
40
30
20
10
0
HB
sAg
(IU/m
L)
Control Treated
LLoDLLoD
Myr2 108 163 389
HBVpreS/2-48myr IC50: ~8 nM2v 2 48

Entry of HBVinto cell
Targeting cccDNA
Repair
Transcription
TranslationCore assembly
and RNA packaging
Recycling
HBV
Core particleminus strand
synthesis
Core particleplus strandsynthesis
Vesicular transport
to cellmembrane
2cccDNA
HBsAg
HBeAg

Depleting or Inactivating cccDNA
Key issues: – cccDNA = reservoir of infection
– Formation of new cccDNA can be blocked by inhibiting replication
– Existing cccDNA is not affecteddirectly by current therapies and hasa long half-life
– Is it possible to silence cccDNA epigenetically?
– Is it possible to destabilize cccDNA?

Belloni L. J. Clin Invest 2012; 122:529-537
Epigenetic Silencing of cccDNA by Interferon-alfa
cccDNALevels
HBV RNALevels
cccDNAAcylation
cccDNA “silenced”, not depletedPossible to identify other ways to “silence” cccDNA?Zinc finger motifs in Duck Hepatitis model
10
1.0
0.1
Log
cccD
NA
/hu-
cell
0.10
0.08
0.06
0.04
0.02
pgR
NA
/hu-
GA
PDH
1.0
0.8
0.6
0.4
0.2
preS
/S R
NA
/hu-
GA
PDH
Fold
indu
ctio
n
NTIFN-α
1.0
0.8
0.6
0.4
0.2 *

ZFP Decreases HBV Replication in Hep AD38 Cells
Weber et al, PLoS ONE 2014: 9(5): e97579.

TALENs• transcription activator-like effector nucleases
Chen et al, Molecular Therapy 2014; 22(2):303–311

Entry of HBVinto cell
Targeting Encapsidation
Repair
Transcription
TranslationCore assembly
and RNA packaging
Recycling
HBV
Core particleminus strand
synthesis
Core particleplus strandsynthesis
Vesicular transport
to cellmembrane
3
cccDNA
HBsAg
HBeAg

BAY 41-4109*EC50 = 50 nM
*Deres, Science 2003; 299: 893-896; Weber et al. Antiviral Res, 2002; 54:69-78
HBV Capsid Inhibitors
Key Issue: Will capsid inhibitors impact HBsAg loss or only have antiviral activity like nucleosides?Phase 1 clinical trial is planned with HBV capsid inhibitor
8.0x1005
7.0x1005
6.0x1005
5.0x1005
4.0x1005
3.0x1005
2.0x1005
1.0x1005
0.0x1005
Treatment (14 days BID)
Placebo2x30mg/kg 3TC2x30mg/kg BAY 41-41092x15mg/kg BAY 41-41092x7.5mg/kg BAY 41-4109
** *
HB
V-D
NA
[gen
ome
copi
es/1
0ul p
lasm
a]

Entry of HBVinto cell
Targeting HBV Replication
Repair
Transcription
TranslationCore assembly
and RNA packaging
Recycling
HBV
Core particleminus strand
synthesis
Core particleplus strandsynthesis
Vesicular transport
to cellmembrane
4
cccDNA
HBsAg
HBeAg

Entry of HBVinto cell
Targeting Envelopment and Secretion
Repair
Transcription
TranslationCore assembly
and RNA packaging
Recycling
HBV
Core particleminus strand
synthesis
Core particleplus strandsynthesis
Vesicular transport
to cellmembrane
5
cccDNA
HBsAg
HBeAg

Inhibition of HBsAg Secretion
Dougherty AM et al. Antimicrob Agents Chemother, 2007; 51:4427-4437
Key Issues:– Will suppression of HBsAg antigenemia restore T cell responsiveness?
– Mechanism undefined, potential to inhibit host protein secretion?
HBF-0259Formula Weight = 364.21cLogP = 4.97
RI
CIF
NH
NN
N
N
CI
R2
76
54
12
3
100 23 42 618.0 4.0 2.0D
MSO HBF-0259 (µM)
Secr
eted
Density (%)
LM
AGP

Target the Host
• Host proteins necessary for viral replication
• Innate or adaptive immune system
Novel Strategies to Eradicate HBV

Mechanisms of Persistence

GS-9620, an orally available agonist Selective for antiviral vs proinflammatory responsePreclinical studies: Reduces sAg, viral DNA in woodchucks & chimpanzeesPhase 1a (SAD) complete: Safety shown in healthy volunteers
N
N N
HN
O
NH2O
N
MYD88
IRF7 NFkB
IRF7 IRF7 NFkB
Pro-inflammatoryIFN, ISGs
TLR-7 Agonist for HBV
Lopatin U et al. Antivir Ther 2013; 18:409-418

-3
-2
-1
0
4 0
6 0
8 0
1 0 0
1 2 0
-2 8 7 1 4 2 5 3 1 4 5 5 7 7 9 9 3
D a y
Ch
ang
e in
Ser
um
HB
V D
NA
(log
IU/m
L)
Ch
ang
e in S
erum
HB
sAg
(% P
re-Tx)
Oral TLR7 Agonist GS-9620 Highlights Potential of Immunotherapy for Chronic HBV
Lanford et al. Gastroenterology 2013;144:1508-17.
1 mg/kg 2 mg/kg
HBV DNAHBsAg
n=3

Adaptive Immunity in Chronic Hepatitis B Infection

Effect of PD-1/L1 on Antiviral Immunity

Expansion of HBV-specific CD8 T Cell Response by Blocking PD-1/L1/2 Interaction In Vitro
Sherman AC et al. AIDS Res Hum Retr 2012
10
1
0.10
0.01
IFN
-γ s
ecre
ting
CD
8+T
Cel
ls (%
) PBMC (untreated)Anti-PD-1/L1/2
HBV CMV
*

Effect of anti-PD-1 or PD-L1 Antibodies in Cancer
June 28, 2012 No. 6Vol. 366
Safety, Activity, and Immune Correlates of Anti–PD-1 Antibody in Cancer
SL Topalian, M Sznol et al.
Safety and Activity of Anti–PD-L1 Antibody in Patients with Advanced Cancer
JR Brahmer, JM Wigginton et al.

• Blocks PD-1
• Acts on T cells
• More efficient blocking?
• More adverse events
• Risk benefit
• Blocks PD-L1
• Acts on APCs
• Less efficient blocking
• Less adverse events
• Risk benefit
PD-1 antibody PD-L1 antibody
Blocking PD-1/L1 to Enhance HBV Immunity

Chimeric Antigenic Receptors (CAR)
June CH et al Blood 2014

Therapeutic Vaccines
Li et al J Biotechnology 2012

Our goal is to achieve sustained suppression of HBV and HBsAg loss after cessation of therapy
Approaches to target virus include inhibition of viral entry, HBV antigen production, and elimination or silencing of cccDNA
Approaches to target host include non specific inhibition of immunoregulatory pathways and boosting of HBV specific immunity
Realistically, a combination approach may be necessary to achieve sustained virologic remission
Conclusions