Committes of hospital
26
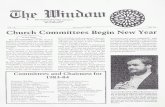
Purpose The Credentials and Privileges Committee reviews the credentials of providers applying for initial appointment or reappointment to the Medical Staff at SHC, and makes recommendations for membership and delineation of privileges in compliance with the Medical Staff Bylaws, Credentialing Policies and Procedures, and Clinical Service requirements; reviews and approves new or revised credentials and privileges, forms and processes; reviews and approves credentialing policies and procedures. In addition, the Credentials and Privileges Committee reviews and acts upon reports from the Interdisciplinary Practice Committee (IDPC) of appointment and evaluations of Advanced Practice Providers. The IDPC is a subcommittee of the Credentials and Privileges Committee and is accountable to the Medical Executive Committee and the Governing Body. Chair Hospital Committee General functions: Formulate policies Coordinate Monitor Areas of responsibility Execom (Executive Committtee) Quality services and organizational direction Mancom (Management Committee) Quality services and operational management Quality Council Quality services and quality management system Committee on Medical Services Quality medical services rendered by physicians Bioethics Committee Bioethical matters in patient care Pharmacy and Therapeutic Committee Drug therapy
description
describing hospital committees
Transcript of Committes of hospital

Purpose
The Credentials and Privileges Committee reviews the credentials of providers applying for initial appointment or
reappointment to the Medical Staff at SHC, and makes recommendations for membership and delineation of
privileges in compliance with the Medical Staff Bylaws, Credentialing Policies and Procedures, and Clinical Service
requirements; reviews and approves new or revised credentials and privileges, forms and processes; reviews and
approves credentialing policies and procedures.
In addition, the Credentials and Privileges Committee reviews and acts upon reports from the Interdisciplinary
Practice Committee (IDPC) of appointment and evaluations of Advanced Practice Providers. The IDPC is a
subcommittee of the Credentials and Privileges Committee and is accountable to the Medical Executive Committee
and the Governing Body.
Chair
Hospital Committee General functions:
Formulate policiesCoordinate
Monitor
Areas of responsibility
Execom (Executive Committtee)
Quality services and organizational direction
Mancom (Management Committee)
Quality services and operational management
Quality Council Quality services and quality management system
Committee on Medical Services
Quality medical services rendered by physicians
Bioethics Committee Bioethical matters in patient care
Pharmacy and Therapeutic Committee
Drug therapy
Infection Control Committee
Infection control
Waste Management Committee
Waste management
Medical Audit and Tissue Committee
Outcome in patient care such as mortality, morbidity, and tissue review
Tumor Board Cancer managementMedical Records Committee
Medical records

Credentials Committee Credentialing of physicians
Blood Transfusion Committee
Blood transfusion
Home
» Medical Staff Main Page
» e-Newsletters
» Medical Staff Leader Connection
RSS
ShareThis
Credentialing monthly: What is the role of the credentials committee in addressing unprofessional conduct?Medical Staff Leader Connection, November 18, 2009
Want to receive articles like this one in your inbox?Subscribe to Medical Staff Leader Connection !
If you believe everything you read, it may appear that we are in the midst of a disruptive physician behavior epidemic.
As I travel to hospitals across the country, I am not convinced that the frequency or severity of unprofessional
conduct (the term I prefer to use instead of “disruptive behavior”) has increased. Rather, I believe that we are
changing our expectations of physician behavior.
In other words, medical staffs are no longer tolerating behavior that they tolerated in the past. The Joint Commission
has weighed in on this issue withSentinel Event Alert #40, which highlights the adverse affect unprofessional conduct
has on patient safety. The Joint Commission also issued leadership standard LD.03.01.01, which requires hospitals
to address unprofessional conduct throughout all levels of the hospital, including management, staff, and board
members—not just physicians.
As members of the self-governed medical staff, department chairs are accountable for the behavior of physicians
within their department. Thus, they are responsible for intervening when a physician displays inappropriate or
disruptive behavior.

In addition to department chairs, the credentials committee plays an important role in keeping problem behavior in
check. I’d like to share with you a clear set of actions a credentials committee can take to fulfill its role in eliminating
unprofessional conduct:
1. Take a close look at the criteria for medical staff membership, which are located in your bylaws or
credentials manual, and make sure they address professional conduct. If you don’t have criteria in place
that address professional conduct, consider this sample language: “Physician must produce a history of
consistently acting in an appropriate and professional manner in previous clinical settings.” This would
not preclude a physician who has had a rare outburst from joining your medical staff if he or she acts in
an appropriate and professional manner the majority of the time. This would however, prevent chronic
offenders from joining your medical staff.
2. Once the credentials committee has established criteria for membership that address professional
conduct, it now has the grounds for gathering information on an applicant’s conduct in previous clinical
settings. This is where references come in handy, especially those your medical staff services
department sends to MSPs at those settings (not the handpicked references of the applicant’s choosing).
The credentials committee owns the content of those reference queries and needs to ensure it has
answered any questions about an applicant’s conduct.
3. One of the credentials committee’s most important roles is to prevent what I like to call an “information
error.” An information error occurs when information existed that your hospital could have or should have
discovered but didn’t, and that information would have caused the committee to make a different
credentialing decision. In this case, the credentials committee needs to gather all the information it needs
regarding the applicant’s behavior in previous clinical settings to make a well informed decision. If the
committee has any concerns about the applicant’s conduct, the committee should drill down into those
concerns to resolve them to the satisfaction of your medical staff’s professional conduct policy. The
credentials committee is responsible for making sure this policy is well written and consistently
implemented. The credentials committee should not make any decisions regarding an applicant when
concerns regarding his or her conduct remain unresolved.
4. The credentials committee needs to guard against the second kind of credentialing mistake: a “decision
error.” A decision error occurs when the medical staff and hospital are aware of potential issues
regarding an applicant but lack the wisdom, clarity, or courage to make a wise decision. When the
credentials committee receives a recommendation from the department chair regarding each applicant
and re-applicant, it is responsible for ensuring that the department chair appropriately understood the
physician’s past behavior and made a wise decision. Typical concerns that occur at this stage include:

The physician admits a lot of patients to the hospital and may have been given too much
latitude with his or her behavior in the past.
The physician is well-liked, resulting in their friends on the credentials committee approving the
reapplication based on camaraderie, not objective evidence.
Members of the credentials committee or others are afraid to lose referrals from the applicant or
reapplication and continue to approve his or her membership on the medical staff in spite of
significant, chronic behavior problems.
The physician threatens to sue the hospital if it tries to affect his or her membership or privileges
based on behavior concerns, and the hospital backs down.
Credentials committee members and other medical staff leaders lack a consensus concerning
whether to take poor physician conduct seriously and what types of behavior are tolerable.
5. The credentials committee needs to remember that the goal of the medical staff professional conduct
policy is not to “kick physicians off the staff” for bad behavior, but to help every physician act in an
appropriate and professional manner as much as possible. Therefore, the credentials committee should
recognize when to recommend to a department chair that further interventions are warranted to address
a physician’s behavior. This may warrant initial or reappointment for a period of less than two years while
the interventions regarding their behavior are carried out.
By fulfilling its role, your credentials committee can help make unprofessional conduct a thing of the past, and in so
doing enhance patient safety and collegiality throughout your hospital.
Richard A. Sheff, MD, CMSL, is the chair and executive director of The Greeley Company, a division of HCPro, Inc. in
Marblehead, MA.
Want to receive articles like this one in your inbox?Subscribe to Medical Staff Leader Connection !
PROFESSIONAL STAFF
ORGANIZATION

AND
FUNCTIONS MANUAL
Carondelet Health Network
Carondelet Holy Cross Hospital
Nogales, Arizona
PROFESSIONAL STAFF ORGANIZATION AND FUNCTIONS MANUAL Carondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 1
Carondelet Holy Cross Hospital
TABLE OF CONTENTS
TOPIC PAGE
Enabling Procedures ........................................................................................
Approval and Modification..............................................................................
Current Organization .......................................................................................
Departments .....................................................................................................
Divisions ..........................................................................................................
Committees ......................................................................................................
Medical Executive Committee.........................................................................
Infection Control Function...............................................................................
Quality Council (QC) ......................................................................................
Credentials Committee of the Board of Directors ...........................................
Carondelet Health Network Human Subjects Committee ...............................
Nominating Committee....................................................................................

Carondelet Health Network Pharmacy & Therapeutics Committee................
Professional Behavior Committee ......................................
ORGANIZATION AND FUNCTIONS MANUAL
ENABLING PROCEDURES
This Organization and Functions Manual has been created pursuant to and under the authority of
the Professional Staff Bylaws of Carondelet Holy Cross Hospital. The purpose of the Manual is
to describe the current organization of the Professional Staff and to define the mechanisms that
the Professional Staff will utilize to accomplish the following functions as outlined in the current
Professional Staff Bylaws.
This Manual is one of three that have been designed to support the Professional Staff Bylaws.
1. Credentialing Policy and Procedures Manual
2. Organization and Functions Manual
3. Professional Staff Rules and Regulations
This Manual and its contents are subject to the approval of the Medical Executive Committee
using the procedures found in the Professional Staff Bylaws.
APPROVAL AND MODIFICATION
This Manual and its contents are subject to the approval of the Medical Executive Committee
and of the Board of Directors. Once approved, the Manual will become effective subject to
future amendments as may from time to time be required and approved by the Medical Executive
Committee. All such amendments will be reviewed by the Board of Directors for their
concurrence.
CURRENT ORGANIZATION
The Professional Staff of Carondelet Holy Cross Hospital will be organized as a
departmentalized professional staff. At the present time, three (3) departments exist:
1. Department of Family Practice/Internal Medicine

2. Department of Surgery/OB-Gyn
3. Department of Pediatrics
In addition, the following committees have been created:
* Medical Executive Committee
* Quality Council
* Credentials Committee of the Board
* Carondelet Health Network Human Subjects Committee
* Professional Staff Bylaws Committee
* Nominating Committee
* Professional Behavior Committee
DEPARTMENTSCarondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 2
Professional Staff will be assigned to one of the three (3) departments depending on their
primary area of practice. In the event a member of the Professional Staff wishes to attend
department meetings other than the one to which he/she is assigned, this is entirely permitted.
However, the individual attending a department other than his/her official department will not be
permitted to vote on issues within the department.
At the discretion of the department chairperson, professional staff specific specialties may
organize themselves into "divisions" for purposes of education, discussion, policy direction, or
for purposes of generating recommendations to the department chair concerning departmental
issues. Additionally, divisions may at times be requested to address specific issues pertinent to
their department.
Departments will be required to hold regular meetings, not less than quarterly. At these
meetings, the chairperson of the department (or designee) will present a report of departmental
activities based upon the past quarter's work. This report is expected to include a brief report

covering the quality of services provided by members of the department, any new policies or
procedures that impact a significant number of the department's members, significant hospitalwide/administrative issues, as well as other issues that affect overall departmental organization.
Any specific actions taken by the Medical Executive Committee that should be communicated to
all members of the department will also be touched upon in this report.
Attendance requirements will be determined by each specific department. All members are
encouraged to attend; attendance will be recorded.
DIVISIONS
Any division, if organized, will not be required to hold any number of regularly scheduled
meetings. Nor will attendance be required unless the division chairperson calls a special meeting
to discuss a particular issue. (Such special meetings must be preceded by at least two weeks
prior notification to all of those individuals expected to attend.) The department will select their
chairpersons.
At the present time, the following divisions exist:
1. Department of Surgery/OB-Gyn
• Obstetrics/Gynecology
2. Department of Family Practice/Internal Medicine
• Obstetrics
• Emergency Medicine
COMMITTEES
The professional staff of Carondelet Holy Cross Hospital will operate through the following
committee structure:
MEDICAL EXECUTIVE COMMITTEECarondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 3
The Medical Executive Committee will conduct those activities and functions specified in the

Professional Staff Bylaws but will be specifically required to do or perform the following
functions, though not limited to:
1. Receive, review and act upon the reports of other medical staff committees and
departments responsible to it;
2. Perform the safety oversight function on behalf of the professional staff;
3. Perform the disaster plan oversight on behalf of the professional staff;
4. Provide leadership for the organizational performance improvement and patient safety
activities to include process measurement and improvement;
5. Ensure that process measurement and improvement include:
- medical assessment and treatment of patients
- use of blood and blood components
- use of medications and operative and other procedures
- efficiency of clinical practice patterns;
6. Identify opportunities to improve patient care and patient safety, and set priorities for its
evaluation using relevant indicators, quality, improvement tools and appropriate clinical
criteria;
7. Review reports from Risk Management, Safety and other departments/services;
8. Review Patient Satisfaction Survey results and complaints and make appropriate
recommendations;
9. Receive Performance Improvement (PI) Team Reports;
10. Provide guidance to the review of hospital systems and processes and report findings to
departments with recommendations for improvement;
11. Other patient care functions to include Pharmacy and Therapeutics, Medical Record
review and Sentinel Event review processes; and
12. Approve the sources of patient care provided outside the hospital. This applies to

“medical care providers” caring for hospital patients OUTSIDE of the hospital. The
MEC will ratify any source of patient care service (not the contract) that originates
outside the hospital. The purpose is to assure that there are no “quality problems”
related to a specific provider or group of providers with whom service is being
contemplated.
The Medical Executive Committee will meet at least nine times per year for the performance of
the functions outlined above and further defined elsewhere in this Organization and Functions
Manual. The Medical Executive Committee will maintain a permanent record of its activities
and will be staffed by at least one designee from the medical staff office.
The Medical Executive Committee may go into "executive session" during which time all nonmembers will be excused. The Hospital Chief Executive Officer or designee may remain unless
the Medical Executive Committee wishes to discuss that individual.
NOTE: Any Professional Staff member may submit a request for a meeting with the Medical
Executive Committee. Such request will ordinarily be honored unless the individual has not
discussed the issue with his/her department chair in advance.
The Medical Executive Committee will arrange for the performance of other medical staff
functions such as institutional review of experimental procedures and research protocols,
continuing medical education, ethics and ethics review functions, intensive/coronary care
oversight and monitoring as well as participation in policy and procedure development in all
areas directly impacting upon the provision of medical care provided within the institution. Chief of Staff Duties/Responsibilities:
1. Act in coordination and cooperation with the hospital CEO or designee in all matters of
mutual concern with the hospital;
2. Call, preside at, and be responsible for the agenda of all general meetings of the
Professional Staff;
3. Serve as Chairperson of the Medical Executive Committee;

4. Serve as a voting member of the Board of Directors;
5. Serve as ex officio member of all other Professional Staff committees without vote;
6. Be responsible for the enforcement of Professional Staff Bylaws, Rules and Regulations,
for implementation of sanctions where these are indicated, and for the Professional Staff's
compliance with procedural safeguards in all instances where corrective action has been
requested against a practitioner;
7. Appoint a committee chairperson to all standing special and multidisciplinary Professional
Staff committees except the Quality Council. (This does not include Departments);
8. Appoint a department chairman if the department is unable to vote on one.
9. Represent the views, policies, needs and grievances of the Professional Staff to the Board
of Directors and to the Hospital CEO or designee;
10. Receive and interpret the policies of the Board of Directors to the Professional Staff and
report to the Board of Directors on the performance and maintenance of quality with
respect to the Professional Staff's delegated responsibility to provide medical care;
11. Be responsible for the educational activities of the Professional Staff; and
12. Be the spokesperson for the Professional Staff in its external professional and public
relations.
INFECTION CONTROL FUNCTION
Composition - The Infection Control Function will be delegated to the Quality Council (QC) for
oversight and monitoring. (See Quality Council for composition and functions). These members
of QC will participate actively in the affairs of the Infection Control Function.
QUALITY COUNCIL (QC)
Membership - The Committee shall be multidisciplinary and shall be composed of at least the
following representatives: Physician Chairperson shall be recommended by the Chief of Staff
and the CEO or designee and confirmed by the Medical Executive Committee. The appointment

will be reviewed every 2 years at the time of election of the Chief of Staff Elect. The Medical
Executive Committee may revoke the appointment at any time without cause. Vice Chairperson
may be delegated to assist the Chairperson in all review activities. The remaining members will
include, but not be limited to the following chairpersons or their designees. (The designee must
be a member of the respective Department):
• Department of Pediatrics
• Department of Family Practice/Internal Medicine
• Department of Surgery/OB-Gyn
• Chief of Staff - (optional)
• Chief of Staff Elect
Carondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 4 Other members include:
• Sr. VP/CEO or designee
• Chief Nursing Officer-Acute/Administrator-Long Term Care or designee
• Quality Management Coordinator or designee
• Board of Directors Liaison or designee
• Pharmacy Manager or designee
• Medical/Post-Surgical Service Line Manager or designee
• Long-Term Care/Transitional Care Unit Manager or designee
• Education/Development Specialist or designee
• Infection Control Manager or designee
• Risk Management Director or designee
• Medical Records Manager or designee
• Information Systems Representative or designee
• Laboratory Services Manager or designee

Representatives from other Ancillary/Care Continuum Services shall also be included as
members/participants of the Council.
Members present shall constitute a quorum.
The Chairperson will make a report to the Medical Executive Committee (each month that a
meeting is held) concerning the activities of QC. A report of PA&I activities will be made to the
Board of Directors at least quarterly. (See Appendix A for Quality Information Flow and
Appendix B for Organizational Chart.)
Function - Implementation of the program shall be the responsibility of the Quality Council.
The Committee shall:
1. Receive reports, bring focus and oversee the critical performance standards, expectations,
and improvement activities of the Professional Staff departments and Hospital services
for appropriateness of care, to insure that processes for delivery of care are analyzed for
opportunities to improve patient care, to insure that corrective action/education taken and
the action plans are evaluated for effectiveness in resolving the issue, to spotlight
performance that differs from the norm, to give management an opportunity to remove
roadblocks to success, and to share best practices;
2. Identify opportunities to improve patient care and set priorities for its evaluation using
relevant indicators, quality improvement tools, and appropriate clinical criteria;
3. Apprise Professional Staff and hospital services of opportunities to improve either care or
processes and recommend appropriate reviews for evaluation;
4. Coordinate and integrate activities to pursue the most efficient use of hospital resources
for the greatest benefit of patient care services provided;
5. Insure that ongoing evaluation and improvement in the use of blood and medications is
performed for appropriate utilization;
6. Establish a plan and carry out a program of concurrent utilization management. It shall

revise the program as necessary to analyze and evaluate different aspects of patient care
Carondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 5 or processes. It shall comply with applicable statutes and regulations for review of
patient care;
7. Appoint a Physician Advisor to review and assess activities of non-physician
Performance Assessment & Improvement Department reviewers. It will empower the
Physician Advisor as delegated by the Executive Committee of the medical staff to
perform procedures outlined in the Utilization Management Plan for decertification of
admission and continued stay;
8. Receive reports of Risk Management/Safety activities and provide for professional
review of hospital claims and evaluation of alternative view-points;
9. Receive reports of the hospital’s Quality Indicators and Financial Indicators;
10. Receive QI Team reports;
11. Provide review of Patient Satisfaction Survey results and make appropriate
recommendations;
12. Review hospital procedures and professional staff practices, and report findings to
departments and MEC with recommendations for appropriate changes for improvement;
13. Assist the Professional Staff in carrying out Infection Control, Surveillance and
Prevention. Other functions include:
A. Maintain surveillance over the Hospital's infection control program.
B. Develop a system for reporting, identifying and analyzing the incidence and cause of
all infections.
C. Develop and implement a preventive and corrective program designed to minimize
infection hazards, including establishing, reviewing and evaluating aseptic isolation
and sanitation techniques.

D. Develop, evaluate and review preventive, surveillance and control policies and
procedures relating to all phases of the Hospital's activities, including: operating
rooms, special care units, central service, housekeeping and laundry, sterilization and
disinfection procedures by heat, chemical, or otherwise isolation procedures;
prevention of cross-infection by anesthesia apparatus or inhalation therapy
equipment; testing of Hospital personnel for carrier status; disposal of infectious
material; food sanitation and waste management; and other situations as requested.
E. Review action on findings from the Professional Staff's review of the clinical use of
antibiotics.
F. Conduct on a periodic basis statistical/prevalence studies of antibiotic usage and
susceptibility/resistance trend studies.
G. Submit written reports at least quarterly to each department on the progress and
results of this activity and of any particular policies and procedures which may
impact the affairs of the department or it's members.
H. On an annual basis, the chairperson of QC will present an annual report to the
Medical Executive Committee concerning the status and appropriateness of the
infection control procedures established by the institution; and
14. Other functions include: Pharmacy and Therapeutics and Medical Record Review.
Meetings - The Committee should meet regularly (at least quarterly) at a designated time.
Special meetings may be called at the discretion of the Chairperson. The Quality Council may
recommend specific CQI topics to the Medical Executive Committee for further study and
problem resolution using the CQI Model.
Carondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 6 CREDENTIALS COMMITTEE OF THE BOARD OF DIRECTORS
Composition - There will be a Credentials Committee of the Board of Directors, which will be

composed of the Chief of Staff or designee, Sr. VP/CEO or designee, and the Board Chairperson
or designee.
The Credentials Committee will function pursuant to policies and procedures adopted and
documented in the Credentialing Policy and Procedures Manual.
Purpose: The primary purpose of the Credentials Committee shall be to coordinate all phases of
the credentialing process.
Duties:
1. Coordinate consistency in overall credentialing policies.
2. Develop a Credentialing Policy and Procedures Manual for Carondelet Holy Cross
Hospital.
3. Review privileging criteria and recommend changes, whenever appropriate.
4. Review recommendations on new appointments and reappointments from the Medical
Executive Committee and present these to the Board of Directors for final action.
5. Educate the Board of Directors on current and future national trends in hospital staff
credentialing.
6. Recommend improvements in the credentialing system.
Meetings: The Credentials Committee of the Board shall meet at least ten (10) times per year.
CARONDELET HEALTH NETWORK HUMAN SUBJECTS COMMITTEE
Composition - The chairperson is appointed by Administration, upon approval of the Chiefs of
Staff of St. Mary's Hospital, St. Joseph's Hospital and Holy Cross Hospital. The Committee is
comprised of the physicians appointed by the Chairperson.
Term of Office - Members are appointed for a two (2) year term and may be reappointed to an
additional two (2) year term. Appointments shall be staggered so that no more than half of the
members will be new in any given year.
Quorum - A quorum shall consist of 50% of the voting members of the committee. There shall

be no proxy voting.
Duties - The Carondelet Human Subjects Committee shall review proposals of an experimental
nature, protocols, concerns with use of investigational or experimental drugs, and new
procedures still not generally accepted.
Meetings - The Committee shall meet as needed at the request of the Chairperson.
NOMINATING COMMITTEE
Carondelet Holy Cross Hospital Organization and Functions Manual
Nogales, Arizona 7 Composition - The committee shall be appointed by the Medical Executive Committee and shall
include members of the Medical Executive Committee, the current president of the Professional
Staff and active members of the staff designated by the MEC.
Duties - The Nominating Committee shall provide nominations for staff officers as required.
The committee shall seek and welcome the advice of the members of the Professional Staff.
Meetings - The committee shall meet as required
CARONDELET HEALTH NETWORK PHARMACY & THERAPEUTICS COMMITTEE
Composition: The committee shall be a multidisciplinary team with at least representatives from
Pharmacy, Administration, Nursing, and Members of the Medical Staff.
Duties: The committee will establish procedures for implementing the pharmacy formulary while
continually overseeing formulary changes/revisions. The committee will address Pharmacy
issues as determined appropriate.
Meetings: The committee will meet monthly.
PROFESSIONAL BEHAVIOR COMMITTEE
Composition - Membership is appointed from among members of the medical staff. The
Chairperson of the committee will be a member of the Medical Executive Committee, other than
the Chief of Staff. The committee will consist of three to seven voting members. Voting will be
restricted to members of the Carondelet Holy Cross Hospital Professional Staff. Administration

will be represented by the Chief Medical Officer or designee.
Term - To be determined by the Chief of Staff.
Purpose - The purpose of the Professional Behavior Committee is to review reported instances of
unprofessional behavior by a member of the Professional Staff. Unprofessional behavior
includes, but is not limited to, verbal or physical threats, demeaning or insulting remarks or
comments, sexual harassment of a physical or verbal nature, and any other activity which is
threatening, intimidating or abusive.
Meetings - The committee shall meet as needed at the request of the Chairperson.
Functions
1. Receive and process all alleged incidents of Professional Staff misconduct.
2. Review all alleged incidents of misconduct which have not been resolved by the department
chairperson and the involved physician.
3. Make recommendations to the appropriate department and/or the Medical Executive
Committee on all reviewed incidents of misconduct.
Adopted by: Revised:
Carondelet Holy Cross Hospital