ColaLife Operational Trial Zambia · Executive summary of Plan: ColaLife Operational Trial Zambia...
37
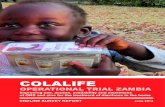
ColaLife Operational Trial Zambia A plan for the first operational trial of the ColaLife concept, in Zambia This is a summary version of the full plan for the ColaLife Operational Trial Zambia Project Outline ColaLife is a non-profit that builds unlikely alliances and develops ‘shared value’, promoting business innovation to help solve developing world issues. A first operational trial with cross-sector partners in Zambia will piggy-back ‘AidPods’ on Coca-Cola’s secondary distribution chain. Fitting into the unused space between crated bottles, each AidPod carries an Anti-Diarrhoea Kit (ADK) for home use by mothers/care-givers in underserved rural communities. Comprised of Oral Rehydration Salts (ORS), zinc, soap and information, education and communication (IEC) materials, they will be sold at an affordable, subsidised price by trained, local retailers in communities, supporting improved livelihoods. Mobile phones provide voucher redemption, authentication and information services. Proof of concept will be assessed through a pre-post test with comparison area as a control, and full evaluation. It will include the collection and dissemination of key lessons learned and proposals for scale up and/or future adaptations. Figure 1: The ColaLife business model ‘[Children’s health] policies will need to be coupled with strengthened distribution systems and new delivery strategies to make a real difference in the availability of the new [ORS] formula to children with diarrhoea.’ WHO/UNICEF, October 2009 ‘Diarrhoea: Why children are still dying and what can be done’
Transcript of ColaLife Operational Trial Zambia · Executive summary of Plan: ColaLife Operational Trial Zambia...

ColaLife Operational Trial Zambia
A plan for the first operational trial of the ColaLife concept, in Zambia
This is a summary version of the full plan for the ColaLife Operational Trial Zambia
Project Outline ColaLife is a non-profit that builds unlikely alliances and develops ‘shared value’, promoting business innovation to help solve developing world issues. A first operational trial with cross-sector partners in Zambia will piggy-back ‘AidPods’ on Coca-Cola’s secondary distribution chain. Fitting into the unused space between crated bottles, each AidPod carries an Anti-Diarrhoea Kit (ADK) for home use by mothers/care-givers in underserved rural communities. Comprised of Oral Rehydration Salts (ORS), zinc, soap and information, education and communication (IEC) materials, they will be sold at an affordable, subsidised price by trained, local retailers in communities, supporting improved livelihoods. Mobile phones provide voucher redemption, authentication and information services. Proof of concept will be assessed through a pre-post test with comparison area as a control, and full evaluation. It will include the collection and dissemination of key lessons learned and proposals for scale up and/or future adaptations. Figure 1: The ColaLife business model
‘[Children’s health] policies will need to be coupled with strengthened distribution systems and new delivery strategies to make a real difference in the availability of the new [ORS] formula to children with diarrhoea.’ WHO/UNICEF, October 2009 ‘Diarrhoea: Why children are still dying and what can be done’

Contents – COTZ Plan - Short Version
Executive summary i
Summary table for administrative information ii
1 Introduction 1
2 Why is the project needed? 1
3 Project purpose and design 4
4 Business model 8
5 Finances 14
Appendices
1 Gantt chart for project implementation 15
2 Organisational roles and profiles 16
3 Project governance and management 20
4 Workpackages – detailed descriptions 22
5 Finances 31
Abbreviations ADK Anti-Diarrhoea Kit ACTs Artemisinin Combination Therapy (anti-malarial drugs) COTZ ColaLife Operational Trial Zambia (name of this project) IEC Information, Education and Communication KZF Keepers Zambia Foundation M&E Monitoring and Evaluation MoH Ministry of Health MSL Medical Stores Ltd MTZL Mobile Transactions Zambia Ltd, trading as Mobile Transactions ORS Oral Rehydration Salts ORT Oral Rehydration Therapy SMS Short Message Service (a text message) WASH Water, Sanitation and Hygiene programmes and techniques WHO World Health Organisation UNICEF United Nations Children’s Fund

Authors:
Jane Berry, Voluntary Director, ColaLife Simon Berry, Voluntary Director, ColaLife Rohit Ramchandani, MPH, DrPH candidate, Johns Hopkins University, USA, previously Senior Advisor, Canadian International Development Agency (CIDA). Contributors: UNCEF, Zambia Jesper Moller, M&E Specialist Dr Ngawa J Nyongani Ngoma, EPI Officer, Health, Nutrition and HIV and AIDS Dr Rodgers K Mwale, Child and Maternal Health Specialist Lusako Sichali, Planning Officer Dr Charlotte Harland, Chief of Social & Economic Policy, Planning, Monitoring & Evaluation Dr Nilda Lambo, Chief, Health, Nutrition and HIV and AIDS.
SABMiller/Zambian Breweries Chibamba Kanyama, Corporate Affairs Director Andrew Ross, Head of Sales and Distribution Panji Banda, Head of Logistics
Keepers Zambia Foundation John Msimuko, Executive Director Ruth Mitimingi, Programme Manager
Medical Stores Ltd Ian Ryden, Director of Logistics Chipopa Kazuma, Essential Drugs Project Manager Acknowledgements
The authors thank all those who have made suggestions on this plan and its precursors and contributed to the development of the ColaLife concept. In particular: Dr Prashant Yadav, Professor of Supply Chain Management at the MIT-Zaragoza International Logistics Center and a Research Affiliate at the MIT Center for Transportation and Logistics; Dr Bonface Fundafunda, Ministry of Health Zambia; Salvatore Gabola and Euan Wilmshurst of The Coca-Cola Company; Patrick Lead, Group Marketing Director, SABMiller, Zambia; Dirk van Wyck, Director, Medical Stores Ltd, Zambia; Victor Simfukwe, TransAid, Zambia; Charles Kalonga, Programme Operations Director, Society for Family Health, Zambia; Monika Tobler and Matthias Saladin of EAWAG; Tielman Nieuwoudt, Supply Chain Lab; Adrian Ristow, Consultant to The Coca-Cola Company; Myles Wickstead; Zahid Torres-Rahman, Business Action for Africa; Claire Matthews, Mohammed Atif and the HORAD Uganda volunteer field work research team; Michael Norton of CIVA, members of the J&J Innovation team and our thousands of supporters online.
We thank funders and supporters who made the planning visits to Zambia and South Africa possible, in particular:
ColaLife supporters who have given time, accommodation and donations for travel expenses The Boulogne to Biarritz cyclists CIVA, the Centre for Innovation in Voluntary Action The Buzzbnk UnLtd SABMiller The World’s Best Hotels
Any errors are the authors’ own and apologies are offered for any inaccuracies.

i
Executive summary of Plan: ColaLife Operational Trial Zambia (COTZ)
The ColaLife concept is based on 3 facts: 1) you can buy a Coca-Cola virtually anywhere in developing countries; 2) in these same places, 1 in 7 children die before their 5th birthday from simple, preventable causes like dehydration from diarrhoea; and 3) over the past 2 decades there has been very slow incremental improvement. A step-change is required to meet the Millennium Development Goals (MDG) for child mortality, which will require truly innovative approaches. Globally, diarrhoea is the second leading cause of mortality in children under 5 years of age, accounting for approximately 15% of all childhood deaths. Six years ago, the World Health Organisation (WHO) and the United Nations Children’s Fund (UNICEF) released a joint statement recommending low-osmolarity oral-rehydration salts (ORS) and zinc supplementation for diarrhoea, yet still few children in the developing world receive these life-saving interventions. Given the scientific consensus and recognition that zinc and low-osmolarity ORS are critical in reducing childhood mortality from diarrhoea, it has been estimated 75% of diarrhoea deaths can be prevented by full coverage and use. Various experts concur, that the problem is worse in rural parts of the developing world where for millions of people ORS/zinc are often not available locally, either because of distance, cost, or stock-outs; providing ORS/zinc solely through public sector clinics has not been effective, comprehensive or sustainable in any country. The roll-out of these effective and simple tools, essential to improving child survival, is in line with current global health policy priorities, but has lost momentum, with calls to re-examine approaches. ColaLife has developed an ‘AidPod’ package that fits between the necks of crated bottles, in un-used space, adding no extra volume and very little weight to a crate. It is working with Coca-Cola and its independent, in-country bottlers to find practical ways to open up their distribution channels in developing countries – in particular the secondary distribution chain - to carry simple medicines and social products the ‘last mile’, to save children's lives. Local agencies will determine the required interventions and models to trial (for example private/retail models; public sector models; hybrid models) and items to distribute, depending on their needs and priorities (eg ORS, zinc, vitamin A, anti-malarials, water purification methods, other medicines or ‘social products’). The model is transferrable to a range of other drinks distributors, commercial operators and products, whilst bearing in mind Base of Pyramid success factors, aspects such as localisation, product sizing and packaging, and costing and pricing could produce a variety of sustainable business models where last mile transport costs are eliminated. For the past 3 years, the concept has been under development, through an ‘open innovation’ process, online and through conferences and meetings. This process continues to be supported by expert leaders in logistics and global health on a pro-bono/voluntary basis, by the ColaLife voluntary Directors, by hundreds of thousands of supporters and by Coca-Cola and its in country bottlers. The last year has involved intensive partnership development, focusing on the localisation of the ColaLife concept for Zambia. Here, limited access of the health supply chain beyond District depots and the line of rail/road, poor availability, stock outs and weak supply management and forecasting beyond district level have led to interest in innovative delivery strategies and private-public partnerships to address issues. Innovation, reach into underserved areas and better promotion of hand-washing are instilled in the local UNICEF Country Plan. A first operational trial has been co-designed to start in late 2011. Costing an estimated USD 1.354m it will focus on delivering Anti-Diarrhoea Kits (ADKs) for mothers and care-givers of under-fives in under-served rural areas, using a subsidised retail model. The implementation partners in Zambia are the Coca-Cola bottler, SABMiller (Zambian Breweries), UNICEF Zambia, Medical Stores Ltd, and Keepers Zambia Foundation, under guidance from Zambia’s Ministry of Health as well as academics, with project management from ColaLife. Key, overarching research questions for this first trial are: • To what extent can the informal Coca-Cola distribution chains be used to improve access to ORS, zinc
and other simple interventions through ‘last mile’ retailers in under-served rural communities? • What effect does this have in supporting mothers/care-givers in home-based management of diarrhoea
in children 0-59 months of age?

ii
Summary of administrative information and workpackage (WP) roles
Project title ColaLife Operational Trial Zambia - COTZ Implementation country Zambia Duration and phasing Phase 1 - 6 months: initiation and product testing; formative evaluation; baseline
establishment; pilot delivery run Phase 2 -12 months: operational trial Post-Trial - 2 month summative evaluation and dissemination
Total cost USD 1,353,789 Funding already secured (cash) USD 250,000 subject to final contract (a Corporate Foundation and Sponsor) Funding pledged in kind USD 97,500 (SABMiller plus oversight from Ministry of Health plus vehicle) Funding sought (cash) USD 1,006,289 Lead organisation/applicant ColaLife Ltd Role Project Manager, Lead for WP01,03,06,09 Address/Post code Registered Office: 18a Regent Place, Rugby, Warwickshire, CV22 7NR Country of applicant/Status UK / Company Ltd by Guarantee 6995665 (UK charity registration underway) Contact name / Title or Post Simon Berry / Director, ColaLife Telephone +44 (0)7932 107109 (UK) +260 (0)9796 73631 (Zambia) Email [email protected] Budget for Lead Organisation USD 339,877 (plus subcontracts and ADK costs as below) Subcontracts to Lead Org USD 159,833 to subcontractors and USD 45,500 for ADK packaging and contents Project Partner 1 Ministry of Health, Zambia Role Governance, Oversight, Lead for WP08 Address/Post code Ndeke House. PO Box 30205, Lusaka, Zambia Country of Partner 1/Status Zambia / Government Department Contact name / Title or Post Dr Bonface Fundafunda / Manager, Drug Supply Budget Line Telephone +260 (0)211 25 41 83 Fax: +260 (0)211 25 33 44 Email [email protected] [email protected] Budget for Partner 1 Will not draw on budget; all time contributed in-kind Project Partner 2 UNICEF Zambia Role Monitoring & Evaluation, Lead for WP02 Address/Post code PO Box 33610, UNDP/UNICEF Building, Alick Nkhata Avenue, Lusaka Country of Partner 2/Status Zambia / International NGO Contact name / Title or Post Jesper Moller / M&E Specialist Telephone + 260 (0)211 252 055 ext. 256 Fax: +260 (0)211 253 389 Email [email protected] Budget for Partner 2 USD 51,000 (plus subcontracts as below) Subcontracts to Partner 2 USD 300,000 (subcontract for Operational Research and M&E) Project Partner 3 SABMiller/Zambian Breweries Role Support, Advice and Facilitation Address/Post code Zambian Breweries Limited, Mungwi Road, Lusaka Country of Partner 3/Status Zambia / Private Sector Contact name / Title or Post Andrew Ross / Sales and Distribution Director Telephone +260 (0)211 241 777 Mob: +260 (0)97 477 1656 Email [email protected] Contribution from Partner 3 Will not draw on budget, Contribution of USD 50,500 (in kind); USD 7,000 (in cash) Project Partner 4 Keepers Zambia Foundation Role: Social Marketing, Lead for WP07 Address/Post code Plot 55 Luwato Road, Roma Township, PO Box 34745, Lusaka Country of Partner 4/Status Zambia, NGO Contact name / Title or Post John Msimuko / Executive Director Telephone +260 (0)211 293333 Email [email protected] Budget for Partner 4 USD 334,250 Project Partner 5 Medical Stores Ltd Role: Logistics/District delivery, Lead for WP04, 05 Address/Post code Medical Stores Limited. Mukwa Road. PO Box 30207, Lusaka Country of Partner 5/Status Zambia / Government owned private sector organisation Contact name / Title or Post Chipopa Kazuma / Project manager Telephone +260 (0)211 242768 / 242346 / 244105 Fax: 246288 Email [email protected] Budget for Partner 5 USD 30,097

1
1 Introduction
ColaLife is a UK-based non-profit organisation specialising in innovation and in creating ‘unlikely alliances’, bringing in the expertise and assets of corporates to assist in solving developing world health issues, creating ‘shared value’, promoting and supporting ‘business innovation’ and testing the potential of ‘hybrid value chains’1. This project will harness the distribution chain of Coca-Cola, recognised globally as one of the most effective in the world2, offering widespread rural penetration in less developed countries3. The secondary Coca-Cola distribution chains, managed independently within an informal market, comprise small scale retailers and often function via bicycle, motorcycle or cart penetrating rural areas more effectively than bespoke public health delivery systems. The model (Figure 1) if effective, is transferrable to other medicines or packs, other distribution chains and countries, and offers potential for speedy scale up. This plan outlines a novel public-private partnership, built on 3 years’ investment in research and concept development, including 9 months’ local partnership development and co-design in Zambia. The ColaLife Operational Trial Zambia (COTZ) will test a highly innovative solution for ‘last mile’ reach of an Anti-Diarrhoea Kit (ADK), using the secondary Coca-Cola4 distribution chain to reach underserved rural communities. Here, diarrhoea accounts for approximately 15% of childhood deaths. Globally, it is the second leading cause of mortality in children under 5 (Figure 2). Research shows that reaching MDG 4 (reduced child mortality) by 2015 will require innovation and a step change in practice (Figure 3).
COTZ will investigate the potential of distributing Anti-Diarrhoea Kits (ADKs). They will be packed by Medical Stores Limited and, in liaison with SABMiller5, taken to district wholesalers of Coca-Cola. From here, village retailers will carry the ‘AidPod’ packs (Figure 4), which are designed to fit in the unused space in the Coca-Cola crates they bring back to their shops, with no additional volume cost and minimal extra weight. ADKs will thus reach households in under-served rural areas, supplying ORS and Zinc closer to the home, together with soap and IEC materials. With a programme of targeted Social Marketing, COTZ will increase accessibility, desirability and use among mothers/care-givers of under fives of a home treatment kit that both equips and educates, to help reduce diarrhoea incidence and severity. A subsidy, based on focus group work, will ensure affordability during the trial, with cost-reduction (eg through localization and economies of scale) for the future, if warranted. Livelihoods of village retailers/micro-distributors will also be improved: ADK packs will be sold, at an affordable price, enabling them to earn a margin on every ADK they carry and sell and by supporting them with training. In Zambia, SABMiller/ Oxfam estimate that a third of small retail outlets that sell Coca-Cola are women-owned2.
2 Why is the project needed?
More than six years have passed since the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) released a joint statement recommending low-osmolarity oral-rehydration salts (ORS) and zinc supplementation for diarrhoea, yet few children in the developing world are receiving these life-saving interventions, prompting renewed calls for action6. WHO/UNICEF report persistently slow
1 Ashoka defines these as business models for commercial partnerships between businesses and citizen sector organizations that leverage critical strengths of each actor to transform markets and meet these critical needs through market access 2 For example, in Zambia, Coca-Cola accounts for 73% of the sparkling beverages market. See: Exploring the Links between international business and poverty reduction, SABMiller, The Coca-Cola Company and Oxfam America, 2010. 3 A recent fieldwork visit by UNICEF Zambia staff to the very remote Shangombo District indicates that even here, the Coca-Cola wholesaler supplied sufficient crates to retailers to cover the number of ADKs required for all of the annual births in the area. 4 In this document we use the term Coca-Cola to mean the Cola-Cola brand and marketing operation (HQ in Atlanta); the independent in-country bottlers; and the distributors and small businesses that work with them to form the distribution chain. 5 SABMiller is the only Coca-Cola bottler in Zambia and one of the largest beverage bottlers in the world. 6 Zinc and low osmolarity ORS for diarrhoea: a renewed call to action, Christa L Fischer Walker, Olivier Fontaine, Mark W Young, Robert E Black, 2009, Bull World Health Organ, 87: 780-786.
‘Coca-Cola cannot do this on its own. If we did, we'd [rightly] be accused of taking over the public health service and meddling where we are not qualified.’ Salvatore Gabola, Coca-Cola's Head of Stakeholder Relations, June 2008

2
progress in diarrhoea treatment; reaching MDG 4 by 2015 requires a step change in practice. About 1.5 million child deaths/yr are due to diarrhoea, killing more than AIDS, malaria and measles combined8. ORS is the ‘gold standard’ of ORT, particularly low-osmolarity ORS combined with zinc. Oral rehydration replaces lost fluids and essential salts thereby preventing or treating dehydration and the risk of death. Glucose contained in ORS enables the intestine to more effectively absorb the fluids and salts. Although zinc, (an essential micronutrient for growth, development and healthy immune system) and ORS in combination have been long recommended for diarrhoea in children7, few trials have investigated how this might best be achieved. WHO state8 71% of children in Africa go without this simple life-saving treatment, with access worse in rural and poor households and that IEC materials also need distributing. WHO recommend a kit using ‘market forces’ and ‘innovative delivery strategies’8. Transport costs can be prohibitive; eg 40% of the price of drugs. Many commentators note the difficulty experienced by the public sector in ensuring adequate supply of drugs, particularly in more rural areas, in developing countries: ‘At public sector health facilities, average availability [of the recommended basic medicines list] is roughly 38 percent; and at private outlets, where products are often unaffordable to most of the population, availability is still under 60 percent’ (WHO/HAI 2008)9. Diarrhoea is seasonal in most of Africa: worse in the rainy season when transport is most difficult and opportunity costs highest. There are virtually no studies that have compared delivery strategies on ORS/zinc uptake, and few examples that countries can build upon10. PSI has had some success in Cambodia with a pack combining ORS and Zinc, Orasel,11 distributing via social marketing partners. Given the scientific consensus and recognition that zinc and low-osmolarity ORS are critical in reducing childhood mortality from diarrhoea, it has been estimated that more than three quarters of diarrhoea deaths can be prevented with full coverage and utilization of these two interventions.12 The problem is even worse in rural parts of the developing world, where for millions of people, ORS/zinc are often not available locally and are hard to come by, either because of distance, cost, or because the supply has run out13. A treatment which is 90% efficacious but delivered to only 20% of those in need clearly has limited operational effectiveness. The roll-out of these effective and simple tools, essential to improving child survival, is in line with current global health policy priorities, but, as pointed out by WHO/UNICEF among other commentators, require innovation and a new impetus14, with interest in harnessing the distribution muscle of the private sector as well as market forces and new business models. In Zambia, bottlenecks exist at district level, with MoH policy to explore public/private partnerships – especially for ‘last mile’ distribution. Health posts can serve communities 30 km away, with walking often the only access option, and queuing for ORS, which, although free, may not be in stock15. The private health sector is one of the smallest in the world with only 70 registered pharmacy retail outlets in 2009, most of these on the line of rail and in major towns16. But in rural communities, it is common to find commercial goods such as bottled colas readily available. Here, diarrhoea is responsible for approximately 15% of all childhood deaths, making it the third major cause of childhood mortality after malaria and pneumonia (WHO, 2008); this is in spite of apparent good knowledge of ORS17 in Zambia; health-seeking behaviour via private sector retailers in rural areas is thought to be low, as provision is so poor. Only 56% of Zambian children under age five with diarrhoea received oral rehydration and continuous feeding (World Bank, 2010). The latest Demographics and Health Survey (DHS) for Zambia notes that six in ten children with diarrhoea were taken to a health provider for diarrhoea related illness (DHS, 2007). Only 60% were treated with solution prepared from an ORS packet; 10% were given recommended home fluids (RHF) prepared at home; and 34% were given increased fluids. 16% of children with diarrhoea did not receive any type of treatment at all.
7 UNICEF, Clinical Management of Acute Diarrhea, WHO/UNICEF, May 2004 8 WHO/UNICEF, 2009, Diarrhoea: Why children are still dying and what can be done. 9 Cited in The Private Sector’s Role in Health Supply Chains: Review of the Role and Potential for Private Sector Engagement in Developing Country Health Supply Chains, October 2008 10 Fischer et al, 2009, The Lancet. 11 Borapich D; Warsh M. Improving Child Health in Cambodia: Social Marketing of Diarrhea Treatment Kit, Results of a Pilot Project. Cases in Public Health Communication & Market- ing. 2010; 4:4-22. Available from: www.casesjournal.org/volume4. 12 Gareth Jones, Richard W Steketee, Robert E Black, Zulfiqar A Bhutta, Saul S Morris, Bellagio Child Survival Study Group, 2003 13 eg see ZICG, 2000; and Werner and Sanders, 1997; and WHO/UNICEF, 2009, Op cit. Discussed further in the full COTZ plan. 14 WHO/UNICEF, 2009, Op cit. 15 Ballou-Ares et al, 2008; author’s field visit to Mpepo Clinic, Mpika District, Zambia, 2010, interview with Dr Rev Samuel Chitundu 16 Disclosure Status of Pharmaceutical Sector Data, ZAMBIA The Medicines Transparency Alliance Zambia, June 2010 17 Peter Berman, Kasirim Nwuke, Ravindra Rannan-Eliya and Allast Mwanza, Zambia, Non Governmental Healthcare Provision, 1995

3
Noting the supplying ORS/zinc solely via public sector clinics has not been effective, comprehensive or sustainable in any country1, one approach that may be effective in improving ORS/zinc usage in areas of limited access is to make it available through the private sector at low cost, with information, education and communication (IEC) on its proper use. Several recent studies have indicated this potential.2 But it is vital to keep in mind that need does not equate to demand. Mothers need to see the values and benefits of giving ORS/zinc to their children, know when and how to use them and where to obtain them locally. There are challenges associated with access, willingness to pay and utilization. Whilst awareness is generally an issue, in Zambia ORS knowledge is well established due to previous Social Marketing campaigns, dating back 10 years or more3, zinc usage less so; yet problems persist here, as elsewhere. Figure 2: Diarrhoea in relation to developing world causes of death in under 5s
Source: UNICEF Hand washing is also considered an issue in Zambia, with UNICEF’s Country Programme Action Plan 2011-2015 seeking for 60% of households in target districts to adopt improved hygiene practices including hand washing with soap by 2015. Figure 3 – Why innovation is needed
Source: UNICEF
1 Fischer et al, 2009, Op cit 2 eg Wang, Wenjuan and Vicki MacDonald. September 2009. Introducing Zinc Through the Private Sector for the Treatment of Childhood Diarrhea: Results from a Population-based Survey in Nepal. 3 Berman et al, 1995 Op cit

4
Zambia has been selected because: • Ministry of Health policy is to encourage innovation and public private partnerships • UNICEF Zambia and other agencies supported the trial design from an early stage • Awareness of ORS alone is good; zinc usage is low • Private sector supply of ORS/zinc is very weak, especially in rural areas • Diarrhoea mortality and dehydration in under 5s still remains a problem • Ease of doing business is relatively high, with English widely used • Mobile phone ownership and penetration is fairly good and improving quickly4 • Mobile money initiatives are established and are developing quickly5 • Projects exist locally from which we can learn6 • The Coca-Cola bottler is supportive, with a track record of innovative CSR projects
Figure 4: Unused space in Coca-Cola crates | AidPods in crate | Sample AidPod contents
Source: ColaLife ADKs will be targeted at mothers/care-givers in underserved rural areas, for home use and are designed to treat two episodes of diarrhoea or 2 children. Subject to final focus group work, the ADK will contain7:
• Four sachets of UNICEF low osmolarity ORS; • Two packets each containing a blister pack of ten 20mg Zinc tablets (PedZinc)8; • Two 25g bars of soap; • Education, Information and Communication (IEC) materials
A programme of community engagement and social marketing will support the use of the ADK and its contents at the community and household level and with retailers. Mobile technology will enable tracking of the ADKs and support anti-tampering and authentication. It will also support subsidies via a voucher system so that local small-scale retailers can make a profit from this new commodity.
3 Project purpose and design
Whilst there has been much discussion in public health circles on the potential of piggy-backing on the Coca-Cola distribution, particularly to reach rural communities9 a fully evaluated trial has not taken place and this project is designed to test and evaluate the concept.
4 40% -50% now own a phone in most rural provinces, with phone borrowing common, raising access to 60%+. See for example, Mobile Communications in Zambia, A demand-side analysis based on the AudienceScapes Survey, David Montez, InterMedia, October 2010 5 Montez, 2010, Op cit. 6 eg MSL and MoH work in health logistics; use of retail routes and subsidised product models eg ACT Anti-malarials; use of e-vouchers by NORAD and others; UNICEF’s Social Cash Transfer programme. 7 Components will be drawn from commodities on the list for Zambia Pharmaceutical Regulatory Authority (PRA) General Sales 8 WHO/UNICEF recommend 20 mg of zinc/day for 10-14 days for children age 6-59 months, and 10 mg for infants up to 6 months. 9 See for example, Always Cola, Rarely Essential Medicines: Comparing Medicine and Consumer Product Supply Chains in the Developing World, Prashant Yadav, Orla Stapleton and Luk N. Van Wassenhove, INSEAD Working Papers, March 2011. http://ssrn.com/abstract=1656386 . And: Personal communications on Coca-Cola’s work with the Government of Tanzania under the Global Fund (Adrian Ristow; Euan Wilmshurst). And: Durgavich, John, Betty Nabirumbi, and Simon Ochaka. (2008). Uganda, Mapping the distribution of retail goods to the last mile. Arlington, Va.: USAID | DELIVER PROJECT, Task Order 1.

5
3.1 Main questions to be answered • To what extent does the Coca-Cola distribution chain improve access to and utilization of
affordable ADKs through ‘last mile’ retailers in under-served rural communities?
• What effect does this have in supporting mothers/care-givers in home-based management of diarrhoea in children 0-59 months old?
3.2 The project logic and expected outputs A Logic Model and Logical Framework have been co-designed by key stakeholders and agreed to by all partners. The model will serve as a key communication planning, management and measurement tool. It describes the project, its overall goal, intermediate and immediate outcomes, outputs and activities. Inputs are also discussed in the accompanying text, as are potential contextual factors that will be considered. The Logic Model is at Figure 5, overleaf. The model is divided into three key streams of work, namely: A) the supply chain stream; B) the knowledge, attitudes and practice stream; and C) the knowledge translation stream. All three streams will work in unison to lead to the overall impact/final outcome of contributing towards MDG 4 – a reduction in child mortality. In addition, the programme will exemplify a key tenet of MDG 8 – promotion of global partnerships for development, especially to provide access to affordable, essential drugs in developing countries. Given the required timelines and resources associated with effective measurement of mortality impact, analysis at this level will be out of scope for the current trial, and it will therefore end at the intermediate outcome level. Key inputs for the trial include funding, programme policies established and planning conducted during the design phase, commodities (e.g. AidPod package, ORS, zinc, soap, etc.), relevant country policies (eg zinc), coordination processes during the project, as well as the relevant human resources and expertise required to make the programme a success. Measurement and development of a strong evidence base is essential for future scale-up and knowledge generation, so key activities within stream C will include implementation of the monitoring and evaluation (M&E) plan, continued execution of the open innovation process (ie leveraging of Social Media tools) as well as the development of an eventual sustainability or exit strategy. Lessons on the value chain, costings for the ADK, its packaging and contents, the potential for future localisation and cost-reduction, transport costings and a comparative value-for-money exercise, will also form key learning elements.
3.3 Project design Of great importance for evaluation design is the level of inference required by decision makers. Due to the strong global interest in this pilot, its potential for health impact, as well as the potential for scale-up, the ColaLife pilot will utilize a plausibility design. These appraisals go beyond adequacy assessments by trying to rule out potential confounding factors which could potentially cause any observed effects27. These types of assessments attempt to control for influence of confounding factors by choosing control groups before an evaluation is begun or during analysis of the data. In this case, an external control group will be used by randomly allocating one of three selected districts as a comparator (i.e. not receiving the intervention) for the two other districts which will receive the intervention. We will utilize a longitudinal-control, which means interventions and control districts will be compared at the beginning and end of the programme cycle. Specifically, we will be utilizing a quasi-experimental pre-post test design with comparator. This helps result in much more plausible conclusions than if no control was used. In many ways, plausibility assessments are akin to the ‘natural experiments’ common in public health27 This design can be diagrammed as follows:
District A O1 X O2 District B O1 X O2 District C O1 O2
Where each row represents a different district, O1 = baseline observation/data collection, O2 = post intervention observation/data collection and X = intervention.
27 Habicht JP, Victora CG, Vaughn JP. Evaluation designs for adequacy, plausibility, and probability of public health programme performance and impact, 1999. Intnl Journal of Epidemiology; 28:10-18

6
Selection of districts in Zambia and the control is under consideration and will include criteria such as:
• capacity of implementing partners in selected districts • presence of multiple private outlets that sell Coca-Cola • remote/rural designation (to be defined based on distance from Lusaka) • poverty level (proportion of population in 4th and 5th socio-economic quintiles) • high rates of diarrhoea • poor access to healthcare
All private shops in the districts that procure Coca-Cola from SABMiller wholesalers will be eligible to participate. Relative changes in key outcome level indicators will be measured prospectively. Methods will likely include retail audits, household surveys, mystery shoppers, review of routine health information systems reporting, and key informant interviews. Qualitative data will be collected to supplement and help interpret quantitative measurements. It is hypothesized that a statistically significant (p<0.05) greater improvement in health and behaviour indicators (i.e. proportion of children aged 0-59 months with diarrhoea who used ORS and zinc from an ADK in the past month) will be achieved in the intervention districts as compared to control districts. Where possible, data and lessons learned from UNICEF Zambia’s social cash transfers programme will be leveraged. In addition to key indicators, documentation will also be collected on various factors outside the implementation of the programme which can influence outcome. These contextual factors may include:
• Proximity to health centre • Climate/altitude/seasonality • Demographics; Socio-economic features • Diarrhoea rates; mortality rates; birth rates • Health facility quality • Other diarrhoea programmes (programme mapping) • Health worker to population ratio • User fees • Epidemics/Crises/etc.
Efforts will be made to ensure that intervention and control districts are as similar as possible with reference to these types of factors. By reducing the non-treatment differences between the experimental and control groups, matching will make it easier to achieve significance on statistical tests, as well as making it possible to reduce sample size. Quasi-experimental designs are not as strong in controlling for threats to the internal and external validity as true controlled experimental design, but these designs are rare in operational public health practice. From an academic perspective, the shortcoming of this type of design is that one cannot completely rule out all alternative explanations for observed differences between intervention and control areas. However, by demonstrating consistent results along the flow of the logic model and taking potential confounders into consideration, alternatives can be demonstrated as to be unlikely enough as to be negligible. The evaluation design and process will be iterative, and is subject to alteration based on ongoing monitoring and feedback, with opportunities for mid-course correction. Investigators of this project will seek approval from the review board at the Johns Hopkins School of Public Health, and also the relevant national review board in the Zambia. The study will adhere to the highest ethical standards for research practice.
3.4 Project partners Partners have been selected on the basis of their expertise and their interest, commitment and contribution to the co-design process. Partners’ profiles and their roles are outlined in more detail in Appendices 2 and 4. In outline, they are: • ColaLife: Project management, vision management; communications and secretariat, Value Chain • UNICEF Zambia: Management of the M&E subcontractor; technical advice • Medical Stores Ltd: Procurement, packing, assembly, storage, delivery to district level • Keepers Zambia Foundation: Community engagement; social marketing • SABMiller: Advice, liaison with wholesalers • Ministry of Health: Oversight and governance, chair of Steering Committee, advice, district liaison Subcontractors include The PI Group (packaging) and Mobile Transactions Zambia Ltd.

7
Title: Figure 5: ColaLife Operational Trial Zambia Project Number: 2011/1 Responsible Officer: Simon Berry, ColaLife
Country: Zambia Budget: USD 1.354m Duration: 20 months
Final Outcome
Contribution towards MDG 4 – reduced childhood mortality – by reducing incidence (and severity) of diarrhoea in children 0-59 months in underserved rural communities
Intermediate Outcomes
Mothers and care-givers of children 0-59 months in underserved rural communities: • increase use of ORS and Zinc in household treatment of diarrhoea • increase use of appropriate hand washing practices
Lessons learnt /results disseminated Sustainability / exit strategy implemented Public Private Partnership established for Last Mile supply chain model to scale up
Immediate Outcomes
(A) Improved access to [affordable] ADKs (anti-diarrhoea kit) in underserved rural communities via profit-driven supply chains
(B) Increased awareness of ADKs and benefits of contents (ORS, Zinc, Soap) among mothers/care-givers
Relevant data effectively collected and analysed Sustainability/exit strategy agreed
Outputs
1 ADKs meet needs at all levels in value chain 2 Novel leverage of the Coca-Cola supply chain meets demand for ADKs in under-served communities 3 Retailers and wholesalers trained in benefits of ADKs
4 IEC/Social marketing programme for mothers/care-givers on benefits of ADKs designed and implemented
Effective M&E programme and learning framework designed and implemented
Activities
1 Design Anti-Diarrhoea Kit (ADK) to meet all needs in the value chain • Procure contents: ORS/Zinc, soap • Design costing, margins, pricing, subsidy/credit availability, vouchers and tracking • Test affordability, desirability and attractiveness of product • Design and test packaging (functionality, fit, robustness/damage, tamper-proofing, attractiveness, messaging)
2 Design and implement novel supply chain leveraging Coca-Cola Last Mile distribution, to meet demand • Implement packing and fulfilment process for the ADK product • Distribute ADKs to wholesaler level • Leverage last mile distribution via Coca-Cola retailers/entrepreneurs
3 Design/deliver awareness raising, training and follow-up to convey benefits of ADKs to retailers and wholesalers
4 Design, test and deliver a social marketing campaign to convey to mothers/care-givers the benefits of ADKs • Design, test and produce IEC materials for inclusion in/on ADKs • Design, test and deliver household-level awareness-raising & training • Design, test and deliver community level activity and media channels
Design and implement effective M&E programme with separate M and E functions and learning framework Formative dissemination of activities and issues (open innovation approach) Design sustainability or exit strategy
Results chain A : Supply Chain Results Chain B : KAP among Mothers/Care-givers Knowledge translation

8
4 The business model
The business model underlying the ColaLife Operational Trial Zambia is shown in Figure 1. The project will focus on getting Anti-Diarrhoea Kits (ADKs) to mothers, care-givers and mothers-to-be in remote rural communities, via the private sector commodity distribution network; the same network that gets Coca-Cola to remote rural areas of Zambia. It will embed private sector motivations into the distribution of these ADKs; the same motivators that get commodities such as cooking oil, salt, washing powder, talk-time and Coca-Cola to remote areas in Zambia. The ADKs will be packed in AidPods that are designed to be inserted into Coca-Cola crates at the Wholesaler level in the distribution chain. This will increase number of saleable units (24 bottles plus 5 ADKs) and therefore the profitability within a crate, as profit will be made from both the sale of the beverages and the ADKs. The ADKs will be assembled by Medical Stores Limited (MSL) in Lusaka and packed into standard cardboard cartons. The cartons of ADKs will be distributed to participating wholesalers by MSL. The retail price of the kits will be based on an assessment of the willingness and ability to pay of mothers, care-givers and mothers-to-be in remote rural communities. Based on this, and the margins that need to be made by wholesalers and retailers, the level of subsidy will be determined and injected at the start of the distribution chain. Crucial to success will be a social marketing campaign aimed at turning ‘need’ into ‘demand’ for ADKs by mothers. This will consist of awareness raising activities by community-based Promoters; IEC campaigns using community drama, household visits, posters and leaflets. Community-based Promoters will carry out follow-up visits to households and target communities to reinforce the other elements of the social marketing effort. To supplement the social marketing work in communities we will:
• Provide vouchers to mothers and care-givers (e.g. at health centres and community meetings) so that their first ADK is free
• Provide a 50% off voucher for the second purchase (e.g. via mobile phone) • Provide training to the Wholesalers and Retailers in the benefits of the ADKs (so that they can sell
them effectively) • Ensure adequate margins are made along the distribution chain
Although highly innovative as a model, most elements already exist in one form or another in the public, private and NGO sectors. The ColaLife Operational Trial Zambia brings partners from the different sectors together and provides the environment for them to work successfully together combining their skills and experience in new ways. Partners’ Roles are in Appendix 2. Subsidy is a characteristic of the business model in the trial period to establish demand in a short timescale and to provide an incentive for all players in the value chain to engage. In the longer term, we believe we can establish a value for the ADKs and a willingness to pay. The trial will be key in establishing the amount that mothers, care-givers are able to pay, and that required for the distribution chain to work in the private sector. In future, cost reductions obtained by economies of scale, localized packaging manufacture, local procurement, review of pack size and contents, and other factors will bring down the cost of each pack. A small subsidy may be required post trial, whilst appreciation of the value of the commodity and its contents develop and are established, and possibly even until improved livelihoods support increased household expenditure. Meanwhile, a parallel, independent investigation will look at ways to generate any cross-subsidy required on a sustainable basis for the short to medium term, with likely assistance from corporate partners, once business benefits are established. Generally speaking, the public sector uses ‘push’ models of distribution. COTZ will be using a combination of push (to district level) and ‘pull’ beyond this (the so-called ‘last mile’) to distribute a public health product through the private sector.
4.1 Social Marketing For the ColaLife business model to work there will need to be demand on the part of mothers and care-givers for ADKs in the under-served, rural communities we are targeting. We are seeking to create a demand for ADKs in the same way that demand has been created for other consumable products like detergent, talk-time and beverages such as Coca-Cola. Many authorities agree on the importance of Social

9
Marketing campaigns, adapted to the product and the customer base. Boggs et al (2007)1 working on Zinc promotion in Cambodia, found that ‘IPC [Inter-Personal Communication] combined with mass media, was critical to the behaviour change success.’ This operational trial will investigate to what extent market forces can be harnessed, by manipulating the 4 Ps of marketing (Product, Price, Place, Promotion). Product ADK is ‘desirable’, contains what a mother/carer need to treat diarrhoea at home;
contains soap – a desirable product. Price Production price for the project is subsidized; voucher renders the product free/low cost
at point of sale; retailer and secondary distributors make small profit on each item; piggy-‐backing cuts/removes transport cost of ADK; social marketing establishes local knowledge of expected price; formative research allows us to price in the appropriate range
Place Local availability in village retail shops; kiosks makes product accessible;more accessible than ORS via a more distant health post.
Promotion Retailers and wholesalers trained in the benefits of ADKs; Social marketing creates awareness and promotes ADK as useful and desirable product (e.g. being a knowledgeable mother); mothers/care-‐givers educated in understanding and using the contents; Vouchers create demand during the project period to ensure ADKs are subject to a ‘pull’ factor, typical of soft drinks and other ‘desired’ products.
Whilst setting the ‘right’ price can only be ascertained by work on the ground during this project for this customer base and this product, there are some indicators of acceptable price parameters. For example, a Nigerian peri-urban study on diarrhoea in under 5s found that median household expenditure per episode was USD 1.202. Borapich et al (2010) set the price of the Orasel Kit used in Cambodia at 1500 Riel or USD 0.38, based on discussion with focus groups and price comparisons with other ORS treatments and ‘comparable products for price decisions’ for Zinc (such as antibiotics). In Cambodia, the Orasel Kit sales reportedly reached double that projected in the project time frame (33,000 packs) and caused stock-outs.
4.1.1 Establishing the foundation for demand creation The social marketing will build on the activities undertaken through other trial workpackages ie:
• Creation of an ADK that mothers and care-givers find attractive • Availability of the ADK at a price mothers/care-givers can afford and are willing to pay • Training of retailers in the benefits of the ADKs so they are more skilled at selling
4.1.2 Demand creation The social marketing workpackage (WP07 – see Appendix 4) will focus on creating a desire among mothers and care-givers to have their own ADK in the home, to include the following activities:
• Selection and training of a ColaLife Promoter from each of the communities • Management of these Promoters to:
o Run awareness-raising events in communities, churches and schools on the value of ADKs and where and how to get them
o Run smaller group events focussing on using the ADK as part of a wider WASH3 regime o Participate in community events being undertaken by others o Undertake household visits o Distribute vouchers to mothers and care-givers and collect mobile phone numbers o Return a limited amount of monitoring information via SMS into a project database
• Production of Information, Education and Communication (IEC) Materials: o Printed on the outside of the ADKs o Provided as a leaflet inside the ADKs
1 Boggs, Malia, Dainah Fajardo, Susan Jack, Susan Mitchell, and Patricia Paredes. October 2007. Social Marketing Zinc to Improve Diarrhea Treatment Practices: Findings and Lessons Learned from Cambodia. 2 Out-of-pocket health expenditure for under-five illnesses in a semi-urban community in Northern Nigeria. 2004 M. N. Sambo, C. L. Ejembi, Y. M. Adamu and A. A. Aliyu Department of Community Medicine, Ahmadu Bello University, Zaria, Nigeria 3 An objective of UNICEF in the area of water, sanitation and hygiene (WASH) is to contribute to the realization of children’s rights to survival and development through promotion of the sector and support to national programmes that increase equitable and sustainable access to, and use of, safe water and basic sanitation services, and promote improved hygiene.

10
• Leaflets for use at community events • Posters for public display in public places (churches, shops, schools, markets, bars)
4.1.3 Demand creation – other supporting measures The social marketing activities in the targeted communities will be supported by:
• Making paper vouchers available at clinics and via Promoters for 100% of the cost of the ADK • eVouchers worth 50%, given to mothers and care-givers who authenticate the ADK (this will be at
the mother’s choice and would be an optional not required action) • SMS messaging to mothers and care-givers who have received a paper voucher and given a mobile
phone contact number (free to the mother). • Features about the project on community radio
4.2 Application of m-Health interventions Mobile phone based systems will support these elements of the project4. This will be managed via a subcontractor to ColaLife, the Lusaka-based, Mobile Transactions (MTZL).
4.2.1 Authentication and tamper evidencing To check that the Anti-Diarrhoea Kit (ADK) is genuine and has not been tampered with, a label carrying a unique authentication code (the ADK Code) will be applied to the ADK as part of the packing process. This will be done so that the ADK cannot be opened without damaging the label. A damaged label would indicate that the ADK had been tampered with. The mother, mother-to-be or care-giver will be able authenticate the ADK using their own SIM, either loaded in their own mobile phone or somebody else’s. We will not be able to enforce authentication but we want to reward it; to encourage authentication. When mothers or care-givers authenticate their ADK, they will receive an eVoucher giving them 50% off the cost of purchasing their next ADK. Authentication SMSs would be free to the mother or care-giver. The system will receive the ADK code on the ADK label by SMS and reply automatically to indicate if the ADK is genuine. It will provide a short amount of additional text thanking the user for authenticating and providing additional ‘what to do next’ type information. The system will record and retain the mobile phone number of the person authenticating, although hidden caller numbers will be permitted.
4.2.2 Voucher redemption - Paper vouchers Paper vouchers will be given to mothers during pregnancy, at the birth of their child or following birth – for example when a mother-to-be or a mother with an under 5 year old presents at a clinic/health post or community event. These vouchers may also be given by community care-givers/promoters or by public health institutions. Some mothers/care-givers may get more than one voucher. All vouchers will be valid. During the project, mothers and care-givers will be able to redeem these paper vouchers for an ADK without the need for a cash payment (ie the ADK will be free to them; this will be reviewed post-project). A mobile phone will be used by the retailer to redeem the voucher. Retailers will be set up with ‘mobile money’ accounts as part of their registration and training. Mobile money accounts are established, easy to set up and quickly becoming more common in Zambia. Participating retailers will be registered during the training delivered by the project and their mobile phone number collected and entered onto the system at this time. Once a mother/care-giver presents at the retailer, the retailer will reveal a code on the voucher (eg by scratching off a concealing strip,) and will send this code (the Voucher Code), together with the ADK code to the mobile system by SMS. The system will respond indicating whether the ADK is genuine or not. In the case that the ADK is genuine and the voucher code is valid the retailer’s mobile money account will be credited with the value of the recommended retail price of the ADK. The system will record and retain the mobile phone number of the retailer. Hidden caller numbers to the voucher redemption part of the mobile system will not be permitted. Only registered and trained retailers will be able redeem vouchers.
4 Mobile elements of the design have taken account of data and conclusions from the AudienceScapes Zambia research at http://www.audiencescapes.org/node/2 and related publications on this site, as well as other sources, including MTZL.

11
In the case that the ADK is not genuine the retailer will be prompted to select another ADK from his/her stock and enter its number until a genuine ADK Code is entered. All non-genuine call data will be maintained by the system for subsequent analysis. In other words, the system will retain the data from all SMS exchanges, valid and invalid. All non-genuine ADK codes will be investigated and followed up by a field visit if necessary.
4.2.3 eVouchers Mothers or care-givers who authenticate their ADK will be rewarded with an eVoucher which will be stored to their SIM. The eVoucher will be worth 50% of the retail price of the ADK. The system will enable the transfer of the eVoucher to the retailer’s SIM and the retailer will be able to redeem the eVoucher in the way described above for the paper voucher. In an eVoucher transaction, the mother or care-giver will be required to pay the remaining 50% in cash to the retailer, if s/he chooses to buy another ADK.
4.2.4 SMS-based health messaging When paper vouchers are given to mothers or care-givers they will be asked to provide a mobile phone number, if they have one. This may be their own SIM number or the number of someone they trust. The person collecting this number will also record the birth date of the child for women with children under 5 years old (or estimated birth date). This information will be used to send regular health messages and reminders to mothers and care-givers using SMS (with options to stop or forward the service). Subject to final agreement, health message content will be provided by Johnson & Johnson based on their experience with the Text4Baby initiative (USA), contextualised for local use.
Figure 6: The mobile phone tracking system
Source: Mobile Transactions – MTZL 1. COTZ deposits funds into their Mobile Transactions account to cover the value to be transferred to retailers for voucher
redemption. 2. A voucher distributor (community-based Promoters) optionally registers a client (mother/care-giver) using a mobile phone and
collects monitoring and evaluation information, including but not limited to mobile number. 3. A voucher distributor uses a mobile phone interface to optionally link a client (eg at a clinic or other convenient location) to a
specific voucher scratch card so that only that person may later redeem the card voucher. 4. Client goes to a participating retailer to redeem the voucher and receive/purchase an ADK. 5. Retailer redeems the voucher using the Mobile Transactions mobile interface to verify the authenticity of the voucher and
optionally that the client has been linked to the voucher. 6. After successful redemption, funds from the COTZ/ Mobile Transactions account are automatically transferred to the retailer’s
account for any subsidy/discount. 7. Real-time reports available to COTZ on system transactions (registered mothers/care-givers, voucher distribution/redemption) Not depicted: 8. Clients may be auto-registered for health messaging (mobile number collected at voucher distribution) 9. COTZ project partners may load health messages into a database using an online interface. 10. The SMS system will periodically send health messages from the database to those registered to receive messages.

12
4.2.5 Additional considerations The target communities will be ‘flooded’ with paper vouchers during the project to help ensure that there is adequate pump priming of the demand for ADKs. We will not be too concerned if mothers or care-givers receive more than one paper or eVoucher and/or if some vouchers are not redeemed. However, redemption/non-redemption data will be valuable for monitoring and evaluation purposes and all data will be retained for monitoring and evaluation purposes. Both types of voucher will have a ‘valid until’ date, to coincide with the end of the project. A fourth service, of prompts/ reminders / advice to retailers may be a consideration. Retail advice content would be provided by the retail training sub-contractor. A budget line for this is included under a sub-contract selected and managed by ColaLife. Final selection will depend on local considerations based on the final selection of districts. Other partners (SABMiller, KFZ) will advise and support.
4.3 Bottom of the pyramid success factors A recent report from the McKinsey Global Institute1 is one among many, which points to the growing economic potential of African countries with their growing consumer spending, burgeoning populations – with around 50% under the age of 16 in many countries - and promising economic growth. At the same time there are persistent issues of poverty, and an urgent need for job creation and improving livelihoods. This is particularly true for the so-called Base of the Pyramid (BoP); those people earning less than USD 1–2 per day. Health and wealth are inextricably linked; for example, it has been estimated that a 5% improvement in child survival rates can raise economic growth by one percentage point a year over the following decade2. The ColaLife model seeks to improve incomes of the smallest rural retail kiosk-owners, for example in this COTZ trial, by enabling them to earn a margin on every ADK they carry and sell, and by supporting them with training. In Zambia, SABMiller/Oxfam estimate that a third of these are women3. Future projects might also require micro-finance, which will be a point of learning from this project. A longer term aim is to localise the production of the ADKs through: the local manufacture of the ADK Packaging and the local manufacture and/or sourcing of the ADK components4. Key publications on serving those at the ‘Base of the Pyramid’ have summarised success factors, which this project attempts to emulate. Improvements in health and wealth are linked. This project seeks ways to improve the livelihoods of those who serve the rural poor, as well as improving health. The following success factors are compiled from CK Prahalad (2010)5 and Ashish et al (2009)6: • Affordability; low cost products (e.g. production localised or adapted for affordability) • Desirability: maintaining quality and desirability of product • Access and availability, delivering products when and where customers need them • Potential to scale up/drive down costs • Adapted business models with a full understanding of the market and customers • End to end organisation of the supply chain • Focus, to build a value system around a narrow range of products • Using ‘soft funding’ to investigate/establish innovations which then convert to marketable products • Time to develop and scale up • ‘Para-skilling’ of non experts (e.g. shop-keepers in simple medicines) • Piggy-backing distribution • Ability to communicate the value proposition to all customers and stakeholders • Sustainability (based on an appropriate combination of at least some of the above factors)
1 Lions on the move: the progress and potential of African Economies, Roxburgh et al June 2010 2 Anderson and Hague (2007) The Impact of Investing in Children: Assessing the Cross-Country Econometric Evidence, ODI Working Paper 280 cited in Eliminating World Poverty: Building our Common Future, Dfid 2009, UK Stationery Office ISBN: 978-0-10-176562-6 3 Exploring the links between international business and poverty reduction. The Coca-Cola value chain impacts in Zambia and El Salvador, Oxfam America, The Coca-Cola Company and SABMiller, 2011 4 Local assembly of the ADKs by Medical Stores Ltd is already a part of this trial; see Appendix 4. 5 The Fortune at the Bottom of the Pyramid, Eradicating poverty through profits, 5th Edition, C K Prahalad (2010) 6 Emerging markets, Emerging Models, Market-based solutions to the challenges of global poverty, Ashish Karamchandani, Michael Kubzansky, and Paul Frandano, March 2009

13
4.4 Feasibility, Assumptions and Risks Feasibility has been assessed, assumptions have been refined and risks have been mitigated, through building a strong partnership over time, through investment in the co-design of the trial, developing trust and seeking inputs from many expert partners and stakeholders, both globally and in Zambia and through reference to both academic papers and learning from practical experience from similar trials in Zambia and elsewhere. We have allowed a 6-month lead in period, to test a range of issues, monitor contextual factors, select districts for requisite factors, establish clear baselines, carry out focus groups work with customers, identify particular areas of the trial for adaptation, strengthening or training, refine details of the ADK and packaging, carry out a full trial delivery run and make final adjustments to the Operational Trial period, where needed. As spillover effects or cross-over contamination from intervention to control areas could pose a risk in a randomized cluster study design, a pre-post trial in two districts with a third control comparison area is currently preferred. This will be finalised upon identification of districts that meet the selection criteria and an alternative study design may be introduced, subject to the local context and budgetary constraints As the ADK is a composite pack there is a risk associated with multiple messaging (ORS, zinc, handwashing). We have mitigated against this in selecting Zambia as the trial location. Here, whilst the package, some elements of its contens and its access points may be new, ORS sachets are well known and recognized. Whilst English is widely spoken and understood, in rural areas around 25% of people have no English7; so we will also use graphical IEC materials and local languages where possible and have selected KZF as an indigenous Zambian NGO for its experience here. Moreover, Social Marketing will re-inforce messaging and provide demonstrations. Care will be needed over the provision of zinc, which is less well known, with clear graphical and local language instruction on halving the dosage (ie half rather than one tablet) for children under 6 months. The selected tablets are marked to aid division into 2 parts. Demonstrations as well as graphics will be used. It is recognized that theft and ‘leakage’ from public health systems is endemic; however, within a retail system, each carrier and stocker of the ADK will have a vested interest in its value. We have planned a tamper-evident label as a seal for the ADK and mothers, carers, retailers and wholesalers will be trained to recognize this and reject spoilt or opened packs. They will be trained on the contents to expect in each pack, so they can reject incomplete packs. An authentication system via SMS will enable sampling and tracking. Costing and pricing are key elements of this trial and the correct balance along the value chain will be key to successful buy-in at all stages. Focus groups at the outset will determine attractiveness and ability/willingness to pay. Discussions with retailers/wholesalers will also inform the business model for the trial and future models. Cell phone technology and the use of SMS messaging is a new area where risks may occur. Information available on cell phone usage in Zambia is good8. In MTZL, we have selected an experienced, local sub-contractor in the use of e-vouchers redeemable by SMS, in tracking and mobile payments. We will select areas with adequate mobile coverage; these are good in Zambia along the line of road/rail, and improving constantly39. Whilst not all mothers/carers will have access to a SIM or mobile phone, the success of the trial does not depend on this. Should selected retailers not have a phone, basic models are made in Zambia at a low price so they could be provided from the Social Marketing budget.
7 AudienceScapes survey research project conducted in Zambia by InterMedia October 2010 8 eg the above AudienceScapes work and publications drawing on it, such as Mobile Communications in Zambia, David Montez, 2010

14
5 Finances
5.1 Financial plan The full cost of the project as detailed in Appendix 5 is calculated as USD 1,353,789. This is derived from full spreadsheets obtained from each partner, and the financial modelling is available in full on request. We have allowed a contingency of 2.75% of the total. Tables in Appendix 5 break down the project costs, by partner and by workpackage. We expect the required fund to be made up as outlined below. Below, we also ascribe an additional value to the planning, preparation and co-design so far invested.
5.2 Sources of funding
Already invested, in kind ColaLife has given the equivalent of 3 full time volunteers on this proposal for the past year, and in addition leveraged expert advice from more than 30 experts, valued at in excess of USD 250,000. During the concept development phase, stakeholders and implementation partners (other than ColaLife) have already donated an estimated 200 hours of staff time, over the past 9 months, to co-designing this project, valued at a minimum of USD 12,000. Johnson & Johnson have given travel, accommodation, training and staff time to developing the project concept, valued in excess of USD 20,000.
Pledged, in cash Subject to approval of this planning document, a corporate foundation has pledged to provide up to USD 250,000 towards project costs, expertise and advice, and a project liaison and technical support role equivalent to one half time post for the duration of the project. We have been invited to approach a second corporate foundation.
Pledged, in kind SABMiller estimate their future in-kind contributions to the project as in excess of USD 50,500 and will cover printing costs (USD 7,000). We are in liaison with a global manufacturer, who have been supporting ColaLife and in response to their offer of donated equipment, we have requested provision of a 4 wheel drive vehicle to the in-country project manager, for the use of the project (budgeted at USD 40,000).
Summary of funding secured and sought (USD) Source Amount/Cash In kind Stage of bid or pledge Comment Corporate Foundation 1 USD 250,000 Verbal agreement Subject to plan approval Corporate USD 250,000 Public funding (innovation) USD 289,855 In discussions Alternative source possible International Foundation USD 466,434 SABMiller contribution USD 7,000 USD 50,500 Pledged Printing costs plus time Other partners MoH not drawing on budget Global manufacturer USD 40,000 In discussions 4 WD vehicle donation

15
Appendix 1: Gantt chart
The timeline has been worked out through face to face meetings and a co-design workshop with partners. Up until project inception (anticipated last quarter 2011) preparatory work will continue to ensure all the required funding, legalities and governing documents are finalised. The implementation of the trial will begin with a 6-month preparatory period (Phase 1) which will cover product refinement with the target group (mothers/care-givers) and an end-to-end rehearsal of the distribution mechanism through one of the selected wholesalers to a small sample of retailers. A 12-month operational trial phase (Phase 2) allows for any variation across seasons. We have allowed for a 2-month period to wrap up the trial and undertake the summative evaluation. We anticipate a start before the end of 2011, subject to securing the funding package required. All implementation partners are ready to proceed.

16
Appendix 2: Organisation profiles and roles
ColaLife
ColaLife is a new organisation specialising in innovation and in building ‘unlikely alliances’ with 5 highly experienced voluntary directors. Two (see CVs) have executive roles and have each spent more than a decade in the developing world, including 3 years in Zambia, as well as working up to government level in the UK. ColaLife’s Voluntary Directors include Treasurer, Jo Knowles, a qualified accountant with 20 years’ experience in senior finance roles in international and national NGOs. In addition, ColaLife can draw on voluntary/pro-bono input from over 30 expert advisors and their networks. Legal Advisors include experts in charity law, contract law and IP at Allen Overy, London. Technical advice includes the commitment of Rohit Ramchandani, MPH, DrPH candidate on a full-time stipend. ColaLife (the organisation) has driven the development of this project, including the vision and innovation, and has led on preparation and collation of project bid documents. ColaLife will lead on the applications to funders. At the request of partners, ColaLife will provide the overall project management (WP01) and provide the secretariat to the project’s Steering Committee (within WP08). The 2 Directors implementing the project plan to move to Lusaka by autumn 2011, subject to immigration formalities, and will remain there until the project’s completion. Developing stakeholder relations has been a key part of the preparatory work, and on-going partnership relations, reaching out to other stakeholders and leading on succession planning for the future will continue to be key functions led by ColaLife. ColaLife will lead on WP03 (ADK Packaging), to manage the packaging sub-contractor: PI Global. ColaLife will also lead on Workpackage 06 (The Value Chain) supported by Johnson &Johnson, subject to final confirmation. The Value Chain work (WP06) will include: the assessment of what mothers would find attractive in an ADK and their ability/willingness to pay; the mobile phone elements of the project (authentication, voucher redemption and messaging); the establishment of the supply chain margins and distribution costs and the training of wholesalers and retailers (including training on the benefits of the ADKs). Mobile phone elements of WP06 will be sub-contracted to Mobile Transactions (MTZL) and managed by ColaLife. Simon Berry, Voluntary Executive Director & Founder, ColaLife Role in project: Project Manager
Profile Highly innovative and effective partnership and stakeholder development specialist with a background combining 12 years in Developing World capacity building and 20 years in charity development, government consulting and leading edge ICT. Experience at international level, in UK government departments, and to CEO level in the UK non-profit sector. Consultant and international speaker, with well established reputation and proven experience in new technologies for engagement and community empowerment. A widely acknowledged and effective Project Manager of large and complex international partnerships. Expert facilitator for collaboration, alliance-building and partnership development with experience at grass roots level working directly with communities. Horizon scanner; demonstrable experience in forming strategies to ensure community engagement and empowerment – in UK and beyond. Highly numerate and comfortable interpreting research data. Personally committed to making a real difference to people's ability to shape their community, services, and quality of life Rohit Ramchandani, MPH, DrPH candidate, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Consultant to ColaLife (voluntary to date) Role in project: Public Health Advisor, M&E/trial design Advisor, Knowledge translation.
Profile Prior to starting his Doctor of Public Health (DrPH) at Johns Hopkins Bloomberg School of Public Health, Rohit worked as a Senior Health Advisor to the Canadian International Development Agency (CIDA) where he worked in areas including tuberculosis, malaria, as well as Canada’s work on the G8 Maternal and Child Health Initiative (Muskoka Initiative). He is currently a member of the Innovation and Financial Gap Working Groups of the United Nations Secretary General’s Global Strategy for Women’s and Children’s Health and Principal at Antara Global Health Advisors. Rohit has been supporting ColaLife since 2009 on a voluntary basis including technical aspects of bid outlines, public health insights and research, trial design, advice on M&E and data collection and data

17
analysis. His expertise and contacts will be invaluable in academic aspects of the project including knowledge translation within the global public health community and helping in terms of advocacy and engaging relevant stakeholders. He will be lead author in the write-up/publication of the trial results. Jane Berry, Voluntary Executive Director, ColaLife Role in project: Value Chain Workpackage management (WP06), learning and knowledge transfer, research, communications and secretariat, fund-raising.
Profile 15 years’ experience as a Project Manager specialising in innovative projects involving analysis of lessons learnt and knowledge transfer. A qualified Business Advisor for Social Business and new micro-business creation. A creative presenter and facilitator, writer, community engagement practitioner and tools designer, with a wide range of experience in capacity building for Third Sector Organisations (NGOs). Track record of successful partnership working with Local Authorities, Government Departments, non-departmental bodies, HE and institutions; NGOs; Social Enterprises and community groups. A researcher able to collate and digest detail quickly; consummate ‘completer-finisher’ with proven ability to plan and deliver to deadline and budget. Highly literate and numerate bid writer, with experience of designing, winning an implementing large multi-partner projects.
UNICEF Zambia
UNICEF will commission and manage the Operational Research and Monitoring & Evaluation (M&E) subcontractor (WP02), ensuring quality, robustness and measurable outcomes. During the design of this trial plan, a close relationship has been established between UNICEF and the ColaLife team, including our research adviser, Rohit Ramchandani, currently undertaking his Doctor of Public Health (DrPH) at Johns Hopkins Bloomberg School of Public Health. Close liaison will continue during the implementation of the M&E elements of the project, including insights into the choice of districts/communities. Rohit will be using the outcomes of this work to contribute to his Doctoral thesis. UNICEF staff and Rohit Ramchandani have had a key role in the design of the project plan presented here, the Project Logic Model and the full Logical Framework, which is under final development. As well as managing WP02, UNICEF will play an active part in the Steering Committee, continue to provide technical support and information to the project throughout. UNICEF is currently facilitating liaison with the Pharmaceutical Regulation Authority, with support from the Ministry of Health (Dr Bonface Fundafunda) to ensure the ADK package fulfils all local requirements as regards contents and labelling.
Organisation Profile UNICEF Zambia’s work areas include: Health, Nutrition, & HIV and AIDS - contributing to child survival through an integrated response to the HIV and AIDS pandemic, improving maternal, newborn and child health, enhancing nutritional status. Education: increasing access for all children to quality basic education. Child Protection: Enhancing protection, care and security, especially for the most vulnerable. Water, Sanitation, and Hygiene, Increasing access to clean water and sanitation. UNICEF Zambia considers the country to offer a superb environment to conduct innovative development work. With a highly supportive Government, vibrant civil society, improving infrastructure, and a nation with a long commitment to peace and democratic principles, Zambia is well-known as an incubator of new ideas and strategies. The UNICEF Programme of Cooperation 2011-2015 with the Government of the Republic of Zambia (GRZ) is designed to address and mitigate the poverty the country’s children face, while responding to the needs with interventions addressing the multiple causative factors. In response to the combination these threats involve the Programme supports national efforts to improve service delivery in the key areas of:
a) child health and nutrition and HIV and AIDS b) quality basic education, c) water, sanitation and hygiene education, d) child protection and social policy, e) advocacy and communication.
Strategies for implementing, monitoring and evaluating the Programme’s component parts are based on a human rights approach and include:

18
• Outreach to the most vulnerable and marginalized children, especially those orphaned and those living in remote rural areas;
• Capacity-building of all stakeholders to understand and fulfill children’s rights; assisting children, young people and communities to participate in and lead their own development;
• Advocacy for child rights within policy development, placing children at the centre of the debate and of all poverty reduction and human development programmes;
• Mainstreaming HIV and AIDS in all aspects of the programmes. Overall, the 2011-2015 Programme seeks to integrate between and among sectors, with a number of cross-cutting components, so that it works harmoniously in a unified way to deliver measurable gains for children. The ColaLIfe Operational Trial Zambia contributes to a) and c) and will contribute to UNICEF’s stated undertakings to work across sectors, to seek innovative approaches, to ensure reach to children in remote and underserved rural areas and seek measurable gains. It will support UNICEF’s programmed aims on handwashing, proposing improvements of 60% in target areas by 2015. Personnel involved in the ColaLife Project implementation and its design include:
• Jesper Moller, M&E Specialist • Lusako Sichali, Planning Officer • Dr Ngawa J Nyongani Ngoma, EPI Officer, Health, Nutrition and HIV and AIDS • Dr Rodgers K Mwale, Child and Maternal Health Specialist
With the support of:
• Dr Charlotte Harland, Chief of Social & Economic Policy, Planning, Monitoring & Evaluation • Dr Nilda Lambo, Chief, Health, Nutrition and HIV and AIDS.
UNICEF Zambia will draw on the range of expertise of its staff to support the ColaLIfe Operational Trial Zambia, as required, and work closely with all partners and the Public Health Advisor Rohit Ramchandani in his capacity as M&E/Trial Design Advisor and M&E Mentor.
SABMiller/Zambian Breweries
SABMiller will not lead any of the workpackages but will contribute in the following areas: • Liaison with ColaLife and the PI Group on ADK packaging and design • Selection of and liaison with wholesalers, and insights into distribution/logistics • The Value Chain workpackage (WP06). SABMiller will contribute, primarily in an advisory capacity, to
the following activities: the assessment of what mothers and care-givers would find attractive in an ADK; the assessment of the willingness to pay for ADKs; the mobile phone elements of the project (authentication and voucher redemption); the establishment of the value chain margins and the training of wholesalers and retailers.
• The Social Marketing workpackage (WP07). Contributions will include cross sector insights on: the design of the social marketing methods; assistance with the production and distribution of social marketing materials.
Organisation Profile SABMiller is an international brewer and one of the world’s largest bottlers of Coca-Cola products. Zambian Breweries is the main bottler for The Coca-Cola Company in Zambia, and is owned by SABMiller. In 2009 it held 64% of the sparkling beverages category in Zambia. Coca-Cola products comprise 73% of this category. In 2009 Zambian Breweries generated revenues of USD 39.9m. It has recently made a significant investment in glass bottles. SABMiller believes that a robust approach to sustainable development underpins both its ability to grow and its license to operate, and that to achieve competitive advantage sustainable development needs to be part of what a company does every day. This strategic focus is underpinned by 10 Sustainable Development Priorities, which include: Encouraging enterprise development in our value chain; Benefiting Communities; Contributing to the reduction of HIV/AIDS and Respecting human rights. Each SABMiller operating business, including Zambian Breweries, reports their progress against these priorities through an online Sustainability Assessment Matrix (see www.sabmiller.com/sam). SABMiller in Zambia has recently

19
taken part in a Poverty Footprint research study exploring the links between business and poverty reduction, with Oxfam America and The Coca-Cola Company.
Medical Stores Limited Zambia
MSL will lead on the assembly of the ADKs including the procurement of the component parts (WP04) and will distribute ADKs to the participating wholesalers at district level (WP05). MSL already stocks UNICEF ORS packets. The other components will be drawn from commodities on the Pharmaceutical Regulatory Authority (PRA) General Sales13 list.
Organisation Profile MSL was established in 1976 as a semi-commercial, limited company under the Companies Act. Its original mandate was to carry out procurement, storage and distribution of all essential drugs for Zambia’s public health sector. In 1996, the responsibility for drug procurement was transferred to the Ministry of Health as part of a general government policy of re-locating public procurement activity into relevant line ministries. MSL’s key functional operational competence since 1996 is warehousing and distribution.
Keepers Zambia Foundation
KZF will lead on the Social Marketing workpackage (WP07), which includes: the production of the IEC materials, with reference to previous examples and good practice; the design of the social marketing methods; the recruitment, training and management of community-based Promoters in target Districts and oversight of media campaigns. KZF promote WASH (Water, Sanitation and Hygiene) programmes and have 15 years’ experience working to support the health and livelihoods of rural communities.
Organisation Profile Keepers Zambia Foundation (KZF) was registered as an NGO in 1996 to respond to poverty in peri-urban and rural households. Its vision is an empowered and economically secure Zambia and it believes in transparency and accountability, sustainability, partnership and equal opportunity. KZF evolved out of the Netherlands government funded Livestock Development Programme implemented in Western Province from the mid-1980s until 1995. Since, its work has expanded from a livestock focus to include work on hygiene and health education, environment and natural resource management, rural enterprise and private sector development, agriculture and food security and social protection. Through its work on Water, Sanitation and Hygiene (WASH), it is developing as the only local expert organisation in Zambia on SODIS (Solar Water Disinfection), supported by the international Swiss Agency, EAWAG. KZF has managed income in the region of 5-6 Billion Kwacha annually. It has forged links with local community-base and non-governmental organisations, international NGOs, the government, donor agencies and the United Nations. The importance of partnerships has been a central theme throughout its work, and partners have included Africare, the Office of the Vice President’s Disaster Management and Mitigation Unit (OVP-DMMU) and the ministries of Health (MoH),Tourism, Environment and Natural Resources (MTENR), Finance and National Planning (MFNP), Community Development and Social Services (MCDSS), Agriculture and Cooperatives (MACO) and Livestock and Fisheries Development (MLFD). European NGO partners have included German Development Service (DED), Self Help Africa (SHA), Village Water, Oxfam GB, the Netherlands Development Organisation (SNV), Concern Worldwide Zambia (CWZ), ActionAid International in Zambia (AAIZ) and CordAid of the Netherlands. It has experience working with stakeholders such as European Commission, the Royal Netherlands embassy, the Danish Association for International Co-operation (DANIDA) and the International Fund for Agricultural development(IFAD).
13 General Sales items are those that can be sold, over the counter, in retail outlets without the supervision of a pharmacist.

20
Appendix 3 Project governance and management
The trial will be overseen and facilitated by the Zambian Ministry of Health, which will also advise on the districts selected for the project, and provide liaison with the Provincial Medical Officers (PMOs) and through these, the District Medical Officers (DMOs) to link the initiative into health clinics and health posts. The Ministry of Health will chair a Project Steering Committee, comprised of implementation partners and others interested in the initiative. ColaLife will provide the secretariat to the Steering Committee. The partnership is in the process of drawing up Memoranda of Understanding (MoUs) to govern the relationships. These are likely to include:
• MoU between ColaLife and SABMiller, Zambia, on project operations • MoU between ColaLife and SABMiller HQ (UK), on communications protocols • Letter of agreement between ColaLife and MoH • MoU between ColaLife and UNICEF Zambia, outlining their fulfillment of the Operational Research
and M&E aspects of the trial • Letter of agreement between ColaLIfe and MSL • A Letter of Agreement between ColaLife and KZF outlining their fulfillment of the Social Marketing
aspects of the trial • Contracts between ColaLife and subcontractors • A contract agreement between ColaLife and the project auditors/Accountable Body
In accordance with usual practice, UNICEF Zambia will issue Project Co-ordination Agreements (PCAs) to those organisations to which it will disperse funds (ie the successful Operational Research and M&E subcontractor). Project management and communications ColaLife (the organisation) will be responsible for overall project management. The project manager will be Simon Berry (see Appendix 2). Project management will involve the planning, organising, securing and managing of the resources to bring about the successful completion of ColaLife Zambia Project in accordance with this project plan. The innovative nature of the ColaLife Zambia Project will mean that the project manager’s role will be very proactive in nature and is likely to involve a certain level of troubleshooting. Progress reporting At quarterly intervals during the project two reports will be produced: the progress report and the financial report. The financial report will be produced by the project auditors and be an output of WP09. The financial report will be produced within one month of the end of the reporting period. Two weeks later the project manager will produce the overall progress report, which will report on progress towards the project’s objectives and relate this to the expenditure to date. Both reports will be confidential documents available to project partners and funders. Subject to the agreement of funders, the project Steering Committee will rule on the elements of the reports that can be made public. The project manager’s office will prepare a Communications Plan, to be circulated to and agreed by partners and presented to the Steering Committee for reference. The Communications Plan will specify:
• protocols and timetables for internal communications • protocols and timetables for external communications • reference to legal matters agreed by the implementing partners (confidentiality, use of IP,
including logos, agreements on assignment of copyright and IP) • reference to editorial guidelines adopted.
Communications and interaction with supporters has been key, and a highly beneficial aspect of ColaLife to date. This will continue into the project implementation phase through the ColaLife blog (http://colalife.org/blog). The project manager will be responsible for reporting progress and issues as the project proceeds according to the agreed online communications guidelines, which will respect agreed confidentiality guidelines. The project manager’s office will be responsible for implementing the Communications Plan, with support and advice from the Steering Committee.

21
Dr Bonface Fundafunda, Drug Supply Budget Line, Ministry of Health has been a key adviser to the project, and we hope this involvement will continue. Dr Fundafunda already works closely with MSL on other initiatives from which the ColaLife Project can learn, for example the work improving the efficiency of supply chains for anti-marlarials (ACTs). Dr Fundafunda is facilitating links with the Ministry of Health’s Directorate of Technical Support Services, currently under Dr Elizabeth Chizema. The project Steering Committee is responsible for providing the Project Manager with the necessary insights and advice for the project to proceed and to help overcome any challenges the trial may face. The Steering Committee will meet quarterly to consider the issues raised by the progress report. The mandate of the project steering committee is to:
• Oversee the execution of the trial • Facilitate the coordination of the work of the project with that of all the known agencies within
Zambia working in related fields • Act as a conduit for the sharing of project findings with relevant agencies • Receive and consider quarterly progress reports collated by the project manager (ColaLIfe) • Review and recommend future action • Advise on the overcoming of challenges the project may face • Provide a mechanism for the resolution of any disputes that may arise within the project
partnership The Project Steering Committee will be made up of named individuals from the represented organisation to maximize continuity and efficacy of the committee. The steering committee members are likely to be:
• Dr E Chizema (DTSS), Ministry of Health (Chair) • Simon Berry, Project Manager, ColaLife (Secretariat) • Dr Nilda Lambo, Chief, Health, Nutrition and HIV and AIDS, UNICEF (M&E Lead) • Mr Andrew Ross, Sales & Distribution Director, Zambian Breweries PLC (SABMiller) • Mr Dirk van Wyk, Managing Director, Medical Stores Ltd • John Msimuko, Executive Director, Keepers Zambia Foundation
In addition, the following people will be invited to join the committee once funding is secured: • Susan Hunter, Chief of Party, STEPS OVC (Adviser and Observer) • Mannasseh Phiri, Chief of Party, SFH (Adviser and Observer) • Walter Proper, Country Director, JSI Inc (Adviser and Observer) • Angela Spilsbury, Human Development Team Leader, DfID (Donor representative – DfID; USAID;
SIDA) • A local representative of the Clinton Foundation (Adviser and Observer) • A local representative of the Gates Foundation (Adviser and Observer)
Through these members, the Health Logistics Steering Committee will also be represented.

22
Appendix 4: Workpackages – detailed descriptions
Workpackage: WP01 Project management and communications Duration 20 months Starts/Ends Month 1 Month 20 Budget for this WP USD 222,302 In kind contributions USD 40,000 Car pledged from Honda Cash USD 182,302 Of which personnel time = USD 137,760 (10%) Lead organisation ColaLife Ltd Also leads on WP03, WP06 Responsible person: Simon Berry Other partners involved All Description Project management The designated Project Manager (PM) is responsible for planning, organising, securing and managing the resources to bring about the successful completion of the project in accordance with the plan and milestones. The innovative nature of the project means the PM’s role will be very proactive in nature and is likely to involve a certain level of troubleshooting. Time-line planning indicates a front- and end-loaded project, ie in the 6-month Phase 1 and 2-month Wind-up and formative evaluation period; this is supported by a full time PM role in this period with 1-2 days a week project support/secretariat. The 12 month operational period will require rolling wave planning (50% PM role with 1+ day a week project support/secretariat). Regular field visits are envisaged, with KZF, MSL and other partners. Progress reporting Each quarter, two reports will be produced: the progress report and the financial report. The financial report will be produced by the Accountable Body as an output of Workpackage 09. The financial report will be produced within one month of the end of the reporting period. Two weeks later the project manager will produce the overall progress report, on progress towards the project’s objectives, related to the expenditure to date. Both reports will be confidential documents available to project partners and funders. Subject to the agreement of funders, the project Steering Committee will rule on the elements of the reports that can be made public. Steering Committee The project Steering Committee meets quarterly to support the Project Manager in the necessary decisions for the project to proceed and to help overcome any problems with advice and insights. The PM’s office will provide the secretariat for the Steering Committee. Communications The project manager’s office will prepare a Communications Plan, to be circulated to and agreed by partners and presented to the Steering Committee for reference. The Communications Plan will lay out:
• protocols and timetables for internal communications • protocols and timetables for external communications • reference to legal matters agreed by the implementing partners (confidentiality, use of IP, including logos,
agreements on assignment of copyright and IP) • reference to editorial guidelines adopted
The PM’s office is responsible for implementing the Communications Plan, with support and advice from the Steering Committee. Open communications and interaction with supporters has been a key, and highly beneficial aspect of ColaLife to date. This will continue into the project implementation phase through the ColaLife blog (http://colalife.org/blog). The PM is responsible for on-going dissemination as the project proceeds according to the agreed online communications protocols, respecting agreed confidentiality guidelines. Learning, Monitoring and Evaluation As this is such a key outcome, the PM is supported by a formative learning and research function for knowledge transfer throughout the project and to produce the Sustainability/Exit plan (approx 1 day a week charged to WP02).

23
Workpackage: WP02 Operational Research, Monitoring and Evaluation Duration 20 months Starts/Ends Month 1 Month 20 Budget for this WP USD 482,948 In kind contributions USD15,000 SABMiller time contribution, included
Not included: - all preparatory work, pre-bid - UNICEF Zambia will host meetings at no charge
Cash USD 467,948 Lead organisation UNICEF Supported by Rohit Ramchandani Responsible person: Jesper Moller Other partners involved All Description Considerable work and expertise has already gone into the design of the trial and the operational research monitoring and evaluation framework. UNICEF Zambia will commission and manage the Operational Research and M&E aspects, through a selected, experienced sub-contractor which offers the best solution and offer, based on Terms of Reference (ToRs) currently being finalized and a competitive bidding process. ToRs are being developed in close liaison with ColaLife and in particular with Rohit Ramchandani. UNICEF Zambia will receive a grant from ColaLife to commission the sub-contractor contract, and will levy on top of this a 7% indirect cost and a 10% Programme Support Cost. UNICEF Zambia will not dedicate specific personnel, but given their now extensive knowledge of the project, this levy will enable UNICEF Zambia to commit Human Resource where it is needed for technical support to the ColaLife team and other partners. This will include:
• Continuing with preparatory work eg on the project design, M&E prior to funding bid confirmation • On-going liaison with Ministry of Health (MoH) and the Pharmaceutical Regulatory Authority (PRA) • Framing the tender and ToRs for the operational research function (with assistance of the Project Manager
and Rohit Ramchandani) • Issuing the tender, receiving proposals and selecting the approved supplier to meet budget and timescales • Issuing and managing contract with the supplier, overseeing timely fulfillment etc • Overseeing the quality aspects of the contractor's work • Receiving the raw data and other commissioned outputs • Passing these to the project manager and Rohit Ramchandani for analysis/further analysis required • Providing technical assistance with M&E matters, health, supply and other technical advice/support • Reviewing and commenting on resulting reports, communications, academic write-up etc • Other support such as dissemination, contacts, networking, access to publications and data, as possible • Attending project and governance meetings and being an active stakeholder in the project • Support in supplying UNICEF ORS sachets for the ADK packs (likely to be in-kind subject to final approvals)
Learning, Monitoring and Evaluation There is an allowance for each partner to dedicate time to this key activity, to pool cross sector expertise, which will be supported by technical staff at UNICEF and the project’s principle academic mentor Rohit Ramchandani.

24
Workpackage: WP03 ADK Package design, test and manufacture Duration 06 months Starts/Ends Month 0 Month 06 Budget for this WP USD 61,225 Includes all import duties and optional tool-up
USD 15,000 to subcontractor USD 30,000 for packaging manufacture
In kind contributions All preparatory work and advice, pre-bid Cash USD 61,225 Managed by subcontract via ColaLife Lead organisation PI Global Managed by ColaLife Responsible person: Chris Griffin Other partners involved ColaLife, SABMiller Description PI Global will report to and through ColaLife on this workpackage, which consists of three principle activities: 1. ADK design 2. ADK testing 3. ADK manufacture The starting point has been the functional specification of the ADK packaging, provided by ColaLife. PI Global is already considering this specification and will produce a selection of design options that fulfill it for consideration. This work has begun in the pre-funding stage on a pro-bono basis. Feedback from ColaLife and other partners will be provided within one calendar month of designs being put forward. PI Global will modify the design according to feedback and produce a prototype and specify a testing process and engage other partners as necessary in the implementation of the tests of the prototype. Any modifications to the prototype that are required as a result of the testing will be undertaken by PI Global before PI Global specify the manufacturing process and oversee this process. 10,000 ADK packages will be required. The costs for this workpackage include the estimated manufacturing costs. Learning, Monitoring and Evaluation Phase 1 (the first 6 months) incorporates close liaison between PI Global and the PM to test, feedback and summarise learning on the packaging and the design process, making adjustments if reuqired. This will be captured for knowledge transfer.

25
Workpackage: WP04 ADK Assembly Duration 16 months Starts/Ends Month 1 Month 16 Budget for this WP USD 17,852 Of which personnel costs to pack USD 2,352 In kind contributions Not quantified All preparatory work and advice, pre-bid
Donated ORS sachets expected via UNICEF (TBA) Other contents may be donated in kind (subject to agreement)
Cash USD 17,852 Includes est cost of ADK Contents USD 15,500 Lead organisation MSL Responsible person: Chipopa Kazuma Other partners involved ColaLife, UNICEF Description MSL will provide resources to enable the consolidation of the components into the Colalife ADK Kit, Storage capacity for the components and the kits and, under WP05, delivery of compiled kits to the relevant distribution outlets in the trial areas. Workpackage 04 consists of three activities:
1. Procurement of ADK components 2. Design and testing of the packing process 3. Assembly of the ADKs and packing into cartons
Procurement and assembly of ADK components The procurement of the components of the ADKs will take place in two phases. The first procurement (Month 01) will be small scale and provide sufficient material to assemble ADKs for the Phase 1 (Stage 1) focus group work with mothers/care-givers. The focus group work may result in modifications to the ADK contents. In Month 04 the major procurement will be undertaken for the ADKs to be used in Phase 2 of the trial. Assembly/consolidation of Kit MSL will receive component parts of the kits from relevant suppliers, store them and consolidate the components into the kits. These will be packed into cartons for onward distribution to the relevant district wholesaler. We are currently assuming around 5 or 6 products are to be consolidated. The key variable is the time it will take to consolidate the products into the ADK box. At present we estimate this to be 3 minutes per ADK. Assumptions include that the AidPods/ADKs are pre branded (no labeling required) and there is no testing of products required (ie they are pre approved). Packing costs are based on our usual hourly rates. (Kwacha 18,375 (approx USD 3.75) We assume 50 man hours per 1,000 ADKs. Full calculations are in the financials spreadsheet. Design and testing of the packing process The packaging to be used will be the output of Workpackage 03. MSL will liaise with PI Global (and/or its subcontractors) to ensure that the ADK packaging produced is compatible. MSL envisage a simple packing process, by hand at a packing table. Storage Charges MSL will be required to store both the components of the kits and the completed kits for a period of time to prior to their onward distribution to the wholesalers. MSL has an existing model for such charging (see spreadsheet) Note: the estimated costs of the ADK components are included in the budget for this workpackage. Learning, Monitoring and Evaluation One day a month in WP05, also lead by MSL, is dedicated to overall management of both WP04 an 05, for monitoring, learning and reporting back, throughout the duration of the project. This is allocated to the total budget for WP02.

26
Workpackage: WP05 ADK Distribution Duration 14 months Starts/Ends Month 4 Month 20 Budget for this WP USD 16,495 Includes all oversight/learning/meetings In kind contributions Not quantified All preparatory work and advice, pre-bid Cash USD 16,495 Managed by MSL Lead organisation MSL Responsible person: Chipopa Kazuma Other partners involved SABMiller, KZF, ColaLife Description This workpackage consists of two activities:
1. Distribution to District/Wholesaler level (MSL) 2. Promotional activities aimed at wholesalers (SABMiller)
There will be a pilot delivery via one wholesaler during months 4-6, as a learning activity. Distribution to District/Wholesaler level As well as overseeing this whole workpackage, MSL distribute packed ADKs in cartons to the wholesalers participating in the project. Distribution to wholesalers will take place during MSL’s usual scheduled runs, selected to best fit the needs of the operational trial. Delivery Charges MSL has an existing model for charging as follows: Pallet USD 114 Carton USD 5.19 We are working on estimated 75 ADKs packed into one carton; this would require 130-140 cartons. Given the relatively small volume, it is not yet clear whether the deliveries required will be 2 one-off bulk deliveries (one to each of the district wholesalers) or staged deliveries. Budgets are therefore based on the carton rate, allowing for 135 cartons, which will allow cartons to be included in MSL’s regular scheduled runs as required. Promotional activities aimed at wholesalers SABMiller will lead this element of the workpackage. They will lead on the selection of wholesalers serving the trial communities and will encourage and facilitate their participation in the project through their existing contact with the wholesalers. (Note: SABMiller will also assist in the training of wholesalers and retailers through their contribution to Workpackage 06). Learning, Monitoring and Evaluation One day a month in WP05 is dedicated to overall management of both WP04 and 05, for monitoring, learning and reporting back, throughout the duration of the project. This is allocated to the total budget for WP02.

27
Workpackage: WP06 Value Chain Duration 18 months Starts/Ends Month 01 Month 20 Budget for this WP USD 114,420 Includes Fees to subcontractors: USD 55,000 In kind contributions USD 32,000 Provided by SABMiller: advice, hosting Cash USD 82,420 Managed by ColaLife Lead organisation ColaLife Responsible person: Jane Berry Other partners involved SABMiller, KZF, UNICEF Description Assess what mothers would find attractive in an ADK and their ability to pay This workpackage will start with an assessment in the target communities of what mothers and care-givers would find attractive in an Anti-Diarrhoea Kit (ADK) and their willingness and ability to pay. This research will be undertaken by the Operational Research and M&E sub-contractor selected by UNICEF to deliver WP02 and will form part of their ToR. Voucher system/tracking A voucher system will be used in the pilot to help ensure a demand for the ADKs until they, and their value, are/is fully understood by mothers and care-givers in the target communities. The system will be designed and implemented by a sub-contractor, likely to be Mobile Transactions (MTZL), managed by the ColaLife Project Manager. The tracking system will be set up in Stage 1 (months 1-3) and tested in Stage 2 (months 4-6), and will be ready to implement by month 07, the first month of Stage 3/Phase 2. It will then run for 12 months. Establish supply chain margins and distribution costs This work will be undertaken in months 1-3 of the project and will be used to verify assumptions and finalise the price points of the ADK along the distribution chain. It will be reviewed periodically as learning emerges. SABMiller as the commercial partner in this workpackage will play a key advisory role in this activity. Training of wholesalers and retailers (inc on the benefits of the ADKs) ADKs will be distributed to selected wholesalers by MSL as part of Workpackage 05. These wholesalers and all parties involved in the supply chain down to and including the retailers in target communities will need to understand the benefits of the ADK so that they can effectively sell the ADK to the next agent in the supply chain. Retailers will need to know the benefits so that they can sell the ADKs to mothers and care-givers in the target communities. ColaLIfe will be responsible for selecting a suitable trainer for village retailers (by month 3-4) based on the language and travel requirements stemming from the districts selected. Design and testing of the training methods and materials will be overseen by ColaLIfe, with advice from KZF, who have experience in local rural micro-enterprise projects, and from SABMiller (who will also liaise directly with wholesalers). Learning, Monitoring and Evaluation This Workpackage is managed by ColaLife; the learning, monitoring and evaluation function for WP06 is amalgamated with WP01. It is allocated to the total budget for WP02.

28
Workpackage: WP07 Social Marketing Duration 20 months Starts/Ends Month 01 Month 20 Budget for this WP USD 342,375 In kind contributions USD 7,000 SABMiller to cover printing costs
Plus SABMiller advice to be given in-kind Cash USD 335,375 KZF budget line is USD 317,375 for this activity
of which personnel costs are USD 136,875 Lead organisation Keepers Zambia Foundation Responsible person: John Msimuko Other partners involved ColaLife, SABMiller Description This workpackage is crucial to the success of the project as it will lay the groundwork and support the ongoing community involvement and engagement required, with the language skills, cultural insights and on-the-ground presence that will follow from selecting and training in-community promoters. Work begins Months 1- 3 (Phase 1, Stage 1) to identify existing IEC materials, review and adapt them; liaise with project partners, wider partners, District officials (supported by MoH) and communities; recruit 2 project officers and facilitators – one for each district and arrange for staff induction. KZF will establish relationships with media/radio stations and identify issues around which programmes can be made. Support will be available for the focus group work on what mothers find attractive, carried out by the M&E subcontractor to UNICEF, and for the retailer training work, based on KZF’s experience in micro-business support. District offices will be established and equipped at this time, and office and accounting procedures put in place with familiarization for all internal staff. Key events for Phase 1 Stage 2 (Months 4-6) include:
- Meeting stakeholders in each district, including engaging with traditional leaders - Running stakeholder meetings and inception workshops (with other partners) - Designing a workplan and materials for community based promoters (posters, meeting and visit formats etc) - Drawing up criteria for recruiting the promoters and selecting them via community meetings - An induction programme for promoters will be followed by on-the-job training/observation and training in
technical issues - The promotional campaigns will begin towards the end of this phase
All promoters will be drawn from the selected communities where the project takes place and will be equipped and incentivized with a bicycle and a T shirt as well as promotional materials, sample AidPods and a number of ADK vouchers for direct distribution. Event costs and subsistence payments for attending is allowed for in the budget. During the 12 month operational phase promotion will continue in person, through community events and drama, household visits, and interaction with retailers on the ground, feeding back any issues arising to the partners and facilitating field visits for learning. We envisage the use of digital cameras to capture learning. There will be strict project accounting and monitoring according to our usual procedures for this level of project. Implementation staff will consist of: Current Executive Director oversight at 20% Senior Programme Manager at 30% Programme Manager, based in Lusaka 80% on the project Project officers one in each district at 100% Field Facilitators one in each district at 100% The Project Accountant based at head office at 50% Finance and Administration Manager at 30% Head office driver at 60%

29
Workpackage: WP08 Governance Duration 20 months Starts/Ends Month 1 Month 20 Budget for this WP USD 9,940 Covering partners’ time in attending In kind contributions USD 3,500 SABMiller time given in kind.
All preparatory work/advice, pre-bid. All MoH time inc chairing meetings/ field officer liaison
Cash USD 6,440 The MoH will not receive or disperse funds. SABMiller contribution of time in kind. The meetings budget will be managed by ColaLife.
Lead organisation Ministry of Health Responsible person: Dr Bonface Fundafunda Other partners involved All Description This workpackage will include advice and guidance, oversight of the project, convening and chairing the Steering Committee, advice and liaison at Ministry level and with District Medical Officers in selected trial districts. Steering Committee meetings will be quarterly, with a Kick Off meeting at the outset and Project Closure meeting at the end. The role of the Steering Committee is to • oversee the execution of the operational trial • receive and consider quarterly progress reports collated by the project manager (ColaLife) • review and consider the issues raised by progress reports • provide insights and advice • advise on overcoming challenges the project may face • facilitate coordination of the project with that of known agencies within Zambia working in related fields • act as a conduit for the sharing of project findings with relevant agencies • review and recommend future action, including reviewing proposed Exit/Sustainability plans • provide a mechanism for the resolution of any disputes that may arise within the project partnership •

30
Workpackage: WP09 Accountable Body/Provision of financial auditing Duration 20 months Starts/Ends Month 01 Month 20 Budget for this WP USD 50,000 In kind contributions None expected Cash USD 50,000 Lead organisation TBA Responsible person: TBA Other partners involved All Description This workpackage will support the operational accounting function at project level and provide the accountable body and audit function required by funders. These details will be finalized in liaison with the project funders to meet their requirements for accountability, disbursement of funds against milestones and auditing. At present the following is envisaged: • The project manager will report on progress against milestones and authorize payments to partners • A financial report will be produced quarterly by the Project Accountant/Accountable Body within one month of
the end of each reporting period, detailing funds dispersed to each partner and funds due. • Each partner will provide its own accounting function, with reports for inspection available to the Project
Accountant/ Accountable Body •

31
Appendix 5: Finances - the full detail behind this summary is available on request.

32