Clinical examination of abdomen medicine
41
ABDOMINAL EXAMINATION Roha shad Ram negi
-
Upload
ram-negi -
Category
Health & Medicine
-
view
963 -
download
4
Transcript of Clinical examination of abdomen medicine
ABDOMINAL
EXAMINATION
Roha shad
Ram negi
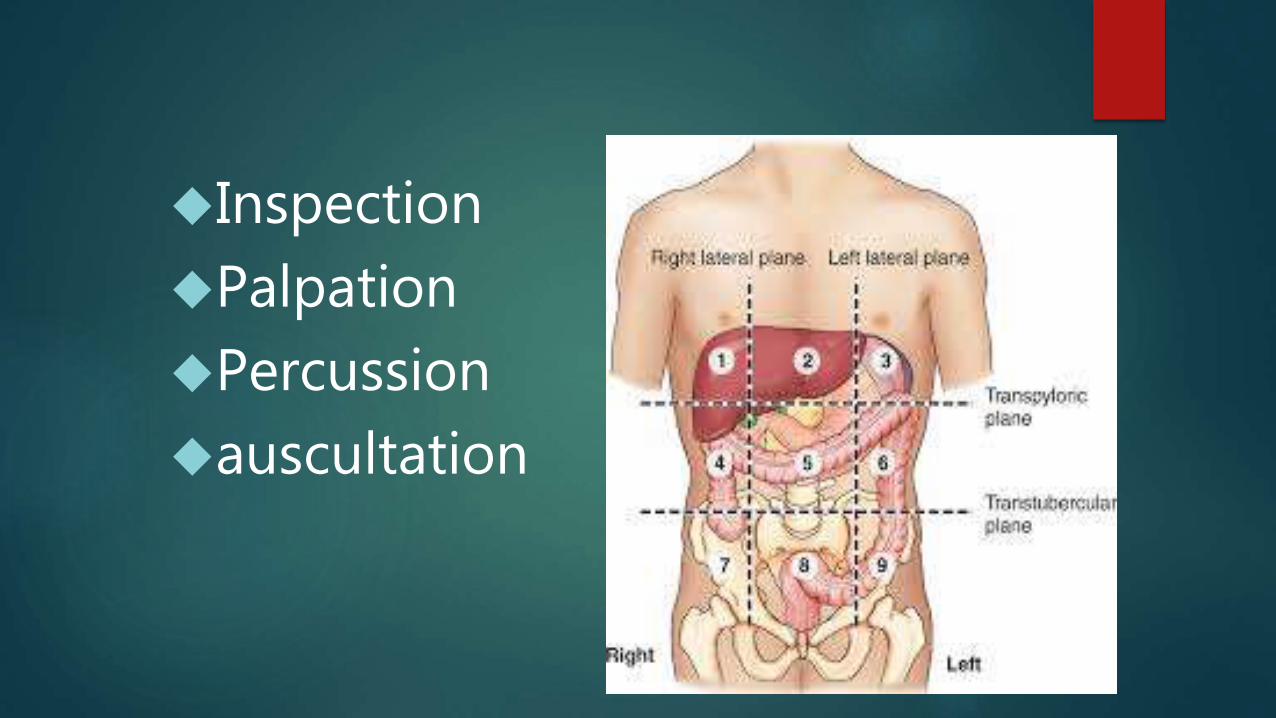
Inspection
Palpation
Percussion
auscultation
INSPECTION
Examine under good light and warm surroundings.
Supine position.
Head supported by pillow.
Expose abdomen from xiphisternum to pubic symphysis.

INSPECTION
Shape
Movements of abdominal wall
Umbilicus
Skin and surface of abdomen
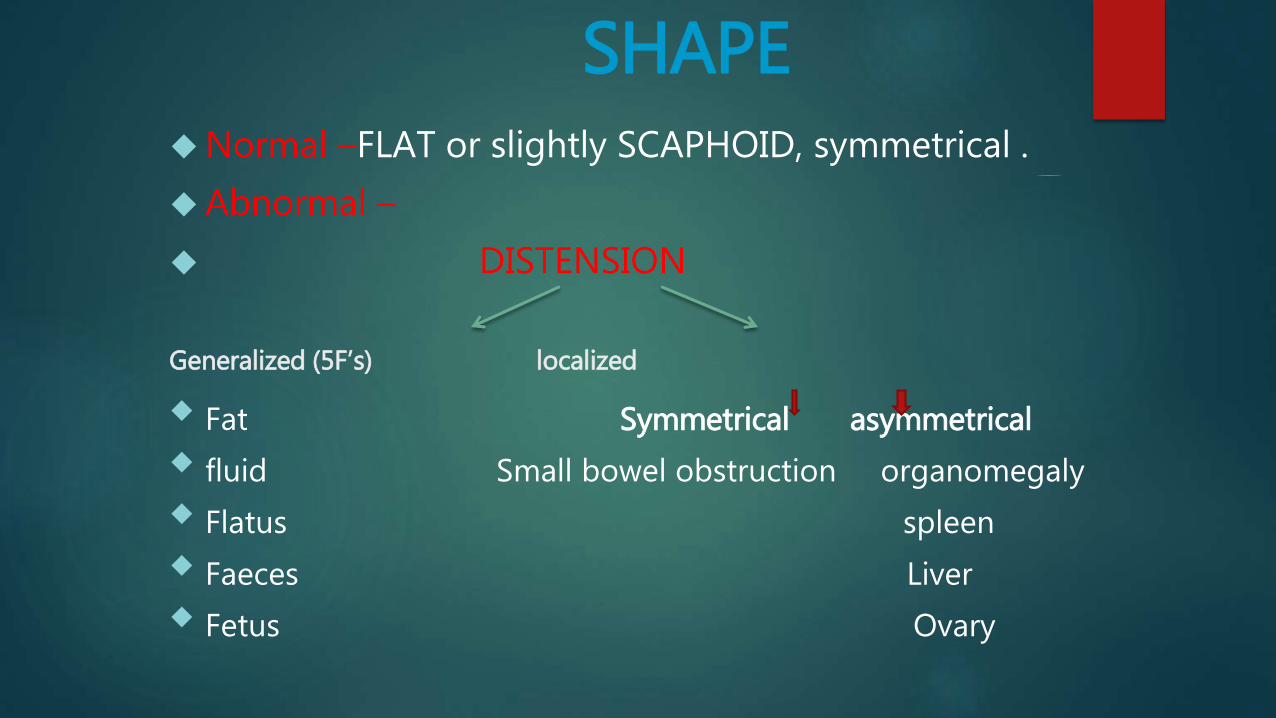
SHAPENormal –FLAT or slightly SCAPHOID, symmetrical .
Abnormal –
DISTENSION
Generalized (5F’s) localized
Fat Symmetrical asymmetrical
fluid Small bowel obstruction organomegaly
Flatus spleen
Faeces Liver
Fetus Ovary

umbilicus Normal- midline at the level of disc between L3, L4 vertebrae.
Shape-retracted and inverted.
Abnormal-
Obese-sunken
Ascitis - flat and everted
MovementsNormal= rise on inspiration and fall
on expiration
Free and equal on both sides
Abnormal=
Absent/diminished- generalized peritonitis(still/silent abdomen)

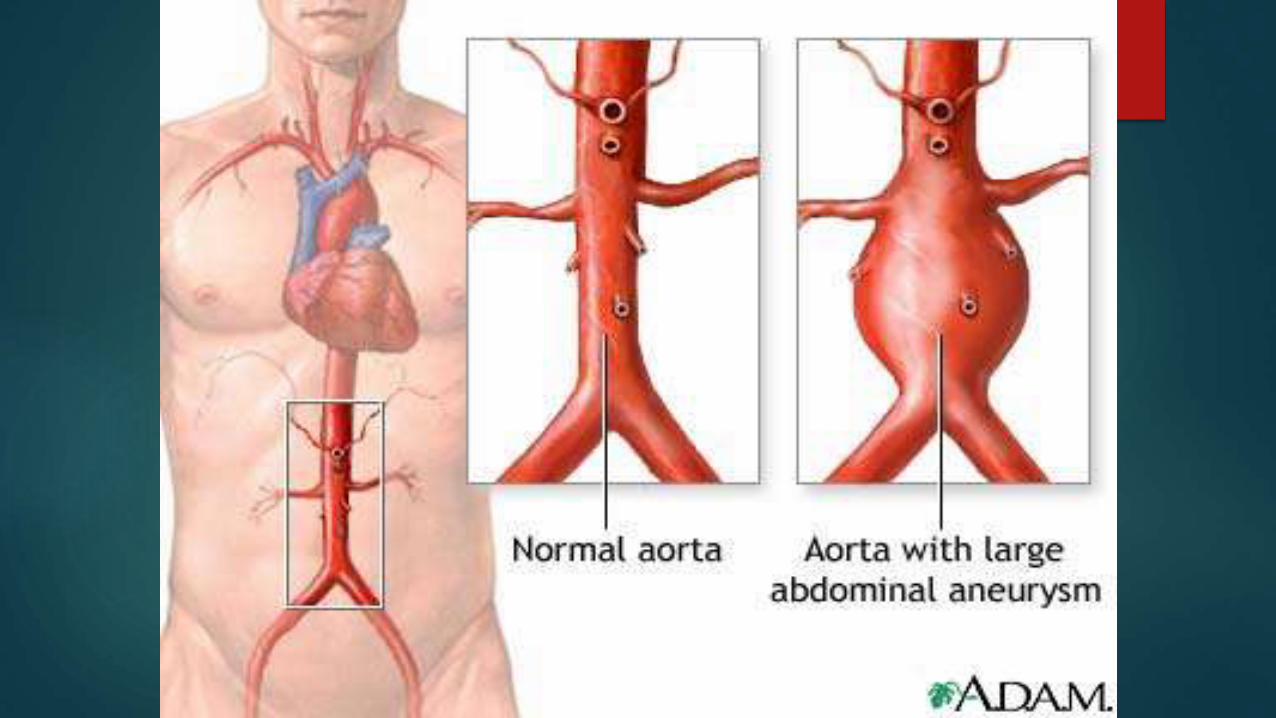
Visible pulsation of abdominal aorta Noticed in epigastrium
Nervous and thin patients
Aneurysm of abdominal aorta
Visible peristalsis-
Obstruction at pylorus
Obstruction in small or large bowel
Normal in elderly - lax abdominal muscles.
Skin and surface
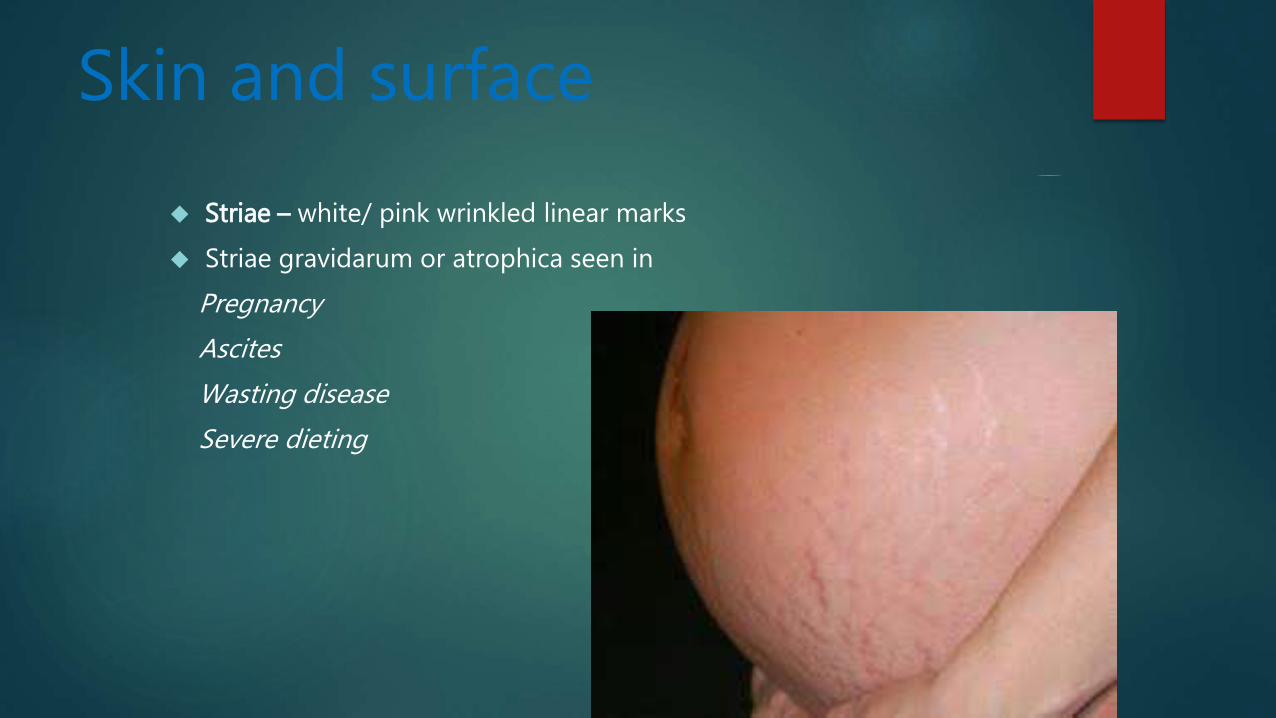
Striae – white/ pink wrinkled linear marks
Striae gravidarum or atrophica seen in
Pregnancy
Ascites
Wasting disease
Severe dieting

scar
red and pink- recent White –old scars

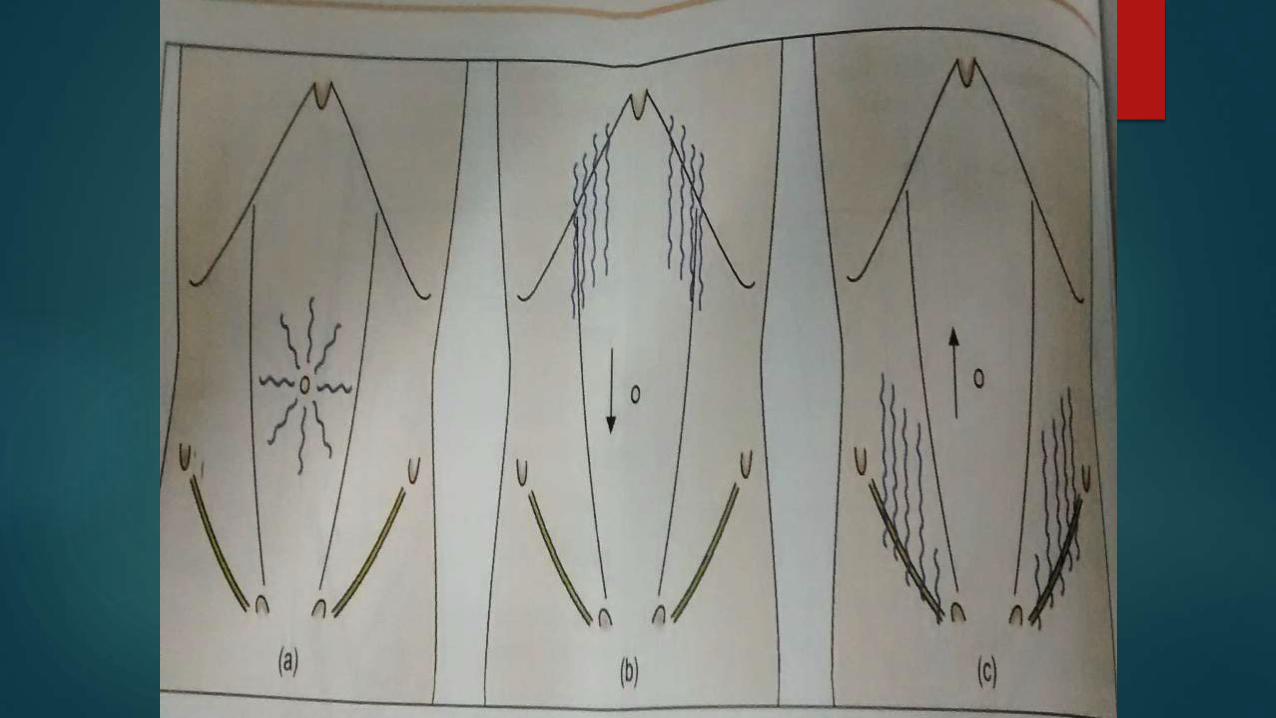
Superficial veinsObstruction of
SVC IVC portal vein
Superficial abdominal veins are dilated- to provide collateral circulation.
These veins represent opening up of anastomosis between portal and systemic veins.

Ascitic abdomen
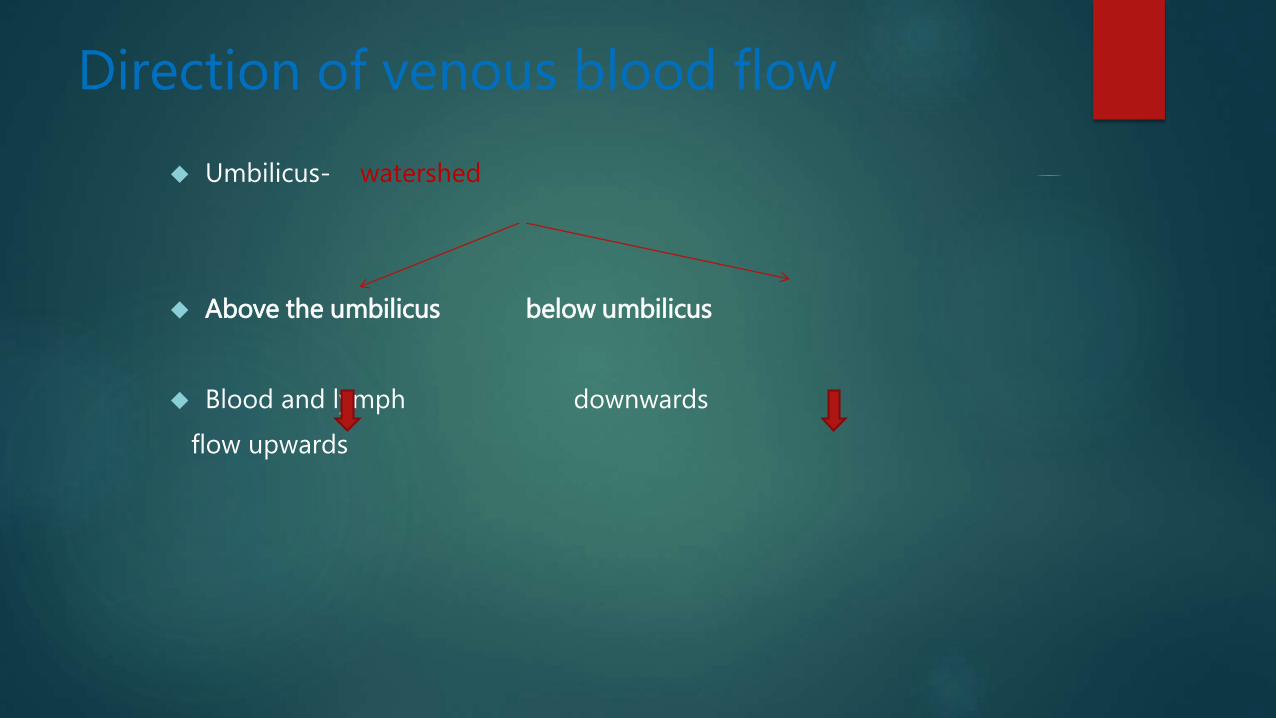
Direction of venous blood flow
Umbilicus- watershed
Above the umbilicus below umbilicus
Blood and lymph downwards
flow upwards

Pigmentation Linea nigra
Erythema ab igne – brown mottled pigmentation
Seborrhoeic warts-pink, brown, or black
haemangiomas-campbell de morgan spots
Campbell de
Morgan spots
ABDOMINAL EXAMINATION
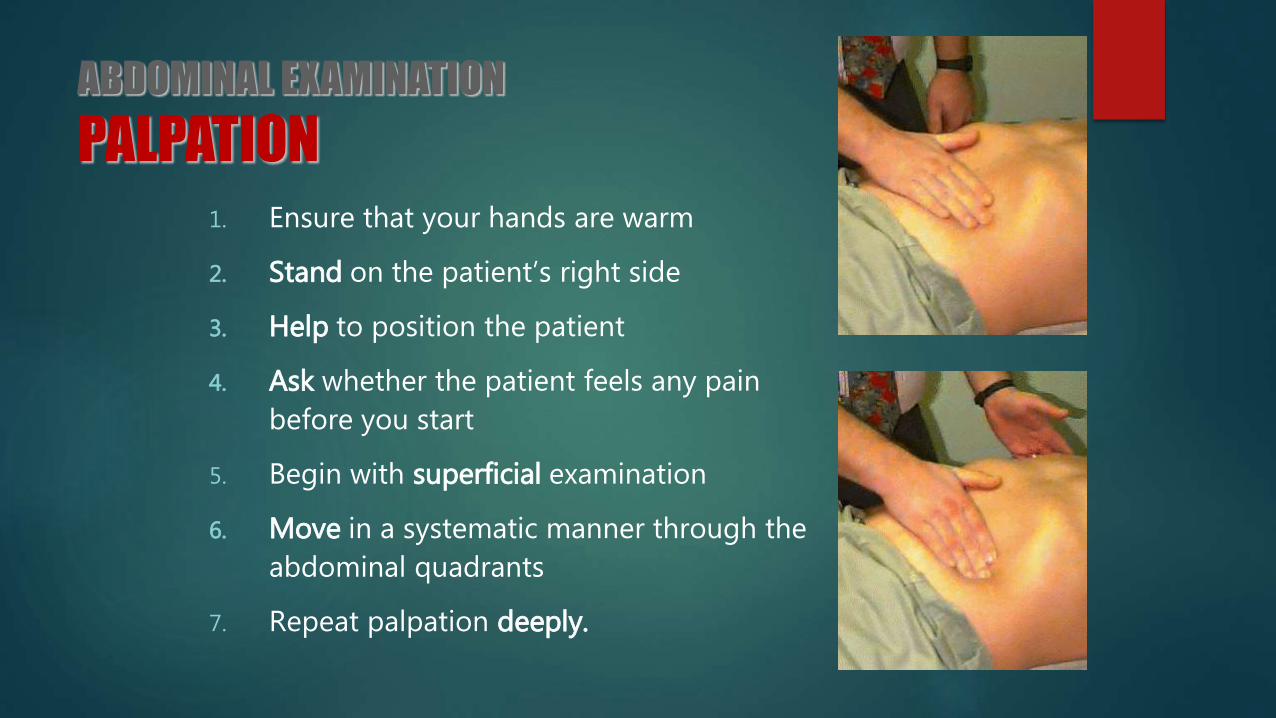
PALPATION1. Ensure that your hands are warm
2. Stand on the patient’s right side
3. Help to position the patient
4. Ask whether the patient feels any pain
before you start
5. Begin with superficial examination
6. Move in a systematic manner through the
abdominal quadrants
7. Repeat palpation deeply.

PALPATION Tenderness: discomfort and resistance to palpation. Note
for it’s site.
Voluntary guarding- voluntary contraction due to pain provoked by palpation.
Involuntary guarding: reflex contraction of the abdominal muscles(board like rigidity seen in parietal peritonitis)
Rebound tenderness: patient feels pain when the hand is released
Tenderness + rigidity: perforated viscus
Palpable mass (enlarged organ, faeces, tumour)
Palpation of liver
Place both the hands flat on abdomen in the right sub costal region.
Ask the patient to breath deeply.
Edge of liver is felt moving downwards.
Hepatomegaly is measured in cms below right costal margin.

Surface-Smooth, soft and tender-RHFFirm and regular-OBSTRUCTIVE JAUNDICEHard, irregular painless-ADVANCED SECONDARY CA
Gall bladder Normal gall bladder can not be felt.
Distended- palpated as firm smooth globular swelling, distinct borders lateral to rectus abdominus near the tip of 9th intercostal margin.
Painless gallbladder- Jaundice in patient with Ca head pancreas or CBD obstruction due to
malignancy.
Mucocele.
Carcinoma gall bladder.

Pain in RUQ
Inflammation of gallbladder
(cholecystitis)
Courvoisier's law states that in the presence of an
enlarged gall bladder which is nontender and accompanied with jaundice, the cause is unlikely to be gallstones.
MURPHY’S SIGN
Palpation of spleen
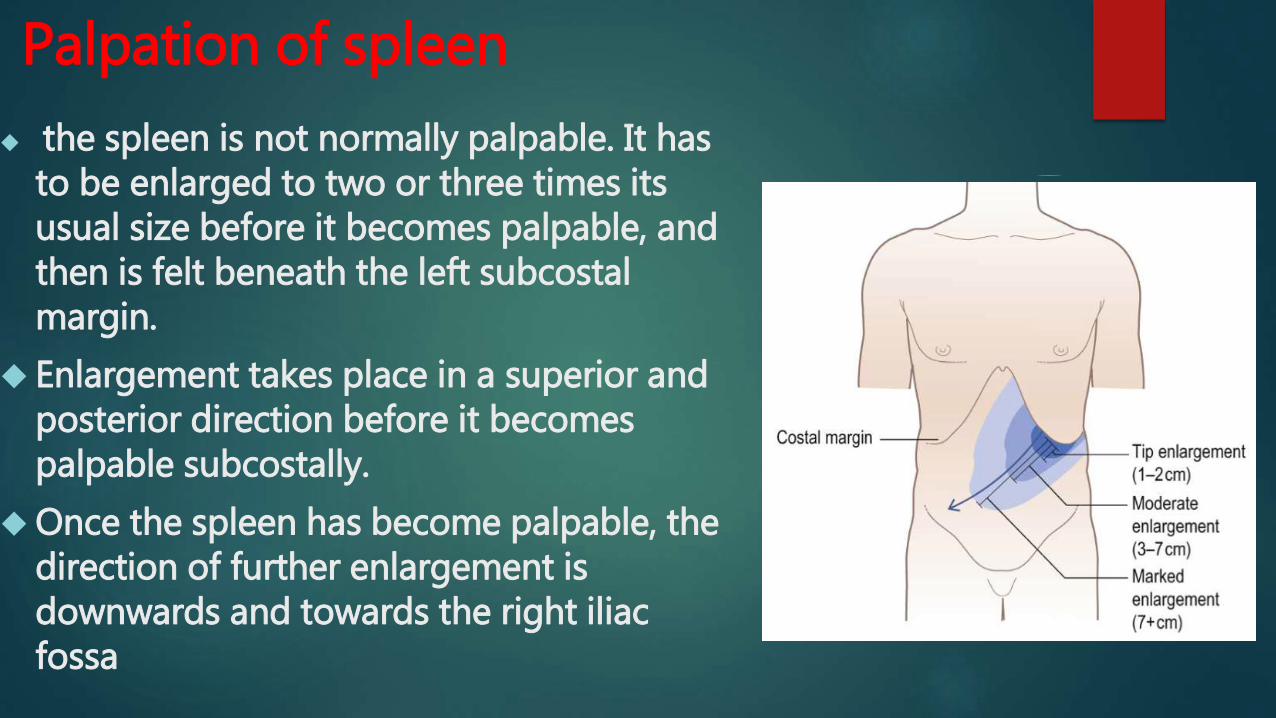
the spleen is not normally palpable. It has to be enlarged to two or three times its usual size before it becomes palpable, and then is felt beneath the left subcostal margin.
Enlargement takes place in a superior and posterior direction before it becomes palpable subcostally.
Once the spleen has become palpable, the direction of further enlargement is downwards and towards the right iliac fossa

Start from the umbilicus. Keep your hand stationary and ask the patient to breathe in deeply through the mouth. Feel for the splenic edge as it descends on inspiration (Fig.A)
Move your hand diagonally upwards towards the left hypochondrium 1 cm at a time between each breath the patient takes.
Feel the costal margin along its length, as the position of the spleen tip is variable.

If you cannot feel the splenic edge, ask the patient to roll towards you and on to his right side; repeat the above. Palpate with your right hand, placing your left hand behind the patient's left lower ribs, pulling the ribcage forward (Fig. B).
Feel along the left costal margin and percuss over the lateral chest wall to confirm or exclude the presence of splenic dullness
Palpation of kidney
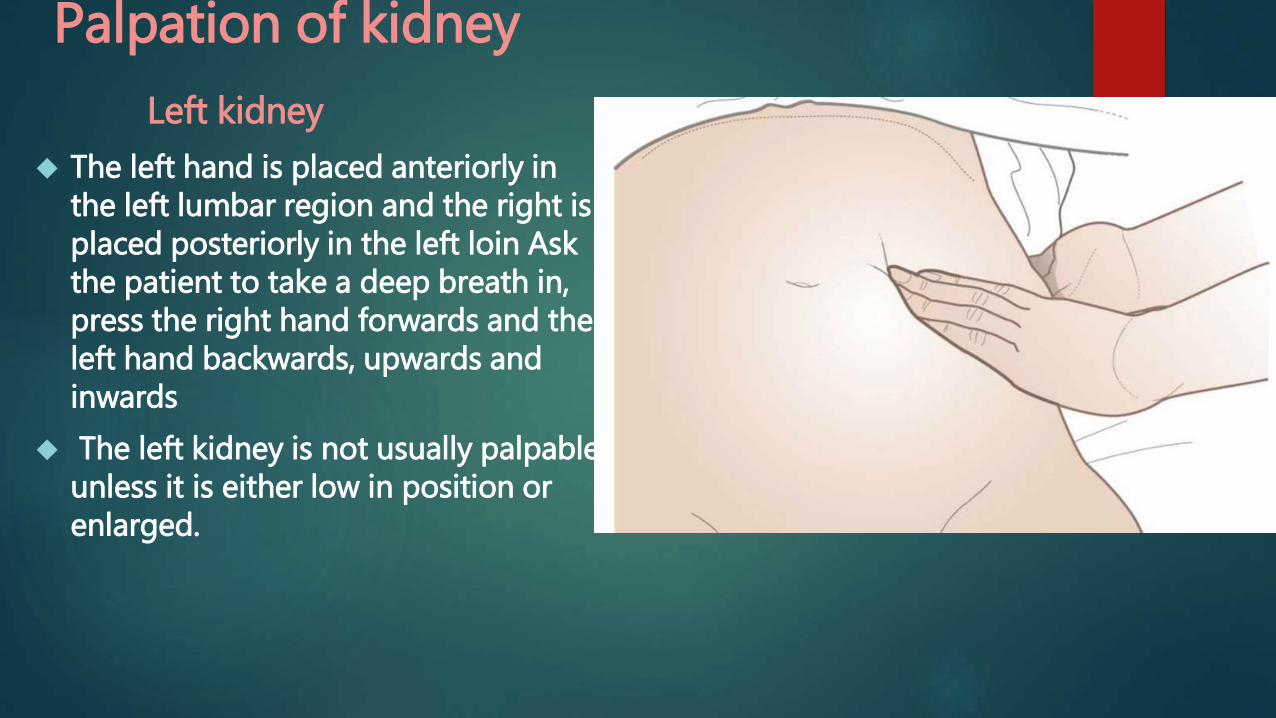
Left kidney
The left hand is placed anteriorly in the left lumbar region and the right is placed posteriorly in the left loin Ask the patient to take a deep breath in, press the right hand forwards and the left hand backwards, upwards and inwards
The left kidney is not usually palpable unless it is either low in position or enlarged.
Right kidney
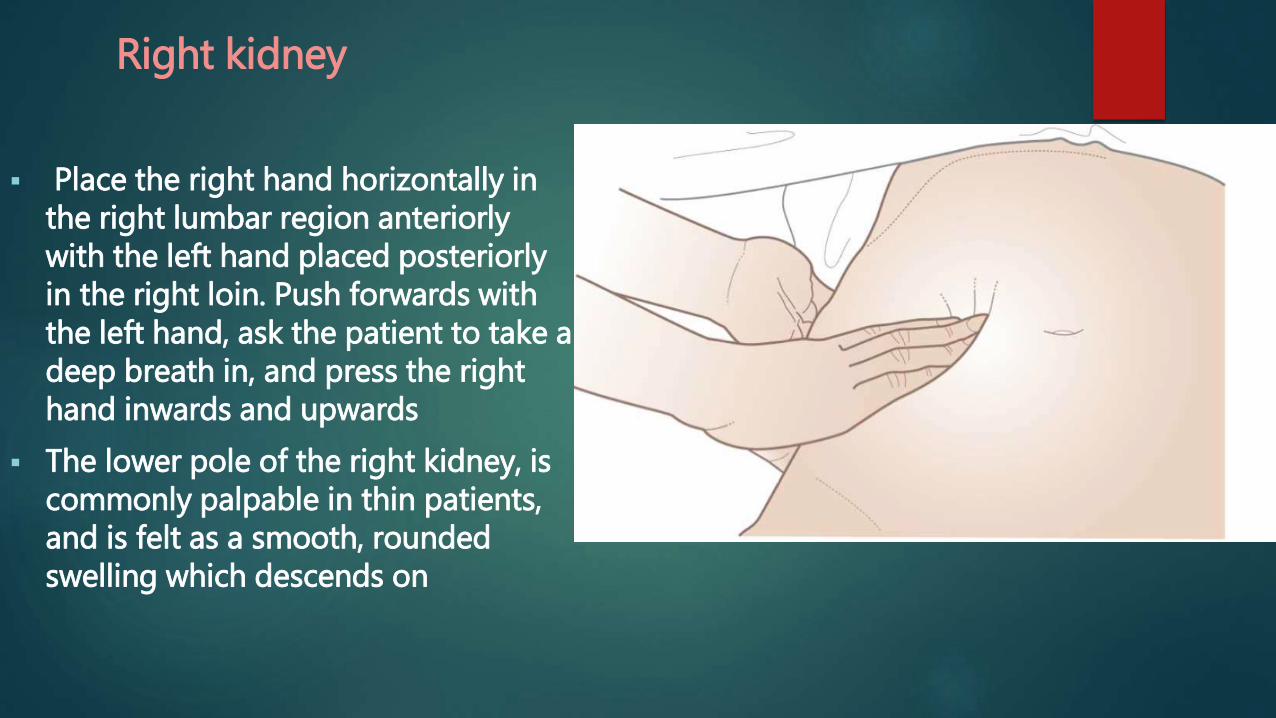
Place the right hand horizontally in the right lumbar region anteriorly with the left hand placed posteriorly in the right loin. Push forwards with the left hand, ask the patient to take a deep breath in, and press the right hand inwards and upwards
The lower pole of the right kidney, is commonly palpable in thin patients, and is felt as a smooth, rounded swelling which descends on
THE URINARY BLADDER
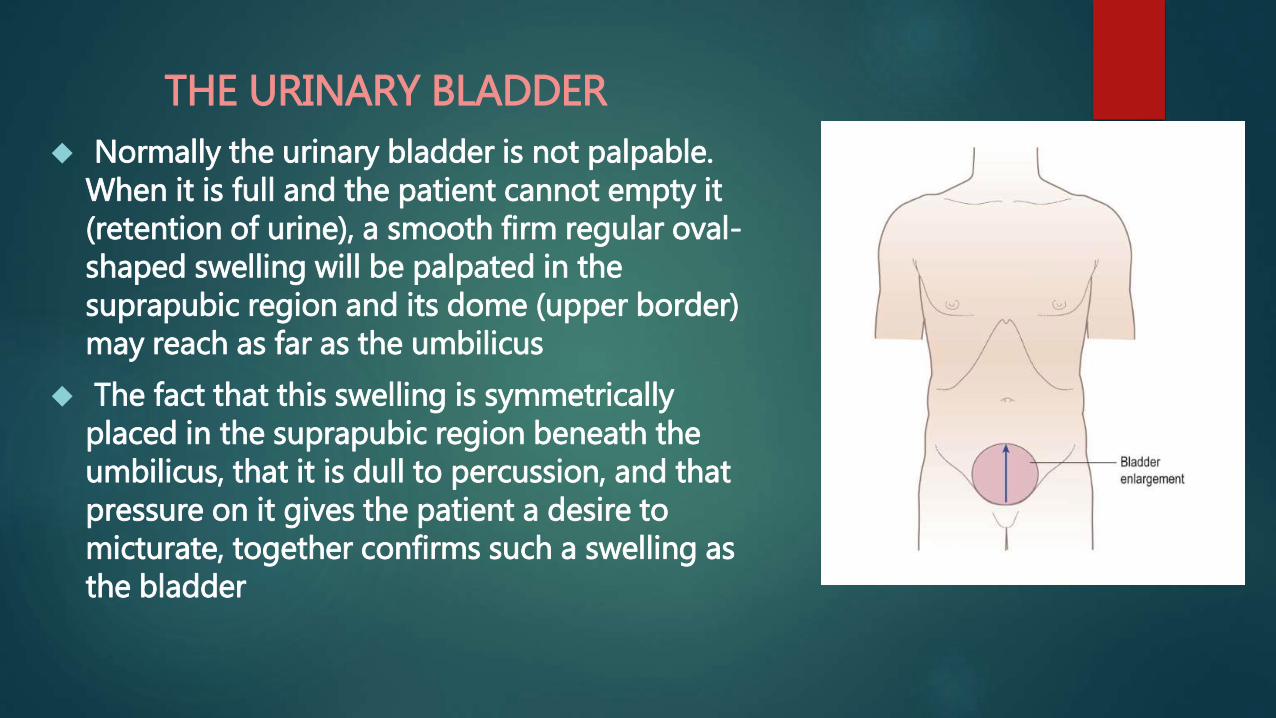
Normally the urinary bladder is not palpable. When it is full and the patient cannot empty it (retention of urine), a smooth firm regular oval-shaped swelling will be palpated in the suprapubic region and its dome (upper border) may reach as far as the umbilicus
The fact that this swelling is symmetrically placed in the suprapubic region beneath the umbilicus, that it is dull to percussion, and that pressure on it gives the patient a desire to micturate, together confirms such a swelling as the bladder

Palpation of abdominal aorta
In most adults the aorta is not readily felt, but with practice it can usually be detected by deep palpation a little above and to the left of the umbilicus.
the fingertips are used as a means of palpation
Press the extended fingers of both hands, held side by side, deeply into the abdominal wall in the position shown.
Remove both hands and repeat the manoeuvre a few centimetres to the right. In this way the pulsation and width of the aorta can be estimated

COMMON FEMORAL VESSELS
• The common femoral vessels are found just below the inguinal ligament at the midpoint between the anterior superior iliac spine and the symphysis pubis
• Place the pulps of the right index, middle and ring fingers over this site in the right groin and palpate the wall of the vessel

PERCUSSION
The normal percussion note over most of the abdomen is resonant (tympanic) except over the liver, where the note is dull.
A normal spleen is not large enough to render the percussion note dull

DEFINING THE BOUNDARIES OF ABDOMINAL ORGANS AND MASSES
Liver
Start anteriorly, at the fourth intercostal space, where the note
will be resonant over the lungs, and work vertically downwards.
Over a normal liver, percussion will detect the upper border at about the fifth intercostal space (just below the right nipple in men). The dullness extends down to the lower border at or just below the right subcostal margin, giving a normal liver vertical height of 12-15cm
Spleen
Dullness extends from the left lower ribs into the left hypochondrium and left
lumbar region.
Urinary bladder
The dullness on percussion, and clear difference from the adjacent bowel, provides
reassurance that the swelling is cystic or solid and not gaseous.
Other masses
The boundaries of any localized swelling in the abdominal cavity, or in the walls of the abdomen, can sometimes be defined more accurately by percussion than palpation, as for the urinary bladder.

DETECTION OF ASCITES AND ITS DIFFERENTIATION FROM OVARIAN CYST AND INTESTINAL OBSTRUCTION
Shifting dullness (ascites) Examination sequence
With the patient supine, percuss from the midline out to the flanks (Fig. Note any change from resonant to dull, along with the areasof dullness and resonance.
Keep your finger on the site of dullness in the flank and ask the patient to turn on to his opposite side. Pause for at least 10 seconds to allow any ascites to gravitate, then percuss again. If the area of dullness is now resonant, shifting dullness is present, indicating ascites
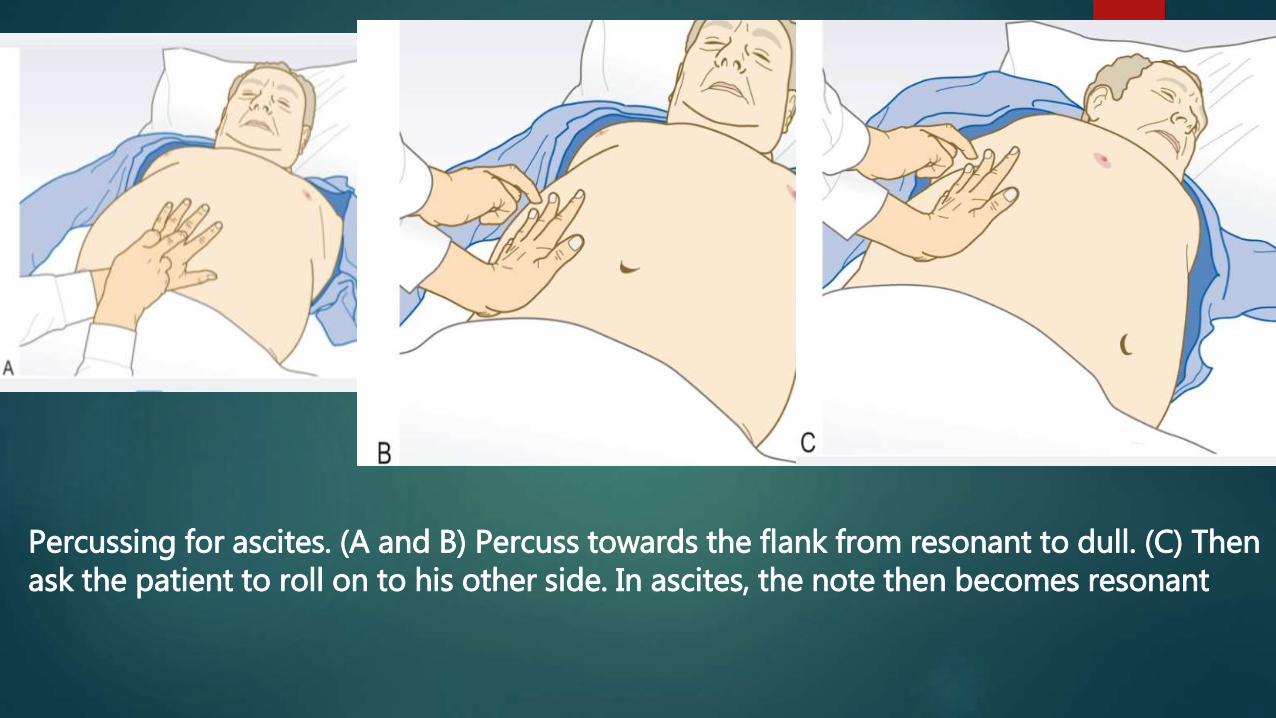
Percussing for ascites. (A and B) Percuss towards the flank from resonant to dull. (C) Then ask the patient to roll on to his other side. In ascites, the note then becomes resonant

Fluid thrill
Place the palm of your left hand flat against the left side of the abdomen and flick a finger of your right hand against the right side of the abdomen.
If you feel a ripple against your left hand, ask an assistant to place the edge of their hand on the midline of the abdomen. This prevents transmission of the impulse via the skin rather than through the ascites. If you still feel a ripple against your left hand, a fluid thrill is present (only detected in gross ascites).
Clinical features of marked abdominal swelling
Gross ascites
Dull in flanks Umbilicus everted and/or hernia present Shifting dullness positive Fluid thrill positive
Large ovarian cyst
Resonant in flank Umbilicus, vertical and drawn up Large swelling felt arising out of pelvis which one cannot 'get below'
Intestinal obstruction
Resonant throughout Colicky pain Vomiting Recent cessation of passage of stool and flatus Increased and/or 'noisy' bowel sounds
AuscultationAuscultation of the abdomen is for detecting bowel sounds and vascular bruits.
BOWEL SOUNDS
The stethoscope should be placed on one site on the abdominal wall (just to the right of the umbilicus is best) and kept there until sounds are heard. It should not be moved from site to site. Normal bowel sounds are heard as intermittent low- or medium-pitched gurgles interspersed with an occasional high- pitched noise or tinkle
Absence of bowel sounds implies paralytic ileus or peritonitis. In intestinal obstruction, bowel sounds occur with increased frequency, volume and pitch, and have a high-pitched, tinkling quality.
VASCULAR BRUITS
Listen above the umbilicus over the aorta for arterial bruits, which suggest an atheromatous or aneurysmal aorta or superior mesenteric artery stenosis.
Now place the stethoscope 2-3 cm above and lateral to the umbilicus and listen for renal artery bruits from renal artery stenosis.
Listen over the liver for bruits due to hepatoma or acute alcoholic hepatitis. A friction rub, which sounds like rubbing your dry fingers together, may be heard over the liver (perihepatitis) or spleen (perisplenitis).