Chiropractic Treatment Options for Shoulder Conditions · •abduct arm to 90°, angle forward 30°...
41
Chiropractic Treatment Options for Shoulder Conditions Wendy Varish, DC, FACO, CCSP, CCOHC, MCS-P Proudly Sponsored by:
Transcript of Chiropractic Treatment Options for Shoulder Conditions · •abduct arm to 90°, angle forward 30°...

Chiropractic Treatment Options for Shoulder
ConditionsWendy Varish, DC, FACO, CCSP, CCOHC, MCS-P
Proudly Sponsored by:

Wendy Varish, DC, FACO, CCSP, CCOHC, MCS-P
Howards Grove Chiropractic
516 S. Wisconsin Drive
Howards Grove, WI 53083
(920) 565-3922
fax (920) 565-2142

Syllabus-Chiropractic Treatment Options for Common Shoulder Conditions
You have a busy office.
You have learned great techniques for treatments at other seminars, but the time it
takes to implement these techniques is just not practical.
From rotator cuff conditions to frozen shoulder, this 4 hour program will provide the
doctor with comprehensive treatment options that can be realistically applied within a
busy office. Advanced therapeutic applications and adjusting techniques will be
highlighted.

2 MINUTE ABC’S EVALUATION
aka… The “Hey Doc, could you please just ‘quick’
check out my shoulder?” Exam

2 Minute ABC’S Evaluation
■ Adhesive Capsulitis vs. Scapular Fixation
■ Bicep Tendon Subluxation
■ Clavicle Fixation
■ SITS/ Supraspinatus or Rotator Cuff Tear

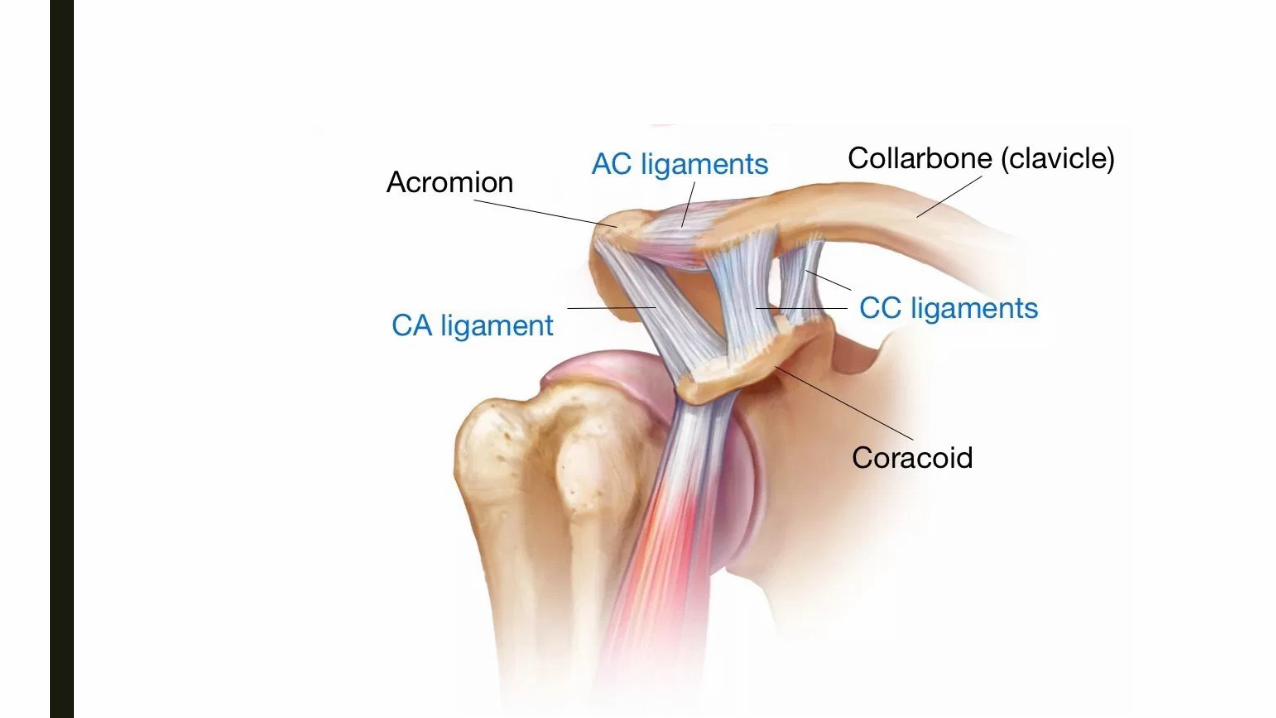
How Many “Joints” in a Shoulder?
■ Glenohumeral
■ Acromioclavicular
■ Sternoclavicular
■ Scapulothoracic




AAdhesive Capsulitis vs.
Scapular Fixation

A: Adhesive Capsulitis vs. Scapular Fixation
■ Patient is unable to perform true
abduction of the arm
■ Evaluate for scapular motion vs. true
adhesions at the GH joint

A: Adhesive Capsulitis vs. Scapular Fixation■ Evaluate for scapular
motion vs. true adhesion of
GH joint/capsule


A: Adhesive Capsulitis vs. Scapular Fixation
■ Before adjusting shoulder, evaluate for upper cervical spine subluxation and
suboccipital involvement
■ Correct spinal subluxation to free CN XI
■ Re-assess shoulder abduction and scapular motion
■ Address trapezius and subscapular muscle adhesions
■ Re-assess
■ Adjunct Therapeutic Options
– Laser/Light Therapy
– Ultrasound

A: Adhesive Capsulitis vs. Scapular Fixation

BBicep Tendon Subluxation
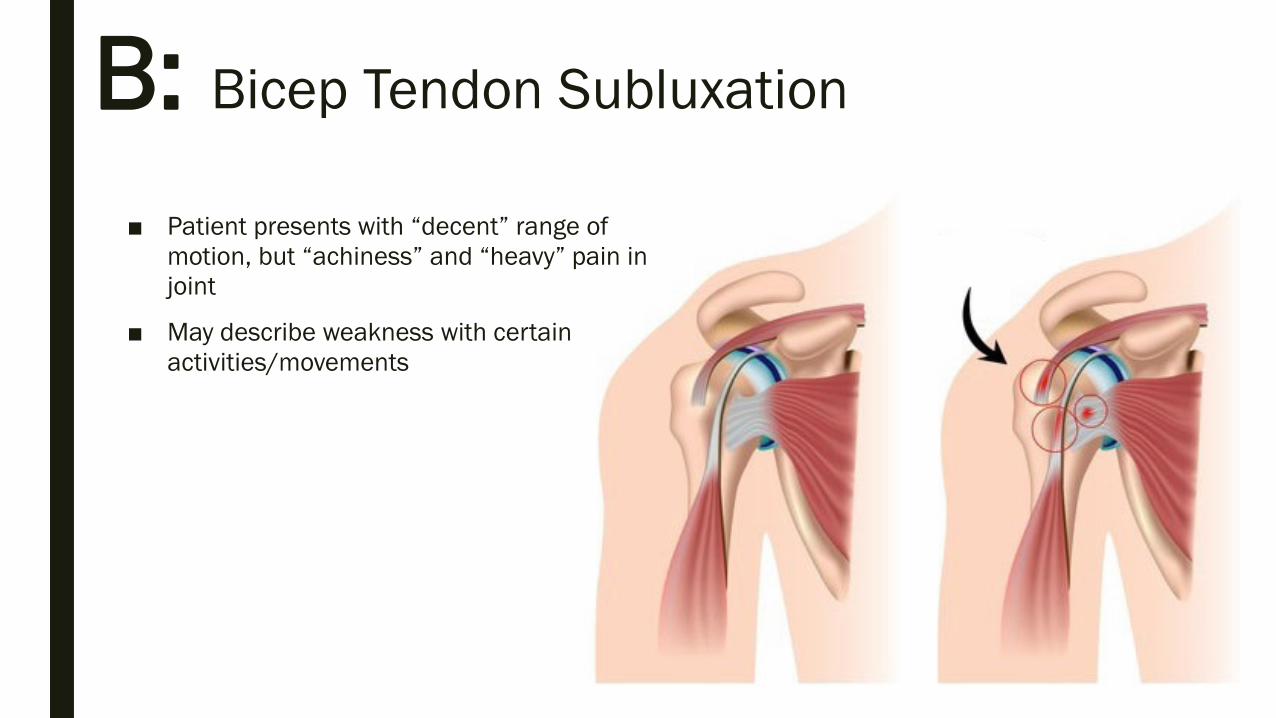
B: Bicep Tendon Subluxation
■ Patient presents with “decent” range of
motion, but “achiness” and “heavy” pain in
joint
■ May describe weakness with certain
activities/movements

B: Bicep Tendon Subluxation
■ Test: Patient seated with arm abducted to 90*. Test
resistance in internal (thumb down) and external
rotation (thumb up)
– Can test opposite side for comparison
■ Tenderness with palpation may be elicited at the
transverse ligament/bicipital groove
■ NOTE: 90*Abduction and ER isometric test ->
palpate biceps tendon in bicipital groove if pain
anterior it's a tendon problem, if the pain is posterior
then it is likely to be internal impingement
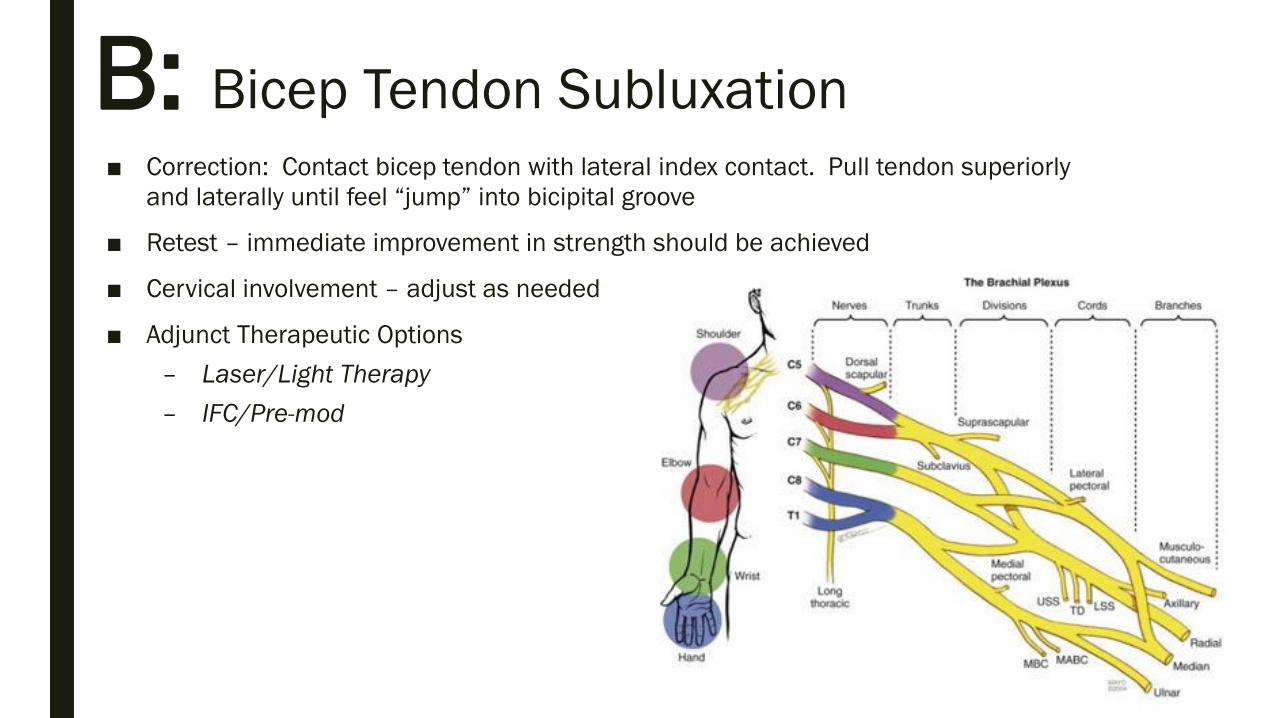
B: Bicep Tendon Subluxation
■ Correction: Contact bicep tendon with lateral index contact. Pull tendon superiorly
and laterally until feel “jump” into bicipital groove
■ Retest – immediate improvement in strength should be achieved
■ Cervical involvement – adjust as needed
■ Adjunct Therapeutic Options
– Laser/Light Therapy
– IFC/Pre-mod

B: Bicep Tendon Subluxation

CClavicle Fixation

C: Clavicle Fixation

C: Clavicle Fixation
■ Patient presents with pain at anterior
shoulder/ chest/ pect
■ General /active ROM may be somewhat
restricted
■ May describe weakness with certain
activities/movements


C: Clavicle Fixation
■ Test: Patient supine. Support patient’s arm and abduct to 90* with elbow bent to
90*. Test passive internal and external rotation
– Determine if clavicle is fixated in external or internal rotation (or both)
■ Consider muscular involvement – address cervical spine subluxations


C: Clavicle Fixation
■ Correction:
– Make correction by adjusting clavicle with rotational impulse into direction of
fixation
– Address cervical subluxations related to muscular attachments
■ Retest
■ Adjunct Therapeutic Options
– Laser/Light Therapy -- to cervical spine, trapezius
– ? Ultrasound or IFC to muscles creating chronic subluxation/fixation

C: Clavicle Fixation
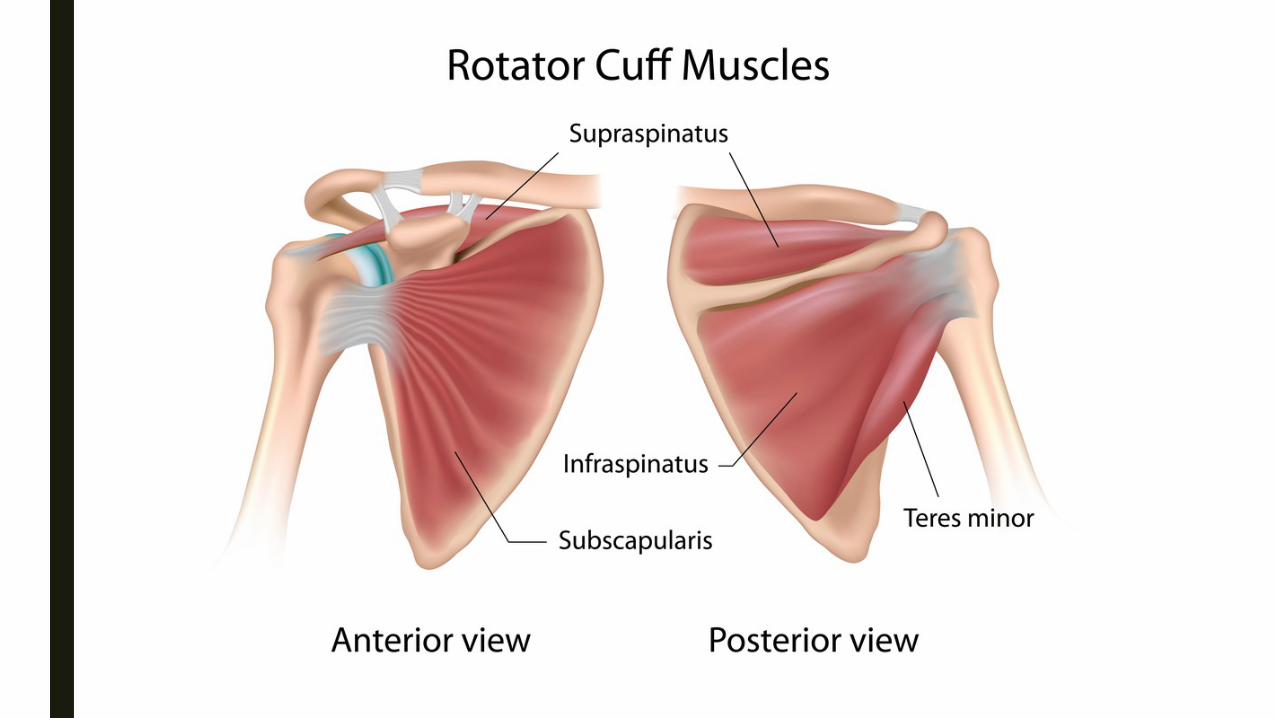
SSITS/Rotator Cuff/
Supraspinatus Tear

■ More involved than just
“primary” tear
■ May present with pain, loss of
ROM, loss of strength,
interference with ADL’s
■ Pain may encompass and
include pathology at other
muscles
– Deltoid(s)
– Biceps
– Subscapularis
S: SITS/Rotator Cuff/Supraspinatus Tear


S: SITS/Rotator Cuff/Supraspinatus Tear
■ Tests:
– Supraspinatus Press Test
– Abduction ROM with “painful arc”
– Drop Arm

• Supraspinatus Strength / Supraspinatus Press Test• strength is assessed using Jobe’s Test (see below) – pain with this test is indicative of a
subacromial bursitis/irritation – not necessarily a supraspinatus tear. Only considered positive for
tear with a true drop arm. i.e. arm is brought to 90° and literally falls down.
• Jobe’s Test (“Empty Can Test”)tests for supraspinatus weakness and/or impingement
• technique
• abduct arm to 90°, angle forward 30° (bringing it into the scapular plane), and internally
rotate (thumb pointing to floor). Then press down on arm while patient attempts to maintain
position testing for weakness or pain.
• Drop Signtests for function/integrity of supraspinatus
• technique
• passively elevate arm in scapular plan to 90°. Then ask the patient to slowly lower the arm.
The test is positive when weakness or pain causes them to drop the arm to their side.
S: SITS/Rotator Cuff/Supraspinatus Tear

■ With “2 Minute” Evaluation - will need to address cervical spine as well as all four
“joints” in order to provide best conditions for healing
■ Therapeutic Modalities:
– Laser/ Light Therapy
■ Progress through Rehab Exercises
– Passive ROM
– Assisted ROM
– Active ROM
S: SITS/Rotator Cuff/Supraspinatus Tear

■ Passive ROM
– Codman’s
– Pulley
– Broomstick/cane
■ Assisted ROM
– Broomstick/cane
– Wall-Walking
■ Active ROM
– Disco / Apple Picking
S: SITS/Rotator Cuff/Supraspinatus Tear
Rehab Exercises

S: SITS/Rotator Cuff/Supraspinatus Tear
Case Studies

30 Second Evaluation?
■ Therapeutic Options
– Laser/Light Therapy
– Rehab Exercises

BEYOND THE 2 MINUTE ABC’S
Shoulder Examination / Evaluation
TUNE IN NEXT TIME!

Wendy Varish, DC, FACO, CCSP, CCOHC, MCS-P
Howards Grove Chiropractic
516 S. Wisconsin Drive
Howards Grove, WI 53083
(920) 565-3922
fax (920) 565-2142