Chinese American Medical Society - Home DOH… · 15.03.2020 · Author: Sally Slavinski Created...
9
Health Alert # 6: COVID-19 Updates for New York City The number of persons diagnosed with COVID-19 in New Yorker continues to rise o Of cases where source of exposure was known (n=56), only 7 (13%) were known to have exposure outside NYC, confirming community-wide transmission o 60% of hospitalized cases were admitted to the ICU, 1 death reported Several commercial and hospital-based testing options for COVID-19 are now available New York City Public Health Laboratory (PHL) will now only accept nasopharyngeal (NP) and oropharyngeal (OP) swabs packaged in the SAME viral transport medium (VTM) collection tube; lower respiratory tract specimens (sputum) can also be submitted MINIMIZE EXPOSURES TO THE PUBLIC, VULNERABLE PATIENTS AND HEALTHCARE WORKERS o Advise patients with mild respiratory illness to STAY HOME; testing is not indicated for mildly ill or asymptomatic persons o This will minimize possible exposures to healthcare workers, patients and the public and reduce the demand for personal protective equipment WE MUST PRESERVE PERSONAL PROTECTIVE EQUIPMENT SUPPLIES o Use standard, contact, droplet precautions, and eye protection when caring for patients who are confirmed or suspected to have COVID-19 Healthcare facilities should plan now for enhanced surge capacity The Provider Access Line (PAL) is intended to receive calls only from healthcare providers. Do not share this number with the public. March 15, 2020 Dear Colleagues: The World Health Organization (WHO) has announced that the current coronavirus disease 2019 (COVID-19) outbreak is now a pandemic. Widespread community transmission of SARS-CoV-2, the virus that causes COVID-19, is occurring in New York City (NYC). To date, 240 cases have been reported in NYC, 28% of which are in patients aged ≥65 years and 58% of which are in males (see data table and figure 1 below). Of cases where source of exposure was known (n=56), only 7 (13%) were known to have exposure outside NYC. Of the 62 cases known to have ever been hospitalized, 60% were admitted to the intensive care unit and 44% required ventilator support. Because NYC DOHMH has prioritized the testing and investigation of severely ill individual cases, these data are likely biased towards that population and may not accurately represent the severity of disease among all infected persons.
Transcript of Chinese American Medical Society - Home DOH… · 15.03.2020 · Author: Sally Slavinski Created...

Health Alert # 6:
COVID-19 Updates for New York City
The number of persons diagnosed with COVID-19 in New Yorker continues to rise o Of cases where source of exposure was known (n=56), only 7 (13%) were
known to have exposure outside NYC, confirming community-wide transmission
o 60% of hospitalized cases were admitted to the ICU, 1 death reported
Several commercial and hospital-based testing options for COVID-19 are now available
New York City Public Health Laboratory (PHL) will now only accept nasopharyngeal (NP) and oropharyngeal (OP) swabs packaged in the SAME viral transport medium (VTM) collection tube; lower respiratory tract specimens (sputum) can also be submitted
MINIMIZE EXPOSURES TO THE PUBLIC, VULNERABLE PATIENTS AND HEALTHCARE WORKERS
o Advise patients with mild respiratory illness to STAY HOME; testing is not indicated for mildly ill or asymptomatic persons
o This will minimize possible exposures to healthcare workers, patients and the public and reduce the demand for personal protective equipment
WE MUST PRESERVE PERSONAL PROTECTIVE EQUIPMENT SUPPLIES o Use standard, contact, droplet precautions, and eye protection when caring for
patients who are confirmed or suspected to have COVID-19
Healthcare facilities should plan now for enhanced surge capacity The Provider Access Line (PAL) is intended to receive calls only from healthcare
providers. Do not share this number with the public.
March 15, 2020
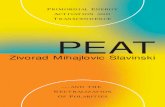
Dear Colleagues: The World Health Organization (WHO) has announced that the current coronavirus disease 2019 (COVID-19) outbreak is now a pandemic. Widespread community transmission of SARS-CoV-2, the virus that causes COVID-19, is occurring in New York City (NYC). To date, 240 cases have been reported in NYC, 28% of which are in patients aged ≥65 years and 58% of which are in males (see data table and figure 1 below). Of cases where source of exposure was known (n=56), only 7 (13%) were known to have exposure outside NYC. Of the 62 cases known to have ever been hospitalized, 60% were admitted to the intensive care unit and 44% required ventilator support. Because NYC DOHMH has prioritized the testing and investigation of severely ill individual cases, these data are likely biased towards that population and may not accurately represent the severity of disease among all infected persons.

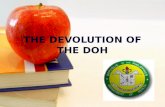
Widespread transmission of SARS-CoV-2 will likely result in large numbers of people needing medical
care in the coming weeks. Syndromic surveillance data continue to show an increase in the number of
persons visiting an emergency department who report influenza-like illness (see figure 2 below). At this
time, providers and healthcare facilities are therefore urged to implement mitigation strategies to lessen
the impact that COVID-19 may have on staff and patients and to ensure continuing operations.
Resources are available on the Greater New York Hospital Association and CDC websites. Providers
should manage any persons with acute febrile or respiratory illness that cannot be attributed to other
causes as being potentially infected with SARS-CoV-2.
COVID-19 LIKE ILLNESS COVID-19 like illness is described as new onset of subjective or measured (≥100.4oF or 38.0oC) fever OR cough OR shortness of breath OR sore throat that cannot be attributed to an underlying or previously recognized condition. In children, fever with sore throat may be attributable to conditions other than COVID-19 (e.g., strep throat) and parent/guardian should be instructed to consult a healthcare provider to rule out other etiologies. A confirmed case of COVID-19 is defined as a person with COVID-19 like illness and a positive laboratory test. A possible case of COVID-19 is defined as a person with COVID-19 like illness for whom testing was not performed. To date, factors associated with severe illness include age ≥50 years (children and young adults appear
to be less affected) and chronic medical conditions, such as chronic lung disease (e.g., asthma,
emphysema), hypertension or diabetes.
TESTING FOR COVID-19 Several commercial and hospital-based laboratories are now offering COVID-19 testing using a molecular assay. However, the DOHMH strongly recommends against testing persons with mild illness who can be safely managed at home, unless a diagnosis may impact patient management. This will minimize possible exposures to healthcare workers, patients and the public and reduce the demand for personal protective equipment. Providers should keep in mind that a negative result in the context of a person who is symptomatic and who is not improving and in whom there is a high index of suspicion for COVID-19 might represent a false negative. If there is reason to suspect a person has COVID-19 despite a negative test result, consider re-testing and continuing infection control practices appropriate for COVID-19. Moving forward, the NYC Public Health Laboratory (PHL) will only accept pre-approved specimens for
hospitalized patients with severe acute lower respiratory illness (e.g., pneumonia). To obtain approval
for PHL testing, contact the NYC Health Department Coronavirus Testing Call Center by calling the
Provider Access Line (PAL) at 866-692-3641. If testing is approved, the clinical team should send patient
specimens to the hospital’s central laboratory and provide the hospital’s central laboratory with the
unique identification number provided by the Call Center. The hospital’s central laboratory should then
submit the necessary laboratory requisition online through PHL’s eOrder (an internet-based application
developed by PHL). The hospital’s central laboratory should then call back the PAL with the eOrder
number and the unique identification number provided by the Call Center to arrange courier
transportation of the specimen to PHL (the hospital can also arrange for its own courier to PHL). If you
do not already have an eOrder account, please visit the PHL website for more information.
Specimens required for COVID-19 testing include 1 nasopharyngeal (NP) swab and 1 oropharyngeal (OP)
swab packaged in the SAME viral transport medium (VTM) collection tube. One lower respiratory tract

specimen (e.g., sputum) can also be submitted if it can be easily collected (e.g., bronchial or tracheal
aspirate in patients who are on ventilator support).
All PHL test reports will be delivered by fax to the submitting laboratory. The report will also be
available in eOrder. Providers should contact their hospital’s central laboratory for test results. The NYC
Health Department will not report back results to patients on behalf of providers.
REPORTING PERSONS WITH SUSPECTED OR CONFIRMED COVID-19 TO THE NYC HEALTH DEPARTMENT The NYC Health Department receives positive test results directly from the laboratory. Providers should report persons who are part of a cluster of 3 or more possible or confirmed cases in a residential congregate setting that serves more vulnerable populations such as an assisted living facility, group home, homeless shelter, or correctional settings. Reports can be made by calling the PAL at (866) 692-3641. PROTECTING PATIENTS AND STAFF Providers should strongly discourage persons who have a mild disease consistent with COVID-19 like illness and who do not require medical care from visiting a healthcare facility. Message clients who are at higher risk for more severe disease (e.g., older adults, persons a compromised immune system or chronic health conditions such as heart disease, diabetes and lung disease) to limit the amount of time they spend with other people, especially outside the home, to reduce the possibility of being infected with the virus. Consider placing signage and greeters at entry points to screen persons seeking care and visitors by asking if they have a COVID-19 like illness. This will help avoid unnecessary exposures within the healthcare facility. As an alternative to in person evaluation, communicate with patients by telephone, electronic messaging or video conferencing. Evaluation for patients with severe illness, which might include worsening symptoms or difficulty breathing, should be done in an acute care facility. If a patient with COVID-19 like illness needs to be evaluated in person, instruct them to minimize contact with other persons, travel by private car if possible and, when available, to use a face mask while traveling to the healthcare facility. INFECTION CONTROL UPDATES Healthcare facilities should implement and adhere to policies and practices that minimize exposures to respiratory pathogens including SARS-CoV-2. A continuum of infection control measures should be implemented before patient arrival, upon arrival, throughout the patient’s visit, and until the patient’s room is cleaned and disinfected. It is particularly important to protect individuals at increased risk for adverse outcomes from COVID-19 (e.g., older persons with comorbid conditions). Triage personnel should have a supply of facemasks and tissues for patients with COVID-19 like illness that can be provided to them upon arrival. Source control (putting a facemask over the mouth and nose of a symptomatic patient) can help to prevent transmission to others.
Additionally, in the setting of a pandemic with widespread community transmission in NYC, all
healthcare workers are at some risk for exposure to COVID-19, whether in the workplace or in the
community. Therefore, the NYC Health Department is asking ALL healthcare workers, regardless of
whether they have had a known SARS-CoV-2 exposure, to self-monitor by taking their temperature
twice daily and assessing for COVID-19 like illness. If healthcare workers develop any signs or
symptoms of a COVID-19 like illness (for healthcare workers, fever cutoff is 100.0oF), they should NOT
report to work. If any signs or symptoms occur while working, healthcare workers should
immediately leave the patient care area, inform their supervisor per facility protocol, and isolate
themselves from other people.

PERSONAL PROTECTIVE EQUIPMENT (PPE) UPDATE:
As per the newest CDC guidance, patients can be managed with droplet precautions along with gown,
gloves, and eye protection. This means that patients can be evaluated in a private examination room
with the door closed. An airborne infection isolation room (AIIR) is no longer required by the CDC
unless the patient will be undergoing an aerosol generating procedure (the CDC does NOT consider
the collection of a NP or OP swab an aerosol generating procedure).
If a private exam room is not readily available in the healthcare facility, ensure that the patient is not
allowed to wait among other patients seeking care. Identify a separate space that allows the patient to
be separated from others by ≥6 feet, with easy access to respiratory hygiene supplies. In some settings,
patients might opt to wait in a personal vehicle or outside the healthcare facility where they can be
contacted by mobile phone when it is their turn to be evaluated.
The safety of healthcare workers is a top priority for the NYC Health Department. As we gain more understanding of COVID-19, our guidance will evolve. The use of standard, contact, and droplet precautions with eye protection is appropriate when caring for patients with possible or confirmed COVID-19. Personal protective equipment (PPE) should include: facemask (procedure or surgical mask) AND gown AND gloves AND eye protection (goggles or face shield). The NYC Health Department recommends healthcare workers do not need to use a fit tested N95 respirator or Powered Air Purifying Respirator (PAPR) for routine (non-aerosol generating) care of a COVID-19 patient. Patients can be evaluated in a private examination room with the door closed. Supplies of PPE must be reserved for high risk procedures due to potential supply chain constraints. Ample studies indicate the safety of droplet precautions which may also help prevent the complete exhaustion of fit tested N95 respirators and PAPRs; higher level PPE will continue to be needed to protect HCWs during critical and medically necessary aerosol generating procedures (e.g., intubation, suctioning) throughout the course of this outbreak. Placing the patient in an AIIR and the use of a fit tested N95 respirator or PAPR is still recommended for
aerosol-generating procedures (e.g., intubation, suctioning, nebulizer therapy) and when caring for
patients with severe illness requiring intensive care. These recommendations are based on our current
knowledge of COVID-19 and other coronaviruses, are endorsed by subject matter experts in the field of
infection control, and are aligned with the WHO Infection Control Guidance for COVID-19. According to
the new Report on the WHO-China Joint Missions on Coronavirus Disease 2019: “Airborne spread has
not been reported for COVID-19 and it is not believed to be a major driver of transmission based on
available evidence; however, it can be envisaged if certain aerosol-generating procedures are conducted
in health care facilities.” Additionally, several studies, including a recent large randomized control trial,
showed no benefit to the use of N95 respirators vs. face masks in preventing influenza and other viral
respiratory infections in healthcare workers (Radonovich, 2019).
These measures are part of an overall infection control package designed to keep healthcare workers
safe: rapid identification and source control of symptomatic patients, strict adherence to respiratory and
hand hygiene practices, training staff on correct use of PPE, and routine cleaning and disinfection of
surfaces and equipment.

HEALTHCARE FACILITY PREPAREDNESS
Healthcare resources in New York City will become strained in the weeks ahead and healthcare facilities
should plan for enhanced surge capacity. Considerations might include closing nonessential services,
cohorting patients, using non-patient care spaces for triage of patients suspected to have COVID-19,
opening closed units, using ambulatory areas, discharging/transferring patients, and creating designated
isolation spaces. Healthcare facilities are also encouraged to implement plans now for canceling elective
admissions and procedures. The American College of Surgeons released a statement on March 13,
2020, recommending that health systems “minimize, postpone, or cancel electively scheduled
operations, endoscopies, or other invasive procedures” and “minimize use of essential items needed to
care for patients, including but not limited to, ICU beds, personal protective equipment, terminal
cleaning supplies, and ventilators.”
TREATMENT Currently, medical care for COVID-19 is supportive. Corticosteroids should be avoided unless they are indicated for other reasons (e.g., COPD exacerbation, septic shock). The antiviral remdesivir is being studied as one experimental treatment. Criteria for compassionate use of the drug as per the manufacturer Gilead include a confirmed SARS-CoV-2 infection, pneumonia, and hypoxia (oxygen saturation ≤94% on room air). Exclusion criteria may include creatinine clearance <30 ml/min and liver function tests >5 times normal. Clinicians interested in obtaining the drug can directly reach out to the National Institutes of Health or Gilead. In addition, see CDCs current Clinical Guidance at https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html
ISOLATION AND QUARANTINE GUIDANCE FOR MANAGING PERSONS WITH POSSIBLE OR CONFIRMED COVID-19 Isolation and quarantine are different. These two terms are not interchangeable. Isolation refers to the separation of sick people with a contagious disease from people who are not sick. Quarantine refers to the separation of asymptomatic people who were exposed to a contagious disease to see if they become sick. Guidance materials will be available on the NYC Health Department website. When preparing to discharge patients with confirmed or possible COVID-19 from the emergency or inpatient department, or sending them home from an outpatient healthcare facility, instruct them to self-isolate and remind their household contacts to self-monitor (see below). The NYC Health Department DOES NOT require a negative COVID-19 test to release a patient from a healthcare facility.. SELF-ISOLATION AT HOME As a routine matter, but especially during the current pandemic, persons who are not hospitalized but who have possible or confirmed COVID-19 should be instructed to isolate themselves in a private residence until 7 days following onset of illness and 72 hours after being consistently afebrile without use of antipyretics and with resolving respiratory symptoms. Caregivers should consult a healthcare provider for children with fever and sore throat to determine if testing is indicated for other illnesses such as strep throat. Persons staying at home because of confirmed or presumed COVID-19 infection should not attend work or school and should avoid public settings and other situations that may permit close contact with others. This guidance applies to any person, regardless of whether they have received a laboratory-confirmed COVID-19 diagnosis, including healthcare workers. Healthcare workers and other staff employed by a facility regulated by the New York State Health Department (e.g., an

Article 28 Facility) or a jurisdiction outside of NYC should check with their employer before returning to work as the employer may have a different policy regarding COVID-19. SOCIAL DISTANCING AND SELF-MONITORING We are entering a phase of the pandemic where social distancing may have the greatest impact on
minimizing transmission. All New Yorkers are asked to practice social distancing, meaning that they
should stay at home to the extent possible and only leave home for essential tasks. All New Yorkers
should consider themselves as possibly exposed to SARS-CoV-2 and must therefore self-monitor for
COVID-19 like illness – especially those who have had close contact with a person with possible or
confirmed COVID-19 and those who are healthcare workers. Close contact includes those persons who
reside or provide care in the same household of the ill person or are an intimate partner of the ill
person. Close contacts should monitor their health at all times, but should be particularly vigilant for 14
days starting from the last time there was close contact with the person while they were ill. Persons in
whom COVID-19 like illness develops should isolate themselves at home and adhere to guidance on self-
isolation at home for persons with confirmed or possible COVID-19 (see above). Such ill persons should
only seek healthcare if they have severe or worsening illness.
As a reminder, patients with mild illness do not need COVID-19 testing, unless it may change
management. Providers with questions can call the NYC Health Department at the Provider Access Line
(PAL) at 1866-692-3641; note that this number is intended only for providers, not the public.
Emotional reactions to this emerging health crisis are expected. Remind yourself, your staff and your
patients that feeling sad, anxious, overwhelmed or having other symptoms of distress such as trouble
sleeping is normal. If symptoms become worse, encourage them, and yourself, to reach out for support
and help. Those living in NYC can call NYC Well at 888-NYC WELL (888 692-9355), or text “WELL” to
65173 for access to a confidential help line.
NYC healthcare providers and institutions are reminded to check COVID-19 resources available on the
NYC Health Department provider webpage (on.nyc.gov/covid19provider), and the CDC website.
Thank you for your collaboration. Sincerely,
Demetre Daskalakis, MD, MPH Deputy Commissioner

2019 Novel Coronavirus (COVID-19) – Data Summary
March 14, 2020
The data in this report reflect events and activities through March 14, 2020.
Includes cases in NYC residents and foreign residents treated in NYC facilities
. Total
Cases
Total 240
Median Age (Range) 48 (7-96)
Age Group
- 0 to 17 13 (5%)
- 18 to 40 81 (34%)
- 41 to 65 78 (33%)
- over 65 68 (28%)
Sex
- Female 98 (42%)
- Male 134 (58%)
Borough
- Bronx 21
- Brooklyn 53
- Manhattan 72
- Queens 78
- Staten Island 16
- Unknown 0
Ever Hospitalized 62
- Discharged 12
- Admitted to ICU 37
- On Ventilator 27
Deaths 1 1Cumulative since January 31, 2020. Data may be updated in between reports on DOHMH's website and/or press releases.

Figure 1. COVID-19 Cases in New York City by Week of Diagnosis*
*Due to day of week effects (lower reporting on weekend), counts of reports represented for the past two days do
not represent a true decrease in incidence.

Figure 2. Influenza-like illness (ILI) emergency department (ED) visits (defined as presence of fever AND cough or
sore throat OR mention of influenza). The lines show the proportion of daily ED visits for ILI comparing four
influenza seasons. The recent increase in ILI visits (highlighted in the circle) is unusual for this time of year.
Caution: Do not over interpret the downturn as this does not mean the pandemic has peaked. Day of the week variation occurs in ED visits where lower numbers are seen on weekends.
Figure 2.