DOH Reengineering Monograph

of 175
-
Upload
anonymous-nnbbgps -
Category
Documents
-
view
231 -
download
0
Transcript of DOH Reengineering Monograph
-
8/19/2019 DOH Reengineering Monograph
1/175
T H E N E E D F O R
H E A L T H R E F O R M S
◘
Historical Background
The Philippine Department of Health (DOH) has a long and distinguished history.
It began as the Board of Health on June 23, 1898 by virtue of a decree by the
new republic under President Emilio Aguinaldo. It has since evolved into one of
the major departments of government with a budget and personnel that has kept it
among the top five agencies of the executive branch. In 1999, under Republic Act (RA)
8745, it had an appropriation of about P12 Billion and a nationally paid workforce of
27,410 employees.
The past twenty years were marked with changes. In
1982, President Ferdinand E. Marcos reorganized the DOH
under Executive Order (EO) 851. This was done to
synchronize health structures and operations with th
shift to a parliamentary form of government. Instead
being referred to as DOH, it became known as the Minist
of Health (MOH)
e
of
ry
.
The Office of the President had control of the ministry,
with supervision provided by the Prime Minister. It wasalso accountable to the Batasang Pambansa or the parliament and to the cabinet to
ensure harmonization of health programs with the rest of the programs of government.
It was during this period that a State Minister for Health with the rank of deputy
minister was appointed from elected members of Parliament. However, its organic
structure remained basically unchanged. There was one line bureau, five staff bureaus,
seven project or technical offices, which focused on diseases or special concerns. They
were later renamed into technical services.
June 23, 1898 – Boardof Health
Pres. Emilio Aguinaldo
EO 851/1982 – Ministryof Health
Pres. Ferdinand E. Marcos
EO 119/1986 –Department of Health
Pres. Corazon C. Aquino
Chapter
1
1
-
8/19/2019 DOH Reengineering Monograph
2/175
The Minister of Health at the same time
supervised a number of medical centers,
hospitals including those with research
functions and attached agencies such as
the Dangerous Drugs Board, the
Philippine Medical Care Commission and
the Schistosomiasis Control Council. For
service delivery, the hierarchy began
with the regional health offices under
which operated provincial health offices
and city or municipal health offices. The
MOH through the Regional Health Offices
administratively and technically
supervised local health services.
The next major change came in 1986
with EO 119, “Reorganizing the Ministryof Health”, by President Corazon C.
Aquino. It was promulgated under the
Freedom Constitution. EO 119 clustered
agencies and programs under the Office
for Public Health Services, Office for
Hospital and Facilities Services, Office
for Standards and Regulations and Office
for Management Services.
An Executive Committee for National
Field Operations was also established
headed by the Minister with a secretariat
headed by the Deputy Minister serving as
Chief of Staff. The Field Offices were
composed of the Regional Health Offices
and National Health Facilities. The latter
was composed of the National Medical
Centers, the Special Research Centers
and Hospitals. Five Deputy Minister
positions were created and a number of
DOH personnel were relieved.
EO 292 known as the Administrative Code
was promulgated under the new
Constitution. It maintained the
organizational structures under EO 119.
The only difference was that the
ministries were now reverted to
departments as the country returned to
the presidential form of government
from the short-lived parliamentary
system.
In 1988, RA 6675, otherwise known as
the Generics Act was passed to promote,
require and ensure the production of
adequate supply, timely distribution,
rational use and acceptance of drugs and
medicines identified by their generic
name. This Act serves as the legal
framework of the Philippine National
Drug Policy Program.
A major shift
took place in
1991 with the
passage of the
Local
Government
Code also known
as Republic Act
(RA) 7160.
Under this law,
all structures,
personnel and
budgetary allocations from the provincial
health level down to the barangays were
devolved to the local government units
to facilitate health service delivery.
Surprisingly, this did not result in an
immediate restructuring of the affected
departments, including the DOH.
1988 Generics Act – RA 6675
1991 Local Government Code
– RA 7180
1992 MO 27 to improve andstreamline operationsof national agencies
1992
Magna Carta for Public
Health Workers – RA7305
On August 13, 1992, Memorandum Order
(MO) 27 was issued by President Fidel V.
Ramos, which mandated all
instrumentalities and agencies of the
national government to streamline and
improve their operations and
2
-
8/19/2019 DOH Reengineering Monograph
3/175
organizations. The restructuring of the
DOH did not push through in spite of
attempts to reconfigure its vision,
mandate, functions and activities in
keeping with a devolved set-up.
On March 26, 1992, a Magna Carta for
Public Health Workers (RA 7305) was
passed providing for social and economic
benefits for public health workers and
called for a corresponding Code of
Conduct for Public Health Workers.
However, it was not fully implemented
that year due to insufficient funds.
To date, only four types of financial
benefits are being given to governmentworkers, namely: subsistence allowance,
clothing allowance, salary differentials;
and for Rural Health Physicians,
representation and transportation
allowance (RATA). Other devolved health
workers were not paid the benefits
mandated under the Act due to
insufficient funds from local government
units. Given the funding problem, the
implementation of RA 7305, had to
proceed in stages. This situation has
demoralized local health officials and
devolved health workers prompting calls
for a re-nationalization of devolved
health services.
Efforts to promote community-based,
primary health care system were
strengthened through the Barangay
Health Worker’s Benefits and Incentives
Act of 1995 (RA 7883). RA 7883 led to
the registration and accreditation of
some 174,569 Barangay Health Workers
(BHWs) by the city and municipal health
boards in 1997.
The national government appropriated
55 Million as subsidy to the fourth, fifth
and sixth class local government units
(LGUs) to provide for the subsistence
allowance of accredited BHWs. However,
the law has encountered several
implementation problems, including the
following: 1) some BHWs have not been
able to avail of the benefits and
incentives due them after being removed
from the BHW list by local chief
executives (LCEs); 2) some LCE-
accredited BHWs have not undergone the
basic training required under the law;
and 3) the need to sustain the subsidy
from the national government has not
been met.
In the interim, there were other policy
developments that impinged on the
health care system. Laws were passed in
support of the
major policy
thrusts of the
DOH as
stipulated in the
National HealthPlan (1995-2020)
and its
accompanying
document, the
10-year public
investment plan entitled “Investing in
Equity in Health”.
1995
BHW Benefits(RA 7883)
1995
NHI Act(RA7875)
1996
ASIN Law (RA 8172)
The National Health Insurance Act (RA
7875) providing for health insurance
coverage to all Filipinos was passed into
law in 1995. A National Health Insurance
Program (NHIP) was institutionalized
giving emphasis on indigents and is
administered by the Philippine Health
3
-
8/19/2019 DOH Reengineering Monograph
4/175
Insurance Corporation (PhilHealth). Since
then, PhilHealth has instituted a number
of measures relative to increasing
membership, claims processing and
benefit packages.
In the field of nutrition, notable
developments included the formulation
and adoption of the Philippine Plan of
Action for Nutrition (PPAN) and the
implementation of an Act Promoting Salt
Iodization Nationwide, or the ASIN Law
(RA 8172). The ASIN Law and its
implementing Rules and Regulations (IRR)
were disseminated nationwide in 1996
and 1997.
Despite these gains, some issues continueto hamper the effective the effective
implementation of the law, such as low
utilization of iodized salt, lack of supply
of iodized salt in the market, absence of
sanctions for violators, absence of a
monitoring system, high prices and high
standard requirement.
4
-
8/19/2019 DOH Reengineering Monograph
5/175
◘The State of the Nation’s Health
While all these developments over the
years have given rise to opportunities
that led to better health care services
and improved state of health for all
Filipinos - there are still many challenges
that the whole health sector has to
address.
Infant Mortality Rate (IMR) and Maternal
Mortality Rate (MMR) have declined, but
the rate of decline has slowed down
since 1992. Over the past years, there
has been no significant change in thesevital health indices.
The health status of the Philippines is
typical of developing countries in
“transition”. With the rapid demographic
changes today, the country faces threats
from infectious diseases and from the
ever-rising tide of degenerative chronic
conditions. Emerging health problems
brought about by environmental andwork-related risks factors have remained
largely unattended. These are diseases
that are usually found in urban
population brought about by
industrialization and development. Over
all, the country suffers from what is
called the double burden of disease
patterns common in developing
countries.
Improvement in the quality of health
care remains wanting in most areas and
yet the cost of such care has become
exorbitantly high and is beyond the reach
of ordinary people. Added to this is the
prohibitive cost of drugs and medicines.
It has become common for some people
to die without seeing a doctor or without
taking medicines. There are indications
that we are not effectively allocating our
health resources. Likewise, our sourcing
of funds remains inefficient.
The health sector in the Philippines falls
short in meeting these problems due to
several reasons:
Inappropriate health delivery system
such as, poor hospital facilities,
fragmented primary health system,
ineffective delivery mechanism for
public health program, misdistribution
of health human resources and
others.
Inadequate health regulatory
mechanisms such as gaps in
regulatory mandates, lengthy and
laborious regulatory systems andprocesses and inadequate human
resources and facilities resulting in
poor quality of health care, high cost
of privately provided health services,
high cost of drugs and others.
Poor health care financing such as,
inadequate funding, inefficient
sourcing and ineffective allocation.
To be able to transform the health system
into one that would ensure the delivery of
cost effective services, universal access
to essential services and adequate and
efficient financing, major reforms must be
undertaken.
5
-
8/19/2019 DOH Reengineering Monograph
6/175
◘ The National Objectives for Health
Major Health Developments inthe Past Decade
Devolution of health services
Passage of the National HealthInsurance Act
Epidemiological, demographic and
environmental shifts affectinghealth patterns
Pursuing the needed improvement in the
health care system is in line with the
administration’s thrust to prioritize
delivery of services to the masses and
improve the quality of life of all Filipinos,
especially the poor. The differences in
health status among various groups and
regions in the country have widened
through the years. These disparities
indicate deficient economic and social
policies and the need to reprioritize
interventions to promote equity, fairnessand immediate action.
Revitalizing the health care system must
be seen within the broader context of
several forces affecting the delivery of
basic health services in the past two
decades. These factors are: devolution of
health services to local government units,
passage of the National Health Insurance
Law, the epidemiological, demographicand environmental shifts that resulted in
the emergence of new diseases and
reversals of past initiatives or successes in
disease prevention and control.
Under these realities, the health sector
must work to attain a common goal. The
DOH as the lead agency on health sets the
vision for the nation’s health, “Health
for All Filipinos”.
The mission for the entire health sector
is, “To ensure accessibility and quality
of health care to improve the quality of
life of all Filipinos, especially the poor”.
The DOH, in partnership with all agencies
and organization in the health sector aims
to achieve for communities, families and
individuals the following medium term
goals:
General health status of the population
is improved.
Morbidity, mortality, disability and
complications from specific diseases
and disorders are reduced.
Some diseases (e.g., schistosomiasis,
malaria, filariasis, leprosy, rabies,
poliomyelitis, measles and others) are
eliminated or eradicated as public
health problems.
Healthy lifestyle is promoted.
Health and nutrition of families and
special populations are promoted.
Environmental health and sustainable
development are pursued.
6
-
8/19/2019 DOH Reengineering Monograph
7/175
◘The Health Secto r Reform Agenda
HSRA GOALS
Efficient and effective health delivery
system
Well-established and strong healthregulatory system
Sustainable health care financing
mechanisms
To bring the country towards the
attainment of this vision, the DOH,
health professionals, healthorganizations and other stakeholders in
health, put together the Health Sector
Reform Agenda (HSRA). The agenda
outlines the problems and reforms
needed to bring about an efficient and
effective health delivery system, a well
established and strong health regulatory
system and sustainable health care
financing mechanisms. The HSRA
prescribes the adoption of the followingstrategies:
On Health Service Delivery
Promoting fiscal autonomy to
government hospitals
Secure funding for priority public
health programs
Developing and strengthening of local
health systems capacities
On Health Regulation
Strengthening capacities of health
regulatory agencies
On Health Financing
Expanding the coverage and benefit
spending of the National Health
Insurance Program (NHIP)
Reforms in these areas are
interconnected and interrelated. Health
financing reforms through the NHIP will
make hospital fiscal autonomy viable;
hospital reforms in turn will free
resources for investments in public
health and in health regulation at both
the national and local levels; and goodpublic health programs will relieve the
NHIP from the burden of having to pay
for increasing number of curative
services and be able to address those
diseases which are preventable.
To get the reforms going, the DOH has to
take the lead role in providing the
direction of the health sector and in
undertaking several initiatives to
implement the reform strategies. These
are:
Formulation of the investment
packages for health
Formulation of new laws and
issuance of new policy directives
Pursuing organizational changes in
the DOH, PhilHealth and LGUs
Improvement of finance andprocurement management systems
The DOH should pursue the
organizational restructuring it had
already initiated several years ago.
7
-
8/19/2019 DOH Reengineering Monograph
8/175
OO rr g g aa nn ii zz aa tt ii oo nn aa ll aa nn dd MM aa nn aa g g ee mm ee nn tt RR ee ff oo rr mm
Part
1
The organizational change in the DOH stems both from the realities within andoutside of the health sector. A movement towards “reinventing” government
has swept bureaucracies all over the world. With greater demand for specific
services and meager resources, government simply cannot provide for all the
needs of its various constituencies.
Governance is no longer an exclusive function of governments but it has to be
distributed rationally to other concerned sectors of society. The paradigm postulates
that what the private sector does better, it should do without undue competition from
government. In addition, non-government organizations should be allowed to
accomplish what they can accomplish on their own or in partnership with government
and other service providers.
Governments must do what only government can do. The Local Government Code of
1991 already laid out the proper role of local governments. The national government
must therefore follow suit. The rethinking of government’s role began with President
Fidel Ramos’ Reengineering the Bureaucracy for Better Governance. This was
reinforced by the guidelines issued by President Joseph Estrada under EO 165, which
directed the formulation of an institutional strengthening program for the Executive
Branch under the Presidential Committee on Effective Governance (PCEG).
There were a number of studies already done on organizational efficiency, as a resultof the devolution of health services. For a number of reasons however, the identified
necessary changes did not materialize.
Between 1992 and 1998, the DOH management undertook three major reorganization
attempts. The first one was during the term of Secretary Juan M. Flavier; the second
began under Secretary Jaime Galvez-Tan and continued under Secretary Hilarion
Ramiro; and the third by Secretary Carmencita N. Reodica. The reorganization under
EO 102 initiated by Secretary Alberto G. Romualdez, Jr. was the fourth major effort at
rationalizing and streamlining the DOH after the devolution of health services to the
local governments.
8
-
8/19/2019 DOH Reengineering Monograph
9/175
◘ Review of Past Studies On DOH
Reorganization
1994 Study - The reorganization studyof 1994 proposed a number of significantchanges. Among these are:
1. Reduction of the number of
undersecretaries from five to
three to take care of the Office
of the Chief of Staff, the Public
Health Group and the Health
Regulation Group; and the
reduction of Assistant Secretaries
from four to two to take care of
Administrative and Technical
Services, respectively.
2. Consolidation of the disease-
specific programs into a Bureau
of Disease Control; the
consolidation of targeted sector
services (such as nutrition,
dental service, family planning
and others) into a Bureau ofPromotive and Preventive
Health, and the setting up of aBureau of Preventive and
Promotive Education.
3. Creation of a Bureau of Hospitals
and Health Facilities, a Bureau of
Research and Laboratories, a
Bureau of Food and Drugs and a
Bureau of Quarantine.
4. Consolidation of the 14
administrative regions into eight
territorial field offices.
It is clear that these changes would have
satisfied some of the requirements of
devolution and the government’s need
for a more streamlined and rationalized
DOH structure. Unfortunately, no
enabling authority was issued, either in
the form of an executive order or a law.
Thus, the proposed reorganizationstructure shown in Figure 1 did not push
through.
9
-
8/19/2019 DOH Reengineering Monograph
10/175
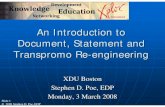
1995 Study - The efforts of Secretary
Jaime Galvez-Tan and Secretary
Hilarion Ramiro differed in the
proposed structure. The Galvez-Tan
organization and management study
focused more on the processes of the
DOH than on its structure.
Among others, it recommended the
adoption of Daily Situationer Briefs,
which will enable the Secretary, Chief
of Staff and other key DOH officers to
quickly address health problems and
opportunities.
Figure 1
Proposed DOH Organizational Structure(1994 Study)
Office of
Public Health
SECRETARY OF HEALTH
BUREAUS
ManagementServices Group
Office of the
Chief of Staff
TechnicalServicesGroup
Health FieldTeams
BUREAUS
Regional
Health Office
RegionalMedical Centers
Hospitals
Office forHealth
Re ulation
It also recommended the fine-tuning of
the existing planning-budget-change
process, the definition of the functions
of the Management Committee,
Executive Committee and the Expanded
Management Committee and the
adoption of a proposed organizational
structure that essentially picks up from
EO 119.
1
-
8/19/2019 DOH Reengineering Monograph
11/175
Following this study, there will be four undersecretaries and an equal number of
assistant secretaries. The undersecretaries will take on the roles of chief of staff,
public health services, hospital and facility services and management services
respectively. Before any of these initiatives could be undertaken, Congressman Hilarion
Ramiro, formerly a public health doctor, was appointed as Secretary of Health. The
corresponding organizational structure for this proposal is shown in Figure 2.
Office of the Chief of StaffUndersecretaryAssistant Secretary
SECRETARY OF HEALTH
Support Services
Office of PublicHealth ServiceUndersecretary
Asst. Secretary
Office for Hospitaland Facility ServicesUndersecretary Asst. Secretary
Programs/
Service Programs/
Service
Hospitals/Medical
Centers
Office for ManagementServicesUndersecretary Asst. Secretary
Programs/
Service
RDs
Figure 2
Proposed DOH Organizational Structure(1995 Study)
11
-
8/19/2019 DOH Reengineering Monograph
12/175
The Ramiro organizational analysis
proposed a continuance of the existing
structure with the addition of sub-
committees headed by assistant
secretaries to handle LGUs and Health
Systems, resource generation and
mobilization and health information and
monitoring. There seemed to have been
a consensus at that time that in the
absence of an enabling law from
Congress, no restructuring or
reengineering could be legally
undertaken.
What appeared to be a major insight of
the Ramiro study is the fact that DOH
programs and activities suffer from afunnel effect. There are 2000 staff
coordinating 62 programs at the national
level; 80 to 100 staff coordinating the
same program at the regional level; 30
personnel implementing programs at the
provincial level; and 10 staff actually
executing these programs at the
municipal level. Clearly, these defy
administrative logic and the very
principles of devolution. Clearly too,these also presented opportunities for
restructuring.
1997 Study. The 1997 study
conducted under Secretary Carmencita
Reodica recognized that there were
unmet health care needs due to
underprovision on the supply side and
underutilization on the demand side. It
also specified that the attainment of
quality health care and high standard of
staffing, facilities and working
relationships would be a major goal of a
reengineered DOH. This study identified
the following as areas for improvement
within DOH:
1. Weak health policy process
2. No strategic planning
3. Poor health program management
4. Inefficient and fragmented
enabling processes and systems
5. Inadequate health advocacy
6. Lack of efficient and effective
health and management
information system
7. Lack of accountability of
management systems
8. Reliance on old work habits
9. Weak networking with health
partners and stakeholders
10. Lack of reward and incentive
systems
11. Structural flaws
12. Too much bureaucratic red tape
The following are the salient features of
the 1997 DOH reengineering proposal:
1. Streamline the DOH topmanagement from four
undersecretaries to one
undersecretary.
2. Develop a scientist and specialist
track for technical personnel.
3. Create non-permanent Cluster on
Health Policy and Program
Innovation.
4. Shift from disease-specific toprocess management teams.
5. Establish two separate offices for
licensing and regulation.
12
-
8/19/2019 DOH Reengineering Monograph
13/175
6. Create advisory boards to the
Office of the Secretary.
7. Create a single office for support
services.
8. Privatize production plants.
9. Strengthen DOH liaisoning
capability.
10. Place retained hospitals under an
Office for Hospital Development.
The proposed DOH organizational
structure under the Reodica
proposal is shown in Figure 3.
FFiigguurree 33
PPrrooppoosseedd DDOOHH OOrrggaanniizzaattiioonnaall SSttrruuccttuurree ((11999977 SSttuuddyy))
Office forHealth
Services
Regulation
OFFICE OF THE
SECRETARY
Office of theUndersecretary Advisory
Boards
Media
Unit
AttachedAgencies
Office forPharmaceuticalsand Radiation
Safety
Office forPublicHealth
Program
Development
Office forPolicy andProgram Support
Office forHospitalDevelop-
mentand
Management
FieldHealth
Units
Cluster for Health Policy and P
13
-
8/19/2019 DOH Reengineering Monograph
14/175
DD ee vv ee ll oo pp mm ee nn tt oo ff tt hh ee DD OO HH RR aa tt ii oo nn aa ll ii zz aa tt ii oo nn aa nn dd SS tt rr ee aa mm ll ii nn ii nn g g PP ll aa nn
Part
2
Executive Order 102 issued in May 1999 “Redirecting the Functions and
Operations of the Department of Health” gave it the mandate to institute the
necessary organizational changes. The issuance and implementation of EO 102 is
based on Sections 77 (Organizational Changes), 78 (Implementation of
Reorganization) and Section 79 (Scaling Down and Phasing Out of Activities of Agencies
within the Executive Branch) of the General Provisions of the General Appropriations
Act (GAA) for 1999. The same provisions were also included in the GAAs of 1995 to
1998, which is in keeping with Section 42, Chapter 5 and Book VI of the Administrative
Code of 1987.
EO 102 mandates the DOH to provide assistance to LGUs, people’s organizations (PO)
and other members of civil society in effectively implementing programs, projects and
services that:
1. Promote the health and well being of every Filipino.
2. Prevent and control diseases among populations at risks.
3. Protect individuals, families and communities exposed to health hazards and
risks.
4. Treat, manage and rehabilitate individuals affected by disease and disability.
Among others, EO 102 stipulates the preparation of a Rationalization and Streamlining
Plan (RSP) for the DOH.
Phase1 of the RSP shall contain all the proposed structures, functions and staffing
pattern of the different offices in the Central Office (CO), including the Bureau of Food
and Drugs (BFAD) and the National Quarantine Office (NQO). Phase 2 shall deal with
streamlining the functions and staffing pattern of the regional offices and retained
hospitals, while Phase 3 shall deal with the DOH attached agencies.
EO 102 is complemented by a later issuance affecting the health care service deliverysystem. EO 205 dated January 31, 2000 provides for the creation of a National Health
Planning Committee (NHPC) and the establishment of Inter-Local Health Zones (ILHZs)
throughout the Philippines. In tandem with EO 102, EO 205 is expected to accelerate
service delivery under a decentralized mode.
14
-
8/19/2019 DOH Reengineering Monograph
15/175
◘Guiding Principles and Parameters
In the formulation of the RSP, the DOH considered the governance framework
formulated by the Presidential Committee on Streamlining the Bureaucracy (PCSB)
under the DBM in August 1995 and reinforced by the PCEG in October 1999. The guidingprinciples of this framework were:
Principle of Frugality and
Prioritization - The scope ofgovernment shall be within available
resources and its activities accordingly
prioritized. Government should have a
conscious and deliberate effort to define
what it will do, must do, can do
and wants to do given the call of the
times, its legal mandate, resources and
constraints. All these shall be defined in
the government’s plans and policy
pronouncements.
Principle of Steering - The role ofthe national government in the sectors
shall be to steer rather than row the
boat. The focus of its sectoral functions
therefore shall be on the following:
1. Policy setting, monitoring and
assessment.
2. Promotion and advocacy.
3. Provision of information and
linkages or access to markets,
services and production inputs and
outputs.
4. Provision of assistance and
incentives that will equalize and
level the playing field.
5. Enforcement of appropriate rules
and regulations.
6. Ensuring the provision of safety
nets for adversely affected
population
This principle also laid down therelationship of the government to the
private sector. It is government’s role to:
1. Promote a stable policy
environment; set minimum and
appropriate rules; provide
information and give support to the
production of goods rather be
directly engaged in it.
2. Encourage sharing of resources and
responsibility.
3. Assume primary responsibility in
the production of public goods and
services.
Principle of Vertical
Compartmentalization –Government should reduce duplication of
effort and maximize the use of allresources to achieve socioeconomic and
political goals. Sectoral activities shall
be properly compartmentalized and
accordingly appropriated between the
government and the private sector.
15
-
8/19/2019 DOH Reengineering Monograph
16/175
Government activities shall be properly
distributed among levels of government
- central government, government
corporations and local government units.
Principle of Devolution - Thenational government and local
government units shall be partners in the
pursuit of the development process. The
proper role of the national government
is to set national policy and standards;
and assist, oversee and, monitor local
government units complementary to the
stronger implementing role that local
governments shall assume.
Parameters - The organizational change in the DOH took into consideration
the following basic policy framework.
1. Leaner and Better Central Office
(CO). Enhancing the central office
function particularly on policy
formulation and on establishingtechnical leadership in health.
2. Stronger and More Responsive
Field Offices and Facilities.
Strengthening of field offices
including hospitals and attached
agencies to support direct service
provision and technical leadership
in health.
3. Technical Leadership Over Health
Programs and Increased Technical
Assistance to Local Health
Systems. Strengthening of DOH’s
advocacy role; emphasizing the
need for stronger external
networking and linkaging.
4. Integration of Public Health
Concepts in the Hospital System.
Ensuring that preventive and
promotive health concepts are alsooperational in hospitals.
5. Stronger Regulatory Systems for
Quality Assurance in Health.
Ensuring enforcement of health
standards by reinforcing standard-
setting activities, focusing on
quality assurance and deploying
more enforcement officers in the
field.
6. Stronger National Health
Insurance System. Strengthening
the national health insurance
system to ensure more access to
health by the less privileged,
especially the indigents.
Guidelines - In addition, the reengineering efforts of DOH were guided by the
following specific guidelines and rules:
1. No person will be laid-off or
demoted in keeping with existing
Civil Service Commission (CSC)
rules on reorganization. The worst
scenario is deployment to the
various hospitals or field officeswhere a person’s security of tenure
is assured unless he or she chooses
to resign, retire or seek voluntary
separation. A six-month period was
provided during which time
16
-
8/19/2019 DOH Reengineering Monograph
17/175
employees may choose which
offices they wish to be deployed
to.
2. CO will attempt to diminish the
number of its personnel by half in
keeping with the realignment of
functions envisioned in the RSP.
3. The grouping of functions will
reflect the DOH’s major reform
areas for the next ten years.
4. The reengineered DOH will have a
personnel budget that does not
exceed its present Personal Service
allocation.
5. A system of incentives will be
developed for relocating personnel
including relocation allowances,
assurance of security of tenure and
equal consideration for career
movement within the DOH,
whether at CO, the field offices,
the hospitals and the attached
agencies.
17
-
8/19/2019 DOH Reengineering Monograph
18/175
◘ Procedures and Processes
At the start of the reorganization
process, the DOH Oversight Committee
on Reengineering directed all heads of
offices to undertake a review of their
existing functions. They were also
advised to propose the corresponding
changes in staffing complement
according to new defined functions and
according to the foundational principles
from the Civil Service Commission (CSC)
and the DBM.
The various offices, bureaus and servicessubmitted draft proposals that were
further deliberated and reviewed both by
the concerned offices and the
Reengineering Secretariat before these
were endorsed to the DOH Oversight
Committee for approval. After the DOH
Oversight Committee has approved the
RSP, this was presented to the DBM,
which reviewed the plan and
recommended some revisions. The DBM
Secretary approved the RSP with the
issuance of the Notice of Organizational
Staffing and Compensation Action
(NOSCA). The plan was then forwarded
to the PCEG, which was headed by the
Executive Secretary. The PCEG through
Memorandum Circular (MC) No. 62 finally
approved the implementation of the RSPon July 17, 2000.
The DOH reorganization proceeded from
the prescribed procedures and steps
shown in Table 1.
TABLE 1 – PROCEDURES AND PROCESSES FOR RATIONALIZATION AND STREAMLINING
ACTIVITY REFERENCE DOCUMENTS OUTPUT
1. Mandate Review 1. EO 102; Health SectorReform Agenda; Pertinentlegislation; and otheradministrative issuances
1.Hierarchy of Functions(Indicate if function isprimary, secondary ortertiary, or if shift in functionis contemplated)
Guide Questions:
a. What will we do now thatwe were not doing before?What activities should westop doing?
b. What cluster of activities
should I belong to:regulation, program, policy,management support andothers
c. Who or which offices shouldbe in which cluster?
18
-
8/19/2019 DOH Reengineering Monograph
19/175
ACTIVITY REFERENCE DOCUMENTS OUTPUT
2. Drawing Up the OrganizationalStructure
2. Output No.1 2. Table of Organization
Guide Questions:
a. What kind of organization do we needto fulfill our functions (bureau, service,unit)?
b. What level or rank should our highestofficial be?
c. What units should we have and whatkind of function should these unitsexercise?
3. Staffing Review 3. Output No. 2 3. Staffing pattern ofunit
Guide Questions:
a. How many people do we need toimplement the functions?
b. What kinds of skills, titles and otherqualifications should they carry?
4. Cost Review 4. Output No. 3; and present costallocation per unit
4. Total personnel costs
Guide Questions:
a. How much will it cost in terms ofhuman resource to pursue thefunctions we will now exercise?
b. Will this represent an increase ordecrease in present costs?
5. Integration of outputs across the DOH 5. Outputs No. 1 to 4 5. Rationalization andStreamlining Plan (RSP)
Guide Questions:
a. Will this RSP meet the intentions ofstrengthening the Region as a technicaland resource center for LGUs?
b.Will this result in eliminatingfunctional/ supervisory overlaps at CO?
c.Will this meet the DOH’s HSRA?
d. What kind of retraining and retoolingwill this require of the DOH personnel?
19
-
8/19/2019 DOH Reengineering Monograph
20/175
As the aforementioned processes were
undertaken, supplemental activities
were on going:
1. Review of pertinent laws such asEO 851 (Reorganizing the Ministry
of Health, 1982), EO 119
(Reorganizing the Ministry of
Health, 1987), EO 292 (Instituting
the Administrative Code, 1987),
EO 102 (Redirecting the Functions
and Operations of the
Department of Health), and the
Magna Carta for Public Health
Workers and other relevant DOHdocuments.
2. Interviews with selected officials
and personnel from DOH CO, field
offices and attached agencies.
3. Interviews with significant DOH
constituencies: Congressmen,
Senators, LGUs and NGOs.
4. Conduct of group meetings with
DOH management.
5. Conduct of orientation workshops
participated by personnel from
all ranks.
2
-
8/19/2019 DOH Reengineering Monograph
21/175
DD OO HH RR aa tt ii oo nn aa ll ii zz aa tt ii oo nn Part3 AA nn dd SS tt rr ee aa mm ll ii nn ii nn g g PP ll aa nn
The DOH Rationalization and Streamlining Plan (RSP) for Phase 1 focusing on
Central Office reorganization was formulated. This was approved by the DBM
through its issuance of the NOSCA with the approved staffing complement and
positions in all offices of the reengineered DOH. The NOSCA was posted in all
offices for guidance and information of all DOH officials and personnel and the
Placement and Selection Committees. The issuance of Memorandum Circular (MC) No.
62, through the PCEG sets into motion the DOH reengineering process.
Memorandum Circular 62 among other things highlighted that the rationalization and
streamlining process in the DOH was in keeping with the health sector reform program.It also called for a more in-depth organizational restructuring at all levels and offices
of the DOH, such that the Centers for Health Development (CHD), retained hospitals
and other attached agencies of the DOH shall follow suit.
Components of the RSP - The RSP shall detail the following shifts:
1. The shifts in policy directions, functions, programs, strategies and activities.
2. The structural and organizational shift, stating the specific functions and
activities by organizational units; and the relationship of each unit.
3. The staffing shift, highlighting and itemizing the existing filled and unfilled
positions.
4. The resource allocation shift, specifying the effects of the streamlined set-up on
the agency budgetary allocation and possible savings.
21
-
8/19/2019 DOH Reengineering Monograph
22/175
◘ Policy and Functional Shifts
The shift in policy directions, functions, programs, strategies and activities of the DOH
are summarized below in Table 2.
TABLE 2 – POLICY AND FUNCTIONAL SHIFTS
Area From To
Policy Direction Planner, formulator andimplementer of public healthpolicies, programs and standards
National technical authority onhealth; providing technical andother resource assistance toconcerned groups
Function Direct provision of service Policy formulation, advocacy,program development,standard setting, regulationand monitoring
ImplementingStrategy
Establishment, operation andmaintenance of health units downto the barangay level
Technical and financialassistance to DOHintermediaries through thefield offices
Approach Individual Health Sector
Constituency Individuals DOH partners, intermediaries,LGUs, NGOs, POs, privatesector
DOH Roles - These shifts are
amplified in the following roles of
the DOH as prescribed in EO 102:
1. Lead agency in articulating national
objectives for health to guide the
development of local health systems,
programs and services.
3. Lead agency in health emergency
preparedness and response
services, including referral and
networking systems for trauma,
injuries and catastrophic events.
4. Technical authority in disease
control and prevention.
2. Direct service provider for specific
programs that affect large segments
of the population, such astuberculosis, malaria,
schistosomiasis, HIV-AIDS and other
emerging infections and
micronutrients deficiencies.
5. Lead agency in ensuring equity,
access and quality of health care
services through policy formulation,standards development and
regulations.
22
-
8/19/2019 DOH Reengineering Monograph
23/175
13. Protector of standards of excellence
in the training and education of
health care providers at all levels of
the health care system.
14. Implementer of the National HealthInsurance Law, providing
administrative and technical
leadership in health care financing.
6. Technical oversight agency in charge
of monitoring and evaluating the
implementation of health programs,
projects, research, training and
services.
7. Administrator of selected health
facilities at sub-national levels that
act as referral centers for local
health system (i.e., tertiary and
special hospitals, reference
laboratories, training centers, center
for health promotion; centers for
disease prevention and control,
regulatory offices among others).
8. Innovator of new strategies for
responding to emerging health needs.
9. Advocate for health promotion and
healthy lifestyles for the general
population.
10. Capacity-builder of LGUs, the private
sector, NGOs, people’s organizations,
national government agencies in
implementing health programs andservices through technical
collaborations, logistical support,
provision of grants and allocation and
other partnership mechanism.
11. Lead agency in health and medical
research.
12. Facilitator of the development of
health industrial complex in
partnership with the private sector to
ensure self-sufficiency in the
production of biologicals, vaccines
drugs and medicines.
DOH Functions - Given these
roles, the DOH has the following
functions under EO 102:
1. Formulate national policies and
standards for health.
2. Prevent and control leading causes
of death and disability.
3. Develop disease surveillance and
health information systems.
4. Maintain national health facilities
and hospitals with modern and
advanced capabilities to support
local services.
5. Promote health and well being
through public information; and to
provide the public with timely and
relevant information on health risks
and hazards.
6. Develop and implement strategies
to achieve appropriate
expenditures patterns in health asrecommended by international
agencies.
23
-
8/19/2019 DOH Reengineering Monograph
24/175
7. Develop sub-national centers and
facilities for health promotion,
disease prevention and control,
standards and regulations and
technical assistance.
8. Promote and maintain international
linkages for technical collaboration.
9. Create the environment for
development of a health industrial
complex.
11. Ensure quality of training and
health human resource
development at all levels of the
health care system.
12. Oversee financing of the health
sector and ensure equity and
accessibility to health services.
13. Articulate the national health
research agenda and ensure the
provision of sufficient resource and
logistics to attain excellence in
evidenced-based interventions for
health.
10. Assume leadership in health in
times of emergencies, calamities,
disasters and systems failures.
All these indicate a de-emphasis on direct
service provision and program
implementation in keeping with
devolution, to an emphasis on policy-
formulation, standard setting and quality
assurance and shift to technical
leadership and resource assistance.
24
-
8/19/2019 DOH Reengineering Monograph
25/175
◘ Structural and Organizational Shifts
With the shift in policy directions,
functions and programs, the structure
and organizational composition of the
DOH were likewise modified. The
principles that guided this shift are:
1. Enhance the CO function
particularly on policy formulation
and on establishing technical
leadership in health.
2. Strengthen the DOH’s advocacy
role, emphasizing the need forstronger external networking and
developing linkages.
3. Strengthen the field offices
including hospitals and attached
agencies to support direct service
provision and technical leadership
in health.
4. Ensure enforcement of health
standards by reinforcing standard-
setting activities, focusing on
quality assurance and deploying
more enforcement officers to the
field.
5. Strengthen the national health
insurance system to ensure more
access to health by the less
privileged.
The structural framework for
organizational reforms and reengineering
efforts undertaken by the DOH under EO
102 is shown in Figure 4.
The organizational structure
encompasses the various DOH units as
well as its attached agencies. The
attached agencies are the Philippine
Health Insurance Corporation (PHIC),
which used to be the Philippine Medical
Care Commission; the Dangerous Drugs
Board ; the two new agencies created by
specific laws - the Philippine Institute
for Traditional and Alternative Health
Care (PITAHC) through RA 8423 and the
Philippine National AIDS Council (PNAC)through RA 8504; and the corporate
hospitals (Philippine Heart Center, Lung
Center of the Philippines, National
Kidney and Transplant Institute and the
Philippine Children’s Medical Center),
collectively called the National Centers
for Specialized Health Care.
There are three major office clusters
under the Office of the Secretary in thenew DOH structure. These are:
Health Regulation Cluster, which
shall initiate standard-setting and policy
formulation for the licensing, regulation
and monitoring of health facilities and
services, food and drugs and health
devices and health-related technology.
Regulation officers in the Centers for
Health Development will enforce these
standards.
External Affairs Cluster, which shall
be responsible for the formulation of
policies and standards pertaining to
international health surveillance,
25
-
8/19/2019 DOH Reengineering Monograph
26/175
linkages of the DOH with the
international community as well as local
government units, non-government
organizations and the private sector.
Health Program Development
Cluster, which shall be the technical
authority for public health surveillance,
disease prevention and control, health
promotion and health facility
development.
These three major office clusters are
composed of bureaus and centers.
Two staff bureaus directly report and
provide support to the Secretary of
Health, the Health Human Resource
Development Bureau and the Health
Policy Development and Planning
Bureau. While these bureaus serve the
internal requirements of the DOH as an
organization, the extent of their work
includes the wider health sector as
policies, plans and human resource
development programs are promulgated
with and for sector-wide constituents
and therefore cannot be limited to
organic DOH staff. To complement these,
a staff unit, the Health Emergency
Management Staff also reporting directly
to the Secretary of Health, was
organized to provide sector-wide
coordination and development on health
emergency preparedness and response.
Internal management support services
are provided by four services namely:
Administrative Service, Information
Management Service, Finance Service
and Procurement and Logistics Service.
The Secretary of Health exercises overall
direction and control over the operations
of the Centers for Health Development
(CHDs). These
CHDs oversee
the
implementati
on of policies
and programs
at the
regional level
and in the
retained
health
facilities within the region.
Four CHD Divisions
ManagementSupport Division
Health OperationsDivision
Health RegulationDivision
There are four divisions under the CHDs,
similar to the number of divisions of the
former Regional Health Offices but with
shift in functions. The Administrative and
Finance Divisions were merged into the
Management Support Division. The
Technical and Training Divisions were
merged into Health Operations Division.However, two new divisions were
created: Health Regulation Division
which will handle enforcement of
regulatory policies and Local Health
Assistance Division which will directly
relate to LGUs, NGOs, POs and the
private sector in the development of
local health systems, extension of
technical and other kinds of assistance in
the field of health.
26
-
8/19/2019 DOH Reengineering Monograph
27/175
Table 3 lists the number of major offices and units within the DOH and its attached
agencies. Overall, there is a net decrease of 30 units.
TABLE 3 – COMPARISON OF ORGANIZATIONAL UNITSIN THE DOH UNDER EO 119 AND EO 102
Organizational
Unit
Existing under
EO 119
(1987)
Created under
EO 102
(1999)
Increase
(Decrease)
1. Executive Offices
1.1 Office of the Secretary 1 1 0
1.2 Office of the Undersecretary 5 3 (2)
1.3 Office of the Asst. Secretary 4 4 0
2. Central Office
2.1 Offices headed by Director IV(Bureaus and National Centers)
4 12 8
2.2 Offices headed by Director III(Services and Staff Offices)
25 5 (20)
2.3 Divisions headed by Positionsat SG 25
37 29 (8)
2.4 Divisions headed by Positionsat SG 24
34 26 (8)
3. Centers for Health Development*
3.1 Office of the Director 15 15 0
3.2 Divisions headed by Positions at SG25
30 30 0
3.3 Divisions headed by Positions at SG24
30 30 0
4. Hospitals *
4.1 Special Hospitals 12 12 0
4.2 Regional Hospitals and MedicalCenters
31 31 0
4.3.Provincial Hospitals 4 4 0
4.4 District Hospitals 5 5 0
4.5.Municipal Hospitals 2 2 0
4.6 Sanitaria 8 8 0
4.7.Research Hospitals 2 2 0
5. Attached Agencies**
5.1 Corporations/Council/Board 2 4 2
5.2 Specialty Hospitals 4 4 0Net Increase / (Decrease) (30)
* For further organizational review under Phase 2 of the reengineering process.** For further organizational review under Phase 3 of the reengineering process.
27
-
8/19/2019 DOH Reengineering Monograph
28/175
Offices of the Undersecretary were
reduced from five to three. One office
for Undersecretary (which is vacant) was
abolished while another office will be
abolished after the Undersecretary
position, which is considered a co-
terminus position, is vacated.
While there is an increase of eight
bureaus headed by Director IV,
significant reductions are realized in the
number of staff services headed by
Director III and divisions headed by
Division Chief occupying positions with
salary grade 25 and salary grade 24.
Table 4 details the 12 newly createdbureau level offices including the
national centers. It will be noted that
three regulatory bureaus are retained,
the functions of the former Bureau of
Research and Laboratories are now
integrated into the National Center for
Health Facility Development, for non-
regulatory functions and the Bureau of
Health Facilities and Services (formerly
the Bureau of Licensing and Regulation)
for regulatory functions. A Bureau of
Health Devices and Technology has been
created with the former Radiation Health
Service as the core with an expanded
function to regulate and determine the
health hazards posed by a myriad of new
health and health-related technology and
devices that have entered the market.
TABLE 4 – BUREAU LEVEL OFFICES
Offices Headed by Director IVCentral Office
Existing Under EO 119 Created Under EO 102
1. Bureau of Licensing andRegulation
2. Bureau of Food and Drugs3. Bureau of Research and
Laboratories
4. National Quarantine Office
1. Bureau of Health Facilities and Services
2. Bureau of Food and Drugs
3. Bureau of Health Devices and Technology
4. Bureau of Quarantine and International HealthSurveillance
5. Bureau of International Health Cooperation
6. Bureau of Local Health Development
7. National Epidemiology Center
8. National Center for Disease Prevention andControl
9. National Center for Health Promotion
10. National Center for Health Facility Development
11. Health Policy Development and Planning Bureau
12. Health Human Resource Development Bureau
28
-
8/19/2019 DOH Reengineering Monograph
29/175
The following Table 5 identifies the five new services headed by a Director III. All the
previous 25 services and staff offices are deemed abolished or integrated into the
newly created bureaus, national centers and services.
TABLE 5 – SERVICE LEVEL OFFICES
Offices Headed by Director III - Central Office
Existing Under EO 119 Created Under EO 102
1. Maternal and Child Health Service 1. Administrative Service
2. Tuberculosis Control Service 2. Information Management Service
3. Family Planning Service 3. Finance Service
4. Environmental Health Service 4. Procurement and Logistics Service
5. Nutrition Service 5. Health Emergency Management Staff
6. Dental Health Service
7. Malaria Control Service
8. Schistosomiasis Control Service
9. Communicable Disease Control Service
10. Non-communicable Disease ControlService
11. Hospital Operations and ManagementService
12. Radiation Health Service
13. Hospital Maintenance Service
14. Health Infrastructure Service
15. Community Health Service
16. Public Information and Health EducationService
17. Health Intelligence Service
18. Internal Planning Service
19. Foreign Assistance Coordination Service
20. Administrative Service
21. Finance Service
22. Management Advisory Service
23. Health Manpower Development andTraining Service
24. Procurement and Logistics Service
25. Biologicals Production Service
29
-
8/19/2019 DOH Reengineering Monograph
30/175
◘ Staff ing Shift
The changes in the structure and the
organizational composition of the DOH
necessitate corresponding changes in
staffing.
Guiding Principles - The
determination of staffing requirements,
position allocation and classification
under the proposed set-up considered
the following factors:
1. Adopt standard staffing pattern as
much as possible for similar units
or posts.
2. Emphasize technical over non-
technical positions consistent with
the redirected functions of the
DOH.
3. Expand the number of positions
charged with substantive functions
and compress positions performing
activities that may be purchasedfrom the private sector.
4. Adopt generic nomenclatures for
positions to accommodate more
professions and disciplines in the
roster of personnel.
Staffing Scheme - The
preparation of the staffing pattern
involved careful deliberations and
selection of the appropriate number and
competencies of the positions proposed.
The proposal assumed a phased
implementation scheme as follows:
1. Stage 1 proposed staffing pattern
includes co-terminus (CT) positions
(i.e., CT/co-terminus with
incumbent (CTI) positions). This
will be the operational staffing
pattern in the course of RSP
implementation.
2. Stage 2 proposed staffing pattern
excludes co-terminus positions
(i.e., without CT/CTI). This will be
the staffing pattern upon full
implementation of the RSP.
In effect, Stage 1 shall serve, as the
interim or transition stage while Stage 2
will be the final stage when RSP is fully
implemented.
For Stage 1, proposed positions were
matched with existing positions with the
same or higher salary grades. This
resulted in the transitory provision of co-
terminus positions in the interim stage.
Also, this meant that the implementation
of the ideal or full staffing pattern (i.e.,
with proposed needed positions) would
be deferred until such time that certain
posts are vacated and resources
generated to fund the desired staffing
changes.
This scheme was resorted to in order to
reconcile two conflicting objectives: (1)limiting funding to existing personnel
services appropriations and (2) providing
a long-term view of the staffing
requirements of a reengineered DOH.
3
-
8/19/2019 DOH Reengineering Monograph
31/175
Moreover, the two-stage implementation
takes into consideration that this
reengineering may have uncovered
redundancies which, for humanitarian
reason will simply be the subject of
deployment with abolition to take place
upon retirement, transfer or promotion,
or resignation of the incumbent,
whichever comes first.
It will also be noted that while around
half of central office staff would be
deployed, these numbers in fact went to
field offices as well as hospitals, which
suffer from chronic personnel shortage.
Also, bureaus and attached corporations
that have been given additionalmandates of new laws were recipients of
deployed positions, mitigating in the
meantime, the creation of new positions.
To minimize staffing problems, the DOH
has chosen to implement its RSP using a
number of interventions. At the onset, it
asked its employees to register for
voluntary deployment to any of its
regions, hospitals or attached agencies
that have sought Department of Budget
and Management (DBM) approval for the
creation of new positions.
In the meantime, it met with central
office staff and other constituencies to
configure the ideal CO structure. Those
who did not volunteer for deployment to
any agency of their choice would
eventually be subject to mandatory
deployment to offices that are in need of
personnel. In any case, there would be
no instance of any demotion in rank,
salary or emoluments subject to existing
CSC guidelines and standards.
Staffing Modification - Some
proposals called for a reclassification of
existing position titles to conform to the
new functions of the DOH. Some
positions were also identified as co-terminus with the incumbents and will
either be abolished or downgraded to its
appropriate rank when the incumbents
retire, resign, transfer or get promotion.
Standard Staffing Pattern - Standard staffing patterns were adopted
for the offices of the Undersecretary,
Assistant Secretary, Bureau Director or
equivalent and Service Director or
equivalent. A standard staff complement
adapted for specific offices are as
follows:
Office of the Undersecretary
1. Undersecretary
2. Executive Assistant IV
3. Administrative Officer II
4. Private Secretary II
5. Computer Operator IV
6. Clerk III
7. Chauffeur I
8. Utility Worker I
Office of the Assistant Secretary
1. Assistant Secretary
2. Executive Assistant III
3. Computer Operator III
4. Private Secretary I
5. Clerk II
6. Driver II
7. Utility Worker I
31
-
8/19/2019 DOH Reengineering Monograph
32/175
The staff complement for the Offices of the Director IV and the Offices of the Director
III at the central office were also standardized as follows:
Office of the Bureau Director
1. Director IV
2. Administrative Officer II
3. Computer Operator II
4. Driver II
Office of the Service Director
1. Director III
2. Administrative Officer I
3. Computer Operator II
4. Driver I
Salary Grade Structure - The
staffing pattern improved the quality of
positions in the DOH towards higherand more substantive posts compared
to administrative/routinary posts in
keeping with the leadership role of
DOH in the health sector. Table 6
shows that there is more technical staffcompared to administrative staff.
TABLE 6 – SUMMARY OF POSITIONS BY OFFICE AND CLASSIFICATION
TECHNICAL STAFF VS. ADMINISTRATIVE SAFF
POSITION CLASSIFICATION TOTALOFFICE
Technical Staff
(SG 11 & Above)
Administrative Staff
(SG 10 & Below)
TOTAL 850 449 1299
Office of the Secretary 78 42 120
OSEC Proper 25 13 38
Office of the Undersecretaries 18 12 30
Office of the Asst. Secretaries 16 12 28
Health Emergency Management Staff 13 3 16
Phil. National AIDS Council 6 2 8
Health Regulation Cluster 355 184 539
Bureau of Health Facilities & Services 56 20 76
Bureau of Food and Drugs 249 147 396
Bureau of Health Devices & Technology 50 17 67
External Affairs Cluster 91 100 191
Bureau of Quarantine & Int’l Health
Surveillance
45 93 138
Bureau of Int’l Health Cooperation 25 3 28
Bureau of Local Health Development 21 4 25
32
-
8/19/2019 DOH Reengineering Monograph
33/175
POSITION CLASSIFICATION TOTALOFFICE
Technical Staff
(SG 11 & Above)
Administrative Staff
(SG 10 & Below)
Health Program Development Cluster 179 41 220
National Epidemiology Center 30 8 38
National Center for Disease Prevention
& Control
73 11 84
National Center for Health Promotion 31 17 48
National Center for Health Facility
Development
45 5 50
Sectoral Support Cluster 53 18 71
Health Human Resource Development
Bureau
23 9 32
Health Policy Development and
Planning Bureau
30 9 39
Management Support Cluster 94 64 158
Administrative Service 20 19 39
Information Management Service 38 11 49
Finance Service 22 13 35
Procurement and Logistics Service 14 21 35
33
-
8/19/2019 DOH Reengineering Monograph
34/175
◘ Resource Allocation Shift
The changes in the structure and staffing
pattern of the DOH effected
corresponding changes in resourceallocation particularly for Personal
Services (PS). Guided by the principle
that the reengineered DOH shall have a
personnel budget that does not exceed
the existing PS allocation, the estimated
PS cost (which only covers basic salary)under the EO 119 and the EO 102
organizational structures are compared
in Table 7.
TABLE 7 – COMPARISON OF PS REQUIREMENTS OF STAFFING PATTERN
UNDER EO 119 AND EO 102 DOH ORGANIZATIONAL STRUCTURE
EO 119 EO 102(Transition stage) *
EO 102(Final stage)**
Offices Required No. of Staff Required No. of Staff RequiredNo. ofStaff
PS under EO102(a)
PS under EO102(a)
PS
Office of the Secretary 309 44,945,376 38 4,013,002 37 3,874,185
Executive Offices 99 13,640,652 58 7,763,256 52 6,849,791
Sectoral Support Cluster 82 9,023,868 87 9,720,648 88 9,809,317
Management SupportCluster
637 66,605,599 159 19,119,021 158 19,030,352
Health Regulation Cluster 509 64,526,800 539 44,644,198 539 44,644,198
External Affairs Cluster 350 32,879,640 191 19,012,176 191 19,012,176
Health ProgramDevelopment Cluster
964 128,926,320 220 23,789,024 218 23,494,058
TOTAL 2,950 360,548,255 1,292 128,061,325 1,283 126,557,928
* Stage I – staffing pattern includes positions, which are co-terminus with incumbent holderof positions (CTI)
** Stage II – staffing pattern upon full implementation of RSP Stage 1, which excludes CTIpositions
(a) Excludes staff of Philippine National AIDS Council
34
-
8/19/2019 DOH Reengineering Monograph
35/175
As shown in Table 7, the PS requirement of the staffing complement of the DOH central
office under EO 119 amounts to P360.5M. Under the transition phase of Stage 1, PS
requirement amounts to P128M. This reduces PS allocation by about 64 percent. In the
final phase of Stage 1, when all the CTI positions have been vacated, an additional
savings amounting to P1, 5M shall be generated.
Phase 1 of the reengineering process immediately generated an estimated savings of
about P56, 754,132. This is broken down as follows:
Direct savings from abolition of vacancies - P15, 000,000
Indirect savings from the deployment of
positions to units created by
special laws
Renationalized hospitals P15, 908,562
PITAHC 17, 514,390
PNAC 1, 233,648
BFAD Satellite Labs
CHD VII 3, 617,356
CHD XI 3, 480,176
TOTAL P56, 754,132
As a result of the proposed staffing changes, there is also a corresponding change in the
budget format and in the program/project/activity (P/P/A) language in the General
Appropriations Act. This simplifies account/item entries in the GAA in consonance with
the HSR objectives.
35
-
8/19/2019 DOH Reengineering Monograph
36/175
M A N A G I N G T H ER E F O R M P R O C E S S
Chapter
2
◘ Management of Change and Expectations
Managing change at the DOH is a daunting proposition. While any kind of
change is expected to meet some measure of resistance, the situation at the
DOH was aggravated by a number of factors.
The first one had to do with RA 7160 or the Local Government Code (LGC).
Implemented in 1992 after its passage in 1991. RA 7160 succeeded in shifting almost
46,000 DOH personnel to LGUs all over the country. This left a still substantial number
of over 27,262 personnel under the DOH national payroll as of December 31, 1999. This
was an awkward situation considering that direct service delivery, which is supposed to
be the more people-intensive part of the DOH functions had already been devolved.
The DOH pre-devolution structure remained untouched, perpetuating practices and
procedures that should have changed with the downloading of the DOH’s service
delivery function. Since form usually defines function, the unchanged DOH structure
continued to operate on old premises. The remaining employees have been led tobelieve that the status quo would remain and that, for the most part, their respective
assignments and responsibilities would not change significantly. This mindset resulted
from failed attempts to restructure the DOH after the enactment of the LGC.
The second factor had to do with the enactment of the Magna Carta for Public Health
Workers or RA 7305. Among others, this law mandates that health workers cannot be
transferred to another station or place of work without their consent. This further
solidified the perception that reorganization would no longer take place, even if the
bureaucracy at the national level remained at levels that were difficult to justify.
The previous experience of devolved employees constitute another source of resistance
by the remaining employees to any form of movement, even if this is merely de-
concentration or movement within the same organization.
36
-
8/19/2019 DOH Reengineering Monograph
37/175
There are more than enough stories of
health workers who, under devolution,
were designated to do jobs other than
what they were trained for; who were
demoted in pay or rank even if this was
explicitly prohibited by existing laws;
who experienced difficulties in the
payment of retirement benefits and who
had to work with local officials whose
priorities did not include health care in
the volume and value attributed to the
earlier national health service delivery
system. Those who thought themselves
lucky to have stayed with the national
government swore that they would not
allow themselves to be caught in a
similar situation in the future.
The growing militancy of government
workers has not spared the DOH. Some of
its employees are allied with the more
militant labor federation and are not
beyond using their network to lobby and
advocate for the maintenance of existing
rights or to protest perceived diminution
of benefits. They are joined by a group
of middle managers and seniorexecutives whose positions may be
deactivated with the shift to a function-
focused CO as opposed to the existing
disease-specific and sector-based
structure.
What was also being questioned is the
authority of the President to effect a
reorganization of specific executive
departments in the absence of any
legislation from Congress. It is held by
some that the authority to reorganize is
an inherent function of Congress and may
not be exercised by any other. Thus, a
reorganization covered by an executive
order may not be carried out without the
risk of being declared void by the proper
courts.
Any change management plan must
address these factors if it is to achieve
some measure of success. It must be
pointed out that while there may be
hindering factors to the change process
that accompanies a reorganization or
reengineering effort at the DOH, there
are also assisting factors that could be
put to work. For instance, the senior
management levels of the DOH are all
“old hands”, so to speak.
Three of the undersecretaries are CareerExecutive Service Officers (CESOs) who
are unlikely to be dislocated by any
reengineering effort. The other
undersecretary and the Secretary of
Health himself were former DOH
officials, serving as Head Executive
Assistant and Assistant Secretary,
respectively during an earlier period. In
terms of understanding the functions,
the structures and the needs of the
organization, they are considered
knowledgeable insofar as the needed
internal reforms are concerned.
There was also some realization that the
previous structure was not working very
well for the immediate as well as the
ultimate clients of the DOH are
concerned. A proposed bill in Congress
seeks the abolition of the DOH regional
units on the perception that these DOH
field offices presently do not serve the
LGUs as well as they should. Seen in this
light, the reengineering of the DOH
became a matter of institutional
survival.
37
-
8/19/2019 DOH Reengineering Monograph
38/175
A number of laws recently passed also
provided for the staffing of new agencies
such as the Voluntary Blood Donation
Program, the Philippine National AIDS
Council, the Philippine Institute of
Traditional and Alternative Health Care,
as well as the increased staffing
requirement of the PhilHealth and the
newly renationalized hospitals.
Since the major shift in the DOH
reengineering is in the thinning out of CO
and building organizational muscle in the
field and operating units such as the
retained as well as the special and
specialty hospitals, dislocations were
minimized by deploying CO personnel to
the new agencies, the field offices and
the operating units.
What also became imminent and
necessary is the retooling and retraining
program, given the new or additional
skills that are required at CO as well as
in the field and the operating units. The
DOH management recognized this and
has in fact allocated funds for this
purpose.
38
-
8/19/2019 DOH Reengineering Monograph
39/175
RR SS PP II mm pp ll ee mm ee nn tt aa tt ii oo nn :: Part1 TT hh ee DD OO HH EE xx pp ee rr ii ee nn cc ee
V arious working groups and committees were created through Department OrderNo. 380-D s. 1999 to affect a unified, smooth process of facilitating the
formulation of the RSP and of implementing change. These groups and
committees were:
Oversight Committee – Provided the
overall direction of the change program.
This committee was composed of the
Health Secretary, Undersecretaries and
Assistant Secretaries.
Reengineering Secretariat –
Provided the staff support to the
Oversight Committee and was
responsible for facilitation, coordination
and provision of technical assistance in
the change program and activities of all
offices in the CO, including the BFAD and
the NQO. A full-time Director under the
Office of the Secretary and a select staff
from the Health Policy Development
Staff and the Administrative Service
composed this group. A major
consideration in the selection of
membership to this group was their
commitment and willingness to work for
change.
Task Force on Personnel
Deployment and Budgetary
Requirements – This group was
organized on account of the inevitabledeployment of some CO personnel. This
group was tasked with the processing of
requests for voluntary deployment,
retirement and separation from office of
those affected by the reengineering
program. Aside from determining the
cost requirements and ensuring financial
resource, it was also responsible for the
development of integration programs for
the deployed personnel in the other DOHoffices.
Task Force on Information and
Communication – This group
developed helpful messages and
information to facilitate the wide
acceptance of the change process; and
disseminated information relative to
activities and programs of the different
committees involved in the DOH
reengineering.
Task Force on Retooling and
Counseling – This group conducted
orientation programs on the rationale
and need for change in the early stages
of the change process. The group
provided emotional support to those who
suffered from the stress brought about
by the organizational change. Prior to
the actual implementation of the neworganizational structure, this group
formulated a retooling/retraining
program that ensured that newly
organized offices and staff measure up to
the expectations of the new roles and
39
-
8/19/2019 DOH Reengineering Monograph
40/175
functions of the DOH. The training
programs were designed for building
capacities for leadership in the health
sector and in support of the HSRA
implementation.
The Reengineering Desk – This washeaded by an Assistant Secretary and
was created primarily for “quick
response” to most of the commonly
asked questions about reengineering.
The group also helped in facilitating
several types of requests from affected
employees such as deployment and
transfer, counseling, retraining among
others.
Three consultants were hired for the
duration of the reengineering exercise in
the CO. They played a significant role in
the formulation and implementation of
the DOH Rationalization and Streamlining
Plan. They acted as a technical resource
in the day-to-day management of
change. In the process, some problems
cropped up with no answers from the
book, but were drawn from experience
and practice. The consultants provided
insights and direction during the change
process.
4
-
8/19/2019 DOH Reengineering Monograph
41/175
The Change Management Process
To support the reengineering process,
the DOH Reengineering Technical
Committees and Secretariat carefullystudied and reviewed other guidelines
issued by the CSC and those enacted by
law, such as RA 6656 or An Act to Protect
the Security of Tenure of Civil Service
Officers and Employees in the
Implementation of Government
Reorganization (1988).
The basis of action and decision made by
the Selection and Placement and Appeals
committees for the implementation of
the approved reengineered DOH was
grounded on these rules and provisions.
The appeals made by protesting
employees also found strength and
support from these provisions.
The following were the activities and
mechanisms that facilitated or mitigated
the effects of the organizational change
process:
1. The Secretary of Health clarified
intentions and directions to the
undersecretaries and assistant
secretaries who acted as the
Oversight Committee and as team
leaders for their respective groups.
2. The Undersecretaries explained
intention and direction of
reorganization to units, agencies,
or bureaus in her/his cluster;
reviewed mandate given under EO
102 and the HSRA; and
documented frequently asked
questions for discussion and
feedback to the Executive
Committee (Execom) or Oversight
Committee.
3. The Secretary of Health
established the Reengineering Desk
headed by an Assistant Secretary
and backstopped by a Technical
Working Group or Secretariat
headed by a Director and
consultants coordinating with
several Task Forces which, sought
clearance from Execom or
Oversight Committee.
4. The Secretary of Health issued
guidelines for reengineering and
retooling. These are:
a. All DOH employees are
expected to be computer
literate thus minimizing the
need for clerical and
secretarial support.
b. CO staff must be retooled for
policy analysis, program
development, resource
coordination, mobilization and
technical supervision.
c. Field Unit staff must be
retooled for networking,
developing linkage, political
sensitivity, grassroots planning,grants administration and
technical assistance.
d. Hospital staff must be retooled
towards integrating public
41
-
8/19/2019 DOH Reengineering Monograph
42/175
health concepts and issues
with clinical care.
e. DOH representatives to LGUs
must be retooled to respond to
LGU needs and not merely to
attend Local Health Board
meetings. They must also be
retooled as local health
advisors on all matters relating
to health.
5. The Secretary of Health issued
guidelines on managing the
reengineering process. These are:
a. DOH managers and senior
officials must present
themselves at all times to
answer all questions about
reorganization honestly and
without equivocation. Those
issues about which officials
were unsure or unhappy about
were brought to the
Execom/Oversight Committee
for quick resolution.
b. The central message was that
even with redeployment, the
DOH remains a family.
Whether one is in the CO, the
regions or any of the hospitals,
one continues to be part of
DOH whose services can be
counted towards retirement
and where security of tenure,
given adequate behavior andperformance, remains assured.
c. Success stories on
redeployment should be
documented and disseminated.
Problems encountered should
similarly be documented and
addressed operationally. An
example was the inability of
the redeployed person to get
his salary as soon as possible.
Another problem was the
unwillingness of the regions to
advance the salary despite
order from the Secretary.
d. Frequently asked questions
should be documented and the
answers to these questions
should be consistent and
widely distributed.
e. Unresolved issues such as
staffing numbers or position
titles were not disseminated
until approved by the
Secretary to prevent
unwarranted speculation. The
only certain thing about the
reengineering exercise is that
nobody will lose his/her job.
f. Alternatives to redeployment
were clearly presented.
Among these are:
Employment in DOH-attached
agencies where additional
staffs are mandated by law but
has not been approved or
confirmed by DBM. Examples
of these are PNAC, PITAHC and
NVBDP.
Redeployment was also made to
special, specialty and retained
hospitals in Metro Manila during
the voluntary deployment
42
-
8/19/2019 DOH Reengineering Monograph
43/175
period. When the staffing
pattern is approved, the
Secretary reserves the right to
re-deploy personnel where they
are most needed.
Retirement or separation
benefits (for those not yet
qualified to retire) were made
available under existing laws.
The reengineering team
deployed available personnel
who computed the amount of
these benefits for specific
employees.
The assistance of DOLE and CSCwere sought relative to job
hunts, both within government
itself (in case employees want to
transfer to other government
agencies) and outside the
country. A job fair put together
overseas, government and
within-DOH jobs that highlighted
other options available to
employees who did not wis