CHAPTER 13 Arrhythmias in acute heart failure
630
Transcript of CHAPTER 13 Arrhythmias in acute heart failure
-
Managing AcuteDecompensated Heart Failure
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page i
-
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page ii
-
Managing AcuteDecompensated Heart Failure
Editors
Christopher M. OConnor MD, FACP, FACCProfessor of Medicine
Duke University Medical CenterDurham, North Carolina, USA
Wendy Gattis Stough PharmDAssistant Clinical Professor in Medicine
Duke University Medical CenterDurham, North Carolina, USA
Mihai Gheorghiade MD, FACCProfessor of Medicine
Northwestern UniversityChicago, Illinois, USA
Kirkwood F. Adams Jr. MDAssociate Professor of Medicine and Radiology
The University of North Carolina School of MedicineChapel Hill, North Carolina, USA
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page iii
-
2005 Taylor & Francis, an imprint of the Taylor & Francis Group
First published in the United Kingdom in 2005 by Taylor & Francis, an imprint of the Taylor & Francis Group, 2Park Square, Milton Park, Abingdon, Oxon OX14 4RN
Tel.: +44 (0)20 7017 6000Fax.: +44 (0)20 7017 6699E-mail: [email protected]: http://www.tandf.co.uk/medicine
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, inany form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the priorpermission of the publisher or in accordance with the provisions of the Copyright, Designs and Patents Act 1988or under the terms of any licence permitting limited copying issued by the Copyright Licensing Agency, 90Tottenham Court Road, London W1P 0LP.
Although every effort has been made to ensure that all owners of copyright material have been acknowledged inthis publication, we would be glad to acknowledge in subsequent reprints or editions any omissions brought to ourattention.
A CIP record for this book is available from the British Library.
Library of Congress Cataloging-in-Publication Data
Data available on application
ISBN 1 84184 374 1ISBN 978-1-84184-374-2
Distributed in North and South America by
Taylor & Francis2000 NW Corporate BlvdBoca Raton, FL 33431, USA
Within Continental USATel: 800 272 7737; Fax: 800 374 3401Outside Continental USATel: 561 994 0555; Fax: 561 361 6018E-mail: [email protected]
Distributed in the rest of the world byThomson Publishing ServicesCheriton HouseNorth WayAndover, Hampshire SP10 5BE, UKTel.: +44 (0)1264 332424E-mail: [email protected]
Composition by Phoenix Photosetting, Chatham, KentPrinted and bound in Great Britain by CPI, Bath
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page iv
-
Contents
Acknowledgement ix
Contributors xi
Foreword xixRobert M Califf, Robert O Bonow
Color plate section
Part I: Epidemiology and Pathophysiology
1 The history of acute heart failure management: how far have we come? 3Hector O Ventura, Mandeep R Mehra
2 Acute heart failure: nomenclature, pathophysiology, and outcome measures 19Gadi Cotter, Wendy Gattis Stough, G Michael Felker, Eric J Velazquez, Adrian F HernandezJoseph G Rogers, Mihai Gheorghiade, Kirkwood F Adams, Jr, Christopher M OConnor
3 Clinical profile of the acute heart failure patient 39Gregg C Fonarow, Kirkwood F Adams, Jr
4 Sex-related differences in heart failure 53Jalal K Ghali
5 Heart failure in the elderly 71Jalal K Ghali, Dalane W Kitzman
6 Pathophysiology of the spectrum of acute heart failure: de novo heart failure, 87decompensated heart failure, and advanced refractory heart failureGary S Francis, W H Wilson Tang, Kirkwood F Adams, Jr
7 Diastolic heart failure: diagnosis, prognosis, and treatment 95Michael R Zile, Carson S Webb, Catalin F Baicu
8 Pathophysiology of the cardiorenal syndrome in acute heart failure 113Guido Boerrigter, John C Burnett, Jr
Part II: Diagnosis and Evaluation of the Acute Heart Failure Patient
9 Evaluation of the acute heart failure patient: assessment of dyspnea and 127other physical examination parametersJohn R Teerlink, Mark H Drazner
v
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page v
-
10 Biologic markers in acute heart failure 151G Michael Felker, Adrian F Hernandez, Alan Maisel
11 Noninvasive diagnostic evaluation of the acute heart failure patient with 165systolic dysfunction: focus on the electrocardiogram and chest x-rayJason N Katz, Robert C Kowal, Mark H Drazner
12 Noninvasive hemodynamic monitoring of the acute heart failure patient 179Clyde Yancy
Part III: Comorbidities in the Acute Heart Failure Patient
13 Arrhythmias in acute heart failure 193William G Stevenson
14 Mechanical complications of acute decompensated heart failure 209William B Haynos, Ron M Oren
15 Cardiogenic shock 221Gadi Cotter, Olga Milo-Cotter, Edo Kaluski
16 Hypertension in acute decompensated heart failure 241Alan B Miller, Jun R Chiong
17 Psychiatric and psychosocial risks in acutely decompensated chronic heart 253failure patientsWei Jiang, Christopher M OConnor, Ranga R Krishnan
18 Anemia in acute and chronic heart failure 273G Michael Felker, Kirkwood F Adams, Jr
19 Acute pulmonary embolism 285Victor F Tapson
20 The role of myocardial ischemia in acute decompensated heart failure: 301diagnostic and management considerationsJamieson M Bourque, Eric J Velazquez, Christopher M OConnor
Part IV: Treatment Strategies
21 Treatment of acute heart failure in patients with preserved systolic function 325Marvin W Kronenberg
22 Inotropes and other new therapies for acute heart failure 339G Michael Felker, Mihai Gheorghiade
vi
Contents
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page vi
-
23 Diuretics and newer therapies for sodium and edema management in 349decompensated heart failureRobert J Cody
24 Contemporary aspects of intravenous vasodilator therapy with nesiritide or 361nitrates in acute heart failureKirkwood F Adams, Jr
25 Pacing therapy for acute decompensated heart failure 371Aysha Arshad, Shahriar Iravanian, Jonathan S Steinberg
26 Implantable cardioverter defibrillators and biventricular devices in 387acute heart failureSana M Al-Khatib
27 Intraaortic balloon pumps in acute heart failure 403David Bragin-Snchez, Patricia P Chang, E Magnus Ohman
28 Ultrafiltration as a therapy for acute heart failure 415Jonathan D Sackner-Bernstein, Maurizio Porcu, Rimbida Obeleniene
29 Mechanical circulatory support for acute heart failure 429Ashish S Shah, Carmelo A Milano
30 Left ventricular reconstruction for ischemic failing ventricle 443Vincent Dor
31 The Acorn Cardiac Support Device as a therapy for heart failure 453Hani N Sabbah, Elaine J Tanhehco, Victor G Sharov, Robert Brewer, Norman A Silverman
32 The role of continuous positive airway pressure in the management of 461decompensated heart failure complicated by acute pulmonary edemaMichael D Faulx, Mark E Dunlap
33 Exercise training in advanced heart failure: a need for more data 469Ileana L Pia, David J Whellan, Christopher M OConnor
34 Calcium sensitizers in acute heart failure 479John G F Cleland, Krishna M Lalukota, Anne-Marie Seymour
35 Vasopressin antagonists 497Cesare Orlandi, Wendy Gattis Stough, Christopher M OConnor, Kirkwood F Adams, Jr, Mihai Gheorghiade
36 Endothelin receptor antagonists in the treatment of acute heart failure 503John R Teerlink, Christopher M OConnor
vii
Contents
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page vii
-
Part V: Issues in the Management of Acute Heart Failure
37 Advanced nursing aspects of acute heart failure 523Laura H Gaulden, Jana Glotzer
38 The role of the pharmacist in caring for patients with acute heart failure 529Wendy Gattis Stough, J Herbert Patterson
39 Economics and quality of life in the advanced heart failure patient 535David J Whellan, Jonathan E E Yager, Jolle Y Friedman, Kevin A Schulman
40 Disease management in the advanced heart failure patient 555David J Whellan
41 End-of-life care in the acute heart failure patient 569Cheryl H Zambroski, Lynn P Roser, Debra K Moser
viii
Contents
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page viii
-
Acknowledgement
The editors acknowledge Deana Betterton-Lewis for her dedicated editorial work on this textbook.
ix
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page ix
-
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page x
-
Contributors
xi
Kirkwood F Adams, Jr MDAssociate Professor of Medicine and RadiologyDirector, UNC Heart Failure ProgramDivision of CardiologyThe University of North Carolina School of
MedicineChapel Hill, North CarolinaUSA
Sana M Al-Khatib MD, MHS, FACCAssistant Professor of MedicineDepartment of Medicine/Division of CardiologyDuke University Medical CenterDuke Clinical Research InstituteDurham, North CarolinaUSA
Aysha Arshad MBBS, FACCAttending Electrohysiologist, St Lukes-Roosevelt
Hospital CenterAssistant Professor of Medicine, Columbia
University College of Physicians and SurgeonsDivision of Cardiology, St Lukes-Roosevelt
Hospital CenterNew York, New YorkUSA
Catalin F Baicu PhDAssistant Professor of MedicineDivision of CardiologyDepartment of MedicineUniversity of South CarolinaCharleston, South CarolinaUSA
Guido Boerrigter MDInstructor in MedicineDivision of Cardiovascular DiseasesMayo Clinic and Mayo Clinic College of MedicineRochester, MinnesotaUSA
Jamieson M Bourque MD, MHSResearch AssociateDepartment of Internal MedicineDuke University Medical CenterDurham, North CarolinaUSA
David Bragin-Snchez MDCardiomyopathy and Cardiac Transplant
CardiologistCardiovascular Center of Puerto Rico and the
CaribbeanSan Juan, Puerto RicoUSA
Robert Brewer MDSenior Cardiothoracic SurgeonDivision of Cardiothoracic SurgeryHenry Ford Health SystemDetroit, MichiganUSA
John C Burnett, Jr MDProfessor of Medicine and PhysiologyDivision of Cardiovascular DiseasesMayo Clinic and Mayo Clinic College of MedicineRochester, MinnesotaUSA
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xi
-
Patricia P Chang MD, MHS, FACCAssistant ProfessorDirector, Cardiomyopathy and Transplant
ServiceDivision of Cardiology, Department of
MedicineThe University of North Carolina at
Chapel HillChapel Hill, North CarolinaUSA
Jun Ratunil Chiong MDAssistant Professor of MedicineUniversity of FloridaDivision of CardiologyJacksonville, FloridaUSA
John G F Cleland MD, FRCP, FACC, FESCProfessor of CardiologyDepartment of CardiologyUniversity of HullKingston-Upon-HullUK
Robert J Cody MDProfessor of Internal MedicineDivision of Cardiovascular MedicineUniversity of Michigan Health SystemAnn Arbor, MichiganUSA
Gadi Cotter MDAssistant Clinical Professor of MedicineDepartment of Medicine/Division of Clinical
PharmacologyDuke University Medical CenterDurham, North CarolinaUSA
Vincent Dor MDProfessor of Cardiothoracic SurgeryCentre Cardio-Thoracique de MonacoMonaco
Mark H Drazner MD, MScMedical Director, Parkland Memorial Hospital
CHF ClinicAssociate Professor of MedicineDonald W Reynolds Cardiovascular Clinical
Research CenterDivision of Cardiology, University of Texas
Southwestern Medical CenterDallas, TexasUSA
Mark E Dunlap MDDirector, Heart Failure Program and Associate
Chief of CardiologyLouis B Stokes Veterans Affairs Medical CenterAssociate Professor of Medicine, Physiology and
BiophysicsCase Western Reserve UniversityCleveland, OhioUSA
Michael D Faulx MDChief Fellow, CardiologyUniversity Hospitals of ClevelandCase Western Reserve UniversityCleveland, OhioUSA
G Michael Felker MD, MHSAssistant Professor of MedicineDivision of CardiologyDuke University Medical CenterDurham, North CarolinaUSA
Gregg C Fonarow MDProfessor of Medicine, UCLA Division of
CardiologyThe Eliot Corday Chair in Cardiovascular
Medicine and ScienceDirector, AhmansonUCLA Cardiomyopathy
CenterUniversity of California Los AngelesLos Angeles, CaliforniaUSA
xii
Contributors
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xii
-
Gary S Francis MDProfessor of MedicineLerner College of Medicine of Case Western
Reserve UniversityCleveland Clinica FoundationCleveland, OhioUSA
Jolle Y Friedman MPAProject LeaderCenter for Clinical and Genetic EconomicsDuke Clinical Research InstituteDuke University Medical CenterDurham, North CarolinaUSA
Laura H Gaulden RN, MSN, ANPClinical Operations DirectorDuke Heart Failure ProgramDuke University Medical CenterDurham, North CarolinaUSA
Jalal K Ghali MDProfessor of MedicineAssociate Director, Cardiology SectionDirector, Heart Failure and Cardiovascular
Research ProgramLouisiana State University Health Sciences
CenterShreveport, LouisianaUSA
Mihai Gheorghiade MD, FACCProfessor of MedicineAssociate Chief of CardiologyNorthwestern University, Feinberg School of
MedicineChicago, IllinoisUSA
Jana Glotzer RN, MSN, CCRN, ACNP, CHFAcute Care Nurse PractionerUNC Heart Failure ProgramThe University of North Carolina at Chapel HillChapel Hill, North CarolinaUSA
William B Haynos MDHeart Failure Treatment ProgramDepartment of Internal Medicine, Roy J Carver
College of MedicineThe University of IowaIowa City, IowaUSA
Adrian F Hernandez MDAssistant Professor of MedicineDivision of CardiologyDuke University Medical CenterDurham, North CarolinaUSA
Shahriar Iravanian MDMedicine Resident, St Lukes-Roosevelt Hospital
CenterDivision of Medicine, St Lukes-Roosevelt
Hospital CenterNew York, New YorkUSA
Wei Jiang MDAssistant Professor of Medicine, Psychiatry and
Behavioral ScienceDepartment of Internal Medicine, Psychiatry and
Behavioral ScienceDuke University Medical CenterDurham, North CarolinaUSA
Edo Kaluski MD, FACCDirector of the Coronary Care UnitAsaf Harofeh Medical CenterZrifin and The Sackler School of Medicine,
University of Tel AvivTel AvivIsrael
Jason N Katz MDChief Medicine ResidentDepartment of Internal MedicineUniversity of Texas Southwestern Medical CenterDallas, TexasUSA
xiii
Contributors
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xiii
-
Dalane W Kitzman MDProfessor of Internal MedicineSections of Cardiology and GeriatricsDirector of EchocardiographyWake Forest University School of MedicineWinston-Salem, North CarolinaUSA
Robert C Kowal MD, PhDElectrophysiologist, Clinical Associate Professor of
MedicineBaylor University Medical CenterUniversity of Texas Southwestern Medical CenterDallas, TexasUSA
Ranga R Krishnan MDProfessor and ChairmanDepartment of Psychiatry and Behavioral SciencesDuke University Medical CenterDurham, North CarolinaUSA
Marvin W Kronenberg MDProfessor of Medicine and RadiologyDivision of Cardiovascular MedicineDepartment of MedicineVanderbilt University School of MedicineNashville, TennesseeUSA
Krishna Lalukota MBBS, MRCPDepartment of CardiologyUniversity of HullKingston-Upon-HullUK
Alan S Maisel MDProfessor of MedicineUniversity of California, San DiegoDirector, Coronary Care Unit and Heart Failure
Research ProgramSan Diego VA Healthcare CenterSan Diego, CaliforniaUSA
Mandeep R Mehra MDVice Chairman, Department of Cardiovascular
MedicineMedical Director, Cardiomyopathy and Heart
Transplantation CenterOchsner Clinic FoundationNew Orleans, LouisianaUSA
Carmelo A Milano MDAssociate Professor of SurgeryDivision of Thoracic SurgeryDuke University Medical CenterDurham, North CarolinaUSA
Alan B Miller MDProfessor, Internal Medicine/CardiologyUniversity of FloridaJacksonville, FloridaUSA
Olga Milo-Cotter MDDurham, North CarolinaUSA
Debra K Moser DNSc, RN, FAANProfessor and Gill Chair of NursingUniversity of Kentucky, College of NursingLexington, KentuckyUSA
Rimbida Obeleniene MDDivision of CardiologySt Lukes-Roosevelt HospitalNew York, New YorkUSA
Christopher M OConnor MD, FACP, FACCProfessor of MedicineChief, Division of Clinical PharmacologyDirector, Duke Heart Failure ProgramDuke University Medical CenterDurham, North CarolinaUSA
xiv
Contributors
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xiv
-
E Magnus Ohman MD, FACCErnest and Hazel Craige Professor of
Cardiovascular MedicineChief of Division of CardiologyDepartment of Medicine/Division of CardiologyThe University of North Carolina at Chapel HillChapel Hill, North CarolinaUSA
Ron Oren MDProfessor of Clinical MedicineUniversity of IowaHeart Failure Treatment ProgramUniversity of Iowa Hospitals and ClinicsIowa City, IowaUSA
Cesare Orlandi MD, FACCVice President, Clinical DevelopmentOtsuka Maryland Research InstituteRockville, MarylandUSA
J Herbert Patterson PharmD, FCCP, BCPSAssociate Professor of Pharmacy and Research
Associate Professor of CardiologyUniversity of North Carolina at Chapel HillSchool of PharmacyDivision of Pharmacotherapy and Experimental
TherapeuticsChapel Hill, North CarolinaUSA
Ileana L Pia MD, FACCProfessor of MedicineSection of Medicine, Cardiology, Heart Failure
and Case Western Reserve UniversityLouis B Stokes Veterans Medical CenterFood and Drug Administration (FDA) ConsultantChair, Heart Failure Section, American Heart
AssociationCleveland, OhioUSA
Maurizio Porcu MDDirector, Division of Cardiology, Heart Failure
and Cardiac Transplant ProgramAzienda Ospedaliera G Brotzu San MicheleCagliariItaly
Joseph G Rogers MDMedical Director, Cardiac Transplant ProgramDepartment of Medicine/Division of CardiologyDuke University Medical CenterDurham, North CarolinaUSA
Lynn P Roser RN, MSNAssociate Professor of NursingBluegrass Community and Technical CollegeDoctoral Student, University of Kentucky College
of NursingLexington, KentuckyUSA
Hani N Sabbah PhD, FACC, FCCP, FAHAProfessor of Medicine and Director of
Cardiovascular ResearchDivision of Cardiovascular MedicineHenry Ford Health SystemDetroit, MichiganUSA
Jonathan D Sackner-Bernstein MDDirector, Clinical ResearchHeart Failure and Cardiomyopathy CenterNorth Shore University HospitalManhasset, New YorkUSA
Kevin A Schulman MDProfessor of MedicineCenter for Clinical and Genetic EconomicsDuke Clinical Research InstituteDuke University Medical CenterDurham, North CarolinaUSA
xv
Contributors
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xv
-
Anne-Marie Seymour PhDDepartment of Biological SciencesUniversity of HullKingston-Upon-HullUK
Ashish S Shah MDDivision of Thoracic SurgeryDepartment of General and Thoracic SurgeryDuke University Medical CenterDurham, North CarolinaUSA
Victor G Sharov MD, PhDSenior Staff InvestigatorDivision of Cardiovascular MedicineHenry Ford Health SystemDetroit, MichiganUSA
Norman A Silverman MDDivision Head, Cardiothoracic SurgeryDivision of Cardiothoracic SurgeryHenry Ford Health SystemDetroit, MichiganUSA
Jonathan S Steinberg MD, FACCChief, Division of CardiologyDirector, Arrhythmia Service St Lukes-Roosevelt
Hospital CenterProfessor of Medicine, Columbia University
College of Physicians and SurgeonsDivision of Cardiology, St Lukes-Roosevelt
Hospital CenterNew York, New YorkUSA
William G Stevenson MDAssociate Professor of MedicineHarvard Medical SchoolDirector, Clinical Cardiac Electrophysiology
ProgramBrigham and Womens HospitalBoston, MassachusettsUSA
Wendy Gattis Stough PharmDAssistant Clinical Professor in MedicineDepartment of MedicineDivision of CardiologyDuke University Medical CenterDurham, North CarolinaUSA
W H Wilson Tang MDAssociate StaffSection of Heart Failure and Cardiac Transplant
MedicineCleveland Clinic FoundationAssistant Professor in MedicineCleveland Clinic Lerner College of MedicineCleveland, OhioUSA
Elaine J Tanhehco PhDAssociate Staff InvestigatorDivision of Cardiovascular MedicineHenry Ford Health SystemDetroit, MichiganUSA
Victor F Tapson MDProfessor of Medicine, Pulmonary and Critical
Care MedicineDirector, Pulmonary Vascular Disease CenterDuke University Medical CenterDurham, North CarolinaUSA
John R Teerlink MD, FACC, FAHA, FESCAssociate Professor of MedicineDirector of Heart FailureSchool of Medicine, University of CaliforniaSection of Cardiology, San Francisco Veterans
Affairs Medical CenterSan Francisco, CaliforniaUSA
xvi
Contributors
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xvi
-
Eric J Velazquez MDAssistant Professor of MedicineDepartment of Medicine/Division of CardiologyDuke University Medical CenterDirector, Heart Failure ResearchDuke Clinical Research InstituteDurham, North CarolinaUSA
Hector O Ventura MDCardiomyopathy and Heart Transplantation
CenterOchsner Clinic FoundationClinical Professor of MedicineTulane University School of MedicineNew Orleans, LouisianaUSA
Carson S Webb MDCardiology FellowDivision of CardiologyDepartment of MedicineUniversity of South CarolinaCharleston, South CarolinaUSA
David J Whellan MD, MHSAsistant Professor of MedicineDirector of Clinical Trial Outcomes, Department
of MedicineDirector of Clinical Research, Jefferson Heart
InstituteJefferson Medical CollegeThomas Jefferson UniversityPhiladelphia, PennsylvaniaUSA
Jonathan E E Yager MDCardiology FellowDivision of CardiologyDuke University Medical CenterDurham, North CarolinaUSA
Clyde Yancy MD, FACC, FAHAProfessor of Internal Medicine/CardiologyCarl H Westcott Distinguished Chair in Medical
ResearchAssociate Dean of Clinical Affairs, St Paul
University HospitalMedical Director, Heart Failure/TransplantationUniversity of Texas Southwestern Medical CenterDallas, TexasUSA
Cheryl Hoyt Zambroski PhD, RNAssistant Professor of NursingUniversity of Louisville School of NursingLouisville, KentuckyUSA
Michael R Zile MDCharles Ezra Daniel Professor of MedicineDivision of CardiologyDepartment of MedicineUniversity of South CarolinaCharleston, South CarolinaUSA
xvii
Contributors
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xvii
-
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xviii
-
Foreword
In the past decade, a growing number of cardiologists have become concerned about the disparity in atten-tion to clinical trials and guidelines among the different presentations of cardiovascular disease. Duringthis time, the pattern of these discrepancies has become clear. For several decades, ST-segment-elevationacute myocardial infarction had been a focus of clinical trials, resulting in the entry of tens of thousandsof patients into randomized trials and, consequently, the establishment of effective therapies that havebecome standards of care. Similar activity occurred in the field of chronic heart failure, with the subse-quent definition of effective patterns of care based on evidence. In contrast, patients with non-ST-seg-ment-elevation acute coronary syndromes and acute heart failure, though seen in large numbers inpractice, were rarely entered into clinical trials.
Drs. OConnor, Stough, Gheorghiade, and Adams were key leaders in calling attention to the deficitof evidence for practice in caring for patients with acute heart failure, and this text is definitive proof ofthe success of their efforts. Through a series of meetings with thought leaders, government agencies, andleaders in the medical products industry, they have directed attention to the topic of acute heart failure.A similar effort has been underway for non-ST-elevation acute coronary syndromes, with similar results.In both areas, we can now rest assured that the clinical community is convinced of the importance of theproblem and the critical necessity of producing evidence through clinical trials and epidemiologicalstudies.
Beginning with the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations ofChronic Heart Failure (OPTIME-CHF) trial, a series of studies has now identified a variety of therapiesthat seem to have little to offer patients with acute heart failure. Other therapies are promisingbut asyet unprovenin the acute phase of heart failure. These trials have not only served the purpose ofinforming the practice community about therapies, but they have also refocused attention on the com-plexity of the pathophysiology and clinical epidemiology of acute heart failure.
This textbook begins, appropriately, with a definition of the problem, including its scope andepidemiology. The huge number of acute heart failure patients will seem startling to those who have notconsidered this issue before. However, practitioners who see patients in general medicine or cardiologypractice are aware of the onslaught of patients with this problem.
The book then moves on to common complications and comorbid conditions. Given the older age ofmost patients with acute heart failure, it is not surprising that understanding issues such as renalinsufficiency, respiratory insufficiency, diabetes, and stroke is so important in caring for these patients. Forthe most part, decision-making regarding mechanical complications and arrhythmias in the acute phaseof the heart failure admission remains an art rather than a science, but the growing volume of clinicalepidemiological studies is producing a clear picture of critical decision points that will be amenable todeveloping definitive evidence for practice.
The text then provides an in-depth review of the pharmacological therapy for acute heart failure. The
xix
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xix
-
lack of proven, effective medical therapies remains a major concern in this arena. Milrinone anddobutamine have fallen into disfavor due to negative or unfavorable studies, while many other medica-tions, such as nesiritide and endothelin antagonists, have shown promising but unproven benefit. Thegood news is that major clinical outcome studies are under way evaluating both of these exciting newtherapies.
A particularly interesting twist in this book is the focus on integrative care of the patient. The chapterson psychosocial aspects, nursing care, and disease management clarify many critical issues about the totalcare of the patient and family that are usually ignored or given short shrift in most medical textbooks.These chapters in particular represent the selfless manner in which OConnor, Stough, Gheorghiade, andAdams have developed teams dedicated to every aspect of the needs of patients with heart failure.
We hope that future editions of this book will document significant progress in the pursuit of evidenceupon which to base practice. It has been a pleasure to participate in the development of a new field ofcardiology with OConnor, Stough, Gheorghiade, and Adams. We hope that Managing AcuteDecompensated Heart Failure will become an essential companion to practitioners caring for patients withthis increasingly common, difficult, and fatal disease.
Robert M Califf, MD,Duke Clinical Research Institute,
Durham, NC
Robert O Bonow, MD,Northwestern Memorial Hospital,
Chicago, IL
July 2005
xx
Foreword
00-OConnor-Pre-cpp 29/7/05 11:26 AM Page xx
-
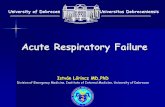
RA (LBBB) LV Paced Bi-V Paced
RV
LV
Figure 25.1. Electrical response with different pacing modes. Toprow: Electrical epicardial activation map of whole heart for threepacing modes. Activation time is color coded (blue early redlate). With right atrial (RA) pacing (left bundle branch block[LBBB]), electrical activation spreads from right to left, whereas LVpacing reversed the pattern but did not reduce conduction delay.Biventricular (BV) pacing, however, showed improved electricalsynchrony. Bottom row: Short-axis slice demonstrating thatactivation time at the endocardial septum was similar to that atepicardial electrodes over the same region. (With permission fromLeclercq et al.74)
43-O-Connor-Color-ppp 21/7/05 11:49 AM Page 1
-
Figure 29.4. The Thoratec extracorporealventricular assist device. (Reprinted with permissionfrom Thoratec Corporation.)
Figure 29.3. A newer paracorporeal device,compatible with the ABIOMED BVS 5000, theAB5000 circulatory support system eliminatesextensive blood tubing and may be less prone tothromboembolic complications
43-O-Connor-Color-ppp 21/7/05 11:49 AM Page 2
-
Figure 29.5. A newer console allows patientsgreater mobility and the potential for home discharge.(Reprinted with permission from ThoratecCorporation.)
Figure 29.6. The textured lining of the HeartMateventricular assist device generates a pseudointimallayer and contributes to decreased thromboemboliccomplications. (Reprinted with permission fromThoratec Corporation.)
43-O-Connor-Color-ppp 21/7/05 11:49 AM Page 3
-
Outflow Graft Flow Probe Outflow Graft Protector
MicroMed DeBakeyVAD Pump
Dacron coverControllerConnector
PercutaneousCable
Inflow Cannula
Sewing Ring
Figure 29.7. The MicroMed DeBakey ventricular assist device axial flow pump represents the nextgeneration in devices. These blood pumps are smaller, quiet and more efficient then previous devices. (Reprintedwith permission from MicroMed Technology, Inc.)
Figure 31.2. Top left: Trichrome stained section of left ventricular myocardium from a dog treated for 3months with the cardiac support device (CSD). The CSD is encapsulated by thin layers of mature connectivetissue (blue-green). There is a clear demarcation between the CSD and the myocardium (M, dark red) with noevidence of invasion of the myocardium by connective tissue. Top right: An epicardial artery (A) coursingbetween the CSD and the epicardial myocardium is normal in appearance. Bottom panels: Scanning electronmicrograph from a dog with heart failure treated for 3 months with the CSD. The micrograph depicts a singleCSD fiber consisting of multiple filaments, the adjacent connective tissue, underlying epicardial myocardiumand an epicardial artery (A) coursing between the CSD and the epicardial myocardium
43-O-Connor-Color-ppp 21/7/05 11:49 AM Page 4
-
PART I
Epidemiology and Pathophysiology
01-OConnor-01-cpp 21/7/05 12:20 PM Page 1
-
01-OConnor-01-cpp 21/7/05 12:20 PM Page 2
-
Introduction
Our understanding of the basic mechanisms asso-ciated with the development of heart failure andadvances in modern pharmacology have reducedthe morbidity and mortality for patients who havethis disorder.
Prior to the twentieth century, heart failure wasknown as dropsy. This term was used to describethe presence of generalized swelling, which was aclinical result of the syndrome. Thus, the treat-ment modalities available for dropsy, whether sur-gical or medical, were aimed at an emptying of thesystem or relieving fluid retention. These remedieswere crude in composition, unpredictable inaction, and associated with untoward side effects.Bloodletting, by venesection, leeches, hydragoguecathartics, squill, or mercury, was a commonmethod for alleviating the patients symptoms.13
The first important innovation in the medicaltreatment of heart failure was the discovery of thepharmacologic properties of foxglove by WilliamWithering in the eighteenth century. His classicmonograph, An Account of the Foxglove, publishedin 1785,4 describes how he had learned from an oldcountrywoman (the so-called Shropshire maid)that tea made from the leaves of the purple fox-glove plant was good for the dropsy.
For many years, digitalis was the only valuabledrug for the treatment of heart failure. It was notuntil 1919 that the diuretic properties of mercury
were demonstrated in patients with syphilis,severe rheumatic heart disease, and anasarca. Thisled to the synthesis of the organic mercurialdiuretics.2,5,6
This chapter provides an historical overview ofthe therapeutic strategies intended to alleviate saltand water retention in patients with heart failure.The fundamental basis by which these therapieswere prescribed related to the concept that heartfailure was an abnormality of cardiac function inwhich reduced ejection and impaired filling led tocirculatory responses such as salt and water reten-tion. This paradigm dominated the thinkingthroughout the first half of the twentieth century,until the utilization of vasodilatory agents in the1970s.7,8
Bloodletting
Bloodletting is one of the oldest remedies known toman. In the past, some commonly used methods forbloodletting included general bloodletting by vene-section or arteriotomy and local bloodletting byscarification with wet cupping, cauterization, andleeches.1 According to Heaths Dictionary ofPractical Surgery:
Bloodletting is said to be general whenthe blood is taken from a vein or artery sothat the amount in the vascular system is
3
CHAPTER 1
The history of acute heart failuremanagement: how far have wecome?Hector O Ventura, Mandeep R Mehra
01-OConnor-01-cpp 21/7/05 12:20 PM Page 3
-
materially diminished as shown by diminu-tion on the tension of the blood vessels: it istermed local when, by means of leeches, cup-ping, or scarification, blood is taken insmaller quantities, with a view of relievinglimited congestion and vascular tension.9
One of the reasons that the practice of bloodlettingcontinued for so long is that the procedure is actu-ally beneficial in reducing the fluid overload asso-ciated with heart failure. Early physicians,however, did not have the physiological under-standing to determine the conditions for whichbloodletting was medically indicated. Therefore,this procedure was used for almost everything,including agitated psychoses when a drop in bloodpressure resulted in sedation. It was John Pancoast,who reported the reason by which bloodletting wasbeneficial in patients with dropsy, the diminutionof the mass of the blood, by which overloaded cap-illary or larger vessels of some affected part may berelieved, the modification of the force and fre-quency of the hearts action.10
From the time of the Egyptians, throughAvicenna and Hippocrates, to the beginning of thetwentieth century, bloodletting was used in variousforms for the treatment of fluid retention. The fol-lowing sections review the therapeutic use ofbloodletting in patients with heart failure through-out history, focusing on some important contribu-tions.
Bloodletting in Roman timesFrom 100 BC to AD 476, the Roman Empire domi-nated the known world. The medicine practiced inRome was largely of Greek origin with excellentclinical descriptions. However, the treatmentstrategies used were largely ineffective and con-sisted of simple measures such as changes in diet,rest, and bloodletting. However, the Romans didmake great progress in the field of public health andsanitation and they founded the first hospitals.11Perhaps one of the most famous names from thisperiod is Celsus (25 BC to AD 40).
Aurelius Cornelius CelsusAurelius Cornelius Celsus, the Roman encyclope-dist, wrote a detailed account of medical practice
in his treatise De Medicina. He describes two basickinds of therapeutic methods:
Now every corporeal aid either dimin-ishes substance or adds to it, either draws itout or represses it, either cools or warms,either hardens or softens Substance iswithdrawn by blood letting, cupping, purg-ing, vomiting, rubbing, rocking, and by bod-ily exercises of all kinds, by abstinence, bysweating.12
In relation to heart failure and its treatment,the following passages are clear and excellentdescriptions of dyspnea and its treatment strategy:
When moderate and without any chok-ing, it is called dyspnoea; when more severe,so that the patient cannot breathe withoutmaking a noise and gasping, asthma; butwhen in addition the patient can hardlydraw his breath unless with the neck out-stretched, orthopnea. Of these the first canlast a long while, the two following are as arule acute.
Blood-letting is the remedy unless any-thing prohibits. Nor is that enough, but alsothe bowels are to be relaxed by milk, thestool being rendered as the body becomesdepleted by the measures the patient beginsto draw his breath more readily. Moreover,even in bed the head is to be kept raised.13
Celsus also describes the technique of bloodlettingas follows:
Blood letting by the incision of the vein,is no novelty now if the object be torelieve the whole body; it ought to be drawnfrom the arm, if to relieve a part, then fromthat part itself, or certainly from that near-est to it.14
Celsuss prescription of bloodletting and the factthat there is an improvement in breathing suggeststhat some of the patients suffered from dyspneaassociated with heart disease. Interestingly, he alsoutilized a very current treatment for pulmonary
4
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 4
-
edema and cardiac asthma, which is to keep thehead raised.
In another chapter of his book, Celsus describesthe technique of paracentesis for dropsicalpatients. He stated that, the tap should be donebelow the navel at the distance of about four digitsto the left.15
Bloodletting in the Middle AgesIn the Middle Ages, cauterization was another tech-nique used to relieve patients with fluid retention. Itwas used as a topical stimulant to attract fluid to thearea involved.1,16 Its use is represented in the fol-lowing passage discussing the disease of Alexius I,ruler of the Byzantine Empire from AD 1081 to 1118.His daughter, who watched Alexiuss attendingphysicians during their deliberations about herfathers disease, describes the following:
[They] felt his pulse and found all kindof irregularities his heart, they said, wasinflamed and was attracting all the superflu-ous matter from the rest of the body every day it grew worse, attacking him nolonger at intervals but relentlessly, with nointerruption. He was unable to lie on eitherside, so weak that every breath involvedgreat effort his condition was serious fornever for one moment could he breathefreely. He was forced to sit upright tobreathe at all but his stomach was visiblyenlarged to a great size and his feet alsoswelled up and fever laid him low, some ofthe doctors with scant regard to fever hadrecourse to cauterization.16
Bloodletting in the RenaissanceAlthough significant advances in the knowledge ofhuman anatomy occurred during the Renaissance,heart failure remained a poorly understood syn-drome.17 At the beginning of the seventeenth cen-tury, Exercitatio Anatomica de Mortu Cordis etSanguinis in Animalibus (On the Motion of the Heartand Blood in Animals) by William Harvey was pub-lished and paved the way to understanding the syn-drome of heart failure. Through experiments inanimals, this text demonstrates that blood circu-lated constantly and that the heart was a pump.
Harvey writes, it must therefore be concluded thatthe blood in the animal body moves around in acircle continuously, and that the action or functionof the heart is to accomplish this by pumping.18This description produced a paradigm shift in med-icine, since the heart was previously thought to bea furnace to heat the blood. After the publicationof Harveys treatise, the heart became known as apump to bring blood to the tissues.7
Using Harveys paradigm, Giorgio Baglivi in histreatise De Praxi Medica (On the Practice ofMedicine), which appeared first in 1669, illustratedthe first acceptable clinical description of pul-monary edema and attempted to establish a mech-anism by which it occurs.19 He writes:
Next to be considered is a dangerous dis-ease of the lungs which is called suffocativecatarrh. It is caused chiefly by stagnation ofthe blood in the lungs and about the peri-cardium In this kind of catarrh the patienthas a cold, and pain in the chest, and diffi-culty in breathing; also interrupted speech,anxiety, cough, stertor, a widely spaced lowpulse, foam at the mouth, and the like The foam at the mouth is caused by impairedcirculation of blood about the lungs and con-sequent circulation of the lymph in the upperparts of the body near the face; hence this[kind of] catarrh comes from sudden stagna-tion of blood in the vicinity of the heart andlungs, and not from phlegm running downfrom head as the ancients believed to be thecondition in this disease. An instant remedyfor this disease during the paroxysm isrepeated bloodletting the disease is veryprecipitous; unless phlebotomy is doneimmediately the blood coagulates more andstagnates. Thus the opportunity for cure islost. The blood should be reduced inamount, the clotting should be undone anda bland sweat should be produced.
In another passage of his treatise Baglivi writesabout asthma:
If anyone in the evening at bedtime, orspecially after three or four hours of sleep, is
5
Bloodletting
01-OConnor-01-cpp 21/7/05 12:20 PM Page 5
-
suddenly aroused by severe asthma or istaken with suffocation and opens the win-dow and wants fresh air, consider it certainthat he is suffering from dropsy of the chest dysuria is beneficial to asthmatics; if thedysuria ceases suddenly, the patients isseized with asthma again. Furthermore, thisgives additional confirmation to what I haverepeatedly observed, namely in the diseasesof the chest the treatment should leadtoward the urinary passages.
Later in the Appendix on Asthma, Baglivi states:
It may be granted that bloodletting curesasthmatic paroxysm immediately. However,frequent bloodlettings weaken the tone ofthe blood more, and enfeeble it; and for thisreason the disease ends in generalizeddropsy. Therefore the cause of the asthmashould be corrected, instead of beingcaressed by frequent phlebotomy.19
Several inferences can be drawn from Baglivisdiscussion. First, Baglivi gives an excellent andclear description of patients with pulmonary edemaand the attack of nocturnal dyspnea. Second, herelates the production of dyspnea and pulmonaryedema to an impaired circulation of blood to thelungs, an explanation based on Harveys ideas.Finally, Baglivi recommends the use of urgent phle-botomy to reduce blood volume for the treatmentof pulmonary edema. The latter comment providesan early example of a physiologic approach to ther-apy in heart failure. In addition, he also cautionsagainst the use of repeated bloodlettings and per-haps erroneously relates this therapy to the pro-duction of chronic fluid retention. It is more likelythat the patient, despite the repeated phle-botomies, progresses to chronic heart failure.Interestingly, he emphasizes that frequent phle-botomies cause only symptomatic relief, but thetreatment should be directed to the underlyingcause of asthma. More intriguing is the statement:
Dysuria is beneficial to asthmatics; if thedysuria ceases suddenly, the patient is seizedwith asthma again. Furthermore, this gives
additional confirmation to what I haverepeatedly observed, namely in the diseasesof the chest the treatment should leadtoward the urinary passages.
Jarcho analyzed this particular remark and con-cluded that perhaps Baglivi intended to writediuresis. If that is the case, Baglivi demonstratesthe association between decrease in diuresis anddyspnea and in addition he points out that thetreatment of the diseases of the chest should befocused on increasing urine output.19
Bloodletting in the nineteenthcenturyThe nineteenth century was a period of greatprogress in cardiology. Several diagnostic toolswere introduced, such as the stethoscope andsphygmomanometer, among others, to aid in theobjective assessment of cardiac diseases.20 Theunderstanding of the pathophysiology of heart fail-ure continued to evolve, including the recognitionof hypertrophy, cardiac enlargement, valvularheart disease, and ischemic heart disease as under-lying causes of heart failure. Despite the evolutionof the concept of heart failure, therapeutic optionsremained limited to the removal of fluids usingbloodletting, starvation, and purgation.21
James HopeJames Hope, one of the most famous English cardi-ologists, published his book, A Treatise on theDiseases of the Heart and Great Vessels, in 1831.22This book contained several classic descriptions ofthe signs and symptoms of heart failure. It alsoadded to the understanding of hypertrophy anddilatation of the heart, described the mechanism bywhich edema develops, and created the concept ofbackward failure. According to Hope, The over-worked ventricle first hypertrophies and thendilates. As it dilates the blood gets dammed upbehind it and an increased venous pressure is trans-mitted ultimately to the capillaries where theedema is formed. Hopes treatment of this disor-der was based on removing fluids by bleeding,puncturing, diaphoretics, emetics, purgatives, andexpectorants.22
Hope also used a combination of three grains
6
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 6
-
of calomel (blue pill), one or half of one of digitalisand one of scillae (squill) given 3 or 4 times a day,for the treatment of dropsy.22
The Irish School of MedicineIn general, the Irish School of Medicine wasopposed to the use of bloodletting in great quanti-ties and one of the champions of this theory wasDominic Corrigan. He stated that, Bleeding afterbleeding, blister after blister were repeated, starva-tion enforced and digitalis exhibited, until thepatient was reduced to such weakness that he hadscarcely strength to rise himself in bed.23
The review of the treatment of heart failure,specifically the chapter on treatment of the weakand probably dilated heart in connexion withenlargement of the liver and pulmonary disease, inWilliam Stokess masterpiece The Diseases of theHeart and the Aorta demonstrates Stokess aversionto the use of bloodletting and the importance ofthe use of mercury instead.2,24 He states that:
We should avoid all reducing measures;we must endeavour to improve the condi-tion of the blood, and, by stimulants andtonics, increase the power of the weakenedand atrophied muscular fibres althoughthe great principles of treatment are thesame in the weakened and dilated heartsuch as occurred in the case of Mr. Colles,and in either form of fatty heart, yet in oneimportant particular we find them to differ.I allude to the beneficial action of mercuryin relieving many of the symptoms, andremoving the consequences of the first ofthese diseases.24
However, in another passage, Stokes recommendsthe use of bloodletting especially in acute decom-pensation:
Mr. Colles from about the year 1834was the subject of a chronic bronchitis, withoccasional exacerbation of the disease in theacute form. During these attacks the perti-nent symptoms were dyspnea and palpita-tion, and the treatment adopted was toemploy small general bleedings.25
Reginald S. SoutheyIn 1877, an interesting development in the treat-ment of fluid retention was the invention, byEnglish physician Reginald Southey, of small rub-ber tubes that were placed in the lower extremitiesto relieve severe edema.26 Although early on thesetubes, known as Southeys tubes, were used for thetreatment of anasarca related to kidney failure,their use evolved in the next century to the treat-ment of obstinate edema in heart failure whenother medical therapies failed.
Bloodletting in the twentiethcenturyWilliam OslerWilliam Osler was born and educated in Canadaand became the first professor of Medicine at JohnsHopkins University. At the end of the nineteenthcentury, he published his book, The Principles andPractice of Medicine, in which he described the nat-ural history of heart failure, focusing on cardiachypertrophy. Cardiac hypertrophy is either adap-tive or maladaptive during the evolution of apatients history.27 Osler stated that, The course ofany case of cardiac hypertrophy may be dividedinto three stages: 1) the period of development, 2)the period of full compensation and 3) the periodof broken compensation.27
The treatment of the stage of broken compen-sation (acute decompensated heart failure[ADHF]) is depicted in the following passage. Herecommends venesection or depletion of the bow-els only in this period.27
Among the first indications are short-ness of breath on exertion or attacks of noc-turnal dyspnea dilatation of the heart,the gallop rhythm, or various forms ofarrhythmia, with or without the existence ofdropsy. Under these circumstances the fol-lowing measures are to be carried out
1 Rest2 Relief of the embarrassed circulation
(a) By venesection. In cases of dilatation,from whatever cause when signsof venous engorgement are markedand when there is orthopnea with
7
Bloodletting
01-OConnor-01-cpp 21/7/05 12:20 PM Page 7
-
cyanosis, the abstraction of fromtwenty to thirty ounces of blood isindicated. This is the occasion inwhich timely venesection may savethe patients life. It is a condition inwhich I have had most satisfactoryresults from venesection. I have onseveral occasions regretted the post-ponement, particularly in instancesof acute dilatation and cyanosis inconnection with emphysema.
(b) By depletion through the bowels. This isparticularly valuable when dropsy ispresent. Of the various purges thesalines had to be preferred, and maybe given by Matthew Hays method.Half an hour before breakfast fromhalf an ounce to an ounce and a halfof Epsom salts may be given in a con-centrated form. This usually producesthree to five liquid evacuations.
Paul Dudley WhitePaul Dudley White published the first edition of hisimportant treatise in cardiology, Heart Disease, in1932.28 Referring to the treatment of heart failure,he established very clearly the use of variousmechanical therapeutic measures. Among thetypes of treatments, he described venesection as:
not often necessary in the treatment of con-gestive heart failure, but sometimes as anemergency measurement it gives relief andprobably saves a few lives. It was much moreoften necessary in the days before there wasa proper appreciation of how to give digi-talisthat is before the time of more or lessuniversal digitalization and maintenance ofdigitalis effect. Venesection is applicable totwo types of patients: first, the cardiacpatient with acute and fulminating conges-tive heart failure, as in cases of cardiacasthma and of marked venous congestionwith tachycardia, and second, the chroniccardiac patient who has obstinate edemaand persistently high venous pressure (over20 cm of water in arm vein) in spite of rest,digitalis, diuretics, and other therapy. Blood
should be removed from the arm vein byknife or needle in amounts between 250 and500 mL (12 to 1 pint). The procedure may berepeated at intervals as needed, but itshould not be done unless the venous pres-sure is elevated.
White also described the use of bloodless blood-letting utilizing upper and lower extremity bandsin patients with decompensated heart failure:
Another way by which temporarily theheart may be relieved of excess blood,reported to be helpful in acute heart failurelike cardiac asthma, is constriction of theproximal parts of all four extremities byblood pressure cuffs or similar bands, cuttingtemporarily the venous circulation.
Paul WoodIn the 1950s, Paul Wood, the director of theInstitute of Cardiology in London, published histextbook, Diseases of the Heart and Circulation.29Similar to White, besides medical therapy, he uti-lized venesection, venous tourniquets in patientswith pulmonary edema, and acupuncture of theextremities, as well as Southeys tubes for treatingmassive edema. The following excerpts are from histextbook:
Venous tourniquets may be appliedaround the thighs to trap blood in the legsor venesection may be preferred.
Venesection deserves a better reputa-tion. It has fallen out of favour because sim-ilar results may be obtained by means ofcertain drugs, but it offers a quick and sureway of lowering the venous pressure andshould not be abandoned. About 600 to750 mL of blood may be withdrawn.
When edema is gross and fails to respond,it may necessary to resort to acupuncture. Atriangular cutting needle is used and about adozen punctures are made in each leg Southeys tubes constitute a cleaner way ofremoving fluid on the same principle.
8
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 8
-
Phlebostasis
Another treatment used in the twentieth centurywas so-called bloodless bloodletting or phlebosta-sis. This was accomplished by inflating cuffs on theextremities and then allowing the air from the cuffsto escape very slowly or by using tourniquets inpatients with cardiac asthma.
A specific case of the use of phlebostasis isdepicted by Dr. Heinrich Stern, a physician whowrote an interesting treatise, The Theory andPractice of Bloodletting, in 1915.30 He described thefollowing case:
male patient, 58 years old; consulted me firstin December 24, 1912. He complainedchiefly of asthmatic attacks coming on afterexertion the amount of his twenty-fourhours urine hardly ever exceeded one liter the physical examination showed thearea of cardiac dullness was markedlyincreased toward the left as well as towardthe right the systolic blood pressure was240 mm Hg On application of phlebosta-sis for three minutes relieved the attacks ofcardiac dyspnea for a number of weeks.
In his treatise, Dr. Stern also reviews the litera-ture on the use of bloodletting either by venesec-tion, leeches, or phlebostasis for heart failure.30Several remarks, especially on the use of bloodlet-ting by James McKenzie, and other recommenda-tions are important to note:
Bloodletting should be performed rap-idly by either venesection or leeches whenthe right heart is distended
Bloodletting acts instantaneously inpulmonary edema.
In pronounced cases of decompensationthe most stressing and alarming symptoms,particularly cardiac asthma, are almostinstantly removed by a timely bloodletting congestive cardiac states, on the otherhand, require repeated withdrawals ofblood.
I wish to emphasize again that inpatients with congestion medicinal orother therapeutic agents generally exert amore prompt and lasting influence afterthan before bloodletting.
As individuals with congenital heartdisease do not bear well the abstraction ofblood, amounts not exceeding 75 mLshould be removed at one time
The primus of modern cardiologists,James McKenzie, holds bloodletting in highesteem in the treatment of the diseases ofthe heart, deploring, however, the tempo-rary character of relief which it affords inextreme cases, McKenzie says, it merelydelays the end.
McKenzie employs bloodletting whenthere is distress in breathing, on account ofgreat distension of the right heart
McKenzie concludes that instantaneousalleviation [with bloodletting] of the dis-tressing phenomena is frequently very strik-ing, particularly in cases with auricularfibrillation, and cases with high blood pres-sure and extreme failure of the heart.
Several authors bear witness that car-diopaths treated with bloodless bloodlet-ting note a subjective improvement of theircondition.
There is no doubt that phlebostasis willserve a good purpose in most cases of heartdisease in which bloodletting is indicated.
Digitalis
An Account of the FoxgloveThe publication of An Account of the Foxglove, andSome of its Medical Uses: With Practical Remarks onDropsy, and Other Diseases by William Witheringmarks one of the defining moments for the treat-ment of patients with heart failure.4 In this book,
9
Digitalis
01-OConnor-01-cpp 21/7/05 12:20 PM Page 9
-
Withering describes in detail his experience withdigitalis, including the evaluation of the doseresponse and the description of the beneficial andtoxic effects of the drug.
This section describes some of the most impor-tant passages from Witherings book, which hasbecome one of the classic monographs in the his-tory of cardiology and pharmacology. The follow-ing passage illustrates both a record of the early useof digitalis in a patient with heart failure and aninteresting example of the practice of medicine inthe late eighteenth century.31
On the 25th of July I was desired to meetDr. Darwin at the ladys house. I found hernearly in a state of suffocation; her pulseextremely weak and irregular, her breathvery short and laborious, her countenancesunk, her arms of a leaden colour, clammyand cold. She could not lye down in bed,and had neither strength nor appetite, butextremely thirsty. Her stomach, legs andthighs were greatly swollen, her urine verysmall in quantity, not more than a spoonfulat a time, and that very seldom. It had beenproposed to scarify her legs, but the proposi-tion was not acceded to. She had experi-enced no relief from any means that hadbeen used In this situation of things Iknew of nothing likely to avail us, exceptthe Digitalis: but I hesitated to propose,from an apprehension that little could beexpected from anything; that anunfavourable termination would tend to dis-credit a medicine which promised to be agreat benefit to mankind, and I might becensured for a prescription which could notbe countenanced by the experience of anyother regular practitioner. But these consid-erations soon gave way to the desire of pre-serving the life of this valuable woman, andaccordingly I proposed the Digitalis to betried; adding, that I sometimes found it tosucceed when other, even the most judi-cious methods had failed
The patient took five of (digitalis)draughts, which made her very sick, andacted powerfully upon the kidneys, for
within the first twenty-four hours she madeupwards of eight quarts of water. The senseof fullness and oppression across the stom-ach was greatly diminished, her breath waseased, her pulse became more regular, andthe swelling of her legs subsided.
This case clearly represents a patient with heartfailure (right and left) and atrial fibrillation (irreg-ular pulse). Although we do not know the anatom-ical diagnosis of this patient, but it might representthe natural history of rheumatic heart disease(mitral stenosis) in which slowing the heart rateleads to clinical improvement.
In the next passage, Withering gives an expla-nation of the types of patients who seemed torespond, and at the end of his book he lists the sideeffects and signs of overdose, the method of secur-ing the optimal dose by dose titration against theonset of the first adverse effect, and finally theinferences of his experience.32
The Foxglove when given in a very largeand quickly-repeated doses, occasions sick-ness, vomiting, purging, giddiness, confusedvision, objects appearing green or yellow;increased secretion of urine, with frequentmotions to part with it, and some timesinability to retain it; slow pulse, even as slowas 35 in a minute, cold sweats, convulsions,syncope, death [The direction requires] attention to the state of the pulse, and itwas moreover of consequence not to repeatthe doses too quickly, but to allow sufficienttime for the effects of each to take place, asit was found very possible to pour an injuri-ous quantity of the medicine, before any ofthe signals for forbearance appeared.
According to Withering, the inferences are:
I. That the Digitalis will not universallyact as a diuretic.
II. That it does do so more generallythan any other medicine.
III. That it will often produce this effectafter every other probable method hasbeen fruitlessly tried.
10
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 10
-
IV. That if it fails, there is but little chanceof any other medicine succeeding.
V. That in proper doses, and under themanagement now pointed out, it ismild in its operation, and gives less dis-turbances to the system, than squill, oralmost any other active medicine.
VI. That when dropsy is attended bypalsy, unsound viscera, great debility,or other complication of disease, nei-ther Digitalis, nor any other diureticcan do more than obtain a truce tothe urgency of the symptoms; unlessby gaining time, it may afford oppor-tunity for other medicines to combatand subdue the original disease.
VII. That the Digitalis may be used inevery species of dropsy, except theencysted.
VIII. That it may be made subservient to thecure of diseases, unconnected withdropsy.
IX. That it has a power over the motion ofthe heart, to a degree yet unobservedin any other medicine, and that thispower may be converted to salutaryends.
Withering thought that digitalis was mainly adiuretic but he also thought that it had cardiacactivity. His ninth inference states that digitalishas a power over the motion of the heart, to adegree yet unobserved in any other medicine, andthat this power may be converted to salutary ends.
More than 200 years have passed since the pub-lication of Witherings masterpiece and digitalis isstill used today in the treatment of heart failure.We have learned more about the effects of digitalis,but the principles of its use which are clearly delin-eated in his book have stood the test of time. AnAccount of the Foxglove represents one of the firstclinical trials and the first piece of what today iscalled evidence-based medicine when the onlytreatment used before that time was bloodletting.The introduction of digitalis into the medicalarmamentarium represents a defining moment forthe treatment of heart failure and is a real triumphin the practice of medicine.
Use of digitalis after the publicationof Witherings BookUnfortunately, despite the fact that Withering haddelineated clear guidelines for the use of digitalis,those guidelines were not followed during the nextcentury. Therefore, the important therapeuticactions of digitalis in heart failure were not appre-ciated until the end of the nineteenth century andthe beginning of the twentieth century.33
In the same year that Withering died, 1799,John Ferriar was the first to describe the cardiaceffects of digitalis. He wrote, the extractions fromthe leaf furnish us a means of regulating the pulseto our wish and supporting it in a given state ofvelocity as long as we may judge it proper .33
The entire nineteenth century was associatedwith several clinical and animal studies on digitalis.Some of these studies are worth mentioning.Fothergill in England poisoned a heart with aconiteand watched its contractility improve with digitalis.Franks experiments in 1895 demonstrated thatdigitalis increased the cardiac output in the abnor-mal heart without any effects in the normal heartsof frogs. This study was confirmed by others, con-cluding that digitalis in the abnormal heart notonly increased cardiac output, but also decreasedright atrial pressure.33
The steps taken to discover the active ingredi-ent of foxglove are beyond the scope of this chap-ter, but suffice it to say that digitalis lanata, a plantrelated to foxglove, produced an entirely new gly-coside called digoxin, the one used today for thetreatment of heart failure.33
In the earlier part of the twentieth century,James McKenzie and Thomas Lewis establishedthe effects of digitalis in humans. They suggestedthat the primary action of digitalis was to slow ven-tricular rate. Therefore, it was beneficial in patientswith heart failure and atrial fibrillation.33
Clinical uses of digitalis in heartfailureThe use of digitalis in the treatment of patientswith heart failure is clearly described in some of themost prestigious textbooks in cardiology publishedprior the 1960s. In 1932, Paul White stated thatdigitalis had been used mainly from the dried leaves
11
Digitalis
01-OConnor-01-cpp 21/7/05 12:20 PM Page 11
-
of the second-year growth of the plant.34 Severalpreparations such as pills, capsules, tincture, infu-sion, and suppositories were in existence and testswere established to achieve a practical standardstrength for universal use. Regarding the action ofdigitalis on the heart, he notes three effects:
(a) In the first place it depresses the pace-making function of the sinoauricular nodeand also the auriculoventricular node, withthe resulting tendency from the heart rateto be slowed (b) a second effect of digi-talis on the heart is on conduction. Thisoccurs all through the heart muscle withincrease in the refractory period of theauricular and ventricular muscle, so thatauricular flutter is converted into auricularfibrillation it is this depressant influenceof digitalis on conduction that explains atleast half of the virtue of the drug. It haslong been known that there is one type ofpatient with congestive heart failure espe-cially helped by digitalis therapy, some-times with astounding success; this type isthe patient who has also auricular fibrilla-tion with more or less rapid ventricularrate (c) a third effect of digitalis on theheart is on contraction.
The therapeutic indications for the use of digitalis,according to White, were as follows:
congestive heart failure with or withoutauricular fibrillation, auricular flutter as atherapeutic test when it is uncertainwhether or not there is a slight degree ofcongestive heart failure, or perhaps as ameans of warding off impending failure the most common method of administrationis by mouth For the very few individualswith congestive heart failure for whom digi-talis is urgently needed because of theirgrave or almost moribund condition, thedrug can be given intravenously in the samedosage that is used by mouth, but more rap-idly there is only one drug besides digi-talis which has digitalis-like action that it isever worthwhile. That is strophanthin or
ouabain. It is necessary only in emergencytreatment.
White also gives the clinical parameters to be fol-lowed when a patient with congestive heart failurereceives digitalis or strophanthin: 1) the apexheart rate and pulse deficit, especially if there isatrial fibrillation, 2) the loss of weight and urineoutput as compared to fluid intake and 3) subjec-tive symptoms of improvement.34
In his textbook on cardiology, Paul Wood statesthat digitalis should be used in heart failure with orwithout atrial fibrillation.35 He also describes theproperties by which digitalis exerts its activity, itlowers the venous pressure, raises the blood pres-sure, slows the heart rate, relieves hepatic disten-sion, increases the vital capacity, shortens thepulmonary circulation time, increases the cardiacoutput and encourages diuresis.
Wood states that ouabain can be used in car-diogenic shock, but cautions against the use ofintravenous digitalis in patients with acute pul-monary edema, he states: Strophanthin and digi-talis are probably best avoided in view of theirpressor actions, indeed, paroxysmal cardiac dysp-nea may occasionally be initiated by intravenousdigoxin. Woods view of avoiding digitalis in pul-monary edema, presumably in patents with hyper-tension and heart failure, is still in use today.
The role of digitalis in the treatment of acuteheart failure is limited and it is more suitable forchronic therapy. Recently, digitalis has been shownto be beneficial in improving symptoms and hospi-talizations of patients with heart failure, and toxic-ity is rarely seen.36 Witherings prediction That it[digitalis] has a power over the motion of the heart,to a degree yet unobserved in any other medicine,and that this power may be converted to salutaryends has become a reality, in the treatment ofheart failure today.
Diuretics
MercuryWilliam Cullen was the Professor of Chemistry atEdinburgh University and one of Witherings men-tors. In 1789, he published a work entitled A
12
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 12
-
Treatise on Materia Medica, in which he describedthe properties of mercury. Cullen states:
I shall treat of this medicine as fully as Ican, as it is the most useful and universalmedicine I known Universally mercury inits active state seems to be the stimulus toevery sensible and moving fibre of the bodyto which is immediately applied: and in con-sequence, it is particularly a stimulus toevery excretory of the system to which it isapplied externally or internally.37
Cullen concluded that this particular ability ofmercury to increase the excretory ability of thesystem to which is applied made mercury a verypowerful therapeutic agent in the practice of med-icine.37
Mercury (calomel) also called the blue pillwas used for centuries in combination with digitalisand squill for the treatment of heart failure.2Several authors, including Hope, Corvisart, Stokes,and Blackall, among others, advocated its use as atherapeutic agent for patients with edema.
John BlackallJohn Blackall made some interesting observationsregarding the clinical characteristics and treatmentof dropsy. In his book, Observations on the Natureand Cure of Dropsies, he made several importantobservations regarding the use of mercury for thetreatment of fluid retention. First, he tried to estab-lish some rules for which patients should be givenmercury.38 He states, In dropsy the mineral [mer-cury] is given in a manner equally indiscriminateand in larger doses, and with such opposite success,as to make it highly desirable that its exhibitionshould, if possible, be not conjectural, but definedand guided by some plain rules. He adds:
Some firmness of the general habit will,I believe, be the best encouragement to it yet I think the characters of the urine aremost easily understood, and the least liableto nay misconception. If that discharge errschiefly by want of dilution, the presence ofbile, mercury is likely to render great serviceto the obstructions which are probably
present, particularly those of the liver, andalso to prove a true diuretic; and theswellings never pass off so readily and freely If on the contrary, the habit is sodepraved that the coagulable part of theblood already passes off the kidneys, theoperation of this mineral is obviously equi-vocal and hazardous.38
This interesting description demonstrates that theevaluation of the urine was a very important andmore objective tool for prescribing mercury, sincethis agent only worked in cases of dropsy in whichthe urine did not coagulate or did not containalbumin. The latter were cases of renal disease. Itwas several years later that Richard Brightreported the association between albuminuria andfullness of the pulse, dropsy, and hardening of thekidneysthe so-called Bright disease. For patientsin which the urine did not contain albumin, mer-cury was a true diuretic and it was beneficial inpatients with dropsy. The allusion to the obstruc-tion of the liver is probably related to liverenlargement secondary to fluid retention in heartfailure.
Alexander Philip Wilson PhilipThe main problem with the use of calomel was itstoxicity, which ranged from lack of appetite, nau-sea, excess salivation, severe gastrointestinal irrita-tion, lack of concentration, and mobility of theteeth to anxiety, insomnia, and depression.Therefore, some of the more practical physicians inthe eighteenth and nineteenth centuries advo-cated the use of calomel in small doses.
In a book published in 1834 entitled, On theInfluence of Minute Doses of Mercury, Dr. AlexanderPhilip Wilson Philip, a practicing physician inEngland, stated that, I was led to them [minutedoses of mercury] by observing that in lessening thedose and increasing its frequency, in proportion aswe lessen the immediate, we increase the alter-ative, effects.39 In relation to the mechanism bywhich mercury exerted beneficial effects on peoplewith dropsy, Dr. Philip added that the mostremarkable of the effects peculiar to mercury, is itsinfluence on the liver, and to prove this point hedescribed a case as follows:
13
Diuretics
01-OConnor-01-cpp 21/7/05 12:20 PM Page 13
-
Mr. Hobson had for thirty-four yearslabored under the symptoms of diseasedheart, to which all the powers of his consti-tutions were yielding. He had become paleand edematous I [Dr. Philip] was led to regard the affection of the heart as chieflysympathetic to the function of the liver,which was more or less, and occasionallymuch disordered. For many months hesteadily pursued the plan of treatment taking half a grain of blue pill three times aday combined with such other means astended to restore the digestive organs, andrelieve the occasional more severe attacks I had the satisfaction to see him relieved fromevery symptom.40
Dr. Philip believed that the mechanism by whichcalomel relieved fluid retention was associatedwith an effect on the digestive system, mainly inthe liver.
William StokesIn his famous treatise, William Stokes describes thecase of Abraham Colles and the use of mercury inhis treatment. First, Dr. Stokes introduces the con-cept using mercury for symptomatic relief specifi-cally when the patient has hepatomegaly andpulmonary disease as compared to cases with sim-ple fatty degeneration. This is an important obser-vation since mercury is prescribed when thepatient is in an edematous state. Interestingly, hecautions against the use of reducing measures(bloodletting). He adds:
It is remarkable, that although the bene-ficial action of mercury in this affection isknown to many practical physicians, but lit-tle information can be found on the subjectin any of our medical works I do not wishit to be believed that by mercury we can curedilatation of the heart; but many years expe-rience has convinced me that by the use ofthis remedy we can delay its production,remove the irregular action which assists incausing the disease, and, above all, prolongthe patients life, and again and again relievehim from dropsy, and from pulmonary and
hepatic congestions, even when they havearrived at a point which threatens speedy dis-solution.41
In the following passage, Stokes describes theguidelines by which mercury should be used inpatients with heart failure and congestion:
The more common examples of weakenedhearts in which so much benefit is derivedfrom mercurial action. In such cases the fol-lowing circumstances are to be met with:
1) The patient is generally advanced in life,most of the cases being in persons offrom 50 to 70 years of age.
2) These individuals are originally ofhealthy constitution and strong habit ofbody.
3) They are liable to some degree of gout,which malady, after having longoccurred in its more regular form,becomes masked or imperfect.
4) They are subject to bronchitis, which,during the aggravation of symptoms,increases as to resemble suffocativecatarrh.
5) The liver is permanently enlarged, yet inmany no appearance of jaundice exists.The hepatic tumour is generally indo-lent, and the epigastric veins are seldomvaricose.
6) Two conditions of the heart may beobserved. In both there is permanentirregularity, always augmented duringthe paroxysm of suffering; but in oneclass of patients the physical signs indi-cate hypertrophy with valvular disease,while in the other the signs are thosewhich have been indicated in the chap-ter on Dilatation of the Heart, unat-tended by any direct indication ofvalvular disease.41
Stokes also attempts to establish the dose and themechanism by which mercury relieves symptoms ofcongestion and is very close to understanding thediuretic effect of the drug. The fact that mercury
14
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 14
-
increases the production of urine is a very importantobservation, since today it is known that the diureticeffect is the mechanism of the action of the mercu-rial agents. In addition, he establishes the use ofmercury in combination with digitalis. He states:
The quantity of the remedy which isrequired, as we might expect, varies in differ-ent cases. In some it is requisite to establishptyalism, while in others the relief of theheart and the disappearance of the dropsy,are observed after the use of a very mildcourse if any of the characteristic action ofmercury can be perceived unless we includediuresis. In other cases it will be necessary touse diuretics following on the mercurialaction, and in this way we often observe a sin-gularly abundant secretion of urine, attendedby rapid subsidence of the dropsy and visceraloppression. We should use various combina-tions of the vegetable and saline diuretics;and even digitalis, in connexion with diuret-ics of the tonic and stimulating class, may beemployed. The success of diuretics appears toturn upon their being preceded by mercury but the truth is, that in these cases we arenot to be over-timid in the repetition of mer-curial medicines; for there is nothing moreremarkable than the power which thepatients exhibit of bearing repeated coursesof mercury not only without injury, but withextraordinary benefit to their general health there has been no unhealthy action on themouth, no periostitis, cutaneous eruptions,or tremors.
He adds:
It need hardly be observed, that the timeat last arrives when, as in the case of DrColles, the system no longer responds to theaction of medicine, and the patient sinkswith dropsy and pulmonary congestion.42
Mercurial diureticsIt was not until 1920, that Saxl and Heilig, in aclassic manuscript, reported the diuretic effect of
merbaphen (Novasurol), which contained mer-cury in complex organic combination and wasoriginally introduced as an antisyphilitic agent.5Alfred Vogl,6 an American student in theWenckebach clinic from 1919 to 1920, describedthe manner in which this finding was accom-plished. He and the nurse noticed that whenNovasurol was given to two patients with syphilis,it produced an increase in urinary output. Afterthis observation, he proceeded to give Novasurol,the wonder drug, to a patient with heart failure.He states:
Soon afterwards there was admitted toour wards a boy with a huge rheumatic heartand tricuspid insufficiency, in severe, water-logged failure, almost anuric and obviouslyterminal. The case seemed hopeless and hesuffered cruelly. In sympathy and despera-tion, we tried our wonder drug. He receivedthis injection and unfortunately expired thefollowing day. Before his death, however, hepassed three liters of urine. Post mortemexamination confirmed the clinical diag-nosis and revealed no evidence of syphilis.
This case represents the first use of an organic mer-curial agent in the treatment of heart failure.
Novasurol was painful and toxic, and was soonreplaced by the more potent yet more benignSalyrgan. These agents became widely used in the1940s as an adjunct therapy in heart failure.However, they were given only parenterally,which was a major drawback for patients whoneeded chronic therapy. Adverse reactions associ-ated with the use of the organic mercurial diuret-ics were very similar to the old inorganiccompounds. These included stomatitis, colitis,albuminuria, hematuria, and sudden death. A testdose of 0.5 mL was utilized 24 hours before thefull therapeutic dose was given and the patientswere observed for side effects. Combinations withtheophylline resulted in a less painful and moreeffective agent.43
Mercurial diuretics exerted their action onpatients with fluid retention and heart failuremainly by decreasing the reabsorption of sodium,potassium, and chloride in the tubular system of
15
Diuretics
01-OConnor-01-cpp 21/7/05 12:20 PM Page 15
-
the kidneys, thereby reducing edema. The declinein blood volume and venous pressure was second-ary to the renal action. The effects were gradual,beginning 1 to 2 hours after the injection.43
Oral diureticsThe development of orally active diuretics startedin the mid-1940s. At that time, several reportsdemonstrated that sulfanilamides and sulfon-amides were specific inhibitors of carbonic anhy-drase. These studies led to the demonstration thatsulfanilamide was a weak natriuretic-diuretic agentin patients with heart failure.2 In 1958, after severalyears of research, Beyer et al. reported on thediuretic and saluretic properties of a sulfonamidecalled chlorothiazide. This compound became thefirst orally-active diuretic and in a very short timethe thiazides became an important component ofdiuretic therapy for patients with hypertension orheart failure.2
Loop diureticsThe introduction of diuretics that act within theloop of Henleloop diureticsdramaticallyaffected the ability of clinicians to improve thesymptoms of heart failure with minimum toxic-ity.2,44 They were eagerly accepted because theycould be given orally as well as parenterally andalso because they possessed potent diuretic capa-bilities. Furosemide, one of the first loop diureticsto be developed, was, and still is, utilized intra-venously in patients with pulmonary edema ordecompensated heart failure to decrease excessivelung water through natriuresis and diuresis. Themost important effect of furosemide in the acutemanagement of acute decompensated heart failure(ADHF) probably relates to its substantial hemo-dynamic effects. Furosemide has been shown toreduce cardiac filling pressures secondary to avasodilatory effect.45,46 The same effect wasobserved in patients with acute myocardial infarc-tion (AMI) and heart failure.47 Conversely, a vaso-constrictor effect with a reduction in cardiacoutput has been reported with the use offurosemide, due to diuretic-induced neurohor-monal activation.48 Other loop diuretics utilized inthe treatment of heart failure are bumetanide andtorsemide (in the 1980s).44 Loop diuretics,
although very effective, should be judiciouslyemployed because they can cause hypotension andbecause of their kaliuretic effect they can causehypokalemia, activation of neurohormones andcardiac arrhythmias.2,45,48
Other Therapeutic Measures
Oxygen and morphine, as well as other diuretics,such as carbonic anhydrase and theobromineinhibitors, have been used down the centuries forpatients with ADHF and pulmonary edema.Oxygen and morphine are still in use today.Conversely, aminophylline, a therapeutic agent,that was very popular from the 1950s until the1970s, is no longer used in patients who presentwith acute pulmonary edema. In his cardiologytextbook, Paul Wood describes the effects ofaminophylline in patients with paroxysmal cardiacdyspnea as follows:
theophylline-ethylene-diamine (amino-phylline) 0.24 to 0.48 gram intravenously,lowers the venous pressure immediately,relieves bronchial spasm, and may have adirect stimulating action on the heart willproduce dramatic improvement amino-phylline suppository of 0.l4 gram. At nightwill prevent both Cheyne-Stokes breathingand paroxysmal nocturnal dyspnea, and indoing so may earn the patients thanks for agood night sleep.49
Another agent used in the treatment of acutepulmonary edema was, and still is, sublingual nitro-glycerin. In 1957, Johnson et al.50 demonstratedthat the symptomatic relief obtained by the use ofnitroglycerin in patients with paroxysmal dyspneaand acute pulmonary edema was related to a rapiddecrease in pulmonary artery and pulmonary capil-lary wedge pressures. Johnson et al. concluded that,the clinical and physiologic data obtained afternitroglycerin administration suggest that this drughas an important place in the management ofpatients with pulmonary-artery hypertension andparoxysmal dyspnea associated with failure of theleft ventricle.50
16
The history of acute heart failure management: how far have we come?
01-OConnor-01-cpp 21/7/05 12:20 PM Page 16
-
Conclusion
In summary, this historical overview describes some,but not all, of the therapies that have been used inthe treatment of heart failure from ancient timesuntil the 1970s. In 1997, the editor of the Lancet,Richard Horton, wrote, Medicine pays almostexclusive homage to the shock of the new weplace constant emphasis on novelty this is an eraof the instantaneous and the immediate.51 It seemsthat medicines concern with the new leaves lit-tle space for history. We do not subscribe to thispoint of view. As T. S. Eliot wrote, the historicalsense involves the perception not only of the past-ness of the past, but of its presence.52 Thus, onecannot appreciate the present separate from themilieu of the past. The newly developed strategiesfor the treatment of acute heart failure will bedetailed in this book. However, the successes of ourpresent days are rooted in the past and that it is whya historical overview of past therapies for patientswith acute heart failure is crucial to recognize notonly how far we have come but also how much wecan accomplish in the future.
References
1. Seigworth GR. Bloodletting over the centuries. N YState J Med 1980; 80: 20222028.
2. Ventura HO, Mehra MR, Young JB. Treatment ofheart failure according to William Stokes: theenchanted mercury. J Card Fail 2001; 7: 277282.
3. Ventura HO, Mehra MR. CollesStokes contribu-tions to the concept of heart failure. Am J Cardiol1998; 81: 14701473.
4. Withering W. An Account of the Foxglove andSome of Its Medical Uses with Practical Remarks onDropsy and Other Diseases (Robinson: Birmingham,1785).
5. Saxl P, Heilig R. ber die diuretische Wirkung vonNuvasurol und anderen Quecksilberinjektionen (Thediuretic effects of Novasurol and other mercuryinjections). Wien Klin Wochnschr 1920; 33:943944.
6. Vogl A. The discovery of the organic mercurialdiuretics. Am Heart J 1950; 39: 881883.
7. Katz AM. Evolving concepts of heart failure: coolingfurnace, malfunctioning pump, enlarging muscle. PartI. J Card Fail 1997; 4: 319334.
8. Cohn JN, Franciosa JA. Vasodilator therapy for heartfailure: (first of two parts). N Engl J Med 1977; 297:2731.
9. Heath C. Dictionary of Practical Surgery (Smith,Elder, & Co.: London, 1886), 162.
10. Pancoast J. Treatise of Operative Surgery (Carey &Hart: Philadelphia, PA, 1844), 15.
11. Majors RH. Medicine in the Roman Empire. In:Majors RH (ed.) A History of Medicine (Charles CThomas: Springfield, IL, 1954), 162219.
12. Celsus A. De Medicina. Translated by Collier GF,(Longman & Co.: London, 1838), IV, 130.
13. Celsus A. De Medicina. Translated by Collier GF,(Longman & Co.: London, 1838), IV, 132133.
14. Celsus A. De Medicina. Translated by Collier GF,(Longman & Co.: London, 1838), II, 52.
15. Celsus A. De Medicina. Translated by Collier GF,(Longman & Co.: London, 1838), VII, 292.
16. Lutz JE. An XII century description of congestiveheart failure. Am J Cardiol 1988; 61: 494495.
17. Jarcho S. A summary of this story. In: The Concept ofHeart Failure: From Avicenna to Albertini (HarvardUniversity Press: Cambridge, MA, 1980), XX,362363.
18. Harvey W. Exercitatio Anatomica de Mortus Cordiset Sanguinis in Animalibus (English translation withannotations by CD Leake) (Charles C. Thomas:Springfield, IL, 1928), 7.
19. Jarcho S. Georgio Baglivi and the practice ofmedicine. In: The Concept of Heart Failure: FromAvicenna to Albertini (Harvard University Press:Cambridge, MA, 1980), 228236.
20. Acierno LJ. Diagnostic techniques. In: Acierno LJ(ed.) The History of Cardiology (The ParthenonPublishing Group Ltd: New York, 1994), 447501.
21. Katz AM. Evolving concepts of heart failure: coolingfurnace, malfunctioning pump, enlarging muscle. PartII: Hypertrophy and dilatation of the failing heart. JCard Fail 1998; 4: 6768.
22. Hope J. A Treatise on the Diseases of the Heart andGreat Vessels (John Churchill: London, 1839),407412.
23. Baldry PE. Pump failure. In: The Battle Against HeartDisease (Cambridge University Press: London, 1971),152156.
24. Stokes W. Treatment of the weak and probablydilated heart in connexion with enlargement of theliver and pulmonary disease. In: Stokes W (ed.) TheDiseases of the Heart and the Aorta, 1st edition(University Press: Dublin, 1853), 352356.
25. Stokes W. Disease of the muscular structures of theheart. In: Stokes W (ed.) The Diseases of the Heart
17
References
01-OConnor-01-cpp 21/7/05 12:20 PM Page 17
-
and the Aorta, 1st edition (University Press: Dublin,1853), 255298.
26. Southey R. Chronic parenchymatous nephritis of rightkidney. Left kidney small and atrophied. Old scrofu-lous pyelitis. Trans Clin Soc London 1877
![Arrhythmias & Heart Failure - divine [id] · Arrhythmias & Heart Failure: ... Palais du Pharo, Marseille, France May 28-30, 2015 Congress directors Fiorenzo ... to follow conferences](https://static.fdocuments.in/doc/165x107/5af59ad97f8b9a74448e6b8b/arrhythmias-heart-failure-divine-id-heart-failure-palais-du-pharo-marseille.jpg)

















