Case Presentation: Pediatric Trauma - University of … Presentation: Pediatric Trauma Jerrod Keith,...
46
Case Presentation: Case Presentation: Pediatric Trauma Pediatric Trauma Jerrod Keith, MD Jerrod Keith, MD University of Colorado University of Colorado General Surgery Grand Rounds General Surgery Grand Rounds October 1 October 1 st st , 2007 , 2007
-
Upload
truongtuyen -
Category
Documents
-
view
216 -
download
3
Transcript of Case Presentation: Pediatric Trauma - University of … Presentation: Pediatric Trauma Jerrod Keith,...

Case PresentationCase PresentationPediatric TraumaPediatric Trauma
Jerrod Keith MDJerrod Keith MDUniversity of ColoradoUniversity of Colorado
General Surgery Grand RoundsGeneral Surgery Grand RoundsOctober 1October 1stst 2007 2007
HPIHPI
4yo healthy male4yo healthy maleMVC headMVC head--on at 65mphon at 65mphBack seat passengerBack seat passengerRestrained by lap beltRestrained by lap beltCrying at the sceneCrying at the sceneUnable to move lower extremitiesUnable to move lower extremitiesTaken to outside hospitalTaken to outside hospital
Outside HospitalOutside Hospital
HypotensiveHypotensive2 units 2 units pRBCspRBCs 800ml NS 800ml NS
hcthct 185 185 INR 172INR 172 72430349137243034913--1313IntubatedIntubatedDislocated right ankleDislocated right ankle
Reduced and splintedReduced and splinted
Head CT Head CT ndashndash normalnormalChest CT Chest CT ndashndash normalnormalAbdominal CTAbdominal CThelliphellip
Abdominal CTAbdominal CT
Aortic thrombosis extending into bilateral Aortic thrombosis extending into bilateral iliacsiliacsL2 Chance fractureL2 Chance fractureFree abdominal fluidFree abdominal fluidMesenteric injuryMesenteric injuryRight sided abdominal wall ruptureRight sided abdominal wall rupture
Transfer to TCHTransfer to TCH
100cc 100cc pRBCspRBCs enrouteenrouteArrived approx 3 hours since MVCABG 703496313 BE -18 Hct 247 platelets 208PT 191 INR 158 PTT 35
Additional fluid resuscitationAdditional fluid resuscitationPlacement of left chest tube for effusionPlacement of left chest tube for effusionTo ORTo OR
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Evacuation of Evacuation of intraperitonealintraperitoneal bloodbloodLigationLigation of bleeding mesenteric vesselsof bleeding mesenteric vessels
Multiple mesenteric tearsMultiple mesenteric tears
Packing of right abdominal wall disruptionPacking of right abdominal wall disruption
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
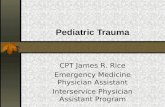
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
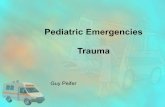
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

HPIHPI
4yo healthy male4yo healthy maleMVC headMVC head--on at 65mphon at 65mphBack seat passengerBack seat passengerRestrained by lap beltRestrained by lap beltCrying at the sceneCrying at the sceneUnable to move lower extremitiesUnable to move lower extremitiesTaken to outside hospitalTaken to outside hospital
Outside HospitalOutside Hospital
HypotensiveHypotensive2 units 2 units pRBCspRBCs 800ml NS 800ml NS
hcthct 185 185 INR 172INR 172 72430349137243034913--1313IntubatedIntubatedDislocated right ankleDislocated right ankle
Reduced and splintedReduced and splinted
Head CT Head CT ndashndash normalnormalChest CT Chest CT ndashndash normalnormalAbdominal CTAbdominal CThelliphellip
Abdominal CTAbdominal CT
Aortic thrombosis extending into bilateral Aortic thrombosis extending into bilateral iliacsiliacsL2 Chance fractureL2 Chance fractureFree abdominal fluidFree abdominal fluidMesenteric injuryMesenteric injuryRight sided abdominal wall ruptureRight sided abdominal wall rupture
Transfer to TCHTransfer to TCH
100cc 100cc pRBCspRBCs enrouteenrouteArrived approx 3 hours since MVCABG 703496313 BE -18 Hct 247 platelets 208PT 191 INR 158 PTT 35
Additional fluid resuscitationAdditional fluid resuscitationPlacement of left chest tube for effusionPlacement of left chest tube for effusionTo ORTo OR
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Evacuation of Evacuation of intraperitonealintraperitoneal bloodbloodLigationLigation of bleeding mesenteric vesselsof bleeding mesenteric vessels
Multiple mesenteric tearsMultiple mesenteric tears
Packing of right abdominal wall disruptionPacking of right abdominal wall disruption
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Outside HospitalOutside Hospital
HypotensiveHypotensive2 units 2 units pRBCspRBCs 800ml NS 800ml NS
hcthct 185 185 INR 172INR 172 72430349137243034913--1313IntubatedIntubatedDislocated right ankleDislocated right ankle
Reduced and splintedReduced and splinted
Head CT Head CT ndashndash normalnormalChest CT Chest CT ndashndash normalnormalAbdominal CTAbdominal CThelliphellip
Abdominal CTAbdominal CT
Aortic thrombosis extending into bilateral Aortic thrombosis extending into bilateral iliacsiliacsL2 Chance fractureL2 Chance fractureFree abdominal fluidFree abdominal fluidMesenteric injuryMesenteric injuryRight sided abdominal wall ruptureRight sided abdominal wall rupture
Transfer to TCHTransfer to TCH
100cc 100cc pRBCspRBCs enrouteenrouteArrived approx 3 hours since MVCABG 703496313 BE -18 Hct 247 platelets 208PT 191 INR 158 PTT 35
Additional fluid resuscitationAdditional fluid resuscitationPlacement of left chest tube for effusionPlacement of left chest tube for effusionTo ORTo OR
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Evacuation of Evacuation of intraperitonealintraperitoneal bloodbloodLigationLigation of bleeding mesenteric vesselsof bleeding mesenteric vessels
Multiple mesenteric tearsMultiple mesenteric tears
Packing of right abdominal wall disruptionPacking of right abdominal wall disruption
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Abdominal CTAbdominal CT
Aortic thrombosis extending into bilateral Aortic thrombosis extending into bilateral iliacsiliacsL2 Chance fractureL2 Chance fractureFree abdominal fluidFree abdominal fluidMesenteric injuryMesenteric injuryRight sided abdominal wall ruptureRight sided abdominal wall rupture
Transfer to TCHTransfer to TCH
100cc 100cc pRBCspRBCs enrouteenrouteArrived approx 3 hours since MVCABG 703496313 BE -18 Hct 247 platelets 208PT 191 INR 158 PTT 35
Additional fluid resuscitationAdditional fluid resuscitationPlacement of left chest tube for effusionPlacement of left chest tube for effusionTo ORTo OR
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Evacuation of Evacuation of intraperitonealintraperitoneal bloodbloodLigationLigation of bleeding mesenteric vesselsof bleeding mesenteric vessels
Multiple mesenteric tearsMultiple mesenteric tears
Packing of right abdominal wall disruptionPacking of right abdominal wall disruption
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Transfer to TCHTransfer to TCH
100cc 100cc pRBCspRBCs enrouteenrouteArrived approx 3 hours since MVCABG 703496313 BE -18 Hct 247 platelets 208PT 191 INR 158 PTT 35
Additional fluid resuscitationAdditional fluid resuscitationPlacement of left chest tube for effusionPlacement of left chest tube for effusionTo ORTo OR
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Evacuation of Evacuation of intraperitonealintraperitoneal bloodbloodLigationLigation of bleeding mesenteric vesselsof bleeding mesenteric vessels
Multiple mesenteric tearsMultiple mesenteric tears
Packing of right abdominal wall disruptionPacking of right abdominal wall disruption
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Evacuation of Evacuation of intraperitonealintraperitoneal bloodbloodLigationLigation of bleeding mesenteric vesselsof bleeding mesenteric vessels
Multiple mesenteric tearsMultiple mesenteric tears
Packing of right abdominal wall disruptionPacking of right abdominal wall disruption
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Aortic repairAortic repairLongitudinal Longitudinal aortotomyaortotomyComplete circumferential transection of the intima Complete circumferential transection of the intima below IMA sliding inferiorly and occluding bilateral below IMA sliding inferiorly and occluding bilateral iliacsiliacsDistal intima pulled up and tacked downDistal intima pulled up and tacked downDistal thrombectomiesDistal thrombectomiesAorta closed longitudinally with running Aorta closed longitudinally with running proleneprolene
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Traumatic transection of the terminal ileum Traumatic transection of the terminal ileum from the cecumfrom the cecumResection of Resection of devascularizeddevascularized bowelbowel
Included some ascending colonIncluded some ascending colon
Three segments of closedThree segments of closed--loop bowelloop bowelvented with drainsvented with drains
Open abdomenOpen abdomen
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
Prophylactic bilateral lower extremity Prophylactic bilateral lower extremity fasciotomiesfasciotomiesRight chest tube for effusionRight chest tube for effusion
To PICU on dopamine and epinephrineTo PICU on dopamine and epinephrineABG 736356720 BE ABG 736356720 BE --5555Hematocrit 39Hematocrit 39Platelets 109Platelets 109INR 117INR 117
Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Emergent Exploratory LaparotomyEmergent Exploratory Laparotomy
EBL 3 Liters Fluid Replacement
14 units pRBCs1 liter FFP13 platelet random donor units24mg Factor VIIa65 L crystalloid500ml Albumin
UOP 1800ml
POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

POD 1POD 1
Continued resuscitationContinued resuscitationProfound respiratory failureARDSProfound respiratory failureARDS
HypoxemiaHypoxemiaSwitched from conventional ventilation to High Switched from conventional ventilation to High Frequency Oscillatory Ventilation (HFOV)Frequency Oscillatory Ventilation (HFOV)Improved respiratory statusImproved respiratory status
Taken back to OR for Taken back to OR for decompensationdecompensationResection of necrotic ileum ascending colon and Resection of necrotic ileum ascending colon and left colonleft colon
Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Postoperative CoursePostoperative Course
Abdominal washout POD 1 and 3Abdominal washout POD 1 and 3Abdominal closure POD 5Abdominal closure POD 5
115cm of proximal small bowel ends as jejunostomy115cm of proximal small bowel ends as jejunostomyTransverse colon mucous fistulaTransverse colon mucous fistulaHartmannHartmannrsquorsquos pouchs pouch
Fevers POD10Fevers POD10Candida from tracheal aspirateCandida from tracheal aspirate
Extubated POD 14Extubated POD 14
Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Postoperative CoursePostoperative Course
Spinal fusion on POD 33Spinal fusion on POD 33
CurrentlyCurrentlyAwake and alertAwake and alertAbdominal wound closedAbdominal wound closedPO intake + tube feedsPO intake + tube feedsParaplegiaParaplegia
Approx T10 levelApprox T10 level
Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Seat Belt SyndromeSeat Belt SyndromeGarret and Garret and BraunsteinBraunstein in 1962in 1962Hip and abdominal contusionsHip and abdominal contusions
ldquoldquoseat belt signseat belt signrdquordquo
Pelvic fracturesPelvic fracturesIntraabdominal injuriesIntraabdominal injuries
Solid and hollow visceraSolid and hollow viscera
Lumbar spine injuriesLumbar spine injuriesSubluxationsSubluxations and compression fractures L2and compression fractures L2--44
Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Abdominal Wall EcchymosisAbdominal Wall Ecchymosis
2004 2004 J Pediatric SurgeryJ Pediatric Surgery Lutz et al Lutz et al147985 children in 102548 crashes147985 children in 102548 crashesOccurred in 133Occurred in 133
Intraabdominal injury occurred in 115Intraabdominal injury occurred in 115Significant intraSignificant intra--abdominal injury 232 times more abdominal injury 232 times more likelylikely
Sensitivity Sensitivity ndashndash 735735Negative predictive value Negative predictive value ndashndash 999999
Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Mechanism of InjuryMechanism of Injury
Improper position of lap belt serves as a fulcrum Improper position of lap belt serves as a fulcrum during rapid decelerationduring rapid deceleration
Spine Spine hyperflexeshyperflexesDirect pressure on abdominal visceraDirect pressure on abdominal viscera
Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Presubmarining and jackknifing
Classic submarining
Submariningjackknifing
IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

IntraIntra--abdominal Injuriesabdominal Injuries
GI tract perforationsGI tract perforationsSmall bowel mesenteric tearsSmall bowel mesenteric tearsSolid organ injurySolid organ injury
Due to direct compressionDue to direct compression
Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Lumbar Spine InjuriesLumbar Spine Injuries
Compression fracturesCompression fracturesChance fracturesChance fractures
Horizontal fracturesHorizontal fracturesSpinous processSpinous processPediclesPediclesVertebral bodyVertebral body
Rupture of posterior ligaments in up to 50Rupture of posterior ligaments in up to 50
Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Seat Belt AortaSeat Belt Aorta
Dissection of the intima caused by direct Dissection of the intima caused by direct compression of the vessel between the compression of the vessel between the horizontal part of the seat belt and the horizontal part of the seat belt and the vertebraevertebraeDescribed in 1979 by Described in 1979 by DajeeDajee et alet alTwo forcesTwo forces
Direct compressionDirect compressionIndirect shear forcesIndirect shear forces
Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Seat Belt AortaSeat Belt Aorta
Blunt injury to Blunt injury to abdominalabdominal aorta is uncommonaorta is uncommonAortic injury after blunt trauma occurs in 10Aortic injury after blunt trauma occurs in 10--1515
lt5 involves abdominal aortalt5 involves abdominal aorta1997 1997 J TraumaJ Trauma ndashndash 62 reported cases62 reported cases
Commonly associated injuriesCommonly associated injuriesSeat belt sign Seat belt sign ndashndash 4747Bowel injury Bowel injury ndashndash 4747LumbosacralLumbosacral spine injury spine injury ndashndash 3535
Mortality rate 24Mortality rate 24
Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Seat Belt AortaSeat Belt Aorta
Recognized abnormalitiesRecognized abnormalities39 39 -- intimal injury with acute and complete vessel intimal injury with acute and complete vessel occlusionocclusion16 16 -- intimal tears without occlusionintimal tears without occlusion15 15 -- true aneurysmstrue aneurysms5 5 -- aortic ruptureaortic rupture
Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Aortic Occlusion Secondary to Aortic Occlusion Secondary to Blunt TraumaBlunt Trauma
2002 2002 J TraumaJ Trauma MeghooMeghoo et al et al 36 reported cases36 reported cases
78 cases from 78 cases from MVCsMVCs
Prolapse of distal intimal flap after Prolapse of distal intimal flap after circumferential tearcircumferential tearAccompanying Accompanying subintimalsubintimal thrombusthrombus
Higher incidence in atherosclerotic diseaseHigher incidence in atherosclerotic disease
Mortality 41Mortality 41
Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Our PatientOur Patient
Rare injury triadRare injury triadAbdominal aortic injuryAbdominal aortic injuryLumbar Chance fractureLumbar Chance fractureMesentericvisceral injuriesMesentericvisceral injuries
12 reported cases in pediatric patients12 reported cases in pediatric patients2006 2006 J TraumaJ Trauma ChoitChoit et alet alAll secondary to All secondary to MVCsMVCs7 lap belts7 lap belts5 unknown restraints5 unknown restraints
Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Proper RestraintsProper Restraints
2007 2007 Journal of TraumaJournal of Trauma ArbogastArbogast et alet alRestrained children with abdominal organ Restrained children with abdominal organ injuriesinjuriesLow injury rates in other vehicle occupantsLow injury rates in other vehicle occupants
40 drivers 40 drivers 10 other child occupants10 other child occupants
Suboptimal restrained kids 38 times more likely Suboptimal restrained kids 38 times more likely to suffer intraabdominal injuryto suffer intraabdominal injury
High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

High Frequency Oscillatory High Frequency Oscillatory Ventilation (HFOV)Ventilation (HFOV)
Introduced in 1972Introduced in 1972Reciprocating pumps or diaphragmsReciprocating pumps or diaphragms
Active inspiration and expirationActive inspiration and expiration
Small tidal volumes (Small tidal volumes (VVTTss))Higher mean airway pressure (mPaw)Higher mean airway pressure (mPaw)
Limits alveolar Limits alveolar derecruitmentderecruitment and overdistentionand overdistention
Rapid respiratory ratesRapid respiratory ratesAdequate gas exchangeAdequate gas exchange
Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Chan K P W et al Chest 20071311907-1916
Schematic representation of the purported waveforms of HFOV and conventional pressure-controlled ventilation in the distal airways
HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

HFOVHFOV
Oscillating piston pump (or diaphragm)Oscillating piston pump (or diaphragm)180 to 600 breathsmin (3 to 10 Hz)180 to 600 breathsmin (3 to 10 Hz)Active inspiration and expirationActive inspiration and expiration
Inspiratory bias gas flow (30 to 60 Lmin)Inspiratory bias gas flow (30 to 60 Lmin)mPawmPaw
Resistance valveResistance valvemPawmPaw
OxygenationOxygenationFiO2 and mPawFiO2 and mPaw
VentilationVentilationRespiratory frequency and pressure amplitudeRespiratory frequency and pressure amplitude
Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Mechanism of Gas TransportMechanism of Gas Transport
Conventional Mechanical Ventilation (CMV)Conventional Mechanical Ventilation (CMV)Convective or bulk flowConvective or bulk flow
HFOVHFOVConvective and diffusiveConvective and diffusive
Bulk flow proximallyBulk flow proximallyAsymmetric velocity profilesAsymmetric velocity profilesTaylor dispersionTaylor dispersionPendelluftPendelluftCollateral ventilationCollateral ventilationCardiogenic mixingCardiogenic mixing
Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

Krishnan J A et al Chest 2000118795-807
Proposed mechanisms of gas transport during HFV
1) Direct Bulk Flow2) Longitudinal (Taylor)
dispersion3) Pendelluft4) Asymmetric velocity
profiles5) Cardiogenic mixing6) Molecular diffusion
VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

VentilatorVentilator--Induced Lung InjuryInduced Lung Injury
Increased in ALIARDSIncreased in ALIARDSBarotraumaBarotrauma
Secondary to pressureSecondary to pressure
VolutraumaVolutraumaAlveolar overdistentionAlveolar overdistentionDistributed to compliant lungDistributed to compliant lung
AtelectraumaAtelectraumaParenchymalParenchymal injuryinjuryRepetitive openingcollapse of distal airwaysRepetitive openingcollapse of distal airways
HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

HFOVHFOV
LungLung--protective strategies developedprotective strategies developedHFOV may be idealHFOV may be ideal
Comparatively higher mPawComparatively higher mPawAllows recruitmentprevents Allows recruitmentprevents derecruitmentderecruitmentHigher endHigher end--expiratory lung volumeexpiratory lung volume
Lower tidal volumeLower tidal volumeGas exchange at lower airway pressuresGas exchange at lower airway pressuresLimits alveolar overdistentionLimits alveolar overdistentionLess cardiovascular effectLess cardiovascular effect
ldquoldquoOpen LungOpen Lungrdquordquo conceptconceptMaintains open airwaysMaintains open airways
HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

HFOVHFOV
Conversion to HFOVConversion to HFOVPeak pressures gt35cm H2OPeak pressures gt35cm H2OmPaw approaches 15 to 18cm H2OmPaw approaches 15 to 18cm H2OFiO2 gt 06FiO2 gt 06
Better to convert earlierBetter to convert earlier of days on CMV was an independent predictor of mortality of days on CMV was an independent predictor of mortality
Initial settingsInitial settingsFiO2 09 FiO2 09 ndashndash 1010mPaw 5cm above last measured mPaw on CMVmPaw 5cm above last measured mPaw on CMVBias flow 40LminBias flow 40LminConsider recruitment maneuversConsider recruitment maneuvers
PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

PRCT CMV PRCT CMV vsvs HFOVHFOV
2002 2002 Am J Am J RespResp CritCrit Care Care DerdakDerdak et alet al148 adults 13 centers148 adults 13 centers
HFOV earlier improvement in PaO2FiO2 ratioHFOV earlier improvement in PaO2FiO2 ratiolt16 hourslt16 hoursDid not persist beyond 24 hoursDid not persist beyond 24 hours
HFOV HFOV nonsignificantnonsignificant trend toward lower 30trend toward lower 30--day mortalityday mortality37 37 vsvs 52 (p=0102)52 (p=0102)
Similar but low adverse eventsSimilar but low adverse eventsPrior to ARDS Network trialPrior to ARDS Network trial
VVTTss 10mlkg used10mlkg used
ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

ARDS in Surgical PatientsARDS in Surgical Patients2006 2006 J TraumaJ Trauma Kao et alKao et al16 surgical patients with ARDS16 surgical patients with ARDS
Oxygenation failureOxygenation failure
HFOV significant findingsHFOV significant findingsIncreased PaO2FiO2 ratio after 30 minIncreased PaO2FiO2 ratio after 30 min
Maintained after 12 hours out to 40 hoursMaintained after 12 hours out to 40 hours
Oxygenation index decreased at 24 and 32 hrsOxygenation index decreased at 24 and 32 hrsOI [ FiO2 x mPaw x 100 PaO2 ]OI [ FiO2 x mPaw x 100 PaO2 ]
No change in systolic BPNo change in systolic BPNo complicationsNo complications
PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

PediatricsPediatrics
No pediatric studies to support lung protective No pediatric studies to support lung protective strategy in ARDSstrategy in ARDSMost HFOV studies looking at neonatesMost HFOV studies looking at neonatesJaballahJaballah et al 20 patientset al 20 patients
Failed CMV switched to HFOVFailed CMV switched to HFOVAfter 1 hourAfter 1 hour
Improved ventilation in all 20Improved ventilation in all 20Improved oxygenation in 1920Improved oxygenation in 1920
Only 1 death from respiratory failureOnly 1 death from respiratory failure
HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

HFOV SummaryHFOV Summary
2007 review of HFOV in ARDS2007 review of HFOV in ARDS2 2 PRCTsPRCTs and 12 case seriesand 12 case seriesSafe and consistently improves oxygenation Safe and consistently improves oxygenation when used as rescue mode for ventilationwhen used as rescue mode for ventilation
Delayed initiation of HFOV is an independent Delayed initiation of HFOV is an independent predictor of deathpredictor of deathTrend towards lower mortalityTrend towards lower mortality
AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

AAP AAP -- Car Seat GuidelinesCar Seat GuidelinesRearRear--facing seatfacing seat
Infant Infant 1 year 1 year andand 20 lbs20 lbsForwardForward--facing seatfacing seat
Until 3Until 3--5 years old or 405 years old or 40--60 lbs60 lbsBooster seat with lapshoulder beltBooster seat with lapshoulder belt
Until approx 8Until approx 8--12 years old12 years oldUntil 4Until 4rsquorsquo 99rdquordquo
Seat beltSeat beltShoulder belt crosses mid chestShoulder belt crosses mid chestLap belt across upper thighs not stomachLap belt across upper thighs not stomachKnees bent over seatKnees bent over seat
ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-

ReferencesReferences
Durbin D et al Seat belt syndrome in children A case report Durbin D et al Seat belt syndrome in children A case report and review of the and review of the literature literature PedPed Emergency CareEmergency Care 2001 1716 4742001 1716 474--477477ArbogastArbogast K et al Mechanisms of abdominal organ injury in seat beltK et al Mechanisms of abdominal organ injury in seat belt--restrained restrained children children J TraumaJ Trauma 2007 6214732007 621473--14806831480683MeghooMeghoo C et al Complete occlusion after blunt injury to the abdominC et al Complete occlusion after blunt injury to the abdominal aorta al aorta J J TraumaTrauma 200355795200355795--799799ChoitChoit R et al Abdominal aortic injuries associated with chance fraR et al Abdominal aortic injuries associated with chance fractures in pediatric ctures in pediatric patients patients J J PedPed SurgSurg 20064111842006411184--11901190Lutz N et al Incidence and clinical significance of abdominalLutz N et al Incidence and clinical significance of abdominal wall bruising in wall bruising in restrained children involved in motor vehicle crashes restrained children involved in motor vehicle crashes J J PedsPeds SurgSurg 2004 399722004 39972--975975LalencetteLalencette M et al SeatM et al Seat--belt aorta A rare injury associated with blunt abdominal belt aorta A rare injury associated with blunt abdominal trauma trauma Ann Ann VascVasc SurgSurg 200620681200620681--Turner D and Arnold J Insights in pediatric ventilation timinTurner D and Arnold J Insights in pediatric ventilation timing of g of intubationintubation ventilatoryventilatory strategies and weaning strategies and weaning Current Opinion in Critical Care Current Opinion in Critical Care 2007 13572007 1357--6363Kao K et al High frequency oscillatory ventilation for surgicKao K et al High frequency oscillatory ventilation for surgical patients with acute al patients with acute respiratory distress syndrome respiratory distress syndrome J TraumaJ Trauma 2006 614837 2006 614837--843843Chan K et al HighChan K et al High--frequency oscillatory ventilation for adult patients with ARDS frequency oscillatory ventilation for adult patients with ARDS ChestChest 2007 131619072007 13161907--19161916Krishnan J and Brower R HighKrishnan J and Brower R High--frequency ventilation for acute lung injury and ARDS frequency ventilation for acute lung injury and ARDS ChestChest 2000 118 7952000 118 795--807807
- Case PresentationPediatric Trauma
- HPI
- Outside Hospital
- Abdominal CT
- Transfer to TCH
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- Emergent Exploratory Laparotomy
- POD 1
- Postoperative Course
- Postoperative Course
- Seat Belt Syndrome
- Abdominal Wall Ecchymosis
- Mechanism of Injury
- Intra-abdominal Injuries
- Lumbar Spine Injuries
- Seat Belt Aorta
- Seat Belt Aorta
- Seat Belt Aorta
- Aortic Occlusion Secondary to Blunt Trauma
- Our Patient
- Proper Restraints
- High Frequency Oscillatory Ventilation (HFOV)
- HFOV
- Mechanism of Gas Transport
- Ventilator-Induced Lung Injury
- HFOV
- HFOV
- PRCT CMV vs HFOV
- ARDS in Surgical Patients
- Pediatrics
- HFOV Summary
- AAP - Car Seat Guidelines
- References
-