Carotid artery stenosis
24
Carotid Artery Stenosis ENDARTERECTOMY vs STENTING
-
Upload
ramachandra-barik -
Category
Health & Medicine
-
view
170 -
download
2
Transcript of Carotid artery stenosis

Carotid Artery StenosisENDARTERECTOMY vs STENTING

Keywords
1. CAS2. CEA3. BMT

Prevalence
ICA stenosis is estimated to be 2% to 3% in the general population, with increased prevalence noted in men and the elderly

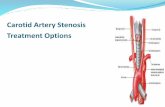
Carotid atheroma
The bifurcation point of the common carotid artery, or carotid bulb,is predisposed to the development of atherosclerosis owing to low wall shear stress and resulting flow stagnation. Narrowing or stenosis of the carotid bulb and ICA because of atherosclerosis can lead to ischemic stroke secondary to plaque embolization or hypo-perfusion

Risk factors
• Smoking• Hypertension• Hyperlipidemia• coronary artery disease (CAD)• diabetes mellitus• peripheral arterial disease• abdominal aortic aneurysm• Racial predilection

Transient ischemic attacks
Stroke like symptoms that last <24 hours, are also associated with an increased risk of early recurrent stroke, particularly in patients with carotid artery atherosclerosis.

STROKE
Acute development of a focal neurological deficit attributable to the disruption of blood flow to the brain, is caused by ischemia or haemorrhage. The majority (>80%) of strokes are of ischemic aetiology, of which ≈15% to 20% are attributable to atherosclerosis of the extra cranial carotid arteries. The risk of death and recurrent stroke increases following an ischemic stroke.

ENDARTERECTOMY
surgical removal of part of the inner lining of an artery, together with any obstructive deposits, most often carried out on the carotid artery or on vessels supplying the legs.

STENTING
In medicine, a splint placed temporarily inside a duct, canal, or blood vessel to relieve an obstruction

Diagnosis
1. Non-invasive :Duplex ultrasound, computed tomographic angiography, and magnetic resonance angiography have essentially replaced cerebral angiography, given their high sensitivity and specificity for identifying high grade carotid stenosis.
2. Invasive : Conventional cerebral angiography is considered the gold standard test for the diagnosis of carotid artery stenosis

Prevent stroke
1. Best medical therapy (BMT)2. Carotid endarterectomy (CEA) 3. Carotid artery stenting (CAS)

Decision is affected by
1. Patient factors:Age,sex,life expectancy ,comorbidity, operative risk ,preference
2. Disease factors: Risk of stroke and anatomical consideration 3. Skill of the operator
1. a minimum of 30 to 150 diagnostic cervicocerebral angiograms, and 25 to 75 CAS procedures
2. operator volume of ≥6 cases per year and center experience of >150 CAS procedures associated with the best outcomes

CREST and metanalysis
Age ≥70 years has been associated with increased periprocedural riskwith CAS in comparison with CEA

Unstable plaques
1. Ulceration2. intraplaque haemorrhage on MRI3. rapid progression4. increased plaque area5. plaque heterogeneity with increased echolucency6. low grey-scale 7. Presence of discrete white areas within the plaque.

Hostile neck
1. Previous radical neck surgery2. External beam radiotherapy3. Contralateral laryngeal nerve palsy4. Tracheostomy

Hostile carotid
Plaque distal to the C2 vertebral body or proximal to the clavicle because they are difficult to tackle surgically
ICA-common carotid artery angulation >60 degrees, targetICA lesion >10 to 15 mm in length, ostial involvement of thelesion, and excessive calcification have been associated with worseoutcomes in CAS-treated patients in comparison with CEA-treatedpatients

CEA is gold standard
1. 2 large RCTs in the 1990s (NASCET, ECST) demonstrated the superiority of CEA over medical management for stroke prevention.
2. 2 large asymptomatic trials (ACAS, ACST) also showed a small (6%) reduction in stroke rate with CEA at 5 years in comparison with medical therapy.
3. Asymptomatic patients for CEA is guided by a detailed assessment of patient life expectancy, comorbid conditions, surgeon/institution stroke rate, and patient preference.

CAS
1. introduction in 19802. Use of stent and embolic protection devices3. Endovascular tools and equipment4. New antiplatelet drugs5. Not superior to CAE

CEA vs CAS

Advantages of CAS
1. Lower risk of perioperative MI2. Suitable option for high-risk patients3. Suitable option for patients with hostile neck or hostile carotid4. Can be performed under local/regional anaesthesia

Disadvantages of CAS
1. Higher risk of perioperative stroke2. Associated with worse outcomes in symptomatic patients and the
elderly3. Not a suitable option for patients with lesions at high risk of
periprocedural embolization4. Evidence for noninferiority in standard-risk and asymptomatic
patients is limited


Current evidence
CEA is the gold standard Rx when the patient is not at high operative risk attributable to a hostile neck or significant comorbidities