Carotid Artery Disease and Carotid StentingAsymptomatic Carotid Artery Stenosis • SMART Study –...
69
Carotid Artery Disease and Carotid Stenting University of Maryland School of Medicine Khanjan H. Nagarsheth MD, MBA, FACS, RPVI Assistant Professor of Surgery Medical Director of Imaging Core Lab Medical Director of Office Based Lab Co-Director Limb Preservation Clinic Medical Director Vascular Surgery Progressive Care Unit Associate Program Director, Vascular Surgery Fellowship Division of Vascular Surgery University of Maryland School of Medicine Baltimore, MD
Transcript of Carotid Artery Disease and Carotid StentingAsymptomatic Carotid Artery Stenosis • SMART Study –...

Carotid Artery Disease and Carotid Stenting
University of Maryland School of Medicine
Khanjan H. Nagarsheth MD, MBA, FACS, RPVIAssistant Professor of Surgery
Medical Director of Imaging Core LabMedical Director of Office Based LabCo-Director Limb Preservation Clinic
Medical Director Vascular Surgery Progressive Care UnitAssociate Program Director, Vascular Surgery Fellowship
Division of Vascular SurgeryUniversity of Maryland School of Medicine
Baltimore, MD

Disclosures• No financial disclosures relevant to this
presentation

The Press
Rabin RC, New York Times, 2/26/2010

Risk of Stroke in Asymptomatic Patients
Chambers et al. NEJM. 315(14):860-5, 1986.Norris et al. Stroke. 22(12):1485-90, 1991.

Which Modality is Superior?Endarterectomy?
Stenting?
Best Medical Therapy?

Medical Therapy• Modulators of the Renin Angiotensin System**
– Ace Inhibitors– Angiotensin Receptor Blockers
• HMG CoA Reductase Inhibitors**
• New antiplatelet therapies**
**These therapies did not exist during the pivotal carotid revascularization trials

The PROGRESS Trial
PROGRESS Collaborative Group. Lancet. 358(9287):1033-41, 2001.

The SPARCL Trial
Amarenco P et al. NEJM. 355(6):549-59, 2006.

Asymptomatic Carotid Artery Stenosis• SMART Study
– 221 patients with followed for 5 years
• Oxford Vascular Study
– 101 patients followed for 3 years
• <0.5% stroke risk per year in patients with >50% carotid artery stenosis
Goessens BM et al. J Vasc Surg. 43(3):525-32, 2006.Marquardt L et al. Stroke. 41(1):e11-7, 2010.

Asymptomatic Moderate to Severe Stenosis
• Overall annual risk of stroke ~0.5 - 1% with medical management
• Carotid duplex US q 6 month at first, then annually if stable
• If stenosis worsens despite maximum medical management, consider revascularization
• Lifestyle modification (quit smoking, eat better, exercise)
• Antiplatelet monotherapy preferred to combination
• Target LDL <70
• Unilateral asymptomatic stenosis (>70%) BP goal <140/90

Medical Management Prevention of Disease Progression
Conrad MF et al. J Vasc Surg. 60(5):1218-25, 2014.

Carotid Endartectomy• The model of evidenced based medicine in surgery
• Most common procedure performed by vascular surgeons in this country
• Long term benefits and stroke from survival
• The standard against which we measure everything else for carotid disease

Adoption of New Technologies
20122015
1989
2006

Disruptive Technology

Disruptive Technology

Outcomes of Carotid Revascularization Trials
Asymptomatic
Symptomatic

Carotid Stents

Carotid Stent Approval• FDA
– Asymptomatic >80% stenosis, high risk for CEA– Symptomatic >50% stenosis, high risk for CEA
• CMS
– Symptomatic >70% stenosis, high risk for CEA– Must use embolic protection device– Must use single stent– Must be Rankin 0-3– Must be certified by CMS as a qualified center and all cases must be
entered into the CMS database

SAPPHIRE Trial• 723 patient enrolled• >50% ICA stenosis with symptoms• >80% ICA stenosis with no symptoms• > 1 comorbid condition
• Randomized – Stenting with embolic protection – 159 patients– CEA – 151 patients
• Enrolled into registry– Refused surgery – 409 patients– Refused stent – 7 patients
• Primary endpoint – 30 day stroke, death, MI
Yadav et al. NEJM. 351(15):1493-501, 2004.

SAPPHIRE Trial• Outcomes for stents:
– Death 0.6%– Major Stroke 0.6%– Minor Stroke 3.2%– MI 2.6%– Combined endpoint 5.8%
• Outcomes for CEA– Death 2%– Major Stroke 2%– Minor Stroke 3.3%– MI 7.3%– Combined endpoint 12.6%
Yadav et al. NEJM. 351(15):1493-501, 2004.

SAPPHIRE Trial• No difference in occurrence of major adverse
event at 3 years
• No difference in death at 3 years
• No difference in ipsilateral stroke at 3 years
• No difference in need for reintervention
Yadav et al. NEJM. 351(15):1493-501, 2004.

Event Rates of Carotid Stenting Trials

EVA-3S Trial• Stent-protected angioplasty v. CEA in symptomatic patients
with >60% ICA stenosis
• 872 patients needed for non-inferiority• 527 patients enrolled – trial stopped for safety and futility
reasons
• Primary endpoint – 30-day stroke/death– CEA 3.9% v. CAS 9.6%– 6 month stroke/death – CEA 6.1% v. CAS 11.7%
• 17% of patients did not get loaded with Plavix prior to CAS
Mas et al. NEJM. 355;1660:2006.

EVA-3S Revisited• Follow up revealed no difference in stroke
rates between CEA and CAS at 4 years

PROTECT Trial• 30-day major adverse events in high risk patients
– Death 0.5%
– Stroke 0.5%
– MI 0.4%
– Combined endpoint 2.3%
– Annulaized ipsilateral stroke rate of 0.4% following CAS
Matsumura JS, et al. J Vasc Surg. 55(4);968-976, 2012.

CREST• Prospective, multicenter, randomized, controlled trial
with blinded endpoint adjudication
• CAS v. CEA in 2300 patients with symptomatic and asymptomatic stenosis
• 117 total sites between USA and Canada
• Only 52% of applicants were selected as CAS operators due to a rigorous credentialing process

CREST
Carotid Stent Endarterectomy p-Value
Periop Stroke 4.1% 2.3% 0.01
MI 1.1% 2.3% 0.03
Stroke/Death/MI 5.2% 4.5% 0.38
Major Stroke 0.9% 0.6% 0.52
Cranial nerve injury 0.3% 4.7% <0.01

CREST• No difference for primary endpoint at follow
up

CREST• Long term mortality was correlated more
strongly with MI
Gray et al. Circulation 2012…

CREST• Neither age nor presence of symptoms
affected primary EP
Gray et al. Circulation 2012…

CREST
Gray et al. Circulation 2012…

CREST• Cranial nerve injuries examined
Gray et al. Circulation 2012…

CREST• Critics of the study align with either CEA or CAS
• Those in favor of CEA claim:– Strokes are more likely with CAS than CEA and patients care more
about stroke than MI– Most MI were minor (troponin spill)– Most cranial nerve injuries resolved
• Those in favor of CAS claim:– CAS technology in CREST is now considered outdated– Early learning curve for CAS makes it accessible by most operators– Cranial nerve injury and MI are very morbid for patients

Largest Trials for CAS v. CEA
Trial 30-Day Outcome for Stroke and MICEA CAS p-Value
EVA-3S 3.9% 9.6% 0.01
SPACE 6.3% 6.8% 0.09
ICSS 4.7% 8.5% 0.001
CREST (symptomatic) 5.4% 6.7% 0.30

CEA versus CAS in Symptomatic Patients
• CAS and CEA are equivalent in primary endpoint and long-term stroke prevention in CREST
• Large, controlled single arm studies of high risk patientsAHA guideline standard recommendation
– EU trials were flawed in design
– Significant improvement in devices, technology and distal protection during the course of studies
– More wound complications and cranial nerve injury with CEA

CEA versus CAS in Asymptomatic Patients
• Asymptomatic carotid stenosis is a risk factor for stroke• Surgical revascularization is proven beneficial v. unmonitored
medical therapy
• CAS outcomes have equivalent outcomes to CEA (CREST), achieved AHA guidelines and have a Class IIb recommendation in asymptomatic patients– CEA is Class Iia
• The available randomized controlled data supports revascularization in suitable patients with high grade asymptomatic stenosis– Medical therapy is attractive but not proven head to head

Extra-cranial Vascular Disease Guidelines
Stroke, 2011;42:e464-e540.

Classification of Recommendations

Recommendations Based on ECVD Guidelines
Symptomatic Symptomatic Asymptomatic
50-69% stenosis 70-99% stenosis 70-99% stenosis
CEA Class I Level B Class I Level A Class IIa Level A
CAS Class I Level B Class I Level B Class IIb Level B

Cost Comparison CEA v. CAS

The Plot Thickens

International Carotid Stenting Study
• 1710 patients enrolled, all who were recently symptomatic with stroke or TIA
• Primary goal was to determine long term survival, free of disabling stroke
• Had 3-year follow up data
Lancet February 2010

International Carotid Stenting Study

CREST 2• Carotid revascularization and medical
management for asymptomatic carotid disease
• Parallel study design with 1240 patients in each trial

Definition• Criteria for > 70% ICA stenosis
– PSV >230 cm/sec plus one of the following criteria
– EDV > 100 cm/sec
– ICA/CCA > 4
– > 70% stenosis on MRA
– >70% stenosis on CTA

Interventionalist Eligibility• Must have done at least 50 total procedures
• If <50, then must have done at least 8 in last 2 years
• Each operator must have been reviewed and approved by the CREST-2 IMC

Which Trial Should Patients Be Put In?• Based on CREST
– Patients 50-74 years old had equivalent outcomes– Patients <50 years old did better with CAS– Patient >74 years old did better with CEA
• But in CREST asymptomatic patients had few events and very wide confidence intervals
– Therefore the choice of procedure cannot be mandated in CREST 2

CREST-2 Exclusions• Excessive or circumferential calcification of the stenotic lesion
• Lesion >20mm length, sequential lesions
• Inability to use embolic protection devices
• Excludes octogenarians
• Excludes high risk for CAS– Advanced age– Recent symptoms– Challenging anatomy

TCAR• Trans carotid artery revascularization

Periprocedural Stroke Rates Presentations & Publications of TCAR & CEA
1.3% 1.4% 1.1% 1.0%1.4% 1.2%
2.3%
3.6%
PROOF ROADSTER
UnivRochester& StonyBrook
UH,Cleveland
Multi-Center
VQI - TCARSurveillanc
eVQI - CEA CREST
SSRSVS HSR
REGISTRY
Stroke 1.3% 1.4% 1.1% 1.0% 1.4% 1.2% 2.3% 3.6%
High Surgical Risk Patients
PROOF: J Endovasc Ther. 2017 Apr;24(2):265-270ROADSTER: J Vasc Surg. 2015 Nov;62(5):1227-34. The Silk Road System for Transcervical Access with Reversal of Flow to Perform TCAR: Results of the ROADSTER Trial - VEITH, 2016Univ Rochester & Stony Brook: Transcarotid Arterial Revascularization: First Post-Approval Safety & Efficacy Study – VAM, 2018 Poster PresentationUH Cleveland: A Multi Institutional Analysis of TCAR Compared to CEA – VAM, 2018 Poster PresentationVQI TCAR + CEA: In-Hospital Outcomes of TCAR & CEA in the SVS-VQI TCAR Surveillance Project – VEITH Symposium 2018 Presentation Unadjusted Outcomes – M. Schermerhorn, MDCREST Standard Surgical Risk: N Engl J Med. 2016 Mar 17;374(11):1011-20.SVS Registry: J Vasc Surg. 2013 May;57(5):1318-24.
n=219 n=2,545n=75
TCAR
n=1,240n=292n=88
CEA
n=43,114
P=.27
n=6,370

In-Hospital Outcomes of TCAR and CEA in the SVS-VQI TCAR Surveillance ProjectMarc Schermerhorn, MD; Patric Liang, MD; Hanaa Dakour Aridi, MD; Vikram Kashyap, MD; Grace Wang, MD; Brian Nolan, MD; Jack Cronenwett, MD; Jens Eldrup-Jorgensen, MD; Mahmoud Malas, MD, MHS – VEITH Symposium Presentation, November 2018
Baseline Characteristics TCAR N=2,545
CEAN=43,114 P-value
Age, Mean (SD) 73.1 + 9.4 70.6 + 9.6 <.001
Female 36% 39% <.01
Black 5% 5% .61
Hypertension 90% 89% .50
Diabetes Mellitus 37% 36% .52
Coronary Artery Disease 51% 27% <.001
CHF 19% 11% <.001
COPD 29% 23% <.001
Chronic Kidney Disease (GFR <60) 41% 34% <.001
Prior CEA/CAS 31% 15% <.001
Asymptomatic 53% 51% .37
General Anesthesia 83% 92% <.001
Unadjusted Outcomes TCARN = 2,545
CEAN = 43,114 P-value
Stroke/Death 1.8% 1.4% .09
Stroke/Death/MI 2.1% 1.8% .17
Stroke 1.4% 1.2% .27
In-hospital Death 0.5% 0.3% .04
30-day Death 0.9% 0.6% .08
Myocardial Infarction 0.4% 0.4% .71
Hemodynamic Instability
Hypertension 12% 20% <.001
Hypotension 13% 10% <.001
Bleeding with Intervention 1.4% 1.0% .05
Reperfusion Syndrome 0.2% 0.2% .54
CNI 0.2% 2.7% <.001
Operative Time, Mins, Mean 75 + 31 116 + 45 <.001
LOS, Days, Median (IQR) 1 (1-2) 1 (1-2) .34
LOS >1 day 29% 32% <.01

TCAR - TransCarotid Artery Revascularization First Post-Approval Safety and Efficacy Study (2 Center Analysis) - VAM, June 2018Mark D. Balceniuk, MD1, Michael C. Stoner, MD1, Brian C. Ayers, MBA1, Angela Kokkosis, MD2, Apostolos Tassiopoulos, MD2
Patient Characteristics
TCARN=88
Age, Mean 72.3
Age 75+ 45%
Age 80+ 27%
Female 33%
Medical History
Diabetes 36%
Hypertension 93%
CHF 32%
CAD 56%
Current Smoker
30%
Symptomatic 38%
1. Division of Vascular Surgery, Department of Surgery, University of Rochester Medical Center, Rochester, NY2. Division of Vascular and Endovascular Surgery, Stony Brook Medicine, NY
Lesion Characteristics
TCARN=88
Side
Right 55%
Left 45%
Stenosis, Mean 87.6%
Length 20.0mm
Type
Atherosclerosis 82%
Re-stenosis CEA 13%
Re-stenosis stent 6%
Calcification
None 6%
<25% 52%
26 - 50% 23%
51 – 99% 13%
100% 6%
Procedure Detail
TCARN=88
Time (Mean)
Procedure 91.7min
Flow Reversal 13.3min
Fluoro 6.5min
Tech Success 98%
Pre-Dilate 48%
Med Mgmt
DAPT 95%
Statin 95%
Number of Stents
One 91%
Two 8%
Local Anesthesia 32%
30 Day Outcomes TCARN=88
Stroke 1.1% (1)
MI 0% (0)
Death 0% (0)
CONCLUSIONS:• All patients tolerated flow reversal.
There were no MI or death within 30 day. One patient developed a post-op watershed event (1.1%).
• In comparison to the ROADSTER trial, there were more symptomatic patients (26% vs 38%) with a similar profile of major comorbidities.
• In spite of these high risk factors, the data demonstrate an excellent safety profile with only a single post-op neurologic event.

A Multi-Institutional Analysis of TCAR Compared to CEAAlexander H. King, MS1, Vikram S. Kashyap, MD1, Mazin I. Foteh, MD2, Matthew Janko, MD1, Jeffrey Jim, MD3, Raghu Motaganahalli, MD4, Jeffrey M. Apple, MD2, SaideepBose, MD1, Norman H. Kumins, MD1 - VAM, June 2018
Baseline Characteristics TCARN=292
CEAN=371 P-value
Male, Gender 65.8% 59.6% 0.06
Age (yrs) 71.1 70.7 0.73
Symptomatic 35.3% 38.5% 0.42
Diabetes 45.9% 35.6% 0.01
Hyperlipidemia 82.9% 72.8% 0.02
Hypertension 91.1% 87.9% 0.21
Coronary Artery Disease 53.4% 36% <.01
PVD 24.7% 27.9% 0.49
Smoking History 59.6% 72.0% <0.01
Renal Insufficiency 21.2% 12.7% <0.01
Overall Outcomes TCARN =292
CEAN = 371 P-value
Stroke/MI/Death – 30 Day 2.1% 2.4% 0.80
Stroke/Death – 30 Day 1.4% 1.9% 0.76
Stroke – 30 Day 1.0% 1.1% 1.00
Mortality – 30 Day 0.3% 0.8% 0.63
MI – 30 Day 0.7% 0.5% 1.00
Stroke/Death – 1 Year 4.6% 6.8% 0.32
Stroke – 1 Year 2.8% 3.0% 1.00
Mortality – 1 Year 1.8% 3.9% 0.15
CNI 0.3% 4.1% <.01
Unresolved at 6 Months 0.0% 1.9% 0.02
1. Harrington Heart and Vascular Institute, University Hospitals Cleveland Medical Center, Cleveland, OH2. Cardiothoracic and Vascular Surgeons, Austin, TX3. Division of Vascular Surgery, Washington University, St. Louis, MO4. Division of Vascular Surgery, Indiana University School of Medicine, Indianapolis, IN
METHODS:• Multi-center, retrospective review of patients undergoing
TCAR or CEA between 2013-2017• TCAR patients had higher risk factors and most were enrolled
in prospective trials
SUMMARY: • Stroke and death rates were the same at 30 days and 1 year• TCAR demonstrated a significant decrease in CNI• “Particularly in patients at high risk for surgery, TCAR should
be considered in treatment of carotid artery disease.”

ROADSTER StudyProspective, Multi-Center, Single-Arm Trial of TCAR in High Surgical Risk Patients
with Carotid Stenosis - Pivotal + Continued Access Results
1J Vasc Surg 2015;62:227-352 N Engl J Med 2010;363:11-233 Stroke 2011;42(12):3484-904 Circulation 2012;125:2256-2264
Primary EndpointAll stroke, MI & death at 30-days
Clinical Results
*Hierarchical
Demographics and Technical ResultsDemographics and Technical Results Clinical Results
ROADSTER Pivotal ITT1 (n=141) + Continued Access (n=78) = 219
ROADSTER(n=219)
ROADSTER(n=219)
Age (mean)
Age ≥75
Female
Symptomatic
Local Anesthesia
Reverse Flow Time (median)
72.3 ±8.6
41.6%
37.9%
22.4%
47.1%
10 minutes
S/D/MI*
Major Stroke
Minor Stroke
Death
MI
All Stroke
Cranial Nerve Injury
CNI Unresolved 6 mths
8
0
3
2
3
3
1
0
0%
1.4%
0.9%
1.4%
1.4%
3.7%
0.5%
0.0%
CREST2 CEA(n=1,240)
69.2 ±8.7
28.5%3
33.6%
52.7%
10.0%
n/a
Standard RiskHigh Surgical Risk
CREST2 CEA(n=1,240)
0.6%
1.7%
0.3%
2.3%
2.3%
4.5%
5.3%
2.1%4
Standard RiskHigh Surgical Risk

PROOF Study Safety Results1,2 Result (n=75)
Subjects completing 30-day follow-up71
(94.7%)
Primary Endpoint:Composite of any major stroke, myocardial infarction and death from the index procedure through the 30-day post-procedural period
0/71 (0%)
Minor strokeMinor contralateral stroke adjudicated as not device or procedure-related
1/71(1.3%)
Cranial nerve injury (Hoarseness)2/71
(2.7%)
PROOF StudyTCAR – First in Man Experience
1. J Vasc Surg 2011;54:1317-232. J Endovasc Ther. 2017 Apr;24(2):265-2703. Lancet Neurol. 2010 Apr;9(4):353-624. J Am Coll Cardiol. 2012 Jan 19. [Epub ahead of print]
Study Procedure Embolic Protection
Patients
% w/ NewDW-MRI Lesions
ICSS3 CEA Clamp, backbleed 107 17%
PROOF2 TCAR Proximal Flow Reversal 56 23%
(18% Ipsilateral)
PROFI4 Transfemoral CAS
Proximal occlusion (MoMA) 31 45%
ICSS3 Transfemoral CAS Distal filter (various) 51 73%
PROFI4 Transfemoral CAS
Distal filter (Emboshield) 31 87%

TCAR Demonstrates TCD Embolization Rates Comparable to CEA
Vermassen, et al J Endovasc Ther April 2016 23: 249-254
• No significant differences in number of emboli (p=0.486) and seconds of embolic showers (p=0.493) between TCAR and CEA
– TF-CAS showed significantly higher emboli rates compared with CEA or TCAR (p<0.001)
Pre-Protection
• No significant difference b/w TCAR & CEA (p=0.177)
• TF-CAS generated more discrete emboli than TCAR & CEA (p<0.001)
Protection
• No significant difference b/w TCAR & CEA (p=0.424)
• TF-CAS generated more embolic events than TCAR & CEA (p<0.001)
Post-Protection
• All 3 techniques showed similar rates of embolic events
Pre-protectionBefore clamping, filter deployed, or reverse flow established
ProtectionUntil clamp removed, filter retrieved, or antegrade flow reestablished
Post-protection
After clamp/filter removed, or normal flow established

TransCarotid Artery Revascularization (TCAR) vs. Transfemoral Carotid Artery Stenting (TF-CAS) in the SVS Vascular Quality Initiative – J Vasc Surg Vol69, Issue 1, Pages 92–103.e2Malas MB, MD, MHS; Dakour Aridi H, MD, Wang GJ, MD; Kashyap VS, MD; Motaganahalli R, MD; Eldrup-Jorgensen J, MD; Cronenwett JL, MD; Schermerhorn ML, MD
In-Hospital Outcomes TCAR N=638
TF-CASN=10,136 P-value
Stroke 1.4% 2.0% 0.29
Stroke/TIA 1.9% 3.3% 0.04
Stroke/TIA/Death 2.2% 3.8% 0.04
Myocardial Infarction 1.1% 0.6% 0.15
TIA Alone 0.5% 1.3% 0.06
Any Neurological Event 1.9% 3.2% 0.06
Neurological Events/Death 2.2% 3.7% 0.05
Discharge Destination
Home 93.9% 90.8% 0.01
Rehab Unit 3.0% 6.0%
30-Day Mortality 0.9% 1.3% 0.42
Baseline Characteristics TCARN=638
TF-CASN=10,136 P-value
Age, Median (IQR) 74 (66-80) 70 (63-77 <.001
Female 35.1% 35.5 0.83
Coronary Artery Disease 47.3% 34% <.001
CHF 19.8% 15.3% <.01
Prior CABG/PCI 41.5% 19.5% <0.001
Hypertension 91.2% 90.0% 0.31
COPD 26.5% 25.7% .64
Symptomatic 33.5% 41.9% <.001
Prior Ipsilateral CEA or CAS 18.7% 26.9% <.001
Prior Contralateral CEA or CAS 18.3% 13.2% <.001
Anatomic High Risk 50.6% 46.2% 0.03
Medical High Risk 59.4% 41.4% <.001
Local Anesthesia 21% 88.5% <.001

• The rates of in-hospital TIA/Stroke as well as TIA/Stroke/Death were significantly higher with TF-CAS compared to TCAR• TIA/Stroke - 3.3% TF-CAS vs 1.9% TCAR (P=0.04)• TIA/Stroke/Death – 3.8% TF-CAS vs 2.2% TCAR (P=0.04)
• On multi-variable analysis, TF-CAS was associated with TWICE the odds of in-hospital neurologic events and TIA/Stroke/Death compared to TCAR
• “Our results show that patients undergoing TCAR had significantly higher medical comorbidities, but half the risk of in-hospital TIA/Stroke/Death compared to patients undergoing TF-CAS.…this is the first study to confirm the benefit of TCAR compared to TF-CAS in real-world practice.” – Dr. Mahmoud Malas
TransCarotid Artery Revascularization (TCAR) vs. Transfemoral Carotid Artery Stenting (TF-CAS) in the SVS Vascular Quality Initiative – J Vasc Surg Vol69, Issue 1, Pages 92–103.e2Malas MB, MD, MHS; Dakour Aridi H, MD, Wang GJ, MD; Kashyap VS, MD; Motaganahalli R, MD; Eldrup-Jorgensen J, MD; Cronenwett JL, MD; Schermerhorn ML, MD

TransCarotid Artery Revascularization (TCAR) vs. Transfemoral Carotid Artery Stenting (TF-CAS) in the SVS Vascular Quality Initiative – J Vasc Surg Vol69, Issue 1, Pages 92–103.e2Malas MB, MD, MHS; Dakour Aridi H, MD, Wang GJ, MD; Kashyap VS, MD; Motaganahalli R, MD; Eldrup-Jorgensen J, MD; Cronenwett JL, MD; Schermerhorn ML, MD

TCAR - Clinical Studies & Publications
PROOF ROADSTERTCD
CEA v TCAR vs TF-CAS
TCAR vs CEAVQI
TCAR vs TF-CASVQI ROADSTER 2
Study typeFirst In Man& DW-MRI Sub-Study
US Pivotal IDE + Continued
Access
Single Center Transcranial Doppler
TCAR Surveillance Project
TCAR Surveillance Project
US Post-Market Registry
Patients 75 219 34 2,545 638 600+
Profile All-comers HSRSym & Asx
CEA vs TCAR vs TF-CAS
HSRSym & Asx
HSRSym & Asx
HSRSym & Asx
TCAR Outcomes
• 0.0% Major S/D/MI
• 1.3% Minor contralateral stroke
• 17.9% New ipsilateral DWI lesions
• 1.3% All stroke (ITT)
• 0.7% All stroke (PP)
• 0.0% Major stroke
• 0.7% MI• 0.0% CNI at
6mths
• No significant differences in number of emboli and seconds of embolic showers btw TCAR and CEA
• 1.4% In-hospital stroke• 1.8% Stroke/death• AE’s statistically similar
between TCAR & CEA• TCAR shorter procedure &
10x lower CNI rate
• 1.4% In-hospital stroke
• 1.9% Stroke/TIA• 2.2%
Stroke/TIA/Death• 1.1% MI
Procedural Data &
Conclusions
• 53% Local anesthesia
• 76min OR time• 99% Tech
success
• TF-CAS showed significantly higher emboli rates compared with CEA or TCAR (p<0.001)
• TCAR patients significantly higher medical risk
• Statistically similar rates of stroke
• TCAR statistically shorter OR time & 10x lower rate of CNI
• TCAR had significantly higher medical comorbidities, but half the risk of in-hospital TIA/Stroke/Death compared TF-CAS patients
Status / Publication
J Endovasc Ther. 2017 Apr;24(2):265-
270
J Vasc Surg. 2015 Nov;62(5):1227-34
J Endovasc Ther April 2016 23: 249-254
Presented VEITH, 2018M. Schermerhorn, MD
J Vasc Surg. 2018 Vol69 Issue 1 , 92 - 103.e2
Currently Enrolling
PROOF - https://www.ncbi.nlm.nih.gov/pubmed/28335706TCAR vs TF-CAS - https://www.jvascsurg.org/pb/assets/raw/Health%20Advance/journals/ymva/Malas-22.pdf

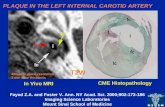
Case #1• 83 year old male with a history of HTN and
HLD presents to the ED with hoarseness
• Has known left internal carotid artery aneurysm that was stented at OSF in Georgia
• Arrives for evaluation because hoarseness is worsening

Case #1



Case #2• 60 year old male with a history of HTN, stroke, HLD and
NSTEMI with vFib arrest within the last 6 months
• Has 2 TIA with right arm weakness and numbness as well as slurred speech within last year
• Was lost to follow up due to NSTEMI, was being worked up for carotid revascularization
• Has a high grade left ICA lesion



Concluding Thoughts• Outcomes in all are evolving and positive
– Especially for carotid artery stenting
• The best evidence supports calculated and selective use of carotid stents by experts so patients have better outcomes
• The take away from CREST should be that non-inferiority does not indicate a competitive role between CEA and CAS…
…But instead these modalities should have complementary role in carotid artery revascularization

Thank You