
C2005 Evidence Evaluation Template - Nov.11,...
117
document.doc Page 1 of 117 Worksheet Author: Brian Steinhart Taskforce/Subcommittee: __BLS __ACLS __PEDS __ID __PROAD X ACS/AMI: Author’s Home Resuscitation Council: __AHA __ANZCOR __CLAR __ERC __HSFC _X_HSFC __RCSA ___IAHF ___Other: Date Submitted to Subcommittee: Aug 15, 2004, Revised 10 Jan 2005 STEP 1: STATE THE PROPOSAL. State if this is a proposed new guideline; revision to current guideline; or deletion of current guideline. Existing guideline, practice or training activity, or new guideline: Existing AHA Guidelines ACC/AHA Guidelines for the Management of Patients With Unstable Angina and Non-ST Segment Elevation Myocardial Infarction (2000): Executive Summary and Recommendations: “Biomarkers of cardiac injury should be measured in all patients who present with chest discomfort consistent with ACS. A cardiac-specific troponin is the preferred marker, and if available, it should be measured in all patients. CK-MB by mass assay is also acceptable. In patients with negative cardiac markers within 6 hours of the onset of pain, another sample should be drawn in the 6-12 hour time frame (eg, at 9 hours after the onset of symptoms).”ClassI, LOE C “For patients who present within 6 hours of the onset of symptoms, an early marker of cardiac injury (eg, myoglobin or CK-MB subforms) should be considered in addition to a cardiac troponin.” Class IIa. LOE C “Total CK (without MB), aspartate aminotransferase (AST,SGOT), b-hydroxybutyrate dehydrogenase, and/or lactate dehydrogenase should be the marker for the detection of myocardial injury in patients with chest discomfort suggestive of ACS.” Class III, LOE C Step 1A: Refine the question; state the question as a positive (or negative) hypothesis. State proposed guideline recommendation as a specific, positive hypothesis. Use single sentence if possible. Include type of patients; setting (in- /out-of-hospital); specific interventions (dose, route); specific outcomes (ROSC vs. hospital discharge). In unselected patients in the pre-hospital and early ED(4-6 hrs) phase,biomarker testing(CK,CK MB, TroponinT/I, myoglobin) is sensitive and specific to diagnose suspected Acute Coronary Syndrome, and to identify patients who are at increased risk of poor outcomes. Step 1B: Gather the Evidence; define your search strategy. Describe search results; describe best sources for evidence. COCHRANE (Database: CDSR, ACP Journal Club, DARE, CCTR) Search Strategy: 1 protein marker:.ab,sh,ti,gn. (25) 2 Creatine Kinase:.ti,sd,ab. (707) 3 Brain Natriuretic Peptide.ti,ab,sd. (116) 4 MYOGLOBIN.mp. (114) 5 Adenosine Diphosphate.mp. [mp=ti, ot, ab, tx, kw, ct, sh, hw] (373) 6 ACTIN:.sd,ti,ab. (4539)
Transcript of C2005 Evidence Evaluation Template - Nov.11,...

document.doc Page 1 of 77
Worksheet Author: Brian Steinhart
Taskforce/Subcommittee: __BLS __ACLS __PEDS __ID __PROAD X ACS/AMI:
Author’s Home Resuscitation Council: __AHA __ANZCOR __CLAR __ERC __HSFC_X_HSFC __RCSA ___IAHF ___Other:
Date Submitted to Subcommittee: Aug 15, 2004, Revised 10 Jan 2005
STEP 1: STATE THE PROPOSAL. State if this is a proposed new guideline; revision to current guideline; or deletion of current guideline.Existing guideline, practice or training activity, or new guideline: Existing AHA Guidelines ACC/AHA Guidelines for the Management of Patients With Unstable Angina and Non-ST Segment Elevation Myocardial Infarction (2000): Executive Summary and Recommendations:
“Biomarkers of cardiac injury should be measured in all patients who present with chest discomfort consistent with ACS. A cardiac-specific troponin is the preferred marker, and if available, it should be measured in all patients. CK-MB by mass assay is also acceptable. In patients with negative cardiac markers within 6 hours of the onset of pain, another sample should be drawn in the 6-12 hour time frame (eg, at 9 hours after the onset of symptoms).”ClassI, LOE C
“For patients who present within 6 hours of the onset of symptoms, an early marker of cardiac injury (eg, myoglobin or CK-MB subforms) should be considered in addition to a cardiac troponin.” Class IIa. LOE C
“Total CK (without MB), aspartate aminotransferase (AST,SGOT), b-hydroxybutyrate dehydrogenase, and/or lactate dehydrogenase should be the marker for the detection of myocardial injury in patients with chest discomfort suggestive of ACS.” Class III, LOE C
Step 1A: Refine the question; state the question as a positive (or negative) hypothesis. State proposed guideline recommendation as a specific, positive hypothesis. Use single sentence if possible. Include type of patients; setting (in- /out-of-hospital); specific interventions (dose, route); specific outcomes (ROSC vs. hospital discharge).
In unselected patients in the pre-hospital and early ED(4-6 hrs) phase,biomarker testing(CK,CK MB, TroponinT/I, myoglobin) is sensitive and specific to diagnose suspected Acute Coronary Syndrome, and to identify patients who are at increased risk of poor outcomes.
Step 1B: Gather the Evidence; define your search strategy. Describe search results; describe best sources for evidence.COCHRANE (Database: CDSR, ACP Journal Club, DARE, CCTR)Search Strategy:1 protein marker:.ab,sh,ti,gn. (25)2 Creatine Kinase:.ti,sd,ab. (707)3 Brain Natriuretic Peptide.ti,ab,sd. (116)4 MYOGLOBIN.mp. (114)5 Adenosine Diphosphate.mp. [mp=ti, ot, ab, tx, kw, ct, sh, hw] (373)6 ACTIN:.sd,ti,ab. (4539)7 Atrial Natriuretic Factor:.ti,sd,sh,ab. (758)8 Aspartate Aminotransferase:.ab,ti,sh. (750)9 Calcitonin Gene Related Peptide:.ti,ab. (88)10 (LACTATE DEHYDROGENASE ISOENZYME: or CREATINE KINASE ISOENZYME: or ISOENZYME).mp. [mp=ti, ot, ab, tx, kw, ct, sh, hw] (308)11 (TROPONIN: or TROPONIN C or TROPONIN T).mp. or TROPONIN I.sd,gn,ti,ab. [mp=ti, ot, ab, tx, kw, ct, sh, hw] (303)12 Lactate Dehydrogenase:.ab,ti,sd. (242) 13 C Reactive Protein.ti,ab. (848)14 (Biologic: Marker: or biochemical marker: or cardiac marker: or clinical marker: or serum marker:).ab,hw,ti. (2535)15 (creatine phosphokinase or adp phosphocreatine phosphotransferase or atp creatine phosphotransferase).ab,ti. (158)16 (brain natriuretic peptide or nesiritide or b-type natriuretic peptide or bnp gene product or bnp-32 or brain natriuretic peptide-32 or natrecor or natriuretic factor-32 or natriuretic peptide type-b or type-b natriuretic peptide or ventricular natriuretic peptide, b-type).ab,hw,ti. (146)17 (myoglobin or hemeprotein: or muscle protein: or biosyn or physiol permitted).ab,ti. (224)18 (adenosine diphosphate or adp or magnesium adp or mgadp or adenosine 5pyrophosphate: or adenosine triphosphate or atp or adenosine triphosphate, calcium salt or adenosine triphosphate, chromium salt or adenosine triphosphate, magnesium salt or adenosine triphosphate, manganese salt or adenylpyrophosphate or caatp or cratp or manganese adenosine triphosphate or mgatp or mnatp or atp-

document.doc Page 2 of 77
mgcl2 or adenosine triphosphate, chromium ammonium salt or adenosine triphosphate, magnesium chloride or atriphos or chromium adenosine triphosphate or crh2o4 atp or magnesium adenosine triphosphate or striadyne).ab,ti,sd,gn. (988)19 (actin: or f-actin or g-actin: or isoactin: or n-actin: alpha-actin: or alpha-isoactin: or beta-actin: or gamma-actin).ab,sd,ti. (4539)20 (atrial natriuretic factor: or receptor: or anf: or anp: or atriopeptins or auriculin: or anf precursor: or anp: or anp prohormone: or anp- or atrial pronatriodilatin: or atriopeptigen: or atriopeptin: or atriopeptin prohormone: or cardiodilatin: or cardiodilatin precursor: or cardionatrin: or prepro-anp: or prepro-cdd-anf or prepro-cardiodilatin-atrial natriuretic factor: or pro-anf: or proanf: or proatrial natriuretic factor: or pronatriodilatin: or alpha anp: or alpha-anp dimmer: or alpha-atrial natriuretic peptide: or beta-anp: or beta-atrial natriuretic peptide: or gamma anp: or gamma-atrial natriuretic peptide:).ab,sh,sd,ti. (13056)21 (aspartate aminotransferases: or aspartate transaminase: or glutamic-oxaloacetic transaminase or sgot or aspartate apoaminotransferase: or glutamate-aspartate transaminase: or l-aspartate-2-oxoglutarate aminotransferase: or serum glutamic-oxaloacetic transaminase:).ab,ti. (275)22 (calcitonin gene-related peptide: or calcitonin gene-related peptide I or calcitonin gene-related peptide ii or alpha-cgrp: or beta-cgrp or isoenzyme: or lactate dehydrogenase:).ab,sd,ti. (584)23 (troponin: or troponin-c or troponin-i or troponin t1 or troponin t2 or troponin-t).mp. (303)24 or/1-23 (23272)25 (emergenc: agent: or emergenc: treatment or emergency health service: or emergency surger: or emgergency or emergency medicine: or emergency ward: or emergency depart: or emergency room: or ER or ED or ambulance: or emergency mobile unit: or mobile emergency unit: or medical emerg: or cris: or hospital emergency service: or emergency outpatient unit: or hospital emergency service: or emergency hospital service: or hospital service emergenc: or emergency care or emergicent: or prehospital emergency care or prehospital: or pre-hospital or emergency care: or critical care or CCU).mp. (5874)26 (Heart Attack, or MI or AMI or ACS or CHF or heart muscle necros: or enzyme-diagnosed MI or biomarker-diagnosed MI or isch?: or adverse cardiac event: or acute chest pain or myocardial reperfus:).ti,ab,sh,sd. (11135)27 (Cardiac Infarct: or Coronary Artery Acute Occlusion: or Coronary Artery Occlusion: or Coronary Occlusion: or Heart Attack: or Heart Infarct: or Heart Micro Infarction: or Heart Muscle Infarction: Infarction, Heart or Myocardial Infarct: or Myocardium Infarct: or Premonitory Infarction Sign: or Second Heart Attack or Subendocardial Infarction: or Transmural Cardiac Infarct: or Transmural Heart Infarct: or Transmural Infarction,Heart or Myocardial Reperfus:).ti,ab,sh,sd. (8952)28 or/26-27 (16474)29 (heart muscle ischemia or heart muscle ischaemia or Acute Heart Muscle Ischemia or Acute Heart Muscle Ischaemia or acute heart disease: or Cardiac Ischemia or Cardiac Muscle Ischemia or Coronary Artery Ischemia or Coronary Ischemia or Coronary Syndrome or Heart Anoxia or Heart Hypoxia or Heart Ischaemia or Heart Ischemia or Heart Ischemic Arrest or Heart Ischemic Attack or Heart Ischemic Time: or Heart Muscle Hypoxia: or Heart Muscle Ischaemia or Heart Muscle Ischemia,Subepicardial or Heart Transient Ischemic Attack: or Hypoxia,Heart or Hypoxic Heart or Ischemic Heart or Ischemic Heart Arrest:).ti,ab,sh,sd. (856)30 (Ischemic Myocardium or Ischemic Time or Myocardial Anoxia or Myocardial or Hypoxia or Myocardial Ischaemia or Myocardial Ischemia or Myocardium or Hypoxia or Myocardium Ischemia or Subendocardial Ischemia or Transient Ischemic Attack,Heart).ab,ti,sd,sh. (12336)31 or/29-30 (12749)32 (sensitvity or specific: or diagnos:).ti,ab,tw,sh,sd. (40136)33 (((diagnos: measurement: or diagnosis measurement) and analys:) or differential diagnos: or diagnos: accurac: or diagnos: error: or diagnos: value: or Receiver Operating Characteristic: or Area Under the Curve: or ROC).sd,ti,ab. (3020)34 (clinical adj1 (impact or assessment: or evaluation:)).ti,ab. (4939)35 (meta-anal: or metaanal: or systematic review:).ti,ab,gn,sd. (2282)36 (random: or random allocation: or random: controlled trial: or controlled clinical trial:).ab,sd,ti. (228986)37 (singl: or doubl: or tripl:).ab,ti. (110829)38 (double blind method: or single blind method: or double-blind method: or single-blind method:).ab,ti. (512)39 (differential diagnos: or diagnos: error: or false negative reaction: or false positive reaction: or observer: variation:).ti,ab. (226)40 (predictive value: or false positive: or false negative: or false rate: or likelihood ratio: or post-test likelihood: or posttest likelihood: or post test likelihood: or post test probabilit: or posttest probabilit: or post-test probability: or ROC: or diagnostic standard: or accurac: or mass screen: or likelihood function:).ti,ab,sd. (5365)41 or/32-40 (289439)42 24 and 25 and 28 and 31 and 41 (49)43 limit 42 to yr=1998 - 2004 [Limit not valid in: DARE; records were retained] (30)44 from 43 keep 1-30 (30)
EMBASE, 1980 to 2004 Week 25-Search Strategy:
1 exp Biological Marker/ (10541)2 exp Creatine Kinase/ (11272)

document.doc Page 3 of 77
3 exp Brain Natriuretic Peptide/ (2445)4 exp MYOGLOBIN/ (4862)5 exp Adenosine Diphosphate/ (13272)6 exp ACTIN/ (23410)7 exp Atrial Natriuretic Factor/ (11772)8 exp Aspartate Aminotransferase/ (10522)9 exp Calcitonin Gene Related Peptide/ (6342)10 exp LACTATE DEHYDROGENASE ISOENZYME/ or exp CREATINE KINASE ISOENZYME/ or exp ISOENZYME/ (16869)
11 exp TROPONIN/ (5543)12 exp TROPONIN C/ or exp TROPONIN T/ or TROPONIN/ or exp TROPONIN I/ (5543)13 exp Lactate Dehydrogenase/ (14942)14 exp C Reactive Protein/ (11348)15 protein marker:.ab,sh,fs,ti. (979)16 (Biological Marker: or biochemical marker: or cardiac marker: or clinical marker: or serum marker: or biologic: marker:).ab,hw,ti. (24595)
17 (creatine phosphokinase or adp phosphocreatine phosphotransferase or atp creatine phosphotransferase).ab,sh,ti. (1937)
18 (brain natriuretic peptide or nesiritide or b-type natriuretic peptide or bnp gene product or bnp-32 or brain natriuretic peptide-32 or natrecor or natriuretic factor-32 or natriuretic peptide type-b or type-b natriuretic peptide or ventricular natriuretic peptide, b-type).ab,hw,sh,ti. (2766)
19 (myoglobin or hemeprotein: or muscle protein: or biosyn or physiol permitted).ab,sh,ti. (10047)
20 (adenosine diphosphate or adp or magnesium adp or mgadp or adenosine 5pyrophosphate: or adenosine triphosphate or atp or adenosine triphosphate, calcium salt or adenosine triphosphate, chromium salt or adenosine triphosphate, magnesium salt or adenosine triphosphate, manganese salt or adenylpyrophosphate or caatp or cratp or manganese adenosine triphosphate or mgatp or mnatp or atp-mgcl2 or adenosine triphosphate, chromium ammonium salt or adenosine triphosphate, magnesium chloride or atriphos or chromium adenosine triphosphate or crh2o4 atp or magnesium adenosine triphosphate or striadyne).ab,hw,sh,ti. (104312)
21 (actin: or f-actin or g-actin: or isoactin: or n-actin: alpha-actin: or alpha-isoactin: or beta-actin: or gamma-actin).ab,hw,sh,ti. (117317)
22 (atrial natriuretic factor: or receptor: or anf: or anp: or atriopeptins or auriculin: or anf precursor: or anp: or anp prohormone: or anp- or atrial pronatriodilatin: or atriopeptigen: or atriopeptin: or atriopeptin prohormone: or cardiodilatin: or cardiodilatin precursor: or cardionatrin: or prepro-anp: or prepro-cdd-anf or prepro-cardiodilatin-atrial natriuretic factor: or pro-anf: or proanf: or proatrial natriuretic factor: or pronatriodilatin: or alpha anp: or alpha-anp dimmer: or alpha-atrial natriuretic peptide: or beta-anp: or beta-atrial natriuretic peptide: or gamma anp: or gamma-atrial natriuretic peptide:).ab,sh,sd,ti. (528132)
23 (aspartate aminotransferases: or aspartate transaminase: or glutamic-oxaloacetic transaminase or sgot or aspartate apoaminotransferase: or glutamate-aspartate transaminase: or l-aspartate-2-oxoglutarate aminotransferase: or serum glutamic-oxaloacetic transaminase:).ab,sh,sd,ti. (2529)
24 (calcitonin gene-related peptide: or calcitonin gene-related peptide I or calcitonin gene-related peptide ii or alpha-cgrp: or beta-cgrp or isoenzyme: or lactate dehydrogenase:).ab,sh,sd,ti. (49498)
25 (troponin: or troponin-c or troponin-i or troponin t1 or troponin t2 or troponin-t).mp. (6306)
26 or/1-25 (811095)
27 exp AGENTS USED IN EMERGENCY MEDICINE/ or exp EMERGENCY TREATMENT/ or exp EMERGENCY HEALTH SERVICE/ or exp EMERGENCY SURGERY/ or exp EMERGENCY/ or exp EMERGENCY MEDICINE/ or exp EMERGENCY WARD/ (214640)
28 (ambulance: or emergency mobile unit: or mobile emergency unit: or medical emerg: or cris: or hospital emergency service: or emergency outpatient unit: or hospital emergency service: or emergency hospital service: or hospital service emergenc: or emergency care or emergicent: or prehospital emergency care or prehospital: or pre-hospital or emergency care: or critical care or CCU or ED or ER).mp. (61540)

document.doc Page 4 of 77
29 or/27-28 (266173)
30 exp Heart Infarction/ (75855)
31 (Heart Attack, or MI or AMI or ACS or CHF or heart muscle necros: or enzyme-diagnosed MI or biomarker-diagnosed MI or isch?: or adverse cardiac event: or acute chest pain or myocardial reperfus:).ti,ab,sh. (181755)
32 (Cardiac Infarct: or Coronary Artery Acute Occlusion: or Coronary Artery Occlusion: or Coronary Occlusion: or Heart Attack: or Heart Infarct: or Heart Micro Infarction: or Heart Muscle Infarction: Infarction, Heart or Myocardial Infarct: or Myocardium Infarct: or Premonitory Infarction Sign: or Second Heart Attack or Subendocardial Infarction: or Transmural Cardiac Infarct: or Transmural Heart Infarct: or Transmural Infarction,Heart or Myocardial Reperfus:).ti,ab,sh. (88200)
33 or/30-32 (237934)34 exp Heart Muscle Ischemia/ (30858)35 (Acute Heart Muscle Ischemia or acute heart disease: or Cardiac Ischemia or Cardiac Muscle Ischemia or Coronary Artery Ischemia or Coronary Ischemia or Coronary Syndrome or Heart Anoxia or Heart Hypoxia or Heart Ischaemia or Heart Ischemia or Heart Ischemic Arrest or Heart Ischemic Attack or Heart Ischemic Time: or Heart Muscle Hypoxia: or Heart Muscle Ischaemia or Heart Muscle Ischemia,Subepicardial or Heart Transient Ischemic Attack: or Hypoxia,Heart or Hypoxic Heart or Ischemic Heart or Ischemic Heart Arrest:).ab,ti,sh. (10871)
36 (Ischemic Myocardium or Ischemic Time or Myocardial Anoxia or Myocardial or Hypoxia or Myocardial Ischaemia or Myocardial Ischemia or Myocardium or Hypoxia or Myocardium Ischemia or Subendocardial Ischemia or Transient Ischemic Attack,Heart).ab,ti. (158380)37 or/34-36 (174173)38 exp "SENSITIVITY AND SPECIFICITY"/ (13772)39 exp "DIAGNOSIS, MEASUREMENT AND ANALYSIS"/ or exp DIAGNOSIS/ or exp DIFFERENTIAL DIAGNOSIS/ (3650888)40 (sensitvity or specific: or diagnos:).mp. (1877236)41 exp Diagnostic Accuracy/ (76051)42 exp Diagnostic Error/ (10905)43 exp Diagnostic Value/ (62964)44 exp Receiver Operating Characteristic/ (2934)45 exp Area Under the Curve/ (17175)46 (clinical adj1 (impact or assessment: or evaluation:)).ti,ab. (30450)47 (meta-anal: or metaanal: or systematic review:).ti,ab,tw. (13876)48 (random: or random allocation: or random: controlled trial: or controlled clinical trial:).ab,ti. (254901)
49 (singl: or doubl: or tripl:).ab,ti. (626304)
50 (double blind method: or single blind method: or double-blind method: or single-blind method:).ab,sh,ti. (225)
51 (differential diagnos: or diagnos: error: or false negative reaction: or false positive reaction: or observer: variation:).ti,sh,ab. (86644)
52 (predictive value: or false positive: or false negative: or false rate: or likelihood ratio: or post-test likelihood: or posttest likelihood: or post test likelihood: or post test probabilit: or posttest probabilit: or post-test probability: or ROC: or diagnostic standard: or accurac: or mass screen: or likelihood function:).ti,ab,sh. (163359)
53 or/38-52 (4656571)54 26 and 29 and 33 and 37 and 53 (756)55 limit 54 to (human and yr=1998 - 2004) (393)
Ovid MEDLINE(R) <1966 to June Week 2 2004>
1 Biological Markers/ (47330)2 exp Creatine Kinase/ (18033)3 exp Natriuretic Peptide, Brain/ (1975)4 exp MYOGLOBIN/ (6705)5 exp Adenosine Diphosphate/ (20884)

document.doc Page 5 of 77
6 exp Adenosine Triphosphate/ (71201)7 exp Actins/ (28224)8 exp Atrial Natriuretic Factor/ (12259)9 exp Aspartate Aminotransferases/ (18183)10 exp Calcitonin Gene-Related Peptide/ (5705)11 exp Isoenzymes/ (61994)12 exp Troponin/ (5222)13 exp TROPONIN T/ (1780)14 TROPONIN/ or TROPONIN I/ (4301)15 exp Troponin C/ (971)16 exp L-Lactate Dehydrogenase/ (28853)17 exp C-Reactive Protein/ (8719)18 (((enzyme marker: or enzyme diagnos: or biomarker diagnos: card: iso: enzyme: or ck-mb mass measure: or ck-mb isoform: or sgot or mb isoform:) and binding protein) or myosin: or ctni or ctnt or creatin: or ck-mb: or ck isoen: or isozym: or troponin: or serum troponin: or myosin atpase or atpase or myoglob: or myosin: or STEMI or NSTEMI).mp. (200317)19 or/1-18 (429838)20 exp AMBULANCES/ (4158)21 exp Critical Care/ (25219)22 exp Emergency Service, Hospital/ (22295)23 exp Emergency Medical Services/ (48966)24 (ccu or emergency care: or critical care or ed or prehospital: or pre-hospital: or emergency health servic: or emergicent:).mp. (47227)25 or/20-24 (96206)26 exp Myocardial Infarction/ (95503)27 (MI or myocardial infarct: or heart attack: or infarct: or heart muscle necros: or enzyme-diagnosed MI or biomarker-diagnosed MI or isch?: or adverse cardiac event: or acute coronary syndrome or ACS or acute chest pain: or coronary heart disease:).mp. (303786)28 or/26-27 (306162)29 "Sensitivity and Specificity"/ (116195)30 exp "Predictive Value of Tests"/st [Standards] (1)31 exp ROC Curve/ (7024)32 exp diagnostic errors/ or false negative reactions/ or false positive reactions/ or observer variation/ (56987)33 exp likelihood functions/ (6185)34 exp Diagnosis, Differential/ (246139)35 exp "Reproducibility of Results"/ (93030)36 exp Area Under Curve/ (7906)37 exp PROBABILITY/ (446404)38 Diagnosis/ (6836)39 di.fs. (1175322)40 ra.fs. (400696)41 ri.fs. (78778)42 us.fs. (94299)43 (sensitivity: or specific: or diagnos:).mp. (2198117)44 (predictive value: or false positive: or false negative: or false rate: or likelihood ratio: or post-test likelihood: or posttest likelihood: or post test likelihood: or post test probabilit: or posttest probabilit: or post-test probability: or ROC: or diagnostic standard: or accurac:).mp. (203129)45 (random: controlled trial or controlled clinical trial:).mp. [mp=Title, original Title, Abstract, name of substance, mesh subject heading] (19398)46 random allocation/ (50890)47 (single blind:3 or double blind:3 or triple blind:3).mp. (73312)48 double blind method/ or single blind method/ (86030)49 or/29-48 (3621737)50 19 and 25 and 28 and 49 (407)51 limit 50 to (human and yr=1998 - 2004) (247)52 from 51 keep 1-247 (247)
Database: Ovid MEDLINE(R) In-Process, Other Non-Indexed Citations, Ovid MEDLINE(R) - Search Strategy:

document.doc Page 6 of 77
1 protein marker:.ab,kw,ti. (909)2 Creatine Kinase:.ti,kw,ab. (11905)3 Brain Natriuretic Peptide:.ti,ab. (1671)4 MYOGLOBIN.mp. (8742)5 Adenosine Diphosphate.ab,ti,ti. (3746)6 ACTIN.ab,ti. (44095)7 Atrial Natriuretic Factor:.ti,ab. (3889)8 Aspartate Aminotransferase:.ab,ti. (6177)9 Calcitonin Gene Related Peptide:.ti,ab. (6512)10 (LACTATE DEHYDROGENASE ISOENZYME: or CREATINE KINASE ISOENZYME: or ISOENZYME).mp. (11531)11 (TROPONIN: or TROPONIN C or TROPONIN T or TROPONIN I).mp. (7176)12 Lactate Dehydrogenase.ab,ti. (17292)13 C Reactive Protein.ti,ab. (10252)14 (Biological Marker: or biochemical marker: or cardiac marker: or clinical marker: or serum marker: or biologic: marker:).ab,tw,kw,ti. (12547)15 (creatine phosphokinase or adp phosphocreatine phosphotransferase or atp creatine phosphotransferase).ab,ti. (3225)16 (brain natriuretic peptide or nesiritide or b-type natriuretic peptide or bnp gene product or bnp-32 or brain natriuretic peptide-32 or natrecor or natriuretic factor-32 or natriuretic peptide type-b or type-b natriuretic peptide or ventricular natriuretic peptide, b-type).ab,hw,ti. (2035)17 (myoglobin or hemeprotein: or muscle protein: or biosyn or physiol permitted).ab,ti. (9746)18 (adenosine diphosphate or adp or magnesium adp or mgadp or adenosine 5pyrophosphate: or adenosine triphosphate or atp or adenosine triphosphate, calcium salt or adenosine triphosphate, chromium salt or adenosine triphosphate, magnesium salt or adenosine triphosphate, manganese salt or adenylpyrophosphate or caatp or cratp or manganese adenosine triphosphate or mgatp or mnatp or atp-mgcl2 or adenosine triphosphate, chromium ammonium salt or adenosine triphosphate, magnesium chloride or atriphos or chromium adenosine triphosphate or crh2o4 atp or magnesium adenosine triphosphate or striadyne).ab,ti,hw. (155374)19 (actin: or f-actin or g-actin: or isoactin: or n-actin: alpha-actin: or alpha-isoactin: or beta-actin: or gamma-actin).ab,ti. (138069)20 (atrial natriuretic factor: or receptor: or anf: or anp: or atriopeptins or auriculin: or anf precursor: or anp: or anp prohormone: or anp- or atrial pronatriodilatin: or atriopeptigen: or atriopeptin: or atriopeptin prohormone: or cardiodilatin: or cardiodilatin precursor: or cardionatrin: or prepro-anp: or prepro-cdd-anf or prepro-cardiodilatin-atrial natriuretic factor: or pro-anf: or proanf: or proatrial natriuretic factor: or pronatriodilatin: or alpha anp: or alpha-anp dimmer: or alpha-atrial natriuretic peptide: or beta-anp: or beta-atrial natriuretic peptide: or gamma anp: or gamma-atrial natriuretic peptide:).ab,sh,ti. (688274)21 (aspartate aminotransferases: or aspartate transaminase: or glutamic-oxaloacetic transaminase or sgot or aspartate apoaminotransferase: or glutamate-aspartate transaminase: or l-aspartate-2-oxoglutarate aminotransferase: or serum glutamic-oxaloacetic transaminase:).ab,ti. (3679)22 (calcitonin gene-related peptide: or calcitonin gene-related peptide I or calcitonin gene-related peptide ii or alpha-cgrp: or beta-cgrp or isoenzyme: or lactate dehydrogenase:).ab,ti. (40172)23 (troponin-c or troponin-i or troponin t1 or troponin t2 or troponin-t).ti,ab. (4937)24 or/1-23 (1018682)25 (emergenc: agent: or emergenc: treatment or emergency health service: or emergency surger: or emgergency or emergency medicine: or emergency ward: or emergency depart: or emergency room: or ER or ED or ambulance: or emergency mobile unit: or mobile emergency unit: or medical emerg: or cris: or hospital emergency service: or emergency outpatient unit: or hospital emergency service: or emergency hospital service: or hospital service emergenc: or emergency care or emergicent: or prehospital emergency care or prehospital: or pre-hospital or emergency care: or critical care or CCU).mp. (135090)26 (Heart Attack, or MI or AMI or ACS or CHF or heart muscle necros: or enzyme-diagnosed MI or biomarker-diagnosed MI or isch?: or adverse cardiac event: or acute chest pain or myocardial reperfus:).ti,ab,hw. (203618)27 (Cardiac Infarct: or Coronary Artery Acute Occlusion: or Coronary Artery Occlusion: or Coronary Occlusion: or Heart Attack: or Heart Infarct: or Heart Micro Infarction: or Heart Muscle Infarction: Infarction, Heart or Myocardial Infarct: or Myocardium Infarct: or Premonitory Infarction Sign: or Second Heart Attack or Subendocardial Infarction: or Transmural Cardiac Infarct: or Transmural Heart Infarct: or Transmural Infarction,Heart or Myocardial Reperfus:).ti,ab,hw. (127158)28 or/26-27 (287552)
29 (heart muscle ischemia or heart muscle ischaemia or Acute Heart Muscle Ischemia or Acute Heart Muscle Ischaemia or acute heart disease: or Cardiac Ischemia or Cardiac Muscle Ischemia or Coronary Artery Ischemia or Coronary Ischemia or Coronary Syndrome or Heart Anoxia or Heart Hypoxia or Heart Ischaemia or Heart Ischemia or Heart Ischemic Arrest or Heart Ischemic Attack or Heart Ischemic Time: or Heart Muscle Hypoxia: or Heart Muscle Ischaemia or Heart Muscle Ischemia,Subepicardial or Heart Transient Ischemic Attack: or Hypoxia,Heart or Hypoxic Heart or Ischemic Heart or Ischemic Heart Arrest:).ti,hw,ti. (8759)30 (Ischemic Myocardium or Ischemic Time or Myocardial Anoxia or Myocardial or Hypoxia or Myocardial Ischaemia or Myocardial Ischemia or Myocardium or Hypoxia or Myocardium Ischemia or Subendocardial Ischemia or Transient Ischemic Attack,Heart).ab,ti,hw,sh. (343464)31 or/29-30 (347214)

document.doc Page 7 of 77
32 (sensitvity or specific: or diagnos:).ti,ab,sh,hw. (2259458)33 (((diagnos: measurement: or diagnosis measurement) and analys:) or differential diagnos: or diagnos: accurac: or diagnos: error: or diagnos: value: or Receiver Operating Characteristic: or Area Under the Curve: or ROC).hw,ti,ab. (113145)34 (clinical adj1 (impact or assessment: or evaluation:)).ti,ab. (37410)35 (meta-anal: or metaanal: or systematic review:).ti,ab,hw. (19258)36 (random: or random allocation: or random: controlled trial: or controlled clinical trial:).ab,hw,ti. (346867)37 (singl: or doubl: or tripl:).ab,ti. (765470)38 (double blind method: or single blind method: or double-blind method: or single-blind method:).ab,ti. (375)39 (differential diagnos: or diagnos: error: or false negative reaction: or false positive reaction: or observer: variation: oe or receiver operat: curve:).ti,ab. (56258)40 (predictive value: or false positive: or false negative: or false rate: or likelihood ratio: or post-test likelihood: or posttest likelihood: or post test likelihood: or post test probabilit: or posttest probabilit: or post-test probability: or ROC: or diagnostic standard: or accurac: or mass screen: or likelihood function:).ti,ab. (159657)41 or/32-40 (3152620)42 24 and 25 and 28 and 31 and 41 (409)43 limit 42 to human [Limit not valid in: Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations; records were retained] (401)44 limit 43 to yr=1998 - 2004 (266)List electronic databases searched (at least AHA EndNote 7 Master library [http://ecc.heart.org/], Cochrane database for systematic
reviews and Central Register of Controlled Trials [http://www.cochrane.org/], MEDLINE [http://www.ncbi.nlm.nih.gov/PubMed/ ], and
Embase), and hand searches of journals, review articles, and books.
Aha Master Library, Embase, Ovid Medline, Cochrane (CDSR, ACP Journal Club, DARE, CCTR), and Pubmed
• State major criteria you used to limit your search; state inclusion or exclusion criteria (e.g., only human studies with control group? no animal studies? N subjects > minimal number? type of methodology? peer-reviewed manuscripts only? no abstract-only studies?)
Diagnosis Filter (Diagnosis); Inclusion criteria: human, abstract available, sensitivity analysis; Exclusion:earlier than 1998. The previous guidelines 2000 included a systematic review of all literature up until approximately 1999. Thus the taskforce agreed to restrict the literature search to 1998 allowing one year of overlap to persist. In addition systematic reviews including literature from before 1998 were included in this search strategy to enhance the aggregate scientific basis for the consensus statement. This electronic search was augmented by a hand search of all bibliographies to identify any key articles missed through the search including those published prior to 1998.
• Number of articles/sources meeting criteria for further review: Create a citation marker for each study (use the author initials and date or Arabic numeral, e.g., “Cummins-1”). . If possible, please supply file of best references; EndNote 6+ required as reference manager using the ECC reference library. Total number of articles reviewed, 141
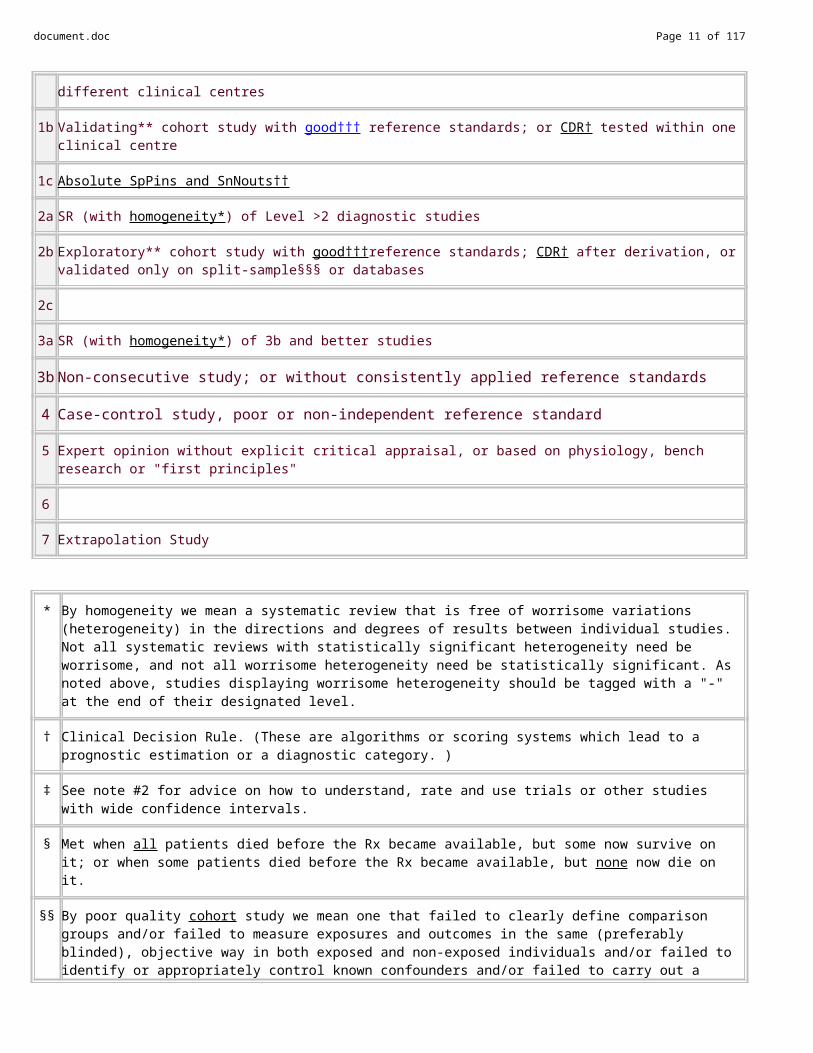
Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001) (http://www.cebm.net/notes)1a SR (with homogeneity*) of Level 1 diagnostic studies; CDR† with 1b studies from different clinical centres
1b Validating** cohort study with good††† reference standards; or CDR† tested within one clinical centre
1c Absolute SpPins and SnNouts††
2a SR (with homogeneity*) of Level >2 diagnostic studies
2b Exploratory** cohort study with good†††reference standards; CDR† after derivation, or validated only on split-sample§§§ or databases
2c
3a SR (with homogeneity*) of 3b and better studies
3b Non-consecutive study; or without consistently applied reference standards

document.doc Page 8 of 77
4 Case-control study, poor or non-independent reference standard
5 Expert opinion without explicit critical appraisal, or based on physiology, bench research or "first principles"
6
7 Extrapolation Study
* By homogeneity we mean a systematic review that is free of worrisome variations (heterogeneity) in the directions and degrees of results between individual studies. Not all systematic reviews with statistically significant heterogeneity need be worrisome, and not all worrisome heterogeneity need be statistically significant. As noted above, studies displaying worrisome heterogeneity should be tagged with a "-" at the end of their designated level.
† Clinical Decision Rule. (These are algorithms or scoring systems which lead to a prognostic estimation or a diagnostic category. )
‡ See note #2 for advice on how to understand, rate and use trials or other studies with wide confidence intervals.
§ Met when all patients died before the Rx became available, but some now survive on it; or when some patients died before the Rx became available, but none now die on it.
§§ By poor quality cohort study we mean one that failed to clearly define comparison groups and/or failed to measure exposures and outcomes in the same (preferably blinded), objective way in both exposed and non-exposed individuals and/or failed to identify or appropriately control known confounders and/or failed to carry out a sufficiently long and complete follow-up of patients. By poor quality case-control study we mean one that failed to clearly define comparison groups and/or failed to measure exposures and outcomes in the same (preferably blinded), objective way in both cases and controls and/or failed to identify or appropriately control known confounders.
§§§ Split-sample validation is achieved by collecting all the information in a single tranche, then artificially dividing this into "derivation" and "validation" samples.
†† An "Absolute SpPin" is a diagnostic finding whose Specificity is so high that a Positive result rules-in the diagnosis. An "Absolute SnNout" is a diagnostic finding whose Sensitivity is so high that a Negative result rules-out the diagnosis.
‡‡ Good, better, bad and worse refer to the comparisons between treatments in terms of their clinical risks and benefits.
††† Good reference standards are independent of the test, and applied blindly or objectively to applied to all patients. Poor reference standards are haphazardly applied, but still independent of the test. Use of a non-independent reference standard (where the 'test' is included in the 'reference', or where the 'testing' affects the 'reference') implies a level 4 study.
††††Better-value treatments are clearly as good but cheaper, or better at the same or reduced cost. Worse-value treatments are as good and more expensive, or worse and the equally or more expensive.
** Validating studies test the quality of a specific diagnostic test, based on prior evidence. An exploratory study collects information and trawls the data (e.g. using a regression analysis) to find which factors are 'significant'.
*** By poor quality prognostic cohort study we mean one in which sampling was biased in favour of patients who already had the target outcome, or the measurement of outcomes was accomplished in <80% of study patients, or outcomes were determined in an unblinded, non-objective way, or there was no correction for confounding factors.
****Good follow-up in a differential diagnosis study is >80%, with adequate time for alternative diagnoses to emerge (eg 1-6 months acute, 1 - 5 years chronic)
Notes
document.doc Page 9 of 77
Users can add a minus-sign "-" to denote the level of that fails to provide a conclusive answer because of:
EITHER a single result with a wide Confidence Interval (such that, for example, an ARR in an RCT is not statistically significant but whose confidence intervals fail to exclude clinically important benefit or harm)
OR a Systematic Review with troublesome (and statistically significant) heterogeneity.
Such evidence is inconclusive, and therefore can only generate Grade D recommendations.
Step 2B: Critically assess each article/source in terms of research design and methods. Was the study well executed? Suggested criteria appear in the table below. Assess design and methods and provide an overall rating. Ratings apply within each Level; a Level 1 study can be excellent or poor as a clinical trial, just as a Level 6 study could be excellent or poor as an animal study. Where applicable, please use a superscripted code (shown below) to categorize the primary endpoint of each study. For more detailed explanations please see attached assessment form.
Component of Study and Rating A B C DDesign &
Methods
Highly appropriate sample or model, randomized, proper controls ANDOutstanding accuracy, precision, and data collection in its class
Highly appropriate sample or model, randomized, proper controlsOROutstanding accuracy, precision, and data collection in its class
Adequate, design, but possibly biased
ORAdequate under the circumstances
Small or clearly biased population or model
ORWeakly defensible in its class, limited data or measures
Step 2C: Determine the direction of the results and the statistics: supportive? neutral? opposed?
DIRECTION of study by results & statistics:
SUPPORT the proposal NEUTRAL OPPOSE the proposal
ResultsOutcome of proposed guideline superior, to a clinically important degree, to current approaches
Outcome of proposed guideline no different from current approach
Outcome of proposed guideline inferior to current approach
Step 2D: Cross-tabulate assessed studies by a) level, b) quality and c) direction (ie, supporting or neutral/ opposing); combine and summarize. Exclude the Poor and Unsatisfactory studies. Sort the Excellent, Good, and Fair quality studies by both Level and Quality of evidence, and Direction of support in the summary grids below. Use citation marker (e.g. author/ date/source). In the Neutral or Opposing grid use bold font for Opposing studies to distinguish them from merely neutral studies. Where applicable, please use a superscripted code (shown below) to categorize the primary endpoint of each study.
Supporting EvidenceIn unselected patients in the pre-hospital and early ED (4-6 hrs) phase, biomarker testing(CK,CK MB, TroponinT/I,myoglobin) is sensitive and specific to diagnose suspected Acute Coronary Syndrome, and to identify patients who are at increased risk of poor
outcomes

document.doc Page 10 of 77
Qua
lity
Excellent Ebell(00:2)b,c,d,h
Fesmire(02)c,d,e,f
Good Fromm(01)c
Goldmann(04) c,e
Porela(00)c,f
McCord(03)c,e,
,d,e
Maisel(00)c,d,e,h Polanczyk(99)c,h
Zimmerman(99)h
Heeschen(00)Morris(00)Alp(01)
De Winter(00) Fesmire(00:2)
Zarich(02)Zarich(04)
FairStork(00) c,e Herkner(01)d,e
Caragher(02)Herren(01)Ng(01:1)c,e
Boersma(00)Esses(01)Young(99)
1a 1b 1c 2a 2b 3a 3b 4CEBM Diagnostic Level of Evidence
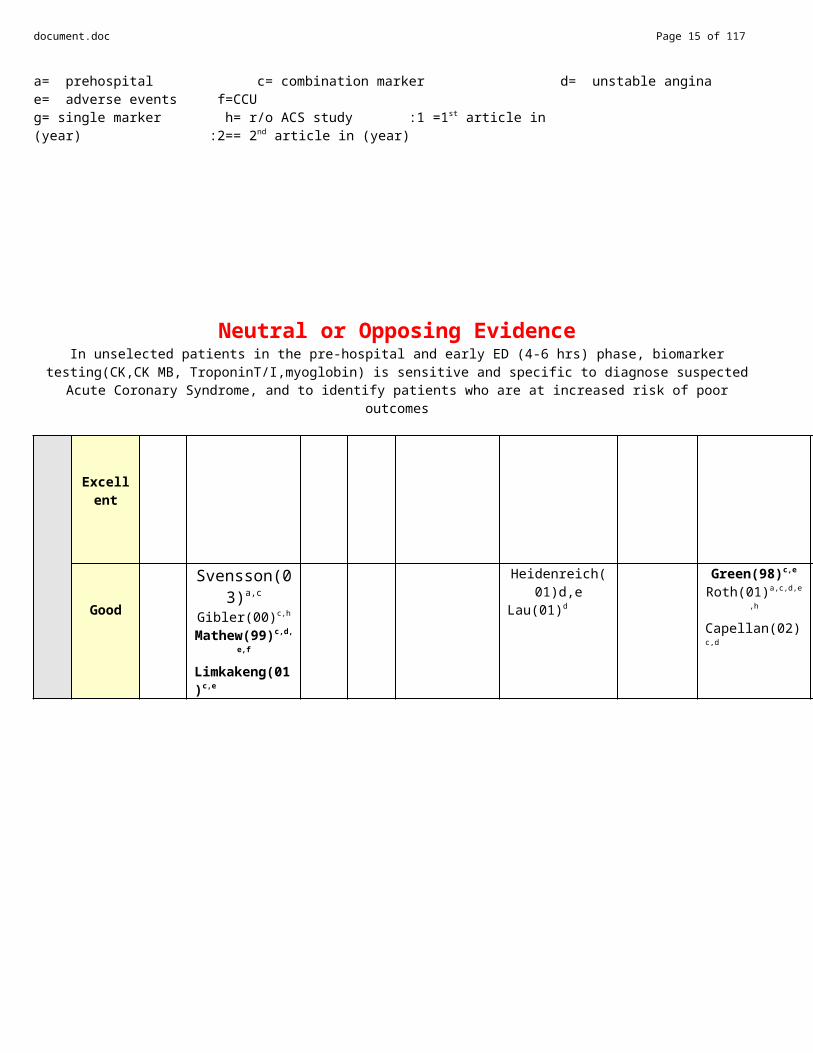
a= prehospital c= combination marker d= unstable angina e= adverse events f=CCU g= single marker h= r/o ACS study :1 =1st article in (year) :2== 2nd article in (year)
Neutral or Opposing EvidenceIn unselected patients in the pre-hospital and early ED (4-6 hrs) phase, biomarker testing(CK,CK MB, TroponinT/I,myoglobin) is sensitive and specific to diagnose suspected Acute Coronary Syndrome, and to identify patients who are at increased risk of poor
outcomes
Qua
lityo
f Evi
denc
e
Excellent
Good
Svensson(03)a,c
Gibler(00)c,h
Mathew(99)c,d,e,f
Limkakeng(01)c,e
Heidenreich(01)d,eLau(01)d
Green(98)c,e
Roth(01)a,c,d,e,h
Capellan(02)c,d
document.doc Page 11 of 77
Fair
Porela(00)c,d,e
Gust(98)a
Ooi(00)c,e
Morrow(98)e
Jurlander(00)c,e Sayre(98)c,e,
Domanovits(02)h,e
Huggon(01)c
Kratz(02)c,d
Newman(99)a,d,
Rebuzzi(98)c,d,e,
Svensson(04)a,c,e
Schuchert(99)a,c,
Liu,T(99)h
Ellestad(00)c,e
Green(00:1)c,e
Heeschen(00)c,e
Alp(01)c,e,f,h
Conti(02)d,e,h
1a 1b 1c 2a 2b 3a 3b 4Level of Evidence
a= prehospital c= combination marker d= unstable angina e= adverse events f=CCU g= single markerh= r/o ACS study :1=1st article in (year) :2= 2nd article in (year)
.
STEP 3: DETERMINE THE CLASS OF RECOMMENDATION. State a Class of Recommendation for the Guideline Proposal. State either a) the intervention, and then the conditions under which the intervention is either Class I, Class IIA, IIB, etc.; or b) the condition, and then whether the intervention is Class I, Class IIA, IIB, etc.Indicate if this is a __Condition or _X_InterventionIn unselected patients in the pre-hospital and early ED (4-6 hrs) phase, biomarker testing(CK,CK MB, TroponinT/I,myoglobin) is sensitive and specific to diagnose suspected Acute Coronary Syndrome, and to identify patients who are at increased risk of poor outcomesFinal Class of recommendation: __Class I-Definitely Recommended _X Class IIa-Acceptable & Useful; good evidence __Class IIb-Acceptable & Useful; fair evidence __Class III – Not Useful; may be harmful __Indeterminate-minimal evidence or inconsistent
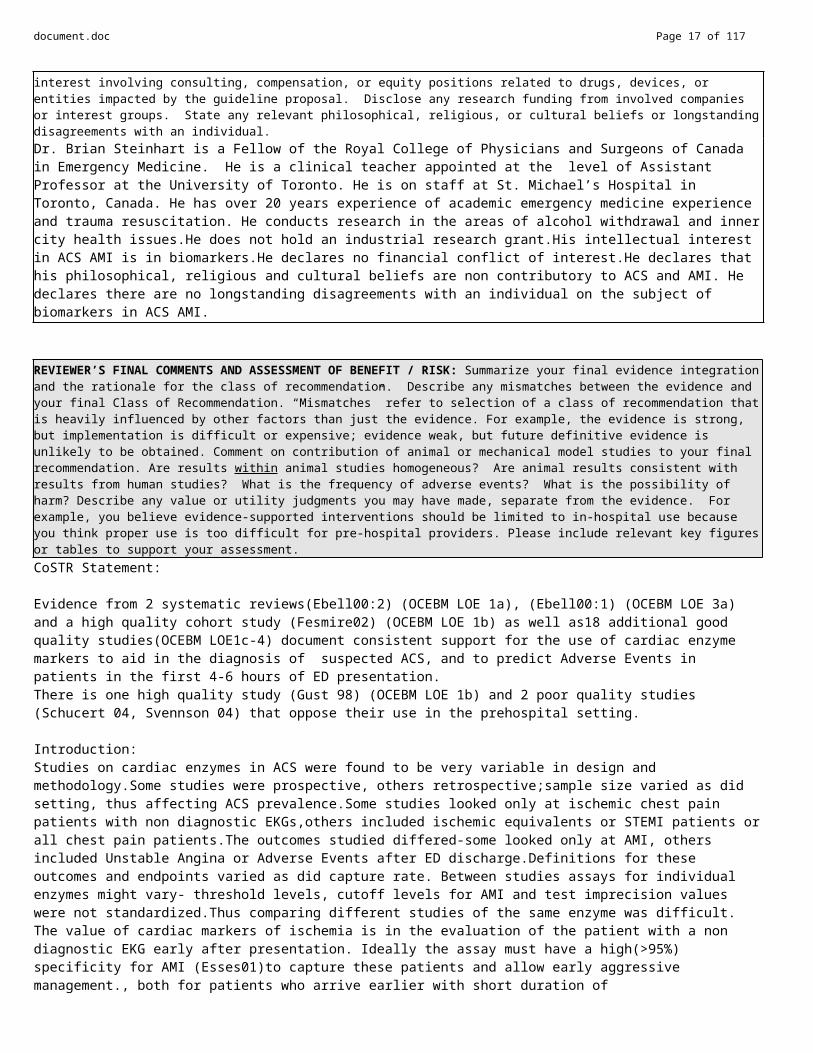
REVIEWER’S PERSPECTIVE AND POTENTIAL CONFLICTS OF INTEREST: Briefly summarize your professional background, clinical specialty, research training, AHA experience, or other relevant personal background that define your perspective on the guideline proposal. List any potential conflicts of interest involving consulting, compensation, or equity positions related to drugs, devices, or entities impacted by the guideline proposal. Disclose any research funding from involved companies or interest groups. State any relevant philosophical, religious, or cultural beliefs or longstanding disagreements with an individual.Dr. Brian Steinhart is a Fellow of the Royal College of Physicians and Surgeons of Canada in Emergency Medicine. He is a clinical teacher appointed at the level of Assistant Professor at the University of Toronto. He is on staff at St. Michael’s Hospital in Toronto, Canada. He has over 20 years experience of academic emergency medicine experience and trauma resuscitation. He conducts research in the areas of alcohol withdrawal and inner city health issues.He does not hold an industrial research grant.His intellectual interest in ACS AMI is in biomarkers.He declares no financial conflict of interest.He declares that his philosophical, religious and cultural beliefs are non contributory to ACS and AMI. He declares there are no longstanding disagreements with an individual on the subject of biomarkers in ACS AMI.
REVIEWER’S FINAL COMMENTS AND ASSESSMENT OF BENEFIT / RISK: Summarize your final evidence integration and the rationale for the class of recommendation. Describe any mismatches between the evidence and your final Class of Recommendation. “Mismatches” refer to selection of a class of recommendation that is heavily influenced by other factors than just the evidence. For example, the evidence is strong, but implementation is difficult or expensive; evidence weak, but future definitive evidence is unlikely to be obtained. Comment on contribution of animal or mechanical model studies to your final recommendation. Are results within animal studies homogeneous? Are animal results consistent with results from human studies? What is the frequency of adverse events? What is the possibility of harm? Describe any value or utility judgments you may have made, separate from the evidence. For example, you believe evidence-supported interventions should be limited to in-hospital use because you think proper use is too difficult for pre-hospital providers. Please include relevant key figures or tables to support your assessment.CoSTR Statement:

document.doc Page 12 of 77
Evidence from 2 systematic reviews(Ebell00:2) (OCEBM LOE 1a), (Ebell00:1) (OCEBM LOE 3a) and a high quality cohort study (Fesmire02) (OCEBM LOE 1b) as well as18 additional good quality studies(OCEBM LOE1c-4) document consistent support for the use of cardiac enzyme markers to aid in the diagnosis of suspected ACS, and to predict Adverse Events in patients in the first 4-6 hours of ED presentation. There is one high quality study (Gust 98) (OCEBM LOE 1b) and 2 poor quality studies (Schucert 04, Svennson 04) that oppose their use in the prehospital setting.
Introduction:Studies on cardiac enzymes in ACS were found to be very variable in design and methodology.Some studies were prospective, others retrospective;sample size varied as did setting, thus affecting ACS prevalence.Some studies looked only at ischemic chest pain patients with non diagnostic EKGs,others included ischemic equivalents or STEMI patients or all chest pain patients.The outcomes studied differed-some looked only at AMI, others included Unstable Angina or Adverse Events after ED discharge.Definitions for these outcomes and endpoints varied as did capture rate. Between studies assays for individual enzymes might vary- threshold levels, cutoff levels for AMI and test imprecision values were not standardized.Thus comparing different studies of the same enzyme was difficult.The value of cardiac markers of ischemia is in the evaluation of the patient with a non diagnostic EKG early after presentation. Ideally the assay must have a high(>95%) specificity for AMI (Esses01)to capture these patients and allow early aggressive management., both for patients who arrive earlier with short duration of symptoms(Ooi00,Lau01) and those with later arrivals and more prolonged symptoms (Jurlander00).As well the assay should have a high sensitivity (Alp01) to allow efficient discharge of the patient. To date there is no good evidence for any one marker with both these qualities, neither those assayed in the prehospital setting (Svensson03,Gust98) nor the first 6 hours in the ED(Ebell00:1).
Of no less importance is the ability to diagnose and rule out Unstable Angina in those patients suspicious for ischemia; studies with good reference standards are few and sensitivity/specificity results are too low to affect decision making.(Mathew99,Balk01,Lau01).No marker at ED presentation has specificity for predicting adverse events(Limkakeng01); all are predictive on later assays(Fromm01).
For an article to be supportive of my hypothesis the Sensitivity of the assay(s) studied for ACS must be in the magnitude of middle 90’s%; thereby capturing patients potentially missed by the clinician. Of the 60 articles included in this review, 30 were deemed supportive of the proposed guideline statement with CEBM LOE from Ia to 7. Of these, 3 studies(Ebell:1,Fesmire02 and Ebell00:2) stand out for their excellent quality.
Ebell(00:2) undertook a systematic review of troponin T and I values on patients with chest pain looking as a prognostic tool with end points being cardiac death and non fatal MI 30 days post emergency room visit. The author searched Medline and also several journals up through and including December 1999 for 1b articles. Their inclusion criteria included only prospective cohort studies adult populations with acute chest pain. Each study had to have had an 80% follow up looking at the outcome of stated. They excluded studies with only in hospital outcomes or where calculations for sensitivity or specificity were not available. They looked at 28 studies; they divided data into just chest pain syndrome or unstable angina (defined as chest pain with EKG changes) and then non Q wave MI group (defined as biochemical criteria for MI but no Q waves on EKG). For chest pain alone they quote Hamm study as being the best one from 1997 where they reported sensitivity of .94, specificity of .81, LR+ of 5.0 and LR- of 0.07. In patients with unstable angina they looked at 3 studies with only death as a follow up between 30 days and 9 months. In the best study they found a sensitivity of 0.52 and specificity of 0.73; the 3 tests studies in summation found a sensitivity of 0.59, specificity of 0.79, a positive LR of 2.8 and a LR- of 0.5. Looking at troponin T they analyzed 3 studies and found sensitivity of 0.63, specificity of 0.66, LR+ of 1.9 and LR- of 0.6. Looking at the third group of unstable angina or non Q wave MI patients with positive biochemical markers (WHO criteria) they a found a range of sensitivity of 0.59 to 1 and specificity of .6 to .74; for troponin T studies positive LR of 1.3 to 1.8 and a LR- of 0 to 0.3. In their conclusion they quote Hamm study that if a troponin T or I level is measured at least 6 hours after the onset of chest pain symptoms and is in the normal range, with a normal EKG, the likelihood of the patient suffering cardiac death or non fatal MI in the next 30 days would be 0.3%.
Fesmire (02) used a 2 panel assay on 2074 patients, at ED presentation and delta 2 hours, as part of an evaluation protocol to reliably identify and exclude ACS as well as predict 30 day AE. This protocol included stress testing all undifferentiated patients with normal delta values at 2 hours and is the only well designed study to incorporate this gold standard for Unstable Angina. Inclusion and exclusion criteria were standard; of note suspected ACS patients who did not have chest pain were excluded. Fesmire found 3.9 hours to be the average duration of pain prior to presentation and 8.6% to be the prevalence for AMI(WHO criteria or TnI >2 ng/mL); both figures are comparable to most EDs.The assay for CK-MB and TnI had acceptable within run precision coefficients of variation (4.5% and 6.1% respectively).The delta values were derived from a mathematical model based on their assay inprecision and had been previously validated.The 30 day Adverse Events were all-encompassing and well defined.The follow up rate was excellent with 94.5% direct and the remainder indirect, allowing 100% capture.Overall therefore the study was well structured. Fesmire’s results showed delta 2 hour values having a Sens 93.2/+LR of 15.2 and a Spec 93.9/–LR of 0.07 for AMI; likewise a Sens 66.1/+LR of 12.78 and Spec 94.9/-LR of 0.36 for 30 day ACS events.Though values are high and Confidence Intervals are narrow, one still cannot reliably exclude ACS as proven by stress testing- Sens 100% and Spec 81.9% for AMI; Sens 99.1% and Sens 87.4% for 30 day ACS.

document.doc Page 13 of 77
Ebell(00:1)undertook a systematic review of troponin T and I at diagnosing AMI. He was very strict in what studies were included. They had to have a prospective data collection, the physician determining whether an MI occurred had to be blinded to the troponin results, the WHO reference standard for diagnosing MI was used and authors had to report data for calculating sensitivities and specificities for at least 1 point from the onset of pain or presentation to the ED for troponin T or I. Included were nonconsecutive studies.This study looked at 124 articles. The authors found great heterogeniticy in the studies. His conclusion is a normal troponin T or I value from blood drawn 8 or more hours from the onset of chest pain is a strong evidence against the presence of AMI. A normal value of troponin T or I at the time of admission or within 4 or fewer hours of the onset of pain does not significantly reduce the likelihood of AMI.
Of the remaining 32 articles, all were either neutral or opposing to my hypothesis; none were deemed excellent in design.To illustrate the evidence against my hypothesis the study by Green(00:2) (OCEBM LOE 7) is representative- This study looked at myoglobin comparing it to other markers for adverse events over 14 days. The inclusion criteria accepted cocaine use and any EKG. 6% of patient population could yield false positive myoglobins by either having renal failure, significant trauma, or recent cocaine use. There were 2 sites involved thus diluting the high Afro American population to a generalized one. AMI was diagnosed by WHO criteria, recurrent unstable angina by clinical means. Myoglobin was assayed with STRATUS system CK-MB activity by Cardio REP, TnT by the ELISA. Once again the authors used ROC curve information to revise the manufacture’s AMI cutoff to optimize results for adverse events.New curves were derived for myoglobin. The myoglobin cutoff of > or = 110 nanograms per L was changed to 69 nanograms per milliliter; CK-MB went from > or = 10 international units to 12 international units per L, and TnT cutoff went to > or = 0.2 nanograms per milliliter to 0.14 nanograms per milliliter. Chest pain patients were analyzed according to symptom times –phlebotomy; < 6 hours or > or = to 6 hours. The AMI rate was 9.6%. With regards to the AMI end point myoglobin had a sensitivity of 28.9, specificity of 91.3; CK-MB 23.7, 98.3; TnT 23.7 and 94.7. There was no statistical significance between these low values. Interestingly, when compared to physician diagnostic ability (blinded to all the biochemical biomarker results) the physician sensitivity was 97.4 and specificity of 44.7. The one MI missed by the physician also had triple marker negative results.
In evaluating the evidence for the Creatinine Kinase class of enzymes, most studies had used WHO criteria employing the same enzyme for the reference standard(Bock99). Therefore incorporation bias makes any conclusions circumspect. Early presenters had better sensitivity/specificity with CK Isoform assays(Zimmermann99). Pentilla(02) showed that there was no difference in CKMB/Isoform assays when TnI levels were used as AMI reference. However CK Isoforms are better at predicting adverse events(Green 00A).
There is good evidence to support Troponin assays as being most specific for late presenters (Mathew99);spurious results, especially with older assays (Ng01:2), decrease its value. Ebell(00:1) found no evidence to support using a single Tn assay within 4 hrs of symptom onset for diagnosing AMI, and showed at least 8 hrs is required to rule it out. It was shown that any positive Troponin was useful in predicting adverse events after ED admission(Ebell00:2); however a normal value did not rule out its occurrence(Heidenreich01).
Myoglobin assay can be helpful in early AMI presentions (deWinter00, Zimmermann99)especially when patients are selected to exclude conditions affecting specificity(Stork00)Otherwise delta values from serial assays are sensitive and more specific(Maisel 00).
Combination marker studies proves their utility (Fesmire00,Young99, Fesmire 02); marker sensitivity was dependent on symptom duration prior to assay(Polarczyk99,Jurlander 00, Balk).Point of Care accuracy has evolved to match that of in- hospital systems with shorter turnaround times (Young99, Goldmann04), . These devices typically have a panel (combination) of enzyme assays for each sample. However it does consume ED personnel time
Preliminary draft/outline/bullet points of Guidelines revision: Include points you think are important for inclusion by the person assigned to write this section. Use extra pages if necessary.
Publication: Chapter: Pages:
Topic and subheading:
CoSTR Statement:Evidence from 2 systematic reviews(Ebell00:2) (OCEBM LOE 1a), (Ebell00:1) (OCEBM LOE 3a) and a high quality cohort study (Fesmire02) (OCEBM LOE 1b) as well as 22 additional quality studies(OCEBM LOE1c-4) document consistent support for the use of cardiac enzyme markers to aid in the diagnosis of suspected ACS, and to predict Adverse Events in patients in the first 4-6 hours of ED presentation. There is one high quality study (Gust 98) (OCEBM LOE 1b) and 2 poor quality studies (Schucert 04, Svennson 04) that oppose their use in the prehospital setting.

document.doc Page 14 of 77
Treatment RecommendationTherefore cardiac enzyme assays, especially serial and multi-marker assays, for ED patients with suspected ACS should be utilized.
Attachments: Bibliography in electronic form using the Endnote Master Library. It is recommended that the bibliography be provided in annotated format.
This will include the article abstract (if available) and any notes you would like to make providing specific comments on the quality, methodology and/or conclusions of the study.
document.doc Page 15 of 77
Citation List
Citation Marker Full Citation*Alp (01) Alp Nj, B. J. A. S. M. (2001). "A rapid troponin-I-based protocol for assessing acute chest pain.[see
comment]." QJM 94(12): 717-8.
In a prospective randomized open trial with 30-day follow-up, we compared a troponin-I-based protocol to 'standard management' for the
diagnosis and risk stratification of patients with acute non-ST-elevationchest pain. Patients with acute chest pain (n=400) were randomized tostandard diagnostic tests and management, or a protocol based on theadmission ECG and the troponin-I result 6 h after onset of chest pain. Lowrisk patients were discharged early from CCU; high-risk patients weretreated with medical therapy or referred for in-patient angiography asappropriate. We measured length of CCU stay, and followed all patients formajor adverse cardiac events (MACE) of death, non-fatal myocardialinfarction (MI), or urgent revascularization during the admission and for 30days post-discharge. The troponin protocol allowed earlier discharge in thelow-risk group (10 vs. 30 h, p<0.001) with no excess of adverse eventscompared to standard management (3% vs. 5%, p=0.32). It identified agroup of patients at moderate risk of cardiac events (15% MACE rateduring admission and 30-day follow-up), and a high-risk group (75% MACErate) more accurately than did standard management. The prognosticpower of troponin testing in combination with the admission ECG washigher than with either test used alone. The protocol improved theefficiency of low-risk patient management, and improved patient riskstratification. This study adds to the evidence favouring troponin evaluationas part of the management of acute coronary syndromes.
This was a prospective randomized trial. The setting was a CCU environment. The inclusion criteria were standard ones: age > 18, no ST segment elevation MI. The reference standard was a CK at 48 hours to rule in or out AMI. There were no criteria for unstable angina. Exercise testing was at the discretion of the physician in charge. They were not blinded to the troponin values. Patients were randomized into the “standard management” arm for a series of CK measurements. The troponin positive patients were treated aggressively with aspirin, beta blockers and heparin. Troponin negative patients with an ischemic EKG were treated the same way at the discretion of the physician. Troponin negative patients were sent out of the CCU to either a medical ward or home. Troponin assay was point of care (POC) by Spectral Cardiac STATus assay at 6 hrs.. The qualitative discriminating value was 0.1 ng per millimeter. There was no comment on coefficient of variation. Outcome measures were major adverse cardiac events (MACE) including cardiac death non-fatal MI and urgent revascularization procedures for thirty day follow up.
Results: 400 patients were entered, 200 in each arm. The authors found, for 30 day MACE, a Sensitivity of 76%, Specificity of 92%, LR+ of 9.7, an LR- 0.15, PPV of 74.5, NPV of 92.8 for troponin positive versus troponin negative in troponin arm patients; when combined with ischemic EKG it jumped to 91.9, 90.5, 9.7 ,0.09, 75.6, and 97.2 respectively. I will consider the latter in ranking.
Thus, their 30 day MACE rate is 3% (95% CI 0-8%) in the low risk troponin group.
CEBM Level of Evidence 4,
Quality of Evidence Good Excellent/Good/Fair (CEBM LOE for Diagnosis = 1b)
Neutral
Balk (01) Balk, E. M., J. P. Ioannidis, et al. (2001). "Accuracy of biomarkers to diagnose acute cardiac ischemia in the emergency department: a meta-analysis." Annals of Emergency Medicine 37(5): 478-94.

document.doc Page 16 of 77
STUDY OBJECTIVE: We sought to evaluate quantitatively the evidence onthe diagnostic performance of presentation and serial biochemical markersfor emergency department diagnosis of acute cardiac ischemia (ACI), including acute myocardial infarction (AMI) and unstable angina.METHODS: We conducted a systematic review and meta-analysis of theEnglish-language literature published between 1966 and December 1998.We examined the diagnostic performance of creatine kinase, creatinekinase-MB, myoglobin, and troponin I and T testing. Diagnosticperformance was assessed by using estimates of test sensitivity and specificity and was summarized by summary receiver-operating characteristic curves. RESULTS: Only 4 studies were found that evaluated all patients with ACI; 73 were found that focused only on a diagnosis of AMI. To diagnose ACI, presentation biomarker tests had sensitivities of 16% to 19% and specificities of 96% to 100%; serial biomarker tests had sensitivities of 31% to 45% and specificities of 95% to 98%. Considering only the diagnosis of AMI, presentation biomarker tests had summary sensitivities of 37% to 49% and summary specificities of 87% to 97%; serial biomarker tests had summary sensitivities of 79% to 93% and summary specificities of 85% to 96%. Variation of test sensitivity was best explained by test timing. Longer symptom duration or time between serial tests yielded higher sensitivity. CONCLUSION: The limited evidence available to evaluate the diagnostic accuracy of biomarkers for ACI suggests that biomarkers have very low sensitivity to diagnose ACI. Thus, biomarkers alone will greatly underdiagnose ACI and will be inadequate to make triage decisions. For AMI diagnosis alone, multiple testing of individual biomarkers over time substantially improves sensitivity, while retaining high specificity, at the expense of additional time. Further high-quality studies are needed on the clinical effect of using biomarkers for patients with ACI in the ED and on optimal timing of serial testing and in combination with other tests. [References: 60]
This was a metanalysis of systematic review of English literature on biomarkers between 1966 and 1998. Most studies were at that time with CK MB and/or myoglobin, only 18 studies included troponin. Most studies were focussing on AMI, not unstable angina or ACS. Studies were very heterogenous. There were great variations in sensitivity and specificity significantly related to variations in duration of symtoms at the time of sampling. Since most studies used WHO criteria I focused on non-CK studies.
Level of Evidence 7
Quality of Evidence Good
Neutral
Bock(99) Bock, J. L., G. X. Brogan, Jr., et al. (1999). "Evaluation of CK-MB isoform analysis for early diagnosis of myocardial infarction." J Emerg Med 17(1): 75-9.
Measurement of CK-MB and its isoforms by high-voltage electrophoresis has been proposed as a sensitive test for early detection of myocardial infarction (MI). We performed a prospective study of this test in 231 patients presenting to the Emergency Department with symptoms consistent with ischemic chest pain. Blood specimens were obtained at 0, 1, and 3 h following presentation, and plasma was immediately frozen and analyzed within 1 week by high-voltage electrophoresis for total CK-MB and isoforms. The test was considered positive whenever total CK-MB was elevated (>6 U/L) or the cardiac isoform MB2 was relatively increased (MB2 > 2 U/L and MB2/MB1 > 1.7). This test had a sensitivity of 68% overall and 55% for specimens collected within 3 h of symptom onset. It was positive within 3 h of presentation in 36/39 (92%) of patients with confirmed MI. Specificity was 92% overall and did not vary with time after symptoms. The CK-MB alone, at the cutoff of 6 U/L, had lower sensitivity overall (56%; p = 0.01) and within 3 h of onset (39%; p = 0.03), and higher specificity overall (98%; p < 0.001). Lowering the cutoff for CK-MB alone to match the sensitivity of the isoform test caused a greater loss of specificity. It is concluded that analysis of CK-MB by high-voltage electrophoresis is an effective method for rapid diagnosis of MI, with the isoform analysis
document.doc Page 17 of 77
enhancing early sensitivity.
Used ROC analysis to derive CKMB cutoff.Compared CK isoforms to CKMB gold standard.Overall isoform Sens for AMI was 68%
Level of Evidence 7
Quality of Evidence Fair
Opposing
Boersma (00)Boersma, E., K. S. Pieper, et al. (2000). "Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. The PURSUIT Investigators." Circulation 101(22): 2557-2567.
BACKGROUND: Appropriate treatment policies should include an accurate estimate of a patient's baseline risk. Risk modeling to date has been underutilized in patients with acute coronary syndromes without persistent ST-segment elevation. METHODS AND RESULTS: We analyzed the relation between baseline characteristics and the 30-day incidence of death and the composite of death or myocardial (re)infarction in 9461 patients with acute coronary syndromes without persistent ST-segment elevation enrolled in the PURSUIT trial [Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using Integrilin (eptifibatide) Therapy]. Variables examined included demographics, history, hemodynamic condition, and symptom duration. Risk models were created with multivariable logistic regression and validated by bootstrapping techniques. There was a 3.6% mortality rate and 11.4% infarction rate by 30 days. More than 20 significant predictors for mortality and for the composite end point were identified. The most important baseline determinants of death were age (adjusted chi(2)=95), heart rate (chi(2)=32), systolic blood pressure (chi(2)=20), ST-segment depression (chi(2)=20), signs of heart failure (chi(2)=18), and cardiac enzymes (chi(2)=15). Determinants of mortality were generally also predictive of death or myocardial (re)infarction. Differences were observed, however, in the relative prognostic importance of predictive variables for mortality alone or the composite end point; for example, sex was a more important determinant of the composite end point (chi(2)=21) than of death alone (chi(2)=10). The accuracy of the prediction of the composite end point was less than that of mortality (C-index 0.67 versus 0.81). CONCLUSIONS: The occurrence of adverse events after presentation with acute coronary syndromes is affected by multiple factors. These factors should be considered in the clinical decision-making process.
This sub study of the PURSUIT trial looked at 9461 patients with acute coronary syndrome that had EKG changes but not persistent ST segment elevation. These patients were followed at 30 days for incidence of death and myocardial reinfarction as diagnosed by a rise in CK MB, or persistent EKG changes. Their conclusion was that amongst other important baseline determinants the cardiac enzymes were significant if raised. They looked only at CK MB values that were drawn “on admission” on patients who had presented with at least 10 minutes of ischemic chest pain and within 24 hours of that episode. The timing of the sampling is not clear.
This article was included only because it is so often quoted.
Level of Evidence 4
Quality of Evidence Fair
Supportive
Capellan(03)Capellan, O., J. E. Hollander, et al. (2003). "Prospective evaluation of emergency department patients with potential coronary syndromes using initial absolute CK-MB vs. CK-MB relative index." Journal of Emergency Medicine 24(4): 361-7.

document.doc Page 18 of 77
We compared the predictive properties of an initial absolute creatinekinase-MB (CK-MB) to creatine kinase-MB relative index (CK-MB RI) fordetecting acute myocardial infarction (AMI), acute coronary syndromes(ACS), and serious cardiac events (SCE). Consecutive patients > 24 yearsof age with chest pain who received an electrocardiogram (EKG) as part oftheir Emergency Department (ED) evaluation had CK and CK-MB drawn atpresentation. Patients were followed prospectively during their hospitalcourse. The main outcome was AMI, ACS or SCE (death, AMI,dysrhythmias, CHF, PTCA/stent, CABG) within 30 days. The sensitivity,specificity, PPV and NPV of CK-MB and CK-MB RI to predict AMI, ACS,and SCE were calculated with 95% CIs. We enrolled 2028 patients. Therewere 105 patients (5.2%) with AMI, 266 (13.1%) with ACS, and 150 withSCE (7.4%). Absolute CK-MB had a higher sensitivity than CK-MB RI forAMI (52.0 vs. 46.9, respectively), ACS (23.5 vs. 20.8, respectively), andSCE (39.6 vs. 36.0, respectively), but a lower specificity than CK-MB RI forAMI (93.2 vs. 96.1, respectively), ACS (93.1 vs. 96.1, respectively) andSCE (93.3 vs. 96.3, respectively); and lower PPV for AMI (35.7 vs. 46.5,respectively), ACS (42.0 vs. 53.4, respectively) and SCE (38.5 vs. 50.5,respectively). The negative predictive values were similar for all outcomes.We conclude that the risk stratification of ED chest pain patients byabsolute CK-MB has higher sensitivity, similar NPV, but a lower specificityand PPV than CK-MB relative index for detection of AMI, ACS, and SCE.The optimal test depends upon the relative importance of the sensitivity orspecificity for clinical decision-making in an individual patient.This study at looked at comparing CK-MB to CK-MB relative index. It was a single centre prospective study. Outcome criteria included AMI by WHO standards (serious incorporation bias) and unstable angina by clinical criteria. Follow up was for a 30 day period and end points included death from cardiac etiology, AMI, serious dysrrhythmias, congestive heart failure, hypotension, respiratory failure, and cardiac interventions.
Only presentation enzymes were looked at. Median duration of pain prior to admission was 4 hours. Results: Primary outcome for comparing the predicted values of the different tests showed very little in the way of the difference (? significance).
Level of Evidence 4
Quality of Evidence Good
Neutral
Caragher (02)Caragher, T. E., B. B. Fernandez, et al. (2002). "Evaluation of quantitative cardiac biomarker point-of-care testing in the emergency department." Journal of Emergency Medicine 22(1): 1-7.
This study was undertaken to evaluate the diagnostic accuracy andpracticality of Emergency Department (ED) testing for cardiac biomarkersin the diagnosis of acute coronary syndromes. All patients presenting withchest pain to the ED of a community-based tertiary care facility over a 16day period (N = 205) had blood drawn and tested for cardiac troponin I,myoglobin, and CK-MB by a quantitative, point-of-care instrument system(Stratus CS). Point-of-care cardiac testing expedited diagnosis bydecreasing the turn-around time by 55% compared to the centrallaboratory. The extreme sensitivity of the cardiac troponin I assay integralto this system was responsible for the high diagnostic accuracy (100%sensitivity; virtually 100% specificity, compared with the final assigneddiagnosis). The assay also identified a clinically significant "high-risk" zonefor near-future cardiac events: 17 patients were identified and four of theseprogressed to further cardiac events in the next 9 months. Further studiesto explore the clinical implications of this high-risk zone are warranted.
This study compared point of care triple marker assay to in hospital assays. The reference

document.doc Page 19 of 77
standard was the assigned FAD(final assigned diagnosis) by review by the unblinded authors.
Level of Evidence 4
Quality of Evidence Fair
Supportive
Conti(02)Conti, A., B. Paladini, et al. (2002). "Effectiveness of a multidisciplinary chest pain unit for the assessment of coronary syndromes and risk stratification in the Florence area." American Heart Journal 144(4): 630-5.
BACKGROUND: In patients seen at the emergency department (ED) with chest pain (CP), noninvasive diagnostic strategies may differentiate patients at high or intermediate risk from those at low-risk for cardiovascular events and optimize the use of high-cost resources. However, in welfare healthcare systems, the feasibility, accuracy, and potential benefits of such management strategy need further investigation. METHODS: A total of 13,762 consecutive patients with CP were screened, and their conditions were defined as high, intermediate, and low risk for short-term cardiovascular events. Patients at high and intermediate risk were admitted. Patients at low risk were discharged from the ED if first line (<6 hours, including electrocardiogram, troponins, and serum cardiac markers) or second line short-term evaluation (<24 hours, including echocardiogram, rest or stress 99m-Tc myocardial scintigraphy, exercise tolerance test, or stress-echocardiography) had negative results. Patients with a diagnosis of coronary artery disease (CAD) were admitted. Patients without evidence of cardiovascular disease underwent screening for psychiatric and gastroesophageal disorders. Inhospital mortality rate was assessed in all patients. RESULTS: Among patients at high and intermediate risk (n = 9335), 2420 patients had acute myocardial infarction (26%, 10.6% mortality rate), 3764 had unstable angina (40%, 1.1% mortality rate), 129 had aortic dissection (1.4%, 23.3% mortality rate), and 408 had pulmonary embolism (4%, 27.6% mortality rate). The remaining 2614 had chronic coronary heart disease in the context of multiple pathology (n = 2256) or pleural or pericardial diseases (n = 358). Among patients at low risk (n = 4427), 2672 were discharged at <6 hours (60%, 0.2% incidence rate of nonfatal CAD at 6 months) and 870 patients were discharged at <24 hours (20%, no CAD at follow-up). The remaining 885 patients were recognized as having CAD (20%, 1.1% inhospital mortality rate). Finally, half of the patients without CAD had active gastroesophageal or anxiety disorders. CONCLUSION: An effective screening program with an observation area inside the ED (1) could be implemented in a public healthcare environment and contribute significantly to the reduction of admissions, (2) could optimize the management of patients at high and intermediate risk and succeed in recognizing CAD in 20% of patients at low risk, and (3) could allow screening for alternative causes of CP in patients without evidence of CAD.This Italian study looked at a large number of chest pain patients treated by protocol. They included a non-validated clinical chest pain scoring system. They analyzed low risk patients with a normal EKG and normal cardiac enzymes drawn between 6 and 12 post chest pain onset. At 6 month follow up 0.2% of the patients were recognized as having non-fatal coronary artery disease thus suggesting a negative predictive value greater than 99%.
This study did not specify which assays were analyzed. There is no mention of percentage follow up or definitions of adverse outcomes.
Level of Evidence 4
Quality of Evidence Fair
Neutral
DeWinter(00)de Winter, R. J., J. G. Lijmer, et al. (2000). "Diagnostic accuracy of myoglobin concentration for the early diagnosis of acute myocardial infarction." Ann Emerg Med 35(2): 113-20.
STUDY OBJECTIVE: We evaluated the diagnostic accuracy of myoglobin determination for the early diagnosis of acute myocardial infarction (AMI). METHODS: Consecutive patients with chest pain were included in the study. Receiver operating characteristic (ROC) analysis was used to assess optimal timing of blood sampling and cutoff values. RESULTS: A total of 309 patients were included, of whom 162 patients had a diagnosis

document.doc Page 20 of 77
of AMI. ROC analysis revealed that the diagnostic accuracy of myoglobin concentration as indicated by the area under the ROC curve (AUC) increased significantly from 3 (0.89+/-0.026) and 4 hours (0.93+/-0.019) to 5 hours after onset of symptoms (0. 96+/-0.014; P=.0040 and.035, respectively). At 5 hours (the earliest time point with maximal AUC), sensitivity was 87% and specificity was 97% using a myoglobin cutoff value of 90 microg/L. With a myoglobin cutoff value of 50 microg/L, sensitivity was 95% (95% confidence interval 90% to 98%), but specificity was 86% (95% confidence interval 80% to 93%). CONCLUSION: Myoglobin has maximal diagnostic accuracy for the diagnosis of AMI at 5 hours after the onset of symptoms, using a cutoff value of 50 microg/L. In combination with the measurement of other biochemical markers, myoglobin determination could be particularly useful for triage of patients with AMI at an early stage.
Looked at 309 pts;162 diagnosed as AMI by WHO criteria and patients with severe muscle damage had been excluded!! Median duration of symptoms 2.25 hrs; very short and would affect myoglobin values.!! With ROC curves found, at 5 hrs post symptom onset, by lowering myoglobin thresholds from 90 ug/L to 50 ug/L the sens/spec went from 87/97% to 95/86%. 24 hr TnT used for specificity analysis.These conclusuions cannot be generalized to all EDs.
Level of Evidence 7Quality-GoodSupportive
Domanovits(02) Domanovits, H., M. Schillinger, et al. (2002). "Acute chest pain-a stepwise approach, the challenge of the correct clinical diagnosis." Resuscitation 55(1): 9-16.
STUDY OBJECTIVE: To assess the safety and the accuracy of a 4 h stepwise diagnostic approach relying on clinical judgement in unselected patients with acute chest pain. DESIGN: Prospective cohort study. SETTING: Emergency department (ED) of a tertiary care university hospital. PATIENTS: 1288 unselected patients presenting with acute chest pain. INTERVENTIONS: After history and physical examination, clinical judgement (step I), governed the need for further patient evaluation: baseline 12 lead electrocardiogramm (ECG) and laboratory examinations (step II), serial 12 lead ECG and laboratory examinations after 4 h (step III), and 4 h troponin T measurement (step IV) to exclude or to confirm a coronary origin of chest pain. Patients were followed clinically for 6 months for future occurrence of cardiac events (myocardial infarction, percutaneous transluminal coronary angioplasty (PTCA), CABG, cardiac death), any death and for accuracy of the ED diagnosis in non-coronary chest pain patients. MEASUREMENTS AND RESULTS: Chest pain was diagnosed to be coronary in origin in 381 and non-coronary in 907 patients, respectively. Cardiac events occurred during follow up in 240 (19%) of 1288 patients, in 233 of 381 (61%) with presumed coronary and seven of 907 (1%) with presumed non-coronary chest pain. Sensitivity, specificity, positive predictive value and negative predictive value for correct detection of coronary chest pain were 97, 86, 61 and 99%, respectively. In non-coronary chest pain patients the agreement between the ED diagnosis and the final diagnosis was good (kappa=0.71, 95% confidence interval (CI) 0.67-0.75). CONCLUSIONS: The 4 h stepwise approach guided by clinical judgement was safe for ruling out impending cardiac events in unselected patients with acute chest pain. However, more extensive evaluation is necessary for accurate rule-in of coronary chest pain.
This Austrian study looked at patients presenting with chest pain and assayed initially for CK-MB if normal repeat assays were done at 4 hours with the option of ordering a troponin T measurement. No description of the assay was mentioned. The study describes a follow up period of 6 months ;they captured 78% of patients. There was a 19% rate of cardiac events including 1% in presumed non coronary chest pain patients. They describe a sensitivity of 97% and specificity of 86% with a PPV of 61% and NPV of 99% however it is unclear what relationship the cardiac enzyme assays had to these values. It is also unclear how they defined their outcome measures.
Level of Evidence 4
Quality of Evidence Fair
Neutral

document.doc Page 21 of 77
Ebell(00:2) Ebell, M. H., L. L. White, et al. (2000). "A systematic review of troponin T and I values as a prognostic tool for patients with chest pain." J Fam Pract 49(8): 746-53.
OBJECTIVE: The accuracy of the troponin T and I test as a prognostic tool for patients with chest pain varies considerably depending on the patient population, the cutoff for an abnormal test result, and other factors. The goal of our systematic review was to synthesize the best available evidence on this topic. SEARCH STRATEGY: We searched the MEDLINE database, bibliographies of identified articles, and articles identified from a previous meta-analysis of diagnosis. SELECTION CRITERIA: We included cohort studies that had at least 80% follow-up and reported useful data. DATA COLLECTION AND ANALYSIS: Data from each study were abstracted by 2 investigators. We calculated sensitivity and specificity for the prediction of death, fatal or nonfatal myocardial infarction (MI), or any cardiac event for each combination of patient population, troponin test, interval from admission to blood draw, and cutoff for an abnormal test result. MAIN RESULTS: For patients with chest pain and a normal electrocardiogram, the peak troponin I level drawn 6 or more hours after the onset of chest pain is useful for identifying patients at low risk of death or nonfatal MI at 30 days (negative likelihood ratio=0.07; probability of outcome=0.3% with a negative test, given a pretest probability of 4.4%). For patients with unstable angina, the sensitivity of troponin I for the identification of patients who die or have a nonfatal MI in the next 30 days is only 59%, and the specificity is only 79%. The sensitivity and specificity varied widely for patients with unstable angina or non-Q-wave MI depending on the inclusion criteria, cutoff used, timing of the blood draw, duration of follow-up, aim other factors. CONCLUSIONS: If the peak troponin T or I level measured at least 6 hours after the onset of chest pain symptoms is in the normal range in a patient with a normal electrocardiogram, it is very unlikely that the patient will die or have a nonfatal MI in the next 30 days (< or =1%). The initial troponin value is not as helpful as the peak value at least 6 hours after the onset of chest pain. An abnormal troponin test result for patients with unstable angina or non-Q-wave MI identifies a subset at greater risk of death.
This is a systematic review of troponin T and I values on patients with chest pain looking as a prognostic tool with end points being cardiac death and non fatal MI 30 days post emergency room visit. The author searched Medline and also several journals up through and including December 1999 for CEBM 1b articles. Their inclusion criteria included only prospective cohort studies of adult populations with acute chest pain. Each study had to have had an 80% follow up looking at the outcome stated. They excluded studies with only in hospital outcomes or where calculations for sensitivity or specificity were not available.
They looked at 28 studies; they divided data into just chest pain syndrome or unstable angina (defined as chest pain with EKG changes) and then non Q wave MI group (defined as biochemical criteria for MI but no Q waves on EKG). For chest pain alone they quote Hamm 1997 study as being the best, where they reported sensitivity of .94, specificity of .81 LR+ of 5.0 and LR- of 0.07. In patients with unstable angina they looked at 3 studies with only death as a follow up between 30 days and 9 months. In the best study they found a sensitivity of 0.52 and specificity of 0.73; the 3 tests studies in summation found a sensitivity of 0.59, specificity of 0.79 a positive LR of 2.8 and a LR- of 0.5; looking at troponin T they analyzed 3 studies and found summary tests characteristics of sensitivity of 0.63, specificity of 0.66, LR+ of 1.9 and LR- of 0.6. Looking at the third group of unstable angina or non Q wave MI patients with positive biochemical markers (WHO) criteria they a found a range of sensitivity of 0.59 to 1 and specificity of .6 to .74;for troponin T studies a positive LR of 1.3 to 1.8 and a LR- of 0 to 0.3.
They quote Hamm study that if a troponin T or I level is measured at least 6 hours after the onset of chest pain symptoms and is in the normal range, with a normal EKG, the likelihood of the patient suffering cardiac death or non fatal MI in the next 30 days would be less than 1%.
Level of Evidence 1a
Quality of Evidence Excellent
Supportive
Ebell(00:1)Ebell, M. H., D. Flewelling, et al. (2000). "A systematic review of troponin T and I for diagnosing acute myocardial infarction.[see comment]." Journal of Family Practice 49(6): 550-6.

document.doc Page 22 of 77
OBJECTIVE: Elevations of serum troponin T and I values are being used to diagnose acute myocardial infarction (AMI) and to rule out the condition in patients before their discharge from the emergency department (ED). However, the sensitivity and specificity of these tests vary considerably. Our goal was to systematically review the data on the accuracy of troponin T and I for the diagnosis of AMI in the ED. SEARCH STRATEGY: We searched the MEDLINE database using the following strategy: troponin (text word) and diagnosis (medical subject heading [MeSH]) or troponin/diagnostic use (MeSH). The references of articles meeting our inclusion criteria were searched for additional articles. SELECTION CRITERIA: We evaluated each study for quality. Only prospective blinded cohort studies with an adequate reference standard were included in the analysis. DATA COLLECTION/ANALYSIS: Data from each study were abstracted by 2 investigators. We graphed sensitivity and specificity for different points in time from arrival in the ED or from the onset of pain and calculated summary estimates when appropriate and possible. MAIN RESULTS: Sensitivity increases for both troponin T and I from 10% to 45% within 1 hour of the onset of pain (depending on the cutoff) to more than 90% at 8 or more hours. Specificity declines gradually from 87% to 80% from 1 to 12 hours after the onset of chest pain for troponin T and is approximately 95% for troponin I. The peak abnormal value in the first 24 hours after admission to the ED has an area under the receiver operating characteristic curve of 0.99 and is very useful at ruling out AMI if negative. CONCLUSIONS: Although troponin T and I values are useful tools for the diagnosis of AMI, they must be interpreted according to the number of hours from the onset of chest pain. The test is particularly useful at ruling out MI when the value is negative at 8 or more hours after the onset of chest pain. [References: 24]
This systematic review of troponin T and I. It looked only at diagnosing AMI and not unstable angina. It was very strict in what studies it included and excluded. It had to be a prospective data collection, the physician determining whether an MI occurred had to be blinded to the troponin results, it used the WHO reference standard for diagnosing MI, authors had to report data for calculating sensitivities and specificities for at least 1 point from the onset of pain or presentation to the ED for troponin T or I. Included were nonconsecutive studies! This study looked at 124 articles. The authors found great heterogeniticy in the studies. Their conclusion is a normal troponin T or I value from blood drawn 8 or more hours from the onset of chest pain is a strong evidence against the presence of AMI. A normal value of troponin T or I at the time of admission or within 4 or fewer hours of the onset of pain does not significantly reduce the likelihood of AMI.
Level of Evidence 7
Quality of Evidence Excellent
Supportive
Ellestad(00)Ellestad, M. H., R. Startt-Selvester, et al. (2000). "The utility of four biochemical markers in the triage of chest pain patients." Cardiology 93(4): 242-8.
Four biochemical markers, creatine kinase (CK)-MB isoenzyme, myoglobin, myosin light chains and troponin I, were studied in 1,338 patients presenting to the emergency department with chest pain suggestive of coronary artery disease (CAD). One hundred and eighty-seven patients had an acute myocardial infarction (MI). At least one of the four markers was over the threshold on the first sample in 78% of MI patients, as compared to only 40% with an elevated CK-MB. After 4 h, 88% had at least one marker elevated. None of the 69 patients with atypical chest pain, no history of CAD, no markers over threshold on the first sample and a normal electrocardiogram had an acute MI or unstable angina. If we had discharged this group, we would have saved USD 264,000, estimating a cost of USD 2,000 per day. Using four biochemical markers improved the early diagnosis of CAD and may help identify groups suitable for early discharge. Copyright 2000 S. Karger AG, Basel
This study looked at 4 markers STAT assay and then at 4 hours and 8 hours, Included were patients suspicious for ACS but not in cardiogenic shock or cardiac arrest prior to arrival. Assays were for CK-MB myoglobin myosin light chain and troponin I. This study was supported by Spectral Diagnostics. Diagnosis of MI was criteria that included LDH or AST elevation!, for unstable angina using AHCPR guidelines for high, intermediate, and low risk unstable angina. Follow up was at 3 months, but only 84% could be reached. There is no change in diagnosis determined from

document.doc Page 23 of 77
hospital data on the initial visit. This is a very unusual statistic. The results include data from which specificity and sensitivity can be derived; in those patients with an MI documented, levels of myoglobin, CK-MB, myosin light chain and troponin were elevated in 67, 64, 67, and 71% of the time respectively at 4 hours. One of the 4 markers was elevated in 78% on admission and 88% after 4 hours. There were no specificity values nor subsets analyzed based on duration of pain prior to assay. This was a large study in 2 centers involving 1, 338 patients of which 187 had an AMI.
Level of Evidence 4Quality of Evidence FairNeutral
Esses(01)Esses, D., E. J. Gallagher, et al. (2001). "Six-hour versus 12-hour protocols for AMI: CK-MB in conjunction with myoglobin." American Journal of Emergency Medicine 19(3): 182-6.
The objective was to test the hypothesis that a protocol using myoglobin and creatine kinase-MB (CK-MB) can rapidly and safely exclude myocardial infarction (MI). The study used a prospective, convenience cohort of ED patients with clinically suspected myocardial ischemia. Myoglobin was measured on presentation, 2 and 6 hours later; CK-MB was measured on presentation, 6, 12, and 18 hours later. Of 519 patients, 76 (15%) had MIs, all of whom "ruled in" within 12 hours using a combination of myoglobin and CK-MB, for a sensitivity of 100% (95% CI, 95% to 100%), specificity of 92% (95% CI, 89% to 94%), LR (+) of 12 (95% CI, 9 to 16), and an LR (-) of 0.03 (95% CI, 0.0 to 0.05). Of the 76 patients with MIs, 73 ruled in with a 6 hour protocol, also using a combination of CK-MB and myoglobin, for a sensitivity of 96% (95% CI, 89% to 99%), specificity of 92% (95% CI, 89% to 94%), LR (+) of 11 (95% CI, 8 to 16), and an LR (-) of 0.04 (95% CI, 0.01 to 0.12). Our results support the hypothesis that, using an abbreviated protocol with CK-MB and myoglobin, MI can be reliably ruled out in ED patients with suspected ischemia.
This study looked solely at CK-MB and myoglobin in the diagnoses of AMI. 519 patients were enrolled. EKG changes and renal failure patients were not excluded. CK-MB assays were defined as positive if greater than 4 ng per milliliter or greater than 5% of the CK-MB ratio. Myoglobin was defined as greater than 100 ng per ml. The study found that 6 hour assays were very good in diagnosing AMI. The combination of the 2 studies at 6 hours had a sensitivity of 96% and a specificity of 92% with a positive likelihood ratio of 11 a negative ratio of 0.04 with 95% CI being 0.01 to 0.12.
The AMI diagnosis was based on an elevated CK MB at 18 hours and so incorporation bias is high.
Level of Evidence 4
Quality of Evidence Fair
Supportive
Fesmire (02)Fesmire, F. M., A. D. Hughes, et al. (2002). "The Erlanger chest pain evaluation protocol: a one-year experience with serial 12-lead ECG monitoring, two-hour delta serum marker measurements, and selective nuclear stress testing to identify and exclude acute coronary syndromes.[see comment]." Annals of Emergency Medicine 40(6): 584-94.
CONTEXT: The rapid and accurate diagnosis of the etiology of chest pain is of central importance in the triage of patients presenting to emergency departments. The "first-draw" sensitivity of serum cardiac markers is known to be low on initial presentation; however, less is understood regarding the predictive value of a positive test in this situation. OBJECTIVE: To determine the ability of a critical pathway combining medical history and physical examination, electrocardiographic findings, point-of-care testing, and central laboratory data to accurately predict the presence of acute coronary ischemia. METHODS: We investigated the positive predictive value of a testing algorithm for first-draw specimens in clinical practice, combining a qualitative, point-of-care, triple-screen testing panel for cardiac markers, including myoglobin, creatine kinase-MB, and cardiac troponin I, with confirmation of the rapid assay in the central hospital laboratory by quantitative assays for creatine kinase-MB and cardiac troponin T. RESULTS: While a positive result on any of the individual cardiac markers of the point-of-care test had a positive predictive

document.doc Page 24 of 77
value for the acute coronary syndrome of only 36% (creatine kinase-MB, 41%; myoglobin, 36%; and troponin I, 65%), the positive predictive value for the diagnosis of acute coronary syndrome increased to 76% if all 3 point-of-care markers were simultaneously positive. The positive predictive value for acute coronary syndrome for a positive confirmatory result in the hospital laboratory for either creatine kinase-MB or cardiac troponin T was 61%. Among those patients with a positive marker on both the point-of-care test and the laboratory test, a careful retrospective review of the clinical history (with exclusion of patients with nonischemic cardiac pathologies and renal insufficiency) increased the positive predictive value of this algorithm to 98%. CONCLUSIONS: Our data suggest that qualitative, point-of-care, triple-screen cardiac marker testing of patients with chest pain at initial presentation may exhibit relatively low positive predictive values. Positive predictive value can be significantly improved by rapid confirmation in the hospital laboratory and careful review of clinical findings.
Well designed; looked at delta 2hr change in CK MB and TnI (minimum thresholds based on previous protocol using 4X imprecision for the assay).Median duration of pain was 3.9 hrs prior to evaluation.At 2 hrs the Sens/Spec/PPV/NPV was 93.2/93.9/15.3/0.07 for AMI vs baseline 58.1/99.4/247/0,74. The data for 30 day adverse outcome, baseline assays/2 hr delta values, were as follows: 37.6/66.1, 99.5/94.9, 82.3/12.78, 0.63/0.36The SECG ( serial EKGs) incorporated added a neglible increase.
Level of Evidence 1bQuality of Evidence ExcellentSupportive
Fesmire (00:2)Fesmire, F. M. (2000). "A rapid protocol to identify and exclude acute myocardial infarction: continuous 12-lead ECG monitoring with 2-hour delta CK-MB." American Journal of Emergency Medicine 18(6): 698-702.
A prospective observational study was performed in 706 chest pain patients who underwent our chest pain evaluation protocol which consists of continuous 12-lead ST-segment monitoring with automated serial ECG (SECG) and a 2-hour delta (delta) CK-MB level determination before ED physician making final disposition decision to determine the incremental value of our 2-hour protocol for identifying myocardial infarction (MI) as compared with the initial ECG in combination with a baseline CK-MB. The initial ECG was obtained on presentation and considered positive if it revealed injury or ischemia. SECGs were obtained at least every 10 minutes and considered positive if it revealed new injury or ischemia. The baseline CK-MB value was considered positive if it was > or =12 ng/mL and index > or =4%. ACK-MB was defined as a difference between the 2 hour and baseline CK-MB and was considered positive if the value was > or =+1.5 ng/mL. MI was defined as acute myocardial infarction (AMI) or recent AMI (ie, AMI patients presenting on falling curve of CK-MB). The incremental value of the 2 hour protocol (ie, SECG in conjunction with deltaCK-MB) was more sensitive for identification of MI than the baseline protocol (ie, initial ECG in conjunction with the baseline CK-MB) (94.0% versus 55.4%; P < .0001) and reliably both identified (+LR = 14.6) and excluded MI (-LR = 0.06). SECG monitoring in conjunction with the 2 hour deltaCK-MB allows for early identification and exclusion of MI, and can assist the ED physician in making appropriate treatment and disposition decisions.
Baseline/ 2hr marker sens/spec/+LR/-LR: 55.4%/94.0%, 98.6%/93.6%, 38.4/14.6, 0.45/0.06.This includes an incorporated Serial EKG sens that jumped sens 20%. This is the traditional 12 lead monitoring that
Is prevalent in many centers and so I have accepted the analysis. I assume since this study was over 3 years that patients were nonconsecutive. Incorporation bias
Level of evidence 4 Quality of Evidence Good Supportive

document.doc Page 25 of 77
Fesmire(00:1) Fesmire, F. M. (2000). "Delta CK-MB outperforms delta troponin I at 2 hours during the ED rule out of acute myocardial infarction." American Journal of Emergency Medicine 18(1): 1-8.
It has been shown that a rise in creatine kinase MB bank (CK-MB) of > or = + 1.6 ng/mL in 2 hours is more sensitive and equally specific for detection of acute myocardial infarction (AMI) as compared with a 2-hour CK-MB > or = 6 ng/mL during the emergency department (ED) evaluation of chest pain. Because cardiac specific troponin I (cTnI) is thought to have similar early release kinetics as compared with CK-MB mass, we undertook a retrospective cohort study in 578 chest pain patients whose baseline CK-MB and cTnI was less than two times the hospital's upper limits of normal and who underwent a 2-hour CK-MB and cTnI to compare sensitivities and specificities of the 2-hour delta CK-MB (deltaCK-MB) and delta cTnI (delta cTnI) for AMI and 30-day Adverse Outcome (AO). Thirty day AO was defined as AMI, life-threatening complication, death, or percutaneous transluminal coronary angioplasty (PTCA)/coronary artery bypass graft (CABG) within 30 days of ED presentation. Optimum delta values were determined by choosing the smallest cutoff value greater than the assay precision where the deltaCK-MB and delta cTnI had a positive likelihood ratio for 30-day AO of > or = 15. A deltaCK-MB > or = +1.5 ng/mL was more sensitive than a deltaTnI > or = +0.2 ng/mL for AMI (87.7% versus 61.4%; P < .0005) and 30-day AO (56.7% versus 42.3%; P < .005). There were no differences in specificities for AMI and 30-day AO. Combining the two tests (MBdelta > or = +1.5 ng/mL and/or a deltaTnI > or = +0.2 ng/mL) resulted in an incremental increase in sensitivity of 89.5% for AMI and 61.9% for AO (P < .005). Patients with either a rise in CK-MB of > or = +1.5 ng/mL or rise in cTnI of > or = +0.2 ng/mL in 2 hours should receive consideration for aggressive antiischemic therapy and further diagnostic testing before making an exclusionary diagnosis of nonischemic chest pain.
This oft-sited article dealt with 578 consecutive patients who were assessed for acute coronary syndrome using initial screening of EKG and baseline elevation CK-MB or troponin I. Negative patients then went on to have serial EKGs and 2 hour assays of CK MB or troponin looking for a change of elevation of 1.5 ng per milliliter or 0.2 ng per milliliter respectively over 2 hours as well as clinical diagnosis of ACS despite a negative 2 hour evaluation and selective stress testing. Exclusion criteria included patients not undergoing emergency coronary angiography or those with tachydysrythmia, pulmonary edema requiring mechanical ventilation, chest pain deemed not suitable for workup and patients who did not present with chest pain.
The arbitrary delta values were previously derived by Fesmire. The figure of 1.5 ng per milliliter was derived by looking at the manufacture’s measurement of CK-MB inprecision being 0.4 ng per milliliter;therefore a statistical significance of delta CK-MB would be 4 times the possible biologic variation. I’m not aware of any other authors validating these figures. Clinical judgment was always integral to every step in the protocol. 30-day outcomes were very complete both in its definition and retrieval rate.
The baseline assays were drawn at 35 plus minus 30 minutes after ED arrival. The average duration of chest pain was 3.9 hours plus or minus 4.3 hours. The incremental value of the delta serum markers in addition to EKG serum baseline markers and serial EKG testing(the latter was negligible)is as follows for the detection of MI: sensitivity 93.2 specificity 93.9 positive LR 15.2 negative LR of 0.07. The same values for the detection of 30 day ACS are sensitivity 66.1 specificity 94.9 positive LR of 12.75 and negative LR of 0.36.
Level of Evidence 7
Quality of Evidence Good
Supportive
Fesmire(04)Fesmire, F. M., R. H. Christenson, et al. (2004). "Delta creatine kinase-MB outperforms myoglobin at two hours during the emergency department identification and exclusion of troponin positive non-ST-segment elevation acute coronary syndromes." Ann Emerg Med 44(1): 12-9.
STUDY OBJECTIVE: Limited information is available about the diagnostic performance of creatine kinase (CK)-MB and myoglobin levels during the early evaluation of chest pain

document.doc Page 26 of 77
patients using cardiac troponins as the criterion standard for diagnosing acute myocardial infarction. In this study, we compare the sensitivity and specificity of the baseline, 2-hour absolute, and 2-hour delta values of myoglobin and CK-MB mass assay for detection of acute myocardial infarction using cardiac troponin I (troponin) as the sole marker of myocardial necrosis. METHODS: A prospective observational study was conducted of 975 chest pain patients with a baseline troponin level of 1.0 ng/mL or less (Abbott Axsym Assay) and an initial ECG nondiagnostic for injury. CK-MB, myoglobin, and troponin levels were all measured on the Abbott Axsym immunoassay. Acute myocardial infarction was diagnosed if there was at least 20 minutes of chest pain and any one of the following criteria within 24 hours of ED presentation: a serial increase in troponin to more than 1.0 ng/mL, new Q-wave formation in 2 contiguous leads, or patient death by cardiac or unknown cause. The optimal values of CK-MB and myoglobin were chosen at the most accurate value on the receiver operating characteristic (ROC) curve (ie, value with lowest false-negative and false-positive rate) of the 2-hour absolute and 2-hour delta value for predicting acute myocardial infarction. RESULTS: Acute myocardial infarction was diagnosed in 44 (4.5%) of the 975 study patients. ROC curve analysis revealed no statistically significant differences in areas for myoglobin and CK-MB values at baseline and 2 hours for determination of acute myocardial infarction. However, the ROC curve area of the delta CK-MB level significantly outperformed the ROC curve area of the delta myoglobin level for early identification of acute myocardial infarction (0.97 versus 0.81; 95% confidence interval [CI] for difference between areas 0.09 to 0.24). At the most accurate cutoff value, a 2-hour delta CK-MB level more than 0.7 ng/mL had a sensitivity of 93.2% (95% CI 81.3% to 98.5%), a specificity of 94.4% (95% CI 92.7% to 95.8%), a positive likelihood ratio of 16.7, and a negative likelihood ratio of 0.07. CONCLUSION: A 2-hour delta CK-MB level outperforms myoglobin level in the early identification and exclusion of acute myocardial infarction in non-ST-segment elevation chest pain patients. This finding suggests that myoglobin may no longer be the optimal early marker of acute myocardial infarction when troponins are used as the criterion standard.
Looked at 975 Chest pain Pts.with initial Tn levels normal(ESC AMI criteria.4.5% had AMI therefore low prevalence; their median times were 1.5 hrs symptoms to presentation.Of the 931 remaining, 40% underwent stress testing.After ROC analysis they found CK MB performed better than myoglobin – a 2 hr delta myoglobin had Sens 93.2%,spec 94.4%,PPV 16.7,NPV 0.07 for predicting AMI
Level of Evidence 7Quality of Evidence GoodSupportive
Fromm(01)Fromm, R., D. Meyer, et al. (2001). "A double-blind, multicentered study comparing the accuracy of diagnostic markers to predict short- and long-term clinical events and their utility in patients presenting with chest pain." Clinical Cardiology 24(7): 516-520.
Background: Millions of patients present annually with chest pain, but only 10% have myocardial infarction (MI). We recently reported comparative sensitivity and specificity of available markers in the diagnosis of MI; however, optimum interpretation of marker results requires prognostic follow-up data. Hypothesis: The study was undertaken to study the accuracy of CK-MB subforms, troponin I and T, myoglobin, and CK-MB in predicting clinical events at 30 days and 6 months. Methods: In all, 955 consecutive patients with chest pain were enrolled in a prospective, multicenter, double-blind study to test the prognostic accuracy of these markers. Results: Myocardial infarction was diagnosed in 119 by CK-MB mass criteria and unstable angina (UA) in 203 patients by clinical criteria. Follow-up at 30 days and 6 months was available in 824 and 724 patients, respectively, with mortalities of 2.8 and 4.14%, respectively. Cumulative 6-month mortality was 5.6% in MI, 4.4% in UA, and 3.0% in others. Revascularization was reported in 9.3% of patients by 6 months. A positive test on each of the markers except myoglobin was predictive of revascularization. The composite endpoint of death or revascularization occurred in 107 patients by 6 months and a positive result on each of the markers was predictive of this composite endpoint (p < 0.05). The relative risk of death or revascularization for patients who did not have MI but tested positive on each of the markers was > 1.0 but did not reach statistical significance. Conclusions: With the possible exception of myoglobin, each of the diagnostic

document.doc Page 27 of 77
markers displayed similar prognostic performance in patients with chest pain presenting to emergency departments. The most appropriate markers to triage patients with chest pain, which has both adequate early diagnostic sensitivity and prognostic accuracy, are the CK-MB subforms.
This large study out of Texas was a prospective multi center double blinded trial. Multiple markers were assayed and WHO criteria for AMI was the end point. Follow-up was at 1 and 6 months. 12.5% of 995 patients had AMI (119).The threshold levels for assays were as following; CK-MB activity > 120 iu per L; CK-MB mass > 7 nanogram per milliliter; MB isoforms (MB2) > or = 2.6; MB2/MB1 > or = 1.7; CK-MB activity > 9 iu per L; myoglobin > 85 nonograms per milliliter, troponin T > 0.1 nanogram per milliliter; and troponin I > 1.5 nanogram per milliliter. Though assays were taken at multiple times only the 6-hour level is pertinent to my hypothesis. Sensitivities and specificities for AMI at the 6 hour level were as following; MB activity 74.5/97.5; myoglobin 78.7/89.4; TnT 61.7/96.1; TnI 57.5/94.3; MB subforms 91.5/89.
From this study they say that CK-MB subforms are the preferred diagnostic and prognostic marker in the ED. Since AMI was diagnosed by CK MB there is some interdependency.
Level of Evidence 1b
Quality of Evidence Good
Suppo SupportiveGibler (00)
Gibler, W. B., J. W. Hoekstra, et al. (2000). "A randomized trial of the effects of early cardiac serum marker availability on reperfusion therapy in patients with acute myocardial infarction: the serial markers, acute myocardial infarction and rapid treatment trial (SMARTT)." Journal of the American College of Cardiology 36(5): 1500-6.
OBJECTIVES: We sought to determine the predictive ability of troponin I (TnI) in a heterogeneous group of patients with chest pain admitted from the emergency department (ED) for exclusion of myocardial infarction (MI). BACKGROUND: Previous studies in high-risk patients demonstrated that troponin elevations are associated with increased cardiac events. Little information is available on its predictive ability in more heterogeneous, lower risk patients. METHODS: Consecutive patients admitted from the ED for possible MI underwent serial myocardial marker sampling of TnI and creatine kinase, CK-MB over an 8-h period. Patients with ST segment elevation were excluded. End points included MI, death, significant complications (e.g., cardiac or respiratory arrest, intra-aortic balloon pump, pulmonary artery catheter or pacemaker placement, revascularization or inotropic infusion) and significant disease. RESULTS: Events occurred in 513 (27%) of the 1,929 patients evaluated: MI in 175 (9.1%) and death in 34 (1.8%); an additional 248 patients (13%) without MI had complications, and 323 (17%) without MI had significant disease. Sensitivity of TnI for MI was high (96%). Patients without MI who were TnI-positive were more likely to have complications (43% vs. 12%) or significant disease (41% vs. 17%) as compared with those who were TnI-negative; however, the sensitivity of TnI for these two end points was low (14% and 21%, respectively). Predictive values were unchanged after excluding patients with ischemic electrocardiograms. CONCLUSIONS: Troponin I had a high sensitivity for MI when used as part of a rapid rule-in protocol; however, the sensitivity for other end points was low. Use of TnI alone failed to identify the majority of patients who had either significant disease or complications.
This trial looked primarily at whether presentation myoglobin/CK-MB values compared to 3 hour assays would affect the incident of thrombolysis from the emergency department.
There is secondary data on AMI as an endpoint- Myoglobin , CK-MB, Combo Sens/Spec 64.1/90.2,52.6/96.7,72/88.5 respectively.
Level of Evidence 1b
Quality of Evidence Good
Neutral
Goldmann(04)Goldmann, B. U., L. Langenbrink, et al. (2004). "Quantitative bedside testing of troponin T: Is it

document.doc Page 28 of 77
equal to laboratory testing? The cardiac reader troponin T (CARE T) study." Clinical Laboratory 50(1-2): 1-10.
The progressive evolution of cardiac marker testing in patients with acute coronary syndromes has extended their role into risk stratification and guidance of therapeutic regimen. To provide utilization of cardiac markers around the clock and facilitate the diagnostic work-up of patients with acute chest pain in the emergency room, a point-of-care system for quantitative troponin T and myoglobin testing in whole blood samples was developed. Aim of this multicenter study was to evaluate bedside quantitative determination of myoglobin and troponin T in chest pain patients in a clinical routine setting. Five hospitals in Germany were contributing to blood sampling and 741 patients were included four hours (median) after onset of cardiac pain. Comparison between the rapid test and the established laboratory-based method showed a sufficient agreement of results with a correlation of r = 0.89 (Y=0.856x+0.029) for troponin T and r = 0.912 (Y=+1.145x + 3.457) for myoglobin. Diagnostic sensitivity and prognostic power of the troponin T results obtained in the emergency unit were thoroughly equivalent to the laboratory-based method. The results show that the cardiac reader system represents a promising alternative to central laboratory testing with an accuracy sufficiently for rapid decision making in the emergency room. Myoglobin results in this study did not add supplementary information to the cardiac reader troponin result. However, point-of-care testing of troponin T is advantageous whenever marker results could positively effect initial triage decisions and interventional management choices.
This study from 5 hospitals in Germany looked at point of care testing versus in hospital lab testing for ACS. 741 Patients were included with a median 4 hours from onset of chest pain to arrival in the ED. This study was sponsored by ROCHE pharmaceuticals. Inclusion criteria were people with ischemic type chest pain lasting < 12 hours before arrival. Bloods were drawn at times 0 and 2 to 6 hours post enrollment.Initial TnT Sens AMI 62; Sens 4 hr 97
Level of Evidence 1bQuality of Evidence Good
Suppo SupportiveGreen(00:1)
Green, G. B., E. Dehlinger, et al. (2000). "CK-MB isoforms for early risk stratification of emergency department patients." Clinica Chimica Acta 300(1-2): 57-73.
The potential clinical utility of single sample CK-MB isoforms measurement for early risk stratification of Emergency Department (ED) patients with possible myocardial ischemia was evaluated among 405 patients presenting to two urban EDs. Clinical and serologic data were prospectively collected and the occurrence of adverse events (AEs) and myocardial infarction (MI) during the 14-day outcome period was recorded and utilized to calculate and compare relative risks (RR) and predictive values of isoforms and CK-MB alone. Among the 405 patients, 67 accrued 105 AEs. Both isoforms and CK-MB alone were predictive of AEs with RR of 3.32 (2.09, 5.27) and 6.28 (4.64, 8.52), respectively. Isoforms had higher sensitivity for AEs compared to CK-MB (65.7% [54.3, 77.0] vs. 14.9% [6.4, 23.5]; p<0. 01) but lower specificity (69.2% [64.3, 74.2] vs. 99.7% [99.1,100. 0]; p<0.01). Isoforms' superior sensitivity allowed identification of many high risk patients missed by CK-MB alone. Further, for the prediction of MI, isoforms had superior diagnostic sensitivity and equivalent specificity. This investigation supports the emergency department use of early, single sample CK-MB isoform testing.
This prospective 2-site study looked at CK-MB isoforms versus CK-MB and a diagnosis of ACS as well a predictive of adverse events during 14 days after enrollment (half the standard 30 day endpoint). The 2 sites balanced each other for Afro American versus white population. Clinicians were blinded to the results. Myocardial infarction was diagnosed by standard WHO criteria. Unstable angina was a clinical diagnosis. The analyzer used for all 3 assays was a cardio REP analyzer. The authors used a mathematical model to revise the manufactures thresholds such that the CK-MB value was reassigned from 10 now 12 international units per liter, the CK-MB 2 isoform was initially 2.6 and now 1.7 international units per liter and the MB 2 / MB1 ratio went from > or = 1.7 to > 1.9. These were using previous data utilizing ROC curve analysis for adverse events. They state that chest pain patients were one group of inclusion criteria and they were analyzed into 3 groups based on symptom onset - phlebotomy times to < 6 hours, 6 to 12 hours, > or = 12 hours. 405 patients were enrolled; the median time from pain onset to

document.doc Page 29 of 77
phlebotomy was 3.8 hours. There was no sub group analysis. I presume that all assays were done immediately upon inclusion into the study. 72% were admitted and 28% were discharged home. Though 39 patients (9.6%) suffered an MI the time frame was not clear.
This study emphasized adverse events and not AMI. It did not look at unstable angina. The results for AMI:sensitive 56%, specificity 91%, PPV 40, NPV 95: for CK-MB 23.1, 98.4, 60.0 and 92.3 respectively. I felt there was too much incorporation bias.
Level of Evidence 4
Quality of Evidence Fair
NeutralGreen(98)
Green, G. B., D. J. Li, et al. (1998). "The prognostic significance of troponin I and troponin T." Academic Emergency Medicine 5(8): 758-67.
OBJECTIVES: To determine and compare the prognostic abilities of early, single-sample measurements of cardiac troponin I (cTn-I), cardiac troponin T (cTn-T), and creatine kinase-MB (CK-MB) among ED patients with possible myocardial ischemia. METHODS: Prospective collection of clinical and serologic data using an identity-unlinked technique from patients with possible myocardial ischemia at 2 urban EDs. Outcome data concerning the occurrence of adverse events (AEs) during the 14 days after enrollment were used to calculate and compare the relative risks (RRs) and predictive values (with 95% confidence intervals) of the 3 markers for predicting AEs. RESULTS: Among the 401 study patients, 105 AEs occurred in 67 patients. cTn-I, cTn-T, and CK-MB were all significantly predictive of AEs, with RRs of 3.87 (2.39, 6.26), 3.03 (1.92, 4.79), and 6.45 (4.74, 8.77), respectively. For prediction of AEs, sensitivity for each of the 3 markers was low (cTn-I = 15.38, cTn-T = 24.62, CK-MB = 15.38), while specificity was high (cTn-I = 97.62, cTn-T = 93.15, CK-MB = 99.70). No significant difference in predictive ability was found between cTn-I and cTn-T. However, a positive CK-MB result was a stronger predictor of AEs than either cTn-I (p = 0.01) or cTn-T (p = 0.001). CONCLUSIONS: No significant difference in predictive abilities was found between cTn-I and cTn-T. However, routine testing for both CK-MB and either of the troponins may optimize early identification of high-risk patients so they may be targeted for a higher level of care and consideration of more aggressive therapies.
The study looked at triple marker assay and looked at adverse events 14 days following enrollment that included AMI by WHO criteria. There were 2 sites involved inclusion criteria included ischemic equivalence and any of EKG result. It also included cocaine use. Exclusion criteria included were trauma, inability to consent or clearly a non-cardiac etiology. Assay was drawn immediately upon study entry. The median time from chest pain onset to drawing of blood was 3.8 hours. As in Green’s previous study the thresholds were altered to account for adverse events as opposed to strictly AMI. Therefore, TnI was 1.9 nanograms per milliliter (instead of 1.5) TnT was 0.14 nanograms per milliliter instead of (.2 nanograms per milliliter) and CK-MB was 12 iu per L (instead of 10). The prevalence of AMI was 9.5%. A huge list of adverse events over 14 days were looked at (relatively short endpoint).
Level of Evidence 4Quality of Evidence GoodOpposed
Green(00:2)Green, G. B., G. W. Skarbek-Borowski, et al. (2000). "Myoglobin for early risk stratification of emergency department patients with possible myocardial ischemia." Academic Emergency Medicine 7(6): 625-36.
OBJECTIVES: To determine and compare the prognostic abilities of early, single-sample myoglobin measurement with that of creatine kinase-MB (CK-MB), with cardiac troponin T (cTnT), and with physician judgment in the absence of marker results among emergency department (ED) patients with possible myocardial ischemia. METHODS: Prospective collection of clinical and serologic data using an identity-unlinked technique from patients with possible myocardial ischemia at two urban EDs. Outcome data concerning the occurrence of adverse events (AEs) during the 14 days after enrollment were used to calculate and compare the relative risks (RRs) and predictive values (with 95% confidence intervals) of the various markers for predicting

document.doc Page 30 of 77
AEs. RESULTS: Among 396 analyzed patients, 65 (16.4%) accrued 104 AEs, including 13 deaths (3.3%) and 31 (7.8%) myocardial infarctions. Myoglobin predicted AEs (RR = 3.36 [95% CI = 2.19 to 5.15]) with significantly higher sensitivity (50.8% [95% CI = 38.6 to 62.9]) than either CK-MB (15.4% [95% CI = 6.6 to 24.2]) or cTnT (24.6% [95% CI = 14.1 to 35.1]), but with lower specificity (81.9% [95% CI = 77.7 to 86.0]; CK-MB = 99.7% [95% CI = 99.1 to 100]; cTnT = 93.1% [95% CI = 90.3 to 95.8]). Myoglobin had prognostic ability among patients with chest pain (3.86 [95% CI = 2.39 to 6.22]) and atypical (non-chest pain) presentations (2.71 [95% CI = 1.09 to 6.71]), including those with a nondiagnostic electrocardiogram (3.11 [95% CI = 1.44 to 6.69]). The combination of myoglobin and physician decision making identified 63 of the 65 patients (96.9% [95% CI = 92.7 to 100]) with subsequent AEs. CONCLUSIONS: The early prognostic sensitivity of myoglobin may allow identification of some high-risk patients missed by physician judgment, CK-MB, and cTnT. Myoglobin should be considered for use in the ED based on both its diagnostic and prognostic abilities.
This study looked at myoglobin comparing it to other markers for adverse events over 14 days. The inclusion criteria accepted cocaine use and any EKG. 6% of patient population could yield false positive myoglobins by either having renal failure, significant trauma, or recent cocaine use. There were 2 sites involved thus diluting the high Afro American population to a generalized one. AMI was diagnosed by WHO criteria, recurrent unstable angina by clinical means. Myoglobin was assayed with STRATUS system CK-MB activity by Cardio REP, TnT by the ELISA. Once again the authors used ROC curve information to revise the manufacture’s AMI cutoff to optimize results for adverse events.New curves were derived for myoglobin. The myoglobin cutoff of > or = 110 nanograms per L was changed to 69 nanograms per milliliter; CK-MB went from > or = 10 international units to 12 international units per L, and TnT cutoff went to > or = 0.2 nanograms per milliliter to 0.14 nanograms per milliliter. Chest pain patients were analyzed according to symptom times –phlebotomy; < 6 hours or > or = to 6 hours. The AMI rate was 9.6%. With regards to the AMI end point myoglobin had a sensitivity of 28.9, specificity of 91.3; CK-MB 23.7, 98.3; TnT 23.7 and 94.7. There was no statistical significance between these low values. Interestingly, when compared to physician diagnostic ability (blinded to all the biochemical biomarker results) the physician sensitivity was 97.4 and specificity of 44.7. The one MI missed by the physician also had triple marker negative results.
Level of Evidence 7
Quality of Evidence Good
Opposing
Gust(98) Gust, R., Gust, A., Bottiger, B. W., Bohrer, H., & Martin, E. (1998). Bedside troponin T testing is not useful for early out-of-hospital diagnosis of myocardial infarction. Acta Anaesthesiologica Scandinavica, 42(4), 414-417.
A very small study in pre hospital determination in AMI. 68 patients were enrolled. Troponin at the bedside was assayed by TROP T-SCHNELL chest with a qualitative cutoff of 0.2 micrograms per liter. The average time between onset of pain and arrival of EMS was 4.3 hours. Only 5 of the 68% tests (7%) had a positive bedside troponin T. ED sampling of patients revealed 16 out of 68 (24%) had an AMI by WHO criteria. Thus, the sensitivity of this bedside test at this threshold was 25 % with specificity 98%. No comment was made as to how soon after arrival the CK-MB assay was performed or how long were transit times.
Level of Evidence 1bQuality of Evidence FairOpposing
Heeschen(00)Heeschen, C., A. Deu, et al. (2000). "Analytical and diagnostic performance of troponin assays in patients suspicious for acute coronary syndromes [In Process Citation]." Clin Biochem 33(5): 359-68 [MEDLINE record in process].
Background: The controversy whether there is a clinically significant difference between troponin

document.doc Page 31 of 77
T (cTnT) and troponin I (cTnI) in regard to predictive value and cardiac specificity is still ongoing.Methods: We evaluated enzyme-linked immunosorbent assay systems for cTnI and cTnT in patients with acute coronary syndromes and multiple control groups to define threshold values for risk stratification and compare their predictive value.Results: In 312 patients with noncardiac chest pain, cTnI levels were below the detection limit of 0.2 &mgr;g/L and cTnT levels were 0.011 [0.010-0. 013] &mgr;g/L. In patients with end-stage renal failure (n = 26) and acute (n = 38) or chronic (n = 16) skeletal muscle damage, median concentrations were 0.20 [0.20-0.35], below the detection limit, and 0.20 [0.20-0.25] for cTnI, and 0.04 [0.01-0.10], 0.011 [0.005-0.025], and 0.032 [0.009-0.054] &mgr;g/L for cTnT. In patients with acute coronary syndromes (n = 1130), maximized prognostic value for 30-day outcome (death, infarction) was observed at a threshold level of 1.0 &mgr;g/L for cTnI (29.0% positive) and at 0.06 &mgr;g/L for cTnT (35. 0% positive). Significant differences in the area-under-the-curve values were observed between cTnI and cTnT (0.685 vs. 0.802; p = 0. 005). For both markers, the area-under-the-curve values did not increase with the second (within 24 h after enrollment) or third (48 h) blood draw. CTnI showed a less strong association with 30-day outcome than cTnT. When cTnI was put in a logistic multiple-regression model first, cTnT did add significant information.Conclusion: By using the defined threshold values and the employed test systems, single testing for cTnI and cTnT within 12 h after symptom onset was appropriate for risk stratification. Despite the lower cardiac specificity for cTnT, it appears to have a stronger association with the patients' outcome, whereas, as previously shown, the ability to identify patients who benefit from treatment with a GP IIb/IIIa receptor antagonist is similar.
This article compared analytical and diagnostic performance between troponin assays for patients rule out ACS and prediction of 30 day AE .Used ROC data to define best troponin threshold from assays at 0, <24,<48 hrs-after randomization.This long delay from symptom onset explains why there was no statistical difference between the serial sampling.
Level of Evidence 4Quality of Evidence FairOpposing
Heidenreich(01)Heidenreich, P. A., T. Alloggiamento, et al. (2001). "The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes: a meta-analysis." J Am Coll Cardiol 38(2): 478-85.
OBJECTIVES: This study was designed to compare the prognostic value of an abnormal troponin level derived from studies of patients with non-ST elevation acute coronary syndromes (ACS). BACKGROUND: Risk stratification for patients with suspected ACS is important for determining need for hospitalization and intensity of treatment. METHODS: We identified clinical trials and cohort studies of consecutive patients with suspected ACS without ST-elevation from 1966 through 1999. We excluded studies limited to patients with acute myocardial infarction and studies not reporting mortality or troponin results. RESULTS: Seven clinical trials and 19 cohort studies reported data for 5,360 patients with a troponin T test and 6,603 with a troponin I test. Patients with positive troponin (I or T) had significantly higher mortality than those with a negative test (5.2% vs. 1.6%, odds ratio [OR] 3.1). Cohort studies demonstrated a greater difference in mortality between patients with a positive versus negative troponin I (8.4% vs. 0.7%, OR 8.5) than clinical trials (4.8% if positive, 2.1% if negative, OR 2.6, p = 0.01). Prognostic value of a positive troponin T was also slightly greater for cohort studies (11.6% mortality if positive, 1.7% if negative, OR 5.1) than for clinical trials (3.8% if positive, 1.3% if negative, OR 3.0, p = 0.2) CONCLUSIONS: In patients with non-ST elevation ACS, the short-term odds of death are increased three- to eightfold for patients with an abnormal troponin test. Data from clinical trials suggest a lower prognostic value for troponin than do data from cohort studies.
This study was a meta-analysis of the prognostic value of troponin in non-ST segment elevation acute coronary syndrome. They searched Medline and reviewed cited references. They used the word “troponin” in the text words or “ angina” “myocardial infarction” or “ ischemia”. They also searched Embase from 1993-1998. They examined cohort studies and clinical trials

document.doc Page 32 of 77
separately. Their explanation for dividing the articles into those with clinical trials versus cohort studies is that patients recruited for trials were likely to be more highly selected then patients from cohort studies with consecutive patients. They also thought unselected patient populations are more heterogenous and therefore have a greater potential for variation in underlying prognosis than would a more homogenous population enrolled in a clinical trial. They found a total of 33 articles. Overall they found patients with a positive troponin (either I or T) had significantly worse outcomes then patients with a negative troponin. Mortality was 5.2% compared with 1.6% yielding an odds ratio of 3.1 with (95% confidence 2.3 to 4.1) was also associated with high death or MI 13.5 % versus 5.9%, odds ratio 2.5 (95% CI 2.0 to 3.1).
They concluded that any risk assessment couldn’t rely solely on troponin levels because the studies of patients with suspected ACS with a negative troponin had an overall mortality between 0.7 and 2.1%; those with EKG changes suggestive of ischemia ranged from 1.6 to 4.4%. There was no data specifically on sensitivity or specificity- overall stats for Adverse Effects was PPV 28%; NPV 5.4%.
Level of Evidence 3aQuality of Evidence GoodNeutral
Herkner(01)Herkner, H., U. Waldenhofer, et al. (2001). "Clinical application of rapid quantitative determination of cardiac troponin-T in an emergency department setting." Resuscitation 49(3): 259-64.
OBJECTIVES: We analysed the clinical use of Troponin-T compared to creatine kinase MB in a non-trauma emergency department setting. BACKGROUND: A newly established single specimen quantitative Troponin T assay allows the clinical application of this parameter. METHODS. Five-hundred Troponin T tests were provided for use by emergency physicians who could combine them with the routine laboratory tests without restriction as to the indication or number of tests per patient. The number of tests per patient, time frame, final diagnosis and additional clinical information gained were recorded. All patients were followed for at least 6 months to verify the diagnosis and to assess the occurrence of cardiac events (nonfatal AMI or cardiac death). The ability of Troponin T and creatine kinase MB tests to predict cardiac events within 6 months were compared. RESULTS: The 500 Troponin T tests were used in 249 patients (median two tests per patient (range 1-5)) within 41 days. The final diagnosis revealed coronary heart disease in 85, non-coronary heart disease in 39, non-cardiac chest pain in 86 and other diagnoses in 39 of the patients. In 14 patients with an elevated creatine kinase MB, myocardial damage could safely be ruled out by a negative Troponin T, in six patients with a normal creatine kinase MB minor myocardial damage could be detected by a positive Troponin T. During follow up 28 cardiac events were recorded. Troponin T had a significantly higher specificity, positive predictive value and proportion of correct prediction for cardiac events within 6 months compared to creatine kinase MB. CONCLUSIONS: Troponin T has proved to be an useful method for diagnosing myocardial damage in routine clinical use in the non-trauma emergency department.
This study is from Vienna. They entered 212 patients into the study comparing troponin T to CK-MB. The troponin assay was Elecsys system, range up to and including 0.1 ng per milliliter. Assays were done 0 and 4 hours after admission. There was no relationship made to duration of pain. There was no selection criteria. Follow up was carried out at 6 months looking at AMI, cardiac death. Ttroponin showed a sensitivity of 75% and a specificity of 98% and a negative predictive value of 96% and a positive predictive value of 84%. CK-MB showed a sensitivity of 61 %, specificity of 91% MPV of 94% and a PPV of 52%;
Of note 14 patients (7%) were CK-MB positive but TnT negative; follow up showed no adverse affects with these patients.
Level of Evidence 3b
Quality of Evidence Fair
Supportive
Herren(01)

document.doc Page 33 of 77
Herren, K. R., K. Mackway-Jones, et al. (2001). "Is it possible to exclude a diagnosis of myocardial damage within six hours of admission to an emergency department? Diagnostic cohort study." British Medical Journal 323(7309): 372-374.
Objective: To assess the clinical efficacy and accuracy of an emergency department based six hour rule-out protocol for myocardial damage. Design: Diagnostic cohort study. Setting: Emergency department of an inner city university hospital. Participants: 383 consecutive patients aged over 25 years with chest pain of less than 12 hours' duration who were at low to moderate risk of acute myocardial infarction. Intervention: Serial measurements of creatine kinase MB mass and continuous ST segment monitoring for six hours with 12 leads. Main outcome measure: Performance of the diagnostic test against a gold standard consisting of either a 48 hour measurement of troponin T concentration or screening for myocardial infarction according to the World Health Organization's criteria. Results: Outcome of the gold standard test was available for 292 patients. On the diagnostic test for the protocol, 53 patients had positive results and 239 patients had negative results. There were 18 false positive results and one false negative result. Sensitivity was 97.2% (95% confidence interval 95.0% to 99.0%), specificity 93.0% (90.0% to 96.0%), the negative predictive value 99.6%, and the positive predictive value 66.0%. The positive likelihood ratio was 13.9 and the negative likelihood ratio 0.03. Conclusions: The six hour rule-out protocol for myocardial infarction is accurate and efficacious. It can be used in patients presenting to emergency departments with chest pain indicating a low to moderate risk of myocardial infarction.
This study looked at 383 consecutive pts. in an inner city Manchester population. It compared CK-MB at 6 hours to a 48-hour troponin T test. It used this as a gold standard for myocardial injury (though an unusual late time frame this was accepted by me). Obvious EKG changes and hypotension, arrhythmia were excluded. The assay for CK-MB was not discussed, but the cutoff was 0.1 micrograms per liter. 11 patients were lost to follow up. 65 patients did not under go a troponin evaluation. These were applied to the WHO classification. Of note the exclusion did not include evaluation of serum creatinine (both troponin T and CK-MB are influenced by its increase). Sensitivity for CK-MB could be derived fro the tables at 97%; specificity was derived at 93%. These figures are very high. No median times were given for onset of pain to arrival to the ED. Assay description and threshold levels were not given. The 48-hour troponin assay can be extrapolated backwards to a 24-hour level but certainly not to a level any earlier.
Level of Evidence 4
Qualityof Evidence Fair
Supportive
Huggon(01)Huggon, A. M., J. Chambers, et al. (2001). "Biochemical markers in the management of suspected acute myocardial infarction in the emergency department." Emergency Medicine Journal 18(1): 15-9.
OBJECTIVES: To compare cardiac troponin T, myoglobin, CK, CKMB activity, CKMB mass and the initial electrocardiogram in the early diagnosis of myocardial infarction in the emergency department. Methods-Biochemical markers were measured at presentation in patients with a possible diagnosis of acute myocardial infarction. Based on the clinical notes, patients were grouped as "definite myocardial infarction" (n = 50), "definite no myocardial infarction" (n = 81) and "uncertain" (n = 96). Sensitivity and specificity and positive and negative predictive values were calculated using the 131 patients with definitely present or absent myocardial infarction. RESULTS: The initial electrocardiogram was more sensitive than any of the markers in the first six hours from symptom onset-sensitivity 74% (95%CI 61% to 88%). The positive predictive value of the initial electrocardiogram was 97% in the first six hours; the markers ranged from 47% to 67%. The negative predictive value of the initial electrocardiogram was 85% in the first six hours; the markers ranged from 61% to 70%. Four patients with non-diagnostic electrocardiograms presenting beyond six hours after pain onset had a myocardial infarct detected by at least three of the biochemical markers in each case. CONCLUSIONS: The electrocardiogram is of more diagnostic use than biochemical markers in the first six hours after the onset of pain, but biochemical markers give additional positive diagnostic information in patients presenting later than this. The negative predictive accuracy of biochemical markers is too low for a single sample to be useful for

document.doc Page 34 of 77
excluding myocardial infarction in the first six hours after onset of symptoms.
This study looked at troponin T, myoglobin and CK-MB assays in differentiating patients at 6 hours from symptom onset. It used no golden standard for a reference point for a myocardial infarct. This study was retrospective. It excluded those patients with uncertain diagnosis. It did not look at unstable angina. There was no formal follow up. It stated the sensitivity of all markers ranged between 23 and 44% with specificity between 82 and 91%, the positive predictive value was between 47 and 67%, the negative predictive value between 62 and 70%. The design was poor enough to not make these conclusions valid.
Level of Evidence 4
Quality of Evidence Fair
Neutral
Jurlander(00)Jurlander, B., P. Clemmensen, et al. (2000). "Very early diagnosis and risk stratification of patients admitted with suspected acute myocardial infarction by the combined evaluation of a single serum value of cardiac troponin-T, myoglobin, and creatine kinase MB(mass)[see comment]." European Heart Journal 21(5): 382-9.
AIMS: The diagnostic and prognostic capacity of biochemical markers of acute myocardial infarction in the emergency department were evaluated in consecutive patients (n=155) with suspected acute myocardial infarction. METHODS AND RESULTS: Serum myoglobin >/=110 microg. l(-1)and creatine kinase MB(mass)>/=5 microg. l(-1)had a high accuracy (0.77-0.85) (ns) for acute myocardial infarction diagnosis in patients presenting >2 h after symptom onset. Troponin-T (>/=0.10 microg. l(-1)) had a lower accuracy (0.53-0.70) for acute myocardial infarction diagnosis, but was the most important 1-year prognostic marker (cardiac death or non-fatal acute myocardial infarction). In patients without ST elevation, combined analysis of two biochemical tests would accurately identify an additional 20% of acute myocardial infarction patients (predictive value of a positive test=0.82) and also identify those without acute myocardial infarction (predictive value of a negative test=0.80). One-year event-free survival was excellent (96%) for patients with two negative biochemical tests, intermediate (74%) for those with discordant tests, and only 53% for patients with two positive biochemical tests. CONCLUSIONS: Analysis of biochemical tests in the emergency department prior to hospital admission could accurately identify approximately 20% additional acute myocardial infarction patients. The prognosis of these patients is poor, and they may be a target for primary PTCA or new early initiated aggressive medical therapies. Copyright 2000 The European Society of Cardiology.
This study looked at a presentation myoglobin, troponin T and CK-MB mass assay. In patients without ST segment elevation they found a combined analysis of 2 markers having PPV of 82% and an NPV of 80%. They have used the WHO criteria for AMI. Of interest 50% of their population had a chest pain for less than 2 hours on presentation. Of note these figures included all patients including those with ST segmental elevation. When they looked at those patients without ST segment elevation the NPV was only .35. These numbers were very small; total non ST elevation patients n = 96.
Level of Evidence 2b
Quality of Evidence Fair
Opposing
Kratz(02)Kratz, A., J. L. Januzzi, et al. (2002). "Positive predictive value of a point-of-care testing strategy on first-draw specimens for the emergency department-based detection of acute coronary syndromes." Archives of Pathology & Laboratory Medicine 126(12): 1487-93.
OBJECTIVE: To evaluate the individual components of a cardiac multimarker panel in the detection of acute myocardial infarction (AMI) in patients with chest pain across a spectrum of renal dysfunction. METHODS: A total of 817 consecutive patients evaluated for a possible AMI in the emergency department (ED) enrolled in a prospective study of cardiac biomarkers assessed using a point-of-care device with myoglobin (MYO), cardiac troponin I (cTnI), and creatine kinase

document.doc Page 35 of 77
myocardial band (CK-MB), recorded at 0, 1.5, 3, and 9 hours. This study did not exclude patients on the basis of renal dysfunction. Baseline renal function was available in 808 patients. Patients were stratified by corrected creatinine clearance (CorrCrCl) into quartiles, and those on dialysis (n = 51) were considered as a fifth comparison group. Those patients with advanced renal dysfunction (CorrCrCl < 47/mL/min/72 kg) or on dialysis had higher rates of diabetes, hypertension, and prior coronary disease. Agreement for the diagnosis of AMI was required of two independent cardiologists using criteria based on history, electrocardiogram, and central laboratory assessment of serial cardiac markers. RESULTS: More than 99% of all patients were admitted to a chest pain observation unit or the hospital. Mean MYO levels were elevated in the presence of renal dysfunction in those with and without myocardial infarction. Both MYO and CK-MB were correlated with CorrCrCl, (r = -0.36, p < 0.01, and r = -0.10, p = 0.01, respectively), while cTnI was not (r = -0.10, p = 0.12). Using multiple receiver operating characteristic curve testing, cTnI was found to be the most consistent marker across all strata of renal dysfunction, including end-stage renal disease on dialysis. The authors did not find a trend for false-positive cTnI and renal dysfunction. CONCLUSIONS: A point-of-care, rapid cardiac biomarker strategy utilizing cTnI is applicable and superior to MYO or CK-MB in the evaluation of chest pain in patients with renal dysfunction.
This study looked at triple enzyme point of care testing at presentation and related it to 1 hospital third generation CK-MB and troponin T testing, the results gave positive predictive values per individual positive point of care test or all 3 point of care tests. This was a convenience sample of patients, relationship to length of symptoms prior to assay was not disclosed, definitions for unstable angina were very loose and did not involve any specific imaging, and 1/3 of the 413 patients initially enrolled were excluded because of wrong assay results recorded. This made an analysis of the predictive values very difficult. No sensitivities or specificities were outlined.
Level of Evidence 4
Quality of Evidence Fair
Neutral
Lau(01)Lau, J., J. P. A. Ioannidis, et al. (2001). "Diagnosing acute cardiac ischemia in the emergency department: A systematic review of the accuracy and clinical effect of current technologies." Annals of Emergency Medicine 37(5): 453-460.
Study objective: Acute cardiac ischemia (ACI) encompasses the diagnoses of unstable angina pectoris and acute myocardial infarction (AMI). Accurate diagnosis and triage of patients with ACI in the emergency department should increase survival for these patients and reduce unnecessary hospital admissions. Methods: We conducted a systematic review of the English-language literature published between 1966 and December 1998 on the accuracy and clinical effect of diagnostic technologies for ACI. We evaluated prospective and retrospective studies of adult patients who presented to the ED with symptoms suggesting ACI. Outcomes were diagnostic performance (test sensitivity and specificity) and measures of clinical effect. Meta-analyses were performed when appropriate. A decision and cost-effectiveness analysis was conducted that investigated various diagnostic strategies used in the diagnosis of ACI in the ED. Results: We screened 6,667 abstracts, reviewed 407 full articles, and included 106 articles in the main analysis. Single measurements of biomarkers at presentation to the ED have low sensitivity for AMI, although they have high specificity. Serial measurements greatly increase the sensitivity for AMI while maintaining their excellent specificity. Diagnostic technologies to evaluate ACI in selected populations, such as electrocardiography, sestamibi perfusion imaging, and stress ECG, may have very good to excellent sensitivity; however, they have not been sufficiently studied. The Goldman Chest Pain Protocol has good sensitivity (about 90%) for AMI but has not been shown to result in any differences in hospitalization rate, length of stay, or estimated costs in the single clinical effect study performed. Its applicability to patients with unstable angina pectoris has not been evaluated. The use of an Acute Cardiac Ischemia-Time-Insensitive Predictive Instrument led to the appropriate triage of 97% of patients with ACI presenting to the ED and reduced unnecessary hospitalizations. Conclusion: Many of the current technologies remain under-evaluated, especially regarding their clinical effect. The extent to which combinations of tests may provide better accuracy than any single test needs further study.This systemic review of English language literature between 1966 and 1998 was carried out

document.doc Page 36 of 77
looking at accuracy and advocacy in clinical effect of diagnostic technologies for ACS. They evaluated both prospective and retrospective studies. They used the Medline search, a review of references from retrieved articles, assistance from domain experts as well as a references fro the 1997 report of the NHAAP working group on evaluation of technologies for identifying acute coronary ischemia in emergency departments. A total of 106 articles were fully reviewed. Tabulated were the individual enzyme assays. More studies included CK-MB than myoglobin than troponin I or troponin T.
In summary, this SR showed that a single measurement of biomarkers at presentation to the ED had poor sensitivity for AMI although most markers had high specificity (around 90%) Serial measurements greatly increased the sensitivity for AMI and maintained excellent specificity: biomarkers cannot identify most cases of unstable angina. ACI-TIPI did not use Sens./Spec. Presentation Myoglobin had Sens 49/ Spec 91; serial Myoglobin had 89/87 within Class B(some bias) studies.Likewise TnT/I at presenation had 39/93; serial tests yielded 93/85 respectively.
Level of Evidence 3a
Quality of Evidence Good
Neutral
Limkakeng(01)Limkakeng, A., Jr., W. B. Gibler, et al. (2001). "Combination of goldman risk and initial cardiac troponin I for emergency department chest pain patient risk stratification." Academic Emergency Medicine 8(7): 696-702.
Background: Accurate identification of low-risk emergency department (ED) chest pain patients who may be safe for discharge has not been well defined. Goldman criteria have reliably riskstratified patients but have not identified any subset safe for ED release. Cardiac troponin I (cTnI) values have also been shown to risk-stratify patients but have not identified a subset safe for ED release. Objective: To test the hypothesis that ED chest pain patients with a Goldman risk of <=4% and a single negative cTnI (<=0.3 ng/mL) at the time of ED presentation would be safe for discharge [<1% risk for death, acute myocardial infarction (AMI), revascularization]. Methods: A prospective cohort study was performed in which consecutive ED chest pain patients were enrolled from July 1999 to November 2000. Data collected included patient demographics, medical and cardiac history, electrocardiogram, and creatine kinase-MB and cTnI. Goldman risk stratification score was calculated while patients were still in the ED. Hospital course was followed daily. Telephone follow-up occurred at 30 days. The main outcome was death, AMI, or revascularization (percutaneous transluminal coronary angioplasty/stents/coronary artery bypass grafting) within 30 days. Results: Of 2,322 patients evaluated, 998 had both a Goldman risk <=4% and a cTnI <=0.3 ng/mL. During the initial hospitalization, 37 patients met the composite endpoint (3.7%): 6 deaths (0.7%), 17 AMIs (1.7%), 18 revascularizations (1.8%). Between the time of hospital discharge and 30-day follow-up, 15 patients met the composite endpoint: 4 deaths (0.4%), 6 AMIs (0.6%), and 5 revascularizations (0.5%). Overall, 49 patients met the composite endpoint (4.9%; 95% CI = 3.6% to 6.2%): 10 deaths (1.0%; 95% CI = 0.4% to 1.6%); 23 AMIs (2.3%; 95% CI = 1.4% to 3.2%), and 23 revascularizations (2.3%; 95% CI = 1.4% to 3.2%) within 30 days of presentation. Conclusions: The combination of two risk stratification modalities for ED chest pain patients (Goldman risk <=4% and cTnI <=0.3 ng/mL) did not identify a subgroup of chest pain patients at <1% risk for death, AMI, or revascularization within 30 days.
This group out of Philadelphia and other centers carried out a prospective trial utilizing the Goldman risk score. They looked at outcome of 998 patients with a Goldman risk score of less than equal to 4, i.e. very low and initial TnT troponin I less than or equal to .3 ng per milliliter. They were able to follow 90% of these patients at 30 days and their end point was death, AMI or revascularization.AMI defined as elevated CK MB.Median duration of symptoms 4 hours prior to presentation. Of note they had a large (71%) black population who are more prone to hypertension, diabetes, and therefore have a higher prevalence of coronary artery disease. Note they also did not exclude any patients who confessed cocaine abuse. Analysis showed when both of the criteria were applied there was 71% sensitivity , 72% specificity, a PPV of 19.3 and NPV of 96.5 for values greater than 0.3 ng per milliliter or Goldman score greater than 4%.Not acceptable for clinical use .

document.doc Page 37 of 77
Level of Recommendation 1b
Quality of Evidence Good
Opposing
Liu(99)Liu, T., Q. Wang, et al. (1999). "Development of a statistical model for prediction of acute myocardial infarction by biochemical markers." Drug Information Journal 33(1): 141-148.
Diagnosis and management of potential acute myocardial infarction (AMI) patients presenting to the hospital emergency department (ED) with chest pain are difficult. To aid in clinical decision making, a multivariate logistic regression model was developed using the patient's presenting history, electrocardiogram (ECG), and biochemical marker (cardiac Troponin T, cTnT) to predict the probability of AMI. Data from 102 AMI and 619 non-AMI patients from a multicenter clinical trial were used for model building. The World Health Organization criteria were used for AMI diagnosis. Univariate analyses were performed to assess the effect of individual factors. Based on the significance of univariate effect and clinical importance, the following variables were included in a risk factor only model: age, sex, chest pain, systolic blood pressure, smoking, and history of myocardial infarction and hypertension with an area under the receiver operating characteristic (ROC) curve (AUC) of 0.66 (95% confidence interval [CI]: 0.60-0.71) and an R2 of 0.09. The final model, which included the risk factors and results of ECG and cTnT, increased the AUC and R2 values to 0.93 (95% CI: 0.90-0.96) and 0.83, respectively. At the probability level of 0.10 for AMI, the model showed a sensitivity of 78.4% and a specificity of 92.6%. Statistical modeling is a useful tool in predicting risk of chest pain patients in the ED.
Interesting but not validated. No mention of WHEN assay(s?) were done
Quality of Evidence 4
Quality of Evidence Fair
Neutral
Maisel(00)Maisel, A. S., K. Templin, et al. (2000). "A prospective study of an algorithm using cardiac troponin I and myoglobin as adjuncts in the diagnosis of acute myocardial infarction and intermediate coronary syndromes in a veteran's hospital." Clinical Cardiology 23(12): 915-20.
BACKGROUND: Accurate and cost-effective evaluation of acute chest pain has been problematic for years. The high prevalence of missed myocardial infarctions (MI) has led to conservative triage behavior on the part of physicians, leading to expensive admissions to coronary care units. New algorithms are sorely needed for more rapid and accurate triage of patients with chest pain to appropriate treatment settings. HYPOTHESIS: We sought to test an algorithm for rapid diagnosis of MI and acute coronary syndromes using cardiac troponin I (cTnI) and myoglobin as adjuncts to creatine kinase (CK)-MB. We hypothesized our algorithm would be both sensitive and specific at early time points, and would allow safe stratification of patients not ruling in by conventional CK-MB criteria. METHODS: This was a 6-month prospective study of 505 consecutive patients who presented with chest pain at a university-affiliated veteran's hospital. The percentage of MIs at various time points was identified using combinations of markers. Safety outcomes were assessed by follow-up of patients discharged home. Cost savings analysis was assessed by surveying the physicians as to whether the use of the algorithm affected their disposition of patients. Forty-nine patients ruled in for MI. Using the combination of cTnI, 2-h doubling of myoglobin, and CK-MB, 37 (76%) ruled in at the time of presentation, 43 (88%) at 2 h, and 100% by 6 h. RESULTS: Cardiac troponin I plus a 2-h myoglobin was as accurate as the combination of all three markers and performed better than CK-MB in detecting patients presenting late and as a predictor for complications when CK-MB was normal. Of the 456 patients with normal markers after 6 h, only 140 were sent to the coronary care unit (CCU), and 176 were sent home. A 3-month follow-up showed minimal adverse events. One-half of physicians completing a survey stated the use of markers changed their disposition of patients, leading to an estimated 6-month cost savings of a half-million dollars. CONCLUSIONS: We developed an algorithm using troponin I and myoglobin as adjuncts to usual CK-MB levels that allowed for rapid and accurate assessment of patients with acute MI. It also afforded physicians important input into their decision making as to how best to

document.doc Page 38 of 77
triage patients presenting with chest pain. Their comfort in sending home certain subgroups of patients who otherwise would have been admitted to the CCU was rewarded with a good short-term prognosis and a large cost savings to the hospital.
This study looked at triple assays at 0 to 6 and 12 hours in a Veteran’s Affairs medical center (therefore high population of men). The AMI prevalence was 10% based on WHO criteria or elevated TnI or, for the late presenters, positive ECHOs. 62% of the population presented with duration of pain less than 12 hours and 38% > 12 hours; no median time was available. Assay was the Opus Plus analyzer. Threshold levels were not disclosed. 505 patients were entered. A complex algorithm was followed with decision points upon entry, at 2 hours, then based on the change in myoglobin at 6 and 12 hours. Results: Only AMI was looked at( TnI>1.5ng/ml or CKMB.>9ng/ml or new LV dysfn on ECHO?!). The accuracy of markers at presentation showed troponin I sensitivity 76%, specificity 98%, PPV 79 and NPV 97; for CK-MB 49,100, 100, 94; no absolute value of presentation myoglobin was considered as positive. At 2 hours myoglobin doubling was 50, 100, 86 and 99; troponin I and myoglobin doubling was 88/ 98; 81 /99; CK-MB and myoglobin doubling was 60/ 100 /100 and 94 respectively (95% confidence intervals were included) Of 455 patients ruled out for AMI 186 were sent home. 3-month follow-up with 90% response rate revealed only one non Q-wave MI. They reason that the 50% sensitivity of myoglobin was because they only looked at doubling of levels at 2 hours. In no cases in which myoglobin doubled after 2 hours did the patient not subsequently prove to have an MI by CK-MB and or troponin I values. Thus the specificity and positive predictive value of a 2 hour doubling of myoglobin in the present study was 100%. No falsely elevated myoglobin levels were seen since no skeletal muscle injury, trauma or burns were described. If the initial myoglobin was normal and the patient presenting within 4 to 6 hours of chest pain, the lack of doubling of myoglobin ruled out MI 100% of the time. There is no comment as to unstable angina.The 3 month follow had very loosely defined end points and very few.
This study claims 100% Sens/98Spec for AMI at 6 hrs; caveats are 40% of patients presented >12 hrs pain,and I have trouble with their AMI reference standards re incorporation bias and significance of new LV dysfn.
Level of Evidence 1cQuality of Evidence GoodSupportive
Mathew(99)Mathew, T., I. Menown, et al. (1999). "Diagnosis and risk stratification of patients with anginal pain and non-diagnostic electrocardiograms." Qjm 92(10): 565-71.
Patients with acute chest pain suggestive of myocardial ischaemia, and normal or non-diagnostic electrocardiograms, form a difficult subgroup for diagnosis and early risk stratification. We prospectively evaluated the role of troponin T (cTnT), troponin I (cTnI), CKMB mass and myoglobin, in the diagnosis and risk stratification of 214 patients with acute chest pain of < or = 24 h and non-diagnostic or normal ECGs admitted directly to the Cardiac Unit of the Royal Victoria Hospital Belfast from the Mobile Coronary Care Unit or the Accident/Emergency Department. This was a single-centre prospective study, and follow-up (3 months) was complete for all patients. Blood was assessed for quantitative cTnT, cTnI, CKMB mass and myoglobin, and qualitative cTnT on admission and at 12 h. Diagnosis of index event and incidence of new cardiac events (death, non-fatal myocardial infarction, revascularization, or readmission for unstable angina) over 3 months were assessed. Based on standard criteria, myocardial infarction occurred in 37/214 (17%), and unstable angina in 72/214 (34%). At 12 h from admission, cardiac troponins had higher sensitivity for the diagnosis of acute coronary syndromes (myocardial infarction and unstable angina) than conventional markers (cTnI 48%, cTnT 38%, CKMB mass 30% or myoglobin 27%). At 3 months, a new cardiac event had occurred in 42/214 (20%). Significantly higher event rates occurred when any of the biochemical markers was elevated, but the statistical significance was highest for patients with elevated cTnI (p < 0.0001). Whilst gender, history of ischaemic heart disease (IHD), stress test response, cTnT, cTnI, CKMB mass and myoglobin were univariate predictors, cTnI at 12 h and stress test response were the only two independent significant predictors for a subsequent cardiac event at 3 months. Raised cTnI at 12 h after admission had the

document.doc Page 39 of 77
highest sensitivity for the diagnosis of acute coronary syndromes, and was independently associated with a 2-3 times increased risk of future cardiac events within 3 months among patients with acute chest pain suggestive of myocardial ischaemia but with normal or non-diagnostic ECGs.
This study out of Belfast looked at 0 and 12 hour multiple biomarker assays. The typical inclusion and exclusion existed. Troponin T qualitative assays had a cutoff of 01 micrograms per liter, troponin T quantitative assays had the same cutoff, Troponin I had a cutoff of 1.0 micrograms per liter CK-MB mass > or = 13 micrograms per liter and myoglogin > 92 micrograms per liter. These were assayed at time 0 and 12 h ours. Of note, all patients were admitted; unless classic EKG manifestations evolved all patients had either stress testing and or coronary angiography to rule in or out AMI/UA. The median time for onset of symptoms to presentation was 6.6 hours. 37 out of 214 patients were diagnosed as AMI within 72 hours of admission, 72 patients were diagnosed with unstable angina. Quite interesting and puzzling are the O hours sensitivities :TnT qualitative was 12%, TnI 17%, TnT quantitative 15%, CK-MB mass 7 and myoglobin 20. None were acceptable for AMI or UA. These improved with the 12-hour assays. Specificities were not given. Follow-ups for 3 month cardiac events showed no data of significance related to 0 hr. assays.
This is one of few studies that looked at stress tests(gold standard for UA) and correlated it to ED biomarkers; unfortunately only initial levels are pertinent to my statement.
Level of Evidence 1b
Quality of Evidence Good
Opposing
McCord(03) McCord, J., R. M. Nowak, et al. (2003). "The prognostic significance of serial myoglobin, troponin I, and creatine kinase-MB measurements in patients evaluated in the emergency department for acute coronary syndrome." Annals of Emergency Medicine 42(3): 343-50.
STUDY OBJECTIVE: We sought to determine the value of serial measurements of myoglobin, cardiac troponin I (cTnI), and creatine kinase-MB (CK-MB) to predict 30-day adverse events in patients evaluated in the emergency department (ED) for possible acute coronary syndrome. METHODS: Serum myoglobin, cTnI, and CK-MB levels were measured at presentation, 90 minutes, 3 hours, and 9 hours in patients evaluated in the ED for possible acute coronary syndrome. In 764 consecutive patients, the ability of each individual marker and combination of markers to predict a 30-day adverse event (death or myocardial infarction) over time was calculated. RESULTS: There were 109 (14%) patients with an adverse event at 30 days (84 myocardial infarctions and 43 deaths). The sensitivities of initial measurements of myoglobin, cTnI, and CK-MB for identifying adverse events were 60%, 47%, and 52%, respectively. The combined sensitivity of myoglobin and cTnI measurements during a 9-hour period was 94%; specificity was 50%. Measurement of CK-MB did not improve sensitivity. CONCLUSION: The measurement of both myoglobin and cTnI during a 9-hour period was the most predictive of subsequent adverse events in patients evaluated in the ED for possible acute coronary syndrome.
This study out of Henry Ford Hospital looked at triple marker assay i.e. myoglobin, troponin I and CK-MB values at 0 minutes, 90 minutes, 3 hours and 9 hours after presentation. This was a very large Afro American population, 764 patients were included. Those with ST segment elevation EKGs or hemodynamic instability had been excluded.Median times were 4.2 hrs symptoms to presentation.
The results of outcome at 30 days of all cause death at 9 hours was 94 % sensitivity and a specificity of 50% using myoglobin and troponin I. They found that CK-MB did not improve the sensitivity.
They do provide a table for 3 hour assay -highest sensitivity for adverse effects was combination of troponin I and myoglobin with 89% sensitivity and 55.3% specificity and they found CK-MB had the highest PPV of 36.2 and a combination of troponin/myoglobin NPV of 97 at 3 hours.
Level of Evidence 1b
document.doc Page 40 of 77
Quality of Evidence Good
Supportive
McCord(01) McCord, J., R. M. Nowak, et al. (2001). "Ninety-minute exclusion of acute myocardial infarction by use of quantitative point-of-care testing of myoglobin and troponin I." Circulation 104(13): 1483-1488.
Background - Diagnostic strategies with ECG and serum cardiac markers have been used to rule out acute myocardial infarction in 6 to 12 hours. The present study evaluated whether a multimarker strategy that used point-of-care measurement of myoglobin, creatine kinase (CK)-MB, and troponin I could exclude acute myocardial infarction in <=3 hours. Methods and Results - We prospectively enrolled consecutive patients (n=817) in the emergency department who were evaluated for possible acute myocardial infarction. In patients with nondiagnostic ECGs, we measured CK-MB, troponin I, and myoglobin with a point-of-care device at presentation and at 90 minutes, 3 hours, and 9 hours. Standard central laboratory testing of CK-MB was done at the same time intervals, and triage decisions were made by emergency physicians who were unaware of point-of-care results. Sensitivity and negative predictive value were compared for both the multimarker, point-of-care approach and the central laboratory strategy. Sensitivity and negative predictive value for point-of-care combination of myoglobin and troponin I by 90 minutes was 96.9% and 99.6%, respectively. CK-MB measurements and blood sampling at 3 hours did not improve sensitivity or negative predictive value. Median time from sampling to reporting of results was 71.0 minutes for the central laboratory versus 24.0 minutes for the point-of-care device (P<0.001). Conclusions - Acute myocardial infarction can be excluded rapidly in the emergency department by use of point-of-care measurements of myoglobin and troponin I during the first 90 minutes after presentation.
Setting was Henry Ford Hospital and therefore high Afro-American population with a high prevalence of cardiovascular disease. 1024 consecutive encounters were evaluated, 116 were discharged home before the full 9-hour assessment. (1 cardiac death occurring in the next 30 days) thus 817 patients were entered. CK-MB range was > 9 nanograms per milliliter and was the diagnosis for AMI plus agreement between two blinded cardiologists. Assays were the AxSYM analyzer with reference levels CK 0.75, myoglobin 2.70 and troponinI 0.19 nanograms per liter respectively. Of note a full 25% of patients had chronic renal insuffientancy( myoglobin specificity being 35% for the high creatinine group yet 89% for patients with normal creatinines). Median time from symptom onset to presentation was 4.3 hours. ROC curves analysis allowed retrospective assignment of cutoff values. For AMI 90 min Myo/TnI Sens 96.9%/spec 59.7%; little change at 3 hrs.
Sensitivities for assay at times 0 for myoglobin 70.8, CK-MB 75.4, troponin I was 64.6, combination myoglobin/ CK-MB 83.1 and myoglobin/ troponin I 84.6; specificity 75.6 84.7 87.6 70.2 and 66.8 respectively.
At 90 minutes sensitivities were 84.6, 83.1, 76.9, 92.3 and 96.9 respectively; specificity 73, 83, 79, 67.5 and 59.7 respectively. There is no statistically significant difference at 3 hours.
ROC curves used retrospectively define threshold levels.
Level of Evidence 7
Quality of Evidence Good
Supportive
Morris(00) Morris, S. A., D. Helmer, et al. (2000). "Clinical utility of CKMB isoform determinations in patients who present to the emergency department with continuous or resolved chest pain." Journal of Emergency Medicine 19(1): 21-6.
The object of this investigation was to demonstrate that the enhanced sensitivity of the diagnosis of acute myocardial infarction (AMI) using a more-inclusive criterion of CKMB Isoforms may detect earlier stages of AMI (designated Isoform Type 2) than the currently accepted marker for AMI by
document.doc Page 41 of 77
CKMB Isoform (designated Isoform Type 1) in a busy, urban Emergency Department (ED). Two features characterized the study of CKMB Isoforms in a prospective cohort of 223 ED patients: first, nontraumatic chest pain within 12 h before presentation, thought to be of ischemic etiology; and second, normal or nondiagnostic electrocardiogram (EKG). Patients were further divided into two groups characterized as either recent but resolved chest pain at ED visit, or ongoing or staccato chest pain. Sensitivity (S), specificity (SP), positive (PPV) and negative (NPV) predictive values, and 95% confidence intervals (CI) for AMI diagnosis were determined. Two criteria for AMI diagnosis by CKMB Isoforms were tested. The first and currently recommended criterion was identified as Isoform Type 1. An AMI diagnosis by Type 1 criterion requires both CKMB2> or =2.6 IU/L and CKMB2/CKMB1> or =1.7. The second criterion for AMI diagnosis was identified as Isoform Type 2, which is defined as either CKMB2> or =2.6 IU/L or CKMB2/CKMB1> or =1.7. Both Isoform types are predictive of AMI by the gold standard, and addition of EKG changes results in a small improvement. Type 1 demonstrates SP 0.94 (CI 0.90, 0.97) and NPV 0.90 (CI 0.86, 0.94), and Type 2 demonstrates S 0.90 (CI 0.80, 0.97) and NPV 0.97 (CI 0.93, 0.99) for AMI diagnosis. Type 2 criteria can confidently exclude the immediate risk of AMI in patients with resolved chest pain whereas in patients with continuous chest pain, Type 1 criteria may identify those at high risk for AMI.
This study looked at non-consecutive patients enrolled with chest pain and non STEMI EKGs. They further sub divided the group into resolved chest pain or continuing chest pain. Assays were drawn within 30 minutes of presentation. There is no discussion as to duration prior to presentation. The Gold standard was CK-MB activity > 15 international units per liter. AMI rate was 16%. Sensitivities and specificities were tabled for both the resolved chest pain group and the continuous chest pain group.
Major concern is the close relationship the 2 CK-MB isoforms with the gold standard reference for AMI. Type 2 isoform showed Sens 90% for AMI.
Level of Evidence 4
Quality of Evidence Good
Supportive
Morrow(01) Morrow, D. A., N. Rifai, et al. (1998). "C-reactive protein is a potent predictor of mortality independently of and in combination with troponin T in acute coronary syndromes: a TIMI 11A substudy. Thrombolysis in Myocardial Infarction." J Am Coll Cardiol 31(7): 1460-5.
OBJECTIVES: We evaluated C-reactive protein (CRP) alone and in conjunction with a rapid qualitative assay for cardiac-specific troponin T (cTnT) for predicting 14-day mortality in patients with unstable angina or non-Q wave myocardial infarction (NQMI). BACKGROUND: Elevated CRP has been found to correlate with higher risk for cardiac events in patients with coronary disease. METHODS: At enrollment into the Thrombolysis in Myocardial Infarction (TIMI) 11A trial, a dose-ranging trial of enoxaparin for unstable angina and NQMI, serum was obtained for CRP measurement and rapid cTnT assay. RESULTS: Quantitative CRP and rapid cTnT assays were performed in all patients. CRP was higher among patients who died than in survivors (7.2 vs. 13 mg/dl, p = 0.0038). The probability of a positive rapid cTnT assay rose with increasing CRP concentration (p < 0.0001). Among patients with a negative rapid cTnT assay, the mortality rate was higher among patients with CRP > or = 1.55 mg/dl (5.80% vs. 0.36%, p = 0.006). Patients with both an early positive rapid cTnT assay (< or = 10 min until assay positive) and CRP > or = 1.55 mg/dl had the highest mortality, followed by those with either CRP > or = 1.55 mg/dl or an early positive rapid cTnT assay, whereas patients with both a negative rapid cTnT assay and CRP < 1.55 mg/dl were at very low risk (9.10% vs. 4.65% vs. 0.36%, p = 0.0003). CONCLUSIONS: Elevated CRP at presentation in patients with unstable angina or NQMI is correlated with increased 14-day mortality, even in patients with a negative rapid cTnT assay. Quantitative CRP and a rapid cTnT assay provide complementary information for stratifying patients with regard to mortality risk.This substudy looked at the TIMI 11A trial - patients presenting with at least 6 hours after onset of chest pain diagnosed with unstable angina or non-Q wave infarct. Those with less than 6 hours of symptoms were excluded. They compared troponin T assay (drawn>6 hrs after symptom onset….vague!) to C-reactive protein assay for mortality at 14 days. The bedside assay used was

document.doc Page 42 of 77
qualitative in nature and positive results were read both with the intensity of the color change as well off the speed of which it developed.This assay had been previously studied where positivity before 10 minutes of elapsed time confirmed ACS. 437 patients were enrolled, 346 had a negative test, 43 were positive early, the rest(48) were positive later. When mortality was looked at 14 days post admission, they found a sensitivity of 29%, a specificity of 91 and +likelihood ratio of 3 for the troponin T assay.
Not sure of timing of sampling; unable to confirm.
Level of Evidence 2bQuality of Evidence FairOpposing
Newman(99)Newman, J., N. Aulick, et al. (1999). "Prehospital identification of acute coronary ischemia using a troponin T rapid assay." Prehospital Emergency Care 3(2): 97-101.
OBJECTIVE: To evaluate the performance of a rapid assay for cardiac troponin T (cTn-T) in patients with chest pain in the prehospital setting. METHODS: A prospective, observational clinical trial in a rural county served by a single emergency medical services system and two emergency departments. Patients fulfilling prehospital criteria to identify acute coronary ischemia (ACI) had a blood sample applied to the cTn-T rapid-assay device. Quantitative analysis of cTn-T was also performed on each sample at a later time. Medical records were reviewed to determine ultimate diagnoses. Non-admitted patients were followed by telephone at one week. Main outcome measures included the sensitivity, specificity, positive predictive value, and negative predictive value of the rapid cTn-T assay for detecting ACI defined as acute myocardial infarction (AMI) or unstable angina (UA) within one week of presentation. RESULTS: Of 87 patients enrolled, 29 were identified with ACI. This included 15 patients diagnosed as having AMI and 14 patients diagnosed as having UA. The cTn-T rapid-assay device was positive for five of 87 patients (5.7%); three were associated with AMI and two with UA. Measurement of a single cTn-T to detect ACI had a sensitivity of 17.2% (0.058, 0.358), specificity of 100% (0.950, 1), positive predictive value of 100% (0.549, 1), and negative predictive value of 70.7% (0.609, 0.806). CONCLUSION: The cTn-T rapid-assay device may be useful in the prehospital setting to identify a small number of patients with ACI. The authors caution, however, that a negative test in the prehospital setting cannot be used to rule out significant disease.
This is small study of prehospital assessment of troponin T rapid assay compared to in-hospital assessment assay;follow up was 1 week, there was no comment to the interval between the onset of symptoms and the assay time. ACS diagnosis was not defined but thought to be an in hospital TnT value >0.1 ng/ml. Sensitivity was found to be 17.2% (0.058, 0.358) with a specificity of 100% for acute coronary insufficiency (ACI) the assay was colorimetric with a cutoff of 0.18 ng per milliliter.
Level of Evidence 4Quality of Evidence FairOpposing
Ng(01:1) Ng, S. M., P. Krishnaswamy, et al. (2001). "Ninety-minute accelerated critical pathway for chest pain evaluation." American Journal of Cardiology 88(6): 611-7.
Rapid, efficient, and accurate evaluation of chest pain patients in the emergency department optimizes patient care from public health, economic, and liability perspectives. To evaluate the performance of an accelerated critical pathway for patients with suspected coronary ischemia that utilizes clinical history, electrocardiographic findings, and triple cardiac marker testing (cardiac troponin I [cTnI], myoglobin, and creatine kinase-MB [CK-MB]), we performed an observational study of a chest pain critical pathway in the setting of a large Emergency Department at the Veterans Affairs Medical Center in 1,285 consecutive patients with signs and symptoms of cardiac ischemia. The accelerated critical pathway for chest pain evaluation was analyzed for: (1) accuracy in triaging of patients within 90 minutes of presentation, (2) sensitivity, specificity, positive predictive value, and negative predictive value of cTnI, myoglobin, and CK-MB in diagnosing acute

document.doc Page 43 of 77
myocardial infarction (MI) within 90 minutes, and (3) impact on Coronary Care Unit (CCU) admissions. All MIs were diagnosed within 90 minutes of presentation (sensitivity 100%, specificity 94%, positive predictive value 47%, negative predictive value 100%). CCU admissions decreased by 40%. Ninety percent of patients with negative cardiac markers and a negative electrocardiogram at 90 minutes were discharged home with 1 patient returning with an MI (0.2%) within the next 30 days. Thus, a simple, inexpensive, yet aggressive critical pathway that utilizes high-risk features from clinical history, electrocardiographic changes, and rapid point-of-care testing of 3 cardiac markers allows for accurate triaging of chest pain patients within 90 minutes of presenting to the emergency department.
This study looked at 90-minute assay per myoglogin, CK-MB and troponin I and a diagnosis of AMI.However clinicians could order 3 and 6 hr levels if necessary. It did not look at unstable angina. It was a one-center trial from a Veteran’s Affair Hospital and therefore predominately male population only. It looked at a change in myoglobin of 25% during this time period(previously substantiated) or an absolute value of greater than 150 ng per milliliter if the chest pain was less than 6 hours, a sustained elevation in troponin I greater than 0.4 ng per milliliter and or sustained elevation in CK-MB greater than .6 ng per milliliter. It used WHO criteria for outcome confirmation of AMI however it used a 6 hour level only and only with further suspicions by the clinician would a 12 hour panel be drawn. Thus the Gold standard was inconsistent.
Over 50% of patients presented with duration of pain greater than 6 hours. This is an unusual long length of duration of time and would influence the values of myoglobin and troponin as well as CK-MB.
They came to the conclusion the triple assay at 90 minutes was 100% sensitive and 94% specific to rule in AMI. Of note follow up revealed 2.5% AE rate.? Spurious elevated TnI values.
Level of Evidence 4
Quality of Evidence Fair
Supportive
Ng(01:2)Ng, S. M., P. Krishnaswamy, et al. (2001). "Mitigation of the clinical significance of spurious elevations of cardiac troponin I in settings of coronary ischemia using serial testing of multiple cardiac markers." American Journal of Cardiology 87(8): 994-9; A4.
The ability to differentiate between true positives, false positives, and sporadically elevated cardiac troponin levels has grown in importance as cardiac troponins assume an increasingly dominant role in the diagnosis of coronary syndromes. In a population sample of 1,000 patients who presented consecutively to a large urban hospital emergency room, 50 of 112 patients who had elevated troponin levels (> 0.6 ng/ml) during evaluation for myocardial injury were subsequently found to have had an isolated, spurious elevation of cardiac troponin, and not a diagnosed myocardial infarction. Logistic regression analysis shows that by hierarchically analyzing electrocardiographic changes with concurrent creating kinase-MB and myoglobin levels at the time of the troponin elevation, one may predict with 91% accuracy whether the troponin elevation is actually indicative of a myocardial infarction in a patient. Spurious troponin elevations may be a common occurrence, and if not detected, may result in an increased number of falsely diagnosed myocardial infarctions.
This study was a retrospective study using a population of a previous study carried out by the author (setting VA hospital, large male pop). They looked at 1,000 patients worked up for coronary ischemia. These patients had triple enzyme assay by point of care Triage Cardiac System (Biosite Diagnostic); troponins> 1 nanogram per milliliter were diagnostic of MI, those between 0.6 and 1.0 nanograms per milliiter were diagnosed as minor cardiac ischemia. All of these patients were subsequently worked up by radionuclide imaging and/ or coronary angiography. 111 patients were found to be positive for troponin I in at least one assay but only 61 on further workup were found to have coronary disease; 15 patients had no positive studies further and ultimately diagnosed as negative for myocardial injury. The average troponin elevation for MIs was 7.24 nanograms per milliliter whereas those for the “spurious” troponin I elevation was 0.97 nanograms per liter. They then mentioned by logistic regression analysis that they have 91%

document.doc Page 44 of 77
accuracy in picking up these spurious results by monitoring electrocardiographic findings. Though these results are only pertinent to this specific assay utilized in this specific population, I find it applicable to my hypothesis.
Level of Evidence 7Quality of Evidence GoodOpposed
Ooi, S(00)Ooi, S. B., Y. T. Lim, et al. (2000). "Value of troponin-T rapid assay, cardiac enzymes, electrocardiogram and history of chest pain in the initial diagnosis of myocardial infarction in the emergency department." European Journal of Emergency Medicine 7(2): 91-8.
We conducted a prospective study of 152 adult patients presenting to an emergency department with chest pain or symptoms suggestive of acute myocardial infarction (AMI) to evaluate the first electrocardiogram (ECG), creatine kinase (CK)-MB and Troponin-T Rapid Assay (TnT) alone or in combination with chest pain in the initial diagnosis of AMI. A provisional diagnosis was made after the history, physical examination and the first ECG reading. Blood specimens were taken for TnT, CK and CK-MB mass. A final discharge diagnosis of AMI was made according to World Health Organization criteria. Seventy-six (50%) of patients had a final diagnosis of AMI. The sensitivities of the first ECG, first CK-MB mass and first TnT were 76.3% (95% confidence interval (CI), 66.8-85.9), 38.2% (95% CI, 27.2-49.1) and 31.6% (95% CI, 21.2-42.0) respectively. The area under the curve for a combination of ECG, CK-MB mass, TnT and chest pain was the highest at 0.937 when compared with chest pain with varying combinations of tests. A combination of the first ECG, CK-MB mass and TnT had a negative predictive value (NPV) of 87.9% (95% CI, 80.0-95.8). The first ECG was the most sensitive test while the combination of chest pain, ECG, cardiac enzymes and TnT gave the best results in the initial diagnosis of AMI. If the first ECG, CK-MB mass and TnT are all negative, the probability of having an AMI is 12%.
This study out of Singapore was a prospective one looking at 152 patients presenting to the ED. They looked at a presentation CK-MB and a qualitative troponin T rapid assay. (Trop-T, Borehringer Mannhein); the inclusion criteria were traditional except pts with EKG changes were retained. Troponin assay was positive for a concentration greater than 0.2 mg per milliliter. The CK-MB mass was positive for greater than 6 ng per milliliter and a relative percentage > than 5%. The median duration of chest pain prior to presentation was 3 hours with a range of 15 minutes to 720 hours. Interestingly 148 patients were admitted to the hospital because of no emergency/observation unit capacity. They found for myocardial infarction a TnT sensitivity of 31.6 (21.2 – 42.0) with a specificity of 100% (95.3 - 100); CK-MB sensitivity was 38.2 (27.2 - 49.1) and specificity of 97.4 (93.8 - 100). If any test including EKG was positive, still Sens was only 89.4%; my cutoff for clinically applicable test for AMI is Sens>95%.The follow up was 1 week with a repeat EKG and a troponin assay. AMI was based on WHO criteria.
Level of Evidence 1bQuality of Evidence FairOpposing
Peacock(03) Peacock, W. F., C. E. Emerman, et al. (2003). "Retrospective review: the incidence of non-ST segment elevation MI in emergency department patients presenting with decompensated heart failure." Congestive Heart Failure 9(6): 303-8.
The authors performed a 6-month review of heart failure patients presenting to a teaching hospital emergency department to determine the rate of positive serum myocardial infarction markers. All patients with an emergency department discharge diagnosis of heart failure were included; those with a creatinine level >2.0 mg/dL were excluded. There were 151 patients who met the entry criteria, with a mean age of 68.6 +/- 13.6 years, and 84 (56%) were men. The mean ejection fraction was 32%, and the mean Framingham score was 3.8 +/- 1.6. Twenty (14%) had positive markers. Troponin T was positive in 17 (11%), and creatine kinase was positive in nine (6%). Both markers were positive in six (4%). Chest pain was absent in 70% of the positive marker group. The authors conclude that elevated cardiac markers are not rare in decompensated heart failure. These pilot data suggest these tests should be routinely obtained on heart failure patients.

document.doc Page 45 of 77
This was a retrospective review of patients diagnosed with heart failure in one urban centre. They then looked at which patients had had elevated CK MB assays i.e. > 8.8 nanograms per liter or troponin T > 0.1 ug per liter. These levels were diagnostic for MI. They found 11% positive for TnT and 6% for CK MB, however, serial assays had not been routinely ordered. Also, they had not looked at CHF patients with elevated troponins being diagnosed as acute AMI and therefore missed.They did not consider raised enzymes being from a non ischemic nature. Though they did not look formally at follow up, there were an insignificant increased proportion of cardiac marker positive patients that returned between 1 week and 30 days.
Level of Evidence 5Quality of Evidence-PoorSupportive
Penttila(02).Penttila, K., H. Koukkunen, et al. (2002). "Myoglobin, creatine kinase MB isoforms and creatine kinase MB mass in early diagnosis of myocardial infarction in patients with acute chest pain." Clinical Biochemistry 35(8): 647-653.
Objectives: Measurements of myoglobin and creatine kinase (CK)-MB isoforms have been suggested to be sensitive tests for the early diagnosis of myocardial infarction (MI). We have investigated the utility of myoglobin, creatine kinase (CK)-MB isoforms and creatine kinase MB mass (CK-MBm) in early diagnosis of MI using cardiac troponin T (cTnT) positivity as a reference. Design and methods: The study population comprised 440 patients who had had chest pain for less than 12 h. Patients were divided into cTnT negative (cTnT-) or cTnT positive (cTnT+) patients (concentration of cTnT >0.1 [mu]g/L at two different time points during 72 h). Results: At the time of admission to the emergency department receiver operating characteristics (ROC) curves of CK-MB isoforms and CK-MBm were not better than that of myoglobin. Six hours after admission CK-MB isoforms and CK-MBm provided statistically significantly larger areas under the curve (AUC) than myoglobin (p < 0.01). When ROC curves were related to the onset of chest pain (< 3 h, 3-6 h, and > 6 h) there were no significant differences between the cardiac markers studied. Conclusions: According to the present findings, CK-MB isoforms or myoglobin offer no advantage over CK-MBm as early markers of myocardial infarction. (C) 2002 The Canadian Society of Clinical Chemists. All rights reserved.
This study out of Finland looked at 440 consecutive with chest pain under 12-hour duration. It compared myoglobin, CK-MB isoforms and CK-MB mass in relation to the gold standard tropoonin T level (within 72 hours)(ESC/ACC guidelines); samples were drawn at 0, 2, 4 and 6 hours. Clinicians were blinded to the results. ROC curves were analyzed for optimal assay thresholds for AMI. Upper reference levels for CK activity 270 ug per L for men, 170 ug per L for women,; CK-MB activity .5 u/L; myoglobin 65 micrograms per liter for men and 55 micrograms per liter for women; CK-MB isoforms, MB2/MB ratio 1.7 and MB 2.5 ug/L; CK-MB mass 5.0 micrograms per liter; TnT 0.1 micrograms per liter. All analytical coefficients of variation were < 10%.
Results of the 440 patients: 29.5% were positive for AMI- this is a very high rate compared to traditional WHO assays, however the troponin values are much more sensitive and the threshold level ?captured UA cases.
At admission myoglobin was the most sensitive of the markers (p value < 0.001) CK-MB isoforms were not more sensitive than CK-MB mass. At 6 hours post admission CK-MB mass and CK-MB isoforms performed better than myoglobin. At times < 6 hours post onset of pain myoglobin was the most sensitive marker; after 6 hours of onset of pain CK-MB isoforms and myoglobin were more sensitive than CK-MB mass. The specificities of myoglobin were lowest at all times. Thus CK-MB isoform measurement did not produce any additional benefit compared to CK-MB mass measurement in the early diagnosis of MI.
Level of Evidence 7
Quality of Evidence Good
Opposing
Polanczyk(99)
document.doc Page 46 of 77
Polanczyk, C. A., T. H. Lee, et al. (1999). "Value of additional two-hour myoglobin for the diagnosis of myocardial infarction in the emergency department." American Journal of Cardiology 83(4): 525-9.
Myoglobin has been described as an early marker of myocardial injury. It increases within 1 to 3 hours of myocardial injury, and falls back to normal early after the event. Few data suggest that myoglobin can be used to triage patients with chest pain. To assess the diagnostic utility of second myoglobin levels drawn within 2 to 3 hours after presentation to the emergency department for detecting myocardial infarction, we prospectively collected myoglobin levels in 368 patients aged > or = 30 years who were admitted with chest pain. Myoglobin levels were measured at admission and 2 to 3 hours later. Sensitivity and specificity for detecting acute myocardial infarction for a twofold increase in myoglobin level from baseline were 39% and 98%, respectively. The early diagnostic performance of myoglobin at admission, the second level drawn 2 to 3 hours later, and creatine kinase-MB mass drawn at admission were similar (receiver-operating characteristic curves 0.80, 0.86, and 0.85). The diagnostic performance of each of these markers was significantly superior to the absolute change from baseline to second myoglobin (receiver-operating characteristic curve 0.77). In patients who presented within 4 hours of symptom onset, myoglobin drawn 2 to 3 hours later had the highest yield for detecting myocardial infarction. These results suggest that serial myoglobin measurement aiming to detect changes over time is not superior to single marker determinations. Myoglobin measured in 2 to 3 hours from admission may be helpful in triaging patients who present within 4 hours from onset of symptoms.
This subset study looked at 368 patients who presented with chest pain . They had an initial myoglobin drawn within 3 hours of presentation and a second drawn 2 to 3 hours after that,therefore vague timepoints for sampling. They also had CK-MBs drawn at presentation 8, 16 and 24 hours from presentation. Only 42% of patients arrived less than 4 hours of symptoms, a full 40% had symptoms > than 12 hours prior to presentation. This would obviously affect the myoglobin values.
Level of Evidence 3b
Good
Supportive
Porela(00)Porela, P., K. Pulkki, et al. (2000). "Prediction of short-term outcome in patients with suspected myocardial infarction." Annals of Emergency Medicine 35(5): 413-20..0
STUDY OBJECTIVE: Although specific cardiac injury markers have enhanced early patient classification, the ECG remains a necessary investigation in the acute phase of chest pain. Combined use of both tests could further improve the diagnostic and prognostic accuracy. METHODS: We studied 311 consecutive patients who came to the emergency department of a regional referral hospital for the differential diagnosis of acute chest discomfort. The admission ECG was classified using an automated interpretation program and tested together with elevated admission creatine kinase isoform MB (CK-MB) and cardiac troponin I (TnI) concentration for prediction of final myocardial injury (44%) and in-hospital mortality (14%). RESULTS: Combining the information from the admission ECG and cardiac markers, the sensitivity for becoming final myocardial injury (maximal CK-MB >/=11 microg/L) was 90% and specificity 61%. The proportion of false-negative results (10%) was independent of symptom duration. Age, positive ECG findings, and increased admission TnI levels were predictive for in-hospital mortality. CONCLUSION: The commonly available biochemical and ECG criteria allow risk stratification of patients with a suspected acute ischemic event. The data analysis can easily be automated and is independent of patient delay.
This Finnish study looked at 301 consecutive patients, 31% had a previous documented MI. Median delay from symptom onset to ED admission was 240 minutes. WHO criteria were used to diagnose AMI. CK-MB assay was IMX test with a upper reference range of 5 ug per L and a coefficient variation of 4%. First generation troponin I assays used Inno Trac Diagnostics OY. Cutoff was 0.1 ug per L. Inclusion criteria were all patients with suspected MI. The study center was an ED as well as referral cardiac center. Results: 90% of patients were admitted for a 24-

document.doc Page 47 of 77
hour. CK-MB on admission sensitivity was 60%, specificity 92%, PPV of 85, NPV of 75 with LR+ of 7.2 and a LR- of 0.4. Troponin I results respectively 53, 91, 81, 72, 5.4 and 0.5. Of note the final myocardial injury was defined as a maximum CK-MB level > or = 11 ug per L yielding an AMI prevalence of 44%!. Patients with recent trauma or surgery were excluded from this study. It did no discuss renal failure patients. It did not use stress testing or coronary angiography results in its reference standards.
Level of Evidence 1bQuality of Evidence PoorNeutral
Rebuzzi(98)Rebuzzi, A. G., G. Quaranta, et al. (1998). "Incremental prognostic value of serum levels of troponin T and C- reactive protein on admission in patients with unstable angina pectoris." Am J Cardiol 82(6): 715-719.
Management of unstable angina is largely determined by symptoms, yet some symptomatic patients stabilize, whereas others develop myocardial infarction after waning of symptoms. Therefore, markers of short-term risk, available on admission, are needed. The value of 4 prognostic indicators available on admission (pain in the last 24 hours, electrocardiogram [ECG], troponin T, and C-reactive protein [CRP]), and of Holter monitoring available during the subsequent 24 hours was analyzed in 102 patients with Braunwald class IIIB unstable angina hospitalized in 4 centers. The patients were divided into 3 groups: group 1, 27 with pain during the last 24 hours and ischemic electrocardiographic changes; group 2, 45 with pain or electrocardiographic changes; group 3, 30 with neither pain nor electrocardiographic changes. Troponin T, CRP, ECG on admission, and Holter monitoring were analyzed blindly in the core laboratory. Fifteen patients developed myocardial infarction: 22% in group 1, 13% in group 2, and 10% in group 3. Twenty-eight patients underwent revascularization: 37% in group 1, 35% in group 2, and 7% in group 2 (p <0.01 between groups 1 or 2 vs group 3). Myocardial infarction was more frequent in patients with elevated troponin T (50% vs 9%, p=0.001) and elevated CRP (24% vs 4%, p= 0.01). Positive troponin T or CRP identified all myocardial infarctions in group 3. Only 1 of 46 patients with negative troponin T and CRP developed myocardial infarction. Among the indicators available on admission, multivariate analysis showed that troponin T (p=0.02) and CRP (p=0.04) were independently associated with myocardial infarction. Troponin T had the highest specificity (92%), and CRP the highest sensitivity (87%). Positive results on Holter monitoring were also associated with myocardial infarction (p=0.003), but when added to troponin T and CRP, increased specificity and positive predictive value by only 3%. Thus, in patients with class IIIB unstable angina, among data potentially available on admission, serum levels of troponin T and CRP have a significantly greater prognostic accuracy than symptoms and ECGs. Holter monitoring, available 24 hours later, adds no significant information.
This Italian study looked at Braunwald Class lllB unstable angina pts. in 4 Italian hospitals. Of note the average length of pain prior to admission was 11 plus or minus 7 hours (quite prolonged compared to other studies). The troponin assay used on admission was Boehringer Mannheim with a level of sensitivity of 0.2 micrograms per liter and values > 0.20 micrograms per liter considered positive. Follow up occurred for 3 months; MI was diagnosed as per WHO criteria. The authors found a sensitivity for troponin T of 47%,a specificity of 92% a positive predictive value of 50 and a NPV of 91 in the 15 out of 102 patients that developed an MI.No incremental ie serial Tn assays were performed.
Level of Evidence 4Quality of Evidence FairOpposing
Roth(01)Roth, A., N. Malov, et al. (2001). "The "SHAHAL" experience in Israel for improving diagnosis of acute coronary syndromes in the prehospital setting." American Journal of Cardiology 88(6): 608-10.

document.doc Page 48 of 77
The diagnosis of acute coronary syndromes is frequently missed, and many high-risk patients fail to be admitted to hospital. The aim of this study was to assess the value of cardiac markers in ruling out acute ischemic events in patients with symptoms of possible cardiac origin and nondiagnostic electrocardiograms. The data collected between May 1999 and April 2000 for this prospective cohort study were retrieved from the records of 777 consecutive prehospital patients (mean age 70 years, 62.9% men) whose symptoms lasted for 6 to 48 hours, who were treated by mobile intensive care teams, and for whom the physician could not reach a clear-cut decision whether they should be taken to hospital or left at home. The cardiac markers, creatine kinase (CK-MB), myoglobin, and troponin I, were measured at the scene using a rapid Stat kit to qualitatively detect their presence in whole blood samples. Results were determined after 15 minutes at the scene. The assay was positive in 30 patients, 11 of whom had a definite cardiac diagnosis (acute myocardial infarction in 4 and unstable angina pectoris in 7). Positive and negative predictive values of the assay for detecting a significant coronary event were 36.7% and 100%, respectively. Of the 747 patients with a negative result, 6 patients had a false result (1 with myocardial infarction and in 5 with unstable angina) (99.2% negative predictive value). Thus, cardiac markers are useful in ruling out high-risk coronary syndromes in the prehospital setting when the clinical presentation and electrocardiogram are inconclusive.
This Israeli study looked at 777 patients who were at very high risk for a CAD. When the physician in the field could not decide whether the patient should be taken to the hospital, triple marker point of care assay was carried out using the Spectral Diagnostics assay for myoglobin, troponin I, and CK-MB. Patients had to have had pain or other symptoms greater than 6 hours and less than 48 hours prior to assay, EKGs had to show no ST segment elevation or signs of ischemia. Thus a low to intermediate risk population were assayed, but end point was AMI Diagnosis in hospital (NO DEFINITION !). All patients were followed up at 7 days, including a 12 lead transmitted EKG.
30 patients were positive and taken to hospital, however 7 were discharged from the emergency room “after reassessment” and 23 were hospitalized for further investigation. There are no details on these patients. More confusing is the positive and negative predictive values for detection of significant coronary event listed as 36.7% and 100% respectively and they then comment that 6 patients ultimately were diagnosed with significant coronary events revising the negative predictive value to 99.2%.
My biggest concern is that the description of how the gold standard of acute myocardial infarction was defined and derived.
I do not find the conclusions useful.
Level of Evidence 4
Quality of Evidence Good
Opposing
Sayre(98)Sayre, M. R., K. H. Kaufmann, et al. (1998). "Measurement of cardiac troponin T is an effective method for predicting complications among emergency department patients with chest pain.[see comment]." Annals of Emergency Medicine 31(5): 539-49.
STUDY OBJECTIVES: To determine the test performance characteristics of serum cardiac troponin T (cTnT) measurement for diagnosis of acute myocardial infarction (AMI), and to determine the ability of cTnT to stratify emergency department patients with chest pain into high- and low-risk groups for cardiac complications. METHODS: We conducted a prospective observational cohort study with convenience sampling in a tertiary care, urban ED. The study sample comprised 667 patients presenting to the ED with a complaint of chest pain or other symptoms suggesting acute ischemic coronary syndrome (AICS). Patients were assigned to different blood sampling protocols for cTnT therapy on the basis of their ECG at presentation: nondiagnostic for AMI at 0, 3, 6, 9, 12, and 24 hours after ED presentation; or ECG diagnostic for AMI at 0, 1, 2, 3, 4, 5, 6, 7, 8, 9, 12, 18, and 24 hours after ED presentation. RESULTS: Of 667 patients, 34 had AMI diagnosed within 24 hours of ED arrival. Using a .2 microgram/L discrimination level for cTnT, sensitivity for AMI within 24 hours of ED arrival was 97% (95% confidence interval, 91.4% to 99.9%), and specificity was 92% (89.8%-94.1%). When the effects of age, race, sex, and creatine kinase-MB isoenzyme subunit test results were controlled, a patient

document.doc Page 49 of 77
with cTnT of .2 microgram/L or greater was 3.5 (1.4 to 9.1) times more likely to have a cardiac complication within 60 days of ED arrival than a patient with a cTnT value below .2 microgram/L. CONCLUSION: Measurement of cTnT will accurately identify myocardial necrosis in patients presenting to the ED with possible AICS. Elevated cTnT values identify patients at increased risk of cardiac complications.
This group looked at all patients > 25 years of age with chest pain or other symptoms consistent with ACS.Median duration of pain 6.4 hours. This included recent cocaine users. Though serial samples were to be drawn up to 24 hours, patients were released from ED if they were extremely low risk and have negative baseline and 3 hour blood assays. The follow up was 88% at 60 days. It looked at all possible adverse events. The blood analyzer was the ES 300 auto analyzer with a first generation antibody technology. Values greater or equal to 0.2 ug per liter were considered positive. 667 patients were captured with a median duration of pain 6.4 hour to ED presentation. Of concern 76 patients did not have CK-MB testing but I believe were included in the statistic. 69 patients were released less than 6 hours of observation. These were no excluded. 17 patients with creatinines in the elevated range were not excluded. Patients with STEMI were not excluded. The 3-hour values for TnT:sensitivity of 64.5%, a specificity of 92.6%, a LR + 8.7, LR – 0.4 ; for CK-MB respectively 40%, 99.8%, 200, and 0.6. At 6 hours the TnT sensitivity was 78.8%, specificity 93.1%, LR+ 11.4, LR-0.2. The results for CK-MB were respectively 50%, 99.8%, 250 and 0.5. these were values for the detection of AMI. (WHO criteria).
Level of Evidence 3b
Quality of Evidence Fair
Neutral
Schuchert(99) Schuchert, A., C. Hamm, et al. (1999). "Prehospital testing for troponin T in patients with suspected acute myocardial infarction." American Heart Journal 138(1 Pt 1): 45-8.
BACKGROUND: Cardiac troponin T (TnT) is a highly sensitive and specific marker for myocardial damage and can be detected early after myocardial injury. Our hypothesis was to use TnT as an objective marker to verify acute myocardial infarction before hospital admission. METHODS AND RESULTS: We evaluated the sensitivity of a rapid qualitative assay for serum TnT for the detection of acute myocardial infarction in the ambulance and assessed the predictive value of a positive prehospital TnT test for death and myocardial infarction during 6-months of follow-up. The study, conducted in an urban area, included 158 consecutive patients with suspected acute myocardial infarction (93 men aged 69 +/- 13 years). A myocardial infarction was confirmed in 40 and excluded in 118 patients. The prehospital TnT test was positive in 11 patients, of whom 7 had acute myocardial infarction. Fifty-three patients had a positive test result at hospital admission, with evidence of myocardial infarction in 39 of them. The sensitivity to acute myocardial infarction was 18% for the prehospital and 98% for the in-hospital test with 78% and 88% specificity, respectively. During follow-up, patients with a positive prehospital TnT test result had cardiac events more often (9 of 11) than patients with a negative result (26 of 147; P <.0001). CONCLUSIONS: In areas with short transport times to the patient the rapid TnT test performed at the point of care identified only a minority of the patients with acute myocardial infarction. A positive prehospital TnT test result seems to be an objective marker for a worse outcome in patients presenting with suspected acute myocardial infarction.
This study was done in pre hospital field out of Hamburg Germany. This study looked at TnT qualitative point of care assay in pre hospital versus a quantitative TnT assay in hospital with regards to AMI/unstable angina and adverse events. WHO criteria were used for diagnosis. 158 patients were entered. The point of care assay was TROP Boehringer Mannheim, the discriminating value was 0.18 nanograms per milliliter. They found a sensitivity to detect MI of only 18% and a specificity of 97% using point of care: using the in hospital TnT assay they found this jumped to 98% sensitivity and 88% specificity. Apparently this assay was drawn on admission to hospital with? short transfer times between the home and the emergency department. In the

document.doc Page 50 of 77
discussion the author’s quote this threshold level was reduced to 0.08 nanograms per milliliter and that the assay has been replaced with a different one.
Level of Evidence 4
Quality of Evidence Fair
Opposing
Stork(02)Stork, T. V., A. H. Wu, et al. (2000). "Diagnostic and prognostic role of myoglobin in patients with suspected acute coronary syndrome. North-Wurttemberg Infarction Study (NOWIS) Group." Am J Cardiol 86(12): 1371-4, A5.
In patients with suspected acute coronary syndrome, myoglobin is, according to IFCC and NACB guidelines, the marker of choice for early determination of acute infarction, in particular in combination with creatine kinase-MB, 4 hours after admission with a sensitivity of 96%, and correctly excludes Q-wave infarctions. In patients without acute myocardial infarction, a positive troponin T (relative risk 31.5%), but not an elevated myoglobin (relative risk 4.5%), is highly predictive for adverse in-hospital outcome.
This study was a sub study analysis out of Germany (NOWIS). It looked at 253 patients without ST segment elevation; average onset of pain to first sample was 2.6 hours duration. Samples were done at 0, 4, and 24 hours duration for myoglobin, troponin and CK MB. End points were AMI by WHO criteria and unstable angina using Braunwald classification. The AMI prevalence is stated as 26%in one section and 5% in another Patients with a renal history of raised creatinine were excluded. Clinicians based management strategy before biochemical tests were available. Myoglobin cutoff was greater 80ng per milliliter, troponin T greater than 0.1 ng per milliliter and CK MB greater than 100 U/L and greater than 6% CK MB fraction. The results showed on admission myoglobin sensitivity of 62% and myoglobin /CK MB combination sensitivity at 74%. The 4 hour sensitivity was 73% for troponin T, 85% for myoglobin, 85% for CK MB and 96% for a combination of myoglobin/CK MB and 88% for a combination myoglobin/troponin T. They state that the sensitivity at 4 hours for detecting AMI was highest with myoglobin as a single marker However at 4 hours they list myoglobin and CK MB negative predictive value as being 98 and that of myoglobin and troponin T being 94.
One must note the short duration of symptoms prior to entering into this study and its effect on assay positivity,as well as the (apparently) high AMI prevalence.Not transferable togeneral EDs.
Level of Evidence 2b
Quality of Evidence Fair
Supportive
Svensson (03)Svensson, L., C. Axelsson, et al. (2003). "Elevation of biochemical markers for myocardial damage prior to hospital admission in patients with acute chest pain or other symptoms raising suspicion of acute coronary syndrome." Journal of Internal Medicine 253(3): 311-9.
OBJECTIVES: To evaluate the occurrence of elevation of serum biochemical markers for myocardial damage in the prehospital setting amongst patients who called for an ambulance due to a suspected acute coronary syndrome (ACS). DESIGN: Prospective observational study. SUBJECTS: All the patients who called for an ambulance due to suspected ACS. SETTING: South Hospital's catchment area in Stockholm and in the Municipality of Goteborg, Sweden between January and November in the year 2000, were included. INTERVENTIONS: On arrival of the ambulance crew, a blood sample was drawn for bedside analysis of serum myoglobin, creatine kinase MB and troponin I. A 12-lead electrocardiogram (ECG) was simultaneously recorded. MAIN OUTCOME MEASURES: Elevation of biochemical markers prior to hospital admission. RESULTS: In all, 511 patients participated on 538 occasions. Elevation of any biochemical marker was observed in 11% of all patients. The corresponding figure for patients developing myocardial infarction was 21%; for patients with myocardial ischaemia 8%; for patients with a possible myocardial ischaemia 4% and for patients with other diagnoses 5%. Amongst those who had a final diagnosis of acute myocardial infarction (AMI), 47% had ST-elevation on initial ECG and 57% had
document.doc Page 51 of 77
either ST-elevation or elevation of any biochemical marker. CONCLUSION: Bedside analysis of biochemical markers in serum is already feasible prior to hospital admission amongst patients with a suspected ACS. About 20% of patients with AMI have elevated biochemical markers at that stage. When found this data might increase the possibility of diagnosing an AMI very early in the course. However, false positives were found and whether this strategy will improve the triage of these patients in the prehospital setting remains to be proven.
This author out of Sweden looked at 511 patients where an ambulance went to the house with patients complaining of chest pain; doctors were in attendance. Point of care testing for CK-MB and troponin I was carried out. The assay was Cardiac Status Spectro Diagnostics. Myoglobin was > 50 nanograms per milliliter, CK-MB > 5 ng per milliliter, and troponin I > 0.1 ng per milliliter. This was a qualitative assay. MI was subsequently diagnosed by WHO criteria or when troponin T was > 0.05 ng per milliliter. They found a sensitivity of 21% and specificity of 92% for any biochemical marker rise to confirm the diagnosis of AMI(WHO criteria +/- TnT). The interval between onset of symptoms and blood sampling of 158 minutes. Myocardial infarction was the final diagnosis in 31% of patients. Myocardial ischemia or MI was the final diagnosis in 60% of this population. Therefore it was a very high prevalence in this small number study and findings cannot be translated to general EDs.
Level of Evidence 1bQuality of Evidence GoodNeutral
Svensson (04)Svensson, L., C. Axelsson, et al. (2004). "Prognostic value of biochemical markers, 12-lead ECG and patient characteristics amongst patients calling for an ambulance due to a suspected acute coronary syndrome." Journal of Internal Medicine 255(4): 469-77.
OBJECTIVES: To evaluate whether a 12-lead ECG, together with a multi-marker strategy that used point-of-care measurements of myoglobin, creatine kinase (CK-MB) and troponin I, was able to predict patients at short- and long-term risk of death, when simultaneously considering age, gender, previous history, symptoms and clinical findings on arrival of the ambulance. DESIGN: Prospective observational study. SETTING AND SUBJECTS: Consecutive patients (n=511) in ambulances in Stockholm and Goteborg in Sweden who called for an ambulance due to chest pain or other symptoms raising a suspicion of acute coronary syndrome. INTERVENTION: In almost all patients, a diagnostic ECG, patient baseline characteristics and measurements of CK-MB, troponin I and myoglobin were recorded. RESULTS: In univariate analysis, the highest 30-day mortality (17%) was found amongst patients with the combination of ECG signs of myocardial ischaemia and the elevation of any biochemical marker. The highest 1-year mortality (20%) was found amongst patients with ECG signs of myocardial ischaemia and the elevation of any biochemical marker. Increasing age (RR 1.07; 95 CI 1.02-1.13) lack of symptoms of chest pain and a previous history of hypertension (3.02; 1.08-8.79) were independent predictors of 30-day mortality. Myoglobin was the only biochemical marker independently associated with 30-day mortality (6.66; 1.83-22.3). Increasing age (1.11; 1.06-1.16), previous history of diabetes (3.42; 1.41-8.25) heart failure (2.64; 1.26-5.52) and other symptoms than chest pain and dyspnoea (5.23; 2.14-12.76) were independent predictors of 1-year mortality. In many of the variables the confidence limits were wide. CONCLUSION: Amongst patients with a clinical suspicion of acute coronary syndrome, those with the combination of ECG signs of myocardial ischaemia and the elevation of any biochemical marker on arrival of the ambulance form a group with a particularly high risk of death. However, age as well as aspects of clinical history and type of symptoms independently contribute to prognostic information.
This study looked at pre hospital biochemical assay to predict mortalityoutcome at 30 days and 1 year.. This was a study out of Sweden that looked at 511 patients in which doctors in the ambulance assessed patients for acute coronary syndrome. The chest pain median interval between onset of symptoms and analysis was 90 minutes. The assay used was Cardiac Status Spectral Diagnostics who financed this study. It tested for myoglobin, CK and troponin I using a qualitative assessment with a myoglobin cutoff of greater 50 ng per milliliter, CK MB greater than 5 ng per milliliter and troponin I greater than 0.1 ng per milliliter. The study found both troponin I and CK-MB predictive of 30 day mortality but did not directly correlate the assays with the

document.doc Page 52 of 77
diagnosis of acute coronary syndrome in hospital.
Sensitivity/specificity can be derived from data.Percentage capture at endpoints not available.
Level of Evidence 4
Quality of Evidence Fair
Opposing
Young(99).Young, G. P., P. Murthi, et al. (1999). "Serial use of bedside CKMB/myoglobin device to detect acute myocardial infarction in emergency department chest pain patients." Journal of Emergency Medicine 17(5): 769-75.
A qualitative bedside device (Spectral Diagnostics, Toronto, Canada) for CKMB and myoglobin (MYOG) detection was evaluated in emergency department (ED) patients with chest pain to determine performance characteristics. At presentation (0 h) and at three hours (3 h), serum was analyzed in the ED with results considered positive if either 0-h or 3-h CKMB or MYOG bands were visible. The results were compared with the diagnosis of myocardial infarction (MI) per hospital discharge diagnosis (n = 132, 87%) or telephone follow-up (n = 19; 1 patient lost to follow-up). Of 151 study patients, 30 (20%) were diagnosed with MI; all were admitted to hospital. On electrocardiogram (EKG), 17 (57%) MI patients had ST-segment elevation. At 0-h, 26 of 30 (87%) MI patients were positive for CKMB/MYOG. By 3 h, 21 of 23 (91%) MI patients were positive for CKMB/MYOG; 7 MI patients were already admitted to hospital. Combining 0-h and 3-h results, the device sensitivity for MI was 93% (28/30) with specificity of 54%. Combining device results plus diagnostic EKG, sensitivity was found to be 100% (30/30). If the device result was positive, then the odds ratio for having an ischemic complication was 6.5. We conclude that the CKMB/MYOG device identified most MI patients at ED presentation and 3 h later. Combining device results with EKG detected all MI patients in the ED.
This study looked at point of care testing for CK-MB/myoglobin at 0 and 3 hours post presentation. They used the Sp. Diag. assay cardiac STATUS; this was a qualitative colorimetric assay. Cutoffs were 5.0 nanograms per milliliter for CK-MB and 100 nanograms per milliliter for myoglobin. Outcome was AMI by WHO criteria, ie CK MB elevation and so results in incorporation bias . 18 patients not admitted were followed up within 2 weeks for telephone contact. Major adverse cardiac events were looked for. A total of 151 patients by convenience were entered. Of note this study was supported by a grant from Sp Diag. Results: 132 patients were admitted, 30 (20%) had a final diagnosis of AMI(hospital discharge dx), 17 patients having a STEMI. Of note both the physician and the research nurse independently read the results and found concordance. Results were tabulated for CK-MB and myoglbin at time 0 and time 3 hours. The combined CK-MB/myoglobin result at 3 hours was sensitivity 93, specificity 54, positive predictive values 38 and negative predictive value 96. They reported with 95% CI. 19 patients (13%) were discharged form the ED and 18 were followed up with no history of adverse events.
Level of Evidence 4Quality of Evidence FairSupportive
Zarich (02)Zarich, S. W., A. U. Qamar, et al. (2002). "Value of a single troponin T at the time of presentation as compared to serial CK-MB determinations in patients with suspected myocardial ischemia." Clinica Chimica Acta 326(1-2): 185-192.
Background: Prior studies with cardiac markers have focused predominantly on subjects presenting to the emergency department with chest pain or unstable angina, and have relied on serial markers for the diagnosis of acute myocardial infarction. We evaluated the diagnostic utility of a single cardiac troponin T (cTnT) determination at the time of presentation as compared to serial creatine kinase (CK) MB determinations in a broad spectrum of patients with suspected myocardial ischemia. Methods: A total of 267 consecutive patients presenting to the emergency department with suspected myocardial ischemia had a single, blinded cTnT determination drawn at the time of

document.doc Page 53 of 77
presentation to the emergency department in addition to routine serial electrocardiographic and CK-MB determinations. Results: The specificity (93.7% vs. 87.1%; p<0.05) and positive predictive value (80.0% vs. 69.4%; p<0.05) of a single cTnT determination were superior to that of serial CK-MB determinations without compromising sensitivity. Forty-six percent of patients with confirmed myocardial infarction and an abnormal cTnT at presentation had a normal initial CK-MB determination. Conversely, 20% of patients without acute coronary syndromes had an abnormal CK-MB determination in the setting of a normal cTnT. The initial cTnT was abnormal in all patients with confirmed myocardial infarction and a symptom duration of at least 3.5 h. Conclusions: In a heterogeneous population of patients with suspected myocardial ischemia, the initial cTnT determination drawn at the time of presentation is a powerful diagnostic tool that, when used in context with symptom duration, allows for more rapid and accurate triage of patients than serial CK-MB determinations. (C) 2002 Elsevier Science B.V. All rights reserved.
This study looked a single presentation TnT value versus serial CK-MB values. 267 patients were enrolled for suspected myocardial injury. Five were excluded if they had chest trauma or renal failure. Physicians were blinded to the troponin T values, CK and CK- MB determinations, were 0, 4, 8, and 16 hours post presentation. TnT assays were carried out on ES 300 analyzer “first generation” immuno assay; the lower level of detection was 0.05 micrograms per liter with a value of 0.1 micrograms per liter and above was considered abnormal. This new precision was 8.7%. CK-MB values > 150 units per liter in a MB fraction > 17 units per liter or a ratio > 5% were considered abnormal. Diagnosis of MI was by WHO criteria and that of unstable angina by Braunwald classification type 3B. Average length of symptoms prior to presentation was 5.75 hours, somewhat prolonged compared to average. Sensitivity of troponin T for the diagnosis of AMI was 86.7% compared to the initial CK MB of 46.6%; specificity was 93.7 compared with 82.6; PPV was 80.0 versus 44.6 and NPV was 96.0 compared to 84.7.
Many patients would not wait for the extended CK-MB assays in that they were felt to be low risk thus resulting in a relatively high incidence of AMI (22.5%). Their conclusions might be appropriate for AMI, but not ACS.
Level of Evidence 4
Quality of Evidence Good
Supportive
Zarich(04) Zarich, S. W., K. Bradley, et al. (2004). "Minor elevations in troponin T values enhance risk assessment in emergency department patients with suspected myocardial ischemia: Analysis of novel troponin T cut-off values." Clinica Chimica Acta 343(1-2): 223-229.
Background: A consensus document developed by a joint committee of the European Society of Cardiology and the American College of Cardiology redefines myocardial infarction (MI) using an increase of troponin I or T as compared to a reference control population (i.e., troponin T (TnT) of 0.01 [mu]g/l). A clinical problem arises when an arbitrary cut-off point is selected for determination of MI (i.e., TnT>=0.1 [mu]g/l), as minor elevations of troponin are associated with increased cardiovascular risk in selected patients with acute coronary syndromes. Methods: We prospectively studied 420 unselected patients being evaluated for suspected myocardial ischemia in the emergency department (ED). We compared a 99th percentile MI cut-off limit for TnT, determined by constructing a standard receiver operator curve from our ED population in whom an acute coronary syndrome was excluded, to a standard MI cut-off limit of 0.1 [mu]g/l in assessing cardiovascular risk. We also assessed the prognostic value of detectable TnT concentrations below this 99th percentile MI cut-off, but above the upper reference limit of healthy controls. Results: The diagnosis of acute coronary syndromes (ACS) was more frequent in groups with higher TnT concentrations: 16.8% with a normal TnT (<0.03 [mu]g/l), 29.5% with detectable TnT below the 99th percentile MI limit (0.03-0.066 [mu]g/l), 64.3% with detectable TnT between the 99th percentile and standard MI cut-offs (0.067-0.099 [mu]g/l), and 85.4% with TnT>=0.1 [mu]g/l (p<0.001 for the trend). Thirty-day cardiovascular event rates increased for any detectable concentration of troponin: 1.3% with normal TnT, 4.8% with detectable TnT below the 99th percentile MI limit, 15.4% with TnT between the 99th percentile and standard MI cut-off limits, and 12.5% with TnT>=0.1 [mu]g/l (p<0.01 for the trend). Conclusion: Using an MI cut-off

document.doc Page 54 of 77
concentration for TnT from a 'non-ACS reference' improves risk stratification, but fails to detect a positive TnT in 11.7% of subjects with an acute coronary syndrome. (C) 2004 Elsevier B.V. All rights reserved.
This study looked at small increments in elevation of TnT in its relationship to outcome. 420 patients were entered suspicious for ACS. Patients were included if they had more than 30 minutes of symptoms in the absence of ST segment elevation. The bloods were drawn at 0, 3, and 12 hours post presentation. There was no sub group analysis. It is noted that over 50% of the group was discharged prior to the 12 hour assay. The TnT assay was Elecsys troponin t STAT, third generation assay from Roche Diagnostics. The manufacture suggested cutoff was 0.1 ug per liter, CK MB was also assayed with a cutoff of greater than or equal to 17 units per liter. Patients were followed up for 30 days for non-fatal MI or death, follow up was in 395 of patients so 95 % capture. MI was diagnosed using WHO criteria, unstable angina using Braunwald classification type 111B . The 99th percentile for TnT in patients in who ACS was excluded was determined to be 0.067 ug per liter with CV of 8%. This was used for the MI cutoff. A TnT value of less than 0.03 micrograms per liter was considered normal based on a 99-percentile value of 0.01 micrograms per liter in reference controls and a 10% CV limit of less than 0.03 micrograms per liter as suggested by the manufacturer.
4 groups were determined based on the peak troponin T value; less than 0.03 micrograms per liter 0.03; 0.03 – 0.66 micrograms per liter; 0.67 – 0.99 micrograms per liter in greater than or equal to 0.1 micrograms per liter. Results showed final diagnosis of acute coronary syndrome in 111 out of 420 (26.4%) this was associated with 16.8% in the first group, 29.5% in the second group, 64.3% in the third group and 85.4% in the fourth group (P less than 0.001) at the 0.03 microgram per liter cutoff the sensitivity for TnT would be 98.3%, specificity of 88.4%; at 0.67 micrograms per liter it would be 75.9/96.7; at 0.1 microgram per liter it would be 60.3/98.3. The limitations on this trial was that of a single center in that the number of small patients “n=58” with minor TnT elevations below the standard of 0.1 microgram per liter cutoff were small.
Only the authour was involved in Final Diagnosis.
Level of Evidence 4
Quality of Evidence Good
Supportive
Zimmerman(99)Zimmerman, J., R. Fromm, et al. (1999). "Diagnostic marker cooperative study for the diagnosis of myocardial infarction.[see comment]." Circulation 99(13): 1671-7.
BACKGROUND: Millions of patients present annually with chest pain, but only 10% to 15% have myocardial infarction. Lack of diagnostic sensitivity and specificity of clinical and conventional markers prevents or delays treatment and leads to unnecessary costly admissions. Comparative data are lacking on the new markers, yet using all of them is inappropriate and expensive. METHODS AND RESULTS: The Diagnostic Marker Cooperative Study was a prospective, multicenter, double-blind study with consecutive enrollment of patients with chest pain presenting to the emergency department. Diagnostic sensitivity and specificity and frequency of increase in patients with unstable angina were determined for creatine kinase-MB (CK-MB) subforms, myoglobin, total CK-MB (activity and mass), and troponin T and I on the basis of frequent serial sampling for </=24 hours. Of 955 patients with chest pain, 119 (12.5%) had infarction identified by use of CK-MB mass, and 203 (21%) had unstable angina. CK-MB subforms were most sensitive and specific (91% and 89%) within 6 hours of onset, followed by myoglobin (78% and 89%). For late diagnosis, total CK-MB activity (derived from subforms) was the most sensitive and specific (96% and 98%) at 10 hours from onset, followed by troponin I (96% and 93%), but not until 18 hours, and troponin T (87% and 93% at 10 hours). In unstable angina, CK-MB subforms were increased in 29.5%, myoglobin in 23.7%, troponin I in 19.7%, and troponin T in 14.8%. All markers were increased in 99 patients. With each marker as the diagnostic standard, CK-MB subforms and myoglobin remained the most sensitive for early diagnosis. CONCLUSIONS: The CK-MB subform assay alone or in combination with a troponin reliably triages patients with chest pain and should lead to improved therapy and reduced cost.

document.doc Page 55 of 77
This multi center prospective trial was carried out in 4 teaching hospitals. Inclusion criteria included chest pain > 15 minutes within 24 hours of presentation.Median time for onset of symptoms to arrival was 5.7 hrs. Multiple markers were drawn at 0, 1,4 and 6 hours and then every 4 hours there after for 24 hours. The total CK activity was defined as > 120 IU per L. Total CK mass was defined as > 7 ug per L: CK subforms as > 2.5 iu per L, CK-MB activity > 9 iu per L, myoglobin > 85 ng per milliliter, troponin t > 0.1 nanograms per milliliter, Troponin I > 1.5 nanograms per milliliter. MI was diagnosed with a CK-MB mass > 7 and an index > or = 2.5%. Unstable angina was a clinical diagnosis.
Of 955 patients, 119 (12.5%) had an AMI by WHO criteria. The results were grouped as early diagnosis i.e. < or = 6 hour results or late diagnosis i.e. < 10 hours. Looking at early diagnosis, the markers CK-MB subforms and myoglobin exhibited sensitivities of 91 and 78% respectively with similar specificities of around 89%. In contrast, total CK-MB mass, CK activity, troponin I, and T had sensitivities of 66%, 74.5 %, 57.5% and 61.7% respectively. CK-MB subforms from the first sample showed a sensitivity of 48.7% and specificity of 87.6% which was similar to that of myoglobin (48.7% and 87.7%) These 2 markers were found to be most sensitive within 6 hours of onset of symptoms.
Very little was said of unstable angina, which was poorly defined and statistically analyzed. Of note this article did not look at any follow up adverse events.
Iincorporation bias re: CK isoforms was used to derive CK MB activity.
Level of Evidence 4
Quality of Evidence Good
Supportive
from EndNote by selecting the citation, then copying the FORMATTED citation using the short cut, Ctrl-K. After you copy the citation, go back to this document and position the cursor in the field, then paste the citation into the document (use Ctrl-V). For each new citation press Tab to move down to start a new field.
Excluded Articles
Boufous (03)Boufous, S., P. W. Kelleher, et al. (2003). "Impact of a chest-pain guideline on clinical decision-making.[see comment]." Medical Journal of Australia 178(8): 375-80.
Although heart-type fatty acid-binding protein (H-FABP) can be a marker of sarcolemmal injury due to acute myocardial ischemia, the diagnostic or prognostic value is not established in patients with acute chest pain. This multicenter prospective study aimed to determine the diagnostic and prognostic values of H-FABP in 133 patients presenting to an emergency room with suspected acute coronary syndrome (ACS) by comparing with those of conventional biomarkers. H-FABP and myoglobin had greater positive results than did creatine kinase-MB or troponin T. Receiver operating characteristics analysis revealed that H-FABP was the most reliable for detection of ACS and that H-FABP had the greatest sensitivities for identification of patients requiring emergency hospitalization, coronary angiography, and interventional therapy within 7 days among the biomarkers. Thus, H-FABP can be an early diagnostic and prognostic biochemical marker, particularly within the first 6 h from the onset of chest symptoms, in patients with chest pain at an emergency department. Copyright 2003 S. Karger AG, Basel
Rejected because looked at chest pain guideline. Agewall (03)
Agewall, S. (2003). "Evaluation of point-of-care test systems using the new definition of myocardial infarction." Clinical Biochemistry 36(1): 27-30.
OBJECTIVES: To examine the proportion of patients admitted to CCU because of chest pain with a negative quantitative troponin t-test (Cardiac reader; Roche), who despite the negative test, would
document.doc Page 56 of 77
fulfil the new myocardial infarction criteria. A second aim was to evaluate the clinical utility of troponin I. DESIGN AND METHODS: Troponin T (Cardiac reader; Roche) was measured 12 h after the last chest pain episode. If Troponin T was negative the subjects were included in the study. All included subjects were also examined with troponin I (Stratus CS; Dade Behring) and troponin T at the central laboratory (Elecsys 2010) at the same time. 187 patients were included. CKMB was also measured 6 h after the last chest pain (Stratus CS; Dade Behring). RESULTS: Fifteen patients (8.0%) fulfilled the criteria of myocardial infarction, despite a negative Troponin T (Cardiac reader; Roche). CKMB measures did not add useful diagnostic information. The sensitivity and specificity were 100% and 95.3%, respectively for troponin I, when 0.2 microg/L was used as cut off level for myocardial infarction. CONCLUSION: In this low risk group, eight percent of the patients with a negative Troponin T (Cardiac reader; Roche) fulfilled the new criteria of myocardial infarction. Troponin I (Stratus CS; Dade Behring) appeared to be a reliable method in this group.
This study looked at CCU patients admitted with chest pain greater than 12 hours duration
Allman (04)Allman, K. C. and S. B. Freedman (2004). "Emergency department assessment of patients with acute chest pain: Myocardial perfusion imaging, blood test, or both?" Journal of Nuclear Cardiology 11(1): 87-89.
Review article.Antman(00)
Antman, E. M., M. Cohen, et al. (2000). "The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making." JAMA 284(7): 835-42.
CONTEXT: Patients with unstable angina/non-ST-segment elevation myocardial infarction (MI) (UA/NSTEMI) present with a wide spectrum of risk for death and cardiac ischemic events. OBJECTIVE: To develop a simple risk score that has broad applicability, is easily calculated at patient presentation, does not require a computer, and identifies patients with different responses to treatments for UA/NSTEMI. DESIGN, SETTING, AND PATIENTS: Two phase 3, international, randomized, double-blind trials (the Thrombolysis in Myocardial Infarction [TIMI] 11B trial [August 1996-March 1998] and the Efficacy and Safety of Subcutaneous Enoxaparin in Unstable Angina and Non-Q-Wave MI trial [ESSENCE; October 1994-May 1996]). A total of 1957 patients with UA/NSTEMI were assigned to receive unfractionated heparin (test cohort) and 1953 to receive enoxaparin in TIMI 11B; 1564 and 1607 were assigned respectively in ESSENCE. The 3 validation cohorts were the unfractionated heparin group from ESSENCE and both enoxaparin groups. MAIN OUTCOME MEASURES: The TIMI risk score was derived in the test cohort by selection of independent prognostic variables using multivariate logistic regression, assignment of value of 1 when a factor was present and 0 when it was absent, and summing the number of factors present to categorize patients into risk strata. Relative differences in response to therapeutic interventions were determined by comparing the slopes of the rates of events with increasing score in treatment groups and by testing for an interaction between risk score and treatment. Outcomes were TIMI risk score for developing at least 1 component of the primary end point (all-cause mortality, new or recurrent MI, or severe recurrent ischemia requiring urgent revascularization) through 14 days after randomization. RESULTS: The 7 TIMI risk score predictor variables were age 65 years or older, at least 3 risk factors for coronary artery disease, prior coronary stenosis of 50% or more, ST-segment deviation on electrocardiogram at presentation, at least 2 anginal events in prior 24 hours, use of aspirin in prior 7 days, and elevated serum cardiac markers. Event rates increased significantly as the TIMI risk score increased in the test cohort in TIMI 11B: 4.7% for a score of 0/1; 8.3% for 2; 13. 2% for 3; 19.9% for 4; 26.2% for 5; and 40.9% for 6/7 (P<.001 by chi(2) for trend). The pattern of increasing event rates with increasing TIMI risk score was confirmed in all 3 validation groups (P<.001). The slope of the increase in event rates with increasing numbers of risk factors was significantly lower in the enoxaparin groups in both TIMI 11B (P =.01) and ESSENCE (P =.03) and there was a significant interaction between TIMI risk score and treatment (P =. 02). CONCLUSIONS: In patients with UA/NSTEMI, the TIMI risk score is a simple prognostication scheme that categorizes a patient's risk of death and ischemic events and provides a basis for therapeutic decision making. JAMA. 2000;284:835-842
This study was based on TIMI llB trial and the ESSENCE trial. The risk score was derived in a test cohort that included serum cardiac enzymes, both CK MB and troponin. This score was used to

document.doc Page 57 of 77
prognosticate adverse events and death. There were no details as to the times that assays were drawn from onset of chest pain or admission to the emergency department.
Apple(00)Apple, F. S., F. P. Anderson, et al. (2000). "Clinical evaluation of the first medical whole blood, point-of-care testing device for detection of myocardial infarction." Clinical Chemistry 46(10): 1604-9.
Four biochemical markers, creatine kinase (CK)-MB isoenzyme, myoglobin, myosin light chains and troponin I, were studied in 1,338 patients presenting to the emergency department with chest pain suggestive of coronary artery disease (CAD). One hundred and eighty-seven patients had an acute myocardial infarction (MI). At least one of the four markers was over the threshold on the first sample in 78% of MI patients, as compared to only 40% with an elevated CK-MB. After 4 h, 88% had at least one marker elevated. None of the 69 patients with atypical chest pain, no history of CAD, no markers over threshold on the first sample and a normal electrocardiogram had an acute MI or unstable angina. If we had discharged this group, we would have saved USD 264,000, estimating a cost of USD 2,000 per day. Using four biochemical markers improved the early diagnosis of CAD and may help identify groups suitable for early discharge. Copyright 2000 S. Karger AG, Basel
This study looked at comparing 2 different assays. Bloods were drawn at 0, 3 to 6 and then every 3 to 6 hours afterwards. 369 patients with ACS were included. There was no discussion as whether it was consecutive or not. Length of symptoms prior to assay was not revealed. AMI was diagnosed by a modified WHO criteria in that one of the 4 centers at least troponin I was the definitive standard. Analysis was not very good. For most, the peak concentrations over a 24-hour period were used.
Apple(04)Apple, F. S., H. E. Quist, et al. (2004). "Diagnostic and prognostic value of cardiac troponin I assays in patients admitted with symptoms suggestive of acute coronary syndrome." Archives of Pathology & Laboratory Medicine 128(4): 430-4.
CONTEXT: Increasing numbers of patients are presenting to emergency departments with symptoms suggestive of an acute myocardial infarction. OBJECTIVE: To demonstrate the comparative performance of the Ortho Vitros Troponin I and Beckman Access AccuTnI assays used to detect myocardial infarction and to develop risk stratification schemes for all-cause death in patients who presented with myocardial ischemia symptoms that were suggestive of acute coronary syndrome (ACS). DESIGN: The prospective enrollment of patients with ACS and the measurement of serial plasma samples by 2 commercial cardiac troponin I (cTnI) assays. SETTING: A metropolitan medical center that admitted patients with ACS during a 2-month period. PATIENTS: The study population consisted of 200 consecutively admitted patients who presented with symptoms that were suggestive of ACS. RESULTS: Correlation scatterplots showed no significant bias between cTnI assays based on 659 specimens across the dynamic range of each assay. Only minor differences in slopes and intercepts were observed between assays when correlations were based across selected concentration ranges. The receiver operating characteristic curve areas for the detection of myocardial infarction were not significantly different (Ortho,.991; Beckman,.995). At the 99th percentile (Beckman, 0.04 microg/L; Ortho, 0.08 microg/L), each assay demonstrated 100% sensitivity with 78% and 80% specificity, respectively. Kaplan-Meier survival curves and the log-rank test were used to compare time-to-event data. Patients with increased baseline cTnI values had higher odds ratios of death than did those with normal concentrations. For Ortho, the 99th percentile cutoff was 5.9, and the 10% coefficient of variation cutoff was 10.3; for Beckman, the 99th percentile cutoff was 31.4, and the 10% coefficient of variation cutoff was 15.3. CONCLUSIONS: Comparable diagnostic and risk stratification abilities were demonstrated in patients with ACS by the Ortho Vitros and Beckman Access cTnI assays, with no significant analytic bias between cTnI assays.
Serial Tn assays up to 24 hrs post admission usedUsed odds ratio.
Aroney (03)Aroney, C. N., H. L. Dunlevie, et al. (2003). "Use of an accelerated chest pain assessment protocol in patients at intermediate risk of adverse cardiac events.[see comment]." Medical Journal of Australia 178(8): 370-4.

document.doc Page 58 of 77
OBJECTIVE: To determine the feasibility, safety and effectiveness of a structured clinical pathway for stratification and management of patients presenting with chest pain and classified as having intermediate risk of adverse cardiac outcomes in the subsequent six months. DESIGN: Prospective clinical audit. PARTICIPANTS AND SETTING: 630 consecutive patients who presented to the emergency department of a metropolitan tertiary care hospital between January 2000 and June 2001 with chest pain and intermediate-risk features. INTERVENTION: Use of the Accelerated Chest Pain Assessment Protocol (ACPAP), as advocated by the "Management of unstable angina guidelines--2000" from the National Heart Foundation and the Cardiac Society of Australia and New Zealand. MAIN OUTCOME MEASURE: Adverse cardiac events during six-month follow-up. RESULTS: 409 patients (65%) were reclassified as low risk and discharged at a mean of 14 hours after assessment in the chest pain unit. None had missed myocardial infarctions, while three (1%) had cardiac events at six months (all elective revascularisation procedures, with no readmissions with acute coronary syndromes). Another 110 patients (17%) were reclassified as high risk, and 21 (19%) of these had cardiac events (mainly revascularisations) by six months. Patients who were unable to exercise or had non-diagnostic exercise stress test results (equivocal risk) had an intermediate cardiac event rate (8%). CONCLUSIONS: This study validates use of ACPAP. The protocol eliminated missed myocardial infarction; allowed early, safe discharge of low-risk patients; and led to early identification and management of high-risk patients.
This study gives no data on sensitivity or specificity of troponin values at 6-8 hours post admissionAufderheide(01)
Aufderheide, T. P., L. L. Bossaert, et al. (2001). "Cardiopulmonary resuscitation and emergency cardiovascular care. Acute coronary syndromes." Ann Emerg Med 37(4 Suppl): S163-S181.
ReviewBartholomew(04)
Bartholomew, B. A., D. S. Sheps, et al. (2004). "A population-based evaluation of the thrombolysis in myocardial infarction risk score for unstable angina and non-ST elevation myocardial infarction." Clin Cardiol 27(2): 74-8.
BACKGROUND: The Thrombolysis in Myocardial Infarction risk score (TIMI-RS) for unstable angina/non-ST elevation myocardial infarction (MI) was developed in patients presenting with unstable angina accompanied by high-risk features or non-ST elevation MI to determine early risk stratification. HYPOTHESIS: The validity in patients presenting for emergency care with symptoms suggestive of acute coronary syndrome (ACS) has not been well established, and the present study sought to do so by evaluating the TIMI-RS in a prospective fashion. METHODS: A prospective TIMI-RS using seven variables was calculated in 245 patients admitted to the hospital with symptoms suggestive of ACS: (1) age > 65, (2) three or more cardiac risk factors, (3) ST deviation, (4) aspirin use within 7 days, (5) two or more anginal events over 24 h, (6) history of coronary stenosis, and (7) elevated troponin. Patients were contacted at 30 days and data were collected concerning major adverse cardiac events. RESULTS: In patients presenting with chest pain, a higher TIMI-RS was associated with an increase in major adverse cardiac events within 30 days. We found that the 30-day event rate was 0% for a score of 1, 20% for a score of 2, 24% for a score of 3, 42% for a score of 4, 52% for a score of 5, and 70% for a score of 6 or 7 (p < 0.0001). CONCLUSIONS: The TIMI-RS successfully differentiates early risk for major adverse cardiac events in a general population presenting with symptoms suggestive of acute coronary syndrome. A simple bedside calculation of the TIMI-RS provides rapid risk stratification, allowing facilitation of therapeutic decision making in patients with symptoms suggestive of ACS
TIMI-RS study but used Troponins assayed >6 hrs; Odds Ratios used.
Baxt(02)Baxt, W. G., F. S. Shofer, et al. (2002). "A neural network aid for the early diagnosis of cardiac ischemia in patients presenting to the emergency department with chest pain." Annals of Emergency Medicine 40(6): 575-583.
Study objective: Chest pain is the second most common chief complaint presented to the emergency department. Although the causes of chest pain span the clinical spectrum from the trivial to the life threatening, it is often difficult to identify which patients have the most common life-threatening cause, cardiac ischemia. Because of the potential for poor outcome if this diagnosis
document.doc Page 59 of 77
is missed, physicians have had a low threshold for admitting patients with chest pain to the hospital, the vast majority of whom are found not to have cardiac ischemia. In an earlier study with a large chest pain patient registry, an artificial neural network was shown to be able to identify the subset of patients who present to the ED with chest pain who have sustained acute myocardial infarction. The objective of this study was to use the same registry to determine whether a network could be trained accurately to identify the larger subset of patients who have cardiac ischemia. Methods: Two thousand two hundred four adult patients presenting to the ED with chest pain who received an ECG were used to train and test an artificial neural network to recognize the presence of cardiac ischemia. Only the data available at the time of initial patient contact were used to replicate the conditions of real-time evaluation. Forty variables from patient history, physical examination, ECG, and the first set of chemical cardiac marker determinations were used to train and subsequently test the network. The network was trained and tested by using the jackknife variance technique to allow for the network to be trained on as many of the features of the small subset of ischemic patients as possible. Network accuracy was compared with 2 existing aids to the diagnosis of cardiac ischemia, as well as a derived regression model. Results: The network had a sensitivity of 88.1% (95% confidence interval [CI] 84.8% to 91.4%) and a specificity of 86.2% (95% CI 84.6% to 87.7%) for cardiac ischemia despite the fact that a mean of 5% of all required network input data and 41% of cardiac chemical marker data were missing. The network also performed more accurately than the 3 other tested approaches. Conclusion: These data suggest that an artificial neural network might be able to identify which patients who present to the ED with chest pain have cardiac ischemia with useful sensitivities and specificities.
This study looked at 2,204 patients presenting to an ED where a computerized neural network looked at the sensitivity of this network with 40 factors including cardiac enzymes, troponin ,CKMB and CK in diagnosing unstable angina. This was well defined. No mentioned of when in the admission course these enzymes were assayed. Only specific mention was when those enzyme results diagnostic of AMI were removed, the network Sens/Spec fell from 88.1/86.2 to 84.1/80.4.
Bennett (00)Bennett, A. E. and R. L. Bertholf (2000). "Discordant results of CK-MB and troponin I measurements: a review of 14 cases." Annals of Clinical & Laboratory Science 30(2): 167-73.
Case reports Bholasingh (01)
Bholasingh, R., R. J. de Winter, et al. (2001). "Safe discharge from the cardiac emergency room with a rapid rule-out myocardial infarction protocol using serial CK-MB(mass)." Heart (British Cardiac Society) 85(2): 143-8.
OBJECTIVE: To determine whether a new protocol, using a rapid and sensitive CK-MB(mass) assay and serial sampling, can rule out myocardial infarction in patients with chest pain and decrease their length of stay in the cardiac emergency room without increasing risk. DESIGN: The combined incidence of cardiac death and acute myocardial infarction at 30 days, six months, and 24 months of follow up were compared between patients discharged home from the cardiac emergency room after ruling out myocardial infarction with a CK-MB(activity) assay in 1994 and those discharged home after a rapid CK-MB(mass) assay in 1996. SETTING: Cardiac emergency room of a large university hospital. PATIENTS: In 1994 and 1996, 230 and 423 chest pain patients, respectively, were discharged home from the cardiac emergency room with a normal CK-MB and an uneventful observation period. RESULTS: The median length of stay in the cardiac emergency room was significantly reduced, from 16.0 hours in 1994 to 9.0 hours in 1996 (p < 0.0001). Mean event rates in patients from the 1994 and 1996 cohorts, respectively, were 0.9% (95% confidence interval (CI) -0.3% to 2.1%) v 0.7% (95% CI -0.1% to 1. 5%) at 30 days, 3.0% (95% CI 0.8% to 5.2%) v 2.8% (95% CI 1.2% to 4. 4%) at six months, and 7.0% (95% CI 3.7% to 10.3%) v 5.7% (95% CI 3. 5% to 7.9%) at 24 months. Kaplan-Meier survival analysis showed no difference in mean event-free survival at 30 days, six months, and 24 months of follow up. CONCLUSIONS: Using a rule-out myocardial infarction protocol with a rapid and sensitive CK-MB(mass) assay and serial sampling, the length of stay of patients with chest pain in the cardiac emergency room can be reduced without compromising safety.
. There were no sensitivity/ specificity analyses of these end points.

document.doc Page 60 of 77
Bholasingh(03)Bholasingh, R., J. H. Cornel, et al. (2003). "The prognostic value of markers of inflammation in patients with troponin T-negative chest pain before discharge from the emergency department." American Journal of Medicine 115(7): 521-528.
PURPOSE: To assess the prognostic value of markers of inflammation for rule-out purposes in patients admitted to the emergency department with troponin T-negative chest pain. METHODS: Patients presenting to the emergency department within 6 hours of symptom onset and who had a normal or nondiagnostic electrocardiogram were eligible. The standard rule-out protocol, which included serial creatine kinase and creatine kinase-MB measurements, was applied, and markers of inflammation (C-reactive protein, erythrocyte sedimentation rate, and total white blood cell count and differential count) were measured. The study group comprised patients with negative serial troponin T results (<0.06 [mu]g/L) who were discharged home after unstable coronary artery disease was ruled out. Endpoints during the 6-month follow-up were cardiac death, myocardial infarction, or rehospitalization for unstable angina. RESULTS: A total of 382 troponin T-negative patients were discharged, of whom 2 died, 2 had a myocardial infarction, and 7 were rehospitalized for unstable angina. A positive C-reactive protein test result (>0.3 mg/dL) was associated with future clinical events (hazard risk [HR] = 4.5; 95% confidence interval [CI]: 1.2 to 17.0; P = 0.03), as was a positive test (>13 mm/h) for erythrocyte sedimentation rate (HR = 5.6; 95% CI: 1.5 to 22.2; P = 0.01). Patients with positive results for both tests were at highest risk of clinical events (9.3%) compared with patients with other combinations of test results (1.1% to 2.1%; HR = 7.5; 95% CI: 2.2 to 25.5; P = 0.001). CONCLUSION: The combination of C-reactive protein and erythrocyte sedimentation rate had prognostic value in patients with troponin T-negative chest pain and a normal or nondiagnostic electrocardiogram in whom unstable coronary artery disease was ruled out. (C) 2003 by Excerpta Medica Inc.
This study looked at comparing markers of inflammation on troponin T – negative chest pain patients
Caragher(00)Caragher, T. E., B. B. Fernandez, et al. (2000). "Long-term experience with an accelerated protocol for diagnosis of chest pain." Archives of Pathology & Laboratory Medicine 124(10): 1434-9.
CONTEXT: More than 6 million patients present annually with chest pain suggestive of acute coronary syndrome. Rapid and accurate diagnosis is essential for best clinical outcomes, for optimal management of hospital resources, and for minimizing medicolegal exposure. OBJECTIVE: To evaluate the clinical and cost outcomes of an accelerated protocol for chest pain triage in a community-based hospital of moderate size. METHODS: One hundred successive patients with chest pain were diagnosed according to the Traditional Chest Pain Protocol, which included testing of serial blood samples for creatine kinase (CK)-MB and total CK. These patients were also subjected to the Accelerated Chest Pain Protocol under evaluation, which included testing at shortened intervals for myoglobin and cardiac troponin I in addition to CK and CK-MB. Diagnostic sensitivity and specificity were compared versus the final assigned diagnosis. The Accelerated Chest Pain Protocol was implemented for routine use. Follow-up evaluations were conducted at 1 month (test group A, N = 180) and 22 months (test group B, N = 180). Costs for diagnosis and treatment of the 2 test groups were compared with those for the control group. RESULTS: The 2 protocols had equivalent specificity values (99%). The sensitivity of the Accelerated Chest Pain Protocol was higher than that of the Traditional Chest Pain Protocol (95% vs 58%). Cost savings of 29% and a reduction in length of stay of 33% were achieved in test group B versus the control group. CONCLUSIONS: The Accelerated Chest Pain Protocol improved the accuracy and timeliness of diagnosis of acute coronary syndrome while reducing costs.
This study used split sampling and emphasized cost efficiencies with their derived/validated protocolThey used marker assays up to 9 hr., no subset analysis of earlier assays was carried out.
Cassin(02)Cassin, M., F. Macor, et al. (2002). "Management of patients with low-risk chest pain at the time of admission: a prospective study on a non-selected population from the Emergency Department." Italian Heart Journal: Official Journal of the Italian Federation of Cardiology 3(7): 399-405.
This study looked at a 5 month period of 346 patients without obvious ACS and were considered
document.doc Page 61 of 77
low risk 0, 6 and 12 hour CK MB and troponin I levels were evaluated. No sub set analysis was done on the 0 and 6 hour samples and so is not pertinent to my hypotheses.
Choy(03)Choy, J. B., P. W. Armstrong, et al. (2003). "Do cardiac troponins provide prognostic insight in hemodialysis patients?" Canadian Journal of Cardiology 19(8): 907-911.
This study looked at troponin I versus troponin T in hemodyalisis patients prognostic for cardiac events at 30 days and 6 months. Though troponin T was found to be an independent prognostic marker, troponin I was also elevated frequently. No statistical analysis using sensitivity or specificity was carried out.
Christenson(01) Christenson RH, e. a. (2001). "Standardization of cardiac troponin I assays: round robin of ten candidate reference materials." Clin Chem 47(3): 431.
This was a biochemical test looking at standardization of assays.Collinson(00)
Collinson, P., S. Premachandram, et al. (2000). "Prospective audit of incidence of prognostically important myocardial damage in patients discharged from emergency department. ." BMJ 320: 1702 - 1705.
No abstract available Collinson(01)
Collinson, P., F. Boa, et al. (2001). "The measurement of cardiac troponins. ." Ann Clin Biochem.Review
Dadkhah(99)Dadkhah, S., C. Fisch, et al. (1999). "Accelerated coronary reperfusion through the use of rapid bedside cardiac markers--case reports." Angiology 50(1): 55-62.Case reports
Dagnone(00)Dagnone, E., C. Collier, et al. (2000). "Chest pain with nondiagnostic electrocardiogram in the emergency department: a randomized controlled trial of two cardiac marker regimens.[see comment]." CMAJ Canadian Medical Association Journal 162(11): 1561-6.
BACKGROUND: Early detection of acute myocardial infarction (AMI) may save lives. In the emergency setting, it is unclear whether the early use of certain cardiac markers (myoglobin and cardiac troponin I [cTnI]) assists in making appropriate decisions whether to admit or discharge patients with chest pain of possible ischemic cause who have nondiagnostic electrocardiograms (ECGs). We performed a study to determine whether the addition of new cardiac markers in the emergency department results in improved clinical decisions. METHODS: A single-blind randomized controlled trial was conducted between June 1997 and June 1998 in a tertiary care emergency department in Kingston, Ont. Of 296 patients aged 30 years or more who presented to the emergency department with chest pain and nondiagnostic ECGs, 146 were randomly assigned to the intervention group (determination of baseline creatine kinase [CK] level, CK MB fraction and cTnI level, and myoglobin level at baseline and at 2 hours) and 150 to the control group (determination of baseline CK level and CK MB fraction). Outcome measures included the rate of admission to the inpatient cardiology service and length of stay in the emergency department. RESULTS: Of the 296 patients, 34 (11.5%) received a diagnosis of AMI in the emergency department, and 92 (31.1%) had chest pain of noncardiac cause. Patients in the intervention group were less likely than those in the control group to be admitted to the cardiology service (67 [45.9%] v. 81 [54.0%]). The absolute difference in the proportion (8.1% [95% confidence interval -3.3 to 19.5]), although potentially important clinically, was not statistically significant. The length of stay in the emergency department was essentially the same in the 2 study groups. At 30 days, the proportions of patients with a diagnosis of recurrent angina (58.2% in the intervention group and 58.0% in the control group) and AMI (12.3% and 14.7%) were also similar. INTERPRETATION: The optimal cardiac marker panel to be used in the emergency department remains unknown. The addition of serial testing of myoglobin with cTnI confirmation to the standard panel did not substantially change the clinical management or outcomes of patients presenting with chest pain and nondiagnostic ECGs.
No Sens/Spec

document.doc Page 62 of 77
De Winter(00)De Winter, R. J., J. Fischer, et al. (2000). "C-reactive protein and cardiac troponin T in risk stratification: Differences in optimal timing of tests early after the onset of chest pain." Clinical Chemistry 46(10): 1597-1603.
Background: Increased C-reactive protein (CRP) is an important prognostic indicator for early risk stratification in patients with an acute coronary syndrome (ACS), independent of, and in combination with, increased cardiac troponin T (cTnT). However, increases in both cTnT and CRP also occur secondary to myocardial damage. Methods and Results: In 156 consecutive patients, early release kinetics of CRP and cTnT were analyzed. The cutoff values were 3.0 mg/L for CRP and 0.1 (mu)g/L for cTnT. In the 75 patients with a CRP below the cutoff on admission, there was little change in CRP until 8 h after the onset of symptoms. At 12 h after the onset of symptoms, the cumulative proportions of abnormal CRP and cTnT in non-ST elevation ACS patients were 27% and 89%, respectively (P <0.01). During the first 24 h after the onset of symptoms, the median time above the cutoff was 20 h for CRP and 5 h for cTnT (P <0.0001). CRP was below the cutoff on admission significantly more often among patients receiving thrombolytic therapy than in patients without an indication for reperfusion therapy (51% vs 28%; P = 0.004). Conclusions: Increased CRP as an early independent risk indicator should be measured as soon as possible after the onset of symptoms, whereas increased cTnT is most reliable at 12 or more hours after the onset of symptoms. (C) 2000 American Association for Clinical Chemistry.
This study primarily looked at the relationship of C reactive protein to cardiac troponin T in those patients who were diagnosed with coronary artery disease. The earliest assay data was from 12 hr levels(89% of patients presented <6 hrs from symptom onset).
Diderholm(02)Diderholm, E., B. Andren, et al. (2002). "The prognostic and therapeutic implications of increased troponin T levels and ST depression in unstable coronary artery disease: the FRISC II invasive troponin T electrocardiogram substudy." Am Heart J 143(5): 760-7.
BACKGROUND: In unstable coronary artery disease, both increased troponin T level and occurrence of ST-segment depression are associated with a worse prognosis. In the Fast Revascularisation in InStability in Coronary disease trial II invasive study, we evaluated whether the troponin T level, alone and combined with ST depression, identified more severe coronary artery disease or a greater efficacy of an early invasive strategy. METHODS: In the study, 2457 patients with unstable coronary artery disease were randomized to early invasive or noninvasive strategy. Troponin T value and admission electrocardiogram results were available in 2286 patients. RESULTS: In the noninvasive cohort, death or myocardial infarction occurred in 16.6% with troponin T level > or =0.03 microg/L versus 8.5% with troponin T level < 0.03 microg/L (P <.001). In the invasive group, 49% of patients with both ST depression and troponin T level > or =0.03 microg/L had 3-vessel or left main disease compared with 17% if neither finding was present (P <.001). The invasive strategy reduced death/myocardial infarction at 12 months in the cohort with both ST depression and troponin T level > or =0.03 microg/L from 22.1% to 13.2% (risk ratio, 0.60; 95% confidence interval, 0.43 to 0.82; P =.001). In the cohort with either ST depression or troponin T level > or =0.03 microg/L or neither of these findings, the absolute gain of the invasive strategy was smaller and more uncertain. CONCLUSION: Patients with unstable coronary artery disease with the combination of troponin T level > or =0.03 microg/L and ST depression have a poor prognosis and, in half of the cases, 3-vessel or left main disease. In these patients, an early invasive strategy will substantially reduce death/myocardial infarction.
This was a FRISC II sub study looking at baseline troponin T and electrocardiographic changes and outcome at 1 year. The troponin assays on average were 39 hours from the start of chest pain so are irrelevant to my hypotheses.
Edmond(02) Edmond, J. J., J. K. French, et al. (2002). "Prospective evaluation of a chest pain pathway at Green Lane Hospital." New Zealand Medical Journal 115(1158): U103.
AIMS: To prospectively evaluate the efficacy and safety of a chest pain pathway at Green Lane Hospital. METHODS: Between August 1999 and March 2000, patients with non-traumatic chest discomfort considered to be possibly ischaemic were assessed by history, physical examination, baseline electrocardiographic findings and point of care troponin T tests. Those considered not to be high risk entered the pathway which included repeat cardiac markers and electrocardiograms at
document.doc Page 63 of 77
6-8 hours, followed by optional stress testing. The patients were followed for at least one year. RESULTS: Of 423 patients with chest discomfort compatible with myocardial ischaemia, 173 were enrolled in the pathway, with 19 later transferred off the pathway for clinical reasons. Of the remaining 154 patients, the median duration of hospital stay was 17.3 hours [IQR 8.2, 25.1] (median of 13.1 hours for those who did not undergo stress testing); 111 (72%) stayed in hospital for less than 24 hours. There were no readmissions within 30 days with an acute coronary syndrome. In the year following discharge, three patients had a myocardial infarction (one of whom later died) and four died of non-cardiac causes. At one year, freedom from cardiac death or non-fatal myocardial infarction was 98% [95%CI 95,100]. CONCLUSIONS: The chest pain pathway facilitated patient triage and patients had high event-free survival.
Cannot separate Tn from Stress test GroupFleischmann(02) Fleischmann, K. E., L. Goldman, et al. (2002). "Critical pathways for patients with acute chest pain
at low risk." J Thromb Thrombolysis 13(2): 89-96
This study looked at a very low risk population based on previous protocols in a normal CK-MB assay drawn at least 4 hours after pain. Ensued was a 6 hour observation period with stress testing, this was carried out 7 days a week. Those with normal results were sent home and had a 2% major cardiac event in the ensuing 6 months. The upper limit of normal first CK was 5 nanograms per milliliter. 145 patients were triaged. No statistical assay was carried out.
Gibler(03)Gibler, W. B., A. L. Blomkalns, et al. (2003). "Evaluation of chest pain and heart failure in the emergency department: impact of multimarker strategies and B-type natriuretic peptide." Reviews in Cardiovascular Medicine 4(Suppl 4): S47-55.
Review article on evaluation of chest pain.Goodacre(02)
Goodacre, S. W., F. M. Morris, et al. (2002). "A prospective, observational study of a chest pain observation unit in a British hospital." Emergency Medicine Journal 19(2): 117-21.
This article gave no breakdown of cardiac enzymes sensitivity or specificity.Heeschen(99)
Heeschen, C., C. W. Hamm, et al. (1999). "Troponin concentrations for stratification of patients with acute coronary syndromes in relation to therapeutic efficacy of tirofiban. PRISM Study Investigators. Platelet Receptor Inhibition in Ischemic Syndrome Management." Lancet 354(9192): 1757-1762. This troponin concentration for stratification patients with ACS in relationship to therapeutic efficacy of triofidan is not related to my hypothesis.
Henrikson(04)Henrikson, C. A., E. E. Howell, et al. (2004). "Prognostic usefulness of marginal troponin T elevation." American Journal of Cardiology 93(3): 275-9.
Marginal elevations of troponin T among patients with chest pain are often considered to be insignificant. We sought to define the prognostic value of marginal troponin T elevations in patients presenting to the emergency department with suspected myocardial ischemia. Four hundred twenty-eight consecutive patients presenting to the emergency department with ongoing chest pain were evaluated, followed through their hospital course, and contacted for follow-up 4 months after discharge. Two hundred ninety-nine patients had undetectable troponin T levels (<0.01 microg/L), 76 had marginal troponin T elevations (0.01 to 0.09 microg/L), and 53 had frank troponin T elevations (> or =0.1 microg/L). Patients with either marginally or frank elevated troponin levels were older and more likely to be men, but did not differ from patients with undetectable troponin levels with regard to the prevalence of coronary artery disease risk factors, history of coronary disease, or race. While in the hospital, the undetectable and marginal troponin groups were referred for cardiac testing in equal proportions (58% and 59%, respectively), whereas 87% of the elevated group underwent further testing. After adjustment for possible confounders, a significantly increased rate of death/myocardial infarction/revascularization was observed in the marginal troponin group compared with the undetectable troponin group (p = 0.004). Marginal elevations of troponin T identified a currently underevaluated high-risk subgroup of patients with

document.doc Page 64 of 77
suspected myocardial ischemia who are more likely to have adverse clinical outcomes than those with undetectable troponin levels.
This study looked at the prognostic usefulness of marginally elevated troponin levels to prognosticate negative outcomes at around 4 months. The assay used was Roche labs, the threshold level for cardiac disease was greater or equal to 0.1 ug/L and marginal was defined as 0.01 to 0.09 ug/L. The highest value within 24 hours of presentation was utilized.
Ioannidis(01)Ioannides John, P., Deeb Salem, Priscilla W. Chew, Joseph Lau (2001). "Accuracy of Imaging Technologies in the Diagnosis of Acute Cardiac Ischemia in the Emergency Department: A Meta-Analysis." Annals of Emergency Medicine 37(5): 471-77.
This article dealt with imaging technology and not related to my hypothesis.Johnson(99)
Johnson, P. A., L. Goldman, et al. (1999). "Cardiac troponin T as a marker for myocardial ischemia in patients seen at the emergency department for acute chest pain.[see comment]." American Heart Journal 137(6): 1137-44.
This study looked at 2 or more measurements of troponin T during the first 24 hours after presentation; no subset analysis for those obtained in the first 6 hours were assayed.
Kane(00)Kane, G. R., C. B. Keshavamurthy, et al. (2000). "Troponin-T in unstable angina--a clinical and angiographic study." Journal of the Association of Physicians of India 48(11): 1074-7
This study dealt with ICU patients. No time from arrival from ED to assay or onset of pain to assay was given. No sensitivity or specificity.
Kirk(00)Kirk, J. D., D. B. Diercks, et al. (2000). "Evaluation of chest pain suspicious for acute coronary syndrome: use of an accelerated diagnostic protocol in a chest pain evaluation unit." American Journal of Cardiology 85(5A): 40B-48B; discussion 49B.
Management of patients presenting to the emergency department with chest pain suggestive of acute myocardial infarction (AMI) remains a continuing challenge. A low threshold for admission has been traditional because of concern for patient welfare and the litigation potential associated with the inadvertent discharge of patients with ischemic events. Because of this approach, < 30% of patients admitted for chest pain ultimately are found to have an acute coronary syndrome. To reduce unnecessary admissions, maintain patient safety, and enhance cost-effectiveness, innovative strategies have been applied to the management of patients with chest pain. It is now recognized that a low-risk group can be identified by the clinical presentation and initial electrocardiogram. Chest-pain centers have been developed to provide further risk stratification and systematic management of these patients. We employ an accelerated diagnostic protocol based on immediate exercise treadmill testing to evaluate low-risk patients. Moderate-risk patients are assessed over a 6-hour observation period with serial electrocardiograms and evaluation of cardiac-injury markers. Patients with positive evaluations are admitted. Those with negative results undergo either exercise echocardiography or rest myocardial perfusion imaging utilizing technetium-99m sestamibi. Patients with positive functional tests are admitted. Those with negative studies are discharged with outpatient follow-up. These strategies have provided a safe and accurate means of patient disposition from the emergency department with the potential for vital cost savings. [References: 69]
Descriptive Kleiman(02)
Kleiman, N. S., N. Lakkis, et al. (2002). "Prospective analysis of creatine kinase muscle-brain fraction and comparison with troponin T to predict cardiac risk and benefit of an invasive strategy in patients with non-ST-elevation acute coronary syndromes." Journal of the American College of Cardiology 40(6): 1044-1050.
OBJECTIVES: We sought to determine whether elevation of plasma creatine kinase muscle-brain fraction (CK-MB) would be useful to triage patients with acute coronary syndromes (ACS) to early angiography/revascularization. BACKGROUND: It is unknown whether the measurement of CK-

document.doc Page 65 of 77
MB is effective for triage to an aggressive management strategy. METHODS: Patients in the Treat Angina With Aggrastat and Determine Cost of Therapy With an Invasive or Conservative Strategy (TACTICS-TIMI) 18 study received aspirin, heparin, and tirofiban for treatment of ACS, were randomized to an invasive or a conservative strategy (angiography/revascularization between 4 and 48 h), and were followed up for a composite end point of death, myocardial infarction, or rehospitalization for ACS. RESULTS: Of 2,220 patients, CK-MB was elevated in 826 (37%). Of the patients with negative CK-MB, troponin T was elevated in 361 (31.2%). Event rates at 30 and 180 days were twice as high in patients with elevated CK-MB than in patients without elevated CK-MB. Both groups had similar benefit from an invasive strategy; there was no evidence of interaction between CK-MB elevation and strategy on the composite end point at 30 or 180 days. When patients were stratified according to both CK-MB and troponin status, there was evidence of a benefit in the invasive strategy among patients who were CK-negative but troponin-positive (odds ratios [95% confidence interval]:0.13 [0.04 to 0.39] at 30 days and 0.29 [0.16 to 0.52] at 180 days). CONCLUSIONS: Patients with minimal amounts of recent onset myonecrosis but elevated risk as indicated by CK-MB and troponin, respectively, benefit most from invasive management. Determination of troponin levels yielded significant information regarding triage to an invasive strategy particularly in CK-MB-negative patients. (C) 2002 by the American College of Cardiology Foundation.
This study looked at TACTICS-TIMI 18. Criteria for entry included ischemic chest pain, and history of coronary artery disease or EKG ischemic changes other than ST elevation, or an elevation of CK-MB or troponin. There is no specific time defined when these assays were drawn post arrival to the ED. Only after this time was randomization carried out and further assay done Q8H. Therefore I believe the results are not strictly addressing my hypothesis .
Kontos(00)Kontos, M. C., F. P. Anderson, et al. (2000). "Ability of troponin I to predict cardiac events in patients admitted from the emergency department.[comment][erratum appears in J Am Coll Cardiol 2001 Mar 1;37(3):973]." Journal of the American College of Cardiology 36(6): 1818-23.
Rejected because cumulative 8 hr assays were analyzed.Kontos(98)
Kontos, M. C., J. A. Arrowood, et al. (1998). "Early echocardiography can predict cardiac events in emergency department patients with chest pain." Ann Emerg Med 31(5): 550-7
ECHOKontos (04)
Kontos, M. C., R. Shah, et al. (2004). "Implication of different cardiac troponin I levels for clinical outcomes and prognosis of acute chest pain patients." Journal of the American College of Cardiology 43(6): 958-65.
24 hr assays onlyLateef(01)
Lateef, F., A. B. Storrow, et al. (2001). "Heart emergency room: effective for both geriatric and younger patients." Singapore Medical Journal 42(6): 259-63.
Though this article accumulated CK-MB values at 0, 3, 6, and 9 hours, there was no analysis of these figures.
Lee(01)Lee, J. S., M. Gatien, et al. (2001). "Slic: stat lactate in chest pain for the early detection of acute myocardial infarction." Academic Emergency Medicine 8(5).
This article compared stat lactate levels to troponin I in the diagnoses of AMI. Small numbers, abstract only
Lindahl(01)Lindahl, B., E. Diderholm, et al. (2001). "Mechanisms behind the prognostic value of troponin T in unstable coronary artery disease: a FRISC II substudy." J Am Coll Cardiol 38(4): 979-86.
OBJECTIVES: This study was designed to elucidate possible mechanisms for the prognostic value of troponin T (tnT). BACKGROUND: The reasons for the adverse

document.doc Page 66 of 77
prognosis associated with elevation of troponins in unstable coronary artery disease are poorly understood. METHODS: Patients enrolled in the Fast Revascularization during InStability in CAD (FRISC-II) trial were included. Clinical characteristics, findings at echocardiography and coronary angiography, and prognosis were evaluated in relation to different tnT levels. RESULTS: Absence of significant coronary stenosis was more frequent and three-vessel disease or left main stem stenosis was less frequent in patients without, compared with, detectable tnT. The occurrence of visible thrombus increased with rising levels of tnT. In the group with the highest levels of tnT, occlusion of the left circumflex artery was more common than in the three other tnT groups, as was a left ventricular ejection fraction below 0.45. The one-year risk of death in the noninvasive arm of the study increased by increasing levels of tnT (1.6% to 4.6%), whereas the risk of myocardial infarction showed an inverted U-shaped curve and was lower in the lowest (5.5%) and highest (8.4%) tnT groups than in the two intermediate groups (17.5% and 16.2%). CONCLUSIONS: Any detectable elevation of tnT raises the probability of significant coronary stenosis and thrombus formation and is associated with an increased risk of reinfarction and death. However, at a more pronounced elevation of troponin, a higher proportion of patients has a persistent occlusion of the culprit vessel and reduced left ventricular function, associated with a high mortality but a modest risk of reinfarction.
This was a FRISC II sub study with prospective multi centre trial with 2,457 patients looking at the relationship of the 38.6 hours from the last episode of chest pain troponin T assay and echo and coronary angiogram results.
Manini(02)Manini, A. F., M. A. Gisondi, et al. (2002). "Adverse cardiac events in emergency department patients with chest pain six months after a negative inpatient evaluation for acute coronary syndrome." Academic Emergency Medicine 9(9): 896-902.
No statistical analysis using sensitivity or specificity. Mant(04)
Mant, J., McManus, R. J., Oakes, R. A., Delaney, B. C., Barton, P. M., Deeks, J. J., et al. (2004). Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care. Health Technology Assessment (Winchester, England), 8(2), iii, 1-158.
OBJECTIVES: To ascertain the value of a range of methods - including clinical features, resting and exercise electrocardiography, and rapid access chest pain clinics (RACPCs) - used in the diagnosis and early management of acute coronary syndrome (ACS), suspected acute myocardial infarction (MI), and exertional angina. DATA SOURCES: MEDLINE, EMBASE, CINAHL, the Cochrane Library and electronic abstracts of recent cardiological conferences. REVIEW METHODS: Searches identified studies that considered patients with acute chest pain with data on the diagnostic value of clinical features or an electrocardiogram (ECG); patients with chronic chest pain with data on the diagnostic value of resting or exercise ECG or the effect of a RACPC. Likelihood ratios (LRs) were calculated for each study, and pooled LRs were generated with 95% confidence intervals. A Monte Carlo simulation was performed evaluating different assessment strategies for suspected ACS, and a discrete event simulation evaluated models for the assessment of suspected exertional angina. RESULTS: For acute chest pain, no clinical features in isolation were useful in ruling in or excluding an ACS, although the most helpful clinical features were pleuritic pain (LR+ 0.19) and pain on palpation (LR+ 0.23). ST elevation was the most effective ECG feature for determining MI (with LR+ 13.1) and a completely normal ECG was reasonably useful at ruling this out (LR+ 0.14). Results from 'black box' studies of clinical interpretation of ECGs found very high specificity, but low sensitivity. In the simulation exercise of management strategies for suspected ACS, the point of care testing with troponins was cost-effective. Pre-hospital thrombolysis on the basis of ambulance telemetry was more effective but more costly than if performed in hospital. In cases of chronic chest pain, resting ECG features were not found to be very useful (presence of Q-waves had LR+ 2.56). For an exercise ECG, ST depression performed only moderately well (LR+ 2.79 for a 1 mm cutoff), although this did improve for a 2 mm cutoff (LR+ 3.85). Other methods of interpreting the exercise ECG did not result in dramatic improvements in these results. Weak evidence was found to suggest that RACPCs may be associated with reduced admission to hospital of patients with non-cardiac pain, better recognition of ACS, earlier specialist assessment of exertional angina and earlier diagnosis of non-cardiac chest pain. In a simulation exercise of models of care for investigation of suspected exertional angina,

document.doc Page 67 of 77
RACPCs were predicted to result in earlier diagnosis of both confirmed coronary heart disease (CHD) and non-cardiac chest pain than models of care based around open access exercise tests or routine cardiology outpatients, but they were more expensive. The benefits of RACPCs disappeared if waiting times for further investigation (e.g. angiography) were long (6 months). CONCLUSIONS: Where an ACS is suspected, emergency referral is justified. ECG interpretation in acute chest pain can be highly specific for diagnosing MI. Point of care testing with troponins is cost-effective in the triaging of patients with suspected ACS. Resting ECG and exercise ECG are of only limited value in the diagnosis of CHD. The potential advantages of RACPCs are lost if there are long waiting times for further investigation. Recommendations for further research include the following: determining the most appropriate model of care to ensure accurate triaging of patients with suspected ACS; establishing the cost-effectiveness of pre-hospital thrombolysis in rural areas; determining the relative cost-effectiveness of rapid access chest pain clinics compared with other innovative models of care; investigating how rapid access chest pain clinics should be managed; and establishing the long-term outcome of patients discharged from RACPCs. [References: 244]
Did not pertain to cardiac enzymesMcCullough(02)(A)
McCullough, P. A., R. M. Nowak, et al. (2002). "Emergency evaluation of chest pain in patients with advanced kidney disease." Archives of Internal Medicine 162(21): 2464-8.
CK-MB were assayed but not used to conclude any results. McCullough(02)(B)
McCullough, P. A., R. M. Nowak, et al. (2002). "Performance of multiple cardiac biomarkers measured in the emergency department in patients with chronic kidney disease and chest pain." Academic Emergency Medicine 9(12): 1389-96.
OBJECTIVES: Measurements of myoglobin and creatine kinase (CK)-MB isoforms have been suggested to be sensitive tests for the early diagnosis of myocardial infarction (MI). We have investigated the utility of myoglobin, creatine kinase (CK)-MB isoforms and creatine kinase MB mass (CK-MBm) in early diagnosis of MI using cardiac troponin T (cTnT) positivity as a reference. DESIGN AND METHODS: The study population comprised 440 patients who had had chest pain for less than 12 h. Patients were divided into cTnT negative (cTnT-) or cTnT positive (cTnT+) patients (concentration of cTnT >0.1 microg/L at two different time points during 72 h). RESULTS: At the time of admission to the emergency department receiver operating characteristics (ROC) curves of CK-MB isoforms and CK-MBm were not better than that of myoglobin. Six hours after admission CK-MB isoforms and CK-MBm provided statistically significantly larger areas under the curve (AUC) than myoglobin (p < 0.01). When ROC curves were related to the onset of chest pain (< 3 h, 3-6 h, and > 6 h) there were no significant differences between the cardiac markers studied. CONCLUSIONS: According to the present findings, CK-MB isoforms or myoglobin offer no advantage over CK-MBm as early markers of myocardial infarction. Copyright 2002 The Canadian Society of Clinical Chemists
This study looked at the use of biochemical markers including troponin T CK-MB and myoglobin in the assessment of patients with known kidney disease and chest pain presentation ischemic symptoms or ST segment elevation on EKG. The looked at an outcome of AMI that necessitated a rise in CK-MB knowing full well that this value would go up in renal disease. They had a very large Afro American population (81.3% of 808 patients). Their assays included times 0, 1.5, 3 and 9 hours. They did not break down the data into smaller time periods, but only looked at the summation data.
McErlean(00)McErlean, E. S., S. A. Deluca, et al. (2000). "Comparison of troponin T versus creatine kinase-MB in suspected acute coronary syndromes." American Journal of Cardiology 85(4): 421-6.
Limitations of creatine kinase-MB (CK-MB) have led to alternative biochemical markers, including troponin T (TnT), to detect myocardial necrosis. Limited data are available regarding the predictive value of this new marker in patients with chest pain of uncertain etiology. Therefore, we prospectively compared CK-MB and TnT in a broad population with suspected acute coronary syndromes, including those admitted to a short-stay chest pain unit. CK-MB, quantitative TnT levels, and a rapid bedside assay were performed at 0, 4, 8, and 16 hours. Adverse events, including infarction, recurrent ischemia, coronary surgery, need for catheterization and/or intervention,
document.doc Page 68 of 77
stroke, congestive heart failure, or death, were identified by chart review and by follow-up phone call at 6 months. Of 707 patients, 104 were excluded for creatinine >2 mg/dl or incomplete data, leaving a total cohort of 603 patients. Coronary Care Unit admissions were 18%, intermediate care admissions were 14%, telemetry admissions is 21%, and admissions to 24-hour short-stay area were 47%. TnT (at 0.1 ng/ml) and CK-MB were positive in a similar proportion of patients (20.4% and 19.7%, respectively); however, the patients identified by TnT and CK-MB were not identical. In-hospital adverse events occurred in 37.1% with no differences in positive predictive value for the markers (p = NS). If CK-MB and TnT were negative, the early adverse event rate was 27%. No cardiac marker was positive by 16 hours in 54.9% of patients with an adverse event. Six-month follow-up was obtained in 576 of the 603 patients (95.5%). One hundred fifty-five late adverse events occurred in 134 patients (23.3%) at an average of 3.3+/-2.5 months after discharge. If both markers were negative, the late event rate was 20.2% and did not increase in patients with positive CK-MB or TnT >0.2 ng/ml. However, the late event rate was substantially higher (52.9%) in those with intermediate TnT levels of 0.1 to 0.2 ng/ml (p = 0.002). Thus, TnT is a suitable alternative to CK-MB in patients with suspected acute coronary syndromes. The rapid bedside assay is comparable to quantitative TnT and may enable early diagnosis and triage. A negative cardiac marker value (TnT or CK-MB) does not necessarily confer a low risk of complication in patients presenting with acute chest pain to an emergency department.
This study could not be applied to my hypothesis. This is because samples were done at 0, 4, 8 and 16 hours post presentation. However, this group was not divided into 0, 4 hours for sensitivity or specificity.
Melanson(04)Melanson, S. F., E. L. Lewandrowski, et al. (2004). "Reevaluation of myoglobin for acute chest pain evaluation: Would false-positive results on 'first-draw' specimens lead to increased hospital admissions?" American Journal of Clinical Pathology 121(6): 804-808.
Myoglobin is an early marker of cardiac injury, although positive results occur in the absence of cardiac myonecrosis. We studied data for 537 patients admitted to the emergency department with symptoms suggestive of myocardial injury who underwent testing for troponin I (TnI), creatine kinase isoenzyme (CK-MB), and myoglobin at the point of care. Physicians were blinded to the myoglobin results. Myoglobin had a sensitivity of 69.7% and a negative predictive value of 97.4% for the diagnosis of acute coronary syndrome (ACS) on 'first-draw' specimens. Receiver operating characteristic curve analysis suggested that myoglobin demonstrated optimal sensitivity for ACS, while TnI had optimal specificity. CK-MB was neither the most specific nor the most sensitive marker. More than 80% of the patients with false-positive myoglobin results were admitted to the hospital. These data invalidate concerns regarding the putative overtreatment effect of false-positive cases owing to myoglobin results. Furthermore, our data suggest that myoglobin is superior to CK-MB as an adjunct to TnI.
This study looked at triple marker point of care assay diagnosis of AMI and unstable angina these endpoint references were taken from discharged diagnosis. There was no further definition of how these standards were acquired.
Meyer(98)Meyer, T., L. Binder, et al. (1998). "Superiority of combined CK-MB and troponin I measurements for the early risk stratification of unselected patients presenting with acute chest pain." Cardiology 90(4): 286-94.
This well designed study presented odds ratios and so was rejected.
Morrow(01) Morrow, D. A., C. P. Cannon, et al. (2001). "Ability of minor elevations of troponins I and T to predict benefit from an early invasive strategy in patients with unstable angina and non-ST elevation myocardial infarction: results from a randomized trial." Jama 286(19): 2405-12.
CONTEXT: Cardiac troponins I (cTnI) and T (cTnT) are useful for assessing prognosis in patients with unstable angina and non-ST-segment elevation myocardial infarction (UA/NSTEMI). However, the use of cardiac troponins for predicting benefit of an invasive vs conservative strategy in this patient population is not clear. OBJECTIVE: To prospectively test whether an early invasive strategy provides greater benefit than a

document.doc Page 69 of 77
conservative strategy in acute coronary syndrome patients with elevated baseline troponin levels. DESIGN: Prospective, randomized trial conducted from December 1997 to June 2000. SETTING: One hundred sixty-nine community and tertiary care hospitals in 9 countries. PARTICIPANTS: A total of 2220 patients with acute coronary syndrome were enrolled. Baseline troponin level data were available for analysis in 1821, and 1780 completed the 6-month follow-up. INTERVENTIONS: Patients were randomly assigned to receive (1) an early invasive strategy of coronary angiography between 4 and 48 hours after randomization and revascularization when feasible based on coronary anatomy (n = 1114) or (2) a conservative strategy of medical treatment and, if stable, predischarge exercise tolerance testing (n = 1106). Conservative strategy patients underwent coronary angiography and revascularization only if they manifested recurrent ischemia at rest or on provocative testing. MAIN OUTCOME MEASURE: Composite end point of death, MI, or rehospitalization for acute coronary syndrome at 6 months. RESULTS: Patients with a cTnI level of 0.1 ng/mL or more (n = 1087) experienced a significant reduction in the primary end point with the invasive vs conservative strategy (15.3% vs 25.0%; odds ratio [OR], 0.54; 95% confidence interval [CI], 0.40-0.73). Patients with cTnI levels of less than 0.1 ng/mL had no detectable benefit from early invasive management (16.0% vs 12.4%; OR, 1.4; 95% CI, 0.89-2.05; P<.001 for interaction). The benefit of invasive vs conservative management through 30 days was evident even among patients with low-level (0.1-0.4 ng/mL) cTnI elevation (4.4% vs 16.5%; OR, 0.24; 95% CI, 0.08-0.69). Directionally similar results were observed with cTnT. CONCLUSION: In patients with clinically documented acute coronary syndrome who are treated with glycoprotein IIb/IIIa inhibitors, even small elevations in cTnI and cTnT identify high-risk patients who derive a large clinical benefit from an early invasive strategy.
This very important study showed even minor elevations of troponin were significant for 30 day and 6-month adverse events. This paper will be analyzed by the Reviewers of IIb/IIIa inhibitors.
Newby(01)Newby LK, S. A., Gibler WB, et al: (2001). "Bedside multimarker testing for risk stratification in chest pain units: The chest pain evaluation by creatine kinase-MB, myoglobin, and troponin I (CHECKMATE) study." Circulation 103(14): 1832-7.
This study primarily looked at triple assay markers “myoglobin, CK-MB and troponin I” versus double marker assay “CK-MB troponin I” at times 0, 3, 6, 9 to 12, and 16 to 24 hours after admission with regard to 30 day mortality in infarction. Median duration of symptoms to presentation was 3.3 hrs. A sub analysis revealed that the triple marker therapy became positive sooner than the double marker therapy (2.5 hours versus 2.8 hours T value 0.023). The problem I have is that the study population was fractured in that some patients were sent home after 6 hours with no protocol described, and no justification as to why it was done and therefore a large proportion of the population did not get the full series of assays. Used only Odds Ratios
Noeller (03)Noeller, T. P., Meldon, S. W., Peacock, W. F., Emerman, C. L., McErlean, E. S., Vanlente, F., et al. (2003). Troponin T in elders with suspected acute coronary syndromes. Am J Emerg Med, 21(4), 293-297.
Troponin T (TnT) elevations (> or =0.1 ng/mL) indicate an increased risk of adverse outcomes in patients with acute coronary syndromes (ACS). There is little data on the prognostic significance of TnT in elders with ACS. We sought to define the ability of TnT to predict adverse outcomes in elders with suspected ACS compared with the younger cohort. This is a nested cohort study of patients aged <65 and > or =65 years with suspected ACS. Serial ECGs, CKMB and TnT assays were obtained at presentation and 4, 8, and 16 hours later. Adverse outcomes at hospital discharge included death, nonfatal myocardial infarction, coronary artery bypass grafting, and positive cardiac catheterization. A total of 695 patients were enrolled. A total of 301 (48%) were aged 65 or older. Although there was no difference in TnT sensitivity between the younger and older cohorts, there was a difference in specificity, 94% versus 83% (P <.01), respectively. In both cohorts, renal insufficiency was associated with a significantly lower TnT specificity. In both elders and younger patients with abnormal renal function, low TnT specificity warrants careful consideration of this marker as the sole criterion for aggressive medical management.

document.doc Page 70 of 77
Rejected; Used 16 hour Troponin AssayNovis(04)
Novis, D. A., B. A. Jones, et al. (2004). "Biochemical Markers of Myocardial Injury Test Turnaround Time: A College of American Pathologists Q-Probes Study of 7020 Troponin and 4368 Creatine Kinase-MB Determinations in 159 Institutions." Archives of Pathology & Laboratory Medicine 128(2): 158-164.
UnrelatedO’Rourke(01)
O'Rourke, R. A., J. S. Hochman, et al. (2001). "New approaches to diagnosis and management of unstable angina and non-ST-segment elevation myocardial infarction." Arch Intern Med 161(5): 674-82.
ReviewObrador(03)
Obrador, D. and M. Santalo (2003). "Evaluation of patients with suspected acute coronary syndromes in the emergency department." Nuclear Medicine Communications 24(10): 1041-8.
Review article
Ornato(01)Ornato, J. P., Selker, H. P., & Zalenski, R. J. (2001). Overview: diagnosing acute cardiac ischemia in the emergency department. A report from the National Heart Attack Alert Program. Ann Emerg Med, 37(5), 450-452.
ReviewPanteghini(02).
Panteghini, M. (2002). "Acute coronary syndrome: biochemical strategies in the troponin era. [Review] [69 refs]." Chest 122(4): 1428-35.
ReviewPatti(04)
Patti, G., A. D'Ambrosio, et al. (2004). "Early interleukin-1 receptor antagonist elevation in patients with acute myocardial infarction." Journal of the American College of Cardiology 43(1): 35-8.
Used inflammatory markers.Peacock(01) Peacock, W. F., C. L. Emerman, et al. (2001). "Normal CK, elevated MB predicts complications in
acute coronary syndromes." Journal of Emergency Medicine 20(4): 385-90.
CORONARY REVASCULARIZATION: PTCA in patients with refractory unstable angina is associated with a substantial risk of the following complications: death, myocardial infarction, need for emergency surgery, and restenosis. The introduction of intracoronary stents, however, has improved both short-term and long-term outcomes. The newer adjunctive pharmacologic therapies enhance even further the benefits associated with the use of stents. The decision regarding the specific revascularization procedure to be used (e.g., CABG, PTCA, stent placement, or atherectomy) is based on the coronary anatomy, the left ventricular function, the experience of the medical and surgical personnel, the presence or absence of coexisting illnesses, and the preferences of both the patient and the physician. RISK STRATIFICATION: Among patients with unstable angina or non-Q-wave myocardial infarction, there is an increased risk of death within 6 weeks in those with elevated troponin I levels and the risk of death continues to increase as the troponin level increases. Reversible ST segment depression is associated with an increase by a factor of 3-6 in the likelihood of death, myocardial infarction, ischemia at rest, or provocable ischemia during a test to stratify risk. Exercise or pharmacologic stress testing provides important information about a patient's risk. Although the conditions of the majority of patients with unstable angina will stabilize with effective antiischemic medications, approximately 50-60% of such patients will require coronary angiography and revascularization because of the "failure" of medical therapy. High-risk patients are those who have had angina at rest, prolonged angina, or persistent angina with dynamic ST segment changes or hemodynamic instability, and they urgently require simultaneous invasive evaluation and treatment. Medical therapy should be adjusted rapidly to relieve manifestations of ischemia and should include antiplatelet therapy (aspirin, or ticlopidine or clopidogrel if aspirin is

document.doc Page 71 of 77
contraindicated), antithrombotic therapy (unfractionated heparin or low-molecular-weight heparin), beta-blockers, nitrates, and possibly calcium-channel blockers. Early administration of glycoprotein IIb/IIIa inhibitors may be particularly important, especially in high-risk patients with positive troponin tests or those in whom implantation of coronary stents is anticipated. [References: 46]
This prospective study looked at comparing CK values with MB values over 0, 8 and 16 hours post presentation. The analysis did not isolate the early assays. Therefore one cannot apply this to my hypothesis
Peacock(03)Peacock, W. F., C. E. Emerman, et al. (2003). "Retrospective review: the incidence of non-ST segment elevation MI in emergency department patients presenting with decompensated heart failure." Congestive Heart Failure 9(6): 303-8.
The authors performed a 6-month review of heart failure patients presenting to a teaching hospital emergency department to determine the rate of positive serum myocardial infarction markers. All patients with an emergency department discharge diagnosis of heart failure were included; those with a creatinine level >2.0 mg/dL were excluded. There were 151 patients who met the entry criteria, with a mean age of 68.6 +/- 13.6 years, and 84 (56%) were men. The mean ejection fraction was 32%, and the mean Framingham score was 3.8 +/- 1.6. Twenty (14%) had positive markers. Troponin T was positive in 17 (11%), and creatine kinase was positive in nine (6%). Both markers were positive in six (4%). Chest pain was absent in 70% of the positive marker group. The authors conclude that elevated cardiac markers are not rare in decompensated heart failure. These pilot data suggest these tests should be routinely obtained on heart failure patients.
No correlation with any reference standard for AMI; no sensitivity/specificityPolanczyk(98) Polanczyk, C. A., T. H. Lee, et al. (1998). "Cardiac troponin I as a predictor of major cardiac
events in emergency department patients with acute chest pain.[see comment]." Journal of the American College of Cardiology 32(1): 8-14.
OBJECTIVES: We sought to evaluate the diagnostic and prognostic value of cardiac troponin I (cTnI) in emergency department (ED) patients with chest pain. BACKGROUND: Although cTnI has been shown to correlate with an increased risk for complications in patients with unstable angina, the prognostic significance of this assay in the heterogeneous population of patients who present to the ED with chest pain is unclear. METHODS: cTnI and creatine kinase-MB fraction (CK-MB) mass concentration were collected serially during the first 48 h from onset of symptoms in 1,047 patients > or =30 years old admitted for acute chest pain. Sensitivity, specificity and receiver operating characteristic curves were calculated for cTnI and CK-MB collected in the first 24 h. RESULTS: The sensitivity, specificity and positive predictive value of cTnI for major cardiac events were 47%, 80% and 19%, respectively. Among patients were who ruled out for myocardial infarction, cTnI was elevated in 26% who had major cardiac complications compared with 5% for CK-MB; the positive predictive value for an abnormal cTnI result was 8%. Elevated cTnI in the presence of ischemia on the electrocardiogram was associated with an adjusted odds ratio of 1.8 (95% confidence interval 1.1 to 2.9) for major cardiac events within 72 h. Among patients without a myocardial infarction or unstable angina, cTnI was not an independent correlate of complications. CONCLUSIONS: In patients presenting to the ED with acute chest pain, cTnI was an independent predictor of major cardiac events, However, the positive predictive value of an abnormal assay result was not high in this heterogeneous cohort.
This study used the same population as his earlier study. He looked at troponin I being a predictor for major cardiac outcome events with 72 hours of admission. Of relevance, he sampled on admission, 8 hours and then 16 and 24 hours for both troponin I and CK (upper limit was 1.5 nanograms per milliliter for troponin I and 5 nanograms per milliliter for CK-MB
Pope(03)Pope, J. H. and H. P. Selker (2003). "Diagnosis of acute cardiac ischemia." Emergency Medicine Clinics of North America 21(1): 27-59.
ReviewRahimi(03)
Rahimi, A. R., P. M. Marzano, 3rd, et al. (2003). "Evaluation of lactate and C-reactive protein in

document.doc Page 72 of 77
the assessment of acute myocardial infarction." Southern Medical Journal 96(11): 1107-12.
Evaluated serum lactate levels.Ridker(00)
Ridker, P. M., C. H. Hennekens, et al. (2000). "C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women." N Engl J Med 342(12): 836-43.
Not relatedRoppolo(99)
Roppolo, L. P., R. Fitzgerald, et al. (1999). "A comparison of troponin T and troponin I as predictors of cardiac events in patients undergoing chronic dialysis at a Veteran's Hospital: a pilot study." J Am Coll Cardiol 34(2): 448-454.
OBJECTIVE: The purpose of this study was to prospectively evaluate the usefulness of the cardiac troponins as predictors of subsequent cardiac events in patients with chronic renal failure undergoing dialysis. BACKGROUND: Cardiac troponin T (cTnT) and I (cTnI) are cardiac markers that are specific for cardiac muscle. They are also excellent prognostic indicators for patients presenting with chest pain. Although cardiac disease is the leading cause of death in dialysis patients, standard methods to diagnose acute coronary syndromes in patients with renal failure are often misleading. METHODS: A six-month prospective study was done in a university-affiliated Veterans Hospital's dialysis clinic. Forty-nine patients undergoing chronic dialysis with no complaints of chest pain were followed for cardiac events occurring in the six months after cardiac troponin measurements. These included unstable angina, acute myocardial infarction and cardiac death. An additional 83 patients with renal failure but who were not undergoing dialysis were also examined. RESULTS: Within six months all three dialysis patients with elevated cTnI at entry into the study suffered an adverse complication (specificity and positive predictive value = 100%). Twenty-five patients had cTnT elevated at >0.10 ng/ml (53%). Patients with diabetes were more likely to have elevated troponin T levels (64% vs. 25%, p = 0.01). All six patients developing cardiac events within three months had elevations of cTnT >0.1 ng/ml (sensitivity = 100%). Whereas the specificity of cTnT was only 56% for a near-term cardiac event, the negative predictive value of cTnT using a cutoff of ^ or = 0.1 ng/ml was 100%. On restratifying patients using a cutoff value of cTnT of >0.2 ng/ml, only nine of 49 dialysis patients (18%) had elevated levels. In patients with renal failure not undergoing dialysis, only three of 83 (4%) had elevated troponin I or T. None of these patients suffered a cardiac event in the next six months. CONCLUSIONS: This prospective pilot study clearly delineates the troponins as important prognosticators in asymptomatic otherwise "stable" patients on chronic dialysis, especially those with concomitant diabetes mellitus. It also appears that troponins are more likely to be elevated in dialysis patients than other patients with renal failure not on dialysis. The above suggests that the combination of cTnI and cTnT might be very effective in elucidating cardiac risks of patients with renal failure undergoing chronic dialysis.
This study looked at asymptomatic non-cardiac patients with renal failure with or without dialysis with or without diabetes. Random troponin T and troponin I assays were done on these patients and then used to prognosticate cardiac events in the following 6 month. Though not relevant at strictly speaking to my hypothesis it does show the high prevalence of troponin elevation in this subset of patients.
Ryan(02)Ryan, T. J. and R. M. Melduni (2002). "Highlights of latest American College of Cardiology and American Heart Association Guidelines for Management of Patients with Acute Myocardial Infarction." Cardiology in Review 10(1): 35-43.
GuidelinesSanchis(03)
Sanchis, J., V. Bodi, et al. (2003). "Predictors of short-term outcome in acute chest pain without ST-segment elevation." International Journal of Cardiology 92(2-3): 193-199.
This study looked primarily at low risk population for chest pain that under went stress testing. It used a troponin value of 12 hours after onset of pain. It found a sensitivity of 58% and specificity of 63% in predicting compositeof angina, AMI, or cardiac death.

document.doc Page 73 of 77
Sarko(02)Sarko, J. and C. V. Pollack, Jr. (2002). "Cardiac troponins. [Review] [110 refs]." Journal of Emergency Medicine 23(1): 57-65.
ReviewSelker(98)
Selker, H. P., J. R. Beshansky, et al. (1998). "Use of the acute cardiac ischemia time-insensitive predictive instrument (ACI-TIPI) to assist with triage of patients with chest pain or other symptoms suggestive of acute cardiac ischemia. A multicenter, controlled clinical trial." Annals of Internal Medicine 129(11): 845-55.
This computer generated model incorporated CKMB values as 1 of many variables looking at utilization issues. One could not tease out enzymes in isolation.
Serebruany(01)Serebruany, V. L., D. J. Levine, et al. (2001). "Usefulness of combining necrosis and platelet markers in triaging patients presenting with chest pain to the emergency department." Journal of Thrombosis & Thrombolysis 11(2): 155-62.
This article looked primarily comparing cardiac markers with P-Selectin. Design was very poor, no definition of MI or unstable angina was carried out, no standard reference was adhered to, and no statistical assessment of cardiac markers was analyzed.
Smith(04) Smith, S. W., C. D. Tibbles, et al. (2004). "Outcome of low-risk patients discharged home after a normal cardiac troponin I." Journal of Emergency Medicine 26(4): 401-6.
Patients with symptoms suggestive of, but at low risk for, acute coronary syndrome (ACS), who have a negative electrocardiogram (EKG) and a single normal troponin I at 6-9 h after symptom onset are frequently discharged from our Emergency Department (ED). We sought to determine their rate of adverse cardiac events at 30 days (ACE-30), defined as cardiac death or myocardial infarction (MI), by chart review, telephone interview, or county death records. Of 663 patients, data were available for 588 (89%). Mean age was 48 years; 59% were male. There were 390 patients (66%) who complained of chest pain. Previous coronary artery disease (CAD) was reported in 145 patients (25%). Two patients (0.34%) had ACE-30, both with non-ST elevation MI. There were no cases of cardiac death. None of the patients died in Hennepin County within 30 days. At our institution, low-risk patients with symptoms suggestive of ACS who are discharged home after a normal cTnI drawn 6-9 h after symptom onset have a very low incidence of cardiac events at 30 days.
No calculation of sensitivity or specificity. Solinas(03)
Solinas, L., R. Raucci, et al. (2003). "Prevalence, clinical characteristics, resource utilization and outcome of patients with acute chest pain in the emergency department. A multicenter, prospective, observational study in North-Eastern Italy." Italian Heart Journal: Official Journal of the Italian Federation of Cardiology 4(5): 318-324.
No analysis of enzymesSonel(00)
Sonel, A., B. M. Sasseen, et al. (2000). "Prospective study correlating fibrinopeptide A, troponin I, myoglobin, and myosin light chain levels with early and late ischemic events in consecutive patients presenting to the Emergency Department with chest pain." Circulation 102(10): 1107-1113.
This study looked at troponin I and myoglobin as well as Fibrinopeptide A. Troponin values were at 0, 4 and 8 hours post admission.
Spalding(03)Spalding, L., Reay, E., & Kelly, C. (2003). Cause and outcome of atypical chest pain in patients
document.doc Page 74 of 77
admitted to hospital. Journal of the Royal Society of Medicine, 96(3), 122-125.
In patients with acute chest pain the prime need, usually, is to diagnose and treat myocardial infarction or ischaemia. When a cardiac origin for the pain has been excluded, patients are commonly discharged without either a diagnosis or a plan for follow-up. We studied a group of such patients to see how far causation was pursued and how their mortality compared with that of patients with a proven cardiac cause for their symptoms. The study population was 250 patients admitted over five weeks with chest pain suspected of being cardiac in origin. Initial assessment included an electrocardiogram and measurement of troponin T. If neither of these indicated a cardiac event, the patient was deemed to have 'atypical' chest pain and the cause, where defined, was recorded. Outcomes at one year were determined by questionnaire and by assessment of medical notes. Of the 250 patients, 142 had cardiac pain (mean age 79 years, 58% male) and 108 atypical chest pain (mean age 60 years, 55% male). Of those with atypical pain, 40 were discharged without a diagnosis; in the remaining 68 the pain was thought to be musculoskeletal (25), cardiac (21), gastrointestinal (12) or respiratory (10) in origin. 41 patients were given a follow-up appointment on discharge. At one year, data were available on 103 (96%) patients. The mortality rate was 2.9% (3 patients) compared with 18.3% in those with an original cardiac event. Half of the patients with atypical pain had undergone further investigations and 14% had been readmitted. The yield of investigative procedures was generally low (20%) but at the end of the year only 27 patients remained undiagnosed. Patients with atypical chest pain form a substantial proportion of emergency admissions. The symptoms often persist or recur. The commonest causation is musculoskeletal, but a sizeable minority remain undiagnosed even after follow-up.
No relation to enzymesSvensson(03)
Svensson, L., L. Isaksson, et al. (2003). "Predictors of myocardial damage prior to hospital admission among patients with acute chest pain or other symptoms raising a suspicion of acute coronary syndrome." Coronary Artery Disease 14(3): 225-31.
AIM: To evaluate factors which, prior to hospital admission, predict the development of acute coronary syndrome or acute myocardial infarction among patients who call for an ambulance due to suspected acute coronary syndrome. DESIGN: Prospective observational study. METHODS: All the patients who called for an ambulance due to suspected acute coronary syndrome in South Hospital's catchment area in Stockholm and in the Municipality of Goteborg between January and November 2000, were included. On arrival of the ambulance crew, a blood sample was drawn for bedside analysis of serum myoglobin, creatine kinase (CK)MB and troponin-I. A 12-lead electrocardiogram (ECG) was simultaneously recorded. RESULTS: In all, 538 patients took part in the survey. Their mean age was 69 years and 58% were men. In all, 307 patients (57.3%) had acute coronary syndrome and 158 (29.5%) had acute myocardial infarction. Independent predictors of the development of acute coronary syndrome were a history of myocardial infarction (P=0.006), angina pectoris (P=0.005) or hypertension (P=0.017), ECG changes with ST elevation (P<0.0001), ST depression (P<0.0001) or T-wave inversion (P=0.012) and the elevation of CKMB (P=0.005). Predictors of acute myocardial infarction were being a man (P=0.011), ECG changes with ST elevation (P<0.0001) or ST depression (P<0.0001), the elevation of CKMB (P<0.0001) and a short interval between the onset of symptoms and blood sampling (P=0.010). CONCLUSION: Among patients transported by ambulance due to suspected acute coronary syndrome, predictors of myocardial damage can be defined prior to hospital admission on the basis of previous history, sex, ECG changes, the elevation of biochemical markers and the interval from the onset of symptoms until the ambulance reaches the patient.
Odds RatiosTadros(03)
Tadros, G. M., T. R. McConnell, et al. (2003). "Clinical predictors of 30-day cardiac events in patients with acute coronary syndrome at a community hospital." Southern Medical Journal 96(11): 1113-20.
The study looked at amongst other things, troponin assays at 0, 6 and 12 hours in predicting negative outcomes of cardiac death, AMI or urgent revascularization with 30 days of admission. No subset analysis was carried out and therefore not applicable to my hypothesis.
Tanasijevic(99)

document.doc Page 75 of 77
Tanasijevic, M. J., C. P. Cannon, et al. (1999). "The role of cardiac troponin-I (cTnI) in risk stratification of patients with unstable coronary artery disease." Clin Cardiol 22(1): 13-16.
This was a review article.Taylor(02)
Taylor, C., Forrest-Hay, A., & Meek, S. (2002). ROMEO: a rapid rule out strategy for low risk chest pain. Does it work in a UK emergency department? Emerg Med J, 19(5), 395-399.
AIMS: To examine the feasibility of using the ROMEO (rule out myocardial events on "obs" ward) pathway for low risk patients with chest pain in a UK emergency department. METHODS: A prospective study was undertaken to determine outcomes for the first 100 patients entering the pathway (from May to Oct 1999). Serum troponin levels, serial ECG recordings, exercise test result, total length of stay, and final diagnoses were reviewed. Patients were telephoned after discharge to inquire about persisting or recurrent pain, and further investigations after completing the ROMEO pathway. RESULTS: 82 of 100 (82%) had myocardial damage excluded by serum troponin assay. Sixty two of 82 (76%) of these completed exercise tolerance testing (ETT). Fifty seven of 62 (92%) ETTs were negative. Twenty of 82 (26%) did not undergo ETT because of mobility problems, recent ETT, or if considered very low probability of cardiac pain on consultant review. Five of 100 (5%) had an increased initial troponin and five of 100 (5%) had an increased 12 hour troponin. These patients were referred for admission under the general physicians. Seven of 100 (7%) were referred for other reasons (late ECG changes, continuing or worsening pain). One patient self discharged. Length of stay varied because of changes to arrangements for ETT. The median time for all patients over the period studied was 23 hours. All patients were discharged within an hour of a negative ETT. FOLLOW UP RESULTS: 67 of 74 (91%) eligible patients were contacted by telephone. Forty six of 67 (69%) had no further pain, attendances, or GP consultations. Six of 67 (9%) had further cardiological investigation or treatment. CONCLUSIONS: A rapid rule out strategy such as the ROMEO pathway is feasible in the UK healthcare setting and provides standardised and consistent evaluation.
This was a study that looked at 12 hour troponin I, the assay was not described, follow up was anywhere from 4 months to 10 months, no statistical analysis by sensitivity or specificity was carried out.
Uettwiller-Geiger(02)Uettwiller-Geiger, D., A. H. B. Wu, et al. (2002). "Multicenter evaluation of an automated assay for troponin I." Clinical Chemistry 48(6): 869-876.
Calibration of assay, not applied to cardiac patient population.Van Lente(99)
Van Lente, F., E. S. McErlean, et al. (1999). "Ability of troponins to predict adverse outcomes in patients with renal insufficiency and suspected acute coronary syndromes: a case-matched study." Journal of the American College of Cardiology 33(2): 471-8.
OBJECTIVES: The purpose of this study was to investigate the utility of cardiac troponin T and troponin I for predicting outcomes in patients presenting with suspected acute coronary syndromes and renal insufficiency relative to that observed in similar patients without renal disease. BACKGROUND: Cardiac troponin T and troponin I have shown promise as tools for risk stratification of patients with acute coronary syndromes. However, there is uncertainty regarding their cardiac specificity and utility in patients with renal disease. METHODS: We measured troponin T, troponin I and creatine kinase MB in 51 patients presenting with suspected acute coronary syndromes and renal insufficiency and in 102 patients without evidence of renal disease matched for the same peak troponin T or I value, selected from a larger patient cohort. Blood samples were obtained at presentation to an emergency room 4 hours, 8 hours and 16 hours later. The ability of biochemical markers to predict adverse outcomes in both groups including infarction, recurrent ischemia, bypass surgery, heart failure, stroke, death or positive angiography/angioplasty during hospitalization and at six months was assessed by receiver-operator curve analysis. The performance of both troponins was compared between groups. RESULTS: Thirty-five percent of patients in the renal group and 45% of patients in the nonrenal group experienced an adverse initial outcome; over 50% of patients in all groups had experienced an adverse outcome by 6 months, but these differences were not significant. The area under the curve (AUC) for the ROC curve for troponin T as predictor of initial outcomes was significantly lower in the renal group than in the

document.doc Page 76 of 77
nonrenal group: 0.56+/-0.07 and 0.75+/-0.07, respectively. The area under the curve was also significantly lower in the renal group compared with the nonrenal group for troponin T as predictor of six month outcomes: 0.59+/-0.07 and 0.74+/-0.07, respectively. The area under the curve was also significantly lower in the renal group compared to the nonrenal group for troponin I as predictor of both initial and six month outcomes: 0.54+/-0.06 vs. 0.71+/-0.07 and 0.53+/- 0.06 vs. 0.65+/-0.07, respectively. The sensitivity of troponin T for both initial and six month adverse outcomes was significantly lower in the renal group than in the nonrenal group at a similar level of specificity (0.87): 0.29 vs. 0.60 and 0.45 vs. 0.56, respectively. Troponin I also exhibited similar differences in sensitivity in the renal group (0.29 vs. 0.50 and 0.33 vs. 0.40, respectively). CONCLUSIONS: The ability of cardiac troponin T and troponin I to predict risk for subsequent adverse outcomes in patients presenting with suspected acute coronary syndromes is reduced in the presence of renal insufficiency.
This study looked at troponin t and I in renal patients with a creatinine > 20 milligrams per liter. Diagnosis of AMI was made by WHO criteria. The 6-month outcomes were documented in a blinded fashion. Biochemical markers were assayed at times 0, 4, 8 and 16 hours. No analysis of 0/4 hrs assays were made. Rejected
Venge(02)Venge, P., B. Lagerqvist, et al. (2002). "Clinical performance of three cardiac troponin assays in patients with unstable coronary artery disease (a FRISC II substudy)." Am J Cardiol 89(9): 1035-41.
The assay of cardiac-specific troponins (cTroponins) is a sensitive and specific means to diagnose myocardial injury. Several assays for the measurement of cardiac-specific troponin I (cTnI), but only 1 for the assay of cardiac specific troponin T (cTnT), are commercially available. The aim of this study was to compare 3 of these assays (i.e., Access AccuTnI [cTnI], AxSym [cTnI], and Elecsys 3(rd) generation [cTnI]) and their clinical performances in a group of patients (n = 1,763) with unstable coronary artery disease (Fragmin and fast Revascularisation during InStability in Coronary artery disease [FRISC II] trial). Clinical events after 1-year follow-up, such as death and death and/or acute myocardial infarction, were recorded and the effects of invasive or noninvasive treatment evaluated in relation to cTroponin levels. Overall the 2 cTnI methods showed good correlation (r(s) = 0.96), whereas correlations to the cTnT assay were somewhat lower (r(s) = 0.93). Patients with nonelevated levels, as measured with any of the 3 biomarkers, had a significantly better prognosis than patients with elevated levels (p <0.001). A cohort of 10% to 12.4% of patients with a poor prognosis was identified only by the Access AccuTnI assay. Invasive treatment reduced clinical events only in the group of patients with elevated cTroponin levels. We conclude that stratification of patients with unstable coronary artery disease by means of cTroponin measurements is important in clinical management. It is also apparent that assays with superior sensitivity, such as the Access AccuTnI, identify more patients with poor prognosis who are candidates for early invasive procedures.
This was a FRISC II sub study analysis looking at 3 different types of troponin I assay and T assay with regard to 1 year follow up cardiac events. The average time from onset of pain symptoms to assay was 37 hours. This is not relevant
Venge(03)Venge, P., N. Johnston, et al. (2003). "Clinical and analytical performance of the liaison cardiac troponin I assay in unstable coronary artery disease, and the impact of age on the definition of reference limits. A FRISC-II substudy." Clinical Chemistry 49(6): 880-886.
Sub study of FRISC-11; average time to assay procurement 37 hours after admission to hospital. Welsh(03)
Welsh, R. C., J. Ornato, et al. (2003). "Prehospital management of acute ST-elevation myocardial infarction: a time for reappraisal in North America." Am Heart J 145(1): 1-8.
Review article, ST segment elevation only.Wilcox(01)
Wilcox, G., P. D. Archer, et al. (2001). "Measurement of cardiac troponin I levels in the emergency department: Predictive value for cardiac and all-cause mortality." Medical Journal of Australia
document.doc Page 77 of 77
174(4): 170-173.
This study did not give time from symptoms to assay, did not describe the patient population, did not look at the diagnosis of AMI, only 30 day mortality and gave no figures for sensitivity or specificity.
Wu(99)Wu, A. H. B., F. Ghani, et al. (1999). "Reflex testing II: Evaluation of an algorithm for use of cardiac markers in the assessment of emergency department patients with chest pain." Clinica Chimica Acta 288(1-2): 97-109.
A reflex algorithm was developed and evaluated for the use of serum cardiac markers for the diagnosis and rule out of acute myocardial infarction (AMI), and risk stratification of unstable angina patients for those who present to emergency departments (ED) with chest pain. The process begins with testing of total CK and myoglobin at admission. Based on these results, the algorithm determines the need for subsequent testing for the CK-MB isoenzyme and cardiac troponin I (cTnI). The algorithm also directs the need for further blood collection and cardiac marker testing at 4, 8, and 12 h after presentation. A total of eleven stopping points were identified. For some of these stopping points, the algorithm concluded that further blood collections and testing was unnecessary and redundant. The algorithm was retrospectively evaluated on 101 non-consecutive chest pain patients who presented to the EDs at three hospitals. For the AMI group (n=34), six of nine possible different stopping points were reached: 64.7% of cases were diagnosed with the first sample at admission, an additional 32.3% after 4 h, and 2.9% at 8 h. The 12-h sample was not necessary for any of the AMI patients. For the non-AMI group (n=67), most reached the stopping point of no cardiac injury or risk. There were five unstable angina patients who had minor myocardial damage on the basis of a marginally increased cTnI. Of these, one patient subsequently suffered AMI, and three others required angioplasty or bypass surgery. Compared to performing four tests on all patient samples, the reflex algorithm would have reduced the number of necessary tests from 442 to 130 (71% reduction) for AMI patients, and 871 to 469 (46% reduction) for non-AMI patients, if prospectively implemented. Copyright (C) 1999 Elsevier Science B.V.
This was a retrospective study using a complex algorithm utilizing myoglobin/CK/CK MB/troponin I. No sensitivities or specificities were available for the 0, 4 or 8 hour assay times.
Zalenski(00)Zalenski, R. J., H. P. Selker, et al. (2000). "National Heart Attack Alert Program position paper: chest pain centers and programs for the evaluation of acute cardiac ischemia." Ann Emerg Med 35(5): 462-71.
No assessment of cardiac enzymes by a statistical analysis.Zalenski(98)
Zalenski, R. J. and F. H. Shamsa (1998). "Diagnostic testing of the emergency department patient with chest pain. [Review] [41 refs]." Current Opinion in Cardiology 13(4): 248-53.
ReviewZarich(01)
Zarich, S., K. Bradley, et al. (2001). "Impact of troponin T determinations on hospital resource utilization and costs in the evaluation of patients with suspected myocardial ischemia." American Journal of Cardiology 88(7): 732-6.
This interesting study looked at whether troponin T assays would change length of hospital and secondarily adverse events.It looked at assays drawn at 0, 3 and 12 hours and therefore cannot be applied to my hypothesis.


















