Troponin elevation is not always acss
30
Troponin elevation is not always acute coronary syndrome Dr. Ayman Ahmed Abdelaziz Professor of Cardiology-Egypt
-
Upload
aymanabdelaziz -
Category
Healthcare
-
view
434 -
download
1
Transcript of Troponin elevation is not always acss
Troponin elevation is not always acute coronary syndrome
Dr.
Ayman Ahmed Abdelaziz
Professor of Cardiology-Egypt

•Schematic representation of the cardiac myofibrillar thin filament. Cardiac troponins
exist in a structural (bound) form and in a free
•cytosolic pool. Cardiac troponins are released from myocytes as complexes or as free protein
Cardiac troponins exist in a structural (bound) form and in a free cytosolic pool. They are released from myocytes as complexes or as free protein

Cardiac troponins
Regulatory proteins that form the cornerstone of muscle contraction.
1. Troponin C: binds with calcium.2. Troponin T: binds with tropomyosin.3. Troponin I: inhibites contraction.
Troponin C is not cardiac specific, and thus is not used for the diagnosis of cardiac injury.
CTnT and I are specific markers of myocardial injury ACS
Cardiac troponins (T & I)
Require myocardial necrosis for release.
Early rise (3-4 hours after symptom).
Peak 12-24 hours.
Continuous release up to 10-14 days.

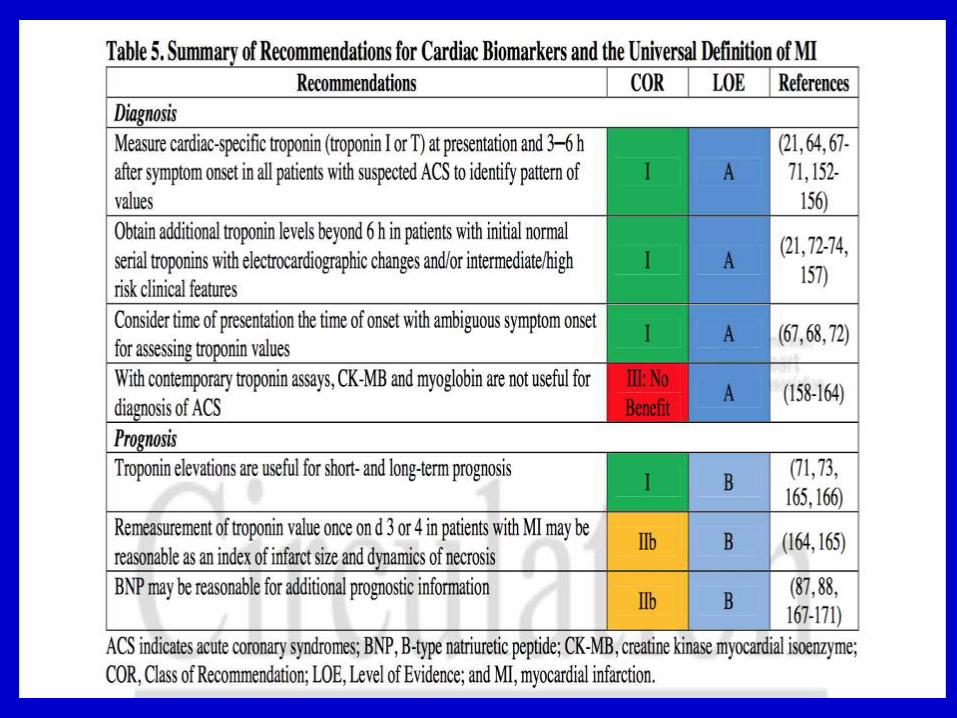
Definition of MI
Detection of rise and/or fall of cardiac biomarkers (preferably troponin) above the 99th percentile of
the upper reference limit + with evidence of
ischaemia with at least one of the following:
Ischaemic symptoms
ECG changes of new ischaemia, development of pathologic Q-waves in the ECG or
Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality.

Peri-procedural myocardial infarction
Post PCI MI: three-fold increase from the normal baseline value.
Post CABG: a five-fold increase from the baseline during 1st 72 hours, along with associated findings, such as new Q waves.
After non-cardiac surgery: The same cut-off levels used to diagnose an acute MI should be used to detect perioperative injury.
Post PCI
MI occurring after PCI (subtype 4a) , as an increase cardiac troponins >3 × the upper reference limit (URL)
5% to 40% of cases, even when the procedure seems successful and uncomplicated
How do troponin compare with
ECG in ACS?
Troponin and EKG changes complementary.
Differentiating the diagnosis of unstable angina and non-ST elevation myocardial infarction
Negative troponin + normal EKG: mortality 1%.
Negative troponin + ischemic EKG: mortality 4% at 1 month.
TIMI score
1. Age 65 years.
2. 3 risk factors for CAD.
3. Coronary stenosis 50%.
4. ASA use in past 7 days.
5. Severe angina 24 hours
6. + cardiac markers.
7. ST deviation 0.5 mm.
Intermediate:3-4 (14-days events:13-20%).
High: 6-7 (14-days events: 40%).

System Causes of Troponin Elevation
Cardiovascular Acute aortic dissection
Arrhythmia
Medical ICU patients
Hypotension
Heart failure
Apical ballooning syndrome
Cardiac inflammation
• Endocarditis, myocarditis, pericarditis
Hypertension
Infiltrative disease
• Amyloidosis, sarcoidosis, hemochromatosis,
Sclerodermia
Left ventricular hypertrophy
Myocardial Injury
Blunt chest trauma
Cardiac surgeries
Cardiac procedures
• Ablation, cardioversion, percutaneous intervention
Chemotherapy
Hypersensitivity drug reactions
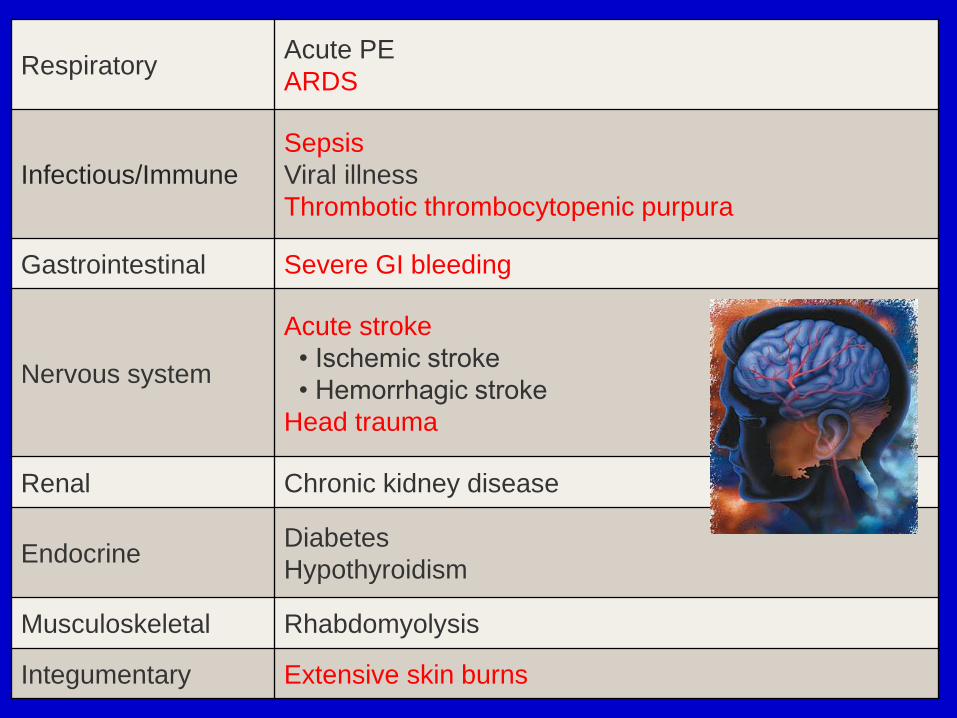
RespiratoryAcute PE
ARDS
Infectious/Immune
Sepsis
Viral illness
Thrombotic thrombocytopenic purpura
Gastrointestinal Severe GI bleeding
Nervous system
Acute stroke
• Ischemic stroke
• Hemorrhagic stroke
Head trauma
Renal Chronic kidney disease
EndocrineDiabetes
Hypothyroidism
Musculoskeletal Rhabdomyolysis
Integumentary Extensive skin burns

Troponins and heart failure
May have chronic elevation of both TnT and TnI.
Diagnosis of ACS require serial measurement.
As low as TnT<0.05 predicts increased risk.
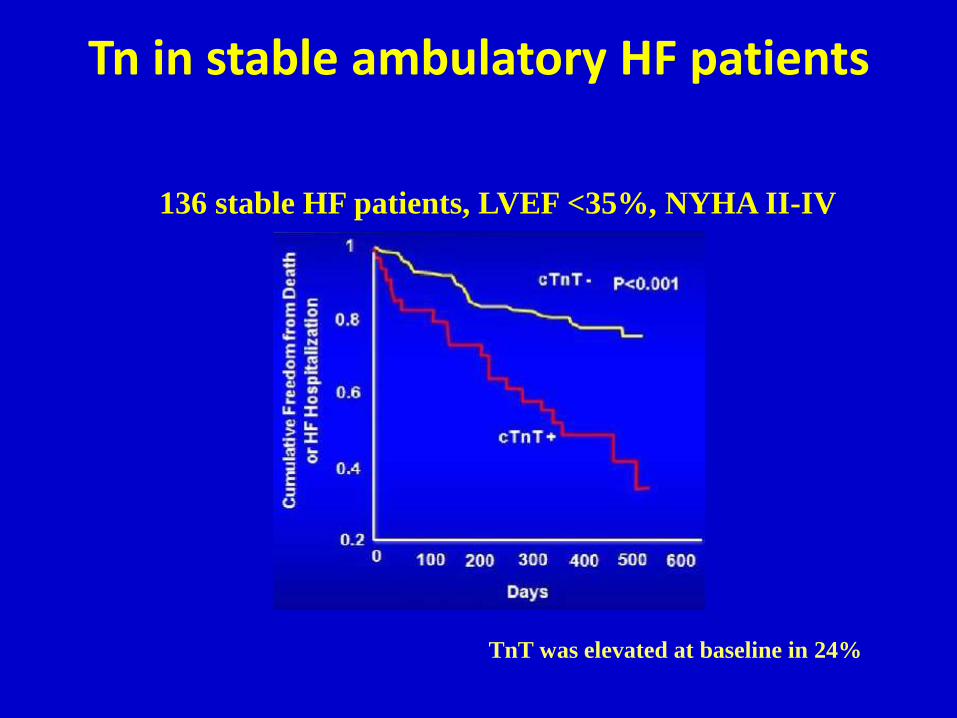
Tn in stable ambulatory HF patients
136 stable HF patients, LVEF <35%, NYHA II-IV
TnT was elevated at baseline in 24%

Causes of Tn release in HF
Type I myocardial infarction
Reduced oxygen supply ( anemia, hypotension)
Increased oxygen demand
Coronary ischemia
Elevation of Tn in a patient with HF should always be interpreted in
the context of Type I MI, especially in the setting of significant rise or
fall of the marker
Type II myocardial infarction
Increased transmural wall stress
Elevated filling pressures
Dilated LV chamber size
Lower tissue perfusion
Stiffer myocardium
Januzzi, et al. Eur Heart J 2012; 33: 2265-71
Cardiac-specific causes of Tn release in HF
Mechanisms other than Type I or II MI
Direct toxicity of circulating neurohormones
Infiltrative processes (amyloidosis etc.)
Toxic exposures (e.g. Alcohol or chemotherapy agents)
Inflammation (myocarditis)
Cardiomyocyte apoptosis or autophagy (wall stretch)
Normal (or abnormal) cardiomyocyte turnover
Stress cardiomyopathy
Tachycardia-induced cardiomyopathy
Pericarditis and myocarditis
32–49% of cases of acute pericarditisReflect myocardial lesion (myopericarditis)Myopericarditis: young, recent fever + GIT symptoms
and/or skeletal muscle myalgia + ST-segment elevation at presentation.
Troponin increase: Extent of myocardial inflammation, but unlike ACS it does not seem to carry an adverse prognosis.
Magnetic resonance imaging (MRI) : diagnostic (delayed enhancement usually involves the subendocardial layer in MI, while it spares the subendocardial layer in myocarditis)

Tako-tsubo (Stress-induced cardiomyopathy)
Older woman with an acute emotional or physiologic stress.
Involvement of apical and/or mid LV with sparing of basal segments.
Modest rise in cTn that peaks within 24 h.
The magnitude of increase in the biomarkers is less than that observed with a STEMI and disproportionately low for the extensive acute regional wall motion abnormalities

Acute pulmonary embolism
High risk PE (PE and shock/ hypotension)
Thrombolytic therapy or embolectomy
Intermediate-risk PE are characterized as patients with a stable circulation but with RV dysfunction or elevated Troponins
Increased cTn values were associated with a higher mortality in the haemodynamically stable patients
Normal echocardiogram + negative cTnI level was most useful to identify patients at lowest risk for early death
Pulmonary embolism
Positive cTnI: correlated with having more segmental defects on ventilation–perfusion scintigraphy.
Causes of elevated troponin in PE : Acute right ventricular strainsHypoxaemia due to perfusion–ventilation
mismatchhypoperfusion as a consequence of low output
and reduced coronary blood flowParadoxical embolism from systemic veins to the
coronary arteries, usually via a PFO.
Troponin in aortic dissection
• CTn is elevated in up to 18% of pts with AAD, indicative of the high acuity of illness than specific to aortic dissection itself.
• Misdiagnosis of AAD may result in incorrect administration of anticoagulation therapy.

Tachycardias
Prolonged episodes of supraventricular tacharrhythmias (SVT)
Shortening of diastole with subsequent subendocardial Ischaemia
Troponin T and renal failure
Chronic elevation.
Not related with frequency and efficacy of dialysis or creatinine level.
Specificity of cTn for ACS is lower compared with pts without renal disease.
CKD patients who present with signs and symptoms suspicious for AMI, a change in troponin concentration (ie, rise or fall over three to six hours after presentation) should be used to define AMI, rather than a single value on presentation.
20 % change in serially measured troponins

Acute illness
Coronary ischemia in the absence of plaque rupture or coronary thrombosis : supply-demand mismatch ( Type II MI).
Severe disease : microvascular dysfunction and myocytotoxiceffects of endotoxin, cytokines, reactive oxygen radicals.
50% of patients with severe sepsis and septic shock may develop impairment of ventricular performance. Elevations in cTncorrelate with the presence of LV systolic dysfunction.
Elevated cTn predicts mortality
Snake or scorpion bitesmyocardial injury by biologic toxins, vasospasm and coagulation abnormalities.
Other Causes

Troponin increases can reach levels typically diagnostic for acute MI.
Less marathon experience and younger age. Muscular fatigue Transiently decreased systolic and diastolic
function (cardiac fatigue) Right ventricular injury Degradation of ‘cytosolic’ troponin or increased
permeability of the cell membranes of myocytes under stress.
Cardiac troponin increases among runners in the Marathon
Cardiac contusion
• Thoracic trauma
• Patient with chest trauma and an absence of other injuries or haemodynamic instability, with normal ECG and cTn can be discharged
• Increased cTn may serve to identify patients at increased risk of mortality
False Positive
• Rarely, elevated troponin concentrations cannot be explained despite thorough clinical examination.
• Related to: heterophilic antibodies, and analyzer malfunction
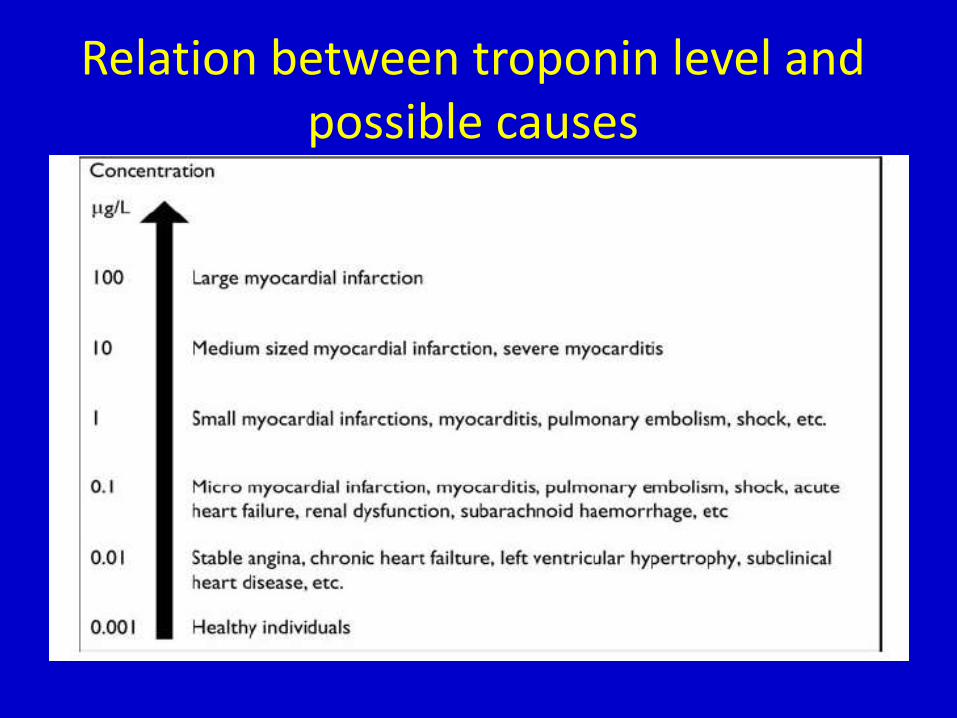
Relation between troponin level and possible causes
Conclusion
Cardiac troponins (cTn) are the most sensitive and specific biochemical markers of myocardial injury and with the new high-sensitivity troponin methods very minor damages on the heart muscle can be detected.
Elevated cTn levels indicate cardiac injury, but do not define the cause of the injury.
Cardiac troponin elevations are common in many disease states and do not necessarily indicate the presence ACS.
Stable cTn values without significant dynamic changes are likely markers of chronic structural heart disease.
Elevated troponins have a strong correlation with adverse cardiovascular outcome whether CAD is present or not.