N N. N N C C N N C C O O N N C C O O T T N N C C O O T T C C.

ISSN 2007-6452
2017 Vol. 6, Núm. 3 Septiembre / Diciembre
C O N T E N I D O / C O N T E N T S
LGII
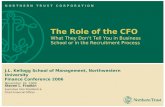
MergepEGFR + Total EGFR
Without EGF Stimulus EGF Stimulus
Fluorophore
Secondary antibodyPrimary antibody
Excitation
Molecular weight marker Interest protein Blocking protein
Light emission
pEGFR Total EGFR
A
B
C D
E
Artículos originales / Original articles
Índice de asistencia en el tratamiento de rehabilitación en adolescentes con parálisis cerebral en un centro del noroeste mexicanoAttendance Index of rehabilitation treatment in adolescents with cerebral palsy at a northwest mexican center
Comparación de los sistemas MicroScan WalkAway y VITEK 2 Compact para la identificación y susceptibilidad de bacterias Gram-positivas y Gram-negativas de aislados clínicosComparison of the MicroScan WalkAway and VITEK 2 Compact systems for the identification and susceptibility of clinical Gram-positive and Gram-negative bacteria
Producción de biopelículas y resistencia antimicrobiana en uropatógenos aislados de catéteres urinarios en un hospital de rehabilitación físicaProduction of biofilms and antimicrobial resistance of uropathogens isolated from urinary catheters in a physical rehabilitation hospital Interés General / General interest
La teoría de las inteligencias múltiples en personas con síndrome de Down. Cuando el talento se transforma en inteligenciaThe theory of multiple intelligences in people with Down’s syndrome. When talent is transformed into intelligence
Western blot: una herramienta en el área biomédicaWestern blot: a tool in the biomedical field


En Internet, compilada en versión completa en:
Literatura Biomédica:
www.medigraphic.com/rid
Editada por Graphimedic, S.A. de C.V.
Investigación en Discapacidad. Año 6, No 3, Septiembre-Diciembre 2017. Es una publicación editada y distribuida por el Instituto Nacional de Rehabilitación «Luis Guillermo Ibarra Ibarra», Calzada México-Xochimilco 289. Col. Arenal de Guadalupe. CP. 14389. Del. Tlalpan. México, DF. Editor responsable: Dr. Jonathan Javier Magaña Aguirre. Reserva de Derechos al Uso Exclusivo No 04-2012-121314173500-102. ISSN 2007-6452. Ambos otorgados por el Instituto Nacional del Derecho de Autor. Licitud de Título y Contenido en
Coquimbo 936, Col. Lindavista, CP. 07300. Del. Gustavo A. Madero, México, DF. Tels. 85898527 al 32. Este número se terminó de imprimir el 12 de octubre de 2017 con un tiraje de 1,000 ejemplares. El contenido de los artículos, así como las fotografías son responsabilidad exclusiva de los autores. La reproducción parcial o total sólo podrá hacerse previa autorización del editor de la revista. Toda correspondencia debe ser dirigida al Editor responsable a los correos electrónicos: [email protected]; [email protected]
Imagen de la portada: A; B. Dicho principio permite la
detección de una proteína en su estado basal C, D. Con lo que es posible realizar un análisis de co-localización E. En la actualidad es una técnica básica para el análisis de proteínas en el área biomédica.
Editor en Jefe: Jonathan Javier Magaña Aguirre Ph.D. (INR-LGII)Co-Editores: Guadalupe Sánchez Bringas Ph.D. (UNAM) y Alberto López Reyes Ph.D. (INR-LGII)
Investigación Básica (Coordinador Editorial)Oscar Hernández Hernández Ph.D. (INR-LGII)
René Abarca Buis Ph.D. (INR-LGII)Isabel Arrieta Cruz Ph.D. (INGER)
Bulmaro Cisneros Vega Ph.D. (CINVESTAV)Ramón M. Coral Vázquez Ph.D. (ESM-IPN)Francisco García Sierra Ph.D. (CINVESTAV)
Luis E. Gómez Quiroz Ph.D. (UAMI) Gerardo Leyva Gómez Ph.D. (UNAM)R. Balam Muñoz Soto Ph.D. (ITESM)
Fernando E. Navarro García Ph.D. (CINVESTAV)David Quintanar Guerrero Ph.D. (UNAM)
José Manuel Rodríguez Pérez Ph. D. (INC-ICH)Roberto Sánchez Sánchez Ph.D. (INR-LGII)Gilberto Vargas Alarcón Ph.D. (INC-ICH)
Investigación Clínica (Coordinador Editorial)Paul Carrillo Mora M.D., Ph.D. (INR-LGII)
José L. Aceves Chimal M.D., M.Sc. (ISSSTE)Salvador Castillo Castillo M.D. (HIM)
Roberto Coronado Zarco M.D., M.Sc. (INR-LGII)Adolfo Chávez Negrete M.D., Ph.D (IMSS)
Victoria del Castillo Ruiz M.D. (INP)Juan Fernández Ruiz M.D., Ph.D. (UNAM)Marwin Gutiérrez Riveros M.D. (INR-LGII)
Victor M. Ilizaliturri Sánchez M.D. (INR-LGII)Vicente Madrid Marina M.D. Ph.D. (INSP)
Carlos Pineda Villaseñor M.D., Ph.D. (INR-LGII)Jimena Quinzaños Fresnedo M.D., M.Sc. (INR-LGII)
Antonio Redón Tavera M.D. M.Sc. (INR-LGII)
Investigación en Ingeniería Biomédica (Coordinador Editorial)
Josefina Gutiérrez Martínez Ph.D. (INR-LGII)
Pablo R. Hernández Rodríguez Ph.D (CINVESTAV)
Lorenzo Leija Salas Ph.D. (CINVESTAV)
Investigación Sociomédica (Coordinador Editorial):
Claudia C. Maya Ampudia Psic. (INR-LGII)Anabella Barragán Solís Ph.D. (ENAH)
Comité InternacionalFrancisco J. Blanco M.D., Ph.D.
(Hospital Universitario A Coruña-ESP)Roger Gutiérrez Juárez M.D., Ph.D.
(Albert Einstein College-USA)Fernando Morales Montero Ph.D. (Universidad de Costa Rica-CR)Anthony Reginato M.D., Ph.D.(Rhode Island Hospital-USA)
Alvaro Rendón Ph.D. (INSERM-U592-FRA)
Luis Velázquez Pérez M.D., Ph.D. (CIRAH-CUB)
Steve J. Winder (University of Sheffield-UK)
Asistente EditorialAraceli Guerra Grajeda M.A.F. (INR-LGII)
Coordinación Administrativa Josué Ugarte Lima B.E.
Enlace de Estadística Editorial Dieter Vega Ruíz B.B.A.
Corrección de IdiomaElia Rodríguez Barraza M. Sc. (INR-LGII)
Diseño GráficoMiguel Ángel González Ocampo Lic. (INR-LGII)
Cuerpo Directivo
Dr. José Narro RoblesSecretario de Salud
Dr. Guillermo Ruiz-Palacios y SantosComisionado Nacional de los Institutos Nacionales
de Salud y Hospitales de Alta Especialidad
Dr. José Clemente Ibarra Ponce de LeónDirector General
Dr. Daniel David Chávez AriasDirector Médico
Dra. Matilde Enríquez SandovalDirectora de Enseñanza
Dr. Juan Antonio MadinaveitiaDirector Quirúrgico
Dr. Carlos Pineda VillaseñorDirector de Investigación
Dra. Maricela Verdejo SilvaDirectora de Administración
Consejo Editorial
María Lucinda Aguirre Cruz M.D. Ph.D. (INNN-MVS)Teresa Corona Vázquez M.D. Ph.D. (INNN-MVS)Julio Granados Arriola M.D., Ph.D. (INNCM-SZ)Enrique Graue Wiechers M.D., Ph.D. (UNAM)
Rosalinda Guevara Guzmán M.D., Ph.D. (UNAM)Luis Guillermo Ibarra Ibarra M.D. (CCINSHAE)
Alberto Lifshitz Guinzberg M.D. (IMSS)Jaime Mas Oliva M.D. Ph.D. (UNAM)
Horacio Merchant Larios M.D. Ph.D. (UNAM)
Coordinadora Editorial Lic. Maricela Hernández

Contenido/ ContentsVol. 6 Núm. 3 Septiembre-Diciembre 2017
Original articles
99 Attendance Index of rehabilitation treatment in adolescents with cerebral palsy at a northwest mexican centerElsa Pérez-Flores, Israel Macías-Hernández, Juan Peña-Bañuelos
105 Comparison of the MicroScan WalkAway and VITEK 2 Compact systems for the identification and susceptibility of clinical Gram-positive and Gram-negative bacteria Melissa Hernández-Durán, Luis E López-Jácome, Claudia A Colín-Castro, Guillermo Cerón-González, Silvestre Ortega-Peña, E Samuel Vanegas-Rodríguez, Jaime A Mondragón-Eguiluz, Rafael Franco-Cendejas
115 Production of biofilms and antimicrobial resistance of uropathogens isolated from urinary catheters in a physical rehabilitation hospitalSilvestre Ortega Peña, Guillermo Cerón González
General interest
122 The theory of multiple intelligences in people with Down’s syndrome. When talent is transformed into intelligenceIgnacio Gutiérrez Delgado
128 Western blot: a tool in the biomedical fieldKarina Martínez-Flores, Ángel Tonatiuh Salazar-Anzures, Javier Fernández-Torres, Carlos Pineda, Carlos Alberto Aguilar-González, Alberto López-Reyes
Artículos originales
99 Índice de asistencia en el tratamiento de rehabilitación en adolescentes con parálisis cerebral en un centro del noroeste mexicanoElsa Pérez-Flores, Israel Macías-Hernández, Juan Peña-Bañuelos
105 Comparación de los sistemas MicroScan WalkAway y VITEK 2 Compact para la identificación y susceptibilidad de bacterias Gram-positivas y Gram-negativas de aislados clínicosMelissa Hernández-Durán, Luis E López-Jácome, Claudia A Colín-Castro, Guillermo Cerón-González, Silvestre Ortega-Peña, E Samuel Vanegas-Rodríguez, Jaime A Mondragón-Eguiluz, Rafael Franco-Cendejas
115 Producción de biopelículas y resistencia antimicrobiana en uropatógenos aislados de catéteres urinarios en un hospital de rehabilitación físicaSilvestre Ortega Peña, Guillermo Cerón González
Interés General
122 La teoría de las inteligencias múltiples en personas con síndrome de Down. Cuando el talento se transforma en inteligenciaIgnacio Gutiérrez Delgado
128 Western blot: una herramienta en el área biomédicaKarina Martínez-Flores, Ángel Tonatiuh Salazar-Anzures, Javier Fernández-Torres, Carlos Pineda, Carlos Alberto Aguilar-González, Alberto López-Reyes

Volumen 6 Número 3 Septiembre-Diciembre 2017 99
www.medigraphic.org.mxPalabras clave:
Pacientes ambulatorios, a dolescentes, parálisis cerebral, rehabilitación, medicina física y
rehabilitación.
Key words: Outpatient, adolescent, cerebral
palsy, rehabilitation, physical medicine and rehabilitation.
Índice de asistencia en el tratamiento de rehabilitación en adolescentes con parálisis cerebral en un centro del noroeste mexicanoAttendance Index of rehabilitation treatment in adolescents with cerebral palsy at a northwest mexican center
Elsa Pérez-Flores,* Israel Macías-Hernández,‡ Juan Peña-Bañuelos§
Artículo original
Vol. 6, Núm. 3 Septiembre-Diciembre 2017
pp 99-104
Resumen
El tratamiento de rehabilitación es parte integral del manejo de los pacientes con parálisis cerebral (PC). Aproximadamente 90% de los pacientes con PC sobreviven hasta la adultez y la etapa de la adolescencia es clave en este proceso, aunque rara vez es estudiada. El cálculo del índice de asistencia (IA) proporciona un indicador preciso del grado en el que los pacientes se adhieren al tratamiento. En el presente estudio se determinan las características asociadas al IA en el tratamiento de rehabilitación en pacientes adolescentes con PC. Se realizó un estudio observacional, transversal y descriptivo en el que se incluyeron pacientes adolescentes que acudieron a un centro de rehabilitación en el periodo de un año. La información se obtuvo del expediente clínico. Se incluyeron 62 pacientes con un promedio de edad de 13.58 ± 2.55 años; 69.4% del sexo masculino. El tipo de PC predominante fue el espástico bilateral (80.6%) y el nivel V de la SCFMG (43.5%). El IA promedio fue de 0.71 ± 0.14. Se dividió la población en grupos de pacientes con asistencia regular y asistencia irregular, como factor asociado al IA sólo se reportó el lugar de residencia de los pacientes (p = 0.007) y se encontró una correlación entre la percepción de falta de recursos económicos y el IA (r = 0.56). Se concluyó que el vivir fuera de la ciudad donde se ubica el centro de rehabilitación y los recursos económicos fueron factores que intervienen en el índice de asistencia en este grupo de pacientes.
Abstract
Therapeutic adherence is a complex and multifactorial phenomenon. Rehabilitation treatment is an important part in the management of patients with cerebral palsy (CP) and is necessary to reduce complications and functional impairment. Calculating the assistance ratio gives an accurate indicator of the degree to which patients adhere to treatment. The objective was to determine the characteristics associated with the rate of assistance to rehabilitation treatment in adolescent patients with CP. This is an observational, transversal and descriptive study. CP patients included adolescents from 10 to 18 years old who that assist to the Rehabilitation Center in the period from January to December 2014. The information was obtained from medical records. 62 patients were obtained with an average age of 13.58 ± 2.55 years; 69.4% male. The predominant type of CP was spastic bilateral (80.6%) and level V of the GMFCS (43.5%). The average attendance ratio was 0.71 ± 0.14. The population was divided into groups of patients with poor and good attendance, only to be reported statistically significant level attendance ratio with the place of residence of patients (p = 0.007) and a moderate correlation in the perception of lack of economical resources and attendance ratio (r = 0.56). Only the living outside the city where the rehabilitation center is found to be a factor in the adherence in this group of patients. The other clinical or demographic characteristics showed no association.
* Médico Especialista en Medi-cina de Rehabilitación. Sub-director Médico de Clínica. Centro de Rehabilitación Infan-til Teletón, Baja California Sur, México.
‡ Médico Especialista en Medici-na de Rehabilitación. Instituto Nacional de Rehabilitación.
§ Médico especialista en Pedia-tría. Jefe de Enseñanza. Centro de Rehabilitación y Educación Especial, La Paz, México.
Dirección para correspondencia:Dra. Elsa María Ivon Pérez FloresAv. Golfo de California Núm. 1310Col. Benito Juárez, La Paz, Baja California Sur, 23090, México.Tel: +52 (612) 175 0929E-mail: [email protected]
Recibido: 19 de octubre de 2016.Aceptado: 25 de julio de 2017.
Conflicto de intereses: Se declara que no existe ningún tipo de conflicto de intereses con ninguno de los autores.
Este artículo puede ser consultado en versión completa en: http://www.medigraphic.com/rid

Investigación en Discapacidad100
Índice de asistencia en adolescentes con PC
www.medigraphic.org.mx
Introducción
La adherencia terapéutica se defi ne como el grado en el que los pacientes se apegan a los componentes de su tratamiento.1 La falta de adherencia terapéutica es un fenómeno mundial que se observa en casi todos los estadios de las enfermedades crónicas y tiende a incrementarse a medida que el paciente lleva más tiempo con el tratamiento.2 Sucede hasta en 65% de los pacientes que llevan a cabo programas de casa y en 10% de quienes llevan programas en instituciones.3
En rehabilitación es frecuente la falta de adherencia debido a factores propios de los pacientes como la presencia de discapacidad o los problemas relaciona-dos con la movilidad y los traslados que les difi cultan acudir a los centros de atención.3 Los porcentajes de asistencia a las sesiones programadas de terapia se utilizan como indicadores de adherencia. El cálculo del índice de asistencia (IA) proporciona un indicador de la frecuencia con la que los pacientes acuden a sus citas programadas, este indicador facilita la posibili-dad de investigar la adherencia a los tratamientos de rehabilitación y es la razón del número de sesiones asistidas entre el número de sesiones programadas.1
La investigación sobre la adherencia a regímenes pediátricos ha captado la atención en los últimos años debido al apego subóptimo que se observa en tratamientos médicos y terapéuticos por las implicaciones personales, sociales y clínicas que sub-yacen tanto en el niño o el adolescente como en su familia o cuidadores.4 La Organización Mundial de la Salud (OMS) defi ne la adolescencia como el periodo de crecimiento y desarrollo humano que se produce después de la niñez y antes de la edad adulta, entre los 10 y 19 años5 y esta etapa de la vida es clave para el diseño de programas de rehabilitación en casa de los pacientes con discapacidad, ya que es indispensable la participación del sujeto con un papel activo en el proceso para mantener o evitar la pérdida funcional, así como promover la participación social y económica del individuo.1,3
Se ha demostrado que hasta 14% de los pacientes adultos que acuden a un servicio de terapia física no regresan a las citas de seguimiento y que la asistencia-adherencia a los tratamientos puede ser de hasta 19.2%.3,6
Los padres de los menores con discapacidad es-tán en riesgo de tener niveles bajos de asistencia, la cual se ha registrado entre 50 y 94%;7 sin embargo, no existen datos en adolescentes con discapacidad.
La parálisis cerebral (PC) se defi ne como un tras-torno del movimiento y la postura que se manifi esta
durante la lactancia o primeros años de la infancia, la cual es causada por una lesión no progresiva del cerebro antes, durante o poco después del nacimien-to, en general la lesión queda establecida durante los primeros dos años de vida postnatal. El daño al cerebro es permanente y no puede curarse, pero las consecuencias pueden minimizarse.8
La PC representa la causa más común de altera-ción motora severa en población pediátrica, con una incidencia mundial de dos a tres casos por cada 1,000 nacidos vivos.9 En México existen publicaciones que describen una tasa de tres casos nuevos por cada 10,000 nacidos vivos. En el año 2006 se estimaba que en México, por lo menos 500,000 personas y sus familias vivían afectadas por algún grado de PC.10
Aproximadamente 90% de los pacientes que se diagnostican con PC sobreviven hasta la adultez como resultado de una mejor intervención, además de ser susceptibles, con un riesgo similar al resto de la población, de adquirir otras condiciones médicas.11
Es importante identifi car los factores que infl uyen en la inasistencia a las sesiones de rehabilitación en este grupo poblacional, ya que se ha demostrado que es posible realizar intervenciones para mejorar la adherencia a los tratamientos y esto sólo se logra al identifi car las características y motivos de inasis-tencia a las citas de un programa de rehabilitación integral institucional, para establecer a futuro planes de intervención que permitan optimizar la utilización de recursos humanos, físicos y tecnológicos. Nuestra hipótesis de trabajo fue que existen factores clínicos y sociodemográfi cos que afectan el índice de asistencia en pacientes adolescentes con parálisis cerebral que acuden a un centro de rehabilitación.
El objetivo de este estudio fue obtener el índice de asistencia al tratamiento de rehabilitación de pacientes de 10 a 18 años de edad con diagnóstico de PC en un centro de rehabilitación, así como describir y analizar las características clínicas y sociodemográfi cas de esta población, junto con la identifi cación de los moti-vos de inasistencia reportados por los padres.
Material y métodos
Se realizó un estudio observacional, descriptivo y transversal en el Centro de Rehabilitación Infantil Te-letón en Baja California Sur en La Paz, México.
Sujetos de estudio. Se incluyeron pacientes con diagnóstico clínico de PC, entre 10 y 18 años de edad, de cualquier sexo, que acudieron al centro en el periodo de enero a diciembre de 2014, cuyos padres aceptaron participar en el estudio bajo fi rma de con-

Volumen 6 Número 3 Septiembre-Diciembre 2017 101
Elsa Pérez-Flores y cols.
www.medigraphic.org.mx
sentimiento informado institucional. Se excluyeron a aquéllos dados de baja o que dejaron de acudir durante el periodo de evaluación. Se eliminaron pacientes que no contaban con registro de citas programadas en el expediente clínico.
Procedimiento. Se realizó la búsqueda y revisión de la información en la base de datos del expediente electrónico seleccionando a aquéllos que cumplieron los criterios de selección. De los 338 pacientes activos en el centro se revisó a los que contaban con diagnóstico de parálisis cerebral, incluyendo a todos los pacientes que cumplieron con los criterios de inclusión, abarcando la población total, no se eliminó ningún paciente.
Se recabaron los datos sociodemográfi cos (edad, sexo, lugar de residencia, escolaridad, ingreso eco-nómico familiar mensual y medio de transporte que el paciente utiliza para llegar al centro de rehabilitación), características clínicas (tipo de parálisis cerebral según el trastorno motor predominante y el nivel del sistema de la clasifi cación de la función motora gruesa SCFMG), así como los datos relacionados con la asistencia a consultas (número de citas programadas tomadas, no tomadas, el motivo de inasistencia y si éste fue repor-tado o no), los cuales provenían de la historia clínica, las notas de la evolución y el registro de las agendas electrónicas del 01 de enero al 31 de diciembre de 2014. Se obtuvo la cantidad total de citas tomadas y no tomadas, dividiendo las no tomadas en inasistencias justifi cadas cuando tenían motivo reportado por los padres y no justifi cadas cuando no se informó el moti-vo. Se incluyeron consultas médicas de rehabilitación, ortopedia, pediatría, neurología, comunicación humana, enfermería, psicología, trabajo social así como los ser-vicios de terapia física, ocupacional, lenguaje y talleres.
Se realizó la revisión y cuantifi cación de los motivos de inasistencias justifi cadas, los cuales pertenecen a categorías predefi nidas en el sistema de agendas y son: actividad escolar, citas en otra institución, contra-tiempos, falta de recursos económicos, enfermedad del paciente y problemas familiares; y como inasisten-cias no justifi cadas aquéllas en las que los padres no notifi caron motivo alguno.
El protocolo fue registrado y aprobado ante el Comi-té de Ética e Investigación del Centro de Rehabilitación Infantil Teletón Baja California Sur.
Análisis estadístico. Se llevó a cabo análisis mediante estadística descriptiva y posteriormente un análisis bivariado mediante Chi cuadrada (χ2) y T de Student para calcular la diferencia de medias o proporciones de acuerdo con el tipo y distribución de variables. Para establecer el análisis de correlación se utilizó la prueba de r de Pearson o rho de Spearman de
acuerdo con el tipo de variable. Se consideró nivel de signifi cancia alfa aquél menor de 0.05. El análisis se realizó en el software estadístico IBM SPSS versión 20.
Resultados
Se recabó una muestra total de 62 pacientes. La edad promedio fue de 13.58 ± 2.55 años. Las característi-cas clínicas y sociodemográfi cas de los pacientes se resumen en el cuadro I.
Cuadro I. Características clínicas y sociodemográficas.
Características n (n = 62) %
Sexo Femenino Masculino
1943
30.669.4
Tipo de PC Espástica bilateral Espástica unilateral Discinética distónica Discinética coreoatetósica Atáxica
506510
80.69.78.11.60
SCFMG I II III IV V
64
111427
9.76.5
17.722.643.5
Paciente escolarizado Sí No
4814
77.422.6
Medio de transporte Transporte público Vehículo propio
2042
32.367.7
Ingreso familiar mensual* < $1,000 pesos $1,001 a $5,000 pesos $5,001 a $15,000 pesos Más de $15,000 pesos
13424
3
1.654.838.7
4.8
Lugar de residencia Local Foráneo
3131
5050
PC = Parálisis cerebral; SCFMG = Sistema de Clasifica-ción de la Función Motora Gruesa. * El ingreso familiar se clasificó acorde a los rangos del Sistema Infantil Teletón.

Investigación en Discapacidad102
Índice de asistencia en adolescentes con PC
www.medigraphic.org.mx
Tras la comparación de las características socio-demográfi cas entre los dos grupos no se encontraron diferencias estadísticamente signifi cativas (p > 0.05) respecto a la distribución por edad, sexo, tipo de PC, SCFMG, escolaridad, medio de trasporte e ingreso familiar mensual; excepto por el lugar de residencia, en el grupo 1 se observó que 65.6% de los pacientes eran foráneos (con lugar de residencia distinto de la ubicación del centro de rehabilitación) y en el grupo 2 fue 33.3% (p = 0.007).
Discusión
En este estudio se calculó un IA de 0.72 en pacientes adolescentes con PC que acudieron a su tratamiento de rehabilitación en el periodo de un año. Contrastando nuestros datos con la literatura, Sabit12 reportó 67% de asistencia a un programa de terapia pulmonar, mientras que en su análisis de la adherencia a los tratamientos de terapia física en población adulta con patología ortopédica Adrián6 observó una asistencia de 80.8%. Bassett et al.1 registraron un porcentaje de asistencia de 85% en pacientes con hernia de disco y de 89% en aquéllos con lumbalgia mecánica. En población pediátrica se reportó que hasta 50% de los padres no se adhieren a regímenes terapéuticos; Law y King14 informaron una asistencia de 66% a un programa de rehabilitación en población pediátrica con parálisis cerebral. Basados en esta revisión el IA en tratamientos de rehabilitación en la población estudiada es similar a lo descrito por otros autores.
Contrario a lo que podría suponerse, las variables como la edad, el tipo de PC o la severidad de la enfermedad medida través del nivel de SCFMG no modifi can el índice de asistencia que se obtuvo, los resultados demuestran que ninguna de las caracte-rísticas clínicas se asoció de forma estadísticamente signifi cativa al IA.
Jin et al.15 describen en una revisión que existe asociación entre la edad y la adherencia al tratamien-to, afi rmando que en poblaciones más jóvenes ésta tiende a ser más baja que en poblaciones adultas y adultas mayores, refi eren que la baja adherencia a los tratamientos ocurre también en adolescentes y niños con enfermedades crónicas. En lo referente al sexo los resultados de los estudios revisados fueron contradictorios y en el nivel educativo o escolaridad se constató que en general no es un buen predictor de asistencia, sin encontrar nosotros tampoco signifi -cancia en ninguna de estas variables.15
A pesar de que los pacientes con niveles III, IV y V del SCFMG por mayor afectación de su movilidad
Durante el periodo evaluado se programó un total de 7,257 citas a los pacientes incluidos en el estudio para los diversos servicios de rehabilitación en el centro de rehabilitación, de las cuales 1,971 (27.2%) se registraron como inasistencias, por lo que el IA global fue de 0.728. El promedio de citas programa-das por paciente fue de 117.05 ± 38.8. Los motivos de inasistencia reportados por los padres o tutores por los que los pacientes no acudieron a sus citas programadas fueron: sin motivo específi co o falta no justifi cada 69.92%, problemas familiares 13.24%, falta de recursos económicos 6.9%, enfermedad del paciente 6.24%, cita en otra institución 2.44%, con-tratiempos automovilísticos 0.66% y por actividad escolar 0.61%.
En el análisis bivariado no se encontraron correla-ciones signifi cativas entre el IA y las características clínicas y sociodemográfi cas y entre las correlaciones entre IA y motivos de inasistencia sólo se detectó una correlación signifi cativa en el reporte de falta de recur-sos económicos (r = -0.558, p = 0.031).
La muestra de pacientes incluidos en el estudio se dividió de manera arbitraria dentro de los rangos de porcentaje de asistencia descritos en la literatura,12,13 creando dos grupos para el análisis estadístico de los datos; el grupo 1 con «asistencia irregular» (IA menor de 0.75) y el grupo 2 con «asistencia regular» (IA mayor o igual de 0.75); 32 pacientes correspon-dieron al grupo 1 y 30 al grupo 2. El IA promedio para el grupo 1 fue de 0.6 ± 0.1 y para el grupo 2 de 0.82 ± 0.05 (Figura 1).
Pobre asistencia < 75% Buena asistencia ≥ 75%Grupo índice de asistencia
Índi
ce d
e as
isten
cia
1.00
.80
.60
.40
.20
.00
Figura 1. Distribución del índice de asistencia en pa-cientes adolescentes con parálisis cerebral agrupados por asistencia regular y asistencia irregular.

Volumen 6 Número 3 Septiembre-Diciembre 2017 103
Elsa Pérez-Flores y cols.
www.medigraphic.org.mx
necesitan para su desplazamiento algún dispositivo de movilidad (silla de ruedas manual o eléctrica, andade-ra, carriola) no se confi rmó que la severidad fuera un factor que interviniera con la asistencia. Estos resul-tados coinciden con lo publicado por otros autores,12,14 pero contrastan con lo descrito por Batysheva,16 quien en un estudio efectuado en padres de pacientes con daño neurológico mostró que factores como el sexo, la edad del niño, el nivel de educación y las caracte-rísticas de la enfermedad afectaban la adherencia al tratamiento.
Este estudio revela una diferencia estadísticamente signifi cativa entre el lugar de residencia y el IA, demos-trando que los pacientes locales acuden más a sus citas. Asefzadeh et al.13 observaron en una muestra de pacientes de todos los grupos de edad (de 14 a 78 años) de una unidad de medicina interna y cardiología que entre los factores reportados con más frecuencia relacionados con la falta de adherencia estaban el tener que recorrer grandes distancias al sitio de la clínica. Esto puede explicarse17 debido a que las fa-milias que perciben que hay más obstáculos son más propensas a no completar todo el programa de terapia o a no seguir las recomendaciones.
Coincidiendo con lo descrito por Law y King14 que refi ere que el estatus socioeconómico no es un factor predictivo de la adherencia de los padres al tratamien-to, nosotros tampoco establecimos ninguna asociación con el ingreso económico. Galil A, Carmel S, Lubetzky H y Vered S7 afi rman que la relación entre estatus so-cioeconómico y la adherencia es inconclusa: algunos estudios no mencionan relación alguna, mientras que en otros se encontró una fuerte relación entre estatus socioeconómico bajo y la falta de adherencia.
Otro estudio realizado en población pediátrica4 con diagnóstico de pie equino varo reveló que las difi cul-tades económicas, distancias muy largas de su casa al hospital, mala comunicación con el médico, falta de apoyo familiar y mucho tiempo de espera en las clínicas son factores que los padres consideraban que afectaban la adherencia al tratamiento, aunque éste fue un estudio de percepción. Se ha descrito3 en otros estudios que los problemas de transporte, necesida-des de cuidado de los niños, horario de trabajo, falta de tiempo, el número de dependientes familiares, las difi cultades fi nancieras, la conveniencia y el olvido son factores que afectan la adherencia. De estos factores los tres que se analizaron en nuestro estudio fueron el medio de transporte utilizado, el cual no resultó signifi cativo; sin embargo, sí se obtuvo una correla-ción signifi cativa entre las inasistencias y el lugar de residencia, así como el reporte de falta de recursos
económicos como motivo de las inasistencias por parte de los padres y el IA, siendo que la percepción de falta de recursos no equivale a la correlación con el ingreso económico, pudiendo arrojar que es necesario explorar más profundamente esta variable incluyendo otros factores contextuales.
Aliabadi et al.17 en su estudio para detectar barreras para acudir a las sesiones de rehabilitación de pacien-tes pediátricos iraníes con discapacidad realizaron la medición del nivel de asistencia a las sesiones, éste se obtuvo acorde al número de sesiones prescritas contra quienes asistieron en el último mes de tratamiento y el cálculo se efectuó multiplicándose por 100. Posterior a esto se clasifi caron en dos categorías: como «apega-dos» y «no apegados», defi niendo como límite 90% y colocando con «buena adherencia» a los padres que se ubicaban por arriba de este nivel y con «adheren-cia defi ciente» a quienes estaban por debajo de esta cifra. En su población detectaron que sólo 47.8% de los menores cumplieron con una asistencia regular a sus sesiones de terapia. Se constató que al dividir los grupos en asistencia regular y asistencia irregular tomando como corte 75%, el porcentaje de pacientes con asistencia regular fue de 48% coincidiendo con el reporte anterior.
Esto último apoya lo que afi rman Law y King14 con respecto a que la asistencia no depende del todo del control de los padres o pacientes pediátricos: existen muchas situaciones en la vida diaria que pueden inter-ferir con la asistencia y no refl eja la motivación de los padres para cumplir con los regímenes terapéuticos. Los clínicos no deben asumir que los pacientes que no se presentan a la terapia de manera frecuente no están cumpliendo con la terapia en casa, deben ser sensibles a las diferentes razones por las cuales no pueden acudir a las sesiones de terapia y entender que la inasistencia puede deberse más a razones prácticas que a la falta de motivación o involucramiento.
Conclusiones
El IA que presenta este grupo de pacientes es similar al publicado en otras poblaciones similares. Tan solo el vivir fuera de la ciudad es un factor que interviene en la adherencia terapéutica en este grupo de pacientes. El resto de las características clínicas o sociodemográ-fi cas no mostró ninguna asociación, aunque hay una correlación entre las inasistencias y el reporte de falta de recursos económicos como motivo de inasistencia por parte de los padres.
Debido a los altos índices de falta de adherencia terapéutica en los tratamientos de rehabilitación, los

Investigación en Discapacidad104
Índice de asistencia en adolescentes con PC
www.medigraphic.org.mx
equipos multidisciplinarios deberían incorporar a la evaluación de rutina de los pacientes el reporte y seguimiento de la adherencia terapéutica como parte de su quehacer cotidiano.
Es necesario en estudios posteriores analizar de manera más amplia y multidimensional los factores que intervienen en la adherencia al tratamiento, bus-cando no sólo los índices de asistencia, sino otras alternativas de abordaje del problema como factores cualitativos internos y externos que pudieran afectar la adherencia y de esta manera diseñar estrategias de intervención. Es posible que se necesite ampliar el periodo de seguimiento para obtener mayores datos.
Bibliografía
1. Bassett S. The assessment of patient adherence to physiotherapy. NZ J Physiother. 2003; 31 (2): 60-66.
2. Silva GE, Galeano E, Correa JO. Adherencia al tratamiento implicaciones de la no-adherencia. Acta Med Colomb. 2005; 30 (4): 268-273.
3. Jack K, McLean SM, Moffett JK, Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. Man Ther. 2010; 15 (3): 220-228. doi:10.1016/j.math.2009.12.004
4. Herman K. Barriers experienced by parents/caregivers of children with clubfoot deformity attending specifi c clinics in Uganda [dissertation] Republic of South Africa: University of the Western Cape. 2006.
5. Borrás ST. Adolescencia: defi nición, vulnerabilidad y oportunidad. Correo Científi co Médico de Holguin. 2014; 18 (1): 5-7.
6. Adrián F. Análisis de la adherencia a los tratamientos kinésicos. Revista del Hospital J.M. Ramos Mejía. 2007; 12 (1): 1-31.
7. Galil A, Carmel S, Lubetzky H, Vered S, Heiman N. Compliance with home rehabilitation therapy by parents of children with disabilities in Jews and Bedouin in
Israel. Dev Med Child Neurol. 2007; 43 (4): 261-268. doi: 10.1111/j.1469-8749.2001.tb00200.x
8. Berker AN, Yalc MS. Parálisis cerebral: aspectos ortopédicos y rehabilitación. Pediatr Clin N Am. 2008; 55: 1209-1225. doi:10.1016/S0186-159X(08)55089-3
9. Reddihough DS, Collins KJ. The epidemiology and causes of cerebral palsy. Aust J Physiother. 2003; 49 (1): 7-12.
10. Guía de Práctica Clínica Abordaje y manejo del niño con parálisis cerebral infantil con comorbilidades neurológicas y musculoesqueléticas. México: Secretaría de Salud, 2010.
11. Redmond R, Parrish M. Variables influencing physiotherapy adherence among young adults with cerebral palsy. Qual Health Res. 2008; 18 (11): 1501-1510. doi: org/10.1177/1049732308325538
12. Sabit R, Griffi ths TL, Watkins AJ, Evans W, Bolton CE, Shale DJ et al. Predictors of poor attendance at an outpatient pulmonary rehabilitation programme. Respiratory Medicine. 2008; 102 (6): 819-824. doi: 10.1016/j.rmed.2008.01.019
13. Asefzadeh S, Asefzadeh M, Javadi H. Care Management: Adherence to Therapies Among Patients at Bu-Alicina Clinic, Qazvin, Iran. JRMS. 2005; 10 (6): 343-348.
14. Law, M, King G. Parent compliance with therapeutic interventions for children with cerebral palsy. Dev Med Child Neurol. 1993; 35 (11): 983-990. doi: 10.1111/j.1469-8749.1993.tb11580.x
15. Jin J, Sklar GE, Min Sen Oh V, Chuen Li S. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther Clin Risk Manag. 2008; 4 (1): 269-286.
16. Batysheva TT, Bykova OV, Vinogradov AV. Family’s adherence to treatment of the child with a neurological pathology. Zh Nevrol Psikhiatr Im S S Korsakova. 2012; 112 (7 Pt 2): 56-63.
17. Aliabadi S, Hatamizadeh N, Vamghi R, Kazemnejad A. Children with disability: barriers to regular attendance in rehabilitation sessions. J Res Rehabil Sci. 2012; 8 (5): 959-969.

Volume 6 Number 3 September-December 2017 105
Key words: Bacteria, susceptibility
antimicrobial test, accuracy, biochemistry/methods.
Palabras clave:
Bacterias, susceptibilidad antimicrobiana, exactitud,
bioquímica/métodos.
www.medigraphic.org.mx
Comparison of the MicroScan WalkAway and VITEK 2 Compact systems for the identification and susceptibility of clinical Gram-positive and Gram-negative bacteria Comparación de los sistemas MicroScan WalkAway y VITEK 2 Compact para la identifi cación y susceptibilidad de bacterias Gram-positivas y Gram-negativas de aislados clínicos
Melissa Hernández-Durán,* Luis E López-Jácome,* Claudia A Colín-Castro,* Guillermo Cerón-González,* Silvestre Ortega-Peña,* E Samuel Vanegas-Rodríguez,* Jaime A Mondragón-Eguiluz,* Rafael Franco-Cendejas*
Original article
Vol. 6, No. 3 September-December 2017
pp 105-114
Abstract
Introduction: The accuracy and fastness in bacterial identification and antimicrobial susceptibility are essentials in the management of the hospitalized patients with infectious diseases. Methodology: This study compares the usefulness of the semi-automated VITEK 2®
Compact system vs. against the MicroScan WalkAway® SI system for bacterial identification and antimicrobial susceptibility. We included 54 bacterial strains isolated from hospitalized patients, 20 were Gram-positive cocci, 34 Gram-negative rods and 13 reference strains. Results: Of these strains, 89.5% were successfully identified at the species level by both systems. Concordance in susceptibility was 90.2% for Gram-negative and 96.3% for Gram-positive bacteria. Median delay time in obtaining the results of susceptibility testing was 6.5 h for VITEK 2 and 12.5 h for MicroScan. The MicroScan system presented a longer delay in obtaining results and greater difficulty in the correct identification of Gram-negative bacteria, Conclusions: Identification systems are a necessary tool in microbiological laboratories. Prompt and correct identification of clinical isolates aids in appropriate antimicrobial treatment.
Resumen
Introducción: La precisión y rapidez en la identificación bacteriana y la susceptibilidad an-timicrobiana son esenciales en el manejo de los pacientes hospitalizados con enfermedades infecciosas. Metodología: Este estudio compara la utilidad del sistema semi-automatizado VITEK 2® Compact contra el sistema MicroScan WalkAway® SI para la identificación bacteriana y la susceptibilidad antimicrobiana. Se incluyeron 54 cepas bacterianas aisladas de pacientes hospitalizados, 20 fueron cocos Gram-positivos, 34 bacilos Gram-negativos y 13 cepas de refe-rencia. Resultados: De estas cepas, el 89.5% fueron identificadas con éxito a nivel de especie por ambos sistemas. La concordancia en la susceptibilidad fue de 90.2% para Gram-negativos y 96.3% para bacterias Gram-positivas. El tiempo medio de demora en la obtención de los resultados de la prueba de susceptibilidad fue de 6.5 h para VITEK 2 y 12.5 h para MicroScan. Conclusiones: Los sistemas de identificación son una herramienta necesaria en los laboratorios de microbiología. La identificación rápida y correcta de los aislamientos clínicos ayuda en el tratamiento antimicrobiano apropiado.
* Laboratorio de Infectología, Centro Nacional de Investiga-ción y Atención a Quemados (CENIAQ), Instituto Nacional de Rehabilitación (INR), Mexico City, Mexico.
Mailing address:Rafael Franco Cendejas M.D., MSc.División de Infectología, CENIAQ,Instituto Nacional de Rehabilitación«Luis Guillermo Ibarra Ibarra».Av. México-Xochimilco Núm. 289,Col. Arenal de Guadalupe, 14389, Del. Tlalpan, Ciudad de México, México.Phone: (+52) (55) 5999 1000, ext. 14801Fax: (+52) (55) 5603 9127E-mail: [email protected]
Received: March 10, 2017.Accepted: July 11, 2017.
This article can be read in its full version in the following page:http://www.medigraphic.com/rid

Investigación en Discapacidad106
Bacterial identification and susceptibility systems
www.medigraphic.org.mx
Introduction
Clinical laboratories manage semi automated systems for the identifi cation and bacterial susceptibility that is associated with the increased volume at hospitals, in addition to offering a cost reduction and linking with the laboratory interfaces or hospitalary informatics systems.1 Each system possesses its strengths and weaknesses; however, correct bacterial identifi cation of patients with an infectious process and its corresponding result of susceptibility in vitro constitute a basic tool for accurate treatment of the patient; without correct bacterial identifi cation, morbimortality and health-system costs increase.2 Rapidity in the diagnosis and treatment of the infections is not solely refl ected in the patient’s health, but also in the emergence of strains resistant to multiple antibiotics. The well-aimed, rapid, and timely identifi cation of Multi Drug-Resistant (MDR) clinical isolates in the nosocomial ambit permits the prompt application of precautionary measures to delimit and avoids the propagation of bacteria with these patterns of resistance.3 The grounds for semi automated systems is based on different analytical methods, such as colorimetry, turbidimetry, or fl uorometry, in which bacterial development is detected in micro panels containing different substrates to achieve the identifi cation and serial dilutions of different antibiotics, which in turn allows for establishing minimum inhibitory concentrations (MIC).4 The VITEK 2® Compact system utilizes colorimetric technology accompanied by the employment of three wave longitudes in order to provide the general profi les of clinically important organisms. Antimicrobial susceptibility is performed by means of test cards containing standardized dilutions of distinct antibiotics corresponding to susceptibility cut-off points established by the Clinical and Laboratory Standards Institute (CLSI).5,6 Species identifi cation by this system is completed in a median of 3 hours, but can last from 5–7 hours in slow-growth or problematic microorganisms. Susceptibility results can take up to 15 hours, with a mean of around 9 hours.3,6 On the other hand, the MicroScan WalkAway® SI (MicroScan) system utilizes fl uorescent technology. MicroScan panels are conventional, 96-well microdilution plates. Bacteria can be determined within an average of 4 hours, but can be 6-42 hours in slow-growth bacteria. The results of susceptibilities can be obtained in 20 hours, within a range of 16.8-27.8 hours, depending on the bacteria.3,6 Comparative studies have been conducted between both equipments;7-9 however, there are few studies that compare multiple clinical isolates.9,10 The objective of this study was to compare the results
of the identifi cation and bacterial susceptibility of clinical samples and strains of the American Type Culture Collection (ATCC); comparison of the susceptibility tests by the MIC method were conducted according to CLSI recommendations,11 as well as times for obtaining the results procured by the VITEK 2 and the MicroScan systems.
Material and methods
Clinical isolates and reference strains: fi fty four clinical isolates were analyzed during the months of July and August 2011, in a simultaneous and comparative manner, of Gram-negative bacilli and Gram-positive cocci associated with infectious processes deriving from hospitalized patients; the reason for employing clinical isolates was to manifest a current and real situation of the systems in the clinical laboratory. We also utilized 13 reference strains, which included 9 genuses and 11 species, such as the following: Pseudomonas (1 isolate); Stenotrophomonas (1 isolate); Escherichia (2 isolates); Enterobacter (1 isolate); Proteus (1 isolate); Staphylococcus (2 isolates); Enterococcus (3 isolates); Streptococcus (1 isolate), and Listeria (1 isolate) (Table I).
Identifi cation methods: In all of the strains, Gram staining was carried out in order to classify these according to the staining characteristics conferred by the walls of the bacteria; fast biochemical tests were carried out, which consisted of the fast indole and oxidase reaction for Gram-negative bacilli, while in the case of Gram-positive cocci, catalase and coagulase tests were conducted. For identifi cation and susceptibility by the VITEK 2 system (bioMérieux, Marcy d’Etoile, France), Gram-negative (GN) bacterial and identifi cation test cards were used, which contains 47 substrates and AST-N087, which contains 12 antibiotics. For Gram-positive microorganisms, we utilized Gram-positive (GP) test cards, which contain 43 substrates, and AST-GP67, which has 14 antibiotics. A bacterial concentration at 0.5 in McFarland standards was employed for bacterial identifi cation. A bacterial lo ad of 6.9 × 106 Colony-Forming Units (CFU)/mL was used in Gram-positives and one of 1.2 × 107 CFU/mL Gram-negatives for the susceptibility analysis, and MPI Library ver. 04.02 software was utilized.
For evaluation of the MicroScan WalkAway SI system (Siemens Healthcare Diagnostics, West Sacramento, CA, USA), we utilized Neg 44 Combo panels that contain 33 substrates and 26 antibiotics for Gram-negatives in the same panel, and the Pos 33 Combo panel, which contains 27 substrates and 14 antibiotics for Gram-positives in the same panel.

Volume 6 Number 3 September-December 2017 107
Melissa Hernández-Durán et al.
www.medigraphic.org.mx
LabPro ver. 2.0 software was utilized. Identifi cations were accepted with a level of ≥ 90%. For susceptibility, we evaluated the MIC reported for each system.
Confi rmatory methods: for correct identifi cation of discordant strains, we utilized the conventional biochemical identification schemas according to Murray and colleagues,3 according to each case. For susceptibility, results were proven by MIC, according to CLSI criteria for the corresponding microorganism.5
The antibiotics that were compared by both methods were the following for Gram-negatives: ampicillin; amikacin; gentamicin; ciprofloxacin; cefepime; ceftazidime; ertapenem (except for Pseudomonas aeruginosa); imipenem; meropenem; piperacillin/tazobactam; trimethoprim-sulfamethoxazole, and tigecycline. For Gram-positives, the antibiotics were as follows: ampicillin; ciprofloxacin; erythromycin; linezolid; oxacillin (only for Staphylococcus spp.); rifampicin (except for Enterococcus spp.); quinupristin/dalfoprist in; tr imethoprim-sulfamethoxazole; teicoplanin; vancomycin; high-concentration gentamicin, and high-concentration streptomycin (the latter two only for Enterococcus spp.), according to the case. Discordant results were confi rmed by MIC, which were classifi ed as errors depending on the results in the following manner: serious error, when result was resistant due to the confi rmation method but susceptible due to the system utilized; major error, when the result was susceptible to the confi rmation method but resistant to the system utilized, and minor error, when the result was sensitive or resistant to the conformation method but intermediate to the system utilized. Times were compared in the emission of the defi nitive results of identifi cation and susceptibility obtained for both methods, considering delay time as well as time necessary in hours for emitting the results of identifi cation and antimicrobial susceptibility.
Statistical analysis: to determine whether there were differences in the identifi cation rates between both systems, we utilized χ2 statistical test. The result of each identifi cation result with VITEK 2 system and the MicroScan system was marked as «correct» or «incorrect» in each aspect of genus and species.
Comparison of median time was carried out with the Mann-Whitney U test, considering p < 0.05 as a signifi cant value. The STATA ver.12.0 statistical software program was employed.
Results
The 54 clinical isolates corresponded to 34 Gram-negative bacilli and to 20 Gram-positive cocci (Table I).
Table I. Clinical and reference strains used in the study.
Microorganism n
Clinical isolates
Acinetobacter baumannii 9
Pseudomonas aeruginosa 9
Aeromonas hydrophila 3
Burkholderia cepacia 1
Escherichia coli 6
Citrobacter koseri 1
Citrobacter freundii 1
Serratia marcescens 1
Klebsiella oxytoca 1
Enterobacter cloacae 2
Staphylococcus aureus 3
Staphylococcus epidermidis 2
Staphylococcus conhii 1
Staphylococcus haemolyticus 1
Enterococcus faecalis 9
Enterococcus faecium 2
Enterococcus casseliflavus 1
Streptococcus pneumoniae 1
ATCC strains
Staphylococcus aureus ATCC 29213 1
Staphylococcus sciuri ATCC29061 1
Enterococcus casseliflavus ATCC700327
1
Enterococcus faecalis ATCC 29212 1
Enterococcus faecalis ATCC 51299 1
Listeria monocytogenes ATCC BAA-751
1
Escherichia coli ATCC 25922 1
Escherichia coli ATCC 35218 1
Proteus vulgaris ATCC 6380 1
Enterobacter cloacae ATCC 7003323 1
Stenotrophomonas maltophilia ATCC1766
1
Pseudomonas aeruginosa ATCC 27853
1
Streptococcus pyogenes ATCC 19615
1
Total 67

Investigación en Discapacidad108
Bacterial identification and susceptibility systems
www.medigraphic.org.mx
One hundred percent (100%) identification was achieved for Gram-negative bacilli and for Gram-positive cocci by the VITEK 2 system; however, 31 (91%) Gram-negative bacilli and 18 (90%) Gram-positive cocci were identifi ed by the MicroScan system. Of the 67 isolates, concordance was obtained in bacterial identifi cation at the genus level in 61 (91%) and at
the species level in 60 (89.5%) isolates (Table II). The discordant strains included 4 Gram-positive cocci and 3 Gram-negative bacilli, with the MicroScan system, which only presented discordant strains in 6 clinical isolates (Table III). For ATCC strains (n = 13), 100% reproducibility was obtained in the results for the two systems for Gram-negative bacilli and Gram-positive
Table II. Identification results comparison between VITEK 2 and MicroScan systems.
Microorganisms
VITEK 2 MicroScanConcordance
(%)Genus Species Genus Species
No Enterobacteriaceae (n)
A. baumannii 9 9 8 8 89
P. aeruginosa 9 9 9 9 100
A. hydrophila 3 3 3 3 100
B. cepacia 1 1 0 0 0
P. aeruginosa ATCC 27853 1 1 1 1 100
S. maltophilia ATCC 1766 1 1 1 1 100
Subtotal n (%) 24 (100) 24 (100) 22 (90.9) 22 (90.9)
Enterobacteriaceae (n)
E. coli 6 6 5 5 83.30
C. freundii 1 1 1 1 100
C. koseri 1 1 1 1 100
S. marcescens 1 1 1 1 100
K. oxytoca 1 1 1 1 100
E. cloacae 2 2 2 2 100
E. coli ATCC 25922 1 1 1 1 100
E. coli ATCC 35218 1 1 1 1 100
E. cloacae ATCC 700323 1 1 1 1 100
P. vulgaris ATCC 6380 1 1 1 1 100
Subtotal n (%) 16 (100) 16 (100) 15 (91.6) 15 (91.6)
Staphylococcus sp.
S. aureus 3 3 3 3 100
S. epidermidis 2 2 2 2 100
S. conhii 1 1 1 1 100
S. haemolyticus 1 1 0 0 0
S. aureus ATCC 29213 1 1 1 1 100
S. sciuri ATCC 29061 1 1 1 1 100
Subtotal n (%) 9 (100) 9 (100) 8 (88.8) 8 (88.8)

Volume 6 Number 3 September-December 2017 109
Melissa Hernández-Durán et al.
www.medigraphic.org.mxcocci, and only Listeria monocytogenes ATCC BAA-751 was unable to be identifi ed by the MicroScan system. There was a signifi cant difference between the capacity of identifi cation between the two systems (p = 0.013).
In susceptibility studies for the clinical samples, 49 discordant results were found between both methods,
with 40 discordant results of Gram-negative bacilli in the following antibiotics: amikacin; aztreonam; ceftazidime; ciprofloxacin; cefepime; gentamicin; imipenem; meropenem; piperacillin/tazobactam, and 9 discordant results of Gram-positive cocci in the following: ciprofl oxacin; erythromycin; linezolid;
Table III. Seven discordant identified isolates between VITEK 2 and MicroScan systems.
Identification by conventional
biochemical tests*
Identification by biochemical tests between systems
VITEK 2 MicroScan
No Enterobacteriaceae B. cepacia A. baumannii
B. cepaciaA. baumannii
A. xylosoxidansE. brevis
Enterobacteriaceae E. coli E. coli C. freundii
Enterococcus sp. E. casseliflavusS. pneumoniae
E. casseliflavusS. pneumoniae
E. gallinarumE. faecalis
Staphylococcus sp. S. haemolyticus S. haemolyticus R. mucilaginosa
ATCC strains L. monocytogenesATCC BAA-751
L. monocytogenes N/I
Continuous Table II. Identification results comparison between VITEK 2 and MicroScan systems.
Microorganisms
VITEK 2 MicroScanConcordance
(%)Genus Species Genus Species
Enterococcus sp.
E. faecalis 9 9 9 9 100
E. faecium 2 2 2 2 100
E. casseliflavus 1 1 1 0 50
E. faecalis ATCC 29212 1 1 1 1 100
E. faecalis ATCC 51299 1 1 1 1 100
E. casseliflavus ATCC 700327 1 1 1 1 100
Subtotal n (%) 15 (100) 15 (100) 15 (100) 14 (92.3)
Streptococcus
S. pneumoniae 1 1 0 0 0
S. pyogenes ATCC 19615 1 1 1 1 100
Subtotal (%) 2 (100) 2 (100) 1 (50) 1 (50)
Others
L. monocytogenes ATCC BAA-751 1 1 0 0 0
Total n (%) 67 (100) 67 (100) 61 (91) 60 (89.5)

Investigación en Discapacidad110
Bacterial identification and susceptibility systems
www.medigraphic.org.mx
penicillin, and tetracycline. With ATTC strains, we obtained 10 discordances in susceptibility as follows: 8 in Gram-negative bacilli and 2 in Gram-positive cocci (Tables IV and V). The concordance obtained between these two systems was 89.9% for Gram-negative bacilli and 96.2% for Gram-positives. The 59 discordant results were classifi ed by error: the VITEK 2 system did not demonstrate serious errors, 8 errors (13.5%) were major and 4 (6.8%), minor, obtaining a greater amount of errors in Gram-negative bacilli; for the MicroScan system, 2 (3.4%) serious errors were obtained, in addition to 14 (23.8%) major errors and 31 (52.5%) minor errors, obtaining serious errors in Tetracycline for Gram-positive cocci.
Median time for fi nal identifi cation of Gram-negative Enterobacteriaceae was 5.1/12.33 hours and for non-Enterobacteriaceae of 6.8/26.7 hours, and in Gram-positive cocci, Staphylococcus spp., of 5.6/19.92 hours and Enterococcus spp., of 9.6/16.8 hours for the VITEK 2/MicroScan systems, respectively. The difference between global times between both equipments had a p of < 0.0005.
Discussion
Due to that clinical microbiology laboratories have become increasingly dependent on automated systems, the accuracy of these can be evaluated with clinical as well as with reference samples. In the present study, fi nal concordance of genus and species, as well as the susceptibility tests of different strains between two of the most utilized systems in
the hospital environment, were tested. Distinct studies have evaluated the performance of these systems for the bacterial identification and antimicrobial susceptibility of specifi c isolates;7-9 however, there are few studies with diverse clinical samples. With the advent of MultiDrug-Resistant (MDR) microorganisms, clinical laboratories must provide a result with respect to the causal microorganism and to the susceptibility that these microorganisms possess as soon as possible, these results being reliable for adequate infectious treatment and for maintaining adequate epidemiological vigilance. In this study, the VITEK 2 system demonstrated better performance in terms of strain identifi cation in comparison with the MicroScan system in genus (100 vs. 91%) and species levels (100 vs. 89.5%). Gram-negative bacilli presented more errors of identifi cation, as has been observed in previous reports, in which non-fermenter microorganisms had a higher proportion of identification.12 It has also been suggested that for slow-metabolism bacteria, such as collection strains stored under ultrafreezing, for non-fermenter bacteria, a suffi ciently long, 24-h incubation period is recommended in commercial kits or conventional means with the purpose of better identifi cation.12
With respect to identifi cation of Gram-positive cocci, it was observed that there were better results regarding Gram-negative bacilli, but the MicroScan system failed in three identifi cations, one of these of the genus Enterococcus. It was reported by Moore et al.13 that the VITEK 2 and MicroScan systems correctly identify 72 and 80% of the genus Enterococcus at the species
Table IV. Percentage of susceptibility concordance between VITEK 2 and MicroScan systems.
Gram negative bacilli n = 34
AK AZT CAZ CIP FEP GM ERT IMP MRP TZP SXT TIG
76.5 76.5 91.2 97 91.2 91.2 100 94.2 97 67.7 100 100
ATCC strains n = 6
100 50 66.7 75 100 100 100 100 100 66.7 100 100
Gram positive coccin = 19
AM CIP E LZD OXA P RIFA SYN SXT TE VA GN S ST S
100 89.5 94.8 89.5 100 89.5 100 100 100 89.5 100 100 100
ATCC strainsn = 5
100 80 100 100 100 100 100 100 100 80 100 100 100
AK = amikacin; AM = ampicillin; AZT = aztreonam; CAZ = ceftazidime; CIP = ciprofloxacin; FEP = cefepime; GM = genta-micin; ERT = ertapenem; IMP = imipenem; MRP = meropenem; TZP = piperacillin/tazobactam; SXT = trimethoprim-sulfa-methoxazole; TIG = tigecycline; LZD = linezolid; OXA = oxacillin; P = penicillin; RIFA = rifampicin, SYN = quinupristin-dalfo-printin; TE = tetracycline; VA = vancomycin; GN S = high concentration gentamicin; ST S = high concentration streptomycin.

Volume 6 Number 3 September-December 2017 111
Melissa Hernández-Durán et al.
www.medigraphic.org.mx
level, respectively; however, in the study of Won-Young et al.,9 something different was reported, in that the VITEK 2 and MicroScan systems identifi ed 92.3 and 76.9%, respectively, of the genus Enterococcus at the species level these differences in both studies can be attributed to the discrepancy between the organisms evaluated. In the case of identifi cation of the Staphylococcus genus, this has, to our knowledge, only been reported in an article with a comparison between both systems utilizing 120 clinical samples of Staphylococcus coagulase-negatives, finding correct identifi cation in 87.5 vs. 82.5%, in the VITEK 2 system vs. the MicroScan system.14 In our study of 11 clinical isolates, one Staphylococcus haemolyticus was not identifi ed by the MicroScan system, without observing errors in ATCC strains. Staphylococcus coagulase-negatives are increasingly identifi ed in medical complications, such as their association with medical devices. Thus, clinical laboratories should correctly identify these microorganisms at the species level by means of reliable and reproducible methods. The MicroScan system could not identify a Gram-positive bacillus corresponding to a ATCC strain (Listeria monocytogenes), the latter probably due to that the VITEK 2 system possesses a greater spectrum of microorganisms in its database with respect to the MicroScan system, and to that there can be differences in the software utilized in the equipment of both systems, as has been reported in other studies;15 however, the genus Listeria has been previously compared utilizing the MicroScan vs. the conventional VITEK system,16 employing food-transmitted pathogens, and sensitivity and specifi city for 100% identifi cation was observed of the former in comparison with 97.5% of the latter, which is not in agreement with the results that we obtained.
The accuracy and reproducibility of antimicrobial susceptibility are dependent on the skill and experience of the clinical laboratory staff; thus, the report should be corroborated and validated by the staff members themselves.17 The development of expert automated-equipment systems has allowed for an increase in reproducibility and in the veracity of susceptibility results; unfortunately, numerous studies have reported various errors in these systems when diverse combinations of antimicrobials are evaluated.18-20 Enterobacteriaceae family isolates of nosocomial samples present different mechanisms of resistance to multiple antibiotics, and this has become a general public health problem;21-23 thus, adequate reporting of susceptibility is obligatory. In this study, both systems exhibited adequate correlation in the majority of the
Table V. Percentage in susceptibility concordant results comparison between
VITEK 2 and MicroScan systems and broth microdilution test.
Microorganism n
Percentage of concordance
with BMD
VITEK 2 MicroScan
Gram negative bacilli
40 73.65% 19.6%
Clinical strainsAmikacin 8 100 0
Aztreonam 8 75 25
Ciprofloxacin 1 100 0
Cefepime 3 66.7 0
Ceftazidime 3 100 0
Gentamicin 3 66.7 33.3
Imipenem 2 100 0
Meropenem 1 0 100
Piperacillin/tazobactam
11 54.5 18.1
ATCC strains 8 100% 0%
Aztreonam 3 100 0
Ceftazidime 2 100 0
Ciprofloxacin 1 100 0
Piperacillin/tazobactam
2 100 0
Gram positive cocci
9 80% 20%
Clinical strainsTetracycline 2 100 0
Ciprofloxacin 2 100 0
Erythromycin 1 100 0
Linezolid 2 100 0
Penicillin 2 0 100
ATCC strains 2 100% 0%
Tetracycline 1 100 0
Ciprofloxacin 1 100 0
BMD = broth microdilution.

Investigación en Discapacidad112
Bacterial identification and susceptibility systems
www.medigraphic.org.mx
antibiotics; however, this was < 90% for Gram-negative bacilli of clinical isolates and ATCC strains in amikacin, aztreonam, ceftazidime, and piperacillin/tazobactam when these were compared with MIC with a greater percentage of major (MicroScan) and minor (VITEK 2) errors in this latter antibiotic between both systems, which can imply a lack in identifi cation of resistant strains. The correlation of susceptibility is considered adequate when this is < 10%, with < 1.5% serious errors and < 3% major errors and when total agreement with respect to MIC is > 90% 2. Commercial systems can identify producer strains of Extended-Spectrum Beta Lactamases (ESBL) and/or AmpC strains; however, there is poor capacity for differentiating these with carbapenemase producers, which should be a global priority due to that an increase in the number of these has been registered.21,24,25 For total Gram-positive cocci strains, there was a discordance in ciprofl oxacin and teicoplanin; additionally, the clinical isolates were discordant in penicillin and linezolid, which was reported previously in other studies.26 With the emergence of methicillin-resistant strains, adequate identification of this susceptibility for the genus Staphylococcus is required. These systems have been individually and comparatively evaluated in various studies,15,27-30 exhibiting adequate results with respect to the susceptibility of oxacillin, which is in agreement with our clinical results. We consider that the results found in bacterial identifi cation equipment should be corroborated according to a microbiological verdict with some other test, above all when its therapeutic importance could be relevant. Both systems presented errors in terms of susceptibility, with the MicroScan system presenting two serious errors, 24 major errors, and 31 minor errors, and the VITEK 2 system, 8 major and 4 minor errors. These differences can be due to the lack of standardization of the inoculum, in that the MicroScan system does not possess a constant inoculum. It is of utmost importance that commercial cases maintain updated software programs for adequate interpretation of susceptibility tests in that there can be errors in their fi nal interpretation. In the present study, we corroborated MIC and not interpretation to avoid this bias. Rapidity in obtaining identifi cation as well as susceptibility is one of the most important characteristics for users; in this study, global time was less than that in the VITEK 2 system, with a global median of 6 h (range, 2.75–18 h), presenting a delay in identifi cation of Enterococcus spp. The MicroScan system demonstrated a greater delay in all of the genuses with a median of 18 hr (range, 8–72 h), this greater in the non-Enterobacteriaceae, because
the system’s equipment requires more time for correct growth of the microorganism.
With the advent of novel identifi cation methods, such as systems with technology utilizing mass spectrometry, greater rapidity is promoted in identifi cation,31-33 which has advantages in providing timely treatment; however, the procedures are costly and are not accessible at all hospital units and, at the same time, do not solve the problem inherent in the identifi cation of bacteria highly related in species with similar molecular weights and in susceptibility tests still under development.33 In the present study, accuracy in MicroScan- and VITEK 2-system identification could be infl uenced by the differences in the number and distribution of the species of organisms tested, the software version, and the aptitude of the users. The performance of the two systems can also be related with the number of bacterial species tested by the systems’ manufacturers and enumerated in the systems’ databases. There are some differences in the number of bacterial species between the two systems’ identifi cation kit databases tested in this study, because the number of bacterial species of Gram-negative and -positive bacteria in the databases were 143 and 115 for VITEK 2 and 34 and 58 for MicroScan, respectively. There is no system that can achieve 100% identifi cation of the microorganisms. In addition, the combination of both systems has been recommended, in that this considerably increases the effi ciency of microbiological diagnoses; however, it also increases costs.9 The result of the present study is useful for demonstrating the behavior of two common system equipments during daily performance at a hospital unit. One limitations of this study comprises the amount of clinical isolates employed; however, these represent the microorganisms of the population of this institution, which refl ect the present fi ndings in habitual clinical situations. In conclusion, bacterial identification systems are useful for increasing efficiency in clinical laboratories. The VITEK 2 system appears to possess better performance in antimicrobial identifi cation and susceptibility, including study fi nalization time.
Acknowledgments
The authors thank the staff of the Clinical Pathology Laboratory and that of the Infectious Diseases Laboratory for their support, and the local authorities of the National Institute of Rehabilitation based in Mexico City. This work did not receive any external fi nancing for its realization.

Volume 6 Number 3 September-December 2017 113
Melissa Hernández-Durán et al.
www.medigraphic.org.mx
References
1. Rhoads S, Marinelli L, Imperatrice CA, Nachamkin I. Comparison of MicroScan WalkAway system and Vitek system for identifi cation of gram-negative bacteria. J Clin Microbiol. 1995; 33 (11): 3044-3046.
2. U.S. Food and Drug Administration. Guidance for industry and FDA. Class II special controls guidance document: antimicrobial susceptibility test (AST) systems. Silver Spring, MD: Center for Devices and Radiological Health, U.S. Food and Drug Administration; 2009. Disponible en: http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm071462.pdf
3. Murray P. Manual of clinical microbiology. U.S.A.: American Society for Microbiology; 2007.
4. Dallas AL, Pekarek PM, Mills TJ, Neal WJ, Smallbrook AG, Hejna J. Comparison of BD Phoenix to Biomerieux Vitek for the identifi cation and susceptibility testing of common bacterial isolates. 2005. Poster session presented at the 105th General Meeting of the American Society for Microbiolgy.
5. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; twenty-fi rst informational supplement M100-S19. Wayne, PA: CLSI; 2011.
6. Winstanley T, Courvalin P. Expert systems in clinical microbiology. Clin Microbiol Rev. 2011; 24 (3): 515-556.
7. Jure tschko S, Labombard i VJ , Lerner SA, Schreckenberger PC; Pseudomonas AST Study Group. Accuracies of beta-lactam susceptibility test results for Pseudomonas aeruginosa with four automated systems (BD Phoenix, MicroScan WalkAway, Vitek, and Vitek 2). J Clin Microbiol. 2007; 45 (4): 1339-1342.
8. Woodford N, Eastaway AT, Ford M, Leanord A, Keane C, Quayle RM et al. Comparison of BD Phoenix, Vitek 2, and MicroScan automated systems for detection and inference of mechanisms responsible for carbapenem resistance in Enterobacteriaceae. J Clin Microbiol. 2010; 48 (8): 2999-3002.
9. Jin WY, Jang SJ, Lee MJ, Park G, Kim MJ, Kook JK et al. Evaluation of VITEK 2, MicroScan, and Phoenix for identifi cation of clinical isolates and reference strains. Diagn Microbiol Infect Dis. 2011; 70 (4): 442-447.
10. Hindler JA, Humphries RM. Colistin MIC variability by method for contemporary clinical isolates of multidrug-resistant Gram-negative bacilli. J Clin Microbiol. 2013; 51 (6): 1678-1684.
11. Wikler MA; Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: Nineteenth informational supplement. Wayne, PA.: Clinical and Laboratory Standards Institute; 2009.
12. Jossart MF, Courcol RJ. Evaluation of an automated system for identifi cation of Enterobacteriaceae and nonfermenting bacilli. Eur J Clin Microbiol Infect Dis. 1999; 18 (12): 902-907.
13. Moore DF, Zhowandai MH, Ferguson DM, McGee C, Mott JB, Stewart JC. Comparison of 16S rRNA
sequencing with conventional and commercial phenotypic techniques for identifi cation of enterococci from the marine environment. J Appl Microbiol. 2006; 100 (6): 1272-1281.
14. Kim M, Heo SR, Choi SH, Kwon H, Park JS, Seong MW et al. Comparison of the MicroScan, VITEK 2, and Crystal GP with 16S rRNA sequencing and MicroSeq 500 v2.0 analysis for coagulase-negative Staphylococci. BMC Microbiol. 2008; 8: 233.
15. Eigner U, Schmid A, Wild U, Bertsch D, Fahr AM. Analysis of the comparative workfl ow and performance characteristics of the VITEK 2 and Phoenix systems. J Clin Microbiol. 2005; 43 (8): 3829-3834.
16. Odumeru JA, Steele M, Fruhner L, Larkin C, Jiang J, Mann E et al. Evaluation of accuracy and repeatability of identifi cation of food-borne pathogens by automated bacterial identifi cation systems. J Clin Microbiol. 1999; 37 (4): 944-949.
17. Mittman SA, Huard RC, Della-Latta P, Whittier S. Comparison of BD phoenix to vitek 2, microscan MICroSTREP, and Etest for antimicrobial susceptibility testing of Streptococcus pneumoniae. J Clin Microbiol. 2009; 47 (11): 3557-3561.
18. Donay JL, Mathieu D, Fernandes P, Prégermain C, Bruel P, Wargnier A et al. Evaluation of the automated phoenix system for potential routine use in the clinical microbiology laboratory. J Clin Microbiol. 2004; 42 (4): 1542-1546.
19. Doern GV, Brueggemann AB, Perla R, Daly J, Halkias D, Jones RN et al. Multicenter laboratory evaluation of the bioMérieux Vitek antimicrobial susceptibility testing system with 11 antimicrobial agents versus members of the family Enterobacteriaceae and Pseudomonas aeruginosa. J Clin Microbiol. 1997; 35 (8): 2115-2119.
20. Sader HS, Fritsche TR, Jones RN. Accuracy of three automated systems (MicroScan WalkAway, VITEK, and VITEK 2) for susceptibility testing of Pseudomonas aeruginosa against fi ve broad-spectrum beta-lactam agents. J Clin Microbiol. 2006; 44 (3): 1101-1104.
21. Cornaglia G, Rossolini GM. The emerging threat of acquired carbapenemases in Gram-negative bacteria. Clin Microbiol Infect. 2010; 16 (2): 99-101.
22. Poirel L, Pitout JD, Nordmann P. Carbapenemases: molecular diversity and clinical consequences. Future Microbiol. 2007; 2 (5): 501-512.
23. Queenan AM, Bush K. Carbapenemases: the versatile beta-lactamases. Clin Microbiol Rev. 2007; 20 (3): 440-458, table of contents.
24. Carmeli Y, Akova M, Cornaglia G, Daikos GL, Garau J, Harbarth S et al. Controlling the spread of carbapenemase-producing Gram-negatives: therapeutic approach and infection control. Clin Microbiol Infect. 2010; 16 (2): 102-111.
25. Miriagou V, Cornaglia G, Edelstein M, Galani I, Giske CG, Gniadkowski M et al. Acquired carbapenemases in Gram-negative bacterial pathogens: detection and surveillance issues. Clin Microbiol Infect. 2010; 16 (2): 112-122.
26. Tenover FC, Williams PP, Stocker S, Thompson A, Clark LA, Limbago B et al. Accuracy of six antimicrobial

Investigación en Discapacidad114
Bacterial identification and susceptibility systems
www.medigraphic.org.mx
susceptibility methods for testing linezolid against staphylococci and enterococci. J Clin Microbiol. 2007; 45 (9): 2917-2922.
27. Felten A, Grandry B, Lagrange PH, Casin I. Evaluation of three techniques for detection of low-level methicillin-resistant Staphylococcus aureus (MRSA): a disk diffusion method with cefoxitin and moxalactam, the Vitek 2 system, and the MRSA-screen latex agglutination test. J Clin Microbiol. 2002; 40 (8): 2766-2771.
28. Ligozzi M, Bernini C, Bonora MG, De Fatima M, Zuliani J, Fontana R. Evaluation of the VITEK 2 system for identifi cation and antimicrobial susceptibility testing of medically relevant gram-positive cocci. J Clin Microbiol. 2002; 40 (5): 1681-1686.
29. Nakasone I, Kinjo T, Yamane N, Kisanuki K, Shiohira CM. Laboratory-based evaluation of the colorimetric VITEK-2 Compact system for species identifi cation and of the Advanced Expert System for detection of antimicrobial resistances: VITEK-2 Compact system identifi cation and antimicrobial susceptibility testing. Diagn Microbiol Infect Dis. 2007; 58 (2): 191-198.
30. Swenson JM, Lonsway D, McAllister S, Thompson A, Jevitt L, Zhu W et al. Detection of mecA-mediated resistance using reference and commercial testing methods in a collection of Staphylococcus aureus expressing borderline oxacillin MICs. Diagn Microbiol Infect Dis. 2007; 58 (1): 33-39.
31. Hrabák J, Chudácková E, Walková R. Matrix-assisted laser desorption ionization-time of flight (maldi-tof) mass spectrometry for detection of antibiotic resistance mechanisms: from research to routine diagnosis. Clin Microbiol Rev. 2013; 26 (1): 103-114.
32. Clerc O, Prod’hom G, Vogne C, Bizzini A, Calandra T, Greub G. Impact of matrix-assisted laser desorption ionization time-of-flight mass spectrometry on the clinical management of patients with Gram-negative bacteremia: a prospective observational study. Clin Infect Dis. 2013; 56 (8): 1101-1107.
33. Kok J, Chen SC, Dwyer DE, Iredell JR. Current status of matrix-assisted laser desorption ionisation-time of fl ight mass spectrometry in the clinical microbiology laboratory. Pathology. 2013; 45 (1): 4-17.

Volumen 6 Número 3 Septiembre-Diciembre 2017 115
Palabras clave: Catéteres urinarios,
uropatógenos, susceptibilidad
antimicrobiana, biopelículas.
Key words: Urinary catheters,
uropathogens, antimicrobial susceptibility, biofilms.
www.medigraphic.org.mx
Producción de biopelículas y resistencia antimicrobiana en uropatógenos aislados de catéteres urinarios en un hospital de rehabilitación físicaProduction of biofi lms and antimicrobial resistance of uropathogens isolated from urinary catheters in a physical rehabilitation hospital
Silvestre Ortega Peña,* Guillermo Cerón González*
Artículo original
Vol. 6, Núm. 3 Septiembre-Diciembre 2017
pp 115-121
Resumen
El tratamiento antimicrobiano para infecciones urinarias asociadas a catéter puede fallar en algunos casos debido a que los uropatógenos pueden desarrollar mecanismos que los protegen de los antibióticos, tales como resistencia antimicrobiana y producción de biopelículas. En el presente estudio determinamos la producción de biopelículas y perfil de susceptibilidad antimicrobiana en 98 uropatógenos aislados de cultivos de orina obtenidos de pacientes con infección del tracto urinario asociado a catéter. Los uropatógenos cultivados más frecuentemente fueron Escherichia coli (60%), Enterococcus faecalis (12%), Pseudomonas aeruginosa (11%) y Klebsiella pneumoniae (7%). De los uropatógenos, 77% produjeron biopelículas; de éstos, 14% lo hicieron de forma débil y 63%, fuerte. Encontramos que la mayoría de los uropatógenos poseían altos porcentajes de resistencia a distintas familias de antibióticos, y muchos de ellos produjeron biopelículas en distintos niveles; por ello, es importante implementar estrategias de prevención para evitar la contaminación de los catéteres urinarios con este tipo de uropa-tógenos, al igual que evitar el uso de los catéteres durante largos periodos.
Abstract
Antimicrobial treatment of catheter-associated urinary tract infections may fail in some cases because uropathogens may develop mechanisms that protect them from antibiotics, such as antimicrobial resistance and biofilm production. In this study, we determined the biofilm production and antimicro bial susceptibility profile in 98 uropathogens isolated from urine cultures obtained from patients with catheter-associated urinary tract infections. The most frequently cultured uropathogens were Escherichia coli (60%), Enterococcus faecalis (12%), Pseudomonas aeruginosa (11%), and Klebsiella pneumoniae (7%). Of the uropathogens, 77% produced biofilms, of which 14% did so weakly, and 63% strongly. We found that most uropathogens had high percentages of resistance to different families of antibiotics, and many of them produced biofilms at different levels; therefore, it is important to implement prevention strategies to avoid contamination of urinary catheters with this type of uropathogens, as well as avoiding the use of catheters for long periods.
* Laboratorio de Infectología, Instituto Nacional de Rehabi-litación «Luis Guillermo Ibarra Ibarra». Ciudad de México, México.
Dirección para correspondencia:Silvestre Ortega PeñaCalz. México-Xochimilco Núm. 289,Col. Arenal de Guadalupe, Deleg. Tlalpan, 14389,Ciudad de México, México.Teléfono: 59991000, ext. 14806E-mail: [email protected]
Recibido: 13 de octubre de 2016.Aceptado: 06 de julio de 2017.
Este artículo puede ser consultado en versión completa en: http://www.medigraphic.com/rid

Investigación en Discapacidad116
Producción de biopelículas y resistencia antimicrobiana en uropatógenos aislados
www.medigraphic.org.mx
Introducción
Los catéteres urinarios (CU) son dispositivos médicos que ayudan a drenar la orina desde la vejiga y se usan ampliamente en pacientes que sufren de alguna discapacidad física (fractura de cadera, lesión en los nervios de la vejiga o lesión de médula espinal) que les impide orinar por sí mismos.1,2 Sin embargo, el uso prologando de CU incrementa el riesgo de que los pacientes sufran en algún momento infecciones del tracto urinario asociadas a ellos (ITU-CU) y, en el peor de los casos, bacteriemias secundarias.3
El origen de las ITU-CU se asocia con la contamina-ción del catéter con microorganismos que proceden de la región periuretral.3 Una característica de las ITU-CU es que, en algunos casos, pueden llegar a convertirse en infecciones crónicas y persistentes si no se tratan a tiempo, debido a que los CU podrían contaminarse con uropatógenos que poseen la habilidad de producir biopelículas.2 Estas últimas se defi nen microbiológi-camente como comunidades de células microbianas que crecen rodeadas por una matriz extracelular (ME) que ellas mismas producen y les sirve para adherirse de forma covalente sobre superfi cies vivas o inertes; además, la ME protege a los microorganismos de la respuesta inmune del huésped e impide la penetración de las moléculas con actividad antimicrobiana (anti-bióticos y antisépticos) a su sitio blanco.4 Estudios de susceptibilidad antimicrobiana in vitro han demostrado que los microorganismos que crecen en forma de biopelículas son hasta mil veces más tolerantes a la acción de los antibióticos que los que crecen en forma libre (planctónica).4 Otra característica de las ITU-CU es que su tratamiento puede llegar a ser complicado, no sólo por el crecimiento de los microorganismos en forma de biopelículas, sino porque, en algunos casos, las biopelículas se forman con microorganismos que previamente han desarrollado resistencia a distintos tipos de antibióticos.5 Por ejemplo, en un estudio realizado por Neupane y sus colaboradores, donde correlacionaron entre la formación de biopelículas y la resistencia para los antibióticos más comunes usados para tratar ITU causadas por cepas de Escherichia coli uropatógenas aisladas en un hospital de Nepal, además de que eran multidrogorresistentes por tener betalactamasas de espectro extendido (ESBL), los autores encontraron que las E. coli con ESBL que produjeron biopelículas presentaron alta resistencia a cefalexicina y amoxicilina.6
Las características microbiológicas (perfi l de sus-ceptibilidad antimicrobiana y producción de biopelí-culas) de microorganismos aislados de infecciones
asociadas al uso de dispositivos médicos distintos a CU (catéteres intravasculares, prótesis articulares, et-cétera) ya han sido documentadas en varios estudios; sin embargo, en uropatógenos aislados de ITU-CU, la información de las características antes mencionadas es casi nula.7 Por lo tanto, nosotros decidimos realizar un estudio que nos permitiera describir y documentar las características microbiológicas de los uropatóge-nos aislados de ITU-CU. Este trabajo se realizó en el Instituto Nacional de Rehabilitación «Luis Guillermo Ibarra Ibarra» (INR-LGII), que es un hospital de tercer nivel que recibe y trata a pacientes que padecen de patologías que les causan discapacidad física.
Material y métodos
Realizamos un estudio transversal entre noviembre de 2013 y mayo de 2014 con muestras de orina obte-nidas de pacientes que llevaban usando CU por más de dos semanas y en quienes se sospechó ITU-CU porque presentaban datos clínicos: dolor abdominal, lumbar o fi ebre.
Obtención de la muestra y cultivo
Las muestras de orina fueron colectadas en condi-ciones asépticas con jeringas estériles de la parte fi nal del catéter uretral, y enviadas inmediatamente al Laboratorio de Infectología del INR-LGII para su cultivo. El sembrado de las muestras se hizo en dos medios de cultivo (agar sangre de carnero 5% y agar MacConkey) con asa calibrada (1 μL); luego, los medios se incubaron por 24 horas a 37 oC. El cultivo se consideró positivo cuando se observó desarrollo y cuenta bacteriana ≥ 1 x 103 UFC/mL.
Identificación y pruebas de sensibilidad antimicrobiana
La identifi cación y pruebas de sensibilidad antimi-crobiana de los uropatógenos se hizo en el sistema semiautomatizado Vitek 2® (bioMérieux, Marcy l´Étoile, Francia). Los antibióticos probados en bacterias Gram-negativas fueron amoxicilina/ácido clavulánico (AMC), piperazilina/tazobactam (PTZ), ceftazidima (CAZ), cefepime (FEP), aztreonam (AZT), fosfomicina (FOS), nitrofurantoína (NIT), trimetoprim/sulfametoxa-zole (SXT), ciprofl oxacino (CIP), levofl oxacino (LVX), amikacina (AK), gentamicina (GM), ertapenem (ETP), meropenem (MRP), imipenem (IPM) y colistina (CL); y en Gram-positivas, ampicilina (AMP), penicilina (P), NIT, CIP, LVX, linezolid (LZD) y vancomicina (VAN).

Volumen 6 Número 3 Septiembre-Diciembre 2017 117
Silvestre Ortega Peña y col.
www.medigraphic.org.mx
Resultados
A partir de 230 muestras de orina, se aislaron 98 uropatógenos que se distribuyeron en las siguien-tes especies: E. coli (60%), Enterococcus faecalis (12%), Pseudomonas aeruginosa (11%), Klebsiella pneumoniae (7%), Morganella morganii (4%), Proteus mirabilis (4%), Citrobacter freundii (1%) y Citrobacter braakii (1%).
El porcentaje de resistencia antimicrobiana por especie se muestra en el cuadro I. En general, E. coli fue el uropatógeno que presentó los más altos porcentajes de resistencia, principalmente a los si-guientes antibióticos: fl uoroquinolonas (ciprofl oxacino y levofl oxacino), cefalosporinas de tercera y cuarta generación (ceftazidima y cepefime), aztreonam, trimetoprim/sulfametoxazole y gentamicina. El único microorganismo Gram positivo que se aisló fue E. faecalis, que sólo mostró resistencia a ciprofl oxacino (33%) y levofl oxacino (33%).
Los resultados de los ensayos in vitro para detectar uropatógenos productores de biopelículas mostraron que 77% fueron positivos para la prueba; de éstos, 63% lo hicieron de forma fuerte (Cuadro II). Los uropatóge-nos que produjeron mayores cantidades de biopelículas fueron E. coli, K. pneumoniae, Ps. aeruginosa.
Por último, de los uropatógenos que aislamos con mayor frecuencia y produjeron mayor cantidad de biopelículas (E. coli, K. pneumoniae y Ps. aeruginosa), seleccionamos tres aislados de cada especie (la selec-ción se hizo porque las especies antes mencionadas producían la misma cantidad de biopelículas, resulta-dos no mostrados) y comparamos si había diferencia en la cantidad de biopelículas que producían (Figura 1). Este análisis nos mostró que Ps. aeruginosa y K. pneumoniae fueron los uropatógenos que mayor cantidad de biopelículas producían.
Discusión
El motivo principal que incentivó la realización del si-guiente estudio fue describir las características micro-biológicas (susceptibilidad antimicrobiana y producción de biopelículas) de los uropatógenos aislados de CU en uno de los hospitales de rehabilitación física más importantes en México.
Una característica de las ITU-CU es que si no se tratan a tiempo y de forma adecuada, pueden llegar a convertirse en infecciones crónicas y persistentes debido a que los CU podrían estar contaminados con uropatógenos que posean diferentes mecanismos de defensa que les sirvan para resistir o tolerar los
La interpretación del perfi l de sensibilidad antimi-crobiana se hizo de acuerdo con los criterios de la CLSI (Clinical and Laboratory Standards Institute).8 Los uropatógenos estuvieron almacenados a -70 oC en caldo Müeller Hinton suplementado con 30% de glicerol hasta su análisis.
Producción in vitro de biopelículas
Para la producción de biopelículas se usó el ensa-yo semicuantitativo descrito por Christensen y su grupo,9 con algunas modifi caciones. Cada cepa se creció estáticamente en caldo cerebro corazón su-plementado con 2% de glucosa (CCC-G) a 37 oC por 24 horas. Enseguida, los crecimientos se ajustaron a una concentración 0.5 escala de MacFarland [1.5 x 108 UFC/mL]; después, se diluyeron 1:20 en solu-ción de cloruro de sodio (0.85%, P/V); [5 x 106 UFC/mL]. De la dilución se tomaron 10 μL y depositaron en pocillos individuales de una microplaca estéril de 96 pozos fondo U que contenían 100 μL de CCC-G fresco; la concentración fi nal de los microorganismos en los pocillos fue 5 x 104 UFC/mL. La microplaca se incubó estáticamente a 37 oC por 12 horas. Ense-guida, se decantó el medio de cultivo y los pocillos se lavaron de forma gentil (tres veces) con solución salina estéril. La microplaca fue secada a tempera-tura ambiente por dos horas. Las biopelículas y sus residuos se tiñeron por 20 minutos con 200 μL de una solución de cristal violeta 0.1% (P/V). El colorante se decantó y el exceso se eliminó con solución salina (tres veces). Se extrajo el colorante con 180 μL de etanol 95% por 30 minutos, y enseguida se midió por densidad óptica (DO, 492 no) en un espectrofotóme-tro (xMarkTM, Bio-Rad Laboratories, Inc., California). Las cepas se inocularon por triplicado y se repitió el ensayo dos veces en experimentos independientes. Se promediaron las DO obtenidas de los dos experi-mentos para cada cepa. El punto de corte (DOc) que se usó para defi nir que las cepas eran productoras de biopelículas fue dos veces más la DO que el control negativo. De acuerdo con los valores de DO, las ce-pas se categorizaron en tres grupos: no productoras de biopelículas (OD ≤ DOc), productoras débiles (DOc ≤ DO2 x DOc) y productoras fuertes (2 x DOc < DO). La categorización anterior fue con base en los criterios de Stepanović y sus colegas.10
Análisis estadístico
Se usó estadística descriptiva para determinar fre-cuencias, porcentajes y proporciones.

Investigación en Discapacidad118
Producción de biopelículas y resistencia antimicrobiana en uropatógenos aislados
www.medigraphic.org.mx
tratamientos antimicrobianos.9 Estos mecanismos son adquisición de genes que les confi eren resis-tencia específi ca a los antibióticos y producción de biopelículas; éstas sirven para proteger a las células microbianas de la respuesta inmune del huésped y de moléculas con actividad antimicrobiana: antibióticos o antisépticos.5
En este trabajo determinamos el perfi l de sus-ceptibilidad a distintas familias de antibióticos en todos los uropatógenos que aislamos. En general, encontramos elevados porcentajes de resistencia antimicrobiana, principalmente en el uropatógeno más frecuente: E. coli; la mayoría de las cepas que pertenecían a esta especie microbiana eran mul-tidrogorresistentes. Los resultados de resistencia antimicrobiana que encontramos son similares con los publicados en otras series realizadas en nuestro país,10,11 donde también determinaron la resistencia antimicrobiana en infecciones del tracto urinario, lo que coincide con resultados reportados para otros países de América Latina. El incremento de resisten-cia antimicrobiana entre microorganismos aislados de infecciones del tracto urinario, así como de otro tipo de infecciones, se ha convertido en los últimos años en un importante problema de salud pública debido a que el uso irracional e inadecuado de los antibióti-cos ha propiciado la generación de microorganismos multidrogorresistentes.12
Una difi cultad a la cual se pueden enfrentar los clínicos cuando diagnostican y tratan ITU-CU es que los pacientes no respondan al tratamiento antimicro-
Cua
dro
I. Pa
trón
de
resis
tenc
ia a
ntim
icro
bian
a a
dist
into
s an
tibió
ticos
en
urop
atóg
enos
aisl
ados
de
infe
ccio
nes
del t
ract
o ur
inar
io
asoc
iada
s a
caté
ter (
n =
98)
.
Antib
iotic
orre
siste
ncia
(%)
Uro
pató
geno
sTo
talA
MC
PTZ
CAZ
FEP
ATM
FOS
NIT
SXT
CIP
LVX
AKG
NET
PM
RPIM
PC
LAM
PP
VAN
LZD
Gra
m n
egat
ivos
E. c
oli
580
030
3030
1216
3042
426
230
00
ND
ND
ND
ND
ND
K. p
neum
onia
e 7
00
3 3
3 0
00
3 3
0 0
00
0N
DN
DN
DN
DN
DM
. mor
gani
i 4
00
0 0
0 0
ND
0 0
00
00
00
ND
ND
ND
ND
ND
P. m
irabi
lis 4
00
0 0
0 0
ND
0 0
00
00
00
ND
ND
ND
ND
ND
Citr
obac
ter s
pp.
20
0 0
0 0
0 0
0 0
00
00
00
ND
ND
ND
ND
ND
P. ae
rugi
nosa
110
0 7
7 0
1010
ND
7 7
7 7
ND
00
0N
DN
DN
DN
DG
ram
pos
itivo
sE.
faec
alis
12N
DN
DN
DN
DN
DN
D 0
ND
3333
ND
ND
ND
ND
ND
ND
00
00
Ant
ibió
ticos
: am
oxic
ilina
/áci
do c
lavu
láni
co (A
MC
), pi
pera
cilin
a/ta
zoba
ctam
(PTZ
), ce
ftazi
dim
a (C
AZ),
cefe
pim
e (F
EP),
aztre
onam
(ATM
), fo
sfom
icin
a (F
OS)
, ni
trofu
rant
oína
(NIT
), tri
met
oprim
/sul
fam
etox
azol
e (S
XT),
cipr
oflo
xaci
no (C
IP),
levo
floxa
cino
(LVX
), am
ikac
ina
(AK)
, gen
tam
icin
a (G
N),
erta
pene
m (E
TP),
mer
open
em (M
RP),
imip
enem
(IM
P), c
olist
ina
(CL)
, am
pici
lina
(AM
P), p
enic
ilina
(P),
vanc
omic
ina
(VAN
), lin
ezol
id (L
ZD).
No
dete
rmin
ado
(ND
).
Cuadro II. Evaluación de la biopelícula en uropatógenos aislados de infecciones
asociadas con catéter.
Detección de biopelículas n (%)
Uropatógenos Total Negativo Débil Fuerte
E. coli 58 18 (31) 5 (9) 35 (60)
E. faecalis 12 4 (33) 3 (25) 5 (42)
P. aeruginosa 11 0 0 11 (100)
K. pneumoniae 7 0 0 7 (100)
M. morganii 4 0 0 4 (100)
P. mirabilis 4 0 4 (100) 0
Citrobacter spp. 2 0 2 (100) 0
Total 98 22 (22) 14 (14) 62 (63)

Volumen 6 Número 3 Septiembre-Diciembre 2017 119
Silvestre Ortega Peña y col.
www.medigraphic.org.mx
biano a pesar de conocer el perfi l de susceptibilidad antimicrobiana de los uropatógenos que las están causando; esto puede deberse a que el CU esté contaminado con microorganismos productores de biopelículas que protegen a las células microbianas de las moléculas con actividad antimicrobiana.5 Noso-tros determinamos la frecuencia con la que se aíslan uropatógenos que poseen la habilidad de producir biopelículas; en general, encontramos que el 76% poseían esta habilidad, y de ellos, 63% lo hacían de forma fuerte. La frecuencia que obtuvimos en este estudio fue más alta con respecto a lo publicado por Niveditha, Subramanian y sus respectivos grupos; ambos investigadores realizaron trabajos similares al nuestro y describieron las siguientes frecuencias: 60 y 63%, respectivamente, para los siguientes uropatóge-nos: E. coli, K. pneumoniae y Ps. aeruginosa.13,14 Las diferencias encontradas se deben a que Niveditha, Subramanian y sus colaboradores usaron ensayos in vitro que detectan de forma fenotípica a los microor-ganismos productores de biopelículas (crecimiento en agar rojo Congo o adhesión en tubo), y ésos son ensayos que poseen baja sensibilidad y especifi cidad para ello.6,15 En nuestro caso, usamos un método mucho más sensible y específi co (ensayo semicuan-titativo de Christensen), además de que aplicamos los criterios de Stepanović para clasifi car a los microor-ganismos como no productores, productores débiles o fuertes.8,15 Es importante mencionar que aunque los criterios de Stepanović están bien estandarizados y referenciados para clasifi car a los microorganismos productores de biopelículas como débiles o fuertes,
pequeños incrementos en la densidad óptica (DO) pueden impactar negativamente en la categorización de los microorganismos productores de biopelículas, sobre todo en los productores fuertes. Nosotros ob-servamos lo anterior cuando comparamos el promedio de la DO que se obtuvo entre los uropatógenos que habían sido categorizados como productores fuertes: Ps. aeruginosa, K. pneumoniae y E. coli; en general, los resultados nos enseñaron que aunque las especies microbianas antes mencionadas fueron categorizadas como productoras fuertes, aun así había diferencias entre ellas (Figura 1), que se deben al tipo de molécu-las que producen los microorganismos para formar la ME que va a rodear las biopelículas; en el caso de Ps. aeruginosa y K. pneumoniae, la ME está compuesta en su mayor parte por carbohidratos, a diferencia de E. coli, en la cual se forma con proteínas, de manera predominante.16,17
Una debilidad de nuestro estudio es que no hace-mos una correlación entre producción de biopelículas y resistencia antimicrobiana; sin embargo, algunos otros sí lo han hecho; por ejemplo, Subramanian y su equipo: encontraron que de 60 uropatógenos que ellos analizaron y que producían biopelículas, el 83% eran resistentes a ampicilina, 80% a norfl oxacino, 93% a ácido nalidíxico.16 Mishra y sus colegas analizaron la resistencia en microorganismos aislados de disposi-tivos médicos y la relacionaron con la producción de biopelículas; en general, este grupo de investigadores encontró que los microorganismos que producían biopelículas eran más resistentes que los que no.7 Como ya lo habíamos mencionado anteriormente,
1.8
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
0
Figura 1.
Comparación de la producción de biopelículas de tres especies de uropatógenos: Escherichia coli (E, n = 3), Klebsiella pneumoniae (K, n = 3), Pseudomonas aeruginosa (P, n = 3), y fotografías representativas de los resultados del ensayo semicuantitativo: A) E. coli, B) K. pneumoniae y C) Ps. aeruginosa.
Abso
rban
cia
(DO
492
nm
)
E1 E2 E3 K1 K2 K3 P1 P2 P3
A) B) C)

Investigación en Discapacidad120
Producción de biopelículas y resistencia antimicrobiana en uropatógenos aislados
www.medigraphic.org.mx
el incremento de la resistencia antimicrobiana entre microorganismos productores de biopelículas se debe a que la ME impide el paso de los antimicrobianos a su sitio blanco; además, los microorganismos en el in-terior de las biopelículas sufren cambios morfológicos y metabólicos que generan que sean más tolerantes a los antimicrobianos.5
Por último, aunque los resultados obtenidos en este trabajo sólo muestran las características micro-biológicas (perfi l de susceptibilidad antimicrobiana y producción de biopelículas) de uropatógenos aislados de ITU-CU de nuestro hospital, y no pueden ser extra-polados a otros centros hospitalarios del país, sirven para generar nuevas preguntas que es necesario res-ponder; por ejemplo: ¿la composición de la ME de los uropatógenos productores de biopelículas impacta de forma negativa en la acción de los antibióticos con acti-vidad antibiopelícula (fosfomicina)?,18-20 ¿los antibióticos carbapenémicos (ertapenem, imipenem, meropenem) que se usan para tratar ITU-CU causadas por bacilos Gram-negativos multidrogorresistentes tienen la misma efectividad si éstos producen biopelículas? Si podemos contestar estas preguntas en estudios posteriores y obtenemos resultados positivos, éstos servirán para hacer adecuaciones en las terapias antimicrobianas que se usan para tratar ITU-CU cuando sean causadas por uropatógenos multidrogorresistentes y productores de biopelículas; así, se evitará que los pacientes desa-rrollen secuelas negativas: ITU crónicas o bacteriemias secundarias asociadas a contaminación del CU.
Conclusión
En el presente trabajo encontramos que la mayoría de los uropatógenos poseían altos porcentajes de re-sistencia a distintas familias de antibióticos y muchos de ellos produjeron biopelículas en distintos niveles; por ello, es importante implementar estrategias de prevención para evitar la contaminación de los catéteres urinarios con este tipo de uropatógenos, al igual que evitar su uso durante largos periodos.
Bibliografía
1. Romero-Cullerés G, Planells-Romeo I, Martinez de Salazar-Muñoz P, Conejero-Sugrañes J. Urinary infection in patients with neurogenic bladder: patterns of resistance to the most frequent uropathogens. Actas Urol Esp. 2012; 36 (8): 474-481.
2. González-Chamorro F, Palacios R, Alcover J, Campos J, Borrego F, Dámaso D. Urinary tract infections and their prevention. Actas Urol Esp. 2012; 36 (1): 48-53.
3. Nicolle LE. Catheter-associated urinary tract infections. Antimicrob Resist Infect Control. 2014; 3: 23.
4. Ortega-Peña S, Franco-Cendejas R. Importancia médica del biofi lm de Staphylococcus epidermidis en las infecciones de prótesis articular. Invest Discap. 2014; 3 (3): 106-113.
5. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015; 13 (5): 269-284.
6. Neupane S, Pant ND, Khatiwada S, Chaudhary R, Banjara MR. Correlation between biofi lm formation and resistance toward different commonly used antibiotics along with extended spectrum beta lactamase production in uropathogenic Escherichia coli isolated from the patients suspected of urinary tract infections visiting Shree Birendra Hospital, Chhauni, Kathmandu, Nepal. Antimicrob Resist Infect Control. 2016; 5: 5.
7. Mishra SK, Basukala P, Basukala O, Parajuli K, Pokhrel BM, Rijal BP. Detection of biofilm production and antibiotic resistance pattern in clinical isolates from indwelling medical devices. Curr Microbiol. 2015; 70 (1): 128-134.
8. Clinical and Laboratory Standards Institute. Performance for antimicrobial susceptibility testing; twenty-fifth informational supplement. CLSI document M100-S25. Wayne: Clinical and Laboratory Standards Institute; 2016.
9. Christensen GD, Simpson WA, Younger JJ, Baddour LM, Barrett FF, Melton DM et al. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: a quantitative model for the adherence of staphylococci to medical devices. J Clin Microbiol. 1985; 22 (6): 996-1006.
10. Stepanović S, Vuković D, Hola V, Di Bonaventura G, Djukić S, Cirković I et al. Quantifi cation of biofi lm in microtiter plates: overview of testing conditions and practical recommendations for assessment of biofi lm production by staphylococci. APMIS. 2007; 115 (8): 891-899.
11. Sánchez-de Badajoz E, Sánchez-Gallegos P. The challenge of urinary tract infections. Actas Urol Esp. 2014; 38 (10): 631-632.
12. Páramo-Rivas F, Tovar-Serrano A, Rendón-Macías ME. Resistencia antimicrobiana en pacientes con infección de vías urinarias hospitalizados en el servicio de Medicina Interna del Nuevo Sanatorio Durango, de enero a diciembre de 2013. Med Int Mex. 2015; 31 (1): 34-40.
13. Andrade SS, Sader HS, Jones RN, Pereira AS, Pignatari AC, Gales AC. Increased resistance to fi rst-line agents among bacterial pathogens isolated from urinary tract infections in Latin America: time for local guidelines? Mem Inst Oswaldo Cruz. 2006; 101 (7): 741-748.
14. Marston HD, Dixon DM, Knisely JM, Palmore TN, Fauci AS. Antimicrobial resistance. JAMA. 2016; 316 (11): 1193-1204.

Volumen 6 Número 3 Septiembre-Diciembre 2017 121
Silvestre Ortega Peña y col.
www.medigraphic.org.mx
formation in the clinical isolates. Braz J Infect Dis. 2011; 15 (4): 305-311.
18. Bales PM, Renke EM, May SL, Shen Y, Nelson DC. Purification and characterization of biofilm-associated EPS exopolysaccharides from ESKAPE organisms and other pathogens. PLoS One. 2013; 8 (6): e67950.
19. Mann EE, Wozniak DJ. Pseudomonas biofi lm matrix composition and niche biology. FEMS Microbiol Rev. 2012; 36 (4): 893-916.
20. Falagas ME, Vouloumanou EK, Samonis G, Vardakas KZ. Fosfomycin. Clin Microbiol Rev. 2016; 29 (2): 321-347.
15. Niveditha S, Pramodhini S, Umadevi S, Kumar S, Stephen S. The isolation and the biofi lm formation of uropathogens in the patients with catheter-associated urinary tract infections (UTIs). J Clin Diagn Res. 2012; 6 (9): 1478-1482.
16. Subramanian P, Shanmugam N, Sivaraman U, Kumar S, Selvaraj S. Antiobiotic resistance pattern of biofi lm-forming uropathogens isolated from catheterised patients in Pondicherry, India. Australas Med J. 2012; 5 (7): 344-348.
17. Hassan A, Usman J, Kaleem F, Omair M, Khalid A, Iqbal M. Evaluation of different detection methods of biofi lm

Investigación en Discapacidad122
Palabras clave: Sistema educativo,
síndrome de Down, inteligencias múltiples,
fracaso educativo, programa de intervención.
Key words: Educational system, Down’s syndrome,
multiple intelligences, educational failure,
intervention program.
www.medigraphic.org.mx
La teoría de las inteligencias múltiples en personas con síndrome de Down.Cuando el talento se transforma en inteligenciaThe theory of multiple intelligences in people with Down’s syndrome.When talent is transformed into intelligence
Ignacio Gutiérrez Delgado*
Interés general
Vol. 6, Núm. 3 Septiembre-Diciembre 2017
pp 122-127
Resumen
Debemos partir del hecho de que toda persona, con o sin discapacidad, es poseedora de aptitudes o destrezas en ciertas disciplinas. En el sistema educativo, en ocasiones, éstas no se ven reflejadas, ya que se valora principalmente la destreza matemática y lingüística. Las personas con síndrome de Down tienen un importante déficit en ambas. ¿Significa esto que no son inteligentes? Al contrario, Howard Gardner en su teoría de las inteligencias múltiples defiende que todos tenemos una inteligencia o potencialidad, la cual deberemos desarrollar y será el motor para acceder al conocimiento, sobre la que girará todo el aprendizaje de la persona, favoreciendo así su autoestima y liberándola del estigma social del fracaso educativo. Para ello, en el presente trabajo se muestra la necesidad de conocer al colectivo de síndrome de Down y la evolución del concepto de inteligencia para aterrizar en la teoría de las inte-ligencias múltiples y cómo puede llevarse a cabo un programa de intervención, a través de ellas, en personas con síndrome de Down.
Abstract
We must start from the fact that every person, with or without disability, possesses aptitudes or skills in certain disciplines. In the educational system, sometimes, these are not reflected, since the mathematical and linguistic dexterity is mainly valued. People with Down’s syndrome have an important deficit in both. Does that mean they are not intelligent? On the contrary. According to Howard Gardner and his theory of multiple intelligences defend that we all have an intelligence or potentiality, which we must develop and will be the motor to access knowledge, which will revolve the whole learning of the person, thus favoring their self-esteem and freeing it from social stigma of educational failure. To do this, it will be necessary to know the Down’s syndrome group, as well as the evolution of the concept of intelligence, to end up landing in the theory of multiple intelligences and how an intervention program can be carried out, through them, in people with Down’s syndrome.
* Educador y Preparador Laboral en la Asociación Síndrome de Down de Burgos.
Dirección para correspondencia:Ignacio Gutiérrez DelgadoCalle Virgen del Manzano 26, 6oB,09004, Burgos, España.Teléfono: 606345326E-mail: [email protected]
Recibido: 02 de marzo de 2017.Aceptado: 18 de julio de 2017.
Este artículo puede ser consultado en versión completa en: http://www.medigraphic.com/rid
«El gran reto, tanto para el docente como para el alumno, es encontrar ese equilibrio
entre grado de desafío de una actividad y el grado de habilidad de la persona que la realiza».
(Howard Gardner)
Introducción
El sistema educativo español (similar a lo sucedido en sistemas educativos de poblaciones hispanoha-blantes) ha vivido durante mucho tiempo encorsetado en una misma manera de enseñar y de evaluar. Los

Volumen 6 Número 3 Septiembre-Diciembre 2017 123
Ignacio Gutiérrez Delgado
www.medigraphic.org.mx
docentes nunca se salían del guion preestablecido, realizando de forma ritualista las mismas enseñanzas, utilizando igual metodología y empleando similares frases célebres de profesor.
Por suerte, no todos eran así. Siempre hubo, ha ha-bido y habrá innovadores, a los cuales se les tachaba de locos por querer cambiar «el método». Al mismo tiempo surgió la integración educativa (hoy llamada inclusión). Para muchos docentes esto les supuso una carga adicional, en cambio para otros les proporcionó un aliciente en su formación y una amplitud en su visión del mundo educativo.
Gracias a estos visionarios, hoy en día en las es-cuelas se están empleando metodologías innovadoras, dirigidas a la inclusión y a la atención a la diversidad, por ejemplo, el aprendizaje cooperativo, las inteligen-cias múltiples, trabajar por proyectos y competencias, etc., creando un modelo pedagógico globalizado e integrador en el que todos los alumnos aprenden de distinta forma y alcanzando metas muy satisfactorias.
Será prioritario el conocimiento de nuestros alum-nos, en este caso personas con síndrome de Down, sus características y peculiaridades, así como sus puntos fuertes y débiles para poder implementar con éxito cualquier modelo pedagógico.
Síndrome de Down
El síndrome de Down debe su nombre al médico británico John Langdon Down, quien en el año 1866 fue el primero en identifi carlo clínicamente. Pero no fue hasta el año 1959 y gracias al Dr. Lejeune cuando se conoció la naturaleza cromosómica del síndrome.
En 2006, Flórez (citado por Ruiz, 2009) lo defi nió como el síndrome de Down o trisomía 21, una anoma-lía genética ocasionada por la presencia de un tercer cromosoma 21 (Figura 1) de las células del organismo humano, la cual constituye la causa genética más fre-cuente de discapacidad intelectual y malformaciones congénitas.1
Según Arraiz (1994), no es posible hablar o decir con certeza y exactitud los factores que causan el síndrome de Down, pero sí ciertas variables asociadas a éste.
Así podemos destacar: factores intrínsecos y factores extrínsecos
• Factores intrínsecos son aquéllos que vienen determinados por la herencia, es decir, hijos con síndrome de Down nacidos de madres con síndro-me de Down, varios niños con este síndrome en la familia próxima, etc., o pueden venir determinados
también por la edad de la madre, debido a que se presenta un alto número de casos cuando la madre rebasa la edad de 35 años.
• Factores extrínsecos o ambientales, los cuales vienen determinados por el ambiente: procesos infecciosos, rubéola, hepatitis, exposición a radia-ciones, agentes químicos, alto contenido de fl úor en el agua, problemas en la madre, tales como falta de vitaminas, desórdenes tiroideos, elevados índices de inmunoglobulina y tiroglobulina en la sangre.2
De acuerdo con Pueschel (1991), el síndrome de Down en función de su clasifi cación puede presentarse de tres formas:
1. Trisomía simple: en 95% de los casos aproxima-damente la totalidad de las células del organismo presentan tres copias completas del cromosoma 21.
2. Trisomía parcial: 3.5% de los casos. Llamada tam-bién translocación, por la que una porción del tercer cromosoma queda adherida a otro cromosoma, normalmente el 14.
3. Mosaicismo: se presenta en 1-2% de los casos con la peculiaridad de que aparecen dos líneas celula-res, una con trisomía 21 completa y otra normal.3
Para poder elaborar un perfi l demográfi co de las personas con síndrome de Down en España se recu-
pppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppphic.orgggggggggg.mxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Fuente: Modificado de https://www.sindrome-de.org/down/
Figura 1. Cariotipo de una persona con síndrome de Down.
9 10 11 12 13 14 15 16
17 18 19 20 21 22 XX XY
1 2 3 4 5 6 7 8
or

Investigación en Discapacidad124
La teoría de las inteligencias múltiples en personas con síndrome de Down
www.medigraphic.org.mx
rrió a fuentes primarias como el II Plan de Acción para Personas con Síndrome de Down en España (2009-2013),4 creado por Down España y la Obra Social Caja Madrid, de las que se han extraído datos de fuentes secundarias como del Estudio Colaborativo Español de Malformaciones Congénitas (2008) y la Encuesta de Discapacidad, Autonomía personal y situaciones de Dependencia (EDAD, 2008), obteniendo los siguientes datos relevantes:
• Durante el periodo 1980-2007 se diagnosticó sín-drome de Down a aproximadamente 11 de cada 10,000 nacidos.
• En España viven aproximadamente 34,000 perso-nas con síndrome de Down, de las cuales 20,000 son varones y 14,000 mujeres.
En términos médicos, un síndrome es un conjunto de signos y síntomas que presentan alguna enferme-dad y que debido a sus características poseen una similitud, concurriendo en tiempo y forma con una etiología variada.
Las personas con síndrome de Down, según Cunningham (1990), no tendrán todos los signos o características propias de este síndrome y algunas características serán más obvias en unas personas que en otras.5
A pesar de ello, Troncoso y del Cerro (1998), afi r-man que entre las personas con síndrome de Down existe una serie de características comunes entre ellos, así como con otras personas que poseen dife-rentes formas de defi ciencia mental y también, con personas que no tienen defi ciencia alguna.6
Cabe mencionar que el curso evolutivo de cada persona depende no sólo del material genético, sino también, y de manera importantísima, de los factores ambientales.
Es preciso conocer en profundidad las peculiari-dades y características consiguientes a la patología cerebral del síndrome de Down y cómo estas carac-terísticas se expresan en una persona concreta que posee una reaccionabilidad y personalidad propia e intransferible. Sólo así conseguiremos que nuestros programas de educación e intervención sean más ajustados y por tanto, más efi caces.
Las personas con síndrome de Down poseen las siguientes características de forma general:
• Físicas: las más comunes, según Ortega (2005),7 son: cráneo pequeño, fi suras palpebrales oblicuas hacia arriba, labios prominentes, cuello corto, etc.
Estas características van acompañadas de alte-raciones respiratorias, bucales, cardiovasculares, digestivas, etcétera.
• Nivel psicomotor: hipotonía muscular y laxitud de los ligamentos. Cierta difi cultad motora tanto en la motricidad fi na (coordinación ojo-mano) como en la gruesa (brazos y piernas).
• Cognitivas: el síndrome de Down siempre se acompaña de discapacidad intelectual, presenta problemas para mantener la atención en periodos largos de tiempo, difi cultades en la memoria a corto y largo plazo. Sin embargo, tienen la memoria pro-cedimental y operativa bien desarrollada, por lo que podrán realizar tareas secuenciadas con precisión. Buen procesamiento de la información a nivel visual.
• Comunicación y de lenguaje: para ellos es más fácil hacer que explicar lo que hacen o lo que deben hacer. Poseen un buen nivel comprensivo, el cual es mucho mejor que el expresivo. Requieren ayuda de especialista en audición y lenguaje.
• Socio-afectivo: suelen mostrarse colaboradores, afables, afectuosos y sociables. Con un buen grado de adaptación social y ofrecen una imagen social más favorable que personas con otras defi ciencias.
• Otras: la esperanza de vida de las personas con síndro-me de Down es de 60-65 años y se debe a una mejora en su calidad de vida. A pesar de dicho dato, hay que mencionar que según Moran (2013), las personas con síndrome de Down pasan por un «envejecimiento acelerado», pudiendo aparecer en torno a los 40 o 50 años de edad y llevando consigo asociada, en mayor o menor medida, la enfermedad de Alzheimer.8
Evolución del concepto de inteligencia
Según la Real Academia Española (RAE) la palabra inteligencia proviene del latín intelligentia, cuyas cinco primeras acepciones son:
1. f. Capacidad de entender o comprender.2. f. Capacidad de resolver problemas.3. f. Conocimiento, comprensión, acto de entender.4. f. Sentido en que puede tomarse una proposición,
un dicho o una expresión.5. f. Habilidad, destreza y experiencia.
La manera de entender y de concebir el concepto de inteligencia a lo largo de la historia ha ido evolu-cionando hasta nuestros días.
Aunque hubo estudios anteriores como los de Broca y Galton, fue en el siglo XX cuando empezó a desarrollarse la noción de inteligencia en profundidad.

Volumen 6 Número 3 Septiembre-Diciembre 2017 125
Ignacio Gutiérrez Delgado
www.medigraphic.org.mx
Entre 1905 y 1911, Alfred Binet y Theodore Simon crearon la primera prueba para medir las capacidades cognitivas en niños con difi cultades de aprendizaje, a partir del nivel de conocimientos que se muestra en un momento dado.
Spearman enunció en 1927 la teoría en la que afi rma que la inteligencia está compuesta por varios factores, un factor general de carácter hereditario que interviene en todas las fases de la conducta humana y un factor especial que representa la habilidad de un sujeto frente a una tarea determinada. Ambos factores tendrían una localización concreta en el cerebro.
Posteriormente, Piaget centró sus estudios en la inteligencia desde el punto de vista del desarrollo cog-nitivo, entendiendo el concepto como una descripción de aquello que es esencial a todos los estadios del desarrollo cognitivo. Describe y analiza el desarrollo del conocimiento y la adquisición de capacidades dependiendo de las etapas evolutivas.
Vigotsky se interesa más en el desarrollo poten-cial de la inteligencia. Para este autor el desarrollo humano se basa en dos procesos: la maduración y el aprendizaje. El aprendizaje humano presupone una naturaleza social específi ca y un proceso mediante el cual los niños acceden a la vida intelectual de aquéllos que les rodean. La inteligencia es, en este sentido, un producto social. La zona de desarrollo potencial será el conjunto de actividades que el niño es capaz de realizar con la ayuda y colaboración de las personas que le rodean.
Y por último, destacar a Gardner y Coleman como principales integrantes del modelo centrado en la comprensión global de la persona para un mejor desarrollo de su vida. Howard Gardner con su teoría de las inteligencias múltiples, la cual se desarrollará a continuación con detalle, y Daniel Goleman que propone que la inteligencia emocional es la capaci-dad de «reconocer nuestros propios sentimientos, los sentimientos de los demás, motivarnos y manejar adecuadamente las relaciones que sostenemos con los demás y con nosotros mismos».9
La teoría de las inteligencias múltiples10
Howard Gardner, psicólogo estadounidense y profesor universitario en la Universidad de Harvard, elaboró en 1983 la llamada teoría de las inteligen-cias múltiples (IM) (Figura 2), misma que le valió el Premio Príncipe de Asturias de Ciencias Sociales en el año 2011.
Para elaborar su teoría Gardner se basó en fuen-tes neurológicas, investigando pacientes con daños
cerebrales y con personas superdotadas y cómo se manifestaba en ellos la inteligencia. Del mismo modo investigó sobre los procesos cognitivos demostrando que las distintas partes del cerebro están implicadas en procesos intelectuales diferentes y que éstos están relacionados con diversas inteligencias. Comprobó que cada inteligencia puede evaluarse con distintas pruebas y por último estudió el desarrollo diferencial en los niños.
Gardner se rebela ante el enfoque tradicional que determina la inteligencia como una capacidad unitaria, la cual es fi ja, general y cuantifi cable mediante pruebas estandarizadas, pudiendo variar en cantidad de unos alumnos a otros.
Cuando nos referimos a inteligencia, en ocasio-nes rápidamente lo relacionamos con el éxito en la escuela, el cual se mide a través de pruebas o test de inteligencia que muestran el cociente intelectual. Cuando hay alumnos con baja puntuación se les presupone que no sirven para estudiar, llevándoles al fracaso escolar, al absentismo en la escuela, etcétera.
Para salir de este error Gardner propone que la inteligencia es un potencial, anteriormente llamado talento, con el que contamos todas las personas y es algo cambiante que se desarrolla a lo largo de la vida del individuo.
Fuente: Acoplado de https://angelmaiquez.files.wordpress.com/2015/07/inteligencias-multiples.jpg
Figura 2. Las ocho inteligencias múltiples de Howard Gardner.
Musical Corporal-cinestésica Interpersonal Lingüístico-verbal Lógico-matemática Naturalista
I
ntra
pers
onal
Visu
al-e
spac
ial
Teoría de las inteligencias
múltiples

Investigación en Discapacidad126
La teoría de las inteligencias múltiples en personas con síndrome de Down
www.medigraphic.org.mx
De acuerdo con Prieto y Ferrándiz (2001), los prin-cipios básicos de la teoría de las IM son:11
• Cada persona posee ocho inteligencias.• Las ocho inteligencias trabajan conjuntamente de
manera compleja.• La mayor parte de las personas pueden desarrollar
cada inteligencia hasta un nivel adecuado de com-petencia.
• Hay muchas maneras de ser inteligentes dentro de cada categoría.
Las ocho inteligencias, según Ruiz (2016):12
– Musical: es la habilidad para percibir, apreciar y producir-reproducir ritmos, tonos y música.
– Lógico-matemática: es la propia de quienes do-minan el razonamiento, la lógica, la resolución de problemas, analizar datos, ordenar, etcétera.
– Lingüístico-verbal: es la empleada para leer, escribir, narrar historias. Se manifi esta en la sensibilidad para entender fonemas, estructuras verbales y todo lo relacionado con el lenguaje.
– Corporal-kinestésica: es la encargada de con-trolar los movimientos corporales y la habilidad para manipular objetos.
– Espacial: es una inteligencia visual que se mues-tra como el sentido para percibir y desarrollar relaciones tridimensionales que permiten captar con precisión el mundo que se despliega ante nuestros ojos.
– Interpersonal: se manifi esta en la sensibilidad para captar y comprender a los demás, empati-zando con sus sentimientos y su forma de ser.
– Intrapersonal: garantiza un buen conocimiento y capacidad para comprender los sentimientos propios, refl exionando sobre sus experiencias y aprender de ellas.
– Naturalista: es la capacidad para organizar los elementos del mundo natural en categorías.
Cada una de las inteligencias tiene la misma importan-cia, aunque unas pueden estar más desarrolladas que otras, todos podemos alcanzar cotas máximas en esas inteligencias innatas y también podemos obtener un de-sarrollo adecuado e incluso bueno en otras inteligencias, siempre y cuando encontremos un ambiente que ofrezca las condiciones necesarias para ello.
Y así nació la teoría de las IM, y con ella la primera defi nición de inteligencia que nos ofrece «capacidad de resolver problemas o crear productos que son va-lorados en uno o más contextos culturales».13
Esta teoría ha supuesto una revolución en el campo educativo, rompiendo con viejos paradigmas de la enseñanza. Implicará una transformación de las aulas en espacios en los que los alumnos puedan aprender de todo partiendo de las características propias de cada uno. Los puntos fuertes de cada alumno han de ser puente para el trabajo de otras capacidades en las que pueda tener más difi cultades.
Todos aprendemos, aunque no de la misma forma. En el caso de un contexto de inclusión, todos tenemos tantas capacidades como limitaciones, se intentará eliminar las barreras de aprendizaje para lograr un desarrollo integral y aprovechar esa diversidad para el enriquecimiento de cada uno.
Ya se habla de «Escuelas de Inteligencias Múltiples», en España uno de los pioneros fue el Colegio Montserrat de Barcelona. En el año 1994 se plantearon adecuar la educación para que fuera efi caz en cada uno. http://www.cmontserrat.org/
Inteligencias múltiples en personas con síndrome de Down
Las personas con síndrome de Down debido a sus características cognitivas tienen una determinada manera de aprender, la cual les conducirá a la inte-riorización de los aprendizajes.
Principios metodológicos básicos:
• Partir de los conocimientos previos y de los puntos fuertes que posee cada alumno.
• Secuenciación en pequeños pasos de las tareas con el apoyo de modelos, modelado, encadenamiento hacia atrás y aproximaciones sucesivas.
• La presentación de los aprendizajes estará apoyada por mediaciones físicas, verbales y visuales que ayuden al alumno en su desarrollo global.
• Alternar las estrategias expositivas con las de in-dagación y experimentación directa.
• Actividades cortas y motivadoras para el alumno, priorizando la funcionalidad de los aprendizajes.
• Usar en la medida de nuestras posibilidades el aprendizaje cooperativo.
• Tener en cuenta las peculiaridades y diferentes ritmos de aprendizaje de cada alumno.
• El éxito de la actividad consiste en la repetición de ésta de diferentes formas, así como el que los alumnos vean que esa actividad es funcional para su vida diaria.
• Crear un clima positivo y motivador. Refuerzo positivo.

Volumen 6 Número 3 Septiembre-Diciembre 2017 127
Ignacio Gutiérrez Delgado
www.medigraphic.org.mx
Según Ruiz (2016), en el caso de las personas con síndrome de Down, sus puntos fuertes están en el ac-ceso a la información por vía visual, su agrado por el contacto interpersonal o su gusto por la música han de utilizarse para ofrecerles la información y siempre que sea posible apoyada en imágenes, gráfi cos, dibujos, esquemas e incluso pictogramas y para ayudarles en la memorización por medio de canciones, melodías o rimas. La presentación multidimensional de los conte-nidos les ayudará también a consolidarlos, si éstos se les exponen utilizando sonidos, imágenes y siempre que sea posible objetos reales que puedan tocar, oler, manipular y practicar. El contacto interpersonal para adquirir conocimientos es para ellos imprescindible.12
Ejemplo práctico–IM y síndrome de Down
Se va a trabajar la comprensión del libro Don Quijote de la Mancha de Miguel de Cervantes, no en su tota-lidad, sólo algunos capítulos relevantes.
Dada su complejidad, se accederá al libro a través de su edición de lectura fácil, usando frases cortas y un vocabulario sencillo.
http://universocervantes.com/Quijote_LF/index.htmlO a través de videos amenos y divertidos: https://
www.youtube.com/watch?v=DESCGF5Us4M
Inteligencias múltiples
Musical: aprenderse la melodía de la serie de televisión española. https://www.youtube.com/watch?v=w4tFzD13hmcO con pictogramas https://www.youtube.com/watch?v=wtJUevFy5PQLógico-matemática: realización de diferentes opera-ciones matemáticas cuyo resultado, si es correcto, se relacionará con un personaje del libro. Creación de un laberinto que une a Don Quijote y Dulcinea.Lingüístico-verbal: hacer un resumen del capítulo, realizar un concurso de lectura, aprenderse rimas relacionadas y sopa de letras.Corporal-kinestésica: creación de un taller de teatro de un capítulo seleccionado donde prime la expresión corporal, la interpretación, etcétera.Espacial: realización de tarjetas de memoria con los diferentes personajes o escenas de los capítulos, te-niendo que emparejarlos. Recreación de una escena con plastilina. Uso de aplicaciones de móvil para An-droid sobre Don Quijote https://play.google.com/store/apps/details?id=com.lasaventurasdedonquijote&hl=esInterpersonal-intrapersonal: explicación breve de la forma de actuar de cada personaje. Interiorizar,
intercambiar los papeles, ponerle en el lugar del otro. Pensar en cómo te sientes siendo Sancho o Don Qui-jote y anotarlo. Explicación de sentimientos, conocerse a uno mismo y relajación.Naturalista: elaboración de un informe sobre la fl ora y fauna del lugar donde se desarrolla el capítulo.
Todo esto contribuye a un mejor desarrollo del paciente con síndrome de Down y potencializa sus capacidades al máximo. Esta mejora puede ser imple-mentada no sólo en nuestra sociedad española, puede llevarse a cualquier población, sólo considerando la idiosincrasia de cada una, así como la adaptación a sus sistemas educativos.
Bibliografía
1. Ruiz E. Síndrome de Down. La etapa escolar: Guía para profesores y familias. 2a edición. Madrid: Editorial Cepe; 2009, p. 34.
2. Arraiz A. Defi ciencia mental: niños con síndrome de Down. Alcoy: Editorial Marfi l; 1994.
3. Pueschel S. Síndrome de Down. Hacia un futuro mejor. Guía para los padres. Barcelona: Editorial Masson; 1991.
4. Down España. II Plan de acción para personas con síndrome de Down 2009-2013. Madrid: Down España y Obra Social Caja Madrid; 2009, pp. 26-27.
5. Cunningham C. El síndrome de Down. Una introducción para padres. Barcelona: Editorial Paidós y Fundación Catalana Síndrome de Down; 1990.
6. Troncoso MV, del Cerro MM. Síndrome de Down: lectura y escritura. Barcelona: Editorial Masson; 1998, p. 5.
7. Ortega J. Nuevas tecnologías y aprendizaje matemático en niños con síndrome de Down. Madrid: FEISD; 2005, p. 29.
8. Moran J. Envejecimiento y síndrome de Down. Una guía de salud y bienestar. Nueva York: National Down Syndrome Society; 2013.
9. Salmerón-Vílchez P. Evolución de los conceptos sobre inteligencia. Planteamientos actuales de la inteligencia emocional para la orientación educativa. Educación [Internet]. 2002; 21 (5): 97-121. [Recuperado el día 2 de febrero de 2016] Disponible en: http://www.redalyc.org/pdf/706/70600506.pdf
10. Gardner H. Inteligencias múltiples: La teoría en la práctica. Barcelona: Ediciones Paidós; 2011.
11. Prieto MD, Ferrándiz C. Inteligencias múltiples y currículum escolar. Málaga: Editorial Aljibe; 2001.
12. Ruiz E. Todo un mundo de emociones. Educación emocional y bienestar en el síndrome de Down. Madrid: Editorial Cepe; 2016.
13. Fundación Mapfre. Las inteligencias múltiples y la escuela inclusiva. [Recuperado el 19 de febrero de 2016] Disponible en: https://www.fundacionmapfre.org/fundacion/es_es/images/inteligencias-multiples_tcm1069-220993.pdf

Investigación en Discapacidad128
Key words: Western blot,
immunodetection, electrophoresis, protein,
immunoblot, antibody.
Palabras clave: Western blot,
inmunodetección, electroforesis, proteína,
inmunoblot, anticuerpo.
www.medigraphic.org.mx
Western blot: a tool in the biomedical fieldWestern blot: una herramienta en el área biomédica
Karina Martínez-Flores,* Ángel Tonatiuh Salazar-Anzures,* Javier Fernández-Torres,* Carlos Pineda,* Carlos Alberto Aguilar-González,* Alberto López-Reyes*
General interest
Vol. 6, No. 3 September-December 2017
pp 128-137
Abstract
The Western blot technique, also called immunoblotting, is a high-sensitivity and semi-quantitative molecular technique that allows the analysis of a specific protein or protein profile. This is a technique for separating proteins according to their charge and molecular weight in polyacrylamide gels and their subsequent transference to a solid membrane, in which a specific antibody detects the protein. Four decades after its creation, the Western blot technique has gained an essential role in the diagnosis of various medical conditions, as well as an everyday tool in biomedical research.
Resumen
La inmunotransferencia de proteínas, o Western blot, es una técnica molecular semicuantitativa de alta sensibilidad que permite la inmunodetección específica de una proteína o perfil de proteínas. Esta técnica se basa en la separación de proteínas de acuerdo con su carga y peso molecular en geles de poliacrilamida y su posterior transferencia a una membrana sólida, en la que un anticuerpo específico detecta la proteína de interés. Cuatro décadas después de su creación, la técnica de Western blot ha ganado un papel importante en el diagnóstico de varias condiciones médicas, además de constituir una herramienta de cada día en la inves-tigación biomédica.
* Laboratorio de Líquido Si-novial, Instituto Nacional de Rehabilitación.
Mailing address:Karina Martínez-FloresCalzada México-Xochimilco Núm. 289,Col. Arenal de Guadalupe, 14389,Ciudad de México, México.Phone: (55) 5999 1000, 19502E-mail: [email protected]
Received: September 08, 2016.Accepted: March 03, 2017.
This article can be read in its full version in the following page:http://www.medigraphic.com/rid
Introduction
The Western blot (WB) analysis is an analytical technique used to detect proteins. The technique is based on the separation of proteins by molecular weight (MW) and electric charge using a gel electrophoresis. Afterwards, the proteins are transferred to a synthetic membrane and they are exposed to antibodies of interest (primary antibodies). Most of the time, the primary antibody must be coupled to a second antibody
attached to a developer that identifi es the protein of interest (Figure 1A).1-3 The WB emerged in 1970, when Ulrich Laemmli used the principle of molecule separation through an electrical gradient using polyacrylamide gels. At the end of this decade, Towbin (1979) described the transfer of proteins from polyacrylamide-urea gels to nitrocellulose sheets, being Burnette two years later, who employed the term Western blot (WB) for the technique using polyacrylamide gels and sodium dodecyl sulfate (SDS-PAGE).4-7 Nowadays, the WB

Volume 6 Number 3 September-December 2017 129
Karina Martínez-Flores et al.
www.medigraphic.org.mx
has become a key technique in the biomedical fi eld for diagnosing infectious, autoimmune, rheumatic and oncologic diseases.3,4,8 This review is centralized in describe and analyze the main characteristics of the WB and the importance of this technic in the biomedical fi eld.
Cell lysis to extract protein
The WB is a versatile technique that detects proteins from animal and herbal tissues, cell cultures, bacteria and yeast. In order to obtain trustworthy results, a good protein extraction is required, which can be performed by mechanical and chemical methods. Within the mechanical methods, the most used are sonication, homogenization using abrasives, and disintegration with glass or metallic beads.9 The chemical methods include the use of buffers capable of solubilizing the proteins, since they contain ionic detergents such as sodium dodecyl sulfate (SDS), deoxycholate and cetyl trimethylammonium bromide (CTAB). It is also possible to use other detergents, such as non-ionic or zwitterionic chemicals, and the choice depends on the speed of the lytic effect, as well as the extraction effi ciency desired. For example, SDS can lyse cells in seconds, but it can denature the proteins. Triton X-100 is a non-ionic detergent that can lyse cells smoothly
and slowly, avoiding protein denaturation and protein complex breakdown; this method is recommended for assays involving protein structure or protein activity. The zwitterionic detergents,-like 3 [(3-cholamidopropyl) dimethylammonium] -1-propanesufonate can be used without affecting the net charge or the charge of the solubilized protein. One of the most widely used buffers for its effi ciency solubilizing proteins is radioimmunoprecipitation assay (RIPA), which contains 50 mM Tris-HCl pH 7.5, 150 mM NaCl, 1% Triton X-100, 0.5% sodium deoxycholate, 0.1% SDS, 5 mM EDTA, and a commercial inhibitor of proteases.10 In HT-29, the colon cancer cell line, this reagent has showed a high effi ciency solubilizing cytoplasmic proteins.11 Besides RIPA, there are buffers for extracting cytoplasmic proteins, such as Tris-Triton (10 mM Tris pH 7.4, 100 mM NaCl, 1 mM EDTA, 1 mM EGTA, 1% Triton X-100, 10% glycerol, 0.1% SDS, 0.5% deoxycholate) and the 20 mM Tris-HCl pH 7.5 for cytoplasmic proteins. The purpose of using lysis-buffer solutions supplemented with proteases inhibitors is to maintain the protein structures. Finally, after the lysis process, the sub-cellular fractions are separated trough differential centrifugations, at the end; it is possible to obtain membrane proteins in the pellet and soluble proteins in the supernatant.4,12
AA
BB CC
Load the proteins The proteins are separate The proteins are transferred from Then membrane is Then the membrane is incubated through electrophoresis and the gel to a synthetic membrane, incubated with with the secondary antibody coupled it’s verify with Coomassie blue migration is confirmed by red the primary antibody to a peroxidase or phosphatase enzyme ponceau that will reveal the protein of interest
Load samples Running
Molecular weight marker
Tracking dye
Figure 1.
(A) The steps of the western blot. a) Loading the protein into the gel, separation by electrophoresis, transfer and immunomarking . (B) The protein sample is loaded using a micropipette for precision (20-40 μg). (C) The separated proteins are visualized with a tracking dye (bromophenol blue) and molecular weight marker.

Investigación en Discapacidad130
Western blot: a tool in the biomedical field
www.medigraphic.org.mx
Protein quantification
Before performing the electrophoresis, the protein content needs to be quantifi ed in order to homogenize the amount deposited in the well of the gel and to determine the protein concentration. A large amount of protein can saturate the immunodetection and yield unspecifi c results.13
There are different methods to quantify proteins. The most used are Lowry, Bradford and bicinchoninic acid (BCA). These colorimetric assays are based on the color change when some protein amino acids react to different reagents.13,14
LOWRY PROTEIN ASSAY
This method is characterized by the use of Follin reagent and copper, it is detected in a wavelength of 750 nm, and the color intensity is based on the protein concentration.15
BRADFORD PROTEIN ASSAY
This method uses Coomasie Brilliant Blue dye, which reacts in the presence of proteins, and the color change is detected in the wavelength range of 465-595 nm.15
BICINCHONINIC ACID ASSAY
The protein assay with bicinchoninic acid (BCA) is highly sensitive and combines the reaction of proteins with Cu2+ ions in an alkaline method in the presence of a reagent that detects Cu+ ions with a high sensitivity, known as BCA. Its variation is minimum. It has been reported that the macromolecular structure of the protein and four specifi c peptides (cysteine, cysteine, tryptophan and tyrosine) are responsible for the change in color in the samples into a purple hue that can be detected at a wavelength of 562 nm.14,15
The electrophoresis gels
Several methods have been used to separate proteins, most notably those involving cellulose acetate paper, a starch gel that improved the resolution, but did not provide control over the pore size. More recently, polyacrylamide gels are used to control the pore size thanks to the regulation of acrylamide (referred to as % T) and bisacrylamide (referred as % C) percentage. With a higher percentage of acrylamide (10-20% T), the pore size is reduced and the gel is optimal for separating low molecular weight proteins (less
than 50 kDa), whereas gels with a lower percentage of acrylamide (< 10% T) are recommended for separating higher molecular weight proteins (greater than 100 kDa).16-18 Adding ammonium persulfate and tetramethylethylenediamine (TEMED) generates free radicals that accelerate the acrylamide polymerization. The versatility of the running buffers for polyacrylamide gels provides a fast method to separate proteins in order to identify them.18
Types of gels
Protein separation through polyacrylamide gels can be performed under naive or denaturing conditions. The non-denaturing polyacrylamide gels (ND-PAGE) keep the protein structure in a tridimensional shape and the separation is based on the electric charge, size and shape. In order to maintain the protein structure, a non-reductive, non-denaturant buffer solution is used, such as tri-glycine within a pH range between 8.3 and 9.5, or tris-borate at a pH of 7.0 to 8.5, and tris-acetate with a pH of 7.2 to 8.5.19 In contrast, in the denaturing polyacrylamide gels (SDS-PAGE), the protein structures are dissociated in peptides using a combination of an anionic detergent (SDS), a reducing agent (beta-mercaptoethanol), and heat. SDS binds and provides negative charge to proteins and breaks the hydrophobic interactions, whereas beta-mercaptoethanol and the heat break the disulfi de bridges (Cys-S-S-Cys) and thiol groups (Cys-SH) present in the polypeptide chains, ensuring protein dissociation (Figure 2A).4,16,18,20 Once the gel is polymerized, a suitable concentration of protein (20-40 μg) is deposited in the well created with the comb (10-15 well) (Figure 1B). Protein supernatant volume and concentration can depend on the well capitation and thickness (0.75-1.5 mm).21
Discontinuous and continuous buffer systems
Depending on the type of buffers, there are two electrophoresis systems, the continuous buffer system of Weber and Osborn, in which the same running buffer is used in the single separator gel and the tank, and the discontinuous buffer or Laemmli system, which employs two types of gels: a «stacking gel» (large-pore) made with 4% of acrylamide and a «resolving gel» (small-pore) that polymerizes on the stacking gel. In the discontinuous system, the buffers used in each gel are made is different with different pH and ionic strength, and the running buffer employed is a different one. The most widely used is the discontinuous system,

Volume 6 Number 3 September-December 2017 131
Karina Martínez-Flores et al.
www.medigraphic.org.mx
where protein mobility in the stacking gel is mediated by the chloride ions (Cl-) in the gel and the glycine ion (Gly-) in the sample buffer, resulting in a zone with low conductivity and voltage difference that favors the protein concentration before the transfer to the resolving gel, where the basic pH promotes glycine ionization for migration along the gel and favors protein separation based on the size.22
Sample preparation
Before carrying out the electrophoresis, the samples are heated in a temperature range between 70-95 oC in a buffer known as «loading buffer», which has the purpose of providing weight, density and color to the sample in order to allow for the sample to load into the well and avoid any leakages. This buffer contains 62.5 mM of Tris-HCl at a pH of 6.8, 2% SDS, 10% glycerol, 100 mM dithiothreitol (DTT) and 0.01% bromophenol blue. Among these components, DTT or beta-mercaptoethanol are the reducing agents that break the disulfi de bonds. On the other hand, SDS allows the denaturation of proteins into a primary structure and covers them with a negative charge, making it possible to separate the proteins based on their molecular weight. Additionally, the reduction and denaturation allows for the antibody to reach its union site.22
In the gel, proteins with a lower molecular weight (MW) migrate to the bottom and those with a higher MW stand in the top of the gel. The protein migration throughout the gel can be observed thanks to the
bromophenol blue dye besides the protein molecular weight marker. The last one helps mainly to identify the protein of interest because this marker contains purifi ed proteins with different MW (Figure 1C).4,16,17,23,24
Transfer of proteins to the membrane
In this technique, proteins must be transferred to a resistant solid support, like a membrane, so they can easily be handled and used in the immunodetection process with specifi c antibodies.25
The transfer principle is similar to the polyacrylamide gel electrophoresis, i.e., negatively charged proteins migrate towards the positive electrode under the infl uence of an electric fi eld.
The membrane is interposed between the gel and the positive electrode (Figure 2B), and the proteins are retained in the membrane with the same distribution they had in the gel. The transfer can be performed through one of two systems: semi-dry or wet. Both systems are characterized by the close contact between the gel and the membrane, but the wet process requires a higher volume of transfer buffer and longer exposure in lower temperature (2-12 h at 4 oC) compared to the semi-dry system (7-30 min at room temperature).22,25
In both types of transference, the use of different buffers is recommended, such as Tris-glycine in a range of several concentrations at a pH of 8.3-9.2 and SDS (0.025-0.1%), with or without 20% methanol, bicarbonate buffer with at a pH of 9.9, SDS (0.025-
Figure 2.
Denaturation and transfer. (A) Protein cleavage requires an anionic detergent, SDS, to provide them with a negative charge, beta-mercaptoethanol, and high temperature to break the disulfide bonds of the polypeptide chains. (B) The transfer takes place from the negatively charged proteins in the gel to the membrane following the same distribution from the gel.
SpongeFilter paperFilter paperFilter paperGelMembraneFilter paperFilter paperFilter paperSpongeBB
AA
TemperatureSDS

Investigación en Discapacidad132
Western blot: a tool in the biomedical field
www.medigraphic.org.mx
0.1%) and 1x TBE (Tris-borate 90 mM, EDTA 1 mM). The Tris-glycine buffer, pH 8.3, containing SDS at 0.1% with methanol at 20% is the most widely used buffer, especially because it is the universal buffer without methanol for the SDS-PAGE gel. The methanol has two main roles: triggering the dissociation of SDS to the protein and drastically improving the adsorption of proteins in the membranes in the presence of SDS. However, these effects may vary among proteins.26
The supports that are frequently used in the transfer are microporous surfaces, such as nitrocellulose membranes or polyvinylidene difluoride (PVDF), which provide different features that affect the result.16,25 These membranes should have important properties, such as a high binding capacity, ease of storage of immobilized molecules in the short and long term, and reproducibility.22,26 The PVDF membrane is stronger and provides better binding to the protein, unlike nitrocellulose. Nevertheless, the nitrocellulose membrane provides less background noise. In comparison to the nitrocellulose membranes, the PVDF membranes need to be moistened in methanol or ethanol before using them due to their highly hydrophobic nature, and they do not have any surfactant. Recently, in order to reduce the background noise, membranes of low autofl uorescence are used.3,17
Immunodetection
Once the proteins are retained in the solid phase (membrane), the non-specifi c and empty sites in the membrane are blocked. The most widely used blocking agents include those that contain proteins because they can bind to the empty sites on the membrane. This reduces the background noise because the antibody added can only bind to the sites of the proteins in question. Some protein-containing blocking agents include horse or fetal calf serum and Tween-20 (a detergent) if there is so much background. However,
non-ionic detergents should be used carefully, since they can solubilize the proteins transferred to the membrane. Nonetheless, non-fat milk and bovine serum albumin (BSA) are the most widely used. Non-fat milk has a sub-optimal behavior in the analysis of phosphorylated proteins because it contains casein, a phosphoprotein that may compete for the antibody target, thus reducing the intensity of a non-specifi c signal.11
The previously blocked membranes are incubated with the primary specifi c antibody of the protein of interest. The antibodies used in WB can be polyclonal antibodies that recognize several regions of the antigen or monoclonal antibodies that recognize a single region of the antigen, as shown in fi gure 3.16
Most of the time, the primary antibody is not coupled to any developing agent. Therefore, incubation is required afterwards with a secondary antibody. The secondary antibodies bind to the primary antibodies that are not bound to antigens, and they are selected depending on the species in which the antibody is made primary.17
Immunodetection of proteins
CHEMILUMINESCENT IMMUNODETECTION
Immunodection by chemiluminescence uses peroxidase or phosphatase enzymes coupled to a secondary antibody that radiates energy in the form of light generated by a reaction of luminescent compounds (luminol). This allows for the detection of the antigen-antibody binding (Figures 4A and 4B). The light reaction is developed in autoradiographic fi lm, and more recently, it is digitally captured using a digital camera to identify the protein of interest.16
The sensit ivity of the chemiluminescence immunodetection technique depends on the linearity of the detection, which generally is present in loads
wwwwwwwwwwwwwwww mmmmmmmmmeeeeeeddddiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiigggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrraaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaappppphhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiccccc....oooooooooooooooooooorrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrggggggggggggggggggggggggggggggggggggggggggggg.....................mmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmxxxx
Polyclonal antibodies
AA BB
Figure 3.
Recogn i t i on d i f f e r ence of primary antibody. (A) Monoc lona l an t i bod i e s recognize a region of the an t i gen . (B ) Po l yc lona l antibodies recognize several antigenic regions.
Monoclonal antibodies

Volume 6 Number 3 September-December 2017 133
Karina Martínez-Flores et al.
www.medigraphic.org.mx
lower than 5 μg.27,28 The signal saturation is directly related to the protein expression, considering this immunodetection method as «semi-quantitative», since the saturation point in the signal is a critical factor for determining the differences in the expression levels of the samples and could lead to inaccurate measurements.28 The captured image allows the pixels quantifi cation of each band that were obtained through a densitometric analysis, using the analysis software included in digital systems (Figures 4C and 4D).7,16,17,29
IMMUNODETECTION WITH FLUORESCENCE
Recently, a fl uorescent immunodetection method has been proposed, in which secondary antibodies couple to a fl uorescent marker or fl uorophore and emit light when they are excited, creating a lineal-detection signal
(Figures 5A and 5B). A digital camera with fi lters of different wavelengths detects the emitted light. Similar to the images revealed by the chemiluminescence technique, the images captured are analyzed with the same principle. However, the result is quantitative because of the signal stability, in contrast to the chemiluminescence immunodetection method (Figures 5C to 5E).1,28,29
WESTERN BLOT APPLICATIONS IN THE BIOMEDICAL FIELD
In the clinical fi eld, the WB technique serves as a diagnostic method for various infectious, autoimmune, and oncological diseases.16,17,30 This technique is one of the most important tools used in medical research. In the infectious diseases area, protein detection through WB supports the diagnosis of various diseases, like
wwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwww...........................mmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmeeeeeeeeeeedddddddiiiiiiiiiiggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrraaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaappppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppppphhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhiiiiiiiiiiiiiiiiiiiiiiiiiccccccccccc.oooooooorrrrrrrrrgggggggg.mmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmxxx
Figure 4.
L u m i n e s c e n t Immunodetec t ion . (A) Immunodetection carried out with a luminescent compound (luminol). (B) The reaction between peroxidase or phosphatase and luminol emits light, allowing for the antigen-antibody detection. (C) The dens i tometr ic analysis determines the molecular weight and (D) the number of pixels on the band of interest.
AA
BB
CC DD
Net intensity (pixels) 64586
Molecular weight 60344,8(Daltons)
Secondary antibody
Primary antibodyLuminol
Molecular weight marker Interest protein Blocking protein
Light emission
HRP
HRP
2MW (Da)60344.8

Investigación en Discapacidad134
Western blot: a tool in the biomedical field
www.medigraphic.org.mx
visceral leishmaniasis, where the strain of the parasite causing the disease can be identifi ed using the WB.31 In the diagnosis of congenital toxoplasmosis, WB has allowed for the identifi cation of proteins involved in the
immune response against the toxoplasma parasite.32,33 The WB has been used as a diagnostic test for Lyme disease (caused by the bacterium Borrelia burgdorferi) transmitted to humans through the bite of an infected
wwwwwwwwww....mmmmmmeeeeeedddddddiiiiiiggggggggggrrrrrrrrrraaaaaaaaaappppppppppp
Figure 5.
F l u o r e s c e n t i m m u n o d e t e c t i o n . ( A ) F l u o r e s c e n t immunodetection performed with secondary antibodies coupled to a fluorophore. (B) When excited, the f luorophore emits l ight for detecting the antigen-antibody interaction. (C) The immunofluorescence images allow for the individual analysis of a protein in its phosphorylated form, as well as (D) the full analysis (E) together (merge).
MergepEGFR + Total EGFR
Without EGF Stimulus EGF Stimulus
Fluorophore
Secondary antibodyPrimary antibody
Excitation
Molecular weight marker Interest protein Blocking protein
Light emission
pEGFR Total EGFR
AA
BB
CC DD
EE

Volume 6 Number 3 September-December 2017 135
Karina Martínez-Flores et al.
www.medigraphic.org.mx
blacklegged tick, and it is used to identify a protein array characteristic of the bacteria in serum.34-37
Moreover, the WB analysis of serum samples of patients with melioidosis also called Whitmore’s disease (caused Burkholderia pseudomallei) has been able to characterize the bacterium proteins causing the disease.38
The WB has been used to confi rm the diagnosis of pulmonary tuberculosis, identifying the mycobacterial antigens characterist ic of M. tuberculosis .39
Additionally, the WB has been considered a high-sensitivity diagnostic test for detecting congenital syphilis in samples of asymptomatic children.40 The WB has served as a 100% reliable test to diagnose the herpes virus infection, detecting 22 serum samples with the virus out of a total of 27.41 The WB has proven to be a non-invasive and highly sensitive diagnostic test detecting 47.8% of patients with duodenal ulcer caused by Helicobacter pylori.42 In the hydatid disease caused by the cestode Echinococcus granulosus, the WB has been able to detect specifi c antibodies for proteins of 39 and 42 kDa in 96% of patients with hydatid disease.43 Recently, this technique has been established as a pre and postsurgical diagnostic test for detecting hydatid cysts because of its demonstrated high sensitivity of 100%.44
The WB has been used to identify proteins in synovial fl uid and serum, allowing for the diagnosis of clinical symptoms of rheumatoid arthritis and osteoarthritis.45-47
Wang et al. (2011) used the WB to determine the expression levels of the follistatin-like protein 1 (FSTL1) as a possible biomarker of damage in the articular level in patients with knee osteoarthritis, since it is involved in the prevention of mechanisms of articular degradation in vivo and in vitro models. Their fi ndings revealed a relationship between the overexpression of FSTL 1 and the osteoarthritis degree.48
Recently, α1-antitrypsin (A1AT), a protease inhibitor, has been reported to be a great load control for the WB in samples of synovial fl uid of patients with osteoarthritis, since it is abundant and constant.49
This technique has managed to show the relationship between the protein expression levels of the leukocyte antigen system class II (HSP60, HSP70, p53 and collagen II) and the development of rheumatoid arthritis (RA) in patients sera.50
The WB technique has been a key factor in the identifi cation of the citrullinated protein (CCP) as a marker for RA in samples of synovial fl uid, given its high sensitivity (80%) and specifi city (98%) values.51
In 2002, Salma et al. used the WB technique to detect proteins of the parasite Sarcocystis in sera samples of RA patients as positive markers for detecting rheumatic diseases.52
Recen t l y , i n samp les o f pa t i en t s w i t h laryngeal cancer, the WB showed for the first time overexpression of a protein called PFN1, responsible for metastasis of this carcinoma (laryngeal), considering it a biomarker for diagnosis and a therapeutic target.53
The WB help in the early diagnosis of liver cancer, identifying the 14-3-3 proteins expressed during progression to hepatocellular carcinoma in patients who have not been diagnosed with the disease.54
In esophageal cancer, the WB has allowed for detecting overexpression of the protein glutathione S-transferase omega 1 (GSTO1), which induces an immune response, considering this protein as a biomarker for early diagnosis of the disease.55
In a mouse model with Alzheimer’s disease (AD), the WB technique identifi ed the overexpression of a drug transporter called ABCG2, which allows the passage of a protein that causes a vascular damage called cerebral amyloid angiopathy (CAA), considering ABCG2 a biomarker for the CAA pathology in patients with Alzheimer’s.56 It has also played a key role in identifying seven prognostic biomarkers for prostate cancer that determine the aggressiveness degree.57
In muscular dystrophies, the WB has been recognized as a reliable technique for routine diagnosis.58
Besides these applications, the WB technique is consider as a helpful tool in several fi elds in the biomedical area, contributing in the boarding of different diseases in order to have a diagnostic and unders tand some phys iopa tho log ica l characteristics.59
Conclusions
For more than four decades, the WB technique has been used as a suitable tool in the biomedical research fi eld due to its application in a wide range of different samples, using photodocumentation equipment that goes from the most simple approach of luminescence detection to the more sophisticated ones that are able to detect specific emission sources for specifi c fl uorophores, which increases the cost, but yields more effi cient results, making it a crucial tool for diagnosing and detecting several diseases, and for fi nding therapeutic targets, giving this technique a major importance in the clinic area.

Investigación en Discapacidad136
Western blot: a tool in the biomedical field
www.medigraphic.org.mx
Bibliography
1. Eaton SL, Roche SL, Llavero-Hurtado M, Oldknow KJ, Farquaharson C, Gillngwater TH et al. Total protein analysis as a reliable loading control for quantitative fl uorescent Western blotting. PLoS One. 2013; 8 (8): e72457. doi: 10.1371/journal.pone.0072457.
2. Yang Y, Ma H. Western blotting and ELISA techniques. Researcher. 2009; 1 (2): 67-86.
3. Kurien BT, Scofi eld RH. Western blotting. Methods. 2006; 38 (4): 283-293.
4. Jensen EC. The basics of Western blotting. Anat Rec (Hoboken). 2012; 295 (3): 369-371.
5. Kistler J, Duncombe Y, Laemmli UK. Mapping nucleolar proteins with monoclonal antibodies. J Cell Biol. 1984; 99 (6): 1981-1988.
6. Burnette WN. Western blotting: electroporectic transfer of proteins from sodium dodecyl sulfate-polyacrilamide gels to unmodified nitrocellulose and radiographic detection with antibody and radioiodinated protein A. Anal Biochem. 1981; 112 (2): 195-203.
7. Towbin H, Staehelin T, Gordo J. Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: procedure and some applications. Proc Natl Acad Sci USA. 1979; 76 (9): 4350-4354.
8. Chang X, Zhao Y, Sun S, Zhang Y, Zhu Y. The expression of PAD14 in synovium of rheumatoid arthritis. Rheumatol Int. 2009; 29 (12): 1411-1416.
9. Martínez-Maqueda D, Hernández-Ledesma B, Amigo L, Miralles B, Gómez-Ruiz JA. Extraction/fractionation techniques for proteins and peptides and protein digestion. In: Proteomics in foods. Springer US: 2013; pp. 21-50.
10. Johnson M. Detergents: Triton X-100, tween-20, and more. Mater Methods. 2013; 3: 163.
11. Perkel-Jeffrey M. Preparing for your Western blot. Science/AAAS Custom. Publishing Offi ce: Western Blotting: A Guide to current methods 2015; pp. 7-8.
12. MacPhee DJ. Methodological considerations for improving Western blot analysis. J Pharmacol Toxicol Methods. 2010; 61 (2): 171-177.
13. Sapan CV, Lundblad RL, Price NC. Colorimetric protein assay techniques. Biotechnol Appl Biochem. 1999; 29 (2): 99-108.
14. Huang T, Long M, Huo B. Competitive binding to cuprous ions of protein and BCA in the Bicinchoninic Acid Protein Assay. Open Biomed Eng J. 2010; 4: 271-278.
15. García-Arellano H, Vázquez-Duhalt R. Cuantifi cación de proteínas: una revisión. BioTecnología. 1998; 3: 77-88.
16. Mahmood T, Yang P. Western blot: technique, theory and trouble shooting. N Am J Med Sci. 2012; 4 (9): 429-434.
17. De la Fuente GA, Rodríguez LJ, Fonseca CE. Análisis de proteínas mediante electroforesis e inmunotransferencia (Western blot). Piel. 2007; 22 (5): 252-258.
18. García PHM. Electroforesis en geles de poliacrilamida: fundamentos, actualidad e importancia. Univ Diag. 2000; 1 (2): 31-41.
19. Pérez-Chabela ML, Soriano-Santos J, Ponce-Alquicira E, Díaz-Tenorio LM. Electroforesis en gel de poliacrilamida-SDS como herramienta en el estudio de las proteínas miofribrilares. Una revisión. Nacameh. 2015; 9 (2): 77-96.
20. Cambell MK, Farrell SO. Bioquímica. 4a edición. México, D.F.: Editorial Thomson; 2004.
21. Lomonte BV. Técnicas de laboratorio en inmunología. 3a edición. San José, Costa Rica: Universidad de Costa Rica; 2009.
22. Kurien BT, Scofi eld RH. Western blotting: methods and protocols. Methods in molecular biology; v. 1312. New York: Springer; 2015: pp. 509.
23. Westermeier R. Electrophoresis in practice. 4th edition. Weinheim, Alemania: Wiley-VCH Verlag GmbH; 2005.
24. Laemmli UK. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature. 1979; 227 (5259): 680-685.
25. González JM, García E, Fernández JL, Gago L, Benito J. Técnicas analíticas para la detección de gluten en alimentos. Madrid, España: Elecé Industria Gráfi ca; 2007.
26. Pettegrew CJ, Javini R, Islam MR. Transfer buffer containing methanol can be reused multiple times in protein electrotransfer. J Biomol Tech. 2009; 20 (2): 93-95.
27. Silva JM, McMahon M. The fastest Western in town: a contemporary twist on the classic Western blot analysis. J Vis Exp. 2014; (84): e51149. doi: 10.3791/51149.
28. Eaton SL, Hurtado ML, Oldknow KJ, Graham LC, Marchant TW, Gillingwater TH et al. A guide to modern quantitative fl uorescent Western blotting with troubleshooting strategies. J Vis Exp. 2014; (93): e52099. doi: 10.3791/52099.
29. Degasperi A, Birtwistle MR, Volinsky N, Rauch J, Kolch W, Kholodenko BN. Evaluating strategies to normalize biological replicates of Western blot data. PLoS One. 2014; 9 (1): e87293. doi: 10.1371/journal.pone.0087293. eCollection.
30. Sarimehmetoglu HO. Application of Western blotting for the immunodiagnosis of Fasciola hepatica in cattle using excretory/secretory antigens. Turk J Vet Anim Sci. 2002; 26: 1061-1065.
31. Carrillo RT, Moreno G, Márquez J. Análisis de inmunoblot de antígenos de Leishmania infantum y Leishmania donavani en sueros de pacientes con leishmaniasis visceral de Venezuela. Rev Fac Farm. 2012; 54 (1): 21-30.
32. Khammari I, Saghrouni F, Yaacoub A, Meksi SG, Ach H, Garma L et al. IgG western blot for confi rmatory diagnosis of equivocal cases of toxoplasmosis by EIA-IgG and fl uorescent antibody test. Korean J Parasitol. 2013; 51 (4): 485-488.
33. Magi B, Migliorini L. Western blotting for diagnosis of congenital toxoplasmosis. New Microbiol. 2011; 34 (1): 93-95.
34. Yun LZ, Qin H, Xia HX, Yi J, Zhen G, Mou WY et al. A study of the technique of Western blot for diagnosis

Volume 6 Number 3 September-December 2017 137
Karina Martínez-Flores et al.
www.medigraphic.org.mx
of Lyme disease caused by Borrelia afzelli in China. Biomed Environ Sci. 2013; 26 (3): 190-200.
35. Donta ST. Issues in the diagnosis and treatment of Lyme disease. Open Neurol J. 2012; 6: 140-145.
36. Brouqui P, Bacellar F, Bacellar F, Baranton G, Birtles RJ, Bjoersdorff A et al. Guidelines for the diagnosis of tick-borne bacterial diseases in Europe. Clin Microbiol Infect. 2004; 10 (12): 1108-1132.
37. Schumann J, Blessing M. Impact of TGF-β, GM-CSF and antibody response for diagnosis as well as etiopathology of Lyme disease. Scand J Lab Anim Sci. 2011; 38 (3): 177-185.
38. Wongratanacheewin S, Tattawasart U, Lulitanond V, Wongwajana S, Sermswan R, Sookpranee M et al. Characterization of Pseudomonas pseudomallei antigens by SDS-polyacrylamide gel electrophoresis and Western blot. Southeast Asian J Trop Med Public Health. 1993; 24 (1): 107-113.
39. Rattan AS. Western blot analysis of immune response in pulmonary tuberculosis. Ind J Tub. 1991; 38 (1): 11-15.
40. Meyer MP, Eddy T, Baughn RE. Analysis of Western blotting (immunoblotting) technique in diagnosis of congenital syphilis. J Clin Microbiol. 1994; 32 (3): 629-633.
41. Meshkat Z, Roostaee MH, Soleimanjahi H. Development of a Western blot assay for detection of antibodies against HSV using purifi ed HSV virons prepared by sucrose density gradient. Iran J Basic Med Sci. 2009; 11 (4): 215-220.
42. Gad NMA, El-Din TG, Glil RRA, Darwish M. Role of Western blotting in serological diagnosis of Helicobacter pylori infection. Egypt J Med Microbiol. 2008; 17 (2): 169-177.
43. Doiz O, Benito R, Sbihi Y, Osuna A, Clavel A, Gómez-Lus R. Western blot applied to the diagnosis and post-treatment monitoring of human hydatidosis. Diagn Microbiol Infect Dis. 2001; 41 (3): 139-142.
44. Haghpanah B, Mosavat B, Ghayour Z, Oreizi F. Diagnostic value of hydatid cyst antigens using Western blotting method. Jundishapur J Microbiol. 2010; 3 (4): 175-185.
45. Sharma S, Ghosh S, Singh LK, Sarkar A, Malhotra R, Garg OP et al. Identification of autoantibodies against transthyretin for the screening and diagnosis of rheumatoid arthritis. Plos One. 2014; 9 (4): e93905. doi: 10.1371/journal.pone.0093905. eColletion.
46. Balakrishnan L, Bhattacharjee M, Ahmad S, Nirujogi RS, Renuse S, Subbannayya Y et al. Differential Proteomic analysis of synovial fl uid from rheumatoid arthritis and osteoarthritis patients. Clin Proteomics. 2014; 11 (1): 1. doi: 10.1186/1559-0275-11-1.
47. Struglics A, Larsson S, Hansson M, Lohmander LS. Western blot quantifi cation of aggrecan fragments in human synovial fl uid indicates differences in fragment
patterns between joint diseases. Osteoarthritis Cartilage. 2009; 17 (4): 497-506.
48. Wang Y, Li D, Xu N, Tao W, Zhu R, Sun R et al. Follistatin-like protein 1: a serum biochemical marker refl ecting the severity of joint damage in patients with osteoarthritis. Arthritis Res Ther. 2011; 13 (6): R193. doi: 10.1186/ar3522.
49. Wang S, Zhou J, Wei X, Li P, Li K, Wang D et al. Identifi cation of α1-antitrypsin as a potential candidate for internal control for human synovial fl uid in Western blot. Rheumatology (Sunnyvale). 2015; Suppl 6: 006.
50. Oliva-Gutiérrez E, Martínez-Godoy MP, Zapata-Zúñiga M, Sánchez-Rodríguez SG. Antígenos reconocidos por el suero de pacientes con artritis reumatoide. Archivos de Medicina. 2012; 8 (2): 1-9. doi: 10.3823/088.
51. Tabushi Y, Nakanishi T, Takeuchi T, Nakajima M, Ueda K, Kotani T et al. Detection of citrullinated proteins in synovial fl uids derived from patients with rheumatoid arthritis by proteomics-based analysis. Ann Clin Biochem. 2008; 45 (Pt 4): 413-417.
52. Abdul-Rahman SM, Rashad SM, Doma MA. Human muscle sarcocystosis in relation to non-specific rheumatic diseases and rheumatoid arthritis. Egypt Rheumatol Rehab. 2002; 29 (5): 743-753.
53. Li L, Zhang Z, Wang C, Miao L, Zhang J, Wang J et al. Quantitative proteomics approach to screening of potential diagnostic and therapeutic targets for laryngeal carcinoma. PLoS One. 2014; 9 (2): e90181. doi: 10.1371/journal.pone.0090181.
54. Liu M, Liu X, Ren P, Li J, Chai Y, Zheng SJ et al. A cancer-related protein 14-3-3ς is a potential inmunodiagnosis of hepatocellular carcinoma. Tumour Biol. 2014; 35 (5): 4247-4256.
55. Li Y, Zhang Q, Penq B, Shao Q, Qian W, Zhang JY. Identifi cation of glutathione S-transferase omega 1 (GSTO1) protein as a novel tumor-associated antigen and its autoantibody in human esophageal squamous cell carcinoma. Tumour Biol. 2014; 35 (11): 10871-10877.
56. Xiong H, Callaghan D, Jones A, Bai J, Rasquinha I, Smith C et al. ABCG2 is up-regulated in Alzheimer’s brain with cerebral amyloid angiopathy and may act as a gatekeeper at the blood-brain barrier for AB1-40 peptides. J Neurosci. 2009; 29 (17): 5463-5475.
57. Morgan C, Jenkins SA, Kynaston HG, Doak SH. The role of adhesion molecules as biomarkers for the aggressive prostate cancer phenotype. PloS One. 2013; 8 (12): 1-7.
58. Cooper ST, Lo HP, North KN. Single section Western blot. Improving the molecular diagnosis of the muscular dystrophies. Neurology. 2003; 61 (1): 93-97.
59. Hernández-San Miguel A, San Miguel R, Martín-Gil FJ. Importancia de las aplicaciones clínicas de la proteómica. Rev Lab Clin. 2010; 3 (1): 40-42.

Revista de Investigación en Discapacidad138
Instrucciones para los autores Vol. 6, Núm. 3 Septiembre-Diciembre 2017
pp 138-139
“Investigación en Discapacidad” tiene como objetivo pu-blicar artículos relevantes, innovadores e informativos en el estudio de las bases patológicas, prevención, diagnóstico, tratamiento y rehabilitación de la discapacidad, desde un punto de vista de investigación básica, clínica, tecnológica, epidemiológica y sociomédica. Los tópicos considerados para su publicación corresponden a las áreas biomédica, clínica, químico-biológica, molecular, psicológica, desa-rrollo tecnológico e investigación social. Investigación en Discapacidad acepta artículos conforme a las siguientes secciones: a) Artículo original; b) Artículo de revisión; c) Caso clínico; y d) Interés general.
Idioma: Los artículos podrán ser escritos en español o en inglés. Será responsabilidad de los autores que los resúmenes y manuscritos estén debidamente redactados en el respectivo idioma.
El Manuscrito: Deberá ir acompañado de una carta de presentación dirigida al editor en jefe, en la cual se describirá
menos 2 revisores y anexar sus datos de contacto (nombre, adscripción, correo electrónico y teléfono), en caso de soli-
Asimismo, se anexará el formato de cesión de derechos de
web de la revista).Todos los escritos deberán llevar una carátula con: título
del artículo, título corto de no más de 45 caracteres, nombre
autor corresponsal, el cual deberá proporcionar un correo electrónico, teléfono y dirección postal completa.
Estructura del manuscrito
Resumen: Los artículos deberán anexar un resumen no mayor de 250 palabras, acompañados por 5 palabras clave basadas en los criterios del Medical Subject Headings-Annotated Alphabetic list (National Institutes of health, national library of Medicine, Library operations, Medical Subject Headings, Bethesda, MD 20894, USA, http://www.nlm.nih.gov/mesh/). Los artículos escritos en español deberán presentar tanto el resumen, como las palabras clave en español e inglés. No deberá citar referencias en el resumen.
Cuerpo del Manuscrito: Dependerá del tipo de artículo a consideración:
a) Artículo de Investigación Original. Serán trabajos de investigación inéditos. Los artículos serán divididos en secciones considerando el siguiente orden: introducción, material y métodos, resultados, discusión, agradecimien-
-critos no deberán exceder 4500 palabras sin considerar las referencias y deberá contener máximo 5 cuadros y
en archivos independientes.b) Artículo de Revisión. Los artículos de revisión serán
aceptados por invitación o podrán ser considerados de
estar actualizados, basados extensamente en reportes
un tema de investigación que sea explicado claramen-te con el objetivo de difundir información actualizada
ser considerado como líder de opinión. Los manuscritos pueden o no incluir subtítulos; deberán contener no más de 6000 palabras sin considerar las referencias. Se re-comienda que el número de referencias no sea menor
cuadros en conjunto.c) Caso Clínico. Descripciones de uno o más casos de
excepcional observación que supongan una aportación
psicopatología, en el campo de la discapacidad (máximo 2500 palabras sin considerar referencias y 3 cuadros y/o
-tación del escrito.
d) Interés General. Los artículos de interés general serán manuscritos y/o reseñas relacionados con la ciencia, con el objetivo de divulgar al público en general aspectos sociales, culturales y educacionales asociados al que-
lenguaje coloquial con un máximo de 3000 palabras.
Agradecimientos: -miento a los participantes cuya contribución no reúne los criterios de autoría, por ejemplo: asistencia técnica u opinión profesional; asimismo, se podrán describir las fuentes de
Referencias: Las referencias deberán ser numeradas en el texto con un superíndice, en números arábigos y se-

Volumen 6 Número 3 Septiembre-Diciembre 2017 139
Instrucciones para los autores
guirán el orden en que sean mencionadas por primera vez. Cuando se cite algún trabajo que ha sido aceptado, pero aún no publicado, deberá referirse como “en prensa”. Para información complementaria se sugiere consultar:
www.icmj.gob; www.nlm.nih.gov/bsd/uniform_requirements.html
Artículo:
correlate with BMP4 expression and apoptosis during limb development. Dev Dyn 2005; 231:148-160
Cuando los autores son más de seis, se deberán mencionar y a continuación añadir la abreviatura et al.
Clin Invest. 2007; 117(1):246-257.
Libro: -
-land, Massachusetts. Sinauer Associates; 2003
Capítulo de libro: Autor/es del capítulo. Título del capí-
-
Cuadros: Deberán ser numerados en forma consecu-tiva de acuerdo con el orden citado en el texto, con los
-turas, así como las notas explicativas al pie. Se deberán
referencias.
Deberán enviarse en archivos separados y en el mismo orden en que se citan en el tra-
resolución mínima de 300 dpi e indicando el número de aparición en el texto en el nombre del archivo. Los pies de
de referencias y cuadros.
Envío del manuscrito
Los escritos serán enviados en formato electrónico vía correo electrónico o en un disco que contenga el texto completo en
texto deberá estar escrito con letra Arial 12, a doble espacio
de la página, las páginas deberán numerarse en la parte central inferior de la hoja.
Los escritos para ser sometidos a publicación serán enviados a la siguiente dirección electrónica:
[email protected]; con copia a [email protected]
o pueden ser enviados en un CD al laboratorio de Me-
-dos a la revista e informará sobre su aceptación, rechazo o condicionamiento con base en la evaluación y revisión de los revisores.
Protección de las personas y de los animales que participen en la investigación: Cuando el estudio se reali-ce con seres humanos, los autores deberán indicar que los procedimientos cumplen los principios éticos de la comisión responsable de la experimentación humana (institucional y
los autores deberán explicar las razones y demostrar que el Comité de Ética de su institución aprobó los aspectos dudosos del estudio. Cuando se realicen experimentos con animales, se deberá indicar el cumplimiento de las normativas nacionales e internacionales para el cuidado
deberán aparecer en la sección de Material y Métodos.
Propiedad Literaria:éste es un trabajo que no ha sido publicado (excepto en for-ma de resumen) y que no será enviado a ninguna otra revista.
Una vez que el manuscrito sea aceptado se le solicitará una carta de cesión de derechos de autor que el editor le
los autores del manuscrito. Los derechos de autor pasan a ser propiedad de la revista Investigación en Discapaci-dad y no podrán ser publicados (ni total, ni parcialmente) en ninguna otra parte sin consentimiento escrito del editor.
Los trabajos aceptados podrán ser consultados en la si-guiente página electrónica: http://www.medigraphic.com/rid