Bio-Mechanic Treatment of Dystonia · I can tell you that neurological symptoms like brain fog,...
52
Transcript of Bio-Mechanic Treatment of Dystonia · I can tell you that neurological symptoms like brain fog,...


Copyright Information Page
This document is a free sample with limited content. It includes:
- Chapters 1 to 4 of Part 1 by Marecello Leonard Mazza PhD
- Chapter 6 of Part 2 by Dr. Jeffrey Brown DDS MBA
Copyright © 2017 by New European Bio-Mechanical DystoniaAssociation. All rights reserved worldwide. No part of thispublication may be replicated, redistributed, or given away inany form without the prior written consent of theauthor/publisher or the terms relayed herein.
New European AssociationBio-Mechanical DystoniaEmail: [email protected]: www.biomechanical-dystonia.net
Dr. Jeffrey Brown DDS MBASleep & TMJ Therapy2841 Hartland Road, Suite 301, Falls Church, VA 22043, USAWeb: www.sleepandtmjtherapy.com

Index
About this Book1. Why?2. How?3. Disclaimer4. The Bio-Mechanical Dystonia Association
Part I: Causes1. Introduction2. What is Dystonia?3. A Bio-Mechanical Approach to the Human Body4. Bio-Mechanics of Dystonia5. The Neurological Consequences6. Neurologists: Killing the Messenger7. Displaced TMJ Disks - By Dr.J. Brown8. The Dental Connection9. Can you Trust your Dentist?
Part II: Treatment1. A Protocol for the Treatment of Dystonia2. Principles of Splint Therapy and the TMJ3. Postural Alignment and the Molar Lever4. Cranial Derangement and the ALF5. Phase 16. Phase 27. Phase 3

Part III: Case Studies and Personal StoriesPart IV: Questions & AnswersPart V: Resources and Bibliography

Page 1
About this Book“Science is the belief in the ignorance of experts”
By Nobel Prize winner Richard Feynman

Page 2
Chapter1Why do we Write this Book?
In 2013 life was great. I was a 43 year old athlete. I could run
10 km and swim 1 km four or five times every week. Life was
great. Roberto, my son, was eleven years old and was a
healthy, fun, intelligent and loving presence in a happy family.
Nancy and I were in love and life was fantastic... Then
suddenly, my life changed. . My name is Marcello.
One day, out of the blue, I decided to get rid of some gold
inlays and amalgam fillings that I had in several teeth since I
was 18 years old. The reason was purely (and in a very stupid
way) aesthetic: I did not like having that much metal in my
mouth. Unconsciously, I had subscribed to the goal of having a
“Colgate white”, Hollywood smile. I also was keen on getting
rid of the risk of mercury based fillings in my teeth.

Page 3
It was the biggest mistake of my life.
Within 24 hours of that dental treatment, I woke up as twisted
and dystonic as Stephen Hawking. I was tormented with
involuntary, asymmetric muscle spasms that twisted my spine
and mandible. Life would never be the same again.

Page 4
In a matter of days, a horrible series of events torqued my
entire body. The mandible moved massively towards the left
and got jammed into the skull pressing against the left ear. The
whole spine twisted -a true postural collapse. The rib cage
deformed, the pelvis tilt asymmetrically, one leg became
shorter than the other, the eyes twisted within the eye sockets
and the spinal chord within the neck became compressed to
the point that you can appreciate in the image above.
Needles to say, I had to stop working. I was disabled. And I
had to start looking for medical advise. In the following two
years, I visited the best medical professionals, professors and
self proclaimed experts in Europe.

Page 5
The Nuerologists that I consulted diagnosed me with Cervical
Dystonia with degenerative affection of neck vertebres C5-C6-
C7. In their opinion there was no cure and the only possible
treatment to manage the symptoms consisted of Botox
injections in the neck every 3 months to weaken the pulling
muscles. Eventually, treatment would be given with systemic
anti-epileptic drugs if the situation evolved unfavorably towards
Generalized Dystonia.
The Maxilofacial Surgeons that I consulted insisted that the
only possible treatment consisted in surgically removing part of
the mandible and surgically changing the inclination and
rotation of the maxilla to realign the plane of dental occlusion
with the axis of the skull.
Many Dentists and self proclaimed experts in Dental
Occlusion and Cranio-Facial Pain insisted that there was no
cure and that the neurological symptoms were not related to
dental occlusion. Most of them were completely ignorant of the
symptoms and characteristics of Cervical Dystonia. Many went
as far as displaying great personal and epistemic arrogance
and ignorance by declaring that it was a psychological issue.

Page 6
Nevertheless, it was evident from the very beginning that the
Dystonic Symptoms were related to dental occlusion: I had a
set of two orthodontic clear retainers that reproduced the
dental occlusion I had before the negligent dental treatment
broke havoc with my body neurological system. They were
manufactured at the end of an orthodontic treatment that
endured 10 years before.
When I slept with the clear retainers, all the symptoms of
Dystonia went into remission and, within the first few weeks
after the iatrogenic (iatrogenic is a great term -it means

Page 7
damage cause by a doctor) dental trauma, even disappeared
completely.
Closing the mandible with the clear retainers in place caused
the Atlas (the first cervical vertebra – C1) and the Axis (second
cervical vertebra - C2) and pelvis to move and re-align
themselves with the skull and spine with loud “pop” sounds.
Finding a Solution
Since the medical experts could not help, I had to do my own
homework. I had no choice: I had to support a family, an
eleven year old son and even an ex-wife. The only path offered
by neurologist meant that I had to get used to being disabled,
in pain, unemployed, broke, and addicted to a wide list of
prescription drugs for the rest of my life as I watched my body
degenerate.
I had to find a solution. There was no other choice.
Since none of the best European experts in dental occlusion
and dentists were able to stabilize my dental occlusion, I
resorted to building my own dental splints. Below you can find
the very first dental splint that I ever made.

Page 8
In my case, the elimination of all non-vertical contacts by a
dentist with a drill resulted in a collapsed occlusion (picture on
the left) that triggered dystonic symptoms. The use of a dental
splint to reestablish diagonal, lateral and torque contacts
between the dental arches (picture on the right) resulted in
discontinuance of all dystonic symptoms.
Based on my experience that is how I decided to create a team
of patients, medical professionals and researchers to try an
experimental treatment based on Bio-Mechanics to treat and
cure Dystonia.
And that is also why I will write this book using mainly the
pronoun “we.” It truly has been a team effort.
We started writing a blog ( www.biomechanical-dystonia.net )
about the journey and research and experimental treatment

Page 9
that we were carrying out. Today, only three years later, more
than 70 thousand patients suffering from Dystonia from over
150 countries read the blog. 500 patients have joined a private
Facebook group where they exchange information, comment
on progress and setbacks, ask questions and get answers
about the implementation of the Protocol for the Bio-Mechanical Treatment of Dystonia that we have developed.
We will describe the Protocol in Part 2 of this book.
We have set up a non-profit organization: the New European
Bio Mechanical Dystonia Association. This book has been
funded by the Bio-Mechanical Dystonia Association.
And... the million dollar question? Am I “cured?”
I can tell you that neurological symptoms like brain fog,
involuntary muscle spasms, twisting of the spine and pain are
a long forgotten distant memory.
I lead a very active, happy and productive professional and
personal life. My job takes me travelling around 3 continents
more than 160 days every year. I do not use any Botox or
prescription drug of any kind. I have not been able to go back
to running -which was my great passion and hobby- because

Page 10
my spine is not sufficiently stable. Instead, I HAVE to do an
hour every day of exercise: yoga, or stretching, or low impact
and high lung capacity sports as roller-blading and swimming.
An excellent physiotherapist takes care of straightening my
body every month. I have to sleep with a dental appliance
every night. I will probably have to do it for the rest of my life.
To me, that means being “cured.”
The picture above shows the effect that 6 months of bio-
mechanical treatment had on my body.
I want to stress that we do not claim to have found a “cure” for
Dystonia. We absolutely do NOT claim that we can “heal”
Dystonia, Parkinson and Tourette’s syndromes. We have just
observed empirically that the application of the Bio-

Page 11
Mechanical Protocol that we describe in this book results in amajor improvement of the quality of life – and often full
discontinuance of neurological symptoms – for the patients
who applied it.
At the end of Part 1 of this book, we will come back to what
“curing Dystonia” really means. First it is necessary to explain
a few concepts of our bio-mechanical approach.
An Experimental Treatment Based on Bio-Mechanics
The line of research that this book follows is based on the
belief that:
The cause of Dystonia is strictly related to the bio-mechanical derangement of the cervical spine, TMJand cranial bones driven by the weight of the skullthat sinks, falls, leans and gets twisted as it lacksproper support in the dental arches

Page 12
According to this approach, the skeletal, neurological, chemical
postural, muscular and psychological symptoms that are
described by the academic, medical and scientific literature are
consequences of the effort produced by the body to adjust to
this mechanical derangement and the mechanical twisting
strain on the brain stem and paresthesia of the trigeminal
nerve caused by the sinking skull.
As a consequence, we wish to document in this book an
experimental treatment directed at curing Dystonia (as
opposed to merely covering the symptoms with proscription
drugs and making the disease chronic) starting from:

Page 13
Reestablishing sound support and alignment of theskull on the cervical spine, dental arches andTemporo-Mandibular Joints (TMJ)
What is Dystonia?
If you are not familiar with what Dystonia is, don’t be surprised.
Many medical professionals -including the overwhelming
majority of dentists- have never heard the word Dystonia.
What most patients (and sadly a great number of medical
professionals) fail to realize is that the word “Dystonia” does
not identify a specific, well-defined disease (like HIV infection,
pneumonia or any other disease with a known pathogenic, with
a well-defined cause and measurable treatment). The word
“Dystonia” is just a description of symptoms.
Dystonia is not a disease. The word “Dystonia” is only a
description of a very wide range of symptoms and literally
means “dysfunctional muscle tone.”
In the picture below, you will find a graphical description of
some of the most extreme cases of Dystonia.

Page 14
As a description, the word “Dystonia” is as vague a medical
definition as the word “overweight.” For example: “Cervical
Dystonia” means dysfunctional muscle tone in the cervical
spine; “Oromandibular Dystonia” means dysfunctional muscle

Page 15
tone in the mouth and mandible; “Torsion Dystonia” means
dysfunctional muscle tone that causes torsion of the spine. And
so on and so forth...
It should come as no surprise, given this broad descriptive
definition, that people diagnosed with Dystonia may actually be
suffering from a very extensive range of symptoms, conditions,
injuries and diseases that may or may not be related.
Some patients sharing the same or similar symptoms may not
be diagnosed with Dystonia. Some alternative and
complementary diagnoses include: scoliosis, Tempo-
mandibular Joint Dysfunction (TMD), postural collapse and
bruxism. In addition, various neuro-muscular, orthopedic, and
rheumatologic conditions can cause symptoms similar to those
associated with Dystonia.
There is no black-or-white, definitive test to determine if
somebody has Dystonia.
An it should not come as a surprise, given this broad
descriptive definition, that academic and clinical medical
research has failed to find a specific cause and a specific cure
for Dystonia.

Page 16
Mainstream academic and clinical Neurology definesDystonia as a neurological disorder with physicalmovement consequences
From a Bio-Mechanical approach, Dystonia is acollection of physical injuries, derangement andimpairments that produce neurologicalconsequences
We approach dystonic symptoms as the consequence of an
impairment of the ability of the neck to support the skull due to
mechanical derangement and injury. We maintain that a
combination of physical injuries and derangement in the lower
cranial and upper cervical area can cause neurological
dystonic symptoms.

Page 17
In a sense, it could be compared to a massive injury of the
knee such as triple broken ligaments and deranged knee-
cap…. except the injury is at the level of the upper cervical and
lower cranial areas (TMJ, dental occlusion, cranial base, Atlas,
Axis, Occiput and Sphenoid bone).
Is this a New “Revolutionary” Approach?
The answer to this question is a clear, resounding, loud and
schocking “NO.”
The bio-mechanical approach has been researched and
developed for decades with proven scientific results on
thousands of patients. These patients are real people: you
can talk and chat with them in any of the dozens of online

Page 18
groups of patients suffering from Dystonia undergoing bio-
mechanical treatments.
The protocol we describe in this book does not invent anything
new. It is the result of extensive study and integration of
decades of previous research, experiments and practice of
medical professionals, professors, dentists, orthodontists,
technicians and practitioners such as: Dr. Gelb (father and
son), Dr. Gerber, Dr. Bennet, Dr. Stacks, Dr. Brown, Dr. Mew
(father and son), Starecta, Dr. Lee, Dr. Nordstrom, Dr. Sims.
Moreover, the correlation between some sort of dental trauma
and the onset of Dystonia (specially Cervical Dystonia) has
been reported in scientific research papers for decades.
If you run a search with the text “peripherally induced
secondary Dystonia originated by dental trauma” on Google
Academics, you will find 668 peer reviewed academic research
papers. Yet, the overwhelming majority of dentists have no
knowledge that dental procedures can be the cause that
triggers the onset of Dystonia.

Page 19
The dental connection with dystonic symptoms is awell established scientific fact
In Part 5 of this book (Bibliography and Resources) you will
find many relevant peer reviewed scientific research papers
describing dystonic symptoms arising within hours of dental
procedures.
A complete bibliography of the relevant research papers is
published in Part 5 of this book. We have included over 100
peer reviewed academic research papers, case studies and
FDA approved clinical trials that deal with the biomechanics of
neurological movement disorders.

Page 20
Anyone who is active in the multiple online support groups for
Dystonia patients knows that the overwhelming majority of
patients suffering from dystonic symptoms have endured major
dental works such as extractions, equilbration, orthodontics,
rapid palatal expansion, head gear, orthognathic surgery or
implants.
Yet, the major organizations and foundations who grant
millions of US$ for Dystonia research have never funded any
study on this correlation. On the other hand, millions of US$
are spent researching genetic correlation with very
unimpressive results.
The Bio-Electrical/Chemical approach of mainstream academic
Neurology can not explain this connection.
In one of the next chapters of this book we will analyze the
effectiveness, desirability and side effects of the treatments of
Dystonia offered by neurologists. At this stage, it is sufficient
to understand that prescribed mainstream treatments include:
Botox injections to inhibit muscle activity; drugs that change
the chemistry of the brain and Deep Brain Stimulation surgery
to implant electrodes in the brain to produce balanced
electrical currents.

Page 21
The cause of the supposed misfiring of the basal ganglia is not
understood by academic and clinical neurology. Research
deals with possible genetic correlations with very limited
practical results.
The effectiveness of all these bio-chemical/electrical
treatments is limited (some sources that we will analyze in the
next chapters put it at 30%) and the side effects are massive
and crippling for patients.
Moreover, these bio-chemical/electrical treatments do not even
try to cure Dystonia: their goal is to cover and manage the
symptoms.
The bio-mechanical approach is not mainstream because of
the way medical academia organizes research and teaching in
separate systems.
From a bio-mechanical point of view, the causes andtreatment of Dystonia sit between Traumatology,Dentistry, TMD, Orthopedics, Physiotherapy andNeurology

Page 22
It is not mainstream because there is no money and incentive
from pharmaceutical laboratories to fund bio-mechanic clinical
studies and research.
Even though the bio-mechanical and the bio-chemical
approaches stem from opposite principles, it is important to
understand that:
Bio-mechanical and bio-chemical/electricaltreatments are compatible and complement oneanother.
It is possible to carry out splint therapy while receiving Botox
injections, Deep Brain Stimulation surgery and any drug
treatment prescribed by a neurologist. On the other hand, often
and in many cases, a bio-mechanical treatment results in
discontinuance of neurological symptoms and makes it
unnecessary to endure the massive side effects of prescription
drugs, Botox and brain surgery.
A bio-mechanical treatment of Dystonia can be long but
remarkably inexpensive and effective. And it can improve the
quality of life of patients to the point that they do not need

Page 23
lifelong drug treatments and can live a normal active, working
and family life.
We can conclude this chapter with a message to some of the
most important readers of this book: patients, dentist and
neurologists.
Dystonia sits between Traumatology, Dentistry, TMD,Orthopedics and Neurology
Physical injuries of the upper cervical, lower cranialarea can produce dystonic symptoms
Negligent dental work can cause Dystonia

Page 24
Chapter 2How do we Write this Book?
We wrote this book to be useful for both sufferers from
Dystonia and medical professionals treating neurological
movement disorders.
You will find that this book shatters a significant number of
beliefs, principles and practices that are mainstream in
dentistry, orthodontics, orthopedics and neurology. We will
demonstrate how traditional clinical medicine has had little to
offer in the way of understanding, treating and improving the
quality of life of patients suffering from neurological movement
disorders. Indeed, too often we see that mainstream teachings
of dental schools are the original cause of neurological
movement disorders.
This is not an academic research paper. It is written to inform.
We voluntarily chose to use a language that can be understood

Page 25
by the “average Joe” in order to be able to reach as wide an
audience as possible.
The intention of this book is to allow patients suffering from
Dystonia to build a cooperative relation with the team of
medical professionals that helps them, from a position of
understanding, knowledge and empowerment.
We will show that the patient suffering form dystonic symptoms
needs to adopt a cooperative approach with a team that
includes an excellent dentist, a neurologist, an osteopath, a
physiotherapist and a dental laboratory trained in the bio-
mechanical protocol.
In Part 1 of this book we will analyze the causes and skeletal-
structural-neurological correlations of neurological movement
disorders from a bio-mechanical point of view.
In part 2 of this book we will outline a bio-mechanical protocol
that we have developed for the treatment of Dystonia.
This Protocol does not invent anything new. It is the result of
extensive study and integration of decades of previous
research, experiments and practice of medical professionals,
professors, dentists, orthodontists, technicians and

Page 26
practitioners such as: Dr. Gelb (father and son), Dr. Gerber, Dr.
Bennet, Dr. Stacks, Dr. Brown, Dr. Mew (father and son),
Starecta, Dr. Lee, Dr. Nordstrom and Dr. Sims.
This protocol has shown to be effective also for the treatment
of other occlusion related movement disorders, with varying
levels of neurological symptoms (from postural collapse driven
by a sinking skull to Parkinson’s, Generalized Dystonia,
Oromandibular Dystonia and Tourette’s).
We do not claim to have found a cure. We have just observed
empirically that the application of this protocol results in a
major improvement of the quality of life – and often
discontinuance of neurological symptoms – for the patients
who have applied it.
In Part 3 of this book we will show through the words of
patients and medical professionals that a bio-mechanical
treatment can bring about better results with less side effects
than most mainstream drug-based treatments prescribed by
clinical and academic neurology for a large number of patients
and conditions.

Page 27
Part 4 will be dedicated to reporting on case studies and
patient testimonials.
This is not an academic research paper. Nevertheless, this
book is based on a strictly scientific approach stemming from 4
decades of research, clinical trials, case studies and peer
reviewed academic research papers.
Within Part 5 of this book, the reader can find a very
comprehensive list of the relevant case studies, FDA approved
clinical trials, peer reviewed academic research paper, online
patient groups, resources and videos.

Page 28
Chapter 3Disclaimer
This book is not intended as a substitute for the medical advice
of physicians. The reader should regularly consult a physician
in matters relating to his/her health and particularly with
respect to any symptoms that may require diagnosis or
medical attention.
We do not promote a “do it yourself” approach to the treatment
of Dystonia. We strongly believe that the patient suffering form
Dystonia needs to adopt a cooperative approach with a team
that includes an excellent dentist, a neurologist, an osteopath,
a physiotherapist and a dental laboratory trained in the bio-
mechanical protocol.
Moreover, we believe it necessary to get advise, guidance and
support from the multiple online communities of patients,

Page 29
dentists, neurologists, physiotherapist and osteopaths who are
applying bio-mechanical treatments for Dystonia.
The intention of this book is to allow patients suffering from
Dystonia to build a cooperative relation with the team of
medical professionals that helps them, from a position of
understanding, knowledge and empowerment.

Page 30
Chapter 4Bio-Mechanical DystoniaNon-Profit Association
This research behind this book has been funded by the New
European Bio-Mechanical Dystonia Association, a non-profit
organization dedicated to the research, development and
implementation of bio-mechanical treatments for neurological
movement disorders.
The activities and goals of the New European Bio-Mechanical
Dystonia Association include:

Page 31
1. Raising public awareness about bio-mechanicaltreatments of neurological movement disorders.
2. Providing access to treatment, information andappliances for bio-mechanical treatments, specially tothose patients who do not have access to it due tofinancial or geographic reasons.
3. Promoting and funding research and publication ofrelevant articles and books.
4. Producing and funding videos and practical how-to guidesfor patients and medical professionals.
5. Training medical professionals.
6. Organizing and running informal online medical trials ofspecific treatment protocols.
7. Managing, moderating and funding online communities,forums and blogs.
8. Researching and publishing correlation statistics aboutdental/occlusion related bio-mechanical impairments anddiseases.
9. Raising awareness among dentists and the general publicabout the consequences of dangerous/negligent dentaltreatments.
10. Organizing and participating in seminars, courses andcongresses.

Page 32
Part I: Causes“Look well to the spine for the Cause of Disease.“
By Hippocrates

Page 33
This free sample of the Book only includes Chapter 6 of Part 1
Displaced TMJ Disks
By Dr. Jeffrey Brown DDS MBA
To get more information or buy the whole book, please visit our
blog or become a member of the Bio-Mechanical Dystonia
Association
New European AssociationBio-Mechanical DystoniaEmail: [email protected]: www.biomechanical-dystonia.net
Dr. Jeffrey Brown DDS MBASleep & TMJ Therapy2841 Hartland Road, Suite 301, Falls Church, VA 22043, USAWeb: www.sleepandtmjtherapy.com

Page 34
Chapter6Displaced TMJ Disks
By Dr. J. Brown
When you go to your so-called ‘TMJ Specialist’, it is critical that
certain protocols are honored. And one of those protocols is to
take an MRI of the temporo-mandibular jaw joints (TMJ) in
order to know what you are dealing with.
As someone who exclusively treats TMJ disorders, I have
found it necessary to understand what is going on with the
articular discs BEFORE the patient begins any treatment,
otherwise you are just shooting in the dark.
The reason for this is that in a fair number of patients that I
meet, the discs are already perforated or torn and there is no
amount of therapy that will fix this problem other than doing the
surgery needed to repair or remove the damaged discs.

Page 35
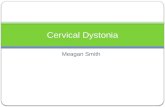
Laterally Displaced TMJ Disk
The image above is a very typical Magnetic Resonance
Imaging scan (MRI) of the TMJ. The top of the jaw bone -
called condyle- is the large whitish thing in the middle of this
image (circle by a white line). The laterally displaced disc is the
black piece hanging off to the left side (circled by a red line).
This is a textbook image of a laterally displaced articular disc.

Page 36
Medially Displaced TMJ Disk
Below is an image of a very medially or inwardly displaced disc.
In both cases, the disc should be almost exactly on top of the
jaw bone, but instead it is pushed off to the side.
In the case of the medial displacement, this is very difficult to
work with because quite often that little disc is tightly ‘jammed’
into the dense tissue in that area and can easily ‘pinch’ nerves
and blood vessels – this is where all the pain comes from.

Page 37
Perforated TMJ Disks
Below is an example of what a perforated disc looks like. As
you can readily see, the condyle (jaw bone) has ground
through the disc and now the condyle is grinding bone on bone
within the socket. This can be not only extremely damaging to
the joint and the condyle, but also very painful as well. This is a
case where surgery is definitely indicated.
This is why the MRI is so critical- why go through all that
appliance treatment if all along you needed surgery anyway?

Page 38
Anteriorly Displaced TMJ Disk
Below, we have the imagery that demonstrates anterior
displacement of the articular disc. This is by far the most
common type of displacement and should be noted that this is
also the easiest type of displacement to correct.
Generally, by wearing a bite splint that takes the pressure off of
the joint region, the discs will self-correct and go back into
proper position if given the chance.
Our appliances are designed to provide freedom of movement
so that the discs can move around enough so that they can
return to proper position over time.

Page 39
How Did the Disk Get Displaced?
One of the most common questions the patients askwhen they discover is: How did this happen?
My response is that the slipped discs are usually caused by
some form of trauma- and that includes birth trauma in many
cases. When a baby is born, and especially if some form of
forceps were used- this is extremely traumatic and it will distort
the skull, twist the cranial bones, and can easily cause the
discs to literally ‘pop’ out of the joints. Years later this will
manifest with the various symptoms that I will describe shortly.
The other question that is often asked of me is: Whydidn’t my doctor/dentist/health care professional tellme about this a long time ago?
Well folks, that’s a great question, and the answer is that none
of this is taught in dental school or medical school. The very
few dentists out there who exclusively treat TMJ disorders
learned through the very few programs out there that teach the
basics, and then there are those like myself who learned by

Page 40
being the apprentice of someone like Dr. Brendan Stack,
arguably the father of TMJ therapy!
Symptoms Associated with Displaced Disks
Now let’s go through some of the obvious symptoms that are
associated with displaced articular discs:
Jaw clicking and or popping are amongst the mostobvious
Headaches and migraines Blepharospasm- lots of eye blinking Brain fog Sleep problems- this may tie into sleep apnea Neck and back pain Comorbidities of TMJ disorder include: Tourette’s,
Parkinson’s, essential tremors, Dystonia, TardiveDyskinesia
Otalgia- Ear Pain Tinnitus- Ringing or buzzing in the ears Inability to open your mouth wide Jaw Pain Jaw clenching/grinding Deviation on opening your mouth
This is why when your doctor examines you for TMJ disorder,
not only must he/she order a well done MRI, but he/she must
also do a thorough exam of the head and neck region.

Page 41
The MRI is sometimes not conclusive due to the patient
moving too much or there might be too much inflammation to
read the images, so treatment might have to be based on
symptoms alone.
Another major facet of diagnosis is the ability of the doctor to
both palpate distorted cranial bones and to see them as well
on the x-ray images. The reason for this is that if the cranial
bones are distorted, oftentimes this means that the joints are
distorted, and therefore the condyles are no longer seated into
level joints – this alone will wreak havoc with the discs as you
can well imagine!
Just think of it like trying to put two new tires on the front of
your car and ignoring that the front end alignment is way off-
your ride will be shaky in no time- just like the jaw bones are
jumping around in those twisted sockets- it simply doesn’t work!
And now just to throw a wrench into the whole thing, taking a
good MRI requires some skill and training. In most cases, I
have had to reject MRI’s done from other imaging centers,
other than the one that I know and approve of.

Page 42
And then we have the issue of reading the actual films, and
that takes some skill as well. Personally, I use Novant imaging
because they have a dedicated Tesla coil just for TMJ imaging.
My other advantage is that the former director of NIH radiology
reads for me- you can’t beat that kind of service! But even
within this group of radiologists that I work with , there is only
the one guy that I trust to read my images- his work is
exemplary- and I have found the other doctors in the same
group sometimes not as capable. So as you can see, it takes a
lot of training and a great radiologist to get good reports on the
MRI images. Even then, I sometimes question the reading of
the MRI- only because all I do is look at these things all day
long!
Admittedly, the field of TMJ and displaced discs is sorely
lacking in consistency and training. There are many doctors
out there who tout themselves as ‘experts’ in the field- hence
my sarcastic statement at the beginning of this chapter. In truth,
there is no specialty at all in TMJ disorders. There are also no
standards that a patient can count on when they see a TMJ
practitioner.

Page 43
For these reasons, many patients end up confused and even
scared as they hop around from one doctor to another. Until
such time as the schools, the dental societies, the ADA, etc.
get some cohesiveness going, patients will be at a loss for
direction.

Page 44
Part II: Treatment“As to methods there may be a million and thensome, but principles are few. The man who graspsprinciples can successfully select his own methods.The man who tries methods, ignoring principles, issure to have trouble.”
By Ralph Waldo Emerson

Page 45
Part III: CaseStudies and
Patient Stories“To study the phenomena of disease without booksis to sail an uncharted sea, while to study bookswithout patients is not to go to sea at all.“
ByWilliam Osler

Page 46
Part IV: Questionsand Answers“To be able to ask a question clearly is two-thirds ofthe way to getting it answered.”
By John Ruskin

Page 47
Part V: Resourcesand Bibliography
““Be sceptical, ask questions, demand proof.Demand evidence. Don't take anything for granted.But here's the thing: When you get proof, you needto accept the proof. And we're not that good atdoing that.”
By Michael Specter

Page 48
You have reached the end of this free sample of the book
“The Bio-Mechanical Treatment of Dystonia”.
To get more information or buy the whole book, please visit our
blog or become a member of the Bio-Mechanical Dystonia
Association.
New European AssociationBio-Mechanical DystoniaEmail: [email protected]
Web: www.biomechanical-dystonia.net