Best Treatment for Barrett's esophagus is Medical George Triadafilopoulos, MD Clinical Professor of...
31
Best Treatment for Barrett's esophagus is Medical George Triadafilopoulos, MD Clinical Professor of Medicine Stanford University School of Medicine M.I.S.S., Salt Lake City, UT, 2.23.2011
-
Upload
angel-fletcher -
Category
Documents
-
view
220 -
download
1
Transcript of Best Treatment for Barrett's esophagus is Medical George Triadafilopoulos, MD Clinical Professor of...

Best Treatment for Barrett's esophagus is Medical
George Triadafilopoulos, MDClinical Professor of Medicine
Stanford University School of Medicine
M.I.S.S., Salt Lake City, UT, 2.23.2011

Outline
• Why acid control is important
• What can we do
• How good are we

Effects of acid: In vitro studies

Acid pulses increase proliferation in Barrett’s esophagus
cpm/mg protein
1
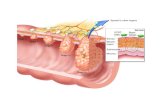
Esophagus
6 18 24
Time (hrs)
0
500
1000
1500
2000
2500
3000
*P<0.001;**P<0.05.
1
Barrett’s Esophagus
6 18 24
Time (hrs)
0
1000
2000
3000
4000
5000
1
Duodenum
6 18 24
Time (hrs)
0
500
1000
1500
2000
2500
3000
+ Acid – Acid
**
**
*
Fitzgerald, RC, et al, JCI 1996

PCNA expression before and after acid suppression+ in Barrett’s esophagus
Ouatu-Lascar et al. Gastro 1999
PCNA units
+Complete: %pH<4%
*

COX-2 expression in Barrett’s esophagus explants and the effect of acid and/or bile salt
exposure
Shirvani V, et al. Gastroenterol. 118: 487-496, 2000

COX-2 inhibition plus PPI decreases PCNA Expression in Barrett’s esophagus
**
*
E40 BID + ASA325
(n = 31)
E40 BID + R25
(n = 34)
E40 BID
(n = 30)
R25
(n = 36)
*P < .05 versus baseline.
*
*
*
Triadafilopoulos G et al. APT 2006

Acid
NOX5-S
ROS
p16 gene hypermethylation
Down-regulation of P16 mRNA
Increase in cell proliferation
Esophageal carcinogenesisHong et al. AJP, 2010

Hong et al. AJP, 2010
Acid-Induced P16 hypermethylation contributes to development of esophageal adenocarcinoma
via activation of NADPH oxidase NOX5-S
Ratioof p16to 18S

Hong et al. AJP, 2010
Acid increases methylation levels of p16 gene promoter in BAR-T cells and OE33 cells
Ratioand % control

2
Smith, et al. Annals of Surgery. 252(1):63-69, 2010.
Number of methylated genes in biopsies of squamous and columnar mucosa from pH normal and pH abnormal fundoplication subjects and no surgery subjects.
Effect of GERD control by fundoplication on aberrant DNA methylation in Barrett Esophagus.


PPI Therapy and Dysplasia
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0 1000 2000 3000 4000 5000 6000 7000
Days of Follow-Up
Dys
plas
ia R
ate
5 year 10 year H2RA/No Therapy
PPI Therapy
El-Serag, Am J Gastroenterol. 2004;99:1877.

Kaplan–Meier curves of the cumulative proportion of patients who were free of low-grade dysplasia (n = 299*)
Hillman L, et al. MJA 2004; 180 (8): 387-391

Conclusions
• In vitro and ex vivo data in cultured cells and Barrett’s esophagus explants suggest that acid exposure is important in Barrett’s carcinogenesis
• Normalization of intra-esophageal acid exposure -albeit not formally proven in RCT studies- should be beneficial and diminish the likelihood of neoplastic progression of Barrett’s esophagus


Treatment options for Barrett’s esophagus
•Control of GERD symtoms
•Healing of co-existing esophagitis
•Prevention of recurrent esophagitis
•Control of bile reflux
•Prevention of stricture formation
•Regression/elimination of Barrett’s surface
•Regression/elimination of dysplasia •Chemoprevention of dysplasia & adenocarcinoma
PPI Rx bid
PPI Rx bid
PPI Rx bid
Fundoplication
PPI/Fundoplication
Ablation + PPI
Ablation + PPI
PPI bid + ASA/COX-2


RFA+PPI versus surgery: Not directly comparable
• Symptoms
• Disease progression
• Disease regression
Time

Distinction• Where PPIs are only able to decrease acid content
in the stomach (and thus change the pH of the refluxate), surgery has the ability to prevent any type of reflux (i.e. bile).
• Fundoplication does not alter the length of Barrett’s esophagus
• In contrast, RFA ablates Barrett’s metaplasia, and, used together with PPI therapy that suppresses acid reflux, leads to squamous re-epitheliazation

Definitions• Progression: A change from either intestinal
metaplasia to any form of dysplasia or an increase in grade of dysplasia or development of adenocarcinoma
• Regression: A change from high-grade dysplasia (HGD) to low-grade dysplasia (LGD) or no dysplasia, change from LGD to metaplasia or loss of metaplasia, and change from IM to squamous epithelium
• Shortening of the segment or development of squamous cell islands, although considered by some as regression, usually is not accurately measured and reported

How good is fundoplication in patients with Barrett’s
esophagus? The LOTUS trial• 554 patients with GERD • 60 had Barrett’s esophagus: 28 randomized to
esomeprazole and 32 to LARS. • 4 of 60 BE patients on either treatment strategy
experienced treatment failure during the 3-year follow-up. • Esophageal pH in BE patients was significantly
better controlled after surgical treatment than after esomeprazole (p = 0.002)
• QoL scores were similar for the two therapies at baseline and at 3 years. Operative difficulty was slightly greater in patients with BE than those without
• There was no difference in postoperative complications or level of symptomatic reflux control
Atwood, SJ. J. Gastrointestinal Surg. 2008; 12:1646-54

Long-term outcomes of fundoplication in Barrett’s esophagus cohorts
%
Wassenaar EB et al WJG 2010
11 studies; N=551; f/u 3.4 years

Antireflux surgery (ARS) does not decrease cancer risk
SIR Lagergren; Gastro. 2010;138:1297–130115 year-long population study

Medical therapy vs surgery for Barrett’s esophagus
3 studies: PPI:708; Nissen 115
%
Wassenaar EB et al WJG 2010

Radiofrequency Ablation for Barrett’s Esophagus

Multi-center, randomized, sham-controlled study of radiofrequency ablation in patients with dysplastic Barrett’s esophagus
2:1 RFA versus shamStratified by:
- degree of dysplasia (LGD vs. HGD)- length of segment (1-4 cm vs 4-8 cm)
Maximum of 4 RFA sessionsIdentical biopsy protocols, equal samplingEsomeprazole 40 mg orallytwice daily 12 month cross-over
Shaheen N, et al. NEJM 2009

RCT of Barrett’s dysplasia: Complete Eradication (ITT)

RCT of Barrett’s dysplasia: Disease Progression

HALO: Long-term dataFleischer D et al. DDW 2010
• 50 patients followed for 5 years• No strictures or mucosal lesions.• Mean per pt # of biopsies: 31• In 46 of 50 patients (92%) had CR-IM, while 4 (8%)
had IM (6 out of 126 specimens).• Single-session focal RFA cleared residual IM
RFA is durable and effective at 5 years

Conclusions
• Although both regression and progression have been noted after ARS, surgery does not completely or substantially eliminate metaplasia
• Esophago-gastric cancer still develops after 15 years of ARS
• Medical therapy (RFA+PPI) is effective and durable but no data on cancer incidence are (yet) available.