Barretts Esophagus, Barrett's Esophagus Hiatal Hernia, Barrett's Esophagus Epithelium
Upload
meducationdotnetCategory
view
259download
0
Charlotte Patterson
The treatment and management of Barrett’s Oesophagus

Barrett’s Oesophagus Affects the distal oesophagus Consequence of chronic pathological reflux of the gastric
content Often asymptomatic, and found as a consequenece of
endoscopic investigation for other conditions.
Risk factor LiteratureGORD (Eisen et al.,
1997)Obesity (El-Serag et al.,
2006)Hiatial hernia (El-Serag et al.,
2006)Absence of H. pylori infection
(Goldblum et al., 1998)

PathophysiologyChronic exposure to gastric content leads
to intestinal metaplasia
Cellular & DNA damage alters the differentiation potential of proliferating epithelial cells.
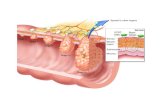
The metaplastic change is macroscopically visible using an endoscope.
Squamous epithelium Columnar epithelium(distal oesophagus) (gastric cardia, fundus, upper intestine)

Pathophysiology cont.Endoscopic changes in BO
Histological changes in BO

MOUTH
STOMACHOESOPHAGUS
DUODENUM
SQUAMOUS EPITHELIUM
COLUMNAR EPITHELIUM

Pathophysiology cont.The intestinal metaplasia may be classified
histologically as:Non-dysplasicLow grade dysplasia (LGD)High grade dysplasia (HGD)
In HGD, dysplastic cells are still confined by the basement membrane. However, due to the large numbers of dysplastic cells there is a high chance of subsequent invasion of the submucosa, and progression to adenocarcinoma.

Pathophysiology cont.

...So what?Individuals with this condition have a 30- to
50- fold increased risk of developing oesophageal cancer (adenocarcinoma). (O'Connor et al., 1999).
The 5 year survival rate with oesophageal cancer is 9% (Kumar & Clark, 2008).
... This makes oesophageal cancer one of the commonest causes of cancer related mortality.

Why diagnose Barrett’s?Part of the reason oesophageal cancer has such a high
mortality, is because 70% patients don’t present until the disease is stage III or higher (TMN classification system)
BO is one of the most important risk factors for oesophageal cancer
Therefore if BO is diagnosed and treated before it becomes dysplastic, could the oesophageal carcinoma associated mortality be reduced?
Staging of oesophageal cancer based on the TNM classification system
Stage of cancer Five year survival
I 80%
II 30%
III 18%
IV 4%

Treatment of Barrett’s?An American study in the 1990s by Cameron
et al. showed the prevalence of Barrett’s to be 0.5% on autopsy.
A more recent Sweedish study showed a prevalence of 1.6% in a cohort of 3000.
Prevalence of BO in patients with GORD is significantly higher- 8-20% in Western countries.
The risk of developing adenocarcinoma from BO is relatively low, at 0.5% per patient year.

Treatment of Barrett’s cont.Treatment of everyone with the condition
would be unfeasible, and place too greater strain financially on the NHS.
Treatment is invasive, and isn’t preferable to patients with asymptomatic Barrett’s.

Current managementNon-dysplastic Barrett’s
Endoscopic surveillance every 2-3 yearsLow-grade dysplasia
Endoscopic surveillance every 2-3 years6-28% risk of developing HGD
High-grade dysplasiaInvasive surgical or endoscopic treatment2.2-11.8% risk of developing adenocarcinoma
AdenocarcinomaInvasive surgical or endoscopic treatment

What is the treatment?SURGICAL
Total oesophagectomy and lymphadenectomy20% post-operative mortality85% 5 year mortality£25,000- before any post-operative complicationsTherefore this treatment is far from ideal...Could it be more successful if the disease was
treated when less dysplastic?o A very extreme treatment option for an
asymptomatic patient with LGD and only a 6-28% chance of developing HGD.
o Financial burden on NHS would increase

What is the treatment cont.ENDOSCOPIC
AblationDestroy the affected tissue, allowing it to be replaced with
the normal squamous epithelium of the oesophagus.However, no sample of the tissue is obtained therefore
infiltration depth of the lesion may be underestimated, and invasion of lymph nodes and blood vessels may not be identified
Therefore this shouldn’t be used as a stand-alone treatment for HGD or adenocarcinoma.
ResectionRemove the mucosa and submucosa, leaving the muscularis
propria exposed.Confirm that the cancerous tissue has margins within the
resected lesion.

Endoscopic resectionThis technique has been used with high success ratesSpecialist centre in Wiesbaden, Germany involving 144 patients
undergoing endoscopic resection for HGD showed a 99% remission rate in patients, with a 98% 5 year survival rate. (Pech et al. 2007).
However, this wasn’t an RCT- these patients were selected as they were considered ‘low-risk’ (ie. The cancer was limited to the mucosal layer).
Studies involving ‘higher-risk’ patients showed poorer results.Reoccurrence is quite frequent, estimated at around 11% (Peters
et al, 2006). However, if patients attend follow-up appointments, complications from this are minimised.
Is this only treating ‘the tip of the iceberg’? Leaving behind residual, potentially cancerous tissue? Could this compromise the long-term prognosis, and chances of actually ‘curing’ the cancer?
No, if used successfully like in Wiesbaden Germany.

Endoscopy vs surgery?At present, most centres in the UK offer oesophagectomy
as first-line treatment for HGD and adenocarcinoma.Endoscopic treatment is considered only if the patient is
considered un-fit for surgery, and as palliative treatment.There has yet to be an RCT comparing the two.However, study using a decision analysis model carried
out based on data from non-RCTs showed:Endoscopic was more effective and less expensive than surgical
treatment.The cost of endoscopic resection was $17,000 and 4.88 Quality
adjusted life years (QALY), compared with a cost of $28,000 and 4.59 QALY for oesophagectomy.
(Pohl et al, 2009)

In conclusion...There are two main ways of treating high-grade
dysplasia.OesophagectomyEndoscopic ablation or resection
Oesophagectomy is the treatment of choice in the UK, but it is expensive and has low success rates.
Endoscopic resection has been used successfully in specialist centres, such as Wiesbaden, Germany with excellent results.
If this technique can be used successfully in other countries, surely it is only a matter of time before this technique is used with similar success rates in the UK?

Thank you for listening!