Microscopic esophagitis and Barrett's esophagus: The histology report
12
Digestive and Liver Disease 43S (2011) S319–S330 Microscopic esophagitis and Barrett’s esophagus: The histology report Roberto Fiocca a, *, Luca Mastracci a , Massimo Milione b , Paola Parente c , Vincenzo Savarino d On behalf of the “Gruppo Italiano Patologi Apparato Digerente (GIPAD)” and of the “Società Italiana di Anatomia Patologica e Citopatologia Diagnostica”/International Academy of Pathology, Italian division (SIAPEC/IAP) a Department of Anatomic Pathology, University of Genova and S. Martino University Hospital, Genoa, Italy 2 Department of Anatomic Pathology B, IRCCS Istituto Nazionale Tumori, Milan, Italy c Istituto Oncologico Veneto (IOV-IRCCS), Padua, Italy d Department of Internal Medicine, University of Genoa, Genoa, Italy Abstract Gastro-esophageal reflux disease (GERD) is the most common digestive disease in industrialized countries (Europe and North America) and is associated with microscopic changes in the squamous epithelium. However, biopsy is not presently included in the routine diagnostic flow chart of GERD. In contrast, esophageal biopsy is mandatory when diagnosing Barrett’s esophagus. High quality histology reports are necessary to provide information on diagnosis and can also be important for research and epidemiological studies. It has been evident for decades that pathology reports vary between institutions and even within a single institution. Standardization of reporting is the best way to ensure that information necessary for patient management is included in pathology reports. This paper details the histological criteria for diagnosing GERD- associated microscopic esophagitis, other forms of esophagitis with specific features and columnar metaplasia in the lower esophagus (Barrett’s esophagus). It provides a detailed description of appropriate sampling criteria, individual lesions and how they contribute to the histology report. © 2011 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved. Keywords: Barrett’s esophagus; Esophagitis; Gastro-esophageal reflux disease; GIPAD report; Histopathology 1. Introduction Gastro-esophageal reflux disease (GERD) is extremely widespread in industrialized countries (Europe and North America) with a prevalence of 10–20% [1]. The prevalence of Barrett’s esophagus among patients undergoing endoscopic List of abbreviations: GERD, gastro-esophageal reflux disease; ERD, erosive reflux disease; NERD, non-erosive reflux disease; EE, eosinophilic esophagi- tis; DIS, dilated intercellular spaces; BE, Barrett’s esophagus; ESEM, en- doscopically suspected esophageal metaplasia; GEJ, gastro-esophageal junc- tion; SCJ, squamo-columnar junction or Z line; LSBE, long segment Bar- rett’s esophagus; SSBE, short segment Barrett’s esophagus. * Correspondence to: Roberto Fiocca, Department of Anatomic Pathology, University of Genova and S. Martino University Hospital, Via De Toni 14, 16132 Genova, Italy. Tel.: +39 010-3537806; fax: +39 010-3537803. E-mail address: fi[email protected] (R. Fiocca). 1590-8658/$ – see front matter © 2011 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved. examination is 1% and reaches 3% if only the patients with reflux symptoms are taken into account [2]. The modern approach to histological diagnosis of non- neoplastic diseases of the esophagus started with the advent of fiber optic endoscopy and the possibility of obtaining endoscopic biopsies. The first great contribution to a better understanding of microscopic lesions associated with gastro- esophageal reflux disease (GERD) came from Ismail-Beigi’s study [3], while the intricate story of Barrett’s esophagus (BE) began in 1950 [4]. The present document is an update to the “guidelines” issued by Gruppo Italiano Patologi dell’Apparato Digerente (GIPAD) in 1998 [5]) and it covers the following topics: 1. Indications for esophageal biopsy 2. Microscopic esophagitis • Individual histologic lesions
Transcript of Microscopic esophagitis and Barrett's esophagus: The histology report

Digestive and Liver Disease 43S (2011) S319–S330
Microscopic esophagitis and Barrett’s esophagus: The histology report
Roberto Fioccaa,*, Luca Mastracci a, Massimo Milioneb, Paola Parente c, Vincenzo Savarinod
On behalf of the “Gruppo Italiano Patologi Apparato Digerente (GIPAD)” and of the “Società Italianadi Anatomia Patologica e Citopatologia Diagnostica”/International Academy of Pathology,
Italian division (SIAPEC/IAP)aDepartment of Anatomic Pathology, University of Genova and S. Martino University Hospital, Genoa, Italy
2Department of Anatomic Pathology B, IRCCS Istituto Nazionale Tumori, Milan, ItalycIstituto Oncologico Veneto (IOV-IRCCS), Padua, Italy
dDepartment of Internal Medicine, University of Genoa, Genoa, Italy
Abstract
Gastro-esophageal reflux disease (GERD) is the most common digestive disease in industrialized countries (Europe and North America) andis associated with microscopic changes in the squamous epithelium. However, biopsy is not presently included in the routine diagnostic flowchart of GERD. In contrast, esophageal biopsy is mandatory when diagnosing Barrett’s esophagus. High quality histology reports are necessaryto provide information on diagnosis and can also be important for research and epidemiological studies. It has been evident for decades thatpathology reports vary between institutions and even within a single institution. Standardization of reporting is the best way to ensure thatinformation necessary for patient management is included in pathology reports. This paper details the histological criteria for diagnosing GERD-associated microscopic esophagitis, other forms of esophagitis with specific features and columnar metaplasia in the lower esophagus (Barrett’sesophagus). It provides a detailed description of appropriate sampling criteria, individual lesions and how they contribute to the histology report.© 2011 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
Keywords: Barrett’s esophagus; Esophagitis; Gastro-esophageal reflux disease; GIPAD report; Histopathology
1. Introduction
Gastro-esophageal reflux disease (GERD) is extremelywidespread in industrialized countries (Europe and NorthAmerica) with a prevalence of 10–20% [1]. The prevalenceof Barrett’s esophagus among patients undergoing endoscopic
List of abbreviations: GERD, gastro-esophageal reflux disease; ERD, erosivereflux disease; NERD, non-erosive reflux disease; EE, eosinophilic esophagi-tis; DIS, dilated intercellular spaces; BE, Barrett’s esophagus; ESEM, en-doscopically suspected esophageal metaplasia; GEJ, gastro-esophageal junc-tion; SCJ, squamo-columnar junction or Z line; LSBE, long segment Bar-rett’s esophagus; SSBE, short segment Barrett’s esophagus.* Correspondence to: Roberto Fiocca, Department of Anatomic Pathology,University of Genova and S. Martino University Hospital, Via De Toni 14,16132 Genova, Italy. Tel.: +39 010-3537806; fax: +39 010-3537803.
E-mail address: [email protected] (R. Fiocca).
1590-8658/$ – see front matter © 2011 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
examination is 1% and reaches 3% if only the patients withreflux symptoms are taken into account [2].
The modern approach to histological diagnosis of non-neoplastic diseases of the esophagus started with the adventof fiber optic endoscopy and the possibility of obtainingendoscopic biopsies. The first great contribution to a betterunderstanding of microscopic lesions associated with gastro-esophageal reflux disease (GERD) came from Ismail-Beigi’sstudy [3], while the intricate story of Barrett’s esophagus (BE)began in 1950 [4].
The present document is an update to the “guidelines”issued by Gruppo Italiano Patologi dell’Apparato Digerente(GIPAD) in 1998 [5]) and it covers the following topics:1. Indications for esophageal biopsy2. Microscopic esophagitis
• Individual histologic lesions
S320 R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330
• Histologic pattern of microscopic esophagitis• Histologic lesions associated with other esophagitis
(eosinophilic, infectious, non infectious)3. Barrett’s esophagus
• Definition• Endoscopic description and biopsy sampling• Individual histologic lesionsThe asterisks in the present article express the levels of
evidence, where one asterisk represents level 1 (evidenceprovided by single studies); two asterisks represent level2 (evidence provided by some clinico-pathological studies,albeit with some notable discrepancies); and three asterisksrepresent level 3 (evidence consistently estabilished by a largebody of clinico-pathological and/or follow-up studies), as de-scribed more in detail in the Foreword in this supplement [6].
2. Clinical indication for esophageal biopsy
2.1. Gastro-esophageal reflux disease
There are no indications for routine esophageal biopsiesin patients with esophageal or extra-esophageal symptoms ofgastro-esophageal reflux disease [7]. The rationale underlyingthis statement is that histological findings do not seem to pro-vide any additional information for patient management whencompared with endoscopy. In other words, it is sufficient todistinguish erosive lesions of any degree by endoscopy (ERD)from non erosive form (NERD) in the absence of endoscop-ically recognizable lesions. Squamous epithelium histologycan provide a better understanding of reflux disease at themucosal level** [8] and enable comparative assessment of theeffect of anti-reflux treatments** [9]. Biopsy contribution issignificant for research purposes only, and presently it is notincluded in the routine diagnostic flow chart for GERD.
2.2. Barrett’s esophagus
Esophageal biopsy is crucial when diagnosing Barrett’sesophagus*** and for monitoring purposes after diagnosis.Columnar metaplasia [10] of the esophageal mucosa has tobe histologically proven in order to correctly define thiscomplication of GERD***.
2.3. Endoscopically suspected esophageal lesions
Esophageal biopsy is mandatory in all suspected lesionsthat are not clearly defined during endoscopy. Histologicalexamination is required whenever an endoscopic finding atany level along the esophagus raises doubts concerning thenature of the lesion (benign vs. malignant) [11].
2.4. Eosinophilic esophagitis
Histology is mandatory in this condition. High eosinophilcount (≥15/HPF) is required for the diagnosis of eosinophilicesophagitis in patients with dysphagia and atopy*** [12].
Biopsy specimens must be taken also from the proximal ormiddle esophagus.
2.5. Infectious esophagitis
Biopsy is required in order to differentiate with certaintyviral or bacterial esophagitis from other types of esophagitis,although this is a relatively rare occurrence in clinical practice.
2.6. Clinical information
As in other digestive diseases, the following informationshould be provided when requiring a histological examination:• reason for the examination;• concomitant diseases (e.g. connective tissue diseases, skin
diseases, allergies, etc.);• endoscopic pattern;• previous and current treatments;• biopsy site;• previous histological examinations.
A list of all useful clinical and endoscopic data would betoo long and beyond the scope of this paper. The importanceof endoscopic-bioptic correlations in the diagnosis of Barrett’sesophagus is covered in a subsequent section of this paper.
2.7. Normal esophageal mucosa (Table 1)
The esophageal mucosa is lined by stratified squamousepithelium. Sparse T lymphocytes (usually <10/HPF) in thesuprabasal area, sparse Langerhans cells and very few mastcells [13] are constitutively present in normal esophagealepithelium. In contrast, no eosinophils or neutrophils arefound. Esophageal biopsy specimens should include the fullepithelial thickness, allow the recognition of the base ofpapillae and be well oriented.
3. Microscopic esophagitis
3.1. Definition
The term “microscopic esophagitis” refers to a group ofhistologic lesions observed in most patients with GERD,both erosive (ERD) and non-erosive (NERD). It is not to beconfused with “esophagitis”, a term that in the gastroentero-logical literature designates endoscopically detectable erosivelesions.
Table 1Criteria for normal esophageal mucosa***
• Basal layer thickness: <20% (at the Z line); <15% (in more proximalbiopsies)†
• Papillary length: <66% (at the Z line); <50% (in more proximalbiopsies)†
• Intraepithelial T lymphocytes: <10/HPF• Absence of intercellular spaces dilation• Absence of intraepithelial eosinophils and neutrophils
†Figures refer to the full thickness of the epithelium.
R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330 S321
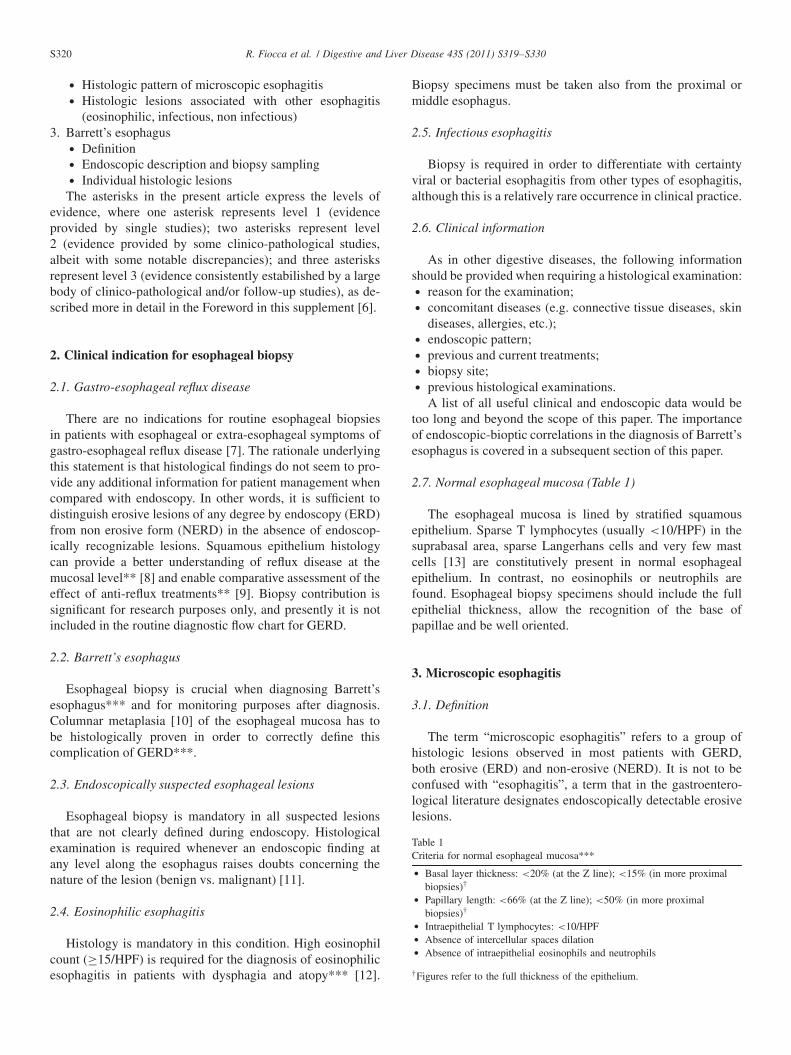
Fig. 1. Mild hyperplasia of the basal layer (<30%) in biopsy performed at 2cm from the Z line. (H-E, 20×)
3.2. Individual histologic lesions
None of the histologic lesions characterizing microscopicesophagitis is specific of and exclusive to reflux disease;the same lesions can be observed also in other types ofesophagitis (infectious, eosinophilic, due to achalasia, etc.).
The assessment of histologic lesions should be performedin well oriented areas of biopsy specimens where lesions aremost severe.
Basal cell hyperplasia*** – thickness of basal layer ≥20%(esophageal side of Z line)* [14] of total epithelial thickness;≥15% (biopsies proximal to Z line)*** [3]. The upper limitof the basal layer is defined as the level where the nuclei ofepithelial cells are separated by a distance greater than theirdiameter [15] (Fig. 1). Basal cell hyperplasia can be graded asmild (<30%) or marked (≥30%).
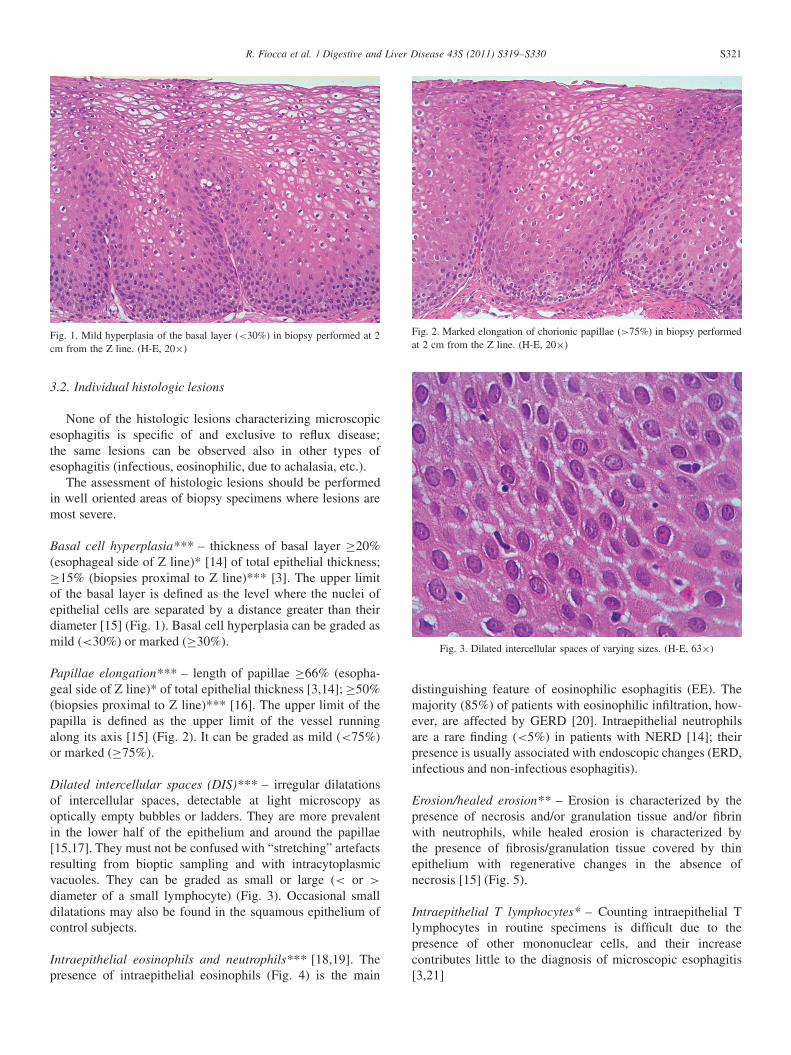
Papillae elongation*** – length of papillae ≥66% (esopha-geal side of Z line)* of total epithelial thickness [3,14]; ≥50%(biopsies proximal to Z line)*** [16]. The upper limit of thepapilla is defined as the upper limit of the vessel runningalong its axis [15] (Fig. 2). It can be graded as mild (<75%)or marked (≥75%).
Dilated intercellular spaces (DIS)*** – irregular dilatationsof intercellular spaces, detectable at light microscopy asoptically empty bubbles or ladders. They are more prevalentin the lower half of the epithelium and around the papillae[15,17]. They must not be confused with “stretching” artefactsresulting from bioptic sampling and with intracytoplasmicvacuoles. They can be graded as small or large (< or >
diameter of a small lymphocyte) (Fig. 3). Occasional smalldilatations may also be found in the squamous epithelium ofcontrol subjects.
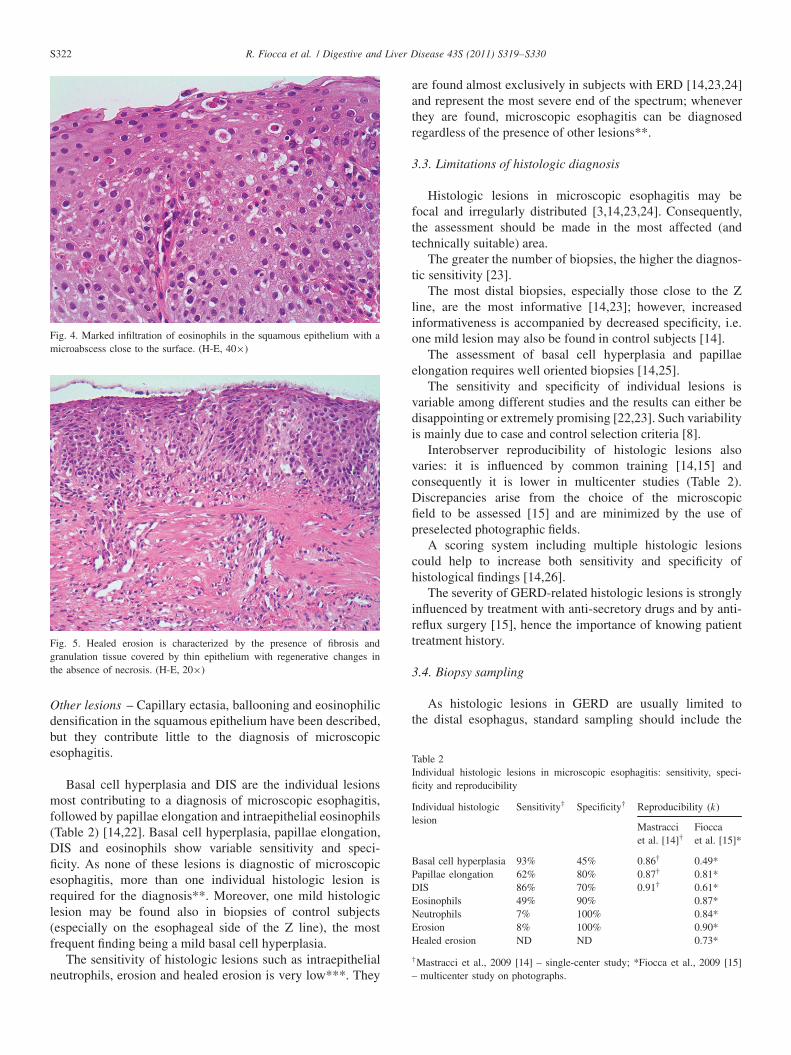
Intraepithelial eosinophils and neutrophils*** [18,19]. Thepresence of intraepithelial eosinophils (Fig. 4) is the main
Fig. 2. Marked elongation of chorionic papillae (>75%) in biopsy performedat 2 cm from the Z line. (H-E, 20×)
Fig. 3. Dilated intercellular spaces of varying sizes. (H-E, 63×)
distinguishing feature of eosinophilic esophagitis (EE). Themajority (85%) of patients with eosinophilic infiltration, how-ever, are affected by GERD [20]. Intraepithelial neutrophilsare a rare finding (<5%) in patients with NERD [14]; theirpresence is usually associated with endoscopic changes (ERD,infectious and non-infectious esophagitis).
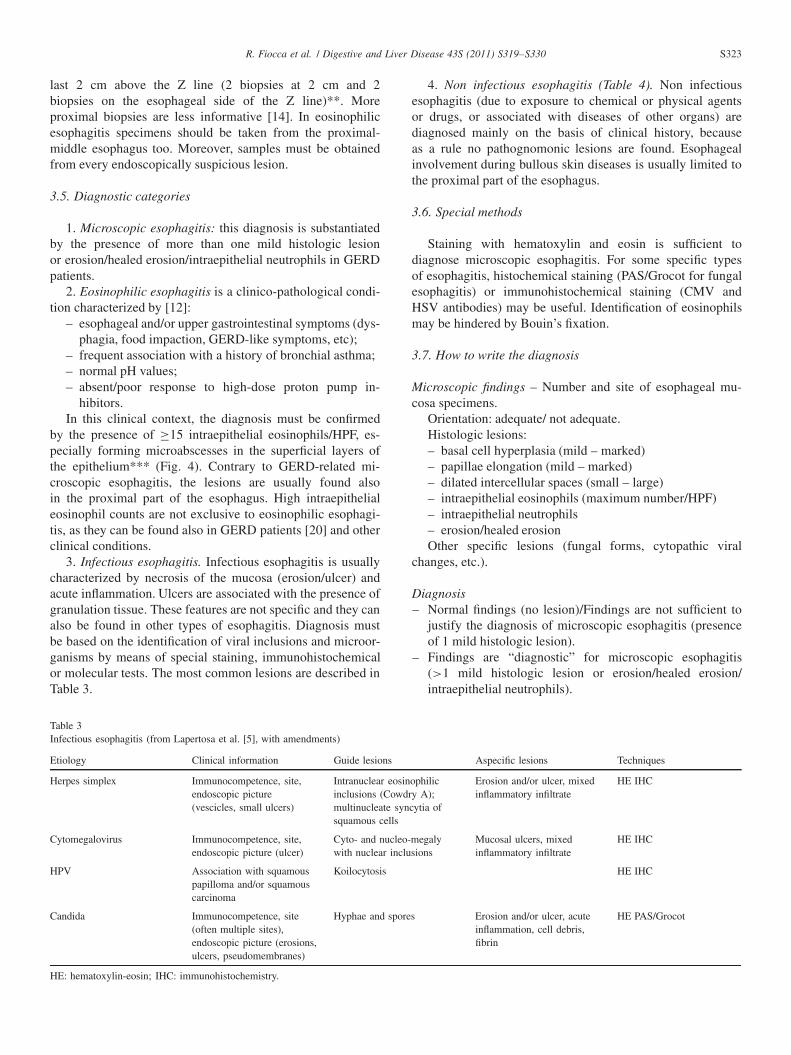
Erosion/healed erosion** – Erosion is characterized by thepresence of necrosis and/or granulation tissue and/or fibrinwith neutrophils, while healed erosion is characterized bythe presence of fibrosis/granulation tissue covered by thinepithelium with regenerative changes in the absence ofnecrosis [15] (Fig. 5).
Intraepithelial T lymphocytes* – Counting intraepithelial Tlymphocytes in routine specimens is difficult due to thepresence of other mononuclear cells, and their increasecontributes little to the diagnosis of microscopic esophagitis[3,21]
S322 R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330
Fig. 4. Marked infiltration of eosinophils in the squamous epithelium with amicroabscess close to the surface. (H-E, 40×)
Fig. 5. Healed erosion is characterized by the presence of fibrosis andgranulation tissue covered by thin epithelium with regenerative changes inthe absence of necrosis. (H-E, 20×)
Other lesions – Capillary ectasia, ballooning and eosinophilicdensification in the squamous epithelium have been described,but they contribute little to the diagnosis of microscopicesophagitis.
Basal cell hyperplasia and DIS are the individual lesionsmost contributing to a diagnosis of microscopic esophagitis,followed by papillae elongation and intraepithelial eosinophils(Table 2) [14,22]. Basal cell hyperplasia, papillae elongation,DIS and eosinophils show variable sensitivity and speci-ficity. As none of these lesions is diagnostic of microscopicesophagitis, more than one individual histologic lesion isrequired for the diagnosis**. Moreover, one mild histologiclesion may be found also in biopsies of control subjects(especially on the esophageal side of the Z line), the mostfrequent finding being a mild basal cell hyperplasia.
The sensitivity of histologic lesions such as intraepithelialneutrophils, erosion and healed erosion is very low***. They
are found almost exclusively in subjects with ERD [14,23,24]and represent the most severe end of the spectrum; wheneverthey are found, microscopic esophagitis can be diagnosedregardless of the presence of other lesions**.
3.3. Limitations of histologic diagnosis
Histologic lesions in microscopic esophagitis may befocal and irregularly distributed [3,14,23,24]. Consequently,the assessment should be made in the most affected (andtechnically suitable) area.
The greater the number of biopsies, the higher the diagnos-tic sensitivity [23].
The most distal biopsies, especially those close to the Zline, are the most informative [14,23]; however, increasedinformativeness is accompanied by decreased specificity, i.e.one mild lesion may also be found in control subjects [14].
The assessment of basal cell hyperplasia and papillaeelongation requires well oriented biopsies [14,25].
The sensitivity and specificity of individual lesions isvariable among different studies and the results can either bedisappointing or extremely promising [22,23]. Such variabilityis mainly due to case and control selection criteria [8].
Interobserver reproducibility of histologic lesions alsovaries: it is influenced by common training [14,15] andconsequently it is lower in multicenter studies (Table 2).Discrepancies arise from the choice of the microscopicfield to be assessed [15] and are minimized by the use ofpreselected photographic fields.
A scoring system including multiple histologic lesionscould help to increase both sensitivity and specificity ofhistological findings [14,26].
The severity of GERD-related histologic lesions is stronglyinfluenced by treatment with anti-secretory drugs and by anti-reflux surgery [15], hence the importance of knowing patienttreatment history.
3.4. Biopsy sampling
As histologic lesions in GERD are usually limited tothe distal esophagus, standard sampling should include the
Table 2Individual histologic lesions in microscopic esophagitis: sensitivity, speci-ficity and reproducibility
Individual histologic Sensitivity† Specificity† Reproducibility (k)lesion
Mastracci Fioccaet al. [14]† et al. [15]*
Basal cell hyperplasia 93% 45% 0.86† 0.49*Papillae elongation 62% 80% 0.87† 0.81*DIS 86% 70% 0.91† 0.61*Eosinophils 49% 90% 0.87*Neutrophils 7% 100% 0.84*Erosion 8% 100% 0.90*Healed erosion ND ND 0.73*
†Mastracci et al., 2009 [14] – single-center study; *Fiocca et al., 2009 [15]– multicenter study on photographs.
R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330 S323
last 2 cm above the Z line (2 biopsies at 2 cm and 2biopsies on the esophageal side of the Z line)**. Moreproximal biopsies are less informative [14]. In eosinophilicesophagitis specimens should be taken from the proximal-middle esophagus too. Moreover, samples must be obtainedfrom every endoscopically suspicious lesion.
3.5. Diagnostic categories
1. Microscopic esophagitis: this diagnosis is substantiatedby the presence of more than one mild histologic lesionor erosion/healed erosion/intraepithelial neutrophils in GERDpatients.
2. Eosinophilic esophagitis is a clinico-pathological condi-tion characterized by [12]:
– esophageal and/or upper gastrointestinal symptoms (dys-phagia, food impaction, GERD-like symptoms, etc);
– frequent association with a history of bronchial asthma;– normal pH values;– absent/poor response to high-dose proton pump in-
hibitors.In this clinical context, the diagnosis must be confirmed
by the presence of ≥15 intraepithelial eosinophils/HPF, es-pecially forming microabscesses in the superficial layers ofthe epithelium*** (Fig. 4). Contrary to GERD-related mi-croscopic esophagitis, the lesions are usually found alsoin the proximal part of the esophagus. High intraepithelialeosinophil counts are not exclusive to eosinophilic esophagi-tis, as they can be found also in GERD patients [20] and otherclinical conditions.
3. Infectious esophagitis. Infectious esophagitis is usuallycharacterized by necrosis of the mucosa (erosion/ulcer) andacute inflammation. Ulcers are associated with the presence ofgranulation tissue. These features are not specific and they canalso be found in other types of esophagitis. Diagnosis mustbe based on the identification of viral inclusions and microor-ganisms by means of special staining, immunohistochemicalor molecular tests. The most common lesions are described inTable 3.
Table 3Infectious esophagitis (from Lapertosa et al. [5], with amendments)
Etiology Clinical information Guide lesions Aspecific lesions Techniques
Herpes simplex Immunocompetence, site,endoscopic picture(vescicles, small ulcers)
Intranuclear eosinophilicinclusions (Cowdry A);multinucleate syncytia ofsquamous cells
Erosion and/or ulcer, mixedinflammatory infiltrate
HE IHC
Cytomegalovirus Immunocompetence, site,endoscopic picture (ulcer)
Cyto- and nucleo-megalywith nuclear inclusions
Mucosal ulcers, mixedinflammatory infiltrate
HE IHC
HPV Association with squamouspapilloma and/or squamouscarcinoma
Koilocytosis HE IHC
Candida Immunocompetence, site(often multiple sites),endoscopic picture (erosions,ulcers, pseudomembranes)
Hyphae and spores Erosion and/or ulcer, acuteinflammation, cell debris,fibrin
HE PAS/Grocot
HE: hematoxylin-eosin; IHC: immunohistochemistry.
4. Non infectious esophagitis (Table 4). Non infectiousesophagitis (due to exposure to chemical or physical agentsor drugs, or associated with diseases of other organs) arediagnosed mainly on the basis of clinical history, becauseas a rule no pathognomonic lesions are found. Esophagealinvolvement during bullous skin diseases is usually limited tothe proximal part of the esophagus.
3.6. Special methods
Staining with hematoxylin and eosin is sufficient todiagnose microscopic esophagitis. For some specific typesof esophagitis, histochemical staining (PAS/Grocot for fungalesophagitis) or immunohistochemical staining (CMV andHSV antibodies) may be useful. Identification of eosinophilsmay be hindered by Bouin’s fixation.
3.7. How to write the diagnosis
Microscopic findings – Number and site of esophageal mu-cosa specimens.
Orientation: adequate/ not adequate.Histologic lesions:– basal cell hyperplasia (mild – marked)– papillae elongation (mild – marked)– dilated intercellular spaces (small – large)– intraepithelial eosinophils (maximum number/HPF)– intraepithelial neutrophils– erosion/healed erosionOther specific lesions (fungal forms, cytopathic viral
changes, etc.).
Diagnosis– Normal findings (no lesion)/Findings are not sufficient to
justify the diagnosis of microscopic esophagitis (presenceof 1 mild histologic lesion).
– Findings are “diagnostic” for microscopic esophagitis(>1 mild histologic lesion or erosion/healed erosion/intraepithelial neutrophils).
S324 R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330
Table 4Non-infectious esophagitis (from Lapertosa et al. [5], with amendments)
Etiology Clinical information Guide lesions Aspecific lesions Techniques
Pill esophagitis Drug treatment NSAIDs,antibiotics, AZT, potassiumchloride, etc.)Site: often at the level ofanatomical strictureType of lesion: ulcer
Erosion, ulcer, acuteinflammation, granulationtissue
HE
Corrosive esophagitis Ingestion of causticsubstances (accidental,suicidal)
Diffuse necrosis HE
Radiation esophagitis Clinical history of radiationtherapy
Cell atypia, vascular changes Ulcer, edema, fibrosis HE
Chemotherapy esophagitis Clinical history ofchemotherapy
Epithelial nuclear atypia,necrosis, granulation tissue
HE
Esophagitis in Crohn’sdisease
Enteric symptoms,topography of lesion (focalulcers)
Focal inflammation,granulomas
Ulcer HE
Esophagitis in connectivetissue disease
Clinical history Microscopic esophagitis-likelesions
HE
Skin diseases Pemphigus vulgaris Intraepithelial bullae,acantholysis, lymphocytesand eosinophils
IF (IgG and C3 deposits inintercellular spaces)
Hailey-Hailey disease Suprabasal bulla HEBullous pemphigoid Subepithelial bulla, mild
inflammationIF (IgG deposits in basalmembrane)
Lichen planus Vacuolization in the basalarea, lymphocytic infiltration
HE
HE: hematoxylin-eosin; IF: immunofluorescence.
– Findings are “suggestive” of eosinophilic esophagitis (≥15eosinophils/HPF, with unknown clinical context) or “diag-nostic” for eosinophilic esophagitis (≥15 eosinophils/HPFin a coherent clinical context).
– Findings are “diagnostic” for specific esophagitis (Candida,CMV, Herpes).
4. Barrett’s esophagus
4.1. Definition
Barrett’s esophagus (BE) is defined as columnar metaplasiaof the distal esophagus, is caused by chronic GERD andrepresents a risk factor for esophageal adenocarcinoma [27].
Two types of columnar epithelium may replace esophagealstratified squamous epithelium*** [10]:1. intestinal-type epithelium2. cardia-type epithelium.
This definition is the result of several reassessments ofhistologic and endoscopical criteria that have led to differentdefinitions of BE over time [10,28,29]. Therefore, the adopteddefinition of BE is based on the current literature and reflectsthe viewpoint of the authors of this article; however, advancesin our understanding of BE may be expected in the nearfuture.
The original description also included a fundic type of
Barrett’s esophagus [28]. However, when oxyntic mucosa isfound in the distal esophagus, it is generally a sign of hiatushernia, whereas it represents ectopia (the so-called “inletpatches”) when found in the mid-proximal esophagus.
4.2. The border area
Even though the “anatomical” gastro-esophageal junction(GEJ) has been variously defined, a recent consensus paper[30] identifies it with the “proximal border of the gastricfolds” when endoscopy is performed with minimal air in-sufflation (Fig. 6A). The “histological” squamo-columnarjunction (SCJ) or Z line is the transition between esophagealsquamous epithelium and the glandular epithelium of thestomach (cardia mucosa): it can be detected endoscopicallydue to the colour change (white vs. pinkish). As a rule, thetwo junctions overlap, but SCJ may be located up to >1 cmproximally to GEJ also in normal subjects [31].
4.3. Endoscopic description
According to the Montreal classification [10], the termESEM (Endoscopically Suspected Esophageal Metaplasia)designates the presence of “salmon pink” mucosa in the distalesophagus at endoscopy: it describes suspected columnarmetaplasia (in the tubular esophagus), to be confirmed byhistology***.
R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330 S325
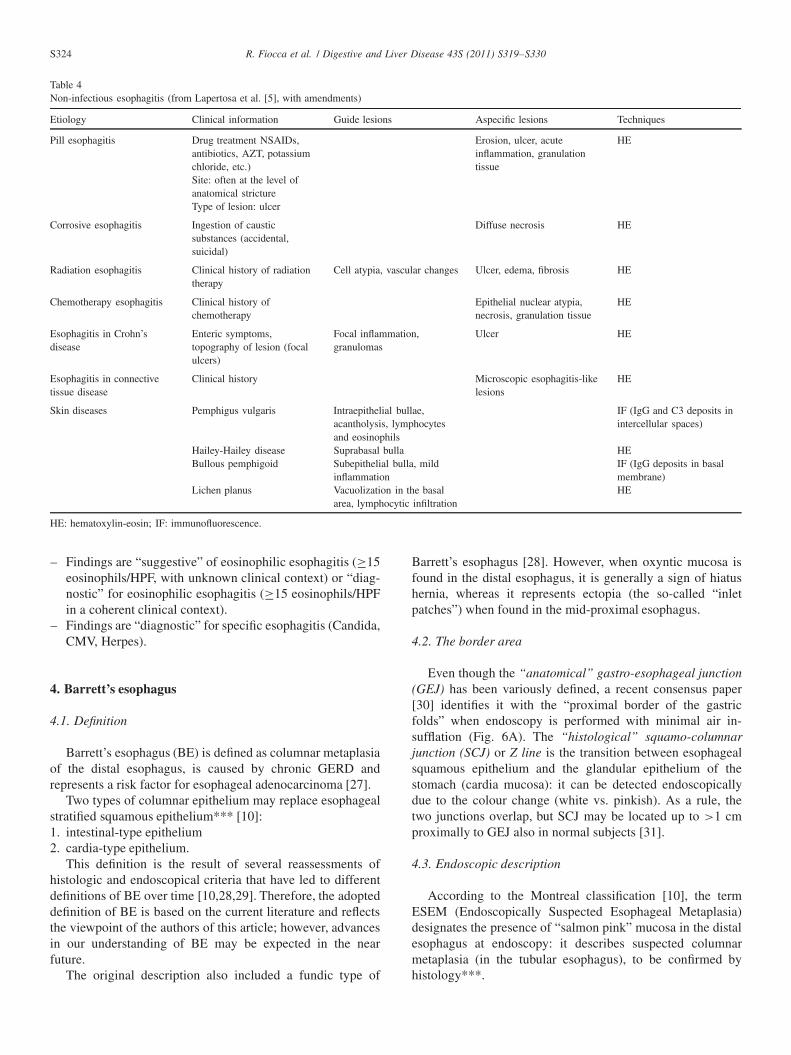
Fig. 6. The anatomic gastric-esophageal junction (proximal limit of gastric folds [white line]) usually coincides with the squamous-columnar junction (blue line= SCJ) (A). In Barrett’s esophagus (an example of long segment is shown) SCJ is located more proximally: distance between white and blue lines = 6.5 cm (i.e.long Barrett segment) (B). According to the Prague criteria, the values of C (= 5 cm) & M (= 6.5 cm) are provided.
Endoscopic diagnosis is carried out in three steps [30]:1. identification of the anatomical gastro-esophageal junction
(GEJ);2. detection of the squamo-columnar junction (SCJ or Z line);3. measurement of columnar segment.
The “C&M” criteria of the Prague classification [30]provide clear rules for reporting endoscopic description andextent of ESEM.
ESEM is measured by two descriptors expressed in cmfrom GEJ (Fig. 6B):– C: circumferential extent– M: maximal extent
Endoscopic findings measured in this way can be classifiedinto three categories:– LSBE: Long Segment Barrett’s Esophagus, ≥3 cm;– SSBE: Short Segment Barrett’s Esophagus, <3 cm;– irregular SCJ/Z line: irregular SCJ <1–0.5 cm (which does
not define ESEM with certainty).The “C&M” criteria have proved to be highly reliable
and reproducible (>90%) both in GEJ detection and indefining SSBE and LSBE. On the other hand irregular Z line(or “ultra short” BE), deals with a heterogeneous group ofendoscopic patterns including SSBE with M <1 cm which ischaracterized by low reproducibility [30,32,33].
LSBE and SSBE share the same epidemiology and likelyrepresent two phases of the same process [27]. The lengthof the metaplastic segment and the presence of intestinalmetaplasia are currently considered major risk factors foradenocarcinoma [34,35].
4.4. Biopsy sampling
Multiple biopsies are required in order to characterizeESEM, their number being correlated to ESEM length [39]:8 biopsies in the metaplastic segment allow detection ofintestinal epithelium in 68% of cases [40], but if biopsies are
performed close to squamo-columnar junction, the percentagerises to 94% even with fewer samples [41]. In patients beingfollowed up for BE, biopsies are recommended in the 4 quad-rants of the distal esophagus (every 2 cm routinely and every 1cm in case of dysplasia [42,43]: unfortunately this sampling isnot frequently performed in routine practice. The widespreadavailability of new advanced endoscopic techniques (narrowband imaging and magnification chromoendoscopy) is ex-pected to increase the detection of dysplasia through a bettertargeting of bioptic sampling.
4.5. Individual histologic lesions
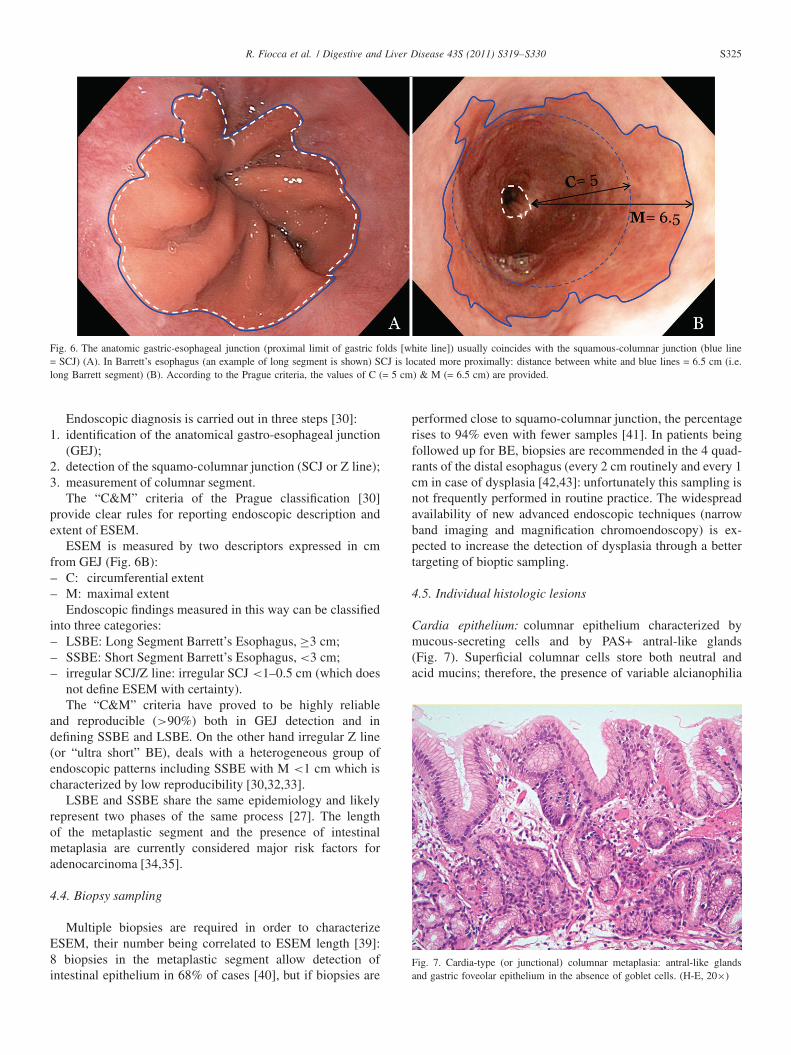
Cardia epithelium: columnar epithelium characterized bymucous-secreting cells and by PAS+ antral-like glands(Fig. 7). Superficial columnar cells store both neutral andacid mucins; therefore, the presence of variable alcianophilia
Fig. 7. Cardia-type (or junctional) columnar metaplasia: antral-like glandsand gastric foveolar epithelium in the absence of goblet cells. (H-E, 20×)
S326 R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330
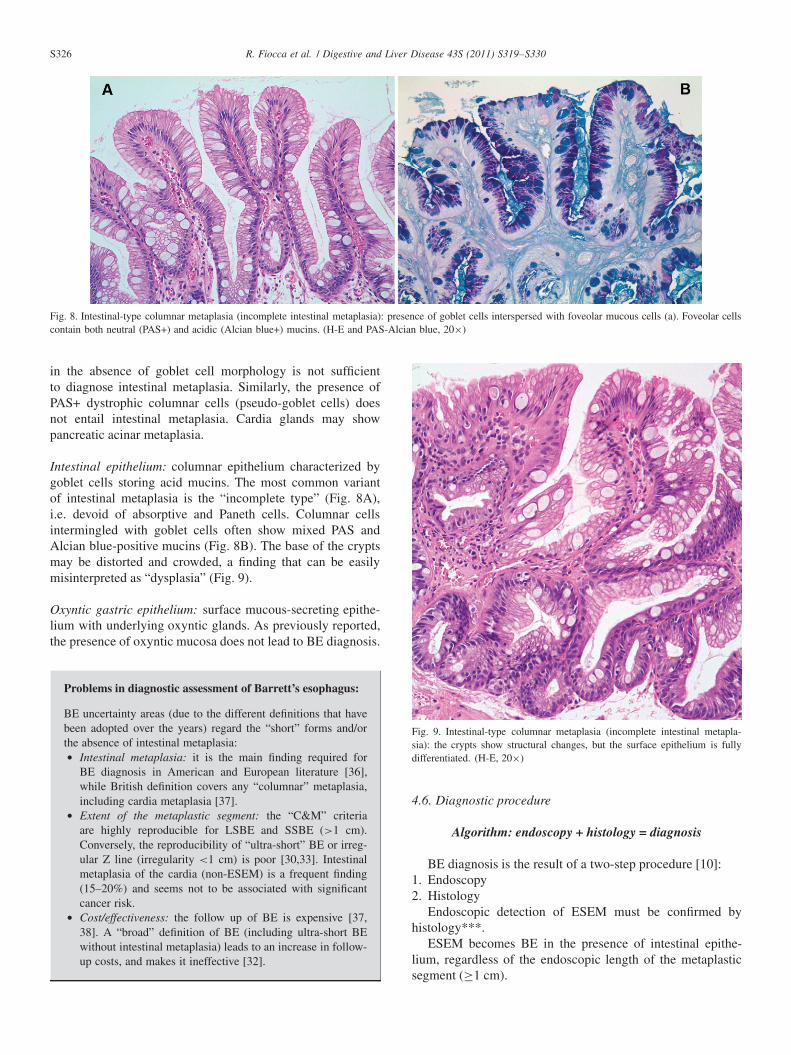
Fig. 8. Intestinal-type columnar metaplasia (incomplete intestinal metaplasia): presence of goblet cells interspersed with foveolar mucous cells (a). Foveolar cellscontain both neutral (PAS+) and acidic (Alcian blue+) mucins. (H-E and PAS-Alcian blue, 20×)
in the absence of goblet cell morphology is not sufficientto diagnose intestinal metaplasia. Similarly, the presence ofPAS+ dystrophic columnar cells (pseudo-goblet cells) doesnot entail intestinal metaplasia. Cardia glands may showpancreatic acinar metaplasia.
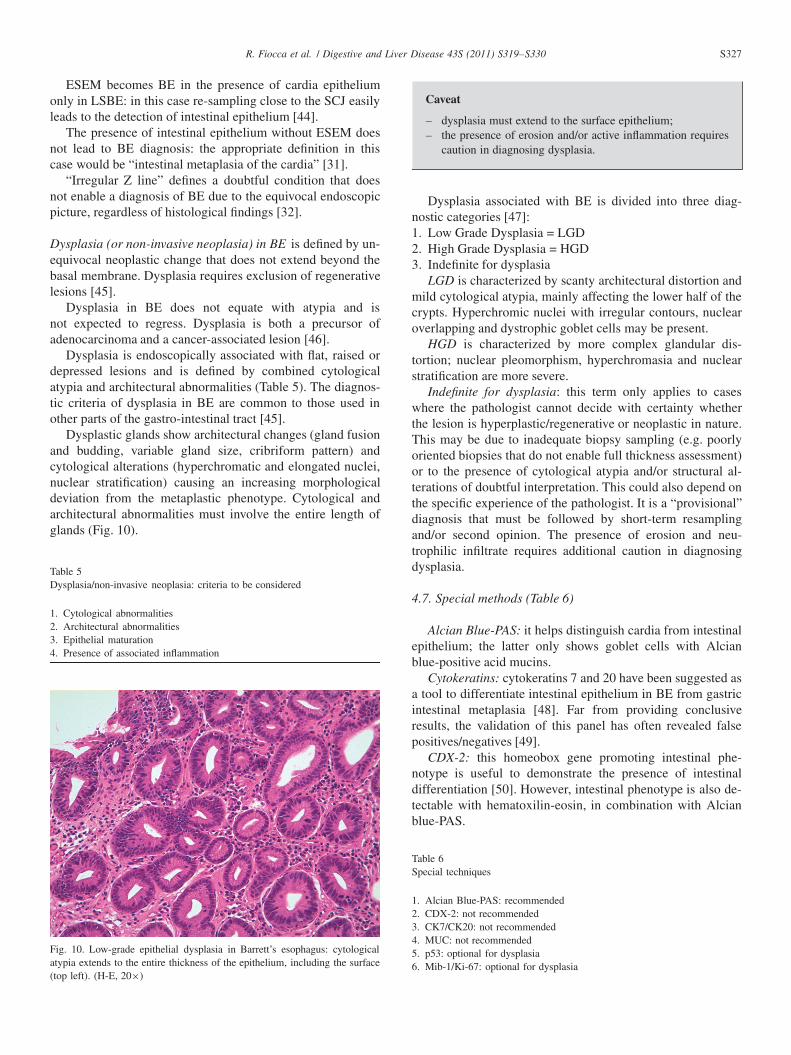
Intestinal epithelium: columnar epithelium characterized bygoblet cells storing acid mucins. The most common variantof intestinal metaplasia is the “incomplete type” (Fig. 8A),i.e. devoid of absorptive and Paneth cells. Columnar cellsintermingled with goblet cells often show mixed PAS andAlcian blue-positive mucins (Fig. 8B). The base of the cryptsmay be distorted and crowded, a finding that can be easilymisinterpreted as “dysplasia” (Fig. 9).
Oxyntic gastric epithelium: surface mucous-secreting epithe-lium with underlying oxyntic glands. As previously reported,the presence of oxyntic mucosa does not lead to BE diagnosis.
Problems in diagnostic assessment of Barrett’s esophagus:
BE uncertainty areas (due to the different definitions that havebeen adopted over the years) regard the “short” forms and/orthe absence of intestinal metaplasia:• Intestinal metaplasia: it is the main finding required for
BE diagnosis in American and European literature [36],while British definition covers any “columnar” metaplasia,including cardia metaplasia [37].
• Extent of the metaplastic segment: the “C&M” criteriaare highly reproducible for LSBE and SSBE (>1 cm).Conversely, the reproducibility of “ultra-short” BE or irreg-ular Z line (irregularity <1 cm) is poor [30,33]. Intestinalmetaplasia of the cardia (non-ESEM) is a frequent finding(15–20%) and seems not to be associated with significantcancer risk.
• Cost/effectiveness: the follow up of BE is expensive [37,38]. A “broad” definition of BE (including ultra-short BEwithout intestinal metaplasia) leads to an increase in follow-up costs, and makes it ineffective [32].
Fig. 9. Intestinal-type columnar metaplasia (incomplete intestinal metapla-sia): the crypts show structural changes, but the surface epithelium is fullydifferentiated. (H-E, 20×)
4.6. Diagnostic procedure
Algorithm: endoscopy + histology = diagnosis
BE diagnosis is the result of a two-step procedure [10]:1. Endoscopy2. Histology
Endoscopic detection of ESEM must be confirmed byhistology***.
ESEM becomes BE in the presence of intestinal epithe-lium, regardless of the endoscopic length of the metaplasticsegment (≥1 cm).
R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330 S327
ESEM becomes BE in the presence of cardia epitheliumonly in LSBE: in this case re-sampling close to the SCJ easilyleads to the detection of intestinal epithelium [44].
The presence of intestinal epithelium without ESEM doesnot lead to BE diagnosis: the appropriate definition in thiscase would be “intestinal metaplasia of the cardia” [31].
“Irregular Z line” defines a doubtful condition that doesnot enable a diagnosis of BE due to the equivocal endoscopicpicture, regardless of histological findings [32].
Dysplasia (or non-invasive neoplasia) in BE is defined by un-equivocal neoplastic change that does not extend beyond thebasal membrane. Dysplasia requires exclusion of regenerativelesions [45].
Dysplasia in BE does not equate with atypia and isnot expected to regress. Dysplasia is both a precursor ofadenocarcinoma and a cancer-associated lesion [46].
Dysplasia is endoscopically associated with flat, raised ordepressed lesions and is defined by combined cytologicalatypia and architectural abnormalities (Table 5). The diagnos-tic criteria of dysplasia in BE are common to those used inother parts of the gastro-intestinal tract [45].
Dysplastic glands show architectural changes (gland fusionand budding, variable gland size, cribriform pattern) andcytological alterations (hyperchromatic and elongated nuclei,nuclear stratification) causing an increasing morphologicaldeviation from the metaplastic phenotype. Cytological andarchitectural abnormalities must involve the entire length ofglands (Fig. 10).
Table 5Dysplasia/non-invasive neoplasia: criteria to be considered
1. Cytological abnormalities2. Architectural abnormalities3. Epithelial maturation4. Presence of associated inflammation
Fig. 10. Low-grade epithelial dysplasia in Barrett’s esophagus: cytologicalatypia extends to the entire thickness of the epithelium, including the surface(top left). (H-E, 20×)
Caveat
– dysplasia must extend to the surface epithelium;– the presence of erosion and/or active inflammation requires
caution in diagnosing dysplasia.
Dysplasia associated with BE is divided into three diag-nostic categories [47]:1. Low Grade Dysplasia = LGD2. High Grade Dysplasia = HGD3. Indefinite for dysplasia
LGD is characterized by scanty architectural distortion andmild cytological atypia, mainly affecting the lower half of thecrypts. Hyperchromic nuclei with irregular contours, nuclearoverlapping and dystrophic goblet cells may be present.
HGD is characterized by more complex glandular dis-tortion; nuclear pleomorphism, hyperchromasia and nuclearstratification are more severe.
Indefinite for dysplasia: this term only applies to caseswhere the pathologist cannot decide with certainty whetherthe lesion is hyperplastic/regenerative or neoplastic in nature.This may be due to inadequate biopsy sampling (e.g. poorlyoriented biopsies that do not enable full thickness assessment)or to the presence of cytological atypia and/or structural al-terations of doubtful interpretation. This could also depend onthe specific experience of the pathologist. It is a “provisional”diagnosis that must be followed by short-term resamplingand/or second opinion. The presence of erosion and neu-trophilic infiltrate requires additional caution in diagnosingdysplasia.
4.7. Special methods (Table 6)
Alcian Blue-PAS: it helps distinguish cardia from intestinalepithelium; the latter only shows goblet cells with Alcianblue-positive acid mucins.
Cytokeratins: cytokeratins 7 and 20 have been suggested asa tool to differentiate intestinal epithelium in BE from gastricintestinal metaplasia [48]. Far from providing conclusiveresults, the validation of this panel has often revealed falsepositives/negatives [49].
CDX-2: this homeobox gene promoting intestinal phe-notype is useful to demonstrate the presence of intestinaldifferentiation [50]. However, intestinal phenotype is also de-tectable with hematoxilin-eosin, in combination with Alcianblue-PAS.
Table 6Special techniques
1. Alcian Blue-PAS: recommended2. CDX-2: not recommended3. CK7/CK20: not recommended4. MUC: not recommended5. p53: optional for dysplasia6. Mib-1/Ki-67: optional for dysplasia
S328 R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330
MUC 1-2-3-4-5: family of genes coding for the gly-coproteins (mucins) that make up intra- and extracellularmucus. The distribution of MUC in the gastrointestinal tractvaries (e.g. MUC 2 is more frequent in colonic epithelium).Cross-reactivity of commercial antibodies has been reported[51].
p53: nuclear accumulation of p53 can help differentiatebetween a reactive/regenerative lesion and dysplasia, withstrong positivity favouring dysplasia. However, it should betaken into account that regenerative metaplastic lesions maybe associated with a variable increase in p53 and, on the otherhand, dysplasia and carcinoma do not always accumulate p53[47].
Mib-1/Ki-67 shows the increased extent of proliferation incase of dysplasia. However, regenerative lesions may also beassociated with high proliferation rate.
In conclusion, so far no specific and reliable markers canreplace conventional histologic examination in the diagnosisof BE.
*The term BE is suggested in this case because it is very likely that a subsequent bioptic sampling, closer to the Z line (SCJ), will show the presence ofintestinal metaplasia [44].
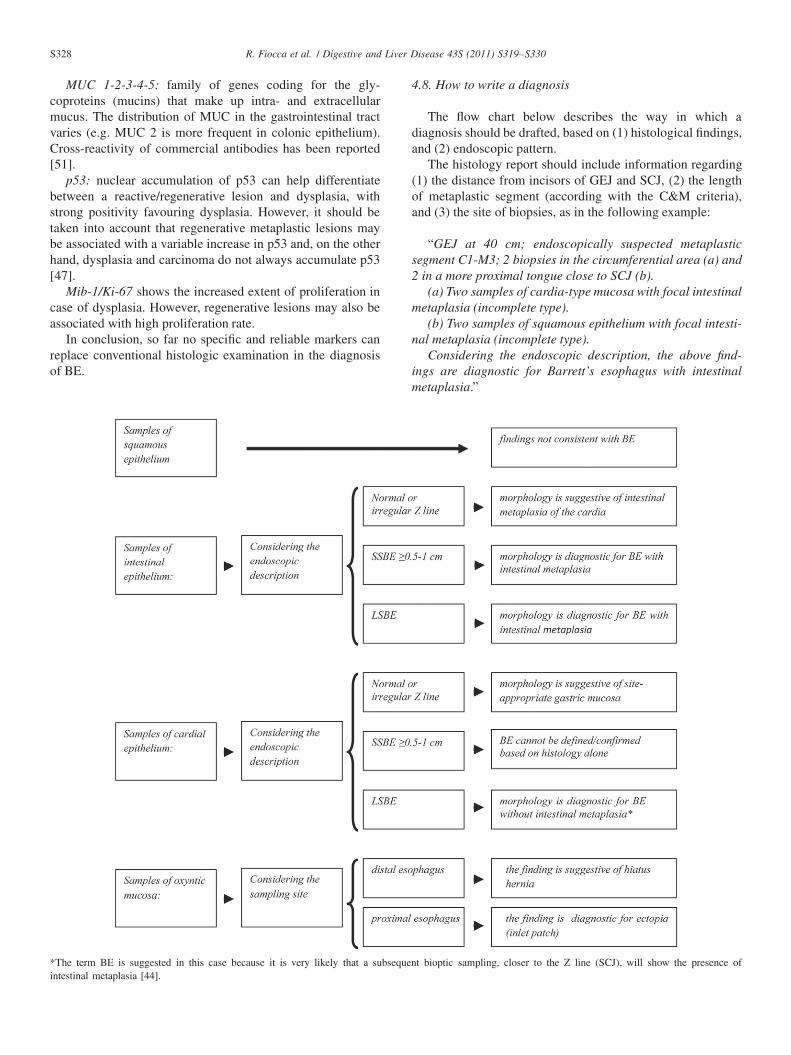
4.8. How to write a diagnosis
The flow chart below describes the way in which adiagnosis should be drafted, based on (1) histological findings,and (2) endoscopic pattern.
The histology report should include information regarding(1) the distance from incisors of GEJ and SCJ, (2) the lengthof metaplastic segment (according with the C&M criteria),and (3) the site of biopsies, as in the following example:
“GEJ at 40 cm; endoscopically suspected metaplasticsegment C1-M3; 2 biopsies in the circumferential area (a) and2 in a more proximal tongue close to SCJ (b).
(a) Two samples of cardia-type mucosa with focal intestinalmetaplasia (incomplete type).
(b) Two samples of squamous epithelium with focal intesti-nal metaplasia (incomplete type).
Considering the endoscopic description, the above find-ings are diagnostic for Barrett’s esophagus with intestinalmetaplasia.”

R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330 S329
In the absence of a complete information about theendoscopic picture and bioptic sampling, the histologicaldiagnosis should be merely “descriptive”.
5. Future perspectives
These “diagnostic guidelines” have been prepared withpractical needs in mind and refer to the current literatureaccording to which BE length and the presence of intestinalmetaplasia are the main cancer risk factors. However, recentstudies seem to demonstrate that:• even cardia-type BE may have some degree of intestinal
differentiation [52];• both cardia and intestinal BE show similar alterations in
DNA content [53];• many esophageal “minute cancers” originate in a non-
intestinal background [54].The real impact of these observations on diagnostic
practice (i.e. the reassessment of risk in cardial BE and of themanagement of such patients) is still to be confirmed [55].
Aknowledgements
This paper has been supported by a grant from FondazioneGuido Berlucchi to R. Fiocca.
Conflict of interest
The authors have no conflicts of interest to disclose.
References
[1] Dent J, El-Serag HB, Wallander MA, et al. Epidemiology of gastro-oesophageal reflux disease: a systematric review. Gut 2005;54:710–7.
[2] Pera M. Trends in incidenze and prevalence of specialized intestinalmetaplasia, Barrett’s esophagus, and adenocarcinoma of the gastroe-sophageal junction. World J Surg 2003;27:999–1108.
[3] Ismail-Beigi F, Horton PF, Pope CE. Histological consequences ofgastroesophageal reflux in man. Gastroenterology 1970;58:163–74.
[4] Barrett NR. Chronic peptic ulcer of the oesophagus and “oesophagitis”.Br J Surg 1950;38:175–82.
[5] Lapertosa G, Parenti A. Esofagiti ed esofago di Barrett: criteri diagnos-tici minimi. Pathologica 1998;90:467–473.
[6] Rugge M. “Die Grenzen meiner Sprache sind die Grenzen meinerWelt" – Pathologists and their readers. Dig Liver Dis 2011;43(Suppl4):S279–81.
[7] Dent J, Brun J, Fendrick A, et al. An evidence-based appraisal of refluxdisease management – the Genval Workshop Report. Gut 1999;44:S1–S16.
[8] Zentilin P, Savarino V, Mastracci L, et al. Reassessment of the di-agnostic value of histology in patients with GERD, using multiplebiopsy sites and an appropriate control group. Am J Gastroenterol2005;100:2299–306.
[9] Fiocca R, Mastracci L, Engström C, et al. Long-term outcome ofmicroscopic esophagitis in chronic GERD patients treated with es-
omeprazole or laparoscopic anti-reflux surgery in the LOTUS trial. AmJ Gastroenterol. 2009;631 [Epub ahead of print].
[10] Vakil N, Zanten SV, Kahrilas P, et al. The Montreal definition andclassification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006;101:1900–20.
[11] Kahrilas PJ, Shaheen NJ, Vaezi MF, et al. American Gastroenterolog-ical Association Medical Position Statement on the management ofgastroesophageal reflux disease. Gastroenterology 2008;135:1383–91.
[12] Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitisin children and adult: a sistematic review and consensus recommanda-tions for diagnosis and treatment. Gastroenterology 2007;133:1342–63.
[13] Geboes K, De Wolf-Peeters C, Rugeerts P, et al. Lymphocytes andLangerhans cells in the human oesophageal ephitelium. Virchows Arch1983;401:45–55.
[14] Mastracci L, Spaggiari P, Grillo F, et al. Microscopic Esophagitis ingastro-esophageal reflux disease: individual lesions, biopsy sampling,and clinical correlations. Virchows Arch 2009;454:31–9.
[15] Fiocca R, Mastracci L, Riddell R, et al. Development of consensusguidelines for the histologic recognition of microscopic esophagitisin patients with gastroesophageal reflux disease: the Esohisto project.Hum Pathol 2010;41:223–31.
[16] Behar J, Sheanhan DC. Histologic abnormalities in reflux esophagitis.Arch Pathol 1985;387–91.
[17] Solcia E, Villani L, Luinetti O, et al. Altered intercellular glycoconju-gates and dilated intercellular spaces of esophageal epithelium in refluxdisease. Virchows Arch.200;436:207–216.
[18] Winter HS, Madara JL, Stafford RJ, et al. Intraepithelial eosinophils:a new diagnostic criterion for reflux esophagitis. Gastroenterology1982;83:818–23.
[19] Brown LF, Goldman H, Antonioli DA. Intraepithelial eosinophils inendoscopic biopsies of adults with reflux esophagitis. Am J SurgPathol 1984;8:899–905.
[20] Rodrigo S, Abboud G, Oh D, et al. High intraepithelial eosinophilcounts in esophageal squamous epithelium are not specific foreosinophilic esophagitis in adults. Am J Gastroenterol 2008;103:435–42.
[21] Schindlbeck NE, Wiebecke B, Klauser AG, et al. Diagnostic value ofhistology in non-erosive reflux disease. Gut 1996;39:151–4.
[22] Vieth M, Peitz U, Labenz J, et al. What parameters are relevant forthe histological diagnosis of gastroesophageal reflux disease withoutBarrett’s mucosa? Dig Dis 2004;22:196–201.
[23] Collins BJ, Elliott H, Sloan JM, et al. Oesophageal histology in refluxoesophagitis. J Clin Pathol 1985;38:1265–72.
[24] Haggitt RC. Histopathology of reflux induced esophageal and suprae-sophageal injuries. Am J Med 2000;108:109–11.
[25] Knuff TE, Benjamin SB, Worsham JF, et al. Histologic evaluation ofchronic gastroesophageal reflux. An evaluation of biopsy methods anddiagnostic criteria. Dig Dis Sci 1984; 29:194–201.
[26] Narayani RI, Burton MP, Young GS. Utility of esophageal biopsy in thediagnosis of nonerosive reflux disease. Dis Esophagus 2003;16:187–92.
[27] Shaheen NJ, Richter JE. Barrett’s oesophagus. Lancet 2009;373:850–61.
[28] Paull A, Trier JS, Dalton MD, et al. The histologic spectrum ofBarrett’s esophagus. N Engl J Med 1976;295:476–80.
[29] Sampliner RE. Updated guidelines for the diagnosis, surveillance, andtherapy of Barrett’s Esophagus. Am J Gastroenterol 2002;97:1888–95.
[30] Sharma P, Dent J, Armstrong D, et al. The Development and Validationof an Endoscopic Grading System for Barrett’s Esophagus: The PragueC&M Criteria. Gastroenterology 2006;131:1392–9.
[31] Goldblum JR. The significance and etiology of intestinal metaplasia ofthe esophagogastric junction. Ann Diagn Patho 2002; 6:67–73.
[32] Richter JE. Short segment Barrett’s esophagus: ignorance may be bliss.Am J Gastroenterol 2006;101:1183–5.
[33] Meining A, Ott R, Becker I, et al. The Munich Barrett follow upstudy: suspicion of Barrett’s oesophagus based on either endoscopy orhistology only – what is the clinical significance? Gut 2004;53:1402–7.
[34] Gopal DV, Lieberman DA, Magaret N, et al. Risk factors for dyspla-

S330 R. Fiocca et al. / Digestive and Liver Disease 43S (2011) S319–S330
sia in patients with Barrett’s esophagus: results from a multi-centerconsortium. Dig Dis Sci 2003;48:1537–41.
[35] Rugge M, Fassan M, Battaglia G, et al. Intestinal or gastric? Theunsolved dilemma of Barrett’s metaplasia. Hum Pathol 2009;40:1206–7.
[36] Wang KK, Sampliner RE. Updated guidelines 2008 for the diagnosis,surveillance and therapy of Barrett’s esophagus. Am J Gastroenterol2008;103:788–97.
[37] Playford RJ. New British Society of Gastroenterology (BSG) guide-lines for the diagnosis and management of Barrett’s oesophagus. Gut2006;55:442.
[38] Sharma P, Sidorenko EI. Are screening and surveillance for Barrett’soesophagus really worthwhile? Gut 2005;54:i27–i32.
[39] Yantiss RK, Odze RD. Optimal approach to obtaining mucosal biopsiesfor assessment of inflammatory disorders of the gastrointestinal tract.Am J Gastroenterol. 2009;104:774–83.
[40] Harrison R, Perry I, Haddadin W, et al. Detection of intestinal meta-plasia in Barrett’s esophagus: an observational comparator study sug-gests the need for a minimum of eight biopsies. Am J Gastroenterol2007;102:1154–61.
[41] Chandrasoma PT, Der R, Dalton P, et al. Distribution and significanceof epithelial types in columnar-lined esophagus. Am J Surg Pathol2001;25:1188–93.
[42] Abela JE, Going JJ, Mackenzie JF, et al. Systematic four-quadrantbiopsy detects Barrett’s dysplasia in more patients than nonsystematicbiopsy. Am J Gastroenterol 2008;103:850–5.
[43] Reid BJ, Blount PL, Feng Z, et al. Optimizing endoscopic biopsydetection of early cancers in Barrett’s high-grade dysplasia. Am JGastroenterol 2000; 95:3089–96.
[44] Chandrasoma P. Four directed biopsies are better than eight randombiopsies to find intestinal metaplasia in columnar lined esophagus.AmJ Gastroenterol 2007;102:2352–3.
[45] Schlemper RJ, Riddell RH, Kato Y, et al. The Vienna classification ofgastrointestinal epithelial neoplasia. Gut 2000;47:251–5.
[46] Spechler SJ. Dysplasia in Barrett’s Esophagus: Limitations of CurrentManagement Strategies. Am J Gastroenterol 2005;100:927–35.
[47] Odze RD. Diagnosis and grading of dysplasia in Barrett’s esophagus. JClin Pathol 2006;59:1029–38.
[48] Ormsby AH, Vaezi MF, Richter JE, et al. Cytokeratin immunoreac-tivity patterns in the diagnosis of short-segment Barrett’s esophagus.Gastroenterology 2000;119:683–90.
[49] Yim HJ, Lee SW, Choung RS, et al. Is cytokeratin immunoreactivityuseful in the diagnosis of short-segment Barrett’s oesophagus in Korea?Eur J Gastroenterol Hepatol 2005;17:611–6.
[50] Shi XY, Bhagwandeen B, Leong AS. CDX2 and villin are usefulmarkers of intestinal metaplasia in the diagnosis of Barrett’s esophagus.Am J Clin Pathol. 2008;129:571–7.
[51] Glickman JN, Shahsafaei A, Odze RD. Mucin core peptide expressioncan help differentiate Barrett’s esophagus from intestinal metaplasia ofthe stomach. Am J Surg Pathol 2003;27:1357–65.
[52] Hahn HP, Blount PL, Ayub K, et al. Intestinal differentiation inmetaplastic, nongoblet columnar epithelium in the esophagus. Am JSurg Pathol 2009 [Epub ahead of print].
[53] Liu W, Hahn H, Odze RD, et al. Metaplastic esophageal colum-nar epithelium without goblet cells shows DNA content abnormali-ties similar to goblet cell-containing epithelium. Am J Gastroenterol2009;104:816–24.
[54] Takubo K, Aida J, Naomoto Y, et al. Cardiac rather than intestinal-type background in endoscopic resection specimens of minute Barrettadenocarcinoma. Hum Pathol 2009;40:65–74.
[55] Riddell RH, Odze RD. Definition of Barrett’s esophagus: timefor a rethink – is intestinal metaplasia dead? Am J Gastroenterol2009;104:2588–94.