Analysis of the Liberian Ebola Survivors Support …...2014/15 Ebola Virus Disease (EVD) outbreak in...
13
Integrative Journal of Global Health 2017 Vol. 1 No. 2: 10 iMedPub Journals ht tp://www.imedpub.com Research Article 1 © Under License of Creative Commons Attribution 3.0 License | This arcle is available in: hp://www.imedpub.com/integrave-journal-of-global-health/ Jessi Hanson 1 , Patrick Seeco Faley 2 and Megan Quinn 3 1 University of Pisburgh, Pisburgh, USA 2 Ebola Survivors’ Network, University of Liberia, Liberia 3 East Tennessee State University, Tennessee, USA Corresponding author: Jessi Hason [email protected] University of Pisburgh, Pisburgh, USA. Tel: 7205487241 Citation: Hanson J, Faley PS, Quinn M. Analysis of the Liberian Ebola Survivors Support System (ESSS). Integr J Glob Health. 2017, 1:2. Analysis of the Liberian Ebola Survivors Support System (ESSS) Abstract A systems theorecal analysis to capture the evoluon and transion of the network systems supporng Ebola survivors and their affected communies, during the 2014-15 Ebola outbreak and recovery phases. The qualitave analysis includes a literature review, archival review, and interviews with representaves of key actors operang in strategic acon fields. This paper uses a series of Diagrams that visually illustrate the various complex phases and their network changes that occurred and were established during the outbreak. This case analysis provides crucial phase informaon that both captures the historical events that informed the systems changes, including the development of the Ebola Survivors’ Support System (ESSS). Secondly, this analysis acts as, a model of understanding how disease support networks first emerge and can be beer supported in other outbreaks. Keywords: Ebola; Evoluon; ESSS; Health Received: June 29, 2017; Accepted: July 17, 2017; Published: July 28, 2017 Introducon This research applies a systems theorecal analysis to capture the evoluon and transion of the network systems supporng Ebola survivors and their affected communies, during the 2014- 15 Ebola outbreak and recovery phases. The qualitave analysis uses a series of Diagrams that visually illustrate the various complex phases and their network changes that occurred and were established during the outbreak. This case analysis provides crucial phase informaon that both captures the historical events that informed the systems changes, including the development of the Ebola Survivors’ Support System (ESSS), and secondly, a model of understanding how disease support networks first emerge and can be beer supported in other outbreaks. With the increase of modern disease outbreaks like Ebola, public systems are burdened to assist new afflicted populaons never- before documented. These new affected populaons provide an oſten-unforeseen policy issue- tracking not only those who become infected but disease survivor clusters to methodically respond to their unique support needs aſter their discharge. Systems theory literature offers soluons to this problem by analyzing already-exisng networks that developed to respond to outbreak-affected populaons. This literature further demonstrates the importance of mapping the process by which a network first develops and changes in the Complex Adapve System (CAS) of a crisis for future knowledge applicaon. The 2014/15 Ebola Virus Disease (EVD) outbreak in Liberia acts as a vital case study in this endeavour. Amid the West African Ebola response CAS, the Liberian Ebola survivors’ support system (ESSS) eventually grew from an emergent field of acon into a legimate network with improved signals and boundaries over the course of the emergency. However, this learning process was hindered by lack of previous knowledge to inform its formaon. There were previous Ebola outbreaks but with lile knowledge retenon or guidance for key actors about providing care for persons directly impacted by a hemorrhagic disease. The Ebola response was ill-prepared for the extent of survivors whose lives were leſt in pieces. The early stages of the ESSS may be characterized as delayed, encumbered, and at mes inefficient at the expense of helping those most affected by the outbreak. The state would later advocate for a mainstreamed approach placing the ESSS as a leading facilitator in partnership collaboraon among fields. This paper aempts to document for one of the first mes a disease survivors support system (DSSS) through a systems theory approach. This analysis tracks the evoluon of the Liberian ESSS as a means of: 1) capturing its transion during different phases of the response, 2) key issues, and 3) system structure changes,
Transcript of Analysis of the Liberian Ebola Survivors Support …...2014/15 Ebola Virus Disease (EVD) outbreak in...

Integrative Journal of Global Health 2017
Vol. 1 No. 2: 10iMedPub Journalshttp://www.imedpub.com
Research Article
1© Under License of Creative Commons Attribution 3.0 License | This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
Jessi Hanson1,Patrick Seeco Faley2 and Megan Quinn3
1 UniversityofPittsburgh,Pittsburgh,USA2 EbolaSurvivors’Network,Universityof
Liberia,Liberia3 EastTennesseeStateUniversity,
Tennessee,USA
Corresponding author: JessiHason
UniversityofPittsburgh,Pittsburgh,USA.
Tel: 7205487241
Citation: HansonJ,FaleyPS,QuinnM.AnalysisoftheLiberianEbolaSurvivorsSupportSystem(ESSS).IntegrJGlobHealth.2017,1:2.
Analysis of the Liberian Ebola Survivors Support System (ESSS)
AbstractA systems theoretical analysis to capture the evolution and transition of thenetwork systems supporting Ebola survivors and their affected communities,duringthe2014-15Ebolaoutbreakandrecoveryphases.Thequalitativeanalysisincludesaliteraturereview,archivalreview,andinterviewswithrepresentativesofkeyactorsoperatinginstrategicactionfields.ThispaperusesaseriesofDiagramsthatvisuallyillustratethevariouscomplexphasesandtheirnetworkchangesthatoccurredandwereestablishedduringtheoutbreak.Thiscaseanalysisprovidescrucialphaseinformationthatbothcapturesthehistoricaleventsthatinformedthesystemschanges,includingthedevelopmentoftheEbolaSurvivors’SupportSystem (ESSS). Secondly, this analysis acts as, a model of understanding howdisease support networks first emerge and can be better supported in otheroutbreaks.Keywords: Ebola;Evolution;ESSS;Health
Received: June29,2017; Accepted: July17,2017; Published: July28,2017
Introduction This research applies a systems theoretical analysis to capturetheevolutionandtransitionofthenetworksystemssupportingEbolasurvivorsandtheiraffectedcommunities,duringthe2014-15Ebolaoutbreakandrecoveryphases.Thequalitativeanalysisuses a series of Diagrams that visually illustrate the variouscomplex phases and their network changes that occurred andwereestablishedduringtheoutbreak.Thiscaseanalysisprovidescrucialphaseinformationthatbothcapturesthehistoricaleventsthat informedthesystemschanges, including thedevelopmentof the Ebola Survivors’ Support System (ESSS), and secondly, amodel of understanding how disease support networks firstemergeandcanbebettersupportedinotheroutbreaks.
WiththeincreaseofmoderndiseaseoutbreakslikeEbola,publicsystemsareburdenedtoassistnewafflictedpopulationsnever-before documented. These new affected populations providean often-unforeseen policy issue- tracking not only thosewhobecome infected but disease survivor clusters to methodicallyrespond to their unique support needs after their discharge.Systems theory literature offers solutions to this problem byanalyzing already-existing networks that developed to respondto outbreak-affected populations. This literature furtherdemonstratestheimportanceofmappingtheprocessbywhichanetworkfirstdevelopsandchanges in theComplexAdaptiveSystem (CAS) of a crisis for future knowledge application. The
2014/15EbolaVirusDisease(EVD)outbreakinLiberiaactsasavitalcasestudyinthisendeavour.
Amid theWestAfricanEbola responseCAS, the Liberian Ebolasurvivors’ support system (ESSS) eventually grew from anemergentfieldofactionintoalegitimatenetworkwithimprovedsignals and boundaries over the course of the emergency.However,thislearningprocesswashinderedbylackofpreviousknowledge to inform its formation. Therewere previous Ebolaoutbreaksbutwithlittleknowledgeretentionorguidanceforkeyactors about providing care for personsdirectly impactedby ahemorrhagic disease. The Ebola response was ill-prepared fortheextentofsurvivorswhoseliveswereleftinpieces.TheearlystagesoftheESSSmaybecharacterizedasdelayed,encumbered,and at times inefficient at the expense of helping thosemostaffectedby theoutbreak. The statewould later advocate for amainstreamedapproachplacingtheESSSasaleadingfacilitatorinpartnershipcollaborationamongfields.
This paper attempts to document for one of the first times adiseasesurvivorssupportsystem(DSSS)throughasystemstheoryapproach.ThisanalysistrackstheevolutionoftheLiberianESSSasameansof:1)capturingitstransitionduringdifferentphasesoftheresponse,2)keyissues,and3)systemstructurechanges,

2 This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
to serve as a guide for amore effective policy process duringfuturecommunicablediseaseoutbreaks.
MethodsThisqualitativeresearchincludes:1)aninitialliteraturereviewofreportsandarticlescoveringtheLiberianEbolaresponseincludingWorldHealthOrganization(WHO)andCenterforDiseaseControl(CDC)situationreportsandsummaryreports;2)anarchivalreviewofdisasterresponsedocumentationcollectedduringPhase2-3oftheoutbreak,includingInformationManagement(IMS)meetingnotesandreports;3)firsthandexperiencesoftwooftheauthorswhoparticipatedinreliefeffortsandledprogrammingforEbolasurvivorsandtheirfamilies,includingdirectworkwiththeESSS;and4), interviewswith various key representativesof strategicactionfieldsactiveintheoutbreak.Thisworkisincoordinationwith Government of Liberia (GoL), with appreciation for theMinistry of Gender Development and the Ministry of Health.Thesetwoministrieshavehadmultipleofficialtitles,butforthisreporttheywillbereferencebysimplifiedtitles.Lastly,ministryofficials and external lead crisis responders later cross-verifiedthe draft of this analysis, providing feedback on the accuracyof its information, findings, and conclusions. All feedback wasincludedinthemodificationofthefinalversion.
Historical Documentation of Disease Survivors Support SystemsThe2014/15Ebolapandemicresultedin28,616cases,ofwhichapproximately one-third were in Liberia [1]. Population datacollected during the outbreak was often inaccurate. Yet, it isestimatedthatthereareover5,000LiberianswhowereinfectedwithEVDandsurvived,latertermedbytheinternationalhealthcommunityasEbolasurvivors.
Since1976,therehadbeenover35knownEVDoutbreaksintheworld,mostly affecting sub-Saharan Africawith a survival raterangingfromabout20-100%.Whilenopreviousoutbreakshadsuchadevastatingtollasthe2014/15crisis,numerousincidencesinvolved victims numbering in the hundreds [2]. A 2014 studypublished in the Journalof theRoyalSociety Interface,“GlobalRise inHuman InfectiousDiseaseOutbreaks,” shows that since1980, the number and frequency of global disease outbreaksandtheirvarietyhavecontinuedtoincrease.Anestimated65%ofthesecontagionsarezoonosisinnaturelikeEbola.Yetglobalpublichealthsystemscontinuetolaginpreparedness[3].
Most Ebola literature and response programming has mainlyfocusedondiseasecontracttracing,isolation,aswellastreatmentandpreventionefforts.Much lessexistsonmapping thenetworksupport for surviving victims of the virus. Other deadly diseasesthatarehemorrhagicortransmittedthroughbodily-fluids,suchasLassa fever andHIV/AIDS, havebetter research informinghow tosystematicallyrespondtotheneedsofsurvivorsortheirhouseholds,in what may be considered a disease survivor support system(DSSS).However,thisresearchdevelopedslowlyoverdecadesafterthevirusesappeared. It iswellknownthatpersons livingwithaninfectious, life-threateningdisease frequentlyareaffectedbeyondthephysicaleffectsof theircondition [4,5].Duringanemergency,theseneedscanbelifealtering.
Phase Transitions - Fields and InteractionsSolé [6] demonstrates that phase transitions happen overtimeoften through interactions among units that drive dynamicchange.Theprocessofchangeofanetworkcanadvancewithinatransformingcomplexadaptivesystem[7-9].TheLiberianEVDresponseCASdemonstratedasubstantial levelofadaptionandlearningduringthefirstthreephasesofthecrisis,whichresultedintheemergenceanddevelopmentoftheESSS.Thischangewasoftenactivatedthroughkeygovernmentalpolicyadoptions.Thesystemsizedependsonthenumberofdifferentactorsandhowtheyadapttoworkbettertogetherasacontinuallearningprocess[6]. Thispaperwill explore the changeof theESSS throughoutthesephases.
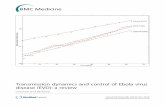
Phase 1: Initial outbreakThe theory of systems by Fligstein and McAdam [7] providesinsight into the social order that develops particularly in anemergent system. Furthermore, Fligstein andMcAdampresenta functional taxonomy for the different actors and fields inoperationinanalyzingtheESSS,whichwillbeappliedfrequentlywithinthisanalysis,includinginthephaseDiagrams.Throughoutthe Liberian EVD crisis, a meso-level social order slowly wasconstructedtosupportsurvivors,flocculatinginsizedependentontheproximatefieldsoperatingwithintheresponseenvironmentatdifferenttimesinthecrisis.Theinitialoutbreakphaseoftheresponse (March to early August 2014) was obstructed by alargediversityof agents attempting to respond to the growingcrisiswith little knowledgeor experience to guide them,oftenoperating independently with little collective action and weakinformationsharing,asshowninDiagrams 1 and 1.1.
ActorsThe Ministry of Health and Social Welfare (MOH), under themandate of the Government of Liberia (GoL), played a crucialmediation and governance role which better stabilized thecollective action of multiple survivor organizations, donorsand response agencies operating in Liberia around the peakphase. Acting as internal governing unit (IGU) of multiplefields overseeing compliance for entities operating in countryon tracking and prevention, treatment, and reintegration ofaffectedpersons, theMoHalongwith leadpartneragenciesofthe IncidenceManagement System (IMS) enactedpolicies thatpromoted the ESSS to become the strategic action field underwhich all coordination efforts were to occur to aid survivors.However, two exogenous shocks had to occur before this finalsettlementcouldbereachedinlate2014.Thefirstshockwastheidentificationofpatientzerowithincountry,inMarch2014,whilethesecondwouldbetheAugustspikeindiseaseincidences.
Early in the first phase, regional coordination response firstaroseacrosstheborderofGuineaandSierraLeonefromLiberiainvolvingkeyinternationalhealthagencieswithsimilarnichesindiseaseresponse,including:theCenterforDiseaseControl(CDC),WorldHealthOrganization(WHO),andMédecinssansFrontièresMSF/DoctorswithoutBorders,andtheRedCross[1,2,10].Theseinternational health agencies worked with Liberian agentslocatedontheground;butmostlytheyoperatedinaconsultative

ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
3© Under License of Creative Commons Attribution 3.0 License
roleasadistantfieldofaction(Diagram 1).InternationalhealthagencieslikeCDCbegansendingmaterialandhumanresourcestoLiberia,butcommunicationsystemswereweak.WhiletheUNmetwithCDC/WHO,theircoordinationwasminimal.TheUnitedNations Office for the Coordination of Humanitarian Affairs
(OCHA)wasnotactivatedwhichmayhavemorequicklyrampedupemergencyresponsecoordination.
Additionally,manykeyinternationaldonors,UnitedNations(UN)agencieslikeUNICEFandtheUNMissionsinLiberia(UNMIL),and
Diagram 1 InitialOutbreakPhase(March-July2014).
Diagram 1.1 MailFieldInformationFlowandSurvivors.

4 This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
nationaland internationalNGOs,andcivilserviceorganizationsoperating in country to support post-war reconstruction andpeace-keeping efforts for over ten years found themselvessuddenly incapable toeffectivelyaid the rapidly growingEbolaresponsecrisis. InaCAS,agentsonthegroundmustongoinglyadapttochangesintheenvironmenttoremainrelevant[8,11].Yetmostofthedevelopmentandpeace-keepingagenciesontheground instead acted as proximate fields resistant to adaptionfromnon-responseprogrammingtoemergencyresponseaction.Theytendedtoviewtheoutbreakasbeyondtheirscopeofworkor expertise. They instead quickly downsized operations andrestrictedcoordinationeffortsoftheirteamsbeyondthesharedboundariesoflogisticalcoordinationandresourcesupporttothestateministryagencies.Somewouldmakethechange.
Piketty[12]depictshowpoliticalandeconomicsysteminfluenceone another often represented in power dynamics betweenactorsandcontroloffinancialresourcing.Earlyinthecrisis,thestateagenciesfrequentlyrequestedfundingtoexpandresponseservices and administration. But, the low number of diseaseincidents and redistribution of annual ministerial budgets topublichealthcoffers temporarilyallowedthestatetoactmoreautonomouslyincombatingEbola.Foratime,thestateagencieswerenot reliantonextensiveexternal fundingby internationaldonors (nowestimatedat$155millionUSD)as thecostof theinitialphasenationallywasrelativelylow.
Key IssuesInthesefirstchaoticmonths,personswhosurvivedthediseasemostly went unnoticed, bleeding into the general emergencylandscape. The first interactions with survivors infrequentlyoccurred informally in person among key stakeholders: stateministry agencies (MOH Ministry of Gender (MOG)), nationaltreatment response actors, and religious organizations, whendischarged survivors would return to Ebola Treatment Units(ETUs)andgovernmentbuildingspleadingforsupport.
ByAugust,thesizeofthepublichealthsectorwasheavilydepletedofhundredsoffrontlineworkersexposedtoextremelyhighratesof EVD infection, and both healthworkers and public servantsabandoningtheirpoststofleethecrisis.Therewerenotenoughvolunteers and private health professionals to supplement thegrowingnumberofopenpositions[13].Thisdecreaseinhumanresourcingweakenedinformationtrackingandsystemflows,asknowledgemanagementsystemsstalled.Liberianorganizationalculture traditionallywashierarchicalwith command structuredcentralizedinministrydepartments,whichasInnesBooher[14]show involve bureaucratic styling that could hamper normallearningprocesses.Liberianstateministryagencycommunicationsystems,oftentoooutdatedfortimelycommunicationrequired,were increasingly stretched thin.Ministerial agencies relied onpast methods of communication sharing through scheduledcoordination meetings and formal printed letters/reportsdeliveredviamessengerafter rigorousadministrativeapproval,including multiple signoffs from departmental heads in thecentralministryandCountyHealthTeam(CHT)requiringhoursif not days. Agents within the National Treatment Responsesharedasimilarcultureofcommunicationastheycomprisedof
mainly nationals includingMOH staff. Yet foreign entities usedelectronic methods (phone, internet) that were more familiarandfrequentlycircumventedministrycollaboration.
Information flows involving survivors occurred between fieldslaterinthefirstphasewhenprofessionalactorsmorefrequentlyinteractedwith survivors (Diagram 1.1). Survivorsweremainlyseekingfundingsupportatfirst,duetotheirpossessionsbeingdestroyedduringdecontaminationorstolenwhileintreatment,aswellasjoblossduetostigmaoftheirinfection-statusandthecrisishaltingtheeconomy[15].Theywerealsosufferingextremepsychologicalstress[16].Buttherewasnobetter-structuredwaytocommunicatetheseneeds(thanbystanding)outsideofETUandministrygates(flaggingtheattentionofprofessionalswalkingintothecompoundsandtalkingwiththemdirectly.Fewsurvivorshadanyothermeansofcommunicatingwithofficialswhocouldhelpthem).Thegrowingnumberofsurvivors(fromafewdozento 260by late July) seekingpersonalmeetingswith professionhealthandministryworkers led to theemergenceof theESSS,andprovidedsignalstocommonneeds.
Transition of System StructureThe policy solution for the MOH was to authorize responseorganizations to hire survivors as temporary paid volunteers,workingmostlyinEbolaTreatmentsUnits(ETUs)andquarantinecenters(ICCs/CCCs).Thedriversforthistransitionwere:1)uniquehuman resource of persons who theoretically were immuneto supplement care for contagious patients; 2) motivation ofaffecting positive change in the face of tragedy [17,18]. Thesurvivors representeda symbolofhope fordespondenthealthteams,particularlyasthevictimdeathrateloweredwithimprovedtreatment,reenergizingthedrivetocollaborateonpriorities.
Throughouttheinitialphase,communicationsbetweenfieldsintheresponseCASremainedweak.However,oncethesurvivors’plight was recognized and championed by key agencies, theESSSwouldactasoneofthelynchpinsthatconnecteddifferentfield agents under a shared common goal in the peak phaseof emergency. Yet, the ESSS remained an emergent field withthe only strong information flows occurring through standardministry response channels to proximate and distant fields ofactionfocusedontracking,treatment,andprevention;survivorsupportinformationwascarriedsecondarily(Diagram 1.1).
Ongoing NeedsComplicatingmatters,identifyingandtrackingsurvivorsbecamedifficultasthenumberofvictimsrosetowardsthepeakphase;anuntoldnumberofinfectedpersonslikelydidnotseekformalcarethroughout thefirst phasesof the crisis, andpaper-based ETUregistrieswerefilledwithincompleteorfalsepersonalidentifiableinformation [19,20]. Survivors learnedmostly throughword ofmouththroughsmallpocketsofsurvivorsupportnetworksandassociates fromETUdischarge aboutwhich officials to contactbyphoneorvisitinpersontoseekhelp[17].Additionally,publicfearofsurvivorswasamassing,asmuchof thepopulationwasboth ill-informed that survivorswerestill contagiousaswellas

ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
5© Under License of Creative Commons Attribution 3.0 License
heldtraditionalvoodoobeliefsofdiseasesbeingaspiritualcurse,which heightened stigma and discriminatory acts against thisvulnerablepopulation[16].
Phase 2: PeakThesecondexogenousshock in thecrisiswas theAugust2014rapidspikeinEbolarates,ledtostrictborderclosuresandmediaattention, an increase in international responseefforts, aswellasaneventualdestabilizationoftheeconomyandinfrastructurecapabilitiesofboththecountryandregion.Thisexogeneousshockshiftedthepoliticalandfinancialdynamicsoftheresponse,whichasPiketty[12]shows,oftenfuelsrelationalchangebetweenleadactors.Dialoguefacilitatesnegotiatingaccesstoneedfundingandresources,yettherearisenewissuesofcompetition.WhereastheLiberianstateandnationalresponseteamhadbeentheprimaryleaderswithsupportfromregionalcoordinationresponseintheearlyphase, thepeakdrove increased international supportasthecrisisbecameapandemic.
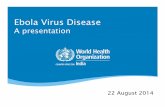
This shift drove a larger diversity of new response actors andspurred many older agents in proximate and distant fields ofaction to adapt their operations to join the response growingfrom a handful of active NGOs to at one time 37 responseNGOs. Coordination between the national treatment responseand regional coordinated response overlapped tighter throughregionalpoliciesdesignedbyinternationalagenciesanddonorsin partnership with the West Africa contingency. However,the influx of new international health actors and transitioningnonprofits (NGOs) changed the power dynamic in terms ofhuman and financial resourcing of the distant and proximatefields(Diagram 2).Feedbackloopswerepoorlyconstructed,analready inefficient information systemwas further constrained,and most collaborative decisions and policies were renderedineffective[18].AsPage[9]demonstrates,toomuchdiversityina systemwith limited common knowledge and agreement canunbalancethesystematicscales.
Key IssuesSolé[6]explainsthatfluctuationsinonesystemmayleadtotheformation of a new system or revisions within it. Additionally,thesystemsizedependsonthenumberofdifferentactorsandhowtheyadapttoworkbettertogetherasacontinuallearningprocess. Slowly, the size and scope of the response CAS grewyetindividualfieldsincreasinglyoverlappedineffort,unifiedbyimprovedsignalsandboundaries,withtheESSSatthecenterofthis newwave of energy serving as a policy tool for improvedcollaborativeaction.However,conflictandcompetitionamongstthedifferent responsefields injecteddivergence in theESSSasthecrisisgrew.
InAugust as thedisease climbed toover 1,300 cases, the IMSCommittee Deputy Minister proposed to the MoH/IMS theformation of the NESNL, which would be internally overseenandmaintained byMoH/IMS representatives andmanaged bynetwork team of Liberian health officials and survivor leaders.TheNESNLwasoneofmultipleclusterswhichwouldlaterdevelopasincumbentswithintheESSS,yieldingasFligsteinMcAdam[7]refertoasadisproportionateinfluencewithintheboundariesofthestrategicactionfields.
Forthisproject,thetermclusterwillrepresentthesmallgroupsthatdevelopedfirstaspocketsofsurvivorsoftenwhokneweachotherfromETUtreatmentorwithintheircommunities,bandingtogether for solidarity and support, and eventually gainedsomefinancialfundingfromdifferentagenciessuchasreligiousorganizations,individualsponsors,civilsocietyorganizations,andeven larger donor or implementing agencies.Numerous bandsdevelopedintoorjoinedclustersastheircontingencyofinformalsurvivormembershipgrew.Theseclusterswereoftenrecognizedasrepresentativebodiesandallowedtospeakontheirbehalfatkeyresponsecoordinationmeetings.
ByNovember 2014, theMOHwas recognizing the difficulty intrackingandmanagingnotonlytheenormousinputoffunding
Diagram 2 PeakPhase(August-December).

6 This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
andagencyactivitiestocombatthedisease,butalsoinworkingwithEVDsurvivorsandvulnerablefamilies.AsshowninDiagram 2.1, communication chains changed and grew more complex,often deviating from older response channels. Although theIMS and the Ebola Emergency 311Hotlinewere in place, theywere relativelynew systemsnot experienced in country.ManyPeakPhaseactionsrecommendedbyexternalpartners liketheCDC/WHO and sanctioned by the statewere strange conceptsto Liberian citizens requiring great adjustment, such as callingforanambulanceorburialteamtotendtovictims.Somewereso culturally foreign (body burning, forced body removal andforcedquarantine)thattheyincreasedfearanddistrustamongstthepopulationofnewstateandresponseCASprotocols.Thesefailuresdroveapoliticalwedgebetweensomeinthestateandtheincoming responseagencies,butministry leadership continuedfurther collaboration. Maintaining cooperation becomesimportant in public policy issues when extreme emotion maydriveirrationality[21].
Asthenumberofvictimsgrewintothethousands,thenumberofsmallpockets(clustersliketheNESNLwithintheESSS)supportingsurvivorsdeveloped.Theyofferedtheirmembersmorethanjustjobsbutstipends(rangingfrom$100-450USD/month)andnon-fooditemsgrew.InPhase2,therewere9identifiedESSSclusters,6 which were unregistered with the state [10]. Each cluster(Diagram 2.1) was actively tracking survivors for membership,solicitingorganizationsanddonorsforportionsoftheincreasedfunds and resources, and representingmembers’ issues in keyresponse coordination meetings. The MOH grew weary of itsinabilitytotrackactionsbetweensurvivorsandexternalpartners.Thequality of information trackingworsened as these clustersreportedduplicatemembershipanduseddifferenttrackingandreportingsystems.
Several clusters were also suspected of including ghostmembership, inwhichanumberof listedmembernamesmaybeinventedorincluderealpersonsfalsifyingtheirstatustoclaimemergencybenefits.GhostmembershipwasacommonissueofcorruptioninLiberiasincewartime,nowrepurposedintoanewform of fraud during the outbreak. Likewise, donors, eager toallocatetheirfunds,andimplementers,underpressuretospendgrantsquickly,frequentlycommunicatedwiththeESSSthroughnew channels including private meetings, phone calls, andevenasabrasivelyasentering formerhotzonesandunloadingsuppliesdirectlyintheaffectedhouseholds(HH),withnoofficialregistriesandwithoutstateguidance.Theseactionsresultedinpoordistributionandpowerstrugglesthatcouldnotcontinue.
Transition of System StructureBy October 2014, the driver of change in the next phasetransitionoftheESSSincluded:1)controllingfinancialallocationsand resource distribution, and 2) improved communicationthat increasedaccuracyof trackingand reportingmechanisms.TowardstheendofthePeakPhaseandintothedeclinephase,thestateministryagenciesenactedaseriesofpoliciesthatrevisedtheinteractionsbetweenoldandnewactorsastheyincreasinglytransitioned into strategic action fields supporting survivors.While these policies were often state imposed, they allowedwhatInnesandBooher[14]refertoascollaborativerationality.
Firstly, in October 2014, all clusters or groups working withsurvivorshad to registerwith the stateand submit all reports,partnership agreements and membership lists or identifiedsurvivor databases to the newly formed, joint MOH/MOGdivision,associatedwiththe IMS.Secondly,thestate in itsroleas the internalgovernmentunit (IGU)of the survivornetwork,
Diagram 2.1 MainFieldInformationFlowandSurvivorsbeforeMandate.

ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
7© Under License of Creative Commons Attribution 3.0 License
facilitatedthefirstnationalmeetingofallidentifiedsurvivorsinMonroviaoncontactlists.Inthislargemeetingwithattendancein thehundreds,survivorswereaskedto formally registerwiththe state to confirm their recovery-status under set protocolincludingdocumentation,andtoencouragetheirpeerstodothesame,tobeprioritizedforbenefits[21].
Next,twoledsurvivorclusters,theEbolaSurvivors’Association(ESA) and the MOH-supported National Ebola Survivors’Network-Liberia (NESNL)were chargedwith taking the leadoncommunicatingthesenewpolicies,includingtravelingintoruralsectors.TheNESNLhadnoresources,sothestatesuppliedtheleadershipwithofficespacewithinthemainMOH-IMSbuilding,as well as resources including computers and phones. WiththeNESNLhoused in theMOH,dialoguewith stateauthoritiesfacilitated engagement and consensus for action, and servedasadirectcommunicationtoolthatquickeneddecision-makingapproval among key departments also set up in the mainbuilding. The state also disbanded several fraudulent groupsposing as clusters. Additionally, another key policy stated thatall implementing agencies had to undergo state-led trainingof protocol in working with vulnerable populations includingsurvivorsandchildren[22].
The increased frequency of interactions with actors and thestate drove further dynamic change, measured in decrease ofconflictingsurvivordatasetsandtheestablishmentofauniversalregistrationtoolsetbyDecember.Additionally,attendanceinIMSandkeystate-ledcoordinationmeetingsgrewwhichstreamlinedinformation sharing, in which the ratio of meetings by thosewithsurvivorissueminutesimprovedfromabout1perevery4meetingsinOctoberto4:4byNovember[10].
Survivorinputalsoexpandedandpermeatednewfieldsthroughparticipatinginkeystrategicandcoordinationmeetings.Likewise,their voices became a universal symbol of overcoming Ebolain distant fields; their testimonials were shared nationally andinternationallythroughsocialmediaandnewsoutlets,promotedby international actors in all fields including UN agencies likeUNICEF and the I Survived Ebola campaign, donors likeUSAID,aswellas INGOslikeSavetheChildrenandMorethanMe.Yetthe state struggled to track socialmediaof survivoradultsbutweremoreeffectiveinprotectiveregulationsinstoriesinvolvingaffectedchildren.Themediaincreasedprioritizationofsurvivorfundingandprogramsbydonorsand incomingor transitioningNGOsinPhase3.
Thesequalitativechanges in thePeakPhase in communicationandinformationexchangehelpedsolidifyconsensusforchangein a more democratic and systematic fashion. Secondly, itreestablished the ministry agencies not only as IGU but in its
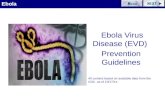
traditionalculturalroleasmanagingauthority,whichwasneededto create improved field stability through setting signals andboundariesreflectedthroughprotocolandpoliciesthatorientedoldandnewagencies (Diagram 2.2).Setpoliciesprovidedtagsfor competing fields, particularly donors and internationalhealthorganizations/transitionedresponseNGOs,ofacceptableboundaries for actions involving survivors, and revised a newshared culture amongst actors. For instance, the MOH beganregulatingtherangeforone-timereliefstipendsandsalarypayforsurvivors thatagenciesallocated, initially raising theminimum-wageand loweringhigh-payoutsbyspecificagenciesthatwerecausingdisgruntlementamongsttheESSS.
Ongoing NeedsHowever, theseboundarieswerenotalwaysrespectedandthecommunicationremainedweakbetweenstateandinternationalimplementingpartners,particularlyincasesofhightransitionandrapidemployeeturnover;manyprojectmanagersandconsultantsonlywerehired forshortstints,andtheir replacementshadtore-orient to the systemcultureandoperations.Therewasalsoincreasingexternalpressurebyregionalandinternationalteamstomaintainstrongbudgetexpenditures,whichcouldbestalledbyfollowingstatemandates.Themorestatecomplianceprotocolswereestablished,thegreaterthebureaucraticinefficiencies.Forinstance, a projectmanagermayneed to haveMemorandumsof Understanding (MoUs) signed with multiple departmentsinmultiple stateministries,whichwasnotconducive totimelyaction in an every-changing emergency response cas. Thiswasone reason, a number of unauthorized communications andpartnershipscontinuedevenafterstateprotocolswereset.Table 1 demonstratesthekeyactorswhoactedasstrategicactionfields(SAFs)interactingwithsurvivorsthroughtheESSS,theirchanginglevel of communications, and the shifting power dynamicsbetweentheactorandthestateagencies(MOH/MOG)intermsofpolicyprotocolcomplianceandfeedbackloops.
Fraudandpoorallocationsofresourcesalsocontinuedthroughthe next phases of the emergency. Survivor clusterswere alsoidentifiedlaterasstillexistingwithoutproperregistration,oftensoliciting funding that could not be accounted for officially.Moreover,competitioncontinuedtogrowamongsttheclustersforfundingfortheirmembersandtheirpriorityofneeds,aswellas recognition and dominance within the ESSS. Some clustersstoppedcomplyingwith theMOH,suchasno longerattendingmandatedmeetings,andoperatedindependentofauthorization.Thistensionrevealedapointofdisagreementandtheneedfornewboundaries[14].
ByDecember 2014, this ongoing gap in collaborationbetweenclusters signalled to the MOH and the Incident Management
Table 1SummaryofSAFsInteractingwithESSSandPowerDynamicswithStateAgencies.
Key SAFPhase Transitions
1 2 3ReligiousOrganizations * *** ***
NationalHealthTreatmentResponse * *** ***Implementers-TransitioningINGOsandHealthINGOs - ** ***
Donors - * ***CommunicationaboutESSS-Low*;Medium**;High***;StateAgencyAdherence-Strong(Green);Weak(Yellow);Contentious(Red)

8 This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
Team theneed to imposeamoreauthoritative transition. Thismove was further advertised to entities through a series ofactions towards the end of Phase 2. Primarily, the November2014 inauguration of the NESNL that included key actors likeUNICEF,aswellasofficialnewspapercoverage,demonstratedthegrowingpartnershiptransitionbetweenthestateandthisclustertodominatetherestofthecrisis[23].
Decline PhasePhase 3, the decline of the outbreak, experienced a shift inthe system fields. International donors and agencies fieldstransitioned into large strategic fields that eventually outsizedboth the fields of the state ministry agencies and nationaltreatment response. However, these four SAFs overlapped intheir coordinationmainly through formalmeetings establishedthrough the IMS and coordinated email groups, co-led by theGoLagencies,theUSmilitary,keyUNagencies,andinternationalresponseagencies.Thenumberofmeetingsdrasticallyincreasedas too did the number of agencies. Other additionalmeetingswereestablishedbyproximatefieldsofoperationswithnationalandinternationaloperators,includingbyUNagencieslikeUNICEF.These meetings had selective membership, such as betweenmostly international agencies coordination and few ministryrepresentatives, often relating to niches of relief work efforts,suchasthemanagementofETUs,CCCs,orhealthinfrastructure.Divisions inUNMIL increasingly joined supporting Ebola, but itremained mostly a distant field when it came to supportingEbolasurvivors.Theregionalcoordinatedresponse increasinglyoverlapped as a proximate field with the main Liberian SAFs,resulting fromLiberia’searlypeakphase. Lastly, theESSSgrewinsizeandresourcing,whileremainingstrategicallywithinclosecoordinationwiththestateministryagencies,yetatthecenterof wheremany SAFs and proximate fields overlapped throughcoordinationmeetings.Thus,thevisibilityoftheESSSadvanced.
Key IssuesInternational funding support for the crisis reached into thebillionsofdollars.Thispledgeofaidhelpedshapeaquickenedrecovery; however, EVD rates had fallen significantly, most inpart to the learning and leadership of the original field actorsoperating on the ground since the beginning of the outbreak.Mostparticularly,underthecommandoftheExecutive,theMOHandMOG jointeffortprovided rational and legitimatedecisionmakingforstate implementers,howeverdepletinggovernmentcoffers.InPhase3(January-May2015),thestatebecameheavilyreliant on external sponsors for funding support, to build newquarantinecenters, fundETUs,hirenewstaffandback-payoldstaffwhohadrepeatedlyworkedwithoutsalary.
Innes and Booher [14] demonstrate how sponsors are crucialfor legitimacy,whichprovidedanewchallengeto thestate formaintaining its leadership.TheMOHandMOGopenednewormorefrequentdialoguethroughaseriesofcontinuousmeetingswith key donor agencies, like USAID-DART/OFDA, EU, andthe African Development Bank (ADB), for improved collectiveaction.Donorsdouble-checkedthat their funded implementersfrequently attended coordinationmeetings, aswell as have allMOUsapprovedbyMOHandCHTleadershipaspartofauditingprocedure[20].Othersimilarexamplesofcollaborationhappenedat top decisionmaking levels andwere enforced onto groundoperations. Work efforts and funding streams further alignedtowards a common vision set by the IMS members and thegovernmenttostartrecoveryeffortsandstoppocketoutbreaks(Diagram 3.1).Mostrelevanttoworkinvolvingsurvivors,theESSSwasbroughtfullyintothecenterofthekeyactionfieldsthroughcrucialstatepolicymainstreamingtheNESNLasthemainsourceofinformationflow(Diagram 3.1).
Diagram 2.2 MainFieldInformationFlowandSurvivorsafterMandate.

ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
9© Under License of Creative Commons Attribution 3.0 License
Transition of System StructureFirstly,theNESNLbecametheumbrellabodyofallthesurvivors.The state informed the other clusters like the ESA that theywould have to join the NESNL umbrella, following the electedleadershipofthenetwork,orelsedisband.Thiscreatedtensionamongstclusters,severalgroupsventedtheirresistancethroughnationalnewspapersandadvocatedforpartnersupportagainstthemandateinresponsemeetings[18].Atonepoint,confirmedauthorization was sent from the President to legitimize thisdecision by the MOH-MOG. Small pockets of unauthorizedoperationscontinuedforatime,buteventuallythegovernmenthalted them.Monthly ESSSmeetings transitioned into NESNL-facilitatedmeetingswhereitsmembershipcontinuedtoincreasebeyonditsoriginal1,500members,andfinalizedaregistryofover5,000 identified survivors by May 2015 [19,20]. Furthermore,thesemeetingsweredecentralized to county levelwithNESNLagainfacilitatingthecommunicationprocesswithMOHfunding.CountysubgroupswereestablishedundertheNESNLforsurvivorstojoinforasupportnetwork.
The central NESNL became permanently housed in the MOHand closely collaborated with MOH-MOG authorities, includingprovidingupdatereportsdailyandprovidedongoingspacetosharekey information on behalf of survivorswith all actors in the IMSandResponsePillarmeetings.All communicationswere funneledthrough the NESNL in established MOH/IMS communicationchannelsnotincreasinglyprovidingtagstoallresponseactorsaswellassurvivormembership.TheNESNLincreasinglyusedpostsonitsFacebookpagetoreachcurrentandpotentialmembers.ByMarch2015,theyreportedover2,000members.
Secondly, the social media and news campaigns championingthestoriesofsurvivorsdominatedmostoutlets,andpositionedfunding support for the ESSS as oneof the key priorities for a
fewbriefmonthsinthethirdphase.Thestateministryagenciesfurther compelled all implementers using these funds to helpsurvivorstosubmitbudgetandworkplanstotheNESNLnotonlyforapprovalthatwouldbecommunicatedbacktotheMOH,butalsotoprovidelistsofsurvivorsandaffectedfamilieswhowereconfirmedvictimsandthusapprovedforresourcesupport[23].TheNESNLcollaboratedwithlargeimplementersliketheNationalInstitutesforHealth(NIH),CDC/WHO,AcademicConsortiumtoCombatEbola inLiberia (ACCEL),andUNICEFtoestablish largescale programs with systematized operations for all registeredsurvivormembers and their families to benefit from, includingfree physical and mental health care, community awarenessbuildingbyCHT,recoverystipends,temporaryjobsandvocationaltraining,andeducationgrants[1,2,20,24].Overtime,thedecisionbytheMOH/MOGdevelopedtheESSSthroughtheNESNLintoauniformedbodywithasetboundariesandculturesofoperations.
ContentioncontinuedwithintheESSSastheNESNLformeditroleastheleadingbody.ThemaincontentioncamefromotherlargeclusterswhichweremergingundertheNESNLthattheiroriginalleadershiphaveequitablechancesatleadershippositionswithinthe future NESNL. The purpose was to help democraticallyrepresent the needs of their original membership now beingjoinedtotheNESNLroster.Thesepositionswouldplayavitalroleindeterminingwhere,howandhowmuchbenefitsandfundingwereallocatedamongsurvivorsandaffectedfamilies.ByMay2015,overadozenmajororganizationshadreportedtotheMOH/MOGtheirbudgetaryplanstodistributeover$1millionUSDaloneinfoodandnon-food items (NFI) kits, vocational training, health and mentalservices,volunteerstipendpay,etc.
Asa result, thecentralNESNLmanagement rose from4keystaffto the formalelectionof7 stablecentralpositionshousedwithintheMOH,and66delegates in11counties.ThebuildingblocksofotherMOH-supportednetworkswere repurposed for theNESNL,
Diagram 3.1 MainFieldInformationFlowandSurvivors.

10 This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
including legal policies and MOUs, as well as the establishmentof an election commission for transparency, which amelioratedcontentionamongsttheclustersforcedtocomeundertheNESNLandyetworriedaboutequitablechancesathavingtheirleadershipvotedintokeypositions.
As the third phase came to a close towards recovery efforts, therepurposing of the NESNL as the singular representative bodymoved the ESSS away from micro-perspectives that insularlyconsideredtheshort-termneedsofthesurvivorsandtransitionedtheESSStoexpanditsvisionforacoordinated,unifiedeffortinthelong-term. The NESNL measured more systematically within itsmeetingsandmonthlysurveysthecommonneedsofthesurvivors,siloed intokeyadvocacypriorities.TheNESNL furtherestablishedthefirstcoremissionandvaluesoftheESSS,establishing itselfasa union-like agency for survivors and their families, receiving andtransmitting updated information through its communicationchains,andcoordinatingamoreequitabledistributionofbenefitsforallmembers.Bytherecoveryphase,theESSSoperationsandsetprotocolshadallbuteliminateddiscordamongstclusterincumbentsandreaffirmedthestateministriesasleadfacilitatorsinpublicandprivatepartnershipsinvolvingsurvivorsandtheirfamilies.
ConclusionsCurrent state of ESSSTheESSSasanemergingsystemplayedanincreasinglyimportantfacilitationrole forhelpingsurvivors’voicestobeheardbykeyactorsinavarietyofactionfieldsthroughoutthecrisis.“Inequityisshapedbythewayeconomic,social,andpoliticalactorsviewwhat is just andwhat is not, aswell as by the relative powerof those actors and the collective choices that result. It is thejoint product of all relevant actors combined” [12]. Over thecourseofthecrisisinLiberia,itprimarilyfelluponcentralstateministryagenciestoformallycoordinateandsetpoliciesfortheESSS to respondmore systematically to the increasingneedofsurvivorsandaffectedhouseholds.Thestateagencies facedanever-changingresponseCASwithavarietyofactors,flocculatingcommunication chains, and resource and funding partnershipcomplianceissues.However,overthecourseof16months,thepriorities of survivorswhoweredisproportionately affectedbythecrisistookprecedenceamongstthemultitudeofactorswhojoinedeffortswithMOH/IMSguidance.Becauseofthis,theESSSgradually transitioned into a legitimatenetwork, authorizedbythestateastheofficialbodyorunionforEVD-affectedpersons,undertheleadershipoftheNESNL.
The NESNL functioned as the umbrella organization that clusterscameunderwhilestillmaintainingsomeautonomyasdecentralizedgroupssolongastheyreporteddirectlytotheNESNLandcompliedwith its mandates. Secondly, they had to report all identifiedsurvivors to the IMS survivor registry and at-risk disease-affectedhouseholds,particularlyvulnerablechildren,totheDivisionofChildProtection. The formal transition continued tomeetmoments ofresistancefromsomeclusters.YetthepolicyprocessthatledtotherestructuringoftheESSSintotheNESNLprovidednotablechangeindynamics,andmainstreamedmoreeffectual,timelyinformationsharing, partnership coordination, and collective action in anequitablemannerimpactingmoresurvivors.
In Liberia, this emerging system is effective in its capacitybeyondtheshort-termandmid-termgoalsoftheresponseandrecovery, but may yield sustainable action in the governmentpolicy to continue to supportEVD survivors for years to come.TheNESNL continues to operate as a formal organizationwithleadership staffed by the state. Budget constraints continuallyplaguetheNESNLeffortstomeetwithsurvivorsindecentralizedand centralized meetings. They currently utilize social mediaand news to transmit key messages to members and theirfamilies.TheNESNLwillneedtorelyonoutsidedonorsupportand implementer programs to address the changing needs ofsurvivors.
ThisnationalESSSalsoplaysasustainableactionroleoutsideofLiberia.TheNESNLmemberstravelledtoSierraLeoneandGuineato train through knowledge sharing forming survivor supportsystemsthatwerenotasadvanced.NESNL leaderscontinuetoconducttrainingsandadvocateforsurvivorsinternationally.Yet,the slowmaturationof the LiberianESSS serves as a reminderofwhatcouldhavebeenachievedhadpreviouslydocumentedsystems informed its emergence. The question remains if theESSScouldhavetransitionedbetweenphasesmorequicklyandsystematically with previous knowledge application from prioroutbreaks?
Informing future disease survivor support systemsAnestablishedDSSSbody,suchastheEbolaSurvivors’Network,canservemultiplepurposes.ExaminingtheESSSdevelopment,the response system in the future can anticipate fields ofactionsandpotentialpartnershipsatdifferentphaseswithintheresponse.
DocumentedactionrecommendationsforfutureDSSSinclude:
• Whenadiseasefirstoutbreaks,thestateandkeyhealthagencies most likely to interact with survivors shouldallocate immediate funding and human resourcing fortheestablishmentofaformalbodytotrackandorganizesurvivors.Thisactionmay includeseveralparts: formingprimary leadership; a basic IMS system with track andregistry tools for the initial DSSS linked to communitiesandETUs/quarantinecenters;clearassignedIGUrolesofspecifiedministerialdepartmentstoguideandcoordinatewith the DSSS leadership.Diagram 4 demonstrates thepotentialroleswithinanemergingDSSSstructure.
• Thestatecanthennegotiatewithagencies transitioningintostrategicactionfields,aswellaswithproximatefields,thepurposeandsystemoftheDSSS,primarilytocoordinateallocationofinitialinvestmentandprogramming.Insteadofhandlingactualbudgets,thealternativestrategyisfortheDSSStobetrainedtonavigateexternalinvestmentsbyconsultingonresourcingprioritiesandtrackingequitabledistribution amongst identifiedand registered survivors,asinthecaseoftheNESNL.
• Eventually, the DSSS (like the NESNL) may select totransition into a lead representative body that providesa safe space for sharing, advocates for survivors’ long-

ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
11© Under License of Creative Commons Attribution 3.0 License
termrecoveryandreintegration,andconsultsonannualprioritization of requested resources and programs,as the needs of survivors change over time. Thistransitionshouldconsiderhowleadershipatcentralanddecentralized levelsareselected,suchasthroughvotingor merit-based hire by government agencies, as wellas the leadership’s individual roles and responsibilities,reportingmechanisms,administrationandbudgeting,andcommunication patternswith disease survivors, donors,andimplementingagencies.
• Advocating for both state and international donors toallocateannualfundingforcost-efficientDSSSoperationswithin their budgets can sustain progress support overtime. This paper advocates for this prioritization ofcontinuedfundingfortheNESNLbyGoLandinternationalagencies, including USAID and WHO/CDC. The NESNLservesnotonlythe5,000identifiedsurvivors,butitmayalso facilitate guiding support for the estimated 25,000direct and indirect affected households in Liberiancommunitiesthatwereformerhotzones.
• Additional funding forNESNL and futureDSSSnetworkscan support regional partnerships between countriesaffectedbytheoutbreakasittransitionsintoapandemic,linkingnetworkcellstogetherforknowledgesharingandtransnational coordination. These DSSS transnationalpartnershipsincludingcollaborationbetweentheLiberianNESNL and emergent ESSS networks in Guinea andSierra Leone shouldbemaintained for two reasons: thelikelihood of the disease reemerging is high followingcurrentdiseasetrends;andsecondly,thenegativeimpactsof diseases like Ebola on affected persons and theirhouseholds continue long beyond the outbreak ends.Stigma, income, and physical and mental health issues
[16,19,25,26]. Regionally, there remain at least 10,000survivorsandtheiraffectedhouseholdsandcommunities.
• As a contingency plan, the ESSS leadership may actas consultations on the startup of a DSSS in the caseof outbreaks involving new strains of EVD or othercommunicablediseases.Thisrolemayincludesitetravelbutonlyonavoluntarybasisandunderstrictprotectionprotocols, asEVDsurvivorsmaynotbe immune tonewstrainsordiseases.Chronicdiseasesandcontagiousvirusesareonasteadyriseglobally[3],includingZika,MiddleEastrespiratorysyndrome(MERS)andsmallresurgentpocketsofEbola.Inearly2017,anewEbolaoutbreakoccurredintheDemocraticRepublicoftheCongowithconfirmedcasesand survivors of the disease. National and internationalagencies must back public health systems to improvethequalityandfrequencyofknowledgeapplicationfrompreviousoutbreaks.Forthepublichealthcommunity,thefindingsfromtheEbolaoutbreakcasewhichdemonstratehowresponsesystemsandsurvivornetworksweresetupmaybeapplied toavarietyofdifferentdiseasesand/ordisaster response situations. The foundational conceptsoftheworkoutlinedinthismanuscriptcanbeapplicablefor response to public health and humanitarian efforts,particularlyinlowresource,underservedsettings.
• TheLiberianESSSisakeycasestudyofanemergentsystemrespondingtheneedsofsurvivorsandtheirfamiliesatthemeso-level,withintheresponsecas.Sole[6]emphasizesthatwhilewecannotforeseethefuture,pastexperiencescan influencepolicyaction.Modeling theprocessunderwhichasystemundergoescancapture.Therateofchange,andpoliticalandculturalvaluesthatinfluencebonds[21].By retaining core knowledge and training through theNESNLleadership,andcarefuldocumentationoftheESSS
Diagram 4 DSSSStructure.

12 This article is available in: http://www.imedpub.com/integrative-journal-of-global-health/
ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
phases,thissystemmayserveasalearningtoolinformingmoreeffectualpolicyprocess for futureoutbreaksusingdeconcentratedprocessesbetweenthenetworkandstateministerial agencies. The ESSS offers a roadmap for aneffective DSSS, established prescriptively in anticipationofneededsurvivorservicesratherthanreactivelyastheinfectioncountgrows.
LimitationsThisresearchisaqualitativeanalysiswhichattemptstocompileathoroughtimelineoftheLiberianEbolaoutbreakandrecoveryatdifferentphases.Aspreviouslymentioned,twooftheauthorswereactivelyinvolvedintheresponse.Oneauthorhelpedintheestablishment and leads management of the ESSS throughoutits infancy into itscurrentroleattimeofdevelopingthiswork.His first-hand knowledge and recount of the ESSS formationservesas abody for this analysis. Theother authorworkedasaninternationaltechnicaladvisertotheESSSthroughoutPhases2-3, and at different times worked as a consultant with some
of the first programs utilizing Ebola survivors in ICCs, as wellas programs providing psychosocial support to survivors, theirfamilies,andcommunities.Disasterresponsesprovidechallengesto capturing timely, accurate data, as primary focus goes totargetingandisolatingtheoutbreak.Archivaldocumentswereachallengingtofindastherewerelimitedknowledgemanagementsystems in place during Phases 1-3. The authors specificallytriangulated collected information using various resources initsliteraturereview,archivalreview,andinterviewstominimizepotentialinaccuraciesandperspectivebiases.Thethirdauthorisanexpert inpublichealthand infectiousdiseaseepidemiology.This research recognizes that there are limitations in thequalitative analysis, which would have been better accountedifaccesstomorecompleteIMSmeetingnotesandreportswasfound,andmoreinterviewswithleadersofSAFscompleted.Asasecondmeasureforaccuracyandtransparency,theanalysiswasprovidedtorepresentativesattheMinistryofGenderandformerresponse coordinatorsworking in proximitywith the ESSS andEbolaprogramming.

ARCHIVOS DE MEDICINAISSN 1698-9465
2017Vol. 1 No. 2: 10
Integrative Journal of Global Health
13© Under License of Creative Commons Attribution 3.0 License
References1 CDC(2016)2014EbolaOutbreakinWestAfrica-CaseCounts.
2 CDC(2015)OutbreaksChronology:EbolaVirusDisease.
3 SokolN,OrdwayD(2016)Globaltrendsinhumaninfectiousdisease:Rising number of outbreaks, fewer per-capita cases. Journalist’sResourceoftheHarvardKennedySchool.
4 FifeBL,WrightER(2000)Thedimensionalityofstigma:AcomparisonofitsimpactontheselfofpersonswithHIV/AIDSandcancer.JournalofHealthandSocialBehaviour,pp:50-67.
5 GoffmanE(1963)Stigma:Notesonaspoiledidentity.JenkinsJH&Carpenter.
6 Sole R (2011) Phase Transitions. Princeton: Princeton UniversityPress,pp:1-5.
7 FligsteinN,McAdamD(2012)Atheoryoffields.OxfordUniversityPress.
8 HollandJ(2012)Signalsandboundaries:Buildingblocksforcomplexadaptivesystems.MITPress.
9 PageS(2011)DiversityandComplexity.PrincetonUniversityPress.
10 MinistryofHealthPsychosocialPillar(MOHPP)(2014)PsychosocialPillarMeetingSummaryNotes:September27-November1,2014.
11 Holland J (1995)Hiddenorder:Howadaptationbuilds complexity.BasicBooks.
12 Piketty T (2014) Capitalism in the Twenty-first Century. HarvardUniversityPress.
13 AlonzoAA,ReynoldsNR(1995)Stigma,HIVandAIDS:Anexplorationandelaborationofastigmatrajectory.SocialScienceandMedicine41:303-315.
14 Stokes E (2015) After Ebola outbreak, Liberia’s healthcare systemstrugglestorebound.AljazeeraAmerica.
15 InnesJ,BooherA(2010)PlanningwithComplexity:AnIntroductiontoCollaborativeRationalityforPublicPolicy.Routledge.
16 GlayweonM(2015)Interview:ESSSleaderandMOHrepresentative.Monrovia.
17 Hanson J, DecosimoA,Quinn A (2016)DiminishedQuality of LifeamongstWomenaffectedbyEbola:WorkingPaper.
18 DavisD(2014)InterviewwithEbolasurvivor,ESSSleaderandUNICEFandICCworker.Monrovia,Liberia.
19 Ziv C (2016) Interview: UNICEF communication and emergencyresponseconsultant.WashingtonDC.
20 GlayweonM,HansonJ(2015)Survivors’networksurveySummaryReport.Monrovia,Liberia.LiberianEbolaSurvivors,NetworkandtheMinistryofHealth-Liberia.
21 Ministry of Health/Information Management System (MOH/IMS)(2015)MOH/IMSMeetingSummaryNotes.
22 NicholsonDM,SchmorrowDD(2012)Advancesindesignforcross-culturalactivities.CRCPress.
23 Ministry of Gender, Children and Social Development (MOGCSD)(2014)GuidelinesforAgencies/InstitutionsImplementingChildren’sProgramsinLiberia.
24 Jackson O (2015) Ebola Survivors, Network Inaugurated. LiberianObserver.
25 NationalInstitutesforHealth(NIH)(2015)StudyofEbolaSurvivorsopen inLiberia:Trial toexamine long-termhealtheffectsofEbolavirusdisease.USDepartmentofHealthandHumanServicesNewsRelease.
26 FallahM(2016)ACohortStudyofSurvivorsofEbolaVirusInfectioninLiberia(PREVAILIII):Abstract.Boston:ConferenceonRetrovirusesandOpportunisticInfections(CROI).