Amblyopia
19
AMBLYOPIA AMBLYOPIA Dr. Christina Samuel
-
Upload
tina-chandar -
Category
Health & Medicine
-
view
146 -
download
0
Transcript of Amblyopia

AMBLYOPIAAMBLYOPIA
Dr. Christina Samuel

It implies a partial loss of sight in one or both eyes For which no cause can be detected by physical examination of the eye

PATHOPHYSIOLOGYPATHOPHYSIOLOGYAmblyopia is believed to result from
inadequate foveal or peripheral retinal stimulation and/or abnormal binocular interaction that causes different visual input from the foveae.

ClassificationClassificationStrabismicAnisometropicStimulus deprivationBilateral ametropicMeridional
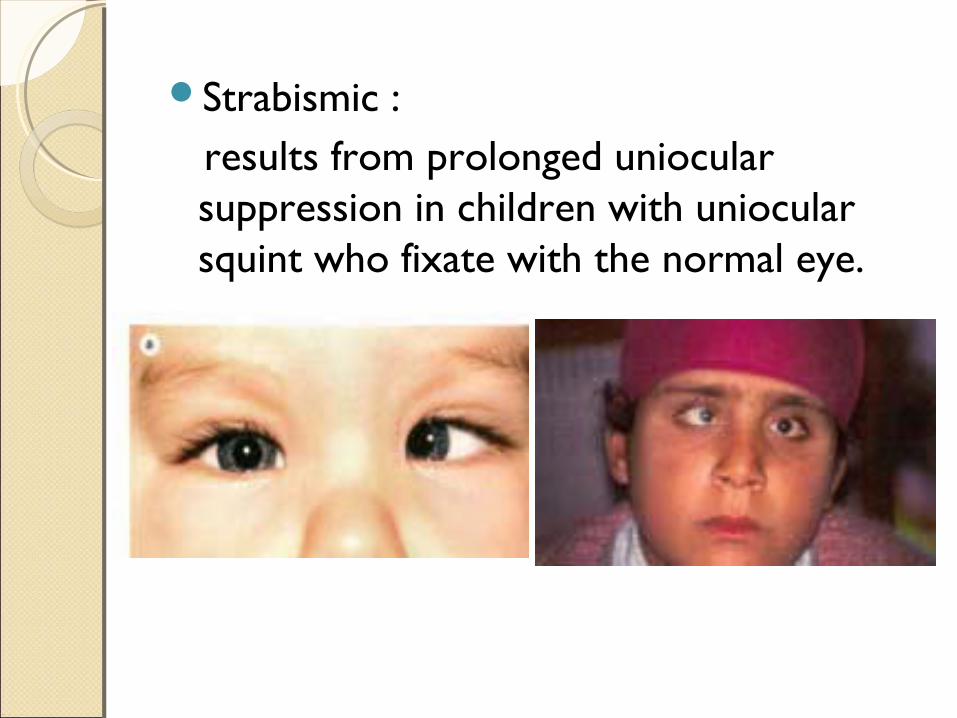
Strabismic : results from prolonged uniocular
suppression in children with uniocular squint who fixate with the normal eye.

Anisometropic:
Caused by difference in refractive error between eyes….one eye having a higher refractive error than the other eye.

Stimulus deprivation: Results from vision deprivation. When one eye is totally excluded from
seeing early in life as in congenital cataract or corneal opacities or ptosis covering the pupil.

Bilateral ametropic:
Results from high symmetrical refractive errors, usually hypermetropia.
Meridional:
Results from image blur in one meridian. It can be unilateral or bilateral and is caused by uncorrected astigmatism usually >1D persisting beyond the period of emmetropization in infancy.

DiagnosisDiagnosisClinical features VA:1. Difference of 2 lines between 2 eyes2. Crowding phenomenon: Single letter
acuity better than linear acuity• Color vision: Abnormal• Contrast sensitivity: Decreased• Stereoacuity: Decreased• ? RAPD

TreatmentTreatment
Treatment of amblyopia involves the following steps:
Eliminating (if possible) any obstacle to vision such as a cataract
Correcting refractive error Forcing use of the poorer eye by limiting
use of the better eye.

Cataract removal Cataract removal Cataracts capable of producing amblyopia
require surgery without delay.Removal of significant congenital lens
opacities during the first 2-3 months of life is necessary for optimal recovery of vision.
In symmetrical bilateral cases, the interval between operations on the first and second eyes should be no more than 1-2 weeks.
Acutely developing severe traumatic cataracts in children younger than 6 years should be removed within a few weeks of injury, if possible.

Refractive correction Refractive correction
In generally, optical prescription for amblyopic eyes should correct the full refractive error as determined with cycloplegic.
Occlusion Occlusion It is the most powerful means of treating
of amblyopia by enforced use of the defective eye.
Occlusion therapy Age to initiate treatment:
– The earlier the better
– After 6-7yrs of age, slow improvement
– Full time vs part time
Methods of occlusion:1. Direct patch over skin: Best
(completely blocks stimulus from sound eye)
2. Patch over back surface of glasses3. Occlusive contact lens for very
uncooperative children

Penalization: Penalization:
A cycloplegic agent (usually atropine 1% or homatropine 5% ) once daily to the better eye
This form of treatment has recently been demonstrated to be as effective as patching for mild to moderate amblyopia.
The time required for completion of treatment depends on the following:
1. Degree of amblyopia
2. Choice of therapeutic approach
3. Compliance with the prescribed regimen
4. Age of the patient

THANK YOUTHANK YOU