Amblyopia: The Pathophysiology Behind It and Its Treatment -The... · Amblyopia: The...
15
Amblyopia: The Pathophysiology Behind It and Its Treatment By Tamara Petroysan, O.D. Amblyopia, commonly referred to as ‘lazy eye’, affects 24% of the population and is a leading cause of unilateral vision loss in twenty to seventy year olds. , Amblyopia causes more 12 vision loss than trauma and ocular disease combined in people less than twenty years old. Despite this, there is much misinformation about the definition of amblyopia as well as its treatment. Here we will review the pathophysiology behind functional amblyopia and perform an up to date, comprehensive overview of the Amblyopia Treatment Studies (ATS) run by the Pediatric Eye Disease Investigator Group (PEDIG). Amblyopia is present when the best corrected visual acuity (BCVA) cannot reach 20/20 or 6/6. It is a mostly unilateral, but sometimes bilateral, decrease of best corrected visual acuity in the absence of any structural or pathological anomalies. Also, one or more of the below amblyogenic factors must be present before the age of six to eight years to qualify the vision loss as functional amblyopia. These factors include (1) a constant, unilateral eso or exotropia, (2) either anisometropia, bilateral isometropia, or unilateral or bilateral astigmatism of amblyogenic amount, or (3) some form of stimulus deprivation or image degradation. These amblyogenic factors 3 prevent a healthy visual pathway from forming between the eye and the brain during the critical period of neurodevelopment (08 years old), thus resulting in a decrease in BCVA. The values 4 for amblyogenic refractive error can be found in Table 1. Functional amblyopia is a diagnosis of exclusion, so if the above mentioned two conditions are not met, functional amblyopia can not be diagnosed. Sometimes other causes for vision loss such as psychological causes (malingering and hysteria) or structural and pathologic causes (nystagmus, optic atrophy, coloboma, achromatopsia, and keratoconus among others) are incorrectly classified as amblyopia. 1 Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf ]. Accessed January 11, 2015. 2 M. Khalaj, M. Zeidi, M. Gasemi1, A. Keshtkar. The effect of amblyopia on educational activities of students aged 9–15. J Biomed Sci Eng, 4 (2011), pp. 516–521 3 Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf ]. Accessed January 11, 2015. 4 Brown, S.A., Weih, L.M., Fu, C.L., Dimitrov, P., Taylor, H.R. and McCarty, C.A. (2000) Prevalence of amblyopia and associated refractive errors in an adult population in Victoria, Australia. Ophthalmic Epidemiol, 7, 249259.
Transcript of Amblyopia: The Pathophysiology Behind It and Its Treatment -The... · Amblyopia: The...

Amblyopia: The Pathophysiology Behind It and Its Treatment By Tamara Petroysan, O.D.
Amblyopia, commonly referred to as ‘lazy eye’, affects
24% of the population and is a leading cause of unilateral vision loss in twenty to seventy year olds. , Amblyopia causes more
1 2
vision loss than trauma and ocular disease combined in people less than twenty years old. Despite this, there is much misinformation about the definition of amblyopia as well as its treatment. Here we will review the pathophysiology behind functional amblyopia and perform an up to date, comprehensive overview of the Amblyopia Treatment Studies (ATS) run by the Pediatric Eye Disease Investigator Group (PEDIG).
Amblyopia is present when the best corrected visual acuity (BCVA) cannot reach 20/20 or
6/6. It is a mostly unilateral, but sometimes bilateral, decrease of best corrected visual acuity in the absence of any structural or pathological anomalies. Also, one or more of the below amblyogenic factors must be present before the age of six to eight years to qualify the vision loss as functional amblyopia. These factors include (1) a constant, unilateral eso or exotropia, (2) either anisometropia, bilateral isometropia, or unilateral or bilateral astigmatism of amblyogenic amount, or (3) some form of stimulus deprivation or image degradation. These amblyogenic factors
3
prevent a healthy visual pathway from forming between the eye and the brain during the critical period of neurodevelopment (08 years old), thus resulting in a decrease in BCVA. The values
4
for amblyogenic refractive error can be found in Table 1. Functional amblyopia is a diagnosis of exclusion, so if the above mentioned two conditions are not met, functional amblyopia can not be diagnosed. Sometimes other causes for vision loss such as psychological causes (malingering and hysteria) or structural and pathologic causes (nystagmus, optic atrophy, coloboma, achromatopsia, and keratoconus among others) are incorrectly classified as amblyopia.
1 Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf]. Accessed January 11, 2015. 2M. Khalaj, M. Zeidi, M. Gasemi1, A. Keshtkar. The effect of amblyopia on educational activities of students aged 9–15. J Biomed Sci Eng, 4 (2011), pp. 516–521 3Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf]. Accessed January 11, 2015. 4 Brown, S.A., Weih, L.M., Fu, C.L., Dimitrov, P., Taylor, H.R. and McCarty, C.A. (2000) Prevalence of amblyopia and associated refractive errors in an adult population in Victoria, Australia. Ophthalmic Epidemiol, 7, 249259.

Table 1: Amblyogenic Refractive Errors
5
Refractive Error Isometropia Anisometropia
Myopia > 8.00D > 3.00D
Hyperopia > 5.00D > 1.00D
Astigmatism > 2.50D >1.50D
The intensity of how vision is affected in amblyopia will depend on several factors such as
age of onset as well as type and severity of the amblyogenic factor. Mild amblyopia is classified as BCVA of 20/2520/40, moderate as BCVA of 20/4020/100, and severe as BCVA of 20/10020/400. The average BCVA on initial presentation is 20/50 for isometropic amblyopia,
6
20/60 for anisometropic amblyopia, 20/74 for strabismic amblyopia, and 20/94 for combined anisometropic and strabismic amblyopia. If the best corrected vision does not grossly correlate
7
with these guidelines, the diagnosis of amblyopia should be reevaluated and other causes explored further.
Table 2: Classification of BCVA in Amblyopia
Severity of Amblyopia BCVA
Mild Amblyopia 20/25 20/40
Moderate Amblyopia 20/40 20/100
Severe Amblyopia 20/100 20/400
Table 3: Expected BCVA on Initial Presentation
Types of Amblyopia Average Initial BCVA
Isometropic 20/50
Anisometropia 20/60
Strabismic 20/74
5Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf]. Accessed January 11, 2015. 6Pediatric Eye Disease Investigator Group. A comparison of atropine and patching treatments for moderate amblyopia by patient age, cause of amblyopia, depth of amblyopia, and other factors. Ophthalmology 2003;110:16328. 7 Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf]. Accessed January 11, 2015.

Combined Mechanism 20/94
Unilateral amblyopes or individuals with a milder form of amblyopia may not discover the
presence of a problem until much later in life since the ‘unaffected’ eye has seemingly good vision. Aside from a decrease in best corrected visual acuity, amblyopes may suffer from an array of associated deficits. Amblyopes will often present with associated increased sensitivity to contour
8
interaction or crowding, spatial distortions, impaired stereoacuity and abnormal binocular summation, unsteady and inaccurate monocular fixation, poor eye tracking skills, reduced contrast sensitivity, and inaccurate accommodation. Although these deficits are much more evident in
9 10
the affected eye, the ‘uninvolved’ eye has been shown to also be affected. Children with 11
amblyopia have been shown to perform poorly relative to their nonamblyopic counterparts in education, employment, sports, and socioeconomic achievement. Given the potential lack of
12 13
symptoms and the adverse effects of amblyopia on visual skills and overall development it is important that a child receive a comprehensive ocular and visual evaluation as early in life as possible. The American Optometric Association recommends that children get their first eye exam between 6 and 12 months of age.
14
Certain populations are at increased risk for amblyopia development, making it that much
more important for them to receive a comprehensive eye exam early in life. These include premature or low birth weight babies, individuals with cerebral palsy or mental retardation, and people with a family history of high refractive error, strabismus, amblyopia, or congenital cataracts.
15
8 Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf]. Accessed January 11, 2015. 9Polat U., MaNaim T., Belkin M., Sagi D. (2004). Improving vision in adult amblyopia by perceptual learning. Proc. Natl. Acad. Sci. U.S.A. 101 6692–6697 10.1073/pnas.0401200101 10 Simonis K (2005). "Amblyopia Characterization, Treatment, and Prophylaxis". Survey of Ophthalmolgy50 (2): 123–166. 11 Simonis K (2005). "Amblyopia Characterization, Treatment, and Prophylaxis". Survey of Ophthalmolgy50 (2): 123–166. 12 Rahi, J.S., Cumberland, P.M. and Peckham, C.S. (2006) Does amblyopia affect educational, health and social outcomes? Findings from 1958 British birth cohort. British Journal of Haematology, 33, 820825. 13 M. Khalaj, M. Zeidi, M. Gasemi1, A. Keshtkar. The effect of amblyopia on educational activities of students aged 9–15. J Biomed Sci Eng, 4 (2011), pp. 516–521 14 American Optometric Association. 2005. InfantSEE: a public health program for infants. [http://infantsee.org/x3445.xml]. Accessed December 27, 2014. 15 Rouse, M. et al. 2004. Care of the patient with amblyopia. [http://www.aoa.org/documents/optometrists/CPG4.pdf]. Accessed January 11, 2015.

Table 4: Overview of amblyopia
Definition of Functional Amblyopia Populations at Increased Risk
Deficits Associated with Amblyopia
BCVA less than 20/20 in one or both eyes Absence of structural or pathological causing
decrease in the BCVA Presence of one or more of the following
before 68 years Constant unilateral esotropia or
exotropia Amblyogenic anisometropia Amblyogenic bilateral isometropia Amblyogenic unilateral or bilateral
astigmatism Stimulus deprivation Image degradation
Premature birth Low birth rate Cerebral palsy Mental retardation Family history of
high refractive error, strabismus, amblyopia, or congenital cataracts
Increased sensitivity to contour interaction / crowding
Spatial distortions Impaired stereoacuity
and abnormal binocular summation
Unsteady and inaccurate monocular fixation
Poor eye tracking Reduced contrast
sensitivity Inaccurate
accommodation
A comprehensive amblyopia evaluation should include a detailed history of the patient’s
prenatal, birth and developmental history. The parent or patient should be questioned about any evident eye turns, habit of closing one eye, difficulty with depth, perceptual deficits, or difficulties in school. The ocular and visual examination should include (1) both a monocular and binocular distance and near visual acuity using a whole chart, an isolated line and an isolated letter to screen for crowding, (2) a dry and wet refraction to screen for latent hyperopia, (3) analysis of monocular fixation to screen for eccentric fixation, (4) vergence, version, and sensorimotor fusion to screen for strabismus, (5) monocular and binocular ocular motility to screen for oculomotor dysfunction, (6) accommodative amplitudes and facility to screen for accommodative dysfunction, and (7) ocular health including color vision and dilated fundus exam to screen for ocular disease or anatomical anomalies which may be the cause of the decreased visual acuity. The average expected values for accommodation and vergence testing are listed in Table 5.
Table 5: Average expected values for accommodation and vergence testing
1617
Test Average Normal Finding Distance Cover Test (DCT) orthophoria Near Cover Test (NCT) 3 exophoria
Near Point of Convergence (NPC) 5 cm / 7 cm RDS Stereopsis 20 seconds
16 Cooper, J et al. 2010. Care of the patient with accommodative and vergence dysfunction. [https://www.aoa.org/documents/CPG18.pdf]. Accessed January 2, 2015. 17 Weddell, L. 2010. Investigative techniques in binocular vision. [http://www.optometry.co.uk/uploads/articles/cetarticle_2611.pdf]. Accessed January 20, 2015.

Distance Phoria 1 exophoria Near Phoria 3 exophoria
Distance Vergence Ranges Base In: x/7/4 Base Out: 9/19/10
Near Vergence Ranges Base In: 13/21/13 Base Out: 17/21/11
Binocular Fused Cross Cylinder +0.50 Accommodative Convergence to Accommodation Ratio (AC/A) 4/1
Negative Relative Accommodation (NRA) +2.50 Positive Relative Accommodation (PRA) 3.00
Accommodative Amplitude 16 – (0.25 x age) Accommodative Facility
(+/ 2.00D lens) Monocular: 11 cpm Binocular: 8 cpm
Vergence Facility (12^BO / 3^BI) 15 cpm
Saccades Smooth and Accurate with slight undershoot
Pursuit Smooth and Accurate
To understand the pathophysiology of amblyopia we must first review the normal visual
pathway. After a visual stimulus hits the retina, both image forming and nonimage forming visual information travels via the retinal ganglion cells through the optic nerve to the optic chiasm into the optic tract and ends at the lateral geniculate nucleus (LGN) of the thalamus. The majority of the fibers will then travel from the LGN to the primary visual cortex (V1) in the occipital lobe. The
18
cortical layers above and below V1 consist of columns that respond to specific characteristics of an image. These ocular dominance columns compare input from the two eyes. Each column responds more to input from one eye or another or equally to both. The visual input then
19 20
leaves the columns and travels on to other areas of the visual cortex for further processing. 21
At birth, the foveal cones are absent. they develop over the first 24 months and continue to
mature into childhood. Thus, the formation of the ocular dominance columns relies on both 22
18 Sundsten, John W.; Nolte, John (2001). The human brain: an introduction to its functional anatomy. St. Louis: Mosby. pp. 410–447. ISBN 0323013201.OCLC 47892833. 19 Adams DL1, Sincich LC, Horton JC. Complete pattern of ocular dominance columns in human primary visual cortex. J Neurosci. 2007 Sep 26;27(39):10391403. 20 Huberman, A.D. et al. (2008) Mechanisms underlying development of visual maps and receptive fields. Annu Rev. Neurosci. 31, 479–509 21 Van Essen DC, Anderson CH, Felleman DJ. Information processing in the primate visual system: an integrated systems perspective. Science 255:419–423, 1992. 22 Vajzovic L1, Hendrickson AE. Maturation of the human fovea: correlation of spectraldomain optical coherence tomography findings with histology. Am J Ophthalmol. 2012 Nov;154(5):779789.e2. doi: 10.1016/j.ajo.2012.05.004. Epub 2012 Aug 13.

nature (guidance cues from retinal ganglion cells) and on visual experience. These synaptic 23 24
connections between the eye and the brain are either strengthened by correlated activity or weakened by uncorrelated activity. Once the initial circuit is formed, there is a critical period of time (up to 68 years old in humans) during which ocular dominance columns can be modified in response to visual experience. Monocular deprivation during the critical period results in a
25
pronounced decrease in the area of V1 representing the deprived eye and a corresponding increase in representation of the unaffected eye. If the visual system is introduced to
26 27 28 29
amblyogenic factors such as vision blur and/or binocular vision suppression, they will cause a progressive reduction of visual acuity. The vision will continue to deteriorate until the end of the critical period at which time visual acuity will stabilize.
30 31 32 33
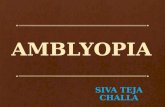
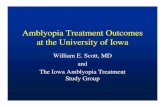
In isometropic amblyopia, the uncorrected refractive error in both eyes creates a blurred
image on both retinas. Over time, this visual blur disrupts normal neurophysiological development of the visual pathway and visual cortex causing vision blur even with optimal visual correction. In anisometropic amblyopia, the uncorrected refractive error in one eye creates a blurred image on one retina disrupting normal visual pathway development for that eye. Over time, the visual system actively starts to inhibit or suppress the blurred image causing cortical spatial changes in the ocular dominance columns that result in a loss of visual acuity. In strabismic amblyopia, each fovea receives a different image. Abnormal binocular inhibition suppresses the image from the deviated eye causing cortical spatial changes that result in a loss of BCVA as well as possible development of eccentric fixation in the deviated eye.
Image 1: Images representing (a) isometropic amblyopia, (b) anisometropic amblyopia,
and (c) strabismic amblyopia 34
23 Stellwagen D, Shatz CJ. An instructive role for retinal waves in the development of retinogeniculate connectivity. Neuron 33: 357–367, 2002. 24 Shatz, C. J. & Stryker, M. P. (1978) Ocular dominance in layer IV of the cat’s visual cortex and the effects of monocular deprivation. Journal of Physiology 281:267–83. 25 Stryker MP, Harris WA. 1986. Binocular impulse blockade prevents the formation of ocular dominance columns in cat visual cortex. J. Neurosci. 6:2117–33 26 Shatz, C. J. & Stryker, M. P. (1978) Ocular dominance in layer IV of the cat’s visual cortex and the effects of monocular deprivation. Journal of Physiology 281:267–83. 27 Crowley J.C. and Katz L.C. (2000) Early development of ocular dominance columns. Science, 290: 1321 – 1324. 28 Stellwagen D, Shatz CJ. An instructive role for retinal waves in the development of retinogeniculate connectivity. Neuron 33: 357–367, 2002. 29 Shatz, C. J. & Stryker, M. P. (1978) Ocular dominance in layer IV of the cat’s visual cortex and the effects of monocular deprivation. Journal of Physiology 281:267–83. 30 Polat, U. Functional architecture of longrange perceptual interactions. (1999) Spat. Vis. 12, 143162. 31Polat U., MaNaim T., Belkin M., Sagi D. (2004). Improving vision in adult amblyopia by perceptual learning. Proc. Natl. Acad. Sci. U.S.A. 101 6692–6697 10.1073/pnas.0401200101 32 Levi, D.M. (2006). "Visual processing in amblyopia: human studies". Strabismus 14 (1): 11–19. 33 Huberman, A.D. et al. (2008) Mechanisms underlying development of visual maps and receptive fields. Annu Rev. Neurosci. 31, 479–509 34 NASA. 1993. Hubble images of M100 before and after mirror repair. [http://dayton.hq.nasa.gov/IMAGES/LARGE/GPN2002000064.jpg]. Accessed January 20, 2015.

The goal of amblyopia treatment is to allow the amblyopic eye to improve its connection with the brain while decreasing inhibition from the sound eye. The treatment is aimed at (a) decreasing image blur which provides inadequate visual input from the eye to the brain and disrupts development and (b) at decreasing bilateral inhibition so that there is equal representation of each eye in the ocular dominance columns.
35 36 37
The Pediatric Eye Disease Investigation Group (PEDIG) is a network of optometrists and
ophthalmologists practicing in every mode of practice. The group was established in 1997 to facilitate multicenter clinical research in pediatric eye disease, including strabismus and amblyopia. The group has performed extensive research on the safety and efficacy of amblyopia treatment in the pediatric and teenage population titled the Amblyopia Treatment Studies (ATS). While there is other research available on amblyopia, the ATS studies are largescale, randomized, controlled, prospective studies that have played a critical role in rethinking amblyopia treatment and will be reviewed here.
In general and unless stated otherwise, these studies were performed on previously untreated children. A computerized singlesurround ETDRS optotype was used to measure visual acuity and the average BCVA on entrance into the study was 20/63 in the amblyopic eye. The major outcome for the studies was final visual acuity and binocular visual function was rarely evaluated. The majority of the studies performed included children 3 to less than 7 years of age. The children were provided with their optimal cycloplegic refractive correction when needed and the spectacles were updated at the following visit if a change in spectacle Rx was noted. Most studies included both moderate (20/4020/100) and severe (2010020/400) amblyopes. We are going to group the studies into separate categories as follows: (a) refractive correction alone, (b) active treatment, (c) benefit of near vision activities, (d) recurrence after treatment, (e) treatment in older children.
Refractive correction alone
35 Levi, D. M., Hariharan, S. & Klein, S. A. (2002) Suppressive and facilitatory spatial interactions in amblyopic vision. Vision Res. 42,13791394. 36 Tychsen, Lawrence (2012). "The cause of infantile strabismus lies upstairs in the cerebral cortex, not downstairs in the brainstem". Archives of Ophthalmology 130 (8): 1060–1061. 37 Shatz, C. J. & Stryker, M. P. (1978) Ocular dominance in layer IV of the cat’s visual cortex and the effects of monocular deprivation. Journal of Physiology 281:267–83.

ATS 5 looked at the effect of refractive correction alone for anisometropic amblyopes. The optimal cycloplegic correction was provided and the children were followed every 5 weeks.
38
Seventy seven percent of the children improved in BCVA by 2 or more lines while 27% of the children had a total resolution of the amblyopia with BCVA reaching 20/20. The majority of vision stabilization occurred within the first five to fifteen weeks and the chance of amblyopia resolution was higher in the moderate versus the severe group. ATS 13 evaluated the effect of refractive correction alone on strabismic and combined mechanism amblyopes. At the end of 18 weeks,
39
the amblyopia had improved by 2 or more lines in 65%, by 3 or more lines in 54%, and fully resolved in 32% of the participants. The ocular alignment had no significant effect on the final improvement in visual acuity. ATS 7 looked at the benefit of refractive correction alone for bilateral refractive amblyopes age 3 to less than 10. At the end of one year, 74% of the children achieved
40
BCVA of 20/25 or better and 60% had a 2 level improvement on the Randot preschool stereoacuity test.
These three studies show that optical treatment alone provides a significant improvement
in visual acuity and sometimes a total resolution in amblyopia of various etiology. Optimal optical correction with frequent follow ups and updates to spectacle Rx should be tried as an initial line of treatment for amblyopia. If the spectacles alone do not resolve the amblyopia, then the improved amblyopic BCVA may lead to better success and compliance with further therapy such as patching.
Active treatment
The goal of penalizing the vision in the non amblyopic eye is to either occlude the vision of
that eye fully or increase the blur of that eye beyond that of the blur of the amblyopic eye to allow normal neurodevelopment between the amblyopic eye and brain. Stick on occlusive patches that cover the whole eye are preferable since the child can not peak above or below the eyepatch and occlusion is guaranteed. Bangerter filters are transparent stick on graded foils that adhere to glasses and modulate the degree of blur by producing diffuse image defocus at all distances. Atropine produces a paresis of the accommodative system thus decreasing visual acuity. The degree of vision blur with atropine depends on the initial refraction, if the child is wearing glasses, and how close an object is. The closer the working distance, the more blur is produced since accommodation is not present to clear the image. Atropine is best used in hyperopic children since myopic children can simply remove their glasses and focus the image on the nonamblyopic eye without accommodative effort.
38 Pediatric Eye Disease Investigator Group.Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology 2006;113:895–903. 39 Pediatric Eye Disease Investigator Group. Optical Treatment of Strabismic and Combined StrabismicAnisometropic Amblyopia. Ophthalmology. 2011 Sep 28. 40 Pediatric Eye Disease Investigator Group. Treatment of bilateral refractive amblyopia in children three to less than 10 years of age. Am J Ophthalmol 2007;144:48796.

ATS 1 studied the effect of 1% daily atropine drops versus 6 hours of patching for treatment of moderate amblyopia. After 6 months, 79% of the patching and 74% of the atropine
41
group had improved by 3 or more lines or had a BCVA of better than 20/32. At the end of 2 years, this increased to 86% for the patching and 83% for the atropine group with a mean visual acuity of 20/32+ in both groups. A younger age at treatment initiation was associated with a better BCVA outcome and the atropine group reported a greater compliance with treatment. ATS 2b compared patching 2 versus 6 hours for moderate amblyopia. After 4 months, both groups had a mean
42
improvement of 2.4 lines in BCVA with the 2 hour group reporting better compliance. ATS 2a compared 6 hours versus full day patching for severe amblyopia. After 4 months, both groups
43
again had an equal improvement in BCVA of 4.8 lines with less patching having a higher compliance rate. ATS 4 compared daily atropine use to weekend only use only for moderate hyperopic amblyopia. After 4 months, both groups improved by an average of 2.3 lines. ATS 10
44
evaluated the effect of Bangerter filters versus 2 hours of patching for 3 to less than 10 year olds. The vision was first stabilized with cycloplegic refraction and after 24 weeks average
45
improvement was 2.3 lines in the patching group and 1.9 lines in the filter group. The second portion ATS 5 looked at the benefit of patching 2 hours a day for moderate
and severe anisometropic and strabismic amblyopia after first stabilizing the BCVA with spectacles. After stabilizing the BCVA with an optimal cycloplegic Rx (usually 16 weeks), the
46
treatment group was patched for 2 hours per day with an hour of near activities versus spectacle Rx alone with an hour of near vision activities. After 5 weeks, the patching group improved by an extra 2.2 lines versus the control group which improved by 1.3 lines. ATS 15 evaluated the effectiveness of increasing daily patching from 2 to 6 hours in children with stable residual amblyopia (20/3220/160) after previously undergoing patching for 2 hours/day . After ten weeks,
47
the average BCVA in the treatment group improved by 1.2 lines versus 0.50 lines in the control group. Forty percent of the treatment group improved by 2 or more lines versus 18% of the control. ATS 8 evaluated atropine plus optical penalization for treating moderate hyperopic amblyopes. After BCVA stabilization with specs, both groups received weekend atropine in the non amblyopic eye. The treatment group received glasses with a plano distance lens for their nonamblyopic eye, effectively blurring them at all distances. The control received their proper
41 Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Arch Ophthalmol 2002;120:26878. 42 Pediatric Eye Disease Investigator Group. A randomized trial of patching regimens for treatment of moderate amblyopia in children. Arch Ophthalmol 2003;121:60311. 43 Pediatric Eye Disease Investigator Group. A randomized trial of patching regimens for treatment of severe amblyopia in children. Ophthalmology 2003;110:207587. 44 Pediatric Eye Disease Investigator Group. A randomized trial of atropine regimens for treatment of moderate amblyopia in children. Ophthalmology 2004;111:207685. 45 Pediatric Eye Disease Investigator Group. A randomized trial comparing Bangerter filters and patching for the treatment of moderate amblyopia in children. Ophthalmology 2010;117(5):9981004. 46 Pediatric Eye Disease Investigator Group. A randomized trial to evaluate 2 hours of daily patching for strabismic and anisometropic amblyopia in children. Ophthalmology 2006;113:904–12. 47 Pediatric Eye Disease Investigator Group. A randomized trial of increasing patching for amblyopia. Ophthalmology 2013 Nov;120(11):22707. Epub 2013 Jun 4

vision correction for distance, leaving them blurred only at near. At the end of 18 weeks, the treatment group improved by 2.8 lines versus 2.4 lines in the control group.
These penalization studies show that both patching and atropine, and to a slightly lesser
effect Bangerter filters, are effective options for treating amblyopia. Optimal improvement can be made if the BCVA is first stabilized via refractive correction and then penalization is initiated for residual visual acuity deficits. If there is residual amblyopia after the active treatment regimen, an increase in patching time or adding optical penalization to atropine may provide further improvement in BCVA.
Benefit of near activities ATS 6 evaluated the benefit of prescribing common, at home near activities during
patching regimens to enhance improvement in visual acuity. After BCVA stabilization with specs the children were patched 2 hours/day at home and performed either common eyehand coordination activities at near or either activities 6 feet away or outdoor play. At the end of 8 weeks, both the distance and near activity groups improved by 2.5 lines. The results were statistically similar at 17 weeks. While refractive correction and penalization may improve the BCVA, they do not provide treatment for all aspects of vision impacted by amblyopia, including binocularity.
A study evaluating doctor supervised vision training would be recommended to further
evaluated the benefit of vision therapy for amblyopia treatment. ATS 12, a study terminated in 2009 due to lack of subject participation, was to look at the effectiveness of patching with active vision therapy versus patching with control vision therapy. ATS 18 started recruiting in 2014 to compare the effectiveness of 1 hour/day of binocular game play with 2 hours/day of patching in children 5 to < 13 years of age.
48
Recurrence after treatment
ATS 2c evaluated the recurrence of amblyopia in previously successfully treated patients.
The children were treated with either atropine or patching and then discontinued treatment and monitored. At the end of one year, 76% had no decrease in BCVA while 24% had a 2 or more line loss in BCVA. The decrease in BCVA was equal in both the patching and atropine groups. For subjects patched 6 to 8 hours/day, the recurrence was increased to 42% if the treatment was abruptly discontinued. If the treatment was first decreased to 2 hours/day for several weeks and then discontinued, the chance of recurrence decreased to 14%. In the group that had recurrence,
48 Pediatric Eye Disease Investigator Group. 2015. Study of binocular computer activities for treatment of amblyopia. [http://pedig.jaeb.org/Studies.aspx?RecID=235]. Accessed January 20, 2015

76% occurred within the first 3 to 6 months. Neither ocular alignment nor level of stereoacuity were protective factors against recurrence.
Treatment in older children
ATS 9 compared vision stabilization with spectacles followed by weekend atropine versus
2 hours of patching for moderate amblyopes age 7 to 12. After 17 weeks, the visual acuity improved by 7.6 letters in the atropine group and 8.6 letters in the patching group. ATS 3 evaluated the benefit of amblyopia treatment for children 718. The control group received optimal refractive correction only while the study group received refractive correction plus either patching (2 to 6 hours) or weekend atropine. A positive response was considered an improvement of 2 lines in BCVA after 24 weeks. In the 712 year group, 53% of the treatment and 25% of the glasses group had a positive response. In the 1317 year group, 25% of the treatment and 23% of the glasses group had a positive response. If the teenage group was further evaluated, in children who had no previous treatment, 47% of the treatment and 20% of the optical only group showed a positive response. The study then went on the evaluate the chance of recurrence after a year without treatment where only 5% of the patients had a decrease in BCVA of 2 or more lines.
These studies show that a child’s age is not a limiting factor for amblyopia treatment. This
is likely due to the neuroplasticity of the brain. Treatment should be initiated in older children, especially if they have never received previous treatment. Further well controlled, prospective studies are needed to evaluate the benefit of amblyopia treatment in adults.
Table 6: Overview of Amblyopia Treatment Studies
Study Number Study Goal Study Outcomes
ATS 5 effect of refractive correction alone for anisometropic amblyopes
77% of the children improved in BCVA by 2 or more lines 27% of the children had a total resolution the majority of vision stabilization occurred within the first 515 weeks the chance of amblyopia resolution was higher in the moderate vs. severe group
ATS 13 effect of refractive correction alone on strabismic and combined mechanism amblyopes
amblyopia improved by 2 or more lines in 65%, by 3 or more lines in 54%, and fully resolved in 32%

ocular alignment had no significant effect on the final improvement in visual acuity
ATS 7 benefit of refractive correction alone for bilateral refractive amblyopes
74% achieved BCVA of 20/25 or better 60% had a 2 level improvement on the Randot preschool stereoacuity test
ATS 1 effect of 1% daily atropine drops versus 6 hours of patching for treatment of moderate amblyopia
after 6 months, 79% of the patching and 74% of the atropine group had improved by 3 or more lines or had a BCVA of better than 20/32. after 2 years, this increased to 86% of the patching and 83% of the atropine group had improved by 3 or more lines or had a BCVA of better than 20/32 a younger age at treatment initiation was associated with a better BCVA outcome Atropine group reported greater compliance with treatment
ATS 2b compared patching 2 versus 6 hours for moderate amblyopia
at 4 months, both groups had a mean improvement of 2.4 lines in BCVA 2 hour group reported better compliance
ATS 2a compared 6 hours versus full day patching for severe amblyopia
at 4 months, both groups had a mean improvement in BCVA of 4.8 lines 6 hour group reported better compliance
ATS 4 compared daily atropine use to weekend only use only for
at 4 months, both groups improved by an average of 2.3 lines

moderate hyperopic amblyopia
ATS 10 effect of Bangerter filters versus 2 hours of patching
after 24 weeks of BCVA stabilization with optical correction, average improvement of 2.3 lines in the patching group and 1.9 lines in the filter group
ATS 5 (second portion) benefit of patching 2 hours a day for moderate and severe anisometropic and strabismic amblyopia
after 16 weeks of BCVA stabilization with optical correction the patching group improved by an extra 2.2 lines versus spectacle only group which improved by 1.3 lines
ATS 15 evaluated the effectiveness of increasing daily patching from 2 to 6 hours in children with stable residual amblyopia
after ten weeks, the average BCVA in the treatment group improved by 1.2 lines versus 0.50 lines in the control group 40% of the treatment group improved by 2 or more lines versus 18% of the control
ATS 8 evaluated atropine plus optical penalization for treating moderate hyperopic amblyopes
at the end of 18 weeks, the treatment group improved by 2.8 lines versus 2.4 lines in the control group
ATS 6 benefit of prescribing common, at home near activities during patching regimens to enhance improvement in visual acuity
at the end of 8 weeks, both the distance and near activity groups improved by 2.5 lines
ATS 2c evaluated the recurrence of amblyopia in previously successfully treated patients
at the end of one year, 76% had no decrease in BCVA while 24% had a 2 or more line loss the decrease in BCVA was equal in both the patching and atropine groups

for the group patched 6 to 8 hours/day, the recurrence was increased to 42% if the treatment was abruptly discontinued. If the treatment was first decreased to 2 hours/day for several weeks and then discontinued, the chance of recurrence decreased to 14% in the group that had recurrence, 76% occurred within the first 3 to 6 months. neither ocular alignment nor level of stereoacuity were protective factors against recurrence
ATS 9 compared vision stabilization with spectacles followed by weekend atropine versus 2 hours of patching for moderate amblyopes age 712
after 17 weeks, the visual acuity improved by 7.6 letters in the atropine group and 8.6 letters in the patching group
ATS 3 evaluated the benefit of active amblyopia treatment for children 718
in the 712 year group, 53% of the treatment and 25% of the glasses group had a positive response in the 1317 year group, 25% of the treatment and 23% of the glasses group had a positive response in children who had no previous treatment, 47% of the treatment and 20% of the optical only group showed a positive response 5% of the patients had a decrease in BCVA of 2 or more lines after one year of no treatment

In conclusion, amblyopia is a diagnosis of exclusion and has strict guidelines which should
be followed when making the diagnosis. When considering initiating amblyopia treatment, it is important to include the parent and/or patient in the decision making process. All treatment options, including their risks, benefits, and alternatives, and expectations should be discussed and a treatment plan that best fits each individual patient should be formulated. While early intervention is ideal, with appropriate management and treatment amblyopia patients are likely obtain a successful outcome, and possibly full resolution, no matter their age. Patients should be monitored closely and frequently during and after amblyopia treatment to allow for treatment modification as needed and to watch for amblyopia recurrence. While optical correction alone can resolve amblyopia, active treatment through penalization or combining different treatment methods can further improve visual acuity in residual amblyopia. Further studies are needed to evaluate the benefit of active in office or home vision training for amblyopia treatment as well as its associated deficits.
____________________________________________________________________________ About our Author
Dr. Tamara Petrosyan graduated with honors from the State University of New York (SUNY) College of Optometry in 2009 and went on to do a residency in vision rehabilitation, head trauma, low vision, and ocular disease at the Northport VA Medical Center. In 2011 she joined the faculty at the SUNY College of Optometry where she precepts third and fourth year interns in the primary care, adults with disabilities, and pediatric units. Dr. Petrosyan also supervises primary care and ocular disease interns and residents at the East New York Diagnostic and Treatment Center in Brooklyn, NY. From 20122014 Dr. Petrosyan was on staff at the Refuah Health Center where she performed direct care pediatric and adult exams and vision therapy training. Dr. Petrosyan is currently on the board of directors for the New Jersey Society of Optometric Physicians (NJSOP) and is the chair of both the vision therapy and infant vision clinical care committees of NJSOP. She is also the coordinator of the NJSOP Young O.D. program and has helped develop NJSOP mentorship program. Dr. Petrosyan is the recipient of the 2013 NJSOP Chairperson of the Year Award, 2014 NJSOP Young O.D. of the Year Award, 2015 AOA Young O.D. of the Year Award, and the 2015 NJSOP Optometric Journalism Award. She lives in New Jersey with her husband and three children. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means (electronic, mechanical, photocopying, recording, or otherwise) without the prior written permission of the publisher. Copyright© 2016 by The American Optometric Association