Amblyopia mahmuda - copy
46
AMBLYOPIA & ITS INVESTIGATION Mahmuda Akter B.optom, 3 rd year Institute of Community Ophthalmology University of Chittagong
-
Upload
zarin45 -
Category
Health & Medicine
-
view
146 -
download
0
Transcript of Amblyopia mahmuda - copy
AMBLYOPIA& ITS INVESTIGATION
Mahmuda Akter
B.optom, 3rd year
Institute of Community Ophthalmology
University of Chittagong

What is Amblyopia?
Unilateral or less commonly bilateral reduction of the best corrected visual acuity that cannot be attributed directly to the effect of any structural abnormality of the eye & the posterior visual pathways.
It is also called lazy eye.

Normal vision Amblyopia ( Loss of vision)

Pathogenesis
Amblyopia is produced by certain amblyogenic factors operating during the cortical period of visual development.
The most sensitive period for development of amblyopia is first 6 months of life & it usually does not develop after the age of 8 years.
PATHOPHYSIOLOGY

ROLE OF RETINA IN THE DEVELOPMENT OF AMBLYOPIA
Decreased sensitivity of foveal cones in amblyopia
The reduced input from rods and cones in the affected eye causes certain neurophysiologic changes, transmitted to the Central Nervous System which triggers amblyopia.
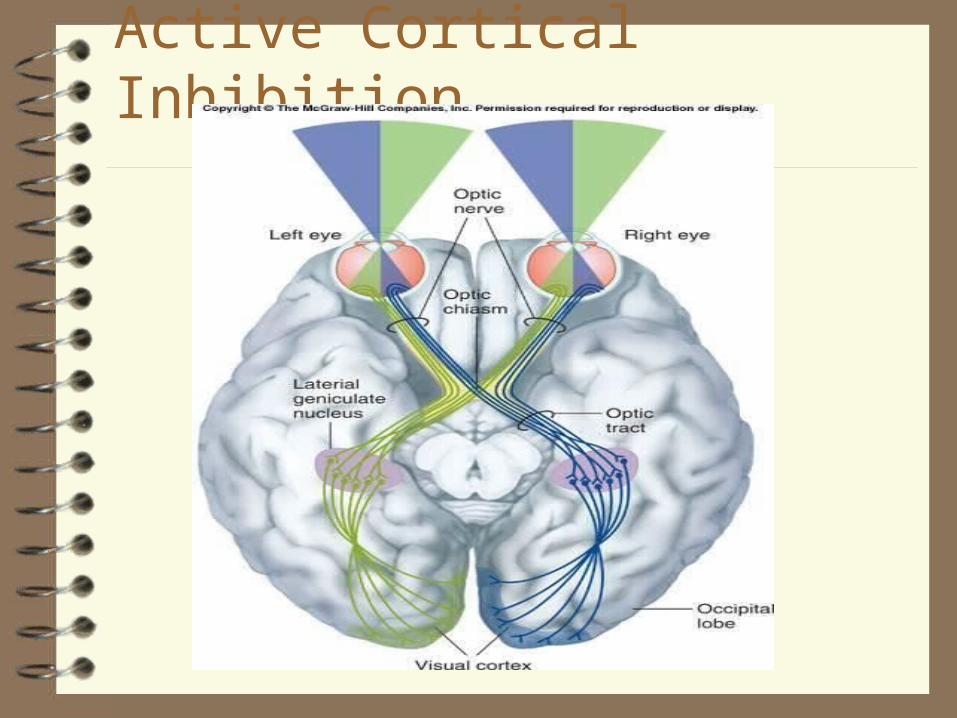
Active Cortical Inhibition
A developmental defect of spatial visual processing occurring in the visual pathway.
Poor transmission from the fovea, optic nerve to the Striate Cortex of the affected eye.
Lateral Geniculate Body & Striate cortex develop abnormally.
Ganglion cells in foveal area are affected; Shrinkage of LGB Nucleus & Striate cortical fibres in the amblyopic eye.
Loss of binocularly driven cells in LGB & Striate Cortex

How does it happen?

What causes of amblyopia? There are four major causes of amblyopia
which are:
1)Unequal/Poor visual acuity Unequal refractive error (Anisometropia)
Bilateral equal high refractive errors (isoametropia)
Uncorrected moderate/high astigmatism
2)Strabismus/Misaligned Eyes
3) Blockage or deprivation
4) Toxic
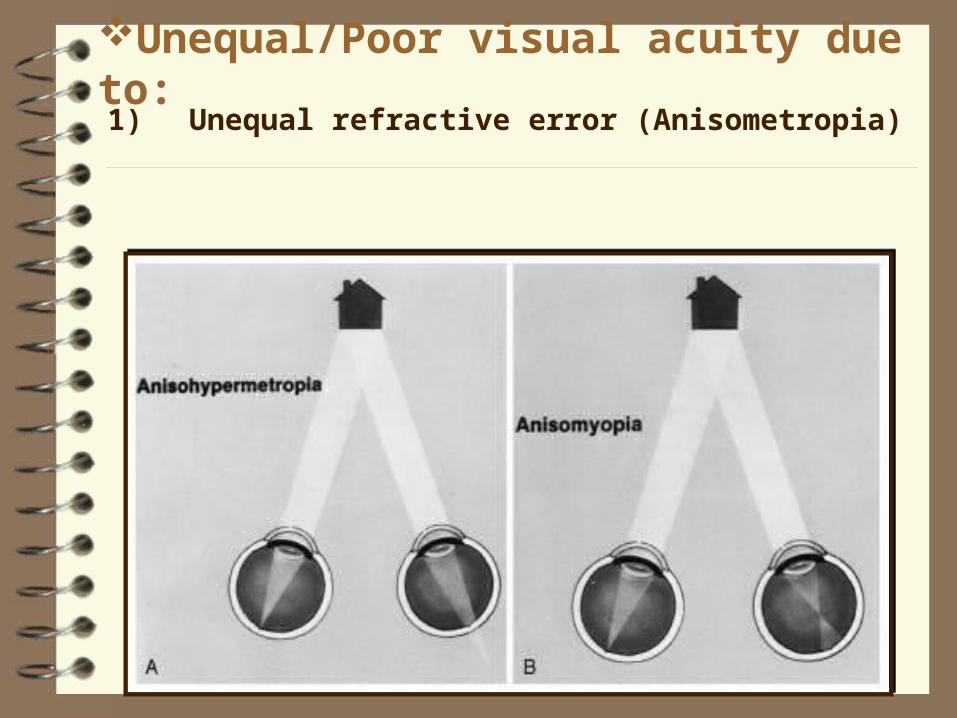
Unequal/Poor visual acuity due to: 1) Unequal refractive error (Anisometropia)
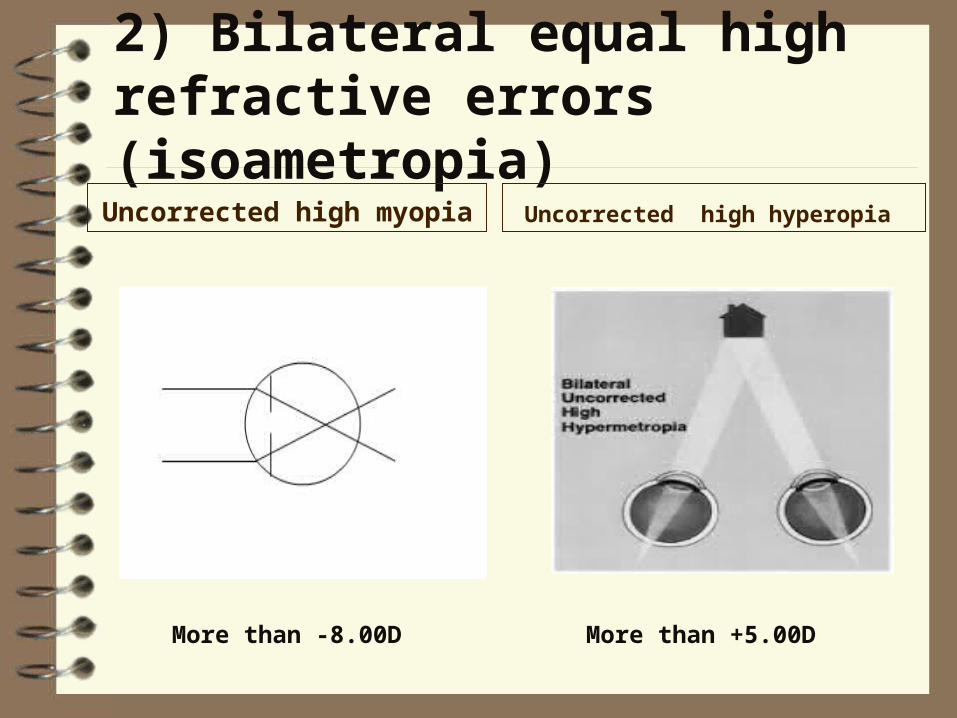
2) Bilateral equal high refractive errors (isoametropia)Uncorrected high myopia Uncorrected high hyperopia
More than -8.00D More than +5.00D
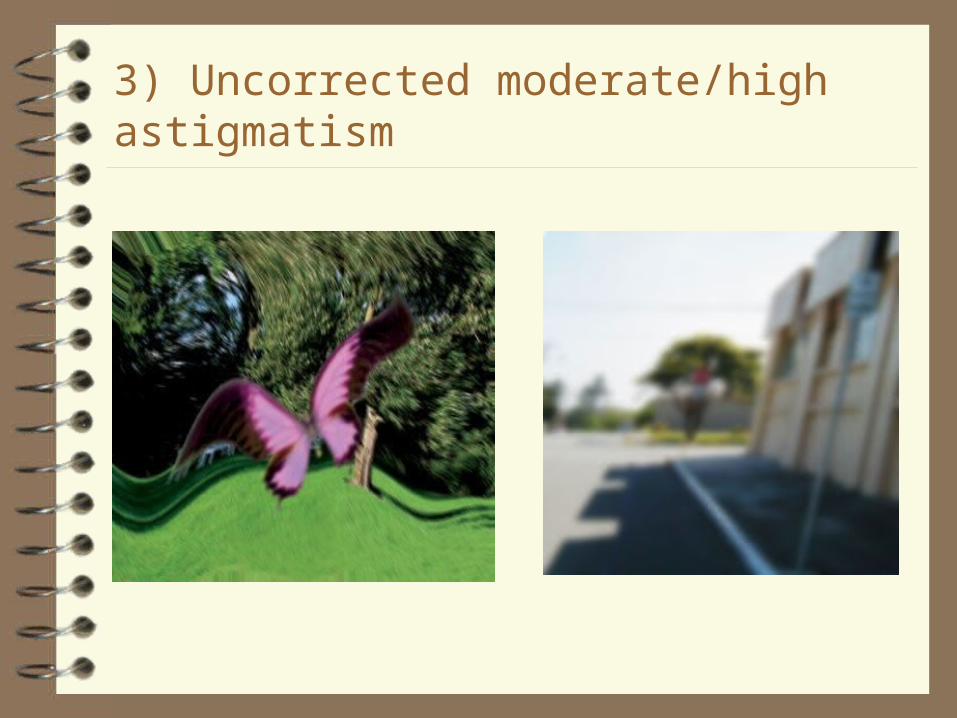
3) Uncorrected moderate/high astigmatism

A Compound myopic
B Simple myopic
C Mixed astigmatism
D Simple hyperopic
E Compound hyperopic
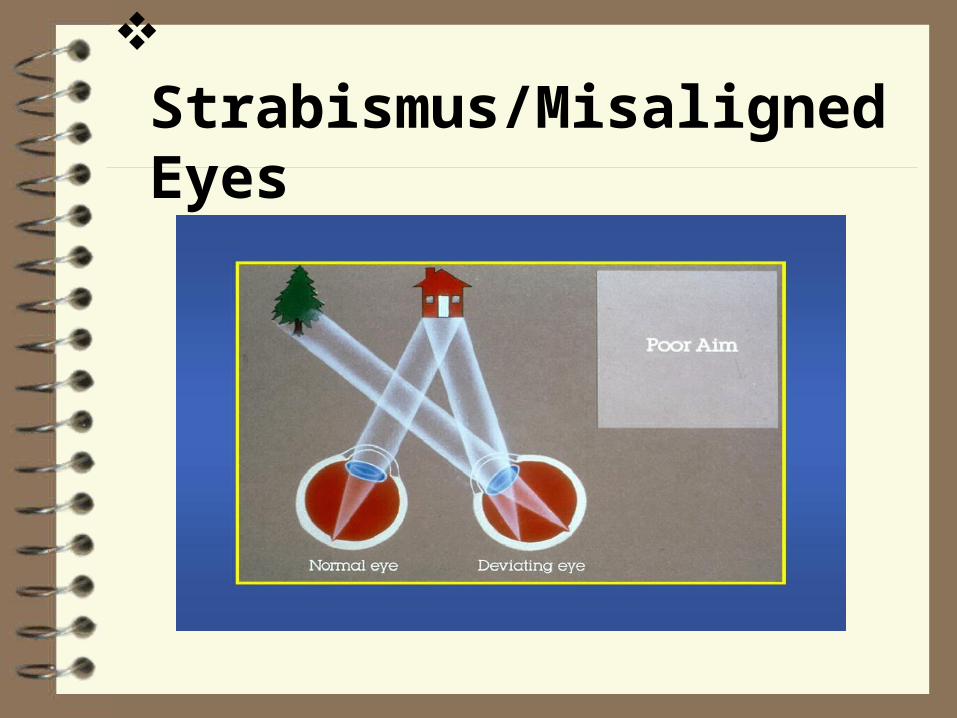
Strabismus/Misaligned Eyes
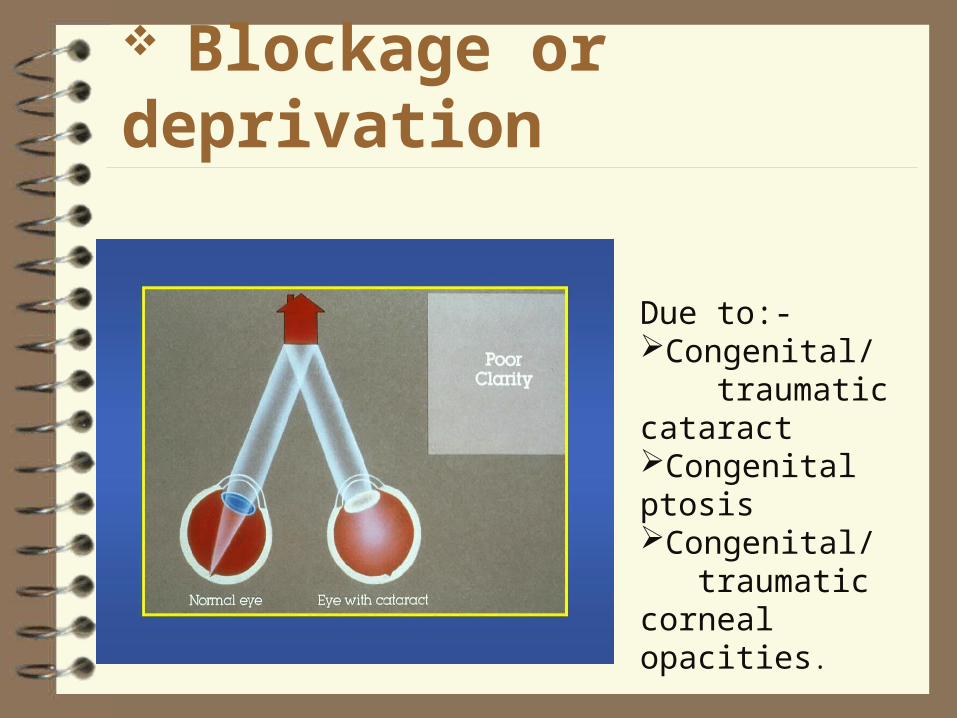
Blockage or deprivation
Due to:-Congenital/ traumatic cataract Congenital ptosisCongenital/ traumatic corneal opacities.
Toxic Drugs – Quinine,ethambutol
Tobacco- pipe smokers, excessive drinkers
Alcohol- Methyl & Ethyl alcoholic
Chemicals- Lead, methanol
Nutritional disorders - such as lack of vitamin A and zinc.
The optic nerve head in acquired optic neuropathies
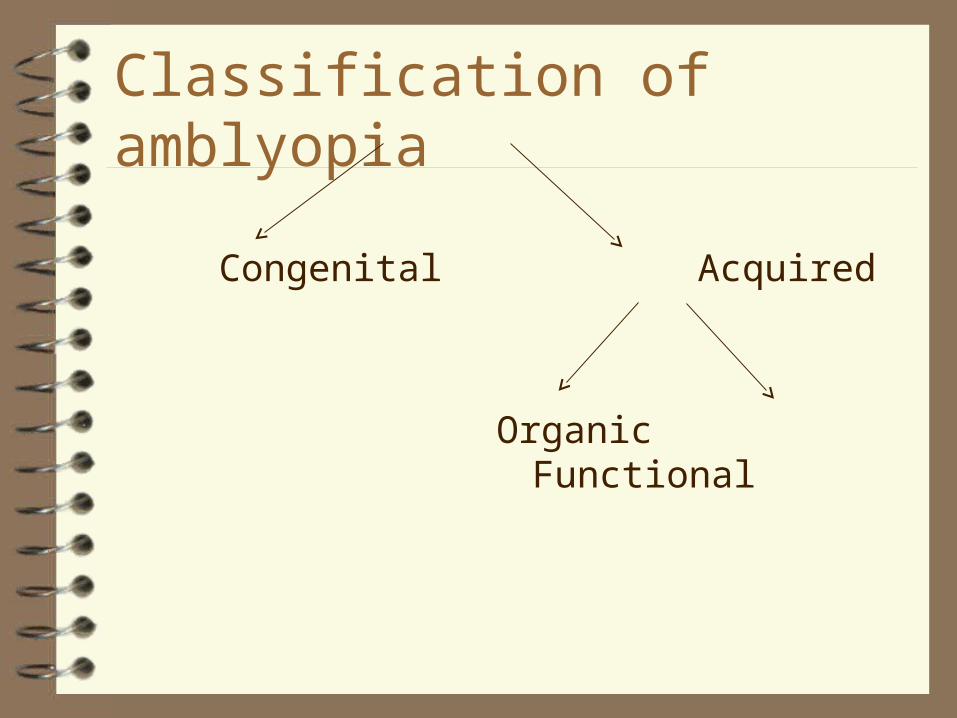
Classification of amblyopia
Congenital Acquired
Organic Functional
Congenital Amblyopia
It is irreversible type. It may occurs due to:- Central nervous system disorder Carebral palsyCongenital cataractDevelopmental delayRetinopathy of prematurityMal orientation of the retinal receptors
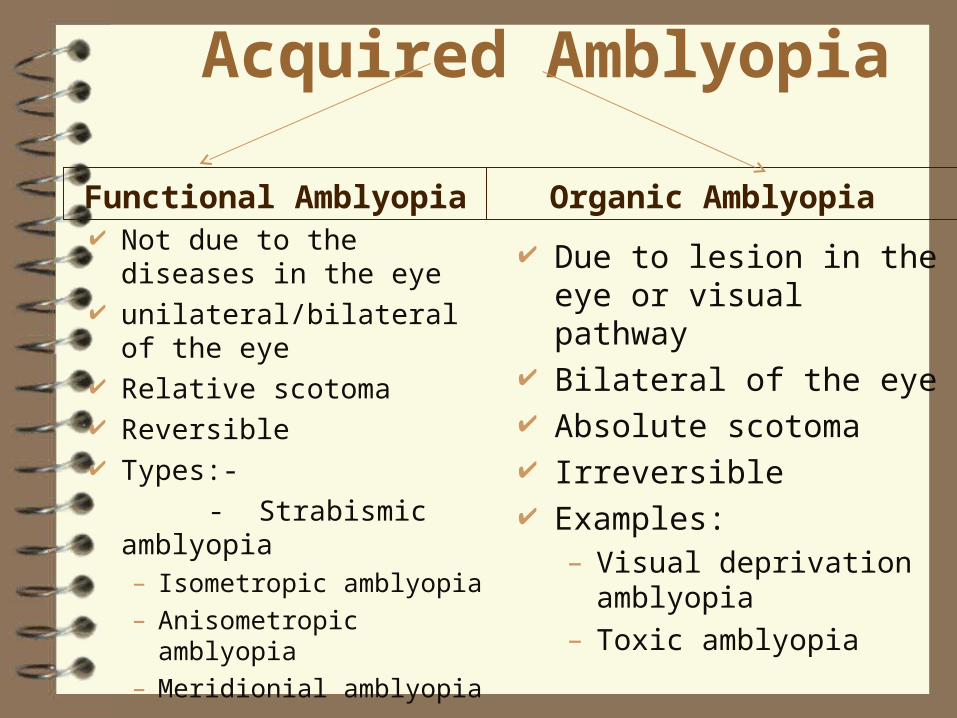
Acquired Amblyopia
Functional Amblyopia Not due to the diseases
in the eye unilateral/bilateral of
the eye Relative scotoma Reversible Types:- - Strabismic
amblyopia– Isometropic amblyopia– Anisometropic
amblyopia– Meridionial amblyopia
Organic Amblyopia
Due to lesion in the eye or visual pathway
Bilateral of the eye Absolute scotoma Irreversible Examples:
– Visual deprivation amblyopia
– Toxic amblyopia
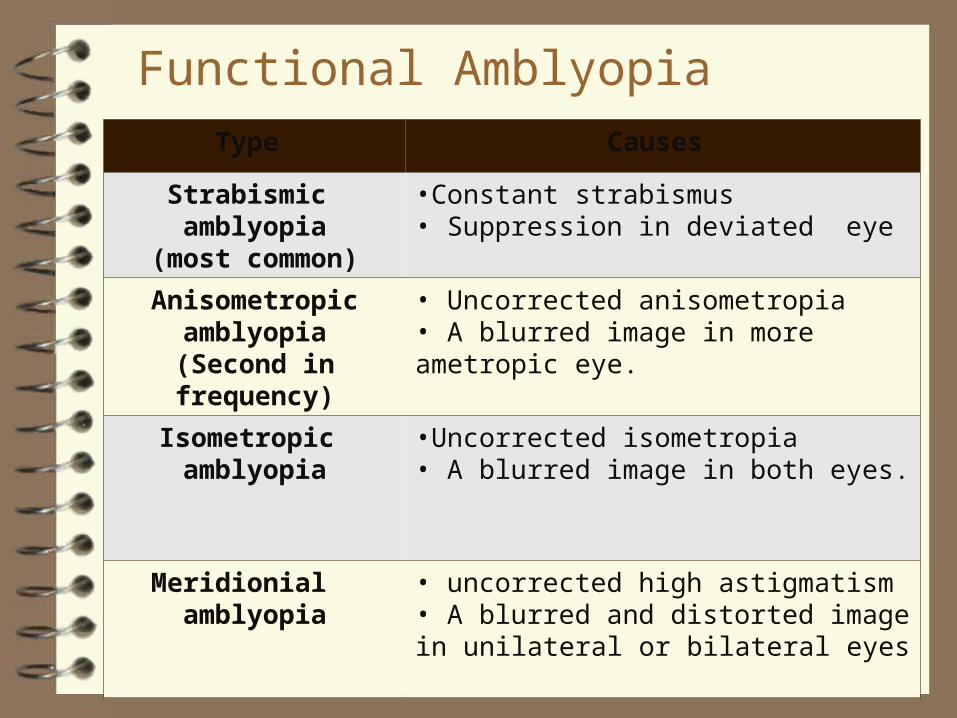
Functional AmblyopiaType Causes
Strabismic amblyopia(most common)
•Constant strabismus• Suppression in deviated eye
Anisometropic amblyopia
(Second in frequency)
• Uncorrected anisometropia• A blurred image in more ametropic eye.
Isometropic amblyopia •Uncorrected isometropia • A blurred image in both eyes.
Meridionial amblyopia • uncorrected high astigmatism• A blurred and distorted image in unilateral or bilateral eyes
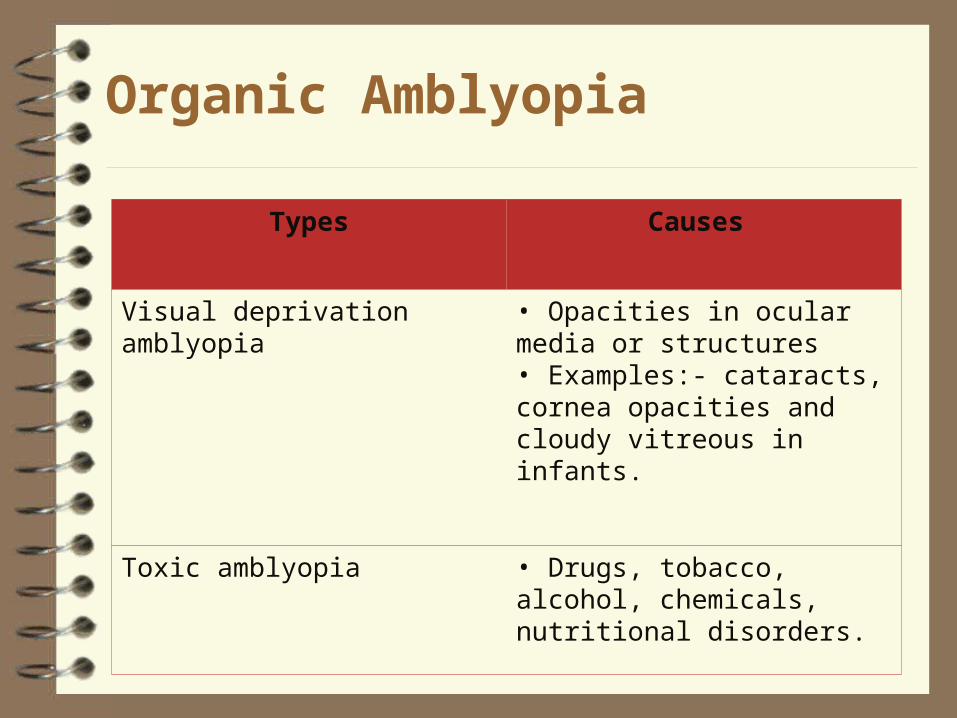
Organic Amblyopia
Types Causes
Visual deprivation amblyopia • Opacities in ocular media or structures• Examples:- cataracts, cornea opacities and cloudy vitreous in infants.
Toxic amblyopia • Drugs, tobacco, alcohol, chemicals, nutritional disorders.

What are the sign and symptoms of amblyopia?
Symptoms Blurred vision Reduced vision Reduced contrast
sensitivity
Signs No obvious sign,
unless severe abnormality is present.
Rubbing or squinting of eyes
Misaligning eyes Reduced Visual Acuity Droopy eyelid
Investigation of Amblyopia
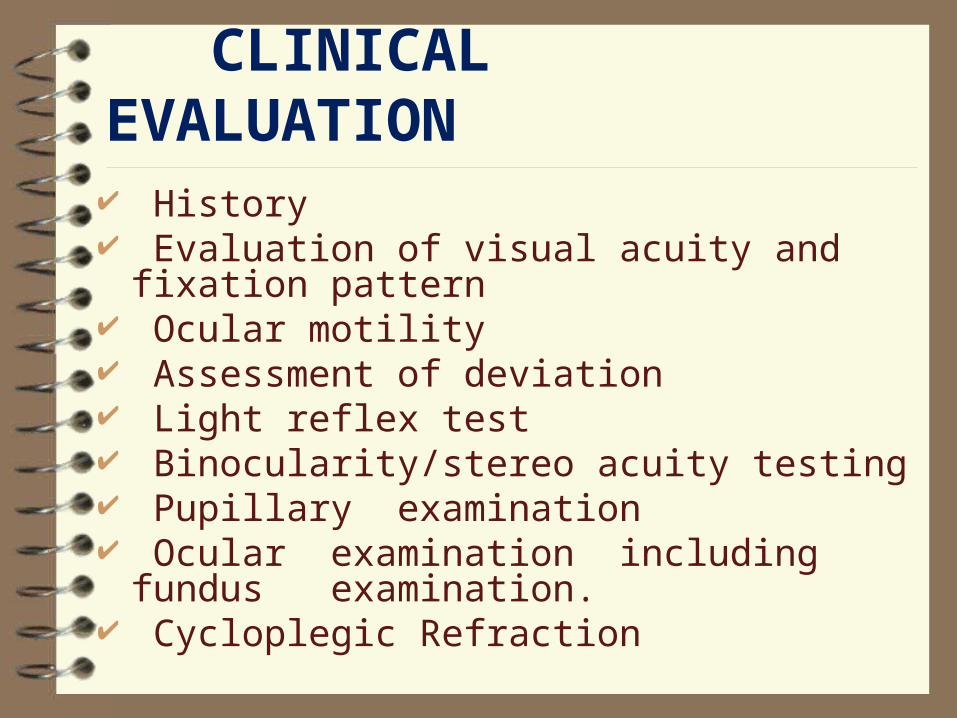
CLINICAL EVALUATION
History Evaluation of visual acuity and fixation pattern Ocular motility Assessment of deviation Light reflex test Binocularity/stereo acuity testing Pupillary examination Ocular examination including fundus
examination. Cycloplegic Refraction
2.Strategies in assessment of amblyopia
1. Visual Acuity (VA)
Degree of amblyopia Crowding
phenomena– Normal Snellen
Chart• Line Acuity
– Single Letter Chart• Single Letter Acuity
2. Neutral Density (ND) Filter
Depth of amblyopia Differentiate
between organic amblyopia or functional amblyopia
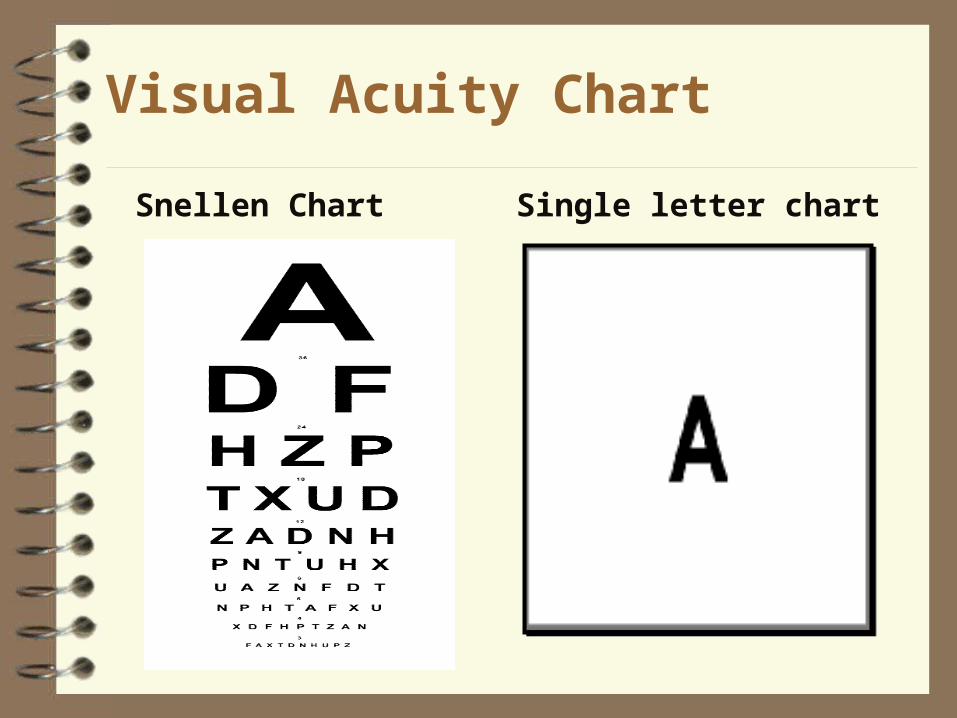
Visual Acuity Chart
Snellen Chart Single letter chart
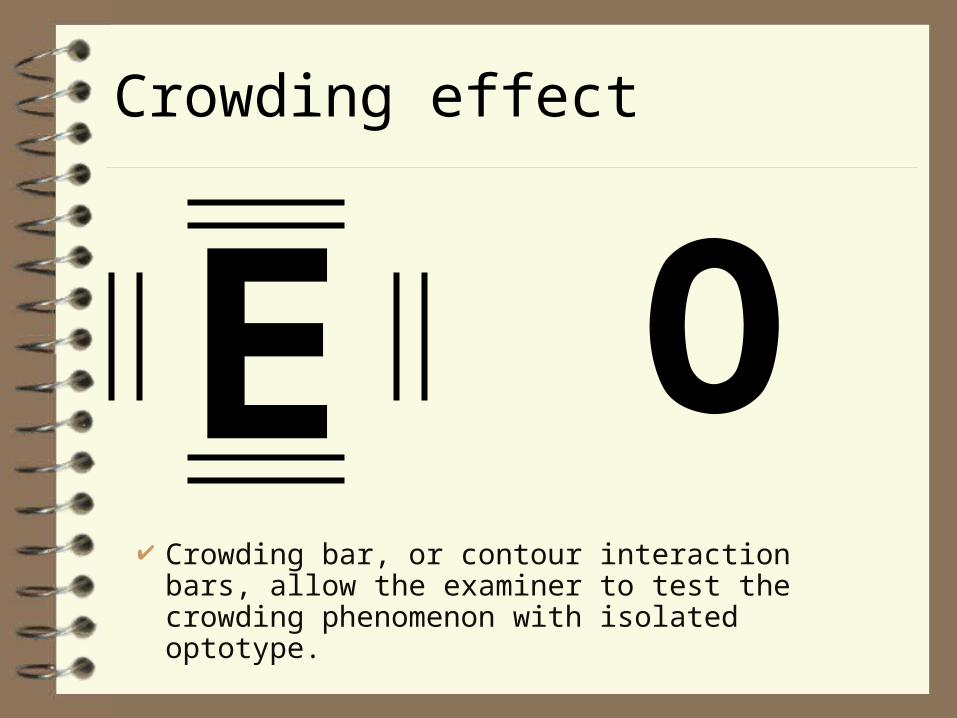
Crowding effect
Crowding bar, or contour interaction bars, allow the examiner to test the crowding phenomenon with isolated optotype.
E O
1. Visual Acuity (VA)
Amblyopes perform better when isolated letters are used instead of full chart.
Crowding effectSingle letter acuity
InfantTeller acuity chart
Preschool-aged childrenLea symbols, HOTV chartBroken wheel cards
School-aged childrenSnellen chart Log MAR chart
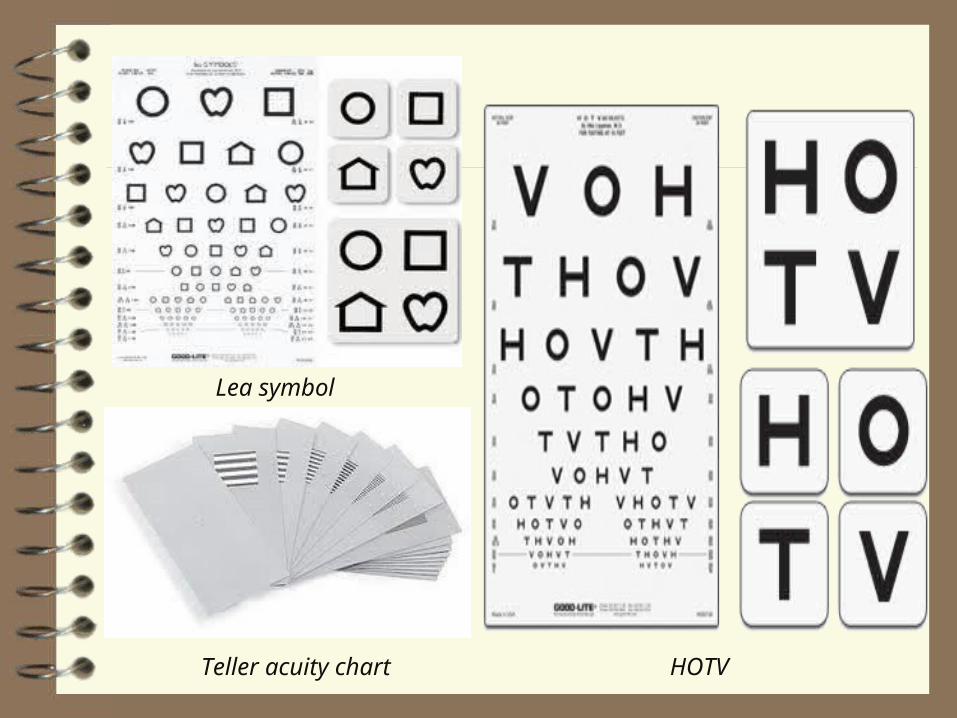
Teller acuity chart HOTV
Lea symbol
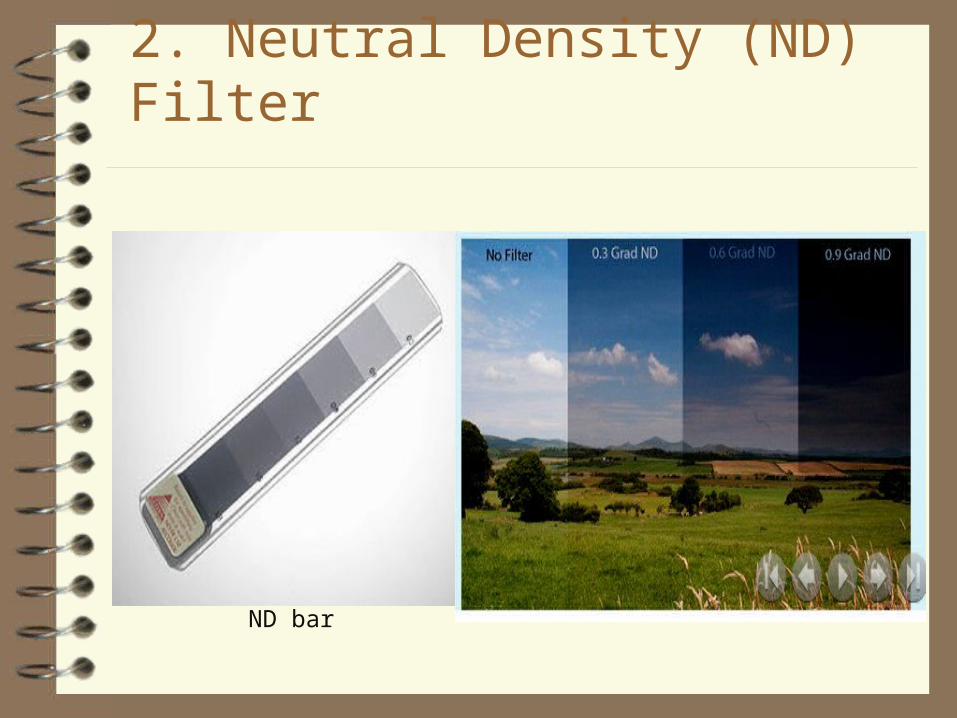
2. Neutral Density (ND) Filter
ND bar
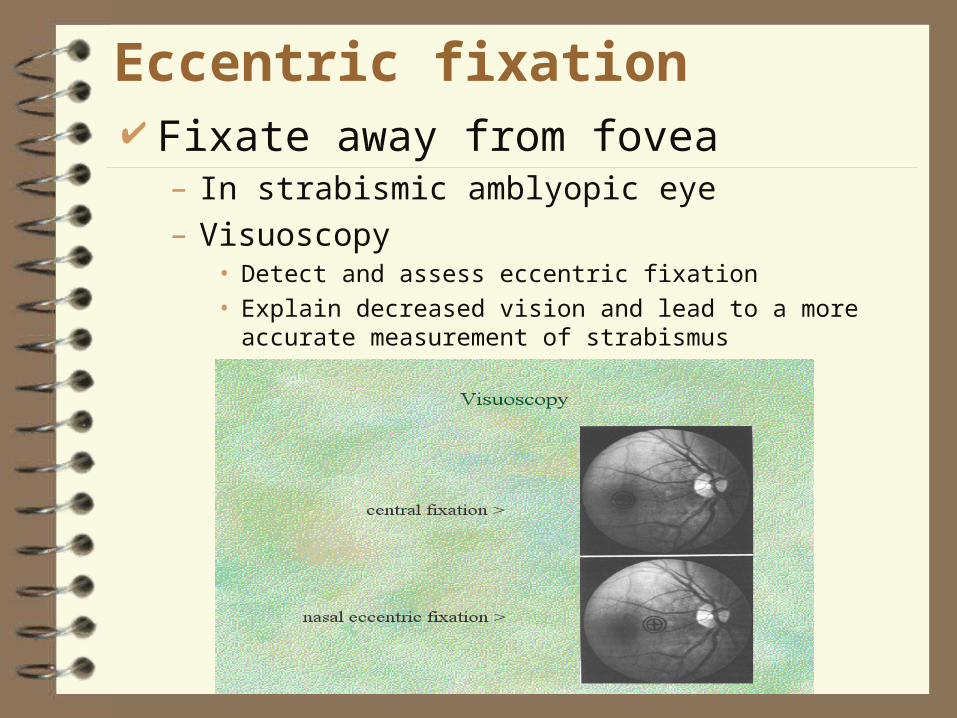
Eccentric fixation Fixate away from fovea
– In strabismic amblyopic eye– Visuoscopy
• Detect and assess eccentric fixation• Explain decreased vision and lead to a more accurate
measurement of strabismus
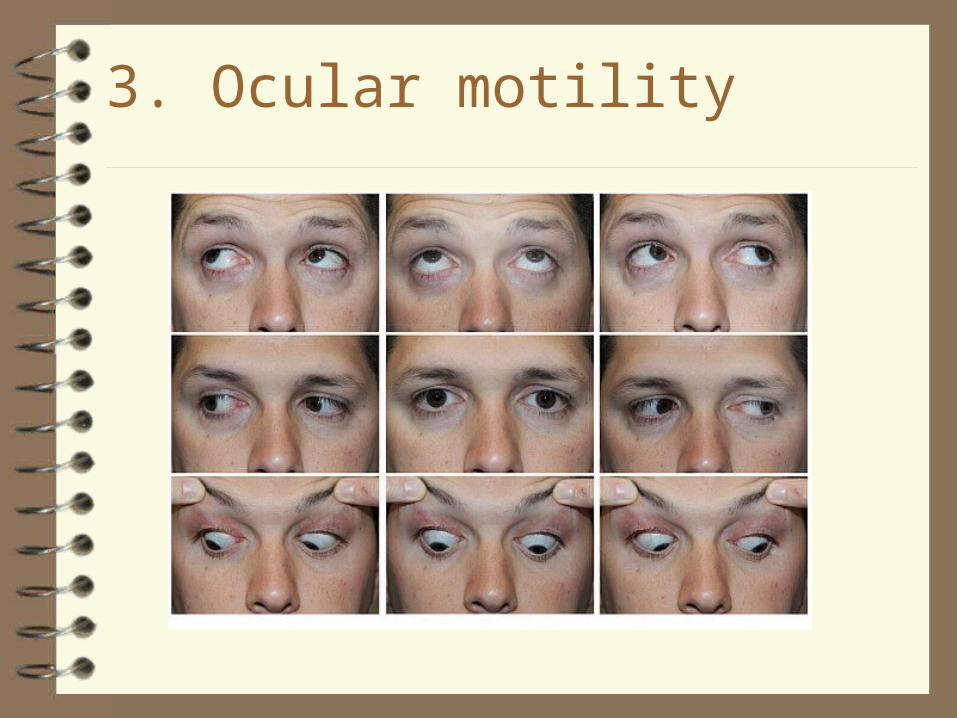
3. Ocular motility
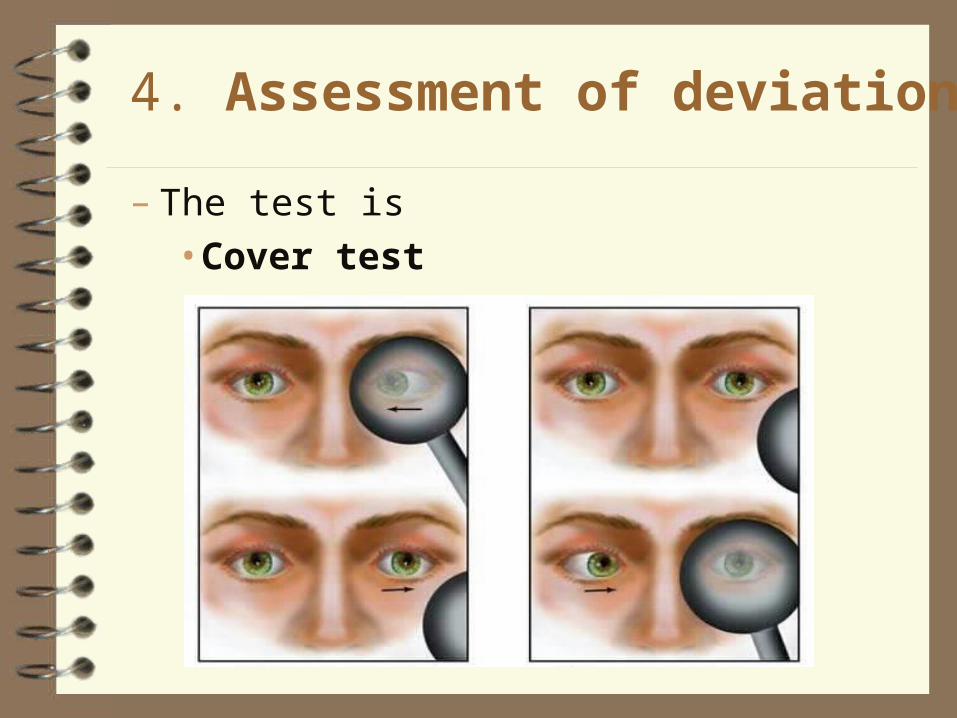
4. Assessment of deviation
– The test is•Cover test
5.Light reflex test
•Hirschberg test– Uses pen torch– Corneal reflexes
•Krimsky test -uses pen torch
-the deviation is measured by the size of the prism required to center the pupillary reflexes
•Bruckner test– Uses ophthalmoscope– Observe the color and brightness of fundus
reflexes and compared
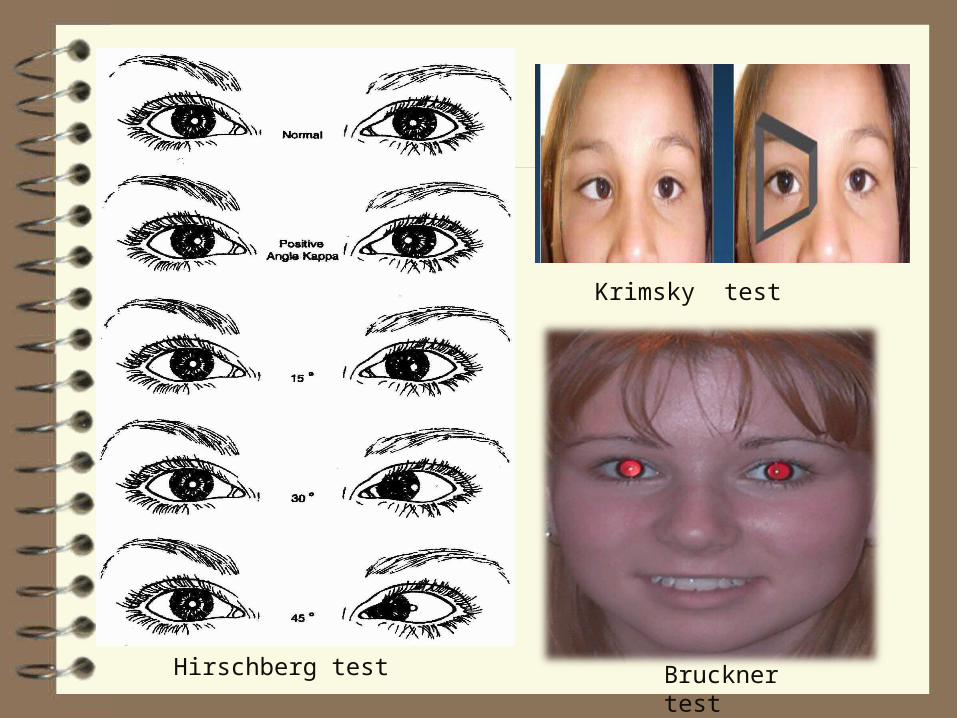
Hirschberg test Bruckner test
Krimsky test
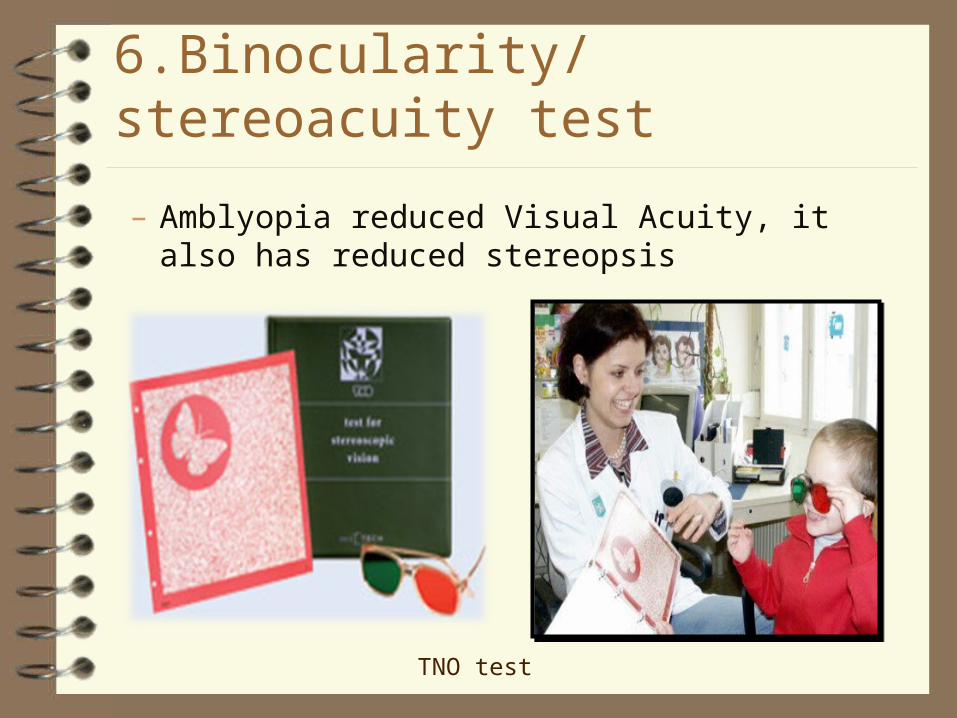
6.Binocularity/stereoacuity test
– Amblyopia reduced Visual Acuity, it also has reduced stereopsis
TNO test
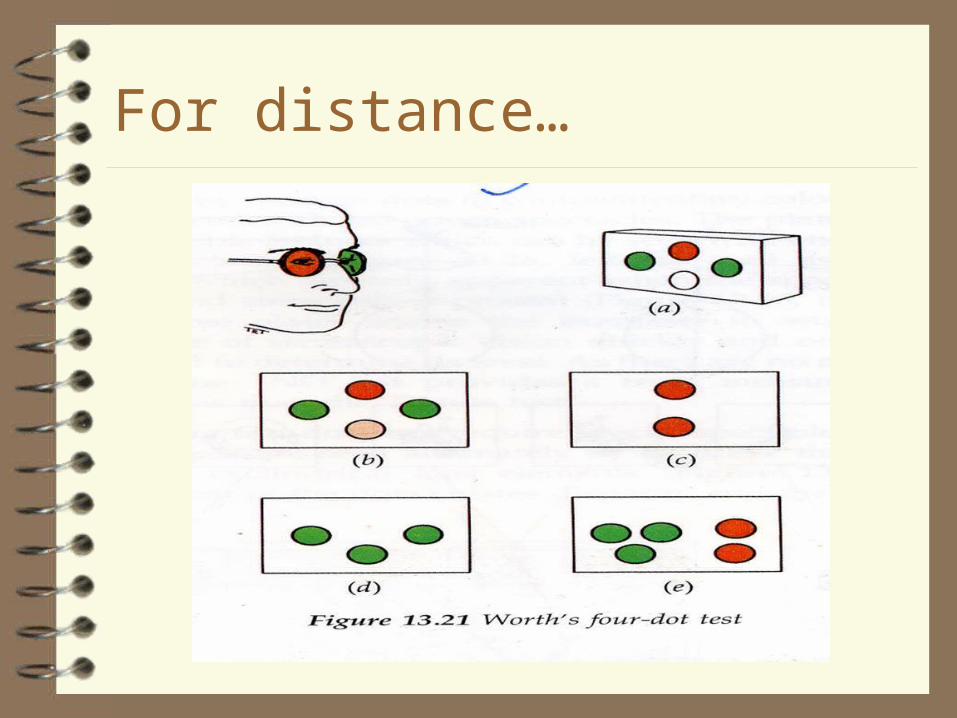
For distance…
8.Pupil examination
Relative apperent pupillary defect (RAPD)-
present in Organic amblyopia
absent in Functional amblyopia
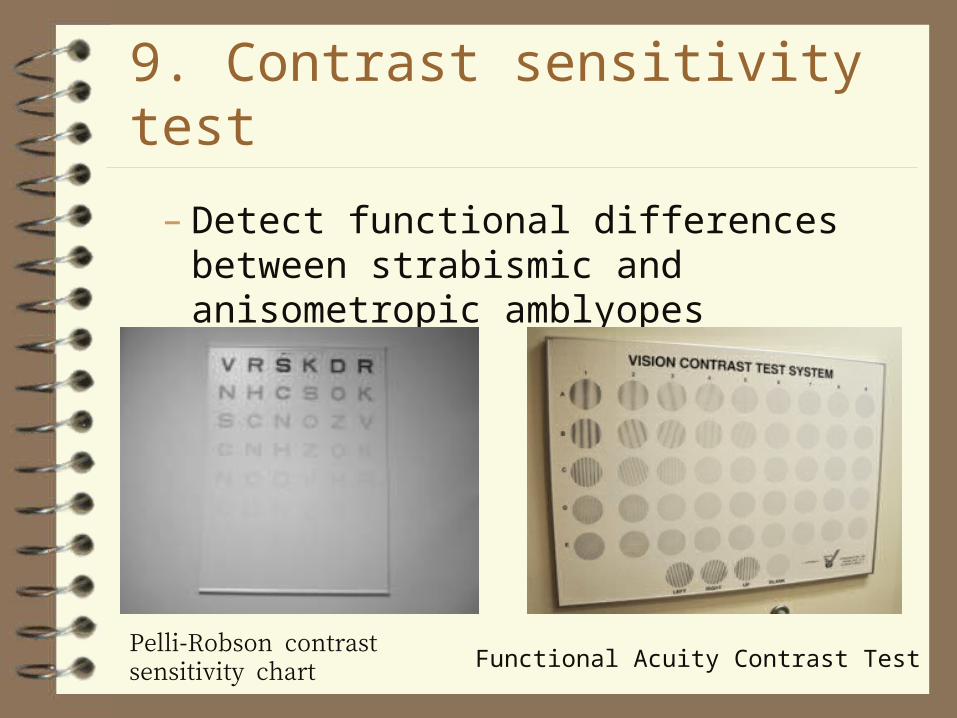
9. Contrast sensitivity test
– Detect functional differences between strabismic and anisometropic amblyopes
Pelli-Robson contrast sensitivity chart Functional Acuity Contrast Test
10.Refraction
– commonly can determine anisometropia– Cycloplegic refraction
•Spasm the ciliary muscle to inactive the accommodation by using drug
- < 2 ½ years, 1% atropine ointment
- < 5 years, 1% Atropine drop- ≥ 5 years, 1% cyclopentolate
hydrochoride,- 2% Homatropine
References
Pediatric ophthalmology & strabismus
-American Academy Of Ophthalmology Pediatric Ophthalmology
-David taylor Pediatric ophthalmology & strabismus
-Kenneth W.Wright
-Peter H. spiegel Clinical management of strabismus
-Elizabeth E.Caloroso

THANK YOU