Acute Intermittent Porphyria: How Would You Manage...
27
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE Supported by an independent educational grant from Recordati Rare Diseases. http://www.medscape.org/spotlight/aip
-
Upload
truongngoc -
Category
Documents
-
view
219 -
download
2
Transcript of Acute Intermittent Porphyria: How Would You Manage...

Acute Intermittent Porphyria:How Would You Manage These Patients? CME/CE
Supported by an independent educational grant from Recordati Rare Diseases.
http://www.medscape.org/spotlight/aip

Pg.2
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
This article is a CME/CE certified activity. To earn credit for this activity visit:
http://www.medscape.org/spotlight/aip
Target Audience This activity is intended for gastroenterologists, emergency medicine physicians, primary care physicians, nurses, nurse practitioners, and other healthcare providers who would benefit from education in diagnosis and management of acute intermittent porphyria.
GoalThe goals of this activity are to improve providers’ ability to recognize, diagnose, and treat an acute porphyric attack.
Learning ObjectivesUpon completion of this activity, participants will be able to:
1. Recognize the clinical presentation of acute intermittent porphyria (AIP)
2. Use the appropriate methods and tools to make a differential diagnosis of AIP
3. Summarize acute management of patients with AIP
Credits AvailableACCME: 0.50 AMA PRA Category 1™ CreditANCC: 0.50 contact hours (0 contact hours are in the area of pharmacology)
Accreditation StatementsFor Physicians Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
Medscape, LLC designates this enduring material for a maximum of 0.50 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
For Nurses Medscape, LLC is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Awarded 0.50 contact hour(s) of continuing nursing education for RNs and APNs; 0.50 contact hours are in the area of pharmacology.
Instructions for Participation and CreditThere are no fees for participating in or receiving credit for this online educational activity. For information on applicability and acceptance of continuing education credit for this activity, please consult your professional licensing board.
CME/CE Released: 06/24/2015; Valid for credit through 06/24/2016

http://www.medscape.org/spotlight/aip
Pg.3
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity online during the valid credit period that is noted on the title page. To receive AMA PRA Category 1 Credit™, you must receive a minimum score of 75% on the post-test. Follow these steps to earn CME/CE credit*:1. Read the target audience, learning objectives, and author disclosures.
2. Study the educational content online or printed out.
3. Online, choose the best answer to each test question. To receive a certificate, you must receive a passing score as designated at the top of the test. We encourage you to complete the Activity Evaluation to provide feedback for future programming.
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate but you cannot alter it. Credits will be tallied in your CME/CE Tracker and archived for 6 years; at any point within this time period you can print out the tally as well as the certificates from the CME/CE Tracker. *The credit that you receive is based on your user profile.
Hardware/Software RequirementsTo access activities, users will need:
• A computer with an Internet connection.
• Internet Explorer 8.x or higher, the latest versions of Firefox or Safari, or any other W3C standards compliant browser.
• Adobe Flash Player and/or an HTML5 capable browser may be required for video or audio playback.
• Occasionally other additional software may be required such as PowerPoint or Adobe Acrobat Reader.
Faculty and DisclosuresAs an organization accredited by the ACCME, Medscape, LLC, requires everyone who is in a position to control the content of an education activity to disclose all relevant financial relationships with any commercial interest. The ACCME defines “relevant financial relationships” as financial relationships in any amount, occurring within the past 12 months, including financial relationships of a spouse or life partner, that could create a conflict of interest.
Medscape, LLC, encourages Authors to identify investigational products or off-label uses of products regulated by the US Food and Drug Administration, at first mention and where appropriate in the content.
Manisha C. Balwani, MD, MSAssociate Professor, Department of Genetics and Genomic Sciences, Icahn School of Medicine at Mount Sinai, New York, New York
Disclosure: Manisha C. Balwani, MD, MS, has disclosed the following relevant financial relationships:Served as an advisor or consultant for: Recordati Rare Diseases
Dr Balwani does not intend to discuss off-label uses of drugs, mechanical devices, biologics, or diagnostics approved by the FDA for use in the United States.
Dr Balwani does not intend to discuss investigational drugs, mechanical devices, biologics, or diagnostics not approved by the FDA for use in the United States.

Pg.4
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Angelika L. Erwin, MD, PhDAssistant Staff Physician, Genomic Medicine Institute, Cleveland Clinic, Cleveland, Ohio
Disclosure: Angelika L. Erwin, MD, PhD, has disclosed no relevant financial relationships.
Dr Erwin does not intend to discuss off-label uses of drugs, mechanical devices, biologics, or diagnostics approved by the FDA for use in the United States.
Dr Erwin does not intend to discuss investigational drugs, mechanical devices, biologics, or diagnostics not approved by the FDA for use in the United States.
Lawrence U. Liu, MDAssistant Professor of Medicine, Division of Liver Diseases, Recanati/Miller Transplantation Institute, Icahn School of Medicine at Mount Sinai, New York, New York
Disclosure: Lawrence U. Liu, MD, has disclosed no relevant financial relationships.
Dr Liu does not intend to discuss off-label uses of drugs, mechanical devices, biologics, or diagnostics approved by the FDA for use in the United States.
Dr Liu does not intend to discuss investigational drugs, mechanical devices, biologics, or diagnostics not approved by the FDA for use in the United States.
Editor(s)Suzanne Bujara, MBAScientific Director, Medscape, LLC
Disclosure: Suzanne Bujara, MBA, has disclosed no relevant financial relationships.
CME Reviewer/Nurse Planner Amy Bernard, MS, BSN, RN-BCLead Nurse Planner, Medscape, LLC
Disclosure: Amy Bernard, MS, BSN, RN-BC, has disclosed no relevant financial relationships

http://www.medscape.org/spotlight/aip
Pg.5
Manisha C. Balwani, MD, MS: Hello. I am Dr Manisha Balwani, associate professor in the Department of Genetics and Genomic Sciences at the Icahn School of Medicine at Mount Sinai in New York City. Welcome to this program on acute intermittent porphyria (AIP).
Joining me today are Dr Angelika Erwin from the Genomic Medicine Institute at the Cleveland Clinic in Ohio and Dr Lawrence Liu, assistant professor of medicine in the Division of Liver Diseases at the Recanati/Miller Transplantation Institute at the Icahn School of Medicine at Mount Sinai in New York. The goals of the program are to describe the presentation of AIP, describe the appropriate diagnostic workup in a patient with suspected AIP, and manage the expectations regarding the acute and long-term management of patients with AIP.
Larry, can you tell us about AIP?

Pg.6
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Lawrence U. Liu, MD: AIP is 1 of several inherited metabolic disorders caused by a defect in the heme biosynthesis pathway. The defect is a partial deficiency of a specific enzyme.[1,2]
Dr Liu: The signs and symptoms of AIP overlap frequently with symptoms of commonly encountered conditions and include abdominal pain, pain in the extremities and the back, nausea and vomiting, tachycardia, and hypertension. Less frequent signs and symptoms include motor weakness, neuropathy, seizures, and hallucinations.[1,3]
Dr Balwani: Why is AIP often overlooked and misdiagnosed?

http://www.medscape.org/spotlight/aip
Pg.7
Dr Liu: The signs and symptoms of AIP are similar to those of other more frequently encountered conditions, so AIP is rarely the first diagnosis that comes to mind. Basic laboratory tests cannot confirm a diagnosis of AIP, but the most striking, although not diagnostic, laboratory abnormality in AIP is hyponatremia.[3,4] Because these patients present with abdominal pain, they are often managed for things that cause gastrointestinal distress and may have their gallbladder or appendix removed or undergo an exploratory laparotomy.[1]
Dr Balwani: What is the best screening test to use for a patient you suspect has AIP?

Pg.8
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Liu: The best screening test is a random urine sample for porphobilinogen (PBG), protected from light as much as possible. We are looking for a PBG level that is at least 10 times above the upper limit of normal.[3,4] A patient’s level might be even higher than 10 times the upper limit of normal, which tells us the patient has AIP. We will test further for the type of acute porphyria.
AIP is 1 of 3 types of porphyrias that cause acute symptoms. The other types are variegate porphyria and hereditary coproporphyria.[5]
Dr Balwani: Are these types rarer than AIP?
Dr Liu: Yes, variegate porphyria and hereditary coproporphyria are much rarer than AIP.
Dr Balwani: Angelika, what should our colleagues know about the role genetics play in AIP?

http://www.medscape.org/spotlight/aip
Pg.9
Angelika L. Erwin, MD, PhD: Acute porphyrias are caused by decreased enzyme activity in the heme biosynthesis pathway, which occurs as a result of mutations in the genes that encode those enzymes. The acute porphyrias are inherited in an autosomal dominant way, meaning that 1 mutation or a mutation on 1 of the 2 copies of a gene is sufficient to cause the disorder. Children or relatives of an infected member have a 50% chance of inheriting this disease-causing mutation and the disorder.[4]
Dr Balwani: What tests would you recommend to confirm the presence of AIP?
Dr Erwin: The diagnosis of AIP can reliably be made by biochemical testing, and specifically by measuring urine PBG levels. Other tests such as urine, plasma, and fecal porphyrin level can be helpful in determining the subtype of acute porphyria. The diagnosis is confirmed by genetic testing, which can be helpful in rare cases in which biochemical testing does not lead to the diagnosis or the determination of the exact underlying subtype.[4,5]
Dr Balwani: What are some of the triggers of AIP?

Pg.10
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Liu: Triggers include medications, such as sulfa drugs and barbiturates; stress; infection; illness; a decrease in carbohydrate and caloric intake; use of recreational drugs; and drinking alcohol.[4] Women have an extra trigger in the form of endogenous hormone levels and are vulnerable during the luteal phase of their menstrual cycles.[4] I check the American Porphyria Foundation and the European Porphyria Network websites to determine which medications may trigger an acute porphyric attack.[5,6]
Dr Balwani: What can patients with AIP do to lower their risk for recurrent acute porphyric attacks?
Dr Liu: Patients should try to identify the potential triggers and avoid them as much as possible. Also, as signs and symptoms may differ among people with AIP, it is helpful if they can recognize signs and symptoms early in the acute porphyric attack.

http://www.medscape.org/spotlight/aip
Pg.11
Dr Balwani: Our first case is a 22-year-old woman who presents to the emergency department (ED) with a 1-day history of unexplained abdominal and chest pain, which progresses to nausea, vomiting, and back pain. This university senior reports that she had a poor diet and drank heavily during her recent spring break.
She was discharged home from the ED without a clear etiology of her symptoms and returned to the ED on 4 consecutive days for similar complaints. She was finally admitted to the hospital for further workup and had an extensive evaluation with a magnetic resonance imaging scan, computed tomography (CT) scan, and endoscopy, but the results were unrevealing. During her stay, she was hypertensive and hyponatremic. Angelika, what about this woman’s presentation would raise the suspicion of AIP?
Dr Erwin: Clinicians must have a high index of suspicion for AIP because the symptoms are nonspecific. In this woman’s case, the feature suggestive of AIP is the poor localization of the abdominal pain. Patients with AIP often report diffuse abdominal pain.[1,4] Other features in this patient that could make you think of AIP are nausea and vomiting, which are often accompanied by constipation, but not diarrhea.
Dr Balwani: What about red or dark urine? That is common in AIP.
Dr Erwin: Red or dark discoloration of the urine is often present in patients who experience acute porphyric attacks, but the absence of red or dark urine does not exclude the diagnosis.[4]

Pg.12
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Balwani: Do you think this patient’s presentation is typical of AIP?
Dr Erwin: Yes. The combination of these symptoms without an obvious underlying cause in a young woman after an episode of poor diet in addition to alcohol consumption is a typical presentation of a first acute porphyric attack.[1,4]
Dr Balwani: Are there other features in her presentation that would make you suspect AIP?
Dr Erwin: This college student had tachycardia and significant hypertension, which we often observe during an acute porphyric attack. Another feature that would raise my suspicion is hyponatremia, which can put patients at high risk for seizures.[1,4] This feature does not have to be present during acute porphyric attacks, so the absence of hyponatremia does not exclude the diagnosis.
Dr Balwani: Larry, how would you evaluate this patient to determine whether she has AIP?

http://www.medscape.org/spotlight/aip
Pg.13
Dr Liu: In the absence of an etiology of her recurring signs and symptoms, we should obtain a random urine sample and test it for PBG. A significantly elevated PBG level -- at least 10 times above the upper limit of normal -- would indicate porphyria.[3] At this point, it is not as important to know which of the 3 acute porphyrias she has, because the management of all 3 acute types is the same.[3,4]

Pg.14
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Balwani: How can we treat this patient’s pain?
Dr Liu: We would administer a high-dose glucose solution such as a D10 infusion (10% dextrose) and intravenous opiates. Then, we would give her hemin, which is the definitive treatment.[4,7,8]
Dr Balwani: How would you manage her hypertension and nausea and vomiting?

http://www.medscape.org/spotlight/aip
Pg.15
Dr Liu: I would manage the woman’s hypertension and tachycardia with a beta-blocker, such as propranolol. For nausea and vomiting, we can use any of the phenothiazines or ondansetron.[4,6] Metoclopramide is not recommended because it might make her symptoms worse.
Dr Balwani: Angelika, once this patient learns that AIP is an inherited disorder, how would you counsel her?
cmalone
Sticky Note
Marked set by cmalone
cmalone
Sticky Note
Marked set by cmalone

Pg.16
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Erwin: In almost all cases, the disease-causing mutation for AIP is inherited from a parent. Given that this is an autosomal dominant disorder, the woman’s siblings, as well as any of her children, have a 50% risk of having inherited mutation.[4] It is important to point out to the patient that only 10% to 20% of mutation carriers will develop symptoms.[5]
Dr Balwani: Who in her family should be tested?
Dr Erwin: We recommend that all first-degree relatives of the patient undergo a genetic test.[3,4] In this case, we would test the patient’s siblings and her parents. We always obtain a pedigree, which can be helpful in determining who in the family is at risk of carrying a disease-causing mutation, based on the family members who have already been identified to be mutation carriers. Identification of other family members who carry the mutation is recommended because these persons are at risk of developing acute porphyric attacks, and we recommend they avoid all known triggers.
Dr Balwani: Angelika, this woman is worried about having another acute porphyric attack. What do you tell her?

http://www.medscape.org/spotlight/aip
Pg.17
Dr Erwin: After an initial acute porphyric attack, it is impossible to predict whether a patient will experience recurrent attacks. Some patients have recurrent attacks, despite avoiding all triggers. If this patient continued to have acute porphyric attacks, I would assess whether there was a relationship between her menstrual cycle and her symptoms. If that were the case, she should receive prophylactic hemin infusions during the week before her menstruation. Another potential treatment option is gonadotropin-releasing hormones to suppress the menstrual cycle.[9] However, this would not be our first-line treatment in a young woman, given its significant adverse effects and the fact that you cannot use this treatment long-term.
Dr Balwani: What should this woman expect in terms of quality-of-life (QoL) and life expectancy?

Pg.18
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Erwin: With the availability of hemin infusion, the life expectancy in patients with AIP should not be shortened. Before hemin became available in the 1970s, there was a significant mortality rate in patients with AIP as a result of respiratory paralysis.[3] Patient QoL depends on the frequency and the severity of acute porphyria attacks. Early recognition of symptoms and prompt treatment are important to prevent complications and to maintain a good quality of life.
Some patients with AIP experience few acute porphyric attacks and respond well to treatment and prophylaxis, whereas others have severe, frequent attacks, despite receiving treatment. These patients are at higher risk of developing neuropathy, muscle weakness, and chronic pain, which can be disabling and severely affect their QoL.[1,3]
Dr Balwani: Larry, at what point might this woman be a candidate for a liver transplant?

http://www.medscape.org/spotlight/aip
Pg.19
Dr Liu: We would consider liver transplantation in this woman as a last resort when all the standard treatment modalities are shown to be ineffective. Liver transplantation for AIP has been performed in Europe, and the results have been excellent. In most of the patients, urine PBG levels normalized early in the posttransplant period, and recurring signs and symptoms resolved.[10-12] The first liver transplant for AIP in the United States was performed at Mount Sinai [New York] 2 years ago. The patient did well postoperatively, and her urine PBG levels normalized. I saw her in the office last week, and she is doing well.

Pg.20
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Balwani: Our second case is a 30-year-old man who presents to the ED with severe abdominal pain and elevated blood pressure. He was given hydromorphone for pain control and had a CT scan, which showed possible colitis. He received antibiotics and was discharged.
This man continued to have nausea, vomiting, and constipation and returned to the ED with severe abdominal pain. A repeat CT scan showed an ileus, so he was admitted for further management. A sigmoidoscopy showed no colitis, and the CT scan performed a few days later showed no significant abnormalities. He had an exploratory laparotomy with an appendectomy, but no significant pathology was noted. He was discharged on analgesics but was readmitted within a week for abdominal pain. Angelika, what red flags would make you suspect AIP in this patient?

http://www.medscape.org/spotlight/aip
Pg.21
Dr Erwin: What stands out in this patient is his recurrent abdominal pain that did not improve, despite treatment. Patients with AIP often have many ED visits, multiple imaging tests, endoscopies, and in some cases, surgical interventions before they are correctly diagnosed.[1,4]
Dr Balwani: Do acute porphyric attacks differ in men and women?
Dr Erwin: Because AIP is inherited in an autosomal dominant way, men and women are at equal risk of inheriting disease-causing mutations; however, women present with acute porphyric attacks more frequently than men.[1,3] The exact underlying cause is not completely understood, but hormonal changes seem to play a role. Men can have severe acute porphyric attacks just like women, but because so few men with acute porphyric attacks are encountered, our index of suspicion has to be even higher, which makes the diagnosis more challenging.
Dr Balwani: Larry, once the diagnosis of AIP is established in this patient, how would you manage him?

Pg.22
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Liu: In addition to a high concentration dextrose solution and an intravenous opiate, I would start him on hemin, which is derived from human blood. We give it intravenously, once daily, for 4 consecutive days.[4,7] Hemin poses a risk for phlebitis, so we administer it through a central line or via a large peripheral vein. Hemin can be diluted in either sterile water or albumin. We prefer to use albumin to keep it stable, and we infuse the solution within an hour.
Dr Balwani: What is the dose of hemin?
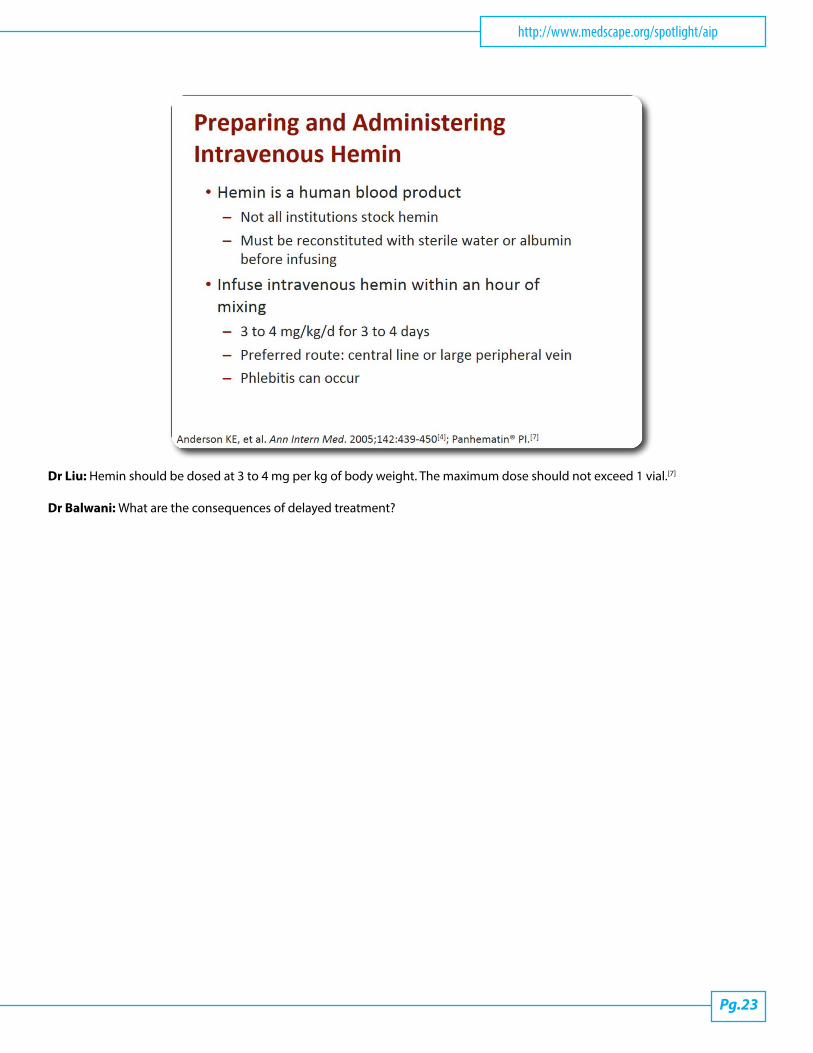
http://www.medscape.org/spotlight/aip
Pg.23
Dr Liu: Hemin should be dosed at 3 to 4 mg per kg of body weight. The maximum dose should not exceed 1 vial.[7]
Dr Balwani: What are the consequences of delayed treatment?

Pg.24
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Liu: If treatment is delayed, seizures, chronic pain, neuropathy, muscle weakness, and in the worst case, respiratory paralysis can occur.[3,4] With the available treatment modalities, mortality has decreased significantly.
Dr Balwani: When this man finds out the genetic nature of AIP, he is concerned about his 2-year-old daughter. How would you counsel him and his family?
Dr Erwin: The risk for his 2-year-old daughter to carry the disease-causing mutation is 50%.[3,4] However, most patients with mutations never have symptoms. Therefore, it is not urgent to do genetic testing on his 2-year-old daughter at this point, but we do recommend testing her before she reaches puberty so that she can avoid AIP triggers if she is a carrier.
Dr Balwani: If this man and his wife are planning to have another child, what are their options?
Dr Erwin: Once the specific mutation is known to be present, the couple has several reproductive options. If they want to avoid having a child with an AIP mutation, we would recommend preconception genetic counseling.
Dr Balwani: Larry, what would you tell this man about how he can try to avoid future acute porphyric attacks?
http://www.medscape.org/spotlight/aip
Pg.25
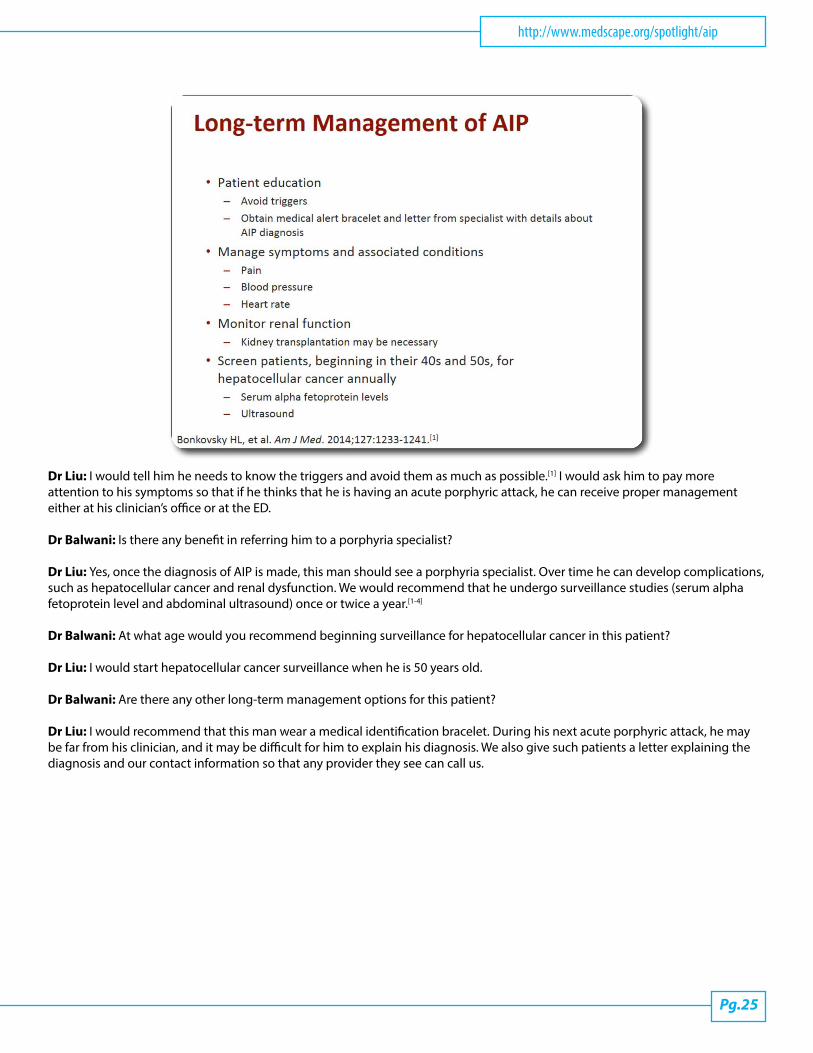
Dr Liu: I would tell him he needs to know the triggers and avoid them as much as possible.[1] I would ask him to pay more attention to his symptoms so that if he thinks that he is having an acute porphyric attack, he can receive proper management either at his clinician’s office or at the ED.
Dr Balwani: Is there any benefit in referring him to a porphyria specialist?
Dr Liu: Yes, once the diagnosis of AIP is made, this man should see a porphyria specialist. Over time he can develop complications, such as hepatocellular cancer and renal dysfunction. We would recommend that he undergo surveillance studies (serum alpha fetoprotein level and abdominal ultrasound) once or twice a year.[1-4]
Dr Balwani: At what age would you recommend beginning surveillance for hepatocellular cancer in this patient?
Dr Liu: I would start hepatocellular cancer surveillance when he is 50 years old.
Dr Balwani: Are there any other long-term management options for this patient?
Dr Liu: I would recommend that this man wear a medical identification bracelet. During his next acute porphyric attack, he may be far from his clinician, and it may be difficult for him to explain his diagnosis. We also give such patients a letter explaining the diagnosis and our contact information so that any provider they see can call us.

Pg.26
Acute Intermittent Porphyria: How Would You Manage These Patients? CME/CE
Dr Balwani: To summarize our discussion, the best test for diagnosing AIP is the PBG level, which can be done from a random
acute illnesses should be treated promptly, and prophylactic hemin can be considered in a select group of patients, particularly those having recurrent acute porphyric attacks.
Thank you, Angelika and Larry, for joining me in this interesting discussion. Thank you for participating in this activity. Click on the Earn CME/CE credit link to take the CME/CE posttest and evaluation.
This transcript has been edited for style and clarity.

http://www.medscape.org/spotlight/aip
Pg.27
REFERENCES1 Bonkovsky HL, Maddukuri VC, Yazici C, et al. Acute porphyrias in the USA: features of 108 subjects from porphyrias consortium. Am J Med. 2014;127:1233-1241. 2 Acute intermittent porphyria. National Organization for Rare Disorders website. https://rarediseases.org/rare-diseases/acute- intermittent-porphyria/. Accessed May 26, 2015.3 Puy H, Gouya L, Deybach JC. Porphyrias. Lancet. 2010;375:924-937. 4 Anderson KE, Bloomer JR, Bonkovsky HL, et al. Recommendations for the diagnosis and treatment of the acute porphyrias. Ann Intern Med. 2005;142:439-450. 5 Diagnostic testing for the acute porphyrias - clarification of testing results. American Porphyria Foundation website. http://www.porphyriafoundation.com/content/diagnostic-testing-acute-porphyrias-clarification-testing-results. Accessed May 27, 2015.6 Drugs and porphyria. European Porphyria Network website. http://www.porphyria-europe.org/03-drugs/drugs-and-porphyrias.asp. Accessed May 27, 2015.7 Panhematin® [product information]. Lebanon, NJ: Recordati Rare Diseases, Inc; 2013.8 Besur S, Hou W, Schmeltzer P, Bonkovsky HL. Clinically important features of porphyrin and heme metabolism and the porphyrias. Metabolites. 2014;4:977-1006. 9 Innala E, Bäckström T, Bixo M, Andersson C. Evaluation of gonadotropin-releasing hormone agonist treatment for prevention of menstrual-related attacks in acute porphyria. Acta Obstet Gynecol Scand. 2010;89:95-100. 10 Singal AK, Parker C, Bowden C, Thapar M, Liu L, McGuire BM. Liver transplantation in the management of porphyria. Hepatology. 2014;60:1082-1089. 11 Dowman JK, Gunson BK, Mirza DF, Bramhall SR, Badminton MN, Newsome PN; UK Liver Selection and Allocation Working Party. Liver transplantation for acute intermittent porphyria is complicated by a high rate of hepatic artery thrombosis. Liver Transpl. 2012;18:195-200. 12 Wahlin S, Harper P, Sardh E, Andersson C, Andersson DE, Ericzon BG. Combined liver and kidney transplantation in acute intermittent porphyria. Transpl Int. 2010;23:e18-e21.
ABBREVIATIONSAIP = acute intermittent porphyriaALA = aminolevulinic acidCT = computed tomographyED = emergency departmentPBG = porphobilinogen
Disclaimer
no association with any actual patient is intended or should be inferred.
medscape.org. These materials may discuss therapeutic products that have not been approved by the US Food and Drug Administration and
Readers should verify all information and data before treating patients or employing any therapies described in this educational activity.
Medscape Education © 2015 Medscape, LLC
cmalone
Sticky Note
Marked set by cmalone