Acls Guidelines 2010 T_ Larabee(1)
36
8/2/2019 Acls Guidelines 2010 T_ Larabee(1) http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 1/36 Todd M. Larabee, MD Department of Emergency Medicine University of Colorado Denver SOM
-
Upload
ankit-sharma -
Category
Documents
-
view
219 -
download
0
Transcript of Acls Guidelines 2010 T_ Larabee(1)

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 1/36
Todd M. Larabee, MDDepartment of Emergency Medicine
University of Colorado Denver SOM

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 2/36
Issues after 2005 Guideline changesILCOR ProcessHighlights of the 2010 Guidelines◦
BLS◦ ACLS◦ PALSSummary

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 3/36
Biggest changes in 2005 were 30:2compression ration and the change indefibrillation sequence
Growing emphasis on high-quality CPRImplementation of the 2005 guidelines didimprove outcomesImplementing new guidelines can take 18months-4 years

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 4/36
Since 2005, there’s been an emphasis tosimplify CPR recommendationsStress high-quality CPR
Stress utility/importance of bystander CPRNeed to remove barriers to performance of bystander CPRDe-emphasis on devices and drugs
Importance of post-cardiac arrest careImportance of continuing education andtraining

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 5/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 6/36
Objectives:◦ Provide a forum for discussion and coordination of
all aspects of cardiopulmonary and cerebralresuscitation worldwide.
◦ Foster scientific research in areas of resuscitation
where there is a lack of data or controversy exists.◦ Disseminate information on training and education
in resuscitation.◦ Provide a mechanism for collecting, reviewing and
sharing international resuscitation data.◦ Produce statements on specific issues related to
resuscitation that reflect international consensus.

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 7/36
Resuscitation Council of Asia (currentmembers Japan, Korea, Singapore,Taiwan)

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 8/36
Task Forces generate worksheets/PICOquestions411 scientific evidence reviews on 277 topicsrelated to resuscitation and ECC356 “experts” from 29 countriesDebates/discussions via telephone/in-person/webinars
Creates the most current and comprehensivereview of resuscitation literature everpublished

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 9/36
In adult patients in cardiac arrest (asystole,pulseless electrical activity, pulseless VT andVF) (prehospital [OHCA], in-hospital [IHCA])
(P), does the use of vasopressors(epinephrine, norepinephrine, others) orcombination of vasopressors (I) comparedwith not using drugs (or a standard drugregimen) (C), improve outcomes (eg. ROSC,survival) (O).

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 10/36
Levels of Evidence for Therapeutic Interventions
LOE 1: Randomised Controlled Trials (or meta-analyses of RCTs)
LOE 2: Studies using concurrent controls without true randomisation (eg. “pseudo” -randomised)(or meta-analyses of such studies)
LOE 3: Studies using retrospective controlsLOE 4: Studies without a control group (eg. case series)
LOE 5: Studies not directly related to the specific patient/population (eg. differentpatient/population, animal models, mechanical models etc.)

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 11/36
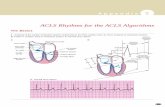
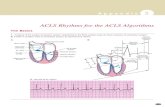
Good
(Goetting and Paradis 1991)A-D(Grmec and Mally 2006)A-C
(Gonzalez, Ornato et al. 1989)E(Lindner, Prengel et al. 1996)A-D
Fair(Paradis, Martin
et al. 1991)E(Barton and Callaham 1991)A(Matok, Vardi et al. 2007)A-C
Poor (Guyette, Guimond et al. 2004)A,E
(Goetting and Paradis 1989)A
1 2 3 4 5
Level of evidence
Evidence Supporting Clinical Question
A = Return of spontaneous circulation C = Survival to hospital discharge E = Other endpointB = Survival of event D = Intact neurological survival Italics = Animal studies

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 12/36
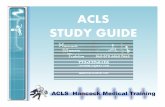
Neutral evidence tableGood
(Aung and Htay 2005)A-D(Brown, Martin et al. 1992)A-D(Callaway, Hostler et al. 2006)A-D(Choux, Gueugniaud et al. 1995)A-D(Gueugniaud, David et al. 2008)A-D
(Gueugniaud, Mols et al. 1998)A-D(Lindner, Dirks et al. 1997)A-D(Lindner, Ahnefeld et al. 1991)A-C(Lipman, Wilson et al. 1993) A,B,E(Olson, Thakur et al. 1989)A-C(Olasveengen, Sunde et al. 2009)A-D(Callaham, Madsen et al. 1992)A-D(Lindner, Ahnefeld et al. 1991) A-C(Patrick, Freedman et al. 1995)A-D(Perondi, Reis et al. 2004)A-C(Sherman, Munger et al. 1997)A-C(Stiell, Hebert et al. 1992)A-D(Stiell, Hebert et al. 2001)A-E(Turner, Parsons et al. 1988)A-D(Wenzel, Krismer et al. 2004)A-D
(Carvolth and Hamilton1996)A-C
Fair(Patterson, Boenning et al. 2005)A-D(Silfvast, Saarnivaara et al. 1985)A(Vandycke and Martens 2000)A-D
(Takeo, Kosaku et al. 2009)A-D
(Herlitz, Ekstromet al. 1995)A-C
(Carpenter and Stenmark 1997)A-D
Poor
(Woodhouse, Cox et al. 1995)A-C
(Morris,Dereczyk et al.
1997) E(Gonzalez,
Ornato et al.1988)E
(Dieckmann and Vardis1995)A-D
(Mally, Jelatancev et al.2007)A-C, E
(Callaham, Barton et al.1991)B-E
(Ong, Tan et al. 2007)A-D1 2 3 4 5
Level of evidence
A = ROSC C = Survival to hospital discharge E = Other endpoint
B = Survival of event D = Intact neurological survival

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 13/36
Opposing evidence table
Good(Behringer, Kittler et al.
1998)A,D
Fair
Poor
(Rivers, Wortsman et al.1994)A, B, E
(Chang, Ma et al.2007)E
(Duncan, Meaney et al.2009)A-E
1 2 3 4 5
Level of evidence
A = Return of spontaneous circulation C = Survival to hospital discharge E = Other endpointB = Survival of event D = Intact neurological survival Italics = Animal studies

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 14/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 15/36
“Look, listen, feel” removed from algorithm◦ delaysEarly activation of EMSCompression-only CPR for the untrained lay-
rescuerHigh-quality CPRMinimize interruptionsDeemphasis on pulse checks during CPR

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 16/36
C-A-B not A-B-C◦ Most arrest are adult; most survivors are
VF/VT◦
Emphasis on performing high-quality CPRand early defibrillation◦ Delay in “C” when attempting “A”◦ May remove barriers to bystander CPR

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 17/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 18/36
Untrained lay-person◦ Hands-only CPR◦ Continue until AED/trained personnel availableTrained lay-person◦ Hands-only CPR◦ If willing to perform ventilations with 30:2 ratio◦ Continue until AED/trained personnel availableHealthcare Provider◦
CPR including ventilations with 30:2 ratio◦ Can tailor sequence of interventions based on
cause of arrest

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 19/36
CPR Techniques and Devices◦ No adjunct has been shown to be superior to
manual CPR◦ ITD (ResQPOD) improved ROSC and short-term
survival◦ Load-band CPR (Autopulse) with no change in 4-hr survival and worsened neurologic outcomes
◦ Mechanical piston devices with varying degrees of success
◦ All require additional equipment and training;training needs to be ongoing
◦ More research needed

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 20/36
Electrical Therapy◦ Emphasis on AEDs and addition of AEDs to
enhance the chain of survival◦ CPR before defibrillation remains unclear◦ Continuing with 1-shock protocol with
minimizing CPR interruptions

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 21/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 22/36
Successful ACLS is predicated on good BLS◦ High-quality CPR with minimal interruptions◦ Early defibrillationFifth link in “Chain of Survival”: Post -Cardiac Arrest Care◦ Multidisciplinary care from BLS to discharge for
good neurologic outcomeQualitative waveform capnography

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 23/36
Airway Management:◦ Qualitative waveform capnography recommended◦ Suppraglottic airway devices are supported as
airway alternative◦
Cricoid pressure is no longer recommendedSymptomatic Dysrrhythmias◦ Adenosine is safe for diagnostics in stable,
undifferentiated wide-complex monomorphic
tachycardia◦ For stable or unstable bradycardia, IV chronotropic
agents recommended as equally effective asexternal pacing

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 24/36
Copyright ©2010 American Heart Association
Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Circular Algorithm

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 25/36
Copyright ©2010 American Heart Association
Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Algorithm

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 26/36
Notice on the charts:◦ Vascular access, drug delivery, advanced airway
placement are recommended but should notinterrupt CPR
◦ Atropine no longer recommended for PEA/asystole◦ Real-time monitoring of CPR quality
Mechanical parametersPhysiologic parameters
◦ Post-arrest care now a component of the algorithm

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 27/36
Post Cardiac-Arrest Care◦ Multidisciplinary team◦ Structured, integrated, bundled system of careKey Objectives◦ Optimize cardiopulmonary function and vital organ
perfusion after ROSC◦ Transport to an appropriate critical care unit withcomprehensive post-cardiac arrest care system
◦ Identify/intervention for ACS◦ Temperature control for improving neurologic
outcomes◦ Prevention and treatment of multi-organ
dysfunction

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 28/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 29/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 30/36
Emphasis on asphyxial arrest combinedwith chest compressionsCompression-only CPR for bystanders
unwilling or unable to perform ventilationsC-A-B for ease of teaching (A-B-Ccontinues in Neonatal Resuscitation)High-quality CPR

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 31/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 32/36
Deemphasis on pulse checksUpdated formula for cuffed tubes in infantsand young children◦
Uncuffed: 4 + (age/4) if > 2yr3.5 up to 1 yr, 4.0 if >1yr◦ Cuffed: 3.5 + (age/4) if >2yr
3.0 up to 1yr, 3.5 if >1yr
Safety and value of cricoid pressurequestioned; can discontinue if impedesairway

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 33/36
Capnography recommendedOptimal defibrillation energy dose uncertain-recommending 2-4J/kg (either waveform)Concerns of hyperoxemia after ROSC

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 34/36

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 35/36
Fewer, less dramatic changes than in 2005Circulation more important than ventilation inmost instancesC-A-B
Goodbye AtropinePost resuscitation care and neurologicoutcomes focus

8/2/2019 Acls Guidelines 2010 T_ Larabee(1)
http://slidepdf.com/reader/full/acls-guidelines-2010-t-larabee1 36/36
Thanks for listening.