ACLS Algorithms Slide

of 26
Transcript of ACLS Algorithms Slide
-
8/10/2019 ACLS Algorithms Slide
1/26
-
8/10/2019 ACLS Algorithms Slide
2/26
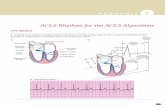
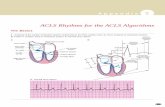
Assess responsiveness (speak loudly, gentlyshake patient if no trauma - "Annie, Annie,
are you OK?"). Call for help/crash cart if unresponsive. ABCDs
irway Open airway, look, listen, and feel for
breathing. reathing If not breathing, slowly give 2 rescue
breaths.C irculation
Check pulse. If pulseless, begin chest compressions at100/min, 15:2 ratio. Consider no defibrillator nearby
Defibrillation Attach monitor, determine rhythm. If VF or pulseless
VT: shock up to 3 times. If not, basic CPR.
Then, move quickly to Secondary Survey.
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
3/26
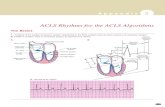
After initial (primary) assessment done Another set of ABCDs
irway Establish and secure an airway device (ETT, LMA,
COPA, Combitube, etc.).
reathing Ventilate with 100% O2. Confirm airway placement
(exam, ETCO2, and SpO2). Remember, nometabolism/circulation = no blue blood to lungs = noETCO2.
C
irculation Evaluate rhythm, pulse. If pulseless continue CPR,
obtain IV access, give rhythm-appropriate medications
D ifferential Diagnosis Identify and treat reversible causes.
-
8/10/2019 ACLS Algorithms Slide
4/26
Treatment Consider bicarb, pacing early
icarb (NaHCO3)
Epinephrine 1 mg IV q3-5 min
tropine 1 mg IV q3-5 min. Max 0.04 mg/kg
Consider possible causesHypoxia, Hyperkalemia, Hypothermia, Drug
overdose (e.g., tricyclics), Myocardial Infarction
Consider termination. If patient had >10minwith adequate resucitative effort and notreatable causes present
Always Primary Survey- Secondary Survey: Confirmrhythm (check monitor, power, different lead)
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
5/26
Primary Survey
Secondary Survey assess need for airway, oxygen, IV, monitor, fluids,
vitals, pulse ox
12-lead ECG, Consider Dx
If AV block:
2nd degree (type 2) or 3rd degree: standby TCP, prepare fortransvenous pacing.
If serious signs or symptoms, tropine
0.5-1.0 mg IV push q 3-5 min. max 0.04 mg/kg
Pacing
Use transcutaneous pacing (TCP) immediately if sx severe
Dopamine 5-20 g/kg/min
Epinephrine 2-10 g/min
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
6/26
Primary Survey, Secondary Survey: Is patient
stable or unstable? stable: determine rhythm, treat accordingly unstable
=chest pain, dyspnea, decreased level of
conciousness, low BP, CHF, AMI If HR is cause of symptom (almost always HR>150):
cardiovert
Specific Rhythms Atrial fib/flutter
Narrow-Complex (Supraventricular) Tachycardia Wide-Complex Tachycardia, Unknown Type Stable Ventricular Tachycardia
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
7/26
Generally not needed for HR150, prepare for immediate cardioversion.May give brief drug trial.
Steps: Prepare emergency equipment
Medicate if possible Cardioversion
monomorphic VT with pulse, PSVT, A fib, A flutter:
100-200-300-360 J* (Synchronized)
may try 50J first for PSVT or A flutter
may use equivalent biphasic (biphasic 70, 120, 150, and 170J)
if machine unable to synchronize and patient critical,defibrillate
polymorphic VT: use VT/VF algorithm
-
8/10/2019 ACLS Algorithms Slide
8/26
Management:Control rate, consider rhythm
cardioversion, and anticoagulateas shown below,according to Category: 1, 2 or 3
Category 1. Normal EF
Rate control: Ca-blocker or beta-blocker.
Cardiovert: If onset < 48 hours, consider DC cardioversionOR with
one of the following agents: amiodarone, ibutilide,procainamide, (flecainide, propafenone), sotalol.
If onset > 48 hours: avoid drugs that may cardiovert(e.g. amiodarone). Either: Delayed Cardioversion: anticoagulate adequately x 3 weeks,
then cardioversion, then anticoagulate x 4 weeks
Early Cardioversion: iv heparin, then TEE, then cardioversionwithin 24 hours, then anticoagulate x 4 weeks
Transesofageal ekokardiogram
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
9/26
Category 2. EF< 40% or CHF
Rate control: digoxin, diltizaem, amiodarone
avoid verapamil, beta-blockers, ibutilide,procainamide (and propafenone/flecainide)
-
8/10/2019 ACLS Algorithms Slide
10/26
Category 3. WPW A fib
Suggested by: delta wave on resting EKG, very
young patient, HR>300 Avoid adenosine, beta-blocker, Ca-blocker, or
Digoxin
If < 48 hour:
If EF normal: one of the following for both rate controland cardioversion: amiodarone, procainamide,propafenone, sotalol, flecainide
If EF abnormal or CHF: amiodarone or cardioversion
If > 48 hour
Medication listed above may be associated with risk ofemboli Anticoagulate and DC cardioversionas in Category 1.
Sindrom Wolff Parkinson White
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
11/26
If unstable, cardiovert No cardioversion for stable SVT with low EF.
Management 12-lead ECG, clinical exam
Vagal stimulation, adenosine. Consider esophageallead
Treat according to specific rhythm:
PSVT
MAT
Junctional
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
12/26
EF normal Refleks Vagal
Ca-blocker> beta-blocker> digoxin> DCCardioversion.
Consider procainamide, sotalol, amiodarone.
If unstable proceed to cardioversion
EF < 40%, CHF No Cardioversion. Digoxin or amiodarone or
diltiazem.
If unstable proceed to cardioversion
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
13/26
EF normal: amiodarone, beta-blocker, Ca-blocker
EF < 40%, CHF: amiodarone Notes
rare, most commonly misdiagnosed PSVT.
likely digoxin or theophylline OD, catecholamine
state no cardioversion
-
8/10/2019 ACLS Algorithms Slide
14/26
If unstable, cardiovert Attempt to establish specific diagnosis
12 leads, esophageal lead, Clinical info
Note: the use of adenosine to differentiate SVT vs
VT is now de-emphasized.
If unable to make Dx, treat according to EF: EF normal: DC cardioversionor procainamide or
amiodarone
EF < 40%, CHF: DC cardioversionor amiodarone Note: no lidocaine and bretylium in protocol
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
15/26
May proceed directly to cardioversion If not, treat according to morphology:
Monomorphic VT
EF normal: one of the following:
procainamide (2a), sotalol (2a) OR amiodarone (2b), lidocaine (2b)
EF poor
amiodarone 150 mg iv over 10 min OR lidocaine 0.5-0.75mg/kg iv push
Synchromized cardioversion
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
16/26
Polymorphic VT
Baseline QT Normal
Possible ischemia (treat) or electrolyte (esp. low K, Mg)abnormality (correct)
EF normal: betablocker, amiodarone, procainamide, orsotalol
EF poor
amiodarone 150 mg iv over 10 min synchromized cardioversion
Prolonged QT baseline (torsade)
Correct electrolyte abnormalities.
Treatment options: magnesium, overdrivepacing, isoproterenol
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
17/26
Primary Survey, then Secondary Survey: rule
out pseudo-PEA (handheld doppler: look forcardiac mechanical activities. If present treatagressively).
Problem
Search for the probable cause... Wide QRS: suggests massive myocardial injury,
hyperkalemia, hypoxia, hypothermia
Wide QRS+Slow: consider drug OD (tricyclics, beta-blockers, Ca-blockers, digoxin)
Narrow complex: suggests intact heart; considerhypovolemia, infection, PE, tamponade
... and treat as needed
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
18/26
Consider fluid challenge empirically Consider bicarbonate
hyperkalemia K (Class 1)
bicarbonate responsive acidosis, tricyclic OD, to alkinalizeurine for aspirin OD (Class2a)
prolonged arrest (Class 2b)
not for hypercarbic acidosis
Epinephrine: 1 mg IV q3-5 min
tropine If bradycardia, 1 mg IV q3-5 min
max 0.04 mg/kg
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
19/26
If you prefer a mechanistic approach (and areused to thinking about MAP, CO, SVR, etc.)think of things that affect forward flow... Decreased Preload: Hypovolemia, Tamponade,
Tension Pneumothorax Increased Afterload: Pulmonary Embolus
Decreased Contractility: Hypoxia, Hypothermia,Acidosis, Myocardial Ischemia
Altered Rate/Rhythm: Hyperkalemia, Drug Overdose
-
8/10/2019 ACLS Algorithms Slide
20/26
Hypovolemia Assess: Collapsed vasculature Tx: Fluids
Hypoxia Assess: Airway, cyanosis, ABGs Tx: Oxygen, ventilation
Hydrogen ion (acidosis) Assess: Diabetic patient, ABGs
Tx: Bicarb 1 mEq/kg, hyperventilationHyperkalemia (preexisting)
Assess: Renal patient, EKG, serum K level Tx: Bicarb, CaCl, albuterol neb, insulin/glucose, dialysis,
diuresis, kayexalate
Hypothermia Assess: Core temperature Tx: Hypothermia Algorithm
-
8/10/2019 ACLS Algorithms Slide
21/26
Tablets/toxins overdose Assess: Hx of medications, drug use Tx: Treat accordingly
Tamponade, cardiac Assess: No pulse w/ CPR, JVD, narrow pulse pressure
prior to arrest Tx: Pericardiocentesis
Tension pneumothorax
Assess: No pulse w/ CPR, JVD, tracheal deviation Tx: Needle thoracostomy
Thrombosis, coronary Assess: History, EKG Tx: Acute Coronary Syndrome algorithm
Thrombosis, pulmonary embolism Assess: No pulse w/ CPR, JVD
Tx: Thrombolytics, surgery
-
8/10/2019 ACLS Algorithms Slide
22/26
Remember: initial stacked shocks are part of theprimary survey Implement the secondary surveyafter your stacked
shocks. Meds: Shock-drug-shock-drug-shock pattern.
Continue CPR while giving meds, and shock (360J or150J if biphasic) within 30-60 seconds. Evaluaterhythm and check for pulse immediately aftershocking.
Epi or vasopressin big drugs (may give either one asfirst choice). If VF/PVT persists, may move on to antiarrhythmics and
sodium bicarb max out one antiarrhythmic before proceeding to the next
in order to limit pro-arrhythmic drug-drug interactions.
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
23/26
Shock 200J* If VF or VT is shown on monitor: shock immediately. Do not lift paddles from chest after shocking -
simultaneously charge at next energy level and evaluate
rhythm.Shock 200-300J*
If VF or VT persists on monitor, shock immediately. Do not check pulse, do not continue CPR, do not lift
paddles from chest. After shocking, simultaneously charge at next energy
level and evaluate rhythm.Shock 360J*
If VF or VT persists, shock immediately.
Epinephrine 1 mg IV q3-5 min. High dose epinephrine is no longer recommended
Vasopressin 40 U IV one time dose (wait 5-10 minutes before starting epi). Preferred first drug?
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
24/26
Shock 360J*
miodarone (Class 2b) 300mg IV push.
May repeat once at 150mg in 3-5 min max cumulative dose = 2.2g IV/24hrs
Shock 360J*
Magnesium Sulfate (Class 2b) 1-2 g IV (over 2 min) for suspected
hypomagnesemia or torsades de pointes(polymorphic VT)
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
25/26
Shock 360J*
icarbonate
1 mEq/kg IV for reasons below: Class 1: hyperkalemia
Class 2a: bicarbonate-responsive acidosis, tricyclicOD, to alkinalize urine for aspirin OD
Class 2b: prolonged arrest
Not for hypercarbia-related acidosis, nor for routineuse in cardiac arrest
http://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.htmlhttp://www.unc.edu/~rvp/old/RP_Anesthesia/Basics/ACLSAlgorithms.html -
8/10/2019 ACLS Algorithms Slide
26/26