](https://static.fdocuments.in/doc/165x107/5556ced7d8b42abb428b5615/acute-myocardial-infarction-final2.jpg)
ABCs of ACS - NCEMSF - acute...ABCs of ACS: ACUTE CORONARY ... Describe the pathophysiology of acute...
48
ABCs of ACS: ACUTE CORONARY ACUTE CORONARY SYNDROME SYNDROME Claudine Hagan, RN MPA Claudine Hagan, RN MPA
Transcript of ABCs of ACS - NCEMSF - acute...ABCs of ACS: ACUTE CORONARY ... Describe the pathophysiology of acute...

ABCs of ACS:
ACUTE CORONARY ACUTE CORONARY SYNDROMESYNDROME
Claudine Hagan, RN MPAClaudine Hagan, RN MPA
Objectives
Define acute coronary syndromeDefine acute coronary syndromeDescribe the pathophysiology of acute Describe the pathophysiology of acute myocardial infarctionmyocardial infarctionDescribe the contributing factors to acute Describe the contributing factors to acute coronary syndromecoronary syndromeIdentify the key elements in treating acute Identify the key elements in treating acute coronary syndrome and the role of the EMS coronary syndrome and the role of the EMS personal personal

Coronary heart disease (CHD) is the leading Coronary heart disease (CHD) is the leading cause of death in America. cause of death in America.
IncidenceIncidence——1.2 million new or recurrent AMI 1.2 million new or recurrent AMI annuallyannually
41% of the 1.2 million are recurrent 41% of the 1.2 million are recurrent MIsMIs38% die from the acute MI38% die from the acute MI
MortalityMortality----1/2 million die annually (1 in 5)1/2 million die annually (1 in 5)PrevalencePrevalence——15,800,000 victims of angina, 15,800,000 victims of angina, heart attack and other forms of CHD are still heart attack and other forms of CHD are still living living (AHA, 2004 Heart Attack and Angina Statistics)(AHA, 2004 Heart Attack and Angina Statistics)
Statistics
Woman and Heart Disease
Myth that heart Myth that heart disease = mandisease = man’’s s diseasedisease1 in 8 woman aged 451 in 8 woman aged 45--64 has heart disease64 has heart disease1 in 4 over 65 have 1 in 4 over 65 have heart diseaseheart diseaseCAD leading cause of CAD leading cause of death in woman in USdeath in woman in US

Definition of ACS
Acute Coronary Syndrome (ACS)Acute Coronary Syndrome (ACS) is a term used is a term used to describe the spectrum of disease of the coronary to describe the spectrum of disease of the coronary arteries that range from unstable angina to acute arteries that range from unstable angina to acute myocardial infarction. myocardial infarction. ACC/AHA Joint Guideline Statement, 2007ACC/AHA Joint Guideline Statement, 2007::
““any constellation of clinical symptoms that are any constellation of clinical symptoms that are compatible with acute myocardial ischemiacompatible with acute myocardial ischemia””
Unstable AnginaUnstable AnginaMI (STEMI & NSTEMI)MI (STEMI & NSTEMI)

Definitions (Cont.)
Myocardial ischemiaMyocardial ischemiaA condition in which oxygen delivery to and metabolite removal from the myocardium fall below normal levels, with oxygen demand exceeding supply
Acute myocardial Acute myocardial infarctioninfarctionAn acute process of myocardial ischemia with sufficient severity and duration to result in permanent myocardial damage
(ACC/AHA Joint Guideline Statement, 2000)

Definitions (Cont.)Angina pectorisAngina pectoris -- a a clinical syndrome clinical syndrome typically characterized by typically characterized by a deep, poorly localized a deep, poorly localized chest or arm discomfort chest or arm discomfort that is reproducible that is reproducible associated with physical associated with physical exertion or emotional exertion or emotional distress and relieved distress and relieved promptly (i.e., <5 min) promptly (i.e., <5 min) with rest or sublingual with rest or sublingual nitroglycerin nitroglycerin
ACC/AHA Joint Guideline Statement, 2000
Presenter
Presentation Notes
It is predictable in pattern then it is considered “stable”. Has not changed in frequency or severity over a period of time. Does not occur at rest!!!!!!!!!!
DefinitionsUnstable AnginaUnstable Angina
Chest pain that is Chest pain that is different different No elevation of No elevation of biomarkersbiomarkersTransient changes in Transient changes in EKGEKG
Should obtain Should obtain during chest painduring chest pain
Cardiac ischemiaCardiac ischemia
NonNon--ST elevation MI ST elevation MI (NSTEMI)(NSTEMI)
Chest pain that is Chest pain that is differentdifferentElevation of Elevation of biomarkersbiomarkersST depressionST depressionProminent TProminent T--wave wave inversioninversionNO ST segment NO ST segment elevationelevationCardiac ischemiaCardiac ischemia--leading to cardiac leading to cardiac infarctioninfarction
Presenter
Presentation Notes
Unstable Angina: a broad category w/pain that has changed or increased in frequency, duration or severity. Those with ischemic pain that occurs at rest or w/normal activity. Pathophysiology of Angina: may occur when the coronary blood flow is reduced as a result of vessel lumen narrowing by plaque or when perfusion is low as in sudden hypotension. Angina may also be due to increased myocardial workflow as in aortic stenosis, when O2 demands are greatly elevated. Workload is increased by pumping against the tremendous resistance to ejection created by the narrowed aortic valve. Dysrhythmias may also cause discomfort by either increased workload (tachycardia) or coronary perfusion deficit (bradycardia)

http://www.pbs.org/wgbh/nova/heart/troubled.html
Presenter
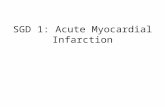
Presentation Notes
Illustrates an artery affected by atherosclerosis. Components of arterial blockage: plaque, fatty material, cholesterol, calcium, blood clot. This is narrowed considerably……
Definitions
ST segment elevation myocardial ST segment elevation myocardial infarction (STEMI)infarction (STEMI) ––an acute process of an acute process of myocardial ischemia with sufficient severity myocardial ischemia with sufficient severity and duration to result in myocardial and duration to result in myocardial necrosis; see ST segment elevationnecrosis; see ST segment elevation
STEMI=AMISTEMI=AMI
(ACC/AHA Joint Guideline Statement, 2000)

Definitions: Older Terms
NonNon--Q wave Q wave myocardial myocardial infarctioninfarction
An AMI that is not An AMI that is not associated with the associated with the evolution of new Q evolution of new Q waves on the ECGwaves on the ECG
Now known as NSTEMINow known as NSTEMI
Q Wave myocardial Q Wave myocardial infarctioninfarction
An AMI that is An AMI that is associated with the associated with the evolution on new Q evolution on new Q waves on the ECGwaves on the ECG
Now known as STEMINow known as STEMI
Presenter
Presentation Notes
Q waves appear as a permanent sign on EKG. It is important to know if a patient has a history of MI with the development of q waves

Q less than 1/4 of the R height, and less than one box wide, is considered normal
http://www.madsci.com/manu/ekg_qwav.htm

Q waves are “significant” if they are greater than 1 box in width (longer than 0.04 msec) OR are larger than 1/4 of the R wave
http://www.madsci.com/manu/ekg_qwav.htm

Causes of ACSClot formationClot formationBuild up of plaque that ruptures causing Build up of plaque that ruptures causing occlusion downstreamocclusion downstreamVentricular hypertrophyVentricular hypertrophyHypoxia due to COHypoxia due to CO22 poisoning or acute poisoning or acute pulmonary disorderspulmonary disordersEmboli to coronary arteriesEmboli to coronary arteriesCoronary artery vasospasmCoronary artery vasospasmCoronary anomaliesCoronary anomaliesCocaine, amphetamines, ephedrineCocaine, amphetamines, ephedrine
Presenter
Presentation Notes
Predominant cause: rupture of atherosclerotic plaque w/subsequent spasm and clot formation Ventricular Hypertrophy-HTN causes increased afterload or resistance, the heart is pumping against a greater force and therefore the left ventricle increases in size; if there is narrowing in the pulmonary vasculature, ie due to pulmonary htn, this will cause an increase in muscle mass on the right side Hypoxia: Carbon dioxide poisoning/acute pulmonary disorders: occur b/c myocardial O2 demands > blood supply CARDIO-ECONOMICS! Emboli to coronary arteries: due to increase in cholesterol or infectious causes Coronary anomalies: can have aneurysms Drugs will be addressed in a minute…..
Presenter
Presentation Notes
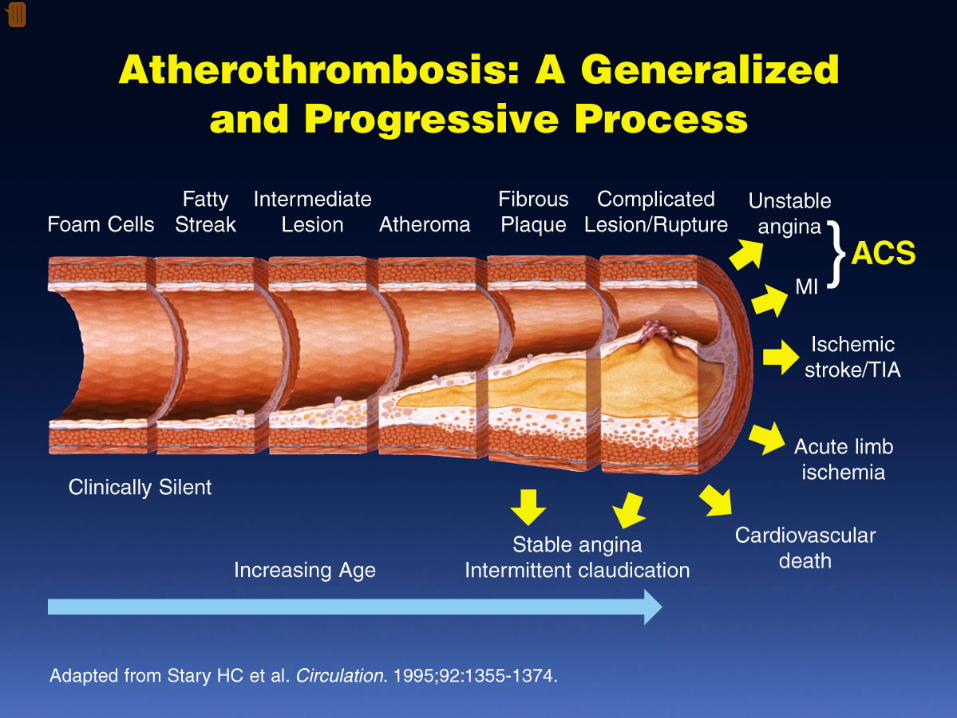
Narrowing of epicardial blood vessels secondary to atheromatous plaque

Presenter
Presentation Notes
Plaque ruptures = exposure of the basement membrane = platelet aggregation = thrombus forms, fibrin accumulates => hemorrhage into the plaque. Medications exist to prevent the platelet plug from forming: IIb/IIIa inhibitors (Intergrillin, Repro)
PathophysiologyNarrowing of epicardial blood vessels secondary to Narrowing of epicardial blood vessels secondary to atheromatous plaqueatheromatous plaquePlaque ruptures = exposure of the basement membrane = Plaque ruptures = exposure of the basement membrane = platelet aggregation = thrombus forms, fibrin accumulates platelet aggregation = thrombus forms, fibrin accumulates => hemorrhage into the plaque. => hemorrhage into the plaque. Varying degrees of vasospasm Varying degrees of vasospasm
Can have partial or complete occlusion of vesselCan have partial or complete occlusion of vesselResults in myocardial ischemiaResults in myocardial ischemia
Total occlusion of vessel for more than 4Total occlusion of vessel for more than 4--6 hrs 6 hrs results in irreversible necrosisresults in irreversible necrosis
Presenter
Presentation Notes
Reperfusion during that 4-6 hr time, can lead to salvage of the myocardium and reduce mortality and morbidity

Illicit Drugs and the HeartCocaine:Cocaine:
Powerful stimulant of the CNS, PNSPowerful stimulant of the CNS, PNSQuickly absorbed Quickly absorbed At risk for cocaineAt risk for cocaine--related deaths even in lowrelated deaths even in low--doses doses ¼¼ of heart attacks in people ages 18of heart attacks in people ages 18--45 are 45 are cocaine relatedcocaine relatedStudy done in Ann Arbor MI in 2003:Study done in Ann Arbor MI in 2003:
Suggested guidelines for ED physicians for Suggested guidelines for ED physicians for treating cocaine related CPtreating cocaine related CP
http://www.med.umich.edu/opm/newspage/2003/cocaineheart.htm
Presenter
Presentation Notes
Causes: Over stimulation of the heart which could result in arrhythmias. Could result in sudden cardiac arrest Could cause narrowing or collapsing of the coronary arteries = MI Long term use could lead to cardiomyopathy Thrombosis Can cause high blood pressure Goal of study published in NEJM was to raise awareness among docs and drug users of the harmful cardiac associated risks even in otherwise healthy young people. One general statistic known prior to the study: ¼ of heart attacks in people ages 18-45 are cocaine related Recent research shows cocaine may cause an abnormal buildup of protein and calcium in heart muscle, can trigger irregular heart rhythms and/or hypertrophy of the muscle Reference for Illicit drug use: http://yourtotalhealth.ivillage.com/illegal-drugs-heart.html?pageNum=2 Authors: David Slotnick, MD, Abdou Elhendy MD PhD FACC FAHA, Lee B Weitzman MD FACC FCCP

Cocaine can cause the blood vessels in the body to constrict, slowing the flow of blood and helping to cause chest pain and even a heart attack.
http://www.med.umich.edu/opm/newspage/2003/cocaineheart.htm

Methamphetamines:Methamphetamines:““Crystal methCrystal meth””Stimulant Stimulant Rapid elevation of Rapid elevation of heart rate and BPheart rate and BP
Heroin:Heroin:Opiate (related to Opiate (related to morphine)morphine)Produces relaxed Produces relaxed effect after initial effect after initial rushrushCauses blood clotsCauses blood clots
Presenter
Presentation Notes
Meth: same etiologies for heart-related issues as cocaine
Ecstasy:Ecstasy:Mild stimulantMild stimulantRaises BPRaises BPReduces pumping Reduces pumping efficiency of the heartefficiency of the heart
Marijuana:Marijuana:Increase HRIncrease HR
Anabolic Steroids:Anabolic Steroids:Can raise LDL levels, Can raise LDL levels, increasing risk of increasing risk of atherosclerosisatherosclerosisHigh BPHigh BPBlood clotsBlood clots
Inhalants:Inhalants:Can lead to tachycardia Can lead to tachycardia ““Sudden sniffing Sudden sniffing deathdeath””
Presenter
Presentation Notes
Ecstasy: body is slow to breakdown the drug. Can raise body temp Marijuana: increases HR which could worsen CAD or high BP. One study has shown that the risk of suffering heart attack increases 5 x in the hour after smoking it. Inhalants: more than 1000 different inhalants are being currently abused. Nail polish to gasoline.
Signs and Symptoms
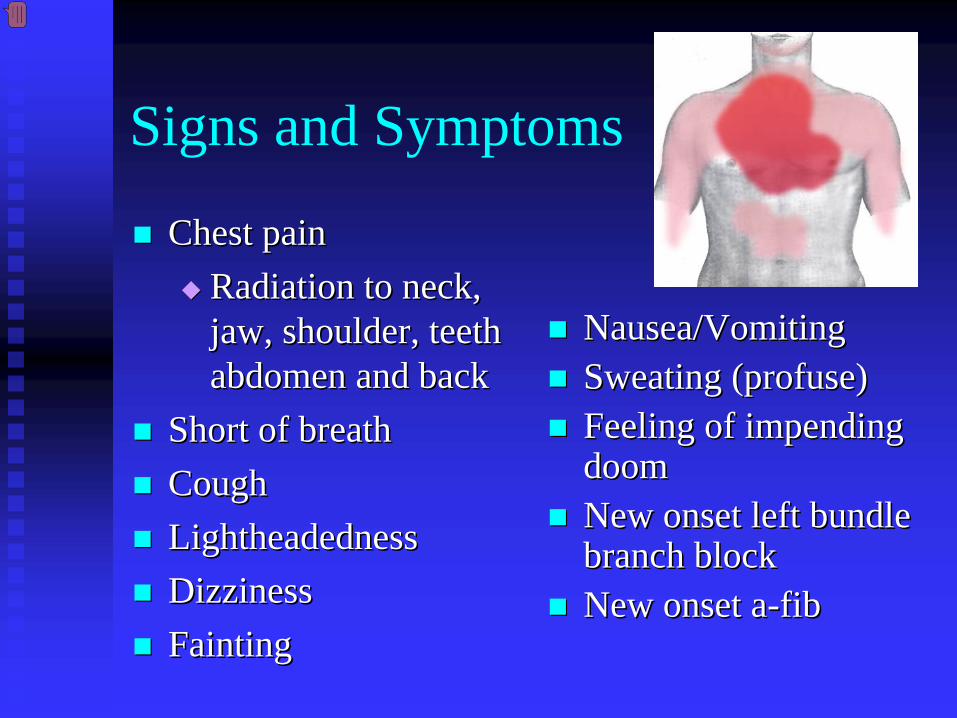
Chest painChest painRadiation to neck, Radiation to neck, jaw, shoulder, teeth jaw, shoulder, teeth abdomen and backabdomen and back
Short of breathShort of breathCoughCoughLightheadednessLightheadednessDizzinessDizzinessFaintingFainting
Nausea/VomitingNausea/VomitingSweating (profuse)Sweating (profuse)Feeling of impending Feeling of impending doomdoomNew onset left bundle New onset left bundle branch blockbranch blockNew onset aNew onset a--fibfib
Presenter
Presentation Notes
Rough diagram of pain zones in myocardial infarction (dark red = most typical area, light red = other possible areas, view of the chest) As with men, women's most common heart attack symptom is chest pain or discomfort. But women are somewhat more likely than men to experience some of the other common symptoms, particularly shortness of breath, nausea/vomiting, and back or jaw pain Patients w/diabetes may have a more subtle presentation as far as pain. May have more fatigue, syncope or weakness. Talk about my OLOL pt: Left hand pain
Assessment of Chest Pain
PP –– precipitating factorsprecipitating factorsQQ –– quality (rate of scale of 1 to 10 with 10 quality (rate of scale of 1 to 10 with 10 being the worst discomfort; this is useful in being the worst discomfort; this is useful in evaluating the effectiveness of nitroglycerin on evaluating the effectiveness of nitroglycerin on the discomfort)the discomfort)RR –– region and radiationregion and radiationSS –– signs/symptoms associated with discomfortsigns/symptoms associated with discomfortTT –– time and response to treatmenttime and response to treatment
Presenter
Presentation Notes
Any patient with chest pain needs a thorough assessment 25 % of MI pts are asymptomatic Differentiate MI chest pain vs angina: VERY CHALLENGING TO DO MI tends to be more intense, > 30 minutes, not relieved w/rest of 3 consecutive NTG

Common Physical Presentation
ObjectiveObjectiveHRHRBPBPRRRRPeripheral perfusionPeripheral perfusionHeart soundsHeart soundsCHFCHF
Clinical PresentationClinical PresentationDiabetics Diabetics WomenWomen
Presenter
Presentation Notes
HR:tachycardia, place on monitor and watch for dysrhythmias may also be bradycardic BP: hyper may precipitate an AMI or reflect elevated catecholamine do to anxiety or pain or hypo indicates ventricular dysfunction due to ischemia. Can indicate large infarct or RV infarct RR elevated to increase oxygen supply PP: cold and clammy due to shunting of blood to major organs Heart Sounds: extra heart sounds MURMUR (if MI secondary to valve issues)

Diagnostic Tests
Initial:Initial:12 lead EKG 12 lead EKG Serial serum cardiac markersSerial serum cardiac markers
CPK, isoenzymes, troponinCPK, isoenzymes, troponinPCXRPCXR
After diagnosis:After diagnosis:Stress testStress testEchocardiogramEchocardiogramCardiac catheterizationCardiac catheterization
Presenter
Presentation Notes
12 lead-all patients with chest pain should have a 12 lead CXR to rule out aortic dissection-will see widened mediastinum; if unable to r/o aortic dssection-get a stat TEE/transthoracic echo or contratst CT or MRI Troponin T rises 3 - 4 hrspeaks 24 hrs Troponin T >0.04 NG/ML - Indicative of MI Creatinine Phosphokinase (CPK) CK-MB rises 4-6 hrspeaks 24 hrsduration 2-3 days Fractionate to CK-MB if CPK increased CK-MB over 5% of total CPK suggests myocardial injury Myoglobin rises 1-2 hrspeaks 4-6 hrsduration 1-2 days If enzymes/ekg are negative-stress test to see if there is an area of reversible ischemia Prep for stress test Echo to look at valve function and ef;valve dysfunction may cause chest pain
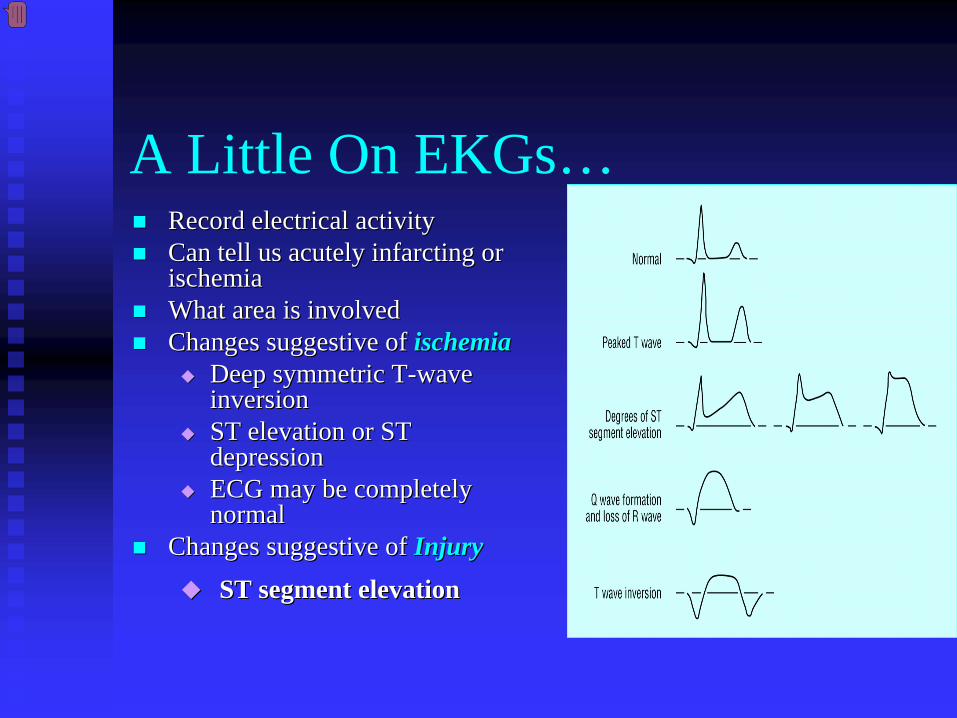
A Little On EKGs…Record electrical activityRecord electrical activityCan tell us acutely infarcting or Can tell us acutely infarcting or ischemiaischemiaWhat area is involvedWhat area is involvedChanges suggestive ofChanges suggestive of ischemiaischemia
Deep symmetric TDeep symmetric T--wave wave inversion inversion ST elevation or ST ST elevation or ST depressiondepressionECG may be completely ECG may be completely normalnormal
Changes suggestive ofChanges suggestive of InjuryInjury
ST segment elevationST segment elevation
Presenter
Presentation Notes
3-10% of MI patients have initial normal EKG 25% of patients with missed MI have misread EKGs Ischemia: Inverted T: especially in V leads. Transient ST depression maybe seen in angina Injury: acute/recent: seen w/ST elevation. Elevation of 1 mm or more in 2 adjacent leads is considered diagnostic

______________
_______
12 Lead EKG (cont.)
Changes suggestive of Changes suggestive of AMI (infarction)AMI (infarction)Q waves (.04sec and 1/3 height of R wave) Q waves (.04sec and 1/3 height of R wave) unless isolated in IIIunless isolated in IIISTST--T elevation (>1mm limb, >2mm precordial)T elevation (>1mm limb, >2mm precordial)ST depression in V1, V2ST depression in V1, V2T wave inversion unless isolated in III or V1T wave inversion unless isolated in III or V1New left bundle branch blockNew left bundle branch block
Presenter
Presentation Notes
These are changes with an acute MI: STEMI (formerly known as Q-wave MI): Usual means more cardiac death, larger in size and can have higher in-hospital mortality When new Q wave present, usually means infarct through entire muscle (remember we need ask history of MIs)
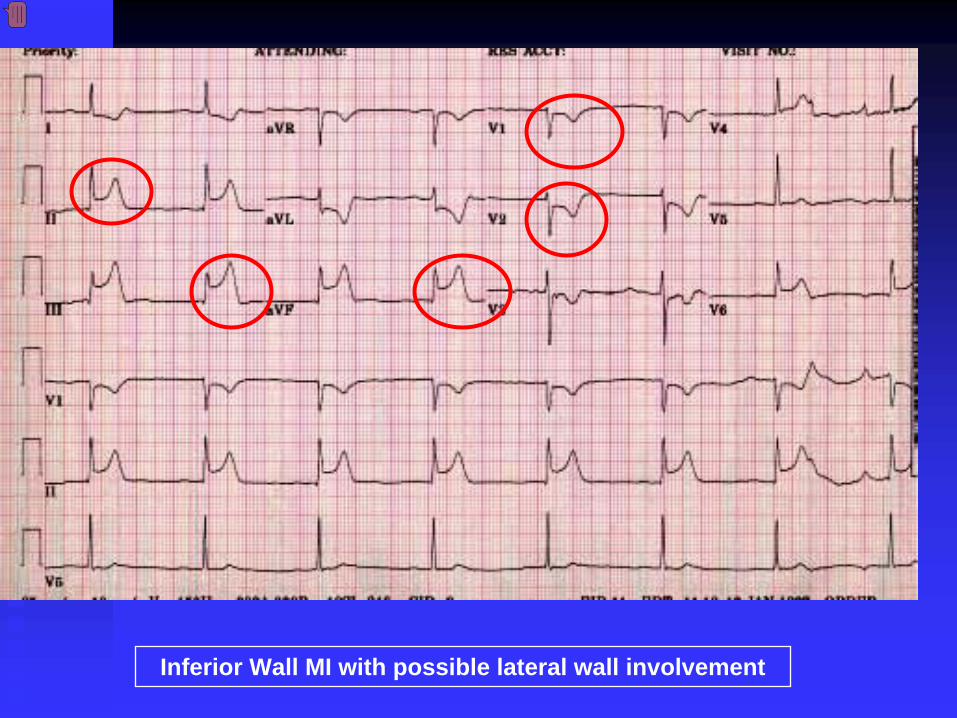
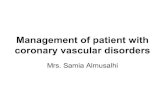
Inferior Wall MI with possible lateral wall involvement
Presenter
Presentation Notes
The EKG shows ST elevation in leads II, III, and aVF suggesting inferior wall myocardial infarction. Reciprocal changes (ST segment depression) may be seen in leads V1 and V2 in inferior wall myocardial infarction as in this patient. In addition there is ST elevation in lead V6 suggesting lateral wall involvement. Lateral infarction produces changes in leads I, avL and V5/6. Key is to have the stat 12 lead read by an MD immediatley

From:http://www.stanfordhospital.com/images/greystone/heartCenter/images/ei_0028.gif

Presenter
Presentation Notes
Looking at EKGs takes time and practice. Knowing the leads and what corresponding coronaries can help to informally diagnosis chest pain pts.

Presenter
Presentation Notes
This should be the decision tree used when someone presents w/chest pain. ACS is the umbrella term and we must decide down which arm the person fits in: Angina vs MI. Treatment choices depend on it.

ACC/AHA GuidelinesPatients w/suspected ACS Patients w/suspected ACS need evaluation ASAPneed evaluation ASAPCP pts transported by CP pts transported by ambulance:ambulance:
1/3 MI1/3 MI1/3 UA1/3 UA1/3 non1/3 non--cardiaccardiac1.5 % of these pts 1.5 % of these pts developed developed cardiopulmonary arrest cardiopulmonary arrest prior to arrival to the prior to arrival to the hospital hospital
Presenter
Presentation Notes
Mortality and morbity from ACS can be reduced significantly if pts and/or bystanders recognize symptoms early, activate EMS Should always be transported to hospital via ambulance 1 in 300 pts w/chest pain transported to ED via private vehicle suffered cardiac arrest en route.
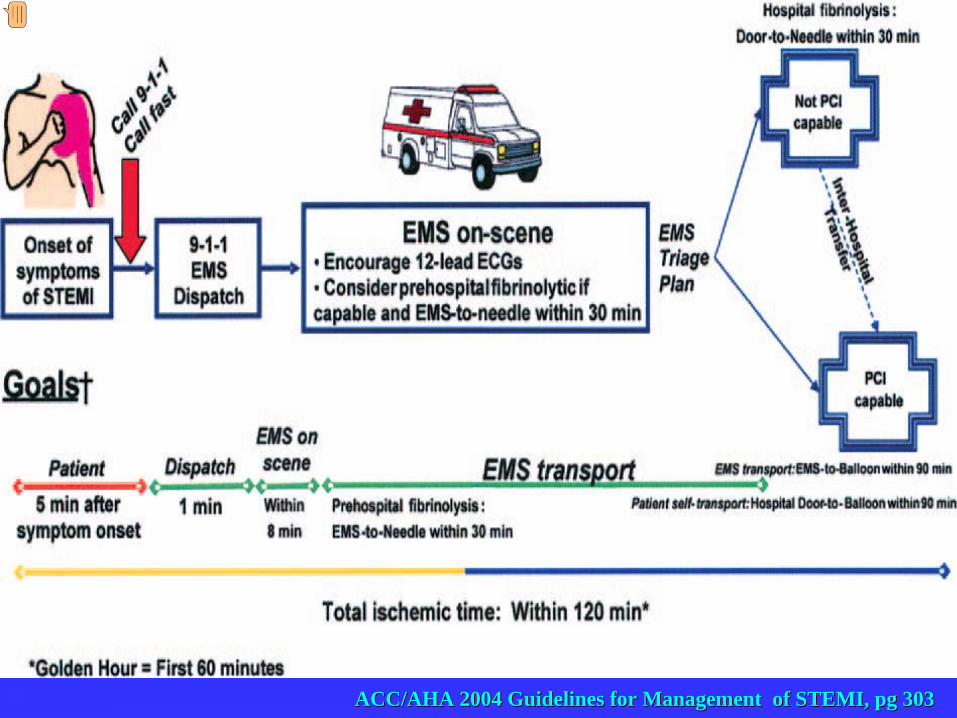
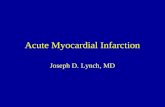
ACC/AHA 2004 Guidelines for Management of STEMI, pg 303ACC/AHA 2004 Guidelines for Management of STEMI, pg 303
Presenter
Presentation Notes
Every community should have written protocols to guide EMS personal. Early administration of reperfusion therapy improves survival in patients w/STEMI. Re-established blood flow. Options: fibrinolytics and primary percutaneous coronary intervention (PCI) http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.107.188209 ACC/AHA 2004 Guidelines for Management of STEMI, 2007 Pg 303 Figure 1. Options for Transportation of STEMI Patients and Initial Reperfusion Treatment Goals Reperfusion in patients with STEMI can be accomplished by pharmacological (fibrinolysis) or catheter-based (primary PCI) approaches. The overarching goal is to keep total ischemic time within 120 minutes (ideally within 60 minutes) from symptom onset to initiation of reperfusion treatment. Within this context, the following are goals for the medical system* based on the mode of patient transportation and the capabilities of the receiving hospital: Medical System Goals: EMS Transport (Recommended): • If EMS has fibrinolytic capability and the patient qualifies for therapy, prehospital fibrinolysis should be started within 30 minutes of arrival of EMS on the scene. • If EMS is not capable of administering prehospital fibrinolysis and the patient is transported to a non–PCI-capable hospital, the door-to-needle time should be within 30 minutes for patients for whom fibrinolysis is indicated. • If EMS is not capable of administering prehospital fibrinolysis and the patient is transported to a PCI-capable hospital, the EMS arrival-to-balloon time should be within 90 minutes. • If EMS takes the patient to a non–PCI-capable hospital, it is appropriate to consider emergency interhospital transfer of the patient to a PCI-capable hospital for mechanical revascularization if X There is a contraindication to fibrinolysis. X PCI can be initiated promptly within 90 minutes from EMS arrival-to-balloon time at the PCI-capable hospital.† X Fibrinolysis is administered and is unsuccessful (i.e., “rescue PCI”).

Reperfusion Therapy
Thrombolytic therapyThrombolytic therapyRestore artery patency after infarctRestore artery patency after infarctIndications:Indications:
Chest pain 12 hours or lessChest pain 12 hours or lessST segment elevation (>0.1mV) in two ST segment elevation (>0.1mV) in two contiguous precordial leads or at least 2 contiguous precordial leads or at least 2 Adjacent limb leads)Adjacent limb leads)New BBB and history suggestive of AMINew BBB and history suggestive of AMIPhysiologic age < 75 years Physiologic age < 75 years
(AHA 2004)(AHA 2004)
Presenter
Presentation Notes
Prehospital fibrinolysis is reasonable in the setting where MD is present in the ambulance or transport time is longer than 60 minutes in high volume EMS system (25,000 runs/year) Ideally initiation of fibrinolytic therapy should be <30 minutes;efficacy diminishes with the passage of time and should be given within the first 2 hours. Little benefit of the therapy if given after 12hrs Recent research shows early access to catheterization/stenting is slightly superior to thrombolytics. Thrombolytics are used heavily in institutions without an interventional lab and when transfer to such a facility would take a prolonged period of time
Reperfusion Therapy (Cont.)
Thrombolytic therapyThrombolytic therapyAbsolute ContraindicationsAbsolute Contraindications
Previous hemorrhagic stroke at any timePrevious hemorrhagic stroke at any timeKnown structural cerebral vascular lesion Known structural cerebral vascular lesion (AVM)(AVM)Ischemic stroke within 3 months (exception Ischemic stroke within 3 months (exception acute stroke within 3 hours)acute stroke within 3 hours)Significant closed head/facial trauma within Significant closed head/facial trauma within last 3 monthslast 3 monthsSuspected aortic dissectionSuspected aortic dissectionActive internal bleeding (excluding menses)Active internal bleeding (excluding menses)

Reperfusion Therapy (Cont.)
Thrombolytic TherapyThrombolytic TherapyRelative ContraindicationsRelative Contraindications
Chronic severe, poorly controlled HTNChronic severe, poorly controlled HTNUncontrolled HTN on presentation (SPB >180 or Uncontrolled HTN on presentation (SPB >180 or DBP>110)DBP>110)Ischemic stoke >3 months, dementia or known Ischemic stoke >3 months, dementia or known intercranial pathologyintercranial pathologyTraumatic or prolonged CPRTraumatic or prolonged CPRMajor surgery (< 3 weeks)Major surgery (< 3 weeks)Recent (2Recent (2--4 weeks internal bleeding4 weeks internal bleedingPregnancyPregnancyCurrent use of anticoagulantsCurrent use of anticoagulantsNon compressible vascular puncturesNon compressible vascular punctures

Reperfusion Therapy (Cont.)Primary PCIPrimary PCI
IndicationsIndicationsWithin 12 hours of symptom onsetWithin 12 hours of symptom onsetWith ST elevation or LBBB who develop shock within 36 With ST elevation or LBBB who develop shock within 36 hours of MI and are suitablehours of MI and are suitableSevere CHF and/or pulmonary edema and onset of symptoms Severe CHF and/or pulmonary edema and onset of symptoms within 12 hourswithin 12 hoursOnset of symptoms within the prior 12 Onset of symptoms within the prior 12 --24 hours and 1 or more 24 hours and 1 or more of the following:of the following:
Severe CHFSevere CHFHemodynamic or electrical instabilityHemodynamic or electrical instabilityPersistent ischemic symptomsPersistent ischemic symptoms
Not recommended in asymptomatic patients > 12 hours Not recommended in asymptomatic patients > 12 hours after onset of STEMI if the patient is hemodynamically after onset of STEMI if the patient is hemodynamically & electrically stable& electrically stable
Presenter
Presentation Notes
Animal models show a correlation b/w duration of coronary artery occlusion and extent of necrosis. Myocardial cell death begins as early as 20 mins after coronary artery occlusion and is usually complete w/in 6hrs Greatest benefit for PCI is w/in the first 2-3 hrs after the onset of symptoms. Time of highest myocardial salvage For that reason, ACC/AHA guidelines are looking at door to balloon times to be less than 90 minutes. When treatment was started w/in 90min after arrival, in-hospital morality was 3%. Increase to 4.2%, 5.7% and 7.4% when delays were 91-120 mins, 121-150 mins and more than 15 mins. Now nationally reported as a quality indicator for hospital performance. Measured by Health Quality Alliance Rescue PCI-PCI within 12 hours after failed fibrinolysis for patients with continuing or recurrent myocardial ishemai “Time to Treatment in Primary Percutaneous Coronary Intervention” Brahmajee K Nallmouthu MD et al. New England Journal of Medicine. October 18,2007; 357: 1631-1638.

Reperfusion Therapy (Cont.)
Primary PCIPrimary PCIAngioplasty Angioplasty Stent placementStent placementArthrectomyArthrectomyAngiojetAngiojetRotabladeRotablade
Presenter
Presentation Notes
PTCA (Percutaneous Translumal cardiac angiography): Includes a whole host of interventions including angioplasty, stenting, arthrectomy, angiojet or laser treatment. One or more may be necessary If more than one coronary is stenosed, the vessel causing the MI will have intervention. Pt then may be scheduled for further intervention at a latter date. This is called staging. When to intervene on other vessels is cardiology dependent. Sometimes more than one vessel will receive intervention. Patient is then at higher risk if the stent fails. Stenting of the main can on occasion be performed. CABG is indicated in patient with >2 vessels, diabetes or other comorbidities, inability to advance wires or perform intervention. It is best is CABG is done under a controlled situation.


Additional Therapies
IABP TherapyIABP TherapyCABGCABGLVAD/LVAD/BiVADBiVADTransplantTransplant
Presenter
Presentation Notes
IABP therapy is part of ACC/AHA guidelines for care of patient w/STEMI. Other modalities are options depending on the extent of myocardial damage done and long-term prognosis for the patient

Complications Post MIArrhythmiasArrhythmiasCardiogenic shockCardiogenic shockCongestive heart failureCongestive heart failureAcute mechanical changesAcute mechanical changesPericarditisPericarditisThromboemboliThromboemboliCardiac tamponadeCardiac tamponadeVentricular aneurysmVentricular aneurysm
Presenter
Presentation Notes
Arrhythmias- Occurs in 90% of patients. Not the MI that causes death by the arrythmia and this risk keeps them in hospital for 3-5 days. Caused by ischemia, hypoxia, autonomic nervous system imbalances, lactic acidosis, electrolyte imbalance, alteration in the conduction pathway. Damage to the areas of the SA/AV node. The heart is irritable for the first 24 hr post MI. Not unusually to v-tach in the first 24 hours. After 24 hours, if patient continues to have runs of vtach will be treated with either antiarrhythmics or AICD. If patient had v-fib arrest as presenting sign of MI they may also receive AICD. Also high risk patients Patients who have persistent bradycardia may need pacer therapy. May insert a pacer so patient can tolerate drug therapy Cardiogenic Shock: Occurs when about 40% or more of the left ventricular myocardium is infarcted. Supportive therapy with Dopamine/Dobutamine and IABP. LVAD and transplant if serious enough CHF: More common with MI to the left side of the heart. Treatment: oxygen, morphine, Lasix. 2Decho checked post MI. A follow up 2d echo is scheduled as an outpatient to look for improvement. Acute mechanical changes: rupture of papillary muscles, ruptured of the free wall of the infarcted ventricle, septal rupture Pericarditis: (Inflammation of the pericardium) Hear a rub, associated w/ anterior chest pain that worsens with respiratory effort. See widespread ST segment elevation. TX: NSAIDS Thromboemboi: “Shower of clots”-can cause CVA if travel to the brain. Can travel to fingers/toes and cause necrosis Cardiac Tamponade: As a result of manipulation of the coronary vessels and the anticoagulants. Can be slow Listen for muffled heart sounds and chest pain Ventricular Aneurysm: May cause free rupture of the ventricular wall,-late occurance, see on echo, tx with surgery

Patient Education
Risk Factor Risk Factor ModificationModificationTreatment of AnginaTreatment of AnginaMedication RegimeMedication RegimeNutritionNutritionResuming Activities Resuming Activities of Daily Livingof Daily LivingCardiac RehabCardiac RehabResourcesResources
Presenter
Presentation Notes
Patient Education is key to prevention of a secondary event. Initially, most patients are grateful to be alive and are very agreeable to change. As they leave the hospital and go home, they slip back into old habits and forget much of what is taught. They need reinforcement. Some are angry at their illness and not ready for change

ACC/AHA 2007 Guidelines pg. e159
Presenter
Presentation Notes
Again, important to remember the decision tree for ACS. Time is Muscle!!! ACC/AHA 2007 Guidelines for UA/NSTEMI (http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.107.181940) Prehospital EMS providers should administer 162 to 325 mg of ASA (chewed) to chest pain patients suspected of having ACS unless contraindicated or already taken by the patient. Although some trials have used enteric-coated ASA for initial dosing, more rapid buccal absorption occurs with non–enteric-coated formulations. (Level of Evidence: C) 5. Health care providers should instruct patients with suspected ACS for whom nitroglycerin [NTG] has been prescribed previously to take not more than 1 dose of NTG sublingually in response to chest discomfort/pain. If chest discomfort/pain is unimproved or is worsening 5 min after 1 NTG dose has been taken, it is recommended that the patient or family member/friend/caregiver call 9-1-1 immediately to access EMS before taking additional NTG. In patients with chronic stable angina, if symptoms are significantly improved by 1 dose of NTG, it is appropriate to instruct the patient or family member/friend/caregiver to repeat NTG every 5 min for a maximum of 3 doses and call 9-1-1 if symptoms have not resolved completely. (Level of Evidence: C) 6. Patients with a suspected ACS with chest discomfort or other ischemic symptoms at rest for greater than 20 min, hemodynamic instability, or recent syncope or presyncope should be referred immediately to an ED. Other patients with suspected ACS who are experiencing less severe symptoms and who have none of the above high-risk features, including those who respond to an NTG dose, may be seen initially in an ED or an outpatient facility able to provide an acute evaluation. (Level of Evidence: C) CLASS IIa 1. It is reasonable for health care providers and 9-1-1 dispatchers to advise patients without a history of ASA allergy who have symptoms of ACS to chew ASA (162 to 325 mg) while awaiting arrival of prehospital EMS providers. Although some trials have used entericcoated ASA for initial dosing, more rapid buccal absorption occurs with non–enteric-coated formulations. (Level of Evidence: B) 2. It is reasonable for health care providers and 9-1-1 dispatchers to advise patients who tolerate NTG to repeat NTG every 5 min for a maximum of 3 doses while awaiting ambulance arrival. (Level of Evidence: C) 3. It is reasonable that all prehospital EMS providers perform and evaluate 12-lead ECGs in the field (if available) on chest pain patients suspected of ACS to assist in triage decisions. Electrocardiographs with validated computer-generated interpretation algorithms are recommended for this purpose. (Level of Evidence: B) 4. If the 12-lead ECG shows evidence of acute injury or ischemia, it is reasonable that prehospital ACLS providers relay the ECG to a predetermined medical control facility and/or receiving hospit

Questions????
BibliographyBaird, Marianne et al. Baird, Marianne et al. ““Manual of Critical Care Manual of Critical Care Nursing: Nursing Interventions and Collaborative Nursing: Nursing Interventions and Collaborative ManagementManagement””.. Elsevier Mosby. 5Elsevier Mosby. 5thth Edition. Edition. 2005. pp 2052005. pp 205--225.225.NallamothuNallamothu, , BrahmajeeBrahmajee et al. et al. ““Time to Treatment Time to Treatment in Primary Percutaneous Coronary Interventionin Primary Percutaneous Coronary Intervention””..New England Journal of Medicine. 2007; New England Journal of Medicine. 2007; 357:1631357:1631--1638.1638.UrdenUrden, Linda D. et al. , Linda D. et al. ““ThelanThelan’’ss Critical Care Critical Care Nursing: Diagnosis and ManagementNursing: Diagnosis and Management””. Elsevier . Elsevier Mosby.Mosby. 55thth Edition. 2006. pp433Edition. 2006. pp433--459.459.
BibliographyFenton, Drew E. et al. Fenton, Drew E. et al. ““Myocardial InfarctionMyocardial Infarction””. Sept 10, 2007. . Sept 10, 2007. www.emedicine.com/EMERG/topic327.htmwww.emedicine.com/EMERG/topic327.htmACC/AHA Guidelines for the Management of Patients with Unstable ACC/AHA Guidelines for the Management of Patients with Unstable Angina/Non STAngina/Non ST--Elevation Myocardial Infarction. Revise to the 2002 Elevation Myocardial Infarction. Revise to the 2002 Guidelines. 2007. Guidelines. 2007. http://circ.ahajournals.orghttp://circ.ahajournals.orgACC/AHA Guidelines for the Management of Patients with STACC/AHA Guidelines for the Management of Patients with ST--
Elevation Myocardial Infarction. Revise to the 2004 Guidelines.Elevation Myocardial Infarction. Revise to the 2004 Guidelines.2007. 2007. http://circ.ahajournals.orghttp://circ.ahajournals.org““This is our heart on drugs: study may help ER doctors identify aThis is our heart on drugs: study may help ER doctors identify and nd treat chest pain caused by cocainetreat chest pain caused by cocaine””. . http://www.med.umich.edu/opm/newspage/2003/cocaineheart.htmhttp://www.med.umich.edu/opm/newspage/2003/cocaineheart.htm““Illicit Drugs and the HeartIllicit Drugs and the Heart”” SlotnickSlotnick, David et al. , David et al. http://yourtotalhealth.ivillage.com/illegalhttp://yourtotalhealth.ivillage.com/illegal--drugsdrugs--heart.html?pageNumheart.html?pageNum=2=2